 Ruoyi Zhang1,2†‡
Ruoyi Zhang1,2†‡ Dan Kang1†‡Siyuan Yang3Dehua Hu4Li Bai4Yongping Ao1Jiaojiao Chen1Yuxian Nie5Xiaowei Zhao4
Dan Kang1†‡Siyuan Yang3Dehua Hu4Li Bai4Yongping Ao1Jiaojiao Chen1Yuxian Nie5Xiaowei Zhao4 Wei Xu1*‡
Wei Xu1*‡ Qiuling Shi1,5*‡
Qiuling Shi1,5*‡- 1School of Public Health, Chongqing Medical University, Chongqing, China
- 2Xian Center for Disease Control and Prevention, Xian, China
- 3School of Nursing, Chongqing Medical University, Chongqing, China
- 4Maternal and Child Health, The Maternity Service Centre of Lueyang Maternal and Child Health Care Hospital, Lueyang, China
- 5State Key Laboratory of Ultrasound in Medicine and Engineering, Chongqing Medical University, Chongqing, China
Background: Reproductive tract infections (RTIs) represent a critical public health concern impacting women’s health, particularly pronounced in developing countries. We aim to investigates the prevalence of self-reported RTI symptoms in women aged 18 to 65 and the factors influencing gynecological examination behavior and associated risks are explored.
Methods: From May 6, 2022, to September 20, 2022, a comprehensive survey engaged 20,864 women aged 18 to 65 in 19 townships in Lueyang, Shaanxi. Each survey team, comprising a gynecologist, two female health center staff, and a master’s student, conducted face-to-face questionnaire surveys in villages and households. The questionnaire featured three sections: prevalence of self-reported RTI symptoms, gynecological examination history, and factors influencing examination behavior.
Results: The high response rate of 98.69% yielded 20,590 valid questionnaires. Among surveyed women, 42.04% reported RTI symptoms, with a higher prevalence in those aged 30 and above, peaking at 44.88% in the 50–59 age group. Vulvar itching (24.73%), abnormal vaginal discharge (17.41%), and urinary tract irritation signs (11.73%) were most common. Older adult women (≥60) reported higher frequency and longer duration of symptoms. Only 9.88% of symptomatic women underwent gynecological examinations in 2022. Examination likelihood decreased with age, presenting a critical gap in healthcare utilization among older women. Reasons for checkups included routine checkups (47.02%), symptom concerns (41.29%), and the availability of free medical checkup programs (9.82%). Barriers included perceived lack of serious symptoms (23.7%), lack of necessity (4.41%) and lack of time (3.98%). Among those examined, 40.58% had a diagnosis of gynecological disorders, including pelvic inflammatory disease, human papilloma virus infection and cervical cancer.
Conclusion: Widespread RTI symptoms, particularly in perimenopausal and older women, underscore the need for enhanced healthcare. Barriers to gynecological examinations include awareness, education, and accessibility issues. Strategies must prioritize health education, routine examinations, and improved healthcare infrastructure in underdeveloped regions.
1 Introduction
Reproductive tract infections (RTIs) represent a critical public health concern impacting women’s health, particularly pronounced in developing countries (1). Early prevention of RTI is paramount as they elevate the risk of severe reproductive diseases, including pelvic inflammatory disease, miscarriage, preterm birth, infertility, sexually transmitted infections, and cervical cancer (2). These infections not only inflict reproductive harm upon women of childbearing age but also pose a heightened risk of malignant tumors, such as cervical cancer, among perimenopausal and older adult women (3).
In underdeveloped regions, the prevalence of RTIs may be underestimated due to factors such as lower educational levels, limited autonomy in personal health decisions, lower economic status, inadequate healthcare facilities, insufficient medical resources, and cultural norms of silence concerning diseases (4). These factors contribute to the poor recognition and management of RTIs, leading to a cycle of poor health outcomes and further socio-economic decline. Approximately 38 to 85% of rural women in China are reported to exhibit at least one symptom indicative of RTIs; however, the utilization of healthcare services remains remarkably low (5).
Laboratory testing is considered the gold standard for accurately measuring RTI prevalence. However, the applicability of such tests is limited in rural areas due to insufficient healthcare facilities and a shortage of specialized gynecologists (6). Therefore, in cost-effective terms, self-reporting of RTI symptoms remains a crucial means of assessing the incidence and impact of RTIs, particularly in underdeveloped regions (7). Globally, most cancers (85–90%) are diagnosed on the basis of symptomatic manifestations, despite the availability of cancer screening programs (8), and self-reporting of RTI symptoms contributes to three-early prevention of the disease (9, 10).
Lueyang County in Shaanxi Province is recognized as one of the regions with the highest incidence of cervical cancer and the lowest average income nationwide (11). Therefore, the aim of this study was to investigate the self-reported RTI symptoms, gynecological examination, and related influencing factors of women in Lueyang County, Shaanxi Province, to clarify the relationship between self-reported RTI symptoms and gynecological disorders, and to provide a preventive strategy to improve the rate of gynecological examination and gynecological health of women in underdeveloped areas.
2 Methods
2.1 Study participants
From May 6, 2022, to September 20, 2022, we conducted a cross-sectional survey of women aged 18 to 65 years in 19 townships in Lueyang County, Shaanxi Province, regarding self-reported RTI symptoms, gynecological examination history, and related influencing factors. The sample for this study was selected based on a census approach, including all eligible women who met the inclusion criteria. The inclusion criteria were: (1) age between 18 and 65 years; (2) residency in Lueyang County for at least 6 months; and (3) complete understanding of the study.
2.2 Survey method
Each survey team comprised one gynecologist from Lueyang County Maternal and Child Health Hospital, two female staff members from township health centers, and one master’s degree student from Chongqing Medical University. In total, six survey teams conducted face-to-face questionnaire surveys by visiting villages and households.
2.3 Questionnaire design
The survey questionnaire was designed based on a literature review and sought input from professional gynecologists and epidemiologists to ensure its alignment with the specific characteristics of Lueyang County (2, 5, 12–14). The questionnaire consisted of three main sections:
Prevalence of self-reported RTI symptoms in the past 6 months: RTI symptoms included vulvar itching, abnormal vaginal discharge (high volume, yellow color, odor, soybean dregs, bloody, pus, foamy), frequent urination, urgency, painful urination, non-menstrual lower back pain, non-menstrual lower abdominal pain, bleeding after sexual intercourse. Women reporting at least one of these symptoms were considered to have a RTI. The frequency of RTI symptoms was categorized as occasional, sometimes, often, and always. The duration of RTI symptoms was classified as <3 months, 3–6 months, 6 months-1 year, 1–3 years, and > 3 years.
Gynecological examination history and gynecological diagnosis history: whether symptomatic women had a gynecological examination in 2022, reasons for having/not having a gynecological examination, and history of gynecological diagnosis.
Factors influencing women with RTI symptoms who did not undergo gynecological examinations: basic information, number of self-reported RTI symptoms in the past 6 months; menstrual history, marital and reproductive history, sexual behavior, hygiene practices, spouse or sexual partner information.
2.4 Statistical analysis
Statistical analyses were conducted using IBM SPSS (version 23.0), SAS (version 9.4), and R (version 4.2.1). Chi-square (χ2) tests were employed for the analysis of count data rates (%), revealing differences in the prevalence of various RTI symptoms across different groups. The Cochran-Armitage trend test was utilized to assess the linear relationship between the prevalence of individual RTI symptoms and age. The Jonckheere-Terpstra trend test was applied to evaluate whether there was a linear relationship between the frequency and duration of various RTI symptoms and age.
