
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
BRIEF RESEARCH REPORT article
Front. Public Health , 24 June 2024
Sec. Infectious Diseases: Epidemiology and Prevention
Volume 12 - 2024 | https://doi.org/10.3389/fpubh.2024.1415778
 Nadja Käding1*†
Nadja Käding1*† Frederike Waldeck1†
Frederike Waldeck1† Bjarne Meier1
Bjarne Meier1 Sébastien Boutin1,2
Sébastien Boutin1,2 Max Borsche3
Max Borsche3 Alexander Balck3Bandik Föh4
Alexander Balck3Bandik Föh4 Jan Kramer5
Jan Kramer5 Christine Klein3
Christine Klein3 Alexander Katalinic6
Alexander Katalinic6 Jan Rupp1
Jan Rupp1Trial registration: Non-pharmaceutical interventions (NPI) have been proven successful in a population-based approach to protect from SARS-CoV-2 transmission during the COVID-19 pandemic. As a consequential-effect, a reduction in the spread of all respiratory viruses has been observed, but the primary factors behind this phenomenon have yet to be identified. We conducted a subgroup analysis of participants from the ELISA study, a prospective longitudinal cohort study on SARS-CoV-2 transmission, at four timepoints from November 2020 – September 2022. The aim was to provide a detailed overview of the circulation of respiratory viruses over 2 years and to identify potential personal risk factors of virus distribution. All participants were screened using qPCR for respiratory viral infections from nasopharyngeal swabs and answered a questionnaire regarding behavioral factors. Several categories of risk factors for the transmission of respiratory viruses were evaluated using a scoring system. In total, 1,124 participants were included in the study, showing high adherence to governmental-introduced NPI. The overall number of respiratory virus infections was low (0–4.9% of participants), with adenovirus (1.7%), rhino−/enterovirus (3.2%) and SARS-CoV-2 (1.2%) being the most abundant. We detected an inverse correlation between the number and intensity of NPI and the number of detected respiratory viruses. More precisely, the attendance of social events and household size was associated with rhino−/enterovirus infection while social contacts were associated with being positive for any virus. NPI introduced during the COVID-19 pandemic reduced the occurrence of seasonal respiratory viruses in our study, showing different risk-factors for enhanced transmission between viruses.
DRKS.de, German Clinical Trials Register (DRKS), Identifier: DRKS00023418, Registered on 28 October 2020.
With the emergence of the coronavirus disease 2019 (COVID-19) pandemic, non-pharmaceutical interventions (NPI) were introduced worldwide to limit SARS-CoV-2 transmission. NPI are pandemic countermeasures that are readily available at all times and in all countries (1). NPI can be roughly divided into interventions that reduce personal contacts (quarantine, isolation, cohorting, stay-at-home orders) and make contacts safer (physical distancing, hand hygiene, masks) (2). The efficacy of NPI on the evolution of pandemics must be weighed against the restriction in personal autonomy of decisions and high economic costs (3, 4). Only a few studies have evaluated the efficacy of NPI on the distribution of respiratory viruses before the COVID-19 pandemic. Since then a growing body of evidence shows the effect of NPI on SARS-CoV-2 transmission and other respiratory viruses (5). The effectiveness of the different NPI is an ongoing matter of debate. Since NPI were introduced in bundles during the COVID-19 pandemic the effect of each NPI is hard to establish: Meta-analysis suggests high influence on SARS-CoV-2 reproduction numbers due to school, workplace, business and venue closure and the ban of public events and intermediate effectiveness of lockdown, travel restrictions, ban of mass gathering and social events as well as public campaigns, wearing a mask and social distancing. Other NPI seems to be less effective including contact tracing and isolation/quarantine (6). Still, the effect of NPI on non-SARS-CoV-2 respiratory diseases has not been well studied thus far.
First restrictions on daily life were implemented in mid-March 2020 in the federal state of Schleswig-Holstein, Germany (7). These included the prohibition of private meetings and social events, and the closure of public institutions, stores, bars and restaurants; moreover, no tourism was allowed. In April 2020, face masks were introduced to reduce virus transmission to and from individuals (8). NPI were adapted throughout the pandemic according to SARS-CoV-2 circulation and the expected number of infected and/or hospitalized patients as well as mortality. NPI furthermore led to a markedly reduced transmission of respiratory viruses, including influenza virus and a strong disruption of the typical seasonal circulation patterns of common respiratory virus infections (9). The COVID-19 pandemic strongly influenced the typical flu season in winter (10), as significantly fewer infections were detected and seasonality of influenza virus infections was no longer observed. Lower numbers of infections with influenza viruses, rhinovirus, human metapneumoviruses, parainfluenza viruses and respiratory syncytial viruses have been detected in Germany since the beginning of the coronavirus pandemic 2020 according to the Robert Koch Institute, as well as reduced cases of acute respiratory infections (ARI) (10, 11).
