 Abena Asefuaba Yalley
Abena Asefuaba Yalley Gabija Jarašiūnaitė-Fedosejeva
Gabija Jarašiūnaitė-Fedosejeva Burcu Kömürcü-Akik
Burcu Kömürcü-Akik Liliana de Abreu
Liliana de Abreu- 1Zukunftskolleg, University of Konstanz, Konstanz, Germany
- 2Department of Politics and Public Administration, University of Konstanz, Konstanz, Germany
- 3Department of Psychology, Vytautas Magnus University, Kaunas, Lithuania
- 4Department of Psychology, Ankara University, Ankara, Türkiye
Background: The mistreatment and abuse of women during childbirth have been recognized as a major global health challenge, impeding facility-based delivery and contributing to the high maternal mortalities globally. The World Health Organization has specifically called for interventions to deal with obstetric violence. This scoping review consolidates the existing literature on interventions aimed at reducing obstetric violence and synthesizes existing knowledge on their impact in promoting respectful maternity care.
Methodology: Thirteen electronic databases were searched for relevant articles from January 2001 to March 2023. A total of 863 records were identified, and 72 full-text articles were retrieved for further screening. The review includes 16 studies, particularly from low- and middle-income countries, with interventions implemented at medical facilities and involving both women and healthcare providers. Eight of the studies were quantitative, three were qualitative and five used a mixed-methods approach.
Findings: The results reveal a promising trend in reducing obstetric violence through various interventions. Ten different types of interventions were identified, highlighting strategies to improve the quality of maternity care and enhance patient-centered care. Improved patient-provider communication skills, increased privacy measures, and reduced abuse and mistreatment emerged as common themes. Enhanced communication skills, including open discussions and the right to be informed, were crucial in reducing obstetric violence. Privacy measures, such as separate rooms, curtains, and birth companions effectively decreased incidents of non-confidential care. General abuse and mistreatment, including physical abuse and neglect, were also reduced, leading to improved perceptions of respectful care during childbirth.
Conclusion: Overall, the interventions had a favorable impact on obstetric violence reduction and women’s childbirth experiences. However, despite promising results, obstetric violence remains prevalent worldwide, necessitating more efforts to implement effective interventions. To the best of our knowledge, this is the first scoping review on obstetric violence interventions, providing a comprehensive overview of the state of the art. We suggest that further research is needed to explore new interventions, particularly gender-sensitive interventions, to contribute to a growing body of knowledge on the prevention of obstetric violence.
Introduction
The Charter on the Universal Rights of Childbearing Women emphasizes the fundamental right to receive dignified and respectful sexual and reproductive healthcare, including during childbirth (1). Thus, mistreatment and violence during childbirth are considered a violation of women’s fundamental human rights. Worldwide, there is clear evidence that demonstrates that a substantial number of women experience poor standards of care and mistreatment during childbirth. These mistreatments, widely conceptualized as obstetric violence, have been recognized as a major global health challenge with devastating impacts on women’s and children’s health. According to Vacaflor (2), obstetric violence refers to ‘the violence exercised by health personnel on the body and reproductive processes of women (during pregnancy or childbirth), as expressed through dehumanizing treatment, medicalization abuse, and the conversion of natural processes of reproduction into pathological ones. Obstetric violence as a concept is relatively new in the global health literature with researchers adopting various terminologies such as ‘disrespect and abuse (D&A),’ ‘mistreatment and abuse,’ ‘dehumanized childbirth,’ and ‘disrespectful maternity care’ to describe violence and abuse in obstetric care. While these terminologies help to clearly categorize the different manifestations of violence, the term ‘obstetric violence’ emphasizes the ‘structural dimensions as a gender-based violence that intersects with institutional violence’ (3, 4). Nonetheless, all the terminologies acknowledge the harmful effects of violence, the dehumanization of childbirth and the violation of women’s rights and dignity. In this study, we use the term ‘obstetric violence’ interchangeably with the other terminologies to cover vast literature. Obstetric violence could manifest in the form of physical violence, denial of birth companion, intimidation, forced medical care, neglect or abandonment, lack of confidentiality, failure to seek consent, unjustified cesarean sections, restrictions on food and mobility, and excessive use of oxytocin to induce labor (3, 5–7). Women are often stripped of the agency to make decisions over their bodies, while some are subjected to dehumanizing treatments. The World Health Organization has recognized it as a torturous phenomenon that is very widespread and called for critical studies that interrogate obstetric violence and interventions to reduce it.
Mistreatment of women during childbirth has been recorded in both high-income (8, 9) and middle-to low-income countries (10–12). Recent studies on obstetric violence reveal a prevalence of 33% in Mexico, 44% in Argentina, 76% in Türkiye, 15% in India, and 17% in the United States (13–17). In Africa, some obstetric violence rates have also been reported: 20% in Kenya, 20–28% in Tanzania, 65.3% in Ghana, 78% in Ethiopia, and 98% in Nigeria (18–22). Similarly, a multi-country study conducted in four Sub-Saharan African countries found that 40% of women experienced obstetric violence during facility birthing (18). Research has also demonstrated that obstetric violence is associated with a higher risk of maternal problems such as obstructed labor and postpartum hemorrhage and even death (23). The psychological consequences of obstetric violence following childbirth include depression and post-traumatic stress disorder (PTSD) (24). The (anticipated) experience of obstetric violence prevents many women from utilizing facility-based services for childbirth (3). Violence during childbirth is the most cited reason for women’s refusal to reuse health facilities in subsequent pregnancies in Latin America (25). As a consequence, this increases women’s risks of preventable complications and maternal mortality. Hence, reducing maternal mortality requires the strengthening of institutional health, particularly of maternity care systems, and addressing barriers that limit access and reduce the quality of obstetric services.
While previous studies have made important contributions to the discourse in this field, the explicit focus on interventions to reduce the prevalence of obstetric violence has not been well articulated in the literature. Particularly, consolidated literature that documents existing interventions for obstetric violence and their effectiveness in reducing the occurrence of violence during obstetric care is scarce. Therefore, the present study reviews the available literature on obstetric violence interventions to examine existing interventions and their effectiveness. We explore the different types of interventions, their underlying theories of change, and their impact on patient knowledge, provider attitudes, communication, and overall quality of care. By examining these interventions, this review aims to provide a comprehensive overview of the strategies used to promote respectful and patient-centered maternity care.
The term ‘intervention’ is used in this study to refer to any actions, programs, or activities that are implemented with the primary aim of improving human health and achieving a better health outcome (26). In the context of obstetric violence, interventions can include programs, activities and actions aimed at reducing violence during childbirth. A review that explores the diverse programs, approaches or interventions builds an evidence base that illuminates the range of interventions used to address this critical global health challenge. This is an important contribution to a growing body of evidence in this field and one that seeks to improve reproductive health and women’s rights within the overall childbearing discourse. This review provides timely input to those seeking to design impactful interventions to address the problem of violence during childbirth to improve the quality of maternity care around the world.
Materials and methods
Inclusion and exclusion
This scoping review examined obstetric violence interventions and synthesized the impact of the interventions in dealing with abuse during childbirth. The study particularly examined a range of interventions implemented to reduce abuse and disrespect during childbirth, enhance patient-provider interactions, and improve the overall quality of obstetric care. We included all primary research (qualitative and quantitative) aimed at evaluating the impact of obstetric violence interventions and only academic peer-reviewed articles published in English. Due to the contemporary nature of the emergence of obstetric violence research, the timeline for the search was from January 2000 to March 2023. For inclusion, the study must have described the interventions that were implemented and utilized empirical data to measure post-intervention outcomes. The interventions must solely focus on dealing with obstetric violence. Studies that described obstetric violence interventions but did not implement the interventions nor evaluate the outcome were excluded. Furthermore, this study excluded publications that were merely based on secondary materials such as literature reviews, commentaries, systematic reviews and descriptions of policies and laws as well as study protocols.
Outcome of interest
The outcome of interest in this scoping review includes a comprehensive understanding of the impact and effectiveness of interventions targeted at reducing obstetric violence. The chosen outcomes align with Bowser and Hills’ (27) framework, which categorizes obstetric violence into distinct forms, allowing for a broader exploration of the interventions. Therefore, the key outcomes included addressing physical abuse, ensuring informed consent for medical procedures, preserving confidentiality, promoting dignified care, eliminating discrimination, and mitigating instances of abandonment or detention during childbirth. Studies included must have measured at least one of these outcomes. These outcomes collectively provide a deeper understanding of the effectiveness of interventions across various dimensions of obstetric violence, contributing valuable insights to the broader discourse on improving maternity care and fostering respectful practices worldwide.
