 Pengwei Yuan
Pengwei Yuan Huifang Liu2
Huifang Liu2- 1Business School, University of Jinan, Jinan, Shandong, China
- 2College of Management and Economics, Tianjin University, Tianjin, China
Infectious diseases pose a severe threat to human health and are accompanied by significant economic losses. Studies of urban outbreaks of infectious diseases are diverse. However, previous studies have neglected the identification of critical events and the evaluation of scenario-based modeling of urban infectious disease outbreak emergency management mechanisms. In this paper, we aim to conduct an empirical analysis and scenario extrapolation using a questionnaire survey of 18 experts, based on the CIA-ISM method and scenario theory, to identify the key factors influencing urban infectious disease outbreaks. Subsequently, we evaluate the effectiveness of urban infectious disease outbreak emergency management mechanisms. Finally, we compare and verify the actual situation of COVID-19 in China, drawing the following conclusions and recommendations. (1) The scenario-based urban infectious disease emergency management model can effectively replicate the development of urban infectious diseases. (2) The establishment of an emergency command center and the isolation and observation of individuals exposed to infectious diseases are crucial factors in the emergency management of urban outbreaks of infectious disease.
1 Introduction
Among public health emergencies, infectious diseases have seriously endangered human health due to their suddenness, contagiousness, epidemic nature, and unpredictability, becoming a significant public health and social problem threatening people’s health and safety. Moreover, they can lead to a range of economic and social issues. Novel infectious diseases may result in severe human casualties, substantial economic losses, and other catastrophic consequences (1). For instance, COVID-19 is wreaking havoc globally. According to the latest statistics from Hopkins University, as of May 24, 2022, Beijing time, there were 523,086,544 cumulative confirmed cases of COVID-19 and 449,678,693 cumulative deaths worldwide. A report by the Asian Development Bank suggests that the global economic damage caused by COVID-19 amounts to 5.5–8.7% of global GDP in 2020 and 3.6–6.3% in 2021. The COVID-19 Updated Assessment of Potential Economic Impacts report indicates that global employment may decline by 158 million to 242 million jobs in 2021. Global labor income may decrease from $1.2 trillion to $1.8 trillion. Additionally, uncertainty surrounding novel viral infections and treatment raises public anxiety and psychological burden, leading to mass panic (2). Misinformation and unverified information regarding COVID-19 spread rapidly on social media and traditional media (3). These social issues also pose significant challenges to national and city emergency management (4).
SRAS, H1N1, and Ebola outbreaks have provided valuable lessons in managing infectious diseases. Lin et al. summarized emergency management procedures in radiology departments during the SARS outbreak (5). Fraser and Donnelly assessed the severity of H1N1 and emphasized the need for effective health measures to combat infectious diseases (6). Brooks et al. emphasized the importance of establishing a functional incident management system (IMS) during the Ebola virus disease outbreak in West Africa (7). Chavez, Long, et al. underscored the crucial role of physicians in controlling emerging infectious diseases in cities (8). In the early stages of a new infectious disease outbreak, it is essential to follow available guidelines and strictly adhere to infection control principles (9). Zhang and Zhou encourage maintaining social distance and implementing measures based on population characteristics after a new infectious disease outbreak (10). Glass and Glass proposed tailored social distancing measures for young people and children in infectious disease contexts (11). In the event of a shortage of public health facilities and medical resources, hospitals must allocate resources equitably based on the best health outcomes, guided by local government or professional bodies (12). Societal-level measures like social isolation, blockades, border closures, and human tracking can help control COVID-19 transmission (13–15). Scenarios are dynamic model forms of events that enable changing outcomes by controlling event likelihood, providing decision-makers with tools to synthesize trends and events into manageable options. They add value to traditional planning techniques (16). Previous studies overlooked the interaction between emergency management elements in reducing urban infectious disease impacts, neglecting scenario-based assessments of urban infectious disease outbreaks, despite their applicability to novel infectious diseases.
This paper aims to address two main questions: What are the relationships between key events in urban outbreak emergency management of infectious diseases, and how do these interactions impact the effectiveness of urban infectious disease emergency management across different scenarios? Additionally, how can practical and effective suggestions be provided for emergency management decision-makers? To tackle these issues, key events in urban infectious disease outbreaks were identified. The paper employs the CIA, ISM, and Delphi methods to establish a scenario-based assessment model for urban infectious disease emergency management. Subsequently, interactions were analyzed, and urban emergency management was simulated under various scenarios to assess the impact of emerging infectious diseases on economic loss, human casualties, disease control, and public trust. Finally, an evaluation of Wuhan, China’s emergency management response to COVID-19, an urban emerging infectious disease, was conducted. The contributions of this paper compared to existing studies include: (1) Extraction of key events for emergency management of emerging urban infectious diseases and clarification of interrelationships among actual events related to urban infectious diseases. (2) Proposal of an integrated model for scenario analysis by combining the CIA, ISM, and Delphi methods. (3) The model’s ability to evaluate the effectiveness of urban infectious disease emergency management and provide proven recommendations for decision-makers through scenario analysis and extrapolation of urban infectious disease development.
2 Literature review
Research on emergency management of infectious diseases has primarily focused on preparedness, transmission modeling, economic loss assessment, and the societal impact of outbreaks. Brouqui et al. developed an infectious disease control framework for managing outbreaks (17). Wong et al. examined emergency preparedness for SARS and avian influenza in Hong Kong and proposed new public health management measures (18). The CDC has implemented measures to address EBOV spread, including monitoring travelers from affected areas and assessing hospital capacities (19). Effective collaboration among medical personnel and sufficient medical resources are crucial in emergency management. Therefore, it is essential to provide a safe working environment, adequate food, rest, and psychological support for healthcare workers globally (20). Lam et al. analyzed the challenges of guideline implementation and emergency management in acute care settings (21). Huang et al. outlined emergency management and infection control strategies in the radiology department, resulting in zero COVID-19 infections among staff (22).
In developing infectious disease transmission models, Kucharski et al. used SARS-CoV-2 transmission data from Wuhan in 2019 to show that regional closures reduce transmission, but delayed closures may lead to widespread outbreaks (23). Wu and Leung utilized exported case data to model outbreaks in major Chinese cities, indicating inevitable global outbreaks in urban centers (24). Razavi-Shearer et al. estimated regional HBV prevalence using a dynamic transmission model in the context of childhood vaccination (25). Chang et al. simulated SARS-CoV-2 spread in 10 United States cities, highlighting mobility’s role in increased infection rates and economic losses (26). Musa et al. modeled COVID-19 transmission and mortality, suggesting that a combination of social distancing and vaccination could reduce mortality in South America (27).
COVID-19 poses significant threats to economic development, social systems, and human life, instigating concerns about potential economic crises or recessions. Kim and Loayza argue that, compared to high-income countries, the benefit governments in low-income nations gain from not intervening in epidemic prevention measures is marginal (28). Maria and Zaid Alsafi provide an overview of COVID-19’s impact on various aspects of the global economy (1, 29).
The array of social crises resulting from infectious diseases should not be underestimated, with panic being a prevalent psychological response to new outbreaks. How governments assess and address public panic can significantly influence the effectiveness of infectious disease emergency management mechanisms (30). A panic-induced rush for supplies is highly probable, underscoring the importance of maintaining adequate supplies during significant public health events (31, 32). Wang et al. utilized the DASS-21 model to evaluate the psychological status of 1738 individuals in China, emphasizing the need to focus on case escalation, promote proper coping mechanisms, and enhance personal protection in response to COVID-19 (33). Rumors often stem from panic, hindering emergency management efforts by spreading misinformation (34). Hui et al. developed a rumor propagation model based on infectious disease models, suggesting effective strategies to counteract the spread of COVID-19 rumors (35). Ning et al. underscore the importance of authoritative announcements in dispelling rumors and mitigating their impact during the early months of the COVID-19 outbreak in China (36). Individuals seek to minimize losses and avert catastrophic consequences through pivotal decisions (37).
While most studies have examined the impact of individual events or factors, emergency management responses to a single factor may prove less effective when multiple events or factors interact. To ensure reliable and effective emergency management of urban COVID-19 outbreaks, management strategies must consider the cross-influences among various factors. The scenario-based approach assesses interactions between critical events within a specified timeframe (38), enhancing managers’ understanding of the factors involved in developing COVID-19 contingency plans and the response measures required. When integrated with other predictive models, scenario models offer flexible approaches to address uncertainty. This paper examines potential future trends in urban infectious disease outbreaks, identifies key factors, and proposes optimal decisions.
3 Research methodology
3.1 Basis of the scenario approach
The scenario-based emergency management model for urban outbreaks of infectious diseases combines the Delphi method, the cross-influence approach (CIA), and the Interpretative Structural Model (ISM). Its purpose is to analyze scenarios and interpret the progression of urban infectious disease outbreaks. The Delphi method and CIA enable the analysis of factors influencing urban outbreaks. CIA identifies relationships between events affecting outcomes, enhancing the stability of identified events. However, using CIA requires presenting a series of interrelated future events. A team of experts conducts a Delphi process to predict event occurrence based on inputs, jointly assessing cross-impacts.
3.2 Creation of event set
Creating the COVID-19 event set is based on observing and studying historical infectious disease cases. Addressing significant health events necessitates considering technical and social factors and obtaining input from experts with diverse experiences and perspectives. This approach aims to identify critical factors and relationships, ensuring decision-making rationality, internal consistency, and usefulness. A comprehensive set of 32 relevant events was selected and categorized into three types. Initial events (ICi): These events occur or not before infectious disease outbreaks. They may reflect emergency management of urban outbreaks, significantly impacting disease development. Experts subjectively estimate initial event probabilities at 0.5. If an event with a probability below 0.5 is anticipated, experts reassess other events’ probabilities.
IC1: Infectious disease isolation and treatment capacity: The city can isolate and treat patients with infectious diseases.
IC2: Infectious disease source detection capability: The city can quickly conduct rapid detection of the cause of the disease.
IC3: Infectious disease infectivity assessment: The city can quickly assess the infectious characteristics or transmission routes of infectious diseases.
IC4: Medical treatment.
IC5: Government emergency response plan: The city has an excellent emergency response plan for infectious diseases.
IC6: Government emergency response capability: The city has an infectious disease control agency, conducts frequent emergency drills, and has good response capability.
IC7: Public self-protection ability: The public knows the general knowledge of infectious diseases and has good self-protection ability.
IC8: Government communication capability: Have internal communication procedures and public communication plans and channels.
IC9: Public trust: The public trusts the government and complies with government emergency instructions.
IC10: Vaccine: There is no vaccine for infectious disease.
Dynamic events (DEi) encompass post-epidemic occurrences, primarily consisting of government emergency management measures and events triggering secondary disasters. These events are assigned a probability of occurrence of 0.5.
DE1: Infectious disease patient treatment: Infectious disease patients are isolated and treated.
DE2: Causal cause identification: The infectious disease causative agent (bacteria, virus) is rapidly identified.
DE3: Infectious disease transmissibility assessment: The transmission route and transmissibility of infectious diseases are rapidly assessed.
DE4: Decontamination action: Disinfect the patient’s activity area after infection.
DE5: Isolate the contacts: Isolate and observe people who are exposed to infectious diseases.
DE6: Leaders do not agree to release information: Local heads do not agree to inform the public about the status of the infectious disease.
DE7: Information leak: Social media leaks information about the infectious disease to the public.
DE8: Emergency command center established: The government establishes an emergency command center and declares a state of emergency.
DE9: Public panic: The public panics and either rushes to buy supplies or leaves the city by transportation if possible.
DE10: Rumors spread: Various rumors appear on the Internet and social software.
DE11: Spread of infectious diseases: Infectious diseases spread among the population.
DE12: Restriction of movement of people: The government restricts the movement and gathering of people.
DE13: Communicating infectious diseases: The government communicates about infectious diseases through the media and widely publicizes the hazards and protection. The government calls on and organizes businesses, non-profit organizations, and individuals for infectious disease prevention and control.
DE14: Emergency medical supplies are distributed to organizations and people in need promptly.
DE15: Some healthcare workers do not cooperate: Some healthcare workers or emergency managers refuse to work on infectious diseases because of a lack of protective materials or fear of being infected.
DE16: Some members of the public do not cooperate: Some people do not comply with government measures for epidemic prevention.
DE17: Area closure: Other cities restrict the entry of people from that city, and people from that city are not allowed to leave the city.
DE18: Development of effective drugs/vaccines: Effective types of existing drugs are proposed, vaccines are developed, and mass production is carried out.
Outcome event (OEi) encompasses various consequences that may arise from an infectious disease event, such as casualties and property damage. The probability of an outcome event is determined accurately at the end of the period, with an initial probability also set to 0.5.
OE1: Economic loss: GDP loss caused by infectious diseases.
OE2: Personnel Casualties: a certain number of infectious disease patients die.
OE3: Infectious disease is controlled: The city’s Infectious disease is controlled in a phased manner, and the number of sick people gradually decreases without spreading to other cities or regions.
OE4: Public trust: The public has a high level of trust in the local government after the epidemic and continues cooperating with the government in its actions.
Expert estimates of the relationship between the three-event sets (initial conditions, dynamic events, and outcome events) were sought.
3.3 Scenario analysis
Eighteen experts in emergency management and frontline rescue were invited to participate in the expert panel. They assessed whether each of the three event sets occurred and estimated the probability of other events happening. Due to the diverse nature of each event, the panel had to make 478 causality estimates, as illustrated in Figure 1.
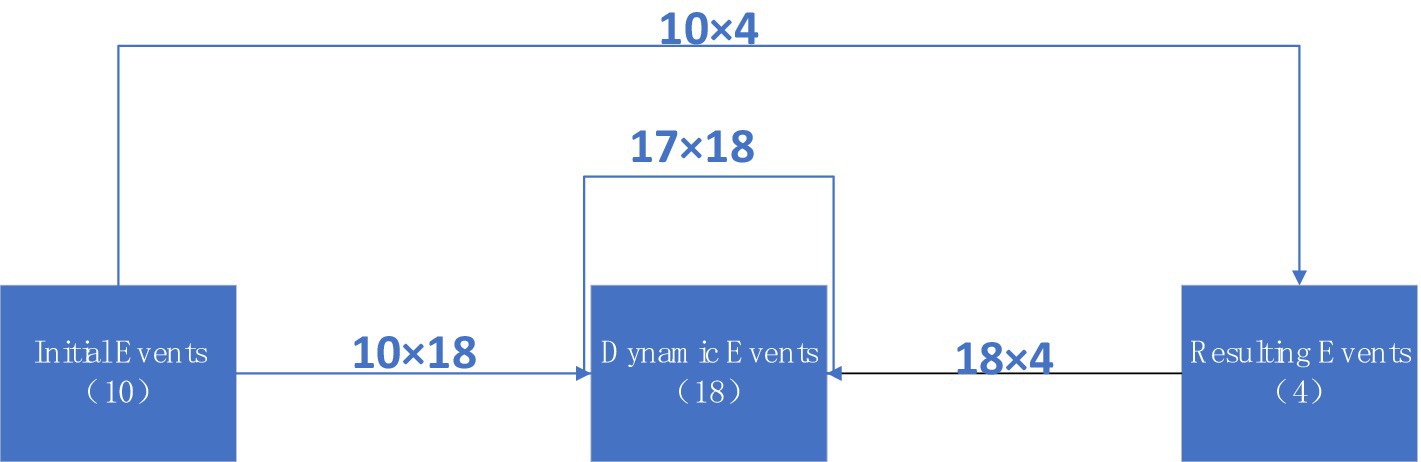
Figure 1. Influence diagram of the number of three event sets and the number of estimates required.
Events within a set are interconnected. However, in the Delphi method, the occurrence or non-occurrence of one event does not impact others in the set. Therefore, we integrated the CIA into the ISM and used it to obtain the three event sets of COVID-19 as input for the ISM. The most critical aspect of CIA-ISM is “structural modeling.” The ISM approach provides a solid mathematical foundation for establishing linear relationships between critical events and their influencing factors. Initially, experts estimate the relationships and probabilities between events. Then, a model is constructed to reflect the complex relationships over time, with the flexibility to receive feedback at different stages, enabling experts to adjust inputs as needed.
The occurrence probability of event i, influenced by event j, follows the rule outlined in Table 1, known as the scoring table. A valid factor metric between i and j is established when at least two-thirds of the individual interaction estimates fall within an interval in the scoring table. The resulting adjacency matrix serves as input for the CIA, where cells represent the linear influence factor of event i on j, denoted as Rij. Diagonal cells indicate the total probability. Using this binary matrix, we can forecast scenarios by assuming event i’s occurrence (or non-occurrence).
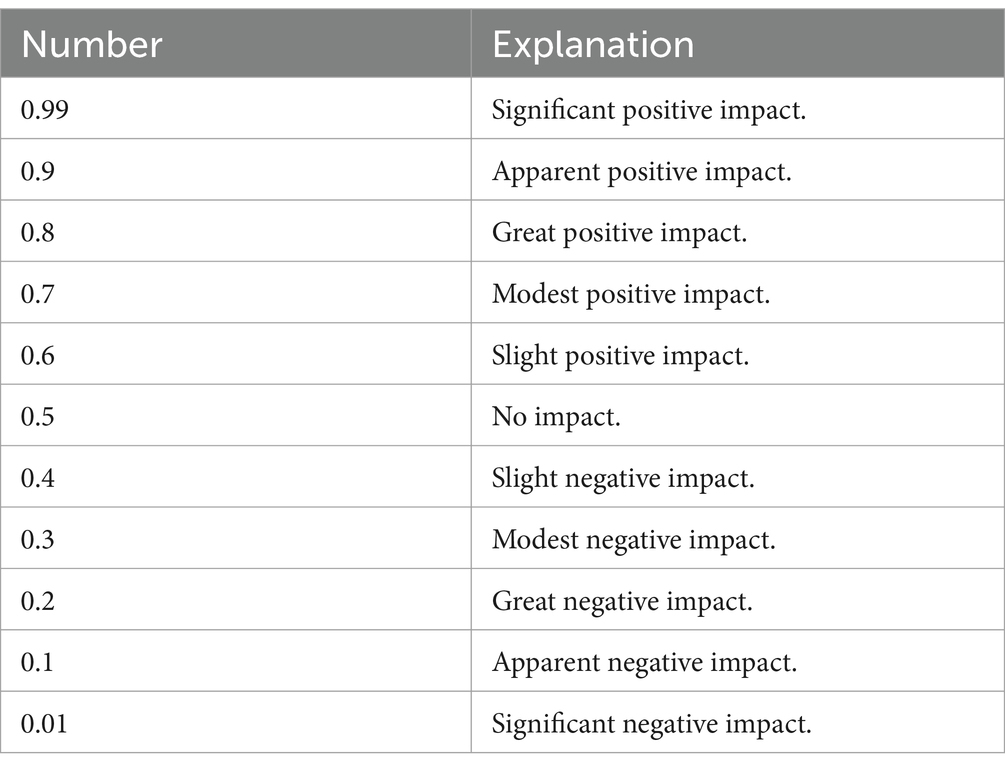
Table 1. Rating scale.