ARI are a common cause of doctor’s consultation, hospitalization and death during the winter season. ARI are associated with high economic costs (550 Million euros within 2010–2019) (12). The annual incidence of ARI remains unclear, but it is estimated that most people suffer from at least one ARI per year (13). Surveillance performed in the United States of America reports yearly >25 million primary care and 9 million emergency department admissions due to ARI (14). Respiratory viruses may be responsible for almost 40% of CAP cases and an even higher proportion of ARIs (15). Therefore, prevention of ARI is a cost-effective and important public health measure.
This study aimed to investigate the impact of the COVID-19 pandemic protection measures including lockdown measures on the epidemiology of seasonal respiratory viruses, including influenza and SARS-CoV-2. We further aimed to describe predictors of virus distribution in Luebeck, Germany.
We conducted a longitudinal, prospective cohort study, which was a sub-study of the Luebeck Longitudinal Investigation of SARS-CoV-2 Infection (ELISA) study. The methods have been described elsewhere (16, 17). In the original ELISA study protocol, the study visits included in our sub-study were previously described as study visit 6, 7 and two follow-ups but for clarity purpose they will be named here as study visit 1–4, respectively.
At each study visit we aimed for 500 participants. During study visit 1 (November 2020) and 2 (February 2021) study participants were randomly selected. While at study visit 3 (March 2022) and 4 (September 2022) study participants could enroll themselves to the sub-study, where we offered maximal 500 appointments. At study visit 2 we had to exclude 110 study participants, since they did not take part in the general testing intervals of the ELISA cohort. In total 1,124 study participants were tested via quantitative real-time polymerase chain reaction (PCR) for respiratory viruses from 1,879 nasopharyngeal swabs using the ampliCube Respiratory Viral Panel 1, 3, 4 and the ampliCube Coronavirus Panel Kits (MIKROGEN, Neuried) (16). Respiratory viruses included in the panels are influenza A/B, SARS-CoV-2, middle east respiratory syndrome coronavirus (MERS-CoV), human coronavirus (hCoV) (229E, HKU1, NL63, OC43), parechovirus, respiratory syncytial virus (RSV), metapneumovirus (HMPV), rhinovirus, enterovirus, and adenovirus.
For antibody testing, a venous blood sample was drawn. The follow-up tests were based on dried blood spots. For anti-nuclear capsid protein immunoglobulin G (anti-NCP IgG) testing, we performed an Anti-SARS-CoV-2-NCP-ELISA (IgG) (EUROIMMUN AG, Lübeck, Germany).
Personal risk factors for the acquisition of respiratory viral infections were inquired via questionnaire. These included household size, social contacts, attendance and size of events, home office, use of public transportation and visit to physician’s office. A scoring system was developed based on the personal risk factors for viral transmission to calculate an overall risk for exposure to viral infections and to perform statistical analysis. Risk factors for viral transmission were weighted according to their reported efficacy in the protection of SARS-CoV-2 transmission, as has been reported in the introduction and in the literature including empirical studies (6, 18, 19). The risk score is shown in Supplementary Table 1. A maximum of 3 points could be achieved in each category. Self-reported greater size of the household and attended events became higher points on the scoring system since the limitation of event size has been reported to be associated with lower SARS-CoV-2 transmission (18). The category “social contacts” accounted for the cumulative risk of different social events including bars, theater and others. Visiting a bar, disco or restaurant was weighted higher than theater, hairdresser and gym, since there were no assigned/stationary seats or masks were not worn during eating and drinking (18).
Descriptive statistics and statistical analysis were performed using IBM SPSS Statistics 27.0 and R 4.2.2. p-values of <0.05 were considered statistically significant. To evaluate the association positivity of viral detection via PCR with the scoring system we analyzed the data in a multivariate logistic regression model (generalized linear model with binomial distribution) with age and gender as co-variates using the R package stats and the adjusted odds ratio (OR) was calculated from the model using the R package epiDisplay. Multi-collinearity was evaluated using Variance inflation factor (VIF) and spearman correlation. VIF were low to moderate (1.02–1.42) indicating low correlation but the spearman correlation indicates a strong association between three scores which were then included as interacting scores in the model (Supplementary Figure 1). To assess whether there is a correlation between the transmission of respiratory viruses and the intensity of NPI, we performed a multivariate analysis on the probability of positivity to any viruses as well as individual probability for the most prevalent viruses; RV/EV, adenovirus and SARS-CoV-2.
The ELISA cohort consisted of 3,051 participants, representing ~1% of the local population in the Luebeck catchment area. Further, the cohort included a high-exposure subgroup to enrich potential positivity based on a profession requiring intense and/or frequent contact with other people, such as healthcare personnel. Study participants of the ELISA cohort had an above-average educational level (17). From the 1,124 participants tested, 517 people (45.9%) were tested once vs. 473 (42.1%) tested twice vs. 120 (10.7%) tested three times and 14 tested four times (1.3%). The median age of the ELISA cohort subgroup was 47 years (SD, 14.4; range, 18–79 years) and 54.5% were females, 13.8% active smokers, corresponding to the ELISA cohort. 56.5% of participants were vaccinated at least once against influenza and 17.2% against pneumococcus. COVID-19 vaccination status is shown in Supplementary Table 2 and corresponds to 0–100% vaccinated participants at timepoint 1–4.
