
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Public Health, 25 June 2024
Sec. Public Mental Health
Volume 12 - 2024 | https://doi.org/10.3389/fpubh.2024.1393729
This article is part of the Research TopicParents with Mental and/or Substance Use Disorders and their Children, Volume IIIView all 33 articles
 Philipp Schöch1,2
Philipp Schöch1,2 Laura Hölzle1,2
Laura Hölzle1,2 Astrid Lampe3
Astrid Lampe3 Christine Hörtnagl1
Christine Hörtnagl1 Ingrid Zechmeister-Koss4
Ingrid Zechmeister-Koss4 Anna Buchheim2
Anna Buchheim2 Jean Lillian Paul1*
Jean Lillian Paul1*Background: Paternal perinatal mental illness (PPMI), which affects around one in 10 fathers, is under-recognised despite increasing awareness of men’s mental health in the perinatal period. Social stigma and men’s reluctance to seek help exacerbate this gap. Neglecting the mental health needs of new fathers not only puts them at increased risk for mental illness themselves, but also has a profound and long-lasting impact on their families, children and their own self-esteem as they navigate their new role in the family dynamic.
Objective: This meta-review systematically identifies instruments assessing PPMI symptoms, evaluates their psychometric properties and applicability, presents key findings from studies using these tools, and identifies gaps and limitations in the literature on PPMI symptom assessment.
Methods: A systematic literature review was conducted using search strategies applied to PubMed, PsycNet APA, Cochrane, and Web of Science, supplemented by hand searches. Relevant information was extracted from each included study. Extracted data were analysed narratively to address the research questions.
Results: Findings identified limitations and gaps in current screening practices. While the Edinburgh Postnatal Depression Scale (EPDS) is the most widely used screening tool for both fathers and mothers, it inadequately captures atypical depressive symptoms in men. Cutoff scores lack consensus, and instrument sensitivity varies significantly due to cultural and sociodemographic factors. A number of other screening tools have been identified, most of which are more general and not specifically designed for perinatal mental health.
Conclusion: This meta-review broadens perspectives on PPMI screening instruments, highlighting key themes, patterns, and differences across the included reviews. While a variety of screening tools are used, the review underscores the necessity for tools specifically tailored to fathers during the perinatal period.
In recent years, there has been a growing acknowledgment of the significance of paternal perinatal mental illness (PPMI) within perinatal research (1). This emerging research emphasizes the critical need for early identification and support for fathers experiencing psychological disorders during their partner’s pregnancy to 1 year postpartum. There is also a growing acknowledgment of the profound impact the transition to parenthood has on paternal mental health and overall family well-being (2). Fatherhood has undergone a significant transformation, particularly in western societies, from rigid, traditional gender roles to a more flexible framework characterised by negotiation and adaptation of parental responsibilities within families (3). While acknowledging the diversity of fathering experiences, it is clear that cultural norms influence parenting roles differently across regions. For example, in countries such as Sweden, active parenting, including shared parental leave and childcare involvement, is typical, while in countries such as Spain, traditional gender roles often persist (4). Active fatherhood is influenced by institutional frameworks such as parental leave policies, cultural norms and values, company culture, as well as individual and partnership factors (5). In Austria, fathers are increasingly acknowledged as crucial participants in family care. However, despite positive shifts in attitudes, their actual involvement remains limited, with only 17% taking parental leave. Traditional gender roles and societal norms serve as significant barriers, highlighting the need for stronger policy measures to encourage a more equitable sharing of family responsibilities (6). Nevertheless, there is a discernible trend across contemporary Western societies where fathers are actively challenging traditional societal expectations. This trend is characterized by a more equitable sharing of housework, childcare, and work responsibilities (7). This societal shift reflects evolving norms and the dynamic nature of family structures. As fathers strive to balance the demands of work and family life, they are prioritising meaningful engagement with their children, contributing to a more equitable distribution of parental roles. This increased involvement highlights the importance of paternal mental health, particularly during the perinatal period, as fathers take on more active parenting roles.
PPMI is associated with an increased risk of inter-parental conflict, higher relationship dissatisfaction, and potential difficulties in infant temperament, highlighting the broader negative impact on family functioning (8). When fathers are emotionally unavailable, it can create tensions within the family dynamics and which may lead to emotional neglect in children, impacting children’s self-esteem, emotional regulation, and social skills development. Additionally, children may develop insecure attachment styles and struggle to form trusting relationships as adults. Emotionally unavailable fathers may inadvertently model unhealthy emotional behaviours or reinforce gender stereotypes, affecting children’s understanding of gender roles (9).
A meta-analysis by Cameron et al. (10) estimated the prevalence of paternal depression during their partner’s pregnancy and up to 1 year postpartum to be around 8%. Depression rates seemed to be higher in the third to sixth months postpartum period and lower during the second trimester of pregnancy. It is important to note that these estimates only include depression and not other types of mental health problems during this period. Other studies that examined diagnosed mental health problems and above-threshold symptoms found that approximately 5–10% of fathers had perinatal depression, and approximately 5–15% experienced perinatal anxiety (10–12).
Still, Fisher et al. (2) suggests that PPMI may be underestimated because men are less likely to report traditional symptoms of depression and may express depression differently for example, by engaging in harmful coping behaviours, such as aggression, substance use, and suicide. Using traditional measures to screen for depression in fathers may give an inaccurate picture of their mental health. Psouni et al. (13) also highlighted a considerable variation in the reported prevalence of paternal postpartum depression (PPPD), which they attribute to a lack of uniform assessment for PPPD, lack of consensus regarding the time period to be considered, or uncertainty about whether minor depression, as defined by DSM-IV (14), should be included.