Univariate and multivariate (Inverse stepwise likelihood ratio test) logistic regression analyses were employed to explore the correlation between women exhibiting RTI symptoms but not undergoing gynecological examinations and the influencing factors obtained from the questionnaire survey. Additionally, the Hosmer-Lemeshow test was conducted to assess the goodness of fit of the models. Risk factors with p < 0.1 in the univariate logistic regression analysis were included in the risk regression analysis. The statistical significance level was set at p < 0.05.
To address issues related to missing data, the mice package and VIM package in R software were employed to explore the proportion and types of missing data. The pattern of missing data was determined through a correlation matrix called a shadow matrix. Multiple imputation techniques were employed to handle missing data, followed by an assessment of the reliability of the imputation results. After multiple imputation, the interpolation results with the highest Cronbach’s alpha coefficient were used for multifactor analysis.
3 Results
3.1 Prevalence of self-reported RTI symptoms
A total of 20,864 women were surveyed, and 20,590 valid questionnaires met the inclusion criteria, with a validity rate of 98.69%. A total of 8,657 women (42.04%) reported RTI symptoms in the past 6 months. The prevalence of RTI symptoms exceeded 40% in women aged 30 and above, peaking at 44.88% among those aged 50–59. Individuals with one, two, and multiple (three or more) symptoms constituted 22.93, 11.98, and 7.13% of the total population, respectively (Table 1).
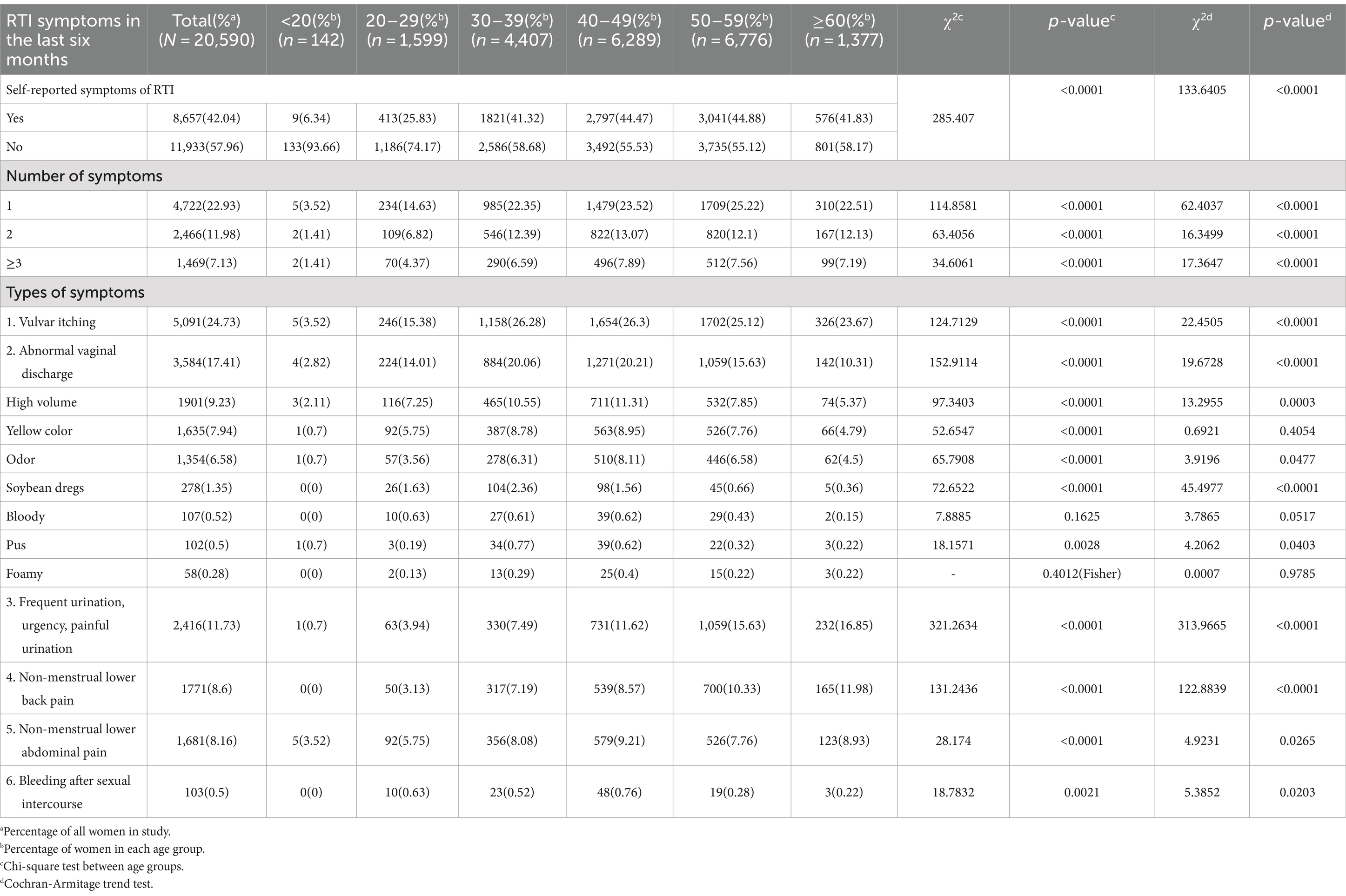
Table 1. Prevalence of self-reported symptoms of RTI in the last 6 months among women of different ages.
The most common RTI symptoms were vulvar itching (24.73%), abnormal vaginal discharge (17.41%), and urinary symptoms including frequency, urgency, and pain (11.73%). The prevalence of non-menstrual lower back pain (8.6%), non-menstrual lower abdominal pain (8.16%), and post-coital bleeding (0.5%) was comparatively lower. Vulvar itching (26.3%), abnormal vaginal discharge (20.21%), non-menstrual lower abdominal pain (9.21%), and post-coital bleeding (0.76%) were most common in the 40–49 age group. Urinary symptoms (16.85%) and non-menstrual lower back pain (11.98%) showed the highest prevalence in individuals aged 60 and above. The prevalence of most symptoms differed across age groups or showed a linear trend with increasing age.
3.2 Frequency of self-reported RTI symptoms
RTI symptoms in females aged 18–65 predominantly exhibit an occasional occurrence, surpassing 40%. Notably, in women aged 60 and above, the proportion of RTI symptoms occurring occasionally decreases, while the occurrence of these symptoms frequently significantly increases in comparison to women under 60 (Figure 1). The Jonckheere-Terpstra trend test showed that the frequency of vulvar itching, vaginal discharge that was heavy, yellowish in color, and foul smelling, urinary frequency, urgency, and pain of urination, non-menstrual lumbosacral pain, and non-menstrual lower abdominal pain increased with age (p < 0.0001; Supplementary Table S1).