Literature search
The review followed the four principal steps according to The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) framework by Liberati et al. (28). These include identification, screening, eligibility, and inclusion. A systematic search was carried out on the Cumulative Index to Nursing and Allied Health Literature (CINAHL), EBSCOhost, PubMed, Web of Science, African online journals, Cochrane Library, SciVerse, Scopus, Google Scholar, PsychINFO, PsychArticles, Medical Literature Analysis and Retrieval System Online, and Maternity and Infant Care to retrieve relevant literature in November 2022. The search terms broadly combined using Boolean expressions formed the first stage of the searching and screening for this review. The search terms and their combinations (see Table 1) were adapted to the specifics of each electronic database.
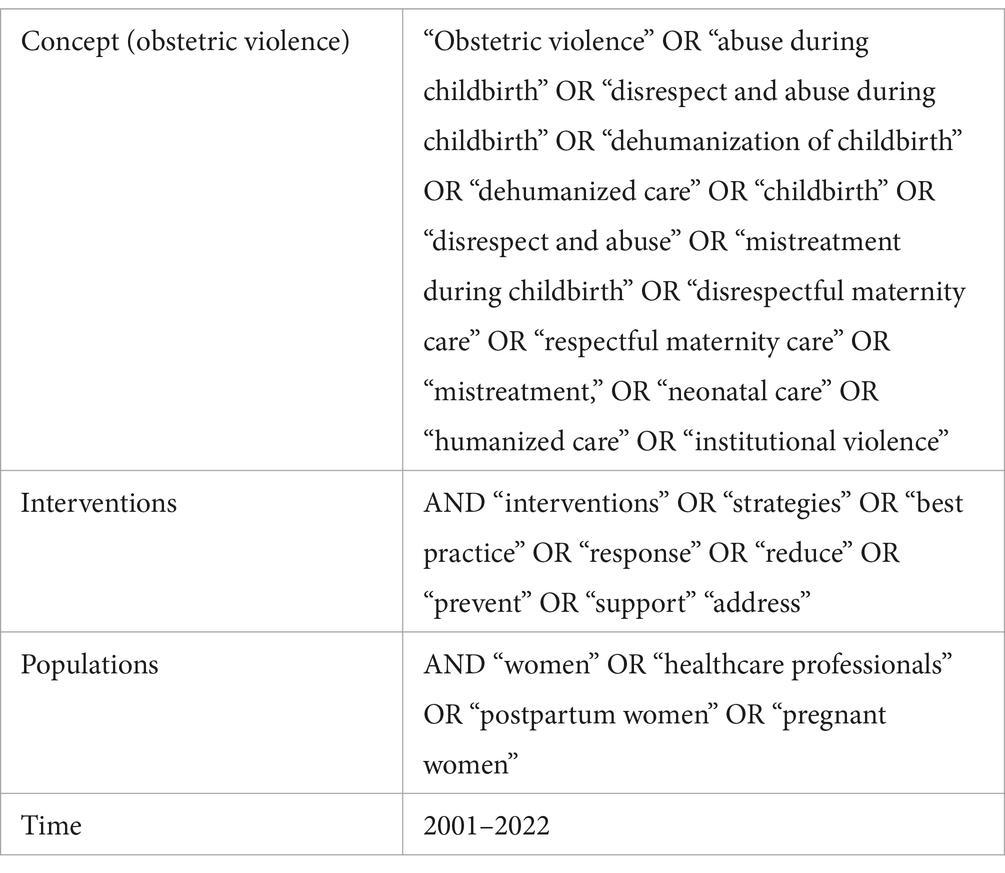
Table 1. Complete list of keywords for search.
Search strategy
The search generated a total of 888 items for screening in the first mapping phase. The results were combined with references suggested by experts and through bibliographic searches, which yielded six additional studies, making a total of 894 studies. A second search was conducted in March 2023 to include studies published from December 2022 to March 2023, but no new study was identified. During the screening, 31 duplicates were identified and deleted. Items identified in the search were then screened for inclusion in the mapping, initially based on title and abstract. The team screened the full text when inclusion or exclusion could not be determined from the title and abstract. The subsequent screening involved two team members (AAY, GJF) who independently screened the 72 items, compared results and resolved any differences in understanding the inclusion/exclusion criteria. The other team members (LA and BKA) were involved when AAY and GJF could not agree on any full-text item. In such cases, decisions were made in favor of an inclusive approach. After a thorough screening of the papers, a total of 16 items were included in the mapping. Figure 1 shows the flow diagram of the searching and screening strategy.
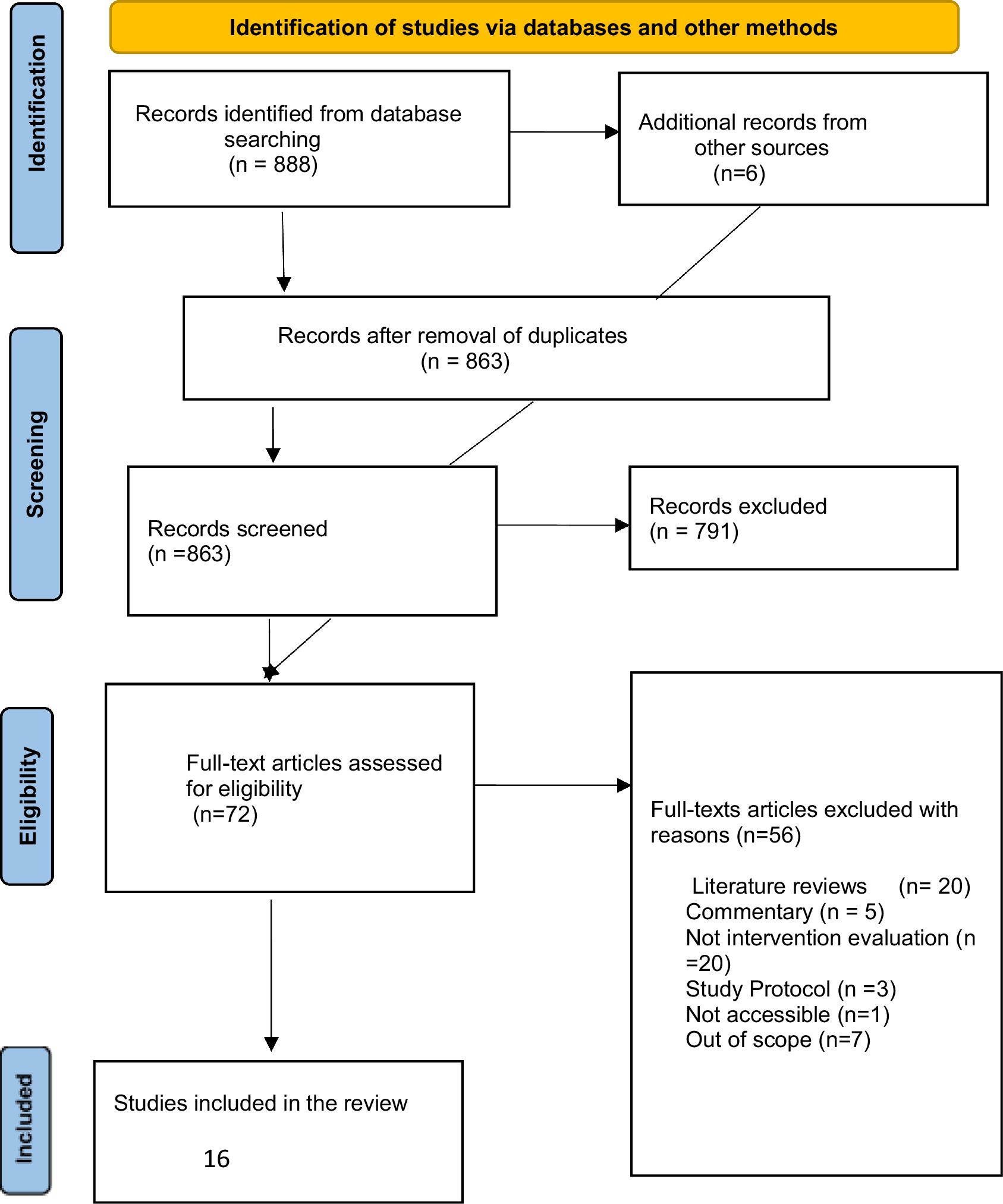
Figure 1. PRISMA flow chart.
