 Adolfo Aramburu1,2*
Adolfo Aramburu1,2* Gandy Dolores-Maldonado1
Gandy Dolores-Maldonado1 Katherine Curi-Quinto1Karen Cueva1
Katherine Curi-Quinto1Karen Cueva1 Giancarlo Alvarado-Gamarra1*Katherine Alcalá-Marcos3
Giancarlo Alvarado-Gamarra1*Katherine Alcalá-Marcos3 Carlos R. Celis1Claudio F. Lanata1,4
Carlos R. Celis1Claudio F. Lanata1,4- 1Centro de Promoción de Estilos de Vida Saludable, Instituto de Investigación Nutricional (IIN), Lima, Peru
- 2Faculty of Science Health, Universidad Peruana de Ciencias Aplicadas, Lima, Peru
- 3Instituto Nacional Cardiovascular “Carlos Alberto Peschiera Carrillo”—INCOR, Lima, Peru
- 4Department of Pediatrics, School of Medicine, Vanderbilt University, Nashville, TN, United States
Introduction: Our objective was to explore the effect of the reduction of saturated fat (SAF) intake on cardiovascular disease, mortality and other health-related outcomes in adults.
Methods: We conducted an umbrella review, searching Medline, Scopus, EMBASE, Cochrane Library, and LILACS databases for systematic reviews from December 1, 2012, to December 1, 2022. We have included meta-analyses of randomized controlled trials (RCTs) and cohort studies. We extracted effect sizes (95%CI), heterogeneity (I2), and evidence quality rating based on the population, intervention, comparator, and outcomes.
Results: 21 meta-analyses were included (three were from RCTs, and 18 were from cohort studies). Among meta-analyses of RCTs, 15 of the 45 associations were significant. The effect of reduction in SAF intake on combined cardiovascular events (RR 0.79, 95%CI 0.66–0.93) was graded as having moderate certainty of evidence. We found no effect on all-cause mortality, cardiovascular mortality, cancer deaths, and other cardiovascular events. Among meta-analyses of cohort studies, five of the 19 associations were significant. There was an increase in coronary heart disease mortality (HR 1.10, 95% CI 1.01–1.21) and breast cancer mortality (HR 1.51, 95% CI 1.09–2.09) in participants with higher SFA intake compared to reduced SFA. We found no effect on all-cause mortality, cardiovascular mortality, and other cardiovascular events.
Conclusion: This umbrella review found the reduction in SAF intake probably reduces cardiovascular events and other health outcomes. However, it has little or no effect on cardiovascular mortality and mortality from other causes. More high-quality clinical trials with long-term follow-up are needed.
Systematic review registration: CRD42022380859.
1 Introduction
Cardiovascular disease (CVD) is the leading global cause of death, generating a significant impact on the public health systems of the United States, Europe, and even in low- and middle-income countries (LMCIs), with a secular tendency to increase in recent years. Also, with high annual direct and indirect costs associated with these deaths, including health expenditures and lost productivity (1–5).The American Heart Association (AHA), in conjunction with the National Institutes of Health (NIH) and other government agencies, provides each year a document named the AHA’s Life’s Essential 8, which include core health behaviors (smoking, physical activity, diet, and weight) and health factors (cholesterol, blood pressure, and glucose control) that contribute to cardiovascular health (6, 7). In this context, improving the nutritional quality of the diet has been recognized as a relevant lifestyle approach to reducing the risk of atherosclerotic cardiovascular disease (ASCVD) (7, 8).
Public health dietary advice on prevention of CVD has changed over time (9). Regarding saturated fat (SAF) intake, both the American College of Cardiology (ACC) and the AHA (5, 10), as well as the European Society of Cardiology (ESC) (11), recommend replacing saturated with unsaturated fats to reduce the risk of ASCVD. However, these recommendations are based on observational studies and some randomized controlled trials (RCTs) that show discrepancies in their results (9, 12–23). In that sense, certain groups suggest that there is not robust evidence supporting the idea that reducing SAF intake, substituting it with unsaturated fats, or adhering to existing population-wide arbitrary upper limits on SAF consumption will effectively prevent CVD mortality (13, 24–27).
On the other hand, most healthcare interventions evaluated in Cochrane Reviews are not supported by high-quality evidence, and harms are under-reported (28). Additionally, some organizations rely on low-quality evidence to formulate recommendations, justifying their decisions as consensus-based guidelines (29). To ensure recommendations based on high-quality evidence, it is essential to develop trustworthy clinical practice guidelines (CPGs) that are informed by a systematic review of evidence and employ a standardized methodology, such as the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) approach (29, 30).
Therefore, this umbrella review aimed to systematically identify meta-analyses of randomized controlled trials (RCTs) and cohort studies investigating the reduction of saturated fat (SAF) intake and its impact on cardiovascular disease, mortality, and other health-related outcomes in adults.
2 Materials and methods
2.1 Protocol and registration
This study was performed according to the recommendations of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) (31). The study protocol was registered in the International Prospective Register of Systematic Reviews (PROSPERO), number CRD42022380859.
2.2 Search strategy
We searched Medline, Scopus, EMBASE, Cochrane Library, and LILACS database of systematic reviews from December 01, 2012, to December 1, 2022. No language restriction. Our search strategy included Medical Subject Title (MeSH) terms and free-text terms such as “Saturated Fatty Acid,” “Dietary Fats,” “Cardiovascular Diseases,” “Heart Disease Risk Factors,” and “cardiovascular outcomes.” We adapted the search algorithms to the requirements of each database. The final search strategy is available as Supplementary Table 1.
2.3 Eligibility criteria
Studies were included if they met the following criteria: (1) Population: Systematic reviews that include primary studies in adults (over 18 years), at any risk of cardiovascular disease, with or without cardiovascular disease (but not acutely ill), using or not using lipid-lowering medication; (2) Systematic reviews with meta-analyses of RCTs or observational studies (cohort); (3) Intervention/comparator: RCTs comparing reduced SFA intake vs. higher SFA intake, and cohort studies comparing categories of low vs. high SFA intake; and (5) Outcomes: studies that reported cardiovascular events and mortality (all-cause mortality, cardiovascular mortality, and cancer deaths) as primary outcomes, and/or other secondary outcomes such as cancer, diabetes, glucose-insulin homeostasis, lipid profile, body weight, blood pressure, and quality of life. We excluded narrative reviews, scoping reviews, meta-analyses of studies with other study designs, comments, editorials, guidelines, and conference abstracts.
2.4 Study selection
Duplicate documents were removed with Endnote X20 software. Six independent authors (AA, GD-M, KC-Q, GA-G, CC, and KA-M) selected the articles by titles and abstracts to identify potentially relevant articles. Then, articles were evaluated in full text to assess their eligibility. Any discrepancies were resolved by discussion with the third reviewer (CFL).
2.5 Data extraction
Four independent authors (AA, GA-G, KA-M, and CC) extracted the data. Discrepancies were resolved with consensus. We recorded the following variables: author, year of publication, study design, number of participants and included studies, type of intervention/comparator, outcomes with their effect size with 95% confidence interval (CI), heterogeneity (I2), study follow-up range, and GRADE rating. Another author (GA-G) checked the quality of the data before analysis.
We assessed the overlapping of studies according to the “corrected covered area (CCA)’” for each outcome. CCA >5% was considered as significant overlap (32). In this case, the study result with the highest score was prioritized in a score based on the date of publication, methodological quality, and number of primary studies included.
2.6 Quality assessment
Four independent authors (AA, GA-G, CC, and KA-M) independently assessed the quality of the included studies using “A Measurement Tool to Assess Systematic Reviews” (AMSTAR-2), a third author (CFL) settled in case of doubt. This tool consists of 16 items (maximum score: 16. and minimum score: 0). Based on the critical domains, we consider high, moderate, low, and critically low quality in the results (33).
2.7 Statistical analysis
We have developed a narrative summary of the data from each included systematic review, including effect estimates with their 95% CI, statistical assessment of heterogeneity (I2), GRADE score (certainty of evidence), and other study characteristics exactly as reported in the included systematic reviews. We performed sensitivity analyses to assess the effect on the outcomes excluded by overlap.
