
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health , 07 August 2024
Sec. Children and Health
Volume 12 - 2024 | https://doi.org/10.3389/fpubh.2024.1420943
 Haibo Zhou1,2,3†
Haibo Zhou1,2,3† Yi Yang3†
Yi Yang3† Peihan Chi1,2Haoyue Cheng1,2
Peihan Chi1,2Haoyue Cheng1,2 Xialidan Alifu1,2Yiwen Qiu1,2Ye Huang1,2
Xialidan Alifu1,2Yiwen Qiu1,2Ye Huang1,2 Libi Zhang1,2Diliyaer Ainiwan1,2
Libi Zhang1,2Diliyaer Ainiwan1,2 Yan Zhuang1,2
Yan Zhuang1,2 Hui Liu4
Hui Liu4 Zhi Chen5*
Zhi Chen5* Yunxian Yu1,2*
Yunxian Yu1,2*Objective: Few comparisons have been implemented between different prenatal care utilization indices and their effects on adverse outcomes. This study investigated the appropriateness of Chinese antenatal care (ANC) regulations and compared Chinese and American adequacy of prenatal care utilization (APNCU) scores.
Methods: From 2010 to 2022, the medical records of 60,114 pregnant women were collected from the electronic medical record system (EMRS) in Zhoushan, China. ANC utilization was measured using the APNCU score and five times antenatal care (ANC5). Birth weight outcomes, including small for gestational age (SGA) and large for gestational age (LGA), low birth weight (LBW), macrosomia, birth weight, and preterm birth (PTB), were utilized as outcomes. Multinomial, linear, and logistic regression were used to analyze the association of ANC5 and APNCU with outcomes, respectively. Crossover analysis was implemented to compare the interaction between ANC5 and APNCU on the outcomes.
Results: Women who received inadequate prenatal care had increased odds for PTB (ANC5: odds ratio (OR) = 1.12, 95% confidence interval (95%CI) = 1.03–1.21; APNCU: OR = 1.18, 95%CI: 1.07–1.29), delivering SGA infants (ANC5: OR = 1.13, 95%CI = 1.07–1.21; APNCU: OR = 1.11, 95%CI = 1.03–1.20). Crossover analysis revealed that inadequate prenatal care in APNCU only was significantly associated with an increased risk of PTB (OR = 1.48, 95%CI: 1.26–1.73).
Conclusion: Women with inadequate prenatal care in ANC5 or APNCU were more likely to suffer from adverse birth outcomes, including PTB, birth weight loss, SGA, and LBW. It indicated that adequate prenatal care is necessary for pregnant women. However, there were interactions between ANC5 and APNCU on PTB, with inadequate prenatal care use by APNCU showing the highest risk of PTB. This indicates that APNCU would be a better tool for evaluating prenatal care use.
Prenatal care is a common health intervention that may lower the incidence of perinatal morbidity and death by treating medical disorders, detecting and minimizing possible hazards, and assisting women in avoiding unhealthy life behaviors that contribute to adverse outcomes (1), such as small for gestational age (SGA) (1), preterm birth (PTB) (2), and low birth weight (LBW) (3). The effect of these outcomes was evaluated to be associated with distress syndrome, infections, and developmental delays, which can extend into adulthood, leading to chronic conditions such as cardiovascular disease and diabetes (4).
Measurements of prenatal care have evolved from pure prenatal care frequency (5) to indices. The first prenatal care index was proposed by Kessner (6) and is called the Kessner Index. After that, many other indices were developed. These indices have been employed in studies assessing prenatal care and birth outcomes to evaluate the appropriateness of prenatal care (7). The Adequacy of Prenatal Care Utilization (APNCU) score is an improvement on the Institute of Medicine’s Kessner Index, which incorporates the trimester of prenatal care commencement and the number of prenatal visits (8). The APNCU index is commonly used for accurate and complete prenatal care measurement (9). Previous studies have shown that APNCU was associated with SGA (1), PTB (2), and LBW (3).
However, the requirements for prenatal care visits vary in different countries (10). In Canada, the Society of Obstetricians and Gynaecologists of Canada (SOGC) mentions that women in developed countries typically have 7 to 11 regular prenatal visits throughout each pregnancy (11). The World Health Organization recommended that women complete at least four times of prenatal care in 2002 and adjusted the frequency to eight times in 2016 (12). In China, although most hospitals adopt suggestions from the American College of Obstetricians and Gynecologists (ACOG), which requires women to attend antenatal care (ANC) once in different intervals in three periods of gestation, the government document National Basic Public Health Service Standard (NBPHS) requires that pregnant women pay at least one visit during five periods in pregnancy. The five corresponding gestational age periods were ≤ 13th, 16 ~ 20th week, 21 ~ 24th, 28 ~ 36th, and 37 ~ 40th week of gestation. For convenience, this five-time-specific ANC was modified to ANC5, which defines pregnant women who obtain at least five times ANC during pregnancy, regardless of the timing period, as having received adequate prenatal care (13, 14). Therefore, it is necessary to estimate the association between ANC5 and adverse birth outcomes.
Furthermore, to comprehensively assess the impact of prenatal care, it is crucial to consider various sociodemographic and medical factors. This study incorporates variables such as age, education level (15), BMI (16), gestational age at the first visit, maternal high-risk pregnancy status, smoking and alcohol consumption during or before pregnancy (17), and parity, which has been reported to be related to maternal adverse outcomes (18). Specifically, high-risk pregnancy (19) status is a critical factor as it may confound the association between prenatal care utilization and birth outcomes. Women with high-risk pregnancies often require more intensive prenatal care, and their adverse outcomes might reflect their underlying risk rather than the adequacy of care received. These variables are selected based on the Andersen Behavioral Model (20), which provides a framework for understanding health service utilization. According to this model, health behaviors and outcomes are influenced by predisposing factors (e.g., education level, pre-pregnancy behaviors, and parity), enabling factors (e.g., BMI and gestational age of the first visit), and need factors (e.g., high-risk pregnancy status). By incorporating these variables, the study aims to provide a more thorough assessment of prenatal care adequacy and its impact on birth outcomes.
