
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health , 05 April 2024
Sec. Digital Public Health
Volume 12 - 2024 | https://doi.org/10.3389/fpubh.2024.1384078
 Dagmawit G. Gashaw1*
Dagmawit G. Gashaw1* Zewdie Aderaw Alemu2
Zewdie Aderaw Alemu2 Freddy Constanzo3,4*Feben T. Belay5Yakob W. Tadesse6Carla Muñoz4Juan Pablo Rojas4
Freddy Constanzo3,4*Feben T. Belay5Yakob W. Tadesse6Carla Muñoz4Juan Pablo Rojas4 Cristobal Alvarado-Livacic4
Cristobal Alvarado-Livacic4Background: The quality assessment of the home-based isolation and care program (HBIC) relies heavily on patient satisfaction and length of stay. COVID-19 patients who were isolated and received HBIC were monitored through telephone consultations (TC), in-person TC visits, and a self-reporting application. By evaluating patient satisfaction and length of stay in HBIC, healthcare providers could gauge the effectiveness and efficiency of the HBIC program.
Methods: A cross-sectional study design enrolled 444 HBIC patients who answered a structured questionnaire. A binary logistic regression model assessed the association between independent variables and patient satisfaction. The length of stay in HBIC was analyzed using Cox regression analysis. The data collection started on April (1–30), 2022, in Addis Ababa, Ethiopia.
Results: The median age was 34, and 247 (55.6%) were females. A greater proportion (313, 70.5%) of the participants had high satisfaction. Higher frequency of calls (>3 calls) (AOR = 2.827, 95% CI = 1.798, 4.443, p = 0.000) and those who were symptomatic (AOR = 2.001, 95% CI = 1.289, 3.106, p = 0.002) were found to be significant factors for high user satisfaction. Higher frequency of calls (>3 calls) (AHR = 0.537, 95% CI = 0.415, 0.696, p = 0.000) and more in-person visits (>1 visit) (AHR = 0.495, 95% CI = 0.322, 0.762, p = 0.001) had greater chances to reduce the length of stay in the COVID-19 HBIC.
Conclusion: 70.5% of the participants had high satisfaction with the system, and frequent phone call follow-ups on patients’ clinical status can significantly improve their satisfaction and length of recovery. An in-person visit is also an invaluable factor in a patient’s recovery.
The global COVID-19 pandemic has had a significant impact on numerous countries, resulting in a staggering number of confirmed cases and deaths worldwide. Specifically, 774,771,942 confirmed cases and 7,035,337 deaths were reported globally. In Africa, approximately 9,576,309 confirmed cases and 175,500 deaths have been recorded, whereas Ethiopia alone has reported 501,157 confirmed cases and 7,574 deaths (1). Given the outbreak’s severity and the prevailing epidemiological situation, the Federal Ministry of Health of Ethiopia has taken swift action by developing, approving, and implementing a national guide on home-based isolation and care (HBIC). This guide is tailored for asymptomatic and mildly confirmed COVID-19 cases (2). Consequently, many patients have enrolled in the system, establishing a comprehensive telephone consultation (TC) service. Healthcare workers from health centers have been diligently monitoring the clinical condition of these patients through regular phone calls or in-person visits (2). The national or regional COVID-19 emergency centers are available for assistance to ensure that patients receive the necessary support and information. Patients facing challenges or requiring guidance on the system’s functioning, worsening symptoms, medication advice, or ambulance requests can reach these centers (2). This approach provides comprehensive care and support to individuals affected by COVID-19 in Ethiopia.
Several studies have emphasized the utilization of teleconsultations (TC) in Sub-Saharan Africa amid the COVID-19 outbreak. For instance, a study conducted at the Aga Khan Hospital in Dar es Salaam, Tanzania, revealed varying frequencies of TC calls over 3 months, with peaks observed at 7 weeks and lows at 13 weeks (3). In Uganda, the Ministry of Health rolled out TC services across multiple health centers simultaneously (4). Similarly, in Cameroon, many physicians resorted to TC consultations during the pandemic, often using WhatsApp applications (5). Despite the progress in telemedicine practices, assessing the quality of care provided through these methods is crucial. Quality indicators for telemedicine outcomes include mortality rates, average length of stay, and complication rates (6). The adoption of telemedicine has played a pivotal role in enhancing the quality of diagnosis and treatment in primary public hospitals (7). This is evident in the reduction of treatment duration, decrease in the average length of hospital stays, and decline in the percentage of critically ill patients (8). Moreover, telemedicine aids in improving personalized care and broadening the accessibility of medical services. Healthcare providers can deliver more efficient and effective patient care by harnessing telemedicine, particularly during crises such as the COVID-19 pandemic (9, 10). Patient satisfaction is a significant indicator of the societal perception of healthcare services, particularly in telemedicine. The practical advantages of telemedicine further underscore its social reputation within primary healthcare facilities. First, Telemedicine plays a crucial role in alleviating the financial burden on patients and their families by eliminating expenses associated with transportation and accommodation (11). Second, the efficient nature of telemedicine expedites disease diagnosis and treatment, thereby mitigating patients’ suffering (11). Lastly, telemedicine’s unique “face-to-face” communication system fosters a novel connection between medical professionals and patients, ultimately enhancing the healthcare experience (12, 13). Despite numerous studies, the findings remain inconclusive and conflicting. Some researchers suggested recruiting adaptable patients who embrace this new technology’s convenience (14). Conversely, others highlight limitations, such as the relative novelty of telehealth in medicine, which makes it challenging to compare its outcomes with those of more traditional interventions (15). In addition, patient satisfaction is a complex and multifaceted concept influenced by various factors. However, the factors influencing patient satisfaction in different settings or conditions remain debated (15).
Patient satisfaction and length of stay are crucial metrics for assessing the quality of healthcare programs. This study aimed to provide insights into the factors influencing the satisfaction and length of stay in HBIC of COVID-19 patients in Addis Ababa, Ethiopia. This study uses traditional care (TC) and hybrid (in-person-TC) approaches in different sub-city areas. By understanding these factors, policymakers can develop strategic plans to improve the quality of healthcare services, thereby ensuring high satisfaction levels and shorter medical residence stays. The findings of this study can also inform the National Public Health Emergency Operation Center and the Federal Ministry of Health in Ethiopia on how to intervene and strengthen the healthcare system. In addition, the results can contribute to expanding telemedicine services and adopting digital health technologies in the country’s healthcare sector.
This study focuses on Addis Ababa, primarily because of the significant burden of COVID-19 cases. Ethiopia alone has reported 501,157 confirmed cases and 7,574 deaths, with nearly 67% of these cases originating in Addis Ababa (1). Moreover, implementing the COVID-19 HBIC model in Addis Ababa surpasses other regions. Furthermore, the HBIC’s self-reporting and follow-up application is exclusively available in Addis Ababa, making it an ideal location for research. Addis Ababa is divided into 11 sub-cities [Addis Ketema, Akaky Kaliti, Arada, Bole, Gullele, Kirkos, Kolfe Keranio, Lideta, Nefas Silk-Lafto, Yeka, Lemi Kura (New)], all of which have adopted the HBIC system for COVID-19 patients since the initial case was identified. The digital follow-up tool was specifically launched in the Bole sub-city (Figure 1).
