 Addisu Alemayehu Gube
Addisu Alemayehu Gube Edit Murányi2
Edit Murányi2 Szimonetta Lohner
Szimonetta Lohner- 1Doctoral School of Health Sciences, Faculty of Health Sciences, University of Pécs, Pécs, Hungary
- 2Department of Public Health Medicine, Medical School, University of Pécs, Pécs, Hungary
- 3Cochrane Hungary, Medical School, University of Pécs, Pécs, Hungary
Background: Maternal health service uptake remains an important predictor of maternal outcomes including maternal mortality. This systematic review and meta-analysis aimed to summarize the available evidence on the uptake of maternal health care services in developing countries and to assess the impact of place of residence, education status, and wealth index on the uptake of these services.
Methods: We examined the databases MEDLINE, Web of Science, Global Index Medicus, and Scopus until June 14, 2022. Cross-sectional studies done between 2015 and 2022 were considered. Mothers of reproductive age and all states of health were included in the study. Independently, two authors determined the eligibility of studies, extracted data, evaluated the risk of bias, and ranked the evidence’s degree of certainty. To combine the data, we performed a random-effects meta-analysis. The PROSPERO registration ID is CRD42022304094.
Results: We included 51 studies. Mothers living in urban areas were three times more likely to receive antenatal care (OR 2.95; 95% CI 2.23 to 3.89; 15 studies; 340,390 participants) than rural mothers. Compared with no education, those with primary education were twice as likely to utilize antenatal care (OR 2.36; 95% CI 1.80 to 3.09; 9 studies; 154,398 participants) and those with secondary and higher education were six and fourteen times more likely to utilize antenatal care, respectively. Mothers in the second wealth index were twice as likely as mothers in the lowest wealth index to utilize antenatal care (OR 1.62; 95% CI 1.36 to 1.91; 10 studies; 224,530 participants) and antenatal care utilization increased further among mothers in the higher wealth index. We observed similar relative inequalities in skilled delivery care and postnatal care utilization based on the pace of residence, education, and wealth index.
Conclusion: In developing countries, the problem of inequity in utilizing maternal health care services persists and needs considerable attention.
Introduction
Health inequality refers to a measurable aspect of difference in health that can be observed across individuals or social groups (1). These differences might exist in health conditions or might be related to access to health prevention, therapy, or rehabilitation (2). The term ‘health inequity’ involves the moral social perception of existing health inequalities and refers to inequalities that are considered unjust by society or that stem from some kind of injustice, mainly affecting groups with less wealth, prestige, and power (3, 4).
Maternal mortality, defined as death during pregnancy or within 42 days after childbirth, is an important indicator of socioeconomic inequalities, as it is influenced by the availability of health care and obstetric care (5). Antenatal care contacts and births attended by skilled health professionals, early routine postnatal care, and timely management and treatment of complications are important aspects of reducing preventable maternal mortality (6, 7).
As part of the Sustainable Development Goals (SDGs), the member states of the United Nations expressed their commitment to reducing maternal mortality to less than 70 maternal deaths per 100,000 live births by 2030 (8). Based on recent data, we are far from reaching these goals, as since 2016 maternal mortality has been reported to decrease in only a part of the world, including Central and South Asia, Australia, and New Zealand, while in Sub-Saharan Africa, Oceania, East and Southeast Asia, and north Africa stagnation in maternal mortality is observed (9). In the same period, maternal mortality increased in Europe, North America, Latin America, and the Caribbean (9). Infectious diseases, adolescent pregnancies, cesarean section, availability of health workforce, coverage of births by health facilities and hospitals, and inequalities in service coverage might play the most important role in maternal mortality (10). Underutilization of maternal and child health care services can put women and their offspring at risk of dying (11).
Worldwide, governments have started to place increasing emphasis on addressing inequities in maternal and child health services and these efforts improved relative equity of the coverage of reproductive and maternal health services across countries over the last decades (12). However, among low and middle-income countries there are still differences in the extent to which equity is reached, and inequity in coverage of health services persists in some of the countries more than in others (13). For the current 2024 fiscal year, low-income economies are defined as those with a Gross National Income (GNI) per capita, calculated using the World Bank Atlas method, of $1,135 or less in 2022; lower middle-income economies are those with a GNI per capita between $1,136 and $4,465; upper middle-income economies are those with a GNI per capita between $4,466 and $13,845; high-income economies are those with a GNI per capita of $13,846 or more. And low-or middle-income countries are referred to as developing countries (14, 15).
Even across different regions of a country, significant differences might be present in the utilization of maternal health services (16). The most important factors indicated in studies to have an important impact on the utilization of maternal health services were education, region of residence, maternal age, and distance to health facilities (17). For example, if a woman lives in an impoverished rural area, like Sub-Saharan Africa and South Asia, where the number of available skilled health professionals is limited, the probability of not receiving sufficient healthcare is extremely high. In high- and upper-middle-income countries more than 90% of all births are attended by a trained midwife, doctor, or nurse. In contrast, in low-income and lower-middle-income countries less than half of all births are assisted by such skilled health personnel (18). According to World Health Organization (WHO), childbearing or reproductive age for women is from 15 to 49 years (19).
A previous systematic review carried out on equity in maternal health care service utilization in developing countries identified 36 studies published between 2005 and 2015, out of which 33 reported severe inequities in maternal health care utilization (20). This systematic review included only studies published in English, and maternal health care services were limited to antenatal care. Data were summarized narratively but not quantitatively. Besides, new studies have been published since then, which might show a more up-to-date picture.
For the present systematic review and meta-analysis, maternal health care services considered based on the literature (21) are antenatal care, skilled delivery care, and postnatal care, while inequity for the services is assessed based on three variables including residence, wealth index, and educational status.
This systematic review and meta-analysis aimed to summarize available evidence related to the uptake of maternal healthcare services in developing countries in the period of 2015 to 2022 and to assess differences across groups with different places of residence, education status, and wealth index.
Methods
The methodology and the results are reported according to the Preferred Reporting Items for Systematic Reviews and MetaAnalyses (PRISMA) reporting guideline (22). This study is registered on PROSPERO with the registration ID: CRD42022304094.
Searches
For this systematic review and meta-analysis, we searched the following electronic databases until 14th June 2022 without restrictions to the language of publications: Ovid MEDLINE (09/06/2022), Web of Science (comprising Science Citation Index and Emerging Citation Index) (14/06/2022), Global Index Medicus comprising African Index Medicus (AIM), Index Medicus for the Eastern Mediterranean Region (IMEMR), Index Medicus for the South-east Asia Region (IMSEAR), Latin America and the Caribbean Literature on Health Science (LILACS) and Western Pacific Region Index Medicus (WPRO) (16/06/2022) and Scopus (14/06/2022). Details of our search strategies are available in the Supplementary material.
We used a snowball search method to identify other potentially eligible studies or supplementary publications by searching the reference lists of included studies. All 51 studies included were published in English.
Study inclusion and exclusion criteria
We included cross-sectional (observational) studies investigating maternal health care services (including antenatal care, skilled delivery care, and postnatal care) utilization either separately or all services together from 2015 to 2022 in developing countries. The participants of the studies were mothers of reproductive age (15–49 years) (19) with all health statuses, residing in and having utilized maternal health care services in developing (low and middle-income) countries. Health status refers to medical conditions (both physical and mental health), claims experience, receipt of health care, medical history, genetic information, evidence of insurability, and disability (23).
A country’s development status was determined using the World Bank Classifications of countries (14).
Using Covidence™ software, two review authors (GA and EM) separately screened the titles and abstracts of each retrieved record. In a subsequent step, all possibly relevant full texts were evaluated for eligibility. Any differences of opinion were settled by consensus or by consulting a third author (SL).
Potential effect modifiers and reasons for heterogeneity
We assessed methodological heterogeneity through the assessment of risk of bias, and clinical heterogeneity through the assessment of similarities and differences between studies in terms of types of participants and outcomes. We considered the size and direction of the effect and used a standard χ2 test with a significance level of α = 0.1 and the I2 statistic, which quantifies inconsistency across studies, to assess the effect of heterogeneity on the metaanalysis. In almost all socioeconomic sub-groups we observed high heterogeneity among studies.
We used funnel plots to assess reporting bias and investigate small-study effects when at least ten studies were included in a metaanalysis.
Study quality assessment
Each included study’s risk of bias was evaluated separately by two review authors (GA and EM), and any discrepancies were settled by consensus. The risk of bias was evaluated with the Joanna Briggs Institute (JBI) critical appraisal checklist for analytical cross-sectional studies (24). Based on the checklist, studies were rated on an 8-point scale (Table 1). Those studies achieving a score exceeding half of the total points were eligible for inclusion in the systematic review and meta-analysis.
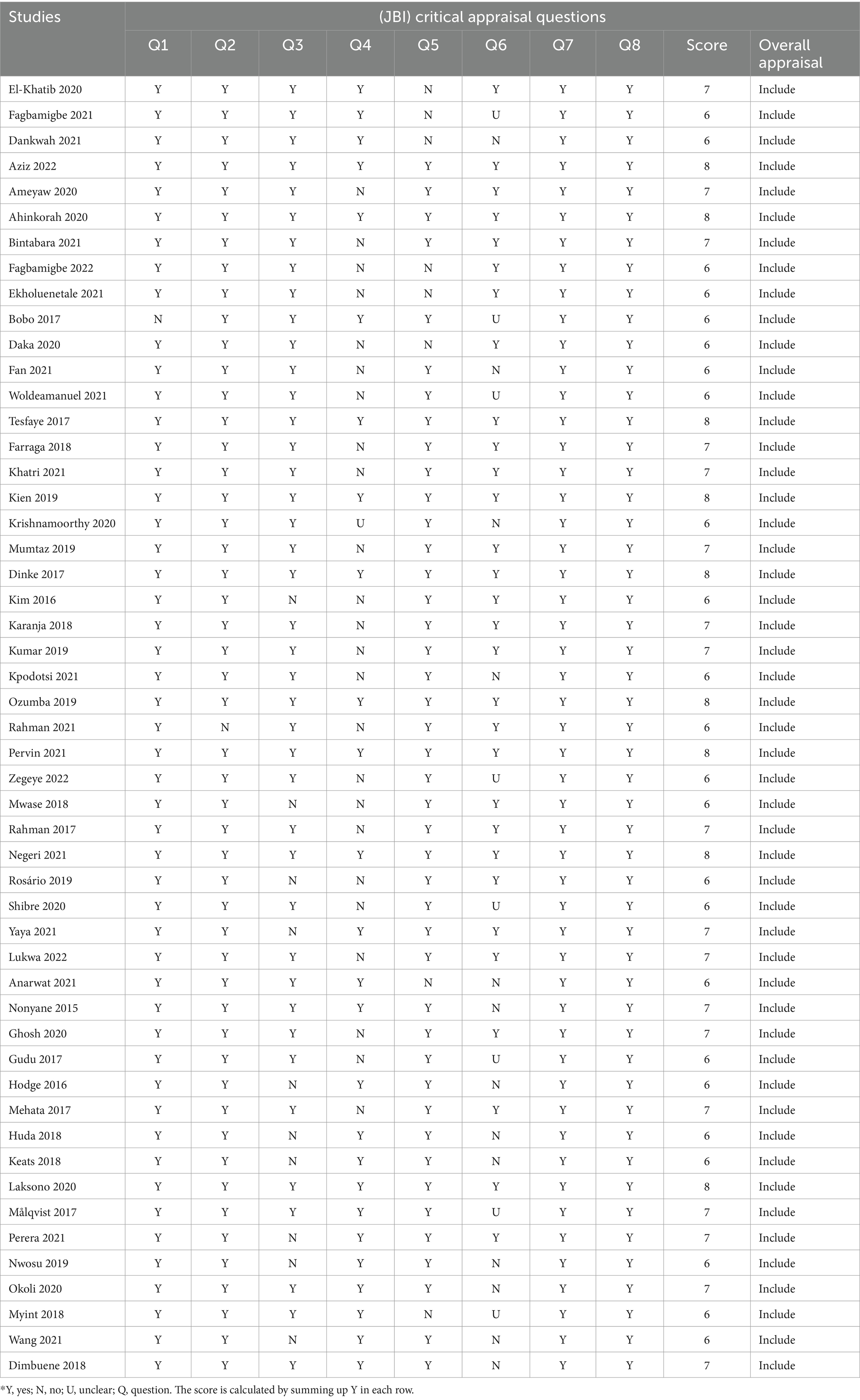
Table 1. Study quality assessment using the Joanna Briggs Institute critical appraisal checklist for analytical cross-sectional studies.
