 Gete Berihun1
Gete Berihun1 Kassahun Ayele Gasheya2*
Kassahun Ayele Gasheya2* Tadiwos Abebaw2
Tadiwos Abebaw2 Masresha Abebe1Adinew Gizeyiatu1Leykun Berhanu1Mengesha Dagne1
Masresha Abebe1Adinew Gizeyiatu1Leykun Berhanu1Mengesha Dagne1 Belay Desye1Zebader Walle3Leul Zewdu4
Belay Desye1Zebader Walle3Leul Zewdu4 Mebrat Gedfie Wondim4
Mebrat Gedfie Wondim4- 1Department of Environmental Health, College of Medicine and Health Sciences, Wollo University, Dessie, Ethiopia
- 2Department of Occupational Health and Safety, College of Medicine and Health Sciences, Wollo University, Dessie, Ethiopia
- 3Department of Public Health, College of Health Sciences, Debre Tabor University, Debre Tabor, Ethiopia
- 4Department of Special Needs and Inclusiveness, College of Social Sciences and Humanities, Debre Tabor University, Debre Tabor, Ethiopia
Introduction: Musculoskeletal disorders are the leading cause of illness, disability, and poor quality of life. Lack of access to potable water in the backyard forces women to take water from off-plot sources every day, which may expose them to various health risks. However, there has been little investigation on the musculoskeletal disorders’ health effects on water-carrying women.
Objective: This study aimed to assess musculoskeletal disorders symptoms and associated factors among water-carrying women in the Legambo district, Northeastern Ethiopia.
Materials and methods: A community-based cross-sectional study was done with 618 water-carrying women chosen using simple random and systematic random sampling techniques. The data were collected using face-to-face interviews with the standard Nordic Musculoskeletal Questionnaire. Data entry were carried out using Epi-data version 4.6 and exported to SPSS version 25.0 for analysis. A binary logistic regression was used to determine the factors associated with self-reported musculoskeletal disorder symptoms at a 95% confidence interval (CI). In the multivariate model, variables with a p-value ≤0.05 and a 95% CI were declared as factors of self-reported musculoskeletal disorder symptoms. The model’s fitness was assessed using Hosmer and Lemeshow, and it was found to be fit.
Results: The prevalence of self-reported MSD symptoms was 72.5% during the previous 12 months. MSD symptoms were significantly elevated among women who carried water from a distance of 501–1,000 m [adjusted odds ratio (AOR) = 5.39, 95% CI = 3.64–9.69] and >1,000 m (5.93, 2.84–12.40), carried a water load of >15 kg during pregnancy (8.29, 2.97–23.09), and carried a water load of >15 kg when not pregnant (1.59, 1.44–2.68).
Conclusion: Three-fourths of the participants had self-reported musculoskeletal disorder symptoms in the past 12 months. Distance of water sources from their house, carrying the same amount of water during pregnancy, and weight of the water load carrying were factors associated with the self-reported musculoskeletal disorder symptoms. Hence, health professionals should raise awareness of the association between carrying high water loads and the development of MSDs, especially during pregnancy. Improvement in water supply infrastructure and enhancing behavioral intervention should be done. Furthermore, Future researchers should assess MSDs using objective measurements and cohort studies should be implemented.
Introduction
Musculoskeletal disorders (MSDs) encompass a wide range of inflammatory and degenerative diseases affecting muscles, ligaments, tendons, nerves, bones, and joints (1–3). They are a major cause of illness in many countries, particularly developing countries, including Ethiopia. Work-related pain is becoming more prevalent, particularly among rural and disadvantaged people in developing countries (4). Workers in a variety of settings, including manufacturing, construction, agriculture, and transportation, who use their bare hands to operate tools, machines, and equipment in their daily lives are frequently subjected to uncomfortable postures, overextension, force exertion, and repetitive movements over long periods, which can result in serious injury or disability (5).
About one-quarter of the global population obtains their water from sources located away from their homes (6, 7). This off-premises water collection is common in low-income and middle-income regions where public water infrastructure is either inadequate or absent (8). As a result, women are often responsible for manually transporting large 20-liter containers of water, typically carrying them on their heads or other body parts (8, 9). More than two-thirds of the population in sub-Saharan Africa are obligated to leave their homes to collect water, and many rural water systems are often non-functional, exacerbating the difficulty of water collection and augmenting health problems (10). This physical water carriage can cause pain and mobility problems, which are key symptoms of musculoskeletal disorders (MSDs). These physical impacts may impair the quality of life and contribute to psychosocial stress for the women tasked with this labor (7, 9–11).
The Joint Monitoring Programme (JMP) report in 2017 revealed that 263 million people spent over 30 min per round trip to collect water from an improved water source (12). People who use unimproved or surface waters are more likely to take over 30 min to collect water (8). A study conducted in sub-Saharan African countries revealed that about 13.54 million women are responsible for household water collection taking more than 30 min per return trip in the region (10).
The impacts of fetching water on women’s health and ability to work are expected to be more pronounced in low- and middle-income nations where a larger number of people have engaged in physically demanding, informal, or poorly regulated work situations. Furthermore, economic, political, and social disparities are mirrored in access to drinking water. Furthermore, the negative economic and health effects of obtaining water are likely to disproportionately affect underprivileged groups (11). Despite water collection can hurt human health, only a few studies have been undertaken on its negative effects, such as weariness, musculoskeletal damage, and early degenerative bone and soft tissue injury (10). The most commonly reported adverse effect among the 39 water transporters in South Africa was spinal pain, at 69% (11). The problem is high in rural areas due to the presence of different confounding factors such as higher rates of poverty, chronic malnutrition, and poor health (10).
In 2017, 785 million people still lacked even a basic drinking water service (13). The problem is highly magnified in sub-Saharan Africa with half of the urban households getting their water sources outside of the home with the highest burden in rural areas reaching up to 89.5% (14). Despite different interventions being implemented to improve the accessibility of safe water supply, the problem still exists in all parts of the world with severe problems in developing countries including Ethiopia. The impacts of water carrying on MSDs are underreported which may be due to the little attention to date (6, 11). Hence, this study aimed to assess the self-reported MSDs symptoms and associated factors among water-carrying women in the Legambo district, Northeastern Ethiopia.