3.4 Cross-impact analysis
In Table 1, a mathematical “+” denotes event facilitation, while a mathematical “-” signifies suppression. These symbols only show the impact’s direction and do not denote magnitude. Equations 1, 2 represents the cross-influence factor and event occurrence probability.
where Gi is the sum of the effects of all possible external events on the event i that are not explicitly represented in the n events included in the model. To obtain a numerical estimate of the total variability in the matrix, we examined the following linear sum of the cross-impact factorΣ|Cij|.
|internal event impact| = Σ|Cij| = 683.8245761.
|initial event impact| = Σ|Cij| = 293.4260838.
|Dynamic event impact| = |internal event impact|-|initial event impact| = Σ|Cij|-Σ|Cij| = 535.9788616.
|External unspecified event impact| = Σ|Cij| = 186.593908.
|Total impact| = |internal event impact| + |external unspecified event impact| = Σ|Cij| + Σ|Cij| = 870.4184841.
Calculate the relative fraction or percentage of impact due to each type of event.
|Dynamic event impact|/|Total impact| = 0.615771461.
|initial event impact|/|total impact| = 0.337109206.
|External unspecified event impact|/|Total impact| = 0.21437264.
Thus, unspecified events (external event impact) contribute to 21.44% of the overall impact, while dynamic events and initial conditions contribute 61.58 and 33.71%, respectively. In total, 78.56% of the impact in the model is attributed to explicit events. This suggests that the event set is relatively comprehensive, rendering the model feasible.
After deriving the cross-impact matrix, we delineate the strong relationships within the directed graph model by partitioning and extracting the matrix model. By employing the CIA-ISM method, we can illustrate the anticipated scenario using a directed graph. Table 2 outlines the direct and indirect effects of each event on the outcome events (cascade effects). The model suggests that event DE1 may either positively impact favorable outcomes or negatively influence adverse outcomes. IC6, IC8, and IC9 directly negatively impact DE15, indicating that government emergency response capacity, establishment of emergency command centers, and public trust can significantly decrease the likelihood of partial health care worker non-cooperation. Similarly, IC2, IC7, and DE2 directly negatively influence DE16, signifying that enhancing infectious disease source detection capabilities, information disclosure, and causation identification would markedly diminish the probability of partial public non-cooperation.
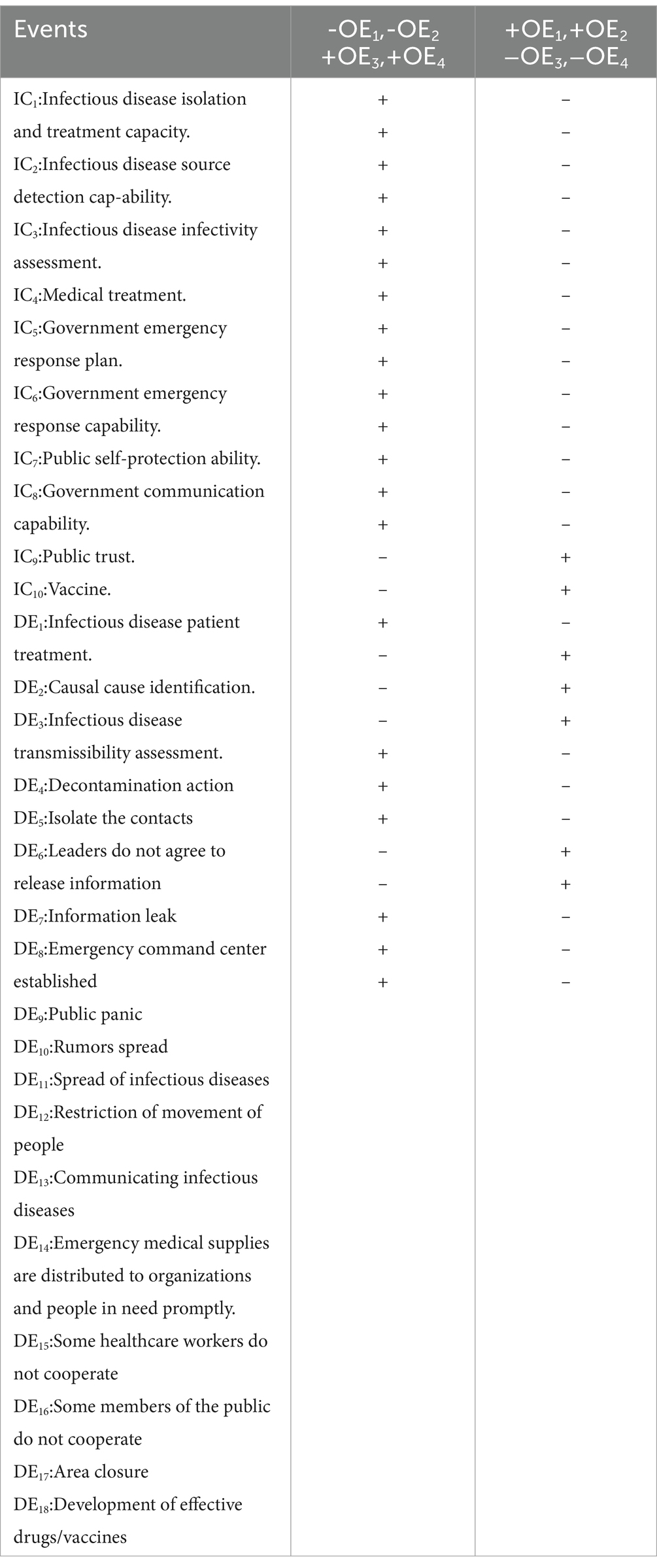
Table 2. Outcome events analysis.
Among all emergency response efforts, the establishment of an emergency command center (DE8) has a direct and significant impact on reducing economic losses (OE1), controlling infectious diseases (OE3), and increasing public trust (OE4). Limiting the movement of people (DE12) made a considerable contribution to increasing public trust (OE4). Among all secondary-derived disasters, the spread of infectious diseases (DE11) directly and significantly impacts human casualties (OE2).
Analyzing outcome events can be enhanced by considering the direct impact of initial conditions and dynamic events on these specific outcomes, as shown in Tables 3–6. For instance, Table 3 demonstrates that the model anticipates leadership disagreement in releasing information, while partial public non-cooperation emerges as the primary precursor to potential economic loss. Conversely, establishing an emergency command center, evaluating infectious disease transmission capacity, and implementing a government contingency plan markedly diminish the probability of such an outcome.
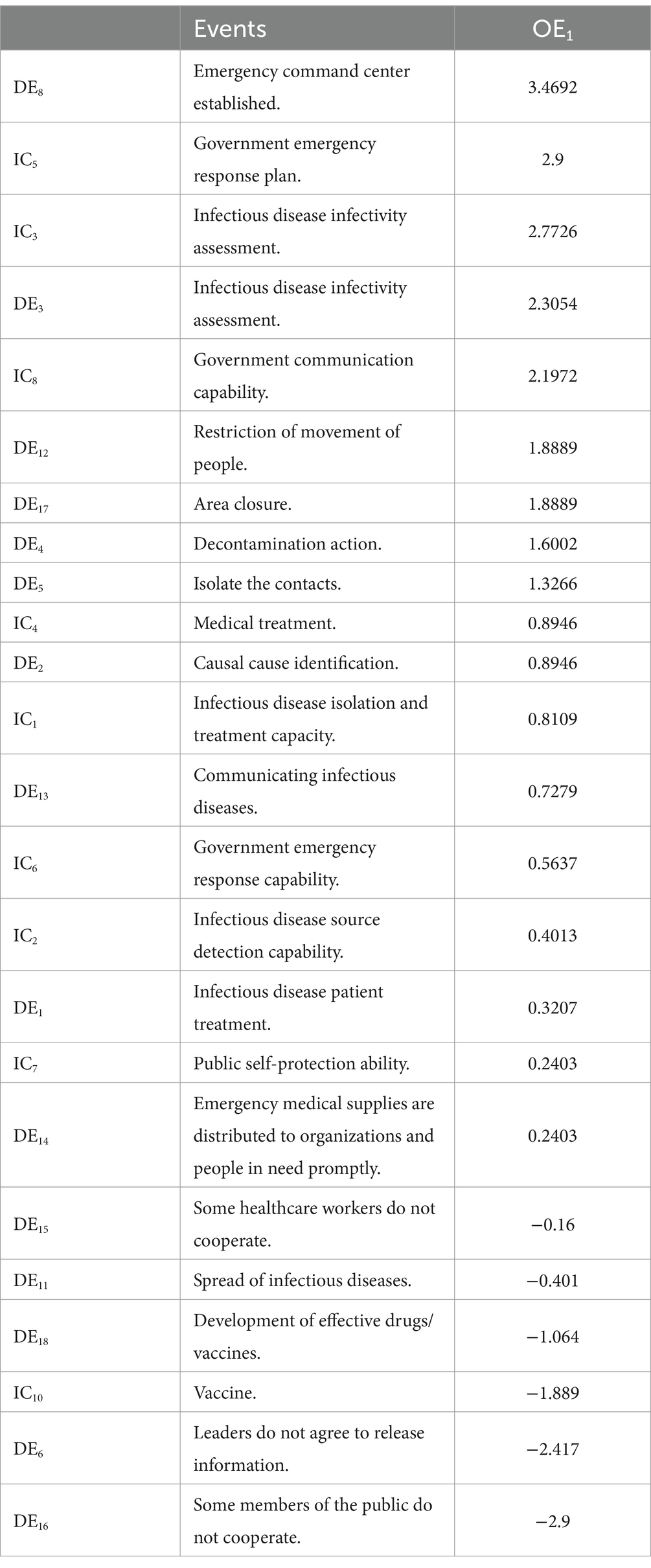
Table 3. OE1 ordered influences table.

Table 4. OE2 ordered influences table.
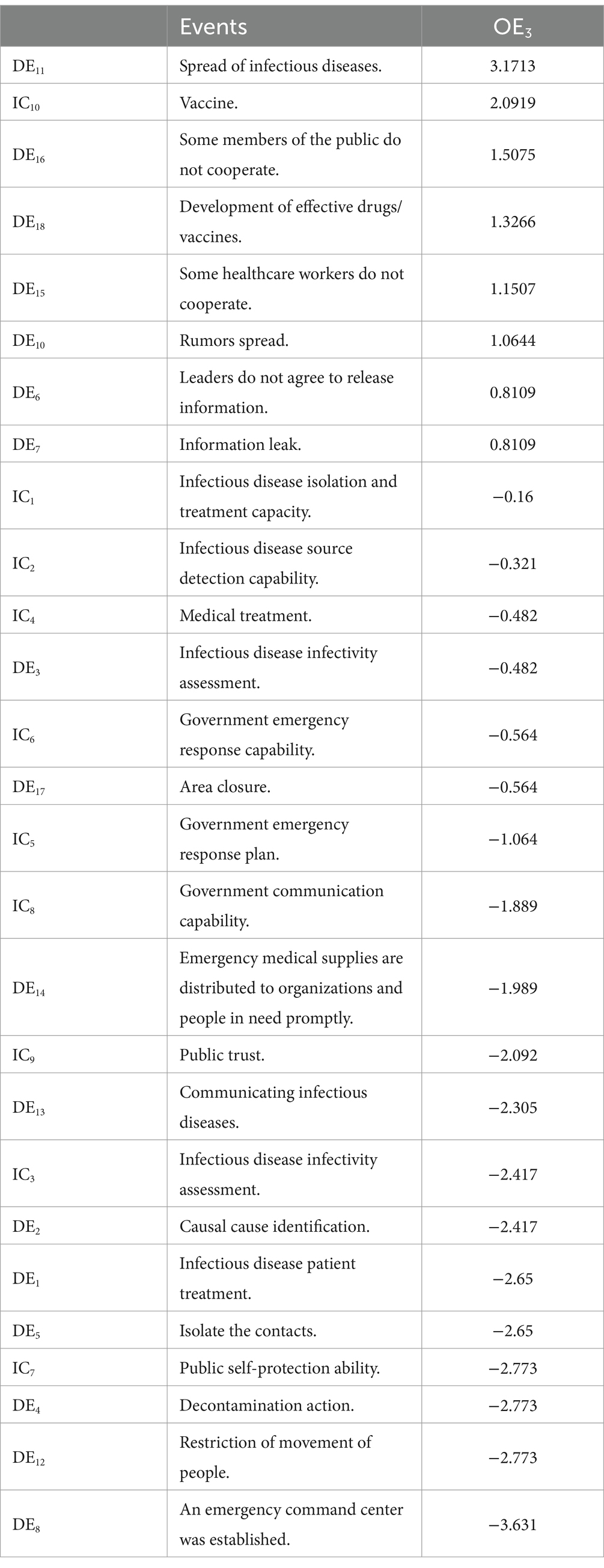
Table 5. OE3 ordered influences table.
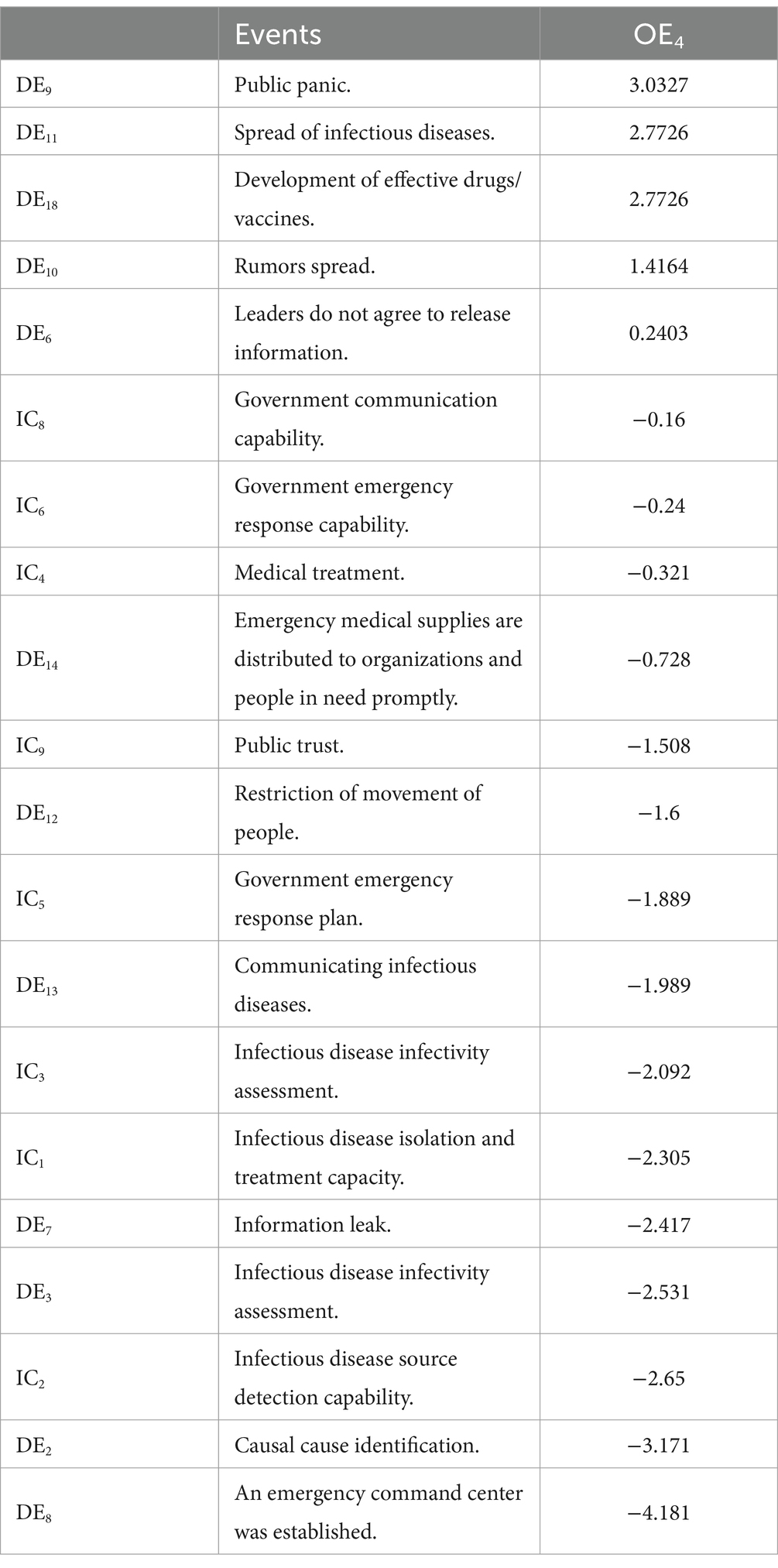
Table 6. OE4 ordered influences table.