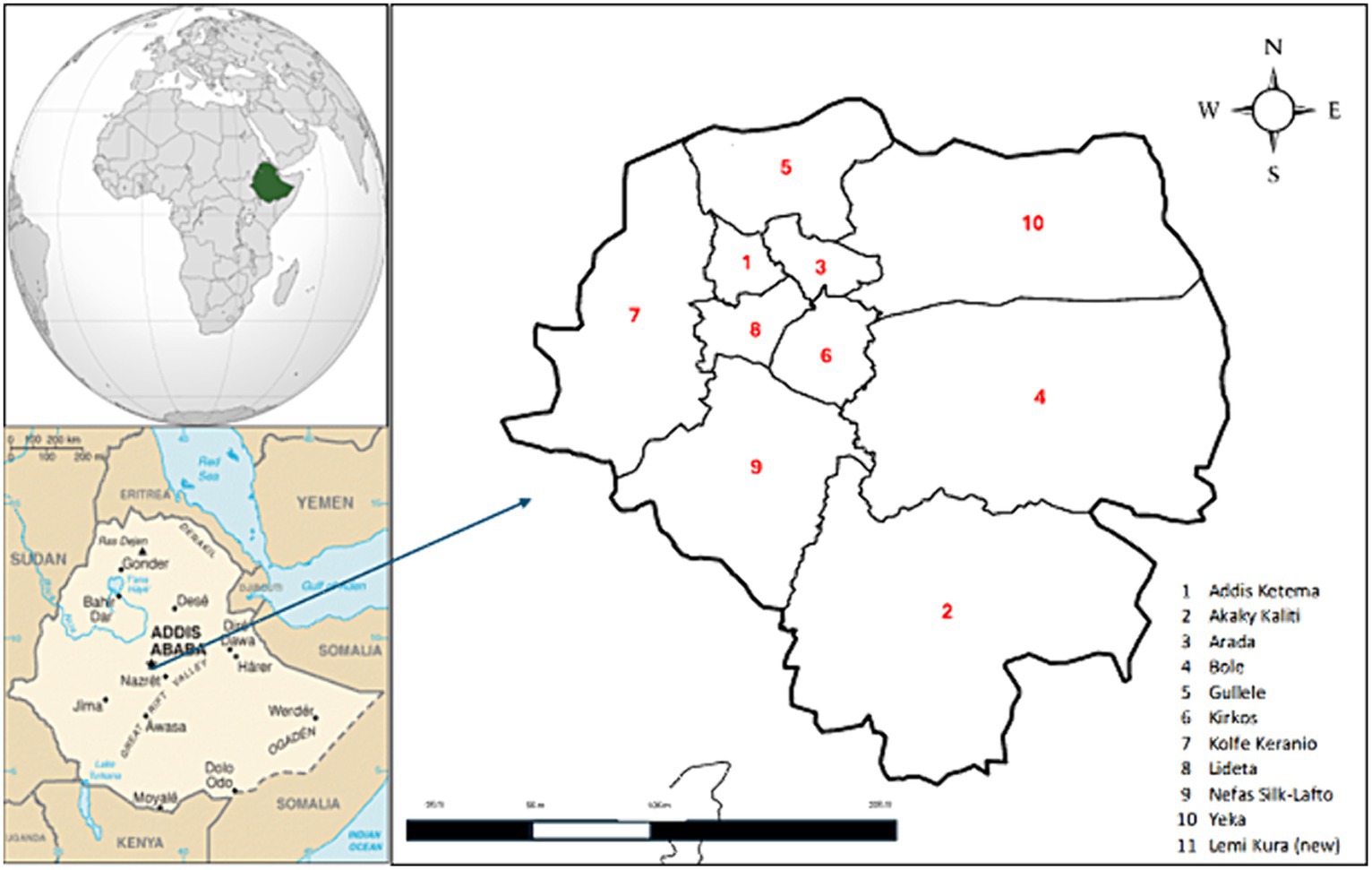
Figure 1. Addis Ababa district locations. This map of the 11 Addis Ababa sub-cities is included in this study. Lemi Kura is a new district and is not included in this map.
The study was conducted from 1 to 30 April 2022 in Addis Ababa, Ethiopia.
Each sub-city is equipped with two to four health centers that serve as the base for the telemedicine medical team. A well-established system ensures that patient data is promptly transmitted to follow-up teams, enabling healthcare workers to initiate their follow-up procedures without delay. To support this initiative, the Ethiopian Public Health Institute and Addis Ababa Health Bureau allocated a tablet with complimentary airtime to each sub-city proportionate to the needs of the telemedicine medical team.
This study encompasses all individuals diagnosed with COVID-19 who were isolated, received care at home, and met the criteria for inclusion. The study population consisted of confirmed COVID-19 cases admitted to HBIC from its inception, aged between 18 and 60, individuals who underwent regular follow-up assessments while at HBIC, and those whose contact information was documented in the registry.
Patients were classified based on the following criteria: Gender (male, female), Age (<30, 31–40, 41–50, 51–60 years), city of residence, education level (no education and elementary, secondary and diploma, degree and above), occupation (government employee, private employee, self-employee, not working), symptoms (asymptomatic, symptomatic), type of attention (only telephone call—TC, telephone call with in-person visits - in-person-TC), frequency of calls (≤2 calls, ≥3 calls), and frequency of in-person visits (no visits, ≤2 visits, ≥3 visits).
A cross-sectional research design assessed two primary variables: patient satisfaction and length of stay in HBIC in days. The formula for a single population proportion was applied to determine the required population size of 385 (with a Z-score of 1.96, an outcome proportion of 50%, and a marginal error of 5%). The technique of proportionate stratified sampling involved dividing the entire population into 11 strata or sub-cities. The total sample size was then distributed proportionally among each sub-city based on the burden of the disease. Study participants were selected from each stratum or sub-city using systematic probability sampling (Figure 2).
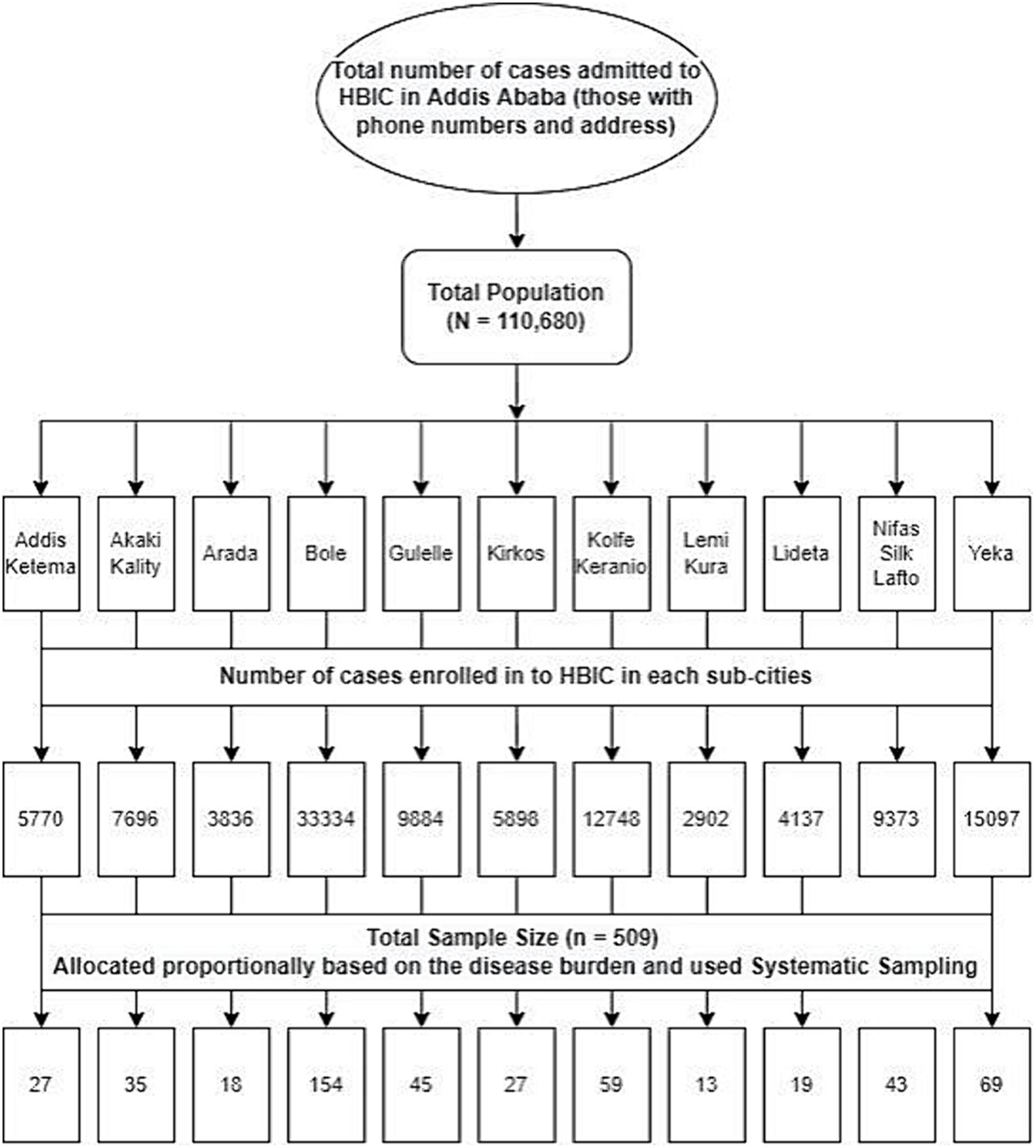
Figure 2. Data collection. Sampling technique from each sub-city in Addis Ababa, Ethiopia.
