 Cristina Barboza-Solis
Cristina Barboza-Solis Rolando Herrero2
Rolando Herrero2- 1Facultad de Odontología, Universidad de Costa Rica, San José, Costa Rica
- 2Agencia Costarricense de Investigaciones Biomédicas, Fundación INCIENSA, San José, Costa Rica
Objective: This study systematically reviews evidence of socioeconomic health disparities in Costa Rica, a middle-income country, to elucidate the relationship between socioeconomic status and health outcomes.
Methods: Published studies were identified through a systematic review of PubMed (English) and Scielo (Spanish) databases from December 2023 to January 2024, following PRISMA guidelines. Search terms included socioeconomic status, social determinants, social gradient in health, and health inequalities.
Results: Of 236 identified references, 55 met the inclusion criteria. Findings were categorized into health inequalities in mortality (among the general population, infants, and older adults), life expectancy, cause-specific mortality, and health determinants or risk factors mediating the association between the social environment and health. The studies indicate higher mortality among the most disadvantaged groups, including deaths from respiratory diseases, violence, and infections. Higher socioeconomic status was associated with lower mortality rates in the 1990s, indicating a positive social gradient in health (RII = 1.3, CI [1.1–1.5]). Disparities were less pronounced among older adults. Urban areas exhibited concentrated wealth and increased risky behaviors, while rural areas, despite greater socioeconomic deprivation, showed a lower prevalence of risky behaviors. Regarding smoking, people living in rural areas smoked significantly less than those in urban areas (7% vs. 10%). Despite the relatively equitable distribution of public primary healthcare, disparities persisted in the timely diagnosis and treatment of chronic diseases. Cancer survival rates post-diagnosis were positively correlated with the wealth of districts (1.23 [1.12–1.35] for all cancers combined).
Conclusion: The study highlights the existence of social health inequalities in Costa Rica. However, despite being one of the most unequal OECD countries, Costa Rica shows relatively modest social gradients in health compared to other middle and high-income nations. This phenomenon can be attributed to distinctive social patterns in health behaviors and the equalizing influence of the universal healthcare system.
1 Introduction
Health is shaped over the life course and is determined by the circumstances in which people are born, grow, live, work, and age (1). According to the World Health Organization, these conditions are molded by political, social, and economic forces (1). The distribution of health determinants between socioeconomic groups creates a socioeconomic gradient in health in the majority of countries (2). Individuals at the bottom of the social hierarchy are more likely to experience unhealthy lives compared to those in the middle, who, in turn, have worse health than those at the top (3). Recognized as systematic, socially produced, modifiable, and unfair (4), the social gradient in health affects a broad range of health indicators, from risk factors to health outcomes (5). The association between measures of socioeconomic status (SES) and diverse health outcomes is a consistent finding in epidemiologic research (6), and continues to be a challenge for both high-income (7) and low- and middle-income countries (LMICs) (8).
Despite recent advances in highlighting social determinants of health (9), research in LMICs remains underrepresented (10). In the case of Latin America and the Caribbean (LAC), shows that lower socioeconomic status (SES) is associated with higher mortality, although research on this topic remains relatively sparse (11, 12). LAC remains one of the most inequitable regions globally, with significant poverty (13), a dual burden of infectious and non-communicable diseases, rapid aging, migration influxes, and weak public health structures for epidemiologic surveillance (8, 14).
For a middle-income country, it is imperative to tackle health inequalities for cost-effective healthcare. These inequalities often result in increased healthcare budgets, a higher proportion of out-of-pocket health expenditures, and increased disability and disease burden, ultimately leading to preventable and premature mortality (15). By reducing socioeconomic disparities in health, our societies move closer to achieving social equity and justice, ensuring a better quality of life and striving for the principle of “leaving no one behind” (16).
Costa Rica, an upper-middle-income country in Central America, has been an OECD member since 2022. With a population of 5 million, mostly urban and concentrated around the capital, 72% live in urban areas and 62% in the metropolitan region (17, 18). In 2022, Costa Rica’s GDP per capita was $13,400, compared to the OECD average of $43,500 (19). The country has significant socioeconomic inequalities, with a Gini Index of 0.472, the second highest among OECD countries, surpassed only by Colombia (20). The wealthiest 10% of households receive 32% of net income, while the poorest 10% receive only 1.5% (17). There are also important differences between urban and rural areas. Urban areas have a 68% higher net income per capita compared to rural areas (21). Costa Rica is structured into three main geographical levels: provinces (7), cantons (81), and districts (489).
Despite the well-established relationship indicating that high GDP per capita lead to high life expectancy, Costa Ricans can expect to live up to 81 years (22), quite similar to high-income countries with higher GDPs (23). The country’s good vital statistics can be partially attributed to the national healthcare insurance system, which is constitutionally universal, mandatory, and based on citizen solidarity. Administered by the Caja Costarricense del Seguro Social (CCSS) since 1941, it covers an estimated 90% of the population (24). Funded by employees, employers, and the government, the CCSS established primary healthcare facilities (Equipos Básicos de Atención Integral en Salud—EBAIS) in the 1990s to decentralize healthcare to cover rural and underserved populations (25). Costa Rica has over 1,000 EBAIS, distributed throughout the national territory, each serving about 4,500 individuals with a team that includes a physician, nursing assistant, and primary care technical assistant. These teams are supported by shared staff, including social workers, nurses, nutritionists, pharmacists, microbiologists, and medical records technicians (26). The CCSS also manages 29 hospitals: 3 national (located in the metropolitan area), 6 specialized, 8 regional, and 12 peripheral (27). However, the country has only 1.2 hospital beds per 1,000 inhabitants, compared to the OECD average of 4.3 (28). Unlike many healthcare systems, there are no out-of-pocket expenses in the CCSS, ensuring that medical care and medications are provided free of charge within the public system. Nonetheless, some healthcare services are inadequately covered, leading to reliance on private providers. As a result, about 21% of healthcare expenditures in Costa Rica are out-of-pocket, similar to the OECD average of 18% (28).
The present study is based on the social epidemiology perspective that explicitly investigates the social determinants of population distributions of health, disease, and wellbeing, considering that health inequalities are a biological expression of social inequality (29). We based our search according to the conceptual framework of the WHO Commission on the Social Determinants of Health (30) that defines the social determinants of health as the “conditions in which people are born, grow, work, live, and age, and the wider set of forces and systems shaping the conditions of daily life. These forces and systems include economic policies and systems, development agendas, social norms, social policies, and political systems” (1).
Research on health inequalities in Costa Rica remains limited, lacking a comprehensive analysis of existing studies. The evolving political and economic circumstances, increasing urbanization, rapid population aging, and shifts towards more Westernized lifestyles underscore the need to report and monitor these disparities, as these circumstances can increase social inequality and thus become health inequalities. This is central to develop better-adapted policies and improving preventive health services.
In the present study, we assess health inequalities in Costa Rica, by reviewing existent literature on health disparities arising from social determinants, evaluating the impact of “equity stratifiers” on health status (31), such as, educational level, urbanicity, income, wealth and other social determinants of health, such as, access to healthcare and health behaviors. This systematic review seeks to provide a comprehensive understanding of the state of health inequalities research and contribute to the broader discourse on the role of social determinants of health in the country. Here, the terms “graded relationship” or “social gradient” refer to the observed phenomenon wherein individuals situated at lower socioeconomic strata experience poorer health outcomes compared to those at higher socioeconomic levels. A reverse social gradient occurs when individuals in lower socioeconomic strata experience better health outcomes compared to those in higher socioeconomic levels.
2 Methods
2.1 Search strategy
Articles assessing social inequalities in health in Costa Rica were retrieved. Published studies were identified by a systematic review in the PubMed electronic database, to identify English articles, and the Scielo electronic database for Spanish articles. PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) was followed. Flow chart for selection of articles is shown in Figure 1. Based on the PICO model, our approach involves: population (Costa Rican inhabitants), Intervention (considering social determinants as exposures), comparison (different socioeconomic subgroups), outcome (health inequalities in mortality, life expectancy, and morbidity). The PICO methodology was employed to select the main groups of search terms. For participants and location, we focused on observational studies conducted among Costa Rican inhabitants. For exposure, we included social determinants and socioeconomic status. For the outcome, we targeted health inequalities, such as inequality, inequity, disparity, and social gradient.
