 Mai A. Khatib
Mai A. Khatib Elham A. Aljaaly
Elham A. Aljaaly Maryam S. Hafiz1
Maryam S. Hafiz1- 1Department of Clinical Nutrition, Faculty of Applied Medical Sciences, King Abdulaziz University, Jeddah, Saudi Arabia
- 2Food, Nutrition, and Lifestyle Unit, King Fahd Medical Research Center, King Abdulaziz University, Jeddah, Saudi Arabia
- 3Obesity Unit, King Abdulaziz University Hospital, King Abdulaziz University, Jeddah, Saudi Arabia
- 4Adult Podiatric Adolescent Obesity Clinic, MNT Unit, King Abdulaziz University Hospital, King Abdulaziz University, Jeddah, Saudi Arabia
Introduction: Low energy availability (LEA) is a state of inadequate energy reserves that results from a negative energy balance. This condition can lead to severe health risks such as amenorrhea and osteoporosis. Various causes for LEA, such as eating disorders and exercise addiction, have been reported in the literature. However, data in Saudi Arabia are lacking. This cross-sectional study measures the prevalence of LEA, eating disorders, and exercise addiction among adult females in Saudi Arabia and identifies possible associated risk factors.
Methods: The sample comprised 119 female athletes who filled out an online survey adapted from the LEA in Females Questionnaire, the Eating Disorder Examination Questionnaire, and the Exercise Addiction Inventory.
Results: Participants showed a high prevalence of LEA (66.4%), eating disorder (33.6%), and exercise addiction (10.1%), confirming the association between normal weight and LEA in females living in Saudi Arabia (p < 0.00).
Discussion and conclusion: With an increasing number of females in the country interested in following a healthy lifestyle, there is a need to raise the awareness of the population on the issues of LEA, eating disorders, and exercise addiction and their effects on the body by developing educational programs about energy intake and healthy physical activity routines.
Introduction
Energy availability is the dietary energy left over to support physiological functions after deducting energy expenditure from exercise (1). Inadequate intake and/or excessive expenditure of energy may lead to a state known as low energy availability (LEA), where the body's ability to support optimal physiological function is compromised (2). Endurance athletes typically exhibit LEA resulting from altered dietary habits and/or high energy expenditure brought on by body dissatisfaction, the notion that becoming lighter will enhance performance and social pressure to maintain a particular appearance. Additionally, athletes may feel pressure from their teammates, coach, or social media (2). It has been suggested that energy savings may serve as a helpful indicator of LEA. In competitive female cyclists, poor aerobic performance and relative energy shortage were both linked to female riders with ratios of measured resting energy expenditure to predicted resting energy expenditure (mREE/pREE) below 0.9, which are associated with LEA (3). Low energy availability in female endurance athletes who do not have disordered eating behavior is common, and studies have stated that it is more common among athletes engaging in weight-sensitive sports when in comparison with sedentary controls (4). Low Energy Availability in Females (LEAF), particularly, leads to undesirable conditions such as poor resting energy expenditure and disruption of a variety of hormonal, metabolic, and functional features; although both genders can develop LEA, which lowers endurance, raises the risk of injury, and depletes glycogen stores (5). As a result, the body attempts to conserve energy, through metabolic changes that maintain homeostasis by decreasing energy expenditure (3). Reduced macronutrient intake in athletes may result in a decline in their physiological capacity for bone production, maintenance of muscle mass, repair of damaged tissue, and recovery after injury (6). Furthermore, during periods of intense exercise training, glycogen stores may not be adequately restored especially when carbohydrate consumption prior the exercise was not insufficient. Moreover, protein needs might also increase since the protein reserves could be utilized as a substitute source of energy. Additionally, micronutrients are necessary for the growth of bones and muscles, the replacement of erythrocytes, and the availability of cofactors for the control of metabolic reactions that produce energy (6). For this reason, a well-balanced and diverse diet that provides all macronutrient needs as well as vitamins, minerals, and sufficient energy should be maintained (7). Insufficient availability of energy results in reduction of energy expenditure by stopping bodily functions, including menstrual periods, hence the main concern will be survival (7). Functional hypothalamic amenorrhea is known as the menstruation absence caused by supressed axis of hypothalamus to ovaries with absence of organic or anatomical reasons (8). It is potentially reversible and frequently manifests itself in conditions of stress, rapid weight loss, and overexertion (8). Usually, secondary amenorrhea, or previously regular menses that cease for at least 3 months or menses already irregular that cease for at least 6 months, calls for evaluation (9). Psychological variables in eating patterns, as in disordered eating, may cause LEA, although LEA in turn can cause severe psychological suffering (10). The two factors, amenorrhea and eating disorders, that come with LEA are also important components called female athlete triad (FAT) (10). The FAT, which includes amenorrhea, osteoporosis, and an eating disorder, was initially identified in 1992 (11). Currently, it has been proposed that the FAT can be defined as the existence of one or more elements in females participating in sports (11). Screening tools for early detection of FAT/LEA symptoms are crucial to protect young athletes from long-term harm brought on by the development potential risks connected to FAT/LEA (12). Several quantitative measurements can be used to test for LEAF, including body compositional analysis, bone mineral density, basal energy expenditure, and day-to-day dietary recall (12). Moreover, a qualitative instrument can be utilized such as the Low Energy Availability in Females Questionnaire (LEAF-Q) (12). It was once thought that the triad only affected professional athletes, but we now know that it can even affect women who are not athletes (11).