3 Results
3.1 Study selection
A total of 2,427 documents were identified, and 579 duplicates were removed. In the review by title and abstract, there were 1848 potentially eligible studies. Then, 15 documents were excluded during the full-text evaluation (justification available in Supplementary Table 2), and finally 21 meta-analyses were included in the study (Figure 1), three articles were meta-analyses of RCTs (9, 34, 35) and 18 were meta-analyses of cohort studies (17–19, 36–50). After the selection criteria, no studies were excluded due to overlap, but some outcomes were not analyzed because of data overlapping (list of excluded outcomes in Supplementary Table 3).
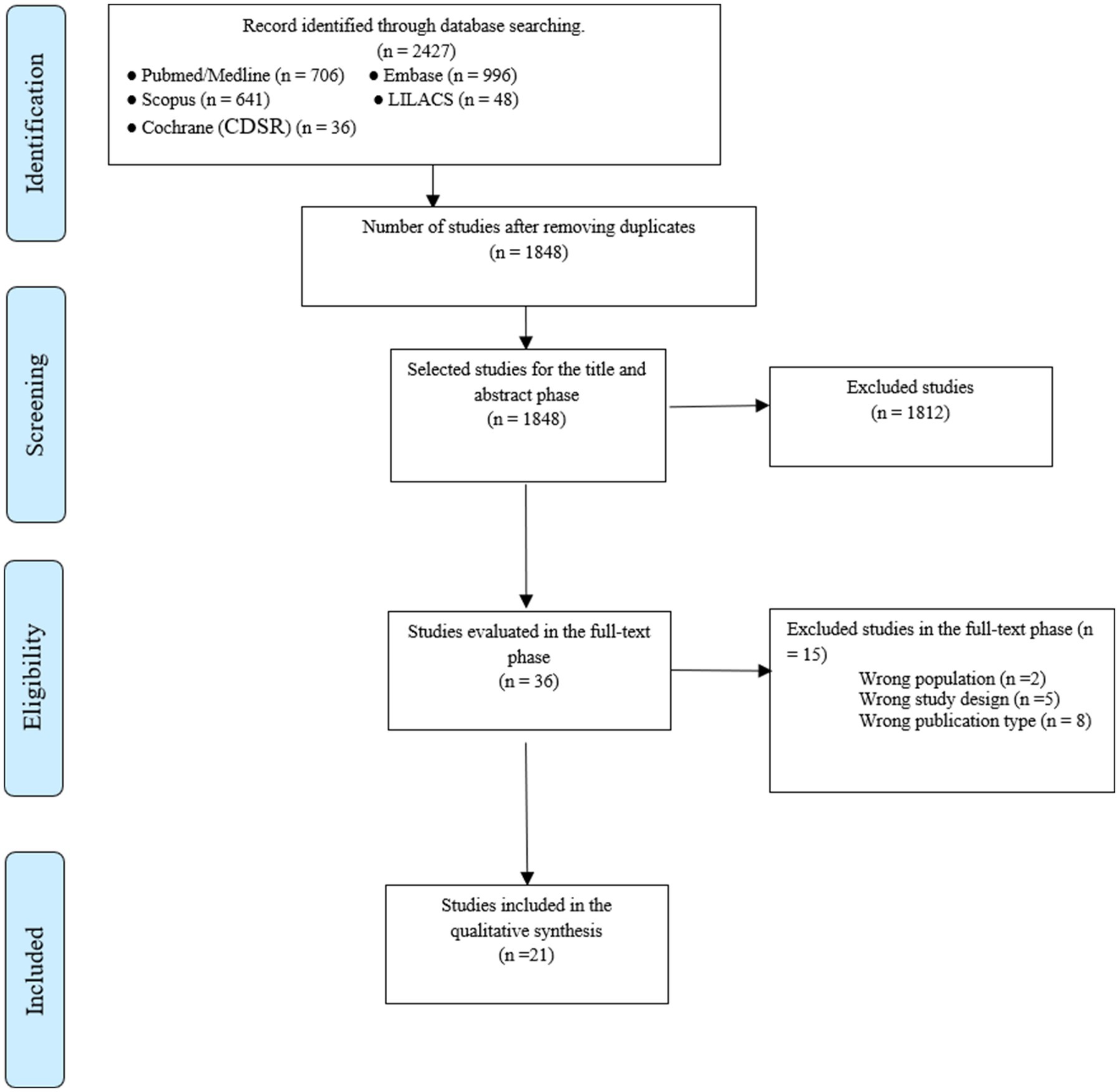
Figure 1. Flow chart of study selection.
3.2 Characteristics of included studies
The three meta-analyses of RCTs (9, 34, 35) described 45 potential associations of cardiovascular disease and mortality associated with reduction in SAF intake. The number of RCTs were 125, with a sample of 663–56,000 participants and a follow-up duration ranging from 3 to 9 years (additional characteristics in Table 1).
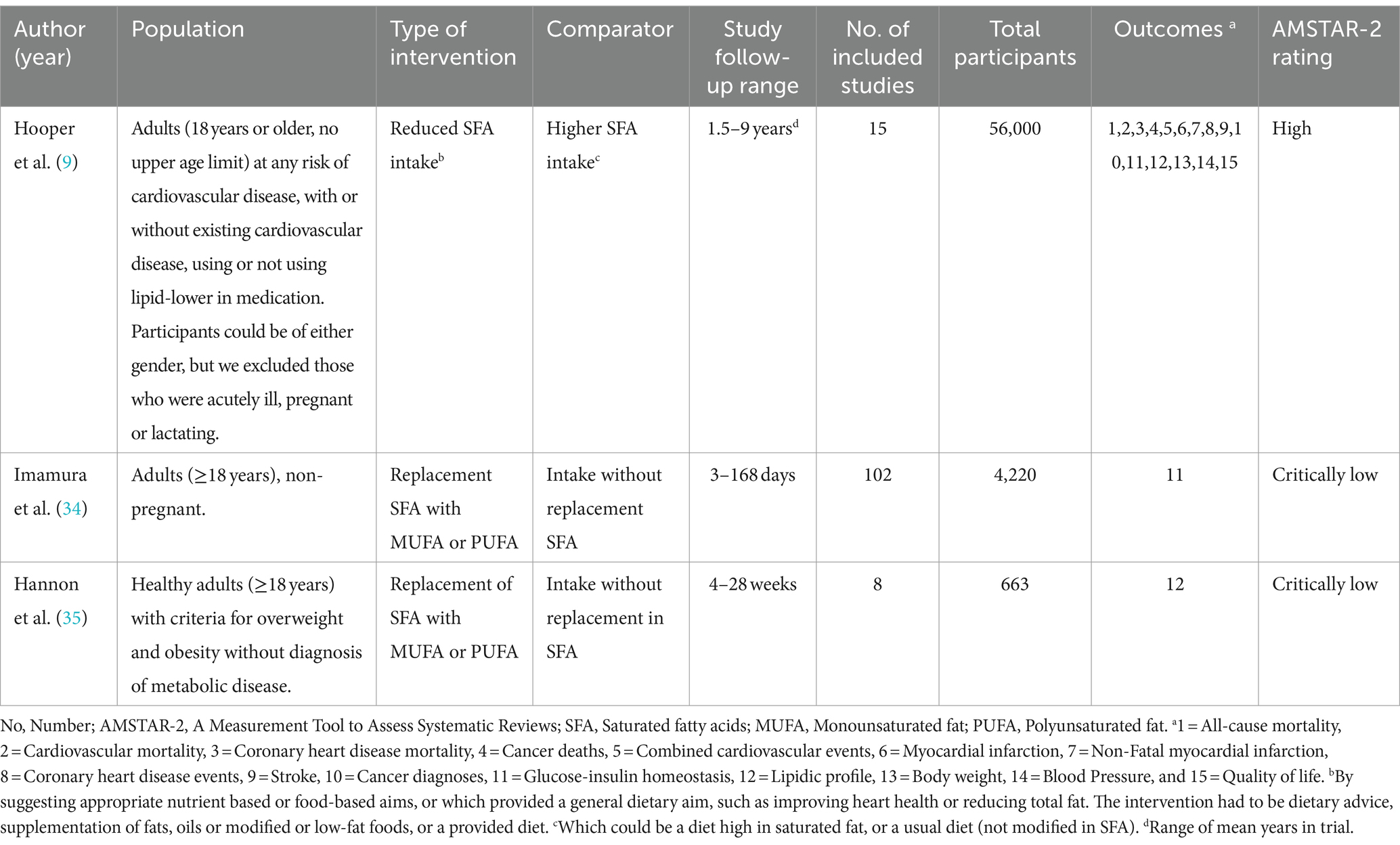
Table 1. Characteristics of meta-analyses of randomized clinical trials studying saturated fat intake.