Data extraction strategy
We retrieved information on study methods, participants, maternal health care services, outcomes, funding sources, and potential conflict of interest statements from full-text publications. One reviewer (GA or EM) extracted the data, while a second reviewer (GA or EM) verified its accuracy, consistency, and completeness.
The outcome of interest for this systematic review was inequity in utilization or uptake of maternal health care services (antenatal care, skilled delivery care, and postnatal care), reported as frequency or percentage by mothers’ residence, educational status, and wealth index.
Data synthesis and presentation
We conducted a metaanalysis for every outcome for which we judged the participants and outcomes to be similar enough to provide meaningful results. We conducted meta-analyses for the following three comparisons: Antenatal care utilization versus non-utilization, skilled delivery care utilization versus non-utilization, and post-natal care utilization versus non-utilization. To assess inequity, we investigated the following three factors in association with maternal health care utilization: place of residence (urban and rural), educational status (no education, primary, secondary, and higher), and wealth index (lowest, second, middle, fourth and highest).
We presented the results as odds ratios (ORs) with 95% confidence intervals because our data were dichotomous. We did statistical analyses using RevMan (version 5.4.1). As we expected differences between studies like differences in sample size, we decided to combine the data using a randomeffects model. We used Mantel–Haenszel weighting because the outcomes are dichotomous.
Results of eligible studies that do not provide data in an appropriate format for meta-analysis are summarized in a narrative format. The result is presented using PRISMA 2020 checklist (Supplementary material).
Results
We retrieved 2,109 studies through database searching. We removed duplicates and screened 2,045 studies based on their titles and abstracts. After removing irrelevant studies, we assessed 221 full-text studies for eligibility to be included in this systematic review. Finally, 51 studies met our inclusion criteria. Of these, we were able to include 34 studies in the quantitative syntheses (meta-analysis) (Figure 1).
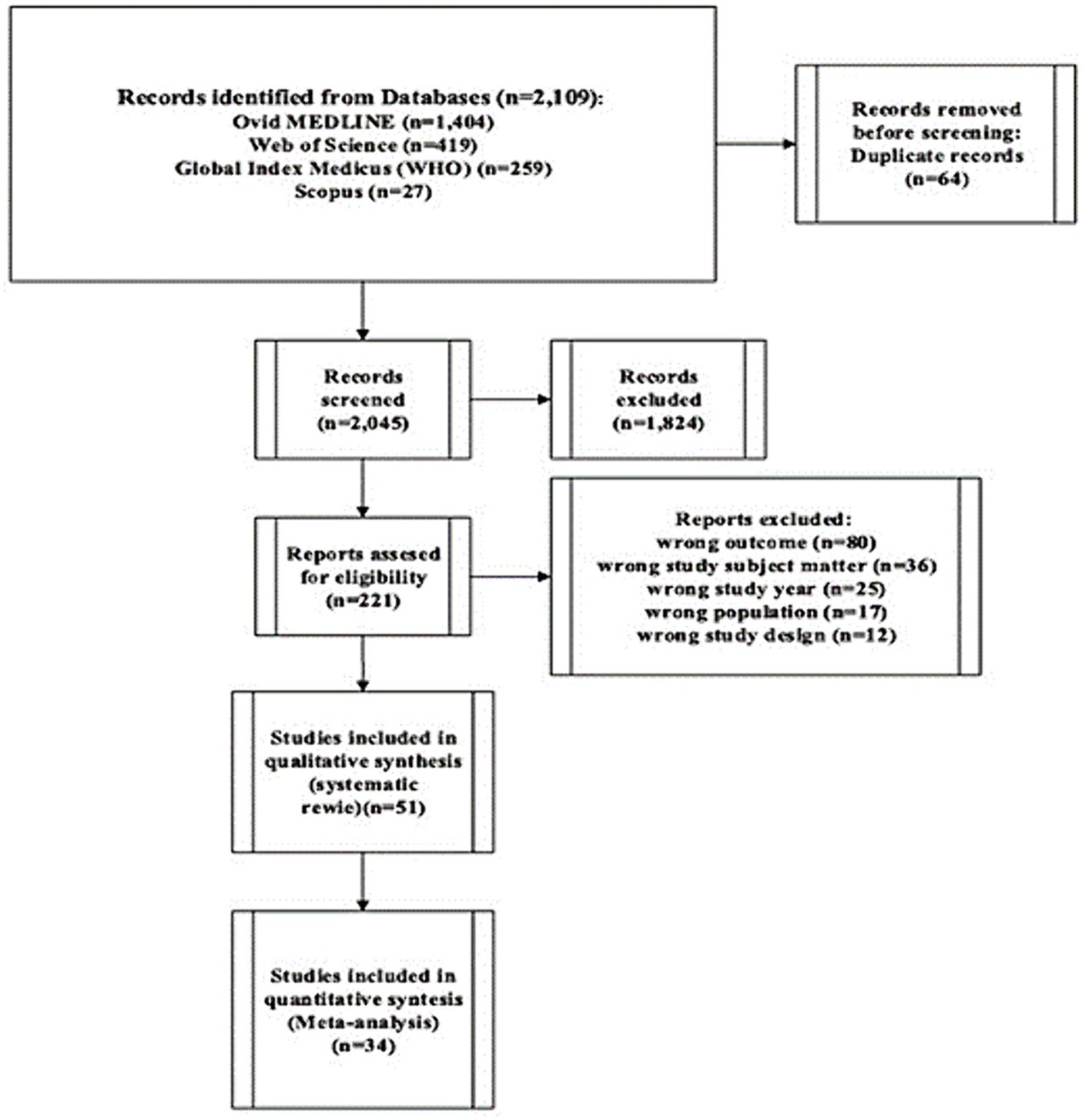
Figure 1. PRISMA flow diagram indicating study selection.
All studies were conducted in low-income and lower-middle-income countries. The age of the participants in the included studies ranged from 15–49 years. The types of maternal health care services were antenatal care in 14 studies, skilled delivery care in 14 studies, postnatal care in 3 studies, and in another 20 studies, the services were at least two of maternal health care services mentioned above (Table 2).
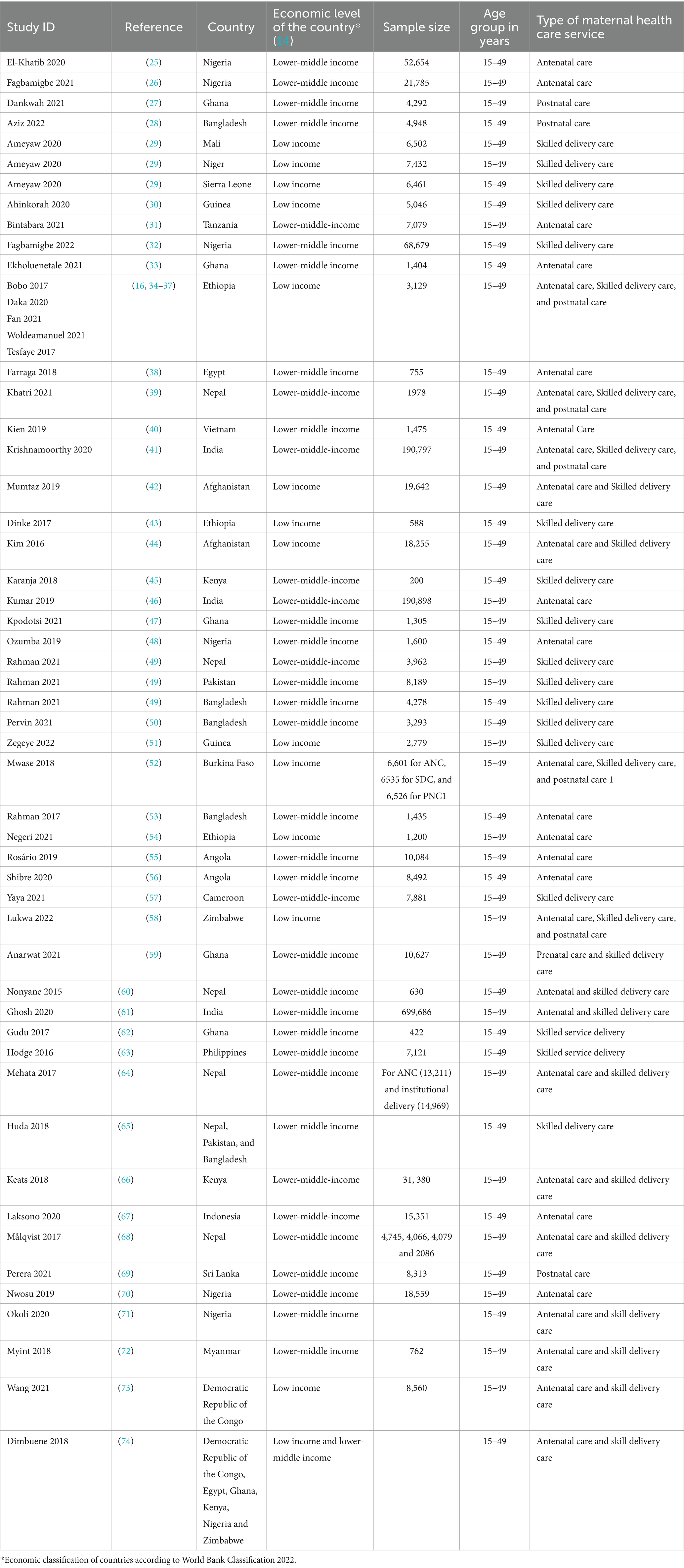
Table 2. Key characteristics of included studies.
The number of women investigated in the included studies ranged from 200 (45) to 699,686 (61). Funnel plots were used to assess reporting bias and investigate small-study effects. The findings from funnel plots indicated symmetrical funnel plots which in turn shows the absences of publication bias (Supplementary material).
Results of the meta-analyses
Antenatal care utilization
Utilization of antenatal care by place of residence
For the place of residence, utilization of antenatal care favors mothers living in urban places than those living in rural places. So, when compared to mothers living in rural areas, mothers living in urban areas utilize antenatal care three times more likely (OR 2.95; 95% CI 2.23, to 3.89; 15 studies; 340,390 participants; p < 0.00001) (Figure 2).