A validated patient satisfaction survey from the teleneurology program in Chile (13) employed a Likert scale to assess the extent of patient satisfaction. To ensure the accuracy and reliability of the data collected, a pretest was conducted on a random sample of 23 (5%) patients. Based on the findings from the pretest, necessary amendments were made to the data collection tool. Additionally, the collected data underwent daily reviews for clarity and completeness checks. Before analysis, the internal consistency of the questionnaire was evaluated using Cronbach’s alpha test (13). The local language was used during data collection to ensure the required information was collected with greater understanding. To facilitate this, the data collection questionnaire was first developed in English and then translated into Amharic, and the data collected were back-translated to English for consistency. The data collectors administered the questionnaire over the telephone, and responses were recorded on the individual datasheets. Training on the basics of the questionnaire and how to use it appropriately was given by the principal investigator for two BSc nurses for 2 days.
The final questionnaire consisted of 17 closed-response questions, each assigned a numerical value ranging from 1 (totally disagree) to 5 (totally agree). The questions were categorized into four contextualized areas. The overall score on the questionnaire, with a maximum of 85 points, served as an indicator of patient satisfaction. The scoring system classified satisfaction levels as follows: very low (17 points or below), low (18–34 points), moderate (35–51 points), high (52–68 points), and very high (69–85 points). Following completion of the survey, patients were divided into two main groups based on their scores: (i) those with a score below 51 points, indicating moderate or low patient satisfaction, and (ii) those with a score over 52 points, indicating high or very high patient satisfaction (Table 1).
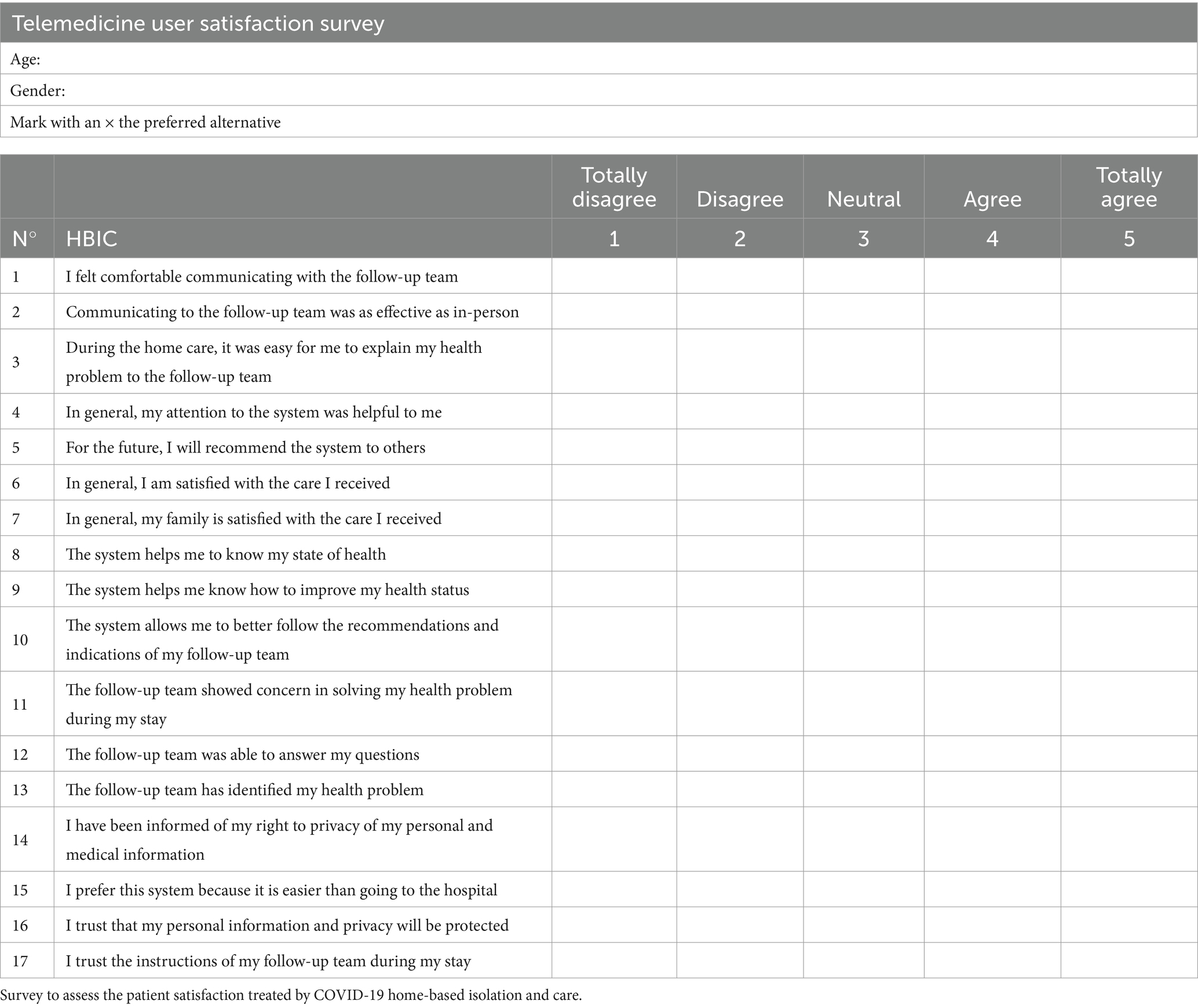
Table 1. Study questionnaire.
Summary statistics, including frequency, percentage, median, and interquartile range, were utilized to summarize the characteristics of patients and other relevant information. This research aimed to assess the relationship between the independent variables and two primary outcomes: (i) the level of patient satisfaction and (ii) the length of stay in the HBIC. The binary logistic regression (Backwald) model was employed to examine the independent variables associated with patient satisfaction, and the findings were presented as odds ratios (OR). Cox regression (Backwald) analysis was conducted to evaluate the independent variables linked to the length of stay in HBIC, and the results were reported as hazard ratios (HR). To compare the means of length of stay in HBIC, a non-normal distribution, the Mann–Whitney U test for independent samples was employed, while the chi-square test was used for categorical variables. The significance level was set at p < 0.05. All statistical analyses were performed using SPSS, version 26.
The study was conducted after obtaining ethical clearance from the Addis Ababa Health Bureau Public Health Research and Emergency Ethical Review Committee. Oral informed consent was obtained from the participants before any form of data collection. Participants’ contact information was obtained after a formal request was made to the Addis Ababa Health Bureau. Demographic data of all participants and survey responses were anonymously collected and entered. Access to the collected information was limited to the authors, and confidentiality was maintained throughout the project.
A 17-question structured questionnaire was developed by reviewing similar studies (Table 1) (13). Upon completing a reliability assessment of the survey, the internal reliability of the survey was robust, as evidenced by a Cronbach’s alpha coefficient of 0.96 (data not shown). The study included 509 patients, yielding a response rate of 87.2% (n = 444). Among the non-respondents (n = 65, 12.8%), the reasons provided for their lack of participation were as follows: 20% (n = 13) had incorrect contact information, and another 20% (n = 13) did not receive any follow-up, either in-person or through phone communication. The remaining 60% (n = 39) of participants displayed uncooperative behavior, as their phones were inactive, unreachable, or did not answer (Figure 3).