The 18 meta-analyses of cohort studies (17–19, 36–50) described 19 potential associations of cardiovascular disease and mortality associated with reduction in SAF intake. The median number of studies per meta-analysis was 11 (interquartile range, IQR, 7–15), the follow-up duration ranged from 1 to 32 years, and the median sample was 462,268 participants (IQR, 318,747-836,322.5 participants) per meta-analysis (additional characteristics in Supplementary Table 4).
3.3 Quality of studies
About meta-analyses of RCTs, the quality assessment revealed that one was rated as high quality (score: 16) (9), while two were assessed as critically low quality (score: 13 and 10) (34, 35). About meta-analyses of cohort studies (17–19, 36–50), analysis revealed that three meta-analyses (16.7%) were of low quality, and 15 meta-analyses (83.3%) were of critically low quality, with a median score of 10.5 (interquartile range: 8–12) (details in Supplementary Table 5).
3.4 Description and summary of associations
3.4.1 Meta-analyses of RCTs
Fifteen of the 45 associations (33.3%) were statistically significant (p < 0.05) based on random-effects models. The identified associations comprised two types of intervention/comparator, including reduced SFA intake vs. higher SFA intake (51.1%) or replacement of SFA with monounsaturated fatty acids (MUFAs) or polyunsaturated fatty acids (PUFAs) vs. intake without replacement in SFA (48.9%). 30 associations analyzed non-repeated outcomes, including nine (30%) cardiovascular and mortality events, six (20%) lipid profile outcomes, nine (30%) glucose-insulin homeostasis outcomes, two (6.7%) blood pressure outcomes, two (6.7%) body weight outcomes, one outcome (3.3%) of quality of life, and another (3.3%) with a diagnosis of cancer. Also, 10 of the 24 associations (41.7%) had heterogeneity (I2) > 50%, and eight (17.8%) of the 45 associations assessed the certainty of evidence using GRADE (three associations were supported by moderate certainty of evidence, others three were supported by very low, and two associations by low certainty of evidence). Summary of all associations in Table 2 and Supplementary Table 6.
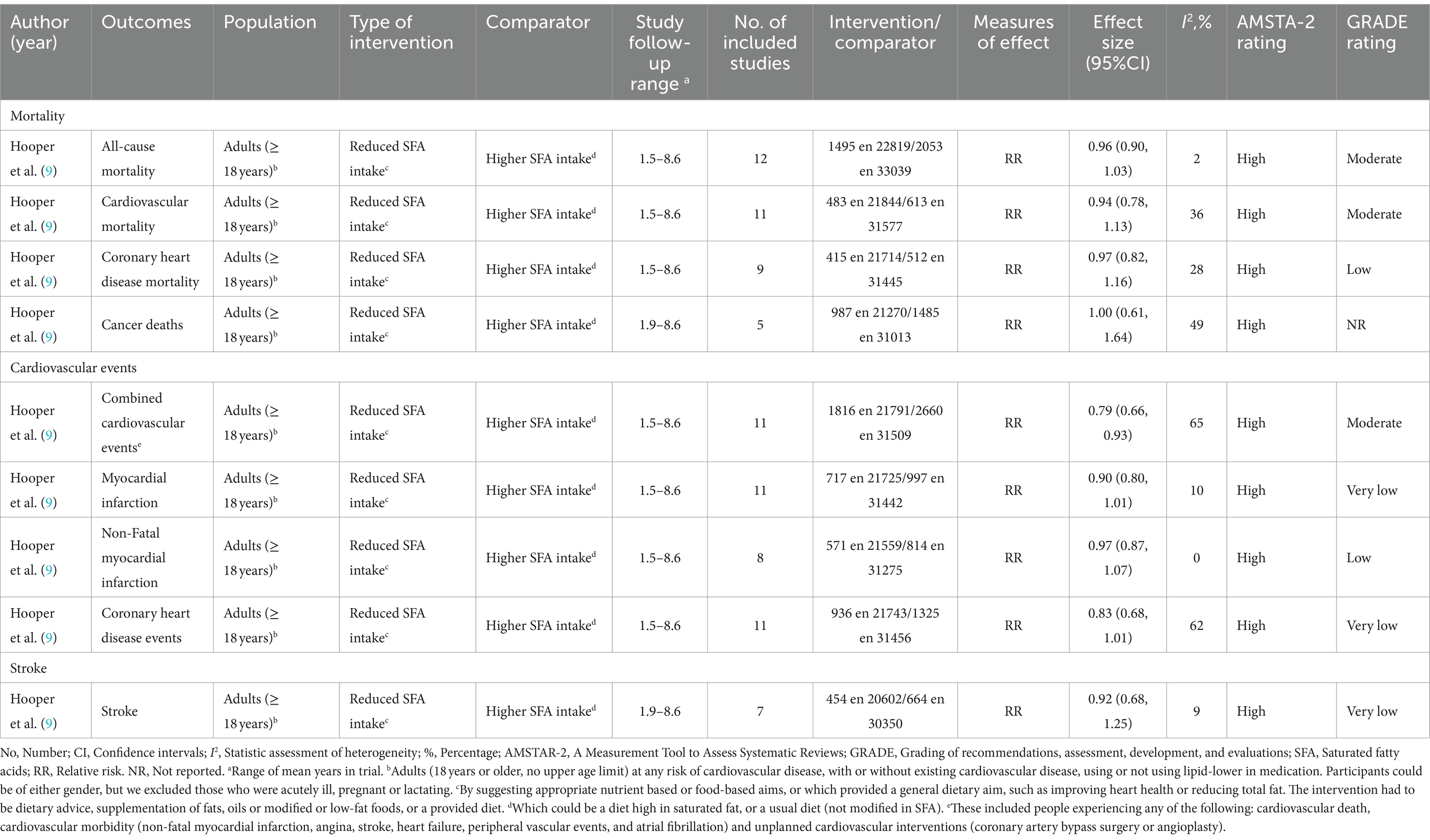
Table 2. Summary of primary findings of meta-analyses of randomized clinical trials studying saturated fat intake.
3.4.2 Meta-analyses of cohort studies
Five of the 19 associations (26.3%) were statistically significant (p < 0.05) based on random-effects models. The identified associations comprised one type of intervention/comparator: higher vs. reduced SFA intake. 18 associations analyzed non-repeated outcomes, including 12 (66.7%) cardiovascular and mortality events, five (27.8%) with a diagnosis of cancer, and one (5.5%) with a diagnosis of diabetes. Additionally, seven of the 17 associations (41.2%) had heterogeneity (I2) > 50%, and two (10.5%) of the 19 associations assessed the strength of evidence using GRADE (both were supported by very low certainty). Summary of all associations in Table 3 and Supplementary Table 7.