In addition, a few studies have been implemented to compare different indices, such as Gindex and Kessner index (21, 22) on different birth outcomes. However, few studies have evaluated which ANC utilization indices, such as APNCU and ANC5, are more suitable for clinical practice. This could be due to the complexity of accurately measuring prenatal care adequacy and the variations in healthcare systems and guidelines across different regions. Additionally, the lack of standardized criteria for evaluating prenatal care indices and the challenges in collecting comprehensive and consistent data may contribute to the limited number of comparative studies. It also needs to be validated whether the Chinese population should use the ACOG prenatal care program or if there is a better way to evaluate prenatal care utilization adequacy. Therefore, this study also aims to compare the association between different prenatal care utilization indices and adverse birth outcomes.
The data were retrieved from the electronic medical record system (EMRS) in Zhoushan City, Zhejiang Province, China. The EMRS, a municipal system built in Zhoushan in 2001, had prenatal health and birth registration data. The EMRS only included the data from Zhoushan Maternal and Child Care Hospital from 2001 to 2009. Starting in 2010, the EMRS covered maternal and pediatric medical information from the whole city.
The prenatal health dataset was used to extract maternal data about sociodemographic information (such as maternal age, educational attainment, parity, last menstrual period, and follow-up date) and health-related features (such as maternal height, weight, systolic and diastolic blood pressure during pregnancy, and liver and kidney diseases). Birth data (such as neonatal gender, birth weight, and gestational age) was also collected. Both databases were connected by a unique personal identification number. The study protocol was approved by the institutional review board of Zhejiang University School of Medicine.
Considering the representation of the population, medical records that included all the people in Zhoushan City after 2010 were included. In this investigation, women who visited hospitals between 2010 and 2022 were considered. Age between 18 and 45 years, first visit after the year 2010, and gestational age at delivery between 28 and 42 weeks were the inclusion criteria for this study. The women who met any one of the following conditions were excluded: (1) multiple births and (2) birth weights of more than 5,000 g or less than 1,000 g. The detailed data flow is presented in Supplementary Figure S1.
A prenatal care visit is a medical appointment that pregnant women attend during pregnancy to receive healthcare services from medical professionals. If many visits were identified at the exact location on the same day, one visit would be recorded. Prenatal care usage was evaluated by APNCU and ANC5. Original APNCU is divided into four categories and calculated based on two components: the month prenatal care began and the number of visits from the first prenatal care to delivery (8). Inadequate ANC utilization is defined as beginning prenatal care after the fourth month of pregnancy or obtaining less than 50% of the needed prenatal care visits based on the ACOG schedule (0–28th week: 1 visit/4 weeks; 29–36th week: 1 visit/2 weeks; 37–42th week: 1 visit/week). Intermediate ANC utilization is initiated before or equal to the fourth month of pregnancy, with 50–79% of routine visits. Adequate ANC utilization is undertaken by the fourth month of pregnancy, with 80–109% of planned visits. Adequate plus ANC utilization is initiated by the fourth month of pregnancy with 110% or more of expected visits (8).
ANC5 was divided into adequate or inadequate. Adequate group means that women obtained at least one prenatal care visit in each time period: ≤13th, 14 ~ 20th, 21 ~ 27th, 28 ~ 36th, and ≥ 37th week of gestation recommended by NBPHS, respectively. Inadequate means that women only completed prenatal care visits in no more than four different periods mentioned above. Additionally, considering that some women might miss the prenatal care visit after the 37th week due to premature delivery from the 29th to the 37th week, these women would be categorized into adequate groups if they completed prenatal care visits in four different periods. Women delivering at the 28th week would also be categorized into adequate groups if they completed prenatal care visits in three different periods.
To compare the association between APNCU and ANC5, APNCU was transformed into a binary variable: adequate plus and adequate were merged into adequate, while intermediate and inadequate were merged into inadequate. Additionally, prenatal care frequency was included and divided into quartiles to facilitate the comparison of their differences. For ease of reading, the frequency in parentheses indicates the range of values within each quartile category: Q1 (1 ~) indicates a frequency from 1 to 10, Q2 (11 ~) indicates a frequency from 11 to 12, Q3 (13 ~) indicates a frequency from 13 to 14, and Q4 (14 ~) indicates a frequency from 14 onwards.
The primary outcomes are PTB, SGA, and LGA. PTB was defined as babies born before 37 weeks of gestation. The birth weight with less than the 10th or greater than the 90th percentile for gestational age was defined as SGA and LGA, respectively. An infant with a birth weight between the 10th and 90th percentile was defined as appropriate for gestational age (AGA). Secondary outcomes are birth weight (g), LBW, and fetal macrosomia (FM). LBW and FM were determined if the birth weight was less than 2,500 g or greater than 4,000 g, respectively.
The potential confounding factors included maternal educational level, risk of pregnancy (low and high), body mass index (BMI), gestational age of the first visit, gestational age of delivery, calendar year of the first visit, alcohol drinking (yes and no) or cigarette smoking (yes and no) before or during pregnancy, and parity (primipara and multipara). Educational level was separated into three tiers (middle school and less, high school and college, and more). Risk pregnancy includes, but is not limited to, situations before or during pregnancy: obstetric history, such as history of cesarean delivery, history of uterine rupture, and history of multiple induced abortions; pregnancy complications, such as excessive amniotic fluid, premature rupture of membranes, fetal growth restriction, and severe pre-eclampsia; and maternal medical conditions, such as epilepsy requiring pharmacological control, unstable thyroid disease, severe anemia, and pulmonary hypertension. It was determined by health professionals. A detailed high risk is defined by the items in Supplementary Table S1. It was divided into high-risk and low-risk groups. High risk means if any of the conditions in Supplementary Table S1 occurred during pregnancy and low risk means none of the situations occurred. The BMI was calculated by weight in kilograms divided by the square of standing height in meters and then categorized into four groups (underweight: <18.5 kg/m2; normal weight: 18.5 ~ 23.9 kg/m2; overweight: 24 ~ 27.9 kg/m2; and obesity: ≥28 kg/m2). The gestational week that women first visited the hospital during the current pregnancy to receive prenatal care was defined as the gestational age of the first visit. The gestational week was defined by the birth date subtracted from the first day of the last normal menstrual cycle and/or the date established by an ultrasound.
Since the time for women to participate in ANC is different, some women with low ANC utilization may start the physical examination in the third trimester of pregnancy. Therefore, women with pre-pregnancy BMI were utilized. We compare the association between prenatal care utilization and adverse outcomes mentioned above with pre-pregnancy BMI and BMI at the first visit, respectively. Considering the sample size reduced drastically, we divided the prenatal care frequency into quartiles within the subgroup analysis. Furthermore, risk pregnancy was believed to be a potential leading bias in the analysis. Therefore, a stratification analysis by risk pregnancy was implemented.