We enumerate the events that directly influence the outcome event, whether positively or negatively. Conversely, critical factors influencing the containment of infectious diseases and fostering public trust included establishing an emergency command center, identifying the causative agent, and limiting people’s movement (see Tables 5, 6). Conversely, factors such as infection spread, public panic, and vaccine unavailability hindered these desired outcomes.
Tables 3–6 present the key events influencing the occurrence or absence of each of the four outcomes. The values in Table 7 are calculated by summing the absolute positive impacts of Cij on the events. Table 8 displays the most significant events contributing to adverse outcomes. The weights presented indicate the cumulative adverse impact, represented by the sum of the absolute negative impacts of Cij on the events.
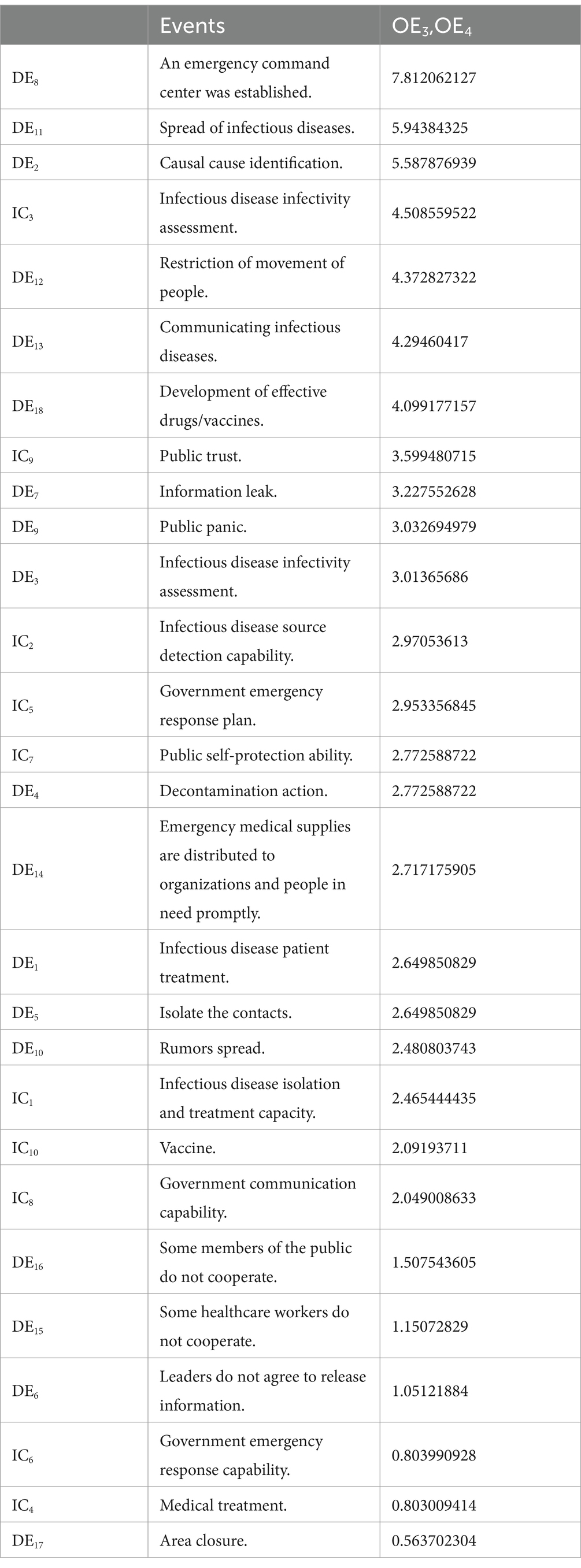
Table 7. Total impact on positive events.
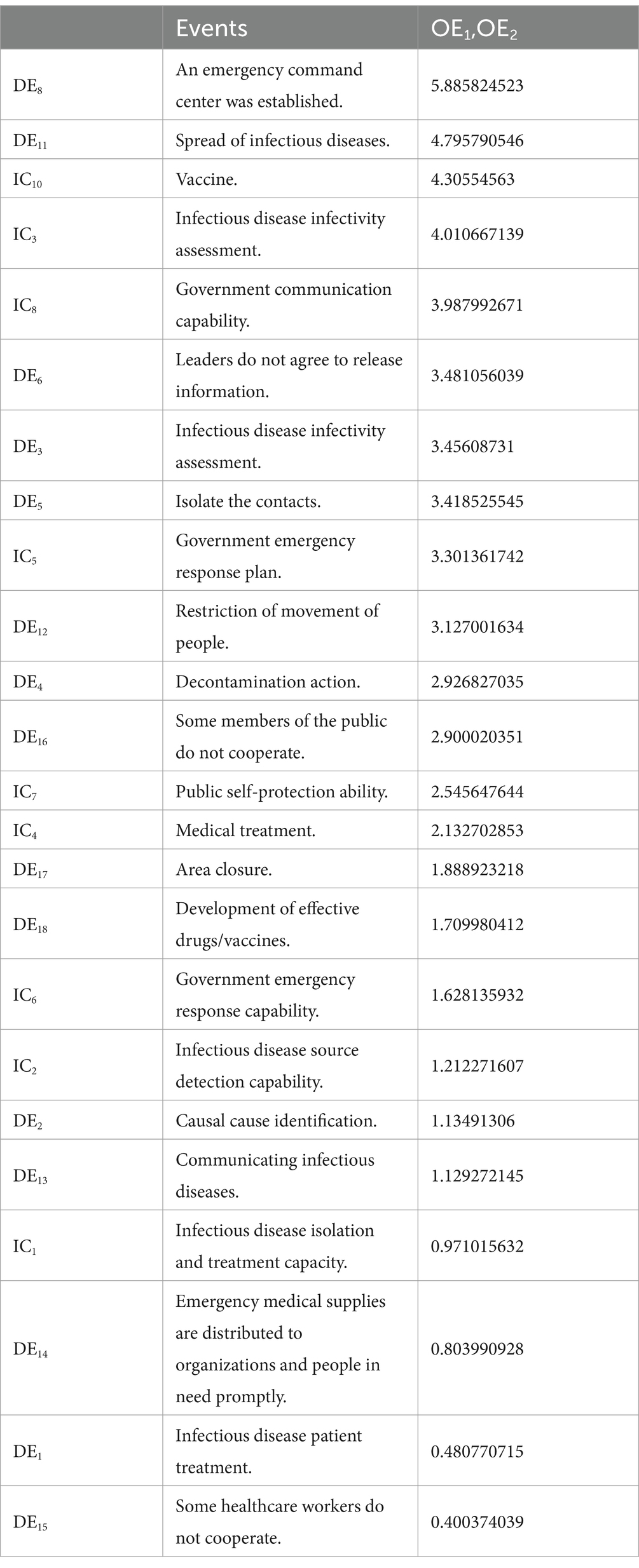
Table 8. Total impact on negative events.
3.5 Incremental analysis
We conduct incremental analysis on the predicted scenarios to comprehend the relationships among different events. The primary approach involves analyzing the distribution of |Cij|. Non-zero |Cij| values are selected, and a histogram illustrating their frequency from zero to the maximum absolute value is plotted, as depicted in Figure 2.
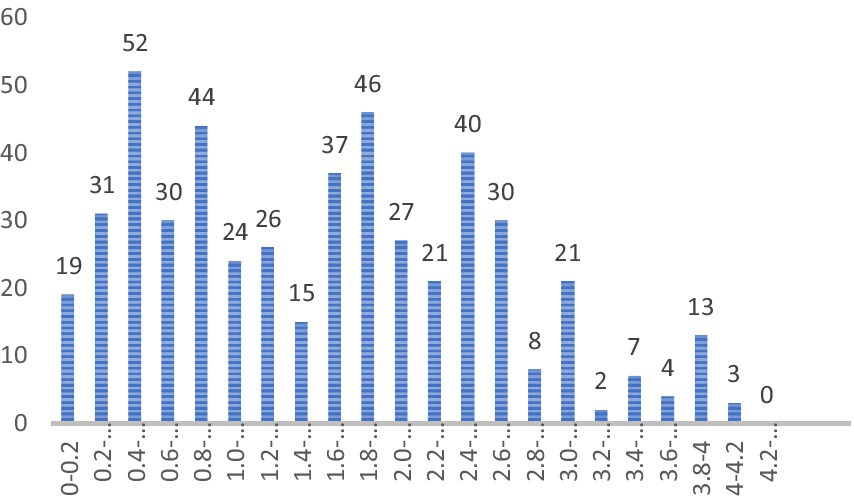
Figure 2. Histogram of |Cij|.
Subsequently, we identify the value of |Cij| representing the highest k% of the distribution as the cut-off point for the directed graph. For instance, selecting 90 and 85% as the cut-off points results in the directed graph highlighting the top 10 and 15% impacts, as illustrated in Figures 3, 4. Lines connecting events of the same color denote positive impacts, while those connecting events of different colors signify negative impacts.
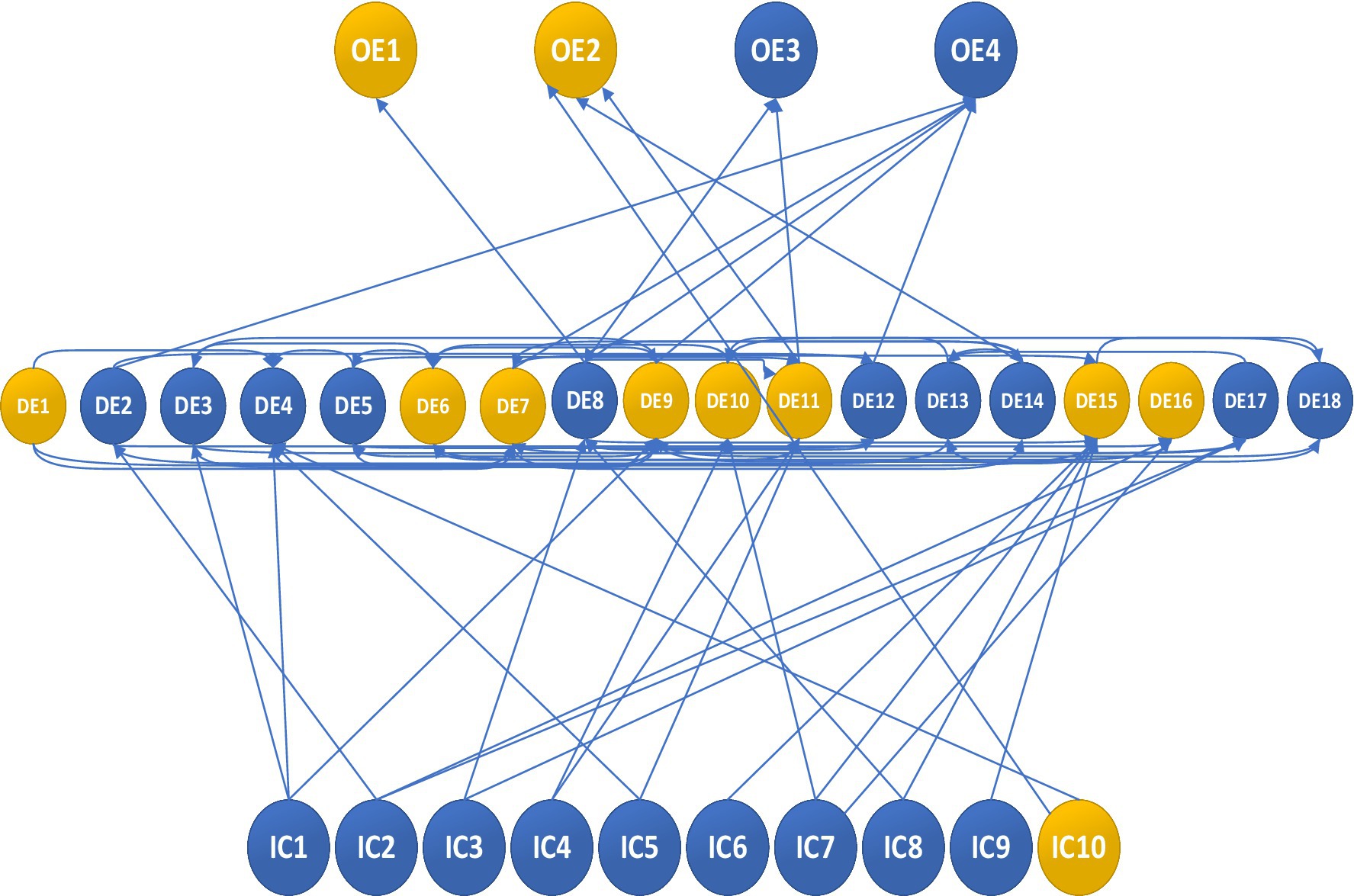
Figure 3. Digraph for the limit value |Cij| = 2.93 – with 15%.
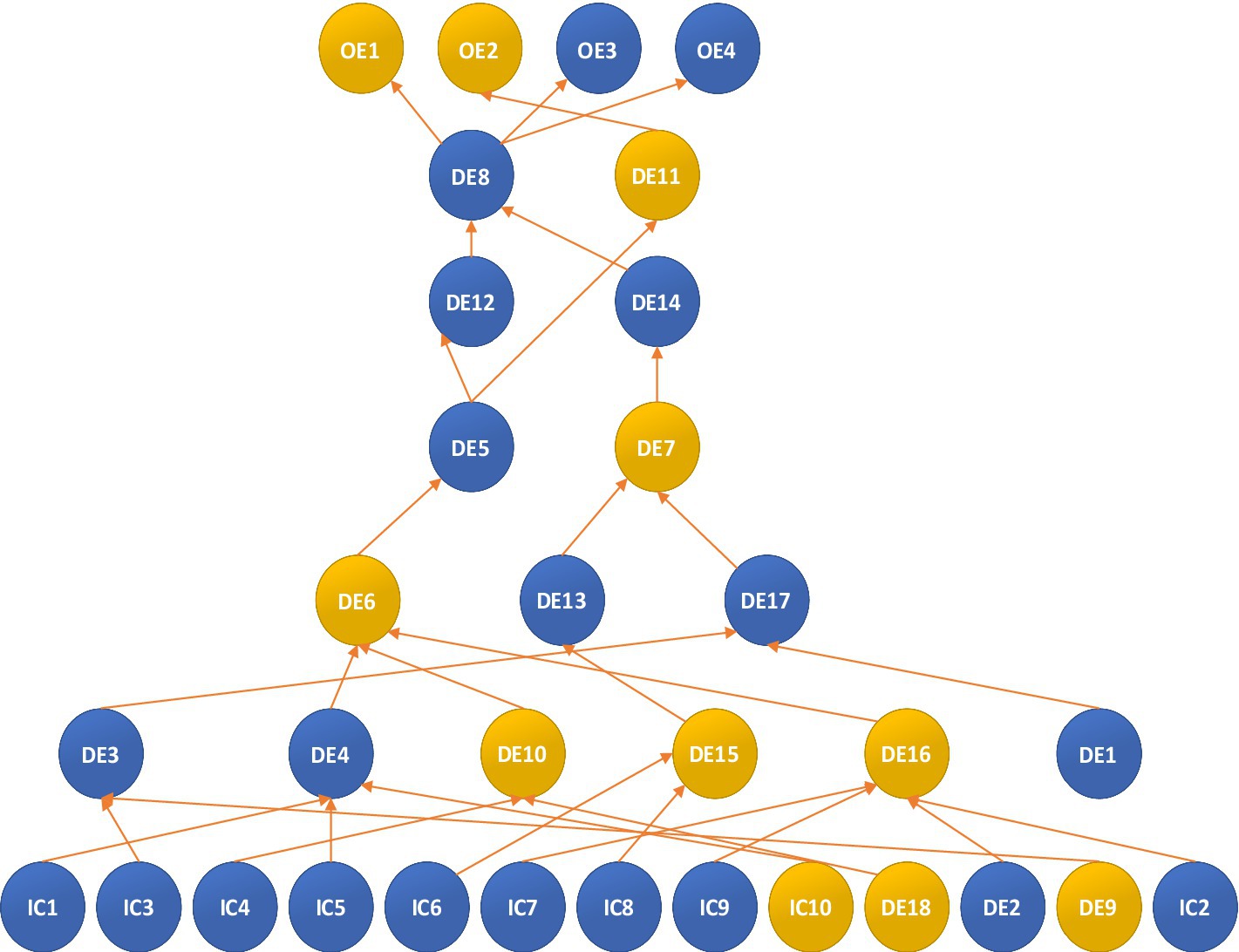
Figure 4. Digraph for the limit value |Cij| = 3.42 – with 5%.
The graph is directed, with the highest 85% of the distribution value determining its structure. At this analytical level, while all events are included, the logical sequence of events is not organized. To refine the model, additional |Cij| factors were integrated into the analysis, considering all |Cij| values greater than or equal to this threshold to establish the final model. At this stage, the |Cij| value of event i is utilized before or after the occurrence and non-occurrence of event j. The histogram of cross-influencing factors indicates that the limit value is |Cij| = 3.42 when extracting the most significant influence of the top 5%. Subsequently, the CIA-ISM output is displayed in Figure 4, with its adversarial plot depicted in Figure 5. If the value of |Cij| equals or surpasses the limit value, a direct connection from node j to node i is established. Identifying the most critical event in the event set through the limit value aids in comprehending the underlying logic of the particular influence path and scenario leading to that outcome, while also facilitating an understanding of the event sequence and its potential impact.