Data extraction and analysis procedure
The following data were extracted for each selected study: name of the first author, year publication, country where the study was undertaken, information about the study (article type, design and aims), study population (sample size and targeted population), type of intervention, length of intervention, control group, data collection mode, measurement point, data analysis, outcome measures and a concise description of the findings of the study. Significant evidence relevant to the goal of the review was systematically extracted, appraised, and reported using the PRISMA-ScR checklist (28, 29). The outcomes of the extracted data were synthesized to answer the research question.
Results
General characteristics of the studies
Study design
Overall, 16 articles were included in the study, with the earliest study published in 2001 while the most recent studies were published in 2021. Thirteen of the reviewed studies employed a comparative before-and-after intervention evaluation approach (19, 30–41). Eight studies used quantitative data (19, 30, 31, 35–38, 40), five studies used a mixed-methods approach (32–34, 39, 41) and three studies collected qualitative data (42–44). The 16 studies were geographically diverse, conducted in 9 countries: Tanzania (n = 2), Kenya (n = 1), Ethiopia (n = 3), Ghana (n = 3), Sri Lanka (n = 2), Brazil (n = 2), South Africa (n = 1), Sudan (n = 1), and Sweden (n = 1). The publication timeline spanned two decades, from 2001 (39) to 2021 (31, 43). A detailed list of the studies and extracted data is presented in Table 2.

Table 2. Characteristics of included articles (n = 16).
Participants and sample
All the included studies involved an intervention at a medical facility, comprising a total of 16 studies. The sampling process encompassed both women and/or medical staff. Specifically, women who had given birth were recruited after their discharge (30). Women between the ages of 15 and 45 who had delivered within 24–48 h at a participating facility were included (19). Women who had recently given birth at any of the 10 midwife-led obstetric units (MOUs) and subsequently visited primary healthcare facilities for a postnatal follow-up appointment within 3 days to 6 weeks post-delivery were included (35). One study selected a sample from 30 births that had been monitored using the Federal Ministry of Health of Ethiopia (FMoH) adopted Safe Childbirth Checklist (SCC) in the previous month (31). The majority of the studies focused on healthcare providers (19, 30–44). The length of intervention varied from half a day (37, 42) to around 3 years (39). One study measured the long-term impacts for 10–11 months following training with total data collected over a period of 27 months (31), while another study conducted workshops on abuse for healthcare staff (AHC) for 13 months (40). Additionally, one study assessed outcomes 10 months after the intervention (30).
Qualitative data in mixed methods and qualitative studies was derived from various empirical tools. These included direct observation of interactions between clients and providers (33), interviews with women after discharge to identify potential mechanisms of change (32), interviews conducted with women 3–6 h after delivery in one study [baseline N = 2000, (33)], community follow-up interviews with women conducted 4–6 weeks after delivery [baseline N = 70, (33)], structured focus group discussions (FGDs) with midwifery, gynecologists (32), FGDs with health professionals who were participants in RMC training (34, 42); in-depth interviews with participants of the RMC training (43), FGDs with health professionals with experiences supporting and listening to pregnant women during community engagement activities (31).
Factors influencing obstetric violence
The factors influencing obstetric violence can be categorized into technical and interpersonal aspects. Most acts of disrespect and abuse occurred within the interactions between healthcare providers and women. Interpersonal violence and abuse were found to be associated with several key issues addressed in the interventions. Firstly, non-confidential care was a prominent concern addressed in 11 studies (19, 30–34, 36, 39, 42–44). Secondly, the issue of non-dignified care was highlighted in seven interventions (19, 30, 32, 33, 36, 41, 43). Thirdly, non-consented care was addressed in seven studies (19, 30, 32–35, 44). Additionally, questions relating to feelings of neglect, humiliation, and disrespect (19, 32, 34, 35), verbal abuse (19, 34, 35, 41), detention (19, 32), abandonment (19, 32, 34), denial of the right to free care or denial of care (32, 44), and physical abuse (19, 30, 32, 34) were also examined in multiple studies. Table 3 shows the synthesis of the results.
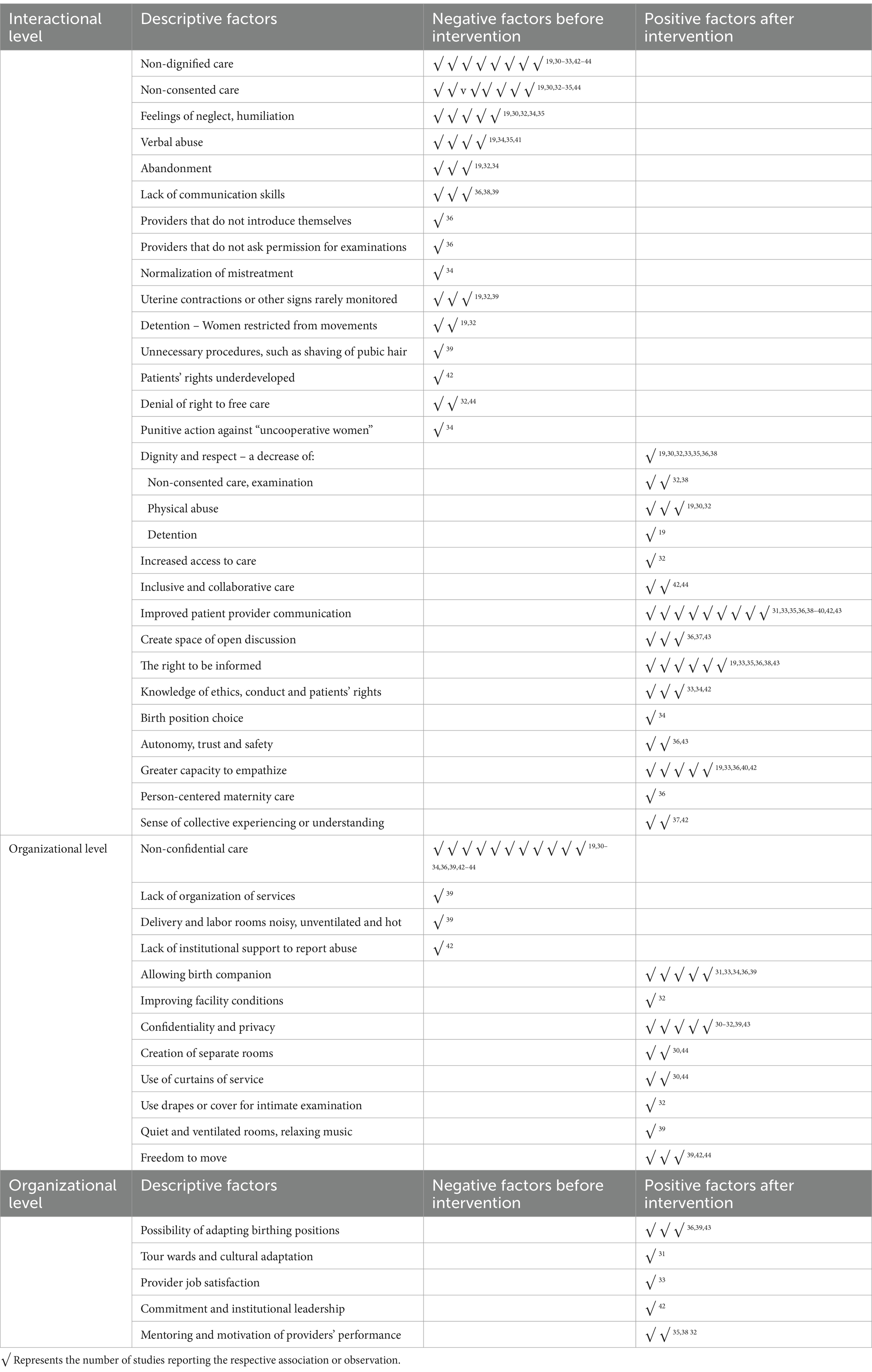
Table 3. Synthesis of the factors whose association with OV was observed in the interventions.
Obstetric violence interventions
In the 16 studies, a total of 10 different types of interventions were identified, ranging from collaborative building curriculum to childbirth checklists. The interventions included a variety of approaches, such as the implementation of client service charters, employing training programs for healthcare providers, using simulation-based team training, changing laboratory methodology, promoting humanization of childbirth initiatives, conducting forum play workshops, and providing communication skills training. Due to the diversity of studies, some research presents outcomes derived from several different approaches.