The random forest was used to impute missing values for variables with fewer than 10% of missing data. Continuous variables were presented as means and standard deviations (mean ± SD). For categorical data, frequencies and percentages (%) were presented. The analysis of variance (ANOVA) and chi-square test were used to compare continuous and categorical data, respectively. The association between prenatal care utilization and adverse pregnancy outcomes was visualized through restricted cubic spline (RCS). Due to the non-linear relationship between prenatal care utilization and adverse pregnancy outcomes, the total number of prenatal care visits was treated as quartile (Q1 ~ Q4). Multiple linear regression was used to analyze the association between prenatal care utilization (including the total number of prenatal care visits, APNCU, and ANC5) and birth weight (continuous variable). The model was adjusted for the following potential confounders: maternal age, educational level, BMI, risk diagnosis, parity, calendar year of the first visit, alcohol or cigarette consumption, gestational age of the first visit, and gestational age of delivery. Multiple logistic regression was used to assess the association between prenatal care utilization and PTB, after adjustment for covariates mentioned above, except the gestational age of delivery. Multinomial logistic regression was used to determine the relationship between prenatal care utilization and categorical outcomes of birth weight (SGA, normal, and LGA; LBW, normal, and macrosomia). The crossover analysis was used to explore the interaction between ANC5 and APNCU on outcomes. Covariates were the same as those in the previous models of corresponding outcomes. All statistical analyses were performed using R (version 4.3.1). The statistical significance was considered as a p-value of <0.05.
Table 1 presents the distribution of maternal characteristics between prenatal care utilization groups. This study included 60,114 pregnant women. The average age and gestational age of delivery were 28.4 ± 4.22 years and 39.09 ± 1.49 weeks, respectively. Most women took their first visit of prenatal care at 12.16 ± 3.33 weeks of gestation. More than half of women received college or higher education (55.2%). Almost 18% of pregnant women were overweight or obese. Most women experienced high-risk pregnancies (60.1%) and primipara (68.7%). Overall, the number of newborns was similar in each calendar year. A few women consumed alcohol or cigarettes (1.3%) before or during pregnancy. Most of the women received adequate prenatal care, despite being estimated by ANC5 (69.6%) or APNCU (82.1%).
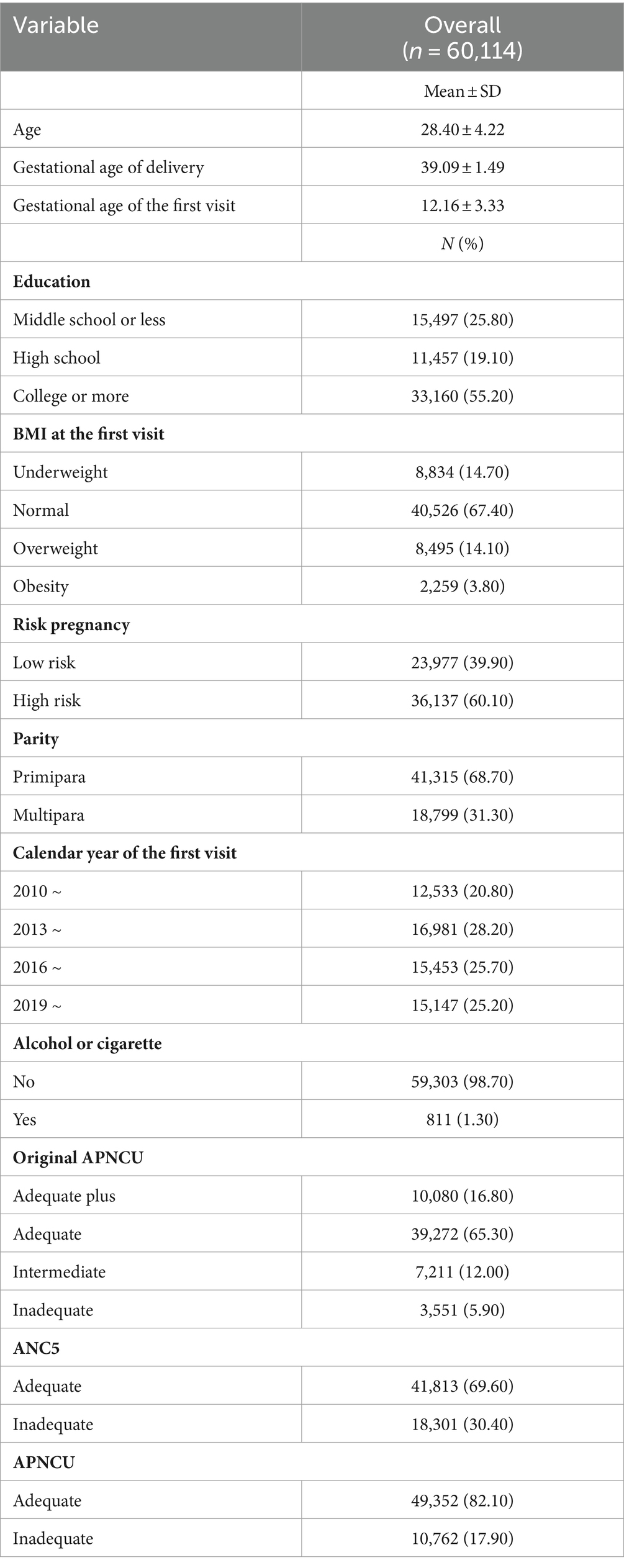
Table 1. Distribution of socio-economic characteristics.
Table 2 shows the association between prenatal care utilization and PTB. Inadequate ANC5 (OR = 1.12, 95%CI:1.03–1.21) and APNCU (OR = 1.18, 95%CI: 1.07–1.29) were associated with PTB. Additionally, it could be inferred that an increase in prenatal care was negatively related to PTB (Q4: OR = 0.40, 95%CI: 0.36–0.45).
