 Yulia A. Levites Strekalova
Yulia A. Levites Strekalova Xiangren Wang
Xiangren Wang Sara Midence
Sara Midence Alexander Quarshie3
Alexander Quarshie3
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
POLICY BRIEF article
Front. Public Health, 14 November 2024
Sec. Public Health Policy
Volume 12 - 2024 | https://doi.org/10.3389/fpubh.2024.1369790
This article is part of the Research TopicSocial Science Contributions to Public HealthView all 5 articles
This paper maps policy instrument use for the social drivers of health (SDoH) data governance in clinical and research settings. In the United States, Centers for Medicare and Medicaid Services (CMS) and National Institutes of Health (NIH) advocate for standardized data capture. Yet, challenges persist, including limited adoption of CMS-issued SDoH risk codes and gaps in reporting SDoH in clinical trial literature. The mapping across clinical and research SDoH reporting emerges as a comprehensive solution that requires policy support. Specifically, the findings presented in this paper support future policy development through regulatory instruments, fiscal incentives, and knowledge exchange. Actionable recommendations for the United States and international contexts include convening interdisciplinary taskforces, developing agency guidelines for process evaluation, and establishing ethical principles for SDoH data use.
The role of social drivers of health (SDoH) has been extensively documented and linked to health outcomes (1, 2). There is a wide-reaching consensus on the importance of capturing the SDoH systematically and rigorously, and research increasingly demonstrates how SDoH contribute to disparities observed across various demographic groups (3–6). Capturing SDoH data in clinical practice is essential for addressing the complex interplay between social factors and health outcomes. Similarly, capturing SDOH in clinical research is essential for understanding and addressing the multifaceted factors that influence patient outcomes. However, the unstructured format of SDoH data in electronic health records limits the ability to address these issues effectively (7). Despite the availability of SDoH data in national sources, there is inconsistency in data collection within health systems, indicating an opportunity for improvement in capturing comprehensive SDoH data. High noncompletion rates in capturing SDoH data underscore the need for evidence-based guidelines to improve data collection in underserved populations (7). Furthermore, barriers such as incentives, training, privacy, and ethical use of data need to be addressed to fully integrate social risk assessment into healthcare delivery systems and translational research (8, 9). Therefore, there is a need for focused efforts to identify and implement evidence-based policy instruments that support the SDoH data governance in both clinical and research contexts.
Health data governance requires established guidelines and procedures to ensure the availability, integrity, security, and usability of both structured and unstructured data and facilitate its strategic management to enhance organizational effectiveness and quality of care (10). The need for SDoH data governance spans clinical practice and clinical research domains as the research-to-practice and practice-to-research issues in SDoH data capture and sharing are multifaceted, involving organizational, ethical, technical, and system behavior challenges (11–13). SDoH data are frequently fragmented across multiple health data sources and healthcare service deliveries (14–16). Healthcare and social service providers can communicate data at the time of care if they have access to interoperable data on particular social hazards and corresponding treatments (13). Population health management, documentation of social needs, intervention implementation and evaluation, and model refinement of care delivery may all be enhanced at the practice level with aggregated social data (4, 17–19). Furthermore, real-world data on SDoH are often derived from multiple sources that include electronic health records, medical claims, and patient-generated data (17, 20–22). While there is a growing recognition of the importance of data sharing to strengthen academic research and clinical practices, it comes with calls for policies to improve data management planning, harmonization of practices, and ethical sourcing and use data (14, 23, 24).
Health policy instruments can be categorized into three main types, each serving distinct functions in governance and public health (25, 26). Legislative and regulatory instruments involve laws, regulations, and standards that mandate or restrict certain behaviors to enforce compliance and protect public health. Economic and fiscal instruments include taxes, subsidies, and pricing strategies designed to influence individual and organizational behaviors. Cooperative and knowledge translation instruments rely on partnerships, coordination, and voluntary agreements between stakeholders, including public-private partnerships and community collaborations, to achieve health objectives without direct regulation. Lastly, we also propose and articulate knowledge translation as a policy instrument that involves the collection and dissemination of scientific evidence to inform policy decisions and promote evidence-based practices, ensuring that health policies are grounded in the latest and most reliable knowledge. Together, these instruments stand to create a comprehensive policy mix that addresses the complexities of SDoH data governance, ensuring that data are collected, managed, and utilized effectively to improve public health outcomes.