Materials and methods
Study area
The study was conducted in Legambo district which is located in South Wollo zone, Amhara Region, Ethiopia. The district has a total population of 189, 898 of which 178,420 were rural inhabitants whereas 11,478 were urban residents (15). The district has an area of 1017.35 km2 and an altitude range of 1,500–3,700 m. In Legambo district, there is one primary hospital, nine health centers, 10 private clinics, three private pharmacies, and 34 health posts (16). The district has 32 kebeles [the smallest administrative unit in Ethiopia (17)].
Study design and period
A community-based cross-sectional study design was done to assess the prevalence of self-reported MSDs and associated factors among water carrier women in Legambo district, Northeastern Ethiopia. The study was conducted from July 1–30, 2022.
Source and study population
The source population of the study was women in the Legambo district, South Wollo zone, Northeastern Ethiopia. On the other hand, women who lived in randomly selected eight kebeles of Legambo district, Northeastern Ethiopia were considered as the study population.
Eligibility criteria
Inclusion criteria
The inclusion criteria were (1) having lived in the study location for at least 12 months; (2) ≥18 years of age; (3) having <5 children; and (4) providing informed consent to participate in the study.
Exclusion criteria
The exclusion criteria were (1) women with non-regular water carrying women; (2) used non-human means of water carrying technique; (3) those with a serious medical illness during the data collection; (4) had a history of previous musculoskeletal surgery; and (5) obvious skeletal deformities.
Sample size estimation and sampling procedures
The sample size was estimated using a single population proportion formula taking the assumptions of the desired level of confidence (95% confidence interval), an acceptable margin of error (0.05), and the design effect of the sampling technique (1.5), the estimated proportion of self-reported MSDs symptoms (50%), and 10% non-response rate which gives the sample size of 633. A mixture of multistage sampling, simple random sampling, and systematic sampling techniques was employed to select participants in the study. Initially, 8 kebeles were selected from a total of 32 kebeles by a simple random sampling technique using a lottery method. Then, the households from the selected kebeles were selected using a systematic random sampling technique which was obtained from the health posts of the respective kebeles. Then, proportional allocations based on the eligible participants were carried out to determine the number of participants in each kebele.
Outcome variable
The outcome variable of the study was self-reported musculoskeletal disorder symptoms with the option either (yes/no).
Operational definitions
Self-reported MSDs symptoms
It is defined as a self-report of one or more body parts having pain, numbness, tingling, aching, stiffness, or burning, Pain continued in any part of body segments (neck, shoulders, upper back, lower back, elbows, wrists/hands, thighs/hips, knees, and ankles) caused, aggravated or exacerbated by workplace exposures pain lasting >3 days during the period for the past 12 months (18–22).
Data collection tools and techniques
Data were collected using a structured questionnaire based on the Standardized Nordic Questionnaire (SNQ). The questionnaire was initially written in English, then translated into the local language (Amharic), and finally returned to English to ensure its consistency. The questionnaire has four sections: Part I: (socio-demographic characteristics of the respondents); Part II: (pregnancy-related conditions); Part III: water-carrying practice; and Part IV: self-reported MSD symptoms in the last 12 months. The presence of self-reported MSD symptoms over the previous 12 months was evaluated. The weight of the load, the weight of the ladies, and the height of the participants were all assessed, and their BMI was determined by dividing the weight in kg by height square in meters. Beam balance was used to measure the weight of the load and the weight of the women. Data were collected using a combination of face-to-face interviews, observation checklists, and physical measurements. The data collection was carried out by four individuals who held Bachelor of Science (BSc) degrees in Nursing and supervised by experts in human anatomy. This data collection took place from July 1 to July 30, 2022.
Data quality assurance
The Data quality were ensured through different measures. A standardized questionnaire was used for data collection. Before data collection, the data collectors and supervisors were given 2 days of training. The contents of the training include the study objectives, content of the questionnaire, data collection procedures, and other relevant issues. Additionally, a pre-test was conducted on 5% of the sample size in the Dessie Zuria district and necessary amendments were carried out based on its feedback. During the final data collection, daily supervision was carried out and immediate correction was done for incomplete or missing data. Furthermore, a quality check was performed on 10% of the entered data to identify and address any data entry errors.
Data management and analysis
Data entry and analysis were carried out using Epi-data version 4.6 and SPSS version 25, respectively. Descriptive statistics were employed to present the findings. A binary logistic regression model with a 95% CI was used to investigate the association between the predictor and outcome variables of the study. Initially, in bi-variable analysis variables with a p-value <0.25 were retained for multivariable logistic regression analysis. Then, in a multivariate analysis, variables with a p-value <0.05 were declared as factors significantly associated with the prevalence of self-reported MSDs among water-carrying women. The multi-collinearity among independent variables were also assessed using standard error at a cutoff value of −2 to +2. The model’s fitness was assessed using the Hosmer–Lemeshow test and it was fit.
Ethics approval
The ethical approval was obtained from Wollo University’s College of Medicine and Health Sciences’ research and ethical committee under the reference number CMHS/526/20/14. Permission was received from the Legambo district administration. Following an explanation of the research purpose, participants who could read and write gave written consent, whereas those who could not verbal consent. The confidentiality of the study participants was assured by avoiding potential identifiers such as their names. Participants were also advised that they might refuse, withdraw, or completely reject their participation in the study. Finally, participants were informed that there were no incentives to engage in this study.
Results
Socio-demographic characteristics of the respondents
Table 1 presents the socio-demographic characteristics of the participants; a total of 618 women participated in the study with a response rate of 97.6%. The mean age of the participants was 33 ± 7 (mean with standard deviation). One-third of the participants were unable to read and write and two-thirds (68.6%) lived their lives through agricultural activities. Two-thirds (67%) of the study participants were underweight (<18.5). More than three-quarters (83.5%) of the participants visited healthcare facilities in the past year.

Table 1. Socio-demographic characteristics of the water-carrying women in Legambo district South Wollo zone, Northeastern Ethiopia in 2022.
Pregnancy-related variables
Table 2 presents and pregnancy-related variables of the participants; nearly three-forth (71.2%) of the respondents had four and above parity. More than half of 300 (55.2%) of the respondents had their first childbirth at the age of less than 18 years old. On the other hand, less than 10 % 45 (7.3%) of the respondents had a history of abortion in their lifetime. Additionally, less than a quarter of the respondents 97 (15.7%) were pregnant during the survey time. Of these, about (10.3%) of the respondents were in the third-trimester stage.