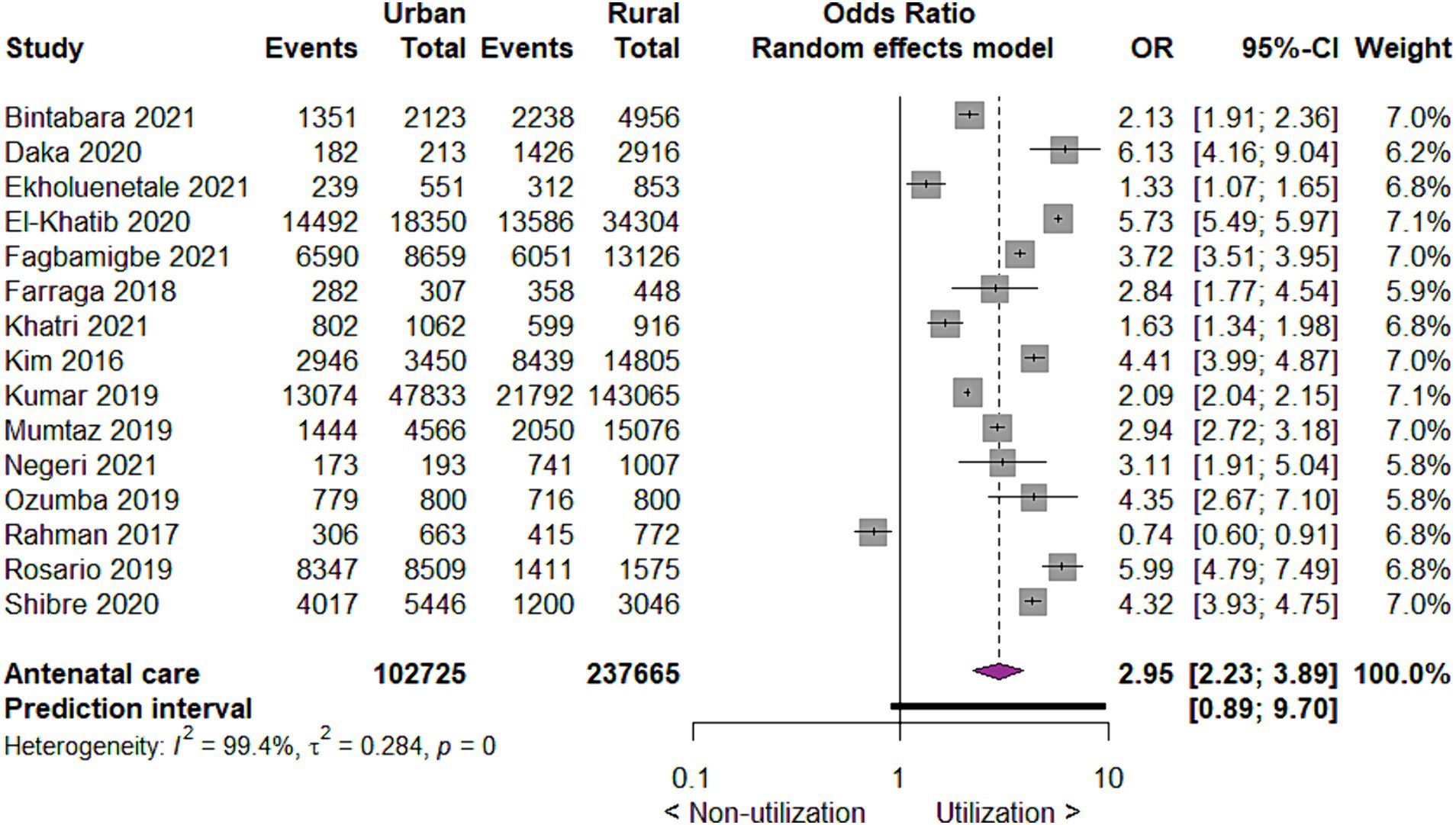
Figure 2. Forest plot showing antenatal care utilization by place of residence in developing countries, 2015 to 2022.
Utilization of antenatal care by the educational status of mothers
For the utilization of antenatal care in relation to the educational status of the mothers, we found that compared to no education, those with primary education utilize antenatal care two times more likely (OR 2.36; 95% CI 1.80 to 3.09; 9 studies; 154,398 participants p < 0.00001). Similarly, compared to mothers with no education, those with secondary and higher education utilized antenatal care six times (OR 6.00; 95% CI 4.13 to 8.73; 9 studies, 154,398 participants, p < 0.00001) and fourteen times (OR 14.27; 95% CI 7.93, 25.67; 9 studies, 154,398 participants, p < 0.00001) more likely, respectively, p < 0.00001 (Figure 3).
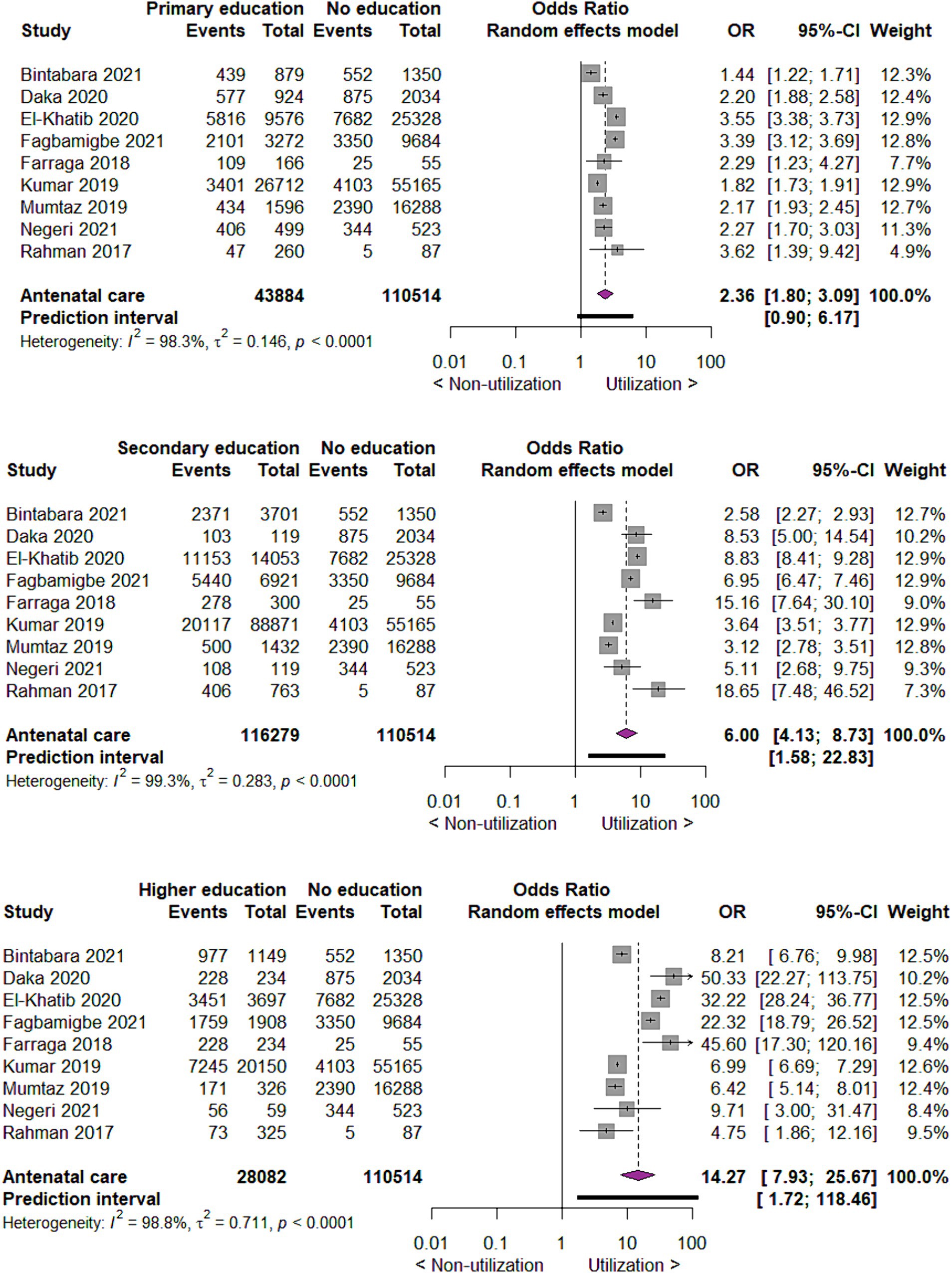
Figure 3. Forest plot showing antenatal care utilization by educational status of mothers in developing countries, 2015 to 2022.
Utilization of antenatal care by wealth index
When we investigated the utilization of antenatal care by wealth index of mothers, we found that compared to mothers with the lowest wealth index, those with the second wealth index utilize antenatal care two times more likely (OR 1.62; 95% CI 1.36 to 1.91; 10 studies; 224,530 participants; p < 0.00001). Those in middle, fourth and highest wealth index utilize antenatal care two times (OR 2.41; 95% CI 1.86 to 3.12; 10 studies 211,910 participants; p < 0.00001), four times (OR 3.73; 95% CI 2.63, 5.29; 10 studies 201,060 participants; p < 0.00001) and seven times (OR 6.72; 95% CI 4.26, 10.59; 10 studies 191,207 participants; p < 0.00001) more likely as compared to mothers in lowest wealth index, respectively (Figure 4).
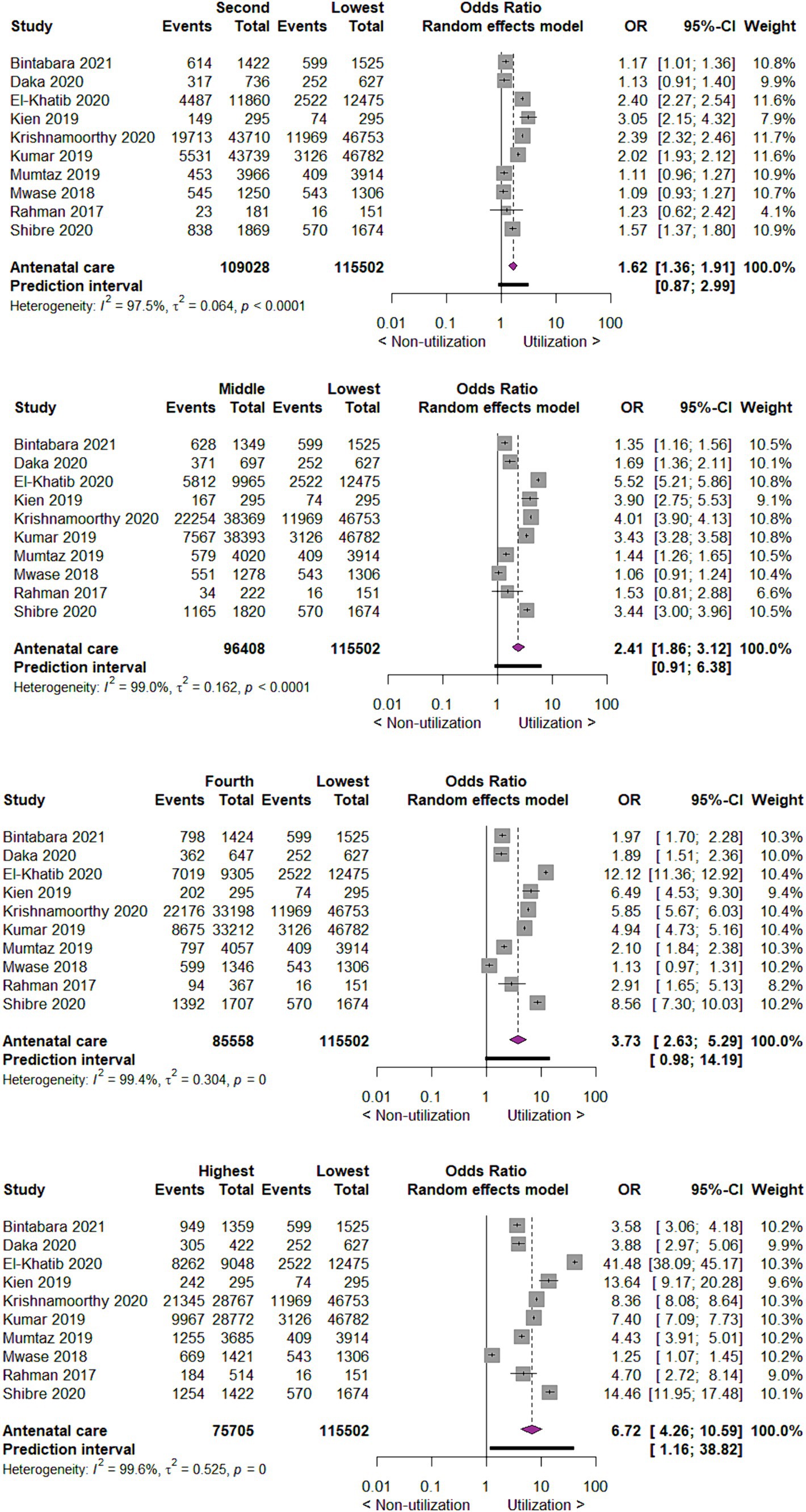
Figure 4. Forest plot showing antenatal care utilization by wealth index of mothers in developing countries, 2015 to 2022.