In this policy brief, we aim to (1) discuss the existing policy efforts made to develop and collect SDoH and (2) suggest future policy development and implementation efforts that can help and direct the SDoH data governance, namely, the collection and use of SDoH data in clinical practice, quality improvement, and partnerships between research and practice.
Policy can support and provide a framework for SDoH data capture in healthcare and research contexts. In the United States, the Centers for Medicare and Medicaid Services (CMS) produced guidelines and created pathways to develop the SDoH data capture systems (1, 27–29). However, because of the complexity of the SDoH domain, there is no consensus on the approach to the SDoH screening and the set of common SDoH elements. As a governmental agency, the CMS actively uses policy to regulate, promote, and encourage this capture (30). Similarly, the National Institute of Health (NIH) and other funding agencies are employing policy tools to promote, encourage, and ensure the standardized capture of the SDoH for research (28, 31). Strategic use of the policy instruments rooted in ethical data governance can promote the systematic, standardized capture of social drivers of health, and foster research-practice partnerships. Next, we will discuss the existing policy efforts for the SDoH data governance in clinical and research domains.
Regulatory policy instruments can provide the guidelines and expectations of required and recommended screening for and capturing of the SDoH. Within patient care, the CMS has, for many years, encouraged the use of Z codes and now requires their inclusion in specific reports. In the United States, the CMS has issued detailed guidelines for systematically implementing Z codes to report SDoH in clinical environments (3). The assessment requires the use of tested and validated tools that cover essential SDoH domains like housing instability, food insecurity, and utility difficulties. Currently, only a minority of patients are screened for SDoH, but the introduction of required SDoH screening for hospital admissions is likely to increase the proportion of the United States population that receives screening (32, 33). Within the context of clinical research in the United States, the NIH requires that human subject studies report the demographics of research participants for planned and actual enrollment. This is another example of a regulatory policy instrument that mandates SDoH data capture (28). While only basic demographics are currently required to be captured for federally funded research studies, NIH efforts are underway to develop a new set of minimum common data elements, including the SDoH (34).
The implementation of SDoH screening requires a technical and financial infrastructure that accounts for the data collection burden. Although the CMS has dedicated considerable resources to advancing the use of Z codes, their widespread integration into healthcare documentation practices still needs to be improved (6). Recent findings reveal that a mere 5% of Medicare recipients have SDoH-related Z codes recorded in the EMR (7, 8). This number is thought to underrepresent the true prevalence of SDoH influences on the health of Medicare beneficiaries, suggesting a discrepancy between recorded data and the actual prevalence of SDoH within the United States population. The CMS is moving toward using economic instruments to promote SDoH screening policies through the proposed reimbursement strategies for SDoH screening, which will reward practices for the time spent conducting SDoH assessments. In 2024, the CMS implemented a new GXXX5 code for administering a standardized, evidence-based SDoH risk to enhance the understanding of a patient’s social history and its influence on health emphasizing the necessity of follow-up actions and interventions after the assessment. Further support for SDoH data capture can be created through fiscal policy instruments such as financial subsidies, grants, and incentives that support the development of legal, technical, and operational infrastructure for data capture, harmonization, management, storage, and use (24).
While regulatory and economic policies can be effective, they are also limited in what they can achieve if implemented in silos. Cooperative policies are the third policy instrument actively applied by government agencies to promote knowledge exchange and coordination of actions. The most common implementation of collaborative policy instruments involves the establishment of taskforces that develop recommendations and pathways for inter-organizational collaboration. As a policy instrument, establishing a taskforce requires a financial and staffing commitment for interagency partnerships among clinical, research, industry, community, and governmental organizations. Ultimately, all agencies are interested in the same goal: identifying social drivers and finding strategies to address them. However, research and practice are at risk of uncoordinated information flow and efforts to establish common data capture approaches (35).
