 Naisa Manafe1,2*†
Naisa Manafe1,2*† Hamida Ismael-Mulungo1Fábio Ponda1Palmira F. Dos Santos1
Hamida Ismael-Mulungo1Fábio Ponda1Palmira F. Dos Santos1 Flávio Mandlate3
Flávio Mandlate3 Vasco F. J. Cumbe4Ana Olga Mocumbi1,3
Vasco F. J. Cumbe4Ana Olga Mocumbi1,3 Maria R. Oliveira Martins2
Maria R. Oliveira Martins2- 1Instituto Nacional de Saúde, Maputo, Mozambique
- 2Global Health and Tropical Medicine, Instituto de Higiene e Medicina Tropical, Universidade Nova de Lisboa, Lisbon, Portugal
- 3Faculty of Medicine, Eduardo Mondlane University, Maputo, Mozambique
- 4Mental Health Department, Ministry of Health, Provincial Health Directorate of Sofala, Beira, Mozambique
Background: Humanitarian emergencies are a major global health challenge with the potential to have a profound impact on people’s mental and psychological health. Displacement is a traumatic event that disrupts families and affects physical and psychological health at all ages. A person may endure or witness a traumatic incident, such as being exposed to war, and, as a result, develop post-traumatic stress disorder (PTSD). There is a lack of information about post-traumatic stress disorder, depression, and anxiety disorder in low and middle-income countries in humanitarian emergency contexts such as Mozambique. This study aimed to assess the prevalence of PTSD, depression, and anxiety, and associated factors among armed conflict survivors in Cabo Delgado, north region of Mozambique in 2023.
Methods: A community-based cross-sectional study was conducted between January and April 2023 among 750 participants, who were selected by convenience. A face-to-face interview used the Primary Care Post-Traumatic Stress Disorder Checklist (PC-PTSD-5) to evaluate PTSD, the Generalized Anxiety Disorder Scale (GAD-7) to evaluate anxiety and the Patient Health Questionnaire – Mozambique (PHQ-9 MZ) to evaluate depression. The association between PTSD and demographic and psychosocial characteristics was analyzed using bivariate and multivariable binary logistic regression. We used a 5% significance level.
Results: The three mental disorders assessed were highly prevalent in our sample with 74.3% PTSD, 63.8% depression, and 40.0% anxiety. The chance of developing PTSD was higher in females (AOR = 2.30, 95% CI 1.50–3.51), in patients with depression symptoms (AOR = 8.27, 95% CI = 4.97–13.74) and anxiety symptoms (AOR = 1.45, 95% CI = 0.84–2.50).
Conclusion: This study reported that the prevalence of PTSD, depression, and anxiety were high. Patients having depressive symptoms, anxiety symptoms, and being female are more at risk of developing PTSD. There is a need to integrate screening for common mental disorders in the context of humanitarian emergencies and its adapted integration of psychosocial interventions.
Introduction
Displacement due to armed conflict in developing countries is increasing (1, 2). Displacement is a traumatic event that disrupts families and affects physical and psychological health at all ages (3–5). At least two-thirds of the countries in Africa have experienced conflicts leading to the displacement of millions of people (6).
Epidemiological evidence shows that the burden of mental disorders is becoming higher, particularly in post-conflict and conflict-affected populations (7, 8).
Mental disorders are a significant public health problem and 14% of the total burden of disease has been attributed to neuropsychiatric disorders including depression and other common mental disorders (9). Additionally, the proportion of global Disability Adjusted Life Years (DALYs) attributed to mental disorders increased to 4.9% (3.9–6.1) and Years lived with disability (YLDs) contributed to most of the mental disorder burden, with 125.3 million YLDs (95% UI 93.0–163.2; 14.6% [12.2–16.8] of global YLDs) in 2019 (10). Exposure to repeated trauma and extreme violence such as torture is associated with an increased risk for a mental disorder, including post-traumatic stress disorder, depression, anxiety, schizophrenia, and bipolar disorder (7, 11–13).
Recent meta-analyses of several studies published between1980 and 2017, where estimated the prevalence of PTSD (96/129; 74.4% of the studies), depression (70/129; 54.3% of the studies), and anxiety (38/129; 29.4% of the studies) identified a relationship between exposure to different types of disaster and conflict-related events and mental health disorders including anxiety, depression, and PTSD (7). The prevalence of mental health diseases was 21% (95% CI 18.8–25.7) at the point in time in the conflict-affected populations assessed (7).
According to the results of another meta-analysis, an estimated 242 million adult war survivors living in post-conflict areas were affected by PTSD, while major depressive disorder affected an estimated 238 million and 117 million suffering from both conditions (14). According to the findings of this meta-analysis, the estimated adult war survivors with PTSD, major depression, and both conditions in Mozambique were 2,339,450 (95% CI, 1,919,902–2,785,528), 2,296,218 (95% CI, 1,933,657–2,679,412) and 1,124,917 (95% CI, 695,524–1,557,525), respectively. (14).
According to studies of the general population, PTSD prevalence ranges between 1 and 5% (15, 16), while it has been shown to range from 3 to 58% in high-risk groups, such as those in conflict areas (16). Another systematic review reported that 3 to 88% of people in the general population have PTSD (7, 17). This is the case in Nepal and Palestine where PTSD prevalence is 53.4% (18) and 68.9% (19) respectively. Additionally, cross-sectional studies conducted among Internally Displaced People (IDP) assessment at community revealed that the prevalence of PTSD was 63% in Nigeria (20), 19.3% in Morocco (21), 28% in South Sudan (22), and 58.4% in the north (23) of Ethiopia.
On the other hand, mental health affects the immune system, damaging the body’s immunity and defenses and leaving the individual more susceptible to infections; the endocrine system, increasing or decreasing the production of certain hormones; the nervous system, interfering with the production of neurotoxins (related to diseases such as Parkinson’s and Alzheimer’s disease), among other problems (24).
Mozambique hosts nearly 32,000 refugees and asylum-seekers, while more than one million people remain displaced internally due to violence perpetrated by non-state armed groups and the devastating impact of the climate crisis (Tropical Cyclone Gombe in March 2022) – where Mozambique is one of the most adversely affected countries in the world (25).
In October 2017, violence erupted in Cabo Delgado, northern Mozambique, when armed men occupied the Mocimboa da Praia district. This violence perpetrated by non-state armed groups worsened in 2020 resulting in an unprecedented humanitarian crisis with close to 1 million people living in a situation of protracted displacement (26). Violence against civilians continued such as killing, beating, extortion, widespread damage to property and core public services, severe violations of children’s rights, and conflict-related sexual violence (27). Due to this violence, 2000 civilians died and around 34% of people and 28% of families including 353,601 children, were displaced/forced to move to different locations within Cabo Delgado province and other regions of Mozambique such as Sofala and Zambezia in the center and Nampula and Niassa in the north (28). The main destinations of IDP arrivals in Cabo Delgado were Pemba, Metuge, Mueda, Ancuabe, and Montepuez districts (29, 30), where displaced people were initially housed in transitional accommodation centers and later resettled or returned to their places of origin. The IDPs still live in small, overcrowded temporary shelters in the camps, without sufficient food, clean water, or toilets. Their lives are on hold, and their futures are uncertain (26–29). Individuals with an experience of abuse/violence were at risk of increasing mental health problems.
Screening is effective only when combined with high-quality services for mental well-being.
One of the challenges to ensuring appropriate services for IDP in Cabo Delgado is the lack of statistical data on the group’s mental health status.
Despite the high prevalence of PTSD, depression, and anxiety in conflict areas around the world, data on the prevalence of PTSD, depression, and anxiety among IDPs in Mozambique, where we lived in a scenario of armed conflict (during 16 years of civil war), current terrorist attacks and violence since 2017, and recurring natural disasters are scarce. It is imperative to conduct research in this field to provide scientific support for the formulation of prevention and treatment plans for mental health issues during current and future civilian attacks or natural disasters. This study aims to assess the prevalence of symptoms and associated factors of post-traumatic stress disorder, depression, and anxiety among those who have experienced traumatic events during the armed conflict in Cabo Delgado province.
Materials and methods
Study design, period, and settings
A community-based, cross-sectional study was conducted with Internally Displaced Persons aged 14 years and over between January 2023 and April 2023.
Internally displaced persons (IDPs), according to the United Nations Guiding Principles on Internal Displacement, are “persons or groups of persons who have been forced or obliged to flee or to leave their homes or places of habitual residence, in particular as a result of or to avoid the effects of armed conflict, situations of generalized violence, violations of human rights or natural or human-made disasters, and who have not crossed an internationally recognized state border (31). In this study, an IDP was considered as someone who answered the questionnaire-screening questions that they had been forced to flee their homes because of the armed conflict and currently living in the IDP resettlement center.
Participants were excluded in cases of mental disability at the time of the survey that impeded their ability to competently consent and people who did not want to talk about their traumatic experience.
The present study was conducted in the 25 de Junho resettlement center in Metuge district, Cabo Delgado Province, north of Mozambique. Cabo Delgado’s capital is the city of Pemba, located about 2,600 km north of Maputo, the country’s capital. The province has an area of 82,625 km2 and had, in 2017, a population of 2,333,278 inhabitants. The province of Cabo Delgado is divided into 17 districts and has 5 municipalities: Chiure, Mocimboa da Praia, Montepuez, Mueda, and Pemba (32).