During study visit 1 (November 2020) rhinovirus and enterovirus (RV/EV) (19 of 500, 3.8% positive) circulation could be observed after a period where restrictions were eased in the summer and early fall, while cases of human coronavirus, SARS-CoV-2, adenovirus and parechovirus could be infrequently detected (Figure 1 and Supplementary Table 2). No respiratory virus could be detected at visit 2 in February 2021 during the complete lockdown. At study visit 3 March 2022 we could observe an increase in RV/EV (24 of 493, 4.9%). During that time point SARS-CoV-2 was detected in 14 participants (2.8%) and human coronavirus in five cases (1%). Low numbers of adenovirus (2/493, 0.4%), RSV (1/493, 0.2%) and HMPV (2/493, 0.4%) could be detected (Supplementary Table 2). At study visit 4 in September 2022, when COVID-19 measures were not present anymore, adenoviruses (28/496, 5.6%), as well as RV/EV (18/496, 3.6%), could be detected in the study group. Only single cases of human coronavirus and SARS-CoV-2 with five cases could be detected (Supplementary Table 2), but no case of influenza. Overall, the most frequent viruses were RV/EV (61/1879, 3.2%) followed by adenovirus (32/1879, 1.7%).
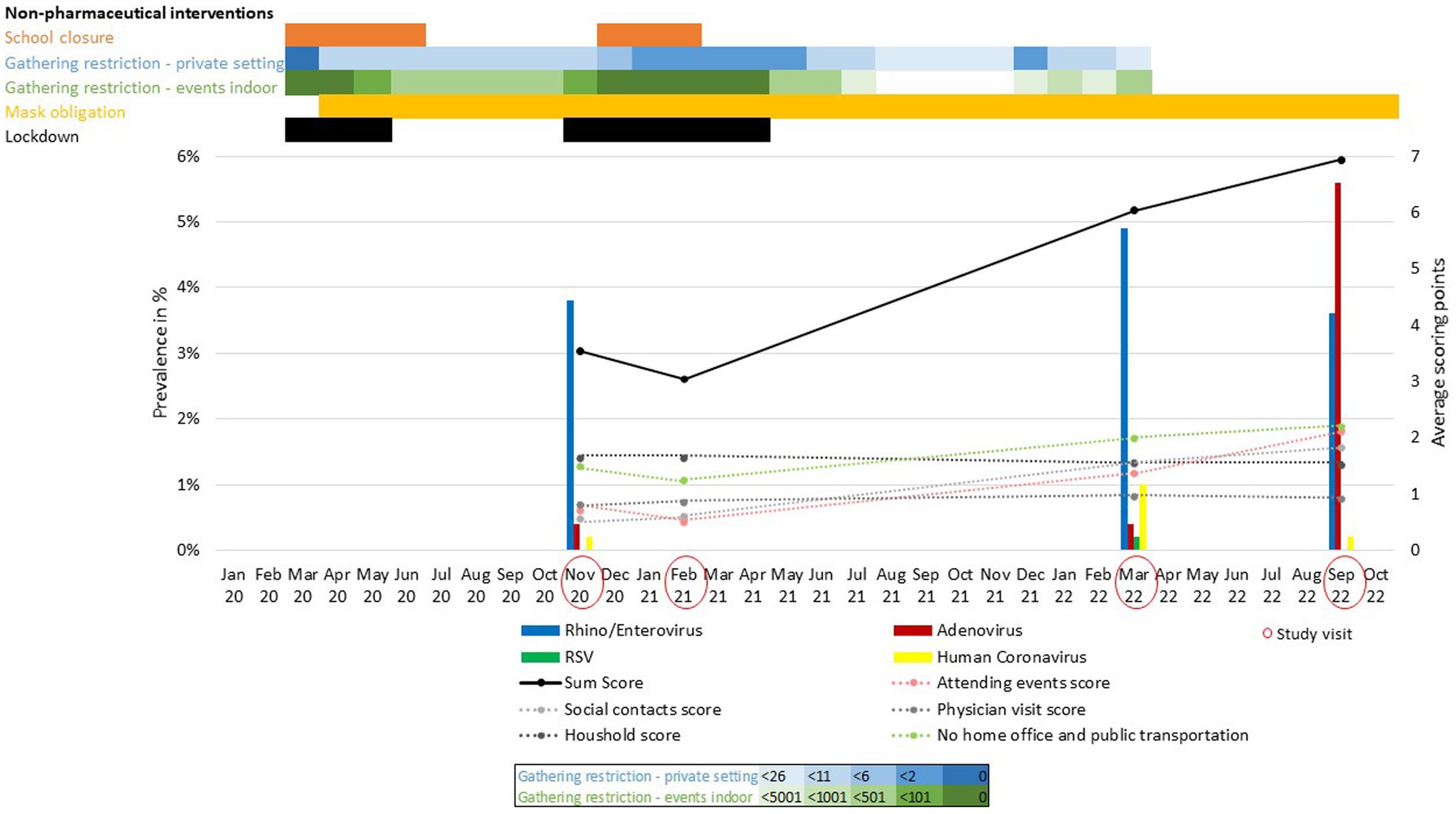
Figure 1. Regional governmental COVID-19 non-pharmaceutical interventions and prevalence of respiratory viruses during the COVID-19 pandemic. Intensity of non-pharmaceutical interventions (NPI) (Law and Ordinance Gazettes of the Government of Schleswig-Holstein, https://www.schleswig-holstein.de/DE/) is indicated by different color intensities. Total score (black line) and single parameters (dotted lines) of the scoring system indicate adherence to NPI during the study period.