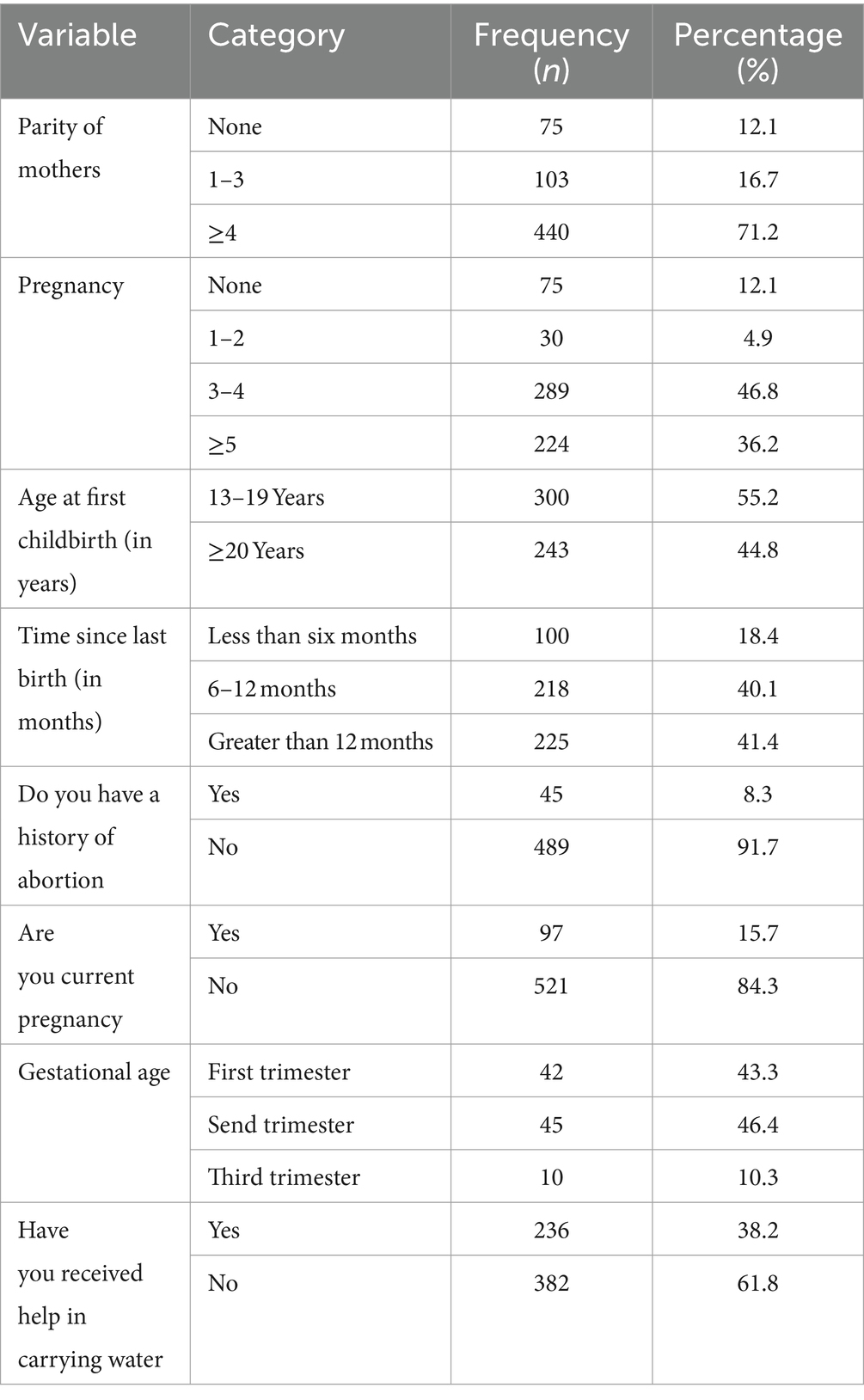
Table 2. Pregnancy-related variables of the water-carrying women in Legambo district, South Wollo zone, Northeastern Ethiopia in 2022.
Water-carrying related factors
Table 3 presents water-carrying related factors of the participants; nearly, two-thirds of 397 (63.6%) of the respondent’s main sources of water supply were located within a 500-meter distance from their house. Three out of five, 372 (60.2%) of the women carry >15 kg of water from the source. Half 284 (52.3%) of the women reported that they had a habit of water carrying during pregnancy with approximately similar load in the absence of pregnancy time. Nearly half of the women carry water two times daily. Furthermore, one-third 205 (33.2%) of the respondents practiced keeping their backs straight. On the other hand, the majority of the respondents 251 (406%) applied Bending knees in the lifting of the water sources.