Metuge is the closest city to Pemba (34 km), with 5 primary healthcare serving a population of 91,000 and 119,317 IDPs resettled (30).
Metuge district was selected because (1) was considered a “safe” district at the time of the study and close to Pemba City (trip to and from Pemba City on the same day) (32); (2) after the Pemba district, Metuge is the district with the highest number of IDPs resettled (30); (3) has a type 2 health facility close to the IDP resettlement with health professionals trained in the management of mental disorders (Figure 1).
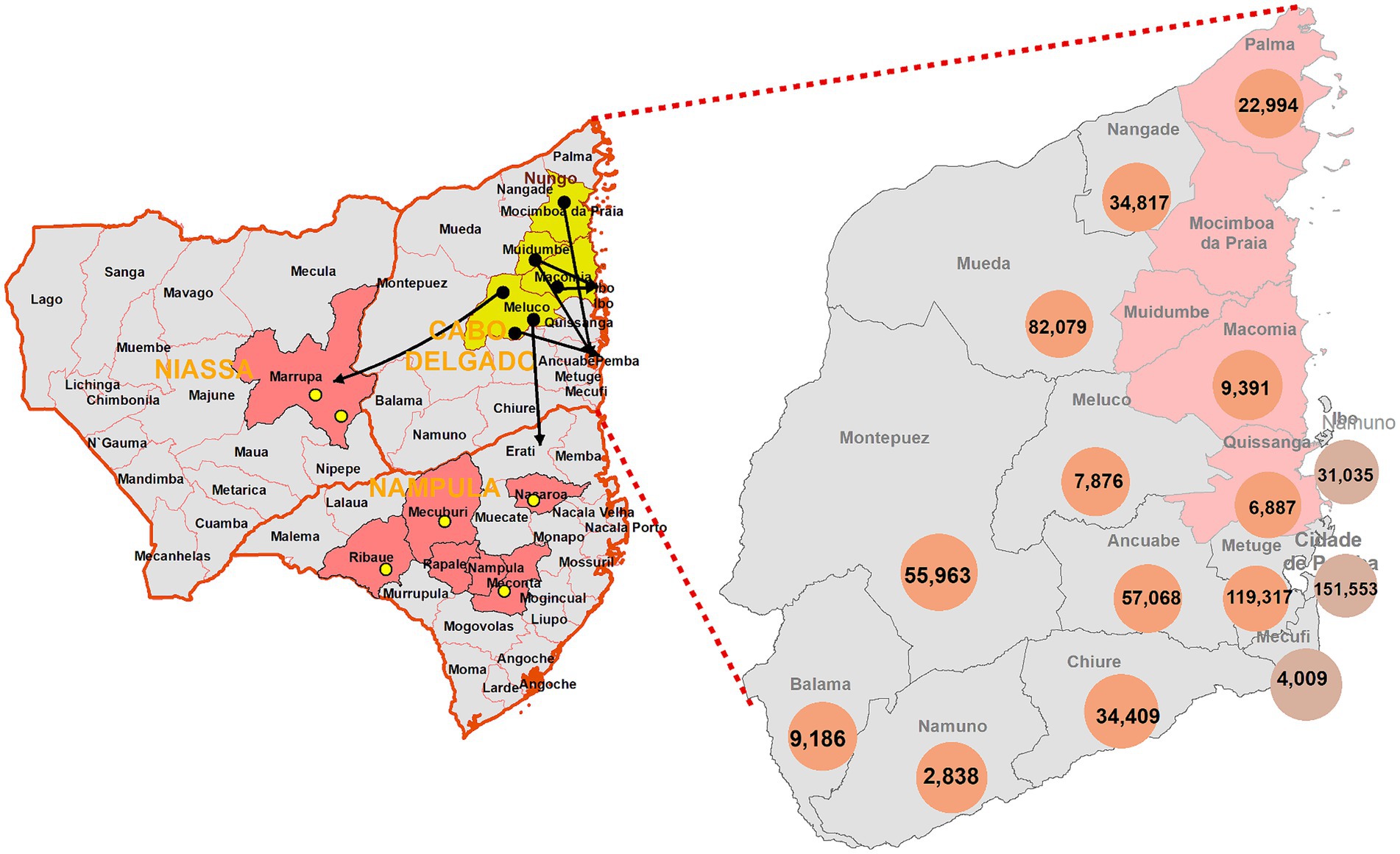
Figure 1. Distribution of internally displaced people in the districts of Cabo Delgado province in March 2021. Source: ADIN, 2020; IOM, 2020, 2021. Available at: https://unhabitat.org/sites/default/files/2021/05/un-habitat_positionpaper_mozambique_pt.pdf.
Study participants and sampling procedure
As the list of all IDPs who are resettled in the selected IDP resettlement was not available, the participants were selected by convenience. There were 7 villages in the reception center (considered as clusters) and the chief of each village was responsible for assisting with recruitment. Based on the time available for the team to be in the field, it was estimated that 50 interviews would be needed per day. So, the aim was to interview around 7–10 participants from each village per day. All houses were contacted by the chief of the village and those who agreed to take part in the study were referred to the project team to be interviewed.
Exposure to war, living in conflict zones, flight, and forced migration may create or increase the risk for broad sequelae of direct and indirect risks for physical and mental health, more so for children and adolescents, even more so for unaccompanied minors separated from their parents; the reason why we included the study participants who were at least 14 years old at the time of data collection. Written informed consent (including the assent term) was obtained from all patients.
Sample size determination
Based on the International Organization for Migration, Displacement Tracking Matrix Mozambique data, the Metuge district had 119,317 IDPs in March 2021 (30, 33). The sample size was calculated based on a confidence interval of 95% and a margin of error (E) of 5%; without general information on the population distributed in IDP camps, or results from the prevalence of PTSD, depression, or anxiety in previous studies, we considered a prevalence of 50%. Considering a 10% non-response rate and a design effect = 1.5 the minimum sample size was equal to 634.
Data collection procedures
From January 2023 to April 2023, three trained data collectors, supervised by the first author (NM), administered a structured questionnaire The face-to-face interview took place 1 person at a time for a maximum of 30 min, to ensure privacy. The respondents were given no monetary or food-item incentives. The questions were read aloud to the respondents 1 question at a time during the interview, and the respondents were asked which of the scale choices was acceptable. The coinvestigators reviewed the data collection sheets for completeness, accuracy, and internal consistency, which the principal investigator confirmed.
The interviews were conducted using tablets and included questions of sociodemographic and displacement characteristics, and screening measures for psychiatric disorders (PTSD, depression, and generalized anxiety).
The first section of the questionnaire assessed sociodemographic characteristics, including age (in years), sex (male or female), marital status [status (never married, widowed or divorced, and married), educational level (none school, primary school, and secondary school), religion (Muslim, Catholic, Protestant)], and provenance as well as psychosocial variables such as chronic medical illness (yes or no), whether family members or friends were killed during the armed conflict (yes or no), frequency of being in an armed conflict (1, 2 or 3 and more), last time were exposed to armed conflict (<12 weeks, 12 weeks to 1 year, and >1 year), missing family member (yes or no) were also recorded. Before administering the questionnaire, each respondent listened to the explanations about the aim of the study and terms of participation. The questionnaire was developed by the authors administered in Portuguese and translated into the local language (dialect) whenever necessary.
The outcome measures were PTSD, depression, and anxiety; these were measured using adapted and validated tools for low-and middle-income countries (LMIC) (34–36) including Mozambique (37–39). The primary care PTSD Screen for DSM-5 (PC-PTSD-5) was used to determine the presence of posttraumatic stress symptoms over the last month (40). It is a 5-item screen designed to identify individuals with probable PTSD in primary care settings in high-income countries (41) and it has been validated for use in LMIC adolescents living with HIV infection in South Africa (36) and Mozambique (37). Each of the five items was rated on a binary scale (0 = No, 1 = Yes) (40). Available data suggest the PC-PTSD-5 screen should be considered “positive” if the respondent answers “yes” to any 3 or more items in the questions (40). A score of = 4 was used as a cut-off for this study (41).
Depression was measured by the Patient Health Questionnaire (PHQ-9) with a recall period of the previous 2 weeks (42). The PHQ-9 is one of the most commonly used depression screening instruments (42, 43) and has been validated for use in adults in numerous community studies in LMIC, including Tanzania (34), South Africa (36), and Mozambique (38).
The PHQ-9 is a multipurpose instrument for screening, diagnosing, monitoring, and measuring the severity of depression. Total scores of 5, 10, 15, and 20 represent cut points for mild, moderate, moderately severe, and severe depression, respectively (42). The following cut-offs correlate with level of depression severity: score 0–4: none or minimal depression; score 5–9: mild depression; score 10–14: moderate depression; score 15–19: moderately severe depression; and score 20–27: severe depression (42). The cut-off score of depression screening was 10 or more in this study according to the results of a tool validation study carried out in Mozambique (37, 38).
Anxiety symptoms were assessed by the GAD-7 scale. The GAD-7 is a commonly used instrument to screen for anxiety in high-income countries (44, 45) that has been validated for use in LMIC adults (36, 42) and adolescents from Mozambique (37, 39). GAD-7 total score for the seven items ranges from 0 to 21 with a recall period of the previous 2 weeks (44). When screening for anxiety disorders, a score of 8 or greater represents a reasonable cut-point for identifying probable cases of generalized anxiety disorder (sensitivity of 92% and specificity of 76%) (44, 45). The following cut-offs correlate with the level of anxiety severity: score 0–4: minimal anxiety; score 5–9: mild anxiety; score 10–14: moderate anxiety and score 15–21: severe anxiety (44). The cut-off score of =10 or more was used as the cut-off for anxiety symptoms in this study (36, 37).
