 Júlia Halamová1*
Júlia Halamová1* Martin Kanovský1,2
Martin Kanovský1,2 Katarina Krizova1
Katarina Krizova1 Bronislava Šoková1
Bronislava Šoková1 Martina Baránková1
Martina Baránková1 Charles Figley3
Charles Figley3- 1Institute of Applied Psychology, Faculty of Social and Economic Sciences, Comenius University in Bratislava, Bratislava, Slovakia
- 2Institute of Social Anthropology, Faculty of Social and Economic Sciences, Comenius University in Bratislava, Bratislava, Slovakia
- 3Traumatology Institute, Tulane University, New Orleans, LA, United States
Background: There is a high probability of compassion fatigue occurring in helping professionals who work with traumatized clients or patients. Several instruments exist for measuring compassion fatigue, but all of them have methodological flaws. The original Compassion Satisfaction/Fatigue Self-Test for Helpers is time-consuming and its psychometric properties, including factor structure, have not been supported in the research.
Methods: Therefore, the goal of this study was to apply a Mokken scale analysis for polytomous items to shorten the Compassion Satisfaction/Fatigue Self-Test for Helpers and improve its psychometric properties. In addition, we wanted to create norms for the helping professional population. The research sample consisted of 2,320 participants from various helping professions.
Results: To improve scalability, most of the scale items were removed. The resulting item scalability coefficients ranged from 0.349 to 0.655 and Molenaar–Sijtsma reliability coefficient ranged between 0.75 and 0.87. The final revised and shortened Compassion Satisfaction and Compassion Fatigue scale (CSCFS) consisted of 5 items for the Compassion Satisfaction—Personal Integrity and Happiness subscale, 5 items for the Compassion Satisfaction—Work Competence and Happiness subscale, 9 items for the Compassion Fatigue—Secondary Traumatic Stress subscale, and 7 for the Compassion Fatigue—Burnout subscale. The newly revised subscales have good reliability coefficients.
Conclusion: The CSCFS appears to be a valid and reliable instrument for assessing compassion satisfaction and compassion fatigue among helping professionals. More research is required to support its factor structure in a range of settings. We recommend testing usability across different helping professions and cultures.
Compassion fatigue and compassion satisfaction
The first person to use the term compassion fatigue was Joinson (54), who noted that nurses who care about their patients may also suffer because they internalize various kinds of stress from their patients. This was later named as the “cost of care” (1). The most well-known person associated with the term compassion fatigue is Figley (2), who suggests that being compassionate has negative consequences for the individual. When empathizing with the suffering of others, the individual often end up suffering themselves. Therefore, compassion fatigue can be defined as a state of emotional and physical exhaustion that leads to a reduced capacity for empathy or compassion and to a reduced capacity to bear the suffering of others (2).
According to Stamm (64), there are two aspects to the compassion experienced by professionals: positive (compassionate satisfaction) and negative (compassion fatigue). Compassion fatigue consists of two parts: burnout and secondary traumatic stress. Burnout is related to workplace stressors and associated with feelings of hopelessness and difficulty coping with work; while secondary traumatic stress is linked to exposure to traumatic stressful events, resulting in fear, sleeping problems, intrusive thoughts, or avoidance.
Compassion fatigue is usually associated with various symptoms (60) resulting from care provision and trauma exposure that are either related to first-hand (primary) trauma or the provision of care to those who have experienced trauma (secondary trauma). Figley (2) describes seven areas affected by compassion fatigue: cognitive, emotional, behavioral, spiritual, personal relations, somatic, and work performance. In the literature several terms are used to describe the negative effects of helping, such as compassion fatigue, secondary traumatic stress, second victim traumatization, client-related burnout, and vicarious trauma. Although there has been some discussion on whether these all these terms refer to the same construct (e.g., 62, 63), so far there is no evidence of differences between these concepts (64). In contrast to compassion fatigue, many helping professionals also have positive experiences of helping, known as compassion satisfaction (64). The term compassion satisfaction refers to the pleasure and satisfaction derived from being able to help others and being committed to and effective in their work (3).
Compassion fatigue is not usually triggered by a single encounter with trauma, but by constant, repetitive exposure to trauma. The costs are huge as it increases the likelihood of mistakes being made and reduces work performance, while leaving helping professionals vulnerable to becoming cold, cynical, robotic, demotivated, and exhausted and, more worryingly, it affects their ability to provide good care (4). Compassion fatigue can impair the ability of helping professionals to provide help and could result in unprofessional decisions, misdiagnosis, mistreatment, malpractice, and even client abuse (5). Therefore, early detection of the signs of compassion fatigue could provide helping professionals with time to learn new coping skills and techniques to prevent the full onset of compassion fatigue (4). This is even more important in settings where insufficient care can have enormous consequences for the physical or mental health of patients or clients, such as in healthcare settings (6). Based on the recent systematic review and meta-analysis of a total of 71 studies by Cavanagh et al. (7) compassion fatigue is distinct from “burnout” and represents a form of psychological distress that can be insidious, affecting all health professions and potentially impairing their ability to deliver care. Professionals who experience high levels of compassion fatigue also often report having various psychopathological symptoms, including substance use, depression, anxiety, and suicidal ideation (55).
These conditions not only undermine the mental health and well-being of healthcare providers but also adversely impact the quality of care they deliver. High levels of these stressors are linked to increased medical errors, lower patient satisfaction, and higher turnover rates among healthcare staff (8, 9).
Since compassion satisfaction and compassion fatigue are of great clinical importance, it is important to expand our knowledge of these constructs and capacity to measure their incidence, which cannot be achieved without psychometrically sound tools. On the top of that, it is hard to start treatment in the absence of screening and early detection. Furthermore, without valid and reliable tools, we cannot accurately measure the effectiveness of interventions aimed at increasing compassion satisfaction and reducing compassion fatigue. Therefore, the availability of sound instruments for measuring compassion fatigue and compassion satisfaction could help to provide better care for patients or clients in the future with earlier diagnosis of compassion fatigue, and therefore harm prevention.
Measuring compassion fatigue and compassion satisfaction
Since compassion fatigue and compassion satisfaction have such a huge impact on the quality of care provided by helping professionals, it is striking that there are few valid and reliable tools to measure them. Additionally, the existing self-rated measuring tools have often been criticized over content and methodological issues, such as the lack of a total score for both positively and negatively worded items and for not being cross-culturally sensitive [e.g., Bride et al. (10) and Kristensen et al. (61)]. As Bride et al. (10) put it, “no single compassion fatigue measure assesses all aspects of the concept of compassion fatigue (i.e., trauma symptoms, cognitive distortions, general psychological distress, burnout, etc.).”
According to Bride et al. (10), the Compassion Fatigue Self-Test (CFST; 60) is the first instrument to measure compassion fatigue. The original version of the CFST consists of 40 items divided into two subscales: compassion fatigue and burnout. Stamm and Figley (11) later revised the CFST by adding questions to measure compassion satisfaction, which resulted in a 66-item version. Several attempts were made to shorten the over-long CFST and improve usage but another problem was that neither the factor structure of the test nor its psychometric properties were published and so remained unknown (10).
Gentry et al. (51) used the Compassion Fatigue Scale—Revised (CFS-R) with a shortened scale of 30 items for measuring compassion fatigue and burnout. Similarly, Adams et al. (63) developed the Compassion Fatigue Short Scale (CF-Short Scale) which has 13-items and two subscales—burnout and secondary trauma. The tool most commonly used to measure compassion fatigue and satisfaction is the Professional Quality of Life Scale (ProQOL; 52) which is a revised version of the Compassion Fatigue Self Test (60). It has three subscales: compassion satisfaction, burnout, and compassion fatigue/secondary traumatic stress. The ProQOL is comprised of 30-items. Since its creation in 1995, the ProQOL has been revised and updated several times. The latest version is the Professional Quality of Life Scale version 5 [ProQOL-5; Stamm (12)]. However, Bride, Radey and Figley (10) note that the validity and factor structure of the ProQOL have not been sufficiently studied. Most authors report only the reliability coefficients. Keesler and Fukui (13) reported that the original three-factor model was not a good fit with the data. Their solution was to delete 7 of the 30 items so that the factor analysis yielded satisfactory results for the three factors. Similarly, Duarte (14) and other authors (15, 16) reported difficulty fitting the factor structure of the ProQOL. Likewise, a meta-analysis by Hotchkiss and Wong (17) found problems with the factor structure of the ProQOL across 27 different cultures and languages. In summary, Hemsworth et al. (15) invited researchers to revise and improve ProQOL 5, while Wessels et al. (18) went even further, stating that there was widespread recognition that the lack of assessment instruments with good psychometric properties supported by rigorous research was seriously hindering both further research developments in the area and attempts to help practicing professionals. The existence of a reliable and valid measure of compassion fatigue and compassion satisfaction could provide important information for early screening, diagnosis, intervention, or treatment, and thereby ensure high-quality care for patients, clients, and customers.
The research aim
Compassion fatigue and satisfaction significantly impact the quality of care provided by helping professionals, yet few valid and reliable tools exist to measure them. The Compassion Fatigue Self-Test (CFST; 60) was the first instrument to measure compassion fatigue. Despite several attempts to shorten and improve the CFST, its factor structure and psychometric properties remained unpublished and unknown (10).
The most frequently used version of the CFST, The Professional Quality of Life Scale (ProQOL; 52) showed to have factor structure problems across 27 cultures and languages based on the meta-analysis by Hotchkiss and Wong (17). Therefore, Wessels et al. (18) highlighted the lack of assessment instruments with robust psychometric properties as a major barrier to further research and practical applications.
To date, there is no scale that measures both compassion satisfaction and compassion fatigue together that has good psychometric properties and is not too long and cumbersome for data collection purposes. Thus, the aim of the present study was to revise, improve, and shorten the Compassion Fatigue and Satisfaction Self-Test for Helpers (11) using Mokken scale analysis for polytomous items (18, 19). In addition, we wanted to create norms for early screening of helping professionals followed by early intervention norms.
Methods
Research sample
The research sample was collected online through social media, contacts through professional associations and databases, personal contacts, and by asking participants to both compete the online questionnaire and forward the link to colleagues. We used REDCap (www.project-redcap.org) as the data-gathering tool. All participants signed an online written consent form.
There were 2,320 participants in total from various helping professions (participants could choose from one of the following: doctor, dentist, psychiatrist, nurse, paramedic, physiotherapist, hospital attendants, home nurse, social worker, psychologist, psychotherapist, coach, nun/monk, teacher, special educator, therapeutic pedagogue, educator, speech therapist, policemen, lawyer, doula, lactation consultant, human resources worker, volunteer, priest/pastor, radiologist, trainer, mentor, professional parent, pharmacist, and other). The research sample consisted of 1783 (76.9%) women, 527 (22.7%) men and 2 (0.1%) non-binary participants. Eight participants (0.3%) chose the option: I do not wish to say. Mean age was 41.74 with SD 11.62 ranging from 18 to 76 years.
Research instruments
We used the Compassion Fatigue and Satisfaction Self-Test for Helpers [CFST; Stamm and Figley (11)]. The CFST is a self-rated 66-item instrument measuring three subscales, namely, Compassion Fatigue (23 items), Compassion Satisfaction (26 items) and Burnout (16 items). Items are scored from 0 (not at all) to 5 (very often) on a Likert-type scale. Compassion satisfaction represents the joy of helping others, e.g., “I find that I learn new things from those I care for.” Compassion fatigue refers to the cost of caring (2), e.g., “I am pre-occupied with more than one person I help.” Burnout is defined as the state of work-related exhaustion, e.g., “I have felt weak, tired, run down as a result of my work as a helper.” The subscale scores are calculated separately for each subscale. The Slovak version of the CFST was first translated, then back translated, and any discrepancies were discussed and resolved with an expert panel consisting of the co-authors.
Research studies using the CFST have reported good reliability coefficients. Figley (60) reported a Cronbach’s alpha ranging from 0.86 to 0.94, and Rudolph et al. (5) reported reliability coefficients of 0.87 for Compassion satisfaction, 0.87 for Compassion fatigue, and 0.90 for Burnout. Ortlepp and Friedman (20)‘s reliability coefficients were 0.84 for compassion fatigue, 0.83 for burnout, and 0.85 for compassion satisfaction, while Conrad and Kellar-Guenther (21) obtained the following reliability coefficients: 0.84 for compassion fatigue, 0.84 for burnout, and 0.86 for compassion satisfaction. Similarly, Steed and Bicknell (22) reported reliability coefficients of 0.87, 0.78, and 0.91 for compassion fatigue, burnout, and compassion satisfaction, respectively. The problem with the previous studies (23) is the small participant samples ranging from 67 (22) to 142 (53) and 363 (21). In addition the samples were highly specific, such as therapists working with perpetrators of sexual abuse (22), which means the results cannot be generalized to other kinds of helping professionals. In addition, there is as yet no published information about the factor structure of the CFST (10), probably because of statistical problems with long scales. The short scale items usually have larger factor loadings, obtained by factor analysis, than the long-scale items (24).
Data analysis
In this paper, we used Mokken scale analysis (18, 19); Sijtsma and Molenaar, (58); to identify items with solid psychometric properties in the Compassion Fatigue and Satisfaction Self-Test for Helpers [CFST; Stamm and Figley (11)]. First, the items were assigned to subscales based on the theoretical framework of Stamm and Figley (11). Second, we performed an iterative Mokken scale analysis (18, 19); Sijtsma and Molenaar (58) on the subscales to check the assumptions of the Mokken double monotonicity model. Where the assumptions of the Mokken double monotonicity model were violated, we identified the items that did not fit the model and removed them until the final subscale provided satisfactory results.