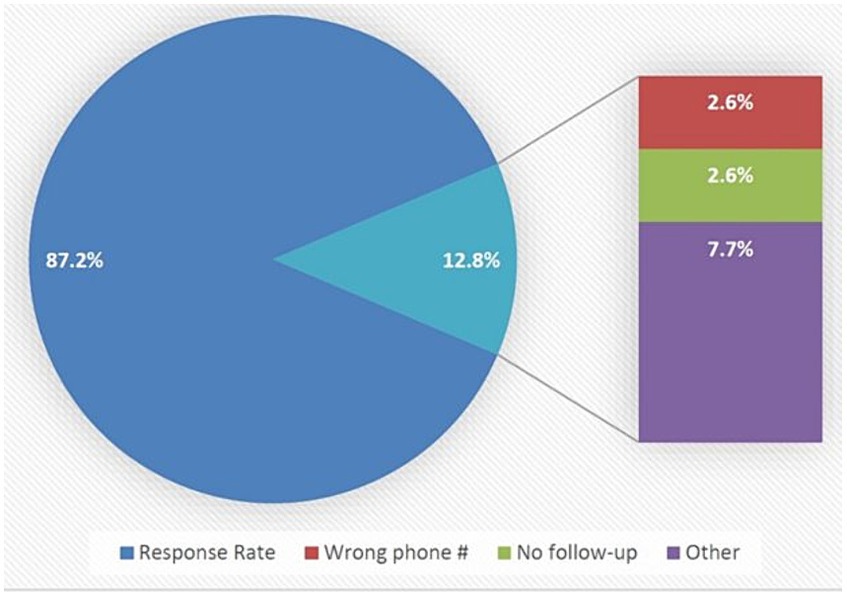
Figure 3. Patient’s response from telephone calls. Response rate and reasons for non-response include: (i) wrong phone number, (ii) no follow-up, and (iii) other.
The descriptive statistics of the 444 patients who participated in the study are below. The median age was 34 ± 15 years, with an age distribution as follows: Age:<30 (n = 164, 36.9%); 31–40 (n = 141, 31.8%); 41–50 (n = 87, 19.6%); and 51–60 (n = 52, 11.7%). The gender distribution of the patients was as follows: Female 247 (55.6%) (Table 2). We outline the performance of the HBIC system according to the patient satisfaction parameter. Due to the low frequency obtained in the lower user satisfaction groups (very low, low, and moderate), we grouped patients into two major groups according to the degree of user satisfaction: low or moderate and high or very high. patients with high or very high user satisfaction represent 313 (70.5%). When we break down this group by gender, we see that women have a slightly higher percentage of high or very high user satisfaction than men, with 177 (56.9%) females. However, no statistically significant differences are observed. Analyzing the distribution of patients with high and very high user satisfaction by age, we observe that more than 50% of patients are concentrated in a population under 40 years old (Table 2). The length of stay for patients with high or very high satisfaction varied depending on certain variables. The average length of stay for females was 15 ± 5 days, while for males, it was 16 ± 5 days, and in terms of age groups, patients showed similar lengths between 14 and 16 days (Table 2).
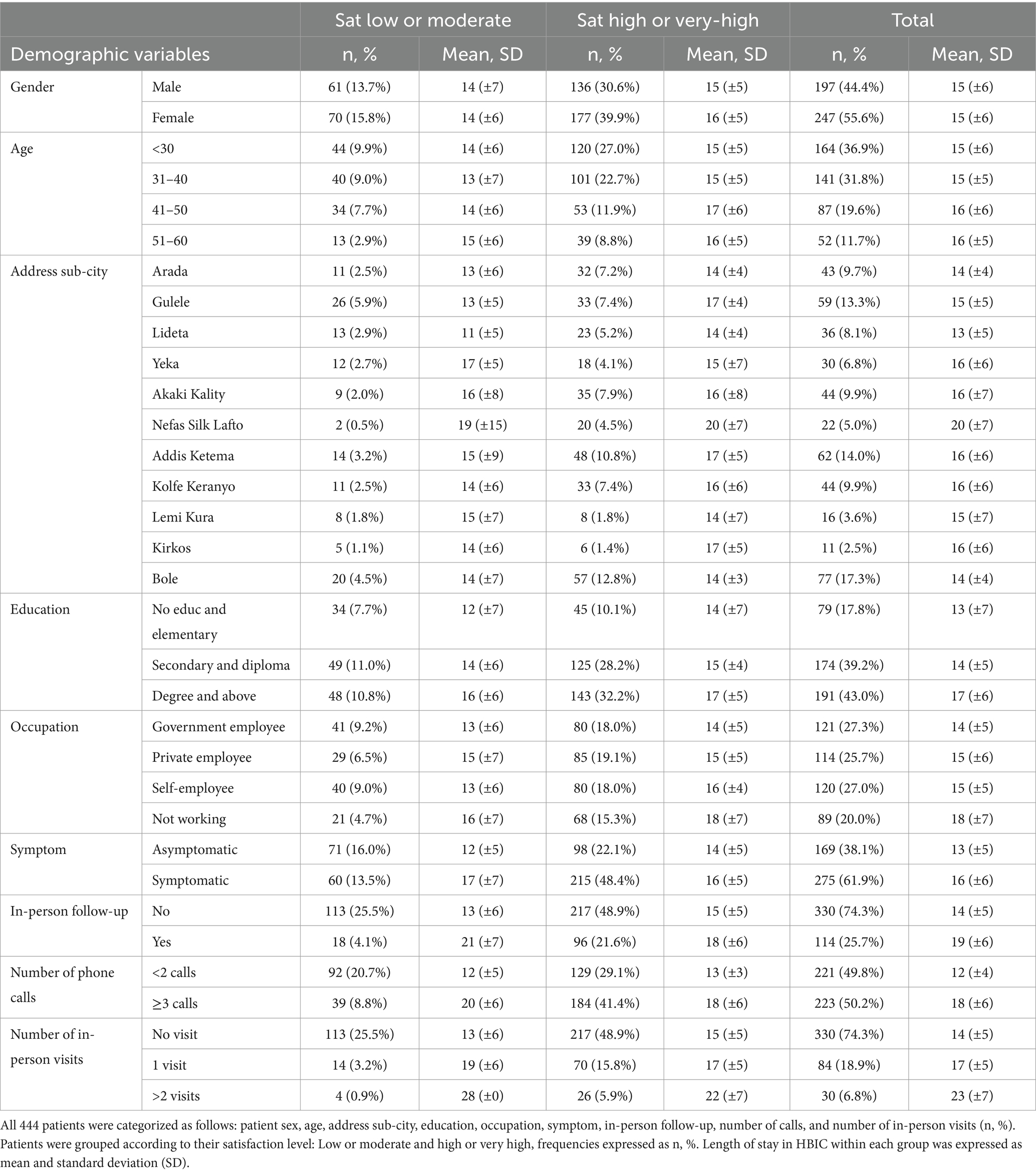
Table 2. Patient’s demographic variables.
The distribution of patients according to sub-city of residence was found to be quite homogeneous, with some exceptions as detailed below: City: Addis Ketema (n = 62, 14.0%), Akaki Kality (n = 44, 9.9%), Arada (n = 43, 9.7%), Bole (n = 77, 17.3%), Gulele (n = 59, 13.3%), Kirkos (n = 11, 2.5%), Kolfe Keranyo (n = 44, 9.9%), Lideta (n = 36, 8.1%), Nefas Silk Lafto (n = 22, 5.0%), Yeka (n = 30, 6.8%), and Lemi Kura (n = 16, 3.6%). Patients with high or very high satisfaction were distributed according to sub-city of residence as follows: City: Addis Ketema (n = 48, 10.8%), Akaki Kality (n = 35), Arada (n = 32, 7.2%), Bole (n = 57, 12.8%), Gulele (n = 33, 7.4%, 7.9%), Kirkos (n = 6, 1.4%), Kolfe Keranyo (n = 33, 7.4%), Lideta (n = 23, 5.2%), Nefas Silk Lafto (n = 20, 4.5%), Yeka (n = 18, 4.1%), and Lemi Kura (n = 8, 1.8%) (Table 2). Regarding the city of origin, the average length of stay varied as follows: Addis Ketema (17 ± 5), Akaki Kality (16 ± 8), Arada (16 ± 5), Bole (14 ± 3), Gulele (17 ± 4), Kirkos (17 ± 5), Kolfe Keranyo (16 ± 6), Lideta (14 ± 4), Nefas Silk Lafto (20 ± 7), Yeka (15 ± 7), and Lemi Kura (14 ± 7) (Table 2).