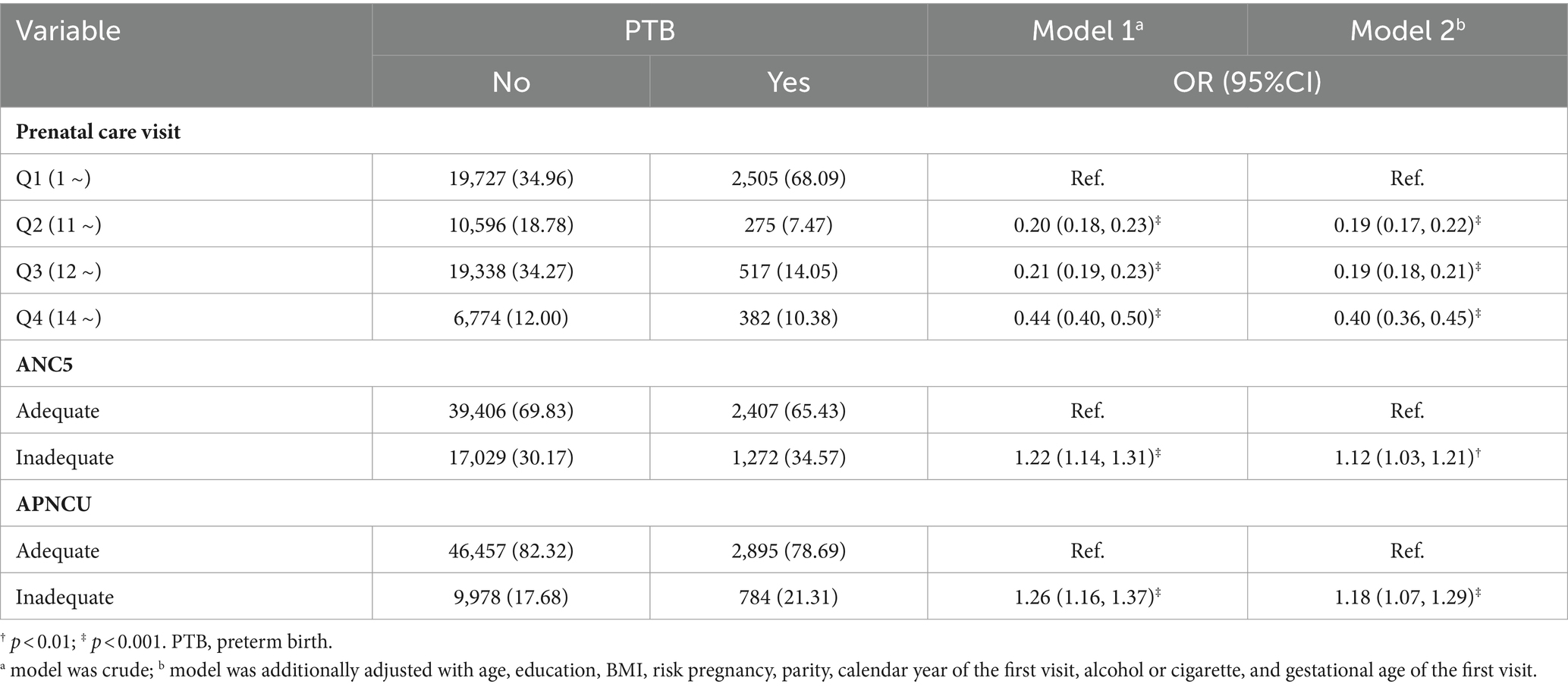
Table 2. Association between prenatal care utilization and PTB.
Table 3 displays the relationship between prenatal care utilization and SGA or LGA. Inadequate prenatal care utilization measured in ANC5 (OR = 1.13, 95%CI: 1.07–1.21) and APNCU (OR = 1.11, 95%CI: 1.03–1.20) were associated with an increased risk of SGA. Increasing prenatal care utilization was associated with a lower risk of SGA (Q4: OR = 0.84, 95%CI: 0.77–0.92) compared to Q1. Moreover, an elevation in prenatal care utilization was associated with an increased risk of LGA (Q4, OR = 1.23, 95%CI: 1.12–1.35). Supplementary Tables S3A,B shows the association between prenatal care visits and birth weight and LBW/FM, respectively. Similar to previous results, inadequate prenatal care in both ANC5 and APNCU was associated with weight loss [ANC5: β (se) = −14.21 (3.87); APNCU: β (se) = −26.68 (4.57)]. However, inadequate ANC5 and APNCU were not associated with LBW.