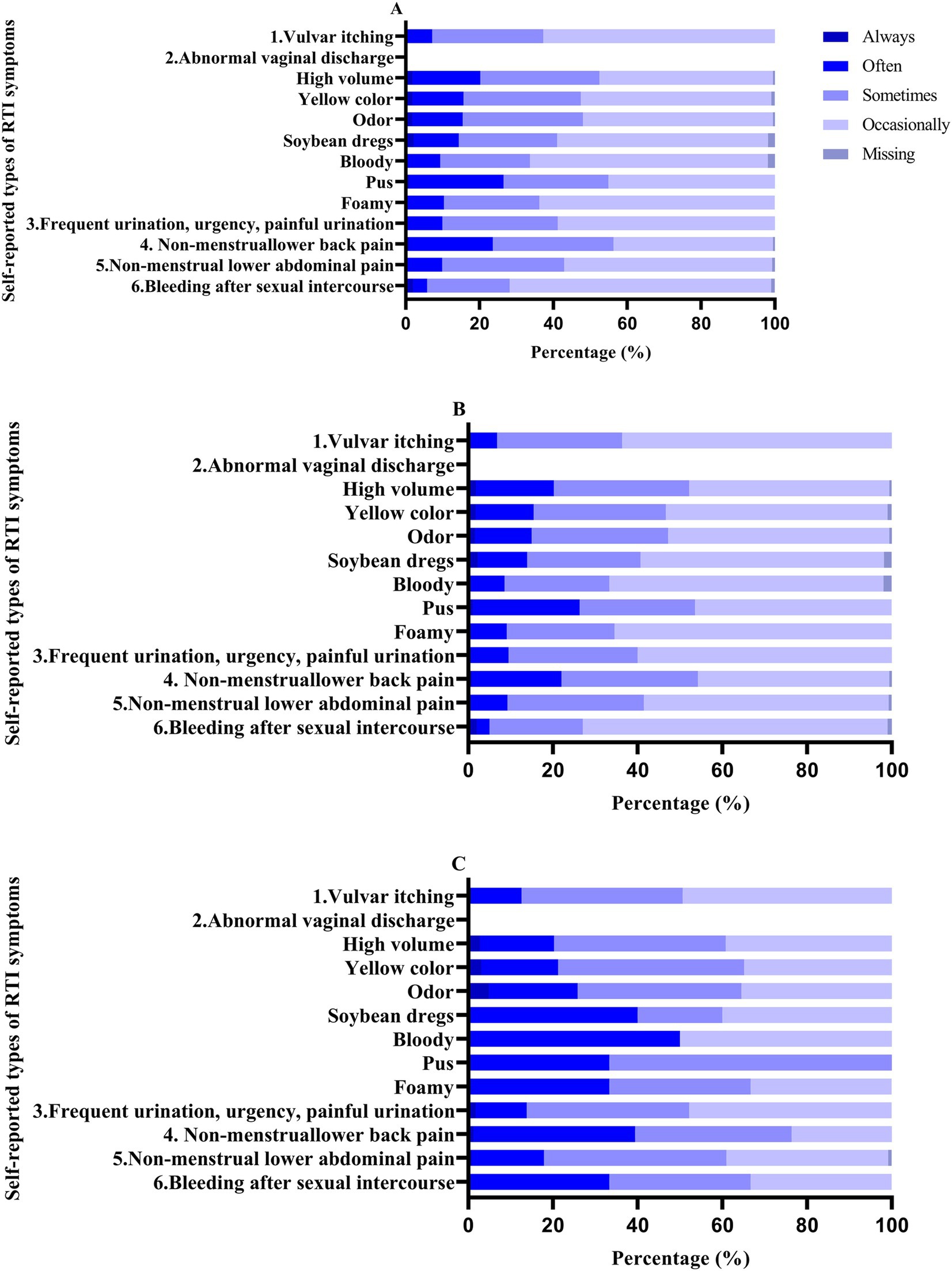
Figure 1. Percentage of self-reported RTI symptom frequencies in patients. A: 18–65 years; b: <60 years; c: ≥60 years.
3.3 Duration of self-reported RTI symptoms
The majority of individuals experiencing self-reported RTI symptoms reported a duration of less than 3 months (>30%). However, a notable proportion of individuals with non-menstrual lower back pain reported a duration exceeding 3 years (33.37%; Figure 2). In the age group of 60 years and above, non-menstrual lower abdominal pain (30.89%), non-menstrual lower back pain (50.3%), increased vaginal discharge (28.38%), yellow-colored discharge (33.33%), malodorous discharge (48.39%), and discharge resembling soybean dregs (40%) had the highest proportions of durations exceeding 3 years.
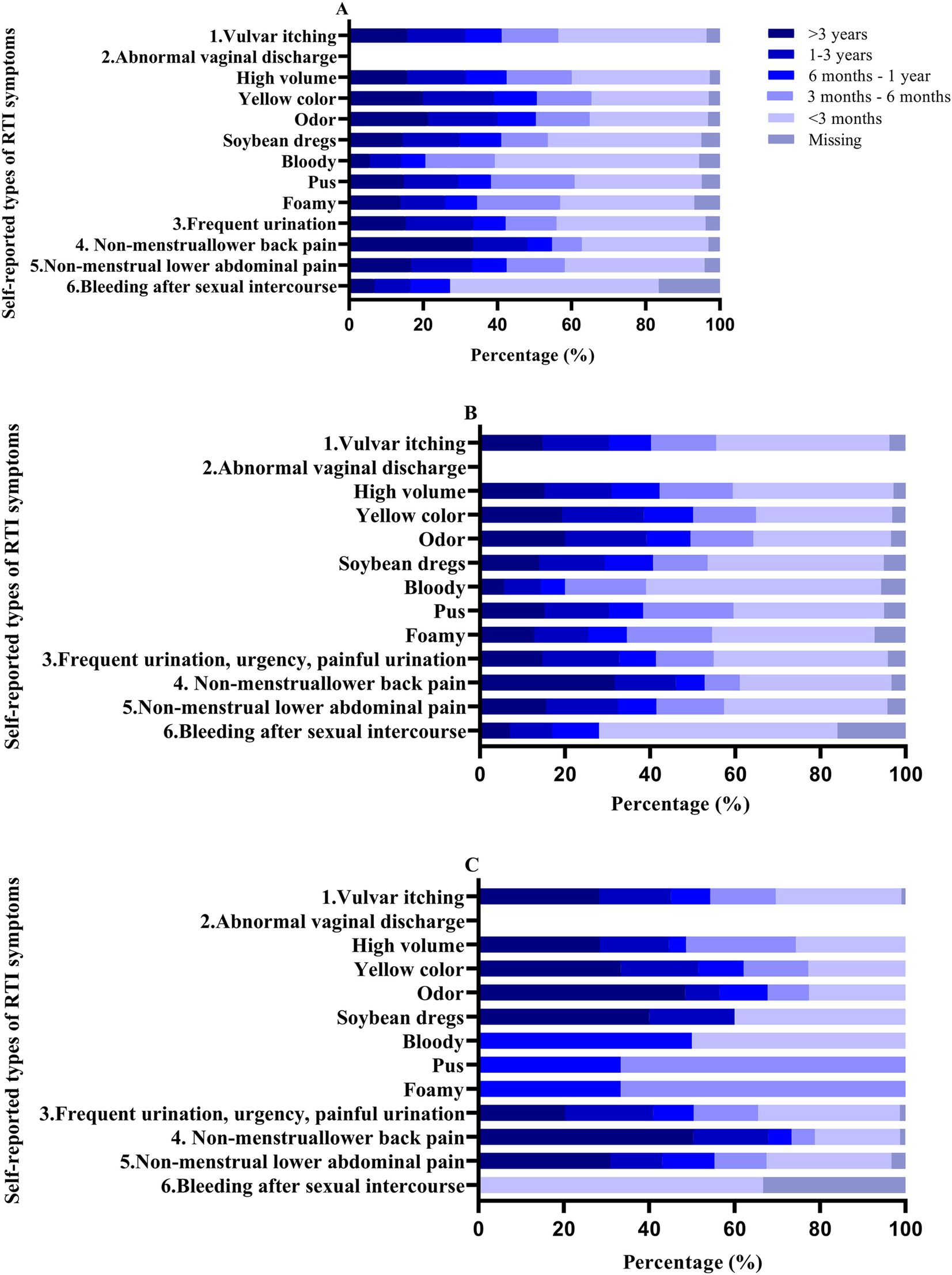
Figure 2. Percentage of duration of self-reported RTI symptoms in patients. A: 18–65 years; b: <60 years; c: ≥60 years.
