 Xenia Chela-Alvarez
Xenia Chela-Alvarez Alfonso Leiva1,2,3
Alfonso Leiva1,2,3 Joan Llobera
Joan Llobera- 1Primary Care Research Unit of Mallorca, Balearic Islands Health Service, Palma, Spain
- 2GrAPP-caIB – Health Research Institute of the Balearic Islands, Palma, Spain
- 3RICAPPS- Red de Investigación Cooperativa de Atención Primaria y Promoción de la Salud - Carlos III Health Institute (ISCIII), Madrid, Spain
Background: Hotel housekeepers constitute an important occupational group in the Balearic Islands (Spain). Housekeeping is considered low-skilled and precarious and typically involves high physical demands and time pressure. The aim of this study is to analyze the association between the socioeconomic determinants of health and hotel housekeepers’ self-rated health.
Methods: This is a cross-sectional study conducted in Primary Health Care in the Balearic Islands (November 2018–February 2019). Hotel housekeepers over 18 years of age with free access to the Balearic Public Health System who had been employed during 2018 were eligible.
Results: We enrolled 1,043 hotel housekeepers; the mean score of health perceived status was 72.4/100 (SD 19.0). Those with a lower self-perceived health were statistically significant older, had Spanish nationality, lower level of studies, permanent or recurring seasonal contract, financial difficulties, a higher level of occupational stress, an external locus of control, reported work-life balance difficulties, were former smokers, insufficiently physical active and obese. We found lower scores in self-perceived health status score of −7.159 (CI95% -10.20- -4.12) among hotel housekeepers with osteoarthritis; −6.858 (CI95% -11.89- -1.82) among those with chronic depression; −3.697 (CI95% -6.08- -1.31) among those who reported difficulties in work-life balance; −2.414 (CI95% -4.69- -0.13) among participants who performed insufficient physical activity; −2.107 (CI% -4.44- -0.23) among those who reported financial strain. Lower self-rated health was also associated to a higher perceived stress, −1.440 (CI95% -2.09- -0.79); BMI (kg/m2), −0.299 (CI95% -0.53- -0.07); and longer time working as HH -0.177 (CI95% -0.33- -0.03).
Conclusion: Our results underscore the importance of psychosocial (such as difficulties in work-life balance and occupational stress) and material factors (such as financial difficulties) when explaining differences in self-perceived health. Public health interventions aimed at improving health status must consider inequalities in material and working conditions.
1 Introduction
In the Balearic Islands, the tourist sector contributed to 44% gross domestic product (pre-pandemic data) (1), with hotel housekeepers (HHs) constituting an essential occupational group (around 13,000). Housekeeping is considered a low-skilled job, physically demanding, involving repetitive tasks, unhealthy postures, high demands, heavy workload and low control (2–9). These characteristics have been related to negative health outcomes, such as musculoskeletal disorders (MSD) (10, 11) and stress (2, 12, 13).
Health status is defined as a measure of how people perceive their health, including physical and mental health (14). Similarly, the World Health Organization defines the concept of health as a “state of complete physical, mental, and social well-being and not merely the absence of disease or infirmity” (15). Among the measures to assess health status, self-rated health (SRH) has been widely used and reported as a good indicator for health problems (16) and a strong predictor for mortality (17). Generally, individuals are requested to rate their health as excellent, very good, good, fair, or poor, or to evaluate it using a visual analog scale. Material, psychosocial and behavioral factors have been widely identified as key contributors to socioeconomic inequalities in health (18, 19). Consequently, individuals from lower socioeconomic status present higher rates of morbidity, mortality and lower SRH compared to their higher socioeconomic status counterparts (20, 21).
Understanding these disparities is crucial for addressing health inequalities. The framework of socioeconomic determinants of health (22, 23) emphasizes that the socioeconomic and political context in which people live influences their socioeconomic position.
The socioeconomic and political context includes the welfare state, governance, macroeconomic policy, social policies, public policy, cultural and societal values and epidemiological conditions. Although data from Southern Europe are relatively scarce (24), studies point to a high prevalence of poor SRH among the population, with no significant gender differences (25).
The second key component are structural determinants and socioeconomic position. Structural determinants play a decisive role in defining the person’s socioeconomic position (23). Research found that people in the lowest socioeconomic positions are more likely to report poor SRH (26–28).
Socioeconomic position affects health through intermediary determinants, which include material and psychosocial circumstances, as well as behavioral and biological factors (23).
As Solar and Irwin (23) note, “socioeconomic health differences occur when the quality of these intermediary factors are unevenly distributed between the different socioeconomic classes.” The main categories of intermediary determinants are: (i) material/structural factors, (i.e., housing conditions, financial problems, employment status and physical work conditions); (ii) behavioral factors, (i.e., smoking, alcohol consumption, dietary habits, physical activity and body mass index (BMI)); (iii) psychosocial factors, linked to life events, psychosocial stressors (e.g., job strain), social support and coping.
Income is considered a material factor within the framework of social determinants of health and has been strongly related to SRH. Financial strain has been described as a significant stressor, affecting both physical and emotional well-being (29, 30). Half of the workers in Southern Europe experienced financial strain and consequently are more likely to report poor SRH status (25, 31).
Other material factors include physical work conditions. In addition to the heavy workload, physical demands and repetitive tasks that involves hotel housekeeping, the total number of hours worked (both paid and unpaid) has been related to health outcomes (32). Women spending more than 36 h per week on housework are more likely to show lower SRH (33). Clearly, caregiving and housework entail exposure to ergonomic and psychosocial risks, primarily due to the physical and mental strain of caring for dependents (34). Kim and Cho (35) found that female workers with higher household burdens and caring responsibilities for older people had a higher prevalence of MSDs than those without such demands. Notably, the number of household members positively correlates with poor SRH in manual workers (36).
This highly demanding work, together with little control and few rewards (37–39), has been reported as a significant source of stress (2). In fact, most jobs in the hospitality sector have been associated with occupational stress (40). Further, higher levels of perceived occupational stress have been related to poorer SRH among workers with lower educational levels (41).
Social support is considered a psychosocial factor and is defined as ‘the degree to which a person’s basic social needs are gratified through interaction with others’ [(42), p. 147]. Lower social support has been associated with worse SRH (43, 44). Also, a study by Brønholt et al. (45) found that exposure to adverse psychosocial work factors (i.e., low social support, low skill discretion, job insecurity, etc.) increased with lower SEP and were associated with poor SRH in women and men.
Furthermore, work–family conflict (WFC), another psychosocial factor, occurs when the responsibilities of one life sphere interfere with the accomplishment of the responsibilities in other life domains (46, 47); that is, when paid work, caregiving and household demands become incompatible WFC is associated with poorer SRH (48–50), has been reported as higher among working-class people (51, 52) and is positively associated with health problems such as depression and poor physical health (24, 53).
The locus of control (LOC) refers to the perception a person has about the control of the events that occur in their life. It is regarded as a psychosocial variable because it encompasses both the psychological domain, reflecting individual beliefs, and the social domain, as it is influenced by social experiences (54). LOC can be internal (people who believe that what happens in their life is consequence of their attitudes, actions and behavior) or external (people who attribute what happens in their life to fortune, fate or others’ decisions) (54). Mounce et al. (55) found that an external LOC was positively associated with the development of multimorbidity and Kesavayuth et al. (56) found that people with an internal LOC had better SRH (both physical and mental).
Regarding behavioral factors, healthy lifestyles are associated with better SRH (57–59). However, a systematic review of Dieker et al. (26) concluded that “work factors seem to be important contributors to socioeconomic inequalities in SRH irrespective of lifestyle behaviors.” Similarly, Brønholt et al. (45) found that work factors explained almost half of the social inequalities in SRH.
Importantly, overweight and obesity have been associated with a reduction of years lived in good health (60) and with poorer overall health compared to having a normal weight (61). The systematic review carried out by Newton et al. (62) reported that “females of lower life course socio-economic status had significantly higher odds of obesity compared with those of higher life course socio-economic status”.
HHs’ health is of particular relevance due to their structural position within society as low skilled workers and as women. Thus, HHs should present a significant relationship between material and psychosocial factors and SRH. This population warrants attention because most existing studies focus on middle-class or highly educated and skilled occupational groups (24).
Building on the conceptual framework on the social determinants of health (23), this study aims to: (i) estimate the personal, occupational, psychosocial, and behavioral characteristics of HHs of the Balearic Islands, a low-status occupational group; and (ii) explore which factors influence their SRH.
2 Materials and methods
Cross-sectional study carried out in 39 out of 58 Primary Health Care Centres in the Balearic Islands between November 2018 and February 2019.
2.1 Subjects
HHs over 18 years of age who had health coverage in the Balearic Public Health System and worked as HHs during 2018 were included after signing the informed consent form. HHs with a language barrier were excluded.
An initial list of about 13,000 possible HHs was available from the Balearic Health Services and Balearic Public Employment Service; 978 HHs were needed to estimate population parameters, with a 3% precision and a confidence of 95%. A randomly sample of 1,043 HHs was selected; in case they did not accept or were not possible to contact them, they were replaced randomly from the initial list.
2.2 Data collection
Data collection was carried out through in-person interviews using a structured questionnaire. Each interview lasted approximately 1 h and was administered by trained nurses. The interviews were conducted in a consultation room at the Primary Health Care Center. Nurses were responsible for the recruitment of study participants: HHs were invited by telephone and if they met the inclusion criteria they were given an appointment in their closest Primary Health Care Center.
A total of 14 nurses were hired by the Project and involved in data collection. They underwent a 3-h training session to become acquainted with the project and learn how to conduct the interviews and administer the questionnaires. This training aimed at standardizing procedures, ensuring data consistency, and minimizing losses and errors.
In order to recruit the required number of HHs, 4,436 phone calls were made (some HHs were called more than once in order to be contacted or recruited). Finally, 1,043 HHs were enrolled: 773 in Mallorca, 89 in Menorca, 137 in Ibiza and 44 in Formentera.