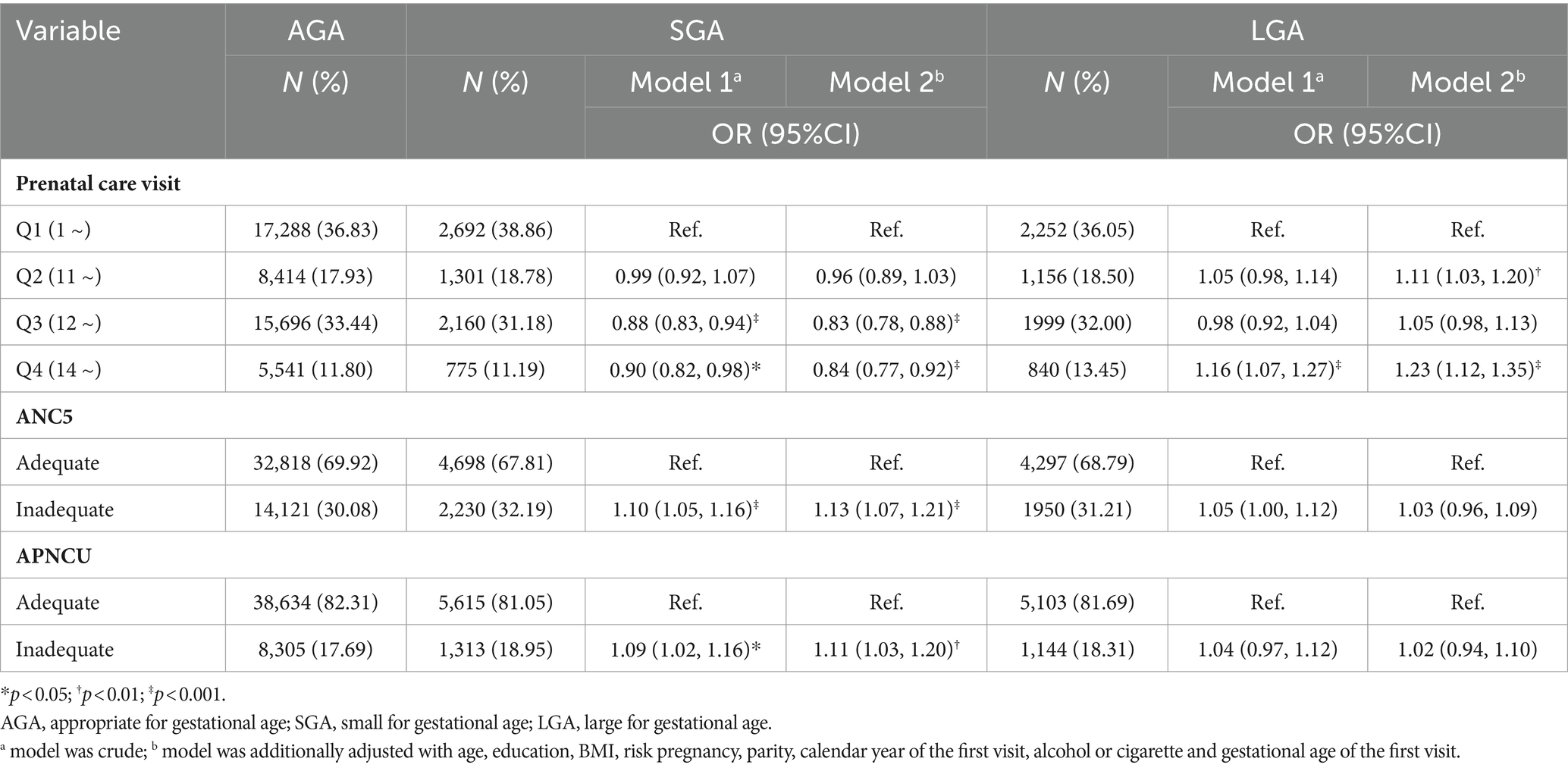
Table 3. Association between prenatal care utilization and SGA and LGA.
The crossover analysis of ANC5 and APNCU on preterm showed that compared to women with both adequate ANC5 and APNCU, only inadequacy in ANC5 (OR = 1.15, 95%CI: 1.05–1.26) or APNCU (OR = 1.48, 95%CI: 1.26–1.73) was both associated with an increased risk of PTB (Table 4). However, a joint effect was not detected.
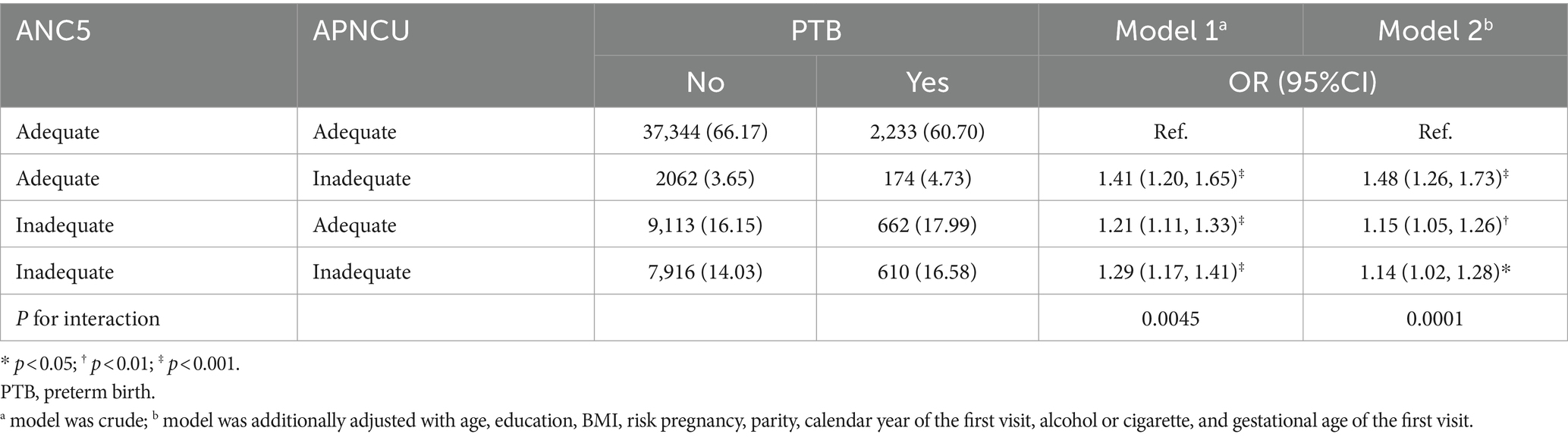
Table 4. Crossover analysis of APNCU on PTB.
Similarly, women had a higher risk of SGA if only the ANC5 (OR = 1.13, 95%CI = 1.06–1.22) or the APNCU (OR = 1.15, 95%CI = 1.00–1.31) were inadequate. No joint effect was detected (Table 5).
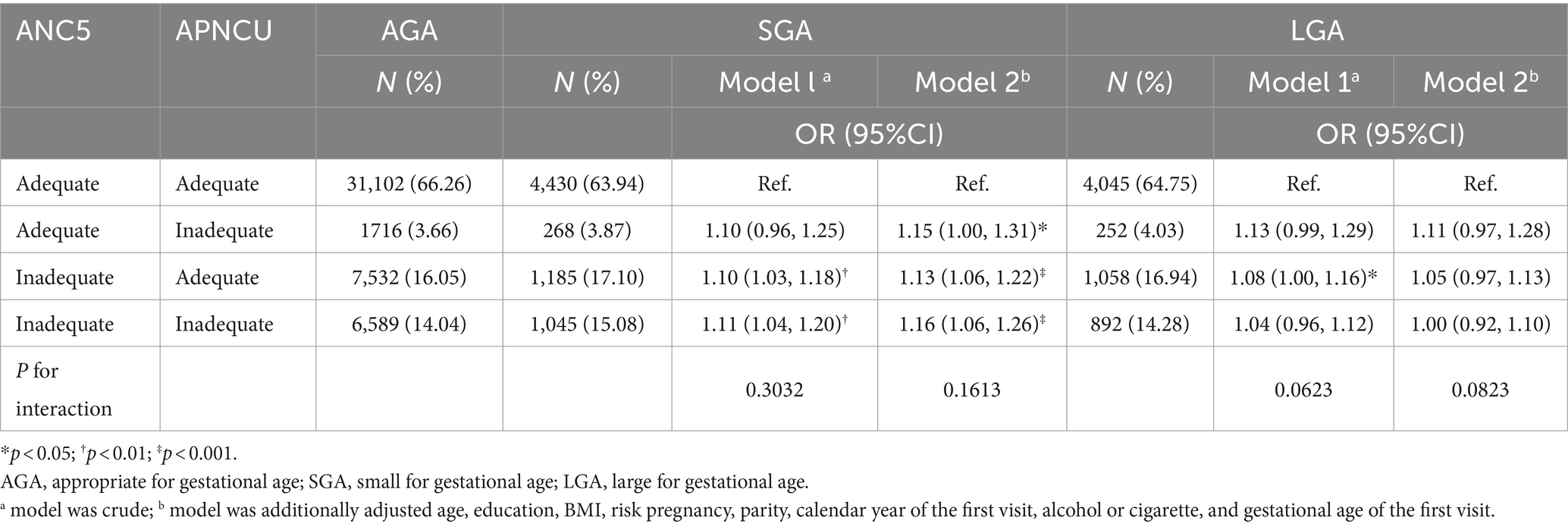
Table 5. Association between ANC5 and APNCU on SGA and LGA.
