 Lema Fikadu Wedajo1*
Lema Fikadu Wedajo1* Mohammedamin Hajure2
Mohammedamin Hajure2 Zakir Abdu3
Zakir Abdu3 Gebremeskel Mulatu Tesfaye3
Gebremeskel Mulatu Tesfaye3 Yadeta Alemayehu Workneh3
Yadeta Alemayehu Workneh3 Wubishet Gezimu3
Wubishet Gezimu3 Mustefa Adem Hussen3
Mustefa Adem Hussen3 Aman Dule Gemeda3Sheleme Mengistu Teferi2
Aman Dule Gemeda3Sheleme Mengistu Teferi2 Solomon Seyife Alemu2
Solomon Seyife Alemu2- 1Wallaga University Institute of Health Sciences, Nekemte, Ethiopia
- 2Madda Walabu University College of Medicine and Health Sciences, Robe, Ethiopia
- 3Mattu University College of Health Sciences, Mattu, Ethiopia
Background: Self-harm is a preventable, but a leading, cause of maternal morbidity and mortality all over the world, with a significant impact on healthcare systems.
Objective: To assess the magnitude of self-harm and associated factors among postnatal mothers attending immunization clinics.
Methods: An institution-based cross-sectional study was employed among postnatal mothers attending infant immunization clinics at public health facilities in Boneya Boshe Woreda, Western Ethiopia, 1 October to 30 October 2023. A pretested, face-to-face interviewer-administered structured questionnaire prepared by Kobo Toolbox was used to collect the data. Both bivariable and multivariable logistic regression analyses were done. The level of significance was declared at p-value <0.05 with a 95% CI.
Results: Among the 423 mothers enrolled in the study, 415 of them finally participated, at a response rate of 98.10%. The magnitude of self-harm was 12.53% (95% CI: 9.33, 15.73). Involvement of husband in maternity and child healthcare (AOR = 1.90; 95% CI: 1.12, 2.10), depression (AOR = 2.79; 95% CI: 2.14, 6.94), loneliness (AOR = 2.49; 95% CI: 1.15, 5.40), postpartum intimate partner violence (AOR = 2.15; 95% CI: 1.01, 4.54), average monthly income (AOR = 3.70; 95% CI: 2.17, 10.50), and postnatal care (AOR = 2.72; 95% CI: 1.28, 5.80) were significantly associated factors.
Conclusion and recommendations: The study sought a magnitude of self-harm that was slightly higher than the previous study conducted in the northern part of Ethiopia. Therefore, healthcare providers should focus on identified factors during postnatal care to overcome them. Similarly, the concerned body should develop an effective strategy based on the identified factors to pay attention to postnatal mothers.
Introduction
Self-harm is an intentional in which a person causes harm to their own selves as a coping mechanism when gripped by difficult or distressing thoughts and feelings. It most frequently takes the form of cutting, burning, or non-lethal overdoses. However, it can also be any behavior that causes injury to the victim, whether it is low or high (1, 2). The term self-harm encompasses a broad spectrum that includes a wide range of behaviors and intentions, including attempted hanging, impulsive self-poisoning, and superficial cutting in response to intolerable life events in the life process (3).
Self-harm is one of the most common reasons for hospital visits. It is a reflection of distress rather than a diagnosis in itself and is currently increasing among women of reproductive age, particularly during the perinatal period (4, 5). This problem is more common in women than men, which is one of the current global health challenges across the world (6).
During perinatal period, women are at the greatest risk of mood changes as a result of hormonal changes and life stress events related to pregnancy and childrearing processes (7–9). Common mental health problems like suicidal behaviors, postpartum psychological distress, anxiety, and postpartum stress disorders can lead to self-harm during the postnatal period if not identified and managed at an early stage (10–12).
Mental health problems are one of the leading global causes of maternal morbidity and mortality, posing the greatest challenge throughout the world (13). They also manifest as self-harm or thoughts of self-harm. The World Health Organization (WHO) estimates the magnitude of self-harm among the general population at 75.5% in both low-and middle-income countries (14). The studies conducted on postpartum mothers in both low-and high-income countries identified a varied magnitude of the problem that ranges from 4.6 to 27.4% (9, 15–17).
As identified by previous research, mental disorders, substance misuse, younger age, being unmarried, and obstetric and neonatal complications were factors leading to self-harm among postnatal mothers (18–20). In addition, lack of social support, lack of emotional support, and intimate partner violence were the other identified factors (5, 21).
Self-harm has significant consequences for infants, family members, and the healthcare system. In addition, it affects the Sustainable Development Goal agenda, which focuses on ending preventable maternal deaths by 2030 (22). Maternal self-harm leads to poor maternal–infant bonding processes that might affect infant health (15, 23). Similarly, the study identified that maternal self-harm thought causes self-harm thought in the offspring in the future and leads to early discontinuation of breastfeeding, which might increase childhood morbidity (24, 25). Maternal self-harm thoughts can also lead to childhood self-harm and suicidal ideations (26).
During the postnatal period, mothers may suffer from life-threatening health problems, including mental health problems. Even though this problem has a multi-dimensional impact, little attention has been given to it in both high-and low-income countries, which can lag behind the sustainable development goal three that focuses on the eradication of preventable causes of maternal deaths. Little attention has been given to maternal deaths all over the world, including in this specific study area, which is the focus of our research.
Therefore, this study aimed to assess the magnitude of self-harm and associated factors among postnatal mothers attending immunization clinics in public health facilities in Boneya Boshe Woreda, Western Ethiopia, in 2023. The findings of this study can be used as an input by healthcare providers to provide an evidence-based care plan to alleviate it. In addition, it may help the government to prevent maternal deaths related to self-harm and may be used as an input by scholars for further research.
Methods and materials
Study design, area, and period
An institution-based cross-sectional study design was conducted in Boneya Boshe Woreda from 1 October to 30 October 2023. This Woreda is found in the East Wallaga Zone of the Oromia region, which is located 81 km from the capital city of the zone, Nekemte town, and 311 km from the capital city of the country, Addis Ababa. Boneya Boshe Woreda is bordered by Nono Benja Woreda in the south, Gobbu Sayo and Sibu Sire Woreda in the north, Bako Tibe and Ilu Galan in the east, and Wahama Hagalo in the west.
In this Woreda, the total population is 73,227, with 14,925 households in 12 Kebeles. Out of this population, 34,803 are in the reproductive age group, of which 16,206 are women in the reproductive age group. This Woreda has an expected delivery rate of 2,541 per year. The 2022 Woreda Health Bureau report revealed that the total delivery in one year was 2,355. This Woreda has three health centers and 12 health posts, with a total of 68 health professionals to carry out healthcare activities.