2.3 Measures
2.3.1 Dependent variable
Self-rated health: participants were asked to rate their overall health on the day of the interview on a 0–100 vertical visual analog scale (VAS), taken from the EuroQoL-5D-5L, a generic instrument for describing and valuing health (63, 64).
2.3.2 Independent variables
2.3.2.1 Socio-demographic and anthropometric
The sociodemographic characteristics were age, nationality and sex. The anthropometric variables were self-reported height and weight; after, BMI index (kilograms/m2) was calculated. Categories obtained were: below normal weight < 18.5; normal weight ≥ 18.5–24.9; overweight≥25–29.9; class I obesity ≥30–34.9; class II obesity ≥35–39.9; class III obesity ≥40.
2.3.2.2 Material/structural factors
We asked about educational level, type of contract (permanent, recurring-seasonal or temporary), type of establishment (apartment, hotel, etc.), hotel category, number of rooms cleaned per day, years working as HHs, months worked last tourist season, and hours worked per week.
Financial strain was measured by asking “A household might have different sources of income and more than a member can contribute with his/her income. Thinking about the total of your household monthly income, can you make ends meet…?” with a 5 option Likert scale from “very easy” to “very difficult.” The question was taken from the EQLS 2016. Following previous studies, we dichotomized the answers (25); answers “with some difficulty,” “with difficulty” and “with great difficulty” were considered as suffering from financial strain.
2.3.2.3 Behavioral factors
Smoking habits: the question had 4 options: do not smoke, former smoker (more than a year without smoking), former smoker (more than 6 months without smoking but less than a year), active smoker (1 or more cigarettes a day). This variable was transformed into a three categories variable (non-smoker, former smoker and active smoker).
Physical activity: we used the validated Spanish version of the Brief Physical Activity Assessment Tool (65), which identifies inactive patients (66). Two questions were asked about the frequency of performing 30 min of moderate and 20 min of vigorous physical activity a week. A total score of 4 or more was considered as sufficiently active (67). Their overall sensitivity in the detection of insufficient physical activity was 79.9% compared with accelerometer (68).
Healthy diet: we used a short, easy-to-administer, and validated screening questionnaire (69), with two questions regarding regular fruit and vegetable intake. A final score ranging from 0 to 10 was obtained: 5 or more points correspond to an intake of 5 servings of fruit or vegetables and thus considered as a healthy diet. The overall sensitivity in the detection of unhealthy diet was 76.8% (LR + = 3.1 and LR- = 0.31). Also, the correlation with the PREDIMED Food Frequency Questionnaire was R spearman 0.65 among women (69).
2.3.2.4 Psychosocial factors
Locus of control (LOC) was assessed through the question ‘To what extent do you agree with the following sentence: «I feel what happens in my life is often determined by factors beyond my control?», with Likert-type response options ranging from 1 (completely disagree) to 6 (completely agree). A forward translation into Spanish of the measurement used by Mounce et al. (55) was made as recommended by Ortiz-Gutiérrez and Cruz-Avelar (70). Internality is considered when the respondent answers options 1 to 3 (disagreement statements).
Level of stress at work was measured with the question, ‘Overall, taking into account the conditions in which you do your work, indicate how you consider the level of stress at your work on a scale from 1 (very stressful) to 7 (not at all stressful)’.
WFC was measured through the question ‘How easy or difficult is it for you to combine work with your care responsibilities?’, with four response options (from “Very easy” to “very difficult”), taken from the European Quality of Life Survey (EQLS, 2016) (51). We dichotomized answers (good work-life balance (WLB) and poor WLB), as done in other studies (71).
Social support was measured by DUKE-UNC-11 (72), an 11-item questionnaire to assess functional elements of social support (including confidant and affective support) validated in the Spanish population (73, 74). Each item is valued in a 5-points scale (ranging from 1 point: “much less than I would like,” to 5 points: “as much as I would like”). A final score ranging from 5 to 55 is obtained; 32 points or below correspond to low social support and more than 32 points to adequate social support (73).
Number of household members: HHs were asked if they lived on their own. In case of a negative response, participants were asked who they were living with. This variable was operationalized as number of people living in the household.
The distribution of domestic tasks and care of people were evaluated through the question ‘At home, who is mainly in charge of household chores and the care of people who are not able of caring for themselves?’. This question had to be answered in relation to four items extracted from the 2011–12 Spanish Health Survey: taking care of children under 15, taking care of a disabled person, taking care of people older than 74 years, and responsibility for domestic tasks (cleaning, ironing, cooking,…). For each item, the response options available were: HHs alone; HHs’ partner alone; shared with their partner; shared with a person other than their partner; another person living at home other than their partner; a hired person; a person who does not reside in the house; social services; him/herself; another situation; do not know/do not answer. It was a multiple answer question. In order to simplify the analysis and the results, for bivariate and multivariate analyses we transformed the care of dependents into a dichotomous variable: being in charge alone of a dependant or not (including the three items). The variable ‘main person in charge of domestic tasks’ was also dichotomized: being the main responsible vs. another situation.
2.3.2.5 Self-reported morbidity
Participants were asked to indicate whether they had any of the following chronic diseases: arterial hypertension, diabetes, chronic depression, osteoarthritis, high cholesterol, chronic obstructive pulmonary disease (COPD), problems in thyroid, asthma, hemorrhoids, malignant tumor, osteoporosis, embolism, heart attack or cerebral hemorrhage, cirrhosis or liver dysfunction, and heart diseases (based on the Spanish National Health Survey).
2.4 Statistical analysis
Categorical variables are presented in absolute numbers, percentages and CI95%, while quantitative variables are presented as means and standard deviations (SD) or medians and interquartile ranges (IQR).
To assess the relationship between material, psychosocial, behavioral factors and chronic conditions with SRH the chi-squared test and Student’s t-test were used; p-values under 0.05 were considered statistically significant (2-sided tests). We only assessed the relationship with SRH for comorbidities with a prevalence greater than 2%.
Generalized linear model with a normal distributed dependant variable and identity link function was performed. Independent variables showing a statistical significance of p < 0.20 and potential confounding factors (smoking, BMI, fruit and vegetable intake, physical activity) were selected. Final predictive variables were selected from a backward stepwise procedure; Akaike’s information criterion AIC (75) and the Bayesian information criterion BIC (76) were used for model selection.
We further tested interactions of age and LOC with lifestyles and occupational stress.
SPSS for Windows version 23.0 and STATA version 13 were used for analyses.
3 Results
A total of 1,043 HHs were included. Their sociodemographic and material characteristics are displayed in Table 1. Most participants were Spanish, had completed compulsory education, worked under a recurring-seasonal contract and in a four-star hotel. The median of hours worked per week was 40 (IQR = 40.0–40.0) and the median of rooms cleaned per day was 18 (IQR = 15.0–22.0). More than a half indicated difficulties making ends meet.
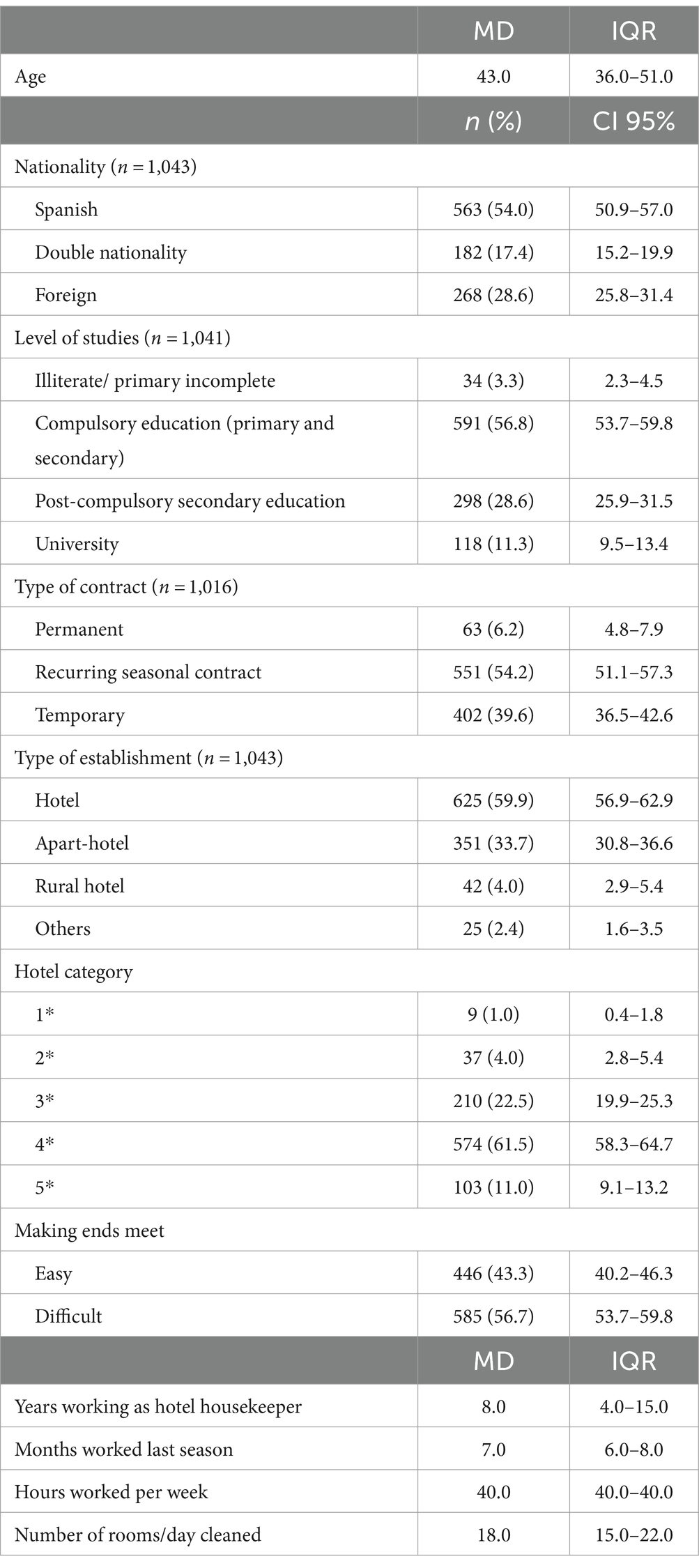
Table 1. Sociodemographic, anthropometric and material characteristics of hotel housekeepers.