Supplementary Tables S4A,B shows the crossover analysis of prenatal care utilization measured in ANC5 and APNCU and birth weight and LBW/FM, respectively. To conclude, compared to women who met adequate criteria of both ANC5 and APNCU, women who completed adequate prenatal care only in APNCU were exposed to weight loss in newborns [β (se) = −42.29 (8.48)]; women were exposed to weight loss ANC5 was adequate [β (se) = −11.17 (4.51)]. An interaction between APNCU and ANC5 was detected in the effect of ANC5 and APNCU on birth weight. Women had a higher risk of LBW when mere inadequacy in APNCU (OR = 1.68, 95%CI: 1.19–2.39) or ANC5 (OR = 1.26, 95%CI: 1.07–1.50) was detected. An interaction was detected between ANC5 and APNCU (p < 0.05).
When changing BMI at the first visit to pre-pregnancy BMI, the association between prenatal care and adverse outcomes remained similar (Supplementary Tables S6A–S10B). In the stratification analysis (Supplementary Tables S11, S12), there was no significant difference in the association between prenatal care and adverse outcomes in different risk groups (p > 0.05).
Our study indicated that inadequate ANC5 and APNCU would lead to birth weight loss and a higher risk of PTB, SGA, and LBW. The crossover analysis showed that women with inadequacies in either ANC5 or APNCU were more likely to deliver babies with small birth weight, LBW, and PTB. Additionally, ANC5 and APNCU had an interaction effect on PTB.
Our study revealed that inadequate prenatal care utilization was associated with a higher risk of PTB. This was in line with one previous study, which showed that prenatal care frequency was negatively related to PTB (23). As for APNCU, our result differed from previous studies (3), which found that women with inadequate prenatal care were exposed to a lower risk of PTB. One explanation could be that the distribution of needed prenatal care utilization in different trimesters was imbalanced, which means APNCU was likely to divide women with shorter gestational lengths into adequate plus category (7). The fact that approximately 80% of the women in our study population paid the first visit before or equal to the 12th gestational week means that the situation mentioned above may only appear in a small number of women. This could lead to a difference in association between APNCU and PTB.
Our study indicated that women paying less than five-time-specific visits had an elevated SGA risk. We also compared our results with previous studies in Brazil (15) and Mexico (24). Both studies suggested that women who paid more visits were less likely to have SGA babies. This differs from an earlier meta-analysis of randomized controlled trials (RCTs), which indicated that reduced ANC would not lead to a higher incidence of SGA (25). However, due to the drawback that the outcome analysis and allocation concealment could not be realized, the reliability of these analyses could be undermined. Besides, the conclusion of that RCT study was based on women with low-risk pregnancies, while there are high-risk women in the study population.
Similar to the result of ANC5, inadequate prenatal care in APNCU was associated with SGA. Our data also suggested that insufficient prenatal care influenced SGA births. Two studies indicated inadequate prenatal care usage was associated with SGA in America (21, 26). One study from America also showed no significant association between APNCU and SGA (18). The negative result could be because our study’s reference group was adequate plus and adequate groups combined. Moreover, those with inadequate prenatal care utilization and disproportionately multiparous mothers may also contribute to the differences observed in the study, even though prenatal care utilization was generally distributed evenly among women with different parities.
Different from preterm and SGA, ANC5 and APNCU showed no association with LBW and birth weight. However, previous studies have revealed that prenatal care frequency reduction (27) and prenatal care less than four times (28) were associated with birth weight loss. In addition, previous studies showed a negative association between prenatal care frequency and LBW (28, 29). This could be because the adequate definition of adequate prenatal care utilization in their study was relatively low- and high-level ANC was relatively low in the population, while the prenatal care level was relatively high in China. The protective effect of prenatal care utilization on LBW may disappear after the most basic prenatal care is completed.
The association between APNCU and LBW was similar to that between ANC5. There was no significant association between inadequate APNCU and LBW. This differs from previous studies (3, 30). Studies also showed that the risk of LBW was higher in the adequate plus and inadequate groups, with women in the adequate plus rank exposed to the highest level of LBW risk (2, 31). The difference in the result may arise from the confounders not being controlled.
A crossover analysis was applied to compare the effects of ANC5 and APNCU on birth weight, PTB, and LBW. What needs to be pointed out is that inadequate APNCU would only bring a higher risk of PTB and birth weight loss than inadequate ANC5. APNCU and ANC5 both showed independent risks for SGA and LBW. This means that although inadequate APNCU would bring more severe birth weight outcomes, ANC5 still influenced the outcome mentioned above in another pathway.
Previous studies have pointed out that there is a selection bias in prenatal care utilization. Specifically, the situations can be categorized into four types based on risk and utilization rates: high risk with high utilization, high risk with low utilization, low risk with high utilization, and low risk with low utilization. Therefore, we conducted a stratification analysis based on the risk of pregnancy. No stable interaction is detected between the risk pregnancy and the prenatal care utilization index. This is out of expectation since one previous study observed aggravation of the LBW outcome in women evaluated as having inadequate prenatal care but with a higher risk (3). One possible reason for the non-significant interaction is that high-risk pregnant women may have received more intensive medical interventions. These interventions could mitigate the differences in outcomes between high-risk and low-risk groups, leading to non-significant interaction terms. Effective management and care provided to high-risk pregnant women may blur the differences that might otherwise be observed. It could be due to the development of technology that fewer prenatal care visits may not necessarily result in worse outcomes. It means that we need to pay attention to both groups of women since they benefit similarly from prenatal care. It could also be that the low-risk standard was too strict. Therefore, it may underestimate the effect of prenatal care on birth outcomes.