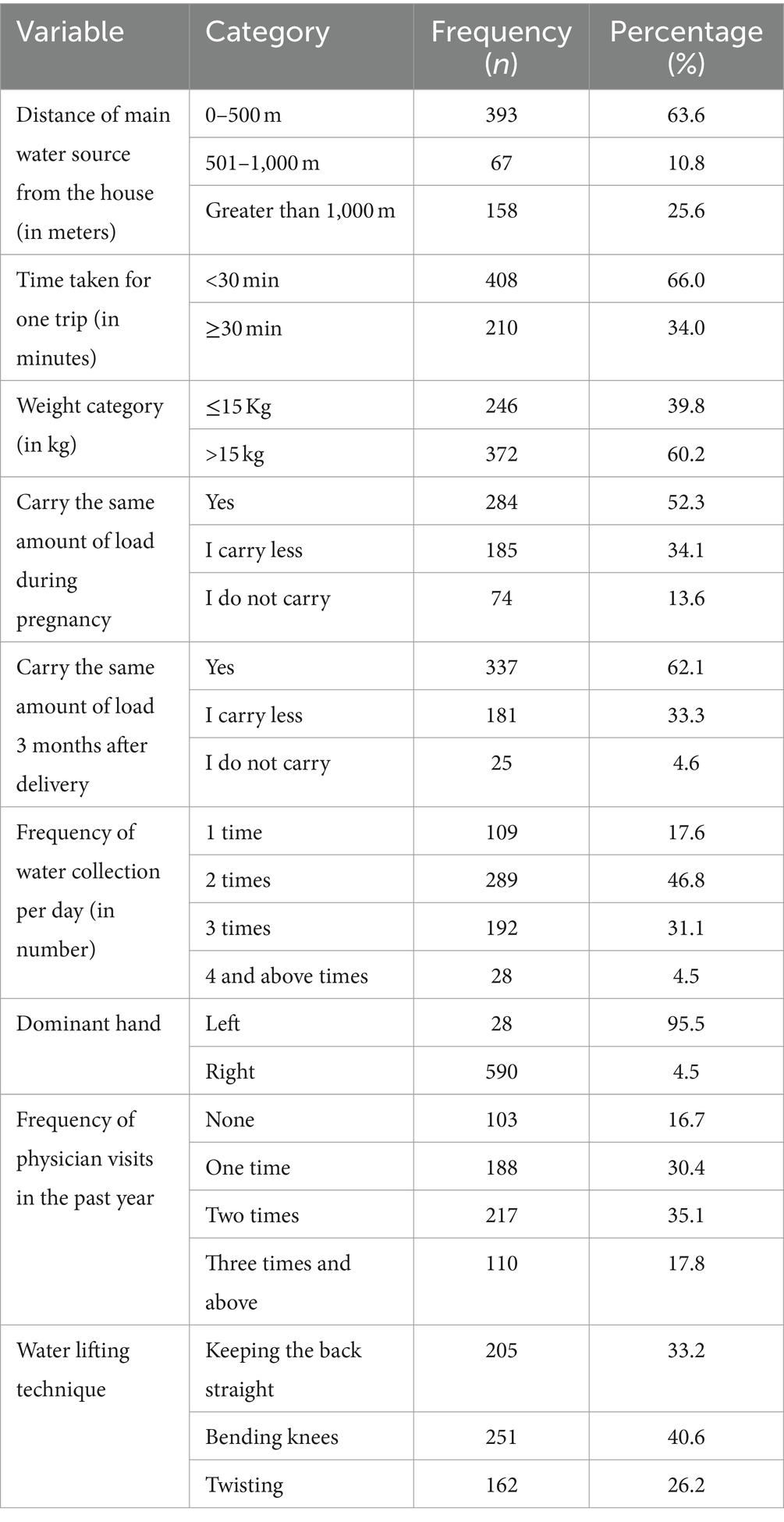
Table 3. Water carrying and related conditions among water-carrying women in Legambo district, South Wollo zone, Northeastern Ethiopia in 2022.
Self-reported MSDs symptoms
Table 4 presents the self-reported MSDs symptoms of the participants; more than two-thirds of 422 (68.3%) of the respondents reported that they had pain or discomfort in the neck during the past year. Additionally, an almost similar number of the participants 420 (68.0%) reported they had pain or discomfort in their lower backs during the past year. On the other hand, nearly two-thirds of 392 (63.4%) of the study participants had pain or discomfort in the shoulders. Generally, this finding revealed that the prevalence of self-reported MSDs symptoms among water-carrying women was 448 (72.5%).
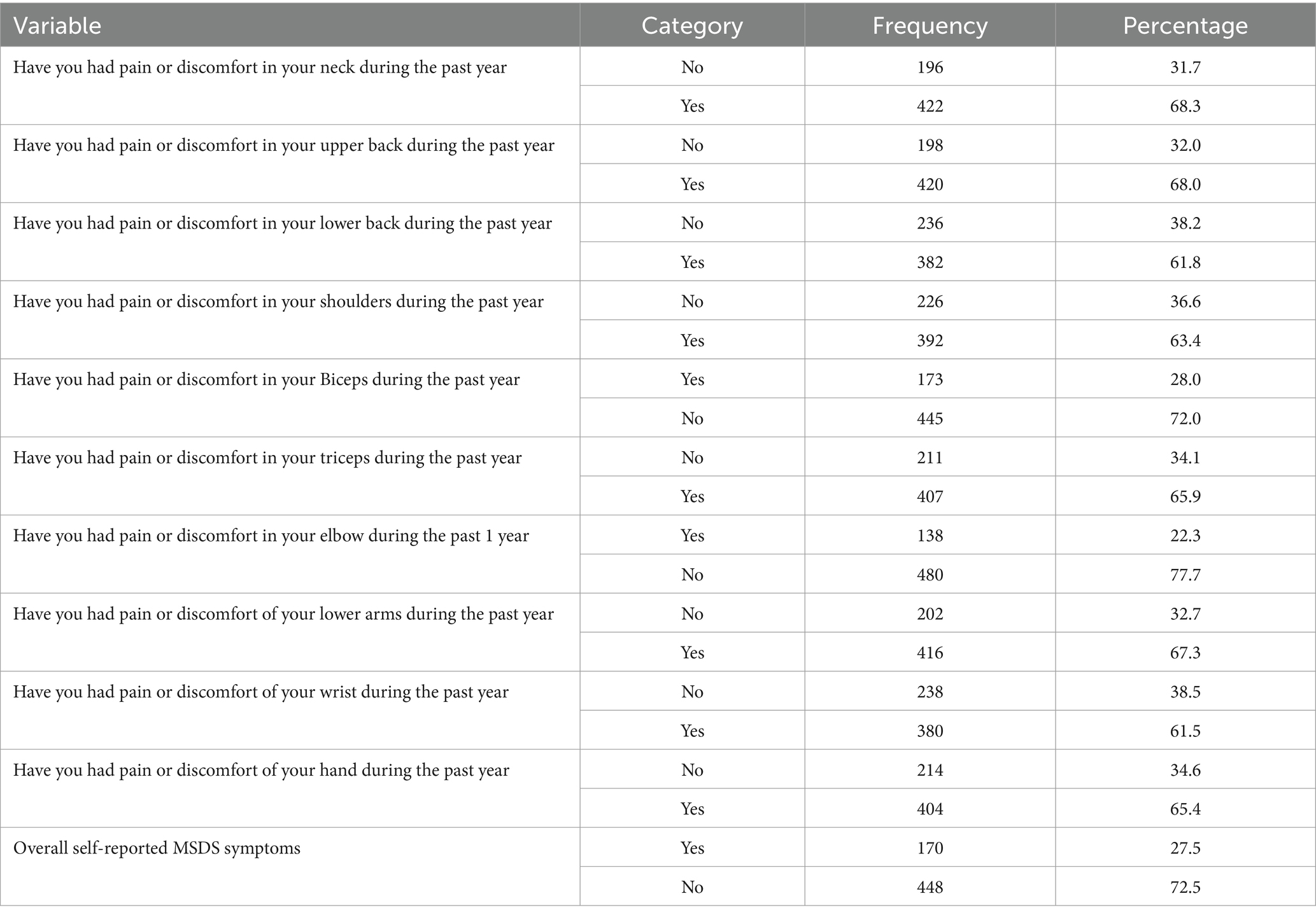
Table 4. Prevalence of self-reported musculoskeletal disorder symptoms in different parts of the body among water-carrying women in Legambo district, South Wollo zone, Northeastern Ethiopia in 2022.