Mokken scale analysis
We performed the Mokken scale analysis separately for each scale. The Mokken model is a nonparametric item-response model, which has to meet the following assumptions (19); Sijtsma and Molenaar (58):
1. Unidimensionality: all the items in the subscale measure a single attribute that is quantified by means of a latent variable denoted Theta.
2. Monotonicity: As Theta increases, the probability of an item scoring a value increases or remains constant but cannot decrease—that means the more a respondent possesses the measured attribute, the more likely s/he is to obtain scores that are representative of responses typical of the higher attribute level.
3. Local independence: items measuring the attribute should correlate positively when respondents vary by Theta. This is implied by the fact that respondents with higher Theta scores are expected to have higher scores for each item than respondents with lower Theta scores, which means these scores should covary. If we remove this source of variation, this relationship between the items should disappear. Consequently, Theta should be the only source of variation and the items will be locally independent.
These three assumptions constitute the monotone homogeneity model for ordering persons. The double monotonicity model for ordering persons and items is stronger (in fact, this is a special feature of the monotone homogeneity model), and validity is only exhibited when these additional assumptions are met:
1. Invariant item ordering: the double monotonicity model implies the ordering of items by means of mean item scores. In other words, item ordering from easiest to hardest in terms of difficulty should be equal for different-ability (Theta) respondents. The double monotonicity model directly implies such an invariant item ordering.
2. Reliability: we will use the Molenaar–Sijtsma (MS) method (59) to estimate test-score reliability. The MS method assumes a stronger double monotonicity model. Its values must be close to 0.90, and over 0.70.
Two important caveats:
1. Sijtsma and van der Ark (19) point out that many researchers overlook the fact that the assumption (4)—invariant item ordering, the defining feature of the double monotonicity model—should be tested separately, and that it is not implied by the fulfilment of other properties (e g. strong scalability etc.).
2. Again, Sijtsma and van der Ark (19) argue that testing the invariant item ordering by means of the assumption that item step response functions (ISRF) should not intersect is inappropriate: a set of non-intersecting ISRFs does not directly imply an invariant item ordering.
Procedure
All the analyses were performed in R version 4.2.1 (25), “mokken” package (26). The procedure was as follows:
1. Unidimensionality: The procedure suggested in Sijtsma and van der Ark (19) was used—for each subscale, we fitted the iteratively automated item selection procedure (AISP), option genetic algorithm (27) with increasing threshold, and observed whether the emergence of one subscale was confirmed.
2. Scalability: on completion of the test of unidimensionality, the initial subscales suggested by AISP with a threshold of 0.3 were selected. Subscales were considered satisfactory when Loevinger’s coefficient H ≥ 0.400, with 0.400 ≤ H < 0.500 indicating a medium strong scale, and H ≥ 0.500 indicating a strong scale. Items in each subscale were removed manually when H < 0.30 (28). Items were removed stepwise by first removing those with the most serious violations and then estimating the model again. This procedure was repeated until Loevinger’s coefficient H for the overall scale reached the value H = 0.400 (a medium strong scale) but considering standard error to ensure that the population value was not lower due to sampling error (e.g., a value of H = 0.405 with standard error 0.013 was not considered satisfactory). If this procedure failed to confirm the Mokken scale, the threshold (Loevinger’s coefficient H for the overall scale) was lowered to value H = 0.300 (a weak scale). If this second procedure failed to confirm the Mokken scale, the final conclusion was that the items were unscalable.
3. Local independence: the method of conditional associations proposed by Straat et al. (29) was used. Items flagged as locally non-independent were removed.
4. Monotonicity: the method suggested by Junker and Sijtsma (30) was used. Items with significant violations of monotonicity are inspected visually if the violation(s) are large enough to affect the monotonicity of the item response functions—especially in larger datasets, even significant violations of monotonicity in some item step response functions of an item could have a negligible effect on the overall item response function of this item. Items which did not pass the visual inspection were removed.
5. Invariant item ordering: the method proposed by Ligtvoet et al. (31) was used. Items violating the invariant item ordering were removed.
6. Reliability was calculated using MS rho reliability Molenaar–Sijtsma reliability coefficient and reported in the tables of results.
7. All descriptive statistics and Loevinger’s coefficients H (with standard errors) for remaining items and subscales were calculated and reported.
8. Norms (percentile rank norms, z-score norms, stanine boundaries) were calculated and reported, together with standard errors and 95% confidence intervals.
Results
Missing data analysis
A missing data analysis was conducted before assessing the subscales. The percentage of responses missing at least one answer was 11.94% (280 out of 2,346), with 15 missing patterns. To impute the missing data, a Bayesian framework was used (32), implemented in “mi” R package (33). As the items are polytomous, an ordered-categorical model with logit link was used. After imputations, the final sample size was 2,320.
Outliers
To handle outlying values for each subscale, the outlier detection method proposed by Zijlstra, Van der Ark and Sijtsma (34) was used. Given the relatively strong skew O+ distributions (Figures 1–3; Supplementary Appendix 1), we used adjusted boxplot (35) to accommodate the skewness. This produced a criterion value for the Compassion Fatigue subscale O+ = 10.53 (lower) and 93.00 (upper), and 30 outlying values were identified (1.28%), the criterion value for the Compassion Satisfaction subscale O+ = 10.67 (lower) and 110.26 (upper), and 28 outlying values were identified (1.19%), and a criterion value for the Burnout subscale O+ = 3.68 (lower) and 67.20 (upper), and only five outlying values were identified (0.21%). The analysis with and without the outliers shows a negligible influence on the outcomes (which comes as no surprise given their minimal rate).
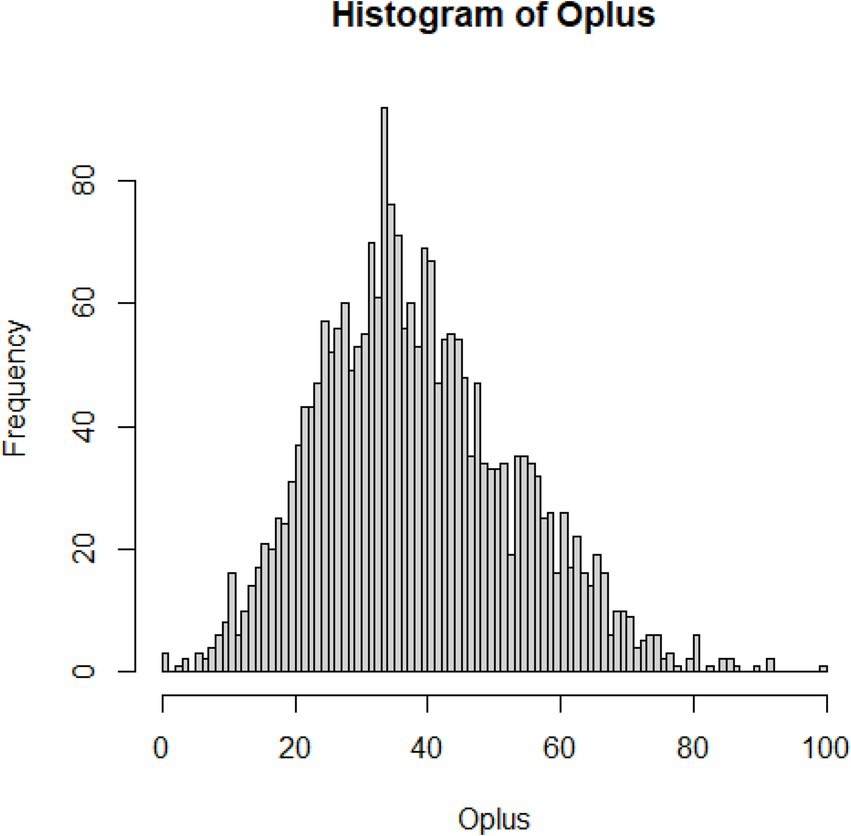
Figure 1. Distribution of errors for compassion fatigue.
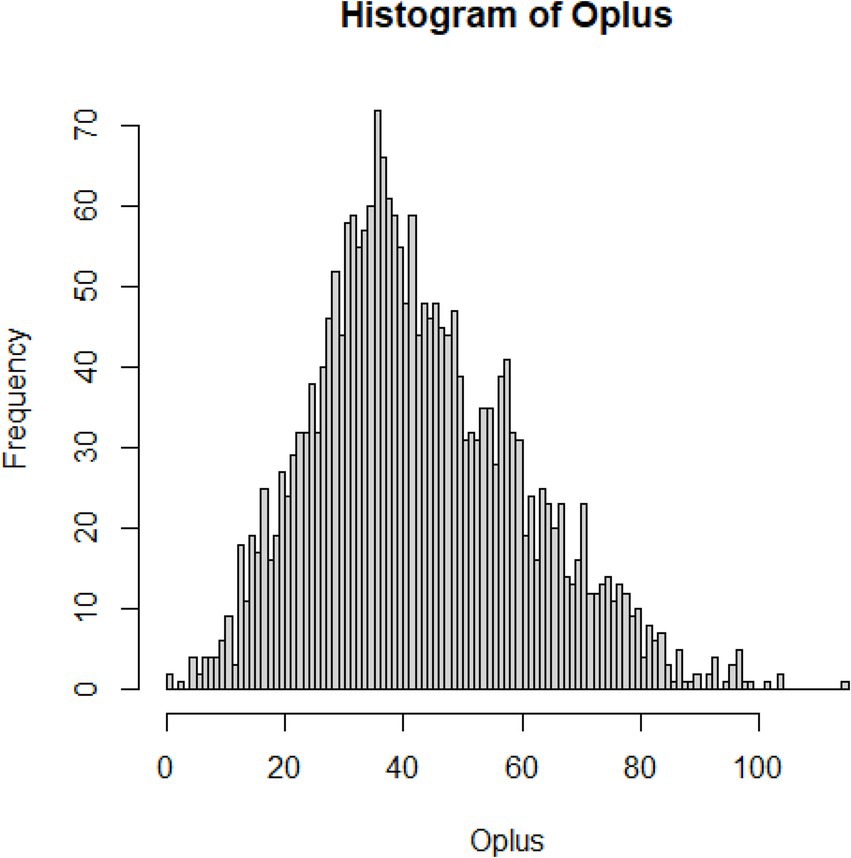
Figure 2. Distribution of errors for compassion satisfaction.
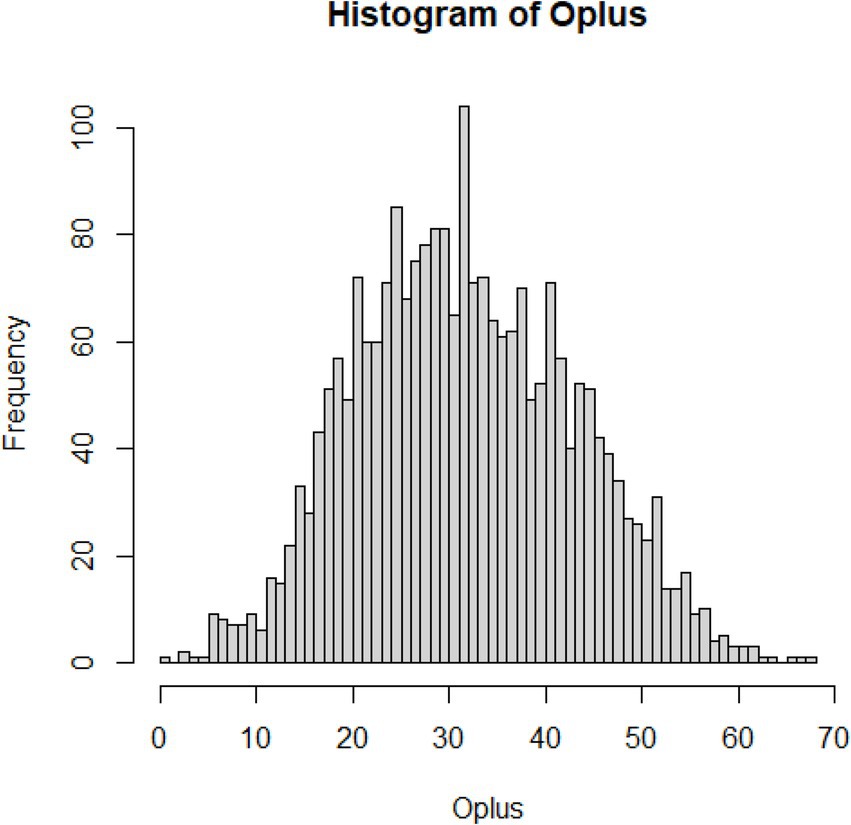
Figure 3. Distribution of errors for Burnout.
Unidimensionality of subscales
The automated item selection procedure (with genetic algorithm) failed to confirm a unidimensional scale for Compassion Satisfaction, but suggested two subscales. Therefore, we analyzed those subscales separately to check if they could constitute Mokken scales on their own.
Descriptive analysis of the items
We calculated the descriptive statistics for items for all four subscales of the newly developed Compassion Satisfaction and Compassion Fatigue scale: Compassion Satisfaction Personal Integrity and Happiness, Compassion Satisfaction Work Competence and Happiness, Compassion Fatigue Burnout and Compassion Fatigue Secondary Traumatic Stress. See Tables 1–4. The descriptive statistics were mean, standard deviation, H item scalability coefficient, standard error of item scalability coefficient, and MS rho reliability Molenaar–Sijtsma reliability coefficient.