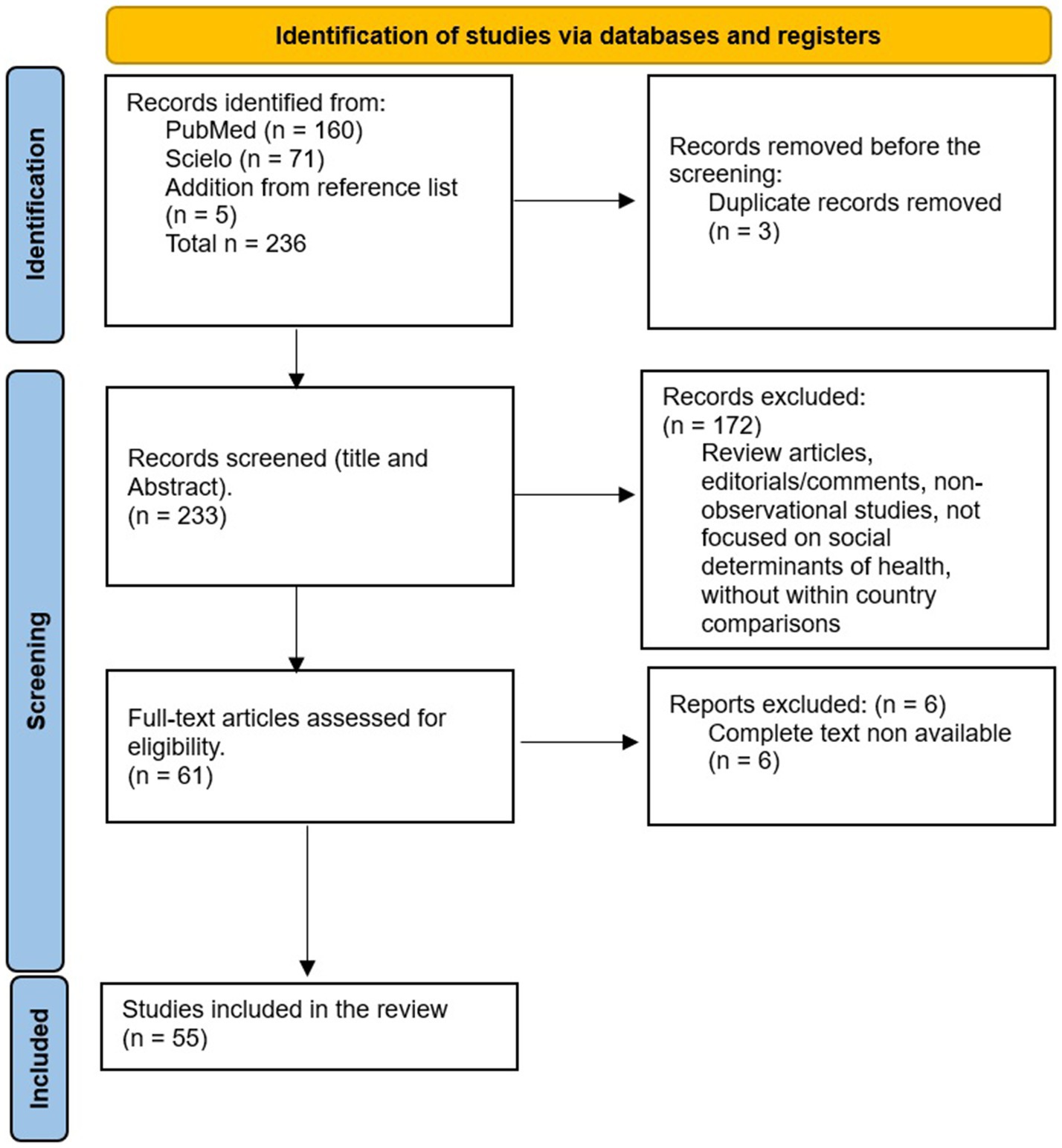
Figure 1. PRISMA flow diagram of the study. From: Mother et al. (32).
Article search was performed from December 2023 to January 2024 in PubMed and Scielo electronic databases. No publication date restrictions were imposed. Articles in English and Spanish were considered. One author (CBS) performed the electronic search in both databases and examined the titles and abstracts identified in the databases search, removed articles that did not meet the inclusion criteria and selected the eligible ones for full-text review. Additional articles (n = 5) were incorporated into the main reference lists that were not initially captured by the electronic search but were deemed relevant. Among these additions was a health agency report on drug consumption. However, we did not find other items of grey literature to include.
The following algorithm built with MeSH terms was used for the PubMed search: (“Costa Rica”[Title/Abstract]) AND ((“social determinant*”[Title/Abstract]) OR (“socioeconomic status”[Title/Abstract]) OR (“social gradient”[Title/Abstract]) OR (inequalit*[Title/Abstract]) OR (disparit*[Title/Abstract]) OR (inequit*[Title/Abstract])). For Scielo, the following algorithm was used: ((ab:(“Costa Rica”)) OR (ti:(“Costa Rica”))) AND ((ab:(“inequidades”)) OR (ti:(“inequidades”)) OR (ab:(“inequidad”)) OR (ti:(“inequidad”)) OR (ab:(“desigualdad”)) OR (ti:(“desigualdad”)) OR (ab:(“disparidad”)) OR (ti:(“disparidad”)) OR (ab:(“disparidades”)) OR (ti:(“disparidades”)) OR (ab:(“desigualdades”)) OR (ti:(“desigualdades”))).
2.2 Selection strategy
The eligibility criteria encompassed observational studies (including cross-sectional, case–control, and cohort studies) as well as ecological studies that reported on health inequalities in mortality, morbidity, health behaviors, risk factors, or those investigating the role of social determinants of health. These studies were required to be conducted in Costa Rica and to include within-country comparisons, with no limitation on publication date or language. Additionally, studies were expected to employ random sampling methods and be representative of at least one locality, city, or region within Costa Rica.
The exclusion criteria were the following: systematic reviews, literature reviews, commentaries, editorials. Studies whose objectives were not related to health outcomes were removed, as well as those articles that only made cross-country comparisons.
2.3 Data extraction
The article selection process involved two main steps. Initially, information on titles and abstracts from the entire set of results obtained from PubMed and Scielo electronic platforms was extracted and processed using a CSV format. Titles and abstracts of all references identified in the search were screened applying exclusion and inclusion criteria. Following this, the preselected articles underwent full-length article readings to identify and exclude any additional articles that did not meet the inclusion criteria.
For the studies finally selected, the following data were extracted: title, last name of first author, study objective, study design (including the cohort or study name), study period, sample size, characteristics of participants (including study period), social determinant used (exposure), health outcome(s) (outcome) and main results.
3 Results
This study is divided in four sections. The first section will lay out the main tenets of health inequalities in overall mortality (in general population, infants and older adults) and life expectancy, the second section will focus on cause-specific mortality. The third section will discuss the main determinants of health inequalities identified or risk factors that can mediate the link between the social environment and health. Finally, the findings and remaining challenges will be discussed.
The initial search strategy identified 232 articles (160 from PubMed and 71 from Scielo), and 5 papers were retrieved from reference lists that were not found in the search. The article selection process and flow chart are presented in Figure 1. Among these, three articles were found to be duplicated. After Title/Abstract screening, 172 articles were rejected for reasons such as only running cross-country comparisons, using Costa Rica only as an example for Latin America, being non-original studies (editorials, commentaries), or not analyzing associations between social determinants and health. Additionally, six articles were excluded due to the unavailability of the complete text. Finally, 55 articles were comprehensively evaluated.
3.1 General characteristics of the studies
General characteristics of the articles included in this systematic review are presented in Table 1. From the 55 articles 31 were cross-sectional, 20 longitudinal, 3 case–control and 1 qualitative study. Studies were conducted between 1984 and 2023 across various population groups. These groups include the general population (ages 20 to 89 years), infants (under 5 years), and older adults (60 years and above) (see Table 1) (33). Sixteen studies used ecological approaches, at the level of the province (7 provinces), county (~ 80 depending on the year in which the study was developed) or district (~ 478). Ecological studies extracted census data from 1984, 2000, 2011 (34), approached SES via household income and wealth (using material deprivation counting assets and characteristics of homes) and urbanicity (territories characterized as rural, mixed or urban). Studies using SES individual measures, collected data on income, education level (primary, secondary and more), occupation or subjective economic situation. They used cross-sectional data of specific projects: SALUBRAL, Global Adults Tobacco Survey, National School Weight/Height Census, Maternal and child National surveys (see Table 1) or were based on the Costa Rican Longevity and Healthy Aging Study (CRELES), including a representative sample of people born between 1945–1955, and a second cohort including people born before 1945 of about 8,000 adults (35).

Table 1. General characteristics of the studies included in the systematic review.
To assess health outcomes, the authors of the studies included in this review utilized the Costa Rican registries, including birth, mortality, and cancer registries, which have been described as comprehensive (36). The cancer registry is considered 100% complete, which is an exceptional country effort (37). Using data from the national cancer registry, several studies characterized the social distributions in cancer incidence, mortality and survival. A Longitudinal Mortality Study of Costa Rican Adults (NLMS) 1984–2007 merged data from the Death Index Registry and the 1984 Census, following more than 16,000 people aged more than 30 years between January 1, 1989 and December 31, 2007, and observed more than 3,700 deaths. Studies also included outcomes from specific studies (e.g., anthropometric measures, cardiovascular health, Diabetes, maternal and child health, self-rated health), collected by cross-sectional studies or from the CRELES cohort. A literature review article (not included in this analysis) presented the main methodologies used to analyze health inequalities in Costa Rica (38).
3.2 Health inequalities in mortality and life-expectancy
3.2.1 In general population
The most extensive study examining mortality inequalities through individual socioeconomic data was conducted by Rosero-Bixby and Dow (39), utilizing data from the Costa Rican Longevity and Healthy Aging Study (CRELES) and the National Longitudinal Mortality Study (NLMS). Their findings revealed a higher mortality rate among individuals in the lowest (SES) ranks compared to those in the highest SES, consistent with results reported by Modrek et al. (40), who used only NLMS data. Rosero-Bixby and Dow (39) found that higher SES was associated with lower mortality rates in the 1990s, indicating a positive social gradient in health (RII = 1.3, CI [1.1–1.5]). The authors observed that mortality decreased with increasing education and wealth. Rural residents exhibit lower mortality rates than their urban counterparts after adjusting for wealth and education. Stratification by age groups revealed social gradients among men and women aged 40–64 years (Relative Inequality Index (RII), RII = 1.3 in men, RII = 1.7 in women), as well as among women aged 65–89 years (RII = 1.5) (39), but no significant gradient was observed among men in the 65–89 age group (RII = 0.8, non-significant). Interestingly, these social gradients were notably less pronounced than those observed in the United States (RII = 3.5 in men, RII = 3.8 in women).