Factors associated with self-reported MSDs symptoms
Table 5 presents factors associated with self-reported MSDs symptoms of the participants; in multivariable logistic regression analysis, the distance of the main source of water, weight of the load carrying, and carrying the same amount of load during pregnancy were factors of self-reported MSDs symptoms among water-carrying women. Those who carried water from 501 to 1,000 m and above 1,000 m distance were AOR = 5.39 (95% CI, 3.64, 9.69) and AOR = 5.93, (95%CI, 2.84, 12.40) times more likely to have self-reported MSDs symptoms than those who carried within a distance of 500 m, respectively. Furthermore, women who carried the same amount of water load during pregnancy were AOR = 8.29 (95%CI, 2.97, 23.09) times more likely to have self-reported MSDs symptoms than those who did not carry water during their pregnancy. Finally, women who carried water more than 15 kg were AOR = 1.59, (95%CI, 1.44, 2.68) times more likely to have a self-reported MSDs symptom than those who carried less than 15 kg.
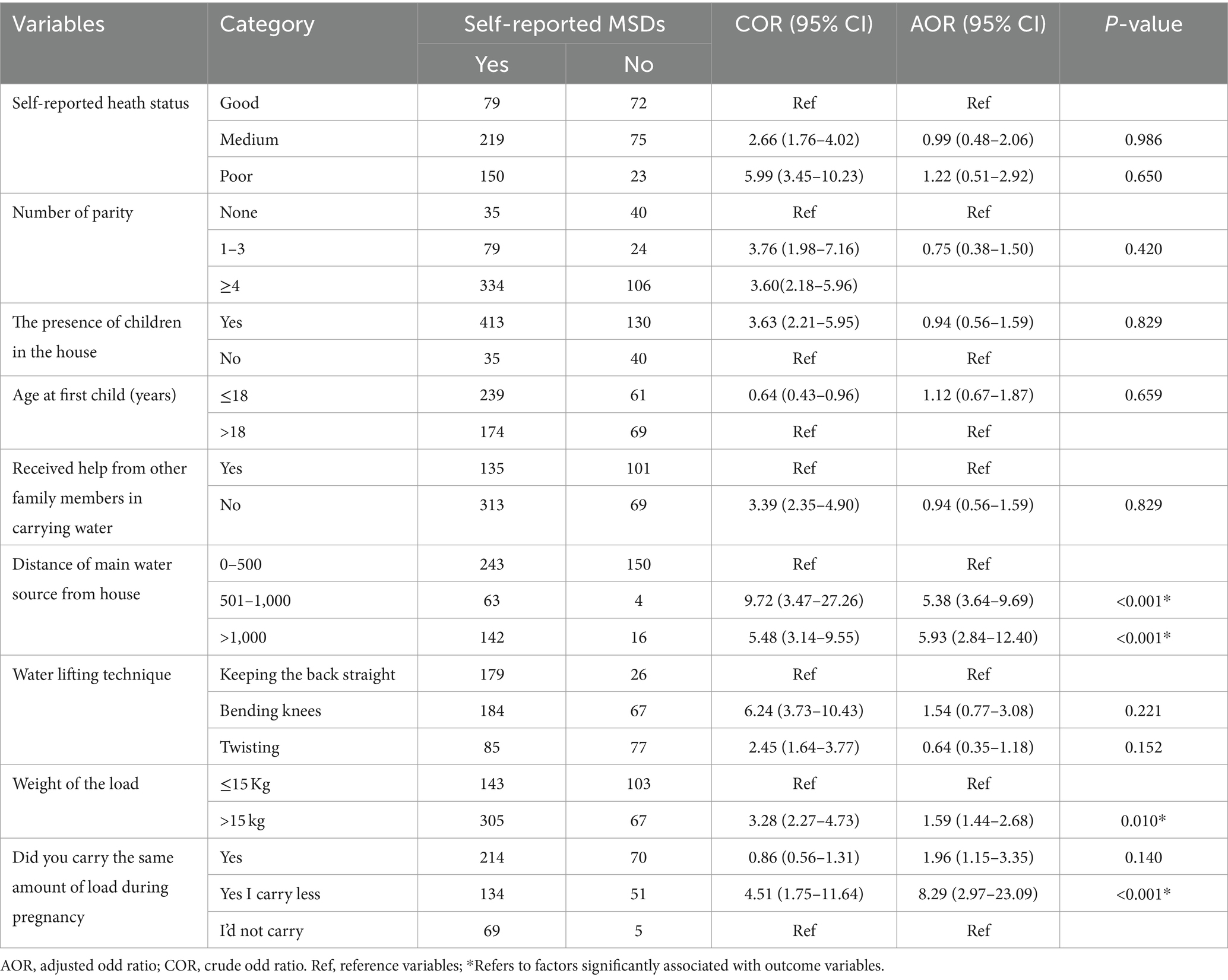
Table 5. Factors associated with self-reported musculoskeletal disorder symptoms among water carrier women in Legambo district, South Wollo zone, Northeastern Ethiopia in 2022.