Moreover, early detection of factors associated with LEA can aid in preventing deterioration in performance and health and in planning protection and proper nutritional intervention programs (10). Specifically, disordered eating behavior was commonly shown among weight-sensitive athletes and considered a significant risk factor for developing LEA (2, 13), although LEA among female endurance athletes without disordered eating was also shown to be common (14). The gold standard for detecting the behavioral symptoms of disordered eating is Eating Disorder Examination Questionnaire (EDE-Q) 6.0 (15, 16).
Physical activity, universally recognized as a healthy habit, has the potential to develop into an unhealthy preoccupation, referred to as exercise addiction (17). The primary addiction to exercise is characterized by exercise addiction that does not accompany disordered eating; while secondary, which can develop in conjunction with eating disorders or because of them (18). Low energy availability can result from either type, but it is still unknown how exercise addiction, separate from disordered eating, contributes to the development of LEA (13, 19). Also, exercise addiction not only runs the risk of causing considerable bodily harm, but those who struggle with this addiction also prioritize exercise over their relationships with family and friends, their health, and their careers (17). Assessment for the risk of exercise addiction is often neglected by health care professionals (17). However, it can be screened for using the Exercise Addiction Inventory Questionnaire (EAI-Q), which is a quick and easy. Based on the available literature on LEAF, more research is required to investigate the link connecting disordered eating behavior to exercise addiction with LEAF, especially in Saudi Arabia that has seen an increasing numbers of females of reproductive age participating in sports. Therefore, the main purpose of this study was to measure the prevalence of LEAF, exercise addiction, and eating disorders among females in Saudi Arabia and to identify the association between LEAF in female athletes with exercise addiction, body mass index, and eating disorders. This will help to understand the magnitude of this problem in the society and aid the Ministry of Health in developing proper approaches and educational programs about appropriate energy intake in addition to helping to understand the effect of healthy food intake and good exercise at the population level.
Materials and methodology
Participants
The sample size was calculated using Epi Info 7.2.4.0 (CDC, Atlanta). Based on the female population in Saudi Arabia in 2022, with an 80% confidence level, 50% expected frequency, and a 5% margin of error, the estimated sample size required for this study was 164 participants. Recruitment took place through the snowball sampling method. Invitations were sent electronically via social media outlets. We included female athletes [who perform 5 h per week or more (20)] from any region of the country, age 18–50 years old, who had no medical conditions that could cause LEA. We excluded women who are active yet perform < 5 h per week, females of menopausal period, females with history of any chronic disease and/or who have taken hormonal replacement therapy over the past year, women taking medication that affects bone mineral density, and pregnant or breastfeeding females prior or at during the study.
Measures
The study was cross-sectional that was conducted from September 2022 until June 2023, female athletes filled out an online questionnaire adapted from three previously validated and published questionnaires (14, 21, 22) concerned with energy availability in females, exercise addiction, and the evaluation of disordered eating behavior in physically active females. The questionnaire also collected demographic data including age, educational level, profession, height, weight, BMI, medical background, use of medications, and smoking (Table 1).
