 Hitesh Chugh1*
Hitesh Chugh1* Oluwatosin Wuraola Akande1
Oluwatosin Wuraola Akande1 Roberto Arroba Tijerino2Moubadda Assi3Metua Bates4Atika Berry5Hebleen Brenes6Dulamragchaa Buyanbaatar7Urtnasan Chuluunbat8Gerelmaa Danzan7
Roberto Arroba Tijerino2Moubadda Assi3Metua Bates4Atika Berry5Hebleen Brenes6Dulamragchaa Buyanbaatar7Urtnasan Chuluunbat8Gerelmaa Danzan7 Oyungerel Darmaa8Ingrid Garcia9Nada Ghosn10Ruba Hikmat11Ana Maria Jimenez12
Oyungerel Darmaa8Ingrid Garcia9Nada Ghosn10Ruba Hikmat11Ana Maria Jimenez12 Shakila Naidu13
Shakila Naidu13 Karen Ngamata4Phuong Nam Nguyen14Beverley Paterson15Nomin-Erdene Tsogtgerel7
Karen Ngamata4Phuong Nam Nguyen14Beverley Paterson15Nomin-Erdene Tsogtgerel7 Andrea Patricia Villalobos16Valentino Wichman17
Andrea Patricia Villalobos16Valentino Wichman17 Kelly Safreed-Harmon18Shoshanna Goldin1Sylvie Briand1
Kelly Safreed-Harmon18Shoshanna Goldin1Sylvie Briand1 Gina Samaan1
Gina Samaan1- 1Epidemic and Pandemic Preparedness and Prevention, World Health Organization, Geneva, Switzerland
- 2Epidemiology Unit, Health Surveillance Directorate, Ministry of Health, San José, Costa Rica
- 3Pandemic Influenza Preparedness, World Health Organization, Beirut, Lebanon
- 4Te Marae Ora, Ministry of Health, Avarua, Cook Islands
- 5Preventive Medicine Department, Ministry of Public Health, Beirut, Lebanon
- 6Institute for Research on Nutrition and Health, Ministry of Health, San José, Costa Rica
- 7Health Emergency, World Health Organization, Ulaanbaatar, Mongolia
- 8The National Influenza Centre, National Center for Communicable Diseases, Ministry of Health, Ulaanbaatar, Mongolia
- 9Disease Prevention and Control and Risk Factors, Pan American Health Organization, Bogota, Colombia
- 10Epidemiological Surveillance Unit, Ministry of Public Health, Beirut, Lebanon
- 11Infectious Hazard Preparedness, World Health Organization, Cairo, Egypt
- 12Communicable Diseases, Pan American Health Organization, San José, Costa Rica
- 13Pacific Health Security and Communicable Diseases, World Health Organization, Suva, Fiji
- 14Infectious Hazard Management, World Health Organization Regional Office for the Western Pacific, Manila, Philippines
- 15National Centre for Epidemiology and Public Health, Australian National University, Canberra, ACT, Australia
- 16Infectious Hazards Management Unit, Health Emergencies Department, Pan American Health Organization, Washington, DC, United States
- 17Central Policy and Planning Office, Office of the Prime Minister, Avarua, Cook Islands
- 18Independent Consultant, Barcelona, Spain
The Preparedness and Resilience for Emerging Threats (PRET) initiative takes an innovative mode-of-transmission approach to pandemic planning by advocating for integrated preparedness and response systems and capacities for groups of pathogens with common transmission pathways. The World Health Organization (WHO) launched this initiative in 2023 with the publication of PRET Module 1 addressing respiratory pathogens. Exercise PanPRET-1 is a customizable tabletop simulation exercise (TTX) package developed to complement PRET Module 1. The exercise scenario focuses on strengthening capacities for multisectoral coordination, risk communication and community engagement, and the triggers for operational decision-making. This article reports on the experiences of the first four countries to implement Exercise PanPRET-1: Cook Islands, Costa Rica, Lebanon and Mongolia. Exercise outcomes demonstrated that PanPRET-1 can be an effective tool for testing pandemic plans in a multisectoral forum and identifying opportunities to improve preparedness and response in key domains. In quantitative evaluations in Cook Islands, Costa Rica and Mongolia, high proportions of exercise participants indicated that multiple aspects of the exercise were well-designed and were beneficial for improving health emergency preparedness. Exercise participants in Lebanon provided qualitative feedback indicating that they found the exercise to be beneficial. Conducting a TTX and monitoring the implementation of action plans based on exercise findings facilitates a country-owned whole-of-society vision for pandemic planning. Countries are encouraged to incorporate TTX such as Exercise PanPRET-1 into a continuous cycle of activity to improve pandemic preparedness.