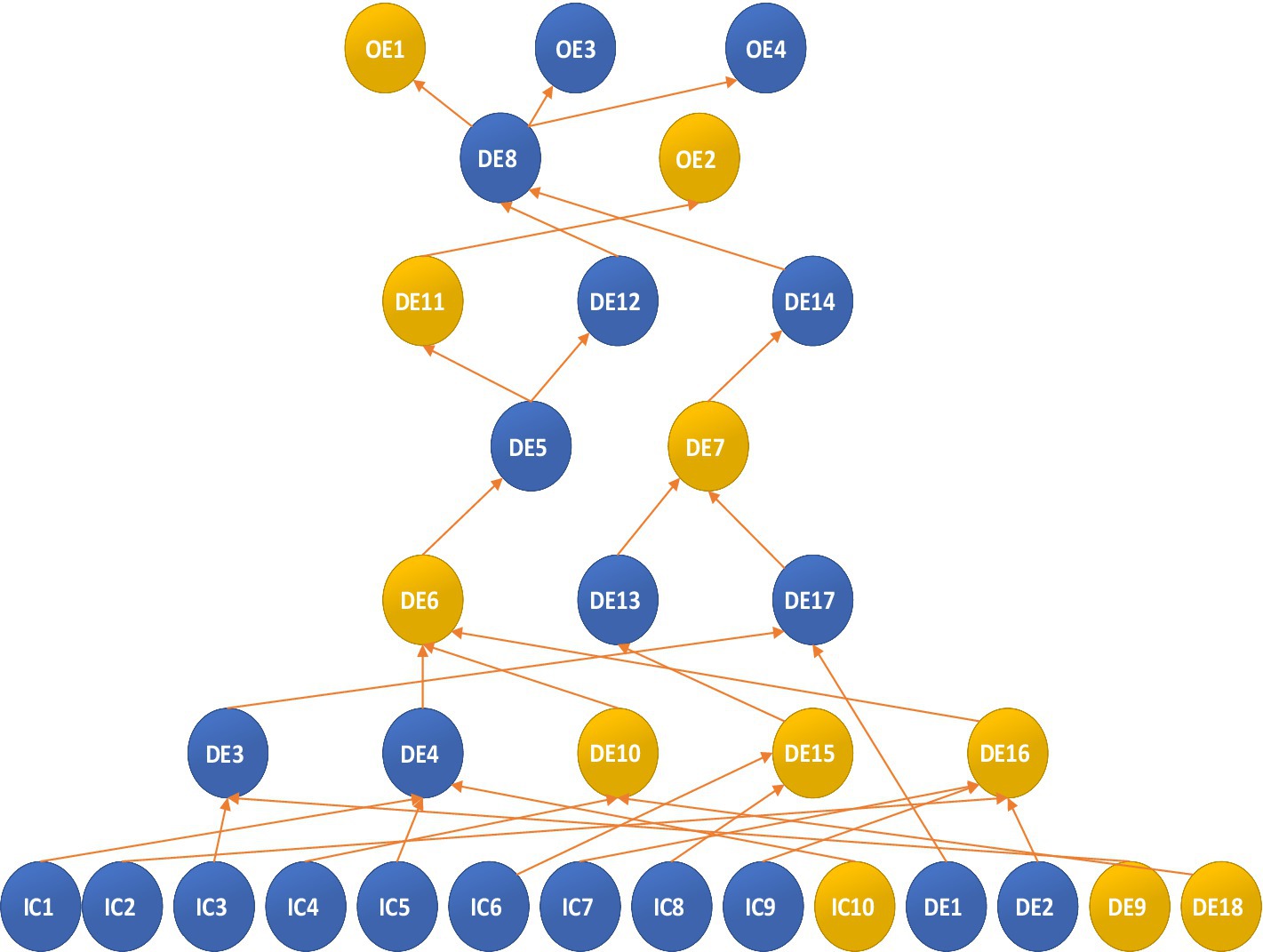
Figure 5. Digraph for the limit value |Cij| = 3.42 – with 5%.
The figure illustrates that vaccines (IC10), capacity for infectious disease isolation and treatment (IC1), medical resource reserves (IC4), government contingency plans (IC5), public trust (IC9), government emergency response capacity (IC6), government communication capacity (IC8), public self-protection (IC7), infectious disease source detection (IC2), and assessment of infectious disease transmission capacity (IC3) trigger a series of dynamic events (DE4, DE9, DE14, DE8, DE15, DE13, DE7, DE6, DE16, DE5, DE11), which decrease the likelihood of death (OE2) and increase the chances of infectious disease control (OE3) and public trust (OE4). Prompt treatment of infected patients (DE1) directly limits movement restrictions (DE17), while vaccine shortages (IC10) negatively impact decontamination efforts (DE4), emphasizing the need for active vaccine development within decontamination measures (DE4). Enhancing the capacity for isolating and treating infectious diseases (IC1), developing government contingency plans (IC5), and creating effective vaccines against novel viruses (IC10) will greatly benefit decontamination operations (DE4). Insufficient medical resource reserves (IC4) and the absence of effective vaccines against novel viruses (IC18) will lead to the spread of rumors (DE10). Reduced public panic (DE9) and low infectious disease transmission capacity (IC3) would significantly improve the assessment of infectious disease transmission capacity (DE3). Strong public trust (IC9), high levels of infectious disease source detection (IC2), effective causative agent identification (DE2), and improved public self-protection (IC7) will notably decrease the likelihood of partial public non-cooperation (DE16). Effective government emergency response (IC6) and communication (IC8) will effectively mitigate non-cooperation among healthcare workers (DE15). Ineffective decontamination operations (DE4), partial public cooperation (DE16), and rumor dissemination (DE10) positively influence leaders’ consent to release information (DE6), suggesting that efficient decontamination operations (DE4), reduced rumor dissemination (DE10), and partial public non-cooperation (DE16) will likely prevent leaders from withholding information (DE6). Assessing infectious disease transmission capacity (DE3) and treating infectious disease patients (DE1) directly impact regional closure (DE17), whereas partial non-cooperation among healthcare workers (DE15) directly affects infectious disease communication (DE13). Disagreement among leaders regarding information release (DE6) directly hinders the implementation of contact isolation (DE5). Regional closure (DE17) and disease communication (DE13) directly decrease the likelihood of information leakage (DE7). Information leakage (DE7) significantly hampers the timely distribution of emergency medical supplies to those in need (DE14). Contact isolation (DE5) not only directly restricts people’s movement (DE12) but also acts as a deterrent to the spread of infectious diseases (DE11). Restricting people’s movement (DE12) and timely distribution of emergency medical supplies (DE14) facilitate the establishment of an emergency command center (DE8), which, in turn, increases the likelihood of disease control (OE3), public trust (OE4), and reduces economic losses (OE1). The diminished impact of contact isolation (DE5) on disease spread (DE11) directly decreases the likelihood of personnel casualties (OE2).
3.6 Sensitivity analysis
This paper aims to model the emergency management of urban infectious disease outbreaks, so the associated events are selected for sensitivity analysis. The impact of critical factors is tested by varying the initial probabilities.
3.6.1 Initial conditions analysis
Based on the preceding analysis, it is evident that IC4, 5, 6, and 8 are events pertinent to emergency management. Sensitivity analysis scrutinizes the outcomes of other events, particularly outcome events, by modifying the initial probabilities of these four events. We establish six scenarios to forecast occurrences where all four crucial events manifest, all fail to occur, and only one materializes. The initial probability of other events is set at 0.5. Utilizing formula (1, 2), we derive the probability of other events occurring across the six scenarios, as presented in Table 9. Economic loss (OE1) is influenced by the initial events in the descending order of IC6, IC5, IC8, and IC4. The government’s emergency response capability (IC6) plays a pivotal role in mitigating economic loss.
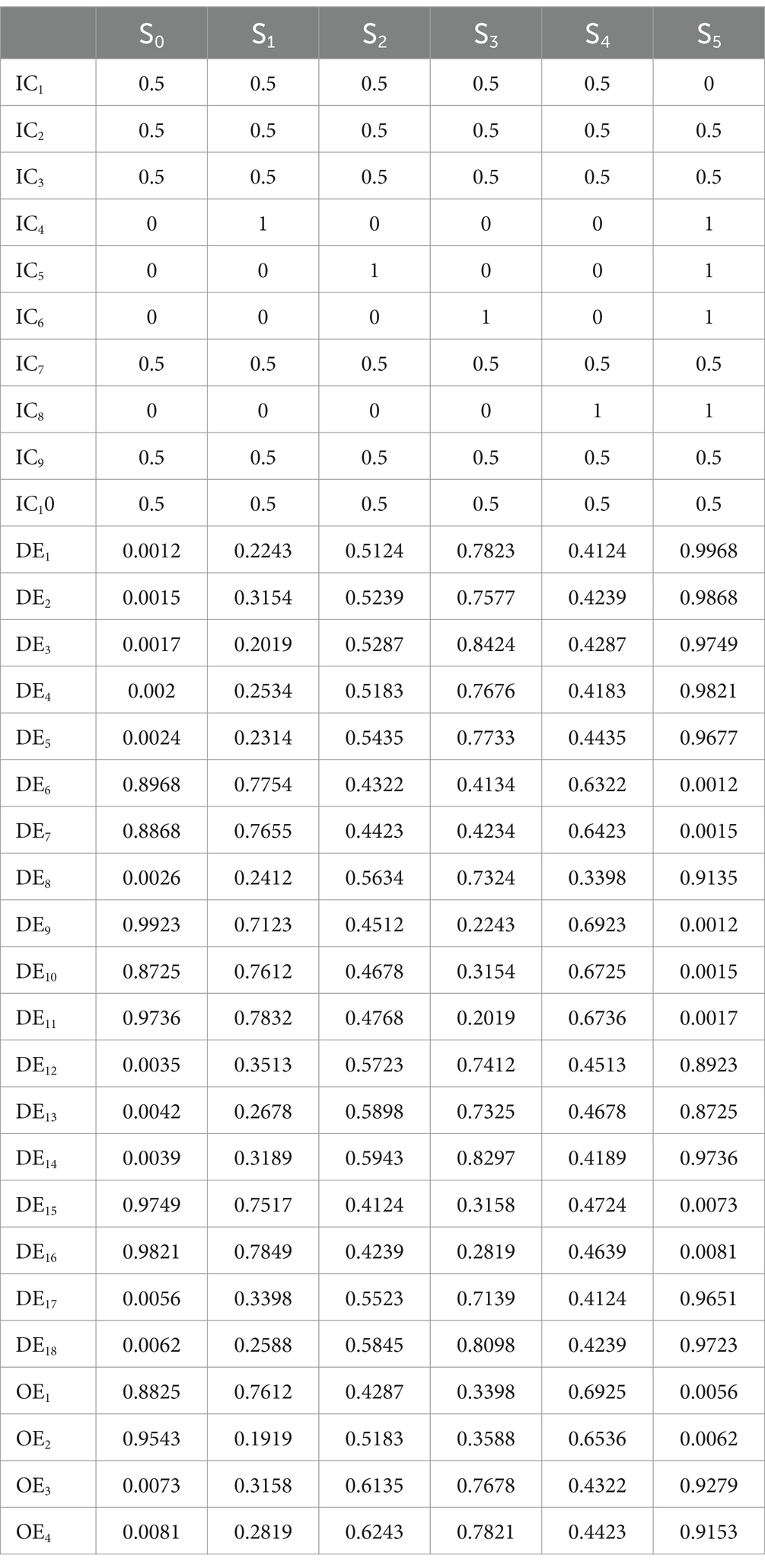
Table 9. Prediction probabilities of the other events in initial conditions analysis.
The government must regularly update its contingency plan for urban infectious disease outbreaks (IC5), assess medical resource reserves (IC4), and promote public awareness of epidemic resistance. Among the four critical events, IC4 significantly decreases casualties (OE2). Therefore, it is crucial for priority hospitals and treatment facilities to maintain sufficient medical resource reserves (IC4) and enhance government emergency response capacity (IC6). A robust government emergency response plan (IC5) is pivotal in bolstering public confidence and fostering public trust (OE3). Collectively, these four initial conditions can greatly mitigate losses, underscoring the need for adequate emergency preparedness to address the human fatalities and economic ramifications associated with COVID-19.
3.6.2 Analysis of dynamic events
The analysis above indicates that dynamic events related to emergency management include DE5, 8, 11, 12, and 14. The impact of these pivotal events can be similarly assessed, as depicted in Tables 10, 11. The establishment of an emergency command center (DE8) significantly reduces economic losses (OE1). Implementation of personnel isolation measures (DE5) can also mitigate economic loss (OE2). While individually, none of these six dynamic events critically affects the four outcome events, their combined effect can be substantial. Therefore, we explored several scenarios (S6, 7, 8, and 9).
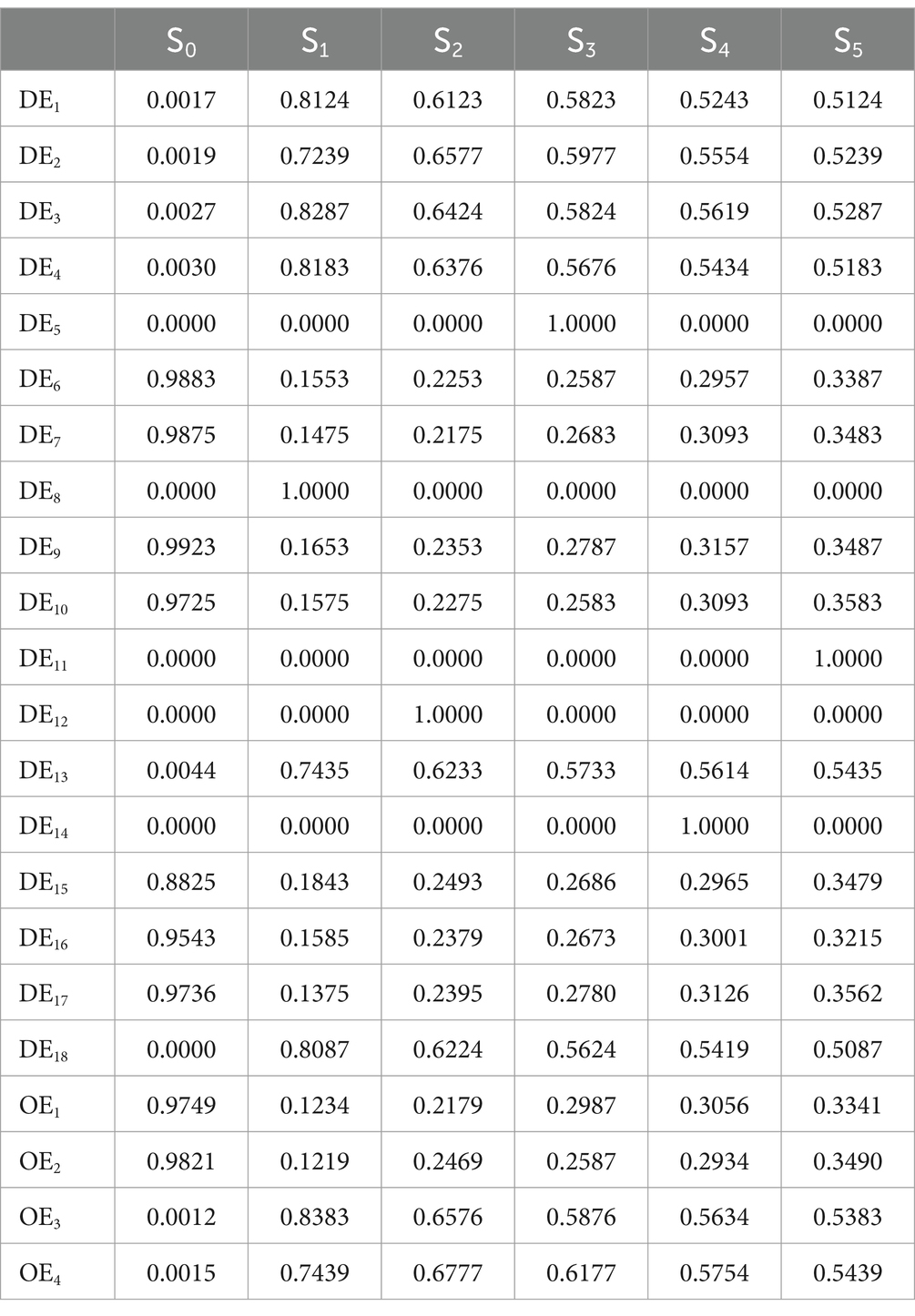
Table 10. Prediction probabilities of the other events in dynamic events analysis.