Respectful Maternity Care (RMC)
Four studies utilized an approach based on Respectful Maternity Care (RMC), combined with patient-centered care, client-provider interaction, and family participation, to address abuse and disrespect (32–34, 43). This approach recognizes that providing compassionate and respectful maternity care during pregnancy is crucial for improving the quality of maternal health services and reducing maternal mortality and morbidity. The World Health Organization (45) defines RMC as “the care organized for and provided to all women in a manner that maintains their dignity, privacy, and confidentiality, ensures freedom from harm and mistreatment, and enables informed choice and continuous support during labor and childbirth.”
The safe childbirth checklist
The Safe Childbirth Checklist collected data on privacy and the availability of a birth companion during labor and childbirth over a 27-month period from 17 health centers and three hospitals (31). This intervention was based on the Ethiopian government’s decision to motivate health professionals to adopt a Compassionate, Respectful, and Caring (CRC) approach. The goal was to institutionalize RMC by integrating, training, and empowering health professionals through life-testimonial video-based training that included participatory discussions, reflections, and local solutions to enhance RMC. Successful ideas for improving women’s care experiences were shared during staff meetings. This intervention involved the collaboration of all facilities at the district level from 12 to 15 months.
The PRONTO training kit
Afulani et al. (36, 41) implemented a collaborative approach using the PRONTO training kit. This low-tech, highly realistic simulation and team training, accompanied by facilitated debriefing, aimed to improve the identification and management of obstetric and neonatal emergencies, as well as team functioning. The PRONTO training kit included a hybrid birth simulator called the PartoPantsTM, which consisted of modified surgical scrubs with anatomical landmarks necessary for delivery. The intervention focused on enhancing the quality of care by emphasizing clinical knowledge and skills, teamwork and communication, and RMC. While RMC was emphasized throughout the PRONTO training, there were no explicit modules solely dedicated to RMC. The curriculum included simulation scenarios, debriefing guides, knowledge reviews, and interactive teamwork and communication activities.
Mother baby-friendly hospital initiative (MBFBF) 10 criteria – the change laboratory methodology
The interventions focused on implementing change: the Change Laboratory (CL) methodology (44). The research initially started in late 2016, and the CL principles were adopted 9 months later, following adjustments to better incorporate the conceptual framework. The CL methodology aimed to address 10 key challenges related to unfriendly childbirth care in hospitals. These challenges include issues such as freedom of movement, eating and drinking during labor and birth, respect for privacy, right to companionship, use of evidence-based care and prevention of inappropriate interventions, freedom from discrimination, freedom from physical and emotional abuse, access to appropriate pain relief, affordability or free care, cultural sensitivity, and ensuring appropriate care for the newborn, including facilitating skin-to-skin mother-baby contact.
The Staha project theory of change and open birth days
The Staha Project Theory of Change (30, 33), was developed through an iterative participatory process involving local community and health systems stakeholders. It consisted of two main components. Firstly, a client service charter was created to establish consensus on norms and standards that promote mutual respect and respectful care. The charter was adapted by the two groups and then revised based on feedback from another group of 70 stakeholders (86% provided feedback). Subsequently, the charter was disseminated to communities and displayed in health facilities within the intervention district. Secondly, a maternity quality improvement process was implemented to activate the content of the charter. Planned interventions included the implementation of the Health Workers for Change curriculum by Ratcliff et al. (33) and the Open Birth Days (OBD) intervention. These interventions aimed to increase patient knowledge about their rights, and birth preparedness, improve patient-provider and provider-administrator communication, and enhance women’s experiences and provider attitudes.
The Heshima’s project
Launched in 2011 in Kenya, the Heshima project included complementary interventions at community-level, facility-level, and policy-level (19). This project also performed quantitative and qualitative assessments to test associations between the implementation of D&A activities and trends in quality of care at intervention facilities. This project included an iterative three-tiered set of interventions of a process of learning-by-doing throughout its design, development and assessment, with the objective of identifying low-cost and feasible policy, facility and community interventions. Facility interventions, which began in six facilities for 20 months, were replicated and refined in seven facilities beginning in November 2012 and continued for 14 months. At the facility level, intervention activities included: training in promoting RMC, quality improvement teams, caring for carers, D&A monitoring, mentorship, and maternity open days. At the community level, interventions included workshops in the community, mediation/dispute resolution and counseling community members.
The CLEVER maternity care and humanization of childbirth
CLEVER Maternity Care stands for Clinical Care and obstetric triage and is about eliminating barriers to care, verifying and monitoring, reflexive and respectful care, and emergency obstetric simulation training (EOST). Oosthuizen and colleagues measured perinatal morbidity and mortality as proxies for quality obstetric care (35). The intervention was implemented in three phases: creating awareness, implementing core activities for behavioral change, and conducting follow-up on the baseline survey.
Humanization of Childbirth involves integrating the Japanese midwifery concept of a “safe and satisfied birthing experience.” This approach aims to empower women, promote active participation and decision making and ensure equality. It utilizes a decentralized system of birth and seeks to be evidence-based as well as financially feasible. A self-controlled experimental study before-and-after design was used to compare the delivery and childbirth situation in five municipalities in a Brazilian state (39). Data was collected at two time points: 1997 and 2000. The participatory intervention firstly consisted of several training activities, including seminars, workshops, in-service training, and training for trainers, and secondly by grouting the learning on participants’ conscious taking.
Forum play workshops
These trainings are based on the pedagogical work of Brazilian stage director, Augusto Boal (Theater of the Oppressed and Forum Theatre) and Paulo Freire, as well as on problem-posing dialogue and empowerment. These methods have been used over several decades on curricula and training development to promote participation, personal and collective reflection and transformative actions in oppressive or ethically complex contexts. The intervention consisted of providing workshops and training to strengthen participants’ abilities to recognize abuse in healthcare and to improve readiness to act in D&A situations (37, 40, 42).
Training on communication skills
This is a quasi-experimental study to improve patient providers’ communication in the labor ward at Omdurman Maternity Hospital, Sudan (38). A situation analysis prior to training, evaluating the existing communication skills of providers and patients’ satisfaction was carried out. A 10% sample of hospital deliveries and all healthcare providers (HCPs) were included in the study before and after the training. The study examined socio-demographic characteristics and evaluated the information given to patients upon admission to the labor ward, as well as the process for obtaining permission and consent for procedures, post-natal follow-up, and patients’ satisfaction before and after training.
Assessment of interventions: main outcomes
From our findings, the greater number of interventions reviewed demonstrated positive outcomes in reducing obstetric violence with only a few exceptions recording no changes post intervention. In the following section, we describe the outcomes of the various studies reviewed in this study.
Enhanced patient-centered communication skills
These interventions focused on improving communication between healthcare providers and women during childbirth. This included creating space for open discussions, encouraging questions, improving patient-provider communication, and guaranteeing women’s right to be informed. Some interventions even included activities such as organizing tours of the birthing ward and allowing cultural celebrations (31). These interventions resulted in increased empowerment, trust, empathy, emotional support, and a more inclusive and collaborative care environment, subsequently leading to an overall reduction in obstetric violence. The enhancement of patient-centered communication skills emerged as a key factor in achieving this reduction. Two specific communication skills were found to have a strong influence. Firstly, creating space for open discussion and encouraging questions empowered women throughout the entire process of childbirth. Several interventions underscored the significance of encouraging communication, recognizing its pivotal role in the childbirth process (31, 35, 36, 39, 42, 43). Secondly, improving patient-provider communication and the right to be informed was identified as crucial in reducing obstetric violence (19, 33, 35, 36, 38, 43). Furthermore, Ratcliffe and colleagues (33) noted a significant improvement in provider knowledge following RMC training. Specifically, there was a 5.4% increase in understanding their code of conduct, ethics, and patient rights. Additionally, a 6.8% increase was observed in their awareness that disrespect and abuse represent a global problem. Creating a trusting and safe environment, providing more empathy and emotional support, and promoting inclusivity, collaboration, and freedom of movement (such as allowing drinking or eating) were also noted as positive factors in reducing obstetric violence (19, 36, 42, 44). Specifically, Afulani et al. (36) observed an 87% increase in communication and autonomy. Indeed, they observed higher changes in the domain of communication and autonomy, with the score nearly doubling. Additionally, Mengistu et al. (31) observed that testimonial videos proved helpful for providers to understand their care from the perspective of their patients. At the same time, quality improvement training and coaching facilitated reflection on potential underlying causes of mistreatment and the development of effective solutions.