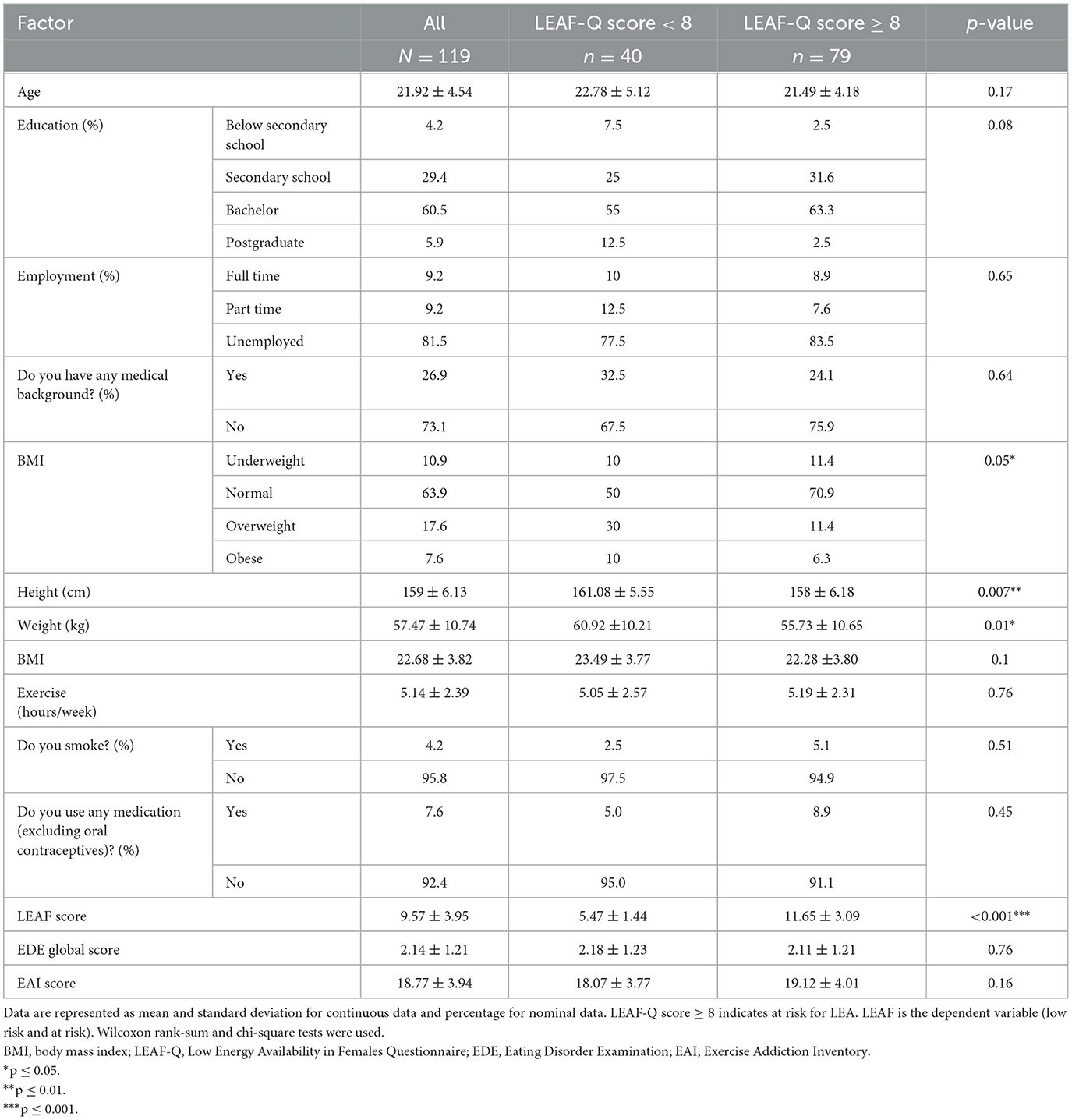
Table 1. Participant sociodemographic and lifestyle characteristics and Low Energy Availability in Females (LEAF) scores (N = 119).
Prior to the study, all four sections of the tool were reviewed, modified, and refined by an expert panel of seven clinical and sports nutrition professionals. The expert panel also observed and approved the translation of the tool into Arabic. To confirm the questionnaire's validity and reliability, it was pilot tested on seven students, who were similar in age to the study population, following the same inclusion criteria, results of which are included in the analysis. The tool was shared with participants all over the country electronically through social media platforms [WhatsApp, X (formerly Twitter), and Instagram] using a poster with the survey barcode.
Ethical approval
The ethical approval for the study was obtained from the Unit of Biomedical Ethics at King Abdulaziz University (Reference number: FAMS-EC2023-01). Strict confidentiality was upheld for the sample and the data collected. Data were de-identified during evaluation, analysis, and any publication. Electronically signed consent was obtained from all participants prior enrolment in the study and answering questions.
Statistical analysis
Statistical analysis was carried out using IBM SPSS Statistics (Version 23.0) with double -tailed significance level set at p ≤ 0.05. The data was inspected and verified as non-normally distributed using one sample Kolmogorov–Smirnov test (p < 0.01), thus the Wilcoxon rank-sum test and score and Mann-Whitney U-test were used. The results are presented as median and interquartile range (Q1 at 25% and Q3 at 75%). We used chi-square test to investigate possible differences among categorical variables in two independent groups. Finally, we used logistic regression to identify potential risk factors for LEA, defined as a LEAF-Q score ≥ or < 8 as the dependent variable. Odds ratios and confidence intervals were used to investigate possible associations among logistic regression model. Variables were expressed as numbers and percentages. To reinforce clear and thorough reporting, the study followed the STROBE checklist (23).
Results
Sociodemographic factors
The total number of responses to the questionnaire received was 184. However, only 119 responses were considered in the analysis after excluding responses with no training status or respondents who did not fulfill the criterion used to define athletes (exercising for five or more hours per week) (20), which is crucial when using the LEAF questionnaire as it was validated for use with female athletes (12, 14) (see Table 1 for sociodemographic data). Average participant age was 21.92 ± 4.54 years. Average body mass index (BMI) was 22.68 ± 3.82 kg/m2 (63.90% had a normal BMI). Only five participants were smokers.
Energy availability risk score
Seventy-nine participants scored 8 or higher on the LEAF-Q (66.4%), qualifying them to be at risk for LEA, and the difference was statistically significant from the number of participants at low risk (40 participants, 33.6%), p < 0.001. Forty participants scored 2.5 or higher on the EDE-Q, qualifying them to be statistically significant at risk for eating disorders (33.6%; p < 0.001). Twelve participants had statistically significant risk for exercise addiction with a score of 24 or higher on the EAI-Q, p < 0.001. Among the participants with LEA (n = 79), four (3.3%) were classified as having primary exercise addiction, 6 (5.0%) had secondary exercise addiction, and 20 (16.8%) had disordered eating without exercise addiction.