Discussion
The MSDs cause an enormous global disease burden with the highest disability and the fourth highest burden of all non-communicable diseases, particularly in developing countries including Ethiopia. However, there are still major gaps in the understanding of the prevalence of the problem and its determinant factors (20). Based on the WHO report in 2019, the MSDs was the leading cause of disabilities worldwide and accounted for the greatest proportion of loss of productivity at the workplace (22). This finding revealed that nearly three-quarters (72.5%) of the participants had self-reported MSDs symptoms in the past 12 months. Distance of main sources of water supply from home, carrying the same amount of water load during the pregnancy, and weight of water load carrying were factors of self-reported MSDs symptoms among participants of the study.
This finding indicated that the overall prevalence of self-reported MSDs symptoms among water-carrying women was 72.5% which was consistent with the study conducted in Brazil (72.7%) (23). However, this result was greater than that of studies done in Ethiopia with healthcare professionals 64.2% (24), 40.1% (25), hairdressers (47.5%) (26), computer users (bankers) (58.8%) (27), and healthcare providers (44.2%) (28), diabetic patients (23.29%) (29), barber workers (55.7%) (30), and cleaners (52.3%) (31).
On the contrary, this finding was lower than the studies conducted among teachers in Chile (88.9%) (32), University teaching staff in Cameroon (80.8%) (22), cleaners of health institutions in Ethiopia (83.1%) (33), school teachers in Chuquisaca, Bolivia 86% (34), heavy load carriers in Yaoundé city, Cameroon 100% (35), restaurant Workers in Ethiopia (81.5%) (36). The possible reason for this variation might be due to the variation in water-carrying practices in different parts of the world such as carrying on the head, on the waist, and the variation in water containers using either a basket or straps tied around the head to carry water containers (20).
Off-plot access to water commonly requires a household member to complete multiple water-collecting trips to meet the needs of the household consumption (13, 37). This finding revealed that more than a quarter of the respondents were obligated to travel to a minimum distance of 1,000 m to reach the main sources of water for a single trip which is a useful indicator of exposure time to sustained compressive loading (11). The burden of water carrying depends not only on its distance but also on other factors such as walking to a source, joining long queues, filling containers, and carrying them home and environmental factors, particularly the incline or gradient of the path along which water is carried are likely to influence the physical work of water carrying (11, 38). People with the problem of MSDs may experience difficulty in carrying water and are obliged to seek help from others. This problem affects the family members in terms of a reduction in the usual volumes of water collected to support health and adequate hygiene (11). The practice of water carrying is one of the known risk factors for the development of MSDs (6, 14). Therefore, women who are responsible for these tasks are highly vulnerable to such types of problems, especially in low and middle-income countries (13).
In Ethiopia, only 50% of rural and urban households have access to essential water services, defined as water from an improved source with a collection time of no more than 30 min round trip (39). The weight load should be in the range of 10 to 15 kg to prevent the occurrences of MSDs (20). This finding showed that nearly two-thirds (60.2%) of the participants carried greater than 15 kg which is a lead for the occurrences of MSDs symptoms. This finding revealed that the weight of the water container was one of the factors that affect the prevalence of MSDs which was matched with other findings (11, 21). Furthermore, the maximum recommended backpack weights should be limited to 10–15% of body weight or less. However, this finding revealed that the ratio reaches up to 50% and above which is 5 times higher than the recommended level. Hence, frequent exposure to such amounts of unbalanced load may lead to increments of the problem (11). The problems may be worsening during the dry season since this study was conducted during the rainy season which has an alternate source of water supply (20).
The recommended maximum loads during the first trimester should be within the range of 7–11 kg and should not be lifted by themselves from the ground. But in this finding, almost all women carried the load by lifting from the ground which contrasts with the standard guideline with frequent practices in the likelihood of different health risks, MSDs. The problem may also result in a three-times-higher risk of preterm labor and miscarriages. Furthermore, it is also recommended that no loads heavier than the baby should be carried until 6 weeks postpartum and no “very heavy loads should be carried until 3 months postpartum”. However, most of the women in low and middle-income countries do not meet this strategy, including the findings of this study (6). The finding of the current study revealed that most of the women during pregnancy and 3 months after delivery carried even an equal load with non-pregnant women was another factor of MSDs among the participants of the study (40). This study’s overall implications could aid in the development of interventions, improve the quality of life for these populations, advance gender equality, and contribute to the body of knowledge regarding the relationship between gender, labor, and health.
Limitations of the study
This study has a few drawbacks. The data were cross-sectional, thus we cannot draw causal conclusions. Additionally, MSDs symptoms were assessed using respondents’ self-reported data, which may be prone to social desirability bias.
Conclusion
In conclusion, over three-quarters of the participants reported MSDS symptoms within the previous year. The distance between water sources and their homes, the practice of carrying the same amount of water during pregnancy, and the weight of the load carried were factors significantly associated with self-reported MSDS symptoms among water-carrying women. Hence, improvements to water supply infrastructure, promotion of intermediary solutions such as carts, bicycles, and self-supply options, particularly for women living in hilly areas, and interventions on behavioral modification should be done. Future research should use objective measurement of diagnosing MSDs diagnosis using a cohort study design. Future research should investigate the association between the intensity, frequency, and duration of water loading and the development of MSDs.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Author contributions
GB: Conceptualization, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. KG: Conceptualization, Formal analysis, Investigation, Methodology, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. TA: Software, Supervision, Validation, Visualization, Writing – review & editing. MA: Formal analysis, Methodology, Supervision, Writing – review & editing. AG: Conceptualization, Software, Supervision, Validation, Writing – review & editing. LB: Conceptualization, Methodology, Supervision, Writing – review & editing. MD: Formal analysis, Software, Supervision, Validation, Writing – review & editing. BD: Supervision, Writing – original draft, Writing – review & editing. ZW: Formal analysis, Methodology, Validation, Writing – original draft, Writing – review & editing. LZ: Supervision, Visualization, Writing – review & editing. MW: Supervision, Validation, Visualization, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. This research project was sponsored by Wollo University with Grant no. WU/7656/201/14.
Acknowledgments
First and foremost, we would like to thank the almighty God for reaching this level. We would like to express our deepest gratitude to Wollo University for funding this research project. We also want to extend our thanks to those who gave valuable comments from proposal development up to the final stage of this research project.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Abbreviations
AOR, Adjusted Odd Ratio; CI, Confidence interval; COR, Crude Odd Ratio; JMP, Joint Monitoring Program; MSD, Musculoskeletal disorder; WHO, World Health Organization.