The multivariate analysis on the probability of positivity to any viruses as well as individual probability for RV/EV, adenovirus and SARS-CoV-2 is shown in Figure 2. The size of social events was associated with being positive for RV/EV (OR: 2.71, 95% CI: 1.43–5.14) and having had recent SARS-CoV-2 infection (positivity for anti-NCP IgG) (OR: 2.25, 95% CI 1.52–3.43). Social contacts were associated with being positive for any virus (OR: 1.95, 95% CI 1.07–3.56) and recent SARS-CoV-2 infection (OR: 2.82, 95% 1.73–4.58). The household size correlated with being RV/EV positive (OR: 1.51, 95% CI 1.01–2.26) and having anti-NCP IgG (OR: 1.3, 95% CI 1.06–1.59). No impact on virus transmission was detected by visiting a physician’s office, using public transportation and going to work.
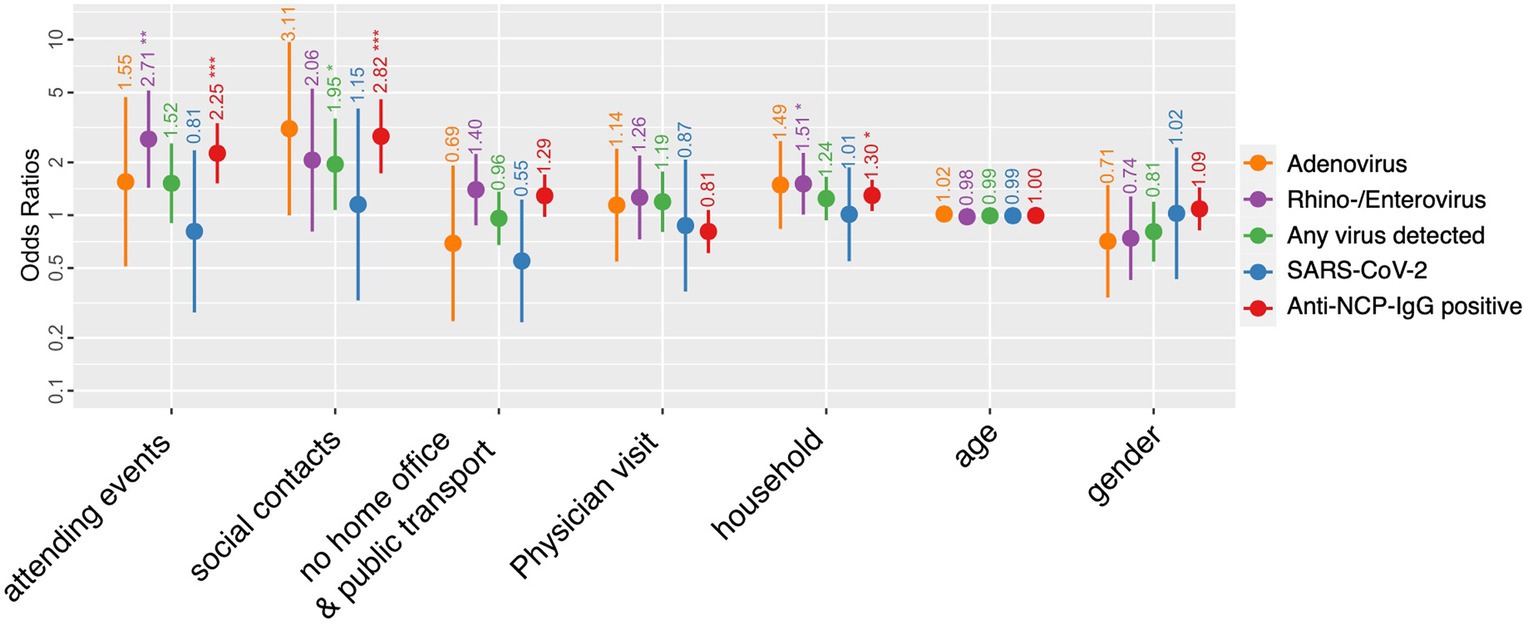
Figure 2. Predisposing factors of respiratory viral infection. Odds ratios and 95% confidence intervals for adenovirus, rhino−/enterovirus and SARS-CoV-2 infection as well as any virus detected and being exposed to SARS-CoV-2 [anti-nucleocapsid (NCP) antibodies positive] for selected parameters of interest. The antibody detection assay was performed as described previously (16). Only the additive factors are displayed but the interaction due to collinearity are shown in the Supplementary Figure 1B.