Moreover, ANC5 was easier for health professionals to calculate and track and more straightforward for pregnant women to follow the medical advice from health professionals than APNCU. Few studies compared indices by crossover analysis. One similar study (18) described the association between prenatal care frequency and the original APNCU and SGA, respectively. It turned out that women with inadequate prenatal care, as measured by the original APNCU, were not exposed to a higher risk of SGA. This could be explained by the difference in the categorization of the index. Our study provided evidence that ANC5’s time-specific track of prenatal care utilization is necessary for women. It proves that ANC5 in China has its appropriateness. More evidence is needed to compare the difference between ANC5 and APNCU.
One significant difficulty in identifying the effect of prenatal care on SGA is that prenatal care visits of women are also influenced by health status in each visit. Accordingly, our study’s strength lies in that women’s health was considered. We used doctors’ diagnoses and women’s symptoms to represent women’s health. Moreover, medical records were utilized to ensure the accuracy of the data collection.
There were also a few drawbacks to our study. First, only including women from Zhoushan could affect the population’s representativeness. Second, essential variables such as income and geographical information were not obtained while investigating the influencing factors, hence introducing confounding bias. Third, more outcomes were needed to compare the two indices.
Women with inadequate prenatal care in ANC5 or APNCU were more likely to suffer from adverse birth outcomes, including PTB, birth weight loss, SGA, and LBW. It indicates that adequate prenatal care is necessary for pregnant women. However, ANC5 and APNCU had an interaction with PTB, and only inadequate prenatal care use by APNCU had the highest risk of PTB, which indicates that APNCU would be a better tool for evaluating prenatal care use.
The data presented in this study are available on request from the corresponding author. The data are not publicly available because they contain information that could compromise the privacy of research participants.
The studies involving humans were approved by the Zhejiang University School of Medicine. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
HZ: Writing – original draft. PC: Formal analysis, Writing – original draft. HC: Writing – review & editing. XA: Methodology, Writing – original draft. YQ: Data curation, Software, Writing – original draft. YH: Investigation, Writing – review & editing. LZ: Resources, Writing – review & editing. DA: Supervision, Writing – review & editing. YZ: Validation, Writing – review & editing. HL: Software, Writing – review & editing. ZC: Investigation, Writing – review & editing. YuY: Conceptualization, Writing – review & editing. YiY: Writing – review & editing.
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. This research was funded by the National Key Research and Development Program of China (grant numbers: 2022YFC2703505 and 2021YFC2701901); the Major Research and Development Projects of the Zhejiang Science and Technology Department (grant number: 2018C03010); the Key Laboratory of Intelligent Preventive Medicine of Zhejiang Province (grant number: 2020E10004); the Leading Innovative and Entrepreneur Team Introduction Program of Zhejiang (grant number: 2019R01007); the Zhejiang Medicine and Health Science and Technology Project (grant number: 2023KY2304); and the Zhoushan Medical Health Science and Technology plan (grant number: 2022YA29).
The authors deeply appreciate the clinicians and all participants in Zhoushan.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2024.1420943/full#supplementary-material
1. Heaman, MI, Newburn-Cook, CV, Green, CG, Elliott, LJ, and Helewa, ME. Inadequate prenatal care and its association with adverse pregnancy outcomes: a comparison of indices. BMC Pregnancy Childbirth. (2008) 8:15. doi: 10.1186/1471-2393-8-15
2. Watson, A, Hernandez, L, and Thompson, D. Adequacy of Prenatal Care Utilization Index and Adverse Birth Outcomes, Florida 2016. (2018). doi: 10.13140/RG.2.2.32402.27844
3. Jogia, PD, and Lodhiya, KK. Antenatal care utilisation among low-risk and high-risk pregnant women & its effects on pregnancy outcome. Obs Gyne Rev J Obstet Gynecol. (2018) 4:82–8. doi: 10.17511/joog.2018.i04.03
4. Blencowe, H, Cousens, S, Oestergaard, MZ, Chou, D, Moller, AB, Narwal, R, et al. National, regional, and worldwide estimates of preterm birth rates in the year 2010 with time trends since 1990 for selected countries: a systematic analysis and implications. Lancet Lond Engl. (2012) 379:2162–72. doi: 10.1016/S0140-6736(12)60820-4
5. Saturno-Hernández, PJ, Martínez-Nicolás, I, Moreno-Zegbe, E, Fernández-Elorriaga, M, and Poblano-Verástegui, O. Indicators for monitoring maternal and neonatal quality care: a systematic review. BMC Pregnancy Childbirth. (2019) 19:25. doi: 10.1186/s12884-019-2173-2
6. Rush, D. Infant death: an analysis by maternal risk and health care, vol 1 of contrasts in health status. Am J Dis Child. (1974) 127:914. doi: 10.1001/archpedi.1974.02110250140032
7. Koroukian, SM, and Rimm, AA. The “adequacy of prenatal care utilization” (APNCU) index to study low birth weight: is the index biased? J Clin Epidemiol. (2002) 55:296–305. doi: 10.1016/s0895-4356(01)00471-1
8. Kotelchuck, M. An evaluation of the Kessner adequacy of prenatal care index and a proposed adequacy of prenatal care utilization index. Am J Public Health. (1994) 84:1414–20. doi: 10.2105/ajph.84.9.1414
9. Mishra, JP. Correlations of APNCU index and fetomaternal out come in tribal area of Chhattisgarh. Int J Multidiscip Curr Res. (2017):5.
10. Beeckman, K, Louckx, F, and Putman, K. Determinants of the number of antenatal visits in a metropolitan region. BMC Public Health. (2010) 10:527. doi: 10.1186/1471-2458-10-527
11. Brenda Wagner et al. Chapter 3: Care during Pregnancy. in Family-Centred Maternity and Newborn Care: National Guidelines. (Public Health Agency of Canada. (2023). p. 3–7.