These results are consistent with a recent study conducted by Fantin et al., which followed all citizens alive in 2010 (24-million person-years follow-up) between 2010 and 2018 (41). The study utilized the district level as the smallest administrative unit to assess SES of each individual. Among both men and women residing in urban areas, those living in the wealthiest districts exhibited a life expectancy more than 2 years higher than those in the poorest districts. Similar trends, but with less pronounced disparities, were observed in rural areas. However, among men, the protective effect of residing in rural areas resulted in comparable mortality rates between the poorest districts (predominantly rural) and the wealthiest districts (mainly urban).
In studies using larger geographical units, such as the canton level, associations between area-level SES and life expectancy become less apparent. For instance, Bilal et al. (12) described geographical disparities but did not find a significant link between ecological socioeconomic level and life expectancy. Similarly, Fantin et al. (42) found relatively similar life expectancies among women when using the province at birth level. However, among men, there was a notable difference in life expectancy, with those born in Limón experiencing over 2 years of lower life expectancy compared to those born in almost all other provinces. The homicide rate and mortality from traffic accidents in Limón partially explain the findings; however, the association continues to be significant after adjustment.
3.2.2 Specific population: infants
In 2021, Costa Rica exhibited low infant and under-5 mortality rates, standing at 6 and 8 per 1,000 live births, respectively (43). Consequently, there are few recent studies, especially on social inequalities. Chamizo-García and Behm-Ammazzini (44) suggested that infant mortality between 2008 and 2012 was slightly higher in the poorest cantons, particularly those located in the southern region of the capital, border areas, or coastal regions. These findings align with previous results from the 1960s and 1980s, during which infant and under-5 mortality rates were significantly higher (45, 46). In 1991, Rosero-Bixby proposed that from 1965 to 1979, infant mortality was closely linked to maternal education level, whereas between 1981 and 1984, the association between infant mortality and maternal education level became less clear (46). Metzger (47) confirmed these results, showing a strong social gradient in 1973, that disappeared in 1984.
3.2.3 Specific population: older adults
In both 2009 and 2016, Rosero-Bixby and Dow observed no social gradient in mortality within the CRELES cohort. Interestingly, they even noted a small reverse gradient among men, employing education level as a SES measure (48). In a separate study, Rosero-Bixby reaffirmed his previous findings, indicating comparable life expectancy at age 60 across different wealth levels (49). Using the education level as proxy of SES, the study showed a small social gradient in women, and a clear reverse social gradient in men. Finally, in men only, life expectancy was higher in rural area compared to urban area. Focusing on a 2,700-participants subsets of the CRELES cohort aged 65 years and above, Sudharsanan et al. (50) found no evidence of a social gradient in mortality according to education level but the follow-up and the sample size were lower compared to Rosero-Bixby’s analysis.
Two additional studies using data other than CRELES, analyzed mortality in older adults. Following a cohort of 876 individuals aged 60 and over between 1984 and 2001, residents of a semi-urban community near the capital (Coronado canton), Rosero-Bixby showed a protective role of education, but no effect of wealth on mortality (51). Finally, Fantin et al. observed that among individuals aged 60 years and older, there was an association between district wealth and mortality in both men and women, evident only in urban areas and not in rural areas. These findings do not necessarily conflict with those of CRELES, as the latter study did not stratify its results by urbanicity. Moreover, Fantin et al. noted that socioeconomic inequalities based on district wealth were less pronounced among individuals aged 60 years and older compared to those aged 20 years and older (41). Consequently, among men aged 60 years and older, life expectancy was 0.7 years higher in the poorest cantons of rural areas compared to the wealthiest cantons of urban areas.
3.3 Health inequalities in mortality, by cause of death
3.3.1 Diseases of the circulatory system
Between 2013 and 2022, diseases of the circulatory system represented 28% of the deaths in women and 25% in men in Costa Rica (52). Various studies converged to show a social gradient in circulatory system mortality. In the 1990s, Rosero-Bixby and Dow (39) identified a social gradient in mortality associated with cerebrovascular disease (RII = 1.5), but not in mortality associated with heart disease (39). Using the NLMS data, Modrek (40) showed lower mortality rates for cardiovascular disease among high-educated individuals, a finding consistent with the results reported by Fantin et al. (41) based on mortality data observed between 2010 and 2018. Indeed, Fantin et al. identified a slightly lower mortality rate in the wealthiest districts compared to the rest of the country, although this finding emerged only after adjusting for urbanicity. Consistently, in a case–control study, people who had a myocardial infarction were found to have, on average, a lower SES compared to people who did not have myocardial infarction (53).
3.3.2 Cancer incidence and mortality
Between 2013 and 2022, cancers represented 24% of the deaths in women and 21% in men in Costa Rica (52). Stomach, colorectum, prostate, breast, and lung, represent half of the all-cancer mortality. In the 1990s, Rosero-Bixby and Dow (39) did not show a social gradient in cancer mortality. Fantin et al. (54) confirmed the absence of social gradient in cancer mortality, but observed a lower mortality in rural areas compared to urban areas, consistent with a previous study (55).
Fantin et al. (56) detailed this result by cancer site. The authors observed a social gradient in cancer mortality for stomach, lung and cervical cancers, consistently with previous results on cancer incidence in Costa Rica (57). Inversely, they observed a reverse social gradient for colorectal cancer, non-Hodgkin lymphoma and leukemia. A reverse social gradient had already been found in the incidence of colorectal cancer (57). A lower mortality in rural areas was observed for most cancers, especially those associated with smoking, but also cervical cancers, prostate and breast cancers (56). Using the same methodology, Barboza-Solis showed in 2021 (58), that people who lived in the most socioeconomically disadvantaged districts had lower probabilities of developing lip, oral cavity and pharynx cancers, than people in the richest districts. Moreover, no evidence was found of a difference according to urbanicity or rurality in lip, oral cavity and pharynx cancers.
Fantin’s mortality and incidence results on cervical cancers are consistent with previous studies. Herrero et al. documented that cervical cancer incidence was higher in low-socioeconomic status, and in coastal areas in the mid-80’s (59). More recently, Santamaría-Ulloa et al. (60) confirmed these results showing a higher incidence in coastal and border areas, where populations are usually less favored.
Fantin’s findings regarding mortality from leukemia are not consistent with the results reported by Hyland et al. (61), who observed no differences in education levels between cases and controls between 1995 and 2000. The differences between the studies might be due to the outcome (mortality versus incidence), the measure of socioeconomic position (district’s wealth versus individual measures) or the sample size (1,449 deaths against 252 cases).
Llorca and Ortún (62) analyzed cancer mortality according to canton financial conditions, and showed an association between breast, uterus and skin cancers mortality and better financial conditions; and an association between prostate benign hyperplasia and financial conditions. Skin cancer mortality has also been found to be higher in rural compared to urban areas, consistently with Fantin’s results on cancer incidence. Llorca found that breast cancer mortality is higher in urban area. Fantin’s results confirmed this association, but attributed it to wealth after adjustment.
3.3.3 Diseases of the respiratory system
Between 2013 and 2022, diseases of the respiratory system represented 9% of the deaths in women and 8% in men in Costa Rica (52). In pre-COVID-19 studies, Rosero-Bixby and Dow (39) in the 1990s and Fantin et al. (41) between 2010 and 2018 found strong social gradients regarding mortality associated with diseases of the respiratory system. The findings of Rosero-Bixby and Dow showed a relative inequality index (RII) of 2.5, (CI [1.5–4.3]). Despite being a rare outcome, Chamizo-García showed that mortality associated with tuberculosis was higher in the poorest cantons compared to the richest cantons (63). The author also suggested that material deprivation is more frequent in extreme poverty households, and where the head of the household has elementary school (64). In relation to COVID-19, Fantin et al. (65) did not identify significant differences based on district wealth. However, the authors observed a lower excess death rate in rural areas compared to urban areas (11% versus 18%), indicating fewer additional deaths attributable to COVID-19 when compared to previous years (65). Using the canton geographical scale, García-Marín confirmed a higher COVID-19 infection risk in urban areas and in poorer areas, but did not find association with mortality risk (66).
3.3.4 External causes of mortality
Between 2013 and 2022, external causes of mortality (mainly car accidents, homicides and suicides) represented 5% of the deaths in women and 15% in men in Costa Rica (52). Car accidents, homicides and suicides represent 5, 4 and 2% of the deaths in men respectively, and 1, 0.5 and 0.6% in women. Rosero-Bixby and Dow in the 1990s (39) and Fantin et al. between 2010 and 2018 (41) found strong social gradients regarding mortality associated with external cause of mortality (54). Fantin et al. observed a more pronounced social gradient in men compared to women. This finding corroborates the results observed in the Limón province, where the lower life expectancy was partly attributed to higher rates of car accidents and homicides (42).