Psychosocial factors and lifestyles of HHs are shown in Tables 2, 3. The median of the level of occupational stress was 5.0 (IQR 4.0–6.0); most of the HHs had normal social support, an external LOC and WLB difficulties. Over 50% were non-smokers and insufficiently physically active. Nearly 80% of the participants ate less than 5 servings of fruit and vegetables a day, and almost 50% had normal weight.
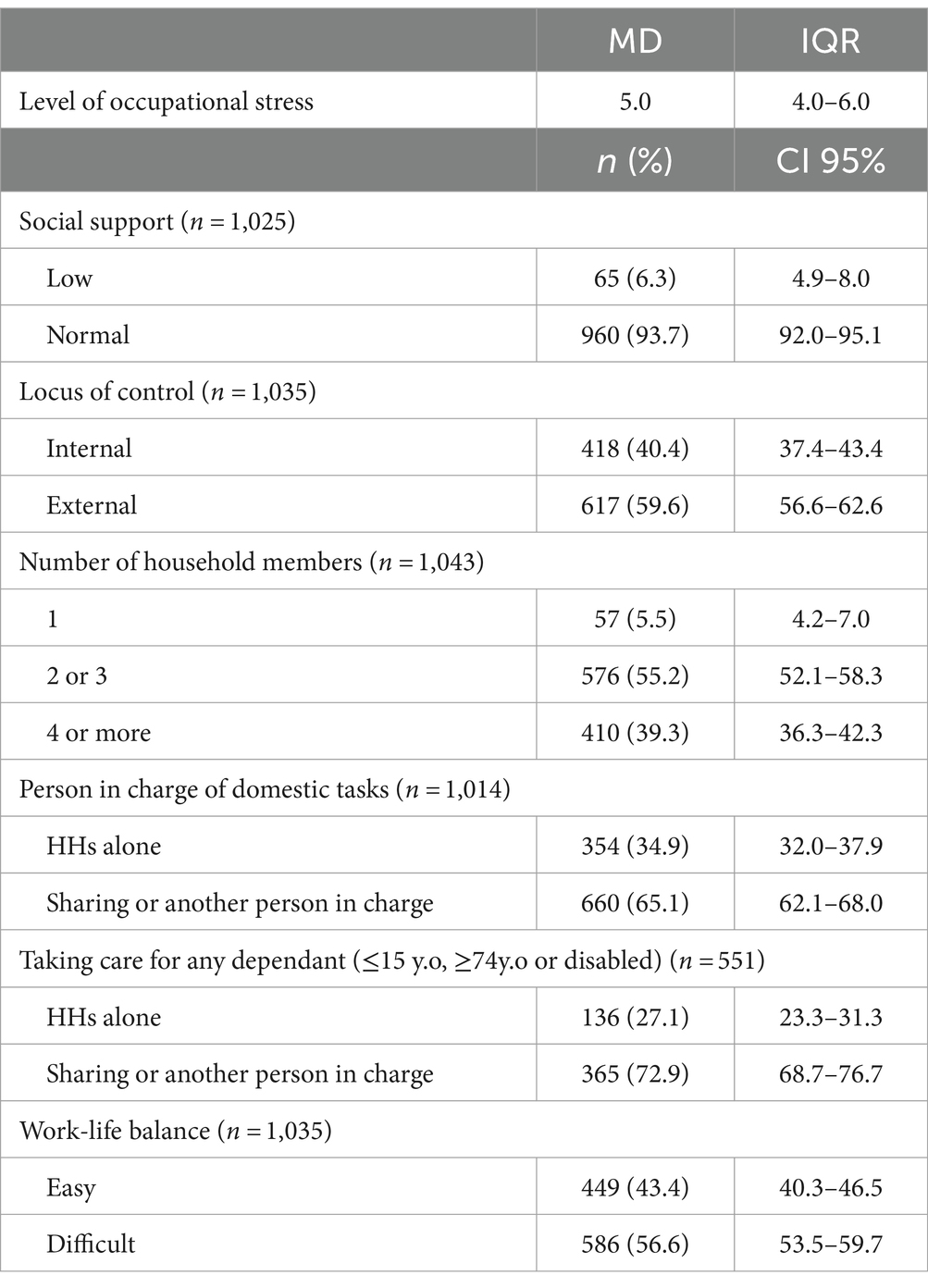
Table 2. Characteristics regarding psychosocial factors of hotel housekeepers.
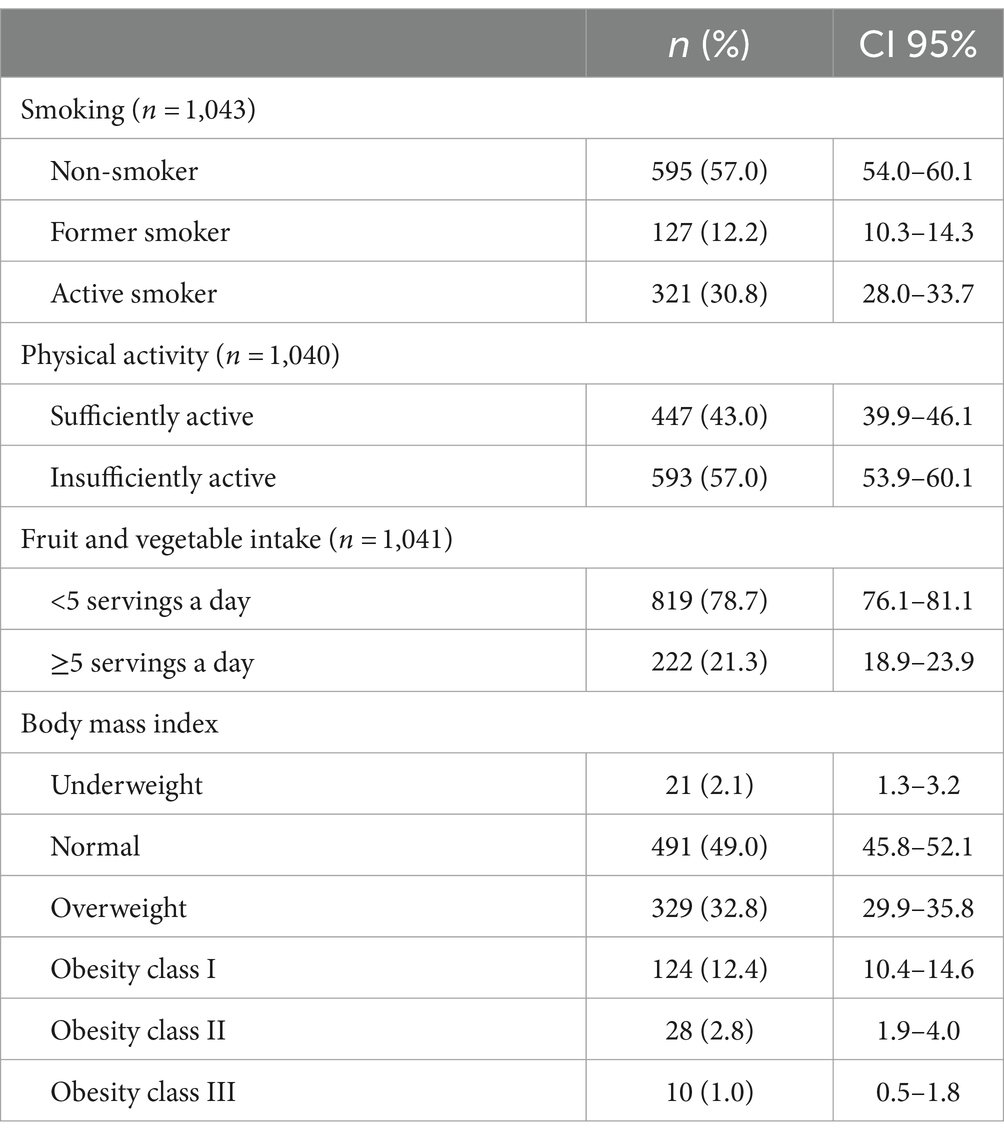
Table 3. Characteristics regarding behavioral factors of HHs.
The mean of the SRH was 72.4 (SD = 19.0). Results of the association between sociodemographic, anthropometric, material, psychosocial and behavioral factors and SRH (Table 4) show that HHs with a lower SRH were older (p < 0.001), had Spanish nationality (p < 0.001), had attained a lower level of studies (p = 0.007), had permanent or recurring seasonal contract (p = 0.039), had been working as HHs for longer (p ≤ 0.001), had financial difficulties (p < 0.001), had a higher level of occupational stress (p < 0.001), an external LOC (p = 0.001), reported WLB difficulties (p < 0.001), were former smokers (p = 0.012), were insufficiently physical active (p = 0.040) and were obese (p = 0.002).