1 Introduction
The SARS-CoV-19 pandemic demonstrated the need for stronger preparedness and response systems to address a wide range of pathogens that may cause health emergencies (1). In early 2023, the World Health Organization (WHO) launched the Preparedness and Resilience for Emerging Threats (PRET) initiative, which takes an innovative mode-of-transmission approach to pandemic planning. In response to requests from WHO Member States (hereafter referred to as “countries”), PRET sets forth a whole-of-society vision for developing integrated preparedness and response capacities in relation to groups of pathogens that have common transmission pathways. The PRET initiative’s first module addresses respiratory pathogens including influenza viruses and coronaviruses (1). Since preparing for different types of respiratory pathogens requires similar actions, the mode-of-transmission approach leverages existing systems and capacities to maximize efficiency and coherence (1). Countries are encouraged to flexibly adapt guidance in PRET Module 1 to focus on the range of respiratory pathogens that are viewed as concerns in their respective contexts (1).
The PRET initiative emphasizes the importance of approaching pandemic preparedness in an iterative manner and engaging different sectors in updating and testing national respiratory pathogen pandemic plans (2). WHO has developed tools to facilitate the uptake of guidance in PRET Module 1, including a tabletop simulation exercise (TTX) package hereafter referred to as Exercise PanPRET-1. Simulation exercises are widely recognized as a useful tool for increasing government and societal readiness to respond to public health emergencies including disease outbreaks (3–5). A TTX brings together key stakeholders in a discussion-based setting to respond to a scripted emergency scenario and collectively address hypothetical events that realistically embody challenges associated with emergencies. According to the WHO Simulation Exercise Manual, a TTX “is designed to elicit constructive discussion between participants; to identify and resolve problems; and to refine existing operational plans” (5).
A TTX has multiple stages at which “injects” are presented to exercise participants asking them to address new developments associated with the emergency. Learnings that arise from the TTX are intended to guide measures to strengthen emergency preparedness. Governments and other actors have conducted TTX focusing on a wide range of pathogens such as coronaviruses (6), salmonella (7), Ebola virus disease (8), cholera (9), smallpox (10), and influenza viruses (11).
This article describes the implementation of Exercise PanPRET-1 in Cook Islands, Costa Rica, Lebanon and Mongolia. It reports on respective country outcomes and considers broader implications of these findings for national governments and other stakeholders. It also reflects on how countries can optimally integrate TTX activities into ongoing respiratory pathogen preparedness and response planning.
2 Developing and implementing the exercise package
2.1 Exercise package development
To help countries learn from pandemic and outbreak experiences, including from COVID-19, WHO staff developed Exercise PanPRET-1 drawing on information and templates in the WHO Simulation Exercise Manual (5). The overall objectives of the exercise package are “to deploy an adaptable tabletop simulation exercise package for countries to test/validate existing preparedness plans; update or develop a new plan; and/or advocate for respiratory pathogen preparedness planning.” The exercise package includes instructions for use, an adaptable draft scenario, templates for slide presentations, guides for facilitators and rapporteurs, and a participant evaluation form. WHO staff developed the package taking into account a range of country contexts, and incorporating best practices from related simulation exercises.
2.2 Exercise focus and content
Exercise PanPRET-1 focuses on three technical areas of respiratory pathogen preparedness and response: multisectoral coordination; risk communication and community engagement (RCCE); and triggers for operational decision-making.
The scenario presented in Exercise PanPRET-1 begins with an outbreak of a novel influenza virus among humans in a country on a different continent. The evolution of the situation is addressed in four stages, with each stage describing a series of events requiring government and societal action. For example, the first in-country cluster of cases of the disease is detected in stage two, misinformation is spreading in stage three, and hospitals are overwhelmed in stage four. Injects are presented at each stage, with accompanying questions asking exercise participants how their country’s preparedness and response systems would function as the scenario evolves.
2.3 Implementing the exercise
Exercise PanPret-1 was implemented in each country by an individual planning group. An exercise controller was appointed to coordinate the overall planning and delivery of the exercise with the assistance of the planning group. The exercise controllers for the Cook Islands, Costa Rica, and Mongolia were either WHO staff or WHO consultants. In Lebanon, the exercise controller was an external consultant recruited specifically for the exercise. Members of the planning group included representatives of the lead Ministry in charge of conducting the exercise (typically the Ministry of Health), the WHO Country Office, the WHO Regional Office, and technical staff from WHO Headquarters.
The planning group began the process by consulting with key stakeholders to determine the specific purpose, technical scope and desired outcomes of the exercise in their country context. The exercise controller and the planning group decided how to adapt the Exercise PanPRET-1 scenario to reflect their needs, taking into account each country’s existing health emergency management policy architecture.