Increased birth companion and privacy
Interventions aimed at increasing confidentiality and privacy in childbirth settings implemented various strategies. These included organizational changes such as creating private or separate rooms for admissions, antenatal care, family planning, and postnatal care, which were previously provided in a single room (30, 31). Additionally, the use of curtains for delivery, examinations, and between beds was employed to enhance privacy (30, 44). A study by Miret et al. (32) assessed non-confidential care and reported a 54.8% reduction in events of non-confidentiality after the intervention, attributing it to the use of drapes or covering intimate parts and ensuring private health information was not discussed in a way that others could hear. Another intervention introduced changes where mothers no longer had to share rooms, allowing for greater privacy, especially when empty rooms were available (44). Some interventions also explored the possibility of having a birth companion in the delivery room, even when multiple women were delivering simultaneously. The findings indicated a positive shift, with a higher percentage of women having a birth companion at the endline compared to the baseline. Specifically, Afulani et al. (36) observed a noteworthy decrease in the proportion of women who reported never being allowed to have a companion during labor, declining from 32% at baseline to 10% at the endline. In the context of open labor wards, the introduction of the option to change birthing positions for enhanced privacy was implemented, as highlighted in the study by Dzomeku et al. (43). The findings suggest that a dedicated refresher training course focusing on provider attitudes, knowledge, and best practices holds the potential for a positive impact on the maternity care environment. Additionally, Ratcliffe et al.’s study (33) observed a significant improvement in patient knowledge following pre and post-tests administered during Open Birth Days sessions. The results demonstrated a noteworthy increase in awareness of various rights during labor and delivery, including the right to consent (rising from 30.1 to 57.8%), the right to be free from physical abuse (increasing from 79.5 to 86.9%), and the right to privacy (climbing from 68.2 to 81.9%) (33).
Several interventions focused on person-centered maternity care and observed positive changes. A study (36) reported significant improvements in person-centered maternity care features after the intervention, including increased introduction of providers, calling patients by their names, explaining the purpose of examinations, procedures, and medications, and obtaining permission. Overall, the average score for person-centered maternity care increased from approximately 43–72%, indicating a relative increase in dignity and respect, communication and autonomy, and supportive care (36). In the study conducted by Swanhnberg (37), participants reported increased involvement in cases of abuse and a higher rate of acting in support of patients after a workshop intervention. The intervention facilitated open discussion, increased awareness of abuse in healthcare, and addressed factors such as stress and lack of knowledge on how to respond to mistreatment. The workshop format, which included the physical use of bodies for learning and facilitated expression of emotions, was highly effective, according to participant feedback. Another study by Zbikowski et al. (40) found that participation in an educational workshop program improved self-reported ability to act according to moral beliefs in risk situations of abuse and enhanced empathy and communication skills among healthcare professionals.
The oldest study included in the report, conducted in 2001 by Misago et al. (39), highlighted several inadequate practices during childbirth, such as noisy and unventilated delivery rooms lacking privacy, restrictions on movement, unnecessary procedures, and unattended women delivering in labor rooms. However, positive changes were observed in hospitals that received “humanization of childbirth” training, including increased numbers of deliveries, frequent use of birth companions, and encouragement of women to bring a family member or significant other. Indeed, Misago and colleagues noted a significant change over time. In 1997, women in labor were frequently unattended, whereas by 2001, there was a noticeable shift, with women consistently accompanied by someone during labor. Only one out of 12 direct delivery observations identified an unaccompanied woman, highlighting a marked improvement in the presence of support during the childbirth process.
Umbeli et al. (38) reported that training in communication skills led to increased support and respect from providers according to patient perceptions. Providers also reported improved knowledge of various aspects of care after the training, informing women about the birth process more often. For example, improvements were seen in informing women on such aspects as fetal condition (from 65.8 to 96.2%), expected duration of birth (from 22.5 to 81.9%), and examinations/procedures (from 20.0 to 81.0%). In the study conducted by Mengistu et al. (31), significant improvements were observed in the percentage of births that received two important elements of respectful maternal care: privacy and birth companionship. Specifically, one district showed a notable increase, with short and long-term regression coefficients of 18 and 27%, respectively, indicating a positive trend over time. However, the results were mixed in the other two districts included in the study, suggesting that the interventions may have had varying effects in different settings.
Decrease of situations of disrespect and abuse
The interventions led to a decrease in the overall prevalence of disrespect and abuse, particularly neglect and physical abuse. Furthermore, the interventions significantly improved the perception of respectful care, with participants reporting excellent or very good ratings for the respect shown by providers and the overall quality of care for delivery.
In the study conducted by Kujawski et al. (30), the intervention showed a significant decrease in the percentage of women who experienced abuse and disrespect during childbirth. The results indicated a 3.39% decrease (p < 0.0001) in the overall prevalence of abuse and disrespect. When adjusting for covariates, the intervention was associated with 66% reduced odds (95% CI: 0.21–0.58, p < 0.0001) of women experiencing disrespect and abuse. Furthermore, women in the intervention facility were significantly less likely to report instances of neglect (OR: 0.36, 95% CI: 0.19–0.71, p = 0.045) and physical abuse (OR: 0.22, 95% CI: 0.05–0.97, p = 0.003) when compared to the control facility, after adjusting for all variables in the conceptual model (30). Additionally, the intervention was associated with an increased likelihood of pregnant women rating the respect shown by providers during their facility stay for delivery as excellent or very good (RR: 3.44, 95% CI: 2.45–4.84, p < 0.0001), as well as rating the overall quality of care for delivery as excellent or very good (RR: 6.19, 95% CI: 4.29–8.94, p < 0.0001).
Afulani et al. (36) observed similar trends with an increase in dignity and respect (15%), and a 55% increase in supportive care after RMC training. Additionally, as reported by Ratcliff et al. (33), reporting situations of D&A increased after intervention, going from no participants reporting these situations at baseline to 10% of women who attended the OBD (Open Birth Days) reporting feeling disrespected during labor and formally filed a complaint. A study (32) revealed that D&A decreased from 71.8% at baseline to 15% at endline with a change of 55% (mean difference: 0.56, 95% CI: 0.55–0.57). Similarly, Abuya and colleagues (19) observed that D&A decreased from 20 to 13% (p < 0.0004) and among four of the six typologies of D&A it was observed a decrease of 40–50% and an overall D&A decrease of 7% reported by postnatal women after their discharge from maternity units. Nonetheless, the frequency of typologies varied considerably in both the interviews and observations. Rates of verbal abuse, for instance, were several times higher than rates of physical abuse, in both interviews and observations. Therefore, some D&A typologies declined more than others, with the greatest decline in detention and physical abuse.
Indeed, certain studies only showed modest improvements in dimensions related to D&A. Asefa et al. (34) observed a marginal decrease in the belief that it is sometimes necessary for providers to yell at a woman during labor from 21.9% pre-test to 20.3% post-test, p = 1.00. Also, Afulani et al. (36) also observed the smallest changes in dignity and respect, but that might be explained by the relatively high scores at baseline. Zbikowski et al. (40) found that participation in an educational workshop program improved the self-reported ability to recognize abuse and act in situations of abuse by healthcare professionals. However, no change was observed in the number of reported occasions of abuse in healthcare between baseline and 1 year after the intervention (40). These findings suggest a notable enhancement in the perception of respectful care and the overall quality of care among women at the intervention facility when compared to the comparison facility with only one exception (40).
Discussion
This scoping review comprehensively synthesized existing literature on interventions aimed at reducing obstetric violence and assessed their effectiveness in promoting respectful maternity care during childbirth. In general, research on obstetric violence interventions is relatively new. Although obstetric violence is a global phenomenon with high prevalence cutting across cultures (14–22), the majority of the studies focusing on interventions were conducted in low- and middle-income countries (LMICs), particularly African Countries. While this expressly reveals Africa’s contribution to knowledge production on obstetric violence, it also points to the rigorous efforts being made to address the high maternal mortality rate on the continent. Sub-Saharan Africa currently accounts for two-thirds of the global Maternal Mortality Ratio (MMR) due to the low utilization of Skilled Birth Attendants (SBA) and poor obstetric care, making research on obstetric violence interventions germane (46, 47). In this review, most of the studies involved interventions at a health facility and the sample groups included both women and medical staff, with the majority focusing on healthcare providers. and were published over a range of 20 years, between 2001 and 2021.
