 Zijun Zhao1†
Zijun Zhao1† Xianyu Xie
Xianyu Xie Qinde Wu
Qinde Wu- 1School of Public Administration & Law, Fujian Agriculture and Forestry University, Fuzhou, Fujian, China
- 2Department of Medical Administration, Fujian Medical University Union Hospital, Fuzhou, Fujian, China
- 3Department of Education Administration, Fujian Medical University Union Hospital, Fuzhou, Fujian, China
Introduction: Medical alliances are essential for constructing an hierarchical diagnosis and treatment (HDT) system; therefore, it is crucial to promote such alliances and evaluate their effectiveness in this regard from the medical staff perspective. This study thus investigated and analyzed the evaluations of medical staff in China concerning the effect of medical alliances on promoting HDT with the intention to encourage further establishment of medical alliances and HDT under China’s new medical reform.
Methods: A total of 616 medical staff personnel from 3 medical alliances in Fujian Province were surveyed, and data were analyzed using SPSS 20.0 software.
Results: The level of medical institutions, posts and satisfaction with their medical alliances influenced the evaluation of medical alliance effectiveness in resolving the problem of expensive medical services. Primary medical institutions are more inclined toward policy formulation and related work; thus, the interests of primary hospitals can be guaranteed. However, tertiary hospitals must provide additional workforce, material, and financial resources to support primary hospitals.
Discussion: Therefore, it is necessary to coordinate the interests of the medical staff at different levels of medical institutions. The study makes a significant contribution to the literature because it highlights the effect of medical alliances in promoting hierarchical diagnosis and treatment.
1 Introduction
In 2009, the Central Committee of the Communist Party of China and the State Council issued a new medical reform policy (1). The goal was to effectively alleviate the problem of “high medical service expenses for the masses” and gradually establish a system of hierarchical diagnosis and treatment (HDT) and two-way referrals. In 2015, the General Office of the State Council published the Guiding Opinions on Promoting the Development of the HDT System and specified the development objectives of the HDT. The construction of a reasonable and orderly HDT system is currently touted as an effective method of solving China’s high medical service expenses problem. Medical alliances are an essential measure for constructing an HDT system. Medical alliances are regional partnerships or mutually beneficial relationships led by general tertiary hospitals. They comprise several tertiary, secondary, and community health service centers (2), which help increase access to additional resources, achieve long-term sustainable savings, and expand reach in communities. Based on the principle of government-led overall planning, a consortium is formed according to the functions, positioning, and levels of different medical institutions. Medical alliances are necessary to promote people to realize the hierarchical diagnosis and treatment pattern of primary diagnosis, two-way referral, acute and chronic division, and upper and lower linkage in the process of medical treatment. It is imperative to focus on the effect of medical alliances on promoting the establishment of an HDT system and whether they have effectively solved the problem of high expenses of medical services for the masses.
Throughout the literature [i.e., (3–6)], many scholars have studied the operational mechanism of medical alliances from different angles. However, evaluation research on medical staff under the medical alliance mode is mostly sporadic, and no scholars have studied the incentive mechanism of medical staff from the perspective of medical alliances. Medical staff is the most flexible part of the medical alliance. How to effectively improve the satisfaction and work enthusiasm of medical staff has become a major issue for the stable development of medical alliances. Medical staff undertake various tasks, including creating schemes, coordinating and organizing referrals, and teaching and training fellows and residents as essential components of medical alliances (7). Therefore, it is crucial to promote and popularize the establishment of medical alliances and evaluate and analyze the effect of these medical alliances on establishing an HDT system from the medical staff perspective (8). This study evaluated the understanding of medical staff in Fujian Province regarding the effect of medical alliances on establishing an HDT system as part of medical reform. The objective was to provide a reference for the role of medical alliances in promoting HDTs in Fujian Province and provide a reference for relevant management personnel in formulating policies and further promoting the formation of medical alliances and HDTs.
2 Materials and methods
2.1 Source of materials
Participants were selected based on the following inclusion criteria: their medical institutions had established medical alliances for more than 5 years, aged 18 years or older, a minimum of 3 years of working experience, and were on duty during the survey. A stratified sampling method was used to select typical and representative medical institutions from nine cities in Fujian Province, including three provincial hospitals, five municipal hospitals, four county hospitals, and nine community medical service or township health centers (see below for explanation of medical institution levels). A total of 21 hospitals at all levels were used as sample institutions. The criteria of stratified sampling were applied according to the proportion of medical staff in each city and each member unit of the medical alliances. The proportion of personnel was randomly selected according to the probability-proportional-to-size sampling method, resulting in 321 people from tertiary hospitals (municipal hospital or provincial hospital), 175 people from secondary hospitals (county-level hospital), and 120 people from primary hospitals (community medical service center or township health center).