Eligibility criteria
All postpartum mothers attending immunization clinics in the first one year after childbirth during data collection period and who presented with their infants whose age was from two weeks after birth to one year were included in the study. However, those mothers who were critically ill during the data collection period and not permanent residents of this Woreda were excluded from the study.
Sample size determination and sampling technique
The sample size was determined by using a single population proportion formula based on assumptions of 95% CI, 5% margin of error, and 50% of the proportion of self-harm since there has been no study done on this population in the study area, as follows:
Then
Finally, by adding 10% of the non-response rate, the final sample size of 423 was arrived at for this study. A systematic random sampling technique was used to select the study participants based on the total number of infants attending immunization clinics. Initially, the total number of infants attending three immunization clinics in this Woreda was obtained from the infant immunization logbooks of each health center. Those health centers are Bilo Health Center, Qidame Health Center, and Jawis Health Center. The number of infants attending immunization clinics were 761 from Bilo Health Center, 692 from Qidame Health Center, and 676 from Jawis Health Center 676. Then it was proportionally allocated, and the allocated mothers were selected by a systematic random sampling method as follows (Figure 1).
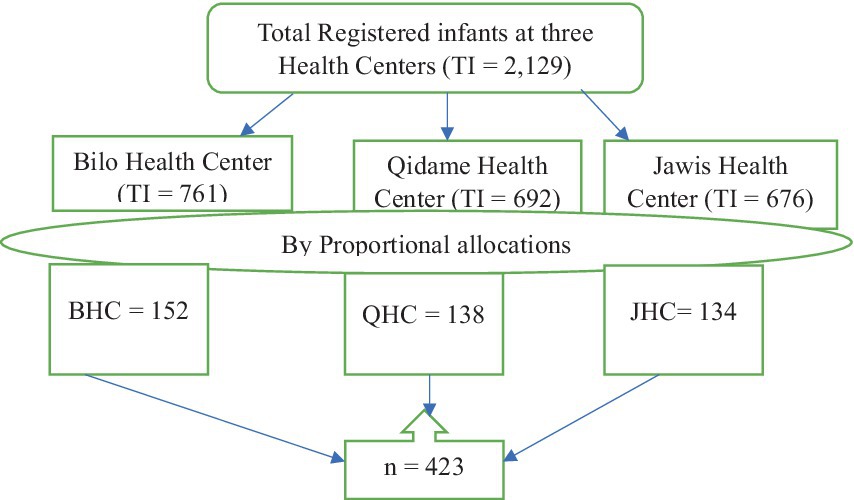
Figure 1. Diagrammatic presentation of sampling procedure to assess the magnitude of self-harm among postnatal mothers in Boneya Boshe Woreda, 2023. BHC, Bilo Health Center; QHC, Qidame Health Center; JHC, Jawis Health Center; TI, Total Infant.
Variables of the study
Dependent variable
The magnitude of self-harm was the dependent variable in this study.
Independent variables
Socio-demographic variables include maternal age, husband’s age, maternal educational level, husband’s educational level, maternal occupation, husband occupation, average monthly income, and family size.
Medical, reproductive history, and substance-related factors
The data collected for the study include the place of delivery, postnatal follow-up, history of adverse pregnancy outcome, maternal history of known diagnosed medical illnesses, history of diagnosed mental health problems during pregnancy, husband’s involvement in maternity and child healthcare, husband’s index of pregnancy during the current baby, husband’s satisfaction with the gender of the current baby, alcohol use by the father and mother of the infant, husband’s khat use, and husband’s smoking habit.
Psychosocial-related factors
Intimate partner violence during the postnatal period, postpartum depression, maternal social support level, loneliness, and the decision-making power of the mother were explored.
Operational definitions and measurements
Intentional self-harm is the condition in which an individual tries to hurt themselves purposefully. They could indulge in self-injurious behaviors like cutting, burning, hitting, hanging, overdosing, poisoning, banging head on objects, scratching the body, bloodletting (intentional act of an individual to let blood from them for self-hurt), strangulating the neck (the act of an individual to forcing or damaging one’s own neck or body for self-hurt), and electrocuting by the mother who intended to harm herself. If she has at least attempted one or more items developed provided in the Self-harm Screening Inventory (SHSI) tool to hurt herself during her first year after childbirth, she is considered to have done intentional self-harm, for which code “1” was assigned. For a mother who has not tried any of the items mentioned in the SHSI tool is considered to have not resorted to intentional self-harm, which was coded as “0” (27).
Partner involvement in maternity and child healthcare: This variable was assessed with nine questions. For each question, the responses were scored between 0 and 1. The total score was 9, with a minimum of 0 and a maximum of 9. Hence, husband’s involvement with a score above the median showed that the husband was involved in maternity an child healthcare (28).
Postpartum depression: The women who had an Edinburgh postnatal depression score of greater than or equal to 13 during their first year after childbirth were considered to be depression, and code “1” was given to them; those who scored less than 13 were not considered to have depression symptoms and coded as “0” (29).
Known medical illness: Women diagnosed with chronic medical illnesses like diabetes, cardiac disease, renal disease, hypertension, liver disease, and tuberculosis that are confirmed by doctors at health institutions are considered to have known medical illness (30).
Decision-making power: This was measured by the ability of women to act independently and decide on household activities including their health, their children’s health, freedom of movement, and control over finances without asking permission from another person. Depending on the items designed to assess maternal decision-making power, “2” was given if she decides by herself, “1” will be given if she decides jointly with her husband, and “0” was given if it is decided by others. Based on items designed to assess household decision-making power, women who scored above the median were considered to have good decision-making power and coded “1,” and those who scored below the median were considered to have poor decision-making power and were coded “0” (31).
Maternal social support: Social support was assessed by three items on the OSLO-3 social support scale. Mothers whose score was 3–8 were considered poor on social support and coded “0”. A score of 9–11 signified moderate social support and assigned the code “1”, and 12–14 indicated strong social support and code “2” was given (32).
Postpartum Intimate partner violence (PIPV): This was assessed by 13 items developed from an adapted tool to assess domestic violence against women in low-income country settings. It includes physical violence, sexual violence, and psychological violence. Any mother who is the victim of at least one type of PIPV was coded “1” and who was not the victim was coded “0” (33).