We found no significant relationship between LEA and eating disorders (p > 0.05), although 40% of subjects that were at greater risk of LEA also scored 2.5 or higher on the EDE-Q (Table 2). No relationship was found between LEA and exercise addiction either (p > 0.05), although 12.7% of subjects that were at greater risk of LEA also scored 24 or higher on the EAI-Q (Table 3). The results revealed a significant association between having a BMI in the normal or underweight range and being at risk for LEA (p < 0.05), as 11.2% of the participants who were underweight according to BMI and 63.2% of participants with normal weight were at greater risk for LEA (LEAF-Q score ≥ 8; Table 4). Logistic regression analysis has revealed that low BMIs were at greater risk of LEA (OR = 0.29; p ≤ 0.01), meaning that BMI can be considered a contributing factor for LEAF (Table 5). There was no statistically significant association between LEA and any of the other variables (Table 5).
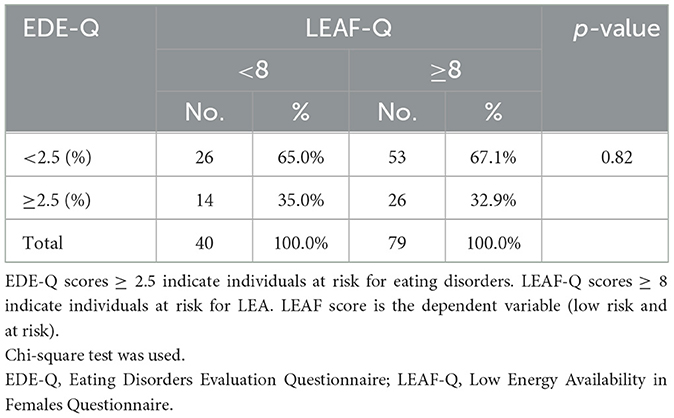
Table 2. Relationship between eating disorders and Low Energy Availability in Females score.

Table 3. Relationship between exercise addiction and Low Energy Availability in Females score.
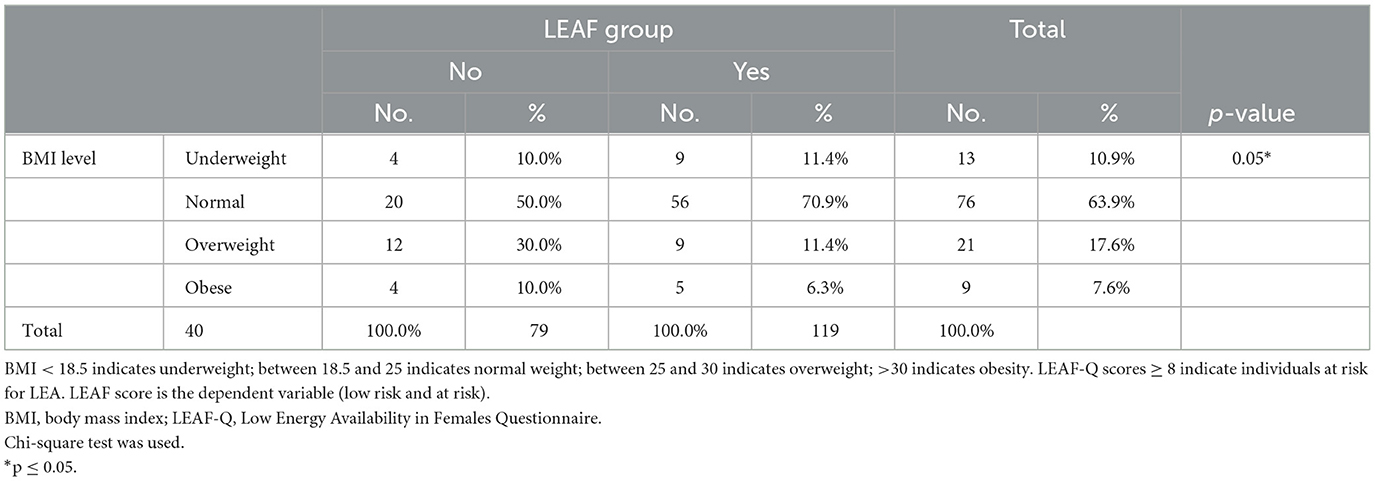
Table 4. Relationship between BMI and Low Energy Availability in Females score.
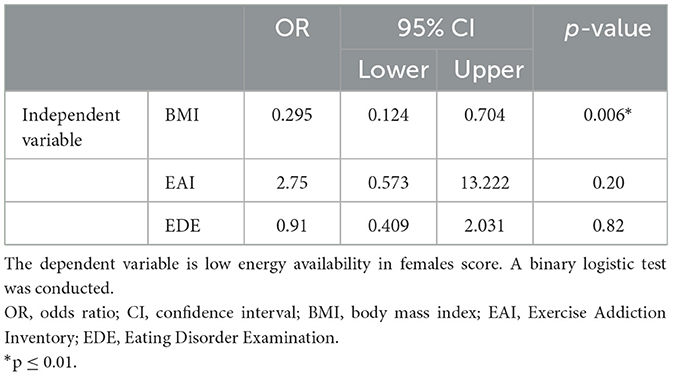
Table 5. Risk factors for low energy availability.