Data analysis
Descriptive statistics, such as percentages, average, median, and standard deviation were used to characterize variables depending on their distribution. We considered three main outcomes (dependent variables): PTSD, anxiety, and depression. The Chi-square or Fisher test was used to assess associations between the main outcomes and the independent variables. To estimate the determinants of PSTD, we calculated crude odds ratio (COR) and adjusted odds ratio (AOR) using logistic regression models.
Variables in the bivariate logistic analysis with a p < 0.2 were included in the multivariable model. We take p < 0.2 as the rule to include variables in the multivariable model as it is the most common rule available in the literature; as such our study will be comparable with others (46, 47).
We considered a 5% significance level. Statistical analysis was conducted using SPSS software version 28.0 (SPSS Inc., Chicago, Illinois, United States).
Results
Sociodemographic characteristics of study respondents
The study included 748 participants of the 750 invited. Of the 748 Metuge IDPs who participated, 487 (65%) were women. The median age of the respondents was 32 (IQ 23–49) years old, with an age range of 14–91 years. More than half of the participants (41.2–55%) were aged between 21 and 44 years old and 521 (69.7%) of the total respondents were married or living with a partner. In terms of occupation, 585 participants (78.2%) were unemployed, 16 were employed (2.1%) and 147 (19.7%) were students.
In addition, 656 of 748 respondents (88%) had a low level of education (35.2–47.1% had a primary school, and 30.4–40.6% did not go to school and could not read or write).
According to the place of provenance, 721 (96.4%) of the IDP participants departed from Quissanga district. In terms of religion, 514 (69%) were Muslim (Table 1).
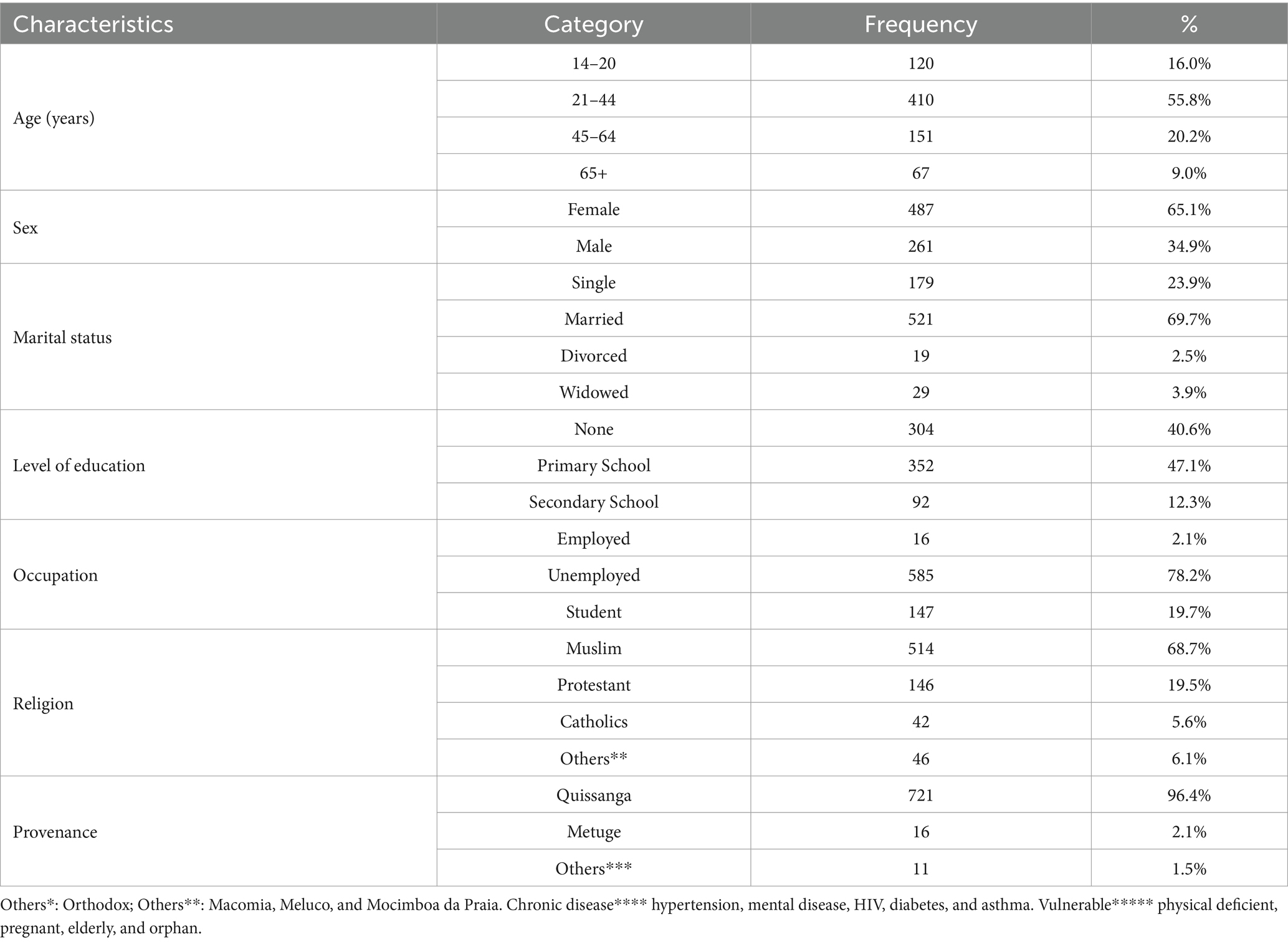
Table 1. Sociodemographic characteristics of study participants from armed conflict area of Metuge district, Cabo Delgado (n = 748).
Potential risk factors for PSTD, depression, and anxiety development
Overall, 114 (15.2%) participants were vulnerable persons (58.8% older adults, 19.2% orphans, 17.5% pregnant, and 4.4% physically deficient). Forty (5.3%) reported the presence of chronic medical illness.
Among the 35 (52.2%) participants with a history of previous mental disorders (anxiety, depression, and epilepsy), 13 (19.4%) reported also having hypertension, 3 (4.5%) HIV infection, 2 (3.0%) diabetes or 2 (3.0%) asthma as self-reported comorbidity.
Regarding trauma exposure, participants reported experiencing a mean of 2.46 trauma events. Approximately 50% (371/748) of IDPs enrolled had been in an attack situation for the third time or more.
About 48% (359/748) of participants lost their family members and 28% (211/748) have witnessed the death of a family member in this war-related event. In terms of the last time that the IDPs were exposed to an attack situation, 65% (484/748) had been in this situation more than 1 year ago (Table 2).
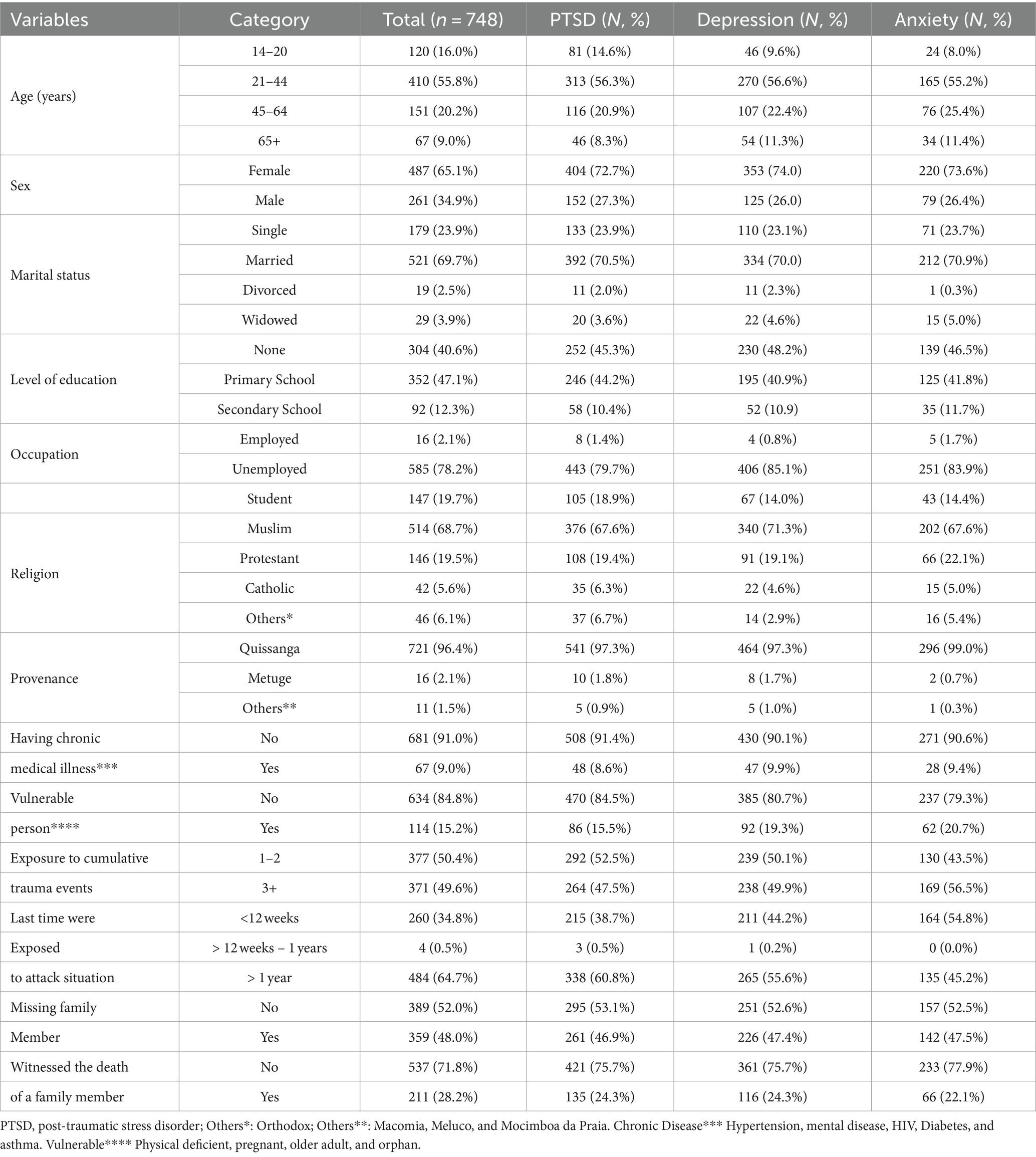
Table 2. Distribution of mental disorders among participants from armed conflict area of Cabo Delgado.