Maternal loneliness: The University of California Los Angeles (UCLA-3) 20-item Loneliness Scale (Version 3) was used to measure maternal loneliness during the first year after childbirth. The UCLA-3 20-item Loneliness Scale was used to gather the total score. Based on this tool, code “0” was given for those mothers who scored <28 (no loneliness) and “1” was given for those who scored ≥28 (had loneliness) (34).
History of adverse pregnancy outcome: Mothers who have a history of abortion, neonates with congenital anomalies that are incompatible with life, stillbirth, and/or neonatal death were considered to have adverse pregnancy outcomes for the purpose of this study.
Average monthly income: Based on this income, the mother was categorized as living above or below the poverty line based on the current classification system by the World Bank group. Earning US$1.90 or 97.85 Ethiopian Birr (ETB) or lower per day meant living below the poverty line. At the current exchange rate of US dollar to Ethiopian Birr, for 30 days, earning 2935.5 ETB or lower indicated that the mother was living below the poverty line (35).
Data collection instruments and procedures
In face-to-face interviewers, structured questionnaires prepared by Kobo Tool Box (an innovative open-source platform for collecting, managing, and visualizing data) was administered to collect the data. The tool has a socio-demographic component, reproductive history, maternal and child healthcare services, and psycho-social factors related to the mother. Postpartum intimate partner violence was assessed by 13 items containing sexual violence, psychological violence, and sexual violence (33). Postnatal depression was assessed by a validated Edinburgh postnatal depression tool that was validated in an Ethiopian context (29).
Maternal social support was assessed by a validated OSLO-3 social support scale that contains three items (32), and loneliness was assessed by the University of California Los Angeles (UCLA-3) 20-item Loneliness Scale (Version 3) (34). The outcome variable was assessed by the SHIS tool, which has 20 items to assess self-harm (27). Husband’s involvement in maternity and child healthcare was assessed by a tool developed from related literature that has nine items (28). Similarly, decision-making autonomy was assessed by nine items developed from the related literature (31).
Data quality assurance
A pretest was done on 10% of the study participants one month before data collection at Wahama Hagalo Woreda. The internal consistency of the tool was checked and had a Cronbach’s α test of 0.79. Initially, the tool was developed in the English language and translated to Afan Oromo for actual data collection, and the Afan Oromo version was retranslated back to English to cross-check the consistency of the tool.
Data was collected from three diploma holder women midwifery health professionals and supervised by three diploma holder women nurses. Training was given for two days on the objectives of the study for data collectors and the training also included participant safety for both data collectors and supervisors. Supervision was carried out by supervisors daily for the sake of clarity, accuracy, and consistency of the data.
Data processing and analysis
The data collected by Kobo Tool Box was exported to SPSS version 25 software for cleaning, coding, and further analysis. Descriptive statistics were done, and the results were presented using diagrams and tables. Both bivariable and multivariable logistic regression analyses were done to identify factors associated with self-harm during the first year after childbirth. Variables with a p-value <0.25 in binary logistic regression analysis were transferred to multivariable logistic regression.
The crude odds ratio (COR) and the adjusted odds ratio (AOR) with a 95% CI were calculated to show association and strength of association, respectively. In multivariable logistic regression analysis, variables with a p-value of <0.05 were reported as statistically significant. The model goodness-of-fit test was done. Finally, the results were presented both in the narrative, diagram, and table forms.
Results
Socio-demographic characteristics
Among the 423 postpartum mothers selected for this study, 415 mothers participated in the study, at a response rate of 98.10%. The study identified that 31.80% of the participants were in the 18–23 age category and 17.00% were in the 41–45 age category. As revealed by this study, 53.30% of the mothers were housewives and 57.38% of their husbands were farmers. In addition, 13.50% of mothers have no formal education, and 9.60% of their husbands have no formal education. Furthermore, 51.30% of mothers have an average monthly income below the poverty line, and 47.50% have family sizes greater than or equal to six (Table 1).
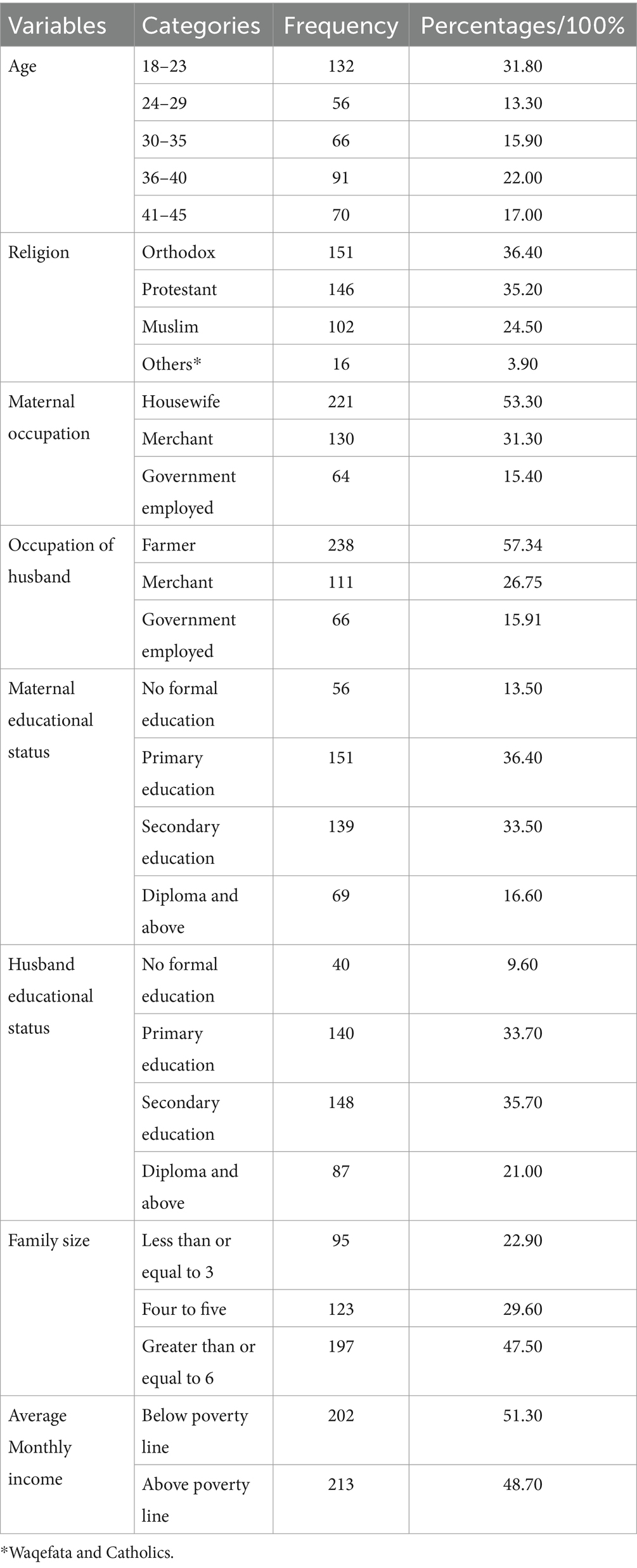
Table 1. Socio-demographic characteristics of the study participants.