In response to the need for standardized SDoH data collection, the National Institute on Minority Health and Health Disparities (NIMHD) led a task force effort to develop a set of consensus-based instruments for use in research studies to assess SDoH and standardize the SDoH screening protocols for clinical research (31). The instruments were selected and evaluated for inclusion in the “Consensus Measures for Phenotypes and eXposures” PhenX toolkit (36). With the introduction of the PhenX Toolkit in May 2020, data capture protocols were encapsulated, offering assessments at the individual and structural levels. Developed protocols included a Core SDoH collection with 16 measurements recommended for all research studies. The Core collection includes demographics (e.g., ethnicity and race, age, gender identity, annual family income, and employment status) and social driver variables that address structural and individual SDoH. Active awards from the NIH National Institute for Minority Health and Health Disparities promote the use of PhenX SDoH Core toolkits. For example, the Research Centers in Minority Institutions (RCMI) program uses PhenX as a guide to develop common data models and protocols for SDoH capture (45). Through the establishment of the RCMI Clinical Research Network for Health Equity (CRNHE), several dynamic clinical networks will collaborate to reach a unanimous agreement on the PhenX SDoH core toolkits. Consensus metrics for SDoH in clinical research, developed by the PhenX Toolkit, are an essential first step toward social driver assessment standards (31). The toolkit supports a transparent approach to include SDoH considerations in clinical research (37).
Knowledge translation as a policy instrument for SDoH data governance leverages practice-based research to bridge the gap between data production and policy implementation, ensure that data capture and use are both informed and actionable (38–40), and integrate evidence-based strategies and stakeholder engagement into the policy-making process (41). Knowledge translation systematically moves research evidence into practice and policy. This process can be guided by the theory of change frameworks that emphasize the iterative of policy development, ensuring that evidence is not only scientifically plausible but also acceptable and practical for implementation (42, 43). As discussed earlier in this brief, there are significant areas of overlap in SDoH data use for clinical and research purposes, which can be further supported through knowledge transfer practices and accepted cross-referencing of the SDoH data elements.
With the increasing reliance on real-world data, the significance of integrating Z codes, PhenX protocols, and SDoH screening tools has become more pronounced. Partnerships between research and practice can be bolstered by employing harmonized coding systems in tandem with validated SDoH screening instruments. Numerous instruments have been developed to collect data (13, 14), and collecting comprehensive SDoH data requires time and a level of rapport and trust that can be difficult to establish in brief clinical encounters (44). The limitations of collecting SDoH variables thus become a significant barrier, impeding the ability of healthcare providers to fully understand and address the broader social and economic factors that influence their patients’ health (26). Integrating research-focused PhenX data and clinically focused Z codes can be achieved by explicitly mapping Z codes onto research instruments and the gradual rollout of requirements to screen for the social drivers of research participants’ health.
When considered broadly, most of the SDoH domains represented by PhenX and can be mapped to Z codes as shown in Table 1. However, mapping the Z codes and PhenX toolkit reveals several disconnects. Notable exceptions from the Z codes are demographic data, such as race, ethnicity, age, and current address, which are expected to be captured at patient intake. While this is a reasonable expectation, demographic point-of-care data capture varies among clinical practices. It may omit questions about birthplace and differentiation between sex assigned at birth and self-reported gender (21). Other constructs related to social integration (Z60), housing stability (Z59), safety (Z62), domestic violence (Z63), and material security (Z58) are included in the Z codes but not in the PhenX Core instruments. This finding highlights the primary focus on interpersonal relationships and factors related to family (27). When assessed in clinical care, these Z codes capture various social issues influencing the patient’s health and well-being. Finally, access to health services identified in PhenX map to a Z code (Z75) outside the Z55-65 range that identifies health hazards related to socioeconomic and psychosocial circumstances.