According to the Jonckheere-Terpstra trend test, the duration of symptoms for vulvar itching, increased vaginal discharge, yellow-colored discharge, odor, discharge resembling soybean dregs, frequent urination, urgency, painful urination, and non-menstrual lower abdominal pain increased with age (p < 0.05; Supplementary Table S2).
3.4 Gynecological examination status of patients with self-reported RTI symptoms
Among the 8,657 women who self-reported RTI symptoms in the past 6 months, only 855 individuals (9.88%) underwent gynecological examinations in 2022. Notably, no women under the age of 20 chose to undergo gynecological examinations, only 2.43% of women aged ≥60 years chose to have a gynecological examination. According to the Cochran–Armitage trend test, the likelihood of undergoing gynecological examinations gradually decreased with increasing age (p < 0.0001; Table 2). Patients reported that the main reasons for undergoing gynecological examinations in the current year were routine check-ups (47.02%), the presence of symptoms (41.29%), and the availability of free medical check-up programs (9.82%; Table 3).

Table 2. Gynecological examination status of patients with self-reported RTI symptoms.
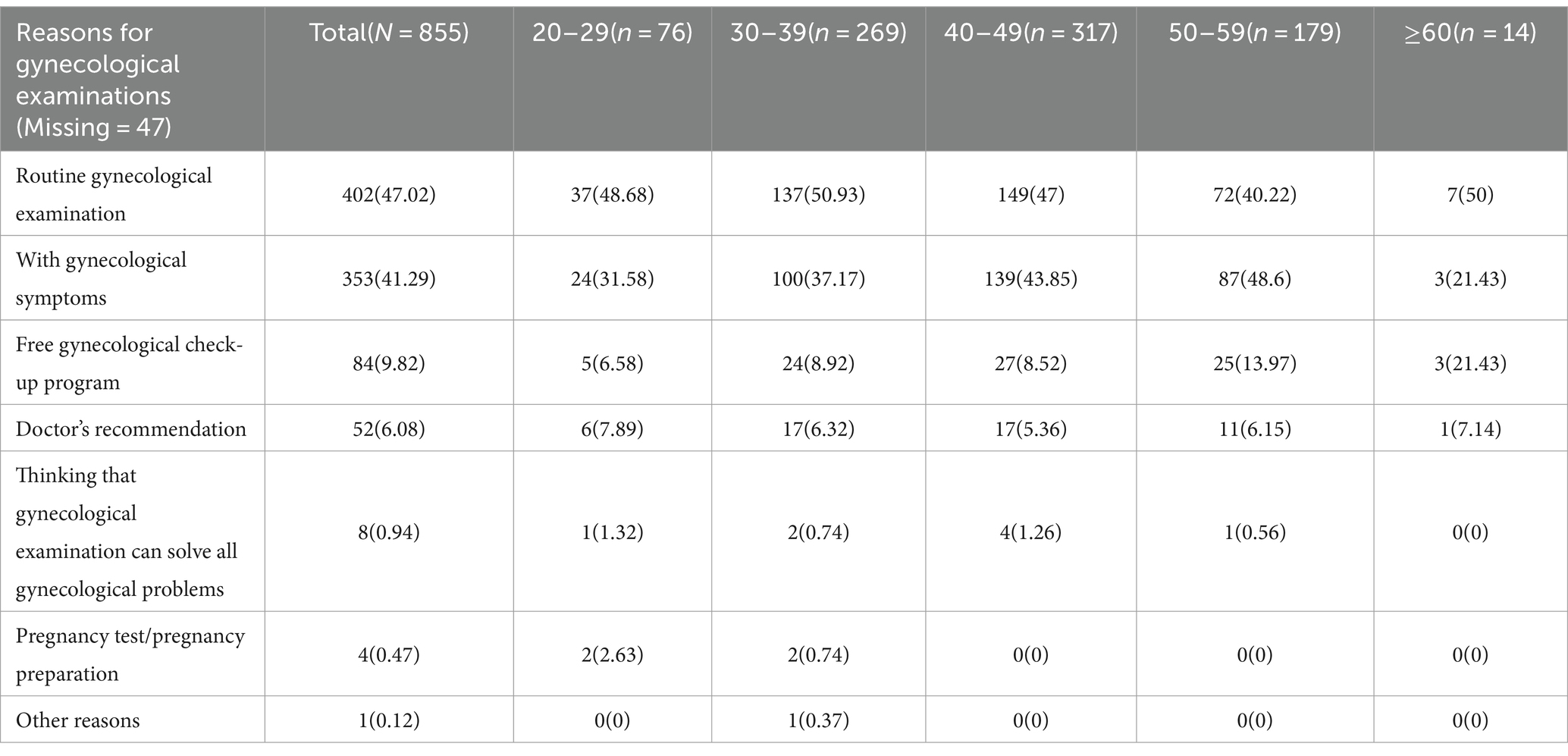
Table 3. Reasons for undergoing gynecological examinations among patients with self-reported RTI symptoms (multiple selections allowed).
Patients who did not undergo gynecological examinations in the current year provided various reasons, with the primary factors being the absence of severe symptoms (23.7%), perceived lack of necessity (4.41%), and time constraints (3.98%). Reasons for not undergoing examinations varied across different age groups. For those under 20 years old, the main reason was being young or unmarried (22.22%). Notably, a significant factor for not undergoing examinations in the 20–29 age group (5.79%), 40–49 age group (2.62%), and those aged 60 and above (6.24%) was a lack of awareness about the need for regular gynecological check-ups (Table 4).