Overall, the interventions demonstrated positive outcomes in reducing obstetric violence and enhancing the childbirth experience for women, particularly with integrated provider training contributing to improved childbirth experiences in resource-limited settings. Based on the results of this scoping review, factors influencing obstetric violence are mostly technical and interpersonal aspects. Non-confidential care, non-dignified care, non-consented care, feelings of neglect and disrespect, verbal abuse, detention, abandonment, and denial of the right to free care are the main issues addressed in various intervention programs.
Effective communication emerged as a crucial factor, highlighting the significance of open discussions, the right to be informed, and the promotion of women’s independence during childbirth. This emphasis on communication underscores the critical role of healthcare professionals’ ability to communicate with women both during and after childbirth, as highlighted in previous studies (48, 49). The identified lack of interpersonal communication skills and attitudes is recognized as a significant weakness in obstetric training (50). Established guidelines for enhancing the quality of obstetric healthcare in countries such as Canada, position communication as a central resource (51). Additionally, within the healthcare context, the element of self-presentation to patients is acknowledged as a key communication aspect for establishing a supportive relationship (52). Furthermore, previous research on obstetric violence has revealed that healthcare professionals often hold misconceptions about this issue. A study (3) conducted in Ghana found that a significant number of healthcare professionals do not perceive acts of mistreatment as abusive. Instead, they view such actions as a form of assistance or ‘help’ beneficial to the newborn, justifying their behavior. Similarly, in India, wrong perspectives on obstetric violence were identified as a major driver of these abuses within healthcare facilities (53). Hence, there is a crucial need for studies to specifically target the healthcare team, addressing and rectifying these misconceptions. Regarding the characteristics of the interventions in our scoping review, we identified a total of 10 different types of interventions across the 16 studies. These interventions assessed several strategies and approaches aimed at promoting respectful and patient-centered maternity care. When compared to pre-intervention, there was a significant improvement in patients’ understanding of the labor process in post-intervention. Higher levels of empathy for women and improved interpersonal relationships were reported by the providers. For example, in the study by Ratcliffe et al. (33), 98.2% of participants said that participation in the intervention improved the communication between patients and providers, and there was a 10.8% increase in providers who agreed that they were able to empathize with their patients. Enhancements in communication were observed and confirmed through direct assessments, as noted by both patients and staff. During childbirth, women reported feeling more in control and assured. Along with evaluations of improved happiness and perceived care quality, provider job satisfaction significantly rose relative to the baseline.
Unfortunately, studies are showing that obstetric violence is still widespread. For example, a study (54) revealed that, regardless of the quality of a healthcare system or a country’s economic well-being, almost two-thirds of the countries across the Eastern Mediterranean Region exhibited six out of seven types of disrespect and abuse during childbirth. Women faced various forms of mistreatment during labor, with physical abuse (particularly the excessive use of routine interventions) and non-dignified care (embedded in patriarchal socio-cultural norms) being most prevalent. In addition, numerous studies emphasize the alarming global spread of abusive and disrespectful practices toward women during childbirth (22, 55). Nevertheless, our scoping review’s findings offer a promising perspective, suggesting that interventions aiming at reducing obstetric violence show success and provide hope for the delivery of respectful care.
When considering the main outcomes of the interventions examined in our study, distinct themes emerge, highlighting the pivotal role of improved patient-centered communication skills and increased use of birth companionship and privacy, all of which contributed to a reduction in situations of abuse and disrespect. Primarily, the interventions underscored the significant refining of patient-centered communication skills as a critical factor in reducing obstetric violence. The establishment of a conducive space for open discussion, combined with the encouragement of questions and the right to be informed, emerged as the first two crucial skills in this context. These skills not only fostered women’s autonomy during childbirth but also significantly enhanced communication between patients and providers. Recognizing the importance of good communication between patients and healthcare providers during childbirth aligns with existing literature emphasizing its critical role in childbirth experiences (46, 47). Furthermore, our study’s findings regarding the positive impact of birth companions are consistent with (56) research in Palestine, revealing a 75% reduction in obstetric violence likelihood among women with birth companions. Additional helpful elements in reducing obstetric violence were building trust and a safe environment, offering more empathy and emotional support, and encouraging inclusivity, collaboration, and freedom of movement (such as allowing drinking or eating).
Again, interventions targeted at ensuring privacy demonstrated notable success in diminishing situations of non-confidential care. These measures include the establishment of separate rooms for admissions, antenatal care, family planning, and postnatal care, using curtains for delivery, vaginal examinations, and between beds, and allowing for changes in birthing positions. Studies demonstrate that obstetric violence often involves privacy breaches (7), categorized as common practices such as gross violations of privacy (26), health system incompetence, and lack of physical privacy in health centers for health examinations (24, 57, 58). Castro and Savage (59) also classify the general lack of privacy, the placement of multiple patients in a single hospital bed, insufficient resources for comfort, and the restriction of visitors or family members as typologies of obstetric violence. Considering these perspectives, our scoping review underscores the pivotal role of privacy maintenance as a key outcome of effective interventions. Consequently, our findings highlight the significance of structural investments and raising awareness among healthcare staff about ensuring privacy as primary factors in interventions aimed at reducing obstetric violence. Also, the interventions resulted in a reduction in the overall prevalence of abuse and disrespect, including both physical abuse and neglect. Participants consistently provided high ratings regarding the improvement of respectful care after interventions (30).
Overall, the interventions had a favorable impact on obstetric violence reduction and women’s childbirth experiences. To guarantee respectful and dignified care during childbirth, the results underlined the significance of patient-centered communication, improved privacy, and birth accompaniment, and addressing abuse and disrespect.
Conclusion
In conclusion, our scoping review examined the multifaceted landscape of obstetric violence interventions, presenting a comprehensive analysis of the available literature. The study identifies key outcomes across 10 interventions, shedding light on their impact on reducing disrespect and abuse during childbirth. Notably, interventions focusing on enhanced patient-centered communication skills, including open discussions and the right to be informed, increased privacy measures, and the involvement of birth companions emerged as pivotal factors in diminishing obstetric violence. Additionally, ensuring privacy through structural investments, such as separate rooms and curtains, significantly decreased instances of non-confidential care. The inclusion of birth companions not only resonated positively with women’s experiences but also demonstrated a substantial reduction in the likelihood of obstetric violence. Overall, the interventions showed positive outcomes. In essence, as obstetric violence continues to be a global health challenge, our study advocates for the continued exploration and implementation of effective interventions to ensure the well-being and rights of childbearing women worldwide.
Strengths and limitations
This is the first scoping review conducted on obstetric violence interventions in healthcare, providing a comprehensive overview of the intervention studies aimed at obstetric violence reduction. Obstetric violence poses a major threat to women’s reproductive wellbeing, contributing to the global high maternal mortality rate, and our study reveals the potential of interventions to deal with this great challenge. However, the studies included in this review were quite heterogeneous, making it difficult to compare, leading to the decision to undertake a scoping rather than a systematic review. Again, most of the included research focused on specific geographic regions, such as Africa and only studies published in English were included which restricts the generalizability of our findings. More often, health providers (rather than the mothers) were the ones who evaluated changes, gave their opinions, and in some cases, interviewed women about the changes, which could lead to research bias. Furthermore, only two studies included in the review had control groups (30, 35). We recommend that future studies on interventions should evaluate interventions more from women’s experiences, implement controlled-experimental trials with comparison groups, address possible social desirability effects and employ randomization in the sampling. Considering the fact that obstetric violence stems from structural and gender inequality, there is also a critical need for gender-based interventions that address gender stereotyping concerning motherhood, birthing and structural inequalities in health systems.
Author contributions
AY: Conceptualization, Data curation, Funding acquisition, Methodology, Validation, Writing – original draft, Writing – review & editing. GJ-F: Data curation, Methodology, Validation, Writing – original draft, Writing – review & editing. BK-A: Data curation, Writing – original draft, Writing – review & editing. LA: Formal analysis, Funding acquisition, Validation, Visualization, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. The authors received funding from the University of Konstanz Open Access Funding.
Acknowledgments
The authors would like to thank Selasie Ahiatrogah for assisting with references and Dorothea von Kalnein for her support with the proofreading of the manuscript.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. White Ribbon Alliance. Respectful maternity care: the universal rights of childbearing women. (2011). Available at: https://whiteribbonalliance.org/wp-content/uploads/2022/05/WRA_RMC_Charter_FINAL.pdf (Accessed January 20, 2024).