Medical, reproductive history, and substance-related factors
As identified by this study, 55.18% of the infants were girls, and 52.00% of the husbands were not satisfied with the gender of their infants. Similarly, 48.00% of mothers did not intend to have the baby during the index of pregnancy. Furthermore, 78.31 and 51.80% of the mothers have antenatal care (ANC) and postnatal care (PNC) follow-up, respectively. From the total study participants, 13.50% of mothers gave birth at home and 10.80% of them have a history of adverse pregnancy outcomes. It was revealed that only 45.10% of husbands were involved in maternity and child healthcare.
In addition, 5.10 and 3.62% of mothers have been diagnosed with medical illnesses and mental illnesses, respectively. Similarly, 2.66% of their husbands have been diagnosed with medical illnesses. Furthermore, 3.90% of mothers have a family history of known diagnosed mental illnesses. Out of the total study participants, 36.39% of mothers and 52.80% of their husbands were alcohol users. Finally, 15.90% of the husband participants consume the khat (Table 2).

Table 2. Medical, reproductive history, and substance-related factors of the study participants.
Psychosocial-related factors
Out of the total study participants, 13.50 and 32.30% of mothers suffered from postnatal depression and postpartum intimate partner violence. In addition, 41.90 and 17.10% of the mothers enjoyed poor and moderate social support, respectively, during their postnatal period. Similarly, 29.40% of the mothers were lonely and only 31.81% of the mothers have decision-making power over household activities (Table 3).
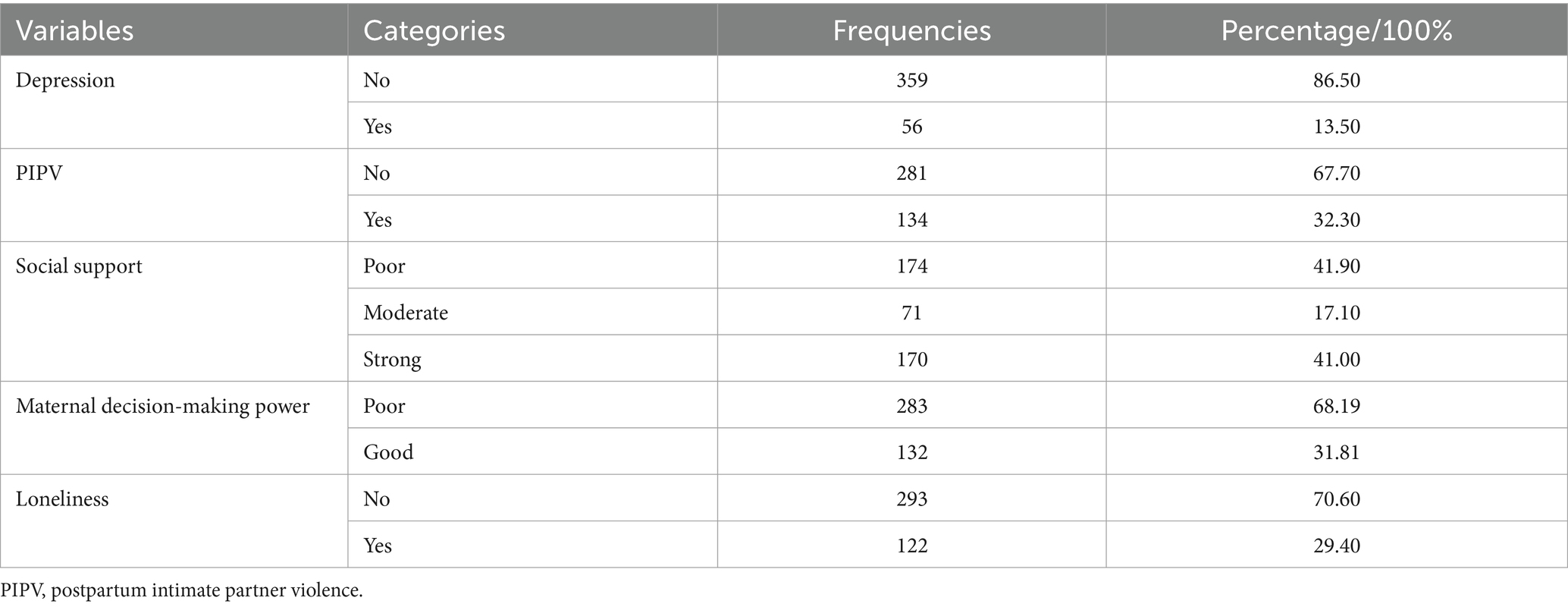
Table 3. Psychosocial-related factors.
Magnitude of self-harm among postnatal mothers attending infant immunization clinics
This study revealed that the magnitude of self-harm among postnatal mothers in this study setting was 12.53% (95% CI: 9.33, 15.73) (Figure 2).