Skilled delivery care utilization
Utilization of skilled delivery care by place of residence
When we investigated the uptake of skilled delivery care by place of residence, the results indicated that mothers living in urban areas utilize skilled delivery care six times more likely than those mothers living in rural areas (OR 6.33; 95% CI 4.95 to 8.09; 16 studies, 166,085 participants; p < 0.00001) (Figure 5).
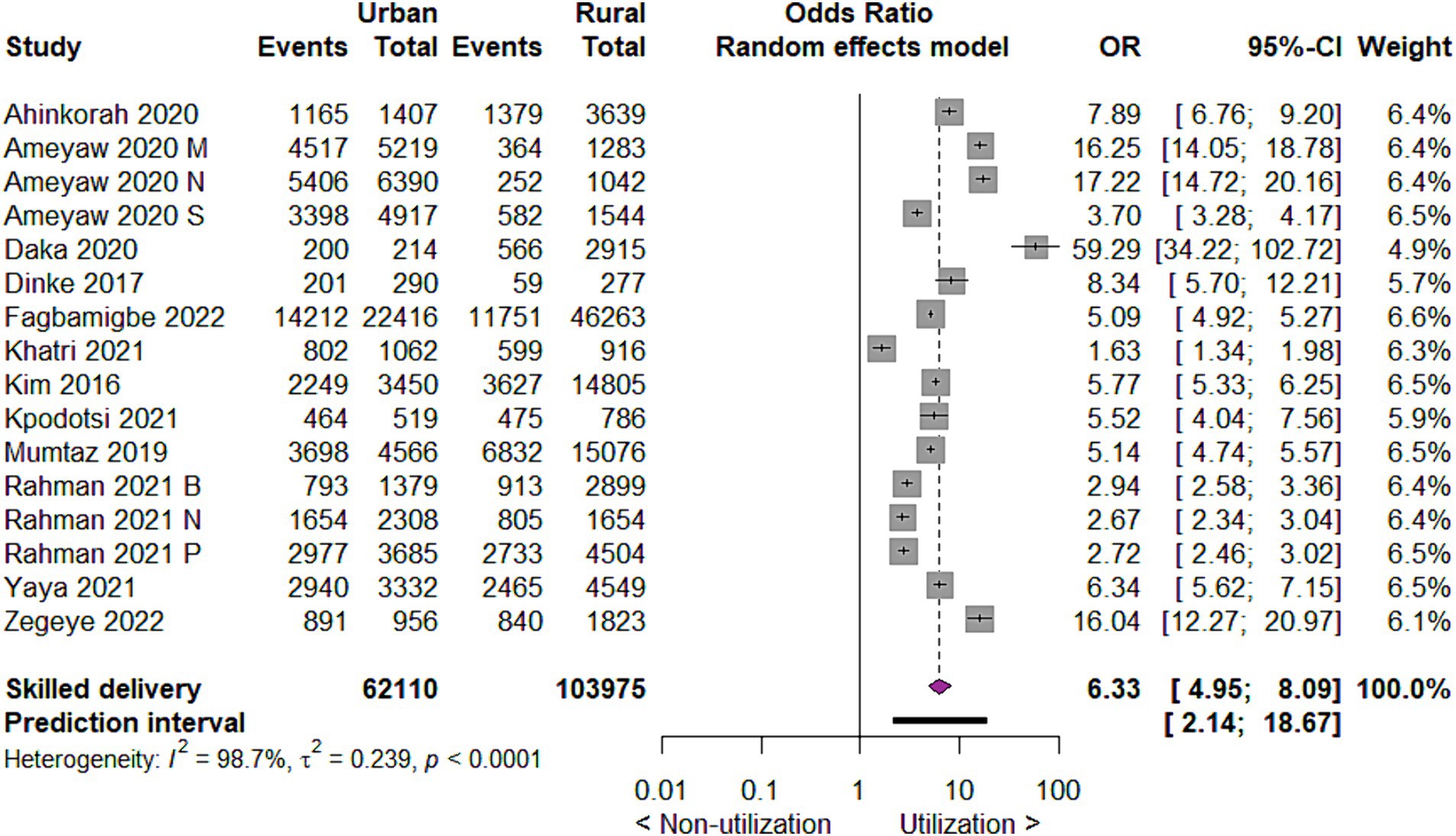
Figure 5. Forest plot showing skilled delivery care utilization by place of residence in developing countries, 2015 to 2022.
Utilization of skilled delivery care by the educational status of mothers
As to the utilization of skilled delivery care by the educational status of mothers, we found that compared to those with no education, those with primary education utilized skilled delivery care three times more likely (OR 2.49; 95% CI 1.89 to 3.29; 9 studies; 53,182 participants, p < 0.00001). Those with secondary and higher education utilized skilled delivery care seven times (OR 6.59; 95% CI 4.24 to 10.26; 9 studies, 53,726 participants, p < 0.00001) and twenty-seven times (OR = 26.53; 95% CI = 16.44, 42.83; 9 studies; 45,880 participants, p < 0.00001) more likely than mothers with no education, respectively (Figure 6).
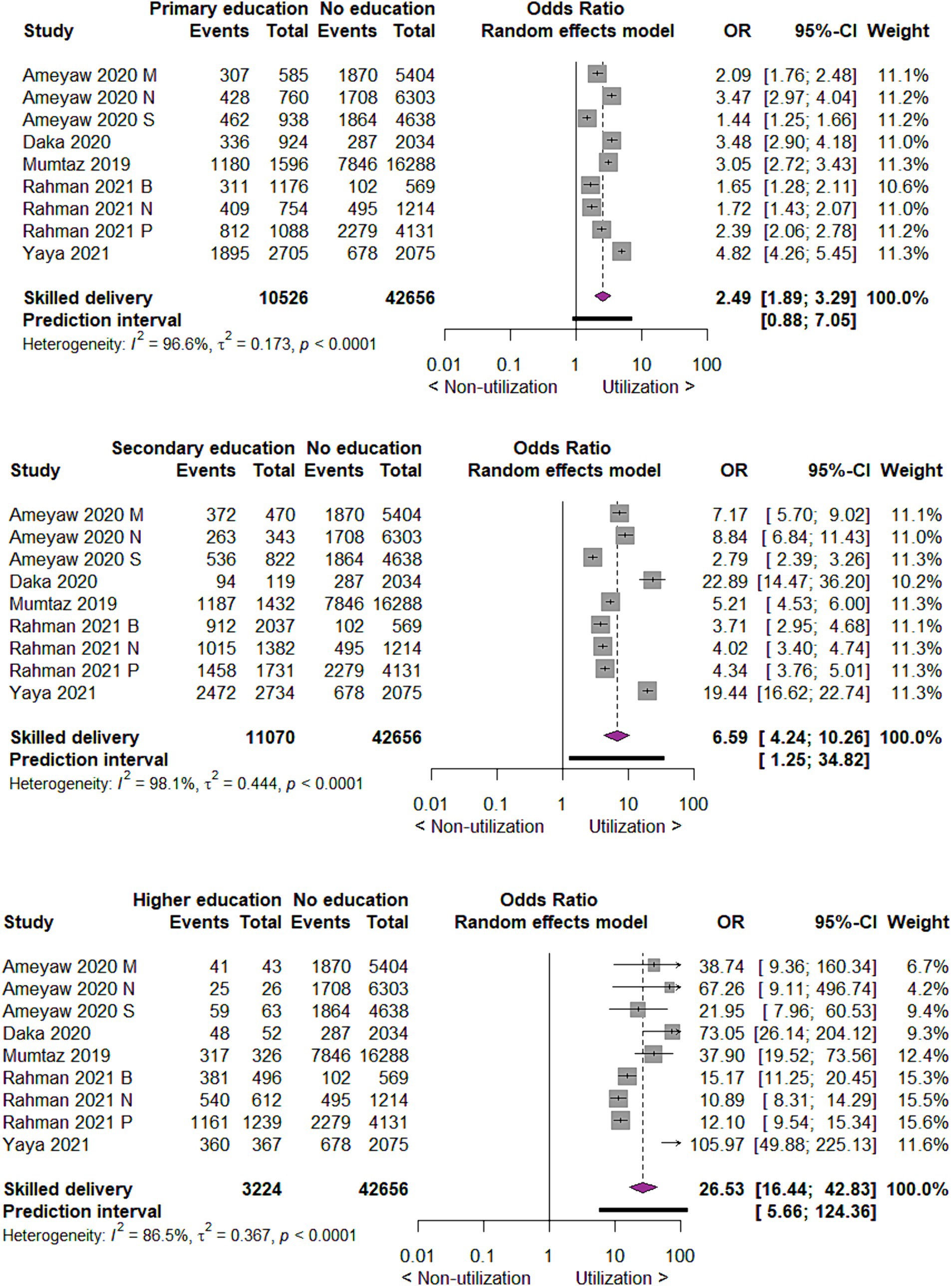
Figure 6. Forest plot showing skilled delivery care utilization by educational status of mothers in developing countries, 2015 to 2022.
Utilization of skilled delivery care by wealth index
Concerning utilization of skilled delivery care by wealth index of mothers, we found that compared to mothers with the lowest wealth index, those with the second wealth index utilize skilled delivery care two times more likely (OR 1.89; 95% CI 1.66 to 2.15; 14 studies; 151,578 participants; p < 0.00001). Those mothers in the middle, fourth, and highest wealth index utilized skilled delivery care three times.
(OR 2.96; 95% CI 2.25 to 3.89; 14 studies; 144,116 participants; p < 0.00001), seven times (OR 6.51; 95% CI 4.59 to 9.24; 14 studies; 137,236; p < 0.00001) and eighteen times (OR 17.80; 95% CI 11.36 to 27.89; 14 studies; 129,419; p < 0.00001) are more likely as compared to mothers in lowest wealth index, respectively (Figure 7).