3.3.5 Other causes of death
In the study on cause-specific mortality between 2010 and 2018, Fantin et al. identified that the two main causes of deaths (diseases of the circulatory system and neoplasms) showed no or a small social gradient, but most of the other causes of deaths had a clear gradient, in particular for mortality associated with infectious diseases, endocrine, nutritional and metabolic diseases, and diseases of the genitourinary system (54). These social patterns increased after adjustment for urbanicity, that can be explained by a protective effect of living in rural area, in particular in men. The only cause of deaths showing a reverse social gradient were the diseases of the nervous system (54).
Chamizo-García showed an association between 2008–2013 mortality for diarrheas and canton development (67). In its analysis at the canton level, Llorca (62) also indicated that mortality for HIV infection was higher in the wealthiest cantons, and that maternal mortality was lower in wealthiest cantons compared to the poorest.
3.3.6 Self-reported health
Using CRELES data in elders, Assari et al. (68) and Rosero-Bixby and Dow (48) found that self-rated health increases with education level and income. Rosero-Bixby and Dow (48) additionally observed that physical and functional disabilities were lower in high-SES compared to low-SES elders. In particular, people without elementary school were at higher risk of functional disability (OR = 1.18, people with elementary school being the reference) than people with high school education (OR = 0.42). Similar results were found for physical frailty (OR = 1.18 and 0.58, respectively).
3.3.7 Depression
There is little information regarding mental health and SES. Rosero-Bixby and Dow (48) found higher prevalence of geriatric depression in low-wealth (OR = 1.51, medium-wealth being the reference) compared to high-wealth (OR = 0.73) using the CRELES data.
3.4 Health determinants
3.4.1 Access to health care
The public health system in Costa Rica provides free access to healthcare for the majority of the population (26). However, in other countries, it has been shown that this does not guarantee equitable distribution of healthcare access across all segments of the population. In 2004, Rosero-Bixby highlighted that the conception and strengthening of the preventive health units (EBAIS) has been pivotal in improving equitable access to healthcare, particularly in rural and impoverished areas. The authors noted that half of Costa Ricans reside less than 1 km away from an outpatient care facility and within 5 km of a hospital. Nonetheless, approximately 12–14% of the population was classified as underserved (69).
Moreover, some people are uninsured, in particular migrants. According to the last national surveys, 10% of the population declared themselves uninsured (70). During the COVID-19 pandemic, a qualitative study conducted with migrants showed that despite the well-known social welfare policies, migrant workers face additional burdens of exclusion and financial barriers (71).
Fantin et al. showed that cancer survival rates post-diagnosis were positively correlated with the wealth of districts, implying potential challenges in accessing timely diagnoses in economically disadvantaged areas. Interestingly, cancer survival rates were found to be similar between rural and urban areas (72). Additionally, Santamaría-Ulloa et al. highlighted in a 2022 study (73) that women residing in economically disadvantaged coastal regions (Chorotega, Central Pacific, and Huetar Caribbean) were less likely to participate regularly in cervical cancer screening. Furthermore, the study found that education level served as a protective factor for undergoing Pap screening and was associated with the reasons explaining why some women did not undergo any Pap screenings.
Brenes-Camacho assessed in 2009 health inequalities in the utilization of preventive health care services in people 60 years and over (25). The group with lower education levels was less likely to maintain blood pressure screenings and controls, as well as to undergo prostate screenings, mammograms, and eye examinations. This finding confirms Santamaria-Ulloa’s results, which indicated better access to screenings among high-SES individuals (73). Contrary to Santamaria-Ulloa’s findings, low-SES individuals were more likely to have frequent Pap smears. However, this discrepancy can be explained by the fact that most participants in Brenes-Camacho’s study were older than 65 years and thus not targeted for Pap smear screenings. Nevertheless, Brenes-Camacho et al. found that low-SES individuals were more likely to receive vaccinations (influenza, tetanus). This result aligns with the observations of Mujica et al. and Restrepo-Méndez et al., who noted in the 2010s that immunization coverage was less prevalent among the wealthiest quintile (74, 75).
Regarding maternal health care, studies did not find a social gradient in health coverage (75). Mujica et al. observed in the 2010’s that women in the richest quintile (Q5) had more antenatal care, compared to, respectively, Q4, Q3, Q2 and Q1 (having the most restricted access). In a classic article from 1986, it was already manifest in 1963, that the number of children decreased with income (76).
When it comes to access to health care that is poorly provided by the public service, inequalities become manifest. Hong et al. (77) observed, using measures of relative inequality, a disproportionate concentration of ophthalmologists among the economically advantaged areas, mainly when comparing the capital versus the rest of the country. Hong et al. found an inequality concentration index of 0.46 in Costa Rica versus 0.26 in average in Latin America. Similarly, dental care is mainly supported by private dentists. Barboza-Solís et al. indicated that dentist’s density was far higher in the wealthiest urban communities, compared to the poorest and/or the rural areas. Local Potential Accessibility to dentists was 9.3 per 100.000 inhabitants in the wealthiest districts against 6.2 in the most disadvantaged districts in the urban area, and 5.2 in the wealthiest districts against 1.9 in the most disadvantaged districts in the rural area. As a result, 16% of the Costa Ricans had very low or no access to dental care (78).
3.4.2 Alcohol consumption
In its report on alcohol consumption based on a national survey in 2015 (79), the Institute on Alcoholism and Drug Dependence (IAFA), indicated that alcohol consumption in the past twelve months was strongly associated with household income in men and in women. Consuming alcohol was 68% in men and 54% in women among the wealthiest households, compared to 33% in men and 19% in women among the poorest households.
This is consistent with Llorca and Ortún’s findings, which showed that mortality due to hepatic disease (secondary to alcohol consumption) was higher in the wealthiest cantons compared to the poorest cantons (62).
3.4.3 Smoking
Smoking prevalence sharply decreased in the last decades. Espinoza-Aguirre et al. (80) estimated smoking prevalence in 2015 to be 13% in men and 4% in women, using a representative sample of Costa Ricans. People who live in rural areas smoke less than those living in urban sites (7% vs. 10%). In 15–34 years age group, smoking prevalence was higher among individuals with low SES, but there was no association between education level or income and smoking prevalence in adults older than 35 years old. The absence of clear social gradient according to the household income in men was confirmed in a IAFA survey which used the household income in 2015 (79). In women, the results of the different surveys have contradictory results on social gradient, but all pointed to the low smoking prevalence (79, 80).
3.4.4 Chronic diseases
All the studies presented in this section used the CRELES data and are therefore focused on elders.
Santamaría-Ulloa et al. presented a lower diabetes prevalence in elder population who completed primary school compared to those who did not, but the authors did not show association between diabetes prevalence and income (81). Longer time to the closest facility translates into a lower probability of having the condition diagnosed, which can indicate that diabetes prevalence is lower or that being diagnosed is more difficult in rural areas (81).
Rosero-Bixby and Dow (48) showed no difference in the prevalence of uncontrolled dysglycemia according to SES, but found a higher prevalence of uncontrolled hypertension in low-SES individuals. In another study, Rosero-Bixby and Dow (48) observed, in elders, that various biomarkers, such as blood pressure, creatinine clearance, epinephrine, triglycerides and DHEA-S levels were in healthier levels in low-SES individuals compared to high-SES individuals. It is important to consider that in this study, high-SES individuals are wealthy metro San Jose residents with post primary education; low-SES individuals are poor lowland residents with no education. Goldman et al. analyzed 10 biomarkers in elder population, according to their education level (82). The authors found few differences according to education level, but confirmed higher levels of glucose and triglycerides in high-educated men compared to low-educated men, and highest level of systolic pressure and HbA1c in low-educated women compared to high-educated women.
3.4.5 Obesity
According to the Latin American Study of Nutrition and Health, the prevalence of obesity was 36% among women aged 15 years and older, and 24% among men aged 15 years and older in the period 2014–2015 (83). Herrera-Cuenca’s investigation did not reveal a distinct social pattern for anthropometric measures, such as waist-hip ratio, neck circumference, and waist circumference (83). The authors reported an increase in body mass index (BMI) with higher socioeconomic status (SES), although these findings are inconsistent across gender and age groups, and do not align with the estimated average, suggesting a potential calculation error. Gómez showed that nutritional diversity scores were found to be significantly lower in the low SES (84). Using data from 2005, Mazariegos et al. (85) did not observe a clear social gradient in obesity prevalence, neither in men nor in women. Additionally, using data from the Costa Rican Longevity and Healthy Aging Study (CRELES), Rosero-Bixby and Dow documented a higher prevalence of obesity, high-calorie diet, and abdominal girth among urban populations with high SES compared to non-urban populations with low SES (48). Similar results were found in children: Gamboa-Gamboa et al. documented using the 2016 National School Weight/Height Census that children overweight and obesity prevalence was lower in the poorest districts compared to the wealthiest districts (30.8% versus 37.5%), and in rural districts compared to urban districts (30.8% versus 35.8%) (33).
3.4.6 Diet
Regarding diet, Santamaría-Ulloa et al. (86) showed in urban women (between 2014–2015) that total protein consumption increases with SES, the prevalence of inadequate protein intake was lower in the higher SES group, and that processed meats are consumed mainly by women in medium, followed by low and high SES groups. Monge-Rojas et al. (87) implemented a Traditional Costa Rica Adolescents Diet Score (TCRAD) to assess the main determinants in 2017, positing that traditional diets in Costa Rica are healthier (intake of beans, vegetables, fruits, dairy products). The authors found that adolescents living in rural areas had higher traditional diet scores compared to urban. Nuñez-Rivas et al. (88) assessed diet quality using a scoring system in adolescents. It was found that individuals from high and medium SES groups backgrounds, as well as those with lower levels of education, tended to have better diets compared to those from low SES groups and with higher levels of education. However, these results should be interpreted with caution due to the authors’ reliance on only bivariate statistics.