The interaction of attending events and social contacts showed a significant association with recent SARS-CoV-2 infection. As well as the interaction of the factor social contacts and using public transportation and going to work. While the interaction of attending events and using public transportation and going to work correlate with being RV/EV positive.
Our data provide a detailed picture of the circulation of respiratory viruses in a population-based prospective study over 2 years during the COVID-19 pandemic. Because of the COVID-19 pandemic, several NPI were implemented by the federal government of Germany (Figure 1). In March 2020 a nationwide lockdown was introduced, followed by school closures, and very limited personal contacts (Figure 1). Further, mask obligation was introduced and lasted for the complete study period. While surveillance tools for respiratory viruses report incidences of symptomatic patients with acute respiratory infections that approach doctor’s offices, our data characterize the “real world” circulation of respiratory viruses in the population. Therefore, the effect of NPI on respiratory virus transmission in the Luebeck area determined by our study can be conveyed to the local population. To the best of our knowledge, this is the first study to show a correlation between specific personal risk factors, including size of household and attended events, and the prevalence of non-SARS-CoV-2 respiratory viruses in the general population.
The inverse correlation between the number and intensity of NPI and the number of detected respiratory viruses, including adenovirus and RV/EV, suggests an influence of NPI on respiratory virus transmission other than SARS-CoV-2. The effect of the bundled NPI (e.g., social distancing, travel ban, lockdown, isolation/quarantine, personal protective equipment, school and workplace closure) on the reduction of SARS-CoV-2 transmission has been established (20). Their impact might be most pronounced and might only work in bundles (21).
Surprisingly, few studies evaluated the effect of NPI on seasonal respiratory viruses. NPI work through the reduction of personal contacts and enforcement of hygiene measures. Most respiratory viruses are transmitted by droplets (9), therefore an impact of COVID-19 NPI was to be expected. Usually, RV circulate all year round, but are reduced during winter season. In the season 2018/19 highest positivity rates for influenza were recorded from January until mid of March. RSV circulates from November through March with a peak at the end of year, while HMPV occurs all year round with higher activity in spring and summer (10, 22). Epidemiological data show a decrease in influenza circulation and an interruption of seasonal circulation of respiratory viruses during the pandemic, which suggests an effect of NPI on respiratory viruses other than SARS-CoV-2 (9). This could be confirmed by our cohort. No respiratory virus could be detected during the complete lockdown with school closures and strong restrictions regarding personal contacts (Figure 1). While total virus numbers partially increased when gathering restrictions were only limited to 25 people and indoor events allowed up to 500 people in the Luebeck area. A decrease has been shown for adenovirus, RSV, human coronavirus, metapneumovirus and influenza (4, 9) and resulted in decreased mortality and hospitalization rates of non-SARS-CoV-2 respiratory viruses (9). Other studies show a weaker effect of NPI on non-enveloped viruses, including adenovirus, bocavirus and RV (23). RV prevalence has been promoted as an indicator of the efficacy of measures against SARS-CoV-2 (24). RV is the most prevalent respiratory virus in humans and is widely distributed in the community (25). It has low seasonality and a similar transmission route as SARS-CoV-2. RV has been shown to respond quickly to anti-COVID-19 measures (26). Our data further stress the importance of reducing social events and contacts to contain respiratory viruses in pandemics. Furthermore, the interaction of NPI (social contact, attending events and public transport/attending work in particular) were associated with spread of SARS-CoV-2 and RV/EV which adds important knowledge for the preparedness to future pandemics. Even though this study was limited to the Luebeck area, similar NPI and a decrease in respiratory virus detection has also been shown for other German regions (21, 23).
RV/EV and adenovirus were the most abundant respiratory viruses, especially in the summer of 2022 in the Luebeck area, when COVID-19 NPI were not present anymore. RV/EV and adenovirus are characterized by the absence of a viral envelope. The absence of a viral envelope may allow infections to quickly increase when infection control measures are relaxed because of increased stability on surfaces (9). Also, adenovirus and RV can be transmitted not only by droplets, but also by direct contact. They are shed from infected vectors for up to 3 weeks, have long stability in the environment and are resistant to disinfectants (5). This might explain why - in contrast to other respiratory viruses which are transmitted via droplet – RV/EV were significantly associated with household and attending events. Therefore, our score differentiates the effect of NPI according to the characteristics of specific respiratory viruses. Studies observed a viral interference between RV and influenza that led to a reduction in influenza infection (22, 27). Previous infection with RV inhibits infection with the influenza A virus by activating antiviral defenses in the target tissue of both viruses (27). At the same time, prior infection with influenza, in turn, may inhibit RV replication (28).