The planning group invited representatives of different sectors to participate in the exercise, and sought to enlist participants from the governmental, private and civil society sectors to advance whole-of-society pandemic planning. Prior to implementation of the exercise, individuals who agreed to participate were provided background information including exercise objectives and current national pandemic plans.
Each country’s exercise was delivered by the exercise controller with assistance from facilitators and rapporteurs. The exercise concluded with a debriefing session whereby exercise and planning participants synthesized findings and identified lessons learned and recommendations. Following the exercise, lessons learned and recommendations were presented to government leaders, civil society and international partner agencies in order to galvanize actions to implement the recommendations.
This article reports on the experiences of the first four countries to implement Exercise PanPRET-1: Cook Islands, Costa Rica, Lebanon and Mongolia. Staff from WHO Country Offices, Regional Offices and Headquarters provided technical support to all four countries. Exercise participants in Cook Islands, Costa Rica and Mongolia completed an exercise evaluation survey. Exercise participants in Lebanon provided open-ended qualitative feedback on the exercise. Findings and lessons from each country (Table 1) were summarized using post-exercise reports that were shared with the exercise planning group and exercise participants.
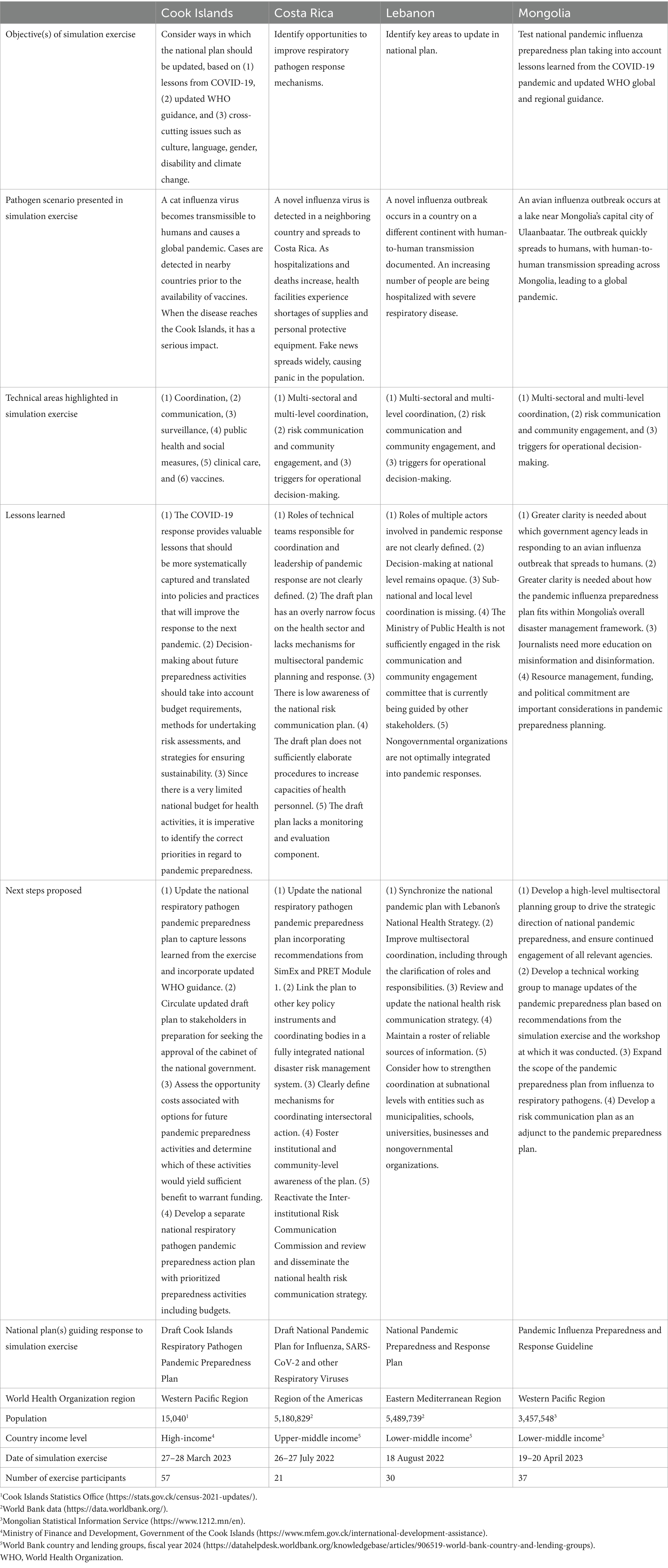
Table 1. Characteristics of table-top simulation exercises in the four countries.