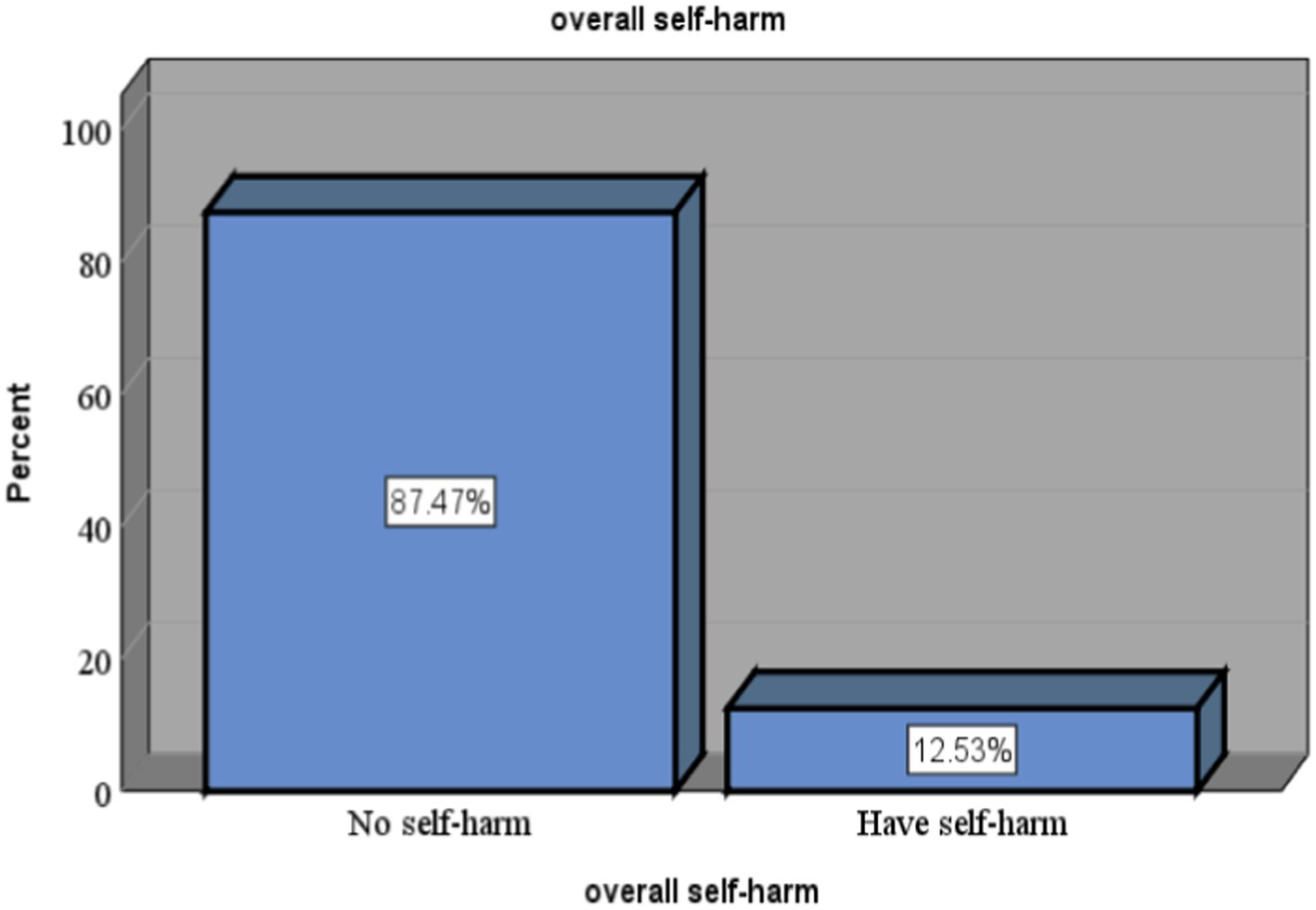
Figure 2. Magnitude of self-harm among mothers attending infant immunization clinics in Boneya Boshe Woreda.
Factors associated with self-harm and associated among postnatal mothers attending immunization clinics at public health institutions in Boneya Boshe Woreda, Western Ethiopia, 2023
From the total variables fitted for binary logistic regression at a p-value less than 0.25, six variables were significantly associated in the multivariable logistic regression model at a p-value less than 0.05 at a 95% CI. Variables significantly associated with self-harm in the final model were husband’s involvement in maternity and child healthcare, depression, loneliness, postnatal follow-up, postpartum intimate partner violence, and average monthly incomes.
This study identified that the odds of self-harm among mothers whose husbands do not participate in maternity and child healthcare were 1.90 times higher than those whose husbands participate in the care (AOR = 1.90; 95% CI: 1.12, 2.10). In addition, the odds of self-harm among mothers who have depression were 2.79 times higher than their counterparts (AOR = 2.79; 95% CI: 2.14, 6.94), and the odds of self-harm among mothers who do not have postnatal follow-up were 2.72 times higher than those who follow their postnatal care (AOR = 2.72; 95% CI: 1.28, 5.80).
Similarly, the odds of self-harm among mothers who have loneliness were 2.49 times higher than their counterparts (AOR = 2.49; 95% CI: 1.15, 5.40), and the odds of self-harm among mothers who suffered from postpartum intimate partner violence were 2.15 times higher than those who did not face the problem (AOR = 2.15; 95% CI: 1.01, 4.54). Finally, the study identified that the odds of self-harm among mothers with average monthly income below the poverty line were 3.70 times higher than those who were above the poverty line (AOR = 3.70; 95% CI: 2.17, 10.50) (Table 4).
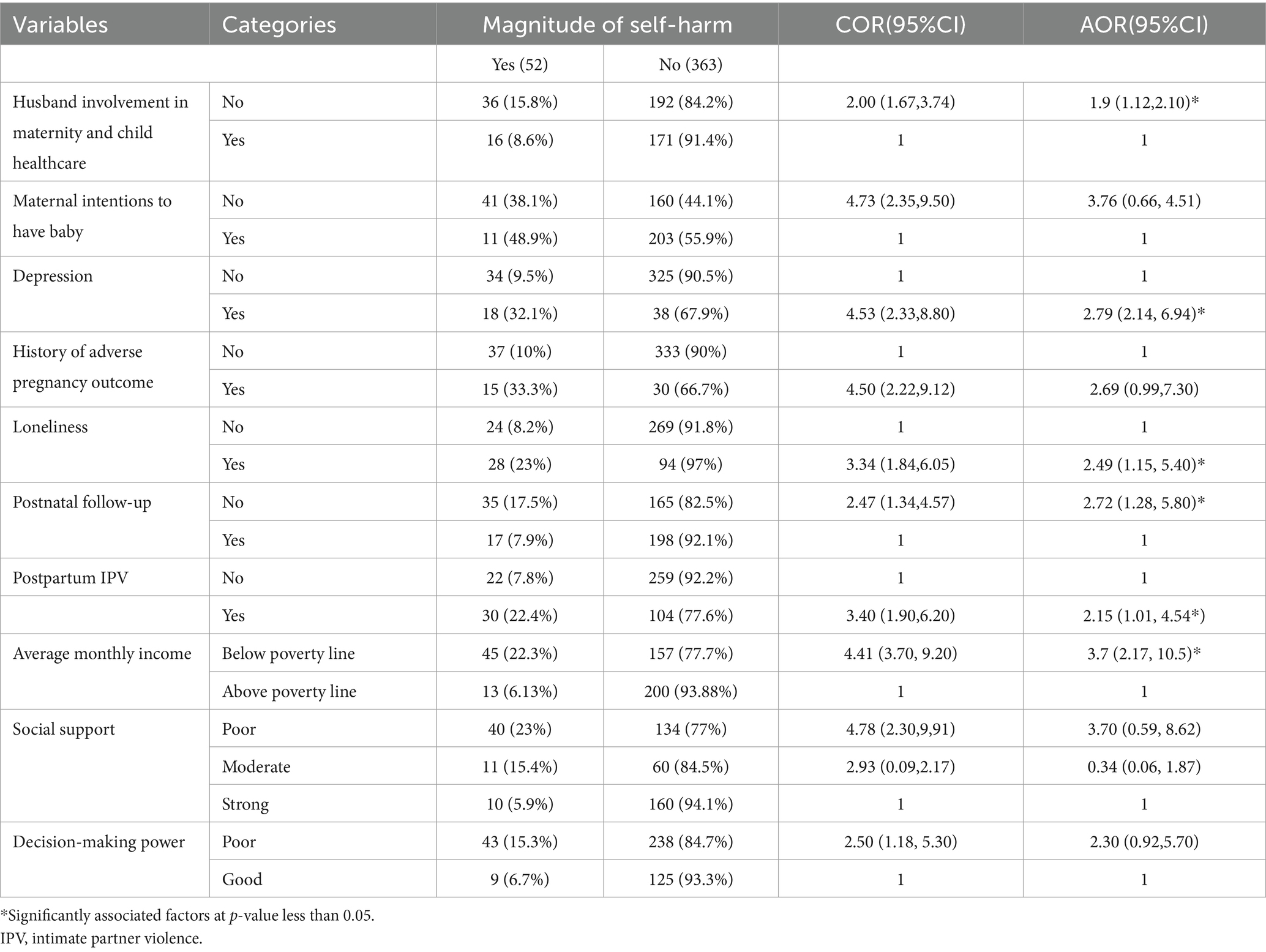
Table 4. Factors associated with self-harm among postnatal mothers attending infant immunization clinics.