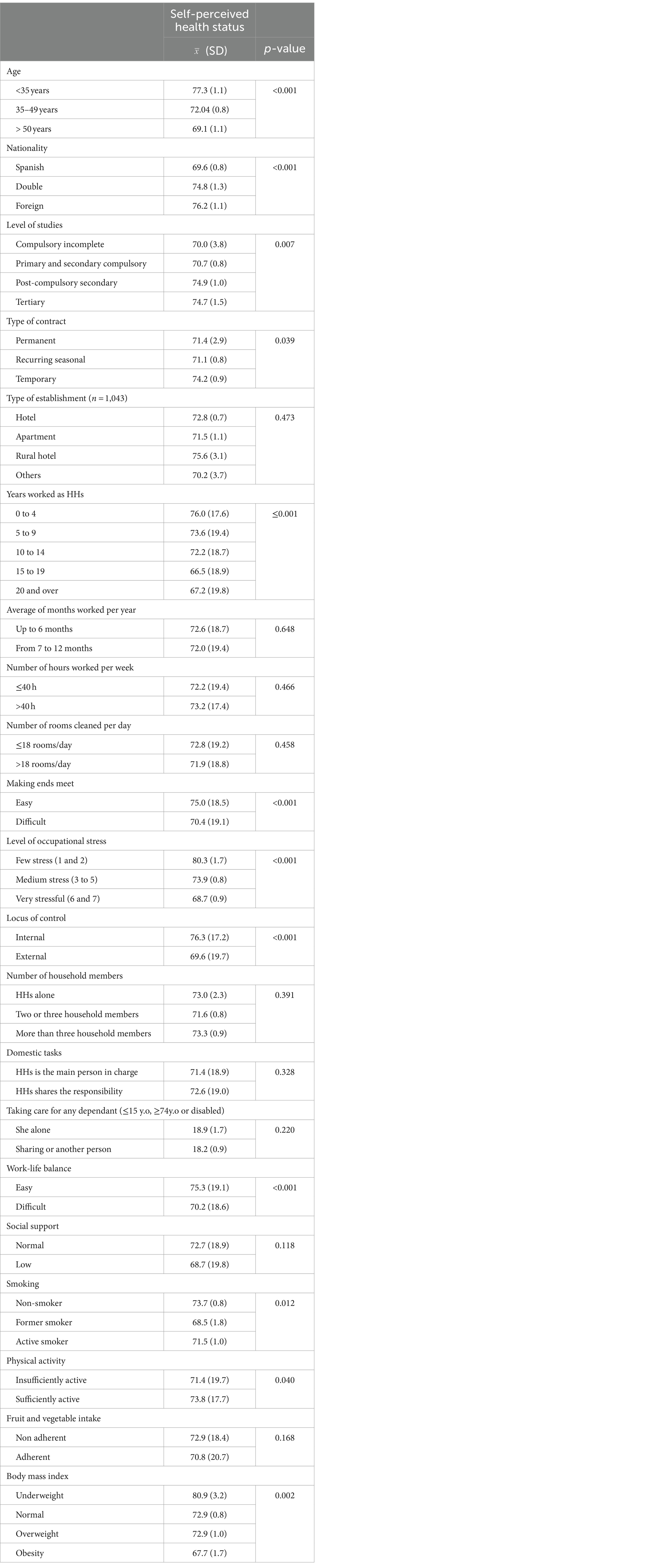
Table 4. Association between individual, material, psychosocial and behavioral factors with self-rated health.
Morbidity was significantly associated with SRH: those with arterial hypertension (p = 0.001), diabetes (p = 0.004), osteoarthritis (p ≤ 0.001) and chronic depression (p ≤ 0.001), COPD (p = 0.003), problems in thyroid (p = 0.007), hemorrhoids (p = 0.008) had lower levels of SRH (Table 5).
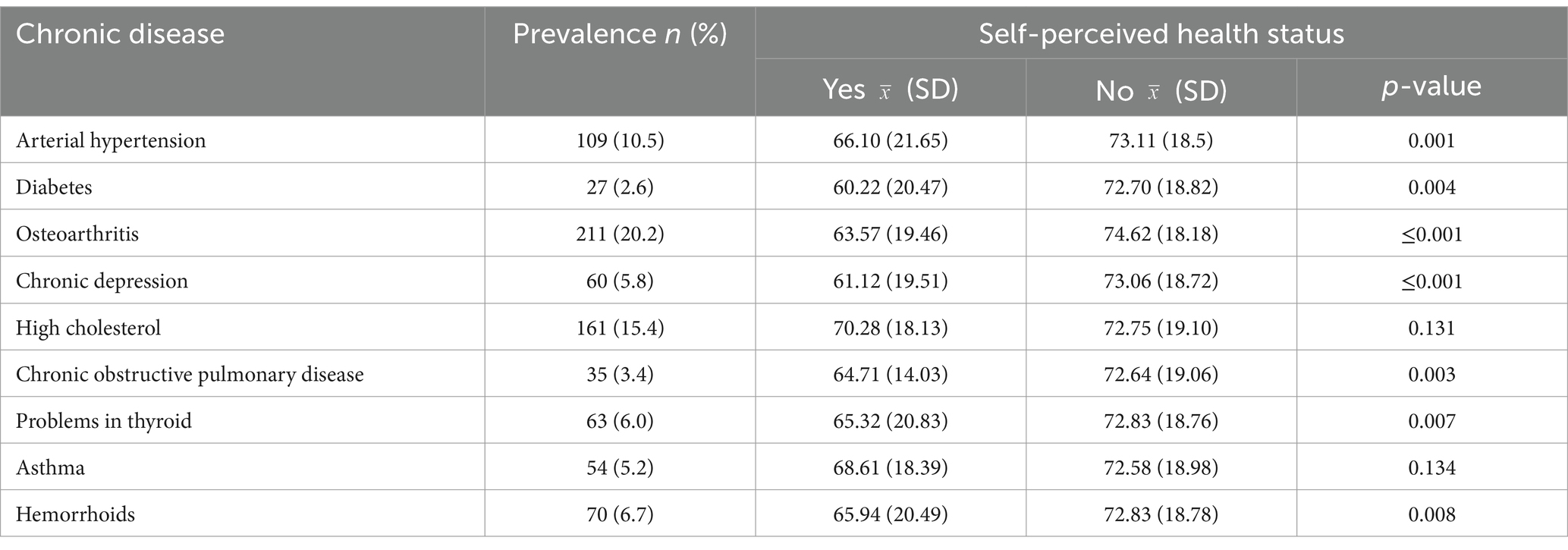
Table 5. Association between self-reported morbidity with self-rated health.
3.1 Determinants of SRH
Lower SRH scores were observed among HHs: with osteoarthritis, mean difference: -7.159 (CI95% −10.20- -4.12); with chronic depression, −6.858 (CI95% -11.89- -1.82); who reported difficulties in WLB, −3.697 (CI95% -6.08- -1.31); who performed insufficient physical activity, −2.414 (CI95% -4.69- -0.13); who reported financial strain, −2.107 (CI% -4.44- -0.23). Lower SRH was also associated to a higher perceived stress, −1.440 (CI95% -2.09- -0.79); BMI (kg/m2), −0.299 (CI95% -0.53- -0.07); and longer time working as HH, −0.177 (CI95% -0.33- -0.03) (Table 6).
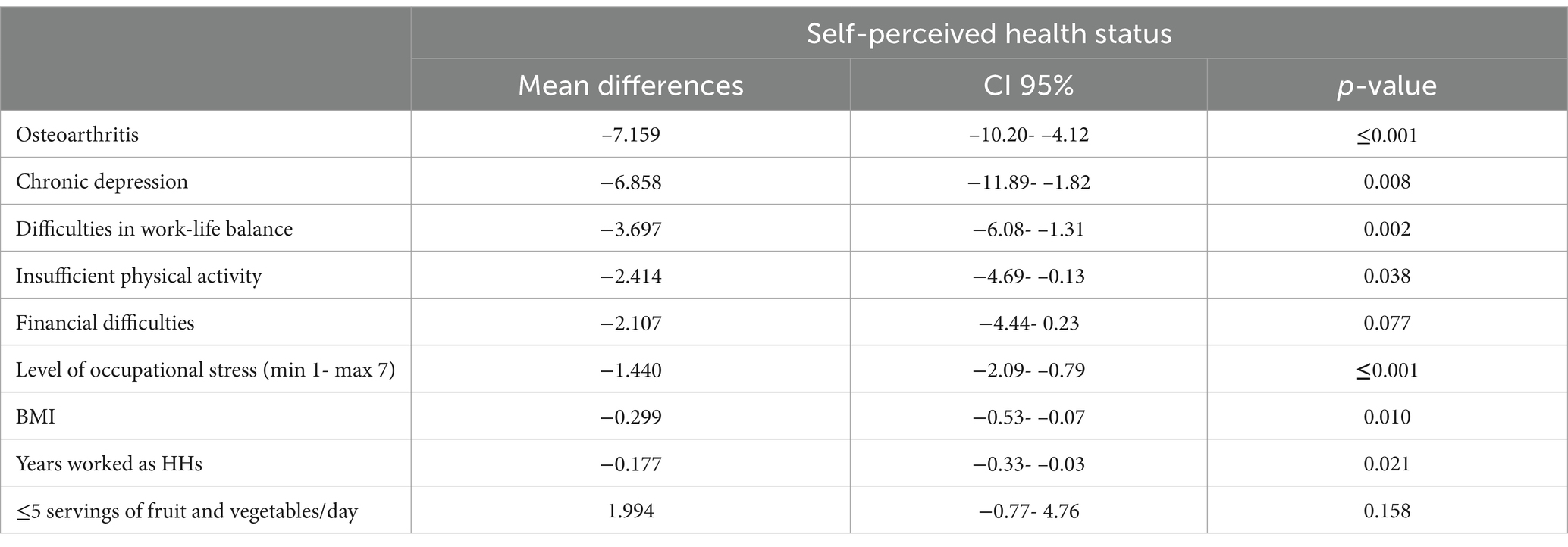
Table 6. Generalized linear model to analyze the association of sociodemographic, anthropometric, psychosocial, behavioral and material characteristics with self-perceived health status in hotel housekeepers, adjusted by age.
Surprisingly, we found a negative association between the recommended fruit and vegetable daily intake and SRH status.