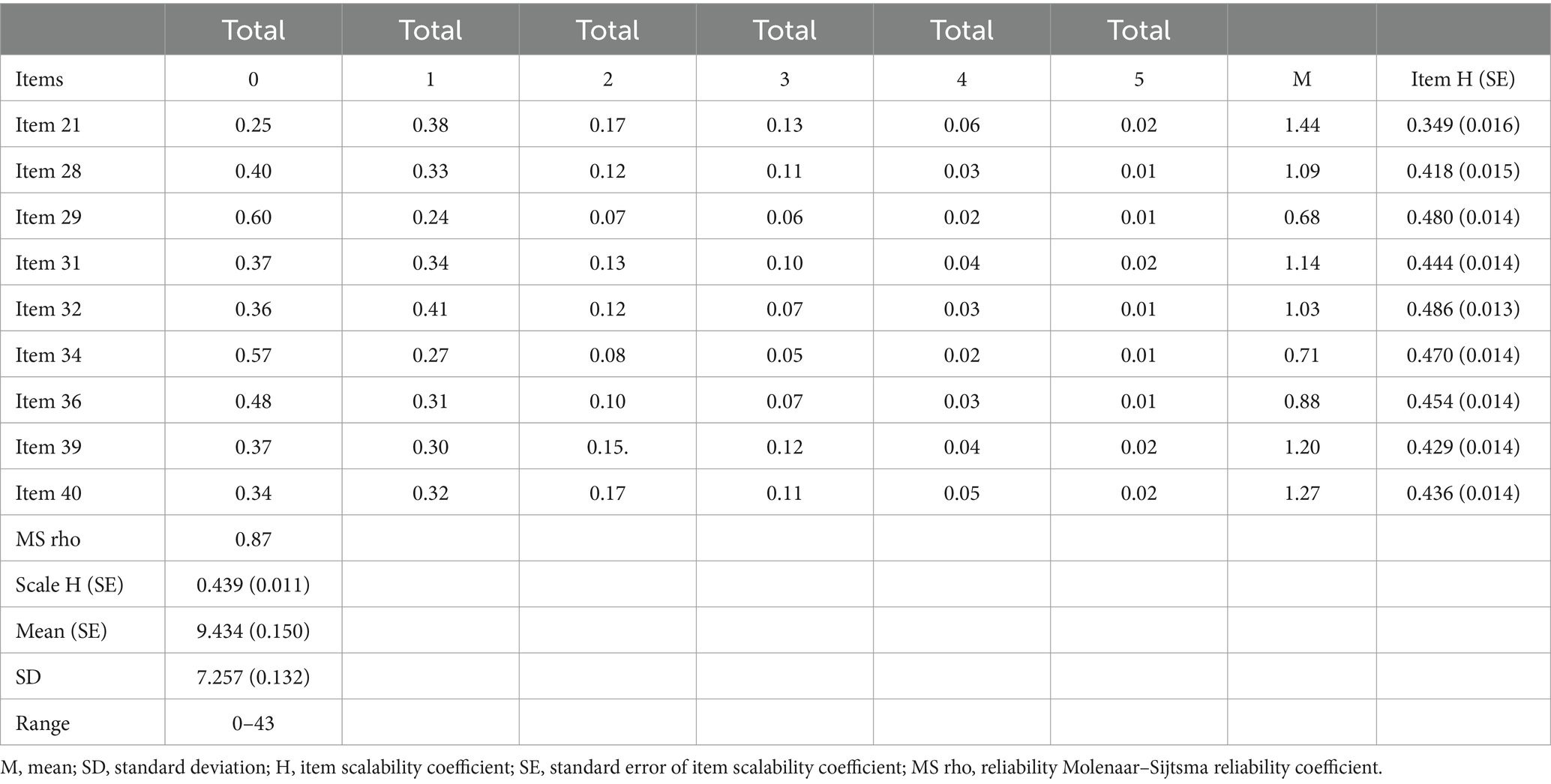
Table 1. Descriptive statistics of items of compassion fatigue secondary traumatic stress.
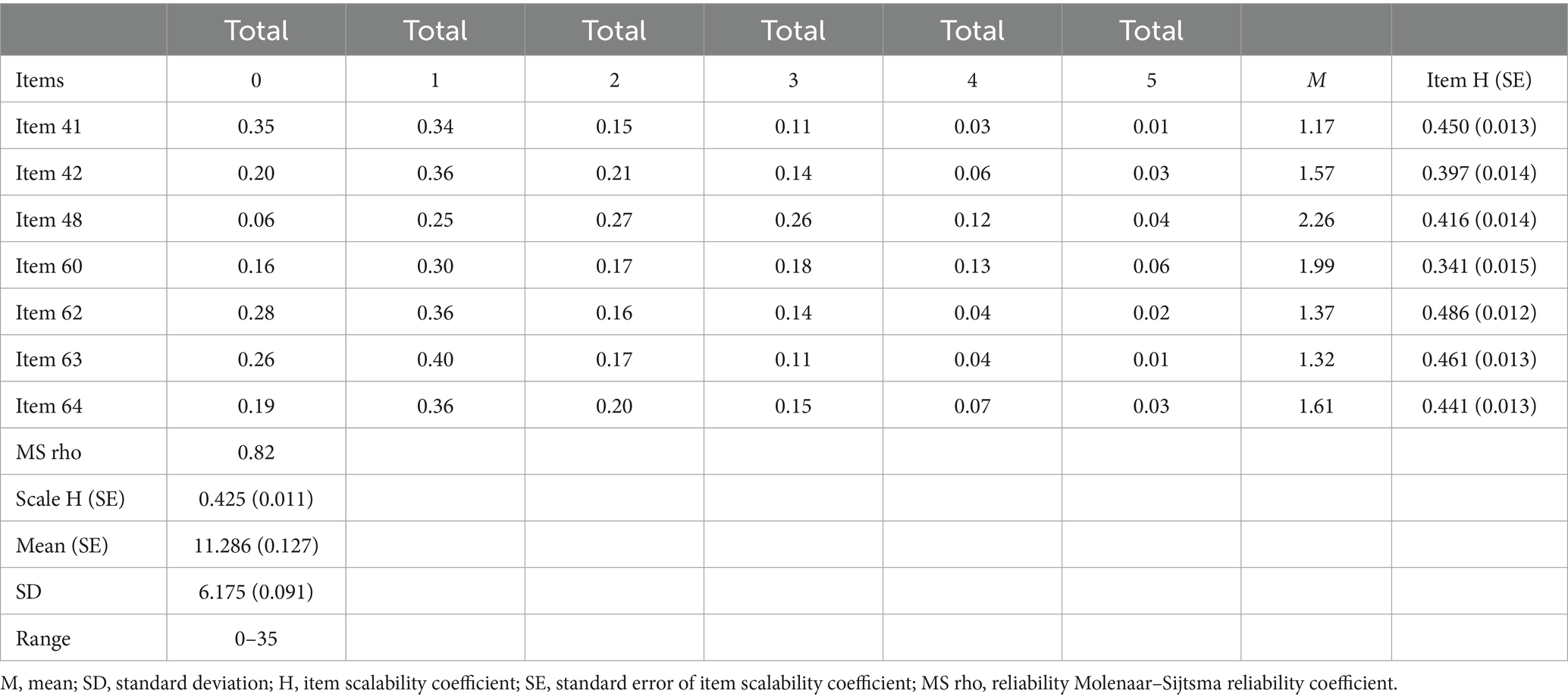
Table 2. Descriptive statistics of items of compassion fatigue Burnout.
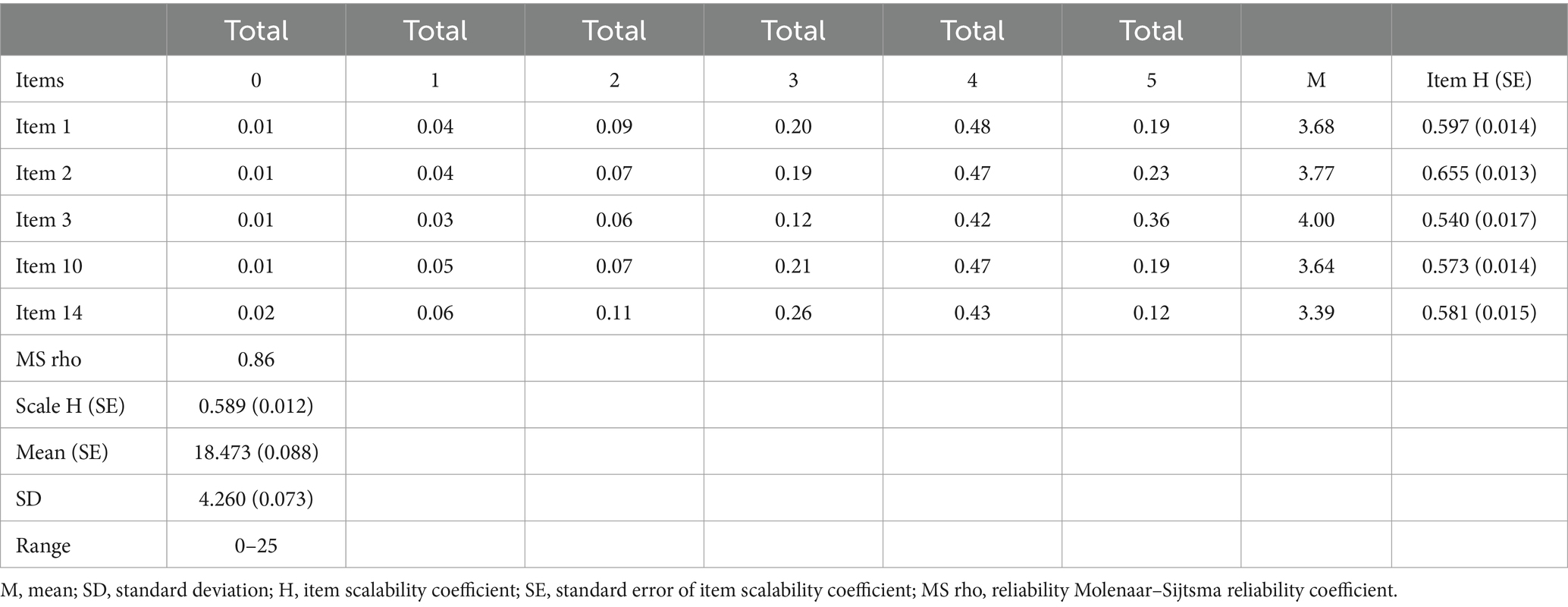
Table 3. Descriptive statistics of items of compassion satisfaction personal integrity and happiness.
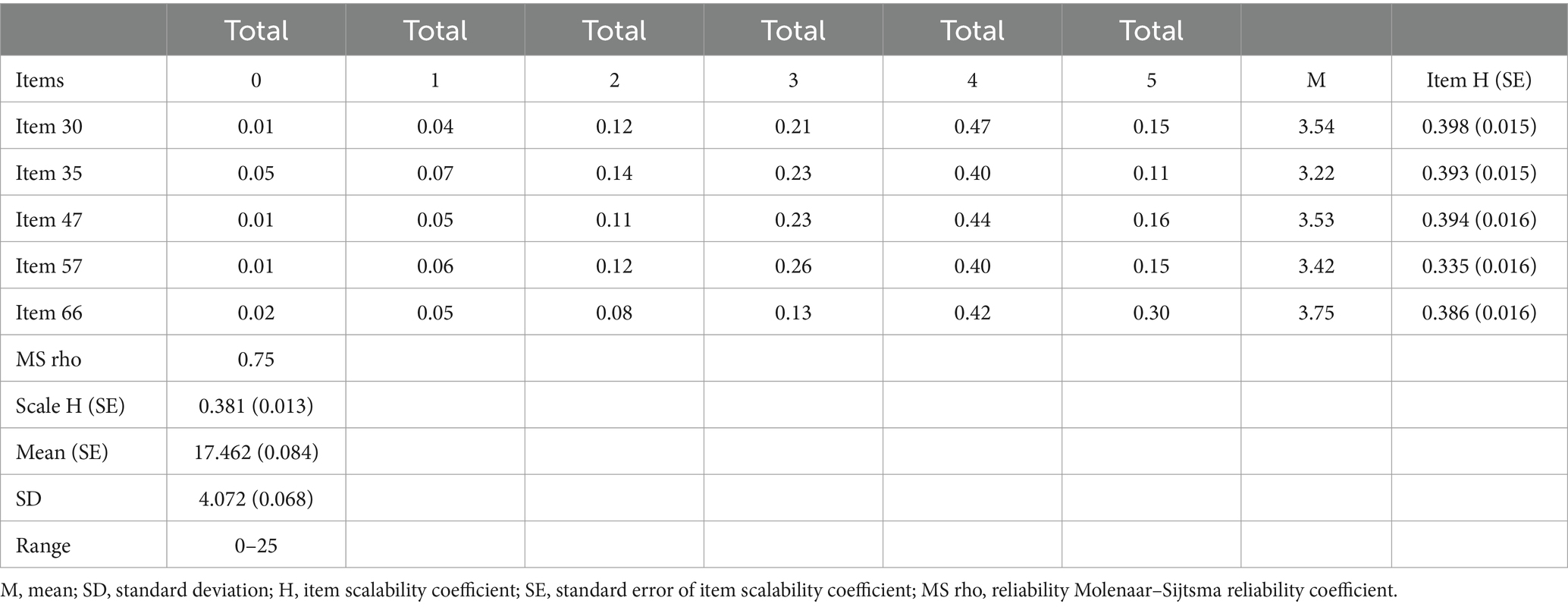
Table 4. Descriptive statistics of items of compassion satisfaction work competence and happiness.