Discussion
The main objective of our study was to measure the prevalence of LEA among active adult females in Saudi Arabia and to identify the contributing factors associated with LEAF. The study found a significant correlation between BMI and LEA; lower BMI status was more prevalent with participants at greater risk for LEA. Our study showed that 66.4% of female athletes were at high risk for LEA, which is similar to 65 and 62.2% cases of LEA in female athletes reported by Fahrenholtz et al. (4) and Melin et al. (14), respectively. However, a lower percentage (31%) was reported by Carr et al. (24), and a higher percentage (79.5%) was reported by Jesus et al. (24, 25). These discrepancies could be related to the different types of sports practiced and the level of activity (26). Despite the reasons associated with LEA, the high prevalence indicates vulnerability of the studied group of females to LEA, which can, consequently, lead to a rise of symptoms related to FAT and relative energy deficiency in sport (RED-S) syndromes (19).
For the majority of female athletes, LEA results unintentionally from appetite suppression post exercise (19, 27), low energy diets (28), An insufficient understanding of ideal sports nutrition (16, 29–31) along with impacts of LEA (32–35), or a busy lifestyle with inadequate time or access to food (29, 36, 37). On the other hand, insufficient balance between caloric intake and expenditure resulting in LEA may lead intentionally in pursuit of optimizing body mass and composition, to avoid gaining weight while downtime, or as a result of eating disorders or exercise dependence and/or addiction (36, 38), although, as previously mentioned, female endurance athletes can have LEA without disordered eating (39). Nevertheless, the present study showed prevalence rates of 32.9 and 12.7% for eating disorders and EA, respectively, among female athletes at high risk for LEA. On the other hand, data analysis revealed no significant association between eating disorders and LEA or between exercise addiction and LEA. This comes contrary to what is published in the literature. Fahrenholtz et al. (4) demonstrated that participants at greater risk for LEA also had high scores for both disordered eating and exercise addiction when compared with participants at low risk (4). This can explain the high prevalence of LEA (62.2%) in their study, since availability of energy results from energy intake and expenditure, and, thus, both disordered eating and exercise addiction should be considered when examining for LEA (4). Collectively, our results suggest a high prevalence of eating disorders and exercise addiction in women, which is concerning.
There are primary and secondary forms of exercise dependence. When it is caused by disordered eating or is associated with it, the condition is secondary (40). However, if it occurs without accompanying symptoms of disordered eating, it is primary exercise dependence (41–44). In the latter, the person exercises continuously for the sole purpose of psychological gratification that results from the exercise itself no other pathologies (40). The current findings show that among the athletes with LEA (n = 79, 66.4%), primary exercise addiction was found in 3.3%, 5.0% had secondary exercise addiction, and 16.8% had disordered eating without exercise addiction. Disordered eating is known as a reason that can cause LEA (19, 45); however, how exercise dependence causes LEA in the absence of disordered eating has not yet been explored. Preliminary studies have pointed to an increase in biochemical markers that indicate LEA (13, 46). However, these results are limited. It is possible that reduced availability of energy may contribute to the eating disorders in secondary exercise dependence. It is crucial, therefore, when developing interventions for athletes with RED-S syndrome to examine both dietary and exercise patterns.
In the present study, a rough measure of BMI was used with the intention to generally investigate the association between BMI and LEA among the population of female athletes. The current findings showed lower BMIs in athletes at greater risk for LEA comparing with athletes at low risk. Moreover, using regression analysis, LEA was found to be influenced by BMI. This could be logically expected, as athletes generally perceive excess fat as a major limiting factor in sport performance and that a higher skeletal muscle mass promotes strength and power (47). Thus, athletes might intentionally decrease their intake in order to reach the desired shape and/or optimal body composition (48). One can speculate from this point of view that LEA is not exclusive to a certain weight group and that it can be suspected even in people of normal weight. This highlights how important it is to promote healthy dietary habits and a positive body image among female athletes, since the current findings showed that most of the athletes at risk for LEA presented a healthy BMI. Although the current outcomes are in line with those of Fahrenholtz et al. and Christo et al. (4, 49), other reports disagree with them (14, 28). This conflict can only suggest that BMI cannot be used alone when screening for LEA, given the potential metabolic compensatory mechanisms and that other measurements of body composition should be used to carefully identify malnutrition and examine athletic health and performance (50–52). Further research is recommended to elucidate this relationship.