2.2 Medical institution levels
Community medical service centers or township health centers: These are primary health care institutions that directly provide comprehensive medical, prevention, rehabilitation, and health services for communities. The total number of these institutions’ hospital beds ranges from 20 to 99.
County-level hospitals: These are regional hospitals providing medical and health services to several communities and technical centers for regional medical prevention. The total number of their hospital beds ranges from 100 to 499.
Municipal and provincial hospitals: These provide medical and health services across regions, provinces, cities, and the entire country. They are medical prevention technology centers with comprehensive medical, teaching, and scientific research capabilities. The total number of their beds is more than 500. Municipal hospitals mainly serve patients in the city area, while provincial hospitals provide medical services for the entire province and in the surrounding provinces and cities.
2.3 Study methods
2.3.1 Questionnaire survey method
Based on the social division of labor and stakeholder theory, self-compiled questionnaires were used to collect information and materials on the medical staff’s evaluation of medical alliances in promoting the HDT system. The questionnaire content included basic information, an evaluation of medical alliances in promoting HDT, and suggestions for improvement. The basic information included medical institution level, medical staff post and professional title, workload changes after medical alliance establishment, and satisfaction with medical alliances. The evaluation of medical alliances in promoting HDT included effect evaluation of medical alliances in promoting the establishment of HDT and solving the problem of high expenses for medical services. Suggestions for improvement included ideas for further measures to improve the formation of medical alliances.
2.3.2 Statistical analysis method
Epidata 3.1 was used to input the questionnaire data and SPSS 20.0 was applied to analyze the data. Measurement data conforming to a normal distribution were expressed as the mean ± standard deviation and compared using an independent sample t-test. Measurement data that did not conform to a normal distribution were expressed as medians (lower quartiles and upper quartiles) and compared using the Kruskal–Wallis and Mann–Whitney U rank sum tests. Count data were expressed as rates and compared using the χ2 test. p < 0.05 was considered statistically significant. Univariate analysis and multivariate linear regression analysis were applied.
We analyzed the reliability of the questionnaire using Cronbach’s alpha coefficient and obtained a coefficient of 0.823; thus, the reliability level was high. The validity of the questionnaire was analyzed and measured using the KMO index. The KMO index value was 0.875, the Bartlett sphericity test chi-square value was 4138.527, and the p-value was 0.000. The validity level was considered good. The reliability and validity of the questionnaire passed the test and were suitable for questionnaire analysis.
2.3.3 Quality control
The surveyors were extensively trained and confidentiality was confirmed before administration of the questionnaire. Each questionnaire was uniformly numbered and reviewed repeatedly and carefully. Therefore, unqualified questionnaires with incomplete information or contradictory answers were removed and excluded. Questionnaires were entered dually to ensure data entry quality.
3 Results
3.1 Basic information about the medical staff
A total of 700 questionnaires were distributed and 656 were collected with a recovery rate of 93.71%. Among them, 616 questionnaires were found to be valid, with an effective rate of 93.90%. Table 1 shows the details of the 616 respondents. Most respondents were employees of municipal hospitals (35.71%), followed by county-level hospitals (28.41%), community medical services or township health centers (19.48%), and provincial hospitals (16.40%). The posts held by the respondents were mainly clinical positions, accounting for 45.45%. The respondents mainly comprised medical staff personnel with junior professional titles (40.91%). Regarding changes in workload after the medical alliance establishment, 53.25% experienced no change, 43.83% experienced an increase, and only 2.92% experienced a decrease. In terms of satisfaction with the medical alliances, 55.19% were satisfied, 40.10% were not satisfied, and 4.71% were generally dissatisfied (Table 1).