4 Discussion
This study analyses the relationship between SRH and sociodemographics, anthropometrics, material, psychosocial and behavioral factors as well as chronic diseases among HHs in the Balearic Islands. HHs mostly worked under recurring seasonal contracts (54.2%), with a median of 7 months worked during the 2018 season, underscoring the financial insecurity of this occupation. Regarding domestic tasks, more than one third reported to be the main person in charge, and almost one third indicated to take care herself alone for dependants. More than half HHs reported difficulties in WLB and making ends meet. One third were active smokers, almost two thirds were insufficiently physically active and more than 75% ate less than five servings of fruit and vegetables a day.
After controlling for confounding factors, we found a reduction in SRH status score among HHs with osteoarthritis, chronic depression, with difficulties in balancing work and life spheres, performing insufficient physical activity, reporting financial strain, and as levels of stress, BMI and years worked as HHs increased.
Besides this, the relevance of this study lies on focusing on a lower-status occupational group, since most previous studies report on skilled professionals (77).
The mean score of SRH is lower compared to that among the Balearic Islands general population: 72.4 (SD 19.0) vs. 75.99 (SD 19.71) (78). Moreover, the mean score among HHs is lower in all age groups compared to the reference norms in Spanish women reported in Hernandez et al. (79). These differences are higher in the youngest groups: HHs younger than 35 years old reported a mean score of 77.3 (SD 1.1) while the score was 84.5 to 87.0 among women between 18 and 34 years old. The high physical demands (3) and high work pace (2, 13) could partly explain this difference. Notably, the systematic review carried out by Dieker et al. (26) revealed that workers with a low socioeconomic status were at higher risk of poor SRH.
Our results indicated that chronic disease was associated with a worse SRH, in line with several studies. Higher number of chronic conditions have been associated with worse SRH (79) and quality of life (80) Concretely, Van Schoor et al. (81) found that clinical osteoarthritis was associated with fair-to-poor SRH, partly mediated by physical function. Val Jiménez et al. (82) identified a weak but negative correlation between the number of articulations affected by osteoarthritis and the SRH status ratings in the EuroQoL VAS.
Also our results indicated a negative relationship between SRH and depression. Previous studies found that, after adjusting for confounding variables, people rating their health as poor to fair were at higher risk of depression and anxiety compared to those who rated their health as good to excellent (83, 84). Notably, low socio-economic status and job strain has also been found to be associated with higher prevalence of depression (85–87).
Chela-Alvarez et al. (88) found that HHs identified stress, anxiety and MSD as the main occupational health problems. Results of Hsieh et al. (13) revealed that Latina HHs working in the United States usually experienced stress. Similarly, in the qualitative study of Chela-Alvarez et al. (2) conducted in the Balearic Islands, HHs emphasized the occupational stress derived from the high demands, and the lack of resources and little control (mainly because of incompatible demands) over their job. Also, this stress increased their levels of anxiety. Several studies carried out among workers found a negative relationship between experiencing stress and SRH (41, 89). Further, Nappo (90) found a negative relationship between working speed and SRH.
Similar to our results, several studies found a statistically significant association between WFC and poorer SRH (24, 48, 1). Despite this, some others suggest that poor SRH precede WFC (49). Lunau et al. (50) found that odd ratios adjusted (aORs) for sociodemographic, occupational, working conditions and household characteristics showed that women with poor WLB were twice more likely to report poor SRH.
Moreover, Nappo (90) found that workers whose job prevented them from devoting the time they wanted to their family and those who keep worrying about work during non-working hours (two components of WFC) were more likely to have low SRH. Studies identified a stronger relationship between WFC and suboptimal SRH also in highly educated women (48); however, results of our study among a low skilled and less educated group corroborate that WFC is an important factor that negatively affects SRH. Although Mensah and Adjei (71) found a higher prevalence of poor WLB in men compared to women, the aOR measuring the association between poor WLB and poor SRH among workers were slightly higher for women [aOR =2.21; CI95%: (1.99–2.45) and for men aOR = 1.97; CI95%: (1.78–2.18)]. Longitudinal studies are still needed to establish the direction of causation.
The proportion of HHs reporting insufficient physical activity outside work (57%) was higher than that among Spanish unskilled workers (41.5%) (91). We hypothesize that the physical tiredness of the HHs’ job prevents them from engaging in physical activity outside work or compensates low levels of physical activity outside work. Moreover, while physical activity has been associated with health benefits (92), worldwide the prevalence of insufficient physical activity is higher among women (93). Consistent with our results, Jepsen et al. (94) found that light or strenuous physical activity decreased the likelihood of fair/poor health; and van Oostrom et al. (41) found that workers with a low educational level who performed insufficient physical activity and were overweight or obese were more likely to report poor health. Also, Zarini et al. (59), after adjusting for age, lifestyles behaviors, ethnicity, health insurance and comorbidities, found that women who were physically inactive were more likely to report poor/fair SRH compared to those physically active. Additionally, Van der Berge et al. (95) found that workers in demanding physical activity occupations, obese and performing low levels of leisure time vigorous physical activity report lower levels of SRH. This association has been explained by “the physical activity paradox” (96): the negative effects of occupational physical activity on workers’ global health.
Data from the Spanish National Health Survey (91) indicated that the prevalence of obesity among unskilled workers (24%) was eight points higher than that described among HHs of this study. The daily physical demands of hotel housekeeping might partly explain this lower proportion of participants with obesity. In our study, after adjusting for age, chronic health conditions, and behavioral, psychosocial and material characteristics, BMI was associated negatively with SRH. Similarly, Hellgren et al. (97) reported a negative association between BMI and SRH at different ages and in both sexes, and independent of comorbidities. Also, Busutil et al. (98) found that, after controlling by chronic diseases, people with obesity reduced EuroQoL’s VAS score by an average of 1.9 and 3.7 points, compared to those with normal weight. And results of the longitudinal case–control study of Hulman et al. (99) indicated that poor SRH was associated with a higher BMI.
Our findings also indicated that financial strain affects negatively HHs’ health status, accordingly to previous research (100–21). Other studies have found a relation between indebtedness and a lower probability of reporting good or very good health (51, 102). Additionally, the study Artazcoz et al. (25) revealed that, after adjusting for age, migrant status, occupational and household characteristics, almost half of the workers in Southern European countries suffered financial strain, which was related to poor SRH and to low psychological well-being. Also, Hsieh et al. (13) revealed that sources of stress among Latina HHs working in the United States were work and family finances.
In our study, the proportion of active smokers (30.8%) was 10 points higher than daily and occasional smokers among Spanish unskilled workers (91). The inverse association between socioeconomic status and smoking has been described, but the work of Martinez et al. (103) included four latent variables (social cohesion, financial strain, sleep disturbance and psychological distress) in the association and found that higher socioeconomic status was negatively related to financial strain, and this “led to an increase in both sleep disturbance and psychological distress, which both resulted in an increase of smoking.” Also, higher socioeconomic status was related to an increased social cohesion, which made decrease smoking habits. The high proportion of HHs who reported financial difficulties and the stress related to their job might be an explanation for this higher proportion of smokers in our study.
Only 21.3% of our sample reported having five or more servings a day of fruit and vegetables; like in the other healthy behaviors, people with higher education levels are more likely to consume more fruits and vegetables (104). There are few studies to analyze the association between fruit and vegetable intake and SRH. In the living from Health program study, they found a positive relationship between fruit and vegetables intake and SRH (59). Our results indicated an inverse association between eating five or more serving of fruit and vegetable and SRH. In this cross-sectional study reverse causation might explain this counterintuitive relationship: people with lower scores of SRH being more aware of a healthy diet.
Despite performing insufficient physical activity and higher BMI, we did not found that lifestyle factors were related to a better SRH. The systematic review by Dieker et al. (26) concluded that socioeconomic inequalities in SRH depended on work factors, irrespective of the lifestyle.
Our findings suggest the importance of adapting interventions to the socioeconomic characteristics of the targeted population and focusing on the improvement of material and psychosocial factors more than behavioral in order to improve health status.
Public health decision makers must take into consideration all these variables when designing interventions to improve HHs’ health. Our results underscore the importance of health conditions, material and psychosocial factors; thus, interventions aimed to improve health status must be adapted to different socioeconomic groups. Also, governments should audit and regulate stress levels in companies. Further, policies and programs aiming to decrease financial strain among lower socioeconomic status families should be strengthen; these might include facilitating access to housing (social housing, subsidies…), enhancing public transport, as well as widening the offer of affordable physical activities. Moreover, since HHs work more intensely during summer months, availability of subsidized summer schools for their children should reduce WFC.
5 Strengths and limitations
As far as we know, this is the largest study conducted among HHs. The sample of 1,043 HHs is sufficient to guarantee its sensitivity and the randomization guarantee its representativeness of the population of HHs in the Balearic Islands. However, there is a limitation inherent to cross-sectional studies: results are susceptible to reverse causality, as we already mentioned in the discussion section, and causation cannot be proved. Also, data were collected in winter, when most HHs do not work or have less workload, since they were more available to participate; this situation might have influenced the results regarding SRH. Furthermore, data collection took place before the COVID19 pandemic, which has probably altered the situation to some degree.
Regarding the dependent variable of our study, the advantages of the EuroQol VAS in determining SRH include its simplicity, ease of administration, and straightforward scoring. However, the EQ-VAS relies on subjective evaluation based on an individual’s self-assessment of their health status, which can be influenced by factors such as locus of control, age, and educational attainment (105). Additionally, some studies have found that the EuroQol VAS is less sensitive and less responsive to changes in clinical outcomes than the completed EuroQol-5D (106). Lastly, work stress was assessed using a single question. This approach may not capture the full complexity of work stress experienced by individuals in specific occupations. Using a more comprehensive work stress scale would have provided a more accurate measurement. Therefore, the reliance on a single-question measure should be acknowledged as a limitation, as it may not fully reflect the multifaceted nature of occupational stress.