Herrera-Cuenca et al. observed that calcium intake was significantly higher in high-SES individuals compared to low-SES individuals (83). Iron intake has been found to be similar according to social class in Herrera-Cuenca et al. (83). Lozoff et al. found in children living in an urban community and followed between 1981–1984 and 2000–2002, that infants in the lower SES level (measured by Hollingshead score) were more likely to be in the chronic-iron-deficiency group than in the non-chronic-iron-deficiency group (89).
3.4.7 Cognitive health in seniors
Finally, when it comes to cognitive health and healthy aging, a study reveal that having more years of education was associated with higher cognitive abilities, with a larger effect in rural group (90). Santamaría-García found that the most relevant risk factors negatively affecting cognition were low education, male sex, having mental health symptoms and older age. Education, sex and age were found associated with functional ability (91).
3.4.8 Severe tooth loss
Tooth loss is associated with poor Self-Rated Health (SRH) (92). Using CRELES data, Barboza-Solís et al. showed that adult tooth loss was strongly associated with SES measures, mainly education level, occupational status and subjective economic situation (93). This association was independent of health behaviors, including alcohol, consumption, smoking status, cariogenic diet and psychosocial factors. Fantin et al. also observed, using CRELES data, that adult tooth loss was strongly determined by early SES (94): 72.4% of the people who experienced the most deprived SES during childhood had severe tooth loss at the time of the interview; vs. 43.3% in the most advantaged (94).
4 Discussion
Studies at both the individual and district levels in Costa Rica have shown a clear, stepwise association between socioeconomic status (SES) and various health outcomes: as SES decreases, health indicators deteriorate correspondingly.
Mortality is often used to observe health inequalities, as it represents the ultimate health outcome, embodying all economic, social, and biological adversities throughout life (95). While some studies have suggested an absence of health inequalities in Costa Rica (48, 49, 96) overall mortality remains higher among individuals in the least socioeconomically advantaged group compared to the most advantaged (41). Specifically, mortality from respiratory diseases, external causes (such as homicides and car accidents), infectious diseases, endocrine, nutritional, and metabolic diseases, and diseases of the genitourinary system is significantly higher in the poorest districts compared to the wealthiest ones (54). The social gradient in mortality is particularly visible in middle-aged adults (41). In older populations, the gradient is less pronounced, especially among men, where some studies have even observed a reverse social gradient (49).
The observed social inequalities can result from a wide range of factors: unhealthy behaviors (e.g., alcohol consumption, smoking), lack of access to good nutrition and health education, obesity, exposure to occupational and environmental hazards, and limited access to an effective healthcare system (including prevention, timely detection and diagnosis, and high-quality treatments). All these factors are related to an individual’s socioeconomic status, income, wealth, and education level.
Analyzing the social determinants of health allows a better understanding of the reasons why, despite being one of the most inequitable countries in the OECD, health inequalities in mortality are less significant in Costa Rica compared to the US and Europe. For instance, the two main causes of death—diseases of the circulatory system (39–41) and neoplasms (39, 54)—are weakly or not at all associated with SES. Furthermore, while our findings indicate the presence of socioeconomic disparities, they also suggest that health inequalities can be partially mitigated by factors such as the concentration of wealth and the prevalence of risky behaviors, which vary between urban and rural areas. Despite prevalent poverty in both urban and rural areas, individuals in rural areas often exhibit better health outcomes, which may be attributed to their adherence to more traditional, less westernized lifestyles (56). Smoking prevalence is lower among individuals residing in rural areas compared to those in urban areas (80). Some studies also suggest that people living in rural areas have healthier and more traditional diets compared to those in urban areas (87). Alcohol consumption is strongly associated with higher SES (79). This phenomenon could highlight a balancing effect where increased access to resources in urban areas is counteracted by higher engagement in risky behaviors, ultimately resulting in relatively small socioeconomic gradients in health outcomes.
Among women, both smoking and alcohol consumption prevalences are low, regardless of whether they reside in urban or rural settings (79, 80). Consequently, these behavioral factors likely exert small impact on mortality rates. Thus, the observed disparities in women between rural and urban areas are more likely attributable to differences in SES, including wealth (41), income, and education levels.
In men, smoking and alcohol consumption prevalences are lower compared to European countries (28); however, they are still significant enough to yield observable consequences at the geographical level. Notably, in terms of cancer mortality, rural areas exhibit lower mortality rates compared to urban areas for most cancer sites associated with smoking (56).
Regarding access to effective healthcare, the public health system based on EBAIS has demonstrated relatively good results in terms of narrowing inequalities (25). It has been suggested that advancements in access to primary healthcare programs in the 1970s significantly contributed to the decrease in infant mortality, particularly among low SES populations (25). However, disparities persist in accessing diagnosis and/or treatment, as evidenced by social inequalities in survival rates after cancer diagnosis (72). Access to other healthcare services that are inadequately provided by the public health system, such as ophthalmology and dental care, remains highly inequitable (77, 78).
In this review, we included all studies focusing on social inequalities in health in Costa Rica. However, the analysis is limited by the scarcity of available literature. Following the conclusion of the CRELES study, which focused on older adults and completed its last wave in 2012–2013, no subsequent cohort study has aimed to longitudinally monitor the general health of a representative sample of the population. Consequently, the most comprehensive individual-level studies on social inequalities predominantly focus on older population. Furthermore, the absence of a new cohort study hinders the analysis of health outcomes from a life course perspective. To address the scarcity of individual-level data, several studies resort to ecological studies utilizing registries, particularly for assessing mortality, cause-specific mortality, life expectancy and cancer incidence. A notable limitation remains in understanding the association between urbanicity, wealth, and health due to the dearth of studies examining primary social determinants of health beyond smoking, alcohol consumption, obesity, physical activity and dietary habits. Moreover, a significant gap exists as the majority of studies reviewed herein do not incorporate other individual-level variables, such as ethnicity or migration status. Only one study intended to examine health disparities among indigenous populations and did not identify additional mechanisms beyond those previously described in the rural and impoverished territories. However, ethnicity was not measured in this study at an individual level and used indigenous territories as a proxy of ethnicity (96). We did not perform a formal quality assessment, including reporting of results or evaluating the validity and reliability of questionnaires. This decision may be considered a limitation in terms of comparing studies. However, our primary objective was to include all available data and interpret general findings, rather than excluding articles based on quality criteria. Furthermore, we encountered challenges when attempting to adapt existing quality assessment tools to the objectives of this comprehensive literature review, including issues with applicability of certain criteria and difficulties in analyzing ecological studies that were combined with other study designs.
This review highlights social inequalities in health within Costa Rica. These disparities are comparatively less pronounced than those observed in the US or Europe (39, 42). In other middle-income Latin American countries, such as Brazil, Chile, and Mexico, health inequalities are more pronounced than those observed in the Costa Rican context. The extent of these disparities can be explained by structural inequalities shaped by each country’s unique historical, social, economic, political, and healthcare specificities (97–99). The public healthcare system likely contributes partially to the reduced gap between high-SES and low-SES individuals in Costa Rica compared to the US and other Latin American countries. Nonetheless, a significant factor that could explain the inequalities mitigation, is the absence or even reverse gradients in risky health behaviors, such as smoking and alcohol consumption, particularly in rural areas (79, 80). Overall, consumption of alcohol and tobacco is relatively low compared to other OECD countries (28). Consequently, while there exists a relatively modest social gradient in health presently, there is a potential for its amplification with the adoption of more westernized behaviors. Previous evidence has suggested that disadvantaged populations tend to systematically bear the brunt of social, economic, political, and health burdens. However, our findings indicate that Costa Rica exhibits a more nuanced pattern, where individuals from the most disadvantaged sectors do not necessarily experience the cumulative burden seen in other contexts. The Costa Rican example demonstrates that when the prevalence of key risky behaviors is low, health inequalities tend to be reduced. Our study also highlights that in LMICs, socioeconomic status is not the sole factor influencing health inequality. Among disadvantaged populations, we observed significant differences between rural and urban residents. These differences, likely due to less westernized behaviors in rural areas, need to be better studied. More importantly, they necessitate the adaptation of public policies to address the specific needs of diverse populations.
In general, effective strategies to reduce health inequalities may include controlling risky behaviors in the general population and progressing towards universal health coverage with good access to primary healthcare facilities. Prevention policies should combine a population-wide strategy with a vulnerable-group approach to enable proportionate universalism. This approach ensures that interventions are tailored to the level of disadvantage, promoting equity in health outcomes. Future research efforts should prioritize monitoring social inequalities in health, particularly as the population ages. Given Costa Rica’s robust registries, there is an opportunity to delve into the study of rare diseases. Establishing new cohort studies and reinvigorating cross-sectional research initiatives are essential for comprehensively examining mortality trends and prevalent diseases. Individual-level data on health determinants including diet, physical activity, alcohol consumption, and stress exposures, stratified by various socioeconomic measures, are crucial for informing targeted interventions. Incorporating a life course approach within cohort studies can enhance our understanding of how early life events influence health outcomes through various pathways. This approach involves integrating data on SES, environmental exposures, risk factors, and biological measures to uncover associations and inform public health strategies effectively (100).