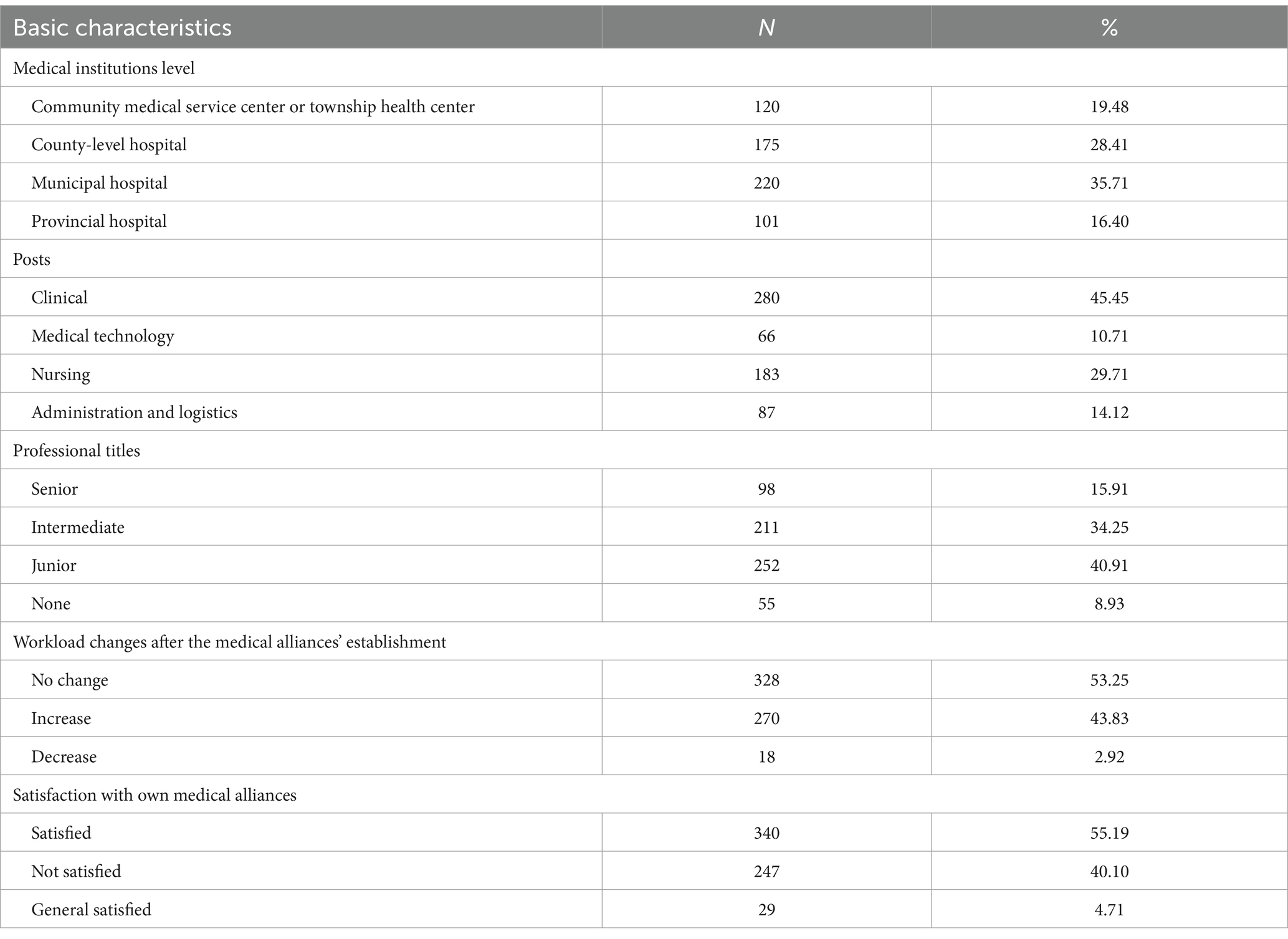
Table 1. Basic information of medical staff surveyed.
3.2 Evaluation of medical alliances in promoting HDT
Regarding the effective evaluation of medical alliances in promoting the establishment of HDTs, among the 616 respondents, 17.37% (n = 107) considered it to have no effect, 50.00% (n = 308) assessed it as having an average effect, 25.65% (n = 158) considered it to have a good effect, and 6.98% (n = 43) considered the effect very good.
In terms of the effective evaluation of medical alliances in solving the problem of high expenses for medical services, of the 616 respondents, 37.50% (n = 231) considered the effect average, 28.73% (n = 177) considered the effect good, 16.07% (n = 99) considered the problem unsolvable, and 17.69% (n = 109) believed that the effect was uncertain.
3.3 Effect evaluation of medical alliances in promoting the establishment of HDT
Univariate analysis showed significant differences in the effect evaluation of medical alliances in promoting the establishment of HDT with different levels of satisfaction with one’s own medical alliances (p < 0.05). The differences in the effect evaluations of medical alliances in promoting the establishment of HDTs with different medical institution levels, posts, professional titles, and workload changes after medical alliance establishment were not significant (p > 0.05) (Table 2).