2. Vacaflor, CH. Obstetric violence: a new framework for identifying challenges to maternal healthcare in Argentina. Reprod Health Matters. (2016) 24:65–73. doi: 10.1016/j.rhm.2016.05.001
3. Yalley, AA. “We beat them to help them push”: midwives’ perceptions on obstetric violence in the Ashante and Western regions of Ghana. Women. (2023) 3:22–40. doi: 10.3390/women3010002
4. Savage, V, and Castro, A. Measuring mistreatment of women during childbirth: a review of terminology and methodological approaches. Reprod Health. (2017) 14:138. doi: 10.1186/s12978-017-0403-5
5. Bellón, Sánchez S. Obstetric violence from the contributions of feminist criticism and biopolitics. (2015). Available at: https://www.dilemata.net/revista/index.php/dilemata/article/view/374/379 (Accessed January 20, 2024).
6. Fernández Guillén, F. What is obstetric violence? Some social, ethical and legal aspects. Dilemata. (2015) 18:113–28.
7. World Health Organization (2014). The prevention and elimination of disrespect and abuse during facility-based childbirth: WHO statement. Available at: https://iris.who.int/bitstream/handle/10665/134588/W?sequence=1 (Accessed January 25, 2024).
8. Schroll, AM, Kjærgaard, H, and Midtgaard, J. Encountering abuse in health care; lifetime experiences in postnatal women - a qualitative study. BMC Pregnancy Childbirth. (2013) 13:74. doi: 10.1186/1471-2393-13-74
9. Swahnberg, K, Thapar-Björkert, S, and Berterö, C. Nullified: women's perceptions of being abused in health care. J Psychosom Obstet Gynaecol. (2007) 28:161–7. doi: 10.1080/01674820601143211
10. D'Ambruoso, L, Abbey, M, and Hussein, J. Please understand when I cry out in pain: women's accounts of maternity services during labour and delivery in Ghana. BMC Public Health. (2005) 5:140. doi: 10.1186/1471-2458-5-140
11. Dixon, E, Hameed, M, Sutherland, F, Cook, DJ, and Doig, C. Evaluating meta-analyses in the general surgical literature: a critical appraisal. Ann Surg. (2005) 241:450–9. doi: 10.1097/01.sla.0000154258.30305.df
12. Chadwick, RJ, Cooper, D, and Harries, J. Narratives of distress about birth in south African public maternity settings: a qualitative study. Midwifery. (2014) 30:862–8. doi: 10.1016/j.midw.2013.12.014
13. Raj, A, Dey, A, Boyce, S, Seth, A, Bora, S, Chandurkar, D, et al. Associations between mistreatment by a provider during childbirth and maternal health complications in Uttar Pradesh, India. Matern Child Health J. (2017) 21:1821–33. doi: 10.1007/s10995-017-2298-8
14. Correa, M, Klein, K, Vasquez, P, Williams, CR, Gibbons, L, Cormick, G, et al. Observations and reports of incidents of how birthing persons are treated during childbirth in two public facilities in Argentina. Int J Gynaecol Obstet. (2022) 158:35–43. doi: 10.1002/ijgo.13938
15. Castro, R, and Frías, SM. Obstetric violence in Mexico: results from a 2016 National Household Survey. Violence Against Women. (2020) 26:555–72. doi: 10.1177/1077801219836732
16. Goli, S, Ganguly, D, Chakravorty, S, Siddiqui, MZ, Ram, H, Rammohan, A, et al. Labour room violence in Uttar Pradesh, India: evidence from longitudinal study of pregnancy and childbirth. BMJ Open. (2019) 9:e028688. doi: 10.1136/bmjopen-2018-028688
17. Aşci, Ö, and Bal, MD. The prevalence of obstetric violence experienced by women during childbirth care and its associated factors in Türkiye: a cross-sectional study. Midwifery. (2023) 124:103766. doi: 10.1016/j.midw.2023.103766
18. Asefa, A, and Bekele, D. Status of respectful and non-abusive care during facility-based childbirth in a hospital and health centers in Addis Ababa, Ethiopia. Reprod Health. (2015) 12:33. doi: 10.1186/s12978-015-0024-9
19. Abuya, T, Ndwiga, C, Ritter, J, Kanya, L, Bellows, B, Binkin, N, et al. The effect of a multi-component intervention on disrespect and abuse during childbirth in Kenya. BMC Pregnancy Childbirth. (2015) 15:224. doi: 10.1186/s12884-015-0645-6
20. Okafor, II, Ugwu, EO, and Obi, SN. Disrespect and abuse during facility-based childbirth in a low-income country. Int J Gynaecol Obstet. (2015) 128:110–3. doi: 10.1016/j.ijgo.2014.08.015
21. Kruk, ME, Kujawski, S, Mbaruku, G, Ramsey, K, Moyo, W, and Freedman, LP. Disrespectful and abusive treatment during facility delivery in Tanzania: a facility and community survey. Health Policy Plan. (2018) 33:e26–33. doi: 10.1093/heapol/czu079
22. Yalley, AA, Abioye, D, Appiah, SCY, and Hoeffler, A. Abuse and humiliation in the delivery room: prevalence and associated factors of obstetric violence in Ghana. Front Public Health. (2023) 11:988961. doi: 10.3389/fpubh.2023.988961
23. Lokugamage, AU, and Pathberiya, SDC. Human rights in childbirth, narratives and restorative justice: a review. Reprod Health. (2017) 14:17. doi: 10.1186/s12978-016-0264-3
24. Bohren, MA, Vogel, JP, Hunter, EC, Lutsiv, O, Makh, SK, Souza, JP, et al. The mistreatment of women during childbirth in health facilities globally: a mixed-methods systematic review. PLoS Med. (2015) 12:e1001847. doi: 10.1371/journal.pmed.1001847
25. Gebremichael, MW, Worku, A, Medhanyie, AA, Edin, K, and Berhane, Y. Women suffer more from disrespectful and abusive care than from the labour pain itself: a qualitative study from Women’s perspective. BMC Pregnancy Childbirth. (2018) 18:392. doi: 10.1186/s12884-018-2026-4
26. World Health Organization. WHO recommendations on health promotion interventions for maternal and newborn health 2015. (2024). Available at: https://www.who.int/publications/i/item/9789241508742 (Accessed January 20, 2024).
27. Bowser, D, and Hill, K. Exploring evidence for disrespect and abuse in facility-based childbirth: report of a landscape analysis. Washington DC: Harvard School of Public Health and University Research (2010).