3 Outcomes
3.1 Overview of exercise implementation
Exercise PanPRET-1 was implemented in Costa Rica, Cook Islands, Lebanon and Mongolia between July 2022 and April 2023 (Table 1). The exercises in Costa Rica, Lebanon and Mongolia were designed to explore the technical areas that were the focus of the base scenario. The Cook Islands exercise was designed to address those areas as well as surveillance; public health and social measures; clinical care; and vaccines. Across the four countries, the number of exercise participants ranged from 21 to 57. Government sectors and technical areas represented in the exercises included human health, animal health, disaster management, emergency coordination, risk communication, hospital management, education, defense and border control. Cook Islands also had nongovernmental sector participation from volunteer service organizations.
3.2 Country findings
In the Cook Islands, planners structured the exercise to encourage participants to draw on the country’s COVID-19 experiences while assessing the functionality of a newly drafted respiratory pathogen pandemic plan. The exercise scenario described an overseas cat influenza outbreak that resulted in a global pandemic among humans. During the COVID-19 pandemic, there were no reported cases in the Cook Islands until February 2022, well after vaccines were available to the population. In the exercise scenario, the hypothetical virus reached Cook Islands before a vaccine had been developed, providing participants with the opportunity to explore a very different pandemic situation. Participants found it difficult to determine whether authorities in the animal or human health sector would coordinate the early response stages. Participants observed that many experiences relating to COVID-19 could inform responses to future pandemics, even if pandemic characteristics were different. For example, COVID-19 learnings pointed to the need for risk communication strategies that take into account unreliable internet access and different information needs across culturally diverse communities. Participants concluded that learnings derived from both successes and failings in the national response to COVID-19 should be systematically captured and translated into policy and operational improvements. They also called attention to the challenge of determining which pandemic preparedness activities should be prioritized in the context of resource limitations.
In Costa Rica, the exercise scenario was based on the detection of a novel influenza virus in a neighboring country. Exercise participants explored how effectively the Draft National Pandemic Plan for Influenza, SARS-CoV-2 and other Respiratory Viruses guided their response to this scenario. Regarding multisectoral coordination and communication, a lack of cohesion in the overall health policy framework was identified. It was noted that the respiratory pandemic plan should be linked to Costa Rica’s National Action Plan for Health Security and Strategy for Health Risks, Disasters and Emergencies. Participants further identified a need for mechanisms to coordinate respiratory pathogen pandemic preparedness and response across all relevant sectors including the private sector. Regarding RCCE, many workshop participants were not familiar with the national Health Risk Communication Strategy. Participants called for this strategy to be reviewed and widely disseminated, and also for Costa Rica’s Inter-institutional Risk Communication Commission to be reactivated. Regarding triggers for escalating and de-escalating activities, participants recommended developing operational flowcharts that include clear definitions of the functions of implementing entities. They also called for greater clarity about the roles of the technical teams engaged in the response.
In Lebanon, the exercise was designed to inform ongoing efforts to strengthen intersectoral preparedness and response efforts under the One Health approach. Implementation of the exercise was viewed as a key step in developing a more contextualized national pandemic preparedness plan. In the course of considering the scenario and injects, participants frequently made reference to lessons learned across the different stages of Lebanon’s COVID-19 response. It was observed that while the Ministry of Public Health leads risk assessments as well as preliminary preparedness and response efforts in the early stages of a pandemic, the Supreme Defense Council plays a progressively larger decision-making role with the escalation of the situation. Participants noted that heterogeneous areas of Lebanon’s health sector need to be well-mapped at the national and subnational levels in order to optimize the use of available resources. Participants also discussed the importance of fostering institutional trust and compliance with recommended public health and social measures through effective risk communication. It was suggested by participants that efforts in this regard should be channeled toward the objectives of improving community engagement and identifying reliable media and information sources.
The exercise in Mongolia was designed to test the existing national pandemic influenza preparedness plan while also taking into account lessons learned from the COVID-19 pandemic and revised WHO global and regional guidance. The exercise scenario described an avian influenza outbreak that began in Mongolia and spread widely through human-to-human transmission, resulting in a global pandemic. Challenges that participants identified included a lack of clarity about which government agency should lead the response to an outbreak that began in animals and spread to humans, as well as uncertainty about how the existing national plan fit within Mongolia’s overall disaster management framework. Participants highlighted the need to estimate financial, human and other resource requirements and improve resource management in future pandemics. They also noted the importance of effective risk communication and observed that it may be beneficial to develop a separate risk communication plan. Participants considered the merits of using a pathogen-specific approach versus a mode-of-transmission approach to pandemic planning. As of this writing, stakeholders in Mongolia were working to determine how the scope of the pandemic plan would be revised accordingly. Participants recommended establishing a high-level multisectoral planning group to guide national pandemic preparedness efforts, with the Deputy Prime Minister serving as the chair of this group.