Finally, data have been collected in just one region of Spain. Housekeeping is a precarious occupation because of the temporality of the economic activity and because it is considered an unskilled job. However, in the Balearic Islands the trade unions have achieved better occupational conditions than other regions. For instance, in the Balearic Islands outsourcing is not allowed and hotel housekeepers work with a contract and not per hours, characteristics that have to be taken into account when comparing our results with those obtained in other settings.
Data availability statement
The datasets presented in this study can be found in online repositories. The names of the repository/repositories and accession number(s) can be found at: https://doi.org/10.5281/zenodo.10610378.
Ethics statement
The study was approved by the Balearic Islands Research Ethics Committee (IB3738/18 PI). An information sheet and informed consent form was given to the participants before being enrolled. Signed agreement of the forms was compulsory to participate. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
Author contributions
XC-A: Conceptualization, Formal analysis, Investigation, Methodology, Project administration, Writing – original draft, Writing – review & editing. AL: Data curation, Formal analysis, Methodology, Writing – review & editing. OB: Conceptualization, Data curation, Investigation, Methodology, Writing – review & editing. JL: Conceptualization, Funding acquisition, Methodology, Project administration, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. This research is part of the wider Project, “Hotel housekeepers and health,” which is funded by Sustainable Tourism’s Tax Fund (Balearic Islands Government), grant no. ITS’17–096. The funders had no role in the design of the study; in the collection, analysis, or interpretation of the data; in the writing of the manuscript, or in the decision to publish the results.
Acknowledgments
We are grateful to all HHs who accepted to participate and were interviewed. We also thank the collaboration of all participating health care centers.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Government of India . Estudio del impacto económico del Turismo sobre la economía y el empleo de las Islas Baleares. (2015). Available at: http://www.exceltur.org/wp-content/uploads/2015/10/IMPACTUR-Baleares-2014-informe-completo.pdf (Accessed October 27, 2023).
2. Chela-Alvarez, X, Bulilete, O, García-Buades, ME, Ferrer-Perez, VA, and Llobera-Canaves, J. Perceived factors of stress and its outcomes among hotel housekeepers in the Balearic Islands: a qualitative approach from a gender perspective. Int J Environ Res Public Health. (2021) 18:18. doi: 10.3390/ijerph18010052
3. Hunter Powell, P, and Watson, D. Service unseen: the hotel room attendant at work. Int J Hosp Manag. (2006) 25:297–312. doi: 10.1016/j.ijhm.2005.04.003
4. Krause, N, Scherzer, T, and Rugulies, R. Physical workload, work intensification, and prevalence of pain in low wage workers: results from a participatory research project with hotel room cleaners in Las Vegas. Am J Ind Med. (2005) 48:326–37. doi: 10.1002/ajim.20221
5. Wami, SD, Abere, G, Dessie, A, and Getachew, D. Work-related risk factors and the prevalence of low back pain among low wage workers: results from a cross-sectional study. BMC Public Health. (2019) 19:1072–9. doi: 10.1186/s12889-019-7430-9
6. Wami, SD, Dessie, A, and Chercos, DH. The impact of work-related risk factors on the development of neck and upper limb pain among low wage hotel housekeepers in Gondar town, Northwest Ethiopia: institution-based cross-sectional study. Environ Health Prev Med. (2019) 24:27. doi: 10.1186/s12199-019-0779-7
7. Rahman, MNA, and Jaffar, MSM. Musculoskeletal symptoms and ergonomic hazards among room attendants in hotel industries. Malays J Hum Factors Ergon. (2017) 1:24–33.
8. Cañada, E . Las que limpian los hoteles. Historias ocultas de precariedad laboral. Barcelona: Icaria (2015).
9. Lee, JW, Lee, JJ, Mun, HJ, Lee, K-J, and Kim, JJ. The relationship between musculoskeletal symptoms and work-related risk factors in hotel workers. Ann Occup Environ Med. (2013) 25:20. doi: 10.1186/2052-4374-25-20
10. Leroux, I, Brisson, C, and Montreuil, S. Job strain and neck-shoulder symptoms: a prevalence study of women and men white-collar workers. Occup Med (Chic Ill). (2006) 56:102–9. doi: 10.1093/occmed/kqj005
11. Sánchez-Rodríguez, C, Bulilete, O, Chela-Alvarez, X, Velasco-Roldán, O, and Llobera-Canaves, J. Chronic pain andWork conditions of hotel housekeepers: a descriptive study. Int J Environ Res Public Health. (2022) 19:3383. doi: 10.3390/ijerph19063383
12. Jerrie Hsieh, YC, and Chen, YL. Hotel housekeepers' job stress In: YC Jerrie Hsieh , editor. Recreation, Parks, and Tourism in Public Health. Bloomington, Indiana: Indiana University Press (2020). 15–32.
13. Hsieh, Y-C, Apostolopoulos, Y, and Sönmez, S. Work conditions and health and well-being of Latina hotel housekeepers. J Immigr Minor Health. (2016) 18:568–81. doi: 10.1007/s10903-015-0224-y
14. Centers for Disease Control and Prevention . Health, United States, 2020-2021. Available at: https://www.cdc.gov/nchs/hus/sources-definitions/health-status.htm (Accessed on July 12, 2024).
15. World Health Organization . Constitution. (2024). Available at: https://www.who.int/about/governance/constitution. (Accessed July 12, 2024).
16. Baćak, V, and Ólafsdóttir, S. Gender and validity of self-rated health in nineteen European countries. Scand J Public Health. (2017) 45:647–53. doi: 10.1177/1403494817717405
17. Schnittker, J, and Bacak, V. The increasing predictive validity of self-rated health. PLoS One. (2014):9. doi: 10.1371/journal.pone.0084933
18. Moor, I, Spallek, J, and Richter, M. Explaining socioeconomic inequalities in self-rated health: a systematic review of the relative contribution of material, psychosocial and behavioural factors. J Epidemiol Community Health. (2017) 71:565–75. doi: 10.1136/jech-2016-207589
19. Prus, SG . Comparing social determinants of self-rated health across the United States and Canada. Soc Sci Med. (2011) 73:50–9. doi: 10.1016/j.socscimed.2011.04.010
20. Balaj, M, Mcnamara, CL, Eikemo, TA, and Bambra, C. The social determinants of inequalities in self-reported health in Europe: findings from the European social survey (2014) special module on the social determinants of health. Eur J Public Health. (2017) 27:107–14. doi: 10.1093/eurpub/ckw217
21. Mackenbach, JP, Martikainen, P, Looman, CWN, Dalstra, JAA, Kunst, AE, Lahelma, E, et al. The shape of the relationship between income and self-assessed health: an international study. Int J Epidemiol. (2005) 34:286–93. doi: 10.1093/ije/dyh338
22. Mackenbach, JP . The persistence of health inequalities in modern welfare states: the explanation of a paradox. Soc Sci Med. (2012) 75:761–9. doi: 10.1016/j.socscimed.2012.02.031
23. World Health Organization . A conceptual framework for action on the social determinants of health. Geneva, Switzerland: World Health Organization (2010).
24. Borgmann, LS, Rattay, P, and Lampert, T. Health-related consequences of work-family conflict from a European perspective: results of a scoping review. Front Public Health. (2019) 7:1–12. doi: 10.3389/fpubh.2019.00189
25. Artazcoz, L, Cortès-Franch, I, Escribà-Agüir, V, and Benavides, FG. Financial strain and health status among European workers: gender and welfare state inequalities. Front Public Health. (2021) 9:9. doi: 10.3389/fpubh.2021.616191
26. Dieker, A, Ijzelenberg, W, Proper, KI, Burdorf, A, Ket, J, Van Der Beek, A, et al. The contribution of work and lifestyle factors to socioeconomic inequalities in self-rated health - a systematic review. Scand J Work Environ Health. (2019) 45:114–25. doi: 10.5271/sjweh.3772
27. Eikemo, TA, Huijts, T, Bambra, C, McNamara, C, Stornes, P, and Balaj, M. Desigualdades sociales en salud y sus determinantes: Principales resultados de la séptima edición de la Encuesta Social Europea (2016). Available at: https://www.europeansocialsurvey.org/sites/default/files/2023-06/TL6_Health-Spanish.pdf. (Accessed December 4, 2024).