The prevalence of PTSSs was 56.3% (313 of 556) for IDPs aged 21–44 years and 14.6% (81 of 556) for those younger than 21 years.
Among married participants, approximately 70% had PTSSs, depression, and anxiety, while among the never-married (single) respondents (23%).
We found that 252 of the 556 participants who did not have formal education (45.3%) had PTSSs.
Employed IDP participants had a lower prevalence of PTSSs, depression, and anxiety (1–2%) than unemployed IDP participants (80–85%).
Prevalence/frequency of PSTD, depression and anxiety
Of the 748 Metuge IDPs, 556 (74.3%) had post-traumatic stress symptoms (PTSSs) (CI = 71.04–77.42) (27.3% men; 72.7% women). The prevalence of depression was 64% (477 of 748; CI = 60.21–67.22) (26% men; 74% women), and the prevalence of anxiety was 40% (299 of 748; CI 36.44–43.58) (26.4%; 73.6% women). Post-traumatic stress disorder was found in 90.1% (CI 87.11–92.67) and 88.6% (CI 84.47–91.99) of patients with depression, and anxiety symptoms, respectively. The commonest level of depression symptoms was severe (171; 22.9%) followed by moderate depression (163; 21.8%). Nearly one-third of all respondents (224; 29.9%) had moderate anxiety and 75 (10%) had severe anxiety (Table 3).
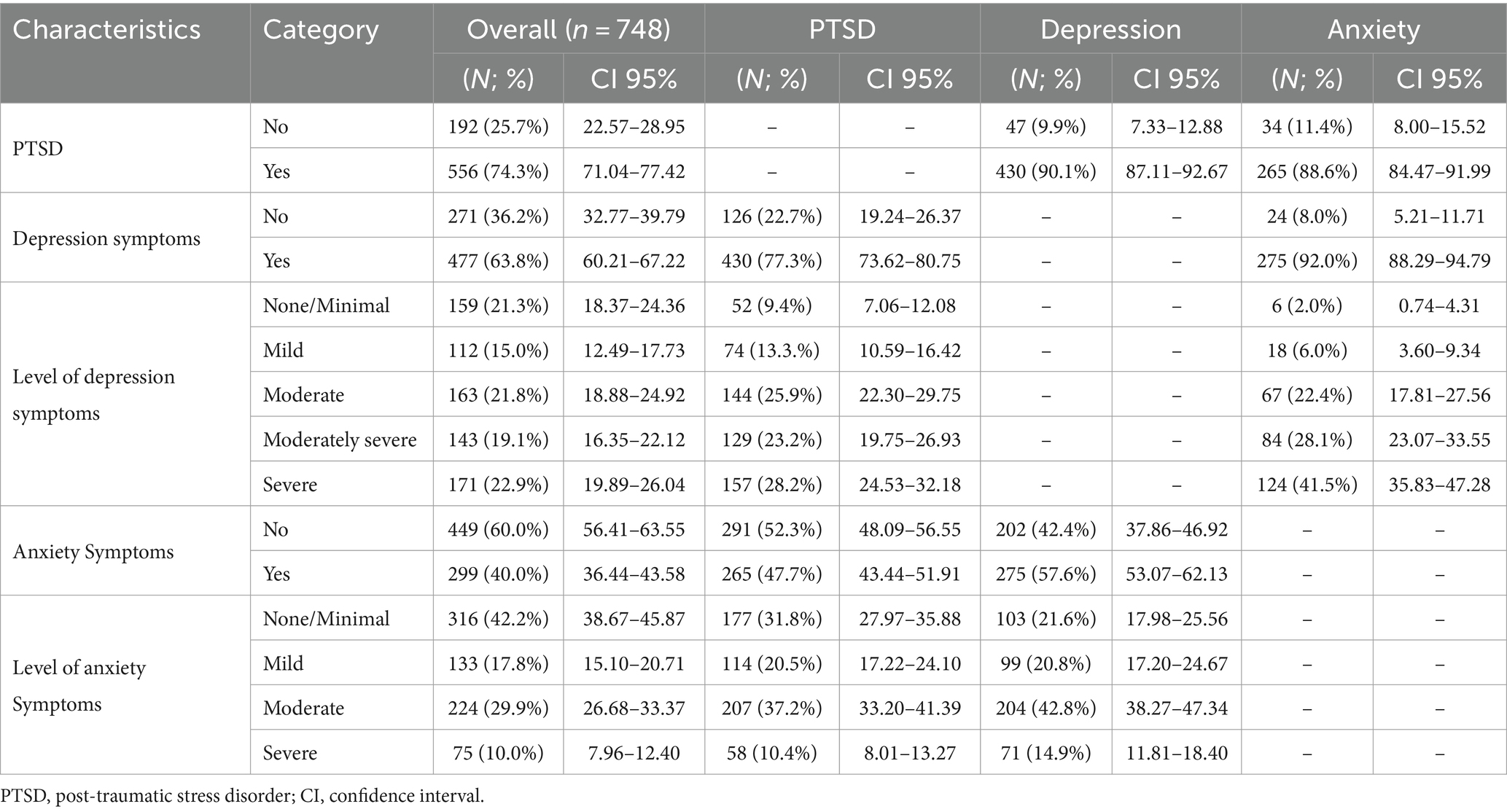
Table 3. Prevalence of post-traumatic stress disorder, depression, and anxiety among the respondents from armed conflict area of Metuge Cabo Delgado, Mozambique.
Proportion of post-traumatic stress among the respondents in war-affected area of Cabo Delgado
Having witnessed the death of a family member, depression, and anxiety symptoms had a statistically higher difference than not having witnessed the death of a family member, without the presence of depression and anxiety symptoms (p < 0.001) to develop PTSSs (Table 4).
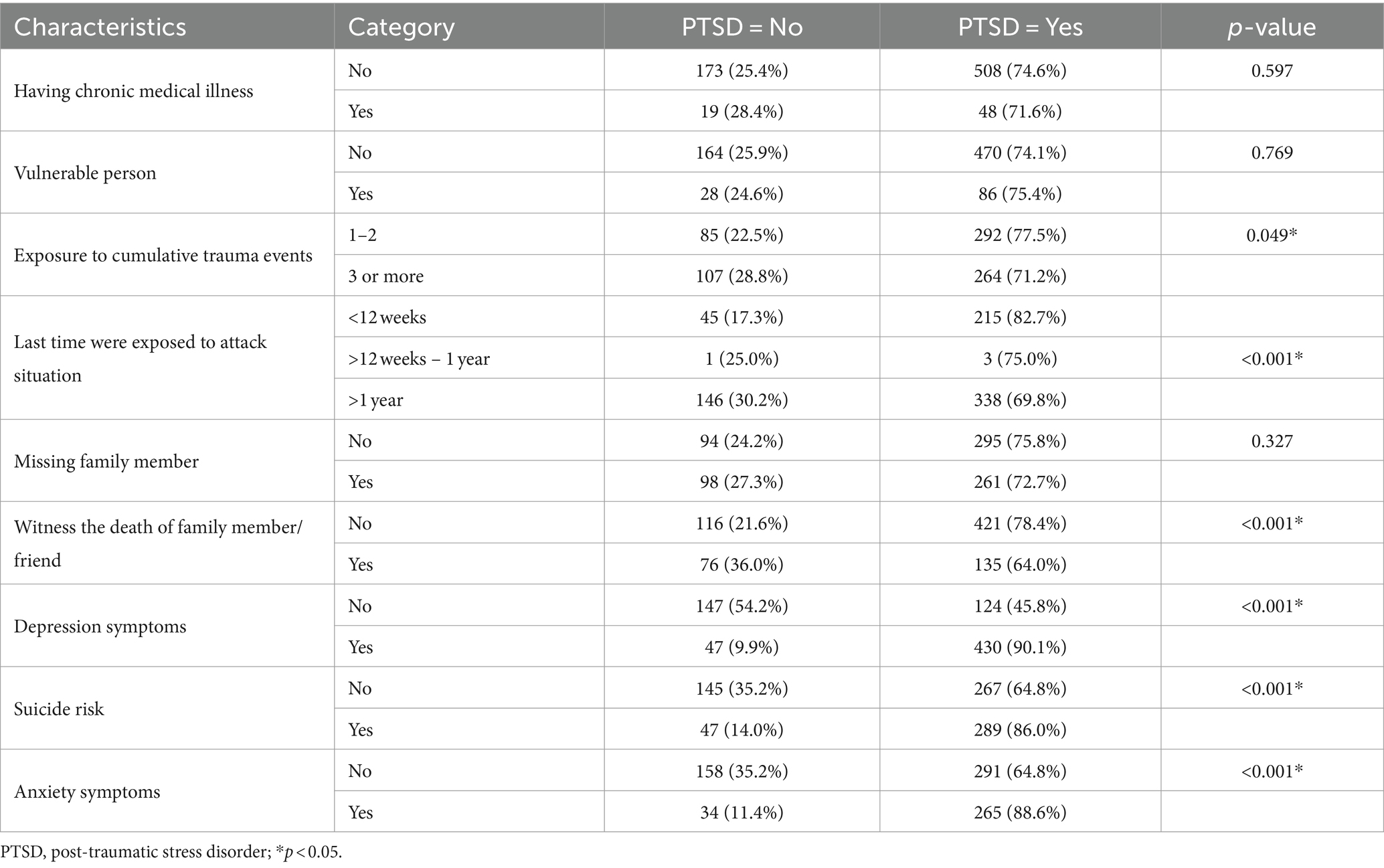
Table 4. Proportion of post-traumatic stress among the respondents from armed conflict area of Metuge, Cabo Delgado, Mozambique.