The study of Psouni et al. (13) underscores the prevalence of “depressive equivalents” in fathers’ symptoms, serving as counterparts to traditional indicators of depression. This implies that an assessment tool, incorporating both typical depression and externalizing (depressive equivalent) symptoms may be more appropriate for evaluating paternal depression. Strikingly, Psouni et al. (13) showed that 83% of fathers scoring above the BDI-II (Beck Depression Inventory II) cut-off for suspected depression had not disclosed their condition to a healthcare professional.
Identifying and addressing PPMI is complicated by various barriers to help-seeking that have been identified, including misconceptions and lack of knowledge about paternal perinatal depression (PPPD), adherence to masculine norms, and the stigma surrounding PPPD (15, 16). Findings from Pedersen et al. (16) interview study indicate that adherence to masculine ideals and parental inequality within the family and healthcare system hinder fathers’ help-seeking behavior. They argue that feelings of being the secondary parent could question the father’s legitimacy for his own mental healthcare needs. Psouni et al. (13) revealed that a significant percentage of fathers experiencing depressive symptoms avoid seeking professional help. That is consistent with the observed low help-seeking behavior commonly observed in men with depression (17).
Evidence suggests that fathers may manifest depressive symptoms differently to mothers, necessitating an exploration of available screening tools to better capture PPMI. The primary aim of this paper is to analyze existing reviews of screening tools to assess paternal mental health during their partner’s pregnancy and the first year postpartum, and to examine the instruments used. It seeks evidence on the reliability and validity of these instruments, while identifying limitations, potential biases and research gaps in the literature on PPMI assessment.
To address the research objective, a systematic review was conducted, adhering to the PRISMA guidelines (18). Given the significant heterogeneity in study designs and outcomes among the included reviews on screening tools for PPMI, a meta-review as described by Hunt et al. (19) and using a narrative synthesis approach was selected and considered appropriate. We used narrative synthesis (20) to qualitatively summarize and compare the findings and characteristics of the reviews without attempting to combine their results quantitatively.
The following databases were searched for relevant articles: PubMed, PsycNet APA, Cochrane, and Web of Science. The search was conducted across all time periods until August 30, 2023, to ensure the inclusion of the recent and relevant studies. A systematic literature search was conducted using the following search strategy, with a combination of keywords and phrases related to PPMI and screening tools:
((“paternal” OR “father*” OR “dad”) AND (“perinatal mental health” OR “postpartum depression” OR “post-partum”)) AND ((“screen*” OR “identif*” OR “specific measure”) AND (“depression” OR “anxiety” OR “stress” OR “well-being”)) AND (“systematic” OR “meta-analysis” OR “review”).
After screening retrieved articles at the title and abstract level for relevance, those deemed potentially eligible were selected for full-text review (PS). Subsequently, a second reviewer (LH) independently reviewed the identified articles to verify their eligibility for inclusion. Utilizing the eligibility criteria outlined below, both primary reviewer (PS) and second reviewer (LH) independently assessed the full-text articles for inclusion. Any discrepancies or uncertainties regarding study inclusion were resolved through consensus discussion between PS and LH to ensure adherence to the eligibility criteria.
Studies were included if they met the following criteria:
• Reviewed screening tools for fathers and/or partners during the perinatal period.
• Were published as systematic reviews, meta-analyses, or reviews.
Studies were excluded if they:
• Were not written in English.
• Were conference abstracts or non-peer-reviewed publications.
• Did not specifically focus on PPMI screening.
• Did not provide sufficient information on the screening tools assessed.
Data were systematically extracted from included reviews to provide a comprehensive overview on the assessment of PPMI. Data exctracted included: author names, publication years, study countries, number of primary studies, research focus, key results, instrument-specific findings, and included instruments. To synthesize the extracted data, we used a narrative approach was employed, focusing on identifying patterns and gaps in the literature regarding screening practices for PPMI. This synthesis aimed to distill the collective insights from the included reviews and to provide a narrative on the current research landscape of PPMI screening.
The quality assessment of the included systematic reviews, meta-analyses, and reviews was conducted by both primary reviewer (PS) and second reviewer (LH) using the AMSTAR 2 Tool (21). This tool was selected for its capability to enhance the transparency and reliability of the quality assessment process. Both PS and LH independently assessed the methodological quality of each included study using the AMSTAR 2 criteria, and any discrepancies or uncertainties were resolved through consensus discussion to ensure consistency and accuracy in the assessment.
A narrative synthesis (20) was chosen as it is versatile, suitable for various review questions, and for its ability to synthesize and interpret findings from multiple studies, particularly when a statistical meta-analysis may not be feasible. To organize the findings from the included reviews, we utilized tables to outline their specific characteristics, facilitating the identification of patterns. In structuring our analysis, we opted to identify overarching themes and center the description around these emergent themes, rather than adhering strictly to predefined data categories. We believe this approach provides a comprehensive understanding of the literature and that synthesizing and interpreting findings allows to generate insights beyond the mere aggregation of data points, thus enriching the overall narrative.
The electronic searches identified 119 records (see Figure 1). In addition, two further records were identified through a supplementary search, resulting in 102 records after removing duplicates. Screening at the title/abstract level resulted in 16 records being obtained in full, with six studies ultimately included in the review.
Figure 1. Modified PRISMA flow diagram based on Page et al. (18)
A total of six reviews (1, 4, 22–25) were included in this meta-review (see Table 1). These were published between 2015 and 2022. They collectively examined 167 primary studies published from 1987 to 2021 and indicating a surge in research over the last decade. Although studies have been conducted around the world, many were concentrated in Europe (75), the United States (23), and Australia (17). Within Europe, there was a notable concentration of research from the United Kingdom (15), Sweden (12) and Italy (10). The scope of the reviews primarily focused on screening tools for paternal mental health during both the prenatal and postnatal periods, with one review additionally considering other co-parents and partners.