Discussion
Self-harm is a significant maternal health problem that can be prevented by screening and providing care for those mothers who have risks related to this problem. This study revealed that the magnitude of self-harm thought among postnatal mothers was 12.53%. The finding is comparable with the study conducted in Canada, which reported self-harm at 10.40% (19). However, the findings of this study were lower than those of the studies conducted in Sri Lanka (27.40%) (9), London (16.79%) (7), and the United States (19.3%) (36). The discrepancies might be due to differences in the assessment methods employed and sample size used for the studies, as these three studies used a larger sample size, which might increase the magnitude of self-harm thoughts.
Conversely, the findings of this study are lower than those of the studies conducted in northern Ethiopia (8.5%), South Africa (7%) (37), and Japan (9.1%) (38). The possible justifications for the discrepancies might be also attributed to the study period or years of the studies. The discrepancies between the study conducted in the northern part of Ethiopia and our study might be due to the current market inflation in Ethiopia, which might increase life expectancy and push mothers to self-harm as they are unable to fulfill the economic demands of their family members in the current market situation.
Husband’s involvement in maternity and child healthcare is significantly associated with self-harm thoughts during the postnatal period. The possible scientific reason might be that women whose husbands are involved in maternity and child healthcare feel confident that their husbands are with them in any ups and downs of life, which may affect their feelings as a result of physiological changes during childbirth (28). In addition, husbands who are involved in maternity and child healthcare consult the health professionals as they observe emotional and psychological changes in their wives during the postnatal period and have obtained information from health professionals regarding their families’ health (39).
Similarly, this study identified that having depression is significantly associated with self-harm thoughts. This evidence is supported by the study conducted in Canada (19). The possible reason might be that depression during the postpartum period pushes mothers to self-harm as a result of the unmanaged postpartum depression, which leads to postpartum psychosis, posing a high level of danger for both maternal and infant’s health, ending up with postpartum morbidity (7).
The study also revealed that loneliness is significantly associated with self-harm thoughts. Even though there was no evidence to support this finding, loneliness pushes the mothers to self-harm, and as a result, they may feel empty as they lack people around them during the postpartum period. If there are no people around them for support, the anxiety levels of mothers increase, which worsens the thoughts of self-harm as a defense mechanism to be out of their feelings, and loneliness leads to mental health problems (40).
In addition, the average monthly income is a significantly associated factor with thoughts of self-harm during the postnatal period. This finding is supported by the study conducted in northern Ethiopia (21). The reason might be that mothers whose monthly income is below the poverty line might be stressed about their income, which might not be sufficient to support the livelihood of the families. Similarly, they lose hope, which pushes them to take action on their lives if they are unable to fulfill their family’s needs due to lack of money to fulfill even their basic needs.
Furthermore, postpartum intimate partner violence is a significant factor associated with self-harm thoughts during the postnatal period. This finding is supported by the study conducted in the northern part of Ethiopia (21). The possible justification might be that mothers who suffer from this problem might fall into psychological crisis as a result of their husband’s bad attitude toward them, and those mothers lose hope, which pushes them to life-threatening problems like self-harm thoughts.
Finally, the study identified that postpartum follow-up is a significantly associated factor with maternal self-harm thoughts. As already known, postpartum follow-up is key for the upkeep of maternal and infant health and may help health professionals screen the problem early to take action. Postpartum follow-up is part of the maternal continuum of care, which improves overall maternal health (41). During postpartum follow-up, mothers may consult their health professionals for any mental health problems that may occur during the postpartum period as a result of hormonal and physiological changes related to childbirth.
Limitations and strengths of the study
Since it was a cross-sectional study, it does not identify cause-and-effect relationships. In addition, since it was an institution-based study, it might lead to an underestimation of the magnitude of self-harm thoughts. The study focused on the neglected areas that hold great significance for reducing preventable causes of maternal deaths and assessed important factors that have a great impact on maternal health.
Conclusion and recommendations
This study revealed that the magnitude of self-harm thoughts during the postnatal period was a significant maternal health problem in the study setting. It was identified that the husband’s involvement in maternity and child healthcare, loneliness, depression, average monthly income below the poverty line, postpartum follow-up, and postpartum intimate partner violence were factors significantly associated with maternal self-harm thoughts. Husband’s involvement in maternity and child healthcare is needed to overcome the problem. In addition, the Ministry of Health should develop an effective strategy for preserving maternal health after childbirth based on the identified factors. The future studies in this direction need to have better study designs and large sample sizes.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The ethical clearance was obtained from the Wallaga University Institute of Health Sciences. Written informed consent was obtained from the study participants after they were informed of the overall nature of the study and its benefits for the mothers and the implications for policymakers.