The novelty in this study is the identified prevalence of LEA, eating disorders, along with exercise addiction among females residing in the various regions of Saudi Arabia. The outcomes of the current research emphasize the importance of the topic and reinforce the need for larger future studies that allow for the detection of comparable differences among the different regions of the country. Due to the cross-sectional design of the study, it was not possible to identify the correlation's direction and, hence, causality. Moreover, hence the data collection involved self-reporting, it might be prone to response bias, denial, and erroneous reporting in studies. Overestimation or underestimation of anthropometric data and food intake was also an issue. Future studies should include measuring the nutritional knowledge of the participated females and categorizing the participated females according to the type of sport practiced during analysis and risk association, since athletes in weight categories of aesthetic sports manipulate their weight when compared to other type of sports. In conclusion, this study showed a high prevalence of LEA (66.4%), eating disorders (33.6%), and exercise addiction (10.1%) and confirmed the association between normal weight and LEA in females living in Saudi Arabia. The high percentage of the affected population elicits the need to raise awareness among females, especially with the increasing trends of practicing sports and following a healthy lifestyle in the country. Further, larger studies should follow to assess the causative relationship between LEA and eating disorders, exercise addiction, and BMI in both genders. The results of the current study should be used as rough estimates for future studies comparing prevalence rates with other Gulf, and neighboring, countries. They will also help the Ministry of Health in developing proper educational programs and approaches for appropriate energy intake as well as understanding the effect of healthy food intake and good exercise at the population level.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Author contributions
MK: Conceptualization, Formal analysis, Resources, Supervision, Writing – original draft, Writing – review & editing. EA: Data curation, Investigation, Methodology, Supervision, Visualization, Writing – review & editing. MH: Methodology, Project administration, Supervision, Visualization, Writing – review & editing. AA: Investigation, Methodology, Writing – original draft, Writing – review & editing. WA: Investigation, Methodology, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Acknowledgments
The authors thank Dina Qahwaji, Haneen Najjar, Shoug Alashmali, and Doaa Alyoubi for their assistance with co-supervising the bachelor degree students while conducting this research. The authors would also like to thank all the volunteers who took part in the study.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Areta JL, Taylor HL, Koehler K. Low energy availability: history, definition and evidence of its endocrine, metabolic and physiological effects in prospective studies in females and males. Eur J Appl Physiol. (2021) 121:1–21. doi: 10.1007/s00421-020-04516-0
2. Wasserfurth P, Palmowski J, Hahn A, Krüger K. Reasons for and consequences of low energy availability in female and male athletes: social environment, adaptations, and prevention. Sports Med. (2020) 6:44. doi: 10.1186/s40798-020-00275-6
3. Jurov I, Keay N, Spudić D, Rauter S. Inducing low energy availability in trained endurance male athletes results in poorer explosive power. Eur J Appl Physiol. (2022) 122:503–13. doi: 10.1007/s00421-021-04857-4
4. Fahrenholtz IL, Melin AK, Wasserfurth P, Stenling A, Logue D, Garthe I, et al. Risk of low energy availability, disordered eating, exercise addiction, and food intolerances in female endurance athletes. Front Sports Act Living. (2022) 4:869594. doi: 10.3389/fspor.2022.869594
5. Ishibashi A, Kojima C, Tanabe Y, Iwayama K, Hiroyama T, Tsuji T, et al. Effect of low energy availability during three consecutive days of endurance training on iron metabolism in male long distance runners. Physiol Rep. (2020) 8:e14494. doi: 10.14814/phy2.14494
6. Kontele I, Vassilakou T. Nutritional risks among adolescent athletes with disordered eating. Children. (2021) 8:80715. doi: 10.3390/children8080715
7. Ryterska K, Kordek A, Załeska P. Has menstruation disappeared? Functional hypothalamic amenorrhea-what is this story about? Nutrients. (2021) 13:82827. doi: 10.3390/nu13082827
8. Master-Hunter T, Heiman DL. Amenorrhea: evaluation and treatment. Am Fam Physician. (2006) 73:1374–82.
9. Klein DA, Paradise SL, Reeder RM. Amenorrhea: a systematic approach to diagnosis and management. Am Fam Physician. (2019) 100:39–48.
10. Melin AK, Heikura IA, Tenforde A, Mountjoy M. Energy availability in athletics: health, performance, and physique. Int J Sport Nutr Exerc Metab. (2019) 29:152–64. doi: 10.1123/ijsnem.2018-0201
11. Witkoś J, Hartman-Petrycka M. The Female Athlete Triad-the impact of running and type of diet on the regularity of the menstrual cycle assessed for recreational runners. PeerJ. (2022) 10:e12903. doi: 10.7717/peerj.12903
12. Łuszczki E, Jagielski P, Bartosiewicz A, Kuchciak M, Dereń K, Stolarczyk A, et al. The LEAF questionnaire is a good screening tool for the identification of the Female Athlete Triad/Relative Energy Deficiency in Sport among young football players. PeerJ. (2021) 9:e12118. doi: 10.7717/peerj.12118
13. Monica Klungland T, Ida Lysdahl F, Mia Beck L, Thomas Birkedal S, Anna Katarina M. Exercise dependence, eating disorder symptoms and biomarkers of Relative Energy Deficiency in Sports (RED-S) among male endurance athletes. Br Med J Open Sport Exer Med. (2019) 5:e000439. doi: 10.1136/bmjsem-2018-000439
14. Melin A, Tornberg AB, Skouby S, Faber J, Ritz C, Sjödin A, et al. The LEAF questionnaire: a screening tool for the identification of female athletes at risk for the female athlete triad. Br J Sports Med. (2014) 48:540–5. doi: 10.1136/bjsports-2013-093240
15. Guest T. Using the eating disorder examination in the assessment of bulimia and anorexia: issues of reliability and validity. Soc Work Health Care. (2000) 31:71–83. doi: 10.1300/J010v31n04_05
16. Sim A, Burns SF. Review: questionnaires as measures for low energy availability (LEA) and relative energy deficiency in sport (RED-S) in athletes. J Eat Disord. (2021) 9:41. doi: 10.1186/s40337-021-00396-7
17. Griffiths MD, Szabo A, Terry A. The exercise addiction inventory: a quick and easy screening tool for health practitioners. Br J Sports Med. (2005) 39:e30. doi: 10.1136/bjsm.2004.017020
18. Kuikman MA, Mountjoy M, Burr JF. Examining the relationship between exercise dependence, disordered eating, and low energy availability. Nutrients. (2021) 13:82601. doi: 10.3390/nu13082601
19. Mountjoy M, Sundgot-Borgen JK, Burke LM, Ackerman KE, Blauwet C, Constantini N, et al. IOC consensus statement on relative energy deficiency in sport (RED-S): 2018 update. Br J Sports Med. (2018) 52:687. doi: 10.1136/bjsports-2018-099193
20. McKinney J, Velghe J, Fee J, Isserow S, Drezner JA. Defining athletes and exercisers. Am J Cardiol. (2019) 123:532–5. doi: 10.1016/j.amjcard.2018.11.001
21. Terry A, Szabo A, Griffiths M. The exercise addiction inventory: a new brief screening tool. Addict R. Theory. (2004) 12:489–99. doi: 10.1080/16066350310001637363
22. Fairburn CG, Beglin SJ. Assessment of eating disorder psychopathology: interview or self-report questionnaire. Int J Eating Disord. (1994) 16:363–70.