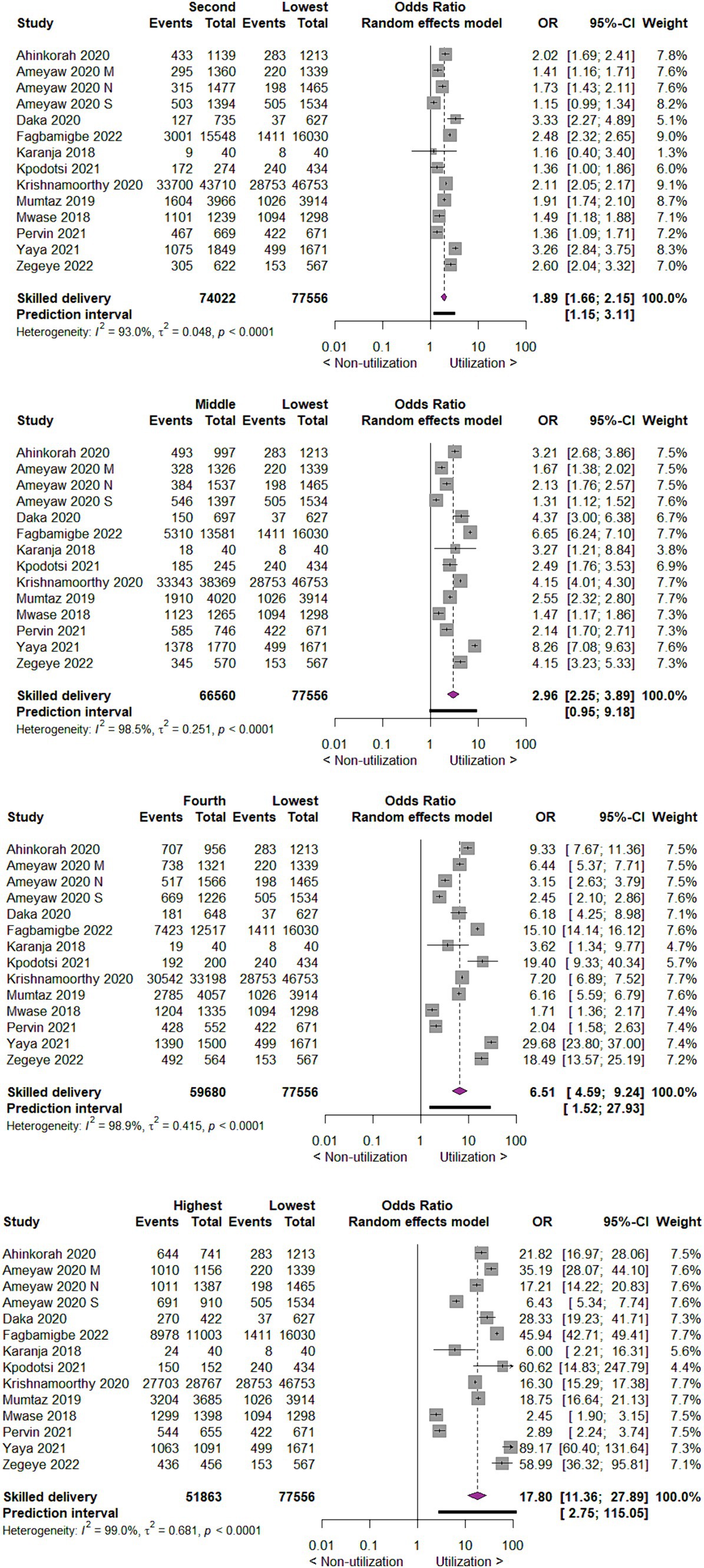
Figure 7. Forest plot showing skilled delivery care utilization by wealth index of mothers in developing countries, 2015 to 2022.
Postnatal care utilization
Utilization of postnatal care by place of residence
As to utilization of postnatal care by place of residence, we found that urban mothers are three times more likely to utilize postnatal care than rural mothers (OR 2.74; 95% CI 1.98 to 3.78; 4 studies; 14,347; p < 0.00001) (Figure 8).
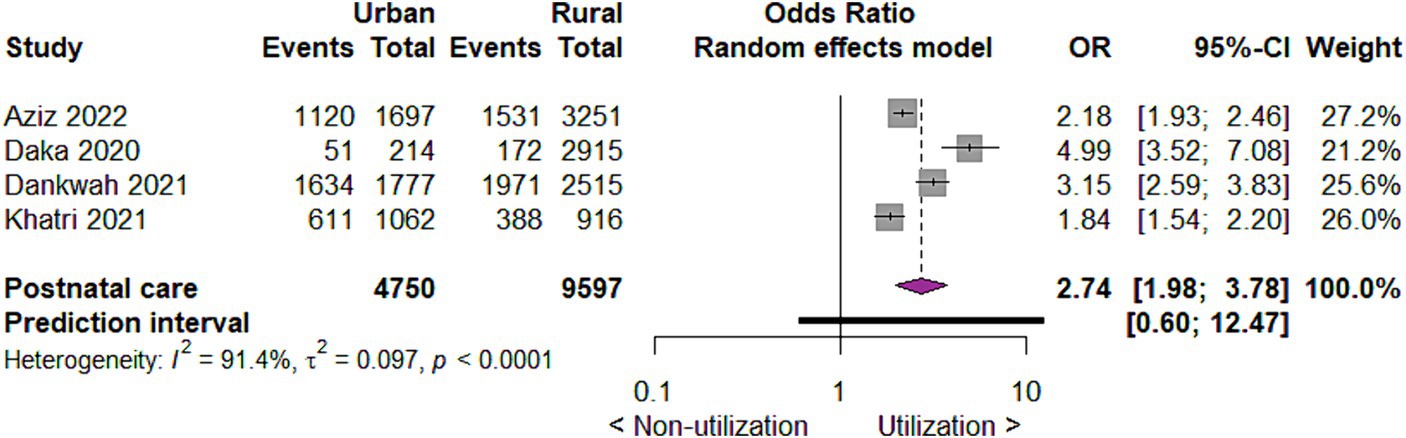
Figure 8. Forest plot showing postnatal care utilization by place of residence in developing countries, 2015 to 2022.
Utilization of postnatal care by educational status of mothers
Concerning the utilization of postnatal care by the educational status of mothers, we found that compared to no education, those with primary education utilize postnatal care two times more likely (OR 1.99; 95% CI 0.78 to 5.04; 2 studies; 4,642 participants; p = 0.15). Those with secondary education utilize postnatal care five times (OR 5.27; 95% CI 1.78 to 15.60; 2 studies; 4,828 participants; p = 0.003) and those with higher education ten times (OR 9.66; 95% CI 7.39 to 12.63, 2 studies; 3,289 participants; p < 0.00001) more likely than mothers with no education (Figure 9).
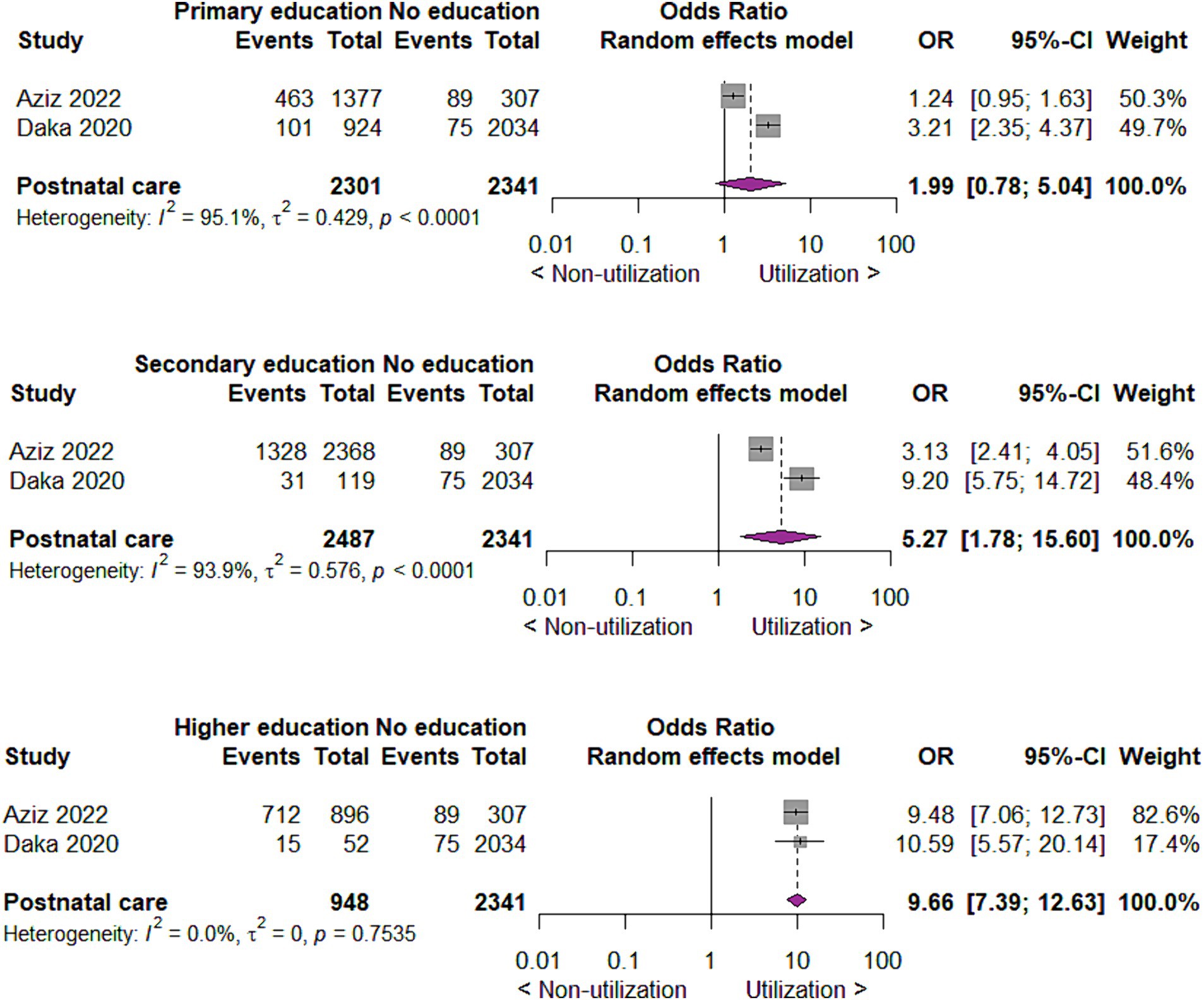
Figure 9. Forest plot showing postnatal care utilization by educational status of mothers in developing countries, 2015 to 2022.
Utilization of postnatal care by wealth index
For the utilization of postnatal care by wealth index of mothers, we found that compared to mothers with the lowest wealth index, those with second wealth index utilize postnatal care two times more likely (OR 1.46; 95% CI 1.10, 1.96; 4 studies; 96,432 participants; p = 0.01). In the same way, compared to mothers in lowest wealth index, those in middle, fourth and highest wealth index utilize postnatal care two times (OR 2.01; 95% CI 1.39, 2.91; 4 studies; 90,962 participants; p = 0.0002), three times (OR 2.62; 95% CI 1.55, 4.44; 4 studies; 85,894 participants; p = 0.0003) and five times (OR 5.06; 95% CI 2.45, 10.45; 4 studies; 81,335 participants; p < 0.0001) more likely, respectively (Figure 10).