Table 1. Characteristics of included reviews.
The systematic data extraction and narrative analysis conducted as part of this meta-review identified a diverse range of screening tools utilized in the assessment of PPMI (see Table 2). The analysis involved a detailed examination of various dimensions extracted from included reviews, including study countries, number of primary studies, research focus, key results, instrument-specific findings, and included instruments. This analysis highlights details about the instruments utilized, their characteristics, and measurement properties, providing specific findings regarding the performance of these instruments in detecting symptoms of PPMI. The analysis revealed notable variations in the use and efficacy of different screening instruments across studies. Furthermore, the analysis identified limitations of currently used screening tools and areas demanding further investigation to enhance screening practices for PPMI.
Table 2. Overview of screening instruments mentioned in included reviews.
The AMSTAR 2 assessment revealed mixed methodological rigour among the reviewed studies. While some showed strengths in protocol clarity, comprehensive searches, and detailed study descriptions, others were lacking in areas such as protocol transparency, duplicate data extraction, and bias assessment (see Tables 3, 4). Notably, Shafian et al. (25) demonstrated robust methodology, including rigorous statistical analysis, likely due to its inclusion of a quantitative meta-analysis.
Table 3. AMSTAR 2 assessment.
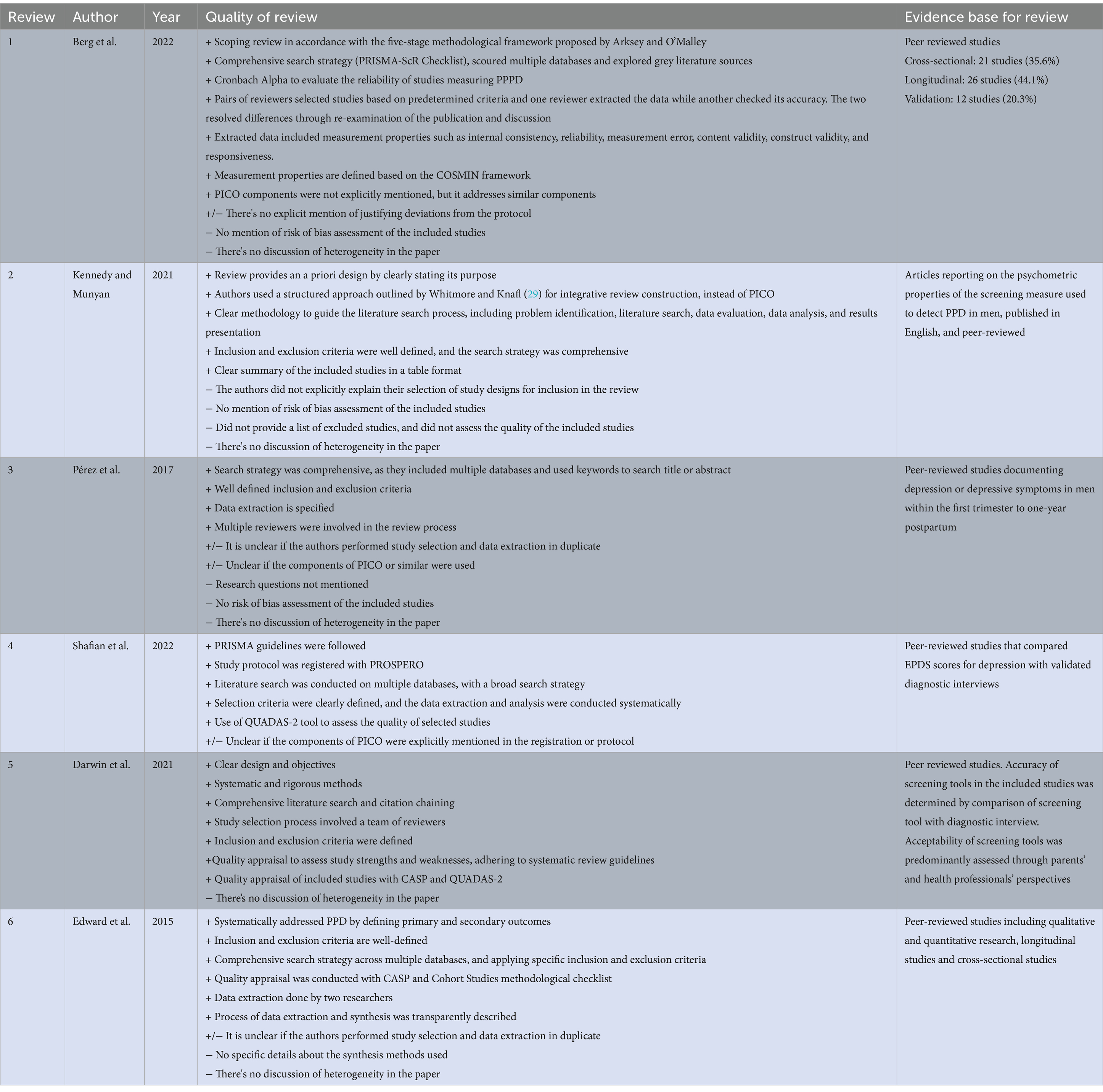
Table 4. Additional information on AMSTAR 2 quality assessment of included reviews.