23. Lachat C, Hawwash D, Ocké MC, Berg C, Forsum E, Hörnell A, et al. Strengthening the reporting of observational studies in epidemiology-nutritional epidemiology (STROBE-nut): an extension of the STROBE statement. PLoS Med. (2016) 13:e1002036. doi: 10.1371/journal.pmed.1002036
24. Carr A, McGawley K, Govus A, Andersson EP, Shannon OM, Mattsson S, et al. Nutritional intake in elite cross-country skiers during two days of training and competition. Int J Sport Nutr Exerc Metab. (2019) 29:273–81. doi: 10.1123/ijsnem.2017-0411
25. Jesus F, Castela I, Silva AM, Branco PA, Sousa M. Risk of low energy availability among female and male elite runners competing at the 26th European Cross-Country Championships. Nutrients. (2021) 13:30873. doi: 10.3390/nu13030873
26. Hoch AZ, Pajewski NM, Moraski L, Carrera GF, Wilson CR, Hoffmann RG, et al. Prevalence of the female athlete triad in high school athletes and sedentary students. Clin J Sport Med. (2009) 19:421–8. doi: 10.1097/JSM.0b013e3181b8c136
27. Howe SM, Hand TM, Larson-Meyer DE, Austin KJ, Alexander BM, Manore MM. No effect of exercise intensity on appetite in highly-trained endurance women. Nutrients. (2016) 8:223. doi: 10.3390/nu8040223
28. Melin A, Tornberg Å B, Skouby S, Møller SS, Sundgot-Borgen J, Faber J, et al. Energy availability and the female athlete triad in elite endurance athletes. Scand J Med Sci Sports. (2015) 25:610–22. doi: 10.1111/sms.12261
29. Benardot D. Energy thermodynamics revisited: energy intake strategies for optimizing athlete body composition and performance. Pensar En Movimiento. (2013) 11:1–14. doi: 10.15517/pensarmov.v11i2.10841
30. Trakman GL, Forsyth A, Devlin BL, Belski R. A systematic review of athletes' and coaches' nutrition knowledge and reflections on the quality of current nutrition knowledge measures. Nutrients. (2016) 8:90570. doi: 10.3390/nu8090570
31. Heikkilä M, Valve R, Lehtovirta M, Fogelholm M. Nutrition knowledge among young Finnish endurance athletes and their coaches. Int J Sport Nutr Exerc Metab. (2018) 28:522–7. doi: 10.1123/ijsnem.2017-0264
32. Folscher LL, Grant CC, Fletcher L, Janse van Rensberg DC. Ultra-marathon athletes at risk for the Female Athlete Triad. Sports Med Open. (2015) 1:29. doi: 10.1186/s40798-015-0027-7
33. Condo D, Lohman R, Kelly M, Carr A. Nutritional intake, sports nutrition knowledge and energy availability in Female Australian Rules Football Players. Nutrients. (2019) 11:50971. doi: 10.3390/nu11050971
34. Logue DM, Madigan SM, Melin A, Delahunt E, Heinen M, Donnell SM, et al. Low energy availability in athletes 2020: an updated narrative review of prevalence, risk, within-day energy balance, knowledge, and impact on sports performance. Nutrients. (2020) 12:30835. doi: 10.3390/nu12030835
35. Tosi M, Maslyanskaya S, Dodson NA, Coupey SM. The Female Athlete Triad: a comparison of knowledge and risk in adolescent and young adult figure skaters, dancers, and runners. J Pediatr Adolesc Gynecol. (2019) 32:165–9. doi: 10.1016/j.jpag.2018.10.007
36. Burke LM, Lundy B, Fahrenholtz IL, Melin AK. Pitfalls of conducting and interpreting estimates of energy availability in free-living athletes. Int J Sport Nutr Exerc Metab. (2018) 28:350–63. doi: 10.1123/ijsnem.2018-0142
37. Logue DM, Mahony L, Corish CA, Tobin D, Doherty R, O'Higgins G, et al. Athletes' and coaches' perceptions of nutritional advice: eating more food for health and performance. Nutrients. (2021) 13:61925. doi: 10.3390/nu13061925
38. Gibbs JC, Williams NI, De Souza MJ. Prevalence of individual and combined components of the female athlete triad. Med Sci Sports Exerc. (2013) 45:985–96. doi: 10.1249/MSS.0b013e31827e1bdc
39. Melin A, Tornberg ÅB, Skouby S, Møller SS, Faber J, Sundgot-Borgen J, et al. Low-energy density and high fiber intake are dietary concerns in female endurance athletes. Scand J Med Sci Sports. (2016) 26:1060–71. doi: 10.1111/sms.12516
40. Cook B, Hausenblas H, Freimuth M. Exercise addiction and compulsive exercising: relationship to eating disorders, substance use disorders, and addictive disorders. In: Brewerton TD, Dennis AB, , editors. Eating Disorders, Addictions and Substance Use Disorders: Research, Clinical and Treatment Perspectives. New York, NY: Springer-Verlag Publishing/Springer Nature (2014). p. 127–44.