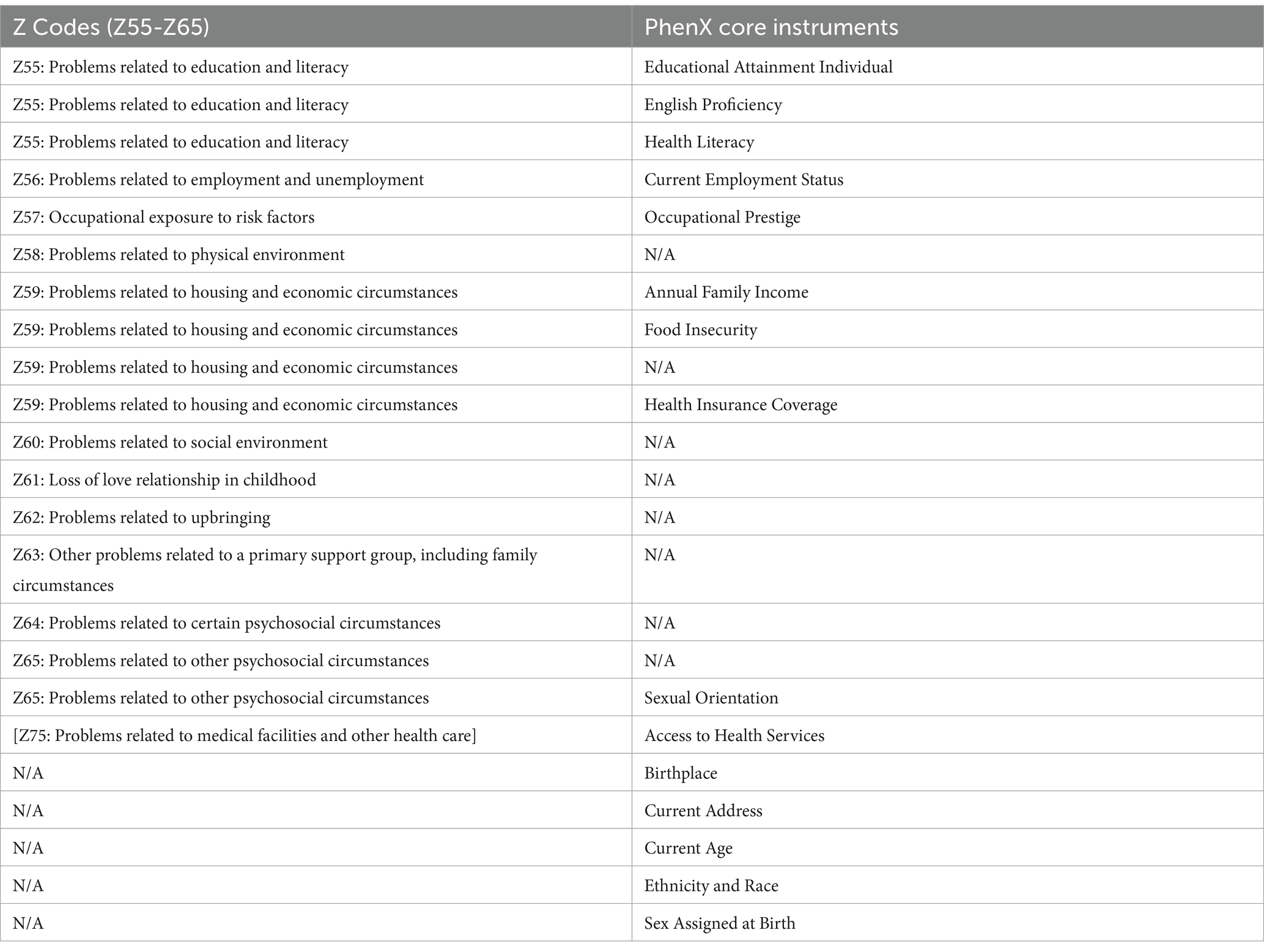
Table 1. SDoH domain mapping.
The policy mapping presented above focuses on the United States policy context. However, the selection of policy instruments can inform policy efforts in other national and regional applications. To enhance the capture and use of SDoH data within clinical and research settings, we provide the following actionable recommendations: a strategic direction and a detailed plan of action, each supported by a brief explanation drawing from current evidence and best practices (6).
It would be essential to convene a team that represents a diversity of perspectives on SDoH data governance and includes the representation of community and patient representatives (41). The task force should first identify barriers such as inconsistent definitions and data quality issues and consider the legal and organizational shortcomings in health data systems. The task force should advocate for resources to enhance data linkage and text classification methods, which show promise for improving SDoH data integration. By addressing these aspects, the task force can effectively advocate for the necessary resources and policies to integrate SDoH data into health systems, ultimately improving health outcomes and equity.