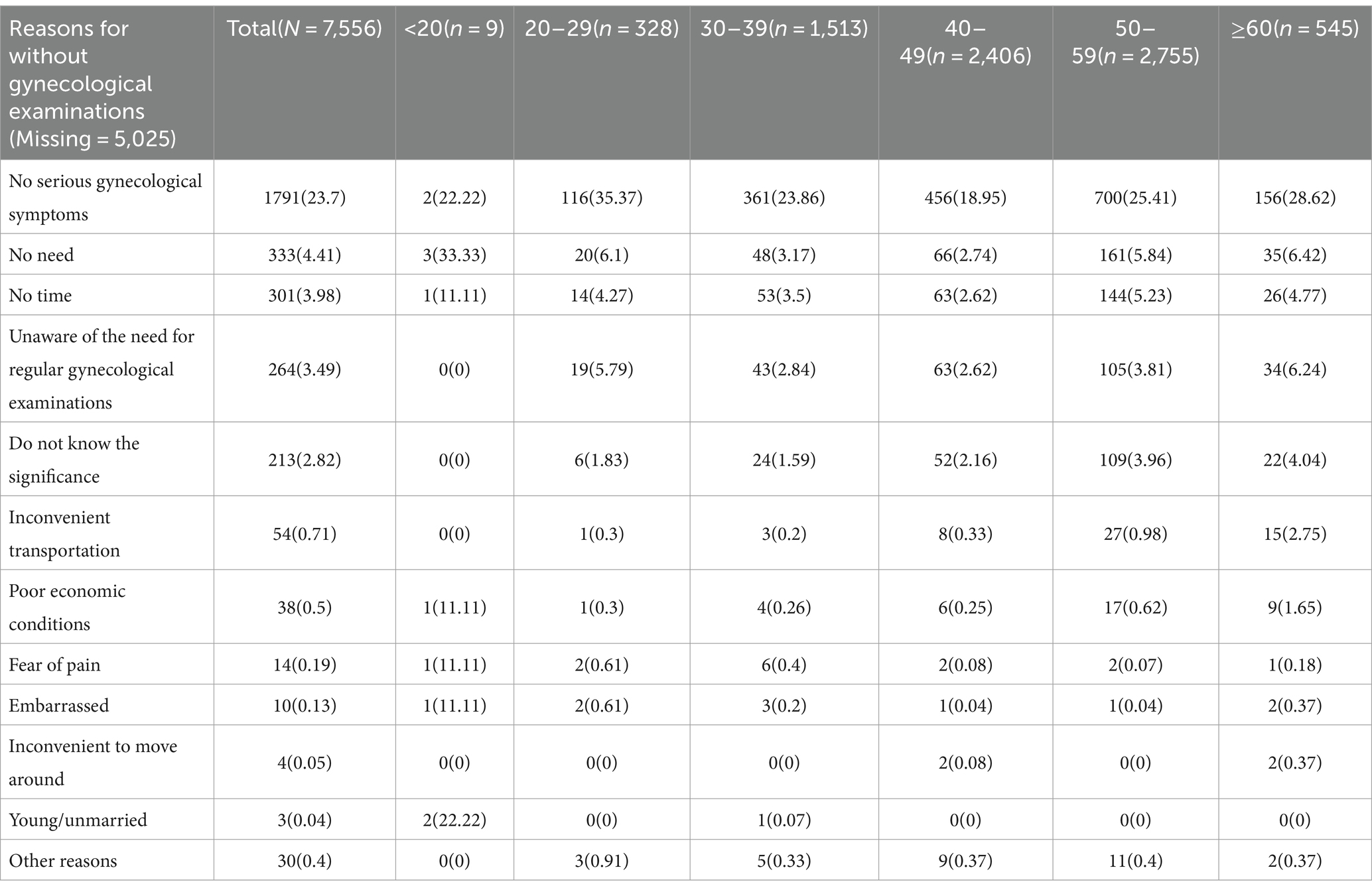
Table 4. Reasons for not undergoing gynecological examinations among patients with self-reported RTI symptoms (multiple selections allowed).
Out of the 855 symptomatic women who underwent gynecological examinations in 2022, a total of 347 individuals (40.58%) had a documented history of gynecological diagnoses. There were no significant differences in the distribution of gynecological diagnostic history across various age groups (Table 5). The top three diagnosed gynecological conditions were vaginitis (75.22%), cervical erosion (38.04%), and uterine fibroids (30.55%). There were differences in gynecological disorders in various age groups, the important gynecological disorders in 20–29, 30–39, 40–49, and 50–59 years of age were: pelvic inflammatory disease (17.24%), pelvic inflammatory disease (30.10%), cervical cysts (30.94%), and uterine polyps (30.00%), respectively (Table 6).

Table 5. Gynecological diagnostic history among patients with self-reported RTI symptoms.
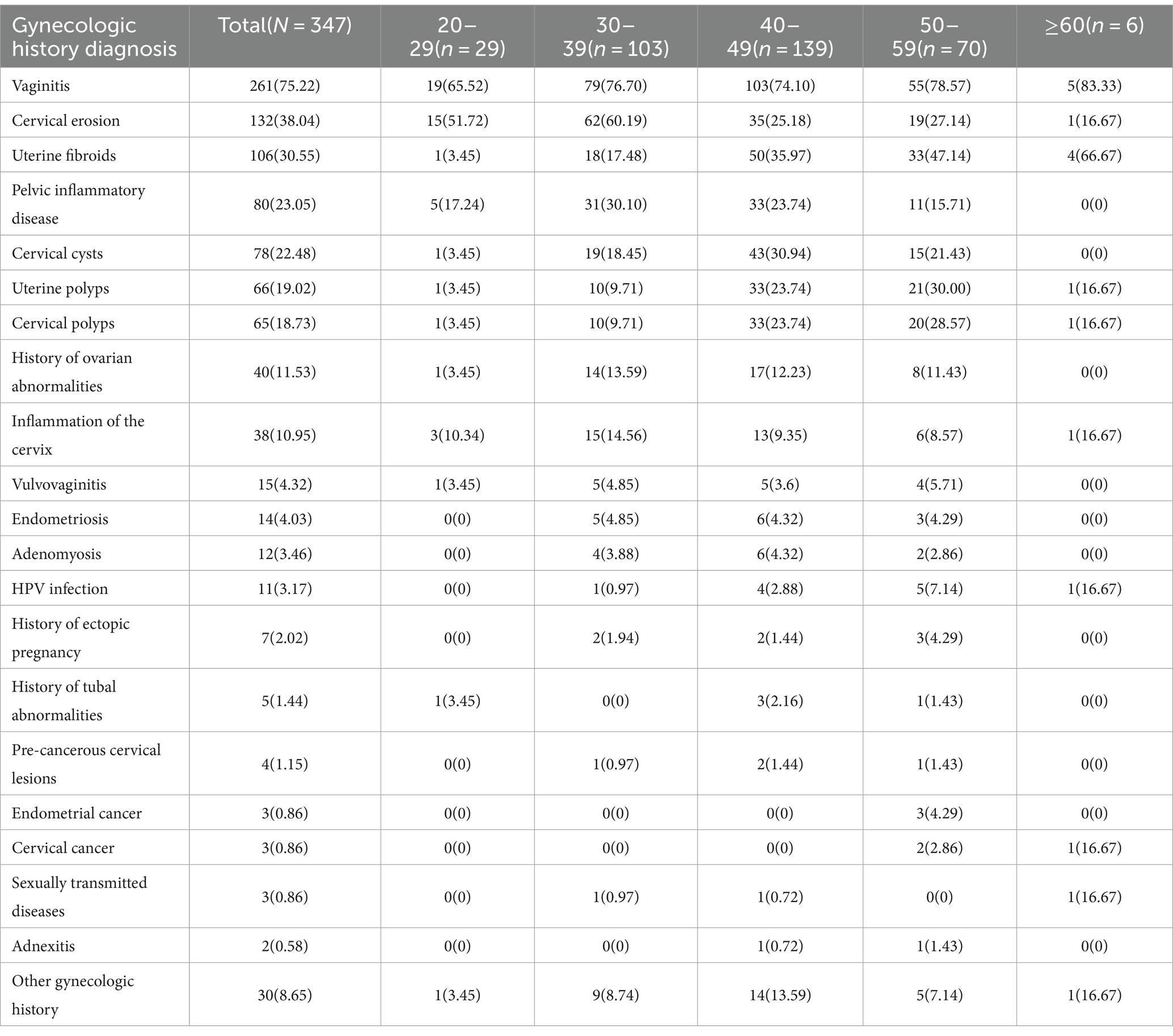
Table 6. Specific diagnoses of gynecological diseases.