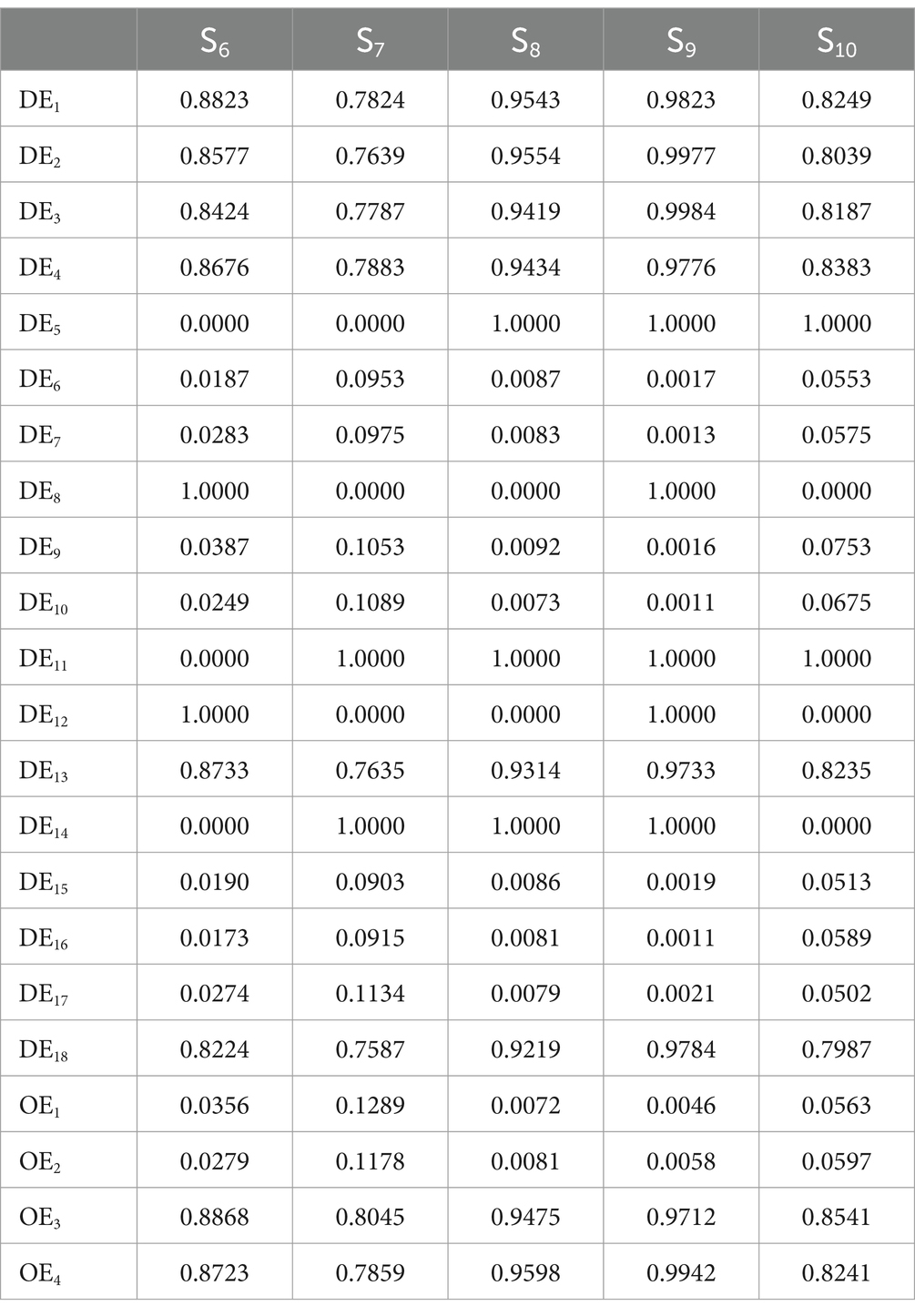
Table 11. Prediction probabilities of the other events in dynamic events analysis.
In S6, where DE12 = DE8 = 1, DE5 = DE14 = DE11 = 0, personnel movement is restricted, and an emergency command center is established. This configuration significantly reduces casualties (OE2) and somewhat mitigates economic losses (OE1). Effective rescue efforts and movement restrictions in the COVID-19-affected area of Wuhan are crucial for minimizing casualties, economic losses, and fostering public trust (OE4). Government initiatives to guide public opinion, disseminate information about infectious diseases through media, and promote awareness about hazards and preventive measures play a crucial role in alleviating social panic (OE4). In scenario 7 (S7), economic losses (OE1) are notably reduced, but the decrease in casualties (OE1) is insignificant and has minimal impact on enhancing public trust (OE3). In scenario 8 (S8), where DE12 = DE8 = 0 and DE5 = DE11 = DE14 = 1, there is a significant decrease in economic losses (OE1), a notable increase in public trust (OE4), and a considerable decrease in casualties (OE2).
4 Applications
4.1 Scenario reasoning for emergency management of COVID-19 in Wuhan, China
Analyzing the epidemic’s progression reveals the critical timeline of anti-epidemic events subsequent to the COVID-19 outbreak in Wuhan, detailed in Table 13. Initially, Wuhan Jinyintan Hospital faced shortages in essential resources for infectious disease control, including protective equipment such as medical gowns, masks, and goggles (39). In December 2019, Wuhan reported pneumonia cases attributed to a novel coronavirus strain, distinct from the 2003 SARS outbreak, prompting speculation about a new coronavirus variant (40). Consequently, IC1 = IC2 = IC3 = 1, and IC4 = 0. Despite advancements in infectious disease management, Wuhan hospitals’ routine infection prevention measures proved insufficient for novel viruses (41). While Wuhan regularly conducted outbreak drills for common infectious diseases, these preparations lacked adequacy for highly transmissible viruses, undermining their response capabilities. Public self-protection measures were initially deficient, with limited access to clear guidance exacerbating the situation (42, 43). Local governments struggled with public communication, lacking comprehensive plans for engagement, although public trust in government instructions remained intact. Given the novelty of the coronavirus, its initial emergence saw no available vaccine (44). To summarize, the initial event probabilities are IC5 = IC6 = IC7 = IC8 = IC10 = 0 and IC9 = 1.
Once dynamic events occur, they have a probability of 1. At the onset of the COVID-19 outbreak, numerous cases emerged both within and outside Hubei Province, with infections also reported in other countries. This situation led to varying degrees of panic among the population (45). Concurrently, a plethora of rumors circulated on the internet and social media platforms, disseminating information about infectious diseases, primarily on platforms like WeChat and Weibo (46). Although routine emergency medical supplies were swiftly distributed to organizations and individuals in need, shortages quickly became apparent (47). Meanwhile, the outbreak rapidly proliferated, spreading to other provinces and cities across China (48). To curb the spread of COVID-19, China enforced traffic control measures in Wuhan city on January 23, 2020, resulting in DE7 = DE9 = DE10 = DE17 = DE6 = 1, DE18 = 0. However, mass production of the vaccine remains unfeasible in the short term (49), and sporadic instances occur where local authorities withhold information about the epidemic’s status from the public (50).
4.2 Results of cross-impact analysis
The probabilities of events in the six scenarios are presented in Table 12, derived from the preceding formula. In accordance with the temporal order of key events, DE8 = DE12 = DE5 = DE14 = DE11 = 1 was established, as illustrated in Table 14. Additionally, leveraging the timeline provided in Table 13, we inferred the epidemic spread scenario post-COVID-19 outbreak in Wuhan using seven steps (51), as depicted in Table 14.
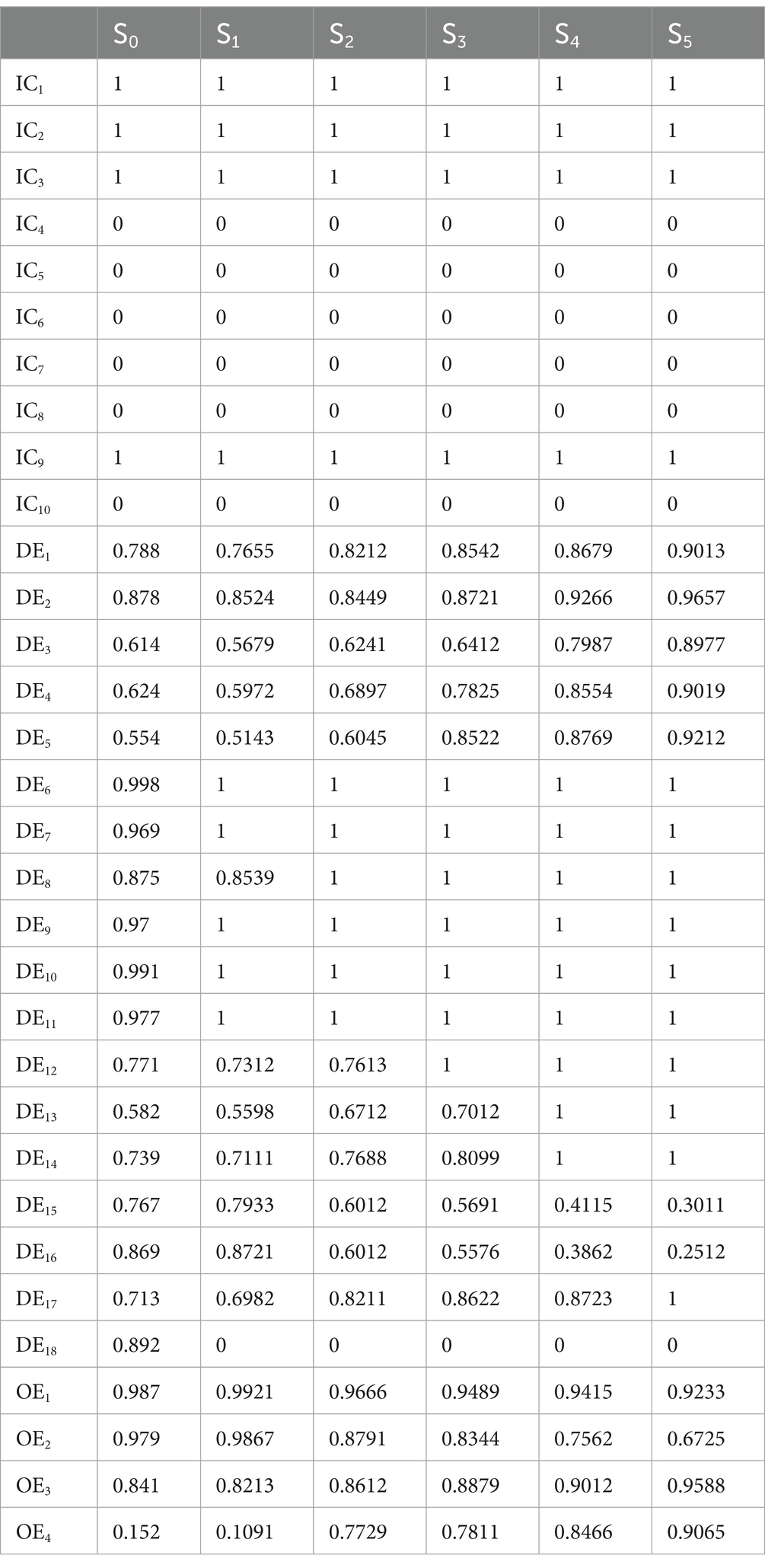
Table 12. Prediction probabilities of the other events under each scenario.
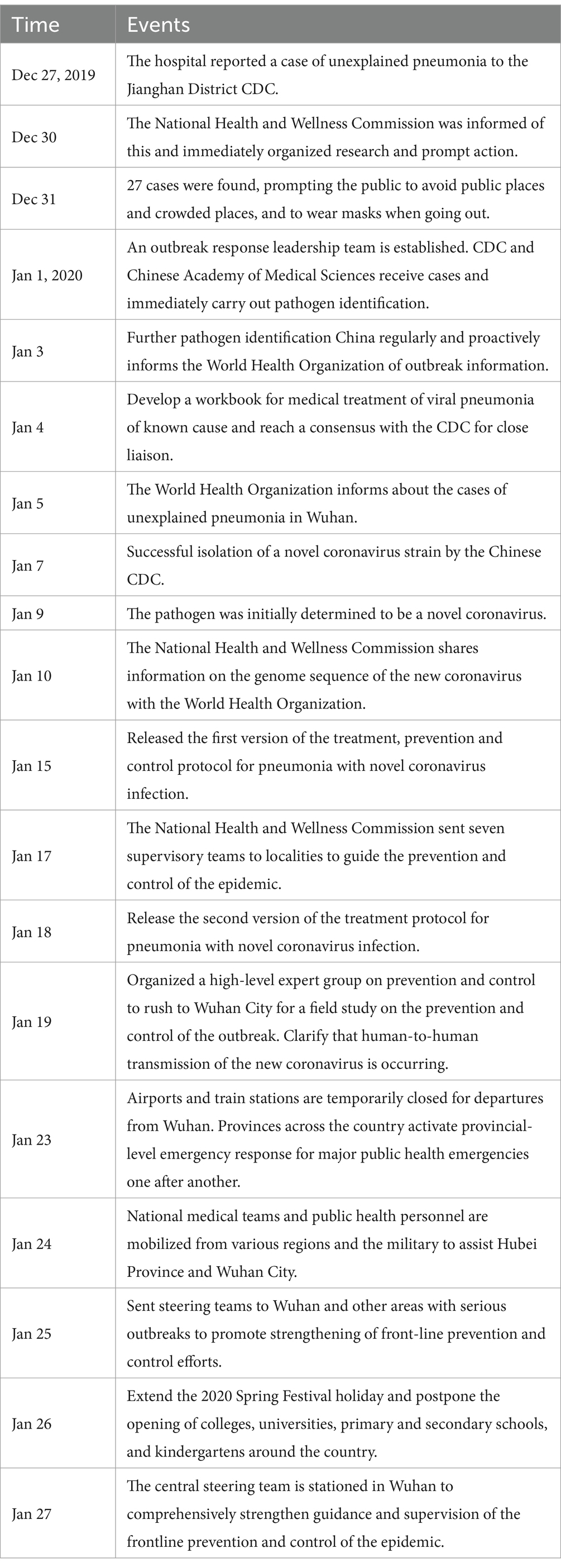
Table 13. Timeline of major rescue events after COVID-19 in Wuhan.
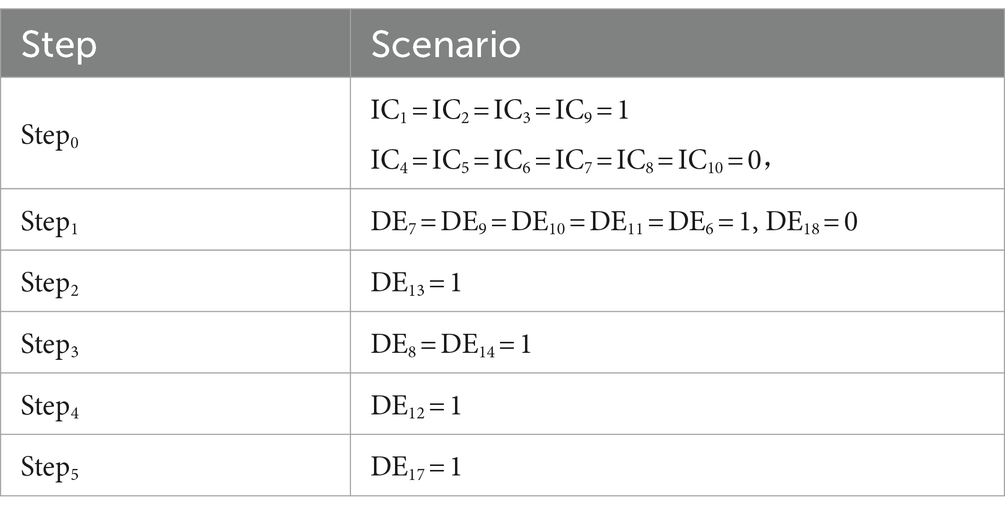
Table 14. Wuhan COVID-19 situational rehearsal setup.
To assess the model’s accuracy, the predicted outcomes were juxtaposed with the actual COVID-19 situation in Wuhan. As of March 10, 2020, at 24:00, Hubei Province had reported a cumulative total of 67,773 confirmed cases, 49,056 recoveries, and 3,046 deaths. Following the initial onset of COVID-19, there was a notable surge in mortality and daily new cases, accompanied by a poor recovery rate, as depicted in Figures 6–8.
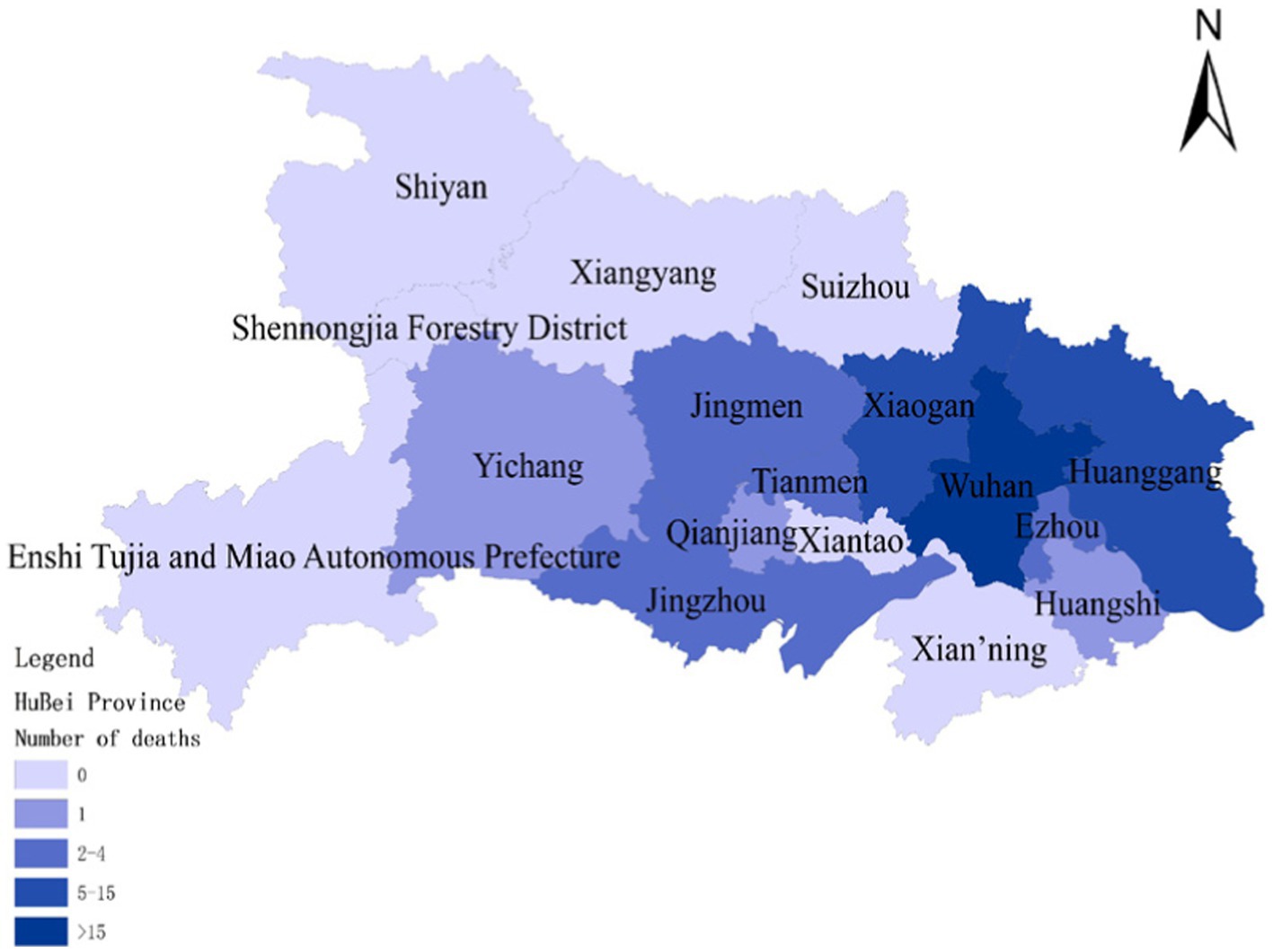
Figure 6. Cumulative deaths due to COVID-19 on January 30.