The Edinburgh Postnatal Depression Scale (EPDS) has been analysed in nearly every single study of the included reviews, and can be considered the primary screening tool for evaluating PPMI and associated mental health concerns in fathers or partners throughout the perinatal phase (see Table 1). The EPDS is a 10-item self-report instrument that takes approximately 5 min to complete and is designed to assess mood and emotional wellbeing in the postpartum period. Scores range from 0 to 30, with 10 or more points suggesting the possibility of depression of varying severity (26). Three other widely used instruments for assessing the mental health of new fathers are: Beck Depression Inventory (BDI), Center for Epidemiologic Studies Depression Scale (CES-D), and Patient Health Questionnaire (PHQ). The BDI (27), although not tailored for the perinatal period, comprises 21 questions designed to assess the severity of depressive symptoms. In contrast, the CES-D (28), which encompasses 20 questions, serves as a comprehensive self-reported questionnaire for assessing depressive symptoms in community populations. It covers cognitive, somatic, and psychological aspects and is also valuable for screening new fathers. The PHQ, including its various versions such as the PHQ-9 (30), is a widely used screening tool for assessing depression severity. The PHQ-9 consists of nine questions specifically designed to evaluate depressive symptoms experienced over the past 2 weeks. While the BDI, CES-D, and PHQ-9 are not explicitly designed for perinatal mental health, the included reviews showed that they can be useful to screen for depression symptoms in fathers or partners during the perinatal period.
While various screening tools have been examined, few were specifically designed to detect postpartum depression (PPPD), with only two targeting male symptomatology: the Perinatal Assessment of Paternal Affectivity (PAPA) and the Gotland Male Depression Scale (GMDS). The GMDS has demonstrated effectiveness comparable to the EPDS in identifying PPPD using a cutoff score of ≥13. A Danish study described the reliability of the GMDS as fair to moderate, with a Cohen’s kappa (κ) value of 0.49, indicating some agreement with the EPDS in identifying PPPD. Additionally, a Swedish study found a moderate correlation between the GMDS and the EPDS (r = 0.76) (1). However, research suggests that neither the GMDS nor the EPDS alone are sufficient for screening males in the postpartum period (24). Data on the sensitivity and specificity of the PAPA tool are limited, as only one study reviewed by Berg et al. (1) analyzed its performance. This study, conducted in Portugal, reported high internal consistency for the PAPA (0.91 antenatal, 0.90 postnatal) and significant correlation with the EPDS, with cutoffs of ≥95 for PAPA-AN and ≥92 for PAPA-PN.
The EPDS is the most extensively studied and validated tool for assessing postpartum depression in both men and women. In Berg et al. (1) review, they found that the EPDS exhibited internal consistency, with a Cronbach’s alpha exceeding 0.70 in 34 out of 38 studies. While an alpha above 0.70 is typically considered acceptable, it is important to consider the context of the EPDS’s 10-item scale, as this may influence the interpretation of these findings. Across all other instruments considered in Berg’s review, internal consistency values ranged from 0.60 to 0.91. Cutoff scores used to detect depression varied across their studies, with the EPDS having optimum cutoff scores from 5 to 13 for fathers. Despite variations in cutoff points, most studies indicated that the EPDS performed as well as or better than other assessment tools when used for fathers. In Shafian’s et al. (25) review, they recommended focusing on the determination of the appropriate cut-off score for EPDS, and that clinicians should use a lower score between 7 to 10, because it appears to strike a balance between sensitivity and specificity when screening for PPPD.
Despite those findings and suggestions, the determination of an ideal cutoff point for the EPDS, as well as for various other available screening instruments, remains a matter of debate in the reviewed studies. Kennedy and Munyan (24) observed cultural variations in recommended cutoff scores for depression screening instruments, and highlighted the importance of considering context-specific factors. It is important to mention that the absence of gender-specific items in the EPDS may lead to under-detection of symptoms in fathers. Berg et al. (1) addressed the lack of gender-specific items in screening tools and concluded that it is unclear whether they uniquely identify symptoms of depression or a broader state of mind, including distress and anxiety. However, Edward et al. (23) noted that the EDPS is a suitable screening tool that could alert a clinician to the need for a full diagnostic interview.
Kennedy and Munyan (24) highlighted that modern fathers experience increased expectations and responsibilities during the 3 to 4-month postpartum period, including childcare, housework, which is changing their previous social role, while also being perceived as the main income providers. Balancing family life and work demands can lead to distress more often than depression. This distress is characterized by feelings of being overwhelmed, helpless, anxious, irritable, self-blaming, using avoidant/escapist activities (e.g., sports, overworking, excessive time on internet/TV, gambling, substance use), and aggressiveness that may be under detected by traditional depression screenings. The analyzed reviews suggest that the EPDS is sensitive to symptoms of depression and distress, but may be less sensitive to depression itself, especially in fathers. The reviews included in this study show the evident value of using multiple screening tools to assess PPPD to enhance sensitivity and specificity. It also indicates the likeliness that neither scale alone is sufficient for depression screening in new fathers. In this context, Psouni et al. (13) showed that a modified EPDS with GMDS items had greater sensitivity than the EPDS alone.
Another study by Tran et al. (31) highlighted that, while all measures had acceptable reliability, the sensitivity of the EPDS in men was significantly lower than in women. Reviewed studies suggest using lower EPDS cut-off scores for PPPD compared to maternal depression. In this context, the crying item of the EPDS is suggested as one item which could for example lead to underreporting due to gendered differences. Societal expectations and gender differences in emotional expression may lead fathers to underreport or express their distress differently than mothers, making this item less reliable for fathers. Shafian et al. (25) noted that their reviewed studies recommend a lower EPDS cutoff score for fathers in comparison to mothers. However, they stated that the result should be interpreted with caution due to the influence of diverse factors such as culture, socioeconomic status, education, and societal context. Moreover, they stressed that the timing of EPDS administration and variations in how male depression is expressed across different cultures can impact EPDS scores.
