 Xuan Liu
Xuan Liu Qiang Li*
Qiang Li*- Department of Physical Education, Ocean University of China, Qingdao, Shandong, China
Background: To systematically review the effects of aerobic exercise and resistance training on Metabolic Health in children and adolescents with overweight/obesity.
Methods: Employing a retrieval strategy that combines subject terms and free terms, searches were conducted in the CNKI, WanFangData, VIP, PubMed, Web of Science, Embase, and Cochrane Library databases up to October 31, 2023.
Results: A total of 29 studies involving 2,195 subjects were included. The combination of aerobic and resistance training significantly reduces body composition and metabolic health in children and adolescents with overweight or obesity, as evidenced by changes in various parameters (BMI, WC, FM, BF%, VO2max, TG, TC, HDL-C, LDL-C, HOMA-IR, FPG, INS). However, there were no significant differences observed in hs-CRP. Subgroup analyses further showed that changes in intervention measurement had a significant effect on the effectiveness of the intervention.
Conclusion: Aerobic exercise combined with resistance training has a positive impact on the physical health of children and adolescents with overweight/obesity. The recommended exercise prescription is at least three sessions of more than 60 min per week for 12 weeks or more for better health benefits.
1 Introduction
The prevalence of obesity has witnessed a significant surge over the past five decades. According to the World Health Statistics (2020) published by the World Health Organization (WHO), more than 340 million children and adolescents aged 5–19 years were overweight or obese worldwide in 2016 (1). Childhood obesity not only elevates the likelihood of becoming obese, facing premature mortality, and disability later in life, but it can also lead to breathing difficulties, a higher chance of bone fractures, high blood pressure, early indicators of heart disease, issues with insulin sensitivity, and psychological health consequences (2).
Recent studies have found that regular participation in exercise not only improves self-efficacy and awareness of exercise in children with obesity but also has a role in controlling weight gain and the development of mental health in children with obesity (3). Physical activity stands as a potent avenue for ameliorating obesity in children and adolescents, with lasting implications for adult physical health.
The Evaluation of Physical Activity Levels of Children and Adolescents Aged 7–18 Years, published by the National Health Inspection Commission (4), states that children and adolescents should spend an average of no less than 70 min of cumulative moderate- and high-intensity physical activity per day, of which at least one session of moderate- and high-intensity physical activity lasting for 10 min or more per day should be carried out. Additionally, the guidelines advocate for aerobic-based physical activity complemented by resistance exercises targeting muscle strength and bone health, to be performed at least thrice weekly.
While numerous investigations have validated the efficacy of exercise in ameliorating obesity in children and adolescents, extant literature predominantly examines the impact of various exercise modalities on body composition in this demographic. It was confirmed that aerobic combined with resistance training was superior to aerobic or resistance training alone in terms of BMI, and BF% (5). Building upon these insights, this research aims to examine the impact of combining aerobic workouts with strength training on body composition and indicators of metabolic health in young individuals who are overweight or obese, with the aim of furnishing evidence-based exercise recommendations for combating obesity in this population.
2 Methods
The execution of this meta-analysis adhered to the guidelines defined by the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) (6).
2.1 PICOS and literature search strategy
The search for keywords was conducted using the Population, Intervention, Comparison, Outcome, and Study design (PICOS) framework (Table 1). The study subjects included children and adolescents with overweight or obesity, with no restrictions on gender or nationality.

Table 1. PICOS chart.
A search was conducted across CNKI, WanFangData, VIP, PubMed, Web of Science, Embase, and Cochrane Library using a mix of controlled vocabulary and free-text terms. The focus was on studies about the effects of combined aerobic and resistance training on body composition and metabolic health in children and adolescents with overweight/obesity, covering literature up to October 31, 2023.The main keywords used were (aerobic exercise OR resistance training or physical activities OR training) AND (obesity* OR overweight OR obese*) AND (child* OR adolescent*).
2.2 Study inclusion and exclusion criteria
The criteria for inclusion are as follows: (1) The literature is a full-text literature in English and Chinese. (2) The test group was aerobic exercise combined with resistance training and the control group was conventional activity. (3) The types of studies encompassed both randomized and non-randomized controlled trials. (4) Study subjects consisted of children and adolescents who were overweight or obese (as judged by the World Health Organization or their respective nationally recognized criteria) with no exercise-related contraindications and no other health problems or complications. (5) Outcome measures included body mass index (BMI), fat mass (FM), body fat percentage (BF%), maximal oxygen uptake (VO2max), triglycerides (TG), total cholesterol (TC), high-density lipoprotein cholesterol (HDL-C), low-density lipoprotein cholesterol (LDL-C), homeostasis model assessment of insulin resistance (HOMA-IR), high-sensitivity C-reactive protein (hs-CRP), fasting plasma glucose (FPG), insulin (INS).
Participants were excluded based on the following conditions: (1) Inclusion of control groups comprising normal-weight children and adolescents. (2) Meta-analysis of the research literature. (3) Programs lacking a combination of aerobic and resistance training. (4) Repetitive publications or literature tangential to the subject matter. (5) Literature lacking original data or precluding the derivation of mean difference (MD) and standardized mean difference (SMD) for outcome indicators.
2.3 Date collection or data synthesis
Literature was meticulously screened, and data were gathered by two researchers in accordance with the research objectives and predetermined criteria. In case of disagreement, a third researcher adjudicated. After perusing the selected literature, the researchers recorded the information on a predefined data collection form, including basic information (author’s name, date of publication, title of the article), number of participants, method of intervention, and outcome indicators.
2.4 Risk of bias assessment
Randomized controlled trials: 2 researchers conducted a comprehensive risk of bias assessment of the 23 included papers according to the Cochrane Handbook.
Non-randomized controlled trials: The methodological index for non-randomized studies (MINORS) (7) was used to evaluate the quality of the 6 articles included in the study, and there were 12 indicators, the first 8 of which were for studies without a control group, with a maximum score of 16 points, and the maximum score for studies with a control group was 24 points. The 12 indicators were evaluated together, with a total maximum score of 24; scores of 0–8 were classified as low quality, 9–16 as moderate quality, and 17–24 as high quality. The MINORS assessment framework stipulated that literature scoring below 12 points should be excluded from meta-analysis. The scoring process was conducted independently by two researchers, and in cases of discordance, resolution was achieved through deliberation or consultation with a third party, ultimately culminating in a consensus.
2.5 Statistical analysis
According to the formula of the Cochrane Toolkit for Systematic Evaluation: within-group difference of Mean = post-intervention in a group of Mean—baseline in a group of Mean, S2 = S12 + S22–2 × R × S1 × S2, where S is the value of within-group standard deviation, S1 is the post-intervention standard deviation, S2 is the baseline standard deviation, and R is a constant taken as 0.4 or 0.5 (8). For studies assessing outcome indicators, only data from the initial and final interventions were used if there were multiple intervention time points.
In this study, we employed Stata 16.0 and Revman 5.4 software for conducting Meta-analysis, using mean difference (MD) or standardized mean difference (SMD) as the indicator of the effect size, When the units of the outcome indicators were identical, MD was chosen as the effect indicator; when the units of the outcome indicators were different, SMD was chosen as the effect indicator (8), and the results were considered statistically significant when p ≤ 0.05 for the effect size. To assess inter-study heterogeneity, we performed quantitative analyses using the I2 statistic; heterogeneity was considered low if p > 0.1 and I2 < 50%, at which point a fixed-effects model was selected for analysis. Sensitivity analyses were conducted using individual study-by-study exclusion methods. In the case of high heterogeneity, we then used the random effects model. In addition, to ensure the credibility of the findings, we also used funnel plots and Egger’s test for the number of studies greater than 10 to assess potential publication bias, with a test level of α = 0.05.
3 Results
3.1 Study selection
After the search, a total of 6,210 pieces of literature were identified. A total of 29 eligible studies were screened for inclusion through an initial review of titles and abstracts, as well as further full-text scrutiny, including 12 in Chinese and 17 in English. The screening process of literature is detailed in Figure 1.
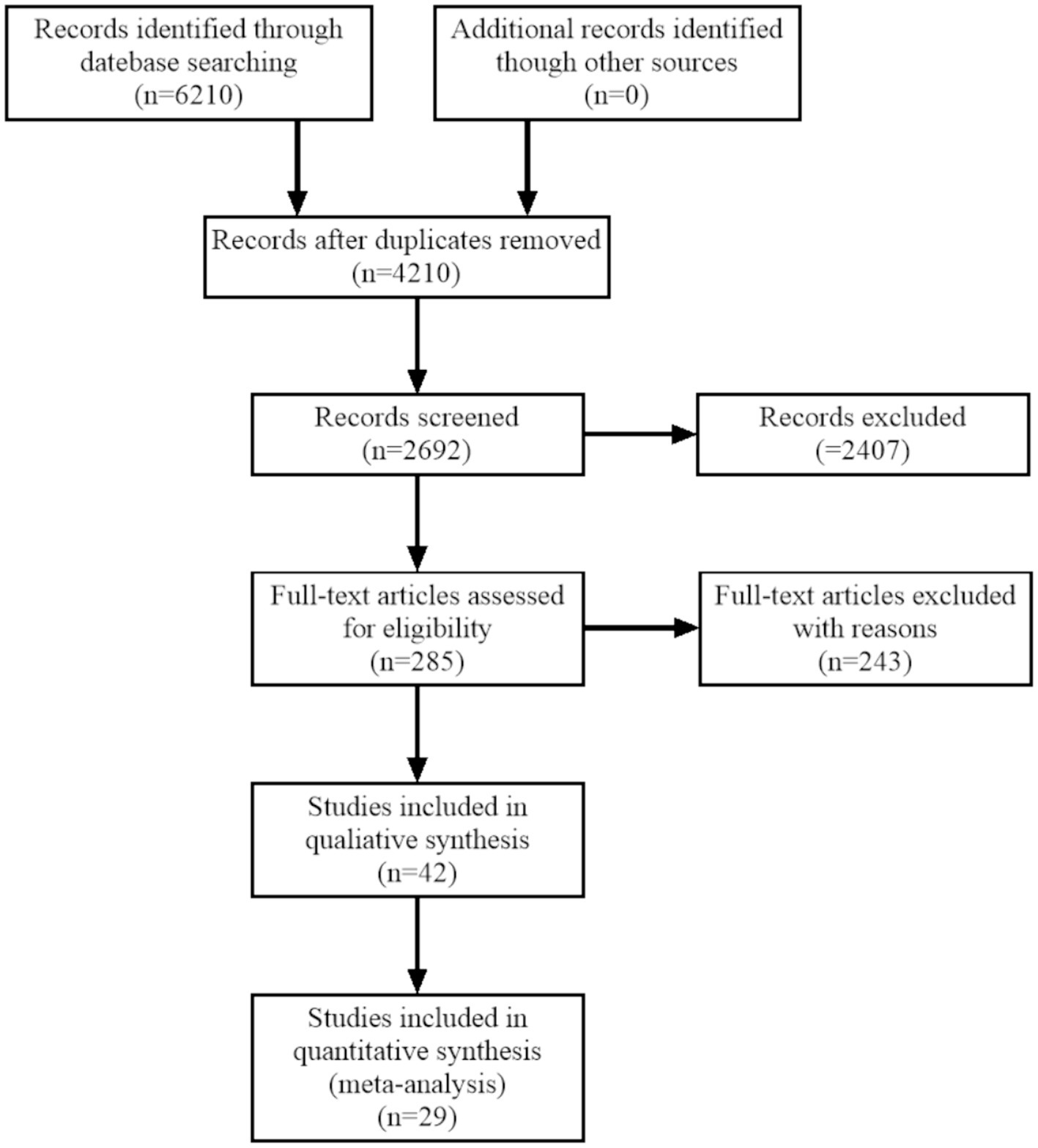
Figure 1. Flow chart of literature retrieval.