3.5 Univariate logistic regression analysis
An exploration of factors influencing the reluctance of patients, reporting symptoms of RTI, to undergo gynecological examinations was conducted through univariate logistic regression analysis. In total, 38 variables were initially subjected to univariate analysis, and subsequently, 23 variables, exhibiting significance at p < 0.10, were selected for inclusion in the multivariate analysis (Supplementary Table S3).
3.6 Proportion and type of missing data
The missing data type was missing at random. Supplementary Figure S1 delineates the pattern and proportion of missing data for variables included in the multifactorial analysis. Specifically, variables such as household annual income (14.39%) and spouse circumcision history (12.01%) exhibited higher rates of missing data.
3.7 Multivariate logistic regression analysis
The multiple imputation for random missing data is detailed in Supplementary Table S4, and the results of the multivariate logistic regression analysis are presented in Table 7. For reference, the analysis without multiple imputation is available in Supplementary Table S5. Women with two or more symptoms, those with two or more marriages, and those with a history of miscarriage showed a lower likelihood of refraining from gynecological examinations after experiencing RTI symptoms. Conversely, factors such as rural residency, infrequent underwear changes (4–7 days per change), low bathing frequency in winter (>7 days/times), and a spouse aged 40 or older were associated with a higher likelihood of non-attendance for gynecological examinations. Moreover, the results from the multivariate logistic regression analysis without multiple imputation indicated that individuals with a BMI of 32 or higher and postmenopausal women were less likely to undergo gynecological examinations.
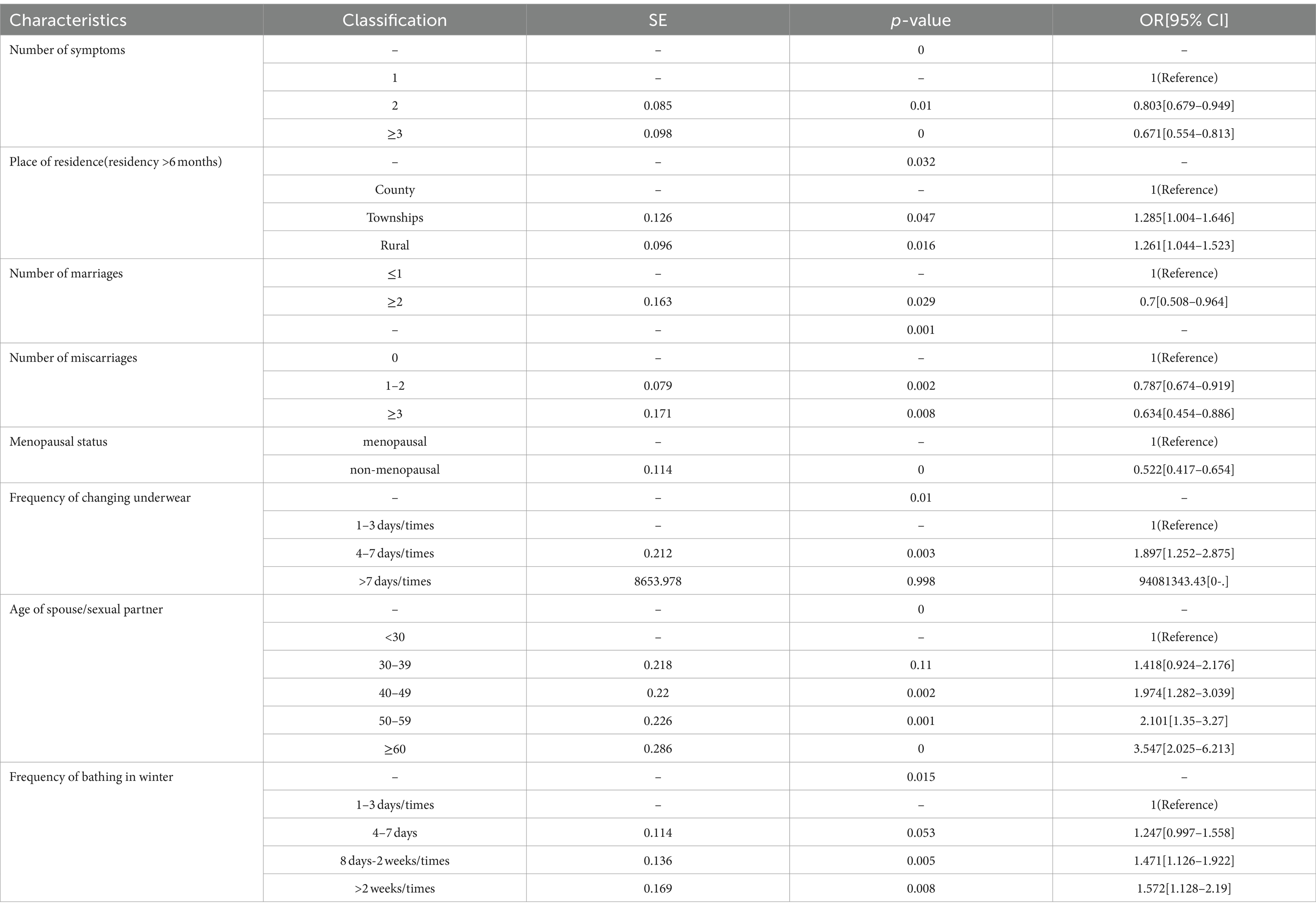
Table 7. Multivariate logistic regression analysis of patients with self-reported RTI symptoms who did not undergo gynecological exams.
4 Discussion
This study reveals the widespread prevalence of self-reported RTI symptoms among women. Women aged 60 and above experience a higher frequency and longer duration of RTI symptoms compared to those under 60. Only a small proportion of women opt for examination when symptomatic. We investigated their reasons for seeking or avoiding gynecological examinations, which are primarily associated with lower levels of awareness, education, economic status, inadequate promotion by healthcare institutions, and difficulties in accessing medical resources.
In this study, the prevalence of self-reported RTI symptoms in women aged 30 and above over the past 6 months exceeds 40%, closely aligning with the national level in India (40%) (15) and surpassing that of rural women in Sichuan Province, China (30.80%) (16) but falling below that of married women in rural Anhui Province, China (58.10%) (17). The most common RTI symptoms in the population are related to urinary tract infections, namely, external genital itching, abnormal vaginal discharge, and urinary irritation, mirroring results from other regions such as India (18, 19). Symptoms linked to cervical cancer, such as non-menstrual lower back pain, non-menstrual lower abdominal pain, and post-coital bleeding, are more prevalent in individuals over 40, emphasizing the need for attention (20). This study suggests that perimenopausal and older women have a higher burden of such symptoms. Women entering menopause and the menopausal period face risks of hormonal changes, gynecological malignancies, and various urogenital system diseases (21). We emphasize the necessity to extend healthcare focus beyond the reproductive period, ensuring perimenopausal and older adult women receive due attention (22, 23).