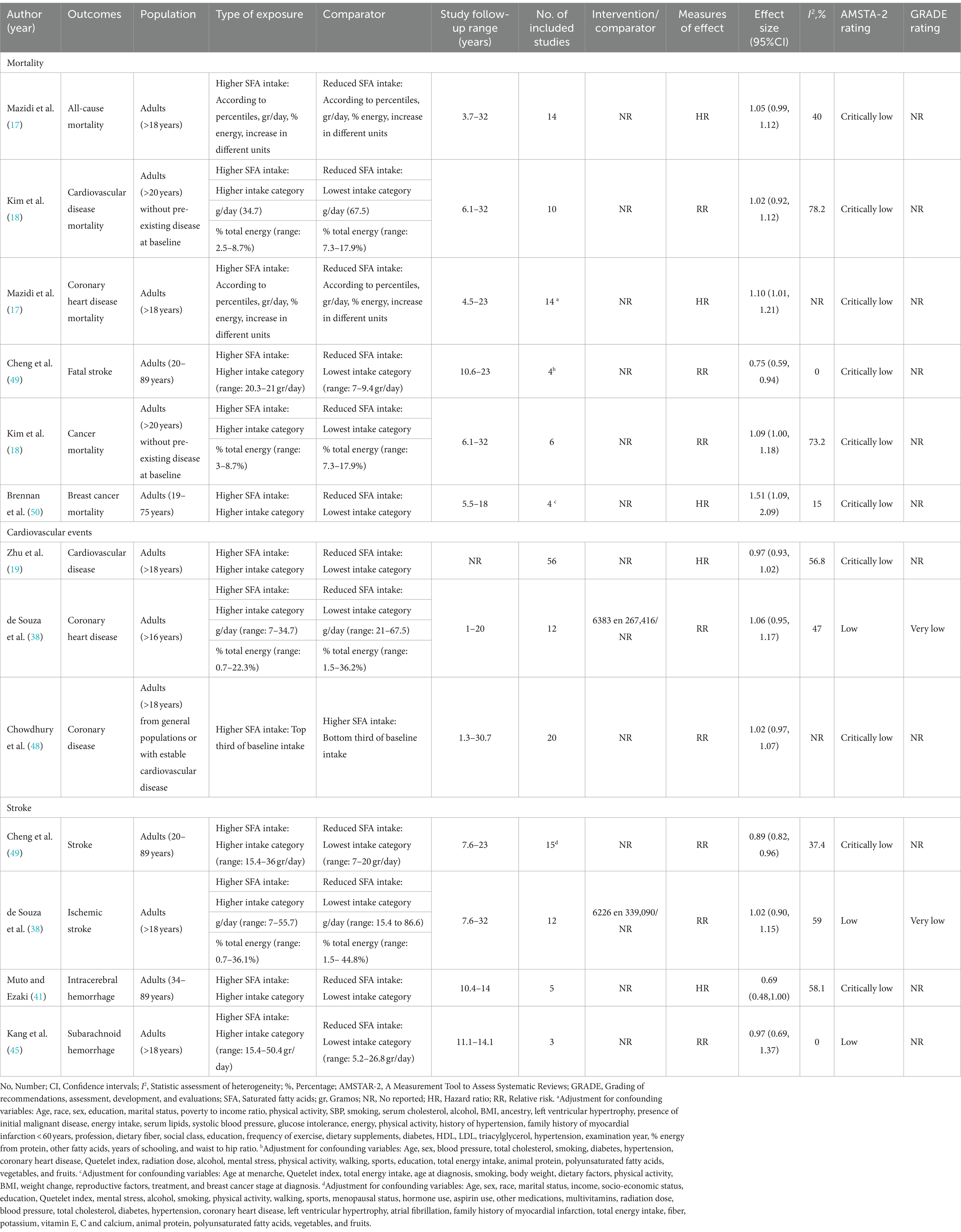
Table 3. Summary of primary findings of meta-analyses of cohorts studying saturated fat intake.
3.5 Findings of outcomes
3.5.1 Meta-analyses of RCTs
There was a 21% reduction in combined cardiovascular events in people who had reduced SFA compared with those on higher SFA intake (RR 0.79, 95%CI 0.66–0.93, I2 = 65%, 11 RCTs) (moderate certainty of evidence, GRADE) (9). We found no effect on all-cause mortality, cardiovascular mortality, cancer deaths, and other cardiovascular events such as myocardial infarction, coronary heart disease events, and stroke (moderate, low, and very low certainty of evidence, GRADE) (summary of the studies in Table 2 and Figure 2; and details of the GRADE assessment in Supplementary Table 8).
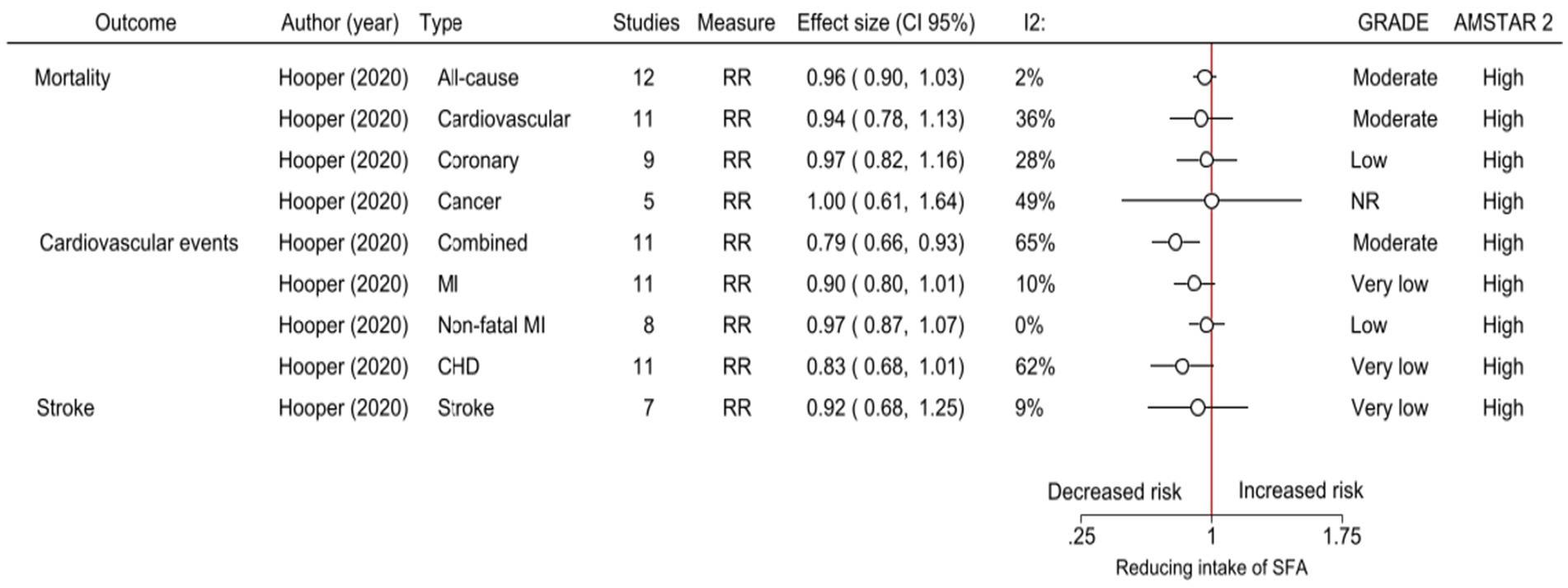
Figure 2. The effects of reduced intake of saturated fats as reported in meta-analyses of RCTs. CI, Confidence intervals; I2, Statistic assessment of heterogeneity; GRADE, Grading of recommendations, assessment, development, and evaluations; AMSTAR-2, A Measurement Tool to Assess Systematic Reviews; RR, Relative risk; MI, Myocardial infarction; CHD, Coronary heart disease; NR, No reported; and SFA, Saturated fatty acids.