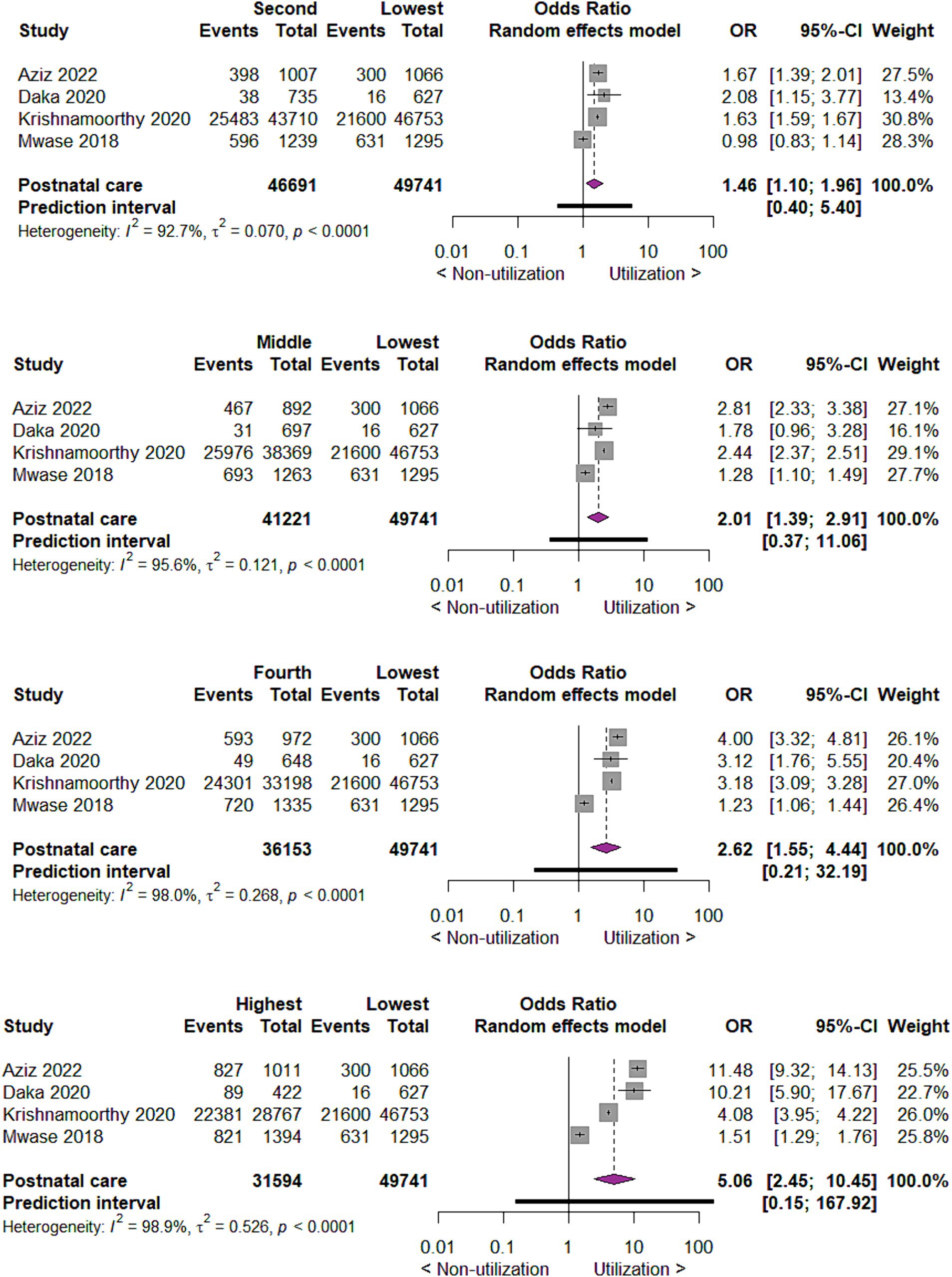
Figure 10. Forest plot showing postnatal care utilization by wealth index of mothers in developing countries, 2015 to 2022.
Additional results from studies not included in meta-analyses
A total of 17 studies were not included in the meta-analysis, but their findings were summarized for the qualitative synthesis only. In these studies, the outcomes were not reported as frequencies or percentages. However, the result agrees with the result from a meta-analysis.
Utilization of antenatal care and skilled delivery care by the educational status of mothers
Among the 17 studies examined, 6 studies have indicated that education has a direct effect on antenatal care and skilled delivery care utilization. Notably, in Ghana, women with secondary school education or higher were more inclined to receive prenatal and skilled delivery care compared to those without formal education (59). Similarly, in Northern Ghana, the educational attainment of mothers significantly correlated with the utilization of skilled delivery services (62).
In Indonesia, evidence indicates that education plays a crucial role in influencing women to undergo more than four antenatal care visits (67). Moreover, in Congo, a higher level of education was associated with increased utilization of antenatal care (73).
A comprehensive study across five African countries demonstrated a positive link between women’s education and various aspects of maternal health care, including the type of antenatal care provider, timing and frequency of antenatal care visits, delivery location, and presence of a skilled birth attendant (74). In Nigeria, the research suggested a consistently higher concentration of maternal healthcare usage among well-educated and wealthier mothers throughout the study period (71).
Utilization of antenatal care and skilled delivery care by wealth index
Out of 17 studies, 10 studies have highlighted the correlation between the wealth index and the utilization of antenatal care and skilled delivery care. Research conducted in Nepal revealed an escalating trend in the utilization of skilled delivery care and antenatal care as the wealth index of mothers transitions from the poorest to the least poor (60). The ratio of utilization for four ANC visits and institutional delivery between the richest and the poorest quintile mothers were 5.08 and 9.00, respectively, (64). Additionally, women from low socioeconomic backgrounds were six times more likely to deliver without skilled assistance compared to those from high socioeconomic backgrounds (68).
In India, the probability of having at least four ANC visits is nearly four times higher for women in the richest households than for those in the poorest households (61). In the Philippines, facility-based delivery coverage was higher for non-poor households compared to poor households (63). A study across three different Asian countries revealed a pro-rich inequality in the use of facility delivery services (65).
For skilled birth attendance and four or more antenatal care visits in Kenya, the absolute difference in coverage between the wealthiest quintile (quintile 5) and poorest quintile (quintile 1) was 61.6 and 31.0%, respectively (66).
In Zimbabwe, women from middle-income and richest households were more likely to utilize antenatal care services than women from the poorest households. Maternal service utilization in Zimbabwe exhibited a pro-rich pattern, indicating a preference for maternal health care utilization among women from wealthy households (58). In Nigeria, the concentration of at least four ANC visits and a higher number of ANC visits were disproportionately higher among the rich (70). Similarly, in Myanmar, the utilization of skilled birth attendants (SBAs) among women was disproportionately concentrated among the affluent, irrespective of maternal characteristics (72).
Utilization of postnatal care by residence
Out of 17 studies, 1 study has highlighted the correlation between the place of residence and the utilization of postnatal care. In Sri Lanka, mothers residing in rural areas are less inclined to receive Full Postnatal care (FPNC) in comparison to their counterparts in urban areas (69).
Discussion
In the present systematic review, we summarized up-to-date evidence about the utilization of maternal health care services, including antenatal care, skilled delivery care, and postnatal care in developing countries. In all three areas of maternal health care services, we have seen that place of residence, education, and wealth index are still important determinants, that is those living in urban areas, having a higher education level, or a higher wealth index utilize maternal health services more often. The greater the difference in education or wealth between the two groups, the greater the difference in the use of maternal health care services between them. The results of this systematic review and meta-analysis clearly indicate that there is a relative inequity in the utilization of antenatal care, skilled delivery care, and postnatal care for mothers in developing countries.
To our knowledge, this is the first systematic review summarizing available evidence on inequity in the uptake of maternal health care services in developing countries not only in a narrative way but also quantitatively, by including meta-analyses. As compared to previous systematic reviews the present systematic review does not only focus on a specific maternal health care service but includes antenatal care, skilled delivery care, as well as postnatal care. Other strengths include a comprehensive search strategy, conducted in electronic databases without imposing language restrictions. This way we think, the likelihood of overlooking published studies was minimal, although there was a potential for missing unpublished ones. We aimed to reduce bias wherever possible by having at least two review authors work independently on study selection, data extraction, and risk of bias assessments.
A previous systematic review carried out on equity in maternal healthcare service utilization in developing countries investigated studies published between 2005 and 2015 (20). The present systematic review summarizes evidence for the period 2015 to 2022. Although the results of these two systematic reviews are only partially comparable due to the more limited questioning and lack of quantitative analysis in the previous review, it can be concluded that inequity in the uptake of maternal health care services described earlier persists in developing countries.
Several interventions might be potentially effective in reducing inequalities in maternal and child health in low- and middle-income settings. Besides immunization campaigns, nutrition supplement programs, and demand-side interventions, healthcare provision improvement interventions are tested in different countries, including different health programs, which aim to improve the uptake of maternal and child healthcare services (75). In Tanzania, simple guidelines, and messages for use in primary health facilities and communities were developed (76). In Brazil, the family health program was introduced, where multi-professional teams were working under the principles of comprehensive care and provided permanent and systematic follow-up of high-risk families residing in a pre-specified area with high infant mortality rates (77). In Bangladesh, voluntary community health workers provide intensive home-based maternal and newborn care. This program aimed to increase the utilization of antenatal care and to train attendants for home delivery (78). Another program addressing both the demand side (education about the benefits of ANC and PNC visits, pathologic signs related to pregnancy and delivery) and supply side interventions (strengthening health facilities, providing trained personnel and equipment) was able to successfully improve the utilization of maternal health services and reduce inequalities (79). In Indonesia, midwives were trained and posted in every village with specific responsibility for pregnancy, delivery, and postpartum care. This way this program focused on inequities in antenatal care check-ups and birth attendance by trained professionals (80). Although the evidence level is generally low, all these programs seemed to be effective in achieving results in the field of equity of maternal and child health care services.
When designing and implementing interventions to reduce inequalities in access to maternal and newborn care, the 5As framework of access developed by Penchansky and Thomas should be borne in mind. They argue that access to care is simultaneously dependent on affordability, availability, accessibility, accommodation, and acceptability (81). These five aspects of access form a chain that is no stronger than its weakest link, so interventions that target only one or two of them may not reduce inequality at all (82, 83). In general, Changes in social determinants of health at the societal level can only be brought about by systemic, complex interventions. The obstacles to decisions leading to such measures are a lack of recognition of the problems, short-term political interests, and limited resources (84, 85).
Further research should be conducted to delve deeper into the effectiveness of the above-mentioned and additional interventions to improve the uptake of maternal health care services. The effectiveness of these interventions should be investigated separately for the different sociodemographic groups. These studies and sub-group analyses might facilitate targeted interventions in the most vulnerable groups. Governments should use the results of research activities to plan the implementation of programs. Progress in equity should be monitored, and recommendations should be forwarded to concerned bodies periodically. In most developing countries, there are demographic and health surveillance sites where demographic and health data are collected, analyzed, and reported regularly. Therefore, monitoring health inequity should be incorporated in these sites as one theme. In summary, this systematic review and meta-analysis synthesized data from 51 cross-sectional studies analyzing the uptake of maternal health care services in developing countries. The findings revealed a consistent and statistically significant effect of place of residence, education, and wealth index of mothers on the uptake of maternal health care services indicating persistence of relative inequity in utilization in developing countries. Currently, the services are mostly utilized by mothers who reside in urban areas, are more educated, and have the highest wealth index. Based on the conclusions of the literature synthesis, recommendations can be formulated for health policy that could increase the uptake of maternity services and reduce inequalities. The article may draw the attention of health policy makers to the fact that the low uptake and inequalities in maternal health care cannot be improved by interventions in the health sector alone, i.e., intersectoral action is needed.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Author contributions
AG: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Resources, Software, Visualization, Writing – original draft, Writing – review & editing. EM: Investigation, Methodology, Resources, Visualization, Writing – review & editing. JV: Resources, Supervision, Visualization, Writing – review & editing. SL: Formal analysis, Investigation, Methodology, Resources, Software, Supervision, Validation, Visualization, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Acknowledgments
Our sincere thanks go to the University of Pécs, Doctoral School of Health Sciences for the provision of easy access to the databases.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2024.1415092/full#supplementary-material
References
1. Arcaya, MC, Arcaya, AL, and Subramanian, SV. Inequalities in health: definitions, concepts, and theories. Glob Health Action. (2015) 8:27106. doi: 10.3402/gha.v8.27106
2. Barreto, ML. Health inequalities: a global perspective. Ciênc Saúde Colet. (2017) 22:2097–108. doi: 10.1590/1413-81232017227.02742017
3. Whitehead, M. The concepts and principles of equity and health. Int J Health Serv. (1992) 22:429–45. doi: 10.2190/986L-LHQ6-2VTE-YRRN
4. Marmot, M, Allen, J, Bell, R, Bloomer, E, and Goldblatt, PConsortium for the European Review of Social Determinants of Health and the Health Divide. WHO European review of social determinants of health and the health divide. Lancet. (2012) 380:1011–29. doi: 10.1016/S0140-6736(12)61228-8
5. Lima Figueiredo, ER, do Socorro Carvalho Miranda, C, Viana Campos, AC, de Campos Gomes, F, Câmara Rodrigues, CN, and de Melo-Neto, JS. Influence of sociodemographic and obstetric factors on maternal mortality in Brazil from 2011 to 2021. BMC Womens Health. (2024) 24:84. doi: 10.1186/s12905-024-02925-3
6. Tey, N-P, and Lai, S-L. Correlates of and barriers to the utilization of health Services for Delivery in South Asia and sub-Saharan Africa. Sci World J. (2013) 2013:423403. doi: 10.1155/2013/423403
7. WHO, Ending preventable maternal mortality (EPMM): a renewed focus for improving maternal and newborn health and well-being, WHO, Editor. (2021), WHO.