This meta-review identified significant variation in the reported prevalence rates of PPMI across the included studies. Pérez et al. (4) conducted a review encompassing 52 single studies and identified prevalence rates based on applied screening tools ranging from as low as 1.8% to as high as 47%, with a mean prevalence of 11.9%. Other included reviews showed similar results, and based on their findings, this wide variation in prevalence can be associated with the screening tool used, diagnostic criteria, and timing of assessment. In regards to the EPDS, sensitivity and specificity showed significant variation across studies for different cutoff scores, with sensitivity ranging from 40 to 100% and specificity from 47.8 to 100%, as demonstrated by Shafian et al. (25). Additionally, the timing of assessments varied across studies, with some focusing on depressive symptoms during partner’s pregnancy and others during the postpartum period. Pérez et al. (4) for example showed in their review that prevalence in Turkey is the lowest and is much higher in Sweden. This is an important observation, as cultural norms and expectations shape how fathers perceive and report their feelings.
Kennedy and Munyan (24) highlighted a number of demographic risk factors. They emphasized that lower education levels, low socioeconomic status, a family with three or more children, and single or widowed marital status were significant contributors to PPPD vulnerability. Additionally, a history of psychiatric treatment, unintended pregnancy, and unstable employment situations heightened the risk. In addition to that, Darwin et al. (22) reported multifaceted obstacles to the acceptability of PPMI screening. These challenges were identified across individual, practitioner, and service levels. Among the key issues were gendered perceptions around fatherhood, practitioner knowledge and confidence, time constraints, and the necessity for resources such as tools, training, and referral pathways. Some fathers in their reviewed studies hesitated to seek help due to cultural and social stigma, while others saw potential in routine screening to destigmatize perceptions and discussions around PPMI. Some fathers reported that they would only open up about their mental health if they felt the health visit focused on them as well as their partner. They also mentioned their reluctance to speak in front of their partners and service limitations (especially conflicting service hours with work commitments) as issues. Darwin’s et al. (22) study also noted gaps in professional training and the unequal perception of fathers as caregivers by some child health nurses. Service-level shortcomings, such as an exclusive focus on birthing mothers, hindered fathers’ engagement. Traditional gender role beliefs explain why some fathers in Darwin et al. (22) review felt it was culturally and socially unacceptable to discuss difficulties with fatherhood. In contrast to that, countries with more egalitarian gender models are likely to report higher instances of PPPD (4). This perception of stigma around mental health and needing to be strong are barriers to assessment, especially for those who strongly internalized those traditional gender roles. These insights underscore the complex interplay of societal norms and individual experiences in the realm of PPMI.
There is a lack of validated and reliable tools for specifically identifying and supporting PPMI during pregnancy and the postpartum period. Reviews show inconsistent use of scales beyond the EPDS and limited analysis of demographic factors impacting sensitivity. Limited research has been conducted on the development of screening tools tailored to new fathers. Pérez et al. (4) advocates moving beyond the EPDS, despite its predominant use in numerous studies, as results have been often inconclusive regarding sensitivity. Their results suggest the development and validation of specialized instruments for screening and diagnosing PPMI. This is based on the observation that males often express depression through atypical (male-specific) symptoms, such as aggression and irritability, rather than exhibiting a typical depressive mood.
A significant increase in studies related to this topic reflects the growing recognition of the importance of including fathers in research within this field. Despite this progress, challenges remain in effectively addressing PPMI. The predominant use of the EPDS highlights the reliance on a tool not explicitly tailored for fathers, raising concerns about its sensitivity and specificity in this population. The EPDS and other screening tools often overlook unique manifestations of PPMI in fathers. The spectrum of applied screening instruments primarily includes either specialized tools tailored to identify symptoms typically associated with maternal depression, such as excessive sadness or mood fluctuations, or non-specialized screening measures for general mental health conditions without a specific gender focus. This issue is also reflected in recent publications (32, 33) highlighting the necessity of gender-specific screening tools for PPMI, pointing out differences in symptom presentation and comorbidities compared to maternal perinatal depression, and advocate for tailored instruments. Men experiencing PPMI may exhibit externalized symptoms like irritability, anger, or increased alcohol consumption, and these are often overlooked. Based on Shafian’s et al. (25) findings, using the EPDS may yield a notable number of false positives, necessitating additional assessments, which can lead to substantial costs for service providers. However, alternative scales used have shown inconsistency across studies and have received limited attention in PPMI research. Comparing the EPDS to these tools (e.g., BDI or PHQ-9), the EPDS has specific questions tailored to postpartum experiences, such as questions about feelings of sadness, guilt or changes in appetite and sleep patterns that are particularly relevant to mothers. Conversely, instruments like the PHQ-9 and BDI encompass a broader spectrum of depressive symptoms that may be encountered by both mothers and fathers. The outcomes of this review underscore that EPDS and GMDS scales measure distinct aspects of paternal depression, supporting the necessity for a more comprehensive approach to its identification and support. Kennedy and Munyan (24) highlighted that neither the EPDS nor the GMDS alone may be adequate for screening, suggesting a combination of scales may be necessary.