Post-traumatic stress disorder determinants among the respondents in the war-affected area of Cabo Delgado
The chance of having post-traumatic stress disorder was higher in females, in individuals having a family member or close friend injured or killed, and in those being screened positive for depression and anxiety symptoms.
Females had 2.2 times the odds of developing PTSSs than males (AOR = 2.30, 95% CI 1.50–3.51). The odds of developing PTSD were 4.8 times higher among had been exposed to war between 12 weeks a year compared with had been exposed to war for 11 weeks or less (AOR = 5.14, 95% CI 0.40–65.83). Having depressive symptoms (AOR = 8.27, 95% CI = 4.97–13.74) and anxiety symptoms (AOR = 1.45, 95% CI = 0.84–2.50) and suicide ideation (AOR = 1.54, 95% CI = 0.94–2.51) were significantly associated with post-traumatic stress disorder (Table 5).
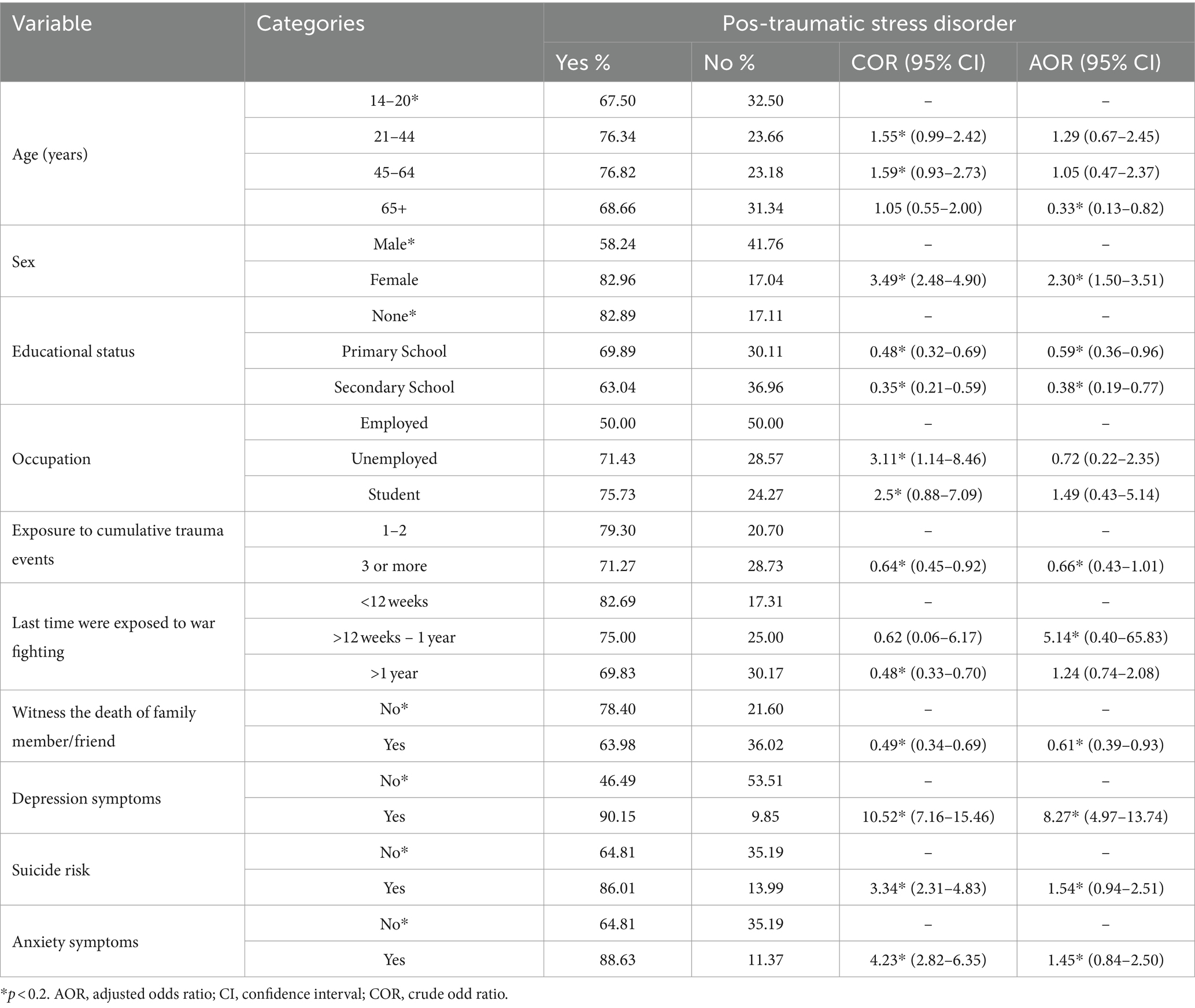
Table 5. Proportion post-traumatic stress disorder and associated factors among the participants from armed conflict area of Metuge district in Cabo Delgado (n = 748).
Discussion
Nearly 120, 000 IDPs have lived in the resettle camps of the Metuge district since October 2017. During the displacement and post-displacement periods, IDPs faced multiple stressors (48). They live in small, overcrowded temporary shelters in the camps, without sufficient food, clean water, or toilets. Their lives are on hold, and their futures are uncertain. Individuals with an experience of abuse/violence were at risk of increasing mental health problems (17). This study provides a detailed view of the symptoms of traumatic distress (PTSD, depression, and anxiety) encountered by 25 de Junho resettle camps in Metuge district, Cabo Delgado province.
This study found a high prevalence of PTSD, depression, and anxiety symptoms in IDPs in Cabo Delgado province. People affected were relatively young, with 71.8% under the age of 44, and predominantly female (65%). The rate of illiteracy was 41% with 80% of respondents unemployed and 96.4% departed from Quissanga district-which is among the most affected by the armed violence affecting the province since October 2017 (30).
Our study participants had lower educational levels (90%) and a 41% illiteracy rate and women are almost twice as likely to be illiterate as men in concordance with the national average (39.9%) (32). The Cabo Delgado province, despite being abundantly rich in mineral and environmental resources, has the highest rate of illiteracy (52.4%; 12.5% above the national average in population aged 15 and above) and multidimensional poverty in the country (32).
Additionally, the study participants had a high unemployment rate (78%) which is in concordance with the last report of the National Statistical Institute in Mozambique (32). The aggregate prevalence of depression, anxiety, and post-traumatic stress was considerably high, with a prevalence rate of 63.8, 40.0 and 74.3%, respectively, when compared with other studies conducted in armed conflict-affected populations (10.8% for depression, 15.3% for PTSD and 21.7% for anxiety) according to a systematic review and meta-analysis (15). Another systematic review (1981–2014) from six countries, five in Africa (18 studies), reported that the most frequent being post-traumatic stress disorder (range 3.1–75.9%), anxiety (range 6.9–75%), and depression (range 8.8–76.5%) (49).
The prevalence of PTSD at 74.3% was in line with the study carried out in Uganda (74%) (50) and lower than a study done in Medellin Colombia (88%) (51) and Iraq (83.4%) (52). Contrarily, the estimated PTSD prevalence of the current study was higher than the studies carried out as 63% in Nigeria (21), 40.8% in northwest and 58.4% in south of Ethiopia (24, 46), 19.3% in Morocco (22), 28% in South Sudan (23), 29.9% in Somalia (53) and 7.7% in Sri-Lanka (54), 46.6% in Bangladesh (55) particularly among women (5, 24, 55, 56).
The possible explanation for the observed difference could be the difference in tools, in which northwest Ethiopia (46), and northeast Ethiopia (56) studies used the post-traumatic stress disorder checklist for DSM (PCL-5), in Sri Lanka and Sweden studies used the Harvard trauma questionnaire (HTQ) (54, 57), and in Somalia and Uganda studies were used the International Neuropsychiatric Interview (MINI) (53, 58).