Author contributions
LW: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing, Funding acquisition. MH: Conceptualization, Investigation, Resources, Supervision, Writing – review & editing. ZA: Conceptualization, Investigation, Resources, Supervision, Writing – review & editing. GT: Conceptualization, Investigation, Resources, Supervision, Writing – review & editing. YW: Conceptualization, Investigation, Resources, Supervision, Writing – review & editing. WG: Conceptualization, Investigation, Resources, Supervision, Writing – review & editing. MAH: Conceptualization, Investigation, Resources, Supervision, Writing – review & editing. AG: Conceptualization, Investigation, Resources, Supervision, Writing – review & editing. ST: Conceptualization, Investigation, Resources, Supervision, Writing – review & editing. SA: Conceptualization, Data curation, Investigation, Methodology, Resources, Supervision, Validation, Visualization, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Acknowledgments
Our heartfelt thanks go to Wallaga University for providing us with ethical clearance, and we express our deepest gratitude to our study participants.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Abbreviations
IPV, intimate partner violence; PNC, postnatal care; AOR, adjusted odds ratio; COR, crude odds ratio.
References
1. Laye-Gindhu, A, and Schonert-Reichl, KA. Nonsuicidal self-harm among community adolescents: understanding the “whats” and “whys” of self-harm. J Youth Adolesc. (2005) 34:447–57. doi: 10.1007/s10964-005-7262-z
2. McHale, J, and Felton, A. Self-harm: what’s the problem? A literature review of the factors affecting attitudes towards self-harm. J Psychiatr Ment Health Nurs. (2010) 17:732–40. doi: 10.1111/j.1365-2850.2010.01600.x
5. Bijjal, SS, Ganiger, FB, Mugali, JD, Shaikh, M, Purad, V, and Anirudh, B. A descriptive review on perinatal deliberate self-harm: an untraversed mental health domain. J Psychiatry Spect. (2023) 2:16–21. doi: 10.4103/jopsys.jopsys_52_22
6. Li, C-Q, Zhang, J-S, Ma, S, Lv, R-R, Duan, J-L, Luo, D-M, et al. Gender differences in self-harm and drinking behaviors among high school students in Beijing, China. BMC Public Health. (2020) 20:1–11. doi: 10.1186/s12889-020-09979-6
7. Pope, CJ, Xie, B, Sharma, V, and Campbell, MK. A prospective study of thoughts of self-harm and suicidal ideation during the postpartum period in women with mood disorders. Arch Womens Ment Health. (2013) 16:483–8. doi: 10.1007/s00737-013-0370-y
8. Healey, C, Morriss, R, Henshaw, C, Wadoo, O, Sajjad, A, Scholefield, H, et al. Self-harm in postpartum depression and referrals to a perinatal mental health team: an audit study. Arch Womens Ment Health. (2013) 16:237–45. doi: 10.1007/s00737-013-0335-1
9. Arachchi, NSM, Ganegama, R, Husna, AWF, Chandima, DL, Hettigama, N, Premadasa, J, et al. Suicidal ideation and intentional self-harm in pregnancy as a neglected agenda in maternal health; an experience from rural Sri Lanka. Reprod Health. (2019) 16:1–7. doi: 10.1186/s12978-019-0823-5
10. Oates, M. Risk and childbirth in psychiatry. Adv Psychiatr Treat. (1995) 1:146–53. doi: 10.1192/apt.1.5.146
11. Stewart, RC, Bunn, J, Vokhiwa, M, Umar, E, Kauye, F, Fitzgerald, M, et al. Common mental disorder and associated factors amongst women with young infants in rural Malawi. Soc Psychiatry Psychiatr Epidemiol. (2010) 45:551–9. doi: 10.1007/s00127-009-0094-5
12. Johannsen, BM, Larsen, JT, Laursen, TM, Ayre, K, Howard, LM, Meltzer-Brody, S, et al. Self-harm in women with postpartum mental disorders. Psychol Med. (2020) 50:1563–9. doi: 10.1017/S0033291719001661
13. Bustreo, F, Say, L, Koblinsky, M, Pullum, TW, Temmerman, M, and Pablos-Méndez, A. Ending preventable maternal deaths: the time is now. Lancet Glob Health. (2013) 1:e176–7. doi: 10.1016/S2214-109X(13)70059-7
14. World Health Organization. Preventing suicide: A global imperative. Geneva: World Health Organization (2014).
15. Gordon, H, Nath, S, Trevillion, K, Moran, P, Pawlby, S, Newman, L, et al. Self-harm, self-harm ideation, and mother-infant interactions: a prospective cohort study. J Clin Psychiatry. (2019) 80:11311. doi: 10.4088/JCP.18m12708
16. Giallo, R, Pilkington, P, Borschmann, R, Seymour, M, Dunning, M, and Brown, S. The prevalence and correlates of self-harm ideation trajectories in Australian women from pregnancy to 4-years postpartum. J Affect Disord. (2018) 229:152–8. doi: 10.1016/j.jad.2017.12.064
17. Coker, JL, Tripathi, SP, Knight, BT, Pennell, PB, Magann, EF, Newport, DJ, et al. Rating scale item assessment of self-harm in postpartum women: a cross-sectional analysis. Arch Womens Ment Health. (2017) 20:687–94. doi: 10.1007/s00737-017-0749-2
18. Ayre, K, Gordon, HG, Dutta, R, Hodsoll, J, and Howard, LM. The prevalence and correlates of self-harm in the perinatal period: a systematic review. J Clin Psychiatry. (2019) 81:15343. doi: 10.4088/JCP.19r12773
19. Palladino, E, Varin, M, Lary, T, and Baker, MM. Thoughts of self-harm and associated risk factors among postpartum women in Canada. J Affect Disord. (2020) 270:69–74. doi: 10.1016/j.jad.2020.03.054
20. Kim, JJ, La Porte, LM, Saleh, MP, Allweiss, S, Adams, MG, Zhou, Y, et al. Suicide risk among perinatal women who report thoughts of self-harm on depression screens. Obstet Gynecol. (2015) 125:885–93. doi: 10.1097/AOG.0000000000000718
21. Tiguh, AE, Wondie, KY, Gessesse, DN, Tsega, NT, Aklil, MB, Temesgan, WZ, et al. Self-harm among post-natal mothers in Northwest Ethiopia: implication for policy and practice. Front Public Health. (2022) 10:916896. doi: 10.3389/fpubh.2022.916896