According to the American College of Obstetricians and Gynecologists (ACOG), all women over the age of 18 are recommended to have annual gynecological exams (24). Similar to other underdeveloped regions, despite the high prevalence of self-reported RTI symptoms among women, the proportion of those seeking gynecological examinations is low (25). Only 2.43% of women over 60 with more severe symptoms choose to undergo gynecological examinations. The primary reasons for older adult women not seeking such examinations are the perception of symptom severity, a lack of necessity, and unawareness of the need for regular gynecological check-ups. Similar reasons have been reported in other studies, where many perceive these symptoms as normal occurrences (26). The fundamental reasons may be attributed to lower levels of awareness and education, insufficient promotion by healthcare institutions, and difficulties in accessing medical resources (4). Conversely, women choosing gynecological examinations report routine check-ups, symptomatic concerns, and access to free medical check-up programs as their main reasons. This suggests that to increase the rate of gynecological examinations among women, efforts should focus on raising awareness and providing free gynecological check-up programs, as demonstrated by China’s initiation of the “two-cancer “free screening program for rural women in 2009, effectively reducing mortality from breast and cervical cancers (27).
In this study, the lower rate of gynecological examinations among symptomatic women with BMI ≥ 32, poor personal hygiene habits, menopausal status, and spouse age ≥ 40 may be attributed to lower levels of education, lower cognitive levels, and poorer health awareness. After we initially identify the reasons why women with RTI symptoms do not undergo gynecological examinations, we can subsequently implement health education measures for these patients to raise awareness, encourage regular gynecological examinations, and promote good hygiene habits. Women residing in rural and communal areas may face lower economic status and unequal distribution of medical resources. Consistent with the results of a review from India (25). Symptomatic women with two or more symptoms, married more than once, or with a history of abortion may be more likely to undergo gynecological examinations, possibly due to the severity of their symptoms. Studies have indicated that health services and delayed treatment are influenced by the severity of symptoms (28).
Among women who underwent gynecological examinations, 40.58% were diagnosed with gynecological diseases, including pelvic inflammatory disease, HPV infection, and cervical cancer, all confirmed to be related to RTIs (29, 30). This indicates that while self-reported symptoms may not be the gold standard for disease diagnosis, it remains a rapid, convenient, and cost-effective choice, aiding in the identification of patients requiring follow-up management, especially in resource-limited regions (5).
The strengths of this study include comprehensive coverage of a large population in Lueyang County using a census approach, which minimizes selection bias. This study also fills a gap in research on RTI symptoms in specific age groups and identifies reasons for delayed gynecological examinations and the actual needs of patients. It provides a scientific basis for improving gynecological health strategies for women in less developed regions. However, this study has limitations. High rates of missing data on household income and sexual behavior were addressed using multiple imputation, highlighting the need for more private and sensitive survey methods in future research. The cross-sectional design also limits the ability to establish causal relationships or track symptom changes over time. Future longitudinal studies are needed to better understand the temporal dynamics of RTI symptoms and their impact on women’s health.
5 Conclusion
The study found high self-reported RTI symptoms but limited gynecological examination rates among women in underdeveloped regions. There was a correlation between reported RTI symptoms and gynecological disorders. Targeted health education campaigns focusing on raising awareness of RTI symptoms and the importance of timely gynecological examination, especially for older women and those with lower levels of education, are necessary to improve healthcare utilization in less developed regions. At the same time, health-care providers should strengthen primary health-care infrastructure in rural areas by expanding free gynecological screening programs and increasing the number of trained gynecologists and other necessary medical resources.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by the Maternity Service Center of Lueyang Maternal and Child Health Hospital. The studies were conducted in accordance with the local legislation and institutional requirements. All participants or their legal guardians/next of kin provided written/electronic informed consent.
Author contributions
RZ: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Resources, Software, Validation, Visualization, Writing – original draft, Writing – review & editing. DK: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Resources, Software, Validation, Visualization, Writing – original draft, Writing – review & editing. SY: Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – review & editing. DH: Methodology, Project administration, Resources, Supervision, Validation, Visualization, Writing – review & editing. LB: Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Writing – review & editing. YA: Investigation, Methodology, Project administration, Software, Supervision, Validation, Writing – review & editing. JC: Investigation, Methodology, Project administration, Software, Supervision, Validation, Writing – review & editing. YN: Project administration, Resources, Supervision, Validation, Writing – review & editing. XZ: Project administration, Resources, Supervision, Validation, Writing – review & editing. WX: Conceptualization, Data curation, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Writing – review & editing. QS: Conceptualization, Data curation, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. This project was funded by the Chongqing social Science Planning Project (No. 2022BS081); China Postdoctoral Science Foundation Funded Project (No. 2022MD723732); Natural Science Foundation of Chongqing, China (No. 2023NSCQ-BHX0036); Supported by Foundation of State Key Laboratory of Ultrasound in Medicine and Engineering (No. 2021KFKT007).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2024.1401474/full#supplementary-material
SUPPLEMENTARY FIGURE S1 | Types and proportions of missing data for variables included in the multifactor analysis.
Abbreviations
RTI, Reproductive tract infection; HPV, Human papillomavirus.
References
1. Brunham, RC, and Paavonen, J. Reproductive system infections in women: lower genital tract syndromes. Pathog Dis. (2020) 78:ftaa022. doi: 10.1093/femspd/ftaa022
2. Baker, KK, Padhi, B, Torondel, B, das, P, Dutta, A, Sahoo, KC, et al. From menarche to menopause: a population-based assessment of water, sanitation, and hygiene risk factors for reproductive tract infection symptoms over life stages in rural girls and women in India. PLoS One. (2017) 12:e0188234. doi: 10.1371/journal.pone.0188234
3. Sawaya, GF, Sung, HY, Kearney, KA, Miller, M, Kinney, W, Hiatt, RA, et al. Advancing age and cervical cancer screening and prognosis. J Am Geriatr Soc. (2001) 49:1499–504. doi: 10.1046/j.1532-5415.2001.4911243.x