28. Kyriopoulos, I, Zavras, D, and Charonis, A. Indebtedness, socioeconomic status, and self-rated health: empirical evidence from Greece. Poverty Public Policy. (2016) 8:387–97. doi: 10.1002/pop4.160
29. Białowolski, P, Węziak-Białowolska, D, and VanderWeele, TJ. The impact of savings and credit on health and health behaviours: an outcome-wide longitudinal approach. Int J Public Health. (2019) 64:573–84. doi: 10.1007/s00038-019-01214-3
30. Tsuchiya, K, Leung, CW, Jones, AD, and Caldwell, CH. Multiple financial stressors and serious psychological distress among adults in the USA. Int J Public Health. (2020) 65:335–44. doi: 10.1007/s00038-020-01354-x
31. Pinillos-Franco, S, and García-Prieto, C. The gender gap in self-rated health and education in Spain. A multilevel analysis. PLoS One. (2017) 12:1–11. doi: 10.1371/journal.pone.0187823
32. Väänänen, A, Kevin, MV, Ala-Mursula, L, Pentti, J, Kivimäki, M, and Vahtera, J. The double burden of and negative spillover between paid and domestic work: associations with health among men and women. Women Health. (2004) 40:1–18. doi: 10.1300/J013v40n03_01
33. Hagqvist, E, Gådin, KG, and Nordenmark, M. Division of labor, perceived labor-related stress and well-being among European couples. Open J Prev Med. (2012) 2:452–60. doi: 10.4236/ojpm.2012.24064
34. Artazcoz, L, Cortès, I, Puig-Barrachina, V, Benavides, FG, Escribà-Agüir, V, and Borrell, C. Combining employment and family in Europe: the role of family policies in health. Eur J Pub Health. (2014) 24:649–55. doi: 10.1093/eurpub/ckt170
35. Kim, YM, and Il, CS. Associations of family demands and work–life conflict with musculoskeletal disorders among korean workers. Int J Environ Res Public Health. (2018) 15:15. doi: 10.3390/ijerph15071419
36. Arcas, MM, Novoa, AM, and Artazcoz, L. Gender inequalities in the association between demands of family and domestic life and health in Spanish workers. Eur J Pub Health. (2013) 23:883–8. doi: 10.1093/eurpub/cks095
37. Hsieh, Y-C, Apostolopoulos, Y, Hatzudis, K, and Sönmez, S. Occupational exposures and health outcomes among Latina hotel cleaners. Hisp Health Care Int. (2014) 12:6–15. doi: 10.1891/1540-4153.12.1.6
38. Hsieh, Y-C, Sönmez, S, Apostolopoulos, Y, and Lemke, MK. Perceived workplace mistreatment: case of Latina hotel housekeepers. Work. (2017) 56:55–65. doi: 10.3233/WOR-162467
40. Zhao, X(R), Qu, H, and Liu, J. An investigation into the relationship between hospitality employees’ work–family conflicts and their leisure intentions. Cornell Hosp Q. (2014) 55:408–21. doi: 10.1177/1938965513517171
41. van Oostrom, S, Nachat, A, Loef, B, and Proper, K. The mediating role of unhealthy behaviors and body mass index in the relationship between high job strain and self-rated poor health among lower educated workers. Int Arch Occup Environ Health. (2021) 94:95–105. doi: 10.1007/s00420-020-01565-y
42. Thoits, PA . Conceptual, methodological, and theoretical problems in studying social support as a buffer against life stress. J Health Soc Behav. (1982) 23:145–59. doi: 10.2307/2136511
43. Passarelli-Araujo, H . The association between social support and self-rated health in midlife: are men more affected than women? Cad Saude Publica. (2023) 39:e00106323. doi: 10.1590/0102-311XEN106323
44. Wang, HH, Wu, SZ, and Liu, YY. Association between social support and health outcomes: a meta-analysis. Kaohsiung J Med Sci. (2003) 19:345–50. doi: 10.1016/S1607-551X(09)70436-X
45. Brønholt, RL, Hansen, MB, Islamoska, S, Christensen, U, Grynderup, MB, and Nabe-Nielsen, K. Physical and psychosocial work factors as explanations for social inequalities in self-rated health. Int Arch Occup Environ Health. (2021) 94:335–46. doi: 10.1007/s00420-020-01582-x
46. Greenhaus, JH, and Beutell, NJ. Sources of conflict between work and family roles. Acad Manag Rev. (2011) 10:76–88. doi: 10.5465/amr.1985.4277352
47. Sirgy, MJ, and Lee, DJ. Work-life balance: an integrative review. Appl Res Qual Life. (2018) 13:229–54. doi: 10.1007/s11482-017-9509-8
48. Griep, RH, Toivanen, S, van Diepen, C, Guimarães, JMN, Camelo, LV, Juvanhol, LL, et al. Work–family conflict and self-rated health: the role of gender and educational level. Baseline data from the Brazilian longitudinal study of adult health (ELSA-Brasil). Int J Behav Med. (2016) 23:372–82. doi: 10.1007/s12529-015-9523-x
49. Leineweber, C, Baltzer, M, Magnusson Hanson, LL, and Westerlund, H. Work-family conflict and health in Swedish working women and men: a 2-year prospective analysis (the SLOSH study). Eur J Pub Health. (2013) 23:710–6. doi: 10.1093/eurpub/cks064
50. Lunau, T, Bambra, C, Eikemo, TA, Van Der Wel, KA, and Dragano, N. A balancing act? Work-life balance, health and well-being in European welfare states. Eur J Pub Health. (2014) 24:422–7. doi: 10.1093/eurpub/cku010
51. Eurofund (editor). European quality of life survey 2016: Quality of life, quality of services and quality of society. Luxembourg: Publications Office of the European Union (2017). 76. Available at: https://www.eurofound.europa.eu/publications/report/2017/fourth-european-quality-of-life-survey-overview-report (Accessed July 11, 2023).
52. Warren, T . Work-life balance/imbalance: the dominance of the middle class and the neglect of the working class. Br J Sociol. (2015) 66:691–717. doi: 10.1111/1468-4446.12160
53. Whiston, SC, and Cinamon, RG. The work-family interface: integrating research and career counseling practice. Career Dev Q. (2015) 63:44–56. doi: 10.1002/j.2161-0045.2015.00094.x
54. Rotter, JB . Generalized expectancies for internal versus external control of reinforcement. Psychol Monogr Gen Appl. (1966) 80:1–28. doi: 10.1037/h0092976
55. Mounce, LTA, Campbell, JL, Henley, WE, Tejerina Arreal, MC, Porter, I, and Valderas, JM. Predicting incident multimorbidity. Ann Fam Med. (2018) 16:322–9. doi: 10.1370/afm.2271
56. Kesavayuth, D, Poyago-Theotoky, J, and Zikos, V. Locus of control, health and healthcare utilization. Econ Model. (2020) 86:227–38. doi: 10.1016/j.econmod.2019.06.014
57. Hämmig, O, Gutzwiller, F, and Kawachi, I. The contribution of lifestyle and work factors to social inequalities in self-rated health among the employed population in Switzerland. Soc Sci Med. (2014) 121:74–84. doi: 10.1016/j.socscimed.2014.09.041
58. Pisinger, C, Toft, U, Aadahl, M, Glümer, C, and Jørgensen, T. The relationship between lifestyle and self-reported health in a general population: the Inter99 study. Prev Med (Baltim). (2009) 49:418–23. doi: 10.1016/j.ypmed.2009.08.011
59. Zarini, GG, Vaccaro, JA, Terris, MAC, Exebio, JC, Tokayer, L, Antwi, J, et al. Lifestyle behaviors and self-rated health: the living for health program. J Environ Public Health. (2014) 2014:1–9. doi: 10.1155/2014/315042
60. Stenholm, S, Head, J, Aalto, V, Kivimäki, M, Kawachi, I, Zins, M, et al. Body mass index as a predictor of healthy and disease-free life expectancy between ages 50 and 75: a multicohort study. Int J Obes. (2017) 41:769–75. doi: 10.1038/ijo.2017.29
61. Wang, M, Yi, Y, Roebothan, B, Colbourne, J, Maddalena, V, Wang, PP, et al. Body mass index trajectories among middle-aged and elderly Canadians and associated health outcomes. J Environ Public Health. (2016) 2016:4857. doi: 10.1155/2016/7014857
62. Newton, S, Braithwaite, D, and Akinyemiju, TF. Socio-economic status over the life course and obesity: systematic review and meta- analysis. PLoS One. (2017) 12:1–15. doi: 10.1371/journal.pone.0177151
63. Herdman, M, Badia, X, Berra, S, and Xavier, B. El EuroQol-5D: una alternativa sencilla para la medición de la calidad de vida relacionada con la salud en atención primaria. Atención Prim. (2001) 28:425–9. doi: 10.1016/S0212-6567(01)70406-4
64. The EuroQol Group . EuroQol-a new facility for the measurement of health-related quality of life. Health Policy (New York). (1990) 16:199–208. doi: 10.1016/0168-8510(90)90421-9
65. Puig-Ribera, A, Martín-Cantera, C, Puigdomenech, E, and Real, J. Screening physical activity in family practice: validity of the Spanish version of a brief physical activity questionnaire. PLoS One. (2015) 10:1–16. doi: 10.1371/journal.pone.0136870
66. Marshall, AL, Smith, BJ, Bauman, AE, and Kaur, S. Reliability and validity of a brief physical activity assessment for use by family doctors. Br J Sport Med. (2005) 39:294–7. doi: 10.1136/bjsm.2004.013771
67. Córdoba, R, Camarelles, F, Muñoz, E, Gómez, JM, San José, J, Ramírez, JI, et al. Recomendaciones sobre el estilo de vida. Actualización PAPPS 2018. Atención Prim. (2018) 50:29–40. doi: 10.1016/S0212-6567(18)30361-5
68. Smith, BJ, Marshall, AL, and Huang, N. Screening for physical activity in family practice: evaluation of two brief assessment tools. Am J Prev Med. (2005) 29:256–64. doi: 10.1016/j.amepre.2005.07.005
69. Bully, P, Sanchez, A, Grandes, G, Pombo, H, Arietalenizbeaskoa, MS, and Arce, V. Metric properties of the “prescribe healthy life” screening questionnaire to detect healthy behaviors: a cross-sectional pilot study. BMC Public Health. (2016) 16:1228–11. doi: 10.1186/s12889-016-3898-8
70. Ortiz-Gutiérrez, S, and Cruz-Avelar, A. Proceso de traducción y adaptación cultural de instrumentos de medición en salud. Actas Dermosifiliogr. (2018) 109:202–6. doi: 10.1016/j.ad.2017.09.012
71. Mensah, A, and Adjei, NK. Work-life balance and self-reported health among working adults in Europe: a gender and welfare state regime comparative analysis. BMC Public Health. (2020) 20:1–14. doi: 10.1186/s12889-020-09139-w
72. Broadhead, WE, Gehlbach, SH, Gruy, FV, and Kaplan, BH. The Duke-UNC functional social support questionnaire. Measurement of social support in family medicine patients. Med Care. (1988) 26:709–23. doi: 10.1097/00005650-198807000-00006
73. Bellón Saameño, JA, Delgado Sánchez, A, del Castillo, JD, and Lardelli, CP. Validity and reliability of the Duke-UNC-11 questionnaire of functional social support. Aten Primaria. (1996) 18:158–63.