12. World Health Organization. Organization. Chapter 4. Implementation of the ANC guideline and recommendations. in WHO Recommendations on Antenatal Care for a Positive Pregnancy Experience p.105 (World Health Organization, Geneva. (2016).
13. Zhao, Q, Huang, ZJ, Yang, S, Pan, J, Smith, B, and Xu, B. The utilization of antenatal care among rural-to-urban migrant women in Shanghai:a hospital-based cross-sectional study. BMC Public Health. (2012) 12:1012. doi: 10.1186/1471-2458-12-1012
14. Fan, X, Zhou, Z, Dang, S, Xu, Y, Gao, J, Zhou, Z, et al. Exploring status and determinants of prenatal and postnatal visits in western China: in the background of the new health system reform. BMC Public Health. (2017) 18:39. doi: 10.1186/s12889-017-4601-4
15. Falcão, IR, Ribeiro-Silva, R d C, de Almeida, MF, Fiaccone, RL, Silva, NJ, Paixao, ES, et al. Factors associated with small-and large-for-gestational-age in socioeconomically vulnerable individuals in the 100 million Brazilian cohort. Am J Clin Nutr. (2021) 114:109–16. doi: 10.1093/ajcn/nqab033
16. Liliane Odette, MO. Measuring the effects of prenatal care on child birth weight in Cameroon. Health Policy Plan. (2021) 36:1625–32. doi: 10.1093/heapol/czab117
17. Arsyi, M, Besral, B, Herdayati, M, and Phalkey, R. Antenatal care services and incidence of low birth weight: a comparison of demographic and health surveys in 4 ASEAN countries. J Prev Med Pub Health. (2022) 55:559–67. doi: 10.3961/jpmph.22.316
18. Shin, D, and Song, WO. Influence of the adequacy of the prenatal care utilization index on small-for-gestational-age infants and preterm births in the United States. J Clin Med. (2019) 8:E838. doi: 10.3390/jcm8060838
19. Bell, JF, and Zimmerman, FJ. Selection bias in prenatal care use by Medicaid recipients. Matern Child Health J. (2003) 7:239–52. doi: 10.1023/a:1027323618314
20. Andersen, RM. Revisiting the behavioral model and access to medical care: does it matter? J Health Soc Behav. (1995) 36:1–10. doi: 10.2307/2137284
21. VanderWeele, TJ, Lantos, JD, Siddique, J, and Lauderdale, DS. A comparison of four prenatal care indices in birth outcome models: comparable results for predicting small-for-gestational-age outcome but different results for preterm birth or infant mortality. J Clin Epidemiol. (2009) 62:438–45. doi: 10.1016/j.jclinepi.2008.08.001
22. Delgado-Rodríguez, M, Gómez-Olmedo, M, Bueno-Cavanillas, A, and Gálvez-Vargas, R. A comparison of two indices of adequacy of prenatal care utilization. Epidemiol Camb Mass. (1996) 7:648–50. doi: 10.1097/00001648-199611000-00016
23. Pervin, J, Rahman, SM, Rahman, M, Aktar, S, and Rahman, A. Association between antenatal care visit and preterm birth: a cohort study in rural Bangladesh. BMJ Open. (2020) 10:e036699. doi: 10.1136/bmjopen-2019-036699
24. EO, O. Maternal risk factors for small-for-gestational-age newborns in Mexico: analysis of a Nationwide representative cohort. Front Public Health. (2021) 9:9. doi: 10.3389/fpubh.2021.707078
25. Dowswell, T, Carroli, G, Duley, L, Gates, S, Gülmezoglu, AM, Khan-Neelofur, D, et al. Alternative versus standard packages of antenatal care for low-risk pregnancy. Cochrane Database Syst Rev. (2015) 2015:CD000934. doi: 10.1002/14651858.CD000934.pub3
26. Partridge, S, Balayla, J, Holcroft, CA, and Abenhaim, HA. Inadequate prenatal care utilization and risks of infant mortality and poor birth outcome: a retrospective analysis of 28,729,765 U.S. deliveries over 8 years. Am J Perinatol. (2012) 29:787–94. doi: 10.1055/s-0032-1316439
27. Wehby, GL, Murray, JC, Castilla, EE, Lopez-Camelo, JS, and Ohsfeldt, RL. Quantile effects of prenatal care utilization on birth weight in Argentina. Health Econ. (2009) 18:1307–21. doi: 10.1002/hec.1431
28. Bountogo, M, Sié, A, Zakané, A, Compaoré, G, Ouédraogo, T, Lebas, E, et al. Antenatal care attendance and risk of low birthweight in Burkina Faso: a cross-sectional study. BMC Pregnancy Childbirth. (2021) 21:825. doi: 10.1186/s12884-021-04310-6
29. Chen, CH, and Lin, HC. Prenatal care and adverse pregnancy outcomes among women with depression: a nationwide population-based study. Can J Psychiatry Rev Can Psychiatr. (2011) 56:273–80. doi: 10.1177/070674371105600506
30. Beyrami, HJ, Alizadeh, M, Bakhshian, F, Khanlarzadeh, E, Heidari, F, and Khamnian, Z. Adequacy of prenatal care and its association with pregnancy outcomes: a comparison of indices in Tabriz, Iran. J Res Clin Med. 3:12–6. doi: 10.15171/jarcm.2015.002
Keywords: prenatal care, birth weight, index, SGA, preterm birth, high-risk pregnancy
Citation: Zhou H, Yang Y, Chi P, Cheng H, Alifu X, Qiu Y, Huang Y, Zhang L, Ainiwan D, Zhuang Y, Liu H, Chen Z and Yu Y (2024) The association of Chinese and American antenatal care utilization indices with birth outcomes. Front. Public Health. 12:1420943. doi: 10.3389/fpubh.2024.1420943
Edited by:
Melaku Tadege Engidaw, Debre Tabor University, EthiopiaReviewed by:
Yohannes Tesfahun Kassie, Debre Tabor University, EthiopiaCopyright © 2024 Zhou, Yang, Chi, Cheng, Alifu, Qiu, Huang, Zhang, Ainiwan, Zhuang, Liu, Chen and Yu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Zhi Chen, emp1Y2hlbnpoaUB6anUuZWR1LmNu; Yunxian Yu, eXVueGlhbnl1QHpqdS5lZHUuY24=
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.