Internal reliability
We calculated the internal reliability through Cronbach alpha polychoric coefficients. For the Compassion Fatigue and Satisfaction Self-Test for Helpers, the Cronbach’s α coefficient was 0.87 for Compassion Fatigue, 0.85 for Compassion Satisfaction, and 0.84 for Burnout subscales. For the Revised Compassion Satisfaction and Compassion Fatigue scale, reliability was calculated using MS rho (Molenaar–Sijtsma) reliability coefficient and indicated the following values for Compassion Satisfaction Personal Integrity and Happiness 0.86, Compassion Satisfaction Work Competence and Happiness 0.75, Compassion Fatigue Burnout 0.82 and Compassion Fatigue Secondary Traumatic Stress 0.87.
Construct validity
The Mokken scale analysis helped us to shorten and improve the CSFT; the final version consisting of 26 items is given in Supplementary Appendix 1. The final item order of the Compassion Satisfaction and Compassion Fatigue scale was randomized via www.random.org.
Norms
For the purposes of early diagnosis and consequently for immediate intervention or treatment and measuring the effectiveness of these, it is important to create a psychometrically sound scale as well as norms for the helping professional population. We calculated the Norms (percentile rank norms, z-score norms, stanine boundaries) and report them together with standard errors and 95% confidence intervals for each of the CSCFS subscales in Tables 5–16.
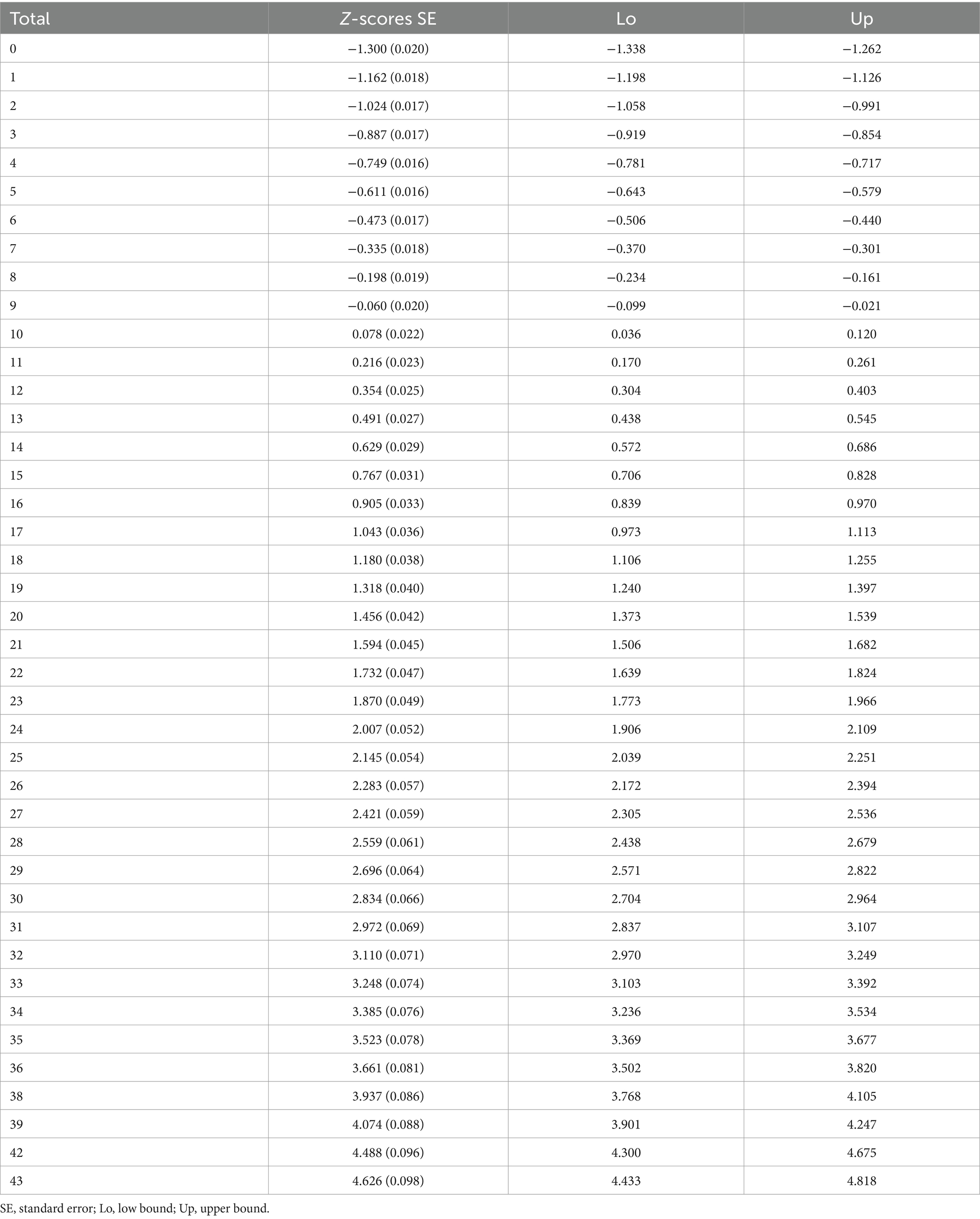
Table 5. Z-scores norms for compassion fatigue secondary traumatic stress.
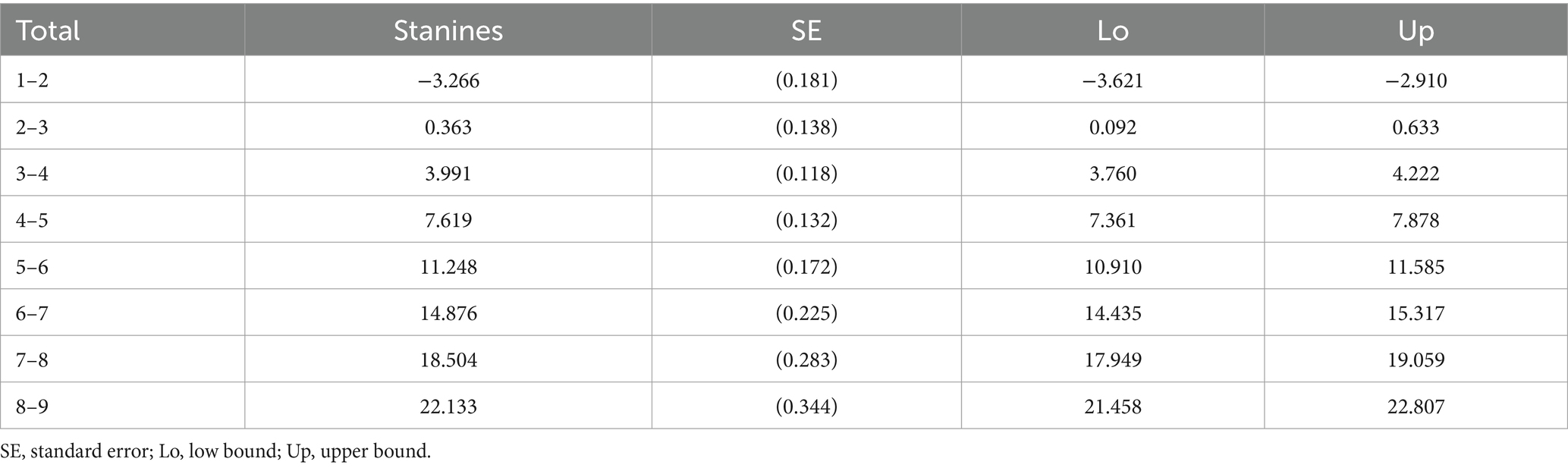
Table 6. Stanines norms for compassion fatigue secondary traumatic stress.
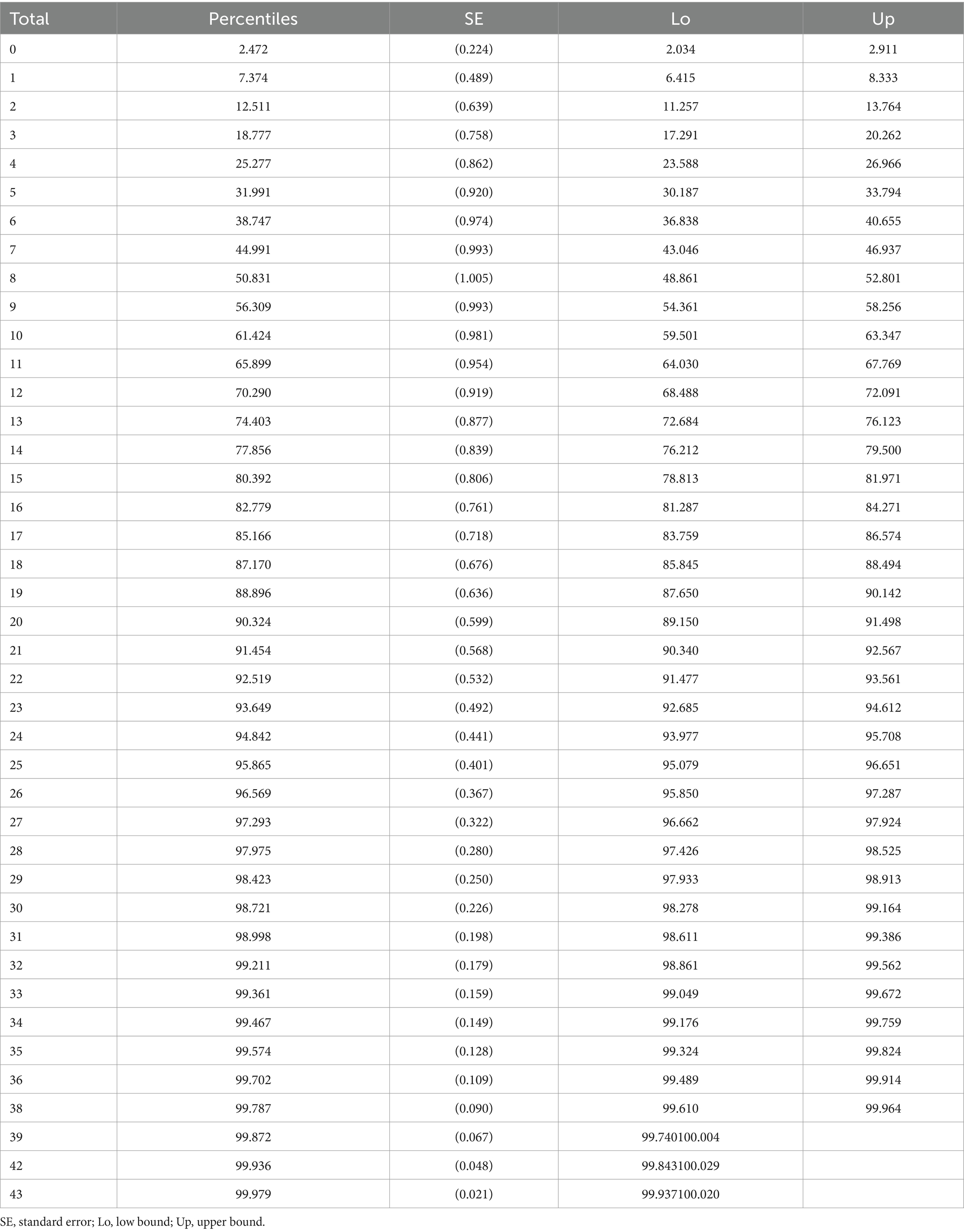
Table 7. Percentiles norms for compassion fatigue secondary traumatic stress.