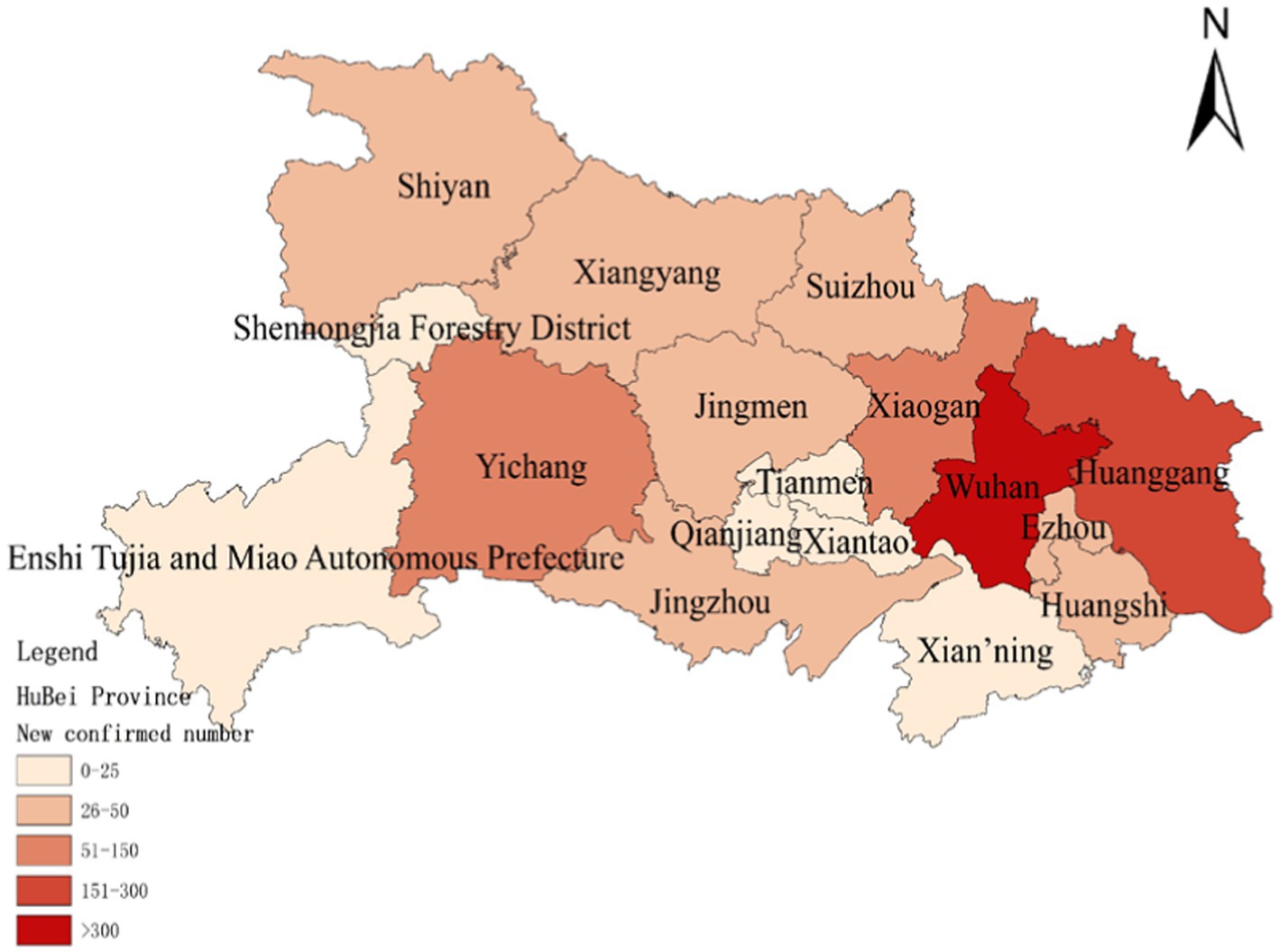
Figure 7. Number of new confirmed COVID-19 diagnoses on January 30.
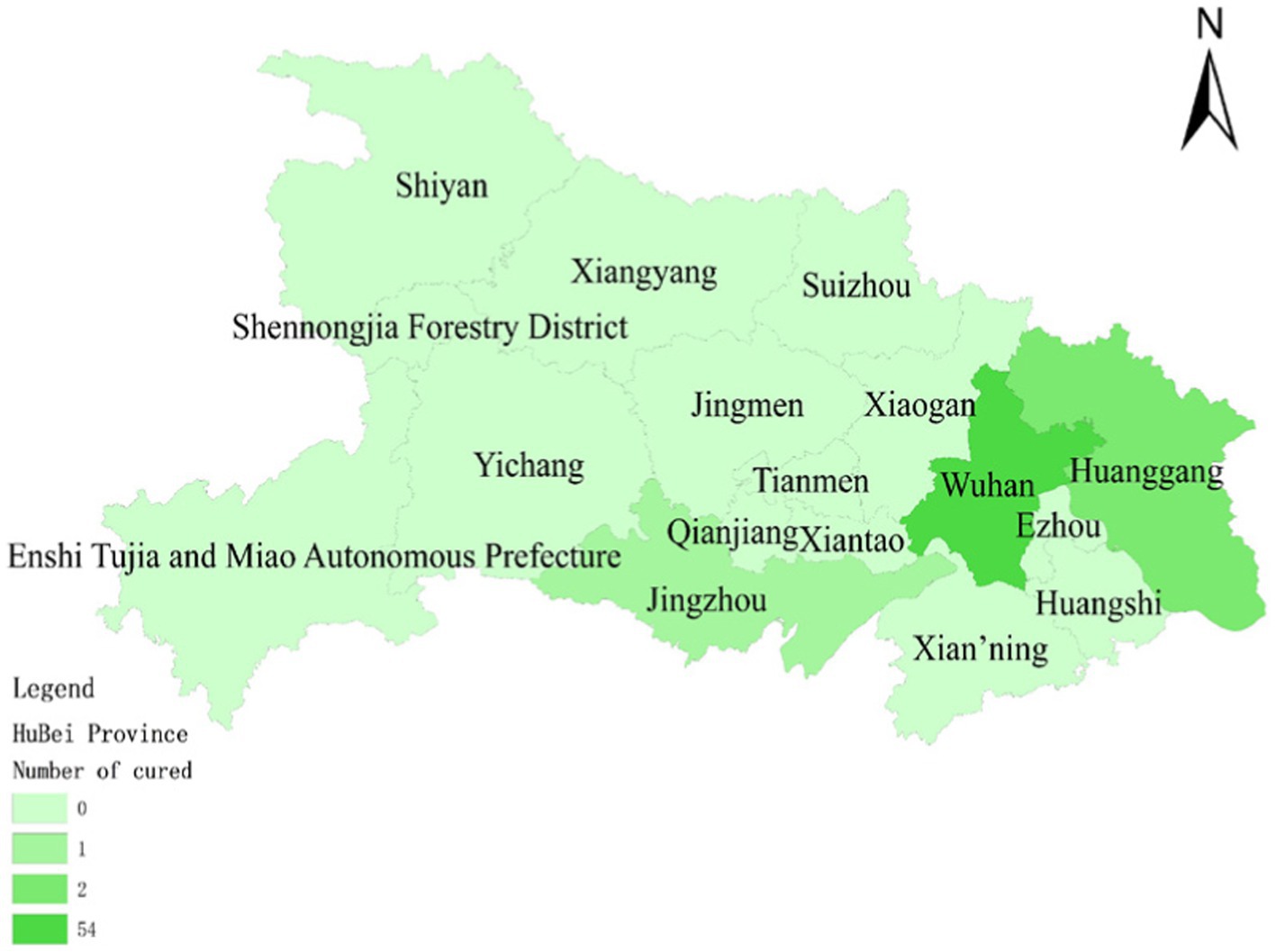
Figure 8. Number of people cured after having COVID-19 on January 30.
The probability of human casualties (OE2) surged from 1.163% to nearly 9%, as illustrated in Figure 9. As Chikyu Wuhan intensified its anti-epidemic efforts, the COVID-19 mortality rate swiftly dropped from 9.026% on January 27 to 5.346% on January 28. In Wuhan, the number of new cases exhibited the initial signs of decline by 2.14, marking the beginning of a downturn in cumulative deaths, while the tally of recoveries continued to rise, as depicted in Figures 10–13.
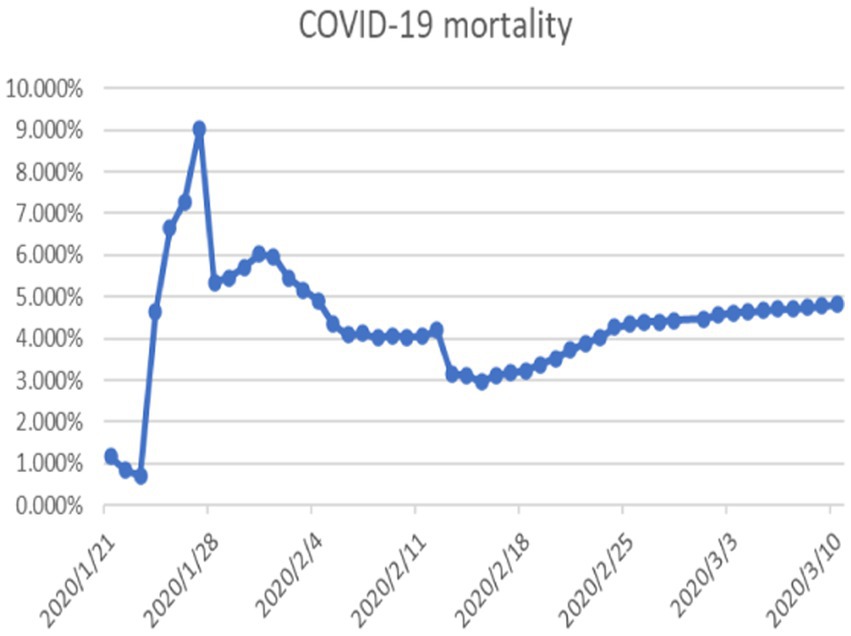
Figure 9. COVID-19 mortality rate.
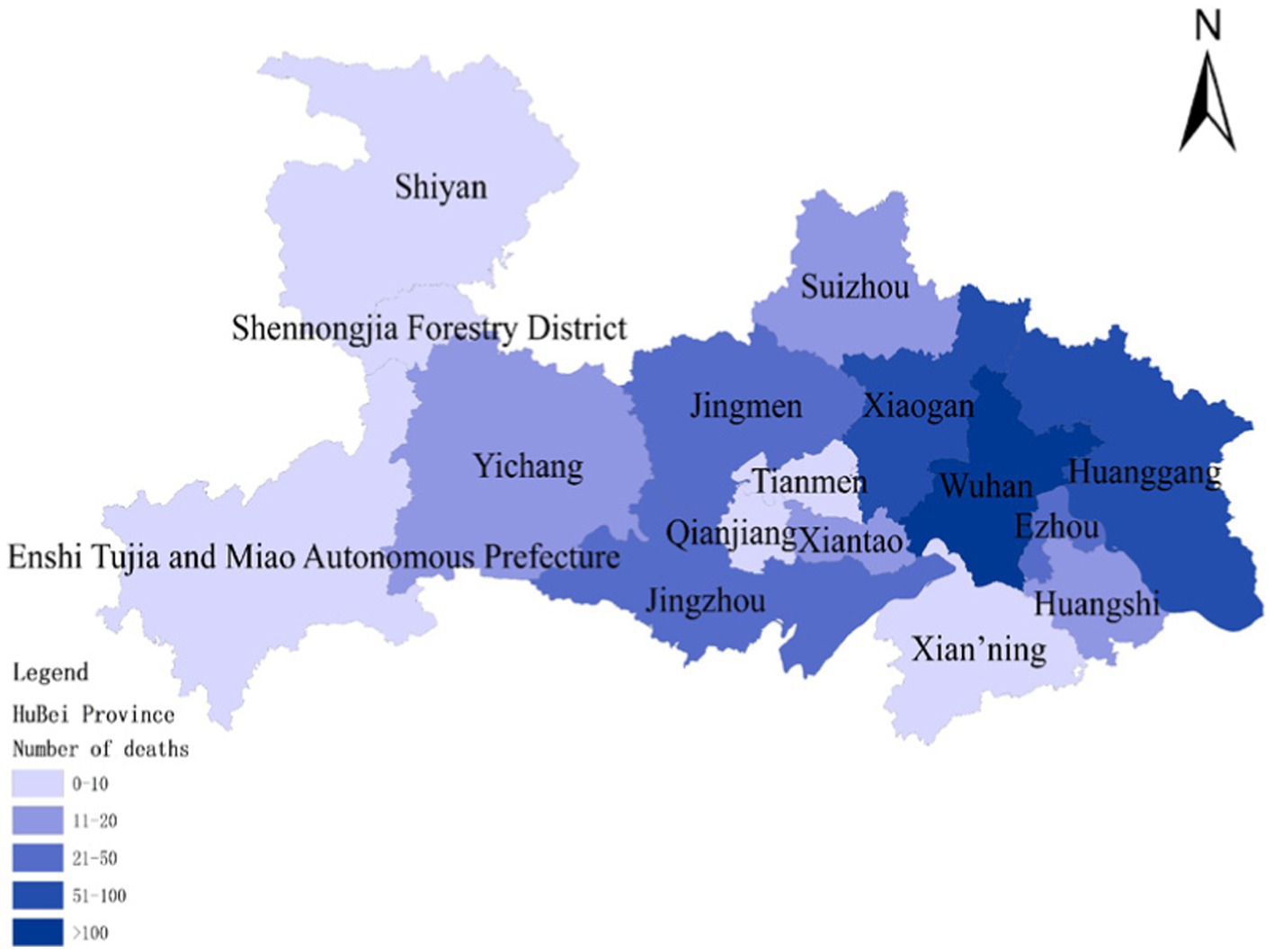
Figure 10. Cumulative deaths due to COVID-19 on February 14.
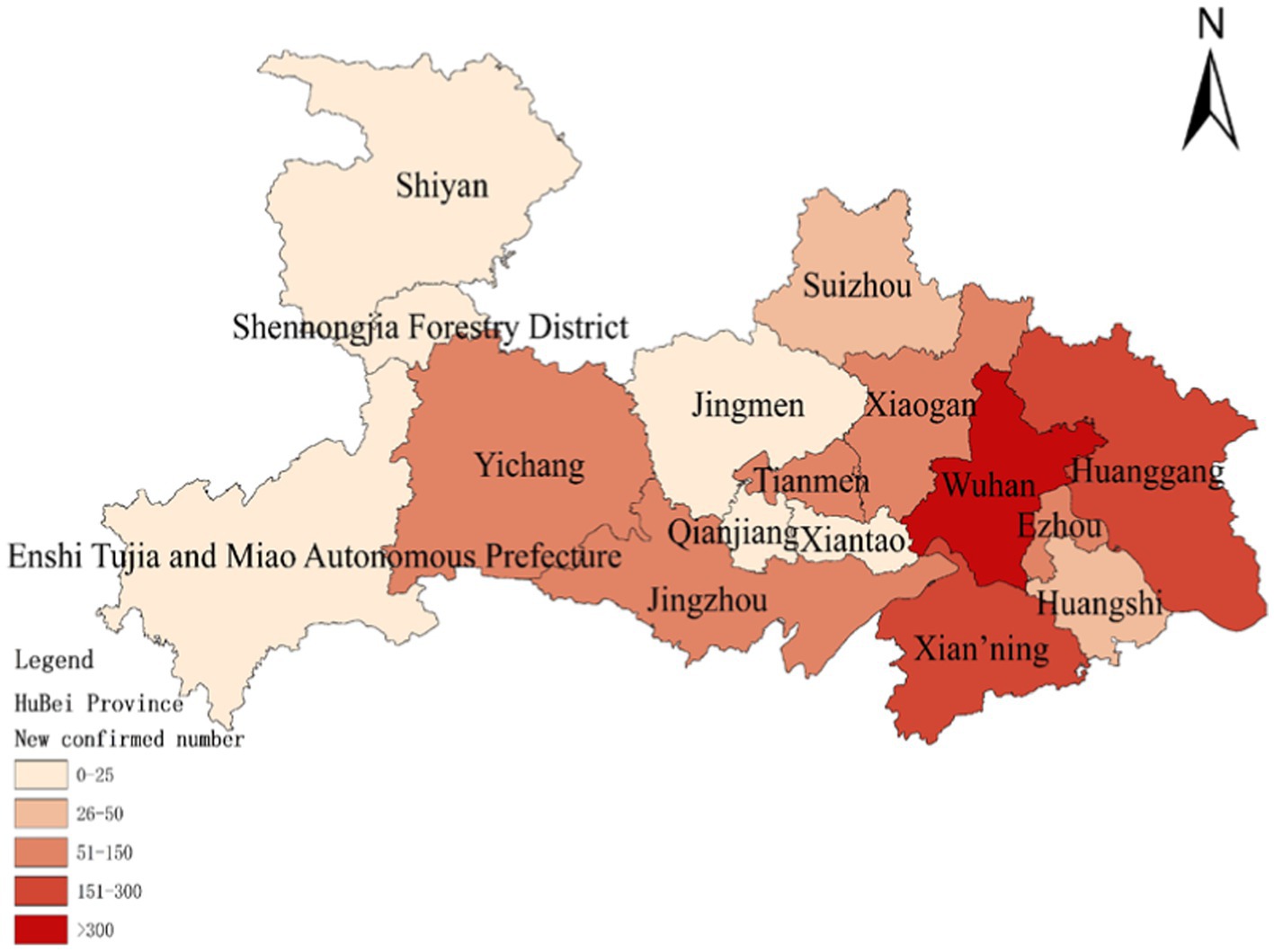
Figure 11. Number of new confirmed COVID-19 diagnoses on February 14.