3.2 Study characteristics
The 29 included studies comprised a total of 2,195 children and adolescents with overweight/obesity, and all of these studies categorized the participants into experimental and control groups. Table 2 displays the fundamental attributes of the studies selected.
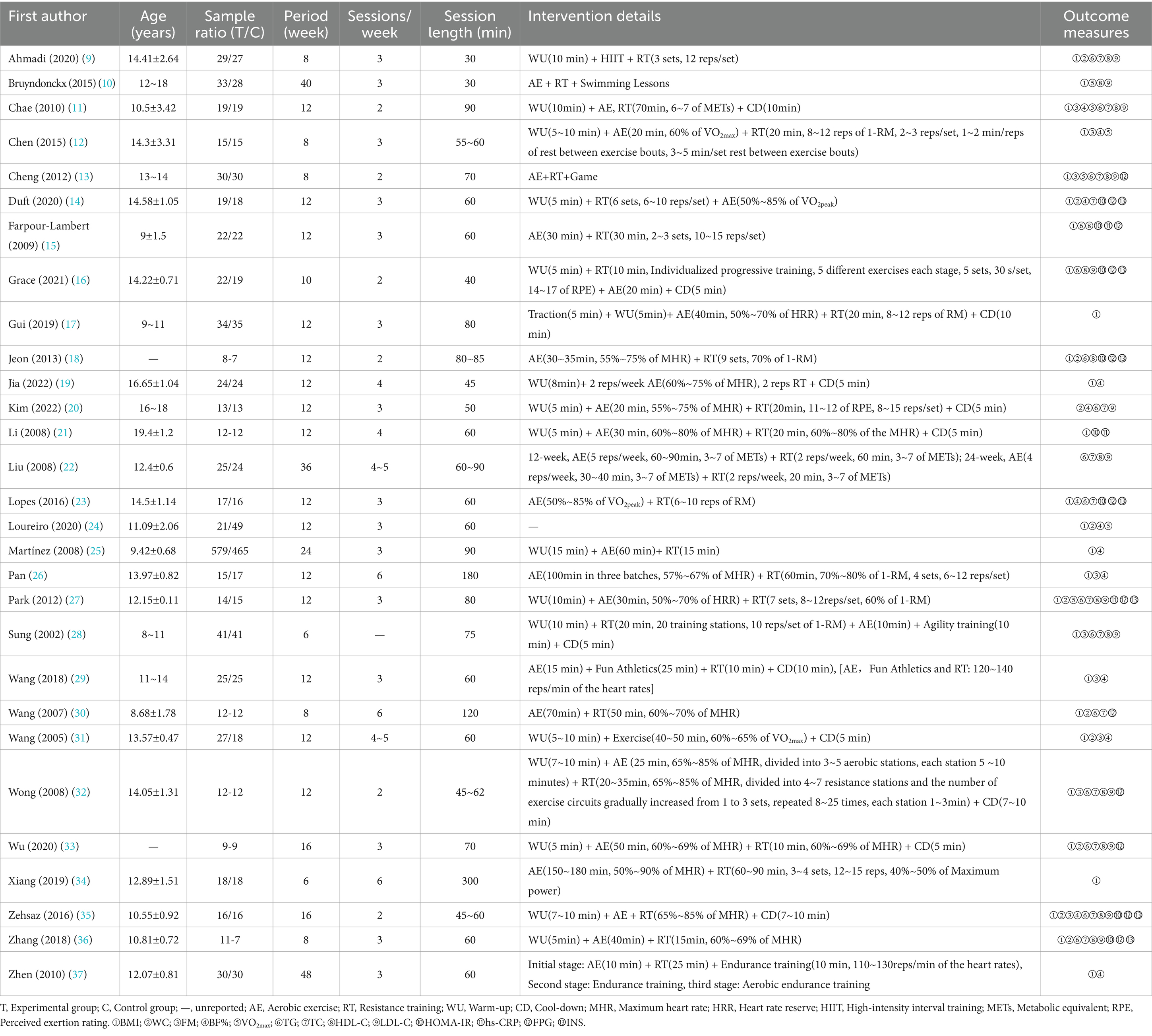
Table 2. General characteristics of the included studies.
3.3 Study quality assessment
The risk of bias assessment showed that of the 23 RCTs included, six described specific randomized sequence methods, six performed allocation concealment, and one used blinding, and all of the included literature had data completeness and were free of other biases and selective reporting. The quality of the literature of the 6 included non-randomized controlled trials was of high quality.
3.4 Meta-analysis
3.4.1 Comparative analysis of BMI interventions
A total of 26 studies reported AE + RT to evaluate BMI in children and adolescents with overweight/obesity. The result of a meta-analysis using a random-effects model showed that the BMI of the trial group was significantly lower than that of the control group after the intervention [MD = −0.96, 95%CI: −1.19, −0.73, p < 0.01] (Figure 2).
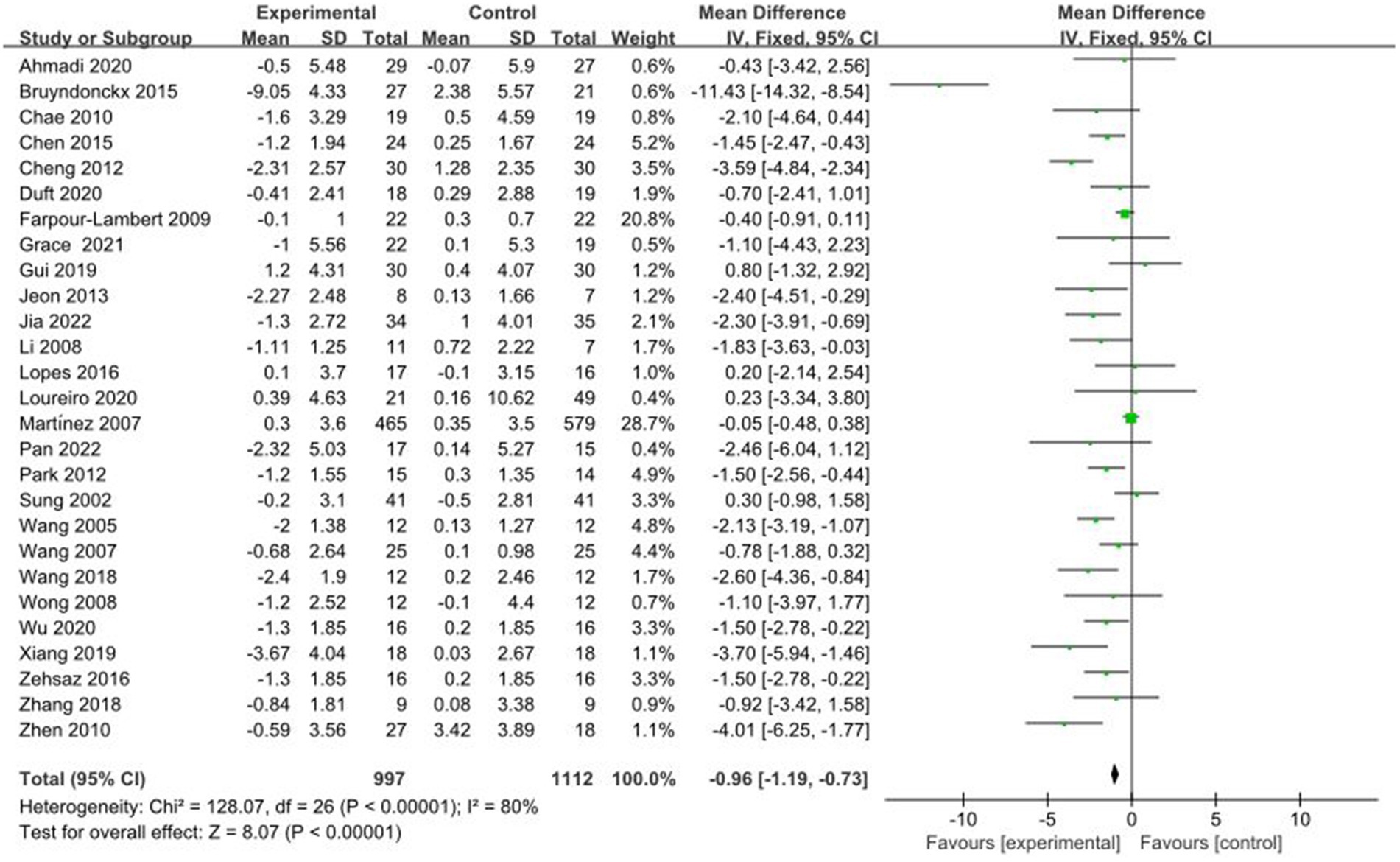
Figure 2. Forest plot of comparison: BMI.
3.4.2 Comparative analysis of WC interventions
A total of 11 studies reported AE + RT to evaluate WC in children and adolescents with overweight/obesity. The result of a meta-analysis using a fixed-effects model showed that WC was significantly lower in the experimental group than in the control group after the intervention [MD = −2.36, 95%CI: −3.64, −1.09, p < 0.01] (Figure 3).
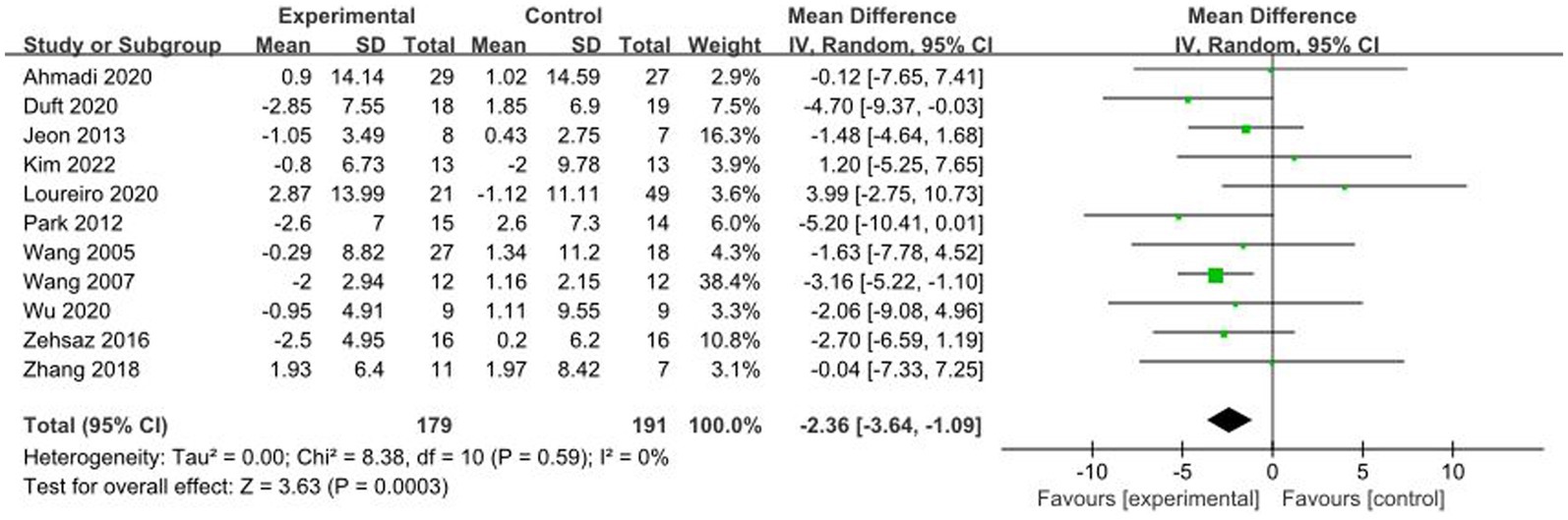
Figure 3. Forest plot of comparison: WC.