Moreover, the variation in prevalence rates reflects the impact of traditional gender roles within different cultures, thereby influencing how fathers respond to questionnaires concerning their emotional wellbeing. Addis (34) emphasized that adherence to traditional gender norms can hinder help-seeking behavior and increase the risk of depression. An additional consideration should be, as Pérez et al. (4) hypothesized, a link between international rates of PPPD and traditional gender role beliefs in their review. They propose that countries with strong patriarchal values, where men are expected to uphold patriarchal ideals (e.g., exhibit dominance and aggression), may have lower rates of identified PPPD. Societal norms may discourage men from expressing their emotions, which can constrict their emotional life and, as a consequence, reduce their susceptibility to PPPD. This idea aligns with previous research, such as Psouni et al. (13) highlighting the coexistence of traditional depressive symptoms and depressive equivalents in fathers, and suggests that a screening tool combining both symptom types may be more appropriate for evaluating PPMI. A study from Salokangos et al. (35) underscores nuanced disparities in how depressive symptoms are reported by men and women. These differences arise from the inclusion of gender-related assessment items, resulting in potentially biased outcomes when measuring depression. Consequently, future research should address the development of assessment tools that mitigate such biases, aiming to enhance diagnostic accuracy and reduce misclassification. However, with respect to cultural differences and expectations, it is also possible that fathers in cultures with strong patriarchal values do not experience PPPD to the same extent as fathers in other cultures. The role of fathers in family dynamics and responsibilities varies greatly across different societies. In cultures where fathers are expected to take on significant caregiving responsibilities and actively participate in childcare, the transition to parenthood might affect their mental health differently compared to cultures where their involvement is minimal. Other factors, such as cultural differences in the understanding and acceptance of mental health issues, variations in healthcare systems, and access to mental health services, could also influence PPPD rates. Consequently, future research should focus on developing assessment tools that account for these complexities, thereby emphasizing the need for culturally sensitive screening approaches tailored to diverse populations.
This paper emphasizes the critical need for valid and culturally sensitive screening tools to detect and support PPMI. Kennedy and Munyan (24) stress the importance of validation studies, particularly considering cultural and socio-demographic variations in cutoff scores. Gressier et al. (36), highlight the link between PPMI and parent–child separation during maternal psychiatric episodes, underlining the importance of involving fathers in screening.
A broader research effort is required to further validate these screening tools and improve our understanding of PPMI. Improved sensitivity in screening instruments is crucial for prevention and treatment. Recommendations include developing combined scale questionnaires and utilizing multiple screening tools, with an emphasis on culturally sensitive approaches (4).
The risk factors associated with PPMI should also be considered when developing screening tools for fathers. A comprehensive meta-analysis by Goodman (37) identified maternal depression as the most robust predictor of paternal postpartum depression. Philpott et al. (38) identified several additional risk factors, previous depression, infants sleep problems, perceived lack of social support, challenging economic circumstances, and no access to or not utilizing paternity leave. Ansari et al. (39) expanded this collection spectrum to include relationship dissatisfaction, low paternal education level, unemployment, work-related stress, low parenting self-efficacy, and perceived stress.
A key challenge identified is the limited involvement of fathers in integrated service provision. While universal screening for fathers is recommended, guidance on optimal timing is still lacking, as noted by Kennedy and Munyan (24). Nevertheless, universal screening could potentially address the issue that Edward et al. (23) mentioned that partners of individuals with PPMI encountered challenges, including a lack of awareness about where to find PPMI resources and difficulties in seeking social support or referrals to healthcare professionals.
In terms of medical encounters and service provision, it would be beneficial to widen the dyadic mother-infant perspective and include the father or partner in the integrated delivery of services. Hambidge et al. (40) emphasize that while fathers may attend some antenatal visits and are typically present at birth, these interactions primarily center around the wellbeing of the mother and baby. Consequently, fathers may perceive their role as secondary to that of the mother and may hesitate to express their need for support. Fletcher et al. (41) highlight fathers’ limited engagement with health services as a significant barrier to their assessment and support during early parenthood. Pérez et al. (4) suggest assessing the co-parental system and emphasize that this assessment should start before birth, with follow-ups during the entire first year postpartum or a long-term perspective on this phenomenon. This could be useful for designing future intervention programs. Moreover, Pedersen et al. (16) suggest that screening for PPMI may facilitate fathers’ help-seeking behavior, requiring further investigation. Research gaps could inform public awareness campaigns, PPMI healthcare guidelines, and healthcare professional training.
Darwin et al. (22) highlighted the ethical challenge of conducting routine PPMI assessments in the absence of follow-up pathways and support services. Identifying PPMI is crucial, but without adequate support, there can be a risk of creating harm for fathers. Establishing accessible interventions alongside screening is essential for ethical and effective PPMI identification. Research can address this gap by informing the development of follow-up pathways and support services.
This study utilizes narrative synthesis to analyze the diverse range of study designs and outcomes among reviewed articles, providing a qualitative and comprehensive analysis. However, the varied study designs posed challenges for certain components of the AMSTAR 2 assessment. It is important to note limitations in applying some elements of the AMSTAR 2 tool to evaluate the methodological quality of systematic reviews in this context. Despite this, the systematic literature search, robust search strategy, and predefined data extraction format enhance the study’s consistency. Additionally, the study’s exclusive focus on reviews may have overlooked relevant individual studies, potentially limiting the current understanding of the topic. Excluding non-English publications may introduce bias by missing valuable literature. The narrative synthesis method does not facilitate quantitative result synthesis, limiting precise statistical conclusions and introducing subjectivity in interpretation.
Fathers, as with mothers, undergo significant emotional and psychological adjustments during the transition to parenthood. The sleepless nights, the added financial responsibilities, and the emotional rollercoaster of caring for a newborn, can exert an immense toll on fathers’ mental wellbeing. Yet, depression in fathers often remains underdiagnosed and undertreated. Enhancing the sensitivity of mental health screening instruments tailored to fathers is not only a matter of equity, but also one of profound consequence. By fine-tuning these tools to include a wider range of depressive symptoms, it may be possible to identify struggling fathers earlier in their journey, and offer them the support and resources they need to cope effectively. Early detection can be pivotal in preventing the escalation of depressive symptoms and, in turn, reducing the risk of adverse outcomes for fathers, their partner and their children.
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
PS: Writing – original draft, Writing – review & editing. LH: Writing – review & editing. AL: Writing – review & editing. CH: Writing – review & editing. IZ-K: Writing – review & editing. AB: Writing – review & editing. JP: Writing – review & editing.