About secondary outcomes, the certainty of evidence by GRADE was not reported. There was a reduction in total cholesterol (mean difference, MD, −0.24 mmol/L, 95% CI −0.36 to −0.13, I2 = 60%, 13 RCTs) and low-density lipoprotein cholesterol (LDL-C) (MD −0.19 mmol/L, 95% CI −0.33 to −0.05, I2 = 37%, five RCTs) in participants with reduced SFA compared to higher SFA (high quality, AMSTAR-2) (9). Also, there was a reduction in body weight (MD −1.77 kg, 95% CI −3.54 to −0.01, I2 = 77%, six RCTs), and body mass index (BMI) (MD −0.42 kg/m2, 95% CI −0.72 to −0.12, I2 = 62%, six RCTs) (high quality, AMSTAR-2) (9). Regarding the glucose-insulin homeostasis, there was a reduction in glucose tolerance test (GTT) after reducing SFA intakes compared to higher SFA (high quality, AMSTAR-2) (9). Replacing SFA with PUFAs or MUFAs lowered fasting glucose, hemoglobin A1c (HbA1c), C-peptide, and homeostatic model assessment of insulin resistance (HOMA-IR) (34). Furthermore, it enhanced insulin secretion capacity (based on acute insulin response) and increased fasting insulin levels (critically low quality, AMSTAR-2) (34). Only one RCT reported assessing quality of life, they found a small improvement in the group with lower SFA intake (high quality, AMSTAR-2) (9). Summary of all significant and nonsignificant associations in Table 2 and Supplementary Table 6.
3.5.2 Meta-analyses of cohort studies
The certainty of evidence evaluated by GRADE was not documented for certain outcomes. There was an increase in coronary heart disease mortality (HR 1.10, 95% CI 1.01–1.21, I2 = not reported, 14 cohort studies) (low quality, AMSTAR-2) (17) and breast cancer mortality (HR 1.51, 95% CI 1.09–2.09, I2 = 15%, four cohort studies) (critically low quality, AMSTAR-2) (50) in participants with higher SFA intake compared to reduce SFA (Table 3).
Among the two associations supported by very low certainty of evidence (GRADE) (38), we found no effect on coronary heart disease (follow-up range: 1–20 years) and ischemic stroke (follow-up range: 7.6–32 years) in participants with higher SFA intake compared to reduced SFA (details of the GRADE assessment in Supplementary Table 9). We also found no effect on all-cause mortality, cardiovascular disease mortality, cancer mortality, and others cardiovascular events as cardiovascular disease, intracerebral hemorrhage, and subarachnoid hemorrhage, with a follow-up range of 1.3–32 years (low and critically low quality, AMSTAR-2) (Table 3).
On the other hand, there was a reduction in fatal stroke (RR 0.75, 95% CI 0.59–0.94, I2 = 0, 4 cohort studies) (critically low quality, AMSTAR-2) (49) and stroke (RR 0.89, 95% CI 0.82–0.96, I2 = 37.4, 15 cohort studies) (critically low quality, AMSTAR-2) (49) in participants with higher SFA intake compared to reduce SFA (summary of the primary outcomes in Table 3 and Figure 3).
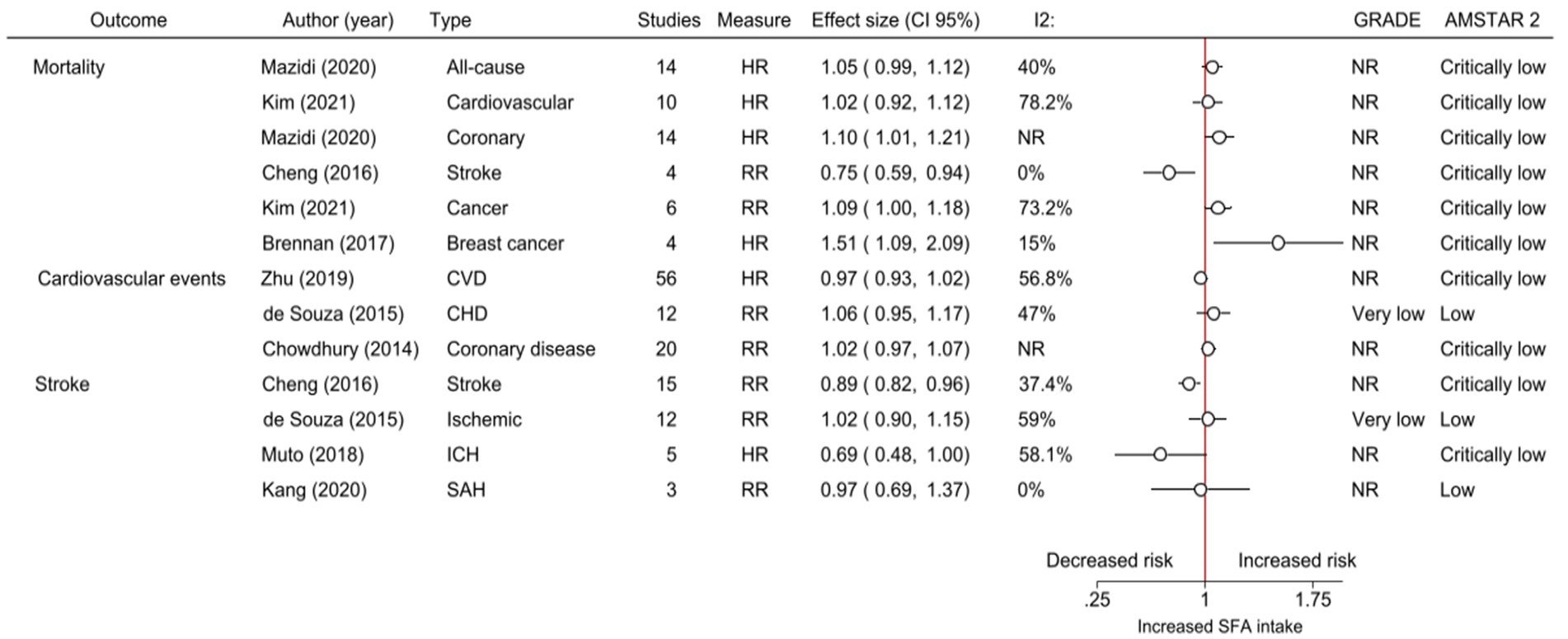
Figure 3. The effects of increased intake of saturated fats as reported in cohort meta-analyses. CI, Confidence intervals; I2, Statistic assessment of heterogeneity; GRADE, Grading of recommendations, assessment, development, and evaluations; AMSTAR-2, A Measurement Tool to Assess Systematic Reviews; HR, Hazard ratio; RR, Relative risk; CVD, Cardiovascular disease; CHD, Coronary heart disease; ICH, Intracerebral hemorrhage; SAH, Subarachnoid hemorrhage; NR, No reported; and SFA, Saturated fatty acids.
About secondary outcomes, there was an increase in liver cancer (RR 1.34, 95% CI 1.06–1.69, I2 = 16.9, 5 cohort studies) (critically low quality, AMSTAR-2) (36) in participants with higher SFA intake compared to reduce SFA (Supplementary Table 7).
In all significant outcomes, adjustment for confounding variables was performed. Summary of all significant and nonsignificant associations in Table 3 and Supplementary Table 7.
3.6 Sensitivity analyses
We have conducted sensitivity analyses, taking into account the potential impact of excluding outcomes due to overlap in cohort studies. We found similar results about mortality (there is no effect on all-cause mortality and cardiovascular disease mortality). In the context of stroke, participants with higher SFA intake experienced a reduction in stroke events compared to those with lower SFA intake. However, differences in the results were observed. While there is no effect on stroke mortality, there was a reduction in events related to stroke subtypes (ischemic and hemorrhagic) (Supplementary Table 10).
4 Discussion
Our findings indicate that the effect of reduction in SAF intake probably reduces cardiovascular events and other health outcomes. However, it has little or no effect on cardiovascular mortality and mortality from other causes. Additionally, we observed a reduction in lipid profile (total cholesterol and LDL-C), body weight, BMI, and an improvement in glucose-insulin homeostasis. Moreover, it could enhance the quality of life and reduce the risk of liver cancer. Finally, participants with higher SFA intake, compared to those with reduced SFA intake, may experience a decrease in fatal stroke and stroke events, as suggested by some observational studies.
In our study, we did not observe differences in mortality in RCTs, including both cardiovascular and other causes. However, we found a little effect in observational studies with wide in confidence intervals, such as Cheng et al. (fatal stroke) (49) and Brennan et al. (breast cancer mortality) (50). This suggests the mortality could occur with considerable variability in other countries or contexts. This could be due to the infrequency of the outcome and the small number of studies included, despite having a large study sample. Furthermore, discrepancies among studies could be attributable to the different biological effects produced by various types of saturated fatty acids, influenced by factors such as the food matrix and dietary carbohydrate content. Individual and methodology factors, including age, sex, adiposity levels, and the shorter follow-up time in RCTs, may also contribute to these variations (24–26, 51, 52). Consistent with our findings, the current recommendations from ACC, AHA, and ESC do not justify their decisions based on mortality results but instead aim to reduce the risk of ASCVD (5, 10, 11).