The patient’s satisfaction and length of stay in HBIC can be influenced by various factors, including the patient’s level of education and occupation. The distribution of patients’ education level is as follows: 79 patients (17.8%) had no education or only completed elementary school, 174 patients (39.2%) had completed secondary school or obtained a diploma, and 191 patients (43.0%) had a degree or higher education. The distribution of patients’ occupation is as follows: 121 patients (27.3%) were government employees, 114 patients (25.7%) were private employees, 120 patients (25.0%) were self-employed, and 89 patients (20.0%) were not working (Table 2). The majority of patients who showed high or very high user satisfaction have higher levels of education: Education: No Educ and Elementary (n = 45, 10.1%), Secondary and Diploma (n = 125, 28.2%), Degree and above (n = 143, 32.2%); however, the distribution was found to be more symmetrical according to the occupational level of these patients: Government employee (n = 80, 18.0%), Private employee (n = 85, 19.1%), Self-employee (n = 80, 18.1%), Not working (n = 68, 15.3%) (Table 2). No significant differences were found in the duration length of stay in HBIC among patients concerning their level of education and occupation type. The respective data for education are as follows: No Education and Elementary 14 ± 7, Secondary and Diploma 15 ± 4, Degree and above 17 ± 5. Similarly, the data for occupation type were: Government employee 14 ± 5, Private employee 15 ± 5, Self-employee 16 ± 4, Not working 18 ± 7 (Table 2).
Most patients who participated in this study were symptomatic, accounting for 275 (61.9%) with an average length of stay for HBIC of 16 (±6). Patients who displayed symptoms were more satisfied (n = 215, 48.5%) than those who were asymptomatic (n = 98, 22.1%). The length of stay in HBIC for asymptomatic patients (14 ± 5), was slightly lower than that of Symptomatic patients (16 ± 5). However, no statistically significant differences were observed (data not shown).
Next, we described the frequency of phone call follow-ups for patients during their stay at HBIC. The most common type of care was TC, with 330 patients (74.3%), followed by in-person and TC visits, with 114 patients (25.7%). The overall frequency of in-person visits was 1 ± 2 visits, and it can be further broken down as follows: no visits (n = 330, 48.9%), ≤2 visits (n = 84, 18.9%), and ≥ 3 visits (n = 30, 6.8%). The average frequency of phone call follow-ups was 3 ± 6 calls, and we observe that the distribution of calls appears to be symmetrical: TC was ≤2 calls (n = 221, 49.8%) and ≥ 3 calls (n = 223, 50.2%).
In terms of the mode of care, patients who were exclusively contacted through teleconsultation (TC) 217 (48.9%) were more satisfied than those receiving hybrid care with both TC and in-person visits 96 (21.6%). Consistent with the findings, patients exhibited higher user satisfaction with an increased frequency of calls in TC, as those patients with more than ≥3 calls (n = 184, 41.4%) expressed greater satisfaction compared to patients with less than or equal to ≤2 calls (n = 129, 29.1%) (Table 2). Upon analyzing the frequency of in-person visits, patients with fewer visits reported higher user satisfaction: No visits (n = 217, 69.3%), 1 visit (n = 70, 22.0%), and ≥ 2 visits (n = 26, 8.3%).
It is important to mention that differences in patient length of stay were observed according to the type of care, as patients treated through the TC system 14 ± 5 stayed for a shorter period than those receiving hybrid care through TC and in-person visits 18 ± 6 (p < 0.05). As expected, patients with more calls stayed longer in the HBIC system as described below: Frequency of calls in TC: ≤2 calls 13 ± 3, and ≥ 3 calls 18 ± 6 (p < 0.05) (Table 2).
A binary logistic regression analysis was utilized to explore the variables associated with high or very high patient satisfaction levels. The results revealed that individuals who placed more than three calls (OR = 2.827, 95% CI = 1.798, 4.443, p = 0.000) and those displaying symptoms (OR = 2.001, 95% CI = 1.289, 3.106, p = 0.002) were more inclined to report increased satisfaction. Nevertheless, no statistically significant relationships were found between user satisfaction and the other independent variables investigated (p > 0.05) (Table 3).
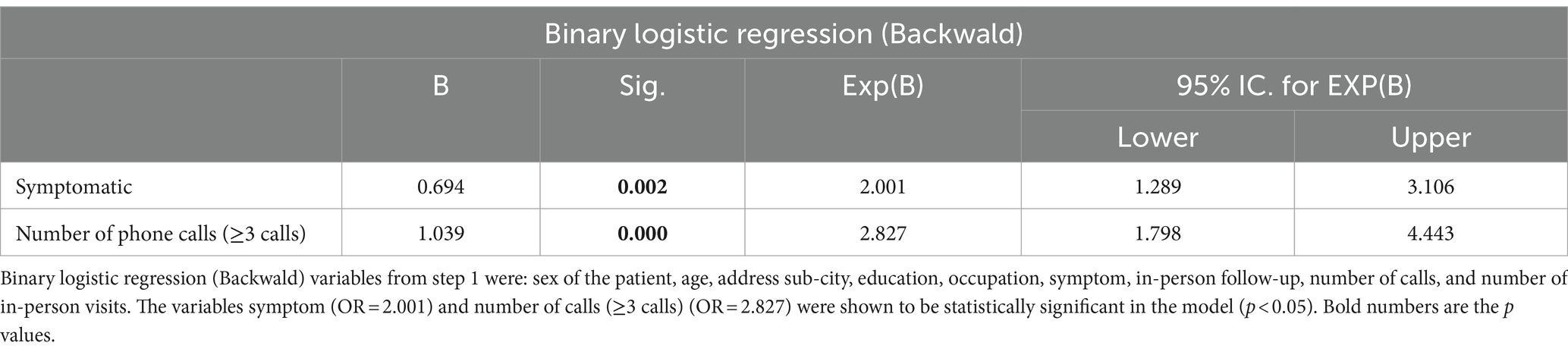
Table 3. Relevant demographic variables that influence patient satisfaction.
A Cox regression analysis was employed to examine the factors influencing the duration of hospital stays in patients who reported high levels of satisfaction. The findings revealed that patients who made more than three phone calls had a significantly lower hazard ratio (HR = 0.537, 95% CI = 0.415, 0.696, p = 0.000), indicating a greater likelihood of reducing their length of stay. Similarly, patients with more in-person visits also exhibited a lower hazard ratio (HR = 0.495, 95% CI = 0.322, 0.762, p = 0.001). However, no statistically significant associations were observed between the length of stay and the other independent variables analyzed (p > 0.05) (Table 4).
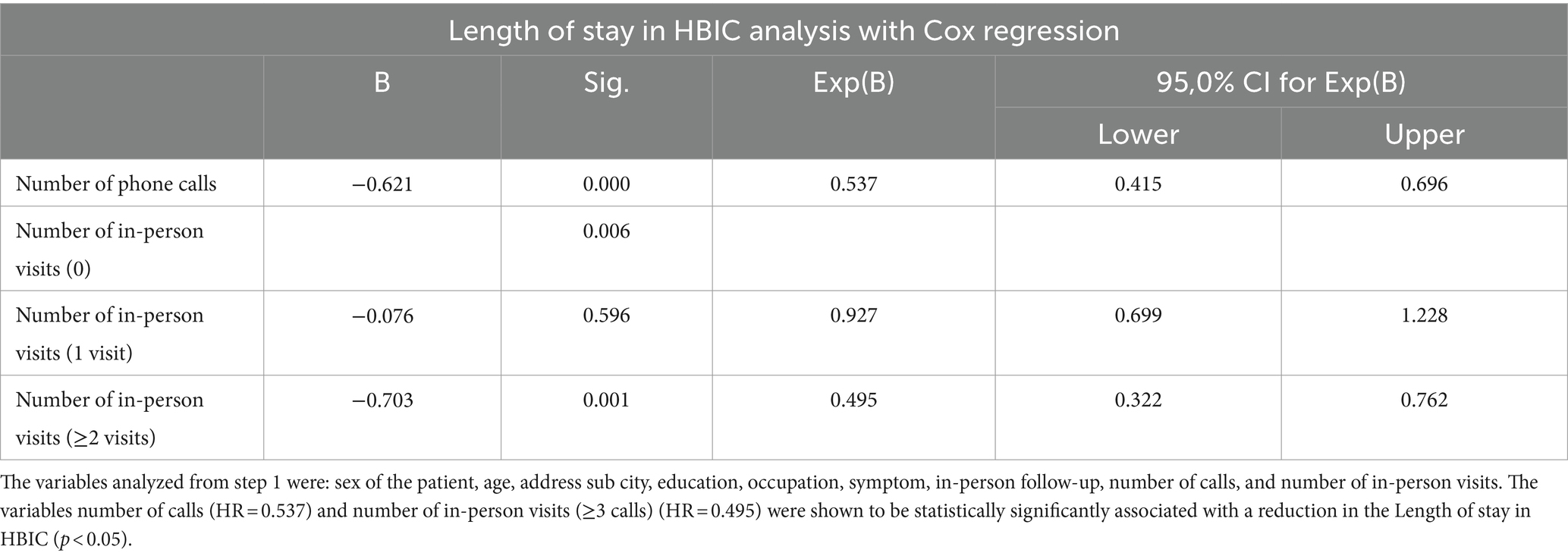
Table 4. Cox regression analysis to elucidate the demographic variables associated with the length of stay in HBIC and patients’ satisfaction.