74. De la Revilla, AL, Bailón, E, de Dios, LJ, Delgado, A, Prados, MA, and Fleitas, L. Validation of a functional social support scale for use in the family doctor’s office. Aten Primaria. (1991) 8:688–92.
75. Akaike, H . Information theory as an extension of the maximum likelihood principle. Second Int Symp Inf Theory. (1973):267–81.
76. Schwarz, G . Estimating the dimension of a model. Ann Stat. (1978) 6:461–4. doi: 10.1214/aos/1176344136
77. Borgmann, LS, Kroll, LE, Müters, S, Rattay, P, and Lampert, T. Work-family conflict, self-reported general health and work-family reconciliation policies in Europe: results from the European working conditions survey 2015. SSM Popul Heal. (2019) 9:100465. doi: 10.1016/j.ssmph.2019.100465
78. Garcia-Gordillo, MA, Adsuar, JC, and Olivares, PR. Normative values of EQ-5D-5L: in a Spanish representative population sample from Spanish health survey, 2011. Qual Life Res. (2016) 25:1313–21. doi: 10.1007/s11136-015-1164-7
79. Hernandez, G, Garin, O, Pardo, Y, Vilagut, G, Pont, À, Suárez, M, et al. Validity of the EQ–5D–5L and reference norms for the Spanish population. Qual Life Res. (2018) 27:2337–48. doi: 10.1007/s11136-018-1877-5
80. Makovski, TT, Schmitz, S, Zeegers, MP, Stranges, S, and Van Den Akker, M. Multiborbidity and quality of life: systematic literature review and meta-analysis. Ageing Res Rev. (2019) 53:100903. doi: 10.1016/j.arr.2019.04.005
81. Van Schoor, NM, Zambon, S, Castell, MV, Cooper, C, Denkinger, M, Dennison, EM, et al. Impact of clinical osteoarthritis of the hip, knee and hand on self-rated health in six European countries: the European project on OSteoArthritis. Qual Life Res. (2016) 25:1423–32. doi: 10.1007/s11136-015-1171-8
82. Val Jiménez, CL, López-Torres Hidalgo, J, García Atienza, EM, Navarro Ruiz, MS, Hernández Cerón, I, and Moreno de la Rosa, L. Situación funcional, autopercepción de salud y nivel de actividad física en pacientes con artrosis. Aten Primaria. (2017) 49:224–32. doi: 10.1016/j.aprim.2016.06.002
83. Ambresin, G, Chondros, P, Dowrick, C, Herrman, H, and Gunn, JM. Self-rated health and long-term prognosis of depression. Ann Fam Med. (2014) 12:57–65. doi: 10.1370/afm.1562
84. Östberg, D, and Nordin, S. Three-year prediction of depression and anxiety with a single self-rated health item. J Ment Health. (2022) 31:402–9. doi: 10.1080/09638237.2021.2022610
85. Freeman, A, Tyrovolas, S, Koyanagi, A, Chatterji, S, Leonardi, M, Ayudo-Mateos, JL, et al. The role of socio-economic status in depression: results from the COURAGE (aging survey in Europe). BMC Public Health. (2016) 16:1098. doi: 10.1186/s12889-016-3638-0
86. Lorant, V, Croux, C, Weich, S, Deliège, D, Mackenbach, J, and Ansseau, M. Depression and socio-economic risk factors: 7-year longitudinal population study. Br J Psychiatry. (2007) 190:293–8. doi: 10.1192/bjp.bp.105.020040
87. Madsen, IE, Nyberg, ST, Hanson, LM, Ferrie, JE, Ahola, K, Alfredsson, L, et al. Job strain as a risk factor for clinical depression: systematic review and meta-analysis with additional individual participant data. Psychol Med. (2017) 47:1342–56. doi: 10.1017/S003329171600355X
88. Chela-Alvarez, X, Bulilete, O, Garcia-Illan, E, Mc, V-T, and Llobera, J. Hotel housekeepers and occupational health: experiences and perceived risks. Ann Occup Environ Med. (2022) 34:e29. doi: 10.35374/aoem.2022.34.e29
89. Sánchez-Recio, R, García-Ael, C, and Topa, G. Investigating the relationship between stress and self-rated health during the financial crisis and recession in 2008: the mediating role of job satisfaction and social support in Spain. J Clin Med. 10:10. doi: 10.3390/jcm10071463
90. Nappo, N . Is there an association between working conditions and health? An analysis of the sixth European working conditions survey data. PLoS One. (2019) 14:e0211294–15. doi: 10.1371/journal.pone.0211294
91. Instituto Nacional de Estadística . Encuesta Nacional de Salud de España (2017). Available at: https://www.ine.es/dyngs/INEbase/es/operacion.htm?c=Estadistica_C&cid=1254736176783&menu=resultados&secc=1254736195650&idp=1254735573175.
92. Füzéki, E, Engeroff, T, and Banzer, W. Health benefits of light-intensity physical activity: a systematic review of accelerometer data of the National Health and nutrition examination survey (NHANES). Sport Med. (2017) 47:1769–93. doi: 10.1007/s40279-017-0724-0
93. Guthold, R, Stevens, GA, Riley, LM, and Bull, FC. Worldwide trends in insufficient physical activity from 2001 to 2016: a pooled analysis of 358 population-based surveys with 1.9 million participants. Lancet Glob Health. (2018) 6:e1077–86. doi: 10.1016/S2214-109X(18)30357-7
94. Jepsen, R, Dogisso, TW, and Dysvik, E. A cross-sectional study of self-reported general health, lifestyle factors, and disease: the Hordaland health study. PeerJ. (2014) 2:1–14. doi: 10.7717/peerj.609
95. Van der Berge, M, van Oostrom, SH, van der Molen, HF, Robroek, SJW, Hulshof, CTJ, van der Beek, AJ, et al. Do overweight/obesity and low levels of leisure-time vigorous physical activity moderate the effect of occupational physical activity on self-rated halth of construction workers? Int Arch Occ Environm Health. (2022) 95:465–75. doi: 10.1007/s00420-021-01771-2
96. Holtermann, A, Hansen, JV, Burr, H, Sogaard, K, and Sjogaard, G. The health paradox of occupational and leisure-time physical activity. Br J Sports Med. (2012) 46:291–5. doi: 10.1136/bjsm.2010.079582
97. Hellgren, MI, Kitsche, E, Groot-Zevert, M, Lindblad, U, and Daka, B. Association between body mass index and self-rated health: a Swedish population-based longitudinal study. Scand J Public Health. (2021) 49:369–76. doi: 10.1177/1403494819875012
98. Busutil, R, Espallardo, O, Torres, A, Martínez-Galdeano, L, Zozaya, N, and Hidalgo-Vega, Á. The impact of obesity on health-related quality of life in Spain. Health Qual Life Outcomes. (2017) 15:197–11. doi: 10.1186/s12955-017-0773-y
99. Hulman, A, Ibsen, DB, Laursen, ASD, and Dahm, CC. Body mass index trajectories preceding first report of poor self-rated health: a longitudinal case-control analysis of the English longitudinal study of ageing. PLoS One. (2019) 14:e0212862–11. doi: 10.1371/journal.pone.0212862
100. Adeline, A, and Delattre, E. Some microeconometric evidence on the relationship between health and income. Health Econ Rev. (2017) 7:27. doi: 10.1186/s13561-017-0163-5
101. Cialani, C, and Moprtazavi, R. The effect of objective income and perceived economic resources on self-rated health. Int J Equity Health. (2020) 19:196. doi: 10.1186/s12939-020-01304-2
102. Richardson, T, Elliott, P, and Roberts, R. The relationship between personal unsecured debt and mental and physical health: a systematic review and meta-analysis. Clin Psychol Rev. (2013) 33:1148–62. doi: 10.1016/j.cpr.2013.08.009
103. Martinez, SA, Beebe, LA, Thompson, DM, Wagener, TL, Terrell, DR, and Campbell, JE. A structural equation modeling approach to understanding pathways that connect socioeconomic status and smoking. PLoS One. (2018) 13:1–17. doi: 10.1371/journal.pone.0792451
104. Holte Stea, T, Nordheim, O, Bere, E, Stornes, P, and Eikemo, TA. Fruit and vegetable consumption in Europe according to gender, educational attainment and regional affiliation- a cross-sectional study in 21 European countries. PLoS One. (2020) 15:1–9. doi: 10.1371/journal.pone.0232521
105. Whynes, DKTombola Group . Correspondence between EQ-5D health state classifications and EQ VAS scores. Health Qual Life Outcomes. (2008) 6:94–9. doi: 10.1186/1477-7525-6-94
106. Golicki, D, Niewada, M, Karlińska, A, Buczek, J, Kobayashi, A, Janssen, MF, et al. Comparing responsiveness of the EQ-5D-5L, EQ-5D-3L and EQ VAS in stroke patients. Qual Life Res. (2015) 24:1555–63. doi: 10.1007/s11136-014-0873-7
107. Rosemberg, MAS, and Tsai, JHC. Connecting gender, race, class, and immigration status to disease management at the workplace. J Health Dispar Res Pract. (2014) 7:13–31.
Keywords: self-rated health, hotel housekeepers, social determinants of health, lifestyles, occupational stress, financial strain, work–family conflict
Citation: Chela-Alvarez X, Leiva A, Bulilete O and Llobera J (2024) Socioeconomic determinants and self-rated health among hotel housekeepers in the Balearic Islands (Spain). Front. Public Health. 12:1390582. doi: 10.3389/fpubh.2024.1390582
Edited by:
Diana Grigsby, Brown University, United StatesReviewed by:
Anabela Rodrigues, Catholic University of Portugal, PortugalAntonio Daponte Codina, Andalusian School of Public Health, Spain
Copyright © 2024 Chela-Alvarez, Leiva, Bulilete and Llobera. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Xenia Chela-Alvarez, eGVuaWEuY2hlbGFAc3NpYi5lcw==