3.4.3 Comparative analysis of FM interventions
A total of 9 studies reported AE + RT to evaluate FM in children and adolescents with overweight/obesity. The result of a meta-analysis using a random-effects model showed that FM was significantly lower in the trial group than in the control group after the intervention [MD = −2.80, 95%CI: −3.84, −1.76, p < 0.01] (Figure 4).
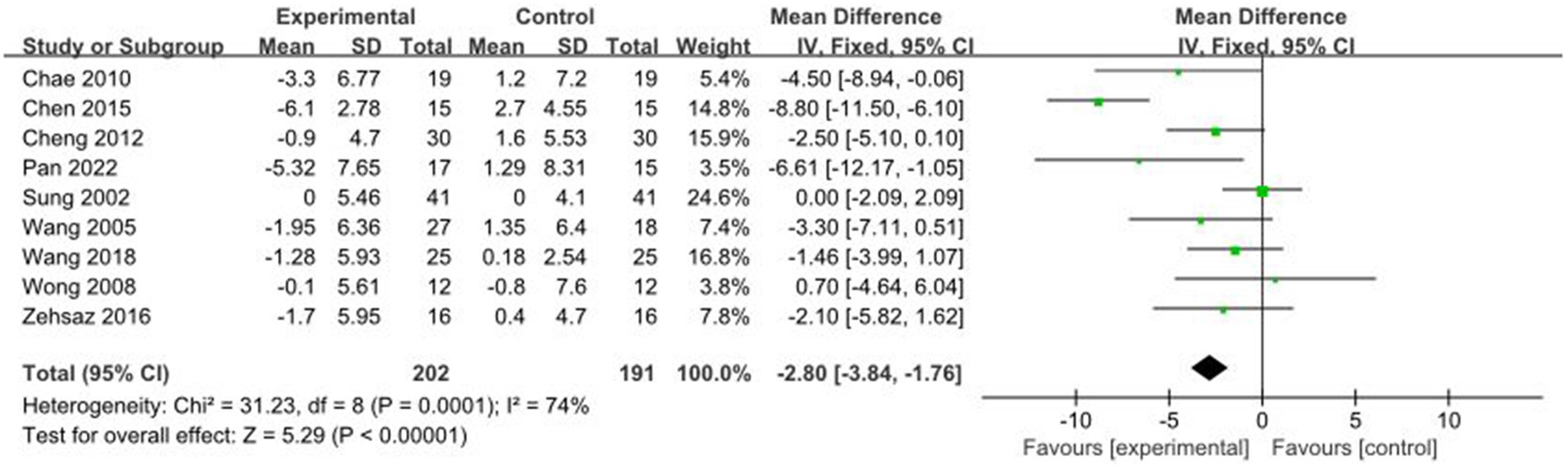
Figure 4. Forest plot of comparison: FM.
3.4.4 Comparative analysis of BF% interventions
A total of 13 studies reported AE + RT to evaluate BF% in children and adolescents with overweight/obesity. The result of a meta-analysis using a random-effects model showed that BF% in the trial group was significantly lower than that of the control group after the interventions [MD = −2.15, 95%CI: −2.75, −1.55, p < 0.01] (Figure 5).
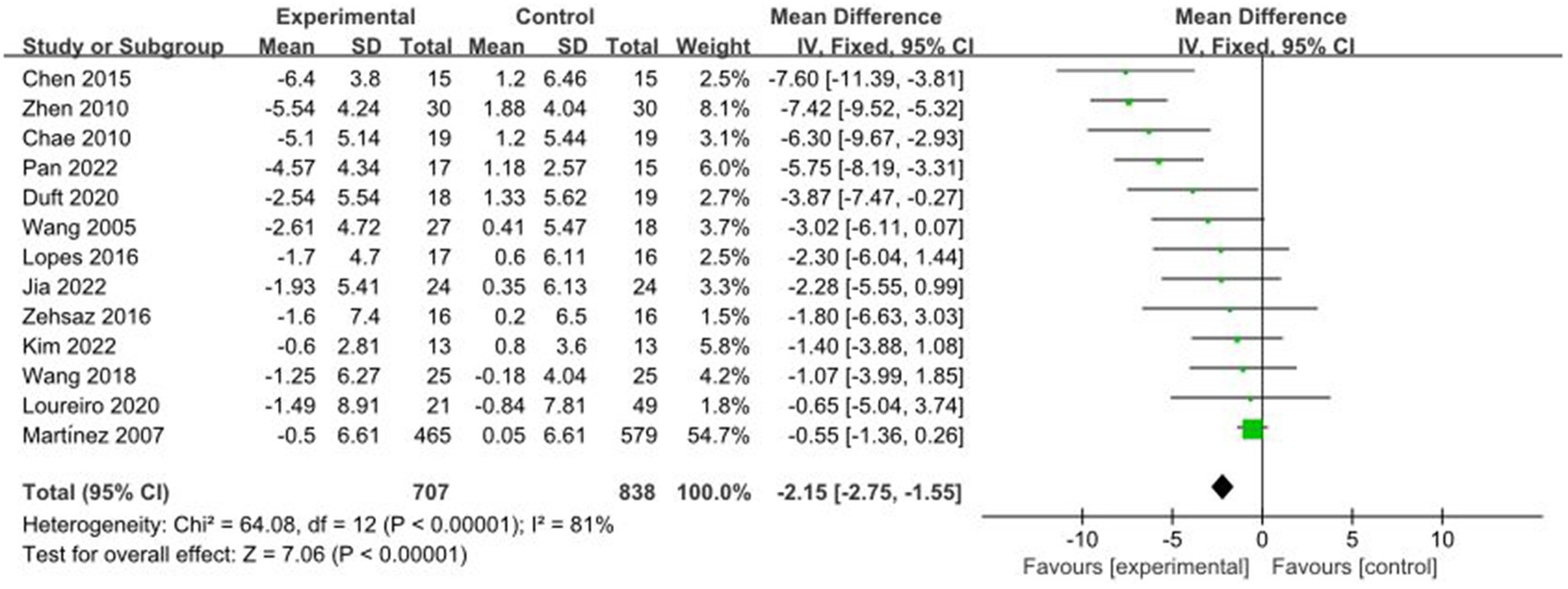
Figure 5. Forest plot of comparison: BF%.
3.4.5 Comparative analysis of VO2max interventions
A total of 5 studies reported AE + RT to evaluate VO2max in children and adolescents with overweight/obesity. The result of a meta-analysis using a random-effects model showed that the VO2max in the trial group was significantly higher than that in the control group after the intervention [MD = 4.73, 95%CI: 3.39, 6.07, p < 0.01] (Figure 6).
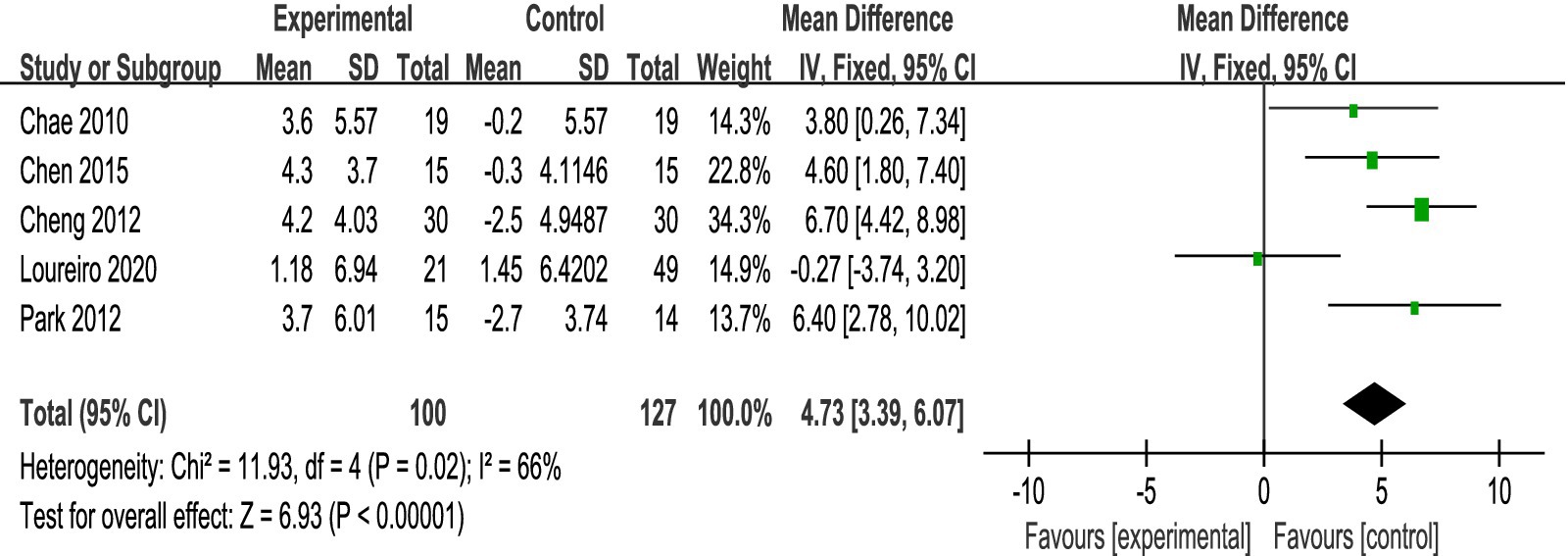
Figure 6. Forest plot of comparison: VO2max.
3.4.6 Comparative analysis of TG interventions
A total of 16 studies reported AE + RT to evaluate TG in children and adolescents with overweight/obesity. The result of a meta-analysis using a random-effects model showed that TG was significantly lower in the trial group than in the control group after the intervention [SMD = −0.30, 95%CI: −0.47, −0.13, p < 0.01] (Figure 7).