Regarding the risk of ASCVD, the CPGs recommendations are derived from a combination of observational studies and data from RCTs (5, 10, 11). However, our findings reveal heterogeneity results. In RCTs, we found significant differences observed when meta-analyzed and when creating a composite outcome that groups various types of cardiovascular events, without differences when meta-analyzed by outcome (9). ACC, AHA, and ESC (5, 10, 11) have taken a conservative approach and decided to recommend replacing SAF by PUFAs, principally. This decision was likely made, emphasizing that even a small percentage reduction in cardiovascular-related health outcomes can substantially decrease the number of people developing CVD, both nationally and globally, along with the associated healthcare costs (5). On the other hand, we observed a reduction in lipid profile, body weight, BMI, and an improvement in glucose-insulin homeostasis. This is compatible with the majority of published data about that (9, 34, 53, 54), and it could be another reason to justify the reduction of SAF intake. Additionally, it could enhance the quality of life and reduce risk of liver cancer, but it is necessary to have more studies to confirm it. Based on these issues, rather than having an universal recommendation, practitioners should give personalized recommendations, taking into account factors such as the habitual dietary patterns of individuals, nutritional status, income level, comorbidities, physical activity, and country-level nutrition data.
It is important to avoid recommendations based on low or very low-quality studies. This is crucial to prevent discordant recommendations, avoid harm to patient care, discourage future RCTs, minimize confusion and frustration among practitioners, and manage health system resources effectively, especially in LMCIs (30, 55). Furthermore, we should assess the benefits of interventions based on critical and important outcomes, avoiding reliance on surrogate measures (56).
In relation to stroke, observational studies suggest a decrease in both fatal stroke and overall stroke events with higher SFA intake. However, there is significant variability among the other studies (13, 17, 41, 45, 49), indicating a complex relationship and highlighting the need for further research to fully understand the underlying mechanisms. Another interesting and dual behavior can be observed with high-density lipoprotein cholesterol (HDL-C) levels. Classically, it is known that HDL-C is inversely associated with CVD risk (11). However, some studies report that very high levels of HDL-C may increase CVD risk and mortality (57, 58). Further clarification is needed in future studies.
4.1 Limitations and strengths
This study has limitations that are important to mention. First of all, due to the study design (umbrella review, where the unit of searching and data analysis is the systematic review rather than the primary study) (59), our intention was to provide a broad overview of the impact of SAF intake on cardiovascular disease. Our aim was not to evaluate this effect on an individual level, nor did we intend to assess all primary studies included in each meta-analysis. Instead, our focus has been on analyzing the methodology and findings of each systematic review, while acknowledging the inherent limitations in this approach. Secondly, despite conducting a systematic review, we were unable to make recommendations comparable to CPGs. High-quality evidence is the cornerstone of assessing the benefits and harms of an intervention. To maximize the trustworthiness of recommendations within the context of CPGs, they should be rigorously and transparently developed using a standardized methodology. This process should take into account expert opinions, as well as considerations of equity, resource utilization, acceptability, and feasibility (59). Third, we could not re-analyze the outcome data of the systematic reviews, as it was not an objective in our study protocol. Instead, we presented the outcome data exactly as they appear in the included systematic reviews. We believe that this overview format is the most appropriate and a feasible way to address our research question. Fourth, a minority of authors reported evaluations of the certainty of the evidence using the GRADE approach (17.8 and 10.5% of associations in meta-analyses of RCTs and observational studies). However, we assessed the quality of all systematic reviews included using the AMSTAR-2 tool. Finally, the maximum follow-up duration reported in RCTs was 9 years. To address concerns about the potential lack of time to obtain mortality outcomes, it may be necessary for RCTs to have a longer duration. On the other hand, systematic reviews of observational studies reported a maximum follow-up of 32 years. While differences in mortality were found in observational studies, these studies showed a small effect, imprecision, heterogeneity, and a high risk of bias. For all these reasons, our results are exploratory, and should be interpreted with caution.
The strength of this study includes a systematic and exhaustive search of the literature, inclusion of a large body of evidence, and the incorporation of systematic reviews of both RCTs and observational studies. Also, this study stands out as the first umbrella review that focuses on SAF intake’s impact on cardiovascular outcomes, considering data from both RCTs and observational studies.
5 Conclusion
This umbrella review found the reduction in SAF intake probably reduces cardiovascular events and other health outcomes. However, it has little or no effect on cardiovascular mortality and mortality from other causes. A healthy diet and physical activity remain the cornerstones of CVD prevention in all individuals. However, recommendations should be individualized considering factors such as nutritional status, comorbidities, and income level. Additionally, high-quality clinical trials with long-term follow-up are needed to investigate the effects of reduced SAF intake on cardiovascular-related health outcomes.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary material; further inquiries can be directed to the corresponding authors.
Author contributions
AA: Writing – original draft, Writing – review & editing. GD-M: Writing – original draft, Writing – review & editing. KC-Q: Writing – original draft, Writing – review & editing. KC: Writing – original draft, Writing – review & editing. GA-G: Writing – original draft, Writing – review & editing. KA-M: Writing – original draft, Writing – review & editing. CC: Writing – original draft, Writing – review & editing. CL: Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. The authors received financial support for the research as part of the “Centro de Promoción de Estilos de Vida Saludable” from the Instituto de Investigación Nutricional, Lima, Peru.