Costa Rican’s health outcomes are also influenced by the country’s history, political stability, its long-standing democracy, and strong institutional autonomy. The Ministry of Health and the Costa Rican Social Security Fund (CCSS) collaborate with various entities, including the public water company, the national insurance institute, universities, private healthcare services, and municipal and community initiatives. This collaborative network highlights the collective mission of promoting the health and well-being of Costa Ricans.
5 Conclusion
The findings highlight social inequalities in health within Costa Rica. Despite being considered one of the most inequitable countries in the OECD, it demonstrates relatively modest social gradients in health compared to other middle and high-income nations. Mortality disparities are shown among middle-aged adults but diminish in the older population. Social patterns in health behaviors can explain the mitigated inequality between rural and urban areas, where rural individuals exhibit lower rates of smoking and alcohol consumption. Additionally, there is an equalizing effect of the Costa Rican universal healthcare system. Disparities persist in accessing diagnosis and treatment, with evidence of social inequalities in cancer survival rates and unequal access to certain healthcare services such as ophthalmology and dental care.
Data availability statement
The original contributions presented in the study are included in the article, further inquiries can be directed to the corresponding authors.
Author contributions
CB-S: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. RH: Conceptualization, Funding acquisition, Methodology, Project administration, Resources, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. RF: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Software, Supervision, Validation, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This work was supported by the University of Costa Rica and the Costa Rican Biomedical Research Agency – Fundación INCIENSA.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. World Health Organization. Social Determinants of Health. Available at: https://www.who.int/health-topics/social-determinants-of-health#tab=tab_1 (Accessed January 2024).
2. Commission on Social Determinants of Health. Closing the gap in a generation. Health equity through action on the social determinants of health. Final Rep Geneva. (2008) 6:102–5. doi: 10.1080/17441692.2010.514617
3. Marmot, M, Friel, S, Bell, R, Houweling, TA, and Taylor, S. Closing the gap in a generation: health equity through action on the social determinants of health. Lancet. (2008) 372:1661–9. doi: 10.1016/S0140-6736(08)61690-6
4. Whitehead, M, and Dahlgren, G. Concepts and principles for tackling social inequities in health: Levelling up part 1. Copenhagen: World Health Organization. (2006). 34 p.
5. Stringhini, S, Carmeli, C, Jokela, M, Avendano, M, Muennig, P, Guida, F, et al. Socioeconomic status and the 25 x 25 risk factors as determinants of premature mortality: a multicohort study and meta-analysis of 1.7 million men and women. Lancet. (2017) 389:1229–37. doi: 10.1016/S0140-6736(16)32380-7
6. Petrovic, D, de Mestral, C, Bochud, M, Bartley, M, Kivimäki, M, Vineis, P, et al. The contribution of health behaviors to socioeconomic inequalities in health: a systematic review. Prev Med. (2018) 113:15–31. doi: 10.1016/j.ypmed.2018.05.003
7. Vineis, P, Avendano-Pabon, M, Barros, H, Bartley, M, Carmeli, C, Carra, L, et al. Special report: the biology of inequalities in health: the Lifepath consortium. Front public Heal. (2020) 8:118. doi: 10.3389/fpubh.2020.00118
8. PAHO. Just Societies: Health Equity and Dignified Lives. (2019). 302 p. Available at: http://iris.paho.org/xmlui/handle/123456789/51571. Accessed January 2024.
9. Islam, MM. Social determinants of health and related inequalities: confusion and implications. Front Public Heal. (2019) 7:11. doi: 10.3389/fpubh.2019.00011
10. Cash-Gibson, L, Rojas-Gualdrón, DF, Pericàs, JM, and Benach, J. Inequalities in global health inequalities research: a 50-year bibliometric analysis (1966-2015). PLoS One. (2018) 13:e0191901. doi: 10.1371/journal.pone.0191901
11. Ferri, CP, Acosta, D, Guerra, M, Huang, Y, Llibre-Rodriguez, JJ, Salas, A, et al. Socioeconomic factors and all cause and cause-specific mortality among older people in Latin America, India, and China: a population-based cohort study. PLoS Med. (2012) 9:e1001179. doi: 10.1371/journal.pmed.1001179
12. Bilal, U, Alazraqui, M, Caiaffa, WT, Lopez-Olmedo, N, Martinez-Folgar, K, Miranda, JJ, et al. Inequalities in life expectancy in six large Latin American cities from the SALURBAL study: an ecological analysis. Lancet Planet Heal. (2019) 3:e503–10. doi: 10.1016/S2542-5196(19)30235-9
13. World Bank. Poverty and shared prosperity 2016: taking on inequality. Washington D.C. (2016). 193. Available at: https://elibrary.worldbank.org/doi/epdf/10.1596/978-1-4648-0958-3 (Accessed: February 2024)
14. Barreto, SM, Miranda, JJ, Figueroa, JP, Schmidt, MI, Munoz, S, Kuri-Morales, PP, et al. Epidemiology in Latin America and the Caribbean: current situation and challenges. Int J Epidemiol. (2012) 41:557–71. doi: 10.1093/ije/dys017
15. PAHO In: B Legetic, A Medici, M Hernández-Ávila, G Alleyne, and A Hennis, editors. Economic dimensions of noncommunicable diseases in Latin America and the Caribbean. Washington D.C: PAHO (2016). 159.
16. United Nations. The sustainable development report goals 2016. Leaving no one behind (2016). Available at: https://unstats.un.org/sdgs/report/2016/leaving-no-one-behind (Accessed: December 2023).
17. INEC. Encuesta Nacional de Hogares (2023). Available at: https://inec.cr/estadisticas-fuentes/encuestas/encuesta-nacional-hogares (Accessed January 2024).
18. Instituto Nacional de Estadísticas y Censos INEC. Proyecciones de Población Distritales (2023). Available at: https://services.inec.go.cr/proyeccionpoblacion/frmproyec.aspx (Accessed February 2024).
19. World Bank. GDP per capita (current US$)—Costa Rica, OECD members Available at: https://data.worldbank.org/indicator/NY.GDP.PCAP.CD?locations=CR-OE. (Accessed December 2023).
20. Organisation for Economic Cooperation and Development. Income inequality. Available at: https://data.oecd.org/inequality/income-inequality.htm (Accessed February 2024).
21. Instituto Nacional de Estadísticas y Censos (INEC). Encuesta Nacional de Hogares Julio 2023: resultados generales. San José, Costa Rica. (2023). 127 p. Available at: https://admin.inec.cr/sites/default/files/2023-10/reenaho2023.pdf (Accessed January 2024).
22. Instituto Nacional de Estadísticas y Censos (INEC). Esperanza de vida al nacer. Available at: https://inec.cr/indicadores/esperanza-vida-al-nacer (Accessed January 2024).
23. Garay, JE, and Chiriboga, DE. A paradigm shift for socioeconomic justice and health: from focusing on inequalities to aiming at sustainable equity. Public Health. (2017) 149:149–58. doi: 10.1016/j.puhe.2017.04.015
24. Instituto Nacional de Estadísticas y Censos (INEC). Encuesta Nacional de Hogares 2021, 2022, 2023. Available at: https://inec.cr/estadisticas-fuentes/encuestas/encuesta-nacional-hogares (Accessed January 2024).
25. Brenes-Camacho, G, and Rosero-Bixby, L. Differentials by socioeconomic status and institutional characteristics in preventive service utilization by older persons in Costa Rica. J Aging Health. (2009) 21:730–58. doi: 10.1177/0898264309338299
26. Sáenz Mdel, R, Acosta, M, Muiser, J, and Bermúdez, JL. Sistema de salud de Costa Rica. Salud Publica Mex. (2011) 53:369–s167. doi: 10.1590/S0036-36342011000500003
27. Caja Costarricense del Seguro Social. CCSS-Hospitales. Available at: https://www.ccss.sa.cr/hospitales?v=1. Accessed February 2024.
28. OECD. OECD Health at a Glance (2023) Country Note: Costa Rica. Available at: https://www.oecd.org/costarica/health-at-a-glance-Costa-Rica-EN.pdf (Accessed February 2024).
29. Krieger, N. A glossary for social epidemiology. J Epidemiol Community Health. (2001) 55:693–700. doi: 10.1136/jech.55.10.693
30. Solar, O, and Irwin, A. A conceptual framework for action on the social determinants of health: social determinants of health discussion paper 2. Geneva: World Health Organization. (2010). 60–68, 28
31. World Health Organization. Handbook on health inequality monitoring: with a special focus on low and middle-income countries. Geneva: WHO Library Cataloguing-in-Publication Data. (2013). 105. Available at: https://www.paho.org/en/documents/handbook-health-inequality-monitoring-special-focus-low-and-middle-income-countries (Accessed: February 2024).
32. Mother, D, Liberati, A, and Tetzlaff, JThe PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLOS Med. (2009) 6:e1000097. doi: 10.1371/journal.pmed.1000097
33. Gamboa-Gamboa, T, Fantin, R, Cordoba, J, Caravaca, I, and Gómez-Duarte, I. Relationship between childhood obesity and socio-economic status among primary school children in Costa Rica. Public Health Nutr. (2021) 24:3825–33. doi: 10.1017/S1368980021002032
34. Instituto Nacional de Estadísticas y Censos (INEC). Censos. Available at: https://inec.cr/estadisticas-fuentes/censos (Accessed: February 2024).