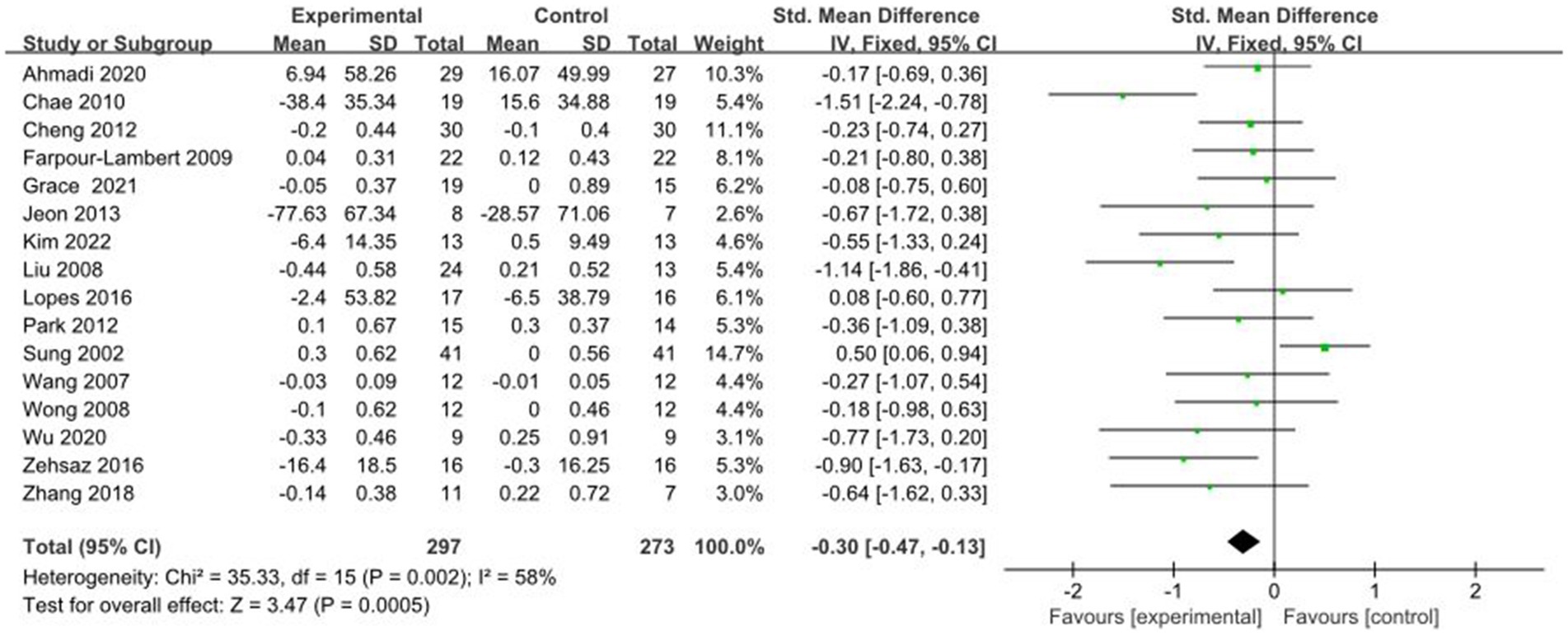
Figure 7. Forest plot of comparison: TG.
3.4.7 Comparative analysis of TC interventions
A total of 14 studies reported AE + RT to evaluate TC in children and adolescents with overweight/obesity. The result of a meta-analysis using a random-effects model showed that TC was significantly lower in the trial group than in the control group after the intervention [SMD = −0.25, 95%CI: −0.44, −0.06, p < 0.01] (Figure 8).
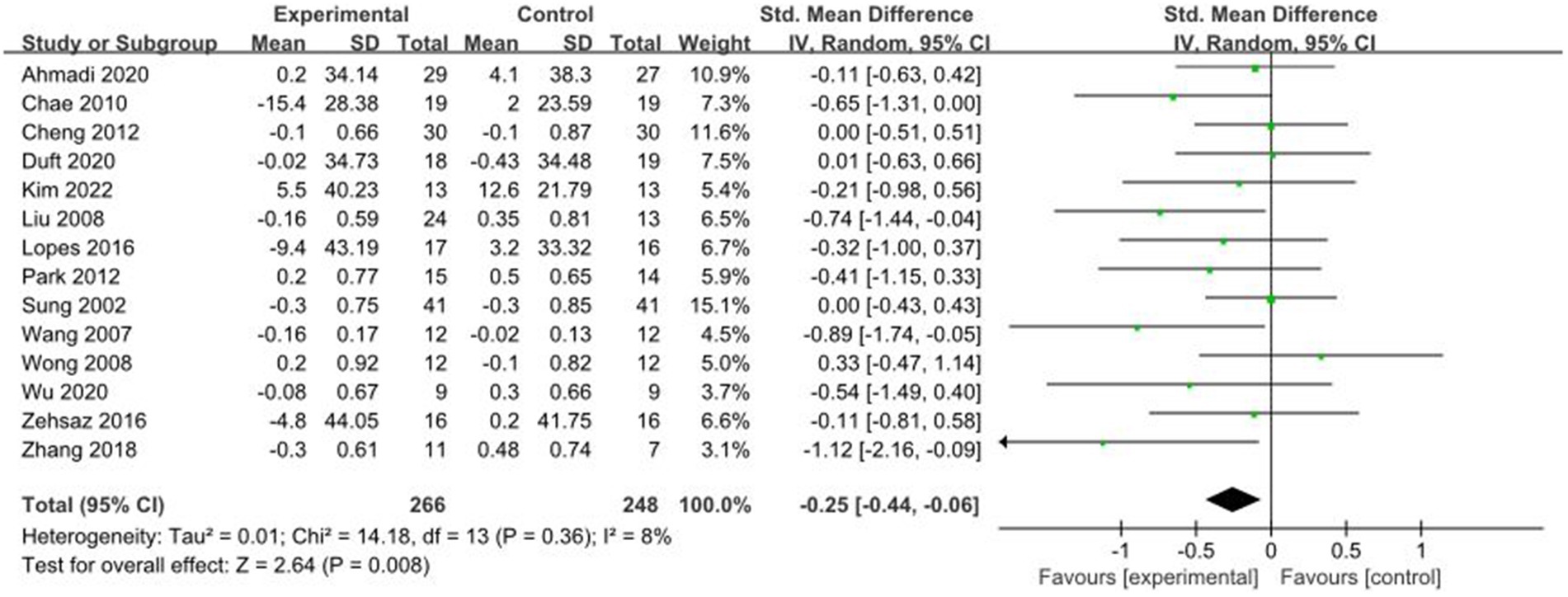
Figure 8. Forest plot of comparison: TC.
3.4.8 Comparative analysis of HDL-C interventions
A total of 14 studies reported AE + RT to evaluate HDL-C in children and adolescents with overweight/obesity. The result of a meta-analysis using a random-effects model showed that HDL-C was significantly higher in the experimental group than in the control group after the intervention [SMD = 0.37, 95%CI: 0.20, 0.55, p < 0.01] (Figure 9).
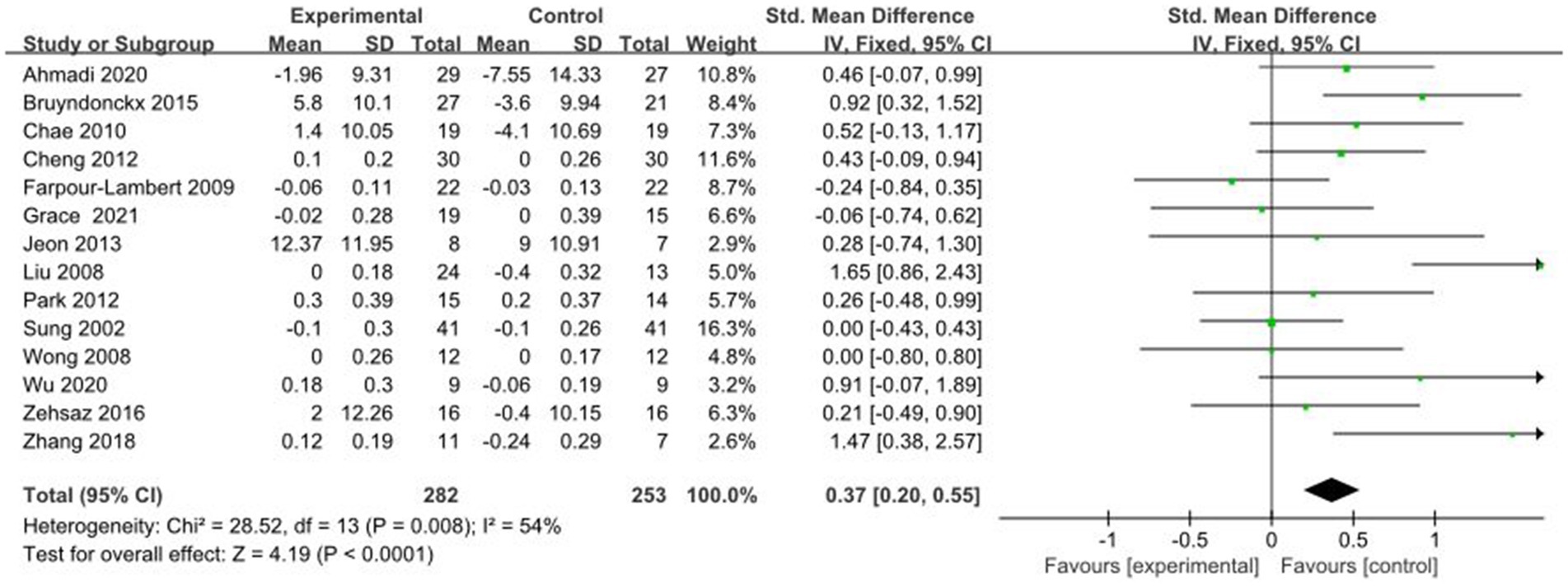
Figure 9. Forest plot of comparison: HDL-C.
3.4.9 Comparative analysis of LDL-C interventions
A total of 13 studies reported AE + RT to evaluate LDL-C in children and adolescents with overweight/obesity. The result of a meta-analysis using a fixed-effects model showed that LDL-C was significantly lower in the experimental group than in the control group after the intervention [SMD = −0.30, 95%CI: −0.48, −0.12, p < 0.01] (Figure 10).
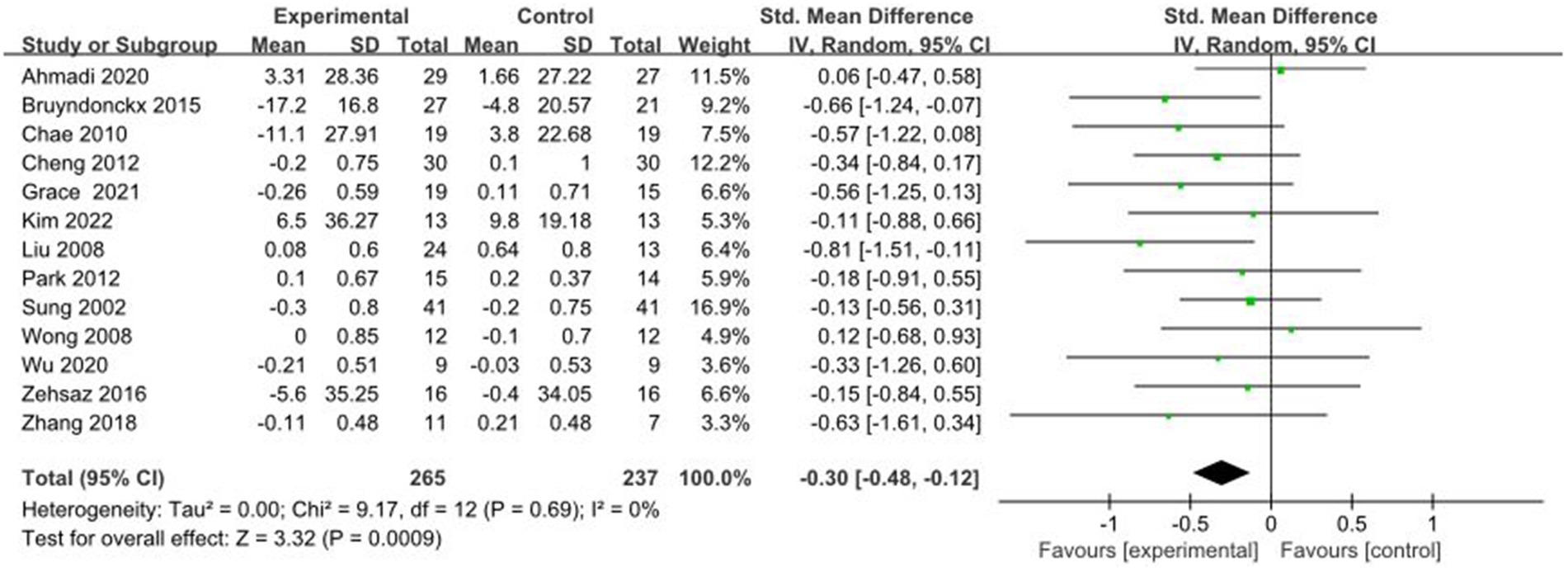
Figure 10. Forest plot of comparison: LDL-C.