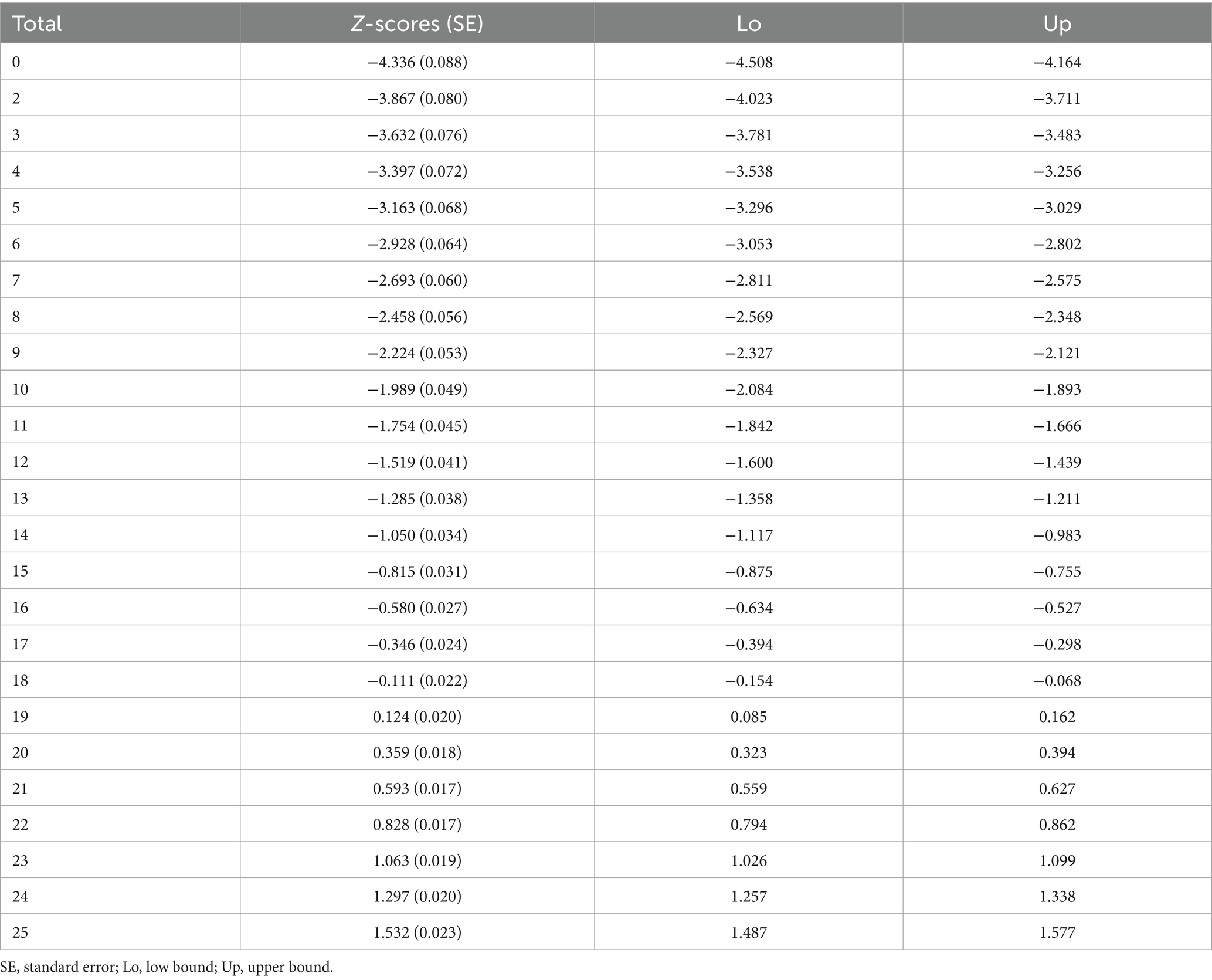
Table 8. Z-scores norms for compassion satisfaction personal integrity and happiness.
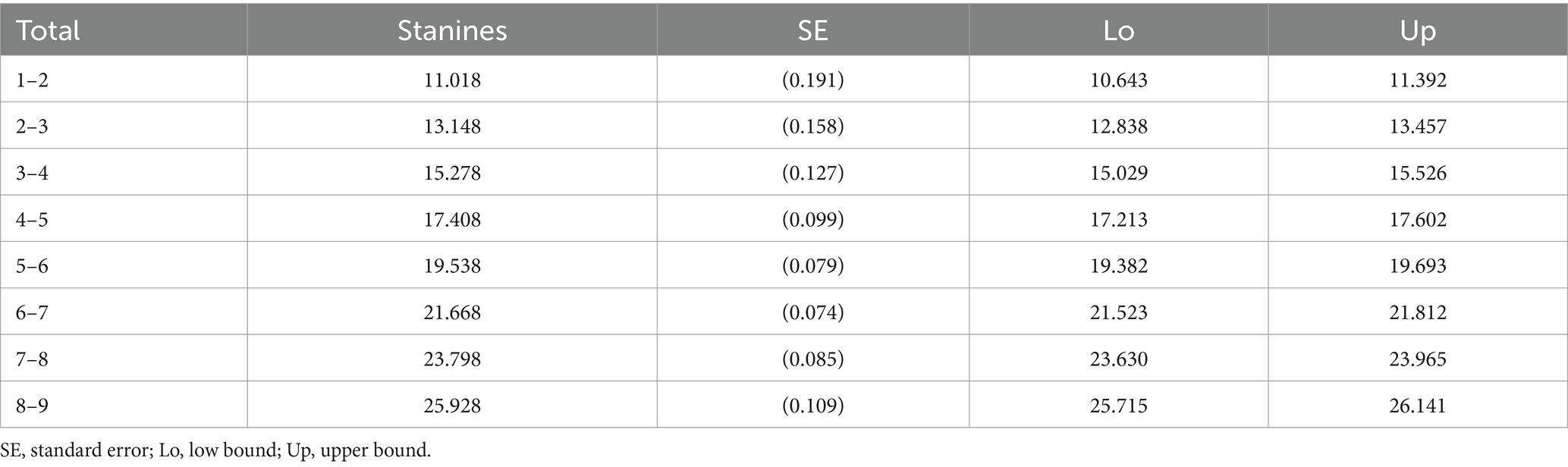
Table 9. Stanines norms for compassion satisfaction personal integrity and happiness.

Table 10. Percentiles norms for compassion satisfaction personal integrity and happiness.
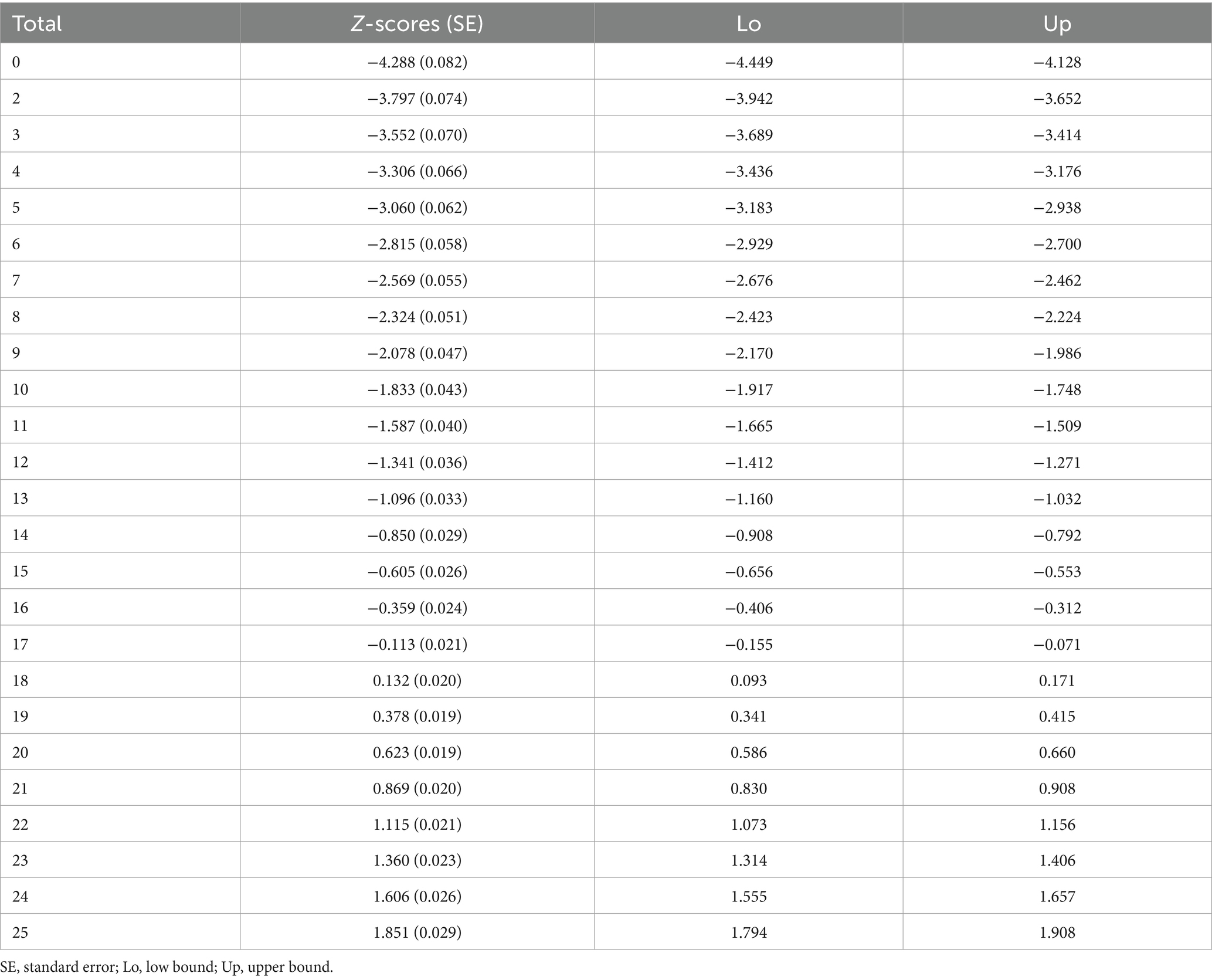
Table 11. Z-scores norms for compassion satisfaction work competence and happiness.
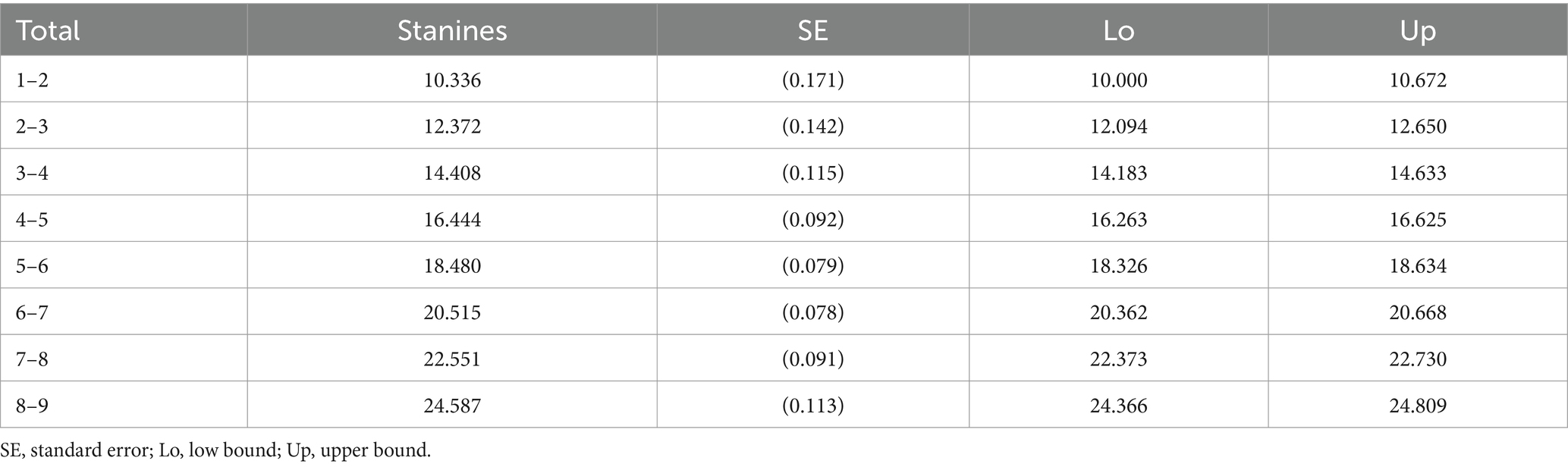
Table 12. Stanines norms for compassion satisfaction work competence and happiness.
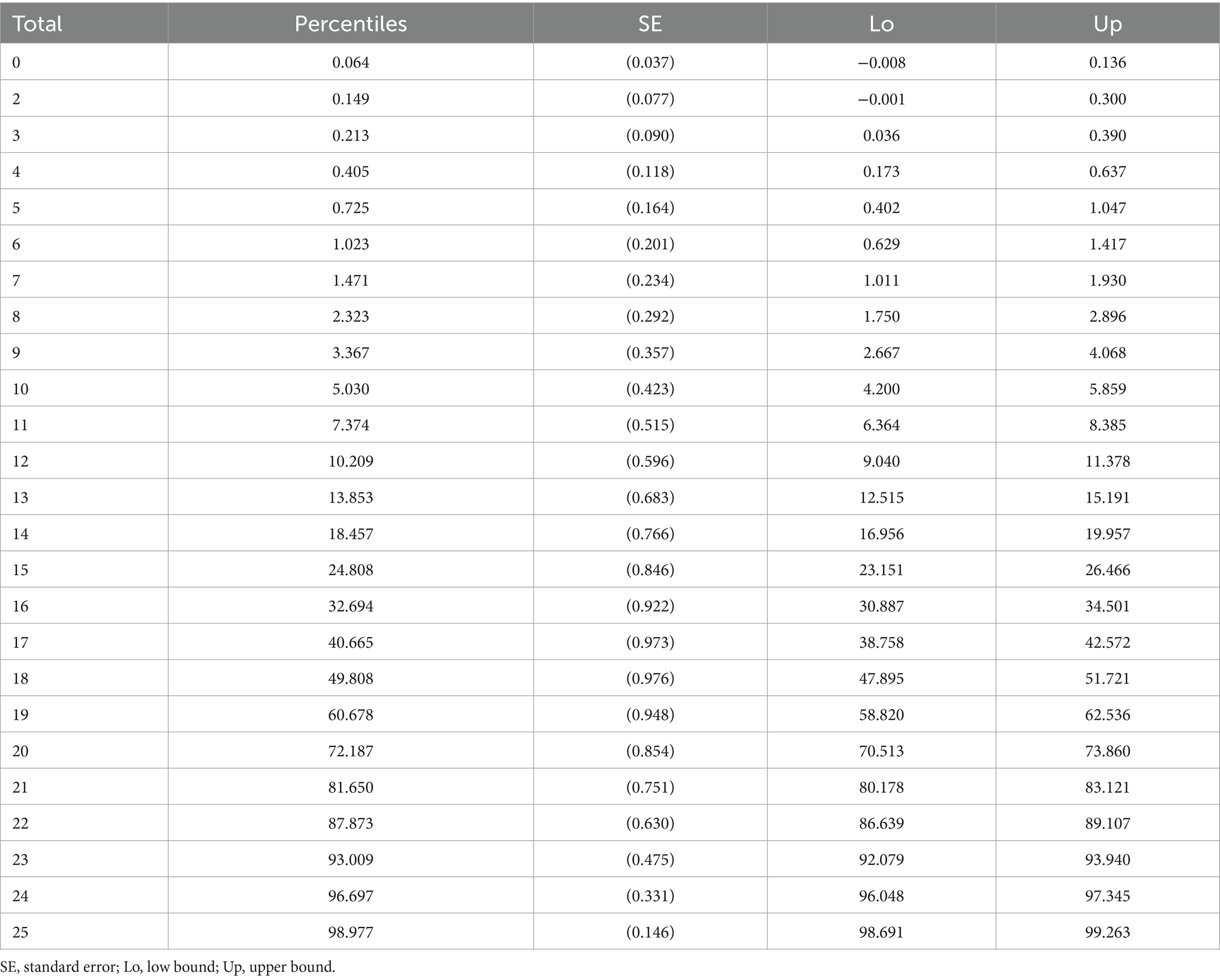
Table 13. Percentiles norms for compassion satisfaction work competence and happiness.