By collecting stakeholders’ suggestions through available comments, the agency ensures that the guidelines are developed with transparency and inclusivity. The stakeholders will be able to contribute to ensuring that the policies are well-rounded and consider the needs (30). To develop agency guidelines for cross-mapping Z codes and PhenX toolkits with input from open comments, it is essential to adopt a multi-stakeholder approach that ensures transparency and inclusivity. Additionally, the guidelines can incorporate ethical considerations surrounding the use of real-world and open-source neighborhood data.
Offer additional funding or resources to support the assessment of SDoH data capture processes. This includes assessing workflows, data accuracy and conciseness, and the impact on patient outcomes (9). By understanding these processes, healthcare and research teams can refine data capture methods to be more effective and less intrusive.
Define a set of guiding principles and requirements for the capture and use of SDoH data in clinical and research contexts. These principles should emphasize ethical considerations (consent and data sovereignty), data quality, privacy, and the meaningful use of data in improving health outcomes. Furthermore, the Findable, Accessible, Interoperable, and Reusable (FAIR) principles should be adopted to promote rigorous and reproducible data collection and management practices.
Advocate for policies that promote the consistent and ethical use of SDoH data, ensuring that it is used to improve patient care and health outcomes without compromising patient privacy or autonomy (14).
The development of robust policy instruments for the governance of SDoH data is critical to advancing health equity through the systematic capture and use of data in both clinical and research contexts. Regulatory instruments, such as those issued by the U.S. Centers for Medicare and Medicaid Services, establish essential frameworks for standardized SDoH data collection. Yet, gaps remain in compliance and data uniformity, necessitating further refinement of these policies to align with evidence-based practices. Economic and fiscal policies, including incentives for SDoH screening, must be expanded to address the financial and infrastructural burdens of data collection, ensuring that healthcare providers are adequately supported. Cooperative instruments, exemplified by the task force-led development of the PhenX SDoH toolkit, underscore the importance of cross-sector collaboration in harmonizing data collection practices across research and clinical settings. Furthermore, the integration of knowledge translation instruments will enable the alignment of real-world clinical data with research outcomes through tools such as ICD-10 and PhenX. Ethical considerations surrounding privacy and data sovereignty must be embedded within governance frameworks to safeguard patient autonomy while enabling the actionable use of SDoH data. Lastly, interdisciplinary task forces should be institutionalized to provide ongoing guidance and ensure the adaptive refinement of SDoH data governance practices, with continuous process evaluations that inform policy adjustments and enhance the efficacy of data-driven interventions aimed at addressing health disparities.
Data governance challenges create barriers in SDoH data sharing, integration, and utilization in clinical practice and research. Strategic use of regulatory, fiscal, cooperation, and knowledge transfer policy instruments is essential for informed public health decision-making and continued progress toward health equity. As the healthcare landscape continues to evolve, the need for such integrative and inclusive approaches in clinical practice and research become increasingly vital. By articulating the types of policy instruments for SDoH data governance, this paper aims to spark further discussion and participatory action toward a more inclusive and effective healthcare system that can better recognize the complex interplay of social, economic, and environmental factors in health and health disparity. This paper identifies existing gaps in the adoption of CMS-issued Z codes and SDoH reporting in clinical trials and offers a structured pathway to bridge these gaps through targeted policy development and application. The actionable recommendations discussed above are grounded in established practices and evidence. Specifically, by proposing concrete actions such as financial incentives and regulatory mandates, this paper emphasizes the importance of policy instruments in facilitating comprehensive data capture. Importantly, the inclusion of ethical principles ensures that policies uphold patient agency, privacy, and consent, thereby promoting equitable health outcomes.
In conclusion, this paper presents a roadmap for policymakers and healthcare leaders to transform SDoH data governance through structured and evidence-based policy tools, advancing the capacity of healthcare systems to address the underlying social, economic, and environmental drivers of health disparities. While addressing specific U.S. policy contexts, this policy mapping brief also provides a framework for future cross-national comparative studies.
YL: Conceptualization, Funding acquisition, Writing – original draft, Writing – review & editing. XW: Writing – original draft, Writing – review & editing. SM: Project administration, Writing – review & editing. AQ: Writing – review & editing.