Acknowledgments
The authors would like to thank the support from the IIN for the conduct of this study. We thank Eda Franco and Yanina Archenti for their edits of this manuscript.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2024.1396576/full#supplementary-material
References
1. Xu, J, Murphy, SL, Kochanek, KD, and Arias, E. Mortality in the United States, 2021. NCHS Data Brief. (2022) 456:1–8.doi: 10.15620/cdc:122516
2. Nawsherwan,, Mubarik, S, Bin, W, Le, Z, Sang, M, Lin, Y, et al. Epidemiological trends in cardiovascular disease mortality attributable to modifiable risk factors and its association with sociodemographic transitions across BRICS-plus countries. Nutrients. (2023) 15:3757. doi: 10.3390/nu15173757
3. Rodzlan Hasani, WS, Muhamad, NA, Hanis, TM, Maamor, NH, Wee, CX, Omar, MA, et al. The burden of premature mortality from cardiovascular diseases: a systematic review of years of life lost. PLoS One. (2023) 18:e0283879. doi: 10.1371/journal.pone.0283879
4. Khaltaev, N, and Axelrod, S. Countrywide cardiovascular disease prevention and control in 49 countries with different socio-economic status. Chron Dis Transl Med. (2022) 8:296–304. doi: 10.1002/cdt3.34
5. Sacks, FM, Lichtenstein, AH, Wu, JHY, Appel, LJ, Creager, MA, Kris-Etherton, PM, et al. Dietary fats and cardiovascular disease: a presidential advisory from the American Heart Association. Circulation. (2017) 136:e1–e23. doi: 10.1161/cir.0000000000000510
6. Zhang, YB, Pan, XF, Chen, J, Cao, A, Xia, L, Zhang, Y, et al. Combined lifestyle factors, all-cause mortality and cardiovascular disease: a systematic review and meta-analysis of prospective cohort studies. J Epidemiol Community Health. (2021) 75:jech-2020-214050–99. doi: 10.1136/jech-2020-214050
7. Tsao, CW, Aday, AW, Almarzooq, ZI, Anderson, CAM, Arora, P, Avery, CL, et al. Heart disease and stroke statistics-2023 update: a report from the American Heart Association. Circulation. (2023) 147:e93–e621. doi: 10.1161/cir.0000000000001123
8. Siri-Tarino, PW, and Krauss, RM. Diet, lipids, and cardiovascular disease. Curr Opin Lipidol. (2016) 27:323–8. doi: 10.1097/mol.0000000000000310
9. Hooper, L, Martin, N, Jimoh OFKirk, C, Foster, E, and Abdelhamid, AS. Reduction in saturated fat intake for cardiovascular disease. Cochrane Database Syst Rev. (2020) 5:Cd011737. doi: 10.1002/14651858.CD011737.pub2
10. Arnett, DK, Blumenthal, RS, Albert, MA, Buroker, AB, Goldberger, ZD, Hahn, EJ, et al. 2019 ACC/AHA guideline on the primary prevention of cardiovascular disease: executive summary: a report of the American College of Cardiology/American Heart Association task force on clinical practice guidelines. Circulation. (2019) 140:e563–95. doi: 10.1161/cir.0000000000000677
11. Visseren, FLJ, Mach, F, Smulders, YM, Carballo, D, Koskinas, KC, Bäck, M, et al. 2021 ESC guidelines on cardiovascular disease prevention in clinical practice. Eur J Prev Cardiol. (2022) 29:5–115. doi: 10.1093/eurjpc/zwab154
12. Wang, DD, Li, Y, Chiuve, SE, Stampfer, MJ, Manson, JE, Rimm, EB, et al. Association of specific dietary fats with total and cause-specific mortality. JAMA Intern Med. (2016) 176:1134–45. doi: 10.1001/jamainternmed.2016.2417
13. Dehghan, M, Mente, A, Zhang, X, Swaminathan, S, Li, W, Mohan, V, et al. Associations of fats and carbohydrate intake with cardiovascular disease and mortality in 18 countries from five continents (PURE): a prospective cohort study. Lancet. (2017) 390:2050–62. doi: 10.1016/s0140-6736(17)32252-3
14. Chen, M, Li, Y, Sun, Q, Pan, A, Manson, JE, Rexrode, KM, et al. Dairy fat and risk of cardiovascular disease in 3 cohorts of US adults. Am J Clin Nutr. (2016) 104:1209–17. doi: 10.3945/ajcn.116.134460
15. Li, Y, Hruby, A, Bernstein, AM, Ley, SH, Wang, DD, Chiuve, SE, et al. Saturated fats compared with unsaturated fats and sources of carbohydrates in relation to risk of coronary heart disease: a prospective cohort study. J Am Coll Cardiol. (2015) 66:1538–48. doi: 10.1016/j.jacc.2015.07.055
16. Jakobsen, MU, O'Reilly, EJ, Heitmann, BL, Pereira, MA, Bälter, K, Fraser, GE, et al. Major types of dietary fat and risk of coronary heart disease: a pooled analysis of 11 cohort studies. Am J Clin Nutr. (2009) 89:1425–32. doi: 10.3945/ajcn.2008.27124
17. Mazidi, M, Mikhailidis, DP, Sattar, N, Toth, PP, Judd, S, Blaha, MJ, et al. Association of types of dietary fats and all-cause and cause-specific mortality: a prospective cohort study and meta-analysis of prospective studies with 1,164,029 participants. Clin Nutr. (2020) 39:3677–86. doi: 10.1016/j.clnu.2020.03.028
18. Kim, Y, Je, Y, and Giovannucci, EL. Association between dietary fat intake and mortality from all-causes, cardiovascular disease, and cancer: a systematic review and meta-analysis of prospective cohort studies. Clin Nutr. (2021) 40:1060–70. doi: 10.1016/j.clnu.2020.07.007
19. Zhu, Y, Bo, Y, and Liu, Y. Dietary total fat, fatty acids intake, and risk of cardiovascular disease: a dose-response meta-analysis of cohort studies. Lipids Health Dis. (2019) 18:91. doi: 10.1186/s12944-019-1035-2
20. Dayton, S, Pearce, ML, Hashimoto, S, Dixon, WJ, and Tomiyasu, U. A controlled clinical trial of a diet high in unsaturated fat in preventing complications of atherosclerosis. Circulation. (1969) 40:II-1–II-63. doi: 10.1161/01.CIR.40.1S2.II-1
21. Leren, P. The Oslo diet-heart study: eleven-year report. Circulation. (1970) 42:935–42. doi: 10.1161/01.cir.42.5.935
22. Miettinen, M, Turpeinen, O, Karvonen, MJ, Pekkarinen, M, Paavilainen, E, and Elosuo, R. Dietary prevention of coronary heart disease in women: the Finnish mental hospital study. Int J Epidemiol. (1983) 12:17–25. doi: 10.1093/ije/12.1.17
23. Miettinen, M, Karvonen, M, Turpeinen, O, Elosuo, R, and Paavilainen, E. Effect of cholesterol-lowering diet on mortality from coronary heart-disease and other causes: a twelve-year clinical trial in men and women. Lancet. (1972) 300:835–8. doi: 10.1016/S0140-6736(72)92208-8
24. Astrup, A, Magkos, F, Bier, DM, Brenna, JT, de Oliveira Otto, MC, Hill, JO, et al. Saturated fats and health: a reassessment and proposal for food-based recommendations: JACC state-of-the-art review. J Am Coll Cardiol. (2020) 76:844–57. doi: 10.1016/j.jacc.2020.05.077
25. Astrup, A, Teicholz, N, Magkos, F, Bier, DM, Brenna, JT, King, JC, et al. Dietary saturated fats and health: are the U.S. guidelines evidence-based? Nutrients. (2021) 13:3305. doi: 10.3390/nu13103305
26. Liu, X, Harding, SV, and Rideout, TC. Saturated fat and cardiovascular health: phenotype and dietary factors influencing interindividual responsiveness. Curr Atheroscler Rep. (2022) 24:391–8. doi: 10.1007/s11883-022-01014-w
27. Krauss, RM, and Kris-Etherton, PM. Public health guidelines should recommend reducing saturated fat consumption as much as possible: NO. Am J Clin Nutr. (2020) 112:19–24. doi: 10.1093/ajcn/nqaa111
28. Howick, J, Koletsi, D, Ioannidis, JPA, Madigan, C, Pandis, N, Loef, M, et al. Most healthcare interventions tested in cochrane reviews are not effective according to high quality evidence: a systematic review and meta-analysis. J Clin Epidemiol. (2022) 148:160–9. doi: 10.1016/j.jclinepi.2022.04.017
29. Yao, L, Guyatt, GH, and Djulbegovic, B. Can we trust strong recommendations based on low quality evidence? BMJ. (2021) 375:n2833. doi: 10.1136/bmj.n2833
30. Quincho-Lopez, A, Chávez-Rimache, L, Montes-Alvis, J, Taype-Rondan, A, and Alvarado-Gamarra, G. Characteristics and conflicting recommendations of clinical practice guidelines for COVID-19 management in children: a scoping review. Travel Med Infect Dis. (2022) 48:102354. doi: 10.1016/j.tmaid.2022.102354
31. Moher, D, Liberati, A, Tetzlaff, J, and Altman, DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. (2009) 6:e1000097. doi: 10.1371/journal.pmed.1000097