3.4.10 Comparative analysis of HOMA-IR interventions
A total of 8 studies reported AE + RT to evaluate HOMA-IR in children and adolescents with overweight/obesity. The result of a meta-analysisusing a random-effects model showed that HOMA-IR was significantly lower in the test group than in the control group after the intervention [SMD = −0.63, 95%CI: −0.90, −0.36, p < 0.01] (Figure 11).
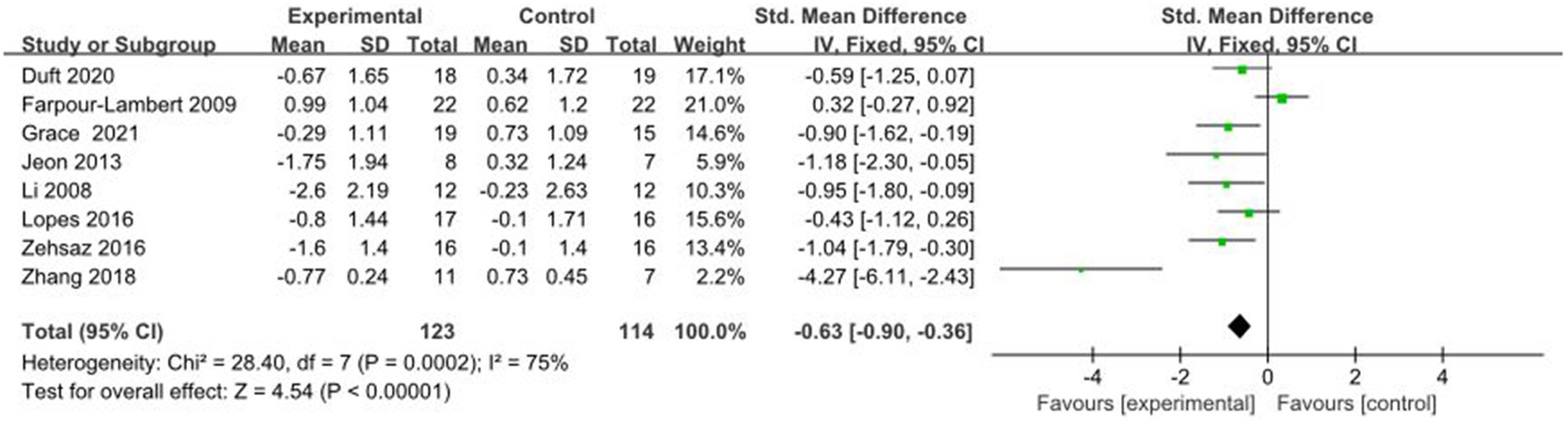
Figure 11. Forest plot of comparison: HOMA-IR.
3.4.11 Comparative analysis of hs-CPR interventions
A total of 3 studies reported AE + RT to evaluate hs-CRP in children and adolescents with overweight/obesity. The result of a meta-analysis using a fixed-effects model showed that hs-CRP was not significant in the test group after the intervention [SMD = −0.00, 95%CI: −0.56, 0.56, p = 0.99] (Figure 12).
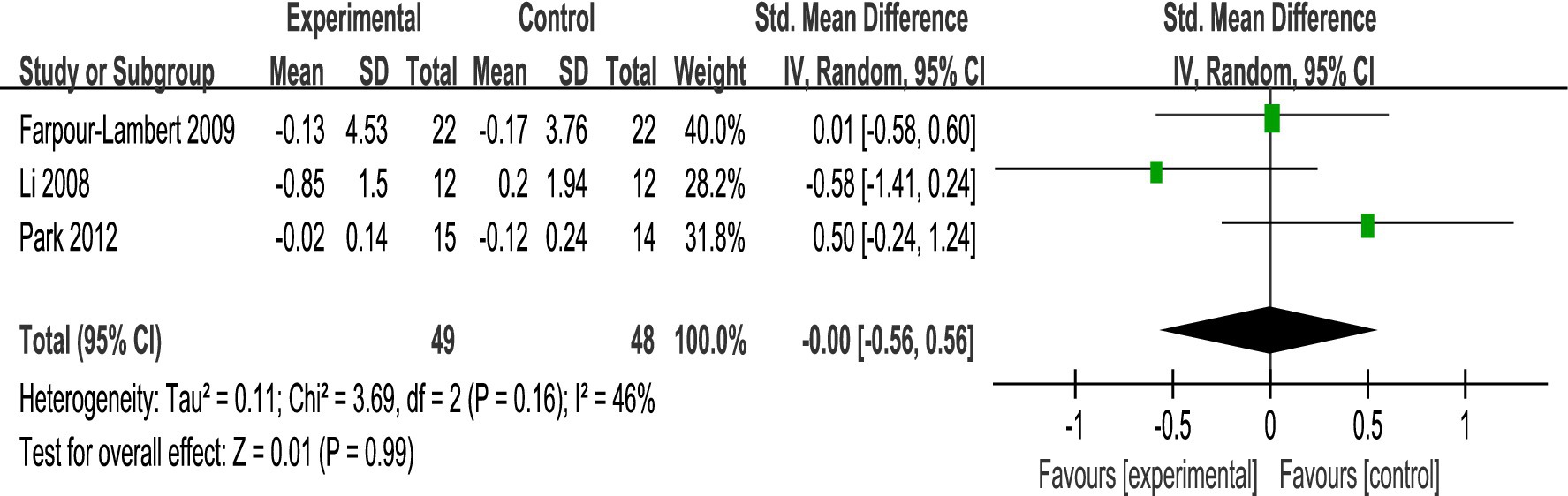
Figure 12. Forest plot of comparison: hs-CRP.
3.4.12 Comparative analysis of FPG interventions
A total of 12 studies reported AE + RT to evaluate FPG in children and adolescents with overweight/obesity. The result of a meta-analysis using a random-effects model showed that FPG was significantly lower in the experimental group than in the control group after the intervention [SMD = −0.34, 95%CI: −0.55, −0.13, p < 0.01] (Figure 13).
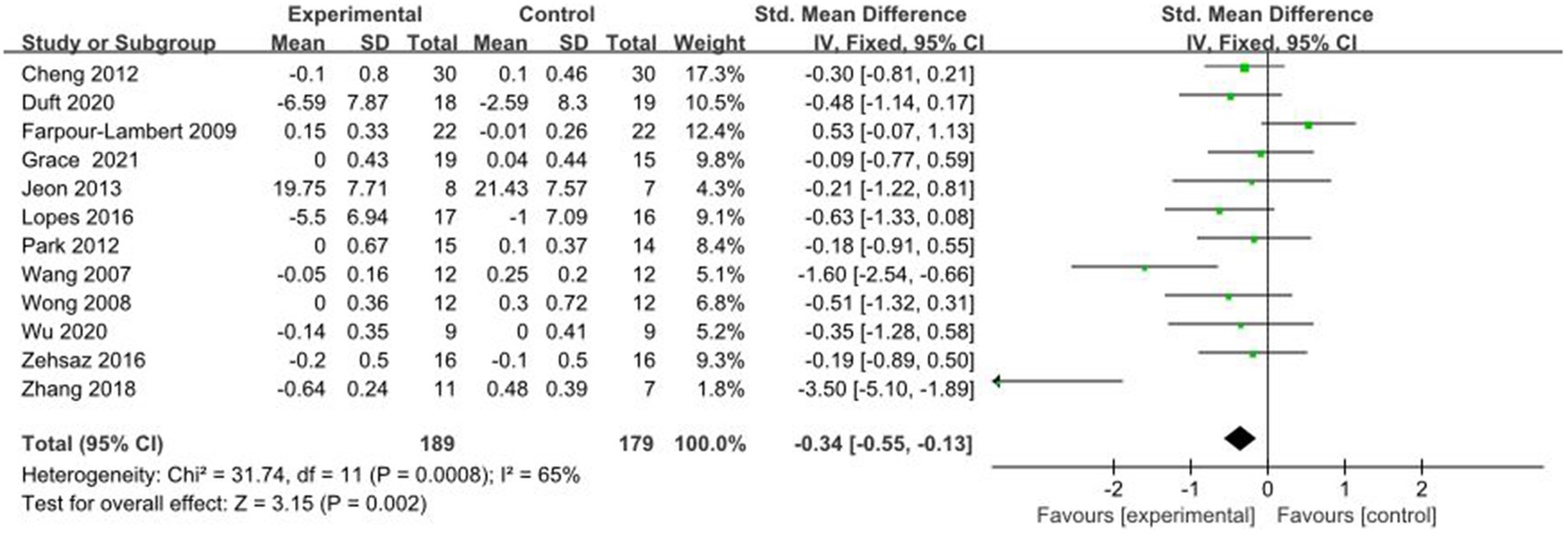
Figure 13. Forest plot of comparison: FPG.
3.4.13 Comparative analysis of INS interventions
A total of 7 studies reported AE + RT to evaluate INS in children and adolescents with overweight/obesity. The result of a meta-analysis using a random-effects model showed that INS was significantly higher in the experimental group than in the control group after the intervention [SMD = −0.70, 95%CI: −0.99, −0.40, p < 0.01] (Figure 14).
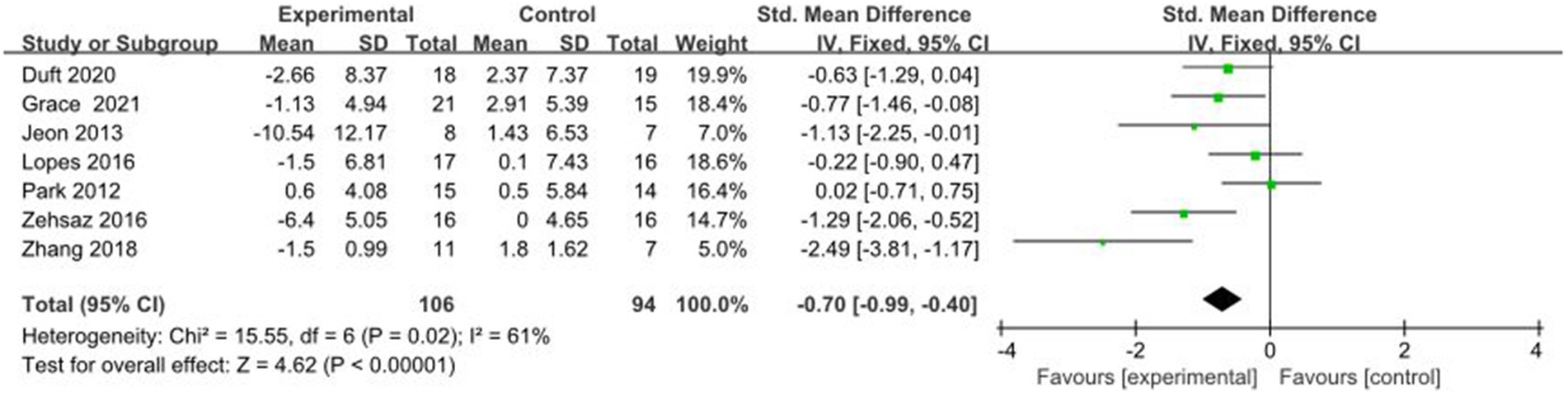
Figure 14. Forest plot of comparison: INS.