Previously, we identified the following variables that significantly influence patient satisfaction and length of stay in HBIC: the presence of symptoms, the number of phone calls, and in-person follow-ups. Subsequently, we examined the relationship between symptoms and patient satisfaction with the number of phone calls and in-person follow-ups (Table 5). It was noted that symptomatic patients with low or moderate satisfaction levels have an OR = 5.7 times higher likelihood of having a greater number of phone calls and 7.6 times higher likelihood of having in-person follow-ups. The length of stay in HBIC for these patients was notably longer for those with a higher number of phone calls. Conversely, patients with high or very high satisfaction levels have a 2.3 times higher likelihood of having a greater number of phone calls and in-person follow-ups. The length of stay in HBIC for these patients was significantly longer for those with in-person follow-up. Sig p < 0.05 (Table 5).
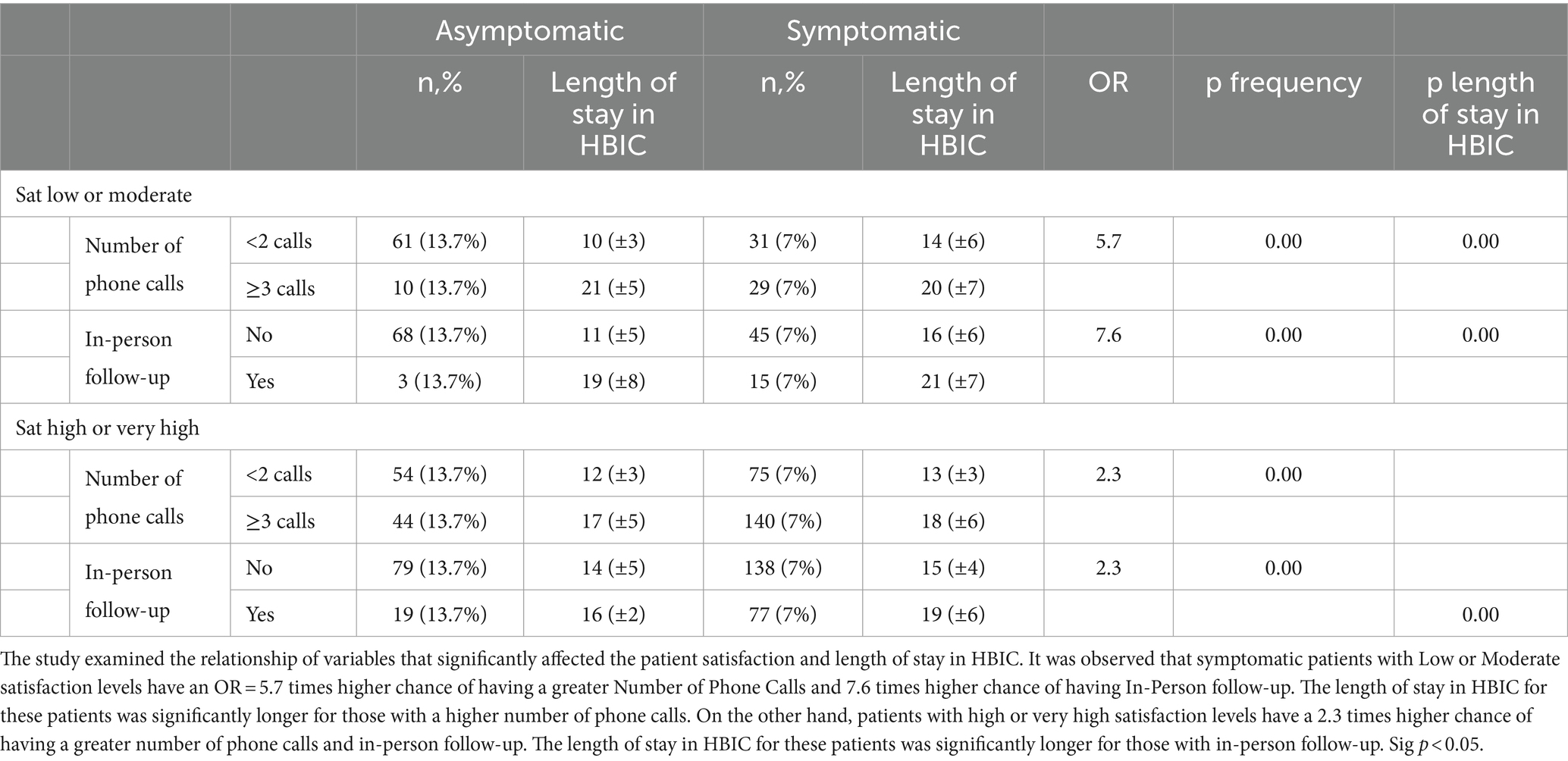
Table 5. Analysis of the variables affecting patient satisfaction and length of stay in HBIC.
This study aimed to evaluate the levels of patient satisfaction and length of stay in HBIC among COVID-19 patients while also examining the different factors that may impact these outcomes. Given the considerable number of COVID-19-positive instances and the limited bed availability at COVID-19-specific hospitals, the HBIC endorsed the practice of home isolation for COVID-19-affected persons. This directive was instituted because most COVID-19 patients were either asymptomatic or displayed mild symptoms. Such cases generally do not necessitate hospitalization at COVID-19-designated medical facilities and can be adequately managed at home with appropriate medical guidance and monitoring. The heightened level of patient satisfaction observed in symptomatic individuals treated by HBIC is supported by an associated investigation conducted through a survey-based study (10, 16–18).
We identified a noteworthy connection between a high or very high satisfaction level and the frequency of phone call follow-ups in patients with COVID-19 symptoms. Essentially, for each increment of one in the frequency of phone call follow-ups, the chances of experiencing high or very high patient satisfaction rose by a factor of 2.8 (OR = 2.827, 95% CI = 1.798, 4.443, p = 0.000). This tendency may be attributed to patients encountering difficulties during their healthcare facility stay, and regular communication with the follow-up team assists in addressing some of these challenges. As per the National HBIC Guideline, the frequency of phone call follow-ups escalates as the severity of the COVID-19 illness worsens, with follow-ups occurring once a week, every 3 days until discharge, and daily until discharge (19). Correspondingly, individuals exhibiting COVID-19 symptoms had 2.0 times greater odds of experiencing high or very high patient satisfaction than those with asymptomatic disease (OR = 2.001, 95% CI = 1.289, 3.106, p = 0.002). Cox regression analysis uncovered a negative correlation between the length of stay in HBIC patients with high or very high satisfaction and the frequency of phone calls, follow-ups, and in-person visits. Specifically, the number of phone calls and in-person visits (with a minimum of two visits) emerged as significant factors impacting the length of stay. Upon adjusting for other variables, it was observed that with each additional phone call, the length of stay in the hospital-based isolation center (HBIC) decreased by 46.3% (HR = 0.537, 95% CI = 0.415, 0.696, p = 0.000). Similarly, after accounting for other covariates, the length of stay among COVID-19 patients who had more than one in-person visit was 50.5% lower compared to patients with no in-person visits (HR = 0.495, 95% CI = 0.322, 0.762, p = 0.001). Finally, this investigation determined that symptomatic patients with Low or Moderate satisfaction had a greater likelihood of experiencing a larger Number of Phone Calls, In-Person follow-ups, and a longer stay at HBIC compared to patients with high or very high satisfaction.