3.3 Exercise evaluation
Exercise participants in Cook Islands, Costa Rica and Mongolia completed quantitative evaluations (Figure 1) after their participation. High proportions of participants in all three countries agreed or strongly agreed that multiple aspects of the exercise were well designed and were beneficial. In Costa Rica and Mongolia, more than 85 percent of participants responded positively in regard to the value of the exercise for strengthening multisectoral coordination and RCCE capacities. In Cook Islands and Mongolia, more than 85 percent of participants agreed or strongly agreed that “at the end of the exercise, I think we are better prepared for a future health emergency.” Qualitative feedback from participants in Lebanon also indicated that the exercise was perceived to make meaningful contributions to respiratory pathogen pandemic preparedness and response. In particular, one participant noted that “this exercise could be replicated at the local level to reinforce Lebanon’s coordination mechanisms between national and local levels.” Participants in Lebanon also highlighted multiple critical actions for strengthening preparedness including developing more tangible pandemic plans and conducting periodic simulation exercises based on Exercise PanPRET-1 that bring together multiple levels and sectors.
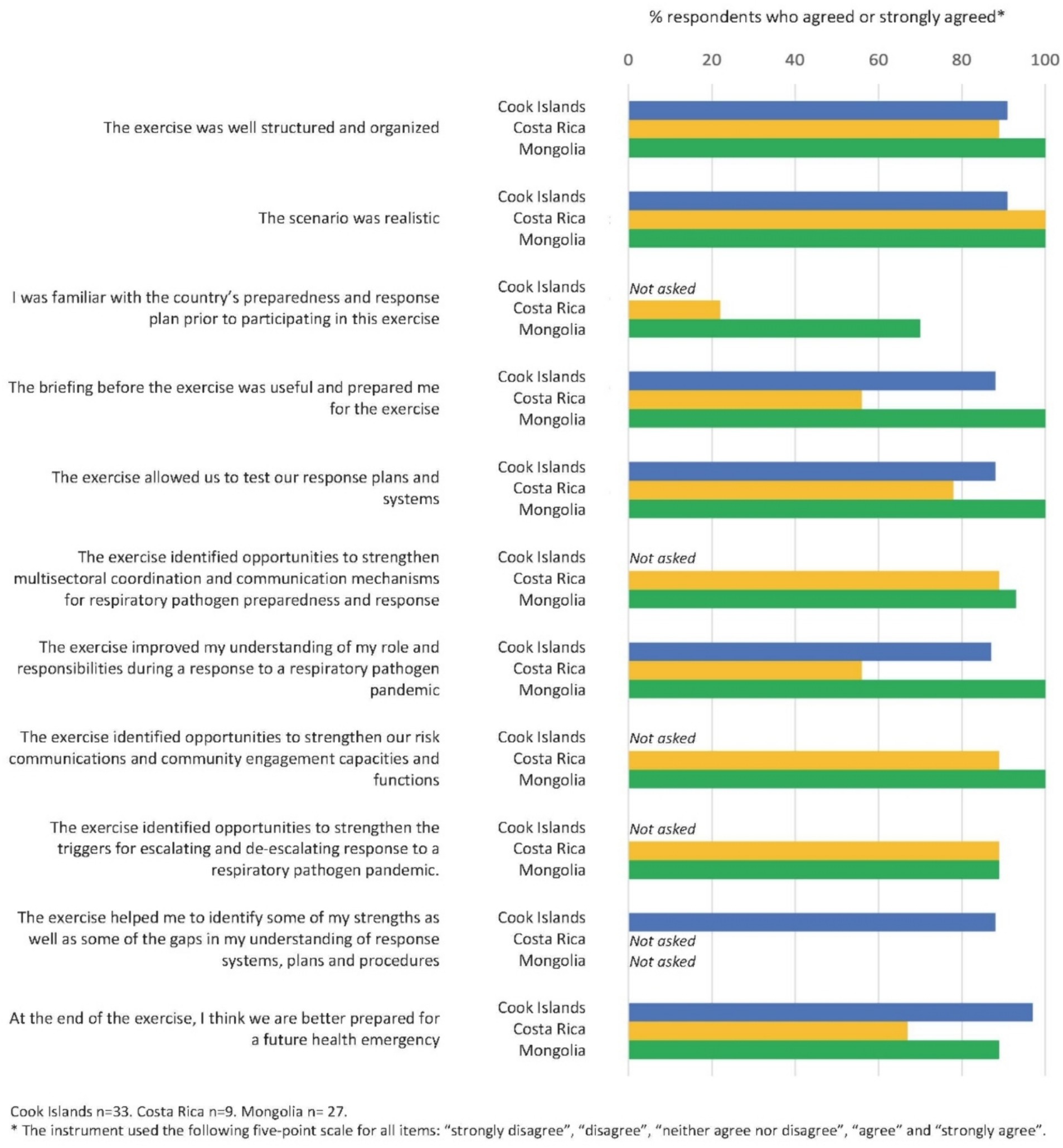
Figure 1. PanPRET-1 exercise evaluations in Cook Islands, Costa Rica, and Mongolia.