8. WHO, Trends in maternal mortality, (2000), To 2020: Estimates by WHO, UNICEF, UNFPA. Geneve, Switzerland: World Bank Group and UNDESA/Population Division. (2023).
9. Souza, JP, Day, LT, Rezende-Gomes, AC, Zhang, J, Mori, R, Baguiya, A, et al. A global analysis of the determinants of maternal health and transitions in maternal mortality. Lancet Glob Health. (2024) 12:e306–16. doi: 10.1016/S2214-109X(23)00468-0
10. Boerma, T, Campbell, OMR, Amouzou, A, Blumenberg, C, Blencowe, H, Moran, A, et al. Maternal mortality, stillbirths, and neonatal mortality: a transition model based on analyses of 151 countries. Lancet Glob Health. (2023) 11:e1024–31. doi: 10.1016/S2214-109X(23)00195-X
11. Tsawe, M, Moto, A, Netshivhera, T, Ralesego, L, Nyathi, C, and Susuman, AS. Factors influencing the use of maternal healthcare services and childhood immunization in Swaziland. Int J Equity Health. (2015) 14:32. doi: 10.1186/s12939-015-0162-2
12. Alkenbrack, S, Chaitkin, M, Zeng, W, Couture, T, and Sharma, S. Did equity of reproductive and maternal health service coverage increase during the MDG era? An analysis of trends and determinants across 74 low- and middle-income countries. PLoS One. (2015) 10:e0134905. doi: 10.1371/journal.pone.0134905
13. UNICEF, Analysis of reproductive, maternal, newborn, child and adolescent health inequities in Latin America and the Caribbean to inform policymaking summary report, Health Equity Report 2016, (2016). UNICEF Panama, Republic of Panama.
14. WBG. Data: World Bank Country and Lending Groups, (2024), Available at: https://datahelpdesk.worldbank.org/knowledgebase/articles/906519-world-bank-country-and-lending-groups
15. Mahler, DG, and Serajuddin, AH Umar. Time to stop referring to the “developing world.”. 2024 (cited 2024 24/05/2024).
16. Daka, DW, Woldie, M, Ergiba, MS, Sori, BK, Bayisa, DA, Amente, AB, et al. Inequities in the uptake of reproductive and maternal health Services in the Biggest Regional State of Ethiopia: too far from "leaving no one behind". Clinicoecon Outcomes Res. (2020) 12:595–607. doi: 10.2147/CEOR.S269955
17. Ahmed, S, Creanga, AA, Gillespie, DG, and Tsui, AO. Economic status, education and empowerment: implications for maternal health service utilization in developing countries. PLoS One. (2010) 5:e11190. doi: 10.1371/journal.pone.0011190
18. WHO/UNICEF, Global indicator framework for the Sustainable Development Goals and targets of the 2030, (2018), Agenda for Sustainable Development.
20. Çalışkan, Z, Kılıç, D, Öztürk, S, and Atılgan, E. Equity in maternal health care service utilization: a systematic review for developing countries. Int J Public Health. (2015) 60:815–25. doi: 10.1007/s00038-015-0711-x
21. Shanto, HH, al-Zubayer, MA, Ahammed, B, Sarder, MA, Keramat, SA, Hashmi, R, et al. Maternal healthcare services utilisation and its associated risk factors: a pooled study of 37 low- and middle-income countries. Int J Public Health. (2023) 68:1606288. doi: 10.3389/ijph.2023.1606288
22. Moher, D, Liberati, A, Tetzlaff, J, and Altman, DGThe PRISMA Group. Preferred reporting items for systematic reviews and Meta-analyses: the PRISMA statement. PLoS Med. (2009) 6:e1000097. doi: 10.1371/journal.pmed.1000097
23. HealthCare.gov. Glossary 2024 [cited 2024 24/05/2024].
24. Moola, S., Munn, Z., Tufanaru, C., Aromataris, E., Sears, K., Sfetic, R., et al., Chapter 7: Systematic reviews of etiology and risk: JBI manual for evidence synthesis JBI, editor. (2020).
25. el-Khatib, Z, Kolawole Odusina, E, Ghose, B, and Yaya, S. Patterns and predictors of insufficient antenatal care utilization in Nigeria over a decade: a pooled data analysis using demographic and health surveys. Int J Environ Res Public Health. (2020) 17:8261. doi: 10.3390/ijerph17218261
26. Fagbamigbe, AF, Olaseinde, O, and Setlhare, V. Sub-national analysis and determinants of numbers of antenatal care contacts in Nigeria: assessing the compliance with the WHO recommended standard guidelines. BMC Pregnancy Childbirth. (2021) 21:402. doi: 10.1186/s12884-021-03837-y
27. Dankwah, E, Feng, C, Kirychuck, S, Zeng, W, Lepnurm, R, and Farag, M. Assessing the contextual effect of community in the utilization of postnatal care services in Ghana. BMC Health Serv Res. (2021) 21:40. doi: 10.1186/s12913-020-06028-1
28. Aziz, S, Basit, A, Sultana, S, Homer, CSE, and Vogel, JP. Inequalities in women’s utilization of postnatal care services in Bangladesh from 2004 to 2017. Sci Rep. (2022) 12:2747. doi: 10.1038/s41598-022-06672-z
29. Ameyaw, EK, and Dickson, KS. Skilled birth attendance in Sierra Leone, Niger, and Mali_ analysis of demographic and health surveys. BMC Public Health. (2020) 20:164. doi: 10.1186/s12889-020-8258-z
30. Ahinkorah, BO. Non-utilization of health facility delivery and its correlates among childbearing women: a cross-sectional analysis of the 2018 Guinea demographic and health survey data. BMC Health Serv Res. (2020) 20:1016. doi: 10.1186/s12913-020-05893-0
31. Bintabara, D, and Basinda, N. Twelve-year persistence of inequalities in antenatal care utilisation among women in Tanzania: a decomposition analysis of population-based cross-sectional surveys. BMJ Open. (2021) 11:e040450. doi: 10.1136/bmjopen-2020-040450
32. Fagbamigbe, AF, and Oyedele, OK. Multivariate decomposition of trends, inequalities and predictors of skilled birth attendants utilisation in Nigeria (1990–2018): a cross-sectional analysis of change drivers. BMJ Open. (2022) 12:e051791. doi: 10.1136/bmjopen-2021-051791
33. Ekholuenetale, M, Nzoputam, CI, and Barrow, A. Prevalence and socioeconomic inequalities in eight or more antenatal care contacts in Ghana: findings from 2019 population-based data. Int J Women’s Health. (2021) 13:349–60. doi: 10.2147/IJWH.S306302
34. Fan, Q, Roque, M, Nuzhath, T, Hossain, MM, Jin, X, Aggad, R, et al. Changes in levels and determinants of maternal health service utilization in Ethiopia: comparative analysis of two rounds Ethiopian demographic and health surveys. Matern Child Health J. (2021) 25:1595–606. doi: 10.1007/s10995-021-03182-8
35. Bobo, FT, Yesuf, EA, and Woldie, M. Inequities in utilization of reproductive and maternal health services in Ethiopia. Int J Equity Health. (2017) 16:105. doi: 10.1186/s12939-017-0602-2
36. Woldeamanuel, BT, and Aga, MA. Trends, regional inequalities and determinants in the utilization of prenatal care and skilled birth attendant in Ethiopia: a multilevel analysis. Clin Epidemiol Global Health. (2021) 11:100771. doi: 10.1016/j.cegh.2021.100771
37. Tesfaye, B, Mathewos, T, and Kebede, M. Skilled delivery inequality in Ethiopia: to what extent are the poorest and uneducated mothers benefiting? Int J Equity Health. (2017) 16:82. doi: 10.1186/s12939-017-0579-x
38. Farrag, NS, Abdelwahab, F, and Ismail, GR. Patterns and factors affecting antenatal care utilization in Damietta governorate, Egypt: a retrospective cross-sectional study. Fam Pract. (2018) 36:479–85. doi: 10.1093/fampra/cmy105
39. Khatri, RB, Alemu, Y, Protani, MM, Karkee, R, and Durham, J. Intersectional (in) equities in contact coverage of maternal and newborn health services in Nepal: insights from a nationwide cross-sectional household survey. BMC Public Health. (2021) 21:1098. doi: 10.1186/s12889-021-11142-8
40. Kien, VD, Jat, TR, Phu, TV, Cuong, LM, Anh, VTM, Chu, NV, et al. Trends in socioeconomic inequalities in the use of antenatal care services by women aged 15 to 49 years in Vietnam. Asia Pacific J Publ Health. (2019) 31:413–21. doi: 10.1177/1010539519857305
41. Krishnamoorthy, Y, Majella, MG, and Rajaa, S. Equity in coverage of maternal and newborn care in India: evidence from a nationally representative survey. Health Policy Plan. (2020) 35:616–23. doi: 10.1093/heapol/czaa020
42. Mumtaz, S, Bahk, J, and Khang, Y-H. Current status and determinants of maternal healthcare utilization in Afghanistan: analysis from Afghanistan demographic and health survey 2015. PLoS One. (2019) 14:e0217827. doi: 10.1371/journal.pone.0217827
43. Dinke, K, and Hunduma, J. Urban-rural disparity and determinants of delivery care utilization in Oromia region, Ethiopia: community-based cross-sectional study. Int J Nurs Pract. (2017) 23:23. doi: 10.1111/ijn.12510
44. Kim, C, Saeed, KMA, Salehi, AS, and Zeng, W. An equity analysis of utilization of health services in Afghanistan using a national household survey. BMC Public Health. (2016) 16:1226. doi: 10.1186/s12889-016-3894-z
45. Karanja, S, Gichuki, R, Igunza, P, Muhula, S, Ofware, P, Lesiamon, J, et al. Factors influencing deliveries at health facilities in a rural Maasai Community in Magadi sub-county, Kenya. BMC Pregnancy Childbirth. (2018) 18:5. doi: 10.1186/s12884-017-1632-x
46. Kumar, G, Choudhary, TS, Srivastava, A, Upadhyay, RP, Taneja, S, Bahl, R, et al. Utilisation, equity and determinants of full antenatal care in India: analysis from the National Family Health Survey 4. BMC Pregnancy Childbirth. (2019) 19:327. doi: 10.1186/s12884-019-2473-6
47. Kpodotsi, A, Baku, EA, Adams, JH, and Alaba, O. Socioeconomic inequalities in access and use of skilled birth attendants during childbirth in Ghana: a decomposition analysis. BMC Pregnancy Childbirth. (2021) 21:850. doi: 10.1186/s12884-021-04290-7
48. Ozumba, BC, Onyeneho, NG, Chalupowski, M, and Subramanian, SV. Inequities in access to maternal health Care in Enugu State: implications for universal health coverage to meet vision 2030 in Nigeria. Int Q Community Health Educ. (2019) 39:163–73. doi: 10.1177/0272684X18819977