32. Lunny, C, Pieper, D, Thabet, P, and Kanji, S. Managing overlap of primary study results across systematic reviews: practical considerations for authors of overviews of reviews. BMC Med Res Methodol. (2021) 21:140. doi: 10.1186/s12874-021-01269-y
33. Shea, BJ, Reeves, BC, Wells, G, Thuku, M, Hamel, C, Moran, J, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. (2017) 358:j4008. doi: 10.1136/bmj.j4008
34. Imamura, F, Micha, R, Wu, JH, de Oliveira Otto, MC, Otite, FO, Abioye, AI, et al. Effects of saturated fat, polyunsaturated fat, monounsaturated fat, and carbohydrate on glucose-insulin homeostasis: a systematic review and meta-analysis of randomised controlled feeding trials. PLoS Med. (2016) 13:e1002087. doi: 10.1371/journal.pmed.1002087
35. Hannon, BA, Thompson, SV, An, R, and Teran-Garcia, M. Clinical outcomes of dietary replacement of saturated fatty acids with unsaturated fat sources in adults with overweight and obesity: a systematic review and meta-analysis of randomized control trials. Ann Nutr Metab. (2017) 71:107–17. doi: 10.1159/000477216
36. Zhao, L, Deng, C, Lin, Z, Giovannucci, E, and Zhang, X. Dietary fats, serum cholesterol and liver cancer risk: a systematic review and meta-analysis of prospective studies. Cancers (Basel). (2021) 13:1580. doi: 10.3390/cancers13071580
37. Zhao, J, Lyu, C, Gao, J, Du, L, Shan, B, Zhang, H, et al. Dietary fat intake and endometrial cancer risk: a dose response meta-analysis. Medicine (Baltimore). (2016) 95:e4121. doi: 10.1097/md.0000000000004121
38. de Souza, RJ, Mente, A, Maroleanu, A, Cozma, AI, Ha, V, Kishibe, T, et al. Intake of saturated and trans unsaturated fatty acids and risk of all cause mortality, cardiovascular disease, and type 2 diabetes: systematic review and meta-analysis of observational studies. BMJ. (2015) 351:h3978. doi: 10.1136/bmj.h3978
39. Qiu, W, Lu, H, Qi, Y, and Wang, X. Dietary fat intake and ovarian cancer risk: a meta-analysis of epidemiological studies. Oncotarget. (2016) 7:37390–406. doi: 10.18632/oncotarget.8940
40. Neuenschwander, M, Barbaresko, J, Pischke, CR, Iser, N, Beckhaus, J, Schwingshackl, L, et al. Intake of dietary fats and fatty acids and the incidence of type 2 diabetes: a systematic review and dose-response meta-analysis of prospective observational studies. PLoS Med. (2020) 17:e1003347. doi: 10.1371/journal.pmed.1003347
41. Muto, M, and Ezaki, O. High dietary saturated fat is associated with a low risk of intracerebral hemorrhage and ischemic stroke in Japanese but not in non-Japanese: a review and meta-analysis of prospective cohort studies. J Atheroscler Thromb. (2018) 25:375–92. doi: 10.5551/jat.41632
42. Lodi, M, Kiehl, A, Qu, FL, Gabriele, V, Tomasetto, C, and Mathelin, C. Lipid intake and breast cancer risk: is there a link? A new focus and meta-analysis. Eur J Breast Health. (2022) 18:108–26. doi: 10.4274/ejbh.galenos.2021.2021-11-2
43. Kim, M, and Park, K. Dietary fat intake and risk of colorectal Cancer: a systematic review and Meta-analysis of prospective studies. Nutrients. (2018) 10:1963. doi: 10.3390/nu10121963
44. Khodavandi, A, Alizadeh, F, and Razis, AFA. Association between dietary intake and risk of ovarian cancer: a systematic review and meta-analysis. Eur J Nutr. (2021) 60:1707–36. doi: 10.1007/s00394-020-02332-y
45. Kang, ZQ, Yang, Y, and Xiao, B. Dietary saturated fat intake and risk of stroke: systematic review and dose-response meta-analysis of prospective cohort studies. Nutr Metab Cardiovasc Dis. (2020) 30:179–89. doi: 10.1016/j.numecd.2019.09.028
46. Harcombe, Z, Baker, JS, and Davies, B. Evidence from prospective cohort studies does not support current dietary fat guidelines: a systematic review and meta-analysis. Br J Sports Med. (2017) 51:1743–9. doi: 10.1136/bjsports-2016-096550
47. Gaeini, Z, Bahadoran, Z, and Mirmiran, P. Saturated fatty acid intake and risk of type 2 diabetes: an updated systematic review and dose-response meta-analysis of cohort studies. Adv Nutr. (2022) 13:2125–35. doi: 10.1093/advances/nmac071
48. Chowdhury, R, Warnakula, S, Kunutsor, S, Crowe, F, Ward, HA, Johnson, L, et al. Association of dietary, circulating, and supplement fatty acids with coronary risk: a systematic review and meta-analysis. Ann Intern Med. (2014) 160:398–406. doi: 10.7326/m13-1788
49. Cheng, P, Wang, J, Shao, W, Liu, M, and Zhang, H. Can dietary saturated fat be beneficial in prevention of stroke risk? A meta-analysis. Neurol Sci. (2016) 37:1089–98. doi: 10.1007/s10072-016-2548-3
50. Brennan, SF, Woodside, JV, Lunny, PM, Cardwell, CR, and Cantwell, MM. Dietary fat and breast cancer mortality: a systematic review and meta-analysis. Crit Rev Food Sci Nutr. (2017) 57:1999–2008. doi: 10.1080/10408398.2012.724481
51. Billingsley, HE, Carbone, S, and Lavie, CJ. Dietary fats and chronic noncommunicable diseases. Nutrients. (2018) 10:1385. doi: 10.3390/nu10101385
52. Givens, DI. Saturated fats, dairy foods and cardiovascular health: no longer a curious paradox? Nutr Bull. (2022) 47:407–22. doi: 10.1111/nbu.12585
53. Mensink, RP (2016). Effects of saturated fatty acids on serum lipids and lipoproteins: A systematic review and regression analysis. Available at: https://apps.who.int/iris/bitstream/handle/10665/246104/9789241565349-eng.pdf?sequence=1 (Accessed December 21, 2023).
54. Guasch-Ferré, M, Satija, A, Blondin, SA, Janiszewski, M, Emlen, E, O’Connor, LE, et al. Meta-analysis of randomized controlled trials of red meat consumption in comparison with various comparison diets on cardiovascular risk factors. Circulation. (2019) 139:1828–45. doi: 10.1161/CIRCULATIONAHA.118.035225
55. Woolf, SH, Grol, R, Hutchinson, A, Eccles, M, and Grimshaw, J. Clinical guidelines: potential benefits, limitations, and harms of clinical guidelines. BMJ. (1999) 318:527–30. doi: 10.1136/bmj.318.7182.527
56. Guyatt, GH, Oxman, AD, Kunz, R, Woodcock, J, Brozek, J, Helfand, M, et al. GRADE guidelines: 8. Rating the quality of evidence--indirectness. J Clin Epidemiol. (2011) 64:1303–10. doi: 10.1016/j.jclinepi.2011.04.014
57. Razavi, AC, Jain, V, Grandhi, GR, Patel, P, Karagiannis, A, Patel, N, et al. Does elevated high-density lipoprotein cholesterol protect against cardiovascular disease? J Clin Endocrinol Metab. (2024) 109:321–32. doi: 10.1210/clinem/dgad406
58. Faaborg-Andersen, CC, Liu, C, Subramaniyam, V, Desai, SR, Sun, YV, Wilson, PWF, et al. U-shaped relationship between apolipoprotein A1 levels and mortality risk in men and women. Eur J Prev Cardiol. (2023) 30:293–304. doi: 10.1093/eurjpc/zwac263
59. Pollock, M FR, Becker, LA, Pieper, D, and Hartling, L (2023). Cochrane handbook for systematic reviews of interventions version 6.4. Chapter V: Overviews of Reviews. Available at: https://training.cochrane.org/handbook/current/chapter-v (Accessed December 15, 2023).
Keywords: adult, cardiovascular diseases, fatty acids, dietary fats, mortality
Citation: Aramburu A, Dolores-Maldonado G, Curi-Quinto K, Cueva K, Alvarado-Gamarra G, Alcalá-Marcos K, Celis CR and Lanata CF (2024) Effect of reducing saturated fat intake on cardiovascular disease in adults: an umbrella review. Front. Public Health. 12:1396576. doi: 10.3389/fpubh.2024.1396576
Edited by:
Maroof Alam, University of Michigan, United StatesReviewed by:
Nihal Medatwal, Stony Brook University, United StatesAzaj Ahmed, The University of Iowa, United States
Copyright © 2024 Aramburu, Dolores-Maldonado, Curi-Quinto, Cueva, Alvarado-Gamarra, Alcalá-Marcos, Celis and Lanata. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Adolfo Aramburu, YWFyYW1idXJ1QGlpbi5zbGQucGU=; Giancarlo Alvarado-Gamarra, YWFsdmFyYWRvQGlpbi5zbGQucGU=