4. Walraven, G, Scherf, C, West, B, Ekpo, G, Paine, K, Coleman, R, et al. The burden of reproductive-organ disease in rural women in the Gambia, West Africa. Lancet (North American ed). (2001) 357:1161–7. doi: 10.1016/S0140-6736(00)04333-6
5. Jiang, Z, Wang, D, Hong, Q, Cherry, N, Cheng, J, Chai, J, et al. Use of health services by women with gynecological symptoms in rural China. World Health Popul. (2010) 11:23–37. doi: 10.12927/whp.2010.21723
6. Wang, Q, Kong, Y, Sun, J, Zhang, Y, Yuan, L, and Wang, J. What are the challenges faced by village doctors in provision of basic public health Services in Shandong, China? A qualitative study. Int J Environ Res Public Health. (2019) 16:2519. doi: 10.3390/ijerph16142519
7. Maitra, K, Degraft-Johnson, J, Singh, KK, and Tsui, AO. Prevalence of self-reported symptoms of reproductive tract infections AMONG recently pregnant women in UTTAR PRADESH, INDIA. J Biosoc Sci. (2001) 33:585–601. doi: 10.1017/S0021932001005855
8. Emery, JD, Shaw, K, Williams, B, Mazza, D, Fallon-Ferguson, J, Varlow, M, et al. The role of primary care in early detection and follow-up of cancer. Nat Rev Clin Oncol. (2014) 11:38–48. doi: 10.1038/nrclinonc.2013.212
9. Luo, ZZ, Li, W, Wu, QH, Zhang, L, Tian, LS, Liu, LL, et al. Population-based study of chlamydial and gonococcal infections among women in Shenzhen, China: implications for programme planning. PLoS One. (2018) 13:e0196516. doi: 10.1371/journal.pone.0196516
10. Harries, J, Scott, SE, Walter, FM, Mwaka, AD, and Moodley, J. Women’s appraisal, interpretation and help-seeking for possible symptoms of breast and cervical cancer in South Africa: a qualitative study. BMC Womens Health. (2020) 20:251. doi: 10.1186/s12905-020-01120-4
11. Yang, S, Bai, L, Xu, W, Zhang, R, Hu, D, Nie, Y, et al. Profiling the real-world management status of high-risk human papillomavirus infection: a protocol to establish a prospective cohort of high-risk human papillomavirus-infected women in Lueyang County, China. BMJ Open. (2022) 12:e062678. doi: 10.1136/bmjopen-2022-062678
12. Huang, DR, Goodship, A, Webber, I, Alaa, A, Sasco, ER, Hayhoe, B, et al. Experience and severity of menopause symptoms and effects on health-seeking behaviours: a cross-sectional online survey of community dwelling adults in the United Kingdom. BMC Womens Health. (2023) 23:373. doi: 10.1186/s12905-023-02506-w
13. Sabarwal, S, and Santhya, KG. Treatment-seeking for symptoms of reproductive tract infections among young women in India. Int Perspect Sex Reprod Health. (2012) 38:090–8. doi: 10.1363/3809012
14. Xia, DY, Liao, SS, He, QY, Choi, KH, and Mandel, JS. Self-reported symptoms of reproductive tract infections among rural women in Hainan, China: prevalence rates and risk factors. Sex Transm Dis. (2004) 31:643–9. doi: 10.1097/01.olq.0000143111.33741.40
15. GOI, MOHFW . National guidelines on prevention, management and control of rtis/stis. (2007). Available from: https://www.nhm.gov.in/index1.php?lang=1&level=2&sublinkid=1085&lid=148 (Acccessed on 2023, Dec 30)
16. Yongjun, T, Samuelson, J, Qingsheng, D, Ali, MM, Li, X, Yanjian, M, et al. The prevalence of sexually transmitted and other lower reproductive tract infections among rural women in Sichuan Province, China. Southeast Asian J Trop Med Public Health. (2009) 40:1038–47. Available from: https://pubmed.ncbi.nlm.nih.gov/19842387
17. Zhang, XJ, Shen, Q, Wang, GY, Yu, YL, Sun, YH, Yu, GB, et al. Risk factors for reproductive tract infections among married women in rural areas of Anhui Province, China. Eur J Obstet Gynecol Reprod Biol. (2009) 147:187–91. doi: 10.1016/j.ejogrb.2009.08.017
18. Nandan, D, Misra, S, Sharma, A, and Jain, M. Estimation of prevalence of RTIs/STDs among women of reproductive age group in district Agra. Indian. J Community Med. (2002) 27:37. Available from: https://journals.lww.com/ijcm/abstract/2002/27030/ESTIMATION_OF_PREVALENCE_OF_RTIs_STDs_AMONG_WOMEN.3.aspx
19. D B, N S . Prevalence of RTI/STI among reproductive age women (15-49 YEARS) in urban slums of Tirupati town, Andhra Pradesh. (2007). Available from: https://www.researchgate.net/publication/268372114_Prevalence_of_RTISTI_among_reproductive_age_women_15-49_YEARS_in_urban_slums_of_Tirupati_Town_Andhra_Pradesh (Accessed on 2023 Dec 30)
20. Mwaka, AD, Orach, CG, Were, EM, Lyratzopoulos, G, Wabinga, H, and Roland, M. Awareness of cervical cancer risk factors and symptoms: cross-sectional community survey in post-conflict northern Uganda. Health Expect. (2016) 19:854–67. doi: 10.1111/hex.12382
21. Pradhan, MR, Mondal, S, and Mudi, PK. Gynecological morbidity and treatment-seeking among older adult (aged 45-59) women in India. Reprod Health. (2023) 20:64. doi: 10.1186/s12978-023-01611-1
22. Whiteley, J, DiBonaventura, M dC, Wagner, JS, Alvir, J, and Shah, S. The impact of menopausal symptoms on quality of life, productivity, and economic outcomes. Womens Health Rep (New Rochelle). (2013) 22:983–90. doi: 10.1089/jwh.2012.3719
23. Woods, NF, and Mitchell, ES. Symptoms during the perimenopause: prevalence, severity, trajectory, and significance in women’s lives. Am J Med. (2005) 118:14–24. doi: 10.1016/j.amjmed.2005.09.031
24. Cansino, C, and Chohan, L. The utility of and indications for routine pelvic examination. Available from: https://www.acog.org/clinical/clinical-guidance/committee-opinion/articles/2018/10/the-utility-of-and-indications-for-routine-pelvic-examination
25. Nagarkar, A, and Mhaskar, P. A systematic review on the prevalence and utilization of health care services for reproductive tract infections/sexually transmitted infections: evidence from India. Indian J Sex Transm Dis AIDS. (2015) 36:18–25. doi: 10.4103/0253-7184.156690
26. Rizwan, S, Rath, RS, Vivek, G, Nitika, AG, Anant, G, Farhad, A, et al. KAP study on sexually transmitted infections/reproductive tract infections (STIs/RTIs) among married women in rural Haryana. Dermatol Online J. (2015) 6:9–12. doi: 10.4103/2229-5178.148919
27. Sun, Y, Ma, Y, Cao, M, Hu, Z, Lin, W, Chen, M, et al. Breast and cervical cancer screening adherence in Jiangsu, China: an ecological perspective. Front Public Health. (2022) 10:967495. doi: 10.3389/fpubh.2022.967495
28. Aroian, KJ, and Vander Wal, JS. Health service use in Russian immigrant and nonimmigrant older persons. Fam Community Health. (2007) 30:213–23. doi: 10.1097/01.FCH.0000277764.77655.b7
29. Hillier, SL, Nugent, RP, Eschenbach, DA, Krohn, MA, Gibbs, RS, Martin, DH, et al. Association between bacterial vaginosis and preterm delivery of a low-birth-weight infant. N Engl J Med. (1995) 333:1737–42. doi: 10.1056/NEJM199512283332604
Keywords: reproductive tract infection (RTI), self-reported symptoms, gynecological examinations, women’s health, underdeveloped regions
Citation: Zhang R, Kang D, Yang S, Hu D, Bai L, Ao Y, Chen J, Nie Y, Zhao X, Xu W and Shi Q (2024) Women’s self-reported symptoms of reproductive tract infection, medical consultations, and factors influencing them in less developed regions: perimenopausal and older women in need of urgent attention. Front. Public Health. 12:1401474. doi: 10.3389/fpubh.2024.1401474
Edited by:
Kevin P. Mollen, University of Pittsburgh, United StatesReviewed by:
Kshitij Karki, Purbanchal University, NepalNaseem Akhtar Qureshi, Al-Falah University, India
Copyright © 2024 Zhang, Kang, Yang, Hu, Bai, Ao, Chen, Nie, Zhao, Xu and Shi. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Qiuling Shi, cXNoaUBjcW11LmVkdS5jbg==; Wei Xu, eHV3ZWl3ZWlAY3FtdS5lZHUuY24=
‡ORCID: Wei Xu, https://orcid.org/0000-0002-7769-9601
Qiuling Shi, https://orcid.org/0000-0003-0660-3809
Ruoyi Zhang, https://orcid.org/0000-0002-9237-0070
Dan Kang, https://orcid.org/0009-0001-8254-3417
†These authors have contributed equally to this work and share first authorship