4 Discussion
To support countries in reviewing and developing national pandemic plans using a mode-of-transmission approach, WHO has introduced the first PRET module on respiratory pathogen pandemic planning along with supporting tools such as Exercise PanPRET-1 (1). The experiences of Exercise PanPRET-1 national implementers in Cook Islands, Costa Rica, Lebanon and Mongolia have demonstrated that this tool can be effective for testing pandemic plans in a multisectoral forum and identifying ways to improve key components of preparedness and response.
Across the four countries, the exercise drew attention to the value of mode-of-transmission planning. In particular, countries saw opportunities to build on pathogen-specific planning and strengthen common systems that could be utilized for influenza, coronaviruses, and other respiratory pathogens. In the debriefing that followed the Mongolia exercise, participants emphasized the potential for a mode-of-transmission approach to promote more efficient capacity-building across Mongolia’s multisectoral pandemic preparedness system and recommended convening a multisectoral planning group to lead the country in this direction. Similarly, the exercise in Lebanon highlighted the utility of a mode-of-transmission approach for specific components of preparedness and response systems such as RCCE. It was noted that holistically building community trust on respiratory pathogen public health and social measures would be more effective than taking disease-specific approaches. Exercise participants in all four countries identified high-level political commitment as a critical pathway forward. They stressed the value of including diverse sectors in pandemic preparedness and response activities, including academia, philanthropy, civil society and the private business sector.
Country exercises also highlighted opportunities for mode-of-transmission planning to build on learnings from COVID-19. Participants in Costa Rica recommended making improvements to decision-making algorithms that were used to guide the country’s COVID-19 response and are also applicable to other respiratory pathogen outbreaks and epidemics. Additionally, countries discussed ways of institutionalizing emerging technical areas that were established during the COVID-19 pandemic. This includes infodemic management in Lebanon and Mongolia, where participants identified the need to proactively manage mis- and disinformation by engaging more systematically with community and media groups to strengthen capacities for health journalism.
The exercise brought to light notable challenges associated with the high-level coordination of multifaceted responses to public health emergencies, consistent with findings from other simulation exercises and with lessons learned from the COVID-19 pandemic (3, 7, 12, 13). In particular, participating countries found that centralized leadership and decision-making was critical for coordinating national responses. Following the COVID-19 pandemic, it was recognized that conducting simulation exercises which included sectors beyond health would strengthen coordination mechanisms and enable countries to be better prepared to deliver large-scale response operations (12, 13). In addition, countries noted that public messaging on pandemic risks and community engagement should be targeted in order to build trust, facilitate tailored community-led responses, and address mis- and dis-information (12, 13).
Exercise participants in some countries commented on the need for pandemic plans to align more fully with other elements of their countries’ health emergency management policy architecture. Participants in two countries reported that greater clarity is required in regard to the respective roles of the animal and human health sectors when a pathogen of concern is spreading among both animals and humans. More generally, uncertainty about how to coordinate the work of various entities involved in responding to pathogen-driven public health threats was observed in all four countries. The complex nature of infodemic management also presented challenges, with exercise participants grappling with how best to adapt traditional risk communication approaches to internet and social media platforms that target diverse communities and age groups.
Findings overall suggest that Exercise PanPRET-1 is a versatile tool for engaging stakeholders in determining how to strengthen pandemic planning in a wide range of national settings. Exercise PanPRET-1 thus can help facilitate global implementation of the International Health Regulations (2005) Monitoring and Evaluation Framework. This framework includes the mandatory States Parties self-assessment annual reporting as well as three optional elements: voluntary external evaluation, after-action reviews, and simulation exercises (14).
As such, countries are encouraged to:
• Implement Exercise PanPRET-1 in a manner that fully integrates the activity into the ongoing planning cycle (1). This can be achieved by bringing together multiple sectors under health sector leadership through the implementation of Exercise PanPRET-1 at all levels, and updating pandemic preparedness plans using a mode-of-transmission approach and exercise recommendations.
• Use Exercise PanPRET-1 as a catalyst to strengthen common systems for pandemic preparedness and response, and to advocate for high-level ongoing national political commitment in the pandemic planning cycle.