3.5 Results of subgroup analyses
3.5.1 Analysis of BMI subgroups
Differences in training parameters may be an important factor influencing fitness, therefore subgroup analyses were performed based on the training period, training frequency, and training time. The results showed that a training period of ≥12 weeks [MD = −1.51, 95%CI: −1.93, −1.08, p < 0.01], a training frequency of ≥3 times/week [WMD = −1.78, 95%CI: −2.35, −1.21, p < 0.01], and a duration of each training session of ≥60 min intervention was the best [MD = −1.49, 95%CI: −2.02, −0.97, p < 0.01] (Table 3).
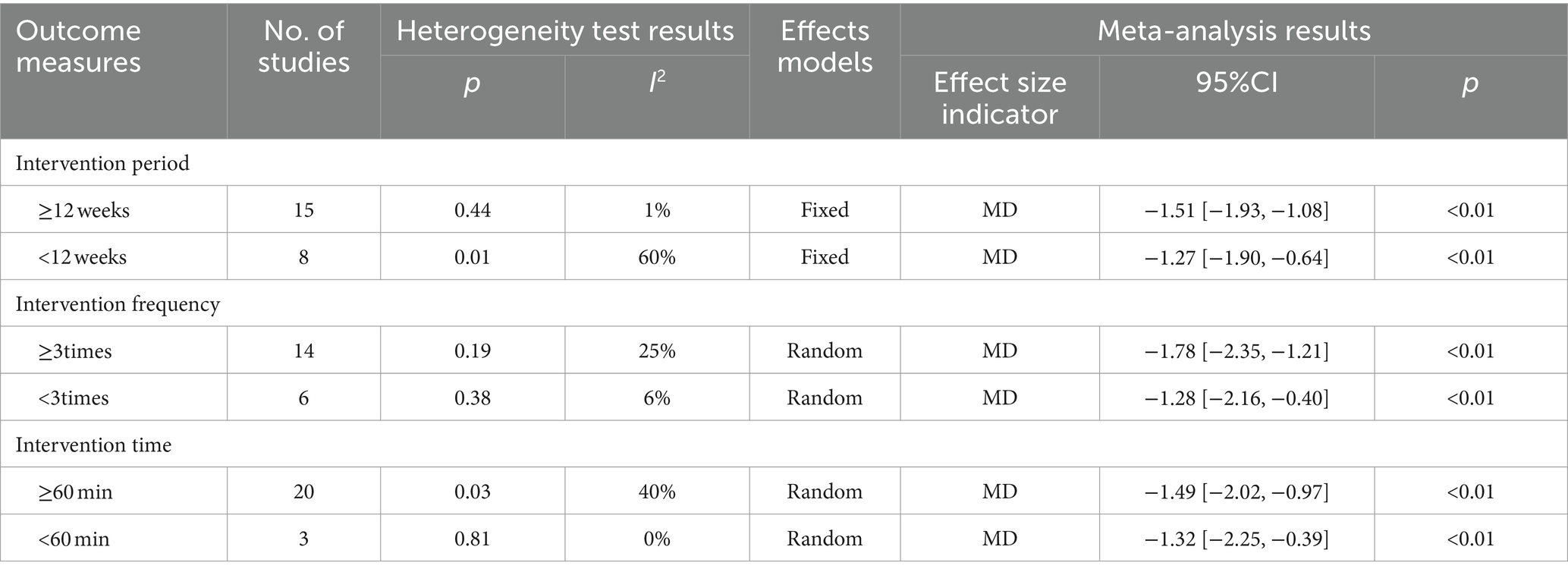
Table 3. Subgroup analysis of BMI.
3.5.2 Analysis of TG subgroups
The results showed that a training period of ≥12 weeks [SMD = −0.66, 95%CI: −1.01, −0.31, p < 0.01], a training frequency of ≥3 times/week [SMD = −0.30, 95%CI: −0.58, −0.02, p < 0.05], and a duration of each training session of ≥60 min intervention was optimal [SMD = −0.27, 95%CI: −0.47, −0.06, p = 0.01] (Table 4).
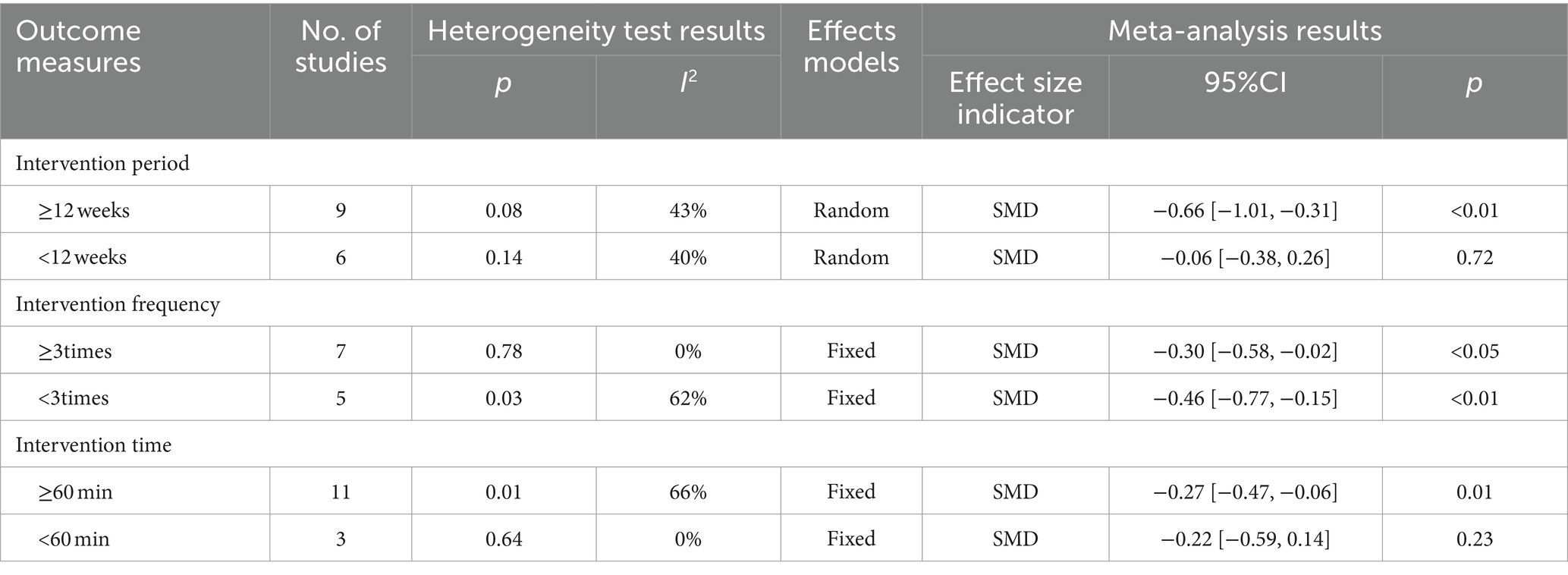
Table 4. Subgroup analysis of TG.
3.5.3 Analysis of HOMA-IR subgroups
The results showed that the best intervention effect was achieved with a training period of ≥12 weeks [SMD = −0.76, 95%CI: −1.11, −0.42, p < 0.01] and a training frequency of ≥3 sessions/week [SMD = −1.21, 95%CI: −2.20, −0.22, p < 0.05] (Table 5).
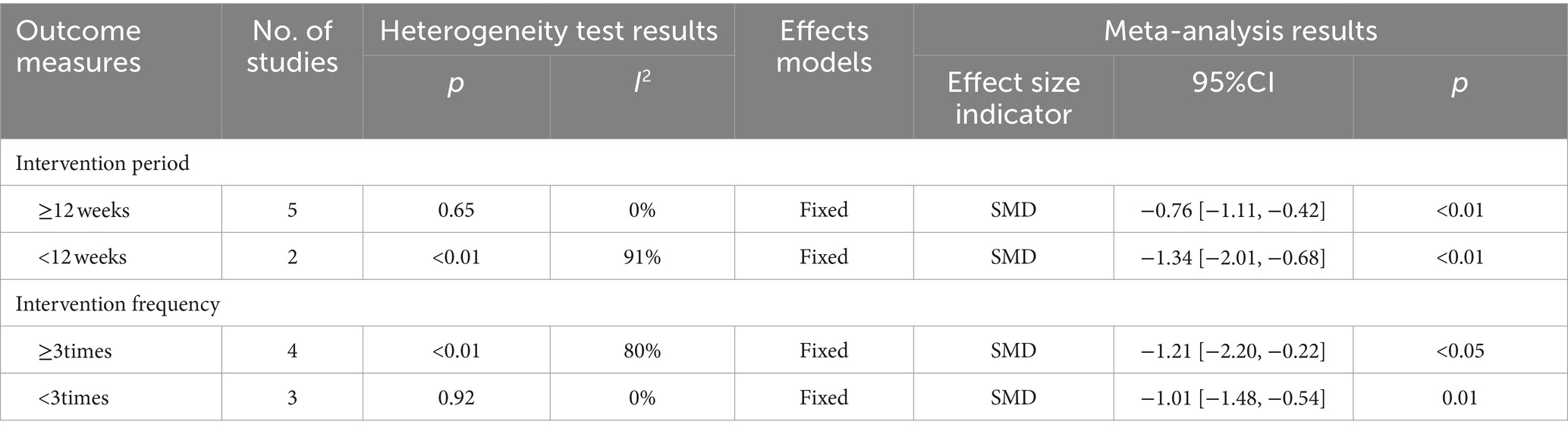
Table 5. Subgroup analysis of HOMA-IR.
3.5.4 Analysis of FPG subgroups
The results showed that the best intervention effect was achieved with a training period of ≥12 weeks [SMD = −0.38, 95%CI: −0.67, −0.09, p = 0.01] and a training frequency of ≥3 times/week [SMD = −0.92, 95%CI: −1.58, −0.25, p < 0.01] (Table 6).