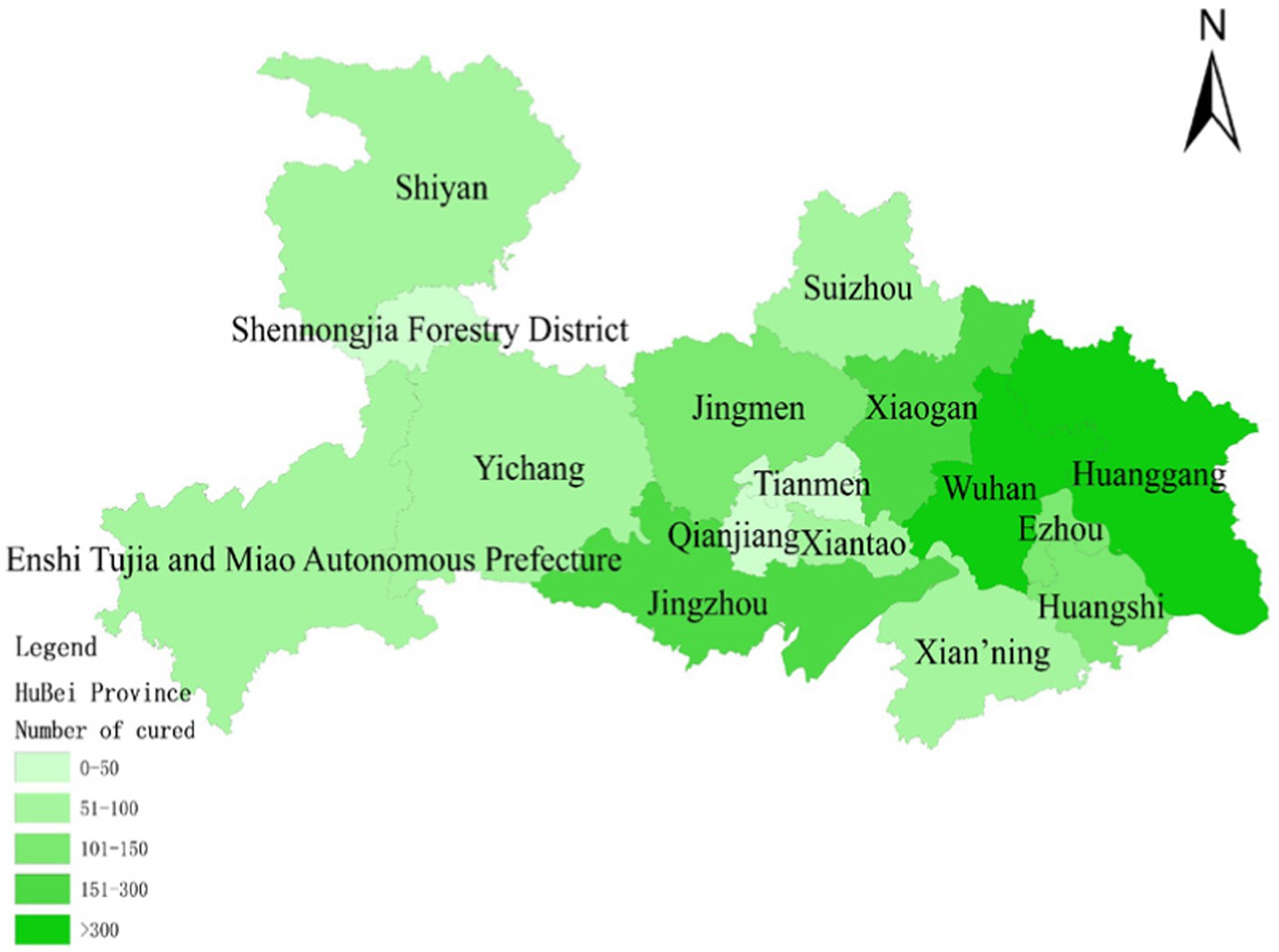
Figure 12. Number of people cured after having COVID-19 on February 14.
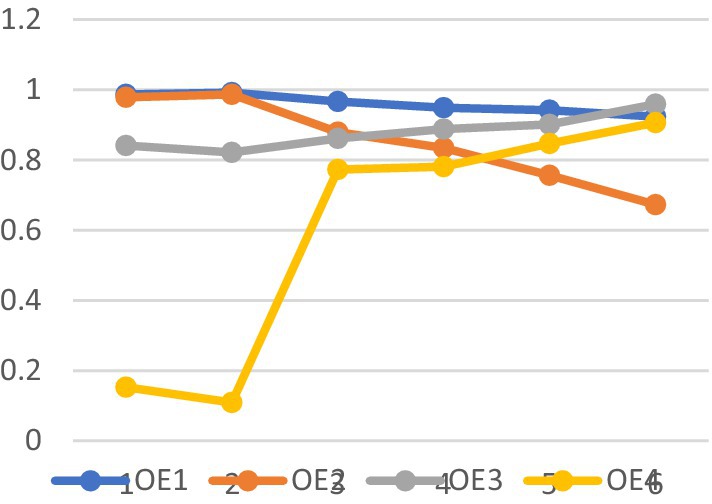
Figure 13. The trend of the prediction probabilities of four outcome events.
Subsequent mortality rates continued to decrease and stabilized below 5%, indicating that the epidemic was largely under control by early March, as evidenced in the attached video. The projected trend aligns with the actual situation outlined in the statistical report.
COVID-19 resulted in damages exceeding $1.1 trillion. Despite substantial donations and supplies raised by the government, they had minimal impact on offsetting the substantial losses. The probability of economic loss (OE1) consistently hovered near 100% with minimal fluctuations, mirroring the actual scenario. Emergency response measures following the COVID-19 outbreak had limited success in mitigating economic losses, emphasizing the need for stronger focus on emergency preparedness. The Chinese government is lauded for its swift emergency response to the COVID-19 outbreak. The central government promptly dispatched medical personnel to affected regions within 4 days of the outbreak. Various departments actively gathered and validated valuable data, while the National Health Commission promptly disseminated the latest updates to the public. The prompt dissemination of authoritative information alleviated public panic and anxiety to some extent, garnering praise domestically and internationally. Following COVID-19, the probability of public trust (OE4) decreased to nearly 10%, reflecting the actual circumstances. Public trust notably surged after the government’s swift relief measures. The government efficiently shaped public opinion and promptly disclosed outbreak information, markedly reducing social panic and enhancing public trust. The probability of public trust was highest upon the arrival of rescue teams and supplies in Wuhan, coupled with the prompt distribution of emergency medical supplies to those in need. The findings suggest that the government actively quelled public panic and fostered public trust, with the establishment of the emergency command center being pivotal. Nonetheless, in the initial scenario (step0), the probabilities of both outcome events reached very high values, underscoring the substantial impact of the lack of emergency preparedness on outcomes resulting in severe losses. The simulation results better align with the actual scenario, as depicted in Figure 12.
The emergency response to the COVID-19 outbreak in Wuhan was swift and effective. However, weak emergency preparedness could still lead to significant casualties and substantial economic losses. Our simulation aims to create dynamic scenarios for potential urban infectious disease outbreaks. Developing scenario-based contingency plans for such outbreaks can assist decision-makers in analyzing potential scenarios during the COVID-19 pandemic and predicting the impact and consequences of various actions they may take. The simulation includes four scenarios: IC4 = 1, IC5 = IC7 = 0; IC5 = 1, IC4 = IC7 = 0; IC7 = 1, IC4 = IC5 = 0; IC4 = IC7 = IC5 = 1. The remaining parameters mirror those of the Wuhan COVID-19 outbreak.
The probabilities of four outcome events - human casualties, economic losses, disease control, and public trust under different scenarios - are illustrated in Figures 14–17, respectively. Figure 15 demonstrates that government communication capacity (IC8) positively impacts reducing economic losses. However, recovering from significant economic losses caused by COVID-19 proves challenging. Figure 15 also highlights the critical roles of medical resource reserves (IC4) and public self-protection capabilities (IC7) in mitigating human casualties, alongside the positive effect of government contingency plans (IC5). Factors such as public panic (DE9), rumor spreading (DE10), disease transmission (DE11), leadership discord in releasing information (DE6), and information leakage (DE7) significantly increase the likelihood of human casualties (Step2). Conversely, Figure 16 indicates that sufficient government contingency plans (IC5) and medical resource reserves (IC4) can expedite disease control, albeit with the risk of heightened social panic (Step2) due to disease spread. Nonetheless, effective emergency preparedness and robust government contingency plans swiftly mitigate public panic and foster public trust, as depicted in Figure 17. Therefore, several recommendations emerge, emphasizing the pivotal role of emergency preparedness in guiding positive responses from both government and the public to COVID-19. Simultaneously, efforts should focus on minimizing associated risks and losses. Easy access to transportation facilities may exacerbate disease spread, necessitating contact isolation measures for transit travelers in managing urban disease outbreak emergencies. Moreover, addressing rumor spreading and information leakage warrants increased governmental attention, along with the development of comprehensive emergency response measures and extensive public education. Frontline medical personnel’s rescue efforts and adequate medical resources are crucial for saving lives, facilitating easier epidemic control and ensuring prompt deployment of medical resources. Given the economic challenge posed by urban disease outbreaks, hospitals’ medical facility performance and local hospitals’ rescue efforts are particularly crucial. Finally, active public opinion guidance and timely, effective dissemination of epidemic-related information are indispensable for reducing social panic and enhancing public trust.
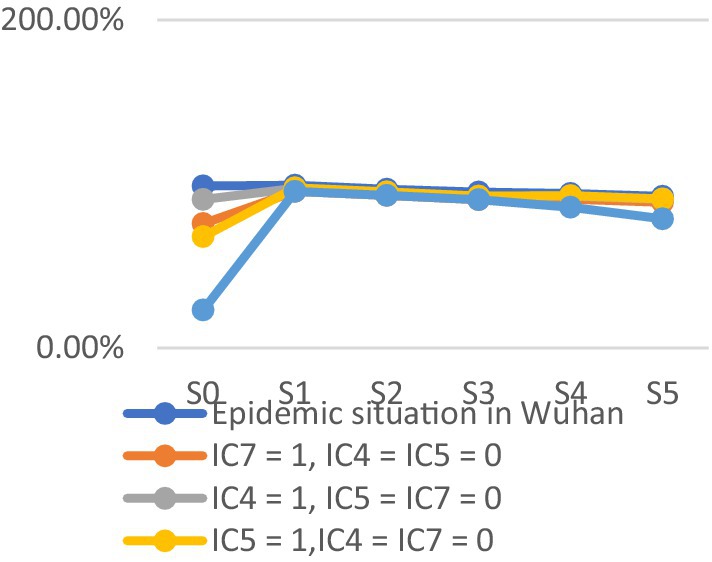
Figure 14. Economic loss.

Figure 15. Personnel death.
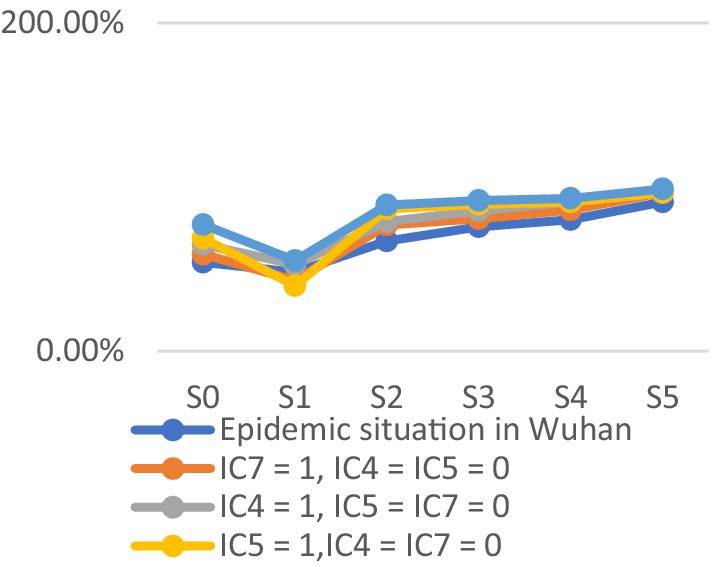
Figure 16. Infectious diseases are under control.

Figure 17. Public trust.
5 Discussion and conclusion
5.1 Discussion
Emergency medical supplies directly impact casualties by being delivered to organizations and people in need, aligning with Tokalić and Viđak’s study (12). Stockpiling medical resources and establishing an emergency command center are crucial priorities in emergency preparedness to prevent mass casualties. Several studies have explored the interplay between infectious diseases and other social crises or urban infrastructure (52, 53). For instance, Jakariya et al. developed an integrated wastewater-based epidemiological system to detect COVID-19 prevalence (54), while Islam et al. emphasized the importance of COVID-19 antibody studies (55). However, this study focuses on the early stages of infectious disease outbreaks and does not include antibodies as a key factor due to their development time (56). Vulnerability to social and political factors may undermine COVID-19 emergency management efforts, consistent with previous findings (57). Global mortality trends of COVID-19 reflect inadequate preparedness worldwide (58). Rahman et al.’s systematic evaluation approach offers valuable insights for this study, particularly in response measures for Southeast and South Asia (59). However, most studies only address single points in emergency management, such as evacuation or healthcare responses (60, 61). Unlike Brooks et al.’s study, this paper examines the dynamic interaction between event sets and constructs a scenario model for analyzing COVID-19 emergency management in Wuhan (7). It presents a hypothetical urban outbreak response scenario based on COVID-19 occurrences, highlighting the impact of critical events on outcomes and using directed graphs to illustrate event relationships. The leaders’ reluctance to share information and healthcare workers’ non-cooperation trigger other dynamic events, emphasizing the importance of emergency preparedness in epidemic response. The model proposed in this research enriches the future pandemic response framework proposed by Amir Khorram-Manesh et al. (62).
5.2 Conclusion
This paper convenes an expert panel of emergency management specialists and Wuhan COVID-19 responders, leveraging insights from prior infectious disease outbreaks like H1N1 and SARS (5). The panel compiles a comprehensive array of critical events pertaining to emergency management decisions. Utilizing the Delphi method, a consistent causality estimation matrix is established among these events. Following the creation of a cross-impact matrix, the most impactful events, representing the top 5 and 15%, are visually depicted. Initially, the model facilitates multiple scenario analyses to identify crucial contingencies. Subsequently, it discerns correlations between actual events to delineate outcome trends stemming from varied courses of action. Emergency management initiatives that synergistically influence one another form micro-sets, enabling the dissection of their impact on human casualties and economic losses. Scenario simulations derived from diverse emergency management strategies prove more scientifically robust than single-factor approaches (19). Concurrently, this study corroborates the adverse effects of rumors and information leakage on infectious disease containment (34). Restricting people’s movement significantly curtails casualties, while the swift depletion of medical supplies and nationwide economic shutdowns exacerbate economic losses. Although rapid economic recovery from infectious disease-induced losses remains challenging, a well-crafted emergency plan serves as a cornerstone for restoring public confidence and bolstering trust. Enhanced public awareness of effective epidemic control measures and self-protection strategies expedites disease coping mechanisms. However, casualties, information leaks, and rumors can escalate public panic, underscoring the need for proactive guidance through essential medical interventions and authoritative dissemination of disease-related information by governmental bodies. The findings underscore the imperative of emergency preparedness in mitigating severe economic losses, casualties, and societal ramifications precipitated by infectious diseases. During the primary stage of emergency response, concerted rescue efforts must collaborate to achieve optimal outcomes. Simulation outcomes demonstrate that the effective implementation of multiple emergency management measures significantly diminishes the probability of infectious disease-related damage. The analysis underscores the pivotal role of establishing an emergency command center and the proactive governmental involvement in assuaging public apprehension and fostering trust. Prioritizing the isolation and monitoring of individuals exposed to infectious diseases emerges as a paramount objective in emergency management, effectively curbing disease transmission and mitigating casualties and economic losses. Drawing from real-world epidemic occurrences and scenario simulations, this paper enables the assessment of the efficacy of critical emergency management measures, the identification of pivotal events for future epidemic combat, and the formulation of targeted recommendations to ameliorate epidemic-induced losses and refine future emergency management protocols.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding authors.