Our data were limited by the low prevalence of viruses and the high adherence of our cohort to governmental-introduced NPIs which could be shown by low total scores, especially during study visit 1 and 2. The recruitment process which tends to include healthy participants which willingly come to the study center might have led to an underestimation of respiratory viruses in the general population. Further, attrition remains a disadvantage of longitudinal studies. Interestingly, with growing rates of vaccinated participants adherence to NPI decreased resulting in higher respiratory virus circulation in the study population. We cannot differentiate the influence of extenuated NPIs from the effect of increasing SARS-CoV-2 vaccination status of participants on respiratory virus circulation. Studies suggest that influenza and pneumococcal vaccination are associated with a reduced risk of SARS-CoV-2 infection (29). Influenza vaccination is associated with reduced risk of ARI in adults (30, 31) and hospitalization due to RSV in children (32). To our knowledge no studies have evaluated the effect of SARS-CoV-2 vaccination on other respiratory viruses. This analysis might be hampered due to NPI which were adapted at the same time as vaccination coverage rate increased during COVID-19 pandemic. Our study is limited to the Luebeck area but markedly decreased rates of respiratory virus circulation have been shown for other German regions which might confirm generalizability of our results (21, 23).
In conclusion, we demonstrate that COVID-19 pandemic protection measures reduced the occurrence of seasonal respiratory viruses in the Luebeck area. Based on the proposed calculated score, we could define risk factors for virus transmission, which can be targeted measures for upcoming pandemics to reduce virus transmission.
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author.
The studies involving humans were approved by Ethics Committee of the University of Luebeck. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
NK: Writing – original draft, Writing – review & editing, Conceptualization, Investigation. FW: Writing – original draft, Writing – review & editing, Conceptualization, Investigation. BM: Formal analysis, Investigation, Writing – review & editing. SB: Formal analysis, Writing – review & editing. MB: Conceptualization, Investigation, Writing – review & editing. AB: Conceptualization, Investigation, Writing – review & editing. BF: Conceptualization, Investigation, Writing – review & editing. JK: Methodology, Resources, Writing – review & editing. CK: Conceptualization, Funding acquisition, Project administration, Supervision, Writing – review & editing. AK: Conceptualization, Funding acquisition, Project administration, Supervision, Writing – review & editing. JR: Conceptualization, Funding acquisition, Project administration, Supervision, Writing – review & editing.
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. This project was funded by the Federal Ministry of Education and Research (BMBF/NUM) within the B-FAST program (AP6 risk settings), the Ministry of Education, Science and Cultural Affairs of the State of Schleswig-Holstein, and a crowdfunding campaign of the University of Luebeck.
We thank Thorsten Niemann for performing the antibody and PCR analysis. Moreover, we would like to thank Sylwia Dankert, Dana Lenke, and Maike Resa for their excellent assistance in organizing the study.
Author JK is employed by LADR GmbH, Germany.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2024.1415778/full#supplementary-material
1. World Health Organization . Non-pharmaceutical public health measures for mitigating the risk and impact of epidemic and pandemic influenza. (2019). Available at: https://iris.who.int/bitstream/handle/10665/329438/9789241516839-eng.pdf?sequence=1
2. Rehfuess, EA, Movsisyan, A, Pfadenhauer, LM, Burns, J, Ludolph, R, Michie, S, et al. Public health and social measures during health emergencies such as the COVID-19 pandemic: an initial framework to conceptualize and classify measures. Influenza Other Respir Viruses. (2023) 17:e13110. doi: 10.1111/irv.13110
3. Brooks, SK, Webster, RK, Smith, LE, Woodland, L, Wessely, S, Greenberg, N, et al. The psychological impact of quarantine and how to reduce it: rapid review of the evidence. Lancet. (2020) 395:912–20. doi: 10.1016/S0140-6736(20)30460-8