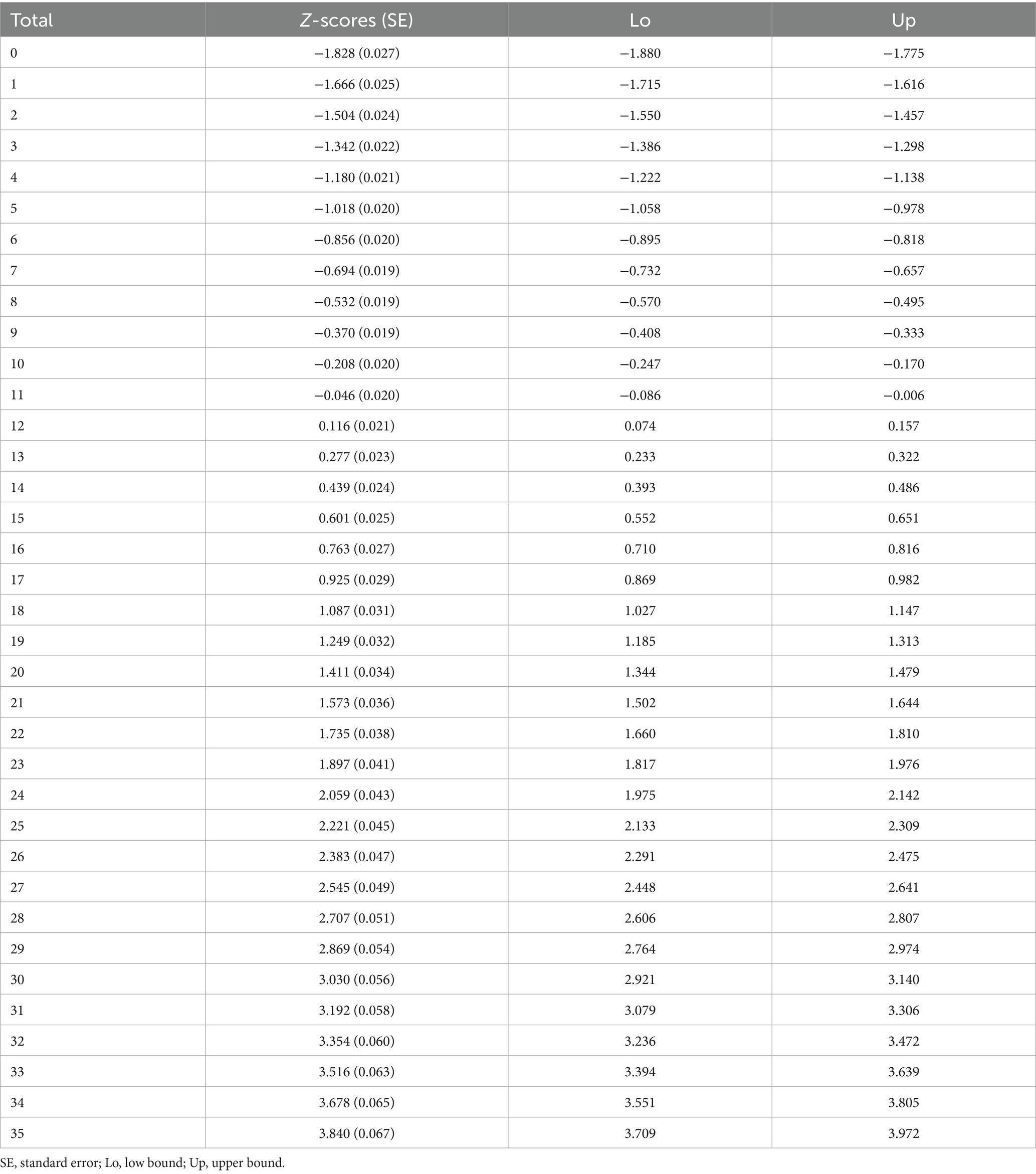
Table 14. Z-scores norms for compassion fatigue Burnout.
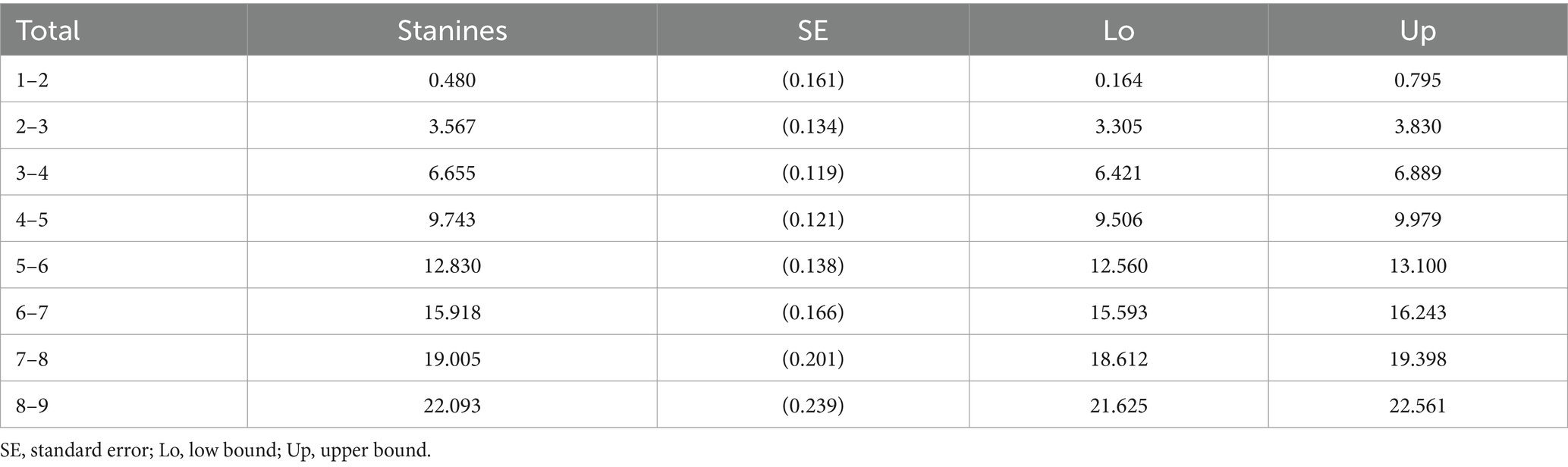
Table 15. Stanines norms for compassion fatigue Burnout.
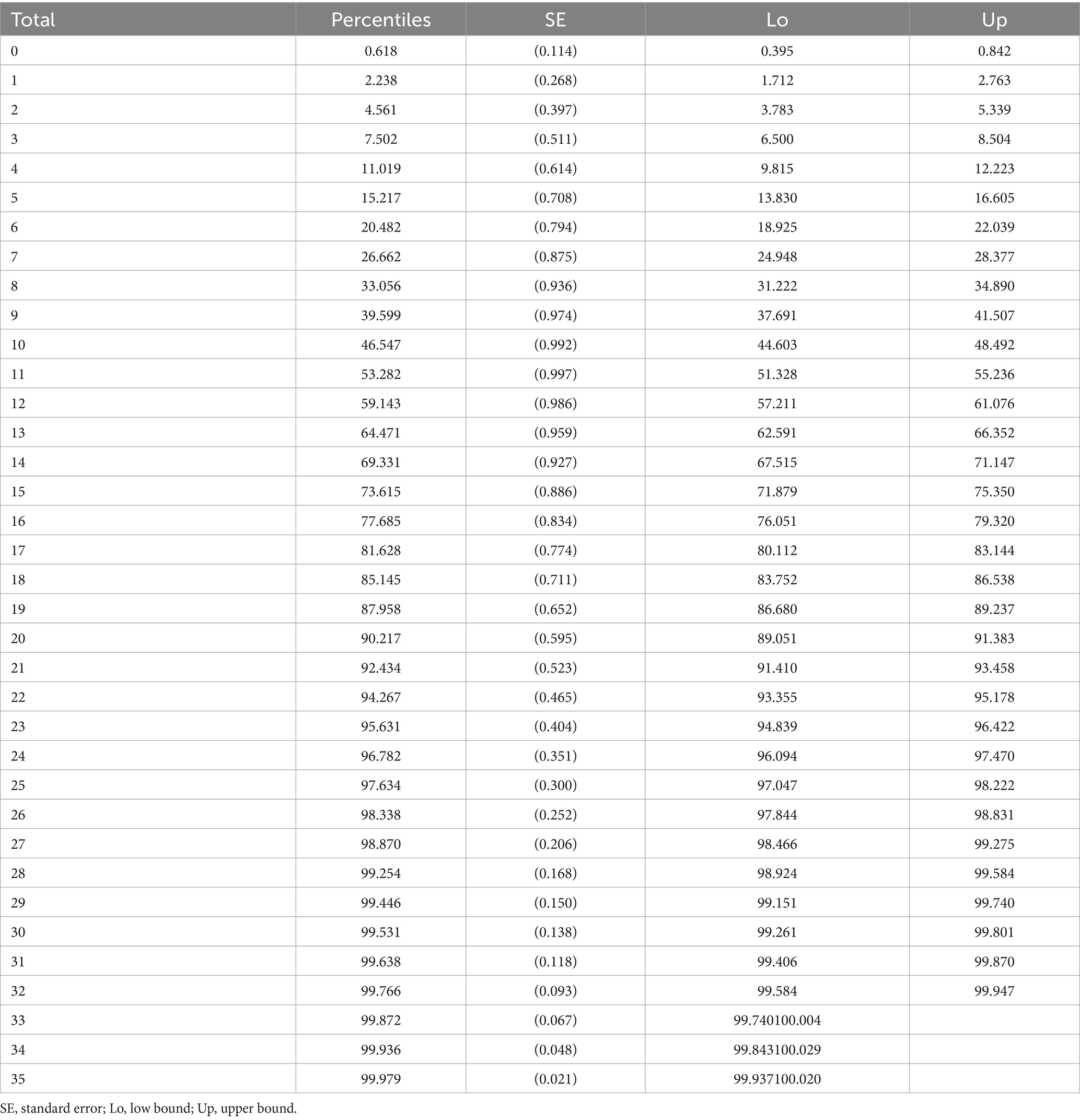
Table 16. Percentile norms for compassion fatigue Burnout.
Mokken analysis
Compassion Fatigue Secondary traumatic stress subscale.
Automated item selection procedure (with genetic algorithm) suggested a unidimensional scale with 12 items (20, 21, 22, 28, 29, 31, 32, 34, 36, 39, 40, 44) out of the original 23 items. Coefficient H for this subscale was H = 0.404 (0.010). Given the standard error, this value is not acceptable. After removing item 44 with H = 0.307 (0.016), the value for the subscale increased to H = 0.423 (0.010). Taking into account the standard error, this value is acceptable for a medium strong scale. Testing for local independence flagged item 20 as positively locally dependent with item 21. After removing item 20, the remaining 10 items were locally independent. The monotonicity test did not flag any of the items. The test for invariant item ordering flagged item 22. After removing item 22, the remaining items were locally independent, and the value for the subscale was H = 0.439 (0.011). The final set of items in this subscale was: 21, 28, 29, 31, 32, 34, 36, 39, 40 (medium strong scale). See Table 1 for details, and Supplementary Appendix 1 for the norms.
Compassion fatigue burnout subscale
Automated item selection procedure (with genetic algorithm) suggested a unidimensional scale with 11 items (23, 24, 41, 42, 45, 48, 49, 60, 62, 63, 64) out of the original 17 items. Coefficient H for this subscale was H = 0.383 (0.009), which is not acceptable. After removing item 23 with H = 0.303 (0.014), the value for the subscale increased to H = 0.404 (0.009). Given the standard error, this value is still not acceptable. After removing another item (24) with H = 0.311 (0.015), the value for the subscale increased to H = 0.430 (0.010). Testing for local independence flagged item 49 as positively locally dependent with item 60, after removing it all the items were locally independent. The monotonicity test did not flag any of the items. The test for invariant item ordering flagged item 45. After removing item 45, all the remaining items were locally independent, and the value for the subscale was H = 0.439 (0.011). The final set of items in this subscale was: 41, 42, 48, 60, 62, 63, 64 (medium strong scale). See Table 3 for details, and Supplementary Appendix 1 for norms.