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. Research reported in this publication was supported in part by the National Institute on Minority Health and Health Disparities, National Institutes of Health (NIH), through Grant Number U24MD015970.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
1. NEJM Catalyst. Social Determinants of Health (SDOH). Care Deliv J. (2017) 3. doi: 10.1056/CAT.17.0312
2. De Lew, N, and Sommers, BD. Addressing social determinants of health in Federal Programs. JAMA Health Forum. (2022) 3:e221064. doi: 10.1001/jamahealthforum.2022.1064
3. Wilder, ME, Kulie, P, Jensen, C, Levett, P, Blanchard, J, Dominguez, LW, et al. The impact of social determinants of health on medication adherence: a systematic review and Meta-analysis. J Gen Intern Med. (2021) 36:1359–70. doi: 10.1007/s11606-020-06447-0
4. Sokol, R, Austin, A, Chandler, C, Byrum, E, Bousquette, J, Lancaster, C, et al. Screening children for social determinants of health: a systematic review. Pediatrics. (2019) 144:e20191622. doi: 10.1542/peds.2019-1622
5. Green, H, Fernandez, R, and MacPhail, C. The social determinants of health and health outcomes among adults during the COVID-19 pandemic: a systematic review. Public Health Nurs. (2021) 38:942–52. doi: 10.1111/phn.12959
6. Buitron de la Vega, P, Losi, S, Sprague Martinez, L, Bovell-Ammon, A, Garg, A, James, T, et al. Implementing an EHR-based screening and referral system to address social determinants of health in primary care. Med Care. (2019) 57:S133–9. doi: 10.1097/MLR.0000000000001029
7. Berg, K, Doktorchik, C, Quan, H, and Saini, V. Automating data collection methods in electronic health record systems: a social determinant of health (SDOH) viewpoint. Health Syst. (2023) 12:472–80. doi: 10.1080/20476965.2022.2075796
8. Fichtenberg, C, and Fraze, TK. Two questions before health care organizations plunge into addressing social risk factors. NEJM Catalyst. (2023) 4. doi: 10.1056/CAT.22.0400
9. Ngongo, WM, Peterson, J, Lipiszko, D, Gard, LA, Wright, KM, Parzuchowski, AS, et al. Examining how social risk factors are integrated into clinical settings using existing data: a scoping review. Ann Fam Med. (2023) 21:S68–74. doi: 10.1370/afm.2932
10. AHIMA Journal (2024). Practice Brief: Healthcare data governance. Available online at: https://journal.ahima.org/page/practice-brief-healthcare-data-governance-14 (Accessed June 18, 2024).
11. Bradshaw, A, Hughes, N, Vallez-Garcia, D, Chokoshvili, D, Owens, A, Hansen, C, et al. Data sharing in neurodegenerative disease research: challenges and learnings from the innovative medicines initiative public-private partnership model. Front Neurol. (2023) 14:1187095. doi: 10.3389/fneur.2023.1187095
12. Muller, SHA, Van Thiel, GJMW, Vrana, M, Mostert, M, and Van Delden, JJM. Patients’ and publics’ preferences for data-intensive Health Research governance: survey study. JMIR Hum Factors. (2022) 9:e36797. doi: 10.2196/36797
13. Wieland-Jorna, Y, Verheij, RA, Francke, AL, Tomassen, M, Houtzager, M, Joling, KJ, et al. Setting up a governance framework for secondary use of routine health data in nursing homes: development study using qualitative interviews. J Med Internet Res. (2023) 25:e38929. doi: 10.2196/38929
14. Kush, RD. Data sharing and reuse of health data for research In: RL Richesson, JE Andrews, and K Fultz Hollis, editors. Clinical Research Informatics. Cham, Switzerland: Springer International Publishing (2023). 147–67.