35. Rosero-Bixby, L. CRELES: Costa Rican Longevity and Healthy Aging Study. Available at: http://www.creles.berkeley.edu/ (Accessed: February 2024).
36. Pérez-Brignoli, H, and López-Ruiz, LA. Evaluación de cobertura: estadísticas de nacimiento y defunción Costa Rica 2000–2012. San José, Costa Rica. (2017). 38 p. Available at: https://docplayer.es/66998522-Evaluacion-de-cobertura-estadisticas-de-nacimiento-y-defuncion-costa-rica.html (Accessed: January 2024).
37. Antón, Z, Ortiz, A, Campos, H, Galán-Rodas, E, and Lajous, M. The Cancer registry of Costa Rica: characteristics, evolution and modernization. Rev Hisp Cienc Salud. (2017) 3:95–102.
38. Fantin, R, Gómez-Duarte, I, Sáenz-Bonilla, JP, Rojas-Araya, K, and Barboza-Solís, C. Measuring socioeconomic position from the social inequalities in health perspective: the case of Costa Rica. Odovtos-Int J Dent Sci. (2019) 21:143–53. doi: 10.15517/ijds.2019.37295
39. Rosero-Bixby, L, and Dow, WH. Exploring why Costa Rica outperforms the United States in life expectancy: a tale of two inequality gradients. Proc Natl Acad Sci. (2016) 113:1130–7. doi: 10.1073/pnas.1521917112
40. Modrek, S, Dow, WH, and Rosero-Bixby, L. Long-term association of economic inequality and mortality in adult Costa Ricans. Soc Sci Med. (2012) 74:158–66. doi: 10.1016/j.socscimed.2011.10.034
41. Fantin, R, Delpierre, C, Kelly-Irving, M, and Barboza-Solís, C. Complex social gradient in life expectancy in Costa Rica: an ecological study with 24-million person-years follow-up. Odovtos-Int J Dent Sci. (2021) 23:447–59. doi: 10.15517/ijds.2021.46128
42. Fantin, R, and Barboza, SC. Health inequalities in life expectancy according to the province of birth in Costa Rica. Población y Salud en Mesoamérica. (2020) 18:28–51. doi: 10.15517/psm.v18i1.39073
43. The World Bank. Mortality rate, infant (per 1,000 live births) – Costa Rica. Available at: https://data.worldbank.org/indicator/SP.DYN.IMRT.IN?locations=CR (Accessed: February 2024).
44. Chamizo García, HA, and Behm, AI. Geographic inequalities in infant mortality in Costa Rica, 2008-2012. Población y Salud en Mesoamérica. (2014) 12:102–17. doi: 10.15517/psm.v12i1.15139
45. McGuire, JW. Politics, policy, and mortality decline in Costa Rica In: Politics, policy, and mortality decline in East Asia and Latin America Wesleyan University (2006, 40)
46. Rosero-Bixby, L. Socioeconomic development, health interventions and mortality decline in Costa Rica. Scand J Soc Med Suppl. (1991) 46:33–42.
47. Metzger, X. Data aggregation in measuring inequalities and inequities in the health of populations. Rev Panam Salud Pública. (2002) 12:445–53. doi: 10.1590/S1020-49892002001200010
48. Rosero-Bixby, L, and Dow, WH. Surprising SES gradients in mortality, health, and biomarkers in a Latin American population of adults. J Gerontol Soc Sci. (2009) 64:105–17. doi: 10.1093/geronb/gbn004
49. Rosero-Bixby, L. High life expectancy and reversed socioeconomic gradients of elderly people in Mexico and Costa Rica. Demogr Res. (2018) 38:95–108. doi: 10.4054/DemRes.2018.38.3
50. Sudharsanan, N, Zhang, Y, Payne, CF, Dow, W, and Crimmins, E. Education and adult mortality in middle-income countries: surprising gradients in six nationally-representative longitudinal surveys. SSM-Popul Heal. (2020) 12:100649. doi: 10.1016/j.ssmph.2020.100649
51. Rosero-Bixby, L, Dow, WH, and Laclé, A. Insurance and other socioeconomic determinants of elderly longevity in a Costa Rican panel. J Biosoc Sci. (2005) 37:705–20. doi: 10.1017/S0021932004006996
52. Instituto Nacional de Estadísticas y Censos (INEC). INEC-Sistema de Consultas. Available at: https://inec.cr/sistemas-de-consulta (Accessed: January 2024).
53. Sotos-Prieto, M, Baylin, A, Campos, H, Qi, L, and Mattei, J. Lifestyle cardiovascular risk score, genetic risk score, and myocardial infarction in Hispanic/Latino adults living in Costa Rica. J Am Heart Assoc. (2016) 5:67. doi: 10.1161/JAHA.116.004067
54. Fantin, R, Delpierre, C, and Barboza-Solís, C. Health inequalities in cause-specific mortality in Costa Rica: a population-based cohort study. Rev Saude Publica. (2023) 57:3. doi: 10.11606/s1518-8787.2023057004331
55. Fantin, R, Barboza-Solís, C, and Santamaría-Ulloa, C. Socioeconomic inequalities in cancer mortality: is Costa Rica an exception to the rule? Int J Cancer. (2020) 147:1286–93. doi: 10.1002/ijc.32883
56. Fantin, R, Sierra, MS, Vaccarella, S, Herrero, R, and Barboza-Solís, C. Social gradient and rural-urban disparities in cancer mortality in Costa Rica. Cancer Epidemiol. (2024) 91:102604. doi: 10.1016/j.canep.2024.102604
57. Fantin, R, Ulloa, CS, and Solís, CB. Social gradient in cancer incidence in Costa Rica: findings from a national population-based cancer registry. Cancer Epidemiol. (2020) 68:101789. doi: 10.1016/j.canep.2020.101789
58. Barboza Solís, C, Reyes-Carmona, J, and Fantin, R. Social inequality in incidence and mortality of malignant neoplasms of lip, oral cavity and pharynx: is Costa Rica an international paradox? Community Dent Oral Epidemiol. (2022) 50:243–50. doi: 10.1111/cdoe.12658
59. Herrero, R, Brinton, LA, Hartge, P, Reeves, WC, Breñes, MM, Urcuyo, R, et al. Determinants of the geographic variation of invasive cervical cancer in Costa Rica. Bull Pan Am Health Organ. (1993) 27:15–25.
60. Santamaría-Ulloa, C, and Valverde-Manzanares, C. Inequality in the incidence of cervical Cancer: Costa Rica 1980-2010. Front Oncol. (2018) 8:664. doi: 10.3389/fonc.2018.00664
61. Hyland, C, Gunier, RB, Metayer, C, Bates, MN, Wesseling, C, and Mora, AM. Maternal residential pesticide use and risk of childhood leukemia in Costa Rica. Int J Cancer. (2018) 143:1295–304. doi: 10.1002/ijc.31522
62. Llorca Castro, F, and Ortún, RV. Unnecessary premature and avoidable mortality in Costa Rica. Rev Esp Salud Publica. (2010) 84:771–87. doi: 10.1590/s1135-57272010000600008
63. Chamizo García, HA. Inequidades geográficas y tuberculosis en Costa Rica, 2008-2012. Población y Salud en Mesoamérica. (2016) 13:20–41. doi: 10.15517/psm.v13i2.21455
64. Chamizo García, HA. Saneamiento ambiental e inequidades en salud, en Costa Rica - Environmental sanitation and inequities in health in Costa Rica. Horiz Sanit. (2021) 20:57–67. doi: 10.19136/hs.a20n1.3718
65. Fantin, R, Barboza-Solís, C, Hildesheim, A, and Herrero, R. Excess mortality from COVID 19 in Costa Rica: a registry based study using Poisson regression. Lancet Reg Heal Am. (2023) 20:100451. doi: 10.1016/j.lana.2023.100451
66. García-Marín, A, and García, FR. COVID-19 in Costa Rica: longitudinal analysis of the transmission and death rates from the social inequality approach. Población y Salud en Mesoamérica. (2022) 20:244–80. doi: 10.15517/psm.v20i1.50200
67. Chamizo García, HA. Mortality due to diarrheas and inequalities in Costa Rica. Horiz Sanit. (2017) 16:16–27. doi: 10.19136/hs.a16n1.1412
68. Assari, S, and Lankarani, MM. Does multi-morbidity mediate the effect of socioeconomics on self-rated health? Cross-country differences. Int J Prev Med. (2015) 6:85. doi: 10.4103/2008-7802.164413
69. Rosero-Bixby, L. Spatial access to health care in Costa Rica and its equity: a GIS-based study. Soc Sci Med. (2004) 58:1271–84. doi: 10.1016/S0277-9536(03)00322-8
70. Instituto Nacional de Estadísticas y Censos (INEC). Sistema de consultas – Censo de Población y Vivienda. Available at: https://inec.cr/sistemas-de-consulta (Accessed: December 2023).