• Use Exercise PanPRET-1 as the basis to systematically and periodically test multi-sectoral approaches to pandemic preparedness capacities across additional technical areas and scenarios not currently covered by the package. This can be achieved by adapting the scenario, based on national requirements, to focus on other technical areas including but not limited to public health and social measures, vaccine deployment, clinical management and/or partner engagement.
Quantitative and qualitative feedback suggested that the value of the exercise may be enhanced by ensuring that all participants are pre-briefed about relevant policies and plans in their respective countries. Potential bottlenecks to following through on exercise recommendations, such as a codifying how accountability for proposed activities will be shared among multiple agencies, should be identified and addressed in post-exercise action plans.
Limitations to these Exercise PanPRET-1 findings include the small country sample and the low level of participation from outside of the government sector. Additionally, the selection of exercise participants may have been biased by factors such as the nature of existing multisectoral collaborations addressing pandemic preparedness in the four countries, and the availability of appropriate technical focal points from participating Ministries. Quantitative participant feedback was only available from three of the four countries, and in the future can be improved by including questions on sector affiliation and roles.
In conclusion, Exercise PanPRET-1 supports countries in addressing pandemic preparedness and response planning through a mode-of-transmission approach and identifying next steps for making improvements. WHO is expanding the applications of Exercise PanPRET-1 by incorporating additional technical areas into the exercise and developing versions for specific stakeholder groups such as for civil society and international partner organizations. The engagement and effective coordination of different types of multisectoral actors and technical teams, including under a One Health framework, is key to strengthening mode-of-transmission pandemic planning. High-level political commitment is also required. Conducting TTX and monitoring the implementation of action plans based on exercise findings is a valuable mechanism for helping stakeholders develop and implement a shared country-owned vision for pandemic preparedness and response. Countries are encouraged to incorporate TTX such as Exercise Pan-PRET-1 into a continuous cycle of activity to improve respiratory pandemic preparedness and response planning.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
Author contributions
HC: Conceptualization, Methodology, Project administration, Supervision, Validation, Writing – review & editing. OA: Conceptualization, Methodology, Project administration, Validation, Writing – review & editing. RA: Writing – review & editing. MA: Writing – review & editing. MB: Writing – review & editing. AB: Writing – review & editing. HB: Writing – review & editing. DB: Writing – review & editing. UC: Writing – review & editing. GD: Writing – review & editing. OD: Writing – review & editing. IG: Writing – review & editing. NG: Writing – review & editing. RH: Writing – review & editing. AJ: Writing – review & editing. SN: Writing – review & editing. KN: Writing – review & editing. PN: Writing – review & editing. BP: Writing – review & editing. N-ET: Writing – review & editing. AV: Writing – review & editing. VW: Writing – review & editing. KS-H: Conceptualization, Methodology, Validation, Writing – original draft, Writing – review & editing. SG: Writing – review & editing. SB: Conceptualization, Supervision, Writing – review & editing. GS: Conceptualization, Methodology, Project Administration, Supervision, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. Funding for the development of Exercise PanPRET-1 was provided by the United States Centers for Disease Control and Prevention through Cooperative Agreement GH19-1967 with the World Health Organization, and the Pandemic Influenza Preparedness (PIP) Framework Partnership Contribution. Additional support for roll-out and implementation at the country level was provided by the Pandemic Influenza Preparedness (PIP) Framework Partnership Contribution. Funding for the implementation of PanPRET-1 in Lebanon was provided by the United States Centers for Disease Control and Prevention through Cooperative Agreement GH19-1967 with the World Health Organization.