49. Rahman, MA, Rahman, MA, Rawal, LB, Paudel, M, Howlader, MH, Khan, B, et al. Factors influencing place of delivery: evidence from three south-Asian countries. PLoS One. (2021) 16:e0250012. doi: 10.1371/journal.pone.0250012
50. Pervin, J, Venkateswaran, M, Nu, UT, Rahman, M, O’Donnell, BF, Friberg, IK, et al. Determinants of utilization of antenatal and delivery care at the community level in rural Bangladesh. PLoS One. (2021) 16:e0257782. doi: 10.1371/journal.pone.0257782
51. Zegeye, B, Ahinkorah, BO, Ameyaw, EK, Budu, E, Seidu, AA, Olorunsaiye, CZ, et al. Disparities in use of skilled birth attendants and neonatal mortality rate in Guinea over two decades. BMC Pregnancy Childbirth. (2022) 22:56. doi: 10.1186/s12884-021-04370-8
52. Mwase, T, Brenner, S, Mazalale, J, Lohmann, J, Hamadou, S, Somda, SMA, et al. Inequities and their determinants in coverage of maternal health services in Burkina Faso. Int J Equity Health. (2018) 17:58. doi: 10.1186/s12939-018-0770-8
53. Rahman, A, Nisha, MK, Begum, T, Ahmed, S, Alam, N, and Anwar, I. Trends, determinants and inequities of 4+ ANC utilisation in Bangladesh. J Health Popul Nutr. (2017) 36:2. doi: 10.1186/s41043-016-0078-5
54. Negeri, MA. Magnitude and associated factors of antenatal care utilization in Western regions of Ethiopia: a study based on demographic and health survey data. J Pharmaceut Res Int. (2021) 33:23–9. doi: 10.9734/jpri/2021/v33i49A33297
55. Rosário, EVN, Gomes, MC, Brito, M, and Costa, D. Determinants of maternal health care and birth outcome in the Dande health and demographic surveillance system area, Angola. PLoS One. (2019) 14:e0221280. doi: 10.1371/journal.pone.0221280
56. Shibre, G, Zegeye, B, Idriss-Wheeler, D, Ahinkorah, BO, Oladimeji, O, and Yaya, S. Socioeconomic and geographic variations in antenatal care coverage in Angola: further analysis of the 2015 demographic and health survey. BMC Public Health. (2020) 20:1243. doi: 10.1186/s12889-020-09320-1
57. Yaya, S, Zegeye, B, Ahinkorah, BO, Seidu, AA, Ameyaw, EK, Adjei, NK, et al. Predictors of skilled birth attendance among married women in Cameroon: further analysis of 2018 Cameroon demographic and health survey. Reprod Health. (2021) 18:70. doi: 10.1186/s12978-021-01124-9
58. Lukwa, AT, Siya, A, Odunitan-Wayas, FA, and Alaba, O. Decomposing maternal socioeconomic inequalities in Zimbabwe; leaving no woman behind. BMC Pregnancy Childbirth. (2022) 22:239. doi: 10.1186/s12884-022-04571-9
59. Anarwat, SG, Salifu, M, and Akuriba, MA. Equity and access to maternal and child health services in Ghana a cross-sectional study. BMC Health Serv Res. (2021) 21:864. doi: 10.1186/s12913-021-06872-9
60. Nonyane, BA, Ashish, KC, Callaghan-Koru, JA, Guenther, T, Sitrin, D, Syed, U, et al. Equity improvements in maternal and newborn care indicators: results from the Bardiya district of Nepal. Health Policy Plan. (2015) 31:405–14. doi: 10.1093/heapol/czv077
61. Ghosh, A, and Ghosh, R. Maternal health care in India: a reflection of 10 years of National Health Mission on the Indian maternal health scenario. Sex Reprod Healthc. (2020) 25:100530. doi: 10.1016/j.srhc.2020.100530
62. Gudu, W, and Addo, B. Factors associated with utilization of skilled service delivery among women in rural northern Ghana: a cross sectional study. BMC Pregnancy Childbirth. (2017) 17:159. doi: 10.1186/s12884-017-1344-2
63. Hodge, A, Firth, S, Bermejo, R, Zeck, W, and Jimenez-Soto, E. Utilisation of health services and the poor: deconstructing wealth-based differences in facility-based delivery in the Philippines. BMC Public Health. (2016) 16:523. doi: 10.1186/s12889-016-3148-0
64. Mehata, S, Paudel, YR, Dariang, M, Aryal, KK, Lal, BK, Khanal, MN, et al. Trends and inequalities in use of maternal health Care Services in Nepal: strategy in the search for improvements. Biomed Res Int. (2017) 2017:5079234. doi: 10.1155/2017/5079234
65. Huda, TM, Hayes, A, and Dibley, MJ. Examining horizontal inequity and social determinants of inequality in facility delivery services in three south Asian countries. J Glob Health. (2018) 8:010416. doi: 10.7189/jogh.08.010416
66. Keats, EC, Akseer, N, Bhatti, Z, Macharia, W, Ngugi, A, Rizvi, A, et al. Assessment of inequalities in coverage of essential reproductive, maternal, newborn, child, and adolescent health interventions in Kenya. JAMA Netw Open. (2018) 1:e185152–2. doi: 10.1001/jamanetworkopen.2018.5152
67. Laksono, AD, Rukmini, R, and Wulandari, RD. Regional disparities in antenatal care utilization in Indonesia. PLoS One. (2020) 15:e0224006. doi: 10.1371/journal.pone.0224006
68. Målqvist, M, Pun, A, Raaijmakers, H, and KC, A. Persistent inequity in maternal health care utilization in Nepal despite impressive overall gains. Glob Health Action. (2017) 10:1356083. doi: 10.1080/16549716.2017.1356083
69. Perera, UAP, Assefa, Y, and Amilani, U. Postnatal care coverage and its determinants in Sri Lanka: analysis of the 2016 demographic and health survey. BMC Pregnancy Childbirth. (2021) 21:299. doi: 10.1186/s12884-021-03770-0
70. Nwosu, CO, and Ataguba, JE. Socioeconomic inequalities in maternal health service utilisation: a case of antenatal care in Nigeria using a decomposition approach. BMC Public Health. (2019) 19:1493. doi: 10.1186/s12889-019-7840-8
71. Okoli, C, Hajizadeh, M, Rahman, MM, and Khanam, R. Geographical and socioeconomic inequalities in the utilization of maternal healthcare services in Nigeria: 2003–2017. BMC Health Serv Res. (2020) 20:849. doi: 10.1186/s12913-020-05700-w
72. Myint, ANM, Liabsuetrakul, T, Htay, TT, Wai, MM, Sundby, J, and Bjertness, E. Inequity in the utilization of antenatal and delivery care in Yangon region, Myanmar: a cross-sectional study. Int J Equity Health. (2018) 17:63. doi: 10.1186/s12939-018-0778-0
73. Wang, H, Frasco, E, Takesue, R, and Tang, K. Maternal education level and maternal healthcare utilization in the Democratic Republic of the Congo: an analysis of the multiple indicator cluster survey 2017/18. BMC Health Serv Res. (2021) 21:850. doi: 10.1186/s12913-021-06854-x
74. Tsala Dimbuene, Z, Amo-Adjei, J, Amugsi, D, Mumah, J, Izugbara, CO, and Beguy, D. WOMEN’S education and utilization of maternal health services in Africa: a multi-country and socioeconomic status analysis. J Biosoc Sci. (2018) 50:725–48. doi: 10.1017/S0021932017000505
75. Yuan, B, Målqvist, M, Trygg, N, Qian, X, Ng, N, and Thomsen, S. What interventions are effective on reducing inequalities in maternal and child health in low- and middle-income settings? A systematic review. BMC Public Health. (2014) 14:634. doi: 10.1186/1471-2458-14-634
76. Masanja, H, Schellenberg, JA, de Savigny, D, Mshinda, H, and Victora, CG. Impact of integrated Management of Childhood Illness on inequalities in child health in rural Tanzania. Health Policy Plan. (2005) 20:i77–84. doi: 10.1093/heapol/czi054
77. Aquino, R, de Oliveira, NF, and Barreto, ML. Impact of the family health program on infant mortality in Brazilian municipalities. Am J Public Health. (2009) 99:87–93. doi: 10.2105/AJPH.2007.127480
78. Quayyum, Z, Khan, MNU, Quayyum, T, Nasreen, HE, Chowdhury, M, and Ensor, T. “Can community level interventions have an impact on equity and utilization of maternal health care”—evidence from rural Bangladesh. Int J Equity Health. (2013) 12:22. doi: 10.1186/1475-9276-12-22
79. Haider, MR, Rahman, MM, Moinuddin, M, Rahman, AE, Ahmed, S, and Khan, MM. Impact of maternal and neonatal health initiatives on inequity in maternal health care utilization in Bangladesh. PLoS One. (2017) 12:e0181408. doi: 10.1371/journal.pone.0181408
80. Hatt, L, Stanton, C, Makowiecka, K, Adisasmita, A, Achadi, E, and Ronsmans, C. Did the strategy of skilled attendance at birth reach the poor in Indonesia? Bull World Health Organ. (2007) 85:774–82. doi: 10.2471/BLT.06.033472
81. Penchansky, R, and Thomas, JW. The concept of access: definition and relationship to consumer satisfaction. Med Care. (1981) 19:127–40. doi: 10.1097/00005650-198102000-00001
82. Kriel, Y, Milford, C, Cordero, JP, Suleman, F, Steyn, PS, and Smit, JA. Access to public sector family planning services and modern contraceptive methods in South Africa: a qualitative evaluation from community and health care provider perspectives. PLoS One. (2023) 18:e0282996. doi: 10.1371/journal.pone.0282996
83. Dotse-Gborgbortsi, W, Nilsen, K, Ofosu, A, Matthews, Z, Tejedor-Garavito, N, Wright, J, et al. Distance is “a big problem”: a geographic analysis of reported and modelled proximity to maternal health services in Ghana. BMC Pregnancy Childbirth. (2022) 22:672. doi: 10.1186/s12884-022-04998-0
84. Farrer, L, Marinetti, C, Cavaco, YK, and Costongs, C. Advocacy for health equity: a synthesis review. Milbank Q. (2015) 93:392–437. doi: 10.1111/1468-0009.12112
Keywords: inequity, maternal health care services, developing countries, systematic review, meta-analysis, low-or middle-income countries
Citation: Gube AA, Murányi E, Vitrai J and Lohner S (2024) Inequity in uptake of maternal health care services in developing countries: a systematic review and meta-analysis. Front. Public Health. 12:1415092. doi: 10.3389/fpubh.2024.1415092
Edited by:
Tracy Reibel, Murdoch University, AustraliaReviewed by:
Lawrence Ulu Ogbonnaya, Ebonyi State University, NigeriaPaola Vasquez, Murdoch University, Australia
Copyright © 2024 Gube, Murányi, Vitrai and Lohner. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Addisu Alemayehu Gube, YWRkaXMxNjZAZ21haWwuY29t