Compassion satisfaction subscale
Automated item selection procedure (with genetic algorithm) failed to confirm a unidimensional scale, but suggested two subscales: the first subscale had 13 items (1, 2, 3, 9, 10, 14, 19, 26, 27, 46, 52, 53, 55) and the second subscale 6 items (30, 35, 47, 57, 61, 66). Therefore, we analyzed these subscales separately to see if they could constitute Mokken scales on their own.
Compassion satisfaction personal integrity and happiness subscale
Testing for the local independence of the first subscale flagged 4 mutually positively locally dependent items (19, 27, 53, 55). After removing them, the remaining 9 items were locally independent. The monotonicity test did not flag any of the items. The test for invariant item ordering flagged items 9, 26, 46, 52. The final set of items in this subscale was 1, 2, 3, 10, 14, and the value for the subscale was H = 0.589 (0.012), a strong scale. See Table 2 for details, and Supplementary Appendix 1 for the norms.
Compassion satisfaction work competence and happiness subscale
Testing for the local independence of the second subscale flagged one item (61) that was positively locally dependent with item 30. After removing it, all remaining 5 items were locally independent. The monotonicity test did not flag any items, and neither did the test for invariant item ordering. The final set of items in this subscale was 1, 2, 3, 10, 14, and the value for the subscale was H = 0.381 (0.013), a weak scale. See Table 2 for details, and Supplementary Appendix 1 for norms.
Discussion
The aim of the present study was to revise the Compassion Fatigue and Satisfaction Self-Test for Helpers (11) using Mokken scale analysis for polytomous items (18, 19) to shorten it and improve its psychometric properties for diagnostic purposes. Additionally, we wanted to create norms for the helping professional population.
Contrary to previous research studies that used the CFST (11) with very small and highly specific samples of helping professionals [e.g., Figley (53) and Steed and Bicknell (22)], our research sample consisted of 2,320 participants from various helping professionals (more than 30 different helping professions) which allows us to generalize the results to all sorts of helping professionals and to create norms (percentile rank norms, z-score norms, and stanine boundaries) for the newly developed scale so that compassion fatigue and compassion satisfaction can be diagnosed among different kinds of helping professionals.
Based on the Mokken scale analysis for polytomous items (18, 19), we deleted most of the items on the CFST (11) to improve scalability. The remaining items showed good scalability (with item scalability coefficients ranging from 0.349 to 0.655 and Molenaar–Sijtsma reliability coefficient between 0.75 and 0.87). As a result, we created a revised and shortened Compassion Satisfaction and Compassion Fatigue scale for the CFST (11) that has four subscales: Compassion Fatigue—Secondary Traumatic Stress, and Compassion Fatigue—Burnout were just shortened and renamed so as to better fit the proposed theory of Stamm (64); however, Compassion Satisfaction was divided into Compassion Satisfaction—Personal Integrity and Happiness, and Compassion Satisfaction—Work Competence and Happiness. The names of the subscales for the compassion fatigue items in our results correspond to the conceptualization that compassion fatigue is a combination of burnout and secondary traumatic stress (64). Accordingly, it corresponds to the names Adams et al. (63) attributed to the subscales of the shortened version of the CSFT (CF-Short Scale): burnout and secondary trauma. All the subscales of the newly developed scale are reliable and have high scalability. As a result, the final version of the revised and shortened CSFT consists of the following four subscales Compassion Satisfaction—Personal Integrity and Happiness (5 items) and Compassion Satisfaction—Work Competence and Happiness (5 items), Compassion fatigue—Secondary Traumatic Stress (9 items) and Compassion Fatigue—Burnout (7 items). The original CSFT has 66 items and the revised shortened version of CSFT has 26 items. The robust statistical analysis allows us to contribute new findings to the theory of professional quality of life developed by Stamm (64). Compassion fatigue stayed as it was, but compassion satisfaction emerged to consist of Personal Integrity and Happiness and Work Competence and Happiness. See Figure 4. Up until now, none of the elements of compassion satisfaction had been theorized or analyzed so this is the first step toward identifying compassion satisfaction and its constituent elements.

Figure 4. Model of professional quality of life.
The newly adapted and shortened scale has good reliability coefficients measured by Cronbach alpha. Regarding reliability, all the Cronbach alpha polychoric coefficients were between 0.75 and 0.89. As they were above 0.70, we can conclude it has good reliability. [e.g., Streiner and Norman (36)]. Our results therefore support previous research findings that reported good reliability coefficients for the CFST (5, 20–22, 60).
In the revised version of the CSCFS, Compassion Satisfaction has two subscales: Personal Integrity and Happiness, and Work Competency and Happiness. Personal Integrity and Happiness is mainly composed of items that demonstrate happiness, satisfaction, and calmness as opposed to stress (1. I am happy. 2. I find my life satisfying. 10. I feel calm) and captured personal integrity (3. I have beliefs that sustain me. 14. I am the person I always wanted to be) indicating that the person lives their life according to their beliefs which may be related to the spiritual sphere (2).
Work Competency and Happiness is comprised of items relating to work happiness and feeling competent at one’s job (30. I have happy thoughts about those I help and how I could help them. 35. I have joyful feelings about how I can help the victims I work with. 47. I feel like I have the tools and resources that I need to do my work as a helper. 57. I am pleased with how I am able to keep up with helping technology). There is one item that describes being a long-term helper (66. I plan to be a helper for a long time).
Similarly to Stamm (64), the compassion fatigue in the revised version of the CSCFS has two subscales: Secondary Traumatic Stress, and Burnout. The Secondary Traumatic Stress subscale of the CSCFS consists of items relating to the symptoms of PTSD (DSM-5., 2013) such as: Intrusion (29. I experience troubling dreams similar to those I help. 31. I have experienced intrusive thoughts of times with especially difficult people I helped. 32. I have suddenly and involuntarily recalled a frightening experience while working with a person I helped), changes in cognition and mood (28. I am frightened of things a person I helped has said or done to me. 36. I think that I might have been “infected” by the traumatic stress of those I help), Altered Arousal and Reactivity (34. I am losing sleep over a person I help’s traumatic experiences) but not in Avoidance. None of the avoidance-related items, be that avoidance of people, things, or activities, was retained in the revised subscale. However, there appears to be a degree of avoidance in the following items: 39. I have felt trapped by my work as a helper and 40. I have a sense of hopelessness associated with working with those I help. This suggests that helping professionals might seek avoidance, but that in practice the nature of their work does not allow them to be avoidant, unless they are willing to quit their job.
One of the selected items of Compassion Fatigue—Secondary Traumatic Stress that remained after the Mokken scale analysis related to previous trauma experience in the person’s life (21. I have had first-hand experience with traumatic events in my childhood). In a systematic review, Bryce et al. (37) indicated that childhood trauma or adversity was indeed associated with the helping professions as a career choice. As Malach-Pines and Yafe-Yanai (38) explains, people are frequently driven to choose a career which corresponds with their childhood experiences, satisfies unmet needs from childhood, and achieves family aspirations. “People strive to actively master what they passively suffer” ((39), p. 55). Eighty percent of mental health professionals reported traumatic experience (56). The correlation between previous traumatic experience and risk of compassion fatigue has been analyzed [e.g., Boscarino et al. (40)].
It is possible that the trauma of clients and patients that helping professionals work with echoes their own unprocessed trauma. It would be interesting to focus on this more in future research and to find out whether helping professionals might be more prone to experiencing secondary traumatisation because they have previously experienced trauma themselves. Further research could also focus on the process of shared trauma [e.g., Tosone (41)], on the possible predictors of exposure-to-repeated-trauma, on posttraumatic growth, on compassion satisfaction trajectory or of exposure-to-repeated-trauma and on compassion fatigue and on mental health problems trajectory.
Based on DSM-5 (42), just as the Compassion Fatigue Secondary Traumatic Stress items are similar to the symptoms of PTSD, Compassion Fatigue Burnout consists of items similar to the symptoms of depression and anxiety. The CSCFS items relating to Anxiety symptoms [DSM-5; American Psychiatric Association (42)] are (41. I have felt “on edge” about various things and I attribute this to working with certain people I help. 48. I have felt weak, tired, run down as a result of my work as a helper.). The CSCFS items relating to Depressive symptoms [DSM-5; American Psychiatric Association (42)] are (48. I have felt weak, tired, run down as a result of my work as a helper. 62. I have a sense of worthlessness/disillusionment/resentment associated with my role as a helper. 63. I have thoughts that I am a “failure” as a helper. 64. I have thoughts that I am not succeeding at achieving my life goals.). However, none of these would be sufficient for a diagnosis of anxiety or depression disorder as the items do not meet the minimum requirements of 3 out of 6 for anxiety or 5 out of 9 for depression. Additionally, the subscale contains items relating to work-life balance and avoidance of helping (60. I find it difficult separating my personal life from my helper life. 42. I wish that I could avoid working with some people I help).
One could hypothesize that in order for helping professionals to help others, they must themselves have a satisfying personal and work life, otherwise they could end up exhausted and drained of resources. According to Kessler et al. (43), being exposed to trauma does not cause pathology. The pivotal things that decide whether a person stays mentally healthy or not are resilience and social support (44). Surprisingly, none of the CSCFS items relate directly to personal relationships or social support. One might argue that happiness is not possible without personal relationships and social support and, therefore, they are included in somewhat more generalized items like “I am happy.” or “I find my life satisfying.”
To manage levels of compassion fatigue and increase compassion satisfaction, it appears that people should build a good life for themselves from the very beginning of their helping profession career, and that this should be part of the curriculum for all helping professionals so they can avoid or prevent compassion fatigue.
Implications
The new scale for measuring compassion fatigue and compassion satisfaction is psychometrically sound and contains a small number of items, facilitating early screening and detection of symptomatology. This enables swift intervention to prevent compassion fatigue and ensure high-quality services. Creating norms for the CSCFS will help professionals make meaningful comparisons against the general population and be vigilant about the various degrees of compassion fatigue screening.
Moreover, the scale can be used for regular monitoring, aiding in the identification of trends and patterns in compassion fatigue and satisfaction over time (64). This can inform the development of targeted interventions and support programs tailored to the specific needs of healthcare professionals (45).
The scale’s brevity and ease of use also make it suitable for integration into routine assessments in various healthcare settings, promoting a culture of mental health awareness and proactive care (46). Additionally, its cross-cultural applicability can enhance global research efforts, allowing for comparative studies and the development of universal strategies to address compassion fatigue and promote well-being among healthcare providers (16).
Using this scale can lead to better resource allocation by identifying departments or teams most at risk of compassion fatigue, thereby directing support and interventions where they are most needed (47). This could ultimately reduce turnover rates and improve job satisfaction, contributing to a more stable and effective workforce (48).
Limitations and future directions
The primary limitation of our study is that the sample consists entirely of Slovak helping professionals, which may introduce cultural biases and limit the generalizability of our findings to other populations. Consequently, the revised version of the Compassion Satisfaction and Compassion Fatigue Scale (CSCFS) may reflect cultural nuances specific to the Slovak context. To address this limitation, future research should test the CSCFS in diverse cultural settings and professional environments to assess its usability and validate its factor structure across a broader range of samples (16). Expanding the study by including different different healthcare professions separately, such as nursing, psychology, and social work, could provide a more comprehensive understanding of the scale’s applicability into specific helping professions (45). Additionally, longitudinal studies would be beneficial to evaluate the stability of the scale over time and its sensitivity to changes in compassion fatigue and satisfaction following various interventions (64). This approach would help in refining the scale and enhancing its utility in diverse contexts.
Conclusion
The Compassion Satisfaction and Compassion Fatigue Scale (CSCFS) appears to be a reliable and valid measure for assessing compassion fatigue and satisfaction, facilitating early screening and diagnosis. This tool provides a valuable means for researchers and practitioners to identify and address compassion fatigue, enabling timely interventions that can enhance the well-being of healthcare providers (49). By measuring the effectiveness of interventions and treatments, the CSCFS helps ensure high-quality care for patients, clients, and customers. As the scale is adopted in various cultural contexts and professional settings, it has the potential to become a standard tool for assessing compassion-related outcomes, thereby contributing to improved healthcare systems and provider well-being globally (46, 50).
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by the Ethical comittee of Faculty of Social and Economic Sciences of Comenius University in Bratislava. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
JH: Conceptualization, Funding acquisition, Methodology, Resources, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. MK: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Software, Validation, Visualization, Writing – original draft, Writing – review & editing. KK: Project administration, Writing – review & editing. BS: Resources, Writing – review & editing. MB: Methodology, Writing – review & editing. CF: Supervision, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. This work was supported by the Slovak Research and Development Agency under the Contract no. PP-COVID-20-0074. Writing this work was supported by the Vedecká grantová agentúra VEGA under Grant 1/0054/24.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2024.1406467/full#supplementary-material
References
1. England, P, and Nancy, F. The cost of caring. Ann Amer Acdmy Polit Soci Sci. (1999) 561:39–51. doi: 10.1177/000271629956100103
2. Figley, CR . Compassion fatigue: psychotherapists’ chronic lack of self care. J Clin Psychol. (2002) 58:1433–41. doi: 10.1002/jclp.10090
3. Ondrejková, N, and Halamová, J. Prevalence of compassion fatigue among helping professions and relationship to compassion for others, self-compassion and self-criticism. Health Soc Care Community. (2022) 30:1680–94. doi: 10.1111/hsc.13741
4. Schwam, K . The phenomenon of compassion fatigue in perioperative nursing. AORN. (1998) 68:642–8. doi: 10.1016/S0001-2092(06)62569-6
5. Rudolph, JM, Stamm, BH, and Stamm, HE. Compassion fatigue: a concern for mental health policy, providers, & administration In: Poster presentation at the annual meeting of the International Society for Traumatic Stress Studies. Montreal, Canada (1997).