User satisfaction and length of stay have shown dissimilar results in different latitudes. A study conducted in general and university hospitals in the Netherlands found no evidence of a correlation between the average length of stay in hospital wards and patient satisfaction (20). Several studies conducted at the Nancy University Hospital Center in France and in training hospitals in Turkey and Japan (21–23) have found a connection between prolonged lengths of stay and decreased patient satisfaction. These studies have highlighted the importance of environmental factors in influencing patient satisfaction (24). However, a distinct study carried out in teaching hospitals in Turkey discovered that patients who stayed longer expressed higher satisfaction levels than those with shorter stays (25). Despite these variations, one can speculate about the reasons for higher user satisfaction in patients with greater follow-ups. Among these reasons, it can be argued that it is well-documented that telemedicine technology has the potential to enhance the quality of primary medical care, shorten the duration of treatment, and decrease the number of severe hospitalization cases (17). Telemedicine expands the availability of medical services and broadens the range of medical care, which is particularly crucial in Ethiopia, with a fragmented healthcare system and limited coverage (26, 27). The sharing of medical resources is especially significant for rural or isolated areas, and telemedicine offers a greater abundance of advanced medical resources for primary hospital consultations in these vast rural regions, thereby enhancing the quality of medical and healthcare services (10, 28, 29).
The incorporation of telemedicine into the healthcare systems of low-and middle-income countries (LMICs), such as Ethiopia, has the potential to bring about cost savings and resource conservation in the long run. Consequently, this could alleviate the financial burden on individuals and enhance their access to affordable healthcare services (17). It is important to note that in many LMICs, a significant portion of overall health spending comes from out-of-pocket payments, as there is often no general health insurance available (30). Moreover, the COVID-19 pandemic has further strained the already fragile healthcare systems in LMICs (10, 31). In this regard, telemedicine services could be crucial in relieving pressure on the healthcare system by saving time and resources and enhancing efficiency and accessibility. Additionally, telemedicine can facilitate social distancing measures and reduce the need for face-to-face interactions in hospitals and clinics, helping prevent the spread of infectious diseases like COVID-19 through physical contact (10, 32). Furthermore, telemedicine can also be instrumental in providing counseling and specific advice to patients during the COVID-19 pandemic, such as guidance on prevention measures. Overall, the adoption of telemedicine in LMICs holds great potential for addressing healthcare challenges, reducing costs, and improving access to quality care. It can serve as a valuable tool in mitigating the impact of the COVID-19 pandemic and strengthening healthcare systems in these countries (33).
Throughout the initial three waves of the COVID-19 pandemic in Ethiopia, most patients seeking medical care were directed to the HBIC. This strategic decision is believed to have effectively alleviated the potential burden of cases and prevented burnout among the existing treatment facilities (2). The HBIC specifically caters to COVID-19 patients and represents our country’s pioneering national telehealth service. Therefore, it is crucial to examine its operational experiences thoroughly. The focus should be on integrating functionalities that encourage community acceptance of this telehealth modality. As COVID-19 patients continue to be enrolled in the HBIC, the findings from this study will serve as a valuable resource for the Ministry of Health and COVID-19 response teams in their efforts to enhance the healthcare system. The HBIC framework offers a practical solution for healthcare providers who aim to extend their services to patients residing in remote areas. Moreover, the growing acceptance and familiarity with telemedicine visits, driven by the pandemic, are likely to shape the future landscape of healthcare delivery for both patients and providers.
The study’s findings should be evaluated considering the strengths and limitations identified. The study’s strength lies in the thorough selection process of participants from various sub-cities throughout the entire duration of the service. The research questions were also carefully developed using a validated tool and assessed for internal consistency, ensuring their comprehensibility.
It is important to acknowledge a limitation of the study, which is the potential recall bias introduced by enrolling most patients during the initial phase of the COVID-19 pandemic. Despite this limitation, this study is expected to pave the way for advancements in telemedical services in Ethiopia. Furthermore, it can potentially expand and incorporate other telemedicine care modalities, such as videoconferencing, in the future.
The investigation evaluated patient satisfaction and length of stay in telemedicine services. The findings revealed that most patients, accounting for over 70.5%, reported high or very high satisfaction with these services. Notably, patients who received frequent follow-up phone calls and exhibited symptomatic COVID-19 disease expressed higher satisfaction. Additionally, it was observed that a higher frequency of phone calls and in-person visits resulted in a shorter stay in the Hospital-Based Isolation Center (HBIC). Consequently, it is crucial to consider the aforementioned factors to enhance patient satisfaction and reduce the length of stay in HBIC or other telemedicine services. It is worth mentioning that the HBIC, which caters specifically to COVID-19 patients, represents the first large-scale national telemedicine service implemented in our country. Therefore, it is imperative to thoroughly examine the experiences gained from this service, with particular attention given to incorporating features that facilitate community acceptance and reimbursement of this mode of healthcare delivery. Meanwhile, as the enrollment of COVID-19 patients in the HBIC continues, the findings of this study will serve as a valuable resource for guiding the Ministry of Health, the Ethiopian Public Health Institute, and the COVID-19 response team in their efforts to improve the system.
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding authors.
The studies involving humans were approved by the Addis Ababa Health Bureau Public Health Research and Emergency Ethical Review Committee. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
DG: Writing – review & editing, Writing – original draft, Visualization, Validation, Supervision, Software, Resources, Project administration, Methodology, Investigation, Formal analysis, Data curation, Conceptualization. ZA: Writing – review & editing, Writing – original draft, Visualization, Validation, Supervision, Software, Resources, Project administration, Methodology, Investigation, Formal analysis, Data curation, Conceptualization. FC: Writing – review & editing, Writing – original draft, Visualization, Validation, Supervision, Software, Resources, Project administration, Methodology, Investigation, Formal analysis, Data curation, Conceptualization. FB: Writing – review & editing, Writing – original draft, Methodology, Investigation, Formal analysis, Data curation, Conceptualization. YT: Writing – review & editing, Writing – original draft, Resources, Project administration, Methodology, Investigation, Formal analysis, Data curation, Conceptualization. CM: Writing – review & editing, Writing – original draft, Supervision, Resources, Methodology, Investigation, Formal analysis, Data curation. JR: Writing – review & editing, Writing – original draft, Validation, Project administration, Methodology, Investigation, Formal analysis, Data curation. CA-L: Writing – review & editing, Writing – original draft, Visualization, Validation, Supervision, Software, Resources, Project administration, Methodology, Investigation, Formal analysis, Data curation, Conceptualization.
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
We offer our deepest gratitude to Tigist Workneh and Diribsa Tsegaye from Gamby Medical and Business College. We want to thank all the research participants and data collectors. We are very grateful for the support of the Biomedical Research Support Unit at Hospital Las Higueras (HHT), especially to the staff members Lorena, Karin, Jeannette, and Yosselyn.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2024.1384078/full#supplementary-material
1. World Health Organization . WHO coronavirus (COVID-19) dashboard | WHO coronavirus (COVID-19) dashboard with vaccination data. (2023). Available at: https://covid19.who.int/
2. Ethiopian Public Health Institute . National implementation guide for COVID-19 home-based isolation and care [internet] Addis Ababa (2023) Available at: https://ephi.gov.et/images/novel_coronavirus/EPHI_PHEOC_COVID-19_Confirmed_Case_Home_Based_Isolation_and_Care_Guide_English.pdf.