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. The research described in this paper was conducted as part of the research project “Healthy Minds,” which received funding from the FWF (Grant DOI 10.55776/CM6 “Co-designing perinatal mental health support in Tyrol”). The project is hosted by the Medical University of Innsbruck.
The authors would like to acknowledge the support from individuals, who provided management, supervision, or administrative support to the research project “Healthy Minds” as part of which this study was conducted. In particular, the authors would like to thank Professor Alex Hofer at the Medical University Innsbruck Department of Psychiatry, Psychotherapy, Psychosomatics, and Medical Psychology, Division of Psychiatry, for hosting the research project within his department.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
PMI, Perinatal mental illness; PPD, Postpartum depression; PPMI, Paternal perinatal mental illness; PPPD, Paternal postpartum depression
1. Berg, RC, Solberg, BL, Glavin, K, and Olsvold, N. Instruments to identify symptoms of paternal depression during pregnancy and the first postpartum year: a systematic scoping review. Am J Mens Health. (2022) 16. doi: 10.1177/15579883221114984
2. Fisher, SD, Cobo, J, Figueiredo, B, Fletcher, R, Garfield, CF, Hanley, J, et al. Expanding the international conversation with fathers’ mental health: toward an era of inclusion in perinatal research and practice. Arch Womens Ment Health. (2021) 24:841–8. doi: 10.1007/s00737-021-01171-y
3. Tiedje, LB, and Darling-Fisher, C. Fatherhood reconsidered: a critical review. Res Nurs Health. (1996) 19:471–84. doi: 10.1002/(SICI)1098-240X(199612)19:6<471::AID-NUR3>3.0.CO;2-L
4. Pérez, F, Brahm, P, Riquelme, S, Rivera, C, Jaramillo, K, and Eickhorst, A. Paternal post-partum depression: how has it been assessed? A literature review. Mental Health Prev. (2017) 7:28–36. doi: 10.1016/j.mhp.2017.07.001
5. Baierl, A., Buchebner-Ferstl, S., and Dörfler-Bolt, S. (2023). Vatersein in Österreich Eine empirische Untersuchung im multi-methoden Design
6. Rille-Pfeiffer, C, and Kapella, O. Evaluierung des neuen Kinderbetreuungsgeldkontos und der Familienzeit: Meta-Analyse. Wien: Social Science Open Access Repository (SSOAR) (2022).
7. Diniz, E, Brandão, T, Monteiro, L, and Veríssimo, M. Father involvement during early childhood: a systematic review of the literature. J Fam Theory Rev. (2021) 13:77–99. doi: 10.1111/jftr.12410
8. Ramchandani, PG, Psychogiou, L, Vlachos, H, Iles, J, Sethna, V, Netsi, E, et al. Paternal depression: an examination of its links with father, child and family functioning in the postnatal period. Depress Anxiety. (2011) 28:471–7. doi: 10.1002/da.20814
9. LeFrançois, BA. Distressed fathers and their children: a review of the literature. Int J Soc Psychiatry. (2012) 58:123–30. doi: 10.1177/0020764010387478
10. Cameron, EE, Sedov, ID, and Tomfohr-Madsen, LM. Prevalence of paternal depression in pregnancy and the postpartum: an updated meta-analysis. J Affect Disord. (2016) 206:189–203. doi: 10.1016/j.jad.2016.07.044
11. Leach, LS, Poyser, C, Cooklin, AR, and Giallo, R. Prevalence and course of anxiety disorders (and symptom levels) in men across the perinatal period: a systematic review. J Affect Disord. (2016) 190:675–86. doi: 10.1016/j.jad.2015.09.063
12. Paulson, JF, and Bazemore, SD. Prenatal and postpartum depression in fathers and its association with maternal depression a meta-analysis. JAMA. (2010) 303:1961–9. doi: 10.1001/jama.2010.605
13. Psouni, E, Agebjörn, J, and Linder, H. Symptoms of depression in Swedish fathers in the postnatal period and development of a screening tool. Scand J Psychol. (2017) 58:485–96. doi: 10.1111/sjop.12396
14. American Psychiatric Association. Quick reference to the diagnostic criteria from DSM-IV-TR (p. 370). Washington, DC: APA. (2000)
15. Möller-Leimkühler, AM. Barriers to help-seeking by men: a review of sociocultural and clinical literature with particular reference to depression. J Affect Disord. (2002) 71:1–9. doi: 10.1016/S0165-0327(01)00379-2
16. Pedersen, SC, Maindal, HT, and Ryom, K. “I wanted to be there as a father, but I couldn’t”: a qualitative study of fathers’ experiences of postpartum depression and their help-seeking behavior. Am J Mens Health. (2021) 15:155798832110243. doi: 10.1177/15579883211024375
17. Schuppan, KM, Roberts, R, and Powrie, R. Paternal perinatal mental health: at-risk fathers’ perceptions of help-seeking and screening. The Journal of Men’s Studies. (2019) 27:307–28.
18. Page, MJ, McKenzie, JE, Bossuyt, PM, Boutron, I, Hoffmann, TC, Mulrow, CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Int J Surg. (2021) 88:105906. doi: 10.1016/j.ijsu.2021.105906
19. Hunt, H, Pollock, A, Campbell, P, Estcourt, L, and Brunton, G. An introduction to overviews of reviews: planning a relevant research question and objective for an overview. Syst Rev. (2018) 7:39. doi: 10.1186/s13643-018-0695-8
20. Popay, J, Roberts, H, Sowden, A, Petticrew, M, Arai, L, Rodgers, M, et al. Guidance on the conduct of narrative synthesis in systematic reviews a product from the ESRC methods programme Peninsula Medical School Universities of Exeter and Plymouth (2006).