6. Francis, R . Report of the mid Staffordshire NHS foundation trust public inquiry. London, UK: The Stationery Office (2013).
7. Cavanagh, N, Cockett, G, Heinrich, C, Doig, L, Fiest, K, Guichon, JR, et al. Compassion fatigue in healthcare providers: a systematic review and meta-analysis. Nurs Ethics. (2020) 27:639–65. doi: 10.1177/0969733019889400
8. Shanafelt, TD, Dyrbye, LN, Sinsky, C, Hasan, O, Satele, D, Sloan, J, et al. Relationship between clerical burden and characteristics of the electronic environment with physician burnout and professional satisfaction. Mayo Clin Proc. (2015) 91:836–48. doi: 10.1016/j.mayocp.2016.05.007
9. Tawfik, DS, Profit, J, Morgenthaler, TI, Satele, DV, Sinsky, CA, Dyrbye, LN, et al. Physician burnout, well-being, and work unit safety grades in relationship to reported medical errors. Mayo Clin Proc. (2019) 93:1571–80. doi: 10.1016/j.mayocp.2018.05.014
10. Bride, BE, Radey, M, and Figley, CR. Measuring compassion fatigue. Clin Soc Work J. (2007) 35:155–63. doi: 10.1007/s10615-007-0091-7
11. Stamm, B. H., and Figley, C. R. (1996). Compassion satisfaction and fatigue test. Available at: http://www.i-su.edu/~bstamm/tests.htm (Accessed May 17, 2023).
12. Stamm, B. H. (2009). Professional Quality of Life: Compassion Satisfaction and Fatigue Version 5 (ProQOL). Available at: www.proqol.org (Accessed May 23, 2022).
13. Keesler, JM, and Fukui, S. Factor structure of the professional quality of life scale among direct support professionals: factorial validity and scale reliability. J Intellect Disabil Res. (2020) 64:681–9. doi: 10.1111/jir.12766
14. Duarte, J . Professional quality of life in nurses: contribution for the validation of the Portuguese version of the professional quality of life Scale-5 (pro-QOL-5). Analise Psicologica. (2017) 35:529–42. doi: 10.14417/ap.1260
15. Hemsworth, D, Baregheh, A, Aoun, S, and Kazanjian, A. A critical enquiry into the psychometric propertiesof the professional quality of life scale (ProQol-5) instrument. Appl Nurs Res. (2018) 39:81–8. doi: 10.1016/j.apnr.2017.09.006
16. Heritage, B, Rees, CS, and Hegney, DG. TheProQOL-21: a revised version of the professional Qualityof life (ProQOL) scale based on Rasch analysis. PLoSONE. (2018) 13:e0193478.
17. Hotchkiss, JT, and Wong, MYC. Factorial structure of the ProQOL—systematic Meta-analysis and integration of 27 international factor analysis studies. Trends Psychol. (2022). doi: 10.1007/s43076-022-00184-5
18. Wessels, D, Van Assen, A, Post, W, and Van der Putten, A. The construct validity and reliability of the motor development list for the assessment of motor skills in children with profound intellectual and multiple disabilities: the next step? J Intellect Develop Disabil. (2023) 48:370–83. doi: 10.3109/13668250.2023.2188877
19. Sijtsma, K, and Van der Ark, LA. A tutorial on how to do a Mokken scale analysis on your test and questionnaire data. Br J Math Stat Psychol. (2017) 70:137–58. doi: 10.1111/bmsp.12078
20. Ortlepp, K, and Friedman, M. Prevalence and correlates of secondary traumatic stress in workplace lay trauma counselors. J Trauma Stress. (2002) 15:213–22. doi: 10.1023/A:1015203327767
21. Conrad, D, and Kellar-, GY. Compassion fatigue, Burnout, and compassion satisfaction among Colorado child protection workers. Child Abuse Negl. (2006) 30:1071–80. doi: 10.1016/j.chiabu.2006.03.009
22. Steed, L, and Bicknell, J. Trauma and the therapist: the experience of therapists working with the perpetrators of sexual abuse. Australas J Disaster Trauma Stud. (2001) 31:25–36. doi: 10.1016/j.cpr.2010.09.004
23. Beck, CT . Secondary traumatic stress in nurses: a systematic review. Arch Psychiatr Nurs. (2011) 25:1–10. doi: 10.1016/j.apnu.2010.05.005
24. Brown, T . Confirmatory factor analysis for applied research. New York, NY: Guildford Press (2014).
25. R Core Team . R: A language and environment for statistical computing. Vienna, Austria: R Foundation for Statistical Computing (2022).
26. van der Ark, LA . Mokken scale analysis in R. J Stat Softw. (2007) 20:1–19. doi: 10.18637/jss.v020.i11
27. Straat, JH, Van der Ark, LA, and Sijtsma, K. Comparing optimization algorithms for item selection in Mokken scale analysis. J Classif. (2013) 30:72–99. doi: 10.1007/s00357013-9122y
29. Straat, JH, Van der Ark, LA, and Sijtsma, K. Using conditional association to identify locally independent item sets. Methodology. (2016) 12:117–23. doi: 10.1027/1614-2241/a000115
30. Junker, BW, and Sijtsma, K. Latent and manifest monotonicity in item response models. Appl Psychol Meas. (2000) 24:65–81. doi: 10.1177/01466216000241004
31. Ligtvoet, R, van der Ark, LA, te Marvelde, JM, and Sijtsma, K. Investigating an invariant item ordering for polytomously scored items. Educ Psychol Meas. (2010) 70:578–95. doi: 10.1177/0013164409355697
32. Gelman, A, Carlin, JB, Stern, HS, and Rubin, DB. Bayesian Data Analysis. 3rd ed. New York: Chapman & Hall, CRC (2013).
33. Su, YS, Gelman, A, Hill, J, and Yajima, M. Multiple imputation with diagnostics (mi) in R: opening windows into the black box. J Stat Softw. (2011) 45:1–31. doi: 10.18637/jss.v045.i02
34. Zijlstra, WP, Van der Ark, LA, and Sijtsma, K. Outlier detection in test and questionnaire data. Multivar Behav Res. (2007) 42:531–55. doi: 10.1080/00273170701384340
35. Hubert, M, and Vandervieren, E. An adjusted boxplot for skewed distributions. Comput Stat Data Anal. (2008) 52:5186–201. doi: 10.1016/j.csda.2007.11.008
36. Streiner, DL, and Norman, GR. Health measurement scales: A practical guide to their development and use. 4th ed. Oxford: Oxford University Press (2008).
37. Bryce, I, Pye, D, Beccaria, G, McIlveen, P, and Du Preez, J. A systematic literature review of the career choice of helping professionals who have experienced cumulative hard as a result of adverse childhood experiences. Trauma Viol Abuse. (2021)
38. Malach-Pines, A, and Yafe-Yanai, O. Unconscious determinants of career choice and burnout: theoretical model and counseling strategy. J Employ Couns. (2001) 38:170–84. doi: 10.1002/j.2161-1920.2001.tb00499.x
39. Savickas, ML . A developmental perspective on vocational behaviour: career patterns, salience, and themes. Int J Educ Vocat Guid. (2001) 1:49–57. doi: 10.1023/A:1016916713523
40. Boscarino, JA, Figley, CR, and Adams, RE. Compassion fatigue following the September 11 terrorist attacks: a study of secondary trauma among new York City social workers. Int J Emerg Ment Health. (2004) 6:57–66.
41. Tosone, C . Therapeutic intimacy: a post-9/11 perspective. Smith Coll Stud Soc Work. (2006) 76:89–98. doi: 10.1300/J497v76n04_12
42. American Psychiatric Association (APA) . Diagnostic and statistical manual of mental disorders. 5th ed Washington DC: American Psychiatric Publishing (2013).
43. Kessler, RC, Sonnega, A, Bromet, E, Hughes, M, and Nelson, C. Posttraumatic stress disorder in the National Comorbidity Survey. Arch Gen Psychiatry. (1995) 52:1048–59. doi: 10.1001/archpsyc.1995.03950240066012
44. King, L, King, D, Fairbank, J, and Adams, G. Resilience-recovery factors in post-traumatic stress disorder among female and male veterans: hardiness, post war social support and additional stressful life events. J Pers Soc Psychol. (1998) 74:420–34. doi: 10.1037/0022-3514.74.2.420
45. Hinderer, KA, VonRueden, KT, Friedmann, E, McQuillan, KA, Gilmore, R, Kramer, B, et al. Burnout, compassion fatigue, compassion satisfaction, and secondary traumatic stress in trauma nurses. J Trauma Nurs. (2014) 21:160–9. doi: 10.1097/JTN.0000000000000055
46. Smart, D, English, A, James, J, Wilson, M, Daratha, KB, Childers, B, et al. Compassion fatigue and satisfaction: a cross-sectional survey among US healthcare workers. Nurs Health Sci. (2014) 16:3–10. doi: 10.1111/nhs.12068
47. Sabo, B . Reflecting on the concept of compassion fatigue. Online J Issues Nurs. (2011) 16:1. doi: 10.3912/OJIN.Vol16No01Man01
48. Kelly, L, Runge, J, and Spencer, C. Predictors of compassion fatigue and compassion satisfaction in acute care nurses. J Nurs Scholarsh. (2015) 47:522–8. doi: 10.1111/jnu.12162
49. Gillepsie, BM, Chaboyer, W, Wallis, M, and Grimbeek, P. Resilience in the operating room: developing and testing of a resilience model. J Adv Nurs. (2007) 59:427–38. doi: 10.1111/j.1365-2648.2007.04340.x
50. Duarte, J, Pinto-Gouveia, J, and Cruz, B. The role of psychological factors in oncology nurses' Burnout and compassion fatigue symptoms. Eur J Oncol Nurs. (2020) 28:101773:114–21. doi: 10.1016/j.ejon.2017.04.002
51. Gentry, JE, Baranowsky, AB, and Dunning, K. ARP: The accelerated recovery program (ARP) for compassion fatigue. In CR Figley (editor), Treating compassion fatigue (New York, NY: Routledge) (2002) pp. 123–137.
52. Stamm, BH . The ProQoL manual. The professional quality of life scale: Compassion satisfaction, burnout, and compassion fatigue/secondary trauma scales. Lutherville, MD: Sidran Press. (2005).
53. Figley, CR, and Roop, RG. Compassion fatigue in the animal care community. Washington, DC: Humane Society Press. (2006).
55. Musetti, A, Schianchi, A, Caricati, L, Manari, T, and Schimmenti, A. (2020). Exposure to animal suffering, adult attachment styles, and professional quality of life in a sample of Italian veterinarians. PLoS One, 15:e0237991. doi: 10.1371/journal.pone.0237991
56. Pearlman, LA, and MacIan, PS. Vicarious traumatization: An empirical study of the effects of trauma work on trauma therapists. Clin Psychol Sci Pr. (1995) 26:558–65.
58. Sijtsma, K, and Molenaar, IW. Introduction to nonparametric item response theory. Thousand Oaks, CA: Sage Publications. (2002).
59. Sijtsma, K, and Molenaar, IW. Reliability of test scores in nonparametric item response theory. Psychometrika (1987) 52:79–97. doi: 10.1007/BF02293957
60. Figley, CR . Compassion fatigue: Toward a new understanding of the costs of caring. In BH Stamm (editor), Secondary traumatic stress: Self-care issues for clinicians, researchers, and educators (The Sidran Press), (1995) pp. 3–28.
61. Kristensen, TS, Borritz, M, Villadsen, E, and Christensen, KB. The Copenhagen Burnout Inventory: A new tool for the assessment of burnout. Work Stress. (2005) 19:192–207.
62. Jenkins, SR, and Baird, S. Secondary traumatic stress and vicarious trauma: A validational study. J Trauma Stress: Official Publication of The International Society for Traumatic Stress Studies, (2002) 15:423–32. doi: 10.1023/A:1020193526843
63. Adams, RE, Boscarino, JA, and Figley, CR. Compassion fatigue and psychological distress among social workers: A validation study. Am J Orthopsychiatry. (2006) 76:103–8.
64. Stamm, BH (2010). The Concise ProQOL Manual. Retrieved from: https://proqol.org/uploads/ProQOLManual.pdf
Keywords: compassion fatigue, compassion satisfaction, helping professionals, psychometrics, self-testing
Citation: Halamová J, Kanovský M, Krizova K, Šoková B, Baránková M and Figley C (2024) The development of the Compassion Satisfaction and Compassion Fatigue scale. Front. Public Health. 12:1406467. doi: 10.3389/fpubh.2024.1406467
Edited by:
Jenni Spannari, University of Helsinki, FinlandReviewed by:
Emanuele Maria Merlo, University of Messina, ItalyFrancesco Franza, Psychiatric Rehabilitation Center Villa dei Pini, Italy
Copyright © 2024 Halamová, Kanovský, Krizova, Šoková, Baránková and Figley. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Júlia Halamová, anVsaWEuaGFsYW1vdmFAZ21haWwuY29t