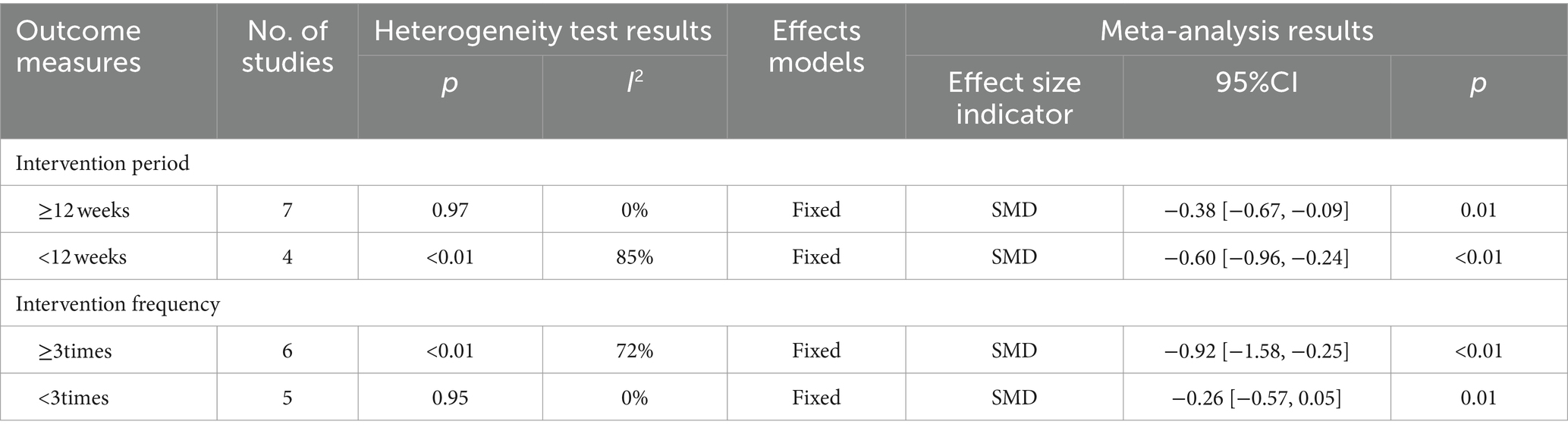
Table 6. Subgroup analysis of FPG.
3.6 Sensitivity analysis
Sensitivity analyses conducted on the included studies revealed no significant directional changes in the combined effect sizes upon the individual exclusion of studies. This indicates a robustness in the results of the meta-analyses. Due to space limitations, detailed results of the sensitivity analyses are available upon request from the corresponding author.
3.7 Publication bias
The funnel plots for studies involving BMI, WC, BF%, TG, TC, HDL-C, LDL-C, and FPG were generated and subjected to Egger’s bias test (Figure 15).
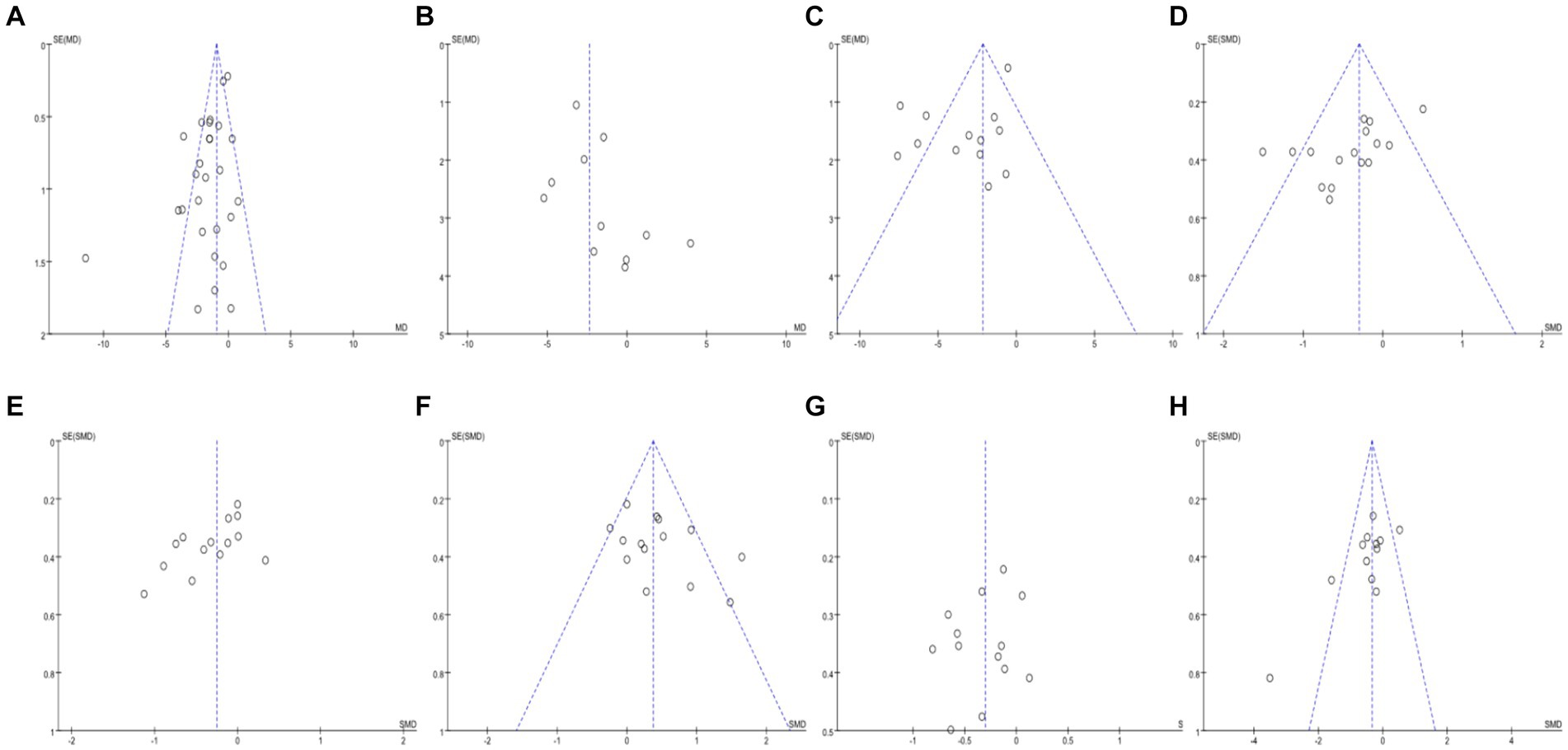
Figure 15. Funnel plots for different outcome indicators.
The distribution of the BMI funnel plot was roughly uneven, and Egger’s test yielded a Pr > |z| = 0.00, which is less than 0.05, indicating the presence of publication bias (Figure 15A). The WC funnel plot distribution was also roughly uneven, but Egger’s test resulted in a Pr > |z| = 0.15, which is greater than 0.05, suggesting no publication bias (Figure 15B). The BF% funnel plot distribution was roughly uneven, with Egger’s test showing a Pr > |z| = 0.00, less than 0.05, indicating publication bias (Figure 15C). The TG funnel plot distribution was roughly uneven, and Egger’s test showed a Pr > |z| value less than 0.05, indicating the presence of publication bias (Figure 15D). The TC funnel plot distribution was also roughly uneven, with Egger’s test yielding a Pr > |z| = 0.02, less than 0.05, indicating publication bias (Figure 15E). The HDL-C funnel plot distribution was roughly uneven, and Egger’s test showed a Pr > |z| = 0.02, less than 0.05, indicating publication bias (Figure 15F). The LDL-C funnel plot distribution was roughly even, and Egger’s test resulted in a Pr > |z| = 0.44, greater than 0.05, suggesting no publication bias (Figure 15G). Finally, the FPG funnel plot distribution was roughly uneven, with Egger’s test showing a Pr > |z| = 0.00, less than 0.05, indicating publication bias (Figure 15H).
4 Discussion
In the present study, AE + RT was found to be effective in improving several health indicators (except hs-CRP) in children and adolescents with overweight/obesity. This finding aligns with a prior study (38), suggesting a potential synergistic effect of AE + RT on diverse health parameters. Long-term and regular aerobic exercise reduces fat accumulation, leads to a decrease in plasma insulin, and improves overall physical function. Resistance exercise sustains energy expenditure after training and promotes muscle tissue production. The scientific arrangement of the two types of exercise contributes to the overall improvement of physical condition (39). The observed high heterogeneity in certain indicators may stem from disparities in training variables and variations in the proportions of AE and RT combinations, leading to notable discrepancies in the outcomes.
HDL-C is commonly associated with a diminished risk of cardiovascular disease due to its role in scavenging excess cholesterol from arterial walls and transporting it to the liver for metabolism and elimination. Data from 14 pieces of literature in this study showed that AE + RT increased HDL-C in children, and the literature was moderately heterogeneous (I2 = 54%). These findings deviate from the results reported in the meta-analysis conducted by Tianhao Chen (40) and other researchers, potentially attributed to the inclusion of studies focusing solely on aerobic exercise in their analyses, thus influencing the outcomes. Additionally, some scholars (41) suggested that HDL-C only improves when exercise intensity or duration reaches a certain threshold.
In our investigation, no significant difference was observed in hs-CRP levels, which contrasts with the findings reported by Jingqi Liu (42) et al. Their study revealed that both AT and AT+RT were effective in reducing CRP levels in adolescents with obesity, with AT+RT demonstrating superiority over AT alone. However, two out of the three studies included in the present study did not show a significant effect, which may be due to the differences in baseline indices, and differences in the duration and methodology of the intervention. Further research is warranted to elucidate the precise reasons underlying these inconsistencies.
Four key outcome metrics (BMI, TG, HOMA-IR, and FPG) were selected for the relevant subgroup analyses. These metrics were chosen to provide comprehensive information for a comprehensive assessment of health problems in children and adolescents with overweight/obesity. They encompass aspects of body mass, cardiovascular health, metabolic health, and insulin metabolism, collectively providing valuable insight into the health status and associated risks of children and adolescents with overweight/obesity.
In the subgroup analyses of the four indicators, studies with training cycles exceeding 18 weeks were excluded to align with practical considerations such as current teaching cycles and school schedules. Upon analyzing the BMI and TG subgroups, it was observed that children and adolescents with overweight/obesity benefited significantly from a training cycle of ≥12 weeks comprising more than three sessions per week, each session lasting over 60 min, resulting in notable improvements in BMI and TG levels. Therefore, it is recommended to adjust the ratio of AE to RT based on these training parameters to obtain a more stable and reliable effect.
When subgroup analyses of HOMA-IR and FPG were performed, training time subgroup analyses were not performed due to the limited number of studies in the training time subgroup. The results of the studies showed that training cycles up to 12 weeks showed larger effect sizes for both HOMA-IR and FPG, but the heterogeneity of the relevant literature was high (I2 > 70%). This discrepancy may be due to the higher sensitivity of human blood glucose levels to AE and the fact that the effect of interventions on glucose metabolism may differ when the ratio of AE to RT is different (43).
This study is subject to several limitations: (1) Dietary interventions and health education were not systematically excluded from the included literature. (2) Subgroup analyses based on age and gender among children and adolescents were not conducted. (3) The study did not conduct comparative analyses with either aerobic or resistance exercise alone, nor did it consider the potential influence of factors such as region, ethnicity, and lifestyle habits. (4) The synergy between aerobic and resistance exercises could not be quantified.
5 Conclusion
In summary, future studies should strive to incorporate detailed considerations of the characteristics of both aerobic and resistance exercises, while also taking into account factors such as age, body mass index, and psychological traits of children and adolescents with overweight/obesity. Based on the current evidence, the recommended exercise prescription is at least three sessions of more than 60 min per week for 12 weeks or more for better health benefits.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
Author contributions
XL: Conceptualization, Data curation, Writing – original draft, Writing – review & editing. QL: Writing – review & editing. FL: Methodology, Software, Supervision, Validation, Writing – review & editing. DZ: Investigation, Supervision, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. World Health Organization. (2018) Available at: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (Accessed January 18, 2022).