41. Blaydon MJ, Linder KJ, Kerr JH. Metamotivational characteristics of exercise dependence and eating disorders in highly active amateur sport participants. Pers Individ Dif. (2004) 36:1419–32. doi: 10.1016/S0191-8869(03)00238-1
42. Blaydon MJ, Lindner KJ. Eating disorders and exercise dependence in triathletes. Eat Disord. (2002) 10:49–60. doi: 10.1080/106402602753573559
43. Cook B, Luke R. Primary and secondary exercise dependence in a sample of cyclists. Int J Ment Health Addict. (2017) 15:444–51. doi: 10.1007/s11469-017-9745-z
44. McNamara J, McCabe MP. Striving for success or addiction? Exercise dependence among elite Australian athletes. J Sports Sci. (2012) 30:755–66. doi: 10.1080/02640414.2012.667879
45. Mountjoy M, Sundgot-Borgen J, Burke L, Carter S, Constantini N, Lebrun C, et al. The IOC consensus statement: beyond the Female Athlete Triad–Relative Energy Deficiency in Sport (RED-S). Br J Sports Med. (2014) 48:491–7. doi: 10.1136/bjsports-2014-093502
46. Lichtenstein MB, Andries A, Hansen S, Frystyk J, Støving RK. Exercise addiction in men is associated with lower fat-adjusted leptin levels. Clin J Sport Med. (2015) 25:138–43. doi: 10.1097/JSM.0000000000000110
47. Pyne DB, Anderson ME, Hopkins WG. Monitoring changes in lean mass of elite male and female swimmers. Int J Sports Physiol Perform. (2006) 1:14–26. doi: 10.1123/ijspp.1.1.14
48. Fairburn CG. Cognitive Behavior Therapy and Eating Disorders. New York, NY: Guilford Press (2008). p. 324.
49. Christo K, Cord J, Mendes N, Miller KK, Goldstein MA, Klibanski A, et al. Acylated ghrelin and leptin in adolescent athletes with amenorrhea, eumenorrheic athletes and controls: a cross-sectional study. Clin Endocrinol. (2008) 69:628–33. doi: 10.1111/j.1365-2265.2008.03237.x
50. Bosy-Westphal A, Schautz B, Later W, Kehayias JJ, Gallagher D, Müller MJ. What makes a BIA equation unique? Validity of eight-electrode multifrequency BIA to estimate body composition in a healthy adult population. Eur J Clin Nutr. (2013) 67(Suppl.1):S14–21. doi: 10.1038/ejcn.2012.160
51. Aragon AA, Schoenfeld BJ, Wildman R, Kleiner S, VanDusseldorp T, Taylor L, et al. International society of sports nutrition position stand: diets and body composition. J Int Soc Sports Nutr. (2017) 14:16. doi: 10.1186/s12970-017-0174-y
Keywords: exercise addiction, eating disorders, female athlete triad, amenorrhea, relative energy deficiency in sport
Citation: Khatib MA, Aljaaly EA, Hafiz MS, Alamri A and Alzahrani W (2024) The risk of low energy availability among athlete females in Saudi Arabia: a cross-sectional study. Front. Public Health 12:1411724. doi: 10.3389/fpubh.2024.1411724
Received: 03 April 2024; Accepted: 14 May 2024;
Published: 30 May 2024.
Edited by:
Pascal Izzicupo, University of Studies G. d'Annunzio Chieti and Pescara, ItalyReviewed by:
Kommi Kalpana, Manav Rachna International Institute of Research and Studies (MRIIRS), IndiaAnastasios Vamvakis, Hellenic Mediterranean University, Greece
Copyright © 2024 Khatib, Aljaaly, Hafiz, Alamri and Alzahrani. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Mai A. Khatib, bWtoYXRpYkBrYXUuZWR1LnNh