71. Poirier, MJP, Barraza, D, Caxaj, CS, Martínez, AM, Hard, J, and Montoya, F. Informality, social citizenship, and wellbeing among migrant Workers in Costa Rica in the context of COVID-19. Int J Environ Res Public Health. (2022) 19:1–14 doi: 10.3390/ijerph19106224
72. Fantin, R, Santamaría-Ulloa, C, and Barboza-Solís, C. Social inequalities in cancer survival: a population-based study using the Costa Rican Cancer registry. Cancer Epidemiol. (2020) 65:101695. doi: 10.1016/j.canep.2020.101695
73. Santamaría-Ulloa, C, Montero-López, M, Quesada-Leitón, H, and Quirós-Rojas, I. Inequalities in the early detection of cervical cancer: a reality in the Costa Rica. Poblac y Salud en Mesoamerica. (2022) 19:598. doi: 10.15517/psm.v0i19.48122
74. Restrepo-Méndez, MC, Barros, AJD, Requejo, J, Durán, P, Serpa La De, F, França, GVA, et al. Progress in reducing inequalities in reproductive, maternal, newborn,' and child health in Latin America and the Caribbean: an unfinished agenda. Rev Panam Salud Publica. (2015) 38:9–16.
75. Mujica, OJ, Sanhueza, A, Carvajal-Velez, L, Vidaletti, LP, Costa, JC, Barros, AJD, et al. Recent trends in maternal and child health inequalities in Latin America and the Caribbean: analysis of repeated national surveys. Int J Equity Health. (2023) 22:125. doi: 10.1186/s12939-023-01932-4
76. Carvajal, MJ, and Geithman, DT. Empirical findings on socioeconomic determinants of fertility differentials in Costa Rica. Int J Sociol Fam. (1986). 16:19–35.
77. Hong, H, Mújica, OJ, Anaya, J, Lansingh, VC, López, E, and Silva, JC. The challenge of universal eye health in Latin America: distributive inequality of ophthalmologists in 14 countries. BMJ Open. (2016) 6:e012819. doi: 10.1136/bmjopen-2016-012819
78. Barboza-Solis, C, Barahona-Cubillo, J, and Fantin, R. Health inequalities in the geographic distribution of dental practitioners in Costa Rica: an ecological study. Community Dent Oral Epidemiol. (2024) 52:39–46. doi: 10.1111/cdoe.12899
79. Instituto sobre Alcoholismo y Farmacodependencia. VI encuesta nacional 2015: Consumo de drogas en Costa Rica. San José, Costa Rica. (2018). 177 p. Available at: https://www.iafa.go.cr/wp-content/uploads/2022/05/Encuesta-Nacional-de-Drogas-2015.pdf (Accessed: December 2023).
80. Espinoza-Aguirre, A, Fantin, R, Barboza-Solís, C, and Salinas-Miranda, A. Sociodemographic characteristics associated with the prevalence of tobacco use in Costa Rica. Pan Am J Public Heal. (2020) 44:1–8. doi: 10.26633/RPSP.2020.17
81. Santamaría-Ulloa, C, Montero-López, M, and Rosero-Bixby, L. Diabetes epidemics: inequalities increase the burden on the healthcare system. Health Policy Plan. (2019) 34:ii45–55. doi: 10.1093/heapol/czz109
82. Goldman, N, Turra, CM, Rosero-Bixby, L, Weir, D, and Crimmins, E. Do biological measures mediate the relationship between education and health: a comparative study. Soc Sci Med. (2011) 72:307–15. doi: 10.1016/j.socscimed.2010.11.004
83. Herrera-Cuenca, M, Kovalskys, I, Gerardi, A, Hernandez, P, Sifontes, Y, Gómez, G, et al. Anthropometric profile of Latin American population: results from the ELANS study. Front Nutr. (2021) 8:740361. doi: 10.3389/fnut.2021.740361
84. Gómez, G, Kovalskys, I, Leme, ACB, Quesada, D, Rigotti, A, Cortés Sanabria, LY, et al. Socioeconomic status impact on diet quality and body mass index in eight latin American countries: ELANS study results. Nutrients. (2021) 13 doi: 10.3390/nu13072404
85. Mazariegos, M, Auchincloss, AH, Braverman-Bronstein, A, Kroker-Lobos, MF, Ramírez-Zea, M, Hessel, P, et al. Educational inequalities in obesity: a multilevel analysis of survey data from cities in Latin America. Public Health Nutr. (2021) 25:1790–8. doi: 10.1017/S1368980021002457
86. Santamaría-Ulloa, C, and Bekelman, TA. Intake of processed meats by Costa Rican women: effect of socioeconomic status. Rev Biol Trop. (2021) 69:665–77. doi: 10.15517/rbt.v69i2.45428
87. Monge-Rojas, R, O’Neill, J, Lee-Bravatti, M, and Mattei, J. A traditional Costa Rican adolescents’ diet score is a valid tool to capture diet quality and identify sociodemographic groups with suboptimal diet. Front Public Heal. (2021) 9:708956. doi: 10.3389/fpubh.2021.708956
88. Núñez-Rivas, HP, Holst-Schumacher, I, and Campos-Saborío, N. New diet quality index for children and adolescents in Costa Rica. Nutr Hosp. (2020) 37:65–72. doi: 10.20960/nh.02695
89. Lozoff, B, Jimenez, E, and Smith, JB. Double burden of iron deficiency in infancy and low socioeconomic status: a longitudinal analysis of cognitive test scores to age 19 years. Arch Pediatr Adolesc Med. (2006) 160:1108–13. doi: 10.1001/archpedi.160.11.1108
90. Valdivieso-Mora, E, Salazar-Villanea, M, and Johnson, DK. Measurement invariance of a neuropsychological battery across urban and rural older adults in Costa Rica. Appl Neuropsychol Adult. (2022). 25:1–12. doi: 10.1080/23279095.2021.2023153
91. Santamaria-Garcia, H, Sainz-Ballesteros, A, Hernandez, H, Moguilner, S, Maito, M, Ochoa-Rosales, C, et al. Factors associated with healthy aging in Latin American populations. Nat Med. (2023) 29:2248–58. doi: 10.1038/s41591-023-02495-1
92. Barboza-Solís, C, Porras-Chaverri, M, and Fantin, R. Is tooth loss important when evaluating perceived general health? Findings from a nationally representative study of Costa Rican adults. Community Dent Oral Epidemiol. (2019) 47:358–65. doi: 10.1111/cdoe.12466
93. Barboza Solís, C, and Fantin, R. The role of socioeconomic position in determining tooth loss in elderly Costa Rican: findings from the CRELES cohort. Odovtos Int J Dent Sci. (2017) 19:79–94. doi: 10.15517/ijds.v19i3.29851
94. Fantin, R, Delpierre, C, Kelly-Irving, M, and Barboza, SC. Early socioeconomic conditions and severe tooth loss in middle-aged Costa Ricans. Community Dent Oral Epidemiol. (2018) 46:178–84. doi: 10.1111/cdoe.12351
95. Krieger, N, and Davey, SG. “Bodies count,” and body counts: social epidemiology and embodying inequality. Epidemiol Rev. (2004) 26:92–103. doi: 10.1093/epirev/mxh009
96. Fantin, R, and Barboza-Solis, C. Mortality differences and their causes: a comparative study between indigenous and non-indigenous areas of Costa Rica. Población y Salud en Mesoamérica. (2022) 20:49807. doi: 10.15517/psm.v20i1.49807
97. Szwarcwald, CL, da Mota, JC, Damacena, GN, and Pereira, TGS. Health inequalities in Rio de Janeiro, Brazil: lower healthy life expectancy in socioeconomically disadvantaged areas. Am J Public Health. (2011) 101:517–23. doi: 10.2105/AJPH.2010.195453
98. Espinoza, MA, Severino, R, Balmaceda, C, Abbott, T, and Cabieses, B. The socioeconomic distribution of life expectancy and healthy life expectancy in Chile. Int J Equity Health. (2023) 22:160. doi: 10.1186/s12939-023-01972-w
99. Addey, T, Alegre-Díaz, J, Bragg, F, Trichia, E, Wade, R, Santacruz-Benitez, R, et al. Educational and social inequalities and cause-specific mortality in Mexico City: a prospective study. Lancet Public Heal. (2023) 8:e670–9. doi: 10.1016/S2468-2667(23)00153-6
100. Kelly-Irving, M, and Vineis, P. Life-course approach: from socioeconomic determinants to biological embodiment In: S Vaccarella, J Lortet-Tieulent, R Saracci, DI Conway, K Straif, and CP Wild, editors. Reducing social inequalities in cancer: Evidence and priorities for research. Lyon, France: International Agency for Research on Cancer (2019). 255.
Keywords: health inequalities, Costa Rica, low and middle-income country, systematic review, social determinants of health, health inequities
Citation: Barboza-Solis C, Herrero R and Fantin R (2024) Health inequalities in a middle-income country: a systematic review of the Costa Rican case. Front. Public Health. 12:1397576. doi: 10.3389/fpubh.2024.1397576
Edited by:
Cyrille Delpierre, INSERM Public Health, FranceReviewed by:
Ezekiel Boro, Liverpool School of Tropical Medicine, United KingdomObasanjo Bolarinwa, York St John University, United Kingdom
Copyright © 2024 Barboza-Solis, Herrero and Fantin. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Cristina Barboza-Solis, Y3Jpc3RpbmEuYmFyYm96YXNvbGlzQHVjci5hYy5jcg==; Romain Fantin, cmZhbnRpbkBhY2liZnVuaW4uY29t