The high prevalence of PTSSs suggests that a scale-up of mental health care is needed, which could be met by increasing medical workers’ capacity in the Metuge health facilities to diagnose and treat patients with mental disorders. However, the current resources for mental health services are insufficient in the Metuge district, and the number of mental health professionals (2) is too low to cover the entire Metuge population in need.
The prevalence of depression symptoms (63.8%) was higher than the studies carried out in Uganda (58%) (58), in the south (53.3%) (24) and North Ethiopia (39.3%) (46), Sweden (40.2%) (57), Sri-Lanka (22.2%) (54) and Somalia (32.1%) (53). Contrarily, the estimated depression symptoms prevalence of the current study was lower than the study carried out at 89% in Bangladesh (59).
Additionally, the prevalence of anxiety symptoms (40.0%) in the current study was lower than the study done in southwestern Uganda (73%) (58). On the other hand, the findings of the current study were higher than the study done in northeast Ethiopia (33.4%) (56), Sweden (31.8%) (57), Somalia (34.9%) (53), and Sri Lanka (32.6%) (54). A possible theory to explain the high prevalence of PTSD, depression, and anxiety symptoms may be the repeated exposure to war attacks and/or violence (previous and current armed conflict, natural disasters, and COVID-19 pandemic) (60) that these displaced individuals had been exposed to several moments (the last attack in Quissanga district being recorded 6 months before the beginning of the study) (61). Of note, the region has recorded extreme weather events, such as Cyclone Kenneth in April 2019, affecting around 500,000 households that saw their homes partially or destroyed, followed by the torrential rains recorded in December 2019 and January 2020 (62). Furthermore, the COVID-19 pandemic and several outbreaks of cholera caused limited access to essential health services and thousands of additional deaths (63).
PTSD was significantly associated with being female (2.2. times), suicide risk (1.54 times), being screened positive for depression (8.27 times), and generalized anxiety (1.45 times).
Approximately half the respondents in our sample were female. The study findings show that mental health symptoms were more prevalent in female IDPs than in male IDPs. The odds of developing PTSD were 2.3 times higher in females compared to males, in line with the findings of other studies done in the south (24, 64) and north of Ethiopia (46, 56), and the fact that females have a higher risk of developing PTSD due to a lower threshold from exposure to psycho-trauma compared to males (51). In addition, many studies show that women were found to have a higher incidence of mental health disorders after rape or sexual assault (12, 65), the violent loss of a partner, or children, and becoming a single parent or widow (50, 66). Another reason could be that females tend to show a more emotional and ruminative response to stress (67). Contrarily, some studies found that symptoms of traumatic distress were more prevalent among male refugees than female refugees. (12, 55, 65)
Our research also found that IDPs who were unable to read or write had a higher prevalence of mental health symptoms (PTSD, depression, and anxiety) than those who had schooling. This finding is comparable to previous research that showed that poor education level was correlated to higher rates of PTSD (55, 68, 69) and increased risk of developing PTSD, depression, and anxiety (70).
Also, married respondents were more likely to have PTSSs, depression, and anxiety than those who were never married. This finding is comparable to findings in previous research (69).
Participants with depression were 8 times more likely to have PTSD when compared to participants without depression. Among patients with PTSD, depressive disorders, anxiety disorders, and drug misuse are 2 to 4 times more prevalent than among patients without PTSD (71). This is consistent with research conducted in Ethiopia (24, 56), Uganda (58), and Kenya (72). This has been related to participants with depression being more likely to have suffered traumatic experiences compared to participants without depression (67). Moreover, PTSD may increase the risk of suicide attempts (73).
Limitations
The results we present derive from a single center sample of IDP. The study participants were selected by convenience; and more representation of females may have impacted the results. Due to the cross-sectional nature of the study, we were not able to verify whether the depression, anxiety symptoms, and substance use, preceded or followed PTSD. Despite this, the findings may be helpful to nations with areas devastated by armed conflicts or war.
Conclusions and recommendations
The high prevalence of self-reported mental health symptoms in this study was found in a displaced working-age population. Being female, having a clinical feature of depression and anxiety, and having antecedents of the death of a family member, were associated with the development of PTSD. These results highlight the need for surveillance and follow-up studies, and training on stress management for their violent memories in the context of humanitarian emergencies in displaced populations, aiming to early diagnose and deliver group or individual psychological support, may reduce the burden of severe mental health symptoms. Likewise, these results highlight the need for more evidence-based research specifically from policymakers and stakeholders at the national and global level to tackle the common mental disorders issues through intervention.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by National Bioethics Committee for Health of Mozambique with registration IRB00002657. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants’ legal guardians/next of kin.
Author contributions
NM: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Visualization, Writing – original draft, Writing – review & editing. HI-M: Investigation, Writing – review & editing. FP: Formal analysis, Software, Writing – review & editing. PD: Validation, Writing – review & editing. FM: Conceptualization, Methodology, Writing – review & editing. VC: Validation, Writing – review & editing. AM: Supervision, Validation, Writing – review & editing. MM: Formal analysis, Funding acquisition, Software, Supervision, Validation, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This study was co-funded by Fundação para a Ciência e Tecnologia, GHTM-UID/04413/2020 and LA-REAL-LA/P/0117/2020 and by the Flemish Government through the Building Institutional Capacity at the Mozambique INS project.
Acknowledgments
We are grateful to the staff from the Mental Health, violence, and trauma Program and Delegação Provincial de Cabo Delgado of Instituto Nacional de Saúde, for their cooperation and support during this study. We also thank all study participants involved in this research, who gave their time, support, and enthusiasm in making this study possible.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Abbreviations
AOR, adjusted odds ratio; CI, confidence interval; COR, crude odd ratio; COVID-19, coronavirus disease 2019; DALY, disability adjusted life years; GAD-7, Generalized Anxiety Disorder Scale; HIV, human immunodeficiency virus; IDP, internally displaced people; LMIC, low- and middle-income countries; NGO, non-government organizations; PHQ-9, patient health questionnaire; PTSD, post-traumatic stress disorder; PTSSs, post-traumatic stress symptoms; PC-PTSD-5, primary care post-traumatic stress disorder checklist; YLD, years lived with disability.
References
1. Roberts, B, Damundu, EY, Lomoro, O, and Sondorp, E. The influence of demographic characteristics, living conditions, and trauma exposure on the overall health of a conflict-affected population in southern Sudan. BMC Public Health. (2010) 10:518. doi: 10.1186/1471-2458-10-518
2. Thapa, SB, and Hauff, E. Perceived needs, self-reported health, and disability among displaced persons during an armed conflict in Nepal. Soc Psychiatry Psychiatr Epidemiol. (2012) 47:589–95. doi: 10.1007/s00127-011-0359-7
3. Internal Displacement Monitoring Centre and Norwegian Refugee Council. Global Report on Internal Displacement. Geneva, Switzerland: Internal Displacement Monitoring Centre and Norwegian Refugee Council (2018).
4. Siriwardhana, C, and Stewart, R. Forced migration and mental health: prolonged internal displacement, return migration and resilience. Int Health. (2013) 5:19–23. doi: 10.1093/inthealth/ihs014
5. Virgincar, A, Doherty, S, and Siriwardhana, C. The impact of forced migration on the mental health of the elderly: a scoping review. Int Psychogeriatr. (2016) 28:889–96. doi: 10.1017/S1041610216000193
6. Burke, MB, Miguel, E, Satyanath, S, Dykema, JA, and Lobell, DB. Warming increases the risk of civil war in Africa. Proc Natl Acad Sci USA. (2009) 106:20670–4. doi: 10.1073/pnas.0907998106
7. Charlson, F, van Ommeren, M, Flaxman, A, Cornett, J, Whiteford, H, and Saxena, S. New WHO prevalence estimates of mental disorders in conflict settings: a systematic review and meta-analysis. Lancet. (2019) 394:240–8. doi: 10.1016/S0140-6736(19)30934-1
8. Hoppen, TH, Priebe, S, Vetter, I, and Morina, N. Global burden of post-traumatic stress disorder and major depression in countries affected by war between 1989 and 2019: a systematic review and meta-analysis. BMJ Glob Health. (2021) 6:e006303. doi: 10.1136/bmjgh-2021-006303
9. Rawal, N, Pradhan, M, Manandhar, P, Adhikari, S, Amatya, R, and Khadka, B. Prevalence of post-traumatic stress disorder and its associated factors among nepali army service members and veterans: 15 years post insurgency. Nepal Med Coll J. (2021) 23:281–9. doi: 10.3126/nmcj.v23i4.42208
10. GBD 2019 Mental Disorders Collaborators. Global, regional, and national burden of 12 mental disorders in 204 countries and territories, 1990-2019: a systematic analysis for the global burden of disease study 2019. Lancet Psychiatry. (2022) 9:137–50. doi: 10.1016/S2215-0366(21)00395-3.