References
1. Erick, PN, and Smith, DR. A systematic review of musculoskeletal disorders among school teachers. BMC Musculoskelet Disord. (2011) 12:260. doi: 10.1186/1471-2474-12-260
2. Claus, M, Kimbel, R, Letzel, S, and Rose, D. Occupational injuries of teachers and educational staff at special schools with multiple and severely handicapped children in Rhineland-Palatinate (Germany): results of a cross-sectional study. J Occup Health. (2015) 57:465–73. doi: 10.1539/joh.14-0210-OA
3. Chakraborty, S, Bhattacharjee, S, Mukherjee, A, and Dasgupta, S. Prevalence of musculoskeletal disorders and their association with ergonomic physical risk factors among women working in tea gardens of Darjeeling district of West Bengal. India Int J Occup Safe Health. (2021) 11:31–9. doi: 10.3126/ijosh.v11i1.35179
4. Jacobs, RJ, Collias, BA, Rana, AM, Wallace, EM, Michael, NK, and Boesler, DR. Identification of musculoskeletal disorders in medically underserved regions of South America and Vietnam. J Osteopath Med. (2015) 115:12–22. doi: 10.7556/jaoa.2015.003
5. Naik, G, and Khan, MR. Prevalence of MSDs and postural risk assessment in floor mopping activity through subjective and objective measures. Safe Health Work. (2020) 11:80–7. doi: 10.1016/j.shaw.2019.12.005
6. Geere, J-A, Bartram, J, Bates, L, Danquah, L, Evans, B, Fisher, MB, et al. Carrying water may be a major contributor to disability from musculoskeletal disorders in low-income countries: a cross-sectional survey in South Africa, Ghana, and Vietnam. J Glob Health. (2018) 8:010406. doi: 10.7189/jogh.08.010406
7. Tomberge, VMJ, Bischof, JS, Meierhofer, R, Shrestha, A, and Inauen, J. The physical burden of water carrying and Women's psychosocial well-being: evidence from rural Nepal. Int J Environ Res Public Health. (2021) 18:7908. doi: 10.3390/ijerph18157908
8. Jo-Anne Lee Geere . Drawers of water for life, but not for health. How water carriage is associated with the health of water carriers. Doctoral thesis. The University of East Anglia, the Norwich School of Medicine (2019).
9. Geere, J-AL, Cortobius, M, Geere, JH, Hammer, CC, and Hunter, PR. Is water carriage associated with the water carrier's health? A systematic review of quantitative and qualitative evidence. BMJ glob. Health. (2018) 3:e000764. doi: 10.1136/bmjgh-2018-000764
10. Graham, JP, Hirai, M, and Kim, S-S. An analysis of water collection labor among women and children in 24 sub-Saharan African countries. PLoS One. (2016) 11:e0155981:6. doi: 10.1371/journal.pone.0155981
11. Geere, J-AL, Hunter, PR, and Jagals, P. Domestic water carrying and its health implications: a review and mixed methods pilot study in Limpopo Province, South Africa. Environ Health. (2010) 9:52. doi: 10.1186/1476-069X-9-52
12. JMP . Progress on drinking water, sanitation, and hygiene: 2017 update and SDG baselines. Geneva: World Health Organization (WHO) and the United Nations Children’s Fund (UNICEF) (2017).
13. Adams E.A, Byrns, S., Kumwenda, S., Quilliam, R., Mkandawire, T., and Price, H. Water journeys: household water insecurity, health risks, and embodiment in slums and informal settlements. Soc Sci Med (2022) 313:115394, doi: 10.1016/j.socscimed.2022.115394
14. Geere, JL, Mokoena, MM, Jagals, P, Poland, F, and Hartley, S. How do children perceive health to be affected by domestic water carrying? Qualitative findings from a mixed methods study in rural South Africa. Child Care Health Dev. (2010) 36:818–26. doi: 10.1111/j.1365-2214.2010.01098.x
15. CSA . Federal Democratic Republic of Ethiopia central statistical agency population projection of Ethiopia for all regions at Woreda level from 2014 – 2017f. Ethiopia: Addis Ababa. (2013).
16. Hassen, S, Getachew, M, Eneyew, B, Keleb, A, Ademas, A, Berihun, G, et al. Determinants of acute respiratory infection (ARI) among under-five children in rural areas of Legambo District, south Wollo zone, Ethiopia: a matched case-control study. Int J Infect Dis. (2020) 96:688–95. doi: 10.1016/j.ijid.2020.05.012
17. Mernie, G, Kloos, H, and Adane, M. Prevalence of and factors associated with acute diarrhea among children under five in rural areas in Ethiopia with and without implementation of community-led total sanitation and hygiene. BMC Pediatr. (2022) 22:148. doi: 10.1186/s12887-022-03202-8
18. Eriyani, E, and Azuhairi, AA. Predictors of musculoskeletal disorders among public elderly care home Workers in West Coast Malaysia. Int J Public Health Clin Sci. (2016) 3:80–93
19. Aghilinejad, M, Choobineh, A, Sadeghi, Z, Nouri, M, and Ahmadi, AB. Prevalence of musculoskeletal disorders among Iranian steel workers. Iran Red Crescent Med J. (2012) 14:198–203.