4. Spiliopoulos, L . On the effectiveness of COVID-19 restrictions and lockdowns: Pan metron ariston. BMC Public Health. (2022) 22:1842. doi: 10.1186/s12889-022-14177-7
5. Shi, HJ, Kim, NY, Eom, SA, Kim-Jeon, MD, Oh, SS, Moon, BS, et al. Effects of non-pharmacological interventions on respiratory viruses other than SARS-CoV-2: analysis of laboratory surveillance and literature review from 2018 to 2021. J Korean Med Sci. (2022) 37:e172. doi: 10.3346/jkms.2022.37.e172
6. Mendez-Brito, A, El Bcheraoui, C, and Pozo-Martin, F. Systematic review of empirical studies comparing the effectiveness of non-pharmaceutical interventions against COVID-19. J Infect. (2021) 83:281–93. doi: 10.1016/j.jinf.2021.06.018
7. Schleswig-Holstein, Ministerium Für Soziales, Gesundheit, Jugend, Familie und Senioren , Eds. Landesverordnung über Maßnahmen zur Bekämpfung der Ausbreitung des neuartigen Coronavirus SARS-CoV-2 in Schleswig-Holstein (SARS-CoV-2-Bekämpfungsverordnung – SARS-CoV-2-BekämpfV). (2020). Available at: https://transparenz.schleswig-holstein.de/dataset/41553002-13e9-467d-ba09-ab4a51542a7e/resource/f5175282-f2f2-4a9a-8790-d2d533a13d25/download/sars-cov-2-bekampfungsvo3810690577184248626.pdf
8. Ministerium Für Inneres, Ländliche Räume und Integration Des Landes Schleswig-Holstein . Gesetz- und Verordnungsblatt für Schleswig-Holstein. (2020). Available at: https://www.schleswig-holstein.de/DE/landesregierung/ministerien-behoerden/IV/Service/GVOBl/GVOBl/2020/gvobl_7_2020.pdf?__blob=publicationFile&v=3
9. Chow, EJ, Uyeki, TM, and Chu, HY. The effects of the COVID-19 pandemic on community respiratory virus activity. Nat Rev Microbiol. (2023) 21:195–210. doi: 10.1038/s41579-022-00807-9
10. Goerlitz, L, Dürrwald, R, An Der Heiden, M, Buchholz, U, Preuß, U, Prahm, K, et al. Erste Ergebnisse zum Verlauf der Grippewelle in der Saison 2019/20: Mit 11 Wochen vergleichsweise kürzere Dauer und eine moderate Anzahl an Influenza-bedingten Arztbesuchen. (2020). Available at: https://edoc.rki.de/handle/176904/6627.2
11. Buchholz, U, Buda, S, and Prahm, K. Abrupter Rückgang der Raten an Atemwegserkrankungen in der deutschen Bevölkerung. (2020). Available at: https://edoc.rki.de/handle/176904/6601.2
12. Goettler, D, Niekler, P, Liese, JG, and Streng, A. Epidemiology and direct healthcare costs of influenza-associated hospitalizations – nationwide inpatient data (Germany 2010-2019). BMC Public Health. (2022) 22:108. doi: 10.1186/s12889-022-12505-5
13. Pham, H, Rahman, A, Majidi, A, Waterhouse, M, and Neale, RE. Acute respiratory tract infection and 25-Hydroxyvitamin D concentration: a systematic review and meta-analysis. Int J Environ Res Public Health. (2019) 16:3020. doi: 10.3390/ijerph16173020
14. Stockwell, MS, Reed, C, Vargas, CY, Wang, L, Alba, LR, Jia, H, et al. Five-year community surveillance study for acute respiratory infections using text messaging: findings from the MoSAIC study. Clin Infect Dis. (2022) 75:987–95. doi: 10.1093/cid/ciac027
15. Torres, A, Cilloniz, C, Niederman, MS, Menéndez, R, Chalmers, JD, Wunderink, RG, et al. Pneumonia. Nat Rev Dis Primer. (2021) 7:25. doi: 10.1038/s41572-021-00259-0
16. Balck, A, Föh, B, Borsche, M, Rahmöller, J, Vollstedt, EJ, Waldeck, F, et al. Protocol of the Luebeck longitudinal investigation of SARS-CoV-2 infection (ELISA) study - a prospective population-based cohort study. BMC Public Health. (2022) 22:1305. doi: 10.1186/s12889-022-13666-z
17. Klein, C, Borsche, M, Balck, A, Föh, B, Rahmöller, J, Peters, E, et al. One-year surveillance of SARS-CoV-2 transmission of the ELISA cohort: a model for population-based monitoring of infection risk. Sci Adv. (2022) 8:eabm5016. doi: 10.1126/sciadv.abm5016
18. Murphy, C, Lim, WW, Mills, C, Wong, JY, Chen, D, Xie, Y, et al. Effectiveness of social distancing measures and lockdowns for reducing transmission of COVID-19 in non-healthcare, community-based settings. Philos Transact A Math Phys Eng Sci. (2023) 381:20230132. doi: 10.1098/rsta.2023.0132
19. Onakpoya, IJ, Heneghan, CJ, Spencer, EA, Brassey, J, Plüddemann, A, Evans, DH, et al. SARS-CoV-2 and the role of close contact in transmission: a systematic review. F1000Res. (2021) 10:280. doi: 10.12688/f1000research.52439.1