28. Tricco, AC, Lillie, E, Zarin, W, O'Brien, KK, Colquhoun, H, Levac, D, et al. PRISMA extension for scoping reviews (PRISMA-ScR): checklist and explanation. Ann Intern Med. (2018) 169:467–73. doi: 10.7326/M18-0850
29. McGowan, J, Straus, S, Moher, D, Langlois, EV, O'Brien, KK, Horsley, T, et al. Reporting scoping reviews-PRISMA ScR extension. J Clin Epidemiol. (2020) 123:177–9. doi: 10.1016/j.jclinepi.2020.03.016
30. Kujawski, SA, Freedman, LP, Ramsey, K, Mbaruku, G, Mbuyita, S, Moyo, W, et al. Community and health system intervention to reduce disrespect and abuse during childbirth in Tanga region, Tanzania: a comparative before-and-after study. PLoS Med. (2017) 14:e1002341. doi: 10.1371/journal.pmed.1002341
31. Mengistu, B, Alemu, H, Kassa, M, Zelalem, M, Abate, M, Bitewulign, B, et al. An innovative intervention to improve respectful maternity care in three districts in Ethiopia. BMC Pregnancy Childbirth. (2021) 21:541. doi: 10.1186/s12884-021-03934-y
32. Mihret, H, Atnafu, A, Gebremedhin, T, and Dellie, E. Reducing disrespect and abuse of women during antenatal care and delivery Services at Injibara General Hospital, Northwest Ethiopia: a pre-post interventional study. Int J Women's Health. (2020) 12:835–47. doi: 10.2147/IJWH.S273468
33. Ratcliffe, HL, Sando, D, Mwanyika-Sando, M, Chalamilla, G, Langer, A, and McDonald, KP. Applying a participatory approach to the promotion of a culture of respect during childbirth. Reprod Health. (2016) 13:80. doi: 10.1186/s12978-016-0186-0
34. Asefa, A, Morgan, A, Bohren, MA, and Kermode, M. Lessons learned through respectful maternity care training and its implementation in Ethiopia: an interventional mixed methods study. Reprod Health. (2020) 17:103. doi: 10.1186/s12978-020-00953-4
35. Oosthuizen, SJ, Bergh, AM, Grimbeek, J, and Pattinson, RC. CLEVER maternity care: a before-and-after study of women's experience of childbirth in Tshwane, South Africa. Afr J Primary Health Care Fam Med. (2020) 12:e1–8. doi: 10.4102/phcfm.v12i1.2560
36. Afulani, PA, Aborigo, RA, Walker, D, Moyer, CA, Cohen, S, and Williams, J. Can an integrated obstetric emergency simulation training improve respectful maternity care? Results from a pilot study in Ghana. Birth. (2019) 46:523–32. doi: 10.1111/birt.12418
37. Swahnberg, K, Zbikowski, A, Wijewardene, K, Josephson, A, Khadka, P, Jeyakumaran, D, et al. Can forum play contribute to counteracting abuse in health care? A pilot intervention study in Sri Lanka. Int J Environ Res Public Health. (2019) 16:1616. doi: 10.3390/ijerph16091616
38. Umbeli, IO, Murwan, A, Kunna, S, Ismail, MM, and Sulman, AE. Impact of health care provider’s training on patients’ communication during labor at Omdurman maternity hospital, Sudan 2011. Sudan J Med Sci. (2014) 9:211–6. doi: 10.4314/SJMS.V9I4
39. Misago, C, Kendall, C, Freitas, P, Haneda, K, Silveira, D, Onuki, D, et al. From 'culture of dehumanization of childbirth' to 'childbirth as a transformative experience': changes in five municipalities in north-East Brazil. Int J Gynaecol Obstet. (2001) 75:S67–72. doi: 10.1016/S0020-7292(01)00511-2
40. Zbikowski, A, Brüggemann, AJ, Wijma, B, and Swahnberg, K. Counteracting abuse in health care: evaluating a one-year drama intervention with staff in Sweden. Int J Environ Res Public Health. (2020) 17:5931. doi: 10.3390/ijerph17165931
41. Afulani, PA, Dyer, J, Calkins, K, Aborigo, RA, Mcnally, B, and Cohen, SR. Provider knowledge and perceptions following an integrated simulation training on emergency obstetric and neonatal care and respectful maternity care: a mixed-methods study in Ghana. Midwifery. (2020) 85:102667. doi: 10.1016/j.midw.2020.102667
42. Infanti, JJ, Zbikowski, A, Wijewardene, K, and Swahnberg, K. Feasibility of participatory theater workshops to increase staff awareness of and readiness to respond to abuse in health care: a qualitative study of a pilot intervention using forum play among Sri Lankan health care providers. Int J Environ Res Public Health. (2020) 17:7698. doi: 10.3390/ijerph17207698
43. Dzomeku, VM, Boamah Mensah, AB, Nakua, EK, Agbadi, P, Lori, JR, and Donkor, P. Midwives’ experiences of implementing respectful maternity care knowledge in daily maternity care practices after participating in a four-day RMC training. BMC Nurs. (2021) 20:39. doi: 10.1186/s12912-021-00559-6
44. Diniz, CSG, Bussadori, JCC, Lemes, LB, Moisés, ECD, Prado, CAC, and McCourt, C. A change laboratory for maternity care in Brazil: pilot implementation of mother baby friendly birthing initiative. Med Teach. (2021) 43:19–26. doi: 10.1080/0142159X.2020.1791319
45. World Health Organization. WHO recommendations: intrapartum care for a positive childbirth experience. Geneva: World Health Organization (2018).
46. World Health Organization. Trends in maternal mortality 2000–2017. Estimates by WHO, UNICEF, UNFPA, World Bank Group and the United Nations Population Division Geneva: Department of Reproductive Health and Research. (2019). Available at: https://apps.who.int/iris/bitstream/handle/10665/327596/WHO-RHR-19.23-eng.pdf (Accessed May 31, 2024).
47. Tuglo, LS, Agbadja, C, Bruku, CS, Kumordzi, V, Tuglo, JD, Asaaba, LA, et al. The association between pregnancy-related factors and health status before and after childbirth with satisfaction with skilled delivery in multiple dimensions among postpartum mothers in the Akatsi South District, Ghana. Front Public Health. (2022) 9:779404. doi: 10.3389/fpubh.2021.779404
48. Annborn, A, and Finnbogadóttir, HR. Obstetric violence a qualitative interview study. Midwifery. (2022) 105:103212. doi: 10.1016/j.midw.2021.103212
49. Gray, T, Mohan, S, Lindow, S, and Farrell, T. Obstetric violence: clinical staff perceptions from a video of simulated practice. Eur J Obstetr Gynecol Reprod Biol. (2019) 1:100007. doi: 10.1016/j.eurox.2019.100007
50. Mena-Tudela, D, Iglesias-Casás, S, González-Chordá, VM, Valero-Chillerón, MJ, Andreu-Pejó, L, and Cervera-Gasch, Á. Obstetric violence in Spain (part III): healthcare professionals, times, and areas. Int J Environ Res Public Health. (2021) 18:3359. doi: 10.3390/ijerph18073359
51. Lefebvre, G, Calder, LA, De Gorter, R, Bowman, CL, Bell, D, Bow, M, et al. Recommendations from a National Panel on quality improvement in obstetrics. J Obstetr Gynaecol Can. (2019) 41:653–9. doi: 10.1016/j.jogc.2019.02.011
52. Thornton, RD, Nurse, N, Snavely, L, Hackett-Zahler, S, Frank, K, and DiTomasso, RA. Influences on patient satisfaction in healthcare centers: a semi-quantitative study over 5 years. BMC Health Serv Res. (2017) 17:361. doi: 10.1186/s12913-017-2307-z
53. Yadav, P, Smitha, MV, Jacob, J, and Begum, J. Intrapartum respectful maternity care practices and its barriers in eastern India. J Family Med Prim Care. (2022) 11:7657–63. doi: 10.4103/jfmpc.jfmpc_1032_22
54. Khalil, M, Carasso, KB, and Kabakian-Khasholian, T. Exposing obstetric violence in the eastern Mediterranean region: a review of Women's narratives of disrespect and abuse in childbirth. Front Glob Women's Health. (2022) 3:850796. doi: 10.3389/fgwh.2022.850796
55. Sadler, M, Santos, MJ, Ruiz-Berdún, D, Rojas, GL, Skoko, E, Gillen, P, et al. Moving beyond disrespect and abuse: addressing the structural dimensions of obstetric violence. Reprod Health Matters. (2016) 24:47–55. doi: 10.1016/j.rhm.2016.04.002
56. Wahdan, Y, and Abu-Rmeileh, NME. The association between labor companionship and obstetric violence during childbirth in health facilities in five facilities in the occupied Palestinian territory. BMC Pregnancy Childbirth. (2023) 23:566. doi: 10.1186/s12884-023-05811-2
57. Diamond-Smith, N, Treleaven, E, Murthy, N, and Sudhinaraset, M. Women’s empowerment and experiences of mistreatment during childbirth in facilities in Lucknow, India: results from a cross-sectional study. BMC Pregnancy Childbirth. (2017) 17:335. doi: 10.1186/s12884-017-1501-7
58. Madhiwalla, N, Ghoshal, R, Mavani, P, and Roy, N. Identifying disrespect and abuse in organisational culture: a study of two hospitals in Mumbai, India. Reprod Health Matters. (2018) 26:36–47. doi: 10.1080/09688080.2018.1502021
Keywords: obstetric violence, humanized childbirth, facility-based delivery, interventions, women
Citation: Yalley AA, Jarašiūnaitė-Fedosejeva G, Kömürcü-Akik B and de Abreu L (2024) Addressing obstetric violence: a scoping review of interventions in healthcare and their impact on maternal care quality. Front. Public Health. 12:1388858. doi: 10.3389/fpubh.2024.1388858
Edited by:
Tsitsi Masvawure, Worcester Polytechnic Institute, United StatesReviewed by:
Tracy Reibel, Murdoch University, AustraliaMuhabaw Shumye Mihret, University of Gondar, Ethiopia
Nicole Miriam Daniels, University of Cape Town, South Africa
Copyright © 2024 Yalley, Jarašiūnaitė-Fedosejeva, Kömürcü-Akik and de Abreu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Abena Asefuaba Yalley, YWJlbmEueWFsbGV5QHVuaS1rb25zdGFuei5kZQ==