15. Mandreoli, F, Ferrari, D, Guidetti, V, Motta, F, and Missier, P. Real-world data mining meets clinical practice: research challenges and perspective. Front Big Data. (2022) 5:1021621. doi: 10.3389/fdata.2022.1021621
16. Milne, R, Sheehan, M, Barnes, B, Kapper, J, Lea, N, N'Dow, J, et al. A concentric circles view of health data relations facilitates understanding of sociotechnical challenges for learning health systems and the role of federated data networks. Front Big Data. (2022) 5:945739. doi: 10.3389/fdata.2022.945739
17. Mohan, G, and Chattopadhyay, S. Cost-effectiveness of leveraging social determinants of health to improve breast, cervical, and colorectal Cancer screening: a systematic review. JAMA Oncol. (2020) 6:1434–44. doi: 10.1001/jamaoncol.2020.1460
18. H1 (2023). The role of SDOH in improving patient outcomes through clinical trials. Available online at: https://h1.co/resources/the-role-of-sdoh-in-improving-patient-outcomes-through-clinical-trials/ (Accessed December 4, 2023).
19. National Academies of Sciences, Engineering, and Medicine. Integrating Social Care into the Delivery of Health Care: Moving Upstream to Improve the Nation’s Health. Washington, DC: The National Academies Press (2019).
20. George, DM, George, AE, and George, KL. Big data just got bigger: implications of real-world evidence and patient-entered data on health care and health care policy. Am J Lifestyle Med. (2020) 14:40–2. doi: 10.1177/1559827619882605
21. Liu, F, and Panagiotakos, D. Real-world data: a brief review of the methods, applications, challenges and opportunities. BMC Med Res Methodol. (2022) 22:287. doi: 10.1186/s12874-022-01768-6
22. Nahm, ES, Zhu, S, Seidl, K, Chen, L, Day, J, and Seong, H. Real-world data for interdisciplinary health care research. Adv Nurs Sci. (2023) 46:349–62. doi: 10.1097/ANS.0000000000000496
23. García-Closas, M, Ahearn, TU, Gaudet, MM, Hurson, AN, Balasubramanian, JB, Choudhury, PP, et al. Moving toward findable, accessible, interoperable, reusable practices in epidemiologic research. Am J Epidemiol. (2023) 192:995–1005. doi: 10.1093/aje/kwad040
24. Yancy, CW, Harrington, RA, and Bonow, RO. Data sharing—the time has (not yet?) come. JAMA Cardiol. (2018) 3:797–8. doi: 10.1001/jamacardio.2018.1939
25. Howlett, M. Policy tools and their role in policy formulation: dealing with procedural and substantive instruments. Handbook Policy Formul. (2017):147–167. doi: 10.4337/9781784719326.00012
26. McCormick, J In: ML Bemelmans-Videc, RC Rist, and E Vedung, editors. Carrots, Sticks & Sermons: Policy Instruments & Their Evaluation. 1st ed. Routledge, New York, NY (2017)
27. Centers for Medicare and Medicaid Services (2023). Improving the collection of social determinants of health (SDOH) data with ICD-10-CM Z codes. Available online at: https://www.cms.gov/files/document/cms-2023-omh-z-code-resource.pdf (Accessed December 14, 2023).
28. National Institutes of Health (2020). NOT-MD-21-003: notice announcing availability of data harmonization tools for social determinants of health (SDOH) via the PhenX toolkit. Available online at: https://grants.nih.gov/grants/guide/notice-files/NOT-MD-21-003.html (Accessed December 1, 2023).
29. Centers for Medicare & Medicaid Services (2023). Using Z Codes. Available online at: https://www.cms.gov/files/document/zcodes-infographic.pdf (Accessed December 1, 2023).
30. Centers for Medicare & Medicaid Services (2023). CMS issues new roadmap for states to address the social determinants of health to improve outcomes, lower costs, support state value-based care strategies | CMS. Available online at: https://www.cms.gov/newsroom/press-releases/cms-issues-new-roadmap-states-address-social-determinants-health-improve-outcomes-lower-costs (Accessed November 1, 2023).