20. Meierhofer, R, Tomberge, VMJ, Inauen, J, and Shrestha, A. Water carrying in hills of Nepal– associations with women's musculoskeletal disorders, uterine prolapse, and spontaneous abortions. PLoS One. (2022) 17:e0269926. doi: 10.1371/journal.pone.0269926
21. Kadota, JL, McCoy, SI, Bates, MN, Mnyippembe, A, Njau, PF, and Ndola, P. The impact of heavy load carrying on musculoskeletal pain and disability among women in Shinyanga region, Tanzania. Annals of. Glob Health. (2020) 86:1–13. doi: 10.5334/aogh.2470
22. Tami, AM, Bika Lele, EC, Mekoulou Ndongo, J, Ayina, CN, Guessogo, WR, Lobe Tanga, M-Y, et al. Epidemiology of musculoskeletal disorders among the teaching staff of the University of Douala, Cameroon: association with physical activity practice. Int J Environ Res Public Health. (2021) 18:6004. doi: 10.3390/ijerph18116004
23. Moreira Couto, MCB, Falcão, IR, Müller, JDS, Alves, IB, Viana, WDS, Lima, VMC, et al. Prevalence and work-related factors associated with lower Back musculoskeletal disorders in female shellfish gatherers in Saubara, Bahia-Brazil. International journal of. Int J Environ Res Public Health. (2019) 16:857. doi: 10.3390/ijerph16050857
24. Yizengaw, MA, Mustofa, SY, Ashagrie, HE, and Zeleke, TG. Prevalence and factors associated with work-related musculoskeletal disorder among health care providers working in the operation room. Ann Med Surg. (2021) 72:102989. doi: 10.1016/j.amsu.2021.102989
25. Alamneh, YM, Sume, BW, and Shiferaw, AA. Musculoskeletal disorders among the population in Northwest Ethiopia. SAGE Open Med. 10:1–8. doi: 10.1177/20503121221085109
26. Hicks, C, Ibitoye, SE, Schweizer, M, Fethke, N, and Baker, K. A meta-analysis of the association between physical demands of unpaid domestic work and back pain among women. BMC Women’s Health (2021). doi: 10.1186/s12905-021-01294-5
27. Demissie, B, Yenew, C, Amsalu, A, Yideg, YG, Dagnew, BN, Walle, G, et al. The magnitude of work-related musculoskeletal disorders and its associated factors among computer user bankers in South Gondar zone, Northwest Ethiopia, 2021. Environ Health Insights. (2022) 16:117863022211250–7. doi: 10.1177/11786302221125048
28. Gashawbeza, B, and Ezo, E. Prevalence and factors associated with low back pain among health care providers in public hospitals of Gamo zone, southern Ethiopia. SAGE Open Med. (2022) 10:1–12. doi: 10.1177/20503121221114311
29. Abebe, G, Hailu, T, Fikadu, T, Gebremickael, A, Temesgen, R, Shibru, T, et al. Magnitude and factors associated with musculoskeletal disorder among patients with diabetes attending chronic care at Arba Minch general hospital, Arba Minch, southern Ethiopia, 2021: a cross-sectional study. BMJ Open. (2022) 12:e059218. doi: 10.1136/bmjopen-2021-059218
30. Mekonnen, TH . The magnitude and factors associated with work-related back and lower extremity musculoskeletal disorders among barbers in Gondar town, Northwest Ethiopia, 2017: a cross-sectional study. PLoS One. 14:e0220035. doi: 10.1371/journal.pone.0220035
31. Melese, H, Gebreyesus, T, Alamer, A, and Berhe, A. Prevalence and associated factors of musculoskeletal disorders among cleaners working at Mekelle university, Ethiopia. J Pain Res. (2020) 13:2239. doi: 10.2147/JPR.S263319
32. Vega-Fernandez, G, Lera, L, Leyton, B, Cortés, P, and Lizana, PA. Musculoskeletal disorders associated with quality of life and body composition in urban and rural public school teachers. Front Public Health. (2021) 9:607318. doi: 10.3389/fpubh.2021.607318
33. Suleyman, J, and Gelaw, AY. Work-related musculoskeletal disorders and associated factors among cleaners of health institutions in Gondar town, Northwest Ethiopia: an institution based cross-sectional study. BMJ [Preprint]. (2021). doi: 10.1101/2021.12.06.21266337
34. Solis-Soto, MT, Schön, A, Solis-Soto, A, Parra, M, and Radon, K. Prevalence of musculoskeletal disorders among school teachers from urban and rural areas in Chuquisaca, Bolivia: a cross-sectional study. BMC Musculoskelet Disord. (2017) 18:425. doi: 10.1186/s12891-017-1785-9
35. Bian, WM, Ndongo, JM, Guessogo, WR, Minye, EE, Ndemba, PBA, Gassina, G, et al. Musculoskeletal disorders and risk factors among heavy load carriers in Yaoundé city, Cameroon. Int J Occup Saf Ergon. (2021) 28:1244–50. doi: 10.1080/10803548.2021.1886452
36. Tegenu, H, Gebrehiwot, M, Azanaw, J, and Akalu, TY. Self-reported work-related musculoskeletal disorders and associated factors among restaurant Workers in Gondar City, Northwest Ethiopia, 2020. J Environ Public Health. (2021) 2021:1–9. doi: 10.1155/2021/6082506
37. Geerea, J-AL, and Huntera, PR. The association of water carriage, water supply, and sanitation usage with maternal and child health. A combined analysis of 49 multiple indicators. Cluster surveys from 41 countries. Int J Hyg Environ Health. (2020) 223:238–47. doi: 10.1016/j.ijheh.2019.08.007
38. Sorenson, SB, Morssink, C, and Campos, PA. Safe access to safe water in low-income countries: water fetching in current times. Soc Sci Med. (2011) 72:1522e1526. doi: 10.1016/j.socscimed.2011.03.010
39. Sisay, SF, Gari, SR, and Ambelu, A. Water safety practices along the water service chain in Addis Ababa: a cross-sectional study in a Cosmopolitan City. Environ Health Insights. (2024) 18:11786302241235006. doi: 10.1177/11786302241235006
Keywords: water carrying practices, musculoskeletal disorders, women’s health, Legambo district, Northeastern Ethiopia
Citation: Berihun G, Gasheya KA, Abebaw T, Abebe M, Gizeyiatu A, Berhanu L, Dagne M, Desye B, Walle Z, Zewdu L and Wondim MG (2024) Self-reported musculoskeletal disorder symptoms and associated factors among water carrying women in Legambo district, Northeastern Ethiopia: a community-based cross-sectional study design. Front. Public Health. 12:1409535. doi: 10.3389/fpubh.2024.1409535
Edited by:
Antonio Caputi, University Hospital “Policlinico” of Bari, ItalyReviewed by:
James Boadu Frimpong, New Mexico State University, United StatesLuenda Charles, Centers for Disease Control and Prevention (CDC), United States
Copyright © 2024 Berihun, Gasheya, Abebaw, Abebe, Gizeyiatu, Berhanu, Dagne, Desye, Walle, Zewdu and Wondim. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Kassahun Ayele Gasheya, YXN0ZWRla2Fzc2FodW5AZ21haWwuY29t