21. Shea, BJ, Reeves, BC, Wells, G, Thuku, M, Hamel, C, Moran, J, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. (2017) 358:j4008. doi: 10.1136/bmj.j4008
22. Darwin, Z, Domoney, J, Iles, J, Bristow, F, Siew, J, and Sethna, V. Assessing the mental health of fathers, other co-parents, and partners in the perinatal period: mixed methods evidence synthesis. Front Psychiatry. (2021) 11:585479. doi: 10.3389/fpsyt.2020.585479
23. Edward, K, Castle, D, Mills, C, Davis, L, and Casey, J. An integrative review of paternal depression. Am J Mens Health. (2015) 9:26–34. doi: 10.1177/1557988314526614
24. Kennedy, E, and Munyan, K. Sensitivity and reliability of screening measures for paternal postpartum depression: an integrative review. J Perinatol. (2021) 41:2713–21. doi: 10.1038/s41372-021-01265-6
25. Shafian, AK, Mohamed, S, Nasution Raduan, NJ, and Hway Ann, AY. A systematic review and meta-analysis of studies validating Edinburgh Postnatal Depression Scale in fathers. Heliyon. (2022) 8:e09441. doi: 10.1016/j.heliyon.2022.e09441
26. Cox, JL, Holdenand, JM, and Sagovsky, R. Detection of postnatal depression development of the 10-item Edinburgh Postnatal Depression Scale. Br J Psychiatry. (1987) 150:782–6. doi: 10.1192/bjp.150.6.782
27. Beck, AT, Ward, CH, Mendelson, M, Mock, J, and Erbaugh, J. An inventory for measuring depression. Arch Gen Psychiatry. (1961) 4:561–71. doi: 10.1001/ARCHPSYC.1961.01710120031004
28. Radloff, LS. The CES-D scale: a self-report depression scale for research in the general population. Appl Psychol Meas. (1977) 1:385–401. doi: 10.1177/014662167700100306
29. Whittemore, R, and Knafl, K. Prenatal and postpartum depression in fathers and its association with maternal depression a meta-analysis. JAMA. (2005) 52:546–53. doi: 10.1111/j.1365-2648.2005.03621.x
30. Kroenke, K, Spitzer, RL, and Williams, JBW. The PHQ-9 validity of a brief depression severity measure. J Gen Intern Med. (2001) 16:606–13. doi: 10.1046/j.1525-1497.2001.016009606.x
31. Tran, TD, Tran, T, and Fisher, J. Validation of three psychometric instruments for screening for perinatal common mental disorders in men in the north of Vietnam. J Affect Disord. (2011) 136:104–9. doi: 10.1016/j.jad.2011.08.012
32. Baldoni, F, and Giannotti, M. Perinatal distress in fathers: toward a gender-based screening of paternal perinatal depressive and affective disorders. Front Psychol. (2020) 11:1892. doi: 10.3389/fpsyg.2020.01892
33. Walsh, TB, Davis, RN, and Garfield, C. A call to action: screening fathers for perinatal depression. Pediatrics. (2020) 145:e20191193. doi: 10.1542/PEDS.2019-1193
34. Addis, ME. Gender and depression in men. Clin Psychol Sci Pract. (2008) 15:153–68. doi: 10.1111/J.1468-2850.2008.00125.X
35. Salokangas, RKR, Vaahtera, K, Pacriev, S, Sohlman, B, and Lehtinen, V. Gender differences in depressive symptoms an artefact caused by measurement instruments? J Affect Disord. (2002) 68:215–20. doi: 10.1016/S0165-0327(00)00315-3
36. Gressier, F, Glangeaud-Freudenthal, NMC, Essadek, A, Falissard, B, Corruble, E, and Sutter-Dallay, AL. Impact of paternal psychiatric disorders on parents-baby separation after mother-baby unit care. Child Abuse Negl. (2024) 149:106652. doi: 10.1016/j.chiabu.2024.106652
37. Goodman, JH. Paternal postpartum depression, its relationship to maternal postpartum depression, and implications for family health. J Adv Nurs. (2004) 45:26–35. doi: 10.1046/j.1365-2648.2003.02857.x
38. Philpott, LF, Phn, P, En, P, Hp, P, and Corcoran, P. Paternal postnatal depression in Ireland: prevalence and associated factors. Midwifery. (2017) 56:121–7. doi: 10.1016/j.midw.2017.10.009
39. Ansari, NS, Shah, J, Dennis, CL, and Shah, PS. Risk factors for postpartum depressive symptoms among fathers: a systematic review and meta-analysis. Acta Obstet Gynecol Scand. (2021) 100:1186–99. doi: 10.1111/aogs.14109
40. Hambidge, S, Cowell, A, Arden-Close, E, and Mayers, A. “What kind of man gets depressed after having a baby?” fathers’ experiences of mental health during the perinatal period. BMC Pregnancy Childbirth. (2021) 21:463. doi: 10.1186/s12884-021-03947-7
Keywords: paternal perinatal depression, paternal mental health, perinatal, depression, anxiety, fathers, screening instruments
Citation: Schöch P, Hölzle L, Lampe A, Hörtnagl C, Zechmeister-Koss I, Buchheim A and Paul JL (2024) Towards effective screening for paternal perinatal mental illness: a meta-review of instruments and research gaps. Front. Public Health. 12:1393729. doi: 10.3389/fpubh.2024.1393729
Edited by:
Christos Theleritis, University General Hospital Attikon, GreeceReviewed by:
Rune Zahl-Olsen, Sørlandet Hospital, NorwayCopyright © 2024 Schöch, Hölzle, Lampe, Hörtnagl, Zechmeister-Koss, Buchheim and Paul. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jean Lillian Paul, amVhbi5wYXVsQGktbWVkLmFjLmF0
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.