3. Adebayo, PB, Jusabani, A, Mukhtar, M, and Zehri, AA. The changing trend of teleconsultations during COVID-19 era at a tertiary facility in Tanzania. Pan Afr Med J. (2020) 35:125. doi: 10.11604/pamj.supp.2020.35.2.24977
4. Kamulegeya, LH, Bwanika, JM, Musinguzi, D, and Bakibinga, P. Continuity of health service delivery during the covid-19 pandemic: the role of digital health technologies in Uganda. Pan Afr Med J. (2020) 35:1–3. doi: 10.11604/pamj.supp.2020.35.2.23115
5. Armand, K, Gaël, A, Marcien, N, Wilson, N, Reine, M, and Claude, N. Telemedicine and COVID-19: experience of medical doctors in Cameroon. Am J Heal Med Nurs Pract. (2021) 6:32–7. doi: 10.47672/ajhmn.666
6. Wan, S, Chen, Y, Xiao, Y, Zhao, Q, Li, M, and Wu, S. Spatial analysis and evaluation of medical resource allocation in China based on geographic big data. BMC Health Serv Res. (2021) 21:1–18. doi: 10.1186/s12913-021-07119-3
7. Constanzo, FM, Aracena-Sherck, P, Peña, L, Marrugo, M, Gonzalez, J, Vergara, G, et al. Characterization of the Teleneurology patients at the hospital Las Higueras de Talcahuano-Chile. Front Neurol. (2020) 11:1438. doi: 10.3389/fneur.2020.595577
8. Constanzo, F, Aracena-Sherck, P, Hidalgo, JP, Peña, L, Marrugo, M, Gonzalez, J, et al. Contribution of a synchronic teleneurology program to decrease the patient number waiting for a first consultation and their waiting time in Chile. BMC Med Inform Decis Mak. (2020) 20:20. doi: 10.1186/s12911-020-1034-2
9. Scudeller, PG, Pereira, AJ, Cerri, GG, Jatene, FB, Bego, M, Amaral, TF, et al. Telemedicine in Brazil: teleconsultations at the largest University Hospital in the Country. Telemed Rep. (2023) 4:193–203. doi: 10.1089/tmr.2023.0012
10. Constanzo, F, Benavides, L, Garcés, J, Villalobos, R, Marrugo, M, Kuzmanic, K, et al. Changes in Televisit modalities due to the COVID-pandemic in Chile: a comparison of patient satisfaction. Cureus. (2024) 16:1–12. doi: 10.7759/cureus.55078
11. Paganoni, S, van de Rijn, M, Drake, K, Burke, K, Doyle, M, Ellrodt, AS, et al. Adjusted cost analysis of video televisits for the care of people with amyotrophic lateral sclerosis. Muscle Nerve. (2019) 60:147–54. doi: 10.1002/mus.26606
12. Centro Nacional de Sistemas de Salud (CENS) . Telemedicina durante la epidemia de COVID-19 en Chile: Guía de Buenas Prácticas y Recomendaciones. (2020). Available at: https://cens.cl/guia-de-buenas-practicas-y-recomendaciones-en-telemedicina/
13. Constanzo, F, Aracena-Sherck, P, Hidalgo, JP, Muñoz, M, Vergara, G, and Alvarado, C. Validation of a patient satisfaction survey of the Teleneurology program in Chile. BMC Res Notes. (2019) 12:359. doi: 10.1186/s13104-019-4358-1
14. Nguyen, M, Waller, M, Pandya, A, and Portnoy, J. A review of patient and provider satisfaction with telemedicine. Curr Allergy Asthma Rep. (2020) 20:72. doi: 10.1007/s11882-020-00969-7
15. Kruse, CS, Krowski, N, Rodriguez, B, Tran, L, Vela, J, and Brooks, M. Telehealth and patient satisfaction: a systematic review and narrative analysis. BMJ Open. (2017) 7:e016242. doi: 10.1136/bmjopen-2017-016242
16. Poitras, ME, Poirier, MD, Couturier, Y, T Vaillancourt, V, Cormier, C, Gauthier, G, et al. Chronic conditions patient’s perception of post-COVID-19 pandemic teleconsulting continuation in primary care clinics: a qualitative descriptive study. BMJ Open. (2022) 12:e066871. doi: 10.1136/bmjopen-2022-066871
17. Tiwari, BB, Kulkarni, A, Zhang, H, Khan, MM, and Zhang, DS. Utilization of telehealth services in low- and middle-income countries amid the COVID-19 pandemic: a narrative summary. Glob Health Action. (2023) 16:2179163. doi: 10.1080/16549716.2023.2179163
18. Vosburg, RW, and Robinson, KA. Telemedicine in primary care during the COVID-19 pandemic: provider and patient satisfaction examined. Telemed J. (2022) 28:167–75. doi: 10.1089/tmj.2021.0174
19. Mekonnen, H . COVID-19 in Ethiopia: assessment of how the Ethiopian government has executed administrative actions and managed risk communications and community engagement. Risk Manag Healthc Policy. (2020) 13:2803–10. doi: 10.2147/RMHP.S278234
20. Borghans, I, Kleefstra, SM, Kool, RB, and Westert, GP. Is the length of stay in hospital correlated with patient satisfaction? Int J Qual Heal Care. (2012) 24:443–51. doi: 10.1093/intqhc/mzs037
21. Nguyen Thi, PL, Briançon, S, Empereur, F, and Guillemin, F. Factors determining inpatient satisfaction with care. Soc Sci Med. (2002) 54:493–504. doi: 10.1016/S0277-9536(01)00045-4
22. Sahin, B, Yilmaz, F, and Lee, KH. Factors affecting inpatient satisfaction: structural equation modeling. J Med Syst. (2007) 31:9–16. doi: 10.1007/s10916-006-9038-8
23. Tokunaga, J, and Imanaka, Y. Influence of length of stay on patient satisfaction with hospital care in Japan. Int J Qual Heal Care. (2002) 14:493–502. doi: 10.1093/intqhc/14.6.493
24. Quintana, JM, González, N, Bilbao, A, Aizpuru, F, Escobar, A, Esteban, C, et al. Predictors of patient satisfaction with hospital health care. BMC Health Serv Res. (2006) 6:102. doi: 10.1186/1472-6963-6-102
25. Findik, UY, Unsar, S, and Sut, N. Patient satisfaction with nursing care and its relationship with patient characteristics. Nurs Health Sci. (2010) 12:162–9. doi: 10.1111/j.1442-2018.2009.00511.x
26. Rajkumar, E, Gopi, A, Joshi, A, Thomas, AE, Arunima, NM, Ramya, GS, et al. Applications, benefits and challenges of telehealth in India during COVID-19 pandemic and beyond: a systematic review. BMC Health Serv Res. (2023) 23:7. doi: 10.1186/s12913-022-08970-8
27. Desta, AA, Woldearegay, TW, Gebremeskel, E, Alemayehu, M, Getachew, T, Gebregzabiher, G, et al. Impacts of COVID-19 on essential health services in Tigray, northern Ethiopia: a prepost study. PLoS One. (2021) 16:e0256330. doi: 10.1371/journal.pone.0256330
28. Seto, E, Smith, D, Jacques, M, and Morita, PP. Opportunities and challenges of telehealth in remote communities: case study of the Yukon telehealth system. J Med Internet Res. (2019) 7:e11353. doi: 10.2196/11353
29. Cochrane Effective Practice and Organisation of Care GroupGonçalves-Bradley, DC, J Maria, AR, Ricci-Cabello, I, Villanueva, G, Fønhus, MS, et al. Mobile technologies to support healthcare provider to healthcare provider communication and management of care. Cochrane Database Syst Rev. (2020) 2020:CD012927. doi: 10.1002/14651858.CD012927.pub2,
30. Sallnow, L, Smith, R, Ahmedzai, SH, Bhadelia, A, Chamberlain, C, Cong, Y, et al. Report of the lancet commission on the value of death: bringing death back into life. Lancet. (2023) 399:837–84. doi: 10.1016/S0140-6736(21)02314-X
31. Asante, A, Price, J, Hayen, A, Jan, S, and Wiseman, V. Equity in health care financing in low- and middle-income countries: a systematic review of evidence from studies using benefit and financing incidence analyses. PLoS One. (2016) 11:e0152866. doi: 10.1371/journal.pone.0152866
32. Eslami Jahromi, M, and Ayatollahi, H. Utilization of telehealth to manage the Covid-19 pandemic in low- and middle-income countries: a scoping review. J Am Med Inform Assoc. (2023) 30:738–51. doi: 10.1093/jamia/ocac250
Keywords: patient satisfaction, COVID-19, home care, telehealth, telemedicine, digital health
Citation: Gashaw DG, Alemu ZA, Constanzo F, Belay FT, Tadesse YW, Muñoz C, Rojas JP and Alvarado-Livacic C (2024) COVID-19 patient satisfaction and associated factors in telemedicine and hybrid system. Front. Public Health. 12:1384078. doi: 10.3389/fpubh.2024.1384078
Edited by:
Charles R. Doarn, University of Cincinnati, United StatesReviewed by:
Jordan Coffey, Mayo Clinic, United StatesCopyright © 2024 Gashaw, Alemu, Constanzo, Belay, Tadesse, Muñoz, Rojas and Alvarado-Livacic. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Dagmawit G. Gashaw, Z2V0YWh1bmRhZ21hd2l0QGdtYWlsLmNvbQ==; Freddy Constanzo, dGVsZW5ldXJvbG9naWFoaHRAZ21haWwuY29t
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.