11. de Jong, JT, Komproe, IH, and Van Ommeren, M. Common mental disorders in post conflict settings. Lancet. (2003) 361:2128–30. doi: 10.1016/S0140-6736(03)13692-6
12. Porter, M, and Haslam, N. Predisplacement and post displacement factors associated with mental health of refugees and internally displaced persons: a meta-analysis. JAMA. (2005) 294:602–12. doi: 10.1001/jama.294.5.602
13. Blanchet, K, Ramesh, A, Frison, S, Warren, E, Hossain, M, Smith, J, et al. Evidence on public health interventions in humanitarian crises. Lancet. (2017) 18;390:2287–2296. doi: 10.1016/S0140-6736(16)30768-1
14. Hoppen, T, and Morina, N. The prevalence of PTSD and major depression in the global population of adult war survivors: a meta-analytically informed estimate in absolute numbers. Eur J Psychotraumatol. (2019) 10:1578637. doi: 10.1080/20008198.2019.1578637
15. Pico-Alfonso, M, Garcia-Linares, M, Celda-Navarro, N, Blasco-Ros, C, Echeburúa, E, and Martinez, M. The impact of physical, psychological, and sexual intimate male partner violence on women’s mental health: depressive symptoms, posttraumatic stress disorder, state anxiety, and suicide. J Women's Health. (2006) 15:599–611. doi: 10.1089/jwh.2006.15.599
16. Frans, Ö, Rimmö, P, Åberg, L, and Fredrikson, M. Trauma exposure and post-traumatic stress disorder in the general population. Acta Psychiatr Scand. (2005) 111:291–12. doi: 10.1111/j.1600-0447.2004.00463.x
17. Steel, Z, Chey, T, Silove, D, Marnane, C, Bryant, R, and Van Ommeren, M. Association of torture and other potentially traumatic events with mental health outcomes among populations exposed to mass conflict and displacement: a systematic review and meta-analysis. JAMA. (2009) 302:537–49. doi: 10.1001/jama.2009.1132
18. Thapa, S, and Hauff, E. Psychological distress among displaced persons during an armed conflict in Nepal. Soc Psychiatry Psychiatr Epidemiol. (2005) 40:672–9. doi: 10.1007/s00127-005-0943-9
19. Sun, J, Luo, Y, Chang, H, Zhang, R, Liu, R, Jiang, Y, et al. The mediating role of cognitive emotion regulation in BIS/BAS sensitivities, depression, and anxiety among community-dwelling older adults in China. Psychol Res Behav Manage. (2020) 13:939–48. doi: 10.2147/PRBM.S269874
20. Taru, M, Bamidele, L, Makput, D, Audu, M, Philip, T, John, D, et al. Post-traumatic stress disorder among internally displaced victims of boko haram terrorism in northeastern Nigeria. J Med. (2018) 12:8–15.
21. Astitene, K, and Barkat, A. Prevalence of posttraumatic stress disorder among adolescents in school and its impact on their well-being: a cross-sectional study. Pan African Med J. (2021) 39:54. doi: 10.11604/pamj.2021.39.54.27419
22. Ayazi, T, Lien, L, Eide, A, Ruom, M, and Hauff, E. What are the risk factors for the comorbidity of posttraumatic stress disorder and depression in a war-affected population? A cross-sectional community study in South Sudan. BMC Psychiatry. (2012) 12:175. doi: 10.1186/1471-244X-12-175
23. Madoro, D, Kerebih, H, and Habtamu, Y. Post-traumatic stress disorder and associated factors among internally displaced people in South Ethiopia: a cross-sectional study. Neuropsychiatry Dis Treat. (2020) 16:2317–26. doi: 10.2147/NDT.S267307
24. Vasile, C. Mental health and immunity (review). Exp Ther Med. (2020) 20:1. doi: 10.3892/etm.2020.9341
25. UNHCR Mozambique Country Factsheet, (2023). Available at: https://reliefweb.int/report/mozambique/unhcr-mozambique-country-factsheet-april-2023 (Accessed October 29, 2023).
26. International Organization for Migration (IOM). DTM Mozambique — Mobility Tracking Assessment Report 17 (November 2022). Mozambique: IOM (2022).
27. UNHCR Mozambique. (2022). Year end Report. Available at: https://data.unhcr.org/en/documents/details/101891 (Accessed October 29, 2023).
28. Save the Children. Joint Briefing Note on the Situation Facing Children in Northern Mozambique; (2021). Available from: https://mozambique.savethechildren.net/news/joint-briefing-note-situation-facing-children-northern-mozambique (Accessed November 3, 2023).
29. International Organization for Migration (IOM). DTM Northern Mozambique Crisis — DTM Baseline Assessment Abridged Report Round 16 (June 2022). Mozambique: IOM (2022).
30. UN-Habitat. A Dimensão Territorial dos Deslocamentos no Norte de Moçambique; (2021). Available at: https://unhabitat.org/sites/default/files/2021/05/un-habitat_positionpaper_mozambique_pt.pdf (Accessed November 6, 2023).
31. IDP Definition. Emergency Handbook. UNHCR (2023). Available from: https://emergency.unhcr.org/search?search=IDP%20definition (Accessed October 29, 2023).
32. INS. IV Recenseamento Geral da População e Habitação 2017 - Resultados Definitivos. Instituto Nacional de Saúde. Mozambique. (2019). Available from: https://www.ine.gov.mz/web/guest/d/censo-2017-brochura-dos-resultados-definitivos-do-iv-rgph-nacional (Accessed October 29, 2023).
33. International Organization for Migration (IOM). DTM Mozambique - Emergency Tracking Tool - Palma Crisis Report | 94 (27 March - 28 May 2021). Mozambique: IOM (2021).
34. Smith Fawzi, MC, Ngakongwa, F, Liu, Y, Rutayuga, T, Siril, H, Somba, M, et al. Validating the patient health Questionnaire-9 (PHQ-9) for screening of depression in Tanzania. Neurol Psychiatry Brain Res. (2019) 31:9–14. doi: 10.1016/j.npbr.2018.11.002
35. Chibanda, D, Verhey, R, Gibson, LJ, Munetsi, E, Machando, D, Rusakaniko, S, et al. Validation of screening tools for depression and anxiety disorders in a primary care population with high HIV prevalence in Zimbabwe. J Affect Disord. (2016) 198:50–5. doi: 10.1016/j.jad.2016.03.006
36. Haas, AD, Technau, KG, Pahad, S, Braithwaite, K, Madzivhandila, M, Sorour, G, et al. Mental health, substance use and viral suppression in adolescents receiving ART at a paediatric HIV clinic in South Africa. J Int AIDS Soc. (2020) 23:e25644. doi: 10.1002/jia2.25644
37. Di Gennaro, F, Marotta, C, Ramirez, L, Cardoso, H, Alamo, C, Cinturao, V, et al. High prevalence of mental health disorders in adolescents and youth living with HIV: an observational study from eight health Services in Sofala Province, Mozambique. AIDS Patient Care STDS. (2022) 36:123–9. doi: 10.1089/apc.2022.0007
38. Cumbe, VFJ, Muanido, A, Manaca, MN, Fumo, H, Chiruca, P, Hicks, L, et al. Validity and item response theory properties of the patient health Questionnaire-9 for primary care depression screening in Mozambique (PHQ-9-MZ). BMC Psychiatry. (2020) 20:382. doi: 10.1186/s12888-020-02772-0
39. Lovero, KL, Adam, SE, Bila, CE, Canda, ED, Fernandes, ME, Rodrigues, TIB, et al. Validation of brief screening instruments for internalizing and externalizing disorders in Mozambican adolescents. BMC Psychiatry. (2022) 22:549. doi: 10.1186/s12888-022-04189-3
40. Prins, A, Bovin, MJ, Kimerling, R, Kaloupek, D. G., Marx, BP, Pless Kaiser, A, et al. (2016). The Primary Care PTSD Screen for DSM-5 (PC-PTSD-5) [Measurement Instrument]. Development and Evaluation Within a Veteran Primary Care Sample. J Gen Intern Med. 31:1206–11. doi: 10.1007/s11606-016-3703-5
41. Bovin, MJ, Kimerling, R, Weathers, FW, Prins, A, Marx, BP, Post, EP, et al. Diagnostic accuracy and acceptability of the primary care posttraumatic stress disorder screen for the diagnostic and statistical manual of mental disorders (fifth edition) among US veterans. JAMA Netw Open. (2021) 4:e2036733. doi: 10.1001/jamanetworkopen.2020.36733
42. Kroenke, K, and Spitzer, RL. The PHQ-9: a new depression diagnostic and severity measure. Psychiatr Ann. (2002) 32:509–15. doi: 10.3928/0048-5713-20020901-06
43. Moriarty, AS, Gilbody, S, McMillan, D, and Manea, L. Screening and case finding for major depressive disorder using the patient health questionnaire (PHQ-9): a meta-analysis. Gen Hosp Psychiatry. (2015) 37:567–76. doi: 10.1016/j.genhosppsych.2015.06.012
44. Spitzer, RL, Kroenke, K, Williams, JB, and Löwe, B. A brief measure for assessing generalized anxiety disorder: the GAD-7. Arch Intern Med. (2006) 166:1092–7. doi: 10.1001/archinte.166.10.1092
45. Plummer, F, Manea, L, Trepel, D, and McMillan, D. Screening for anxiety disorders with the GAD-7 and GAD-2: a systematic review and diagnostic meta-analysis. Gen Hosp Psychiatry. (2016) 39:24–31. doi: 10.1016/j.genhosppsych.2015.11.005