2. Gao, N. Effect of aerobic exercise combined with strength training on lipid and body composition of overweight and obese college students [Master's thesis]. Inner Mongolia: Inner Mongolia Normal University; (2022).
3. Yang, J, Ji, L, Yang, WL, and Jin, J. Research based on the effect of trans-theoretical model intervention of physical exercise on pupil’s self-efficiency, self-esteem and weight. J TUS. (2014) 29:185–9. doi: 10.13297/j.cnki.issn1005-0000.2014.03.007
4. National Disease Control and Prevention Administration. Physical activity level evaluation for children and adolescents aged 7~18 years. Beijing: National Disease Control and Prevention Administration (2023).
5. Fei, X, Li, C, and Li, HJ. Effectiveness of exercise on body composition for overweight and obese children and adolescents: a network meta-analysis. Chin J Sch Health. (2022) 43:372–7. doi: 10.16835/j.cnki.1000-9817.2022.03.013
6. Moher, D, Liberati, A, Tetzlaff, J, and Altman, DGPRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. (2009) 6:e1000097. doi: 10.1371/journal.pmed.1000097
7. Slim, K, Nini, E, Forestier, D, Kwiatkowski, F, Panis, Y, and Chipponi, J. Methodological index for non-randomized studies (minors): development and validation of a new instrument. ANZ J Surg. (2003) 73:712–6. doi: 10.1046/j.1445-2197.2003.02748.x
8. Higgins, JP, Thomas, J, Chandler, J, Cumpston, M, Li, TJ, Page, MJ, et al. Cochrane handbook for systematic reviews of interventions. Hoboken: John Wiley & Sons (2019).
9. Ahmadi, A, Moheb-Mohammadi, F, Navabi, ZS, Dehghani, M, Heydari, H, Sajjadi, F, et al. The effects of aerobic training, resistance training, combined training, and healthy eating recommendations on lipid profile and body mass index in overweight and obese children and adolescents: a randomized clinical trial. ARYA Atheroscler. (2020) 16:226–34. doi: 10.22122/arya.v16i5.1990
10. Bruyndonckx, L, Hoymans, VY, Guchtenaere, AD, Helvoirt, MV, Craenenbroeck, EMV, Frederix, G, et al. Diet, exercise, and endothelial function in obese adolescents. Pediatrics. (2015) 135:e653–61. doi: 10.1542/peds.2014-1577
11. Chae, HW, Kwon, YN, Rhie, YJ, Kim, HS, Kim, YS, Paik, IY, et al. Effects of a structured exercise program on insulin resistance, inflammatory markers and physical fitness in obese Korean children. J Pediatr Endocrinol Metab. (2010) 23:1065–72. doi: 10.1515/jpem.2010.168
12. Chen, Q, Cao, J, Zhao, LJ, and Yi, N. Effects of different exercise modes on body composition,inflammatory factors, and exercise capacity of obese teenagers. J Jilin Univ. (2015) 41:1070–5. doi: 10.13481/j.1671-587x.20150537
13. Cheng, HL, Peng, P, Zhu, R, and Qin, YS. Effects of eight weeks exercise prescription intervention on aerobic capacity, body composition, blood lipid and C-reactive protein in obese adolescents. J Jilin Univ. (2012) 38:745–9. doi: 10.13481/j.1671-587x.2012.04.003
14. Duft, RG, Castro, A, Bonfante, ILP, Lopes, WA, Silva, LRD, Chacon-Mikahil, MPT, et al. Altered metabolomic profiling of overweight and obese adolescents after combined training is associated with reduced insulin resistance. Sci Rep. (2020) 10:16880. doi: 10.1038/s41598-020-73943-y
15. Farpour-Lambert, NJ, Aggoun, Y, Marchand, LM, Martin, XE, Herrmann, FR, and Beghetti, M. Physical activity reduces systemic blood pressure and improves early markers of atherosclerosis in pre-pubertal obese children. J Am Coll Cardiol. (2009) 54:2396–406. doi: 10.1016/j.jacc.2009.08.030
16. Grace, J, Biggs, C, Naicker, A, and Moss, S. Effect of physical activity and nutrition education on body mass index, blood pressure and biochemical variables in overweight and obese adolescents. Ann Glob Health. (2021) 87:1–13. doi: 10.5334/aogh.3147
17. Gui, YL . Effects of 12-week exercise intervention on endothelium function among overweight and obese children. Chin J Sch Health. (2019) 40:26–30. doi: 10.16835/j.cnki.1000-9817.2019.01.007
18. Jeon, JY, Han, J, Kim, HJ, Park, MS, Seo, DY, Kwak, YS, et al. The combined effects of physical exercise training and detraining on adiponectin in overweight and obese children. Integr Med Res. (2013) 2:145–50. doi: 10.1016/j.imr.2013.10.001
19. Jia, ZJ . Effect of aerobic exercise combined with strength on health and physical fitness of overweight and obese students [Master’s thesis]. Inner Mongolia: Inner Mongolia Normal University. (2022).
20. Kim, HJ, Tak, YJ, Lee, SY, and Seo, JP. Effects of a 12-week diet versus diet plus aerobic and resistance exercise program on acylated and desacylated ghrelin, and ghrelin O-acyltransferase in adolescent girls with obesity. Int J Environ Res Public Health. (2022) 19:1480. doi: 10.3390/ijerph19031480
21. Li, X. Research on the effects of exercise on oxidative stress level and its related factors in obese young women [Master's thesis]. Fujian: Fujian Normal University (2008).
22. Liu, W, Cang, CQ, Zhao, XQ, Jiang, X, Chen, ZM, Xie, L, et al. Effect of school-based supervised exercise intervention on body mass index and Glucolipid metabolism in Chinese obese adolescents. Chin J Sports Med. (2008) 27:329–33. doi: 10.16038/j.1000-6710.2008.03.025
23. Lopes, WA, Leite, N, Silva, LRD, Brunelli, DT, Gáspari, AF, Radominski, RB, et al. Effects of 12 weeks of combined training without caloric restriction on inflammatory markers in overweight girls. J Sports Sci. (2016) 34:1902–12. doi: 10.1080/02640414.2016.1142107
24. Loureiro, V, Morais, A, and Leal, J. Anthropometric measures, aerobic and muscular fitness: effect of an exercise program applied in school context. J Sport Health Res. (2020) 12:374–83.
25. Martínez, VV, Salcedo, AF, Franquelo, GR, Solera, MM, Sánchez, ML, Serrano, MM, et al. Assessment of an after-school physical activity program to prevent obesity among 9- to 10-year-old children: a cluster randomized trial. Int J Obes. (2008) 32:12–22. doi: 10.1038/sj.ijo.0803738
26. Pan, X, Xia, T, Gao, Y, Jiang, LP, and Zhang, YF. Randomized controlled study of factors influencing body composition and exercise quality of male adolescents aged 13–15 years based on cross-lagged models: obesity level, salivary testosterone, and exercise combined with caloric restriction intervention. J Men’s Health. (2022) 18:204–11. doi: 10.31083/j.jomh1810204
27. Park, JH, Miyashita, M, Kwon, YC, Park, HT, Kim, EH, Park, JK, et al. A 12-week after-school physical activity programme improves endothelial cell function in overweight and obese children: a randomised controlled study. BMC Pediatr. (2012) 12:111. doi: 10.1186/1471-2431-12-111
28. Sung, TRY, Yu, CW, Chang, SKY, Mo, SW, Woo, KS, and Lam, CWK. Effects of dietary intervention and strength training on blood lipid level in obese children. Arch Dis Child. (2002) 86:407–10. doi: 10.1136/adc.86.6.407
29. Wang, YM . Effect of exercise intervention on physical health of obese adolescents [Master’s thesis]. Shaanx: Xi’an Physical Education University (2018).
30. Wang, ZQ . Analysis on effects of comprehensive behavior intervention in curing the pure obesity of the children [Master’s thesis]. Hunan: Hunan Normal University (2007).
31. Wang, BB . The impact of exercise on body composition, fat distribution,and physical fitness of obese adolescents [Master’s thesis]. Beijing: Beijing Sport University. (2005).
32. Wong, PC, Chia, MY, Tsou, IY, Wansaicheong, KL, Tan, B, Wang, CK, et al. Effects of a 12-week exercise training programme on aerobic fitness, body composition, blood lipids and C-reactive protein in adolescents with obesity. Ann Acad Med Singap. (2008) 37:286–93. doi: 10.47102/annals-acadmedsg.V37N4p286
33. Wu, F. Effect of exercise combined with health education intervention on fat reduction in obese children [Master's thesis]. Yangzhou: Yangzhou University (2020).
34. Xiang, MQ, Liao, JW, Huang, JH, Deng, HL, Wang, D, Xu, ZB, et al. Effect of a combined exercise and dietary intervention on self-control in obese adolescents. Front Psychol. (2019) 10:1385. doi: 10.3389/fpsyg.2019.01385
35. Zehsaz, F, Farhangi, N, and Ghahramani, M. Exercise training lowers serum chemerin concentration in obese children. Science Sports. (2017) 32:39–45. doi: 10.1016/j.scispo.2016.07.007
36. Zhang, JQ . The study of the intervention effect of exercise and health education on serum inflammatory factors and insulin resistance in obese children [Master’s thesis]. Yangzhou: Yangzhou University (2018).
37. Zhen, L. The effects of exercise-based comprehensive long-term intervention on overweight and obese children [Master's thesis]. Beijing: Capital University of Physical Education and Sports; (2010).
38. Kelley, GA, Kelley, K, and Pate, RR. Exercise and adiposity in overweight and obese children and adolescents: a systematic review with network meta-analysis of randomised trials. BMJ Open (2019)9:e031220, doi: 10.1136/bmjopen-2019-031220
39. Xu, XK . Affect research of combining aerobic exercise with strength training in weight-losing. Bull Sport Sci Technol. (2015) 23:79–80.
40. Chen, T, Lin, J, Lin, Y, Xu, L, Lu, D, Li, FP, et al. Effects of aerobic exercise and resistance exercise on physical indexes and cardiovascular risk factors in obese and overweight school-age children: a systematic review and meta-analysis. PLoS One. (2021) 16:e0257150. doi: 10.1371/journal.pone.0257150
41. Rashid, S, and Genest, J. Effect of obesity on high-density lipoprotein metabolism. Obesity (Silver Spring, MD). (2007) 15:2875–88. doi: 10.1038/oby.2007.342
42. Liu, JQ, Lu, JD, Liang, TJ, Chen, SN, and Su, H. Meta-analysis of effectiveness of different exercises on inflammatory response in obese adolescents. Chin J Sch Health. (2022) 43:45–52. doi: 10.16835/j.cnki.1000-9817.2022.01.011
Keywords: aerobic exercise, resistance training, body composition, metabolic diseases, pediatric obesity
Citation: Liu X, Li Q, Lu F and Zhu D (2024) Effects of aerobic exercise combined with resistance training on body composition and metabolic health in children and adolescents with overweight or obesity: systematic review and meta-analysis. Front. Public Health. 12:1409660. doi: 10.3389/fpubh.2024.1409660
Edited by:
Noelia Gonzalez-Galvez, Independent Researcher, Murcia, SpainReviewed by:
Fatemeh Kazeminasab, University of Kashan, IranFernanda Thomazini, Federal University of São Paulo, Brazil
Copyright © 2024 Liu, Li, Lu and Zhu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Qiang Li, ODczOTA1Nzg2QHFxLmNvbQ==