Author contributions
PY: Writing – original draft, Writing – review & editing. HL: Writing – original draft. XD: Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. This study was supported by Research on Resilience Evaluation and Enhancement Mechanism of Urban Associated Lifeline System (ZR2023MG044), the Natural Science Foundation of Shandong Province, China, and the Shandong Province Social Science Planning Major Theoretical and Practical Issues Collaborative Innovation Research Special Project: Research on Mechanisms and Strategies of Resilience Enhancement of Urban Associated Lifeline Systems (Project No. 23CCXJ01).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Nicola, M, Alsafi, Z, Sohrabi, C, Kerwan, A, Al-Jabir, A, Iosifidis, C, et al. The socio-economic implications of the coronavirus pandemic (COVID-19): a review. Int J Surg. (2020) 78:185–93. doi: 10.1016/j.ijsu.2020.04.018
2. Li, X, Zhou, YS, Wong, YD, Wang, XQ, and Yuen, KF. What influences panic buying behaviour? A model based on dual-system theory and stimulus-organism-response framework. Int J Disaster Risk Reduct. (2021) 64:102484. doi: 10.1016/j.ijdrr.2021.102484
3. Cinelli, M, Quattrociocchi, W, Galeazzi, A, Valensise, CM, Brugnoli, E, Schmidt, AL, et al. The COVID-19 social media infodemic. Sci Rep. (2020) 10:16598. doi: 10.1038/s41598-020-73510-5
4. Lu, Y, Ji, Z, Zhang, XQ, Zheng, YQ, and Liang, H. Re-thinking the role of government information intervention in the COVID-19 pandemic: an agent-based modeling analysis. Int J Environ Res Public Health. (2021) 18:147. doi: 10.3390/ijerph18010147
5. Lin, YC, Dong, SL, Yeh, YH, Wu, YS, Lan, GY, Liu, CM, et al. Emergency management and infection control in a radiology department during an outbreak of severe acute respiratory syndrome. Br J Radiol. (2005) 78:606–11. doi: 10.1259/bjr/17161223
6. Fraser, C, Donnelly, CA, Cauchemez, S, Hanage, WP, Van Kerkhove, MD, Hollingsworth, TD, et al. Pandemic potential of a strain of influenza a (H1N1): early findings. Science. (2009) 324:1557–61. doi: 10.1126/science.1176062
7. Brooks, JC, Pinto, M, Gill, A, Hills, KE, Murthy, S, Podgornik, MN, et al. Incident management systems and building emergency management capacity during the 2014-2016 Ebola epidemic - Liberia, Sierra Leone, and Guinea. MMWR Suppl. (2016) 65:28–34. doi: 10.15585/mmwr.su6503a5
8. Chavez, S, Long, B, Koyfman, A, and Liang, SY. Coronavirus disease (COVID-19): a primer for emergency physicians. Am J Emerg Med. (2021) 44:220–9. doi: 10.1016/j.ajem.2020.03.036
9. Hewlett, AL, Varkey, JB, Smith, PW, and Ribner, BS. Ebola virus disease: preparedness and infection control lessons learned from two biocontainment units. Curr Opin Infect Dis. (2015) 28:343–8. doi: 10.1097/qco.0000000000000176
10. Zhang, Y, and Zhou, R. Promoting social distancing and preventing panic buying during the epidemic of COVID-19: the contributions of people's psychological and behavioural factors. Z Gesundh Wiss. (2021) 31:187–201. doi: 10.1007/s10389-021-01497-y
11. Glass, RJ, Glass, LM, Beyeler, WE, and Min, HJ. Targeted social distancing design for pandemic influenza. Emerg Infect Dis. (2006) 12:1671–81. doi: 10.3201/eid1211.060255
12. Tokalić, R, Viđak, M, Kaknjo, MM, and Marušić, A. Antifragility of healthcare systems in Croatia and Bosnia and Herzegovina: learning from man-made and natural crises. Lancet Reg Health Eur. (2021) 9:100216. doi: 10.1016/j.lanepe.2021.100216
13. Chinazzi, M, Davis, JT, Ajelli, M, Gioannini, C, Litvinova, M, Merler, S, et al. The effect of travel restrictions on the spread of the 2019 novel coronavirus (COVID-19) outbreak. Science. (2020) 368:395-+. doi: 10.1126/science.aba9757
14. Rothan, HA, and Byrareddy, SN. The epidemiology and pathogenesis of coronavirus disease (COVID-19) outbreak. J Autoimmun. (2020) 109:102433. doi: 10.1016/j.jaut.2020.102433
15. Van Bavel, JJ, Baicker, K, Boggio, PS, Capraro, V, Cichocka, A, Cikara, M, et al. Using social and behavioural science to support COVID-19 pandemic response. Nat Hum Behav. (2020) 4:460–71. doi: 10.1038/s41562-020-0884-z
16. Banuls, VA, and Turoff, M. Scenario construction via Delphi and cross-impact analysis. Technol Forecast Soc Chang. (2011) 78:1579–602. doi: 10.1016/j.techfore.2011.03.014
17. Brouqui, P, Puro, V, Fusco, FM, Bannister, B, Schilling, S, Follin, P, et al. Infection control in the management of highly pathogenic infectious diseases: consensus of the European network of infectious disease. Lancet Infect Dis. (2009) 9:301–11. doi: 10.1016/s1473-3099(09)70070-2
18. Wong, ATY, Chen, H, Liu, SH, Hsu, EK, Luk, KS, Lai, CKC, et al. From SARS to avian influenza preparedness in Hong Kong. Clin Infect Dis. (2017) 64:S98–S104. doi: 10.1093/cid/cix123
19. Van Beneden, CA, Pietz, H, Kirkcaldy, RD, Koonin, LM, Uyeki, TM, Oster, AM, et al. Early identification and prevention of the spread of Ebola-United States. MMWR. (2016) 65:75–84. doi: 10.15585/mmwr.su6503a11
20. Driggin, E, Madhavan, MV, Bikdeli, B, Chuich, T, Laracy, J, Biondi-Zoccai, G, et al. Cardiovascular considerations for patients, health care workers, and health systems during the COVID-19 pandemic. J Am Coll Cardiol. (2020) 75:2352–71. doi: 10.1016/j.jacc.2020.03.031
21. Lam, SKK, Kwong, EWY, Hung, MSY, and Pang, SMC. Bridging the gap between guidelines and practice in the management of emerging infectious diseases: a qualitative study of emergency nurses. J Clin Nurs. (2016) 25:2895–905. doi: 10.1111/jocn.13343
22. Huang, Z, Zhao, S, Li, Z, Chen, W, Zhao, L, Deng, L, et al. The Battle against coronavirus disease 2019 (COVID-19): emergency management and infection control in a radiology department. J Am Coll Radiol. (2020) 17:710–6. doi: 10.1016/j.jacr.2020.03.011
23. Kucharski, AJ, Russell, TW, Diamond, C, Liu, Y, Edmunds, J, Funk, S, et al. Early dynamics of transmission and control of COVID-19: a mathematical modelling study. Lancet Infect Dis. (2020) 20:553–8. doi: 10.1016/s1473-3099(20)30144-4
24. Wu, JT, Leung, K, and Leung, GM. Nowcasting and forecasting the potential domestic and international spread of the 2019-nCoV outbreak originating in Wuhan, China: a modelling study. Lancet. (2020) 395:689–97. doi: 10.1016/s0140-6736(20)30260-9
25. Razavi-Shearer, D, Gamkrelidze, I, Nguyen, MH, Chen, DS, Van Damme, P, Abbas, Z, et al. Global prevalence, treatment, and prevention of hepatitis B virus infection in 2016: a modelling study. Lancet Gastroenterol Hepatol. (2018) 3:383–403. doi: 10.1016/s2468-1253(18)30056-6
26. Chang, S, Pierson, E, Koh, PW, Gerardin, J, Redbird, B, Grusky, D, et al. Mobility network models of COVID-19 explain inequities and inform reopening. Nature. (2021) 589:82–7. doi: 10.1038/s41586-020-2923-3
27. Musa, SS, Tariq, A, Liu, Y, Wei, HZ, and He, DH. Infection fatality rate and infection attack rate of COVID-19 in south American countries. Infect Dis Poverty. (2022) 11:11. doi: 10.1186/s40249-022-00961-5
28. Altig, D, Baker, S, Barrero, JM, Bloom, N, Bunn, P, Chen, S, et al. Economic uncertainty before and during the COVID-19 pandemic. J Public Econ. (2020) 191:104274. doi: 10.1016/j.jpubeco.2020.104274
29. Nicola, M, O'Neill, N, Sohrabi, C, Khan, M, Agha, M, and Agha, R. Evidence based management guideline for the COVID-19 pandemic-review article. Int J Surg. (2020) 77:206–16. doi: 10.1016/j.ijsu.2020.04.001
30. Taylor, S . The psychology of pandemics. Annu Rev Clin Psychol. (2022) 18:581–609. doi: 10.1146/annurev-clinpsy-072720-020131
31. Li, Q, Chen, T, Yang, J, and Cong, G. Based on computational communication paradigm: simulation of public opinion communication process of panic buying during the COVID-19 pandemic. Psychol Res Behav Manag. (2020) 13:1027–45. doi: 10.2147/prbm.S280825
32. Rajkumar, RP . A biopsychosocial approach to understanding panic buying: integrating neurobiological, attachment-based, and social-anthropological perspectives. Front Psych. (2021) 12:10. doi: 10.3389/fpsyt.2021.652353
33. Wang, CY, Pan, RY, Wan, XY, Tan, YL, Xu, LK, McIntyre, RS, et al. A longitudinal study on the mental health of general population during the COVID-19 epidemic in China. Brain Behav Immunity. (2020) 87:40–8. doi: 10.1016/j.bbi.2020.04.028
34. Chen, B, Chen, XY, Pan, J, Liu, K, Xie, B, Wang, W, et al. Dissemination and refutation of rumors during the COVID-19 outbreak in China: Infodemiology study. J Med Internet Res. (2021) 23:e22427. doi: 10.2196/22427
35. Hui, HW, Zhou, CC, Lu, X, and Li, JR. Spread mechanism and control strategy of social network rumors under the influence of COVID-19. Nonlinear Dyn. (2020) 101:1933–49. doi: 10.1007/s11071-020-05842-w
36. Ning, PS, Cheng, PX, Li, J, Zheng, M, Schwebel, DC, Yang, Y, et al. COVID-19-related rumor content, transmission, and clarification strategies in China: descriptive study. J Med Internet Res. (2021) 23:e27339. doi: 10.2196/27339
37. Deng, SQ, and Peng, HJ. Characteristics of and public health responses to the coronavirus disease 2019 outbreak in China. J Clin Med. (2020) 9:10. doi: 10.3390/jcm9020575
38. Banuls, VA, Turoff, M, and Hiltz, SR. Collaborative scenario modeling in emergency management through cross-impact. Technol Forecast Soc Chang. (2013) 80:1756–74. doi: 10.1016/j.techfore.2012.11.007
39. Lippi, G, and Plebani, M. The critical role of laboratory medicine during coronavirus disease 2019 (COVID-19) and other viral outbreaks. Clin Chem Lab Med. (2020) 58:1063–9. doi: 10.1515/cclm-2020-0240
40. Chan, JFW, Kok, KH, Zhu, Z, Chu, H, To, KKW, Yuan, SF, et al. Genomic characterization of the 2019 novel human-pathogenic coronavirus isolated from a patient with atypical pneumonia after visiting Wuhan. Emerg Microb Infect. (2020) 9:221–36. doi: 10.1080/22221751.2020.1719902
41. Bahl, P, Doolan, C, de Silva, C, Chughtai, AA, Bourouiba, L, and MacIntyre, CR. Airborne or droplet precautions for health workers treating coronavirus disease 2019? J Infect Dis. (2022) 225:1561–8. doi: 10.1093/infdis/jiaa189
42. Chen, HQ, Shi, LY, Zhang, YY, Wang, XH, Jiao, J, Yang, MF, et al. Comparison of public health containment measures of COVID-19 in China and India. Risk Manage Healthc Policy. (2021) 14:3323–32. doi: 10.2147/rmhp.S326775
43. Teslya, A, Pham, TM, Godijk, NG, Kretzschmar, ME, Bootsma, MCJ, and Rozhnova, G. Impact of self-imposed prevention measures and short-term government-imposed social distancing on mitigating and delaying a COVID-19 epidemic: a modelling study. PLoS Med. (2020) 17:e1003166. doi: 10.1371/journal.pmed.1003166
44. Zhang, H, Li, YX, Dolan, C, and Song, ZJ. Observations from Wuhan: an adaptive risk and crisis communication system for a health emergency. Risk Manag HealthcPolicy. (2021) 14:3179–93. doi: 10.2147/rmhp.S287637
45. Khan, K, Li, YY, Liu, S, and Li, CT. Psychological distress and Trust in University Management among International Students during the COVID-19 pandemic. Front Psychol. (2021) 12:8. doi: 10.3389/fpsyg.2021.679661
46. Zhu, BR, Zheng, XQ, Liu, HY, Li, JY, and Wang, PP. Analysis of spatiotemporal characteristics of big data on social media sentiment with COVID-19 epidemic topics. Chaos, Solitons Fractals. (2020) 140:110123. doi: 10.1016/j.chaos.2020.110123
47. Zhou, WK, Wang, AL, Wang, X, Cheke, RA, Xiao, YN, and Tang, SY. Impact of hospital bed shortages on the containment of COVID-19 in Wuhan. Int J Environ Res Public Health. (2020) 17:18. doi: 10.3390/ijerph17228560
48. Hua, JL, and Shaw, R. Corona virus (COVID-19) "Infodemic" and emerging issues through a data Lens: the case of China. Int J Environ Res Public Health. (2020) 17:12. doi: 10.3390/ijerph17072309
49. Zhu, FC, Li, YH, Guan, XH, Hou, LH, Wang, WJ, Li, JX, et al. Safety, tolerability, and immunogenicity of a recombinant adenovirus type-5 vectored COVID-19 vaccine: a dose-escalation, open-label, non-randomised, first-in-human trial. Lancet. (2020) 395:1845–54. doi: 10.1016/s0140-6736(20)31208-3
50. Shangguan, ZH, Wang, MY, and Sun, W. What caused the outbreak of COVID-19 in China: from the perspective of crisis management. Int J Environ Res Public Health. (2020) 17:16. doi: 10.3390/ijerph17093279
51. Roosa, K, Lee, Y, Luo, R, Kirpich, A, Rothenberg, R, Hyman, JM, et al. Real-time forecasts of the COVID-19 epidemic in China from February 5th to February 24th, 2020. Infect Dis Model. (2020) 5:256–63. doi: 10.1016/j.idm.2020.02.002
52. Islam, MA, Rahman, MA, Jakariya, M, Bahadur, NM, Hossen, F, Mukharjee, SK, et al. A 30-day follow-up study on the prevalence of SARS-COV-2 genetic markers in wastewater from the residence of COVID-19 patient and comparison with clinical positivity. Sci Total Environ. (2023) 858:159350. doi: 10.1016/j.scitotenv.2022.159350
53. Islam, MA, Shahi, S, Marzan, AA, Amin, MR, Hasan, MN, Hoque, MN, et al. Variant-specific deleterious mutations in the SARS-CoV-2 genome reveal immune responses and potentials for prophylactic vaccine development. Front Pharmacol. (2023) 14:717. doi: 10.3389/fphar.2023.1090717
54. Jakariya, M, Ahmed, F, Islam, MA, Al Marzan, A, Hasan, MN, Hossain, M, et al. Wastewater-based epidemiological surveillance to monitor the prevalence of SARS-CoV-2 in developing countries with onsite sanitation facilities. Environ Pollut. (2022) 311:119679. doi: 10.1016/j.envpol.2022.119679
55. Islam, MA, Hossen, F, Rahman, MA, Sultana, KF, Hasan, MN, Haque, MA, et al. An opinion on wastewater-based epidemiological monitoring (WBEM) with clinical diagnostic test (CDT) for detecting high-prevalence areas of community COVID-19 infections. Curr Opin Environ Sci Health. (2023) 31:100396. doi: 10.1016/j.coesh.2022.100396
56. Haider, N, Hasan, MN, Guitian, J, Khan, RA, McCoy, D, Ntoumi, F, et al. The disproportionate case–fatality ratio of COVID-19 between countries with the highest vaccination rates and the rest of the world. IJID Reg. (2023) 6:159–66. doi: 10.1016/j.ijregi.2023.01.011
57. Haider, N, Yavlinsky, A, Chang, Y-M, Hasan, MN, Benfield, C, Osman, AY, et al. The Global Health security index and joint external evaluation score for health preparedness are not correlated with countries' COVID-19 detection response time and mortality outcome. Epidemiol Infect. (2020) 148:e210. doi: 10.1017/S0950268820002046
58. Hasan, MN, Haider, N, Stigler, FL, Khan, RA, McCoy, D, Zumla, A, et al. The global case-fatality rate of COVID-19 has been declining since May 2020. Am J Trop Med Hyg. (2021) 104:2176–84. doi: 10.4269/ajtmh.20-1496
59. Rahman, MM, Marzo, RR, Chowdhury, S, Qalati, SA, Hasan, MN, Paul, GK, et al. Knowledge, attitude and practices toward coronavirus disease (COVID-19) in southeast and South Asia: a mixed study design approach. Front Public Health. (2022) 10:875727. doi: 10.3389/fpubh.2022.875727
60. Hasan, MN, Islam, MA, Sangkham, S, Werkneh, AA, Hossen, F, Haque, MA, et al. Insight into vaccination and meteorological factors on daily COVID-19 cases and mortality in Bangladesh. Groundw Sustain Dev. (2023) 21:100932. doi: 10.1016/j.gsd.2023.100932
61. Sangkham, S, Islam, MA, Sarndhong, K, Vongruang, P, Hasan, MN, Tiwari, A, et al. Effects of fine particulate matter (PM2.5) and meteorological factors on the daily confirmed cases of COVID-19 in Bangkok during 2020–2021, Thailand. Case Stud Chem Environ Eng. (2023) 8:100410. doi: 10.1016/j.cscee.2023.100410
Keywords: CIA-ISM, scenario approach, COVID-19, Wuhan, pestilence
Citation: Yuan P, Liu H and Dong X (2024) Scenario-based assessment of emergency management of urban infectious disease outbreaks. Front. Public Health. 12:1368154. doi: 10.3389/fpubh.2024.1368154
Edited by:
Andrea Haselbeck, International Vaccine Institute, Republic of KoreaReviewed by:
Mohammad Nayeem Hasan, Shahjalal University of Science and Technology, BangladeshKrzysztof Goniewicz, Polish Air Force University, Poland
Copyright © 2024 Yuan, Liu and Dong. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Pengwei Yuan, c21feXVhbnB3QHVqbi5lZHUuY24=