31. PhenX (2018). Social determinants of health: Core collection. Accessed December 1, 2023. Available online at: https://www.phenxtoolkit.org/collections/view/6
32. Cook, LA, Sachs, J, and Weiskopf, NG. The quality of social determinants data in the electronic health record: a systematic review. J Am Med Inform Assoc. (2021) 29:187–96. doi: 10.1093/jamia/ocab199
33. Gillespie, C, Wilhite, JA, Hanley, K, Hardowar, K, Altshuler, L, Fisher, H, et al. Addressing social determinants of health in primary care: a quasi-experimental study using unannounced standardised patients to evaluate the impact of audit/feedback on physicians’ rates of identifying and responding to social needs. BMJ Qual Saf. (2023) 32:632–43. doi: 10.1136/bmjqs-2021-013904
34. Request for Information (RFI) (2024). Proposed use of common data elements (CDEs) for NIH-funded clinical research and trials | data science at NIH. Available online at: https://datascience.nih.gov/cde-rfi (Accessed June 18, 2024).
35. Dang, Y, Li, F, Hu, X, Keloth, VK, Zhang, M, Fu, S, et al. Systematic design and data-driven evaluation of social determinants of health ontology (SDoHO). J Am Med Inform Assoc. (2023) 30:1465–73. doi: 10.1093/jamia/ocad096
36. PhenX Toolkit (2023). Protocols. Available online at: https://www.phenxtoolkit.org/protocols/view/270401?origin=subcollection (Accessed November 12, 2023).
37. Levites Strekalova, YA, Wang, X, Sanchez, O, and Midence, S. Trends in publication and levels of social determinants of health reporting in journal of clinical and translational science from 2017 to 2023. J Clin Transl Sci. (2024) 8:e58. doi: 10.1017/cts.2024.508
38. Fafard, P, and Hoffman, SJ. Rethinking knowledge translation for public health policy. Evid Policy. (2020) 16:165–75. doi: 10.1332/174426418X15212871808802
39. Nutbeam, D, and Milat, AJ. Knowledge translation: evidence into action. Public Health Res Pract. (2017) 27. doi: 10.17061/phrp2711700
40. Cochrane Public Health Group,, Toomey, E, Wolfenden, L, Armstrong, R, Booth, D, Christensen, R, et al. Knowledge translation interventions for facilitating evidence-informed decision-making amongst health policymakers. Cochrane Database Syst Rev. (2022) 2022. doi: 10.1002/14651858.CD009181.pub2
41. Levites Strekalova, YA, Nelson, JD, Weber, HM, Wang, X, and Midence, SM. Application of the Delphi method to the development of common data elements for social drivers of health: a systematic scoping review. Transl Behav Med. (2024) 14:426–33. doi: 10.1093/tbm/ibae020
42. Breuer, E, Lee, L, De Silva, M, and Lund, C. Using theory of change to design and evaluate public health interventions: a systematic review. Implement Sci. (2015) 11:63. doi: 10.1186/s13012-016-0422-6
43. Jones, CM, Clavier, C, and Potvin, L. Adapting public policy theory for public health research: a framework to understand the development of national policies on global health. Soc Sci Med. (2017) 177:69–77. doi: 10.1016/j.socscimed.2017.01.048
44. Kaur, R, Lieberman, M, Mason, MK, Dapkins, IP, Gallager, R, Hopkins, K, et al. A feasibility and acceptability study of screening the parents/guardians of pediatric dental patients for the social determinants of health. Pilot Feasib Stud. (2023) 9:36. doi: 10.1186/s40814-023-01269-3
45. RePORTER (2023). RePORT. Available online at: https://reporter.nih.gov/search/OrmKyj7ggEC2jdSOsXZjSw/project-details/10650279 (Accessed December 13, 2023).
Keywords: social drivers of health, Z codes, PhenX toolkit, policy options, health equity
Citation: Levites Strekalova YA, Wang X, Midence S and Quarshie A (2024) Policy instruments for the governance of the social drivers of health data in clinical and research settings: a policy mapping brief. Front. Public Health. 12:1369790. doi: 10.3389/fpubh.2024.1369790
Edited by:
Joanne Taylor, The University of Newcastle, AustraliaReviewed by:
Joy D. Doll, Creighton University, United StatesCopyright © 2024 Levites Strekalova, Wang, Midence and Quarshie. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Yulia A. Levites Strekalova, eXVsaWFzQHVmbC5lZHU=
†ORCID: Yulia A. Levites Strekalova, https://orcid.org/0000-0002-6060-1233
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.