20. Etemad, K, Mohseni, P, Shojaei, S, Mousavi, SA, Taherkhani, S, Fallah Atatalab, F, et al. Non-pharmacologic interventions in COVID-19 pandemic management; a systematic review. Arch Acad Emerg Med. (2023) 11:e52. doi: 10.22037/aaem.v11i1.1828
21. Bremer, V, An Der Heiden, M, and Hicketier, A. Wirksamkeit und Wirkung von anti-epidemischen Maßnahmen auf die COVID-19-Pandemie in Deutschland (StopptCOVID-Studie). (2023). Available at: https://www.rki.de/DE/Content/InfAZ/N/Neuartiges_Coronavirus/Projekte_RKI/StopptCOVID-Bericht.pdf?__blob=publicationFile
22. Dürrwald, R, Wedde, M, Duwe, S, Biere, B, Reiche, J, Köndgen, S, et al. Synopse virologischer Analysen im Nationalen Referenzzentrum für Influenzaviren während der COVID-19-Pandemie. (2022). Available at: https://edoc.rki.de/handle/176904/9779
23. Yan, H, Zhai, B, Yang, F, Wang, P, and Zhou, Y. The impact of non-pharmacological interventions measures against COVID-19 on respiratory virus in preschool children in Henan, China. J Epidemiol Glob Health. (2023) 14:54–62. doi: 10.1007/s44197-023-00168-3
24. Kitanovski, S, Horemheb-Rubio, G, Adams, O, Gärtner, B, Lengauer, T, Hoffmann, D, et al. Rhinovirus prevalence as indicator for efficacy of measures against SARS-CoV-2. BMC Public Health. (2021) 21:1178. doi: 10.1186/s12889-021-11178-w
25. Jacobs, SE, Lamson, DM, St George, K, and Walsh, TJ. Human Rhinoviruses. Clin Microbiol Rev. (2013) 26:135–62. doi: 10.1128/CMR.00077-12
26. Kim, MC, Park, JH, Choi, SH, and Chung, JW. Rhinovirus incidence rates indicate we are tired of non-pharmacological interventions against coronavirus disease 2019. J Korean Med Sci. (2022) 37:e15. doi: 10.3346/jkms.2022.37.e15
27. Wu, A, Mihaylova, VT, Landry, ML, and Foxman, EF. Interference between rhinovirus and influenza a virus: a clinical data analysis and experimental infection study. Lancet Microbe. (2020) 1:e254–62. doi: 10.1016/S2666-5247(20)30114-2
28. Essaidi-Laziosi, M, Geiser, J, Huang, S, Constant, S, Kaiser, L, and Tapparel, C. Interferon-dependent and respiratory virus-specific interference in dual infections of airway epithelia. Sci Rep. (2020) 10:10246. doi: 10.1038/s41598-020-66748-6
29. Wong, A, Barrero Guevara, LA, Goult, E, Briga, M, Kramer, SC, Kovacevic, A, et al. The interactions of SARS-CoV-2 with cocirculating pathogens: epidemiological implications and current knowledge gaps. PLoS Pathog. (2023) 19:e1011167. doi: 10.1371/journal.ppat.1011167
30. Liu, YH, Huang, LM, and Wang, JD. Reduction of acute respiratory illness (ARI) due to a voluntary workplace influenza vaccination program: who are more likely to get the benefit? J Occup Health. (2004) 46:455–60. doi: 10.1539/joh.46.455
31. Maltezou, HC, Fotiou, A, Antonakopoulos, N, Kallogriopoulou, C, Katerelos, P, Dimopoulou, A, et al. Impact of postpartum influenza vaccination of mothers and household contacts in preventing febrile episodes, influenza-like illness, healthcare seeking, and Administration of Antibiotics in young infants during the 2012–2013 influenza season. Clin Infect Dis. (2013) 57:1520–6. doi: 10.1093/cid/cit599
32. Le, H, de Klerk, N, Blyth, CC, Gidding, H, Fathima, P, and Moore, HC. Non-specific benefit of seasonal influenza vaccine on respiratory syncytial virus-hospitalisations in children: an instrumental variable approach using population-based data. Vaccine. (2023) 41:5029–36. doi: 10.1016/j.vaccine.2023.06.085
Keywords: non-pharmaceutical interventions, respiratory viruses, infection risk, virus distribution, behavioral factors
Citation: Käding N, Waldeck F, Meier B, Boutin S, Borsche M, Balck A, Föh B, Kramer J, Klein C, Katalinic A and Rupp J (2024) Influence of non-pharmaceutical interventions during the COVID-19 pandemic on respiratory viral infections – a prospective population-based cohort study. Front. Public Health. 12:1415778. doi: 10.3389/fpubh.2024.1415778
Edited by:
Faris Lami, University of Baghdad, IraqReviewed by:
Randa K. Saad, The Eastern Mediterranean Public Health Network (EMPHNET), JordanCopyright © 2024 Käding, Waldeck, Meier, Boutin, Borsche, Balck, Föh, Kramer, Klein, Katalinic and Rupp. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Nadja Käding, bmFkamEua2FlZGluZ0B1a3NoLmRl
†These authors have contributed equally to this work and share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.