46. Teshome, AA, Abebe, EC, Mengstie, MA, Seid, MA, Yitbarek, GY, Molla, YM, et al. Post-traumatic stress disorder and associated factors among adult war survivors in Northwest Ethiopia: community-based, cross-sectional study. Front Psych. (2023) 14:1083138. doi: 10.3389/fpsyt.2023.1083138
47. Bezabh, YH, Abebe, SM, Fanta, T, Tadese, A, and Tulu, M. Prevalence and associated factors of post-traumatic stress disorder among emergency responders of Addis Ababa fire and emergency control and prevention service authority, Ethiopia: institution-based, cross-sectional study. BMJ Open. (2018) 8:e020705. doi: 10.1136/bmjopen-2017-020705
48. Weine, SM, Ware, N, Hakizimana, L, Tugenberg, T, Currie, M, Dahnweih, G, et al. Fostering resilience: protective agents, resources, and mechanisms for adolescent refugees’ psychosocial well-being. Adolesc Psychiatry (Hilversum). (2014) 4:164–76. doi: 10.2174/221067660403140912162410
49. Ba, I, and Bhopal, RS. Physical, mental, and social consequences in civilians who have experienced war-related sexual violence: a systematic review (1981–2014). Public Health. (2017) 142:121–35. doi: 10.1016/j.puhe.2016.07.019
50. Roberts, B, Ocaka, KF, Browne, J, Oyok, T, and Sondorp, E. Factors associated with the health status of internally displaced persons in northern Uganda. J Epidemiol Community Health. (2009) 63:227–32. doi: 10.1136/jech.2008.076356
51. Richards, A, Ospina-Duque, J, Barrera-Valencia, M, Escobar-Rincón, J, Ardila-Gutiérrez, M, Metzler, T, et al. Posttraumatic stress disorder, anxiety and depression symptoms, and psychosocial treatment needs in Colombians internally displaced by armed conflict: a mixed-method evaluation. Psychol Trauma. (2011) 3:384–93. doi: 10.1037/a0022257
52. Mahmood, HN, Ibrahim, H, Goessmann, K, Ismail, AA, and Neuner, F. Post-traumatic stress disorder and depression among Syrian refugees residing in the Kurdistan region of Iraq. Confl Heal. (2019) 13:51. doi: 10.1186/s13031-019-0238-5
53. Salad, AM, Malik, SMMR, Ndithia, JM, Noor, Z, Madeo, M, and Ibrahim, M. Prevalence of mental disorders and psychological trauma among conflict-affected population in Somalia: a cross-sectional study. Front Public Health. (2023) 11:1219992. doi: 10.3389/fpubh.2023.1219992
54. Husain, F, Anderson, M, Lopes Cardozo, B, Becknell, K, Blanton, C, Araki, D, et al. Prevalence of war-related mental health conditions and association with displacement status in postwar Jaffna District, Sri Lanka. JAMA. (2011) 306:522–31. doi: 10.1001/jama.2011.1052
55. Hossain, A, Baten, RBA, Sultana, ZZ, Rahman, T, Adnan, MA, Hossain, M, et al. Predisplacement abuse and postdisplacement factors associated with mental health symptoms after forced migration among Rohingya refugees in Bangladesh. JAMA Netw Open. (2021) 4:e211801. doi: 10.1001/jamanetworkopen.2021.1801
56. Anbesaw, T, Zenebe, Y, Asmamaw, A, Shegaw, M, and Birru, N. Post-traumatic stress disorder and associated factors among people who experienced traumatic events in Dessie town, Ethiopia, 2022: a community-based study. Front Psych. (2022) 13:1026878. doi: 10.3389/fpsyt.2022.1026878
57. Tinghög, P, Malm, A, Arwidson, C, Sigvardsdotter, E, Lundin, A, and Saboonchi, F. Prevalence of mental ill health, traumas and postmigration stress among refugees from Syria resettled in Sweden after 2011: a population-based survey. BMJ Open. (2017) 7:e018899. doi: 10.1136/bmjopen-2017-018899
58. Bapolisi, AM, Song, SJ, Kesande, C, Rukundo, GZ, and Ashaba, S. Post-traumatic stress disorder, psychiatric comorbidities and associated factors among refugees in Nakivale camp in southwestern Uganda. BMC Psychiatry. (2020) 20:53. doi: 10.1186/s12888-020-2480-1
59. Riley, A, Varner, A, Ventevogel, P, Taimur Hasan, MM, and Welton-Mitchell, C. Daily stressors, trauma exposure, and mental health among stateless Rohingya refugees in Bangladesh. Transcult Psychiatry. (2017) 54:304–31. doi: 10.1177/1363461517705571
60. Said, DS, Lopes, G, Lorettu, L, Farina, G, Napodano, CMP, Amadori, A, et al. Mental health and COVID-19 pandemics: the worrisome humanitarian perspective from the Middle East. J Glob Health. (2021) 11:3014. doi: 10.7189/jogh.11.03014
61. ZITAMAR News Insurgents Attack Quissanga for First Time in Eight Months; (2022). Available at: https://www.zitamar.com/insurgents-attack-quissanga-for-first-time-in-eight-months/ (Accessed November 7, 2023).
62. Mugabe, VA, Gudo, ES, Inlamea, OF, Kitron, U, and Ribeiro, GS. Natural disasters, population displacement and health emergencies: multiple public health threats in Mozambique. BMJ Glob Health. (2021) 6:e006778. doi: 10.1136/bmjgh-2021-006778
63. United Nations. Flash Appeal for COVID-19 Mozambique, (2020). Available at: https://mozambique.un.org/sites/default/files/2020-08/MOZ_20200604_COVID-19_Flash_Appeal_0.pdf (Accessed November 8, 2023).
64. Asnakew, S, Shumet, S, Ginbare, W, Legas, G, and Haile, K. Prevalence of post-traumatic stress disorder and associated factors among koshe landslide survivors, Addis Ababa, Ethiopia: a community-based, cross-sectional study. BMJ Open. (2019) 9:e028550. doi: 10.1136/bmjopen-2018-028550
65. Creamer, M, Burgess, P, and McFarlane, AC. Post-traumatic stress disorder: findings from the Australian National Survey of mental health and well-being. Psychol Med. (2001) 31:1237–47. doi: 10.1017/S0033291701004287
66. Keane, TM, Marshall, AD, and Taft, CT. Posttraumatic stress disorder: etiology, epidemiology, and treatment outcome. Annu Rev Clin Psychol. (2006) 2:161–97. doi: 10.1146/annurev.clinpsy.2.022305.095305
67. Shevlin, M, Hyland, P, Vallières, F, Bisson, J, Makhashvili, N, Javakhishvili, J, et al. A comparison of DSM-5 and ICD-11 PTSD prevalence, comorbidity and disability: an analysis of the Ukrainian internally displaced Person's mental health survey. Acta Psychiatr Scand. (2018) 137:138–47. doi: 10.1111/acps.12840
68. Alpak, G, Unal, A, Bulbul, F, Sagaltici, E, Bez, Y, Altindag, A, et al. Post-traumatic stress disorder among Syrian refugees in Turkey: a cross sectional study. Int J Psychiatry Clin Pract. (2015) 19:45–50. doi: 10.3109/13651501.2014.961930
69. Basheti, IA, Ayasrah, SM, Basheti, MM, Mahfuz, J, and Chaar, B. The Syrian refugee crisis in Jordan: a cross sectional pharmacist-led study assessing post-traumatic stress disorder. Pharm Pract (Granada). (2019) 17:1475. doi: 10.18549/PharmPract.2019.3.1475
70. Jain, N, Prasad, S, Czárth, ZC, Chodnekar, SY, Mohan, S, Savchenko, E, et al. War psychiatry: identifying and managing the neuropsychiatric consequences of armed conflicts. J Prim Care Community Health. (2022) 13:21501319221106625. doi: 10.1177/21501319221106625
71. McCauley, JL, Killeen, T, Gros, DF, Brady, KT, and Back, SE. Posttraumatic stress disorder and co-occurring substance use disorders: advances in assessment and treatment. Clin Psychol. (2012) 19:12006. doi: 10.1111/cpsp.12006
72. Mbwayo, A, Mathai, M, Harder, V, Nicodimos, S, and Vander, SA. Trauma among kenyan school children in urban and rural settings: PTSD prevalence and correlates. J Child Adoles Trauma. (2020) 13:63–73. doi: 10.1007/s40653-019-00256-2
Keywords: post-traumatic stress disorder, anxiety, depression, internally displaced persons, humanitarian emergency, Cabo Delgado, Mozambique
Citation: Manafe N, Ismael-Mulungo H, Ponda F, Dos Santos PF, Mandlate F, Cumbe VFJ, Mocumbi AO and Oliveira Martins MR (2024) Prevalence and associated factors of common mental disorders among internally displaced people by armed conflict in Cabo Delgado, Mozambique: a cross-sectional community-based study. Front. Public Health. 12:1371598. doi: 10.3389/fpubh.2024.1371598
Edited by:
Ahmed Hossain, University of Sharjah, United Arab EmiratesReviewed by:
Mir Nabila Ashraf, University of Regina, CanadaTanay Maiti, Black Country Partnership NHS Foundation Trust, United Kingdom
Copyright © 2024 Manafe, Ismael-Mulungo, Ponda, Dos Santos, Mandlate, Cumbe, Mocumbi and Oliveira Martins. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Naisa Manafe, bmFpc2EubWFuYWZlQGdtYWlsLmNvbQ==
†ORCID: Naisa Manafe, orcid.org/0000-0001-6357-7673