Acknowledgments
The authors acknowledge the following individuals and institutions for their contributions: Fatima Awada, Preventive Medicine Department, Ministry of Public Health, Beirut, Lebanon; Maryo Baaklini, Epidemiological Surveillance Unit, Ministry of Public Health, Beirut, Lebanon; Xiomara Badilla, Caja Costarricense de Seguro Social, San Jose, Costa Rica; Guiselle Guzmán Saborío, Caja Costarricense de Seguro Social, San Jose, Costa Rica; Claudio Soto, Institute for Research on Nutrition and Health, San Jose, Costa Rica; Ministry of Health, Ulaanbaatar, Mongolia; National Center for Communicable Diseases, Ulaanbaatar, Mongolia; National Center for Public Health, Ulaanbaatar, Mongolia; National Center for Zoonotic Diseases, Ulaanbaatar, Mongolia; National Emergency Management Agency, Ulaanbaatar, Mongolia; Ministry of Education and Science, Ulaanbaatar, Mongolia; General Custom Agency, Ulaanbaatar, Mongolia.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. World Health Organization. Preparedness and resilience for emerging threats module 1: planning for respiratory pathogen pandemics. (2023). Available at: https://www.who.int/publications/i/item/9789240084674
2. World Health Organization. Strengthening pandemic preparedness planning for respiratory pathogens: policy brief, 27 April 2022. (2022). Available at: https://www.who.int/publications/i/item/WHO-2019-nCoV-Policy_brief-pandemic_preparedness-2022.1
3. Copper, FA, Mayigane, LN, Pei, Y, Charles, D, Nguyen, TN, Vente, C, et al. Simulation exercises and after action reviews – analysis of outputs during 2016-2019 to strengthen global health emergency preparedness and response. Glob Health. (2020) 16:115. doi: 10.1186/s12992-020-00632-w
4. European Centre for Disease Prevention and Control. Handbook on simulation exercises in EU public health settings: how to develop simulation exercises within the framework of public health response to communicable diseases. (2014). Available at: https://www.ecdc.europa.eu/en/publications-data/handbook-simulation-exercises-eu-public-health-settings
5. World Health Organization. WHO simulation exercise manual: a practical guide and tool for planning, conducting and evaluating simulation exercises for outbreaks and public health emergency preparedness and response. (2017). Available at: https://apps.who.int/iris/handle/10665/254741
6. Center for Health Security, Johns Hopkins Bloomberg School of Public Health. Event 201. (2023). Available at: https://centerforhealthsecurity.org/our-work/tabletop-exercises/event-201-pandemic-tabletop-exercise#scenario
7. Alves, F, Artursson, K, Bloch, J, Brisabois, A, Imberechts, H, Jokelainen, P, et al. A multi-country one health foodborne outbreak simulation exercise: cross-sectoral cooperation, data sharing and communication. Front Public Health. (2023) 11:1121522. doi: 10.3389/fpubh.2023.1121522
8. World Health Organization. South Sudan conducts an Ebola tabletop exercise. (2019). Available at: https://www.afro.who.int/news/south-sudan-conducts-ebola-tabletop-exercise
9. World Health Organization. Préparation et riposte aux épidémies: Des exercices de simulations pour évaluer le dispositif contre une éventuelle flambée de choléra. (2018). Available at: https://www.afro.who.int/node/10511
10. Dausey, DJ, Buehler, JW, and Lurie, N. Designing and conducting tabletop exercises to assess public health preparedness for manmade and naturally occurring biological threats. BMC Public Health. (2007) 7:92. doi: 10.1186/1471-2458-7-92
11. World Health Organization. Pandemic influenza preparedness in WHO member states: report of a member states survey. (2019). Available at: https://apps.who.int/iris/handle/10665/325411
12. European Centre for Disease Prevention and Control. Lessons from the COVID-19 pandemic. (2023). Available at: https://www.ecdc.europa.eu/sites/default/files/documents/COVID-19-lessons-learned-may-2023.pdf
13. World Health Organization. Learnings from COVID-19 for future respiratory pathogen pandemic preparedness: a summary of the literature. (2024). Available at: https://www.who.int/publications/i/item/9789240086531
14. World Health Organization. International health regulations (2005) monitoring and evaluation framework. (2024). Available at: https://www.who.int/publications/i/item/international-health-regulations-(-2005)-ihr-monitoring-and-evaluation-framework
Keywords: pandemic, preparedness, response, exercise, respiratory, pathogen, planning
Citation: Chugh H, Akande OW, Arroba Tijerino R, Assi M, Bates M, Berry A, Brenes H, Buyanbaatar D, Chuluunbat U, Danzan G, Darmaa O, Garcia I, Ghosn N, Hikmat R, Jimenez AM, Naidu S, Ngamata K, Nguyen PN, Paterson B, Tsogtgerel N-E, Villalobos AP, Wichman V, Safreed-Harmon K, Goldin S, Briand S and Samaan G (2024) Preparing for the next respiratory pathogen pandemic: using tabletop simulation exercises to strengthen national planning in Cook Islands, Costa Rica, Lebanon and Mongolia. Front. Public Health. 12:1392894. doi: 10.3389/fpubh.2024.1392894
Edited by:
Tafadzwa Dzinamarira, ICAP in Zimbabwe, ZimbabweReviewed by:
Chalomba Chitanika, ICAP (Zambia), ZambiaNhuNgoc K. Pham, Tulane University School of Public Health and Tropical Medicine, United States
Copyright © 2024 Chugh, Akande, Arroba Tijerino, Assi, Bates, Berry, Brenes, Buyanbaatar, Chuluunbat, Danzan, Darmaa, Garcia, Ghosn, Hikmat, Jimenez, Naidu, Ngamata, Nguyen, Paterson, Tsogtgerel, Villalobos, Wichman, Safreed-Harmon, Goldin, Briand and Samaan. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Hitesh Chugh, Y2h1Z2hoQHdoby5pbnQ=