22. Callister, LC, and Edwards, JE. Sustainable development goals and the ongoing process of reducing maternal mortality. J Obstet Gynecol Neonatal Nurs. (2017) 46:e56–64. doi: 10.1016/j.jogn.2016.10.009
23. Borschmann, R, Molyneaux, E, Spry, E, Moran, P, Howard, LM, Macdonald, JA, et al. Pre-conception self-harm, maternal mental health and mother–infant bonding problems: a 20-year prospective cohort study. Psychol Med. (2019) 49:2727–35. doi: 10.1017/S0033291718003689
24. Paul, E, Kwong, A, Moran, P, Pawlby, S, Howard, LM, and Pearson, RM. Maternal thoughts of self-harm and their association with future offspring mental health problems. J Affect Disord. (2021) 293:422–8. doi: 10.1016/j.jad.2021.06.058
25. Gidai, J, Acs, N, Banhidy, F, and Czeizel, AE. A study of the effects of large doses of medazepam used for self-poisoning in 10 pregnant women on fetal development. Toxicol Ind Health. (2008) 24:61–8. doi: 10.1177/0748233708089016
26. Geulayov, G, Metcalfe, C, Heron, J, Kidger, J, and Gunnell, D. Parental suicide attempt and offspring self-harm and suicidal thoughts: results from the Avon longitudinal study of parents and children (ALSPAC) birth cohort. J Am Acad Child Adolesc Psychiatry. (2014) 53:509–517.e2. e502. doi: 10.1016/j.jaac.2013.12.022
27. Kim, S, Seo, DG, Park, J-C, Son, Y, Lee, J-H, Yoon, D, et al. Development and validation of the self-harm screening inventory (SHSI) for adolescents. PLoS One. (2022) 17:e0262723. doi: 10.1371/journal.pone.0262723
28. Yargawa, J, and Leonardi-Bee, J. Male involvement and maternal health outcomes: systematic review and meta-analysis. J Epidemiol Community Health. (2015) 69:604–12. doi: 10.1136/jech-2014-204784
29. Tesfaye, M, Hanlon, C, Wondimagegn, D, and Alem, A. Detecting postnatal common mental disorders in Addis Ababa, Ethiopia: validation of the Edinburgh postnatal depression scale and Kessler scales. J Affect Disord. (2010) 122:102–8. doi: 10.1016/j.jad.2009.06.020
30. Kebede, AA, Gessesse, DN, Tsega, NT, Aklil, MB, Temesgan, WZ, Abegaz, MY, et al. Prevalence and factors associated with maternal loneliness during the postpartum period in Gondar city. Heliyon. (2022) 8:e09891. doi: 10.1016/j.heliyon.2022.e09891
31. Kebede, AA, Cherkos, EA, Taye, EB, Eriku, GA, Taye, BT, and Chanie, WF. Married women’s decision-making autonomy in the household and maternal and neonatal healthcare utilization and associated factors in Debretabor, Northwest Ethiopia. PLoS One. (2021) 16:e0255021. doi: 10.1371/journal.pone.0255021
32. Kocalevent, RD, Berg, L, Beutel, ME, Hinz, A, Zenger, M, Harter, M, et al. Social support in the general population: standardization of the Oslo social support scale (OSSS-3). BMC Psychol. (2018) 6:31. doi: 10.1186/s40359-018-0249-9
33. Semahegn, A, Torpey, K, Manu, A, Assefa, N, and Ankomah, A. Adapted tool for the assessment of domestic violence against women in a low-income country setting: a reliability analysis. Int J Women's Health. (2019) 11:65–73. doi: 10.2147/IJWH.S181385
34. Russell, DW. UCLA loneliness scale (version 3): reliability, validity, and factor structure. J Pers Assess. (1996) 66:20–40. doi: 10.1207/s15327752jpa6601_2
35. Dibabu, AM, Ketema, TG, Beyene, MM, Belachew, DZ, Abocherugn, HG, and Mohammed, AS. Preoperative anxiety and associated factors among women admitted for elective obstetric and gynecologic surgery in public hospitals, southern Ethiopia: a cross-sectional study. BMC Psychiatry. (2023) 23:728. doi: 10.1186/s12888-023-05005-2
36. Wisner, KL, Sit, DK, McShea, MC, Rizzo, DM, Zoretich, RA, Hughes, CL, et al. Onset timing, thoughts of self-harm, and diagnoses in postpartum women with screen-positive depression findings. JAMA Psychiatry. (2013) 70:490–8. doi: 10.1001/jamapsychiatry.2013.87
37. Rodriguez, VJ, Mandell, LN, Babayigit, S, Manohar, RR, Weiss, SM, and Jones, DL. Correlates of suicidal ideation during pregnancy and postpartum among women living with HIV in rural South Africa. AIDS Behav. (2018) 22:3188–97. doi: 10.1007/s10461-018-2153-y
38. Doi, S, and Fujiwara, T. Combined effect of adverse childhood experiences and young age on self-harm ideation among postpartum women in Japan. J Affect Disord. (2019) 253:410-418. doi: 10.1016/j.jad.2019.04.079
39. Mullany, BC, Becker, S, and Hindin, M. The impact of including husbands in antenatal health education services on maternal health practices in urban Nepal: results from a randomized controlled trial. Health Educ Res. (2007) 22:166–76. doi: 10.1093/her/cyl060
40. Hutten, E, Jongen, EM, Vos, AE, van den Hout, AJ, and van Lankveld, JJ. Loneliness and mental health: the mediating effect of perceived social support. Int J Environ Res Public Health. (2021) 18:11963. doi: 10.3390/ijerph182211963
Keywords: self-harm, immunization clinics, Boneya Boshe, infant immunization, postnatal mothers
Citation: Wedajo LF, Hajure M, Abdu Z, Tesfaye GM, Workneh YA, Gezimu W, Hussen MA, Gemeda AD, Teferi SM and Alemu SS (2024) Magnitude of self-harm and associated factors among postnatal mothers attending immunization clinics at public health facilities in Boneya Boshe Woreda, Western Ethiopia, 2023: institution-based cross-sectional study design. Front. Public Health. 12:1384688. doi: 10.3389/fpubh.2024.1384688
Edited by:
Sami Hamdan, Academic College Tel Aviv-Yaffo, IsraelReviewed by:
Deblina Roy, All India Institute of Medical Sciences, IndiaAnnie Lewis-O'Connor, Harvard Medical School, United States
Copyright © 2024 Wedajo, Hajure, Abdu, Tesfaye, Workneh, Gezimu, Hussen, Gemeda, Teferi and Alemu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Lema Fikadu Wedajo, bGVtYWZpa2EyMDE0QGdtYWlsLmNvbQ==