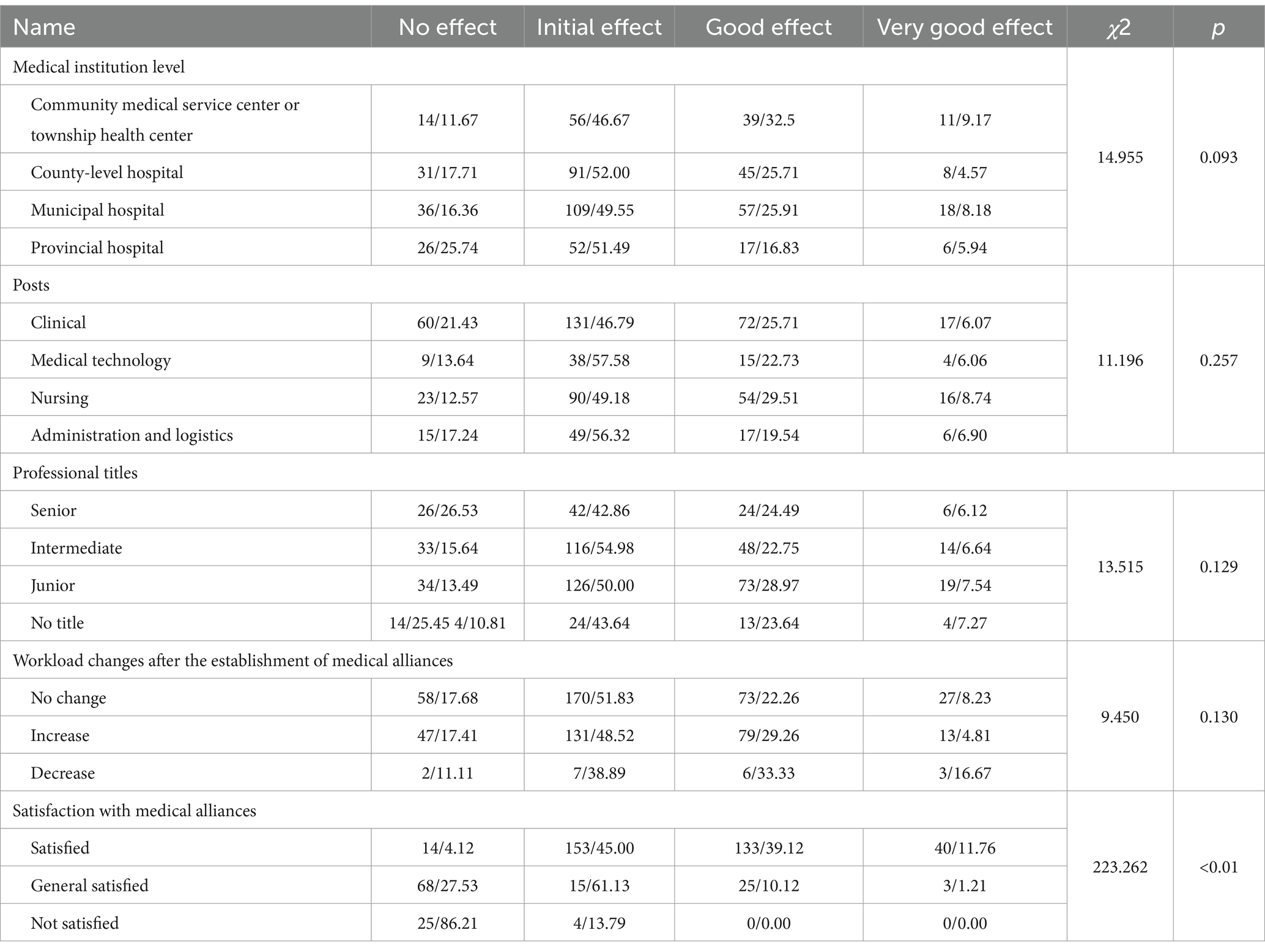
Table 2. Univariate analysis of the effect evaluation of medical alliances in promoting the establishment of HDTs (n/%).
3.4 Effect evaluation of medical alliances in solving the problem of high expenses for medical services
Univariate analysis showed that the differences in the effect evaluation of medical alliances in solving the problem of high expenses for medical services with different medical institution levels, staff posts, professional titles, and satisfaction with one’s own medical alliances and medical institutions were significant (p < 0.05). The differences in the effect evaluation of medical alliances in solving the problem of high expenses for medical services with different workload changes after medical alliance establishment were insignificant (p > 0.05) (Table 3).

Table 3. Univariate analysis of the effect evaluation of medical alliances in solving the problem of “high expenses for medical services” (n/%).
According to univariate analysis, the differences in medical institution levels, staff posts, professional titles, and satisfaction with one’s own medical alliances were significant. Multiple regression analysis was performed considering effect evaluation scores as dependent variables and medical institution levels, staff posts, professional titles, and satisfaction with one’s own medical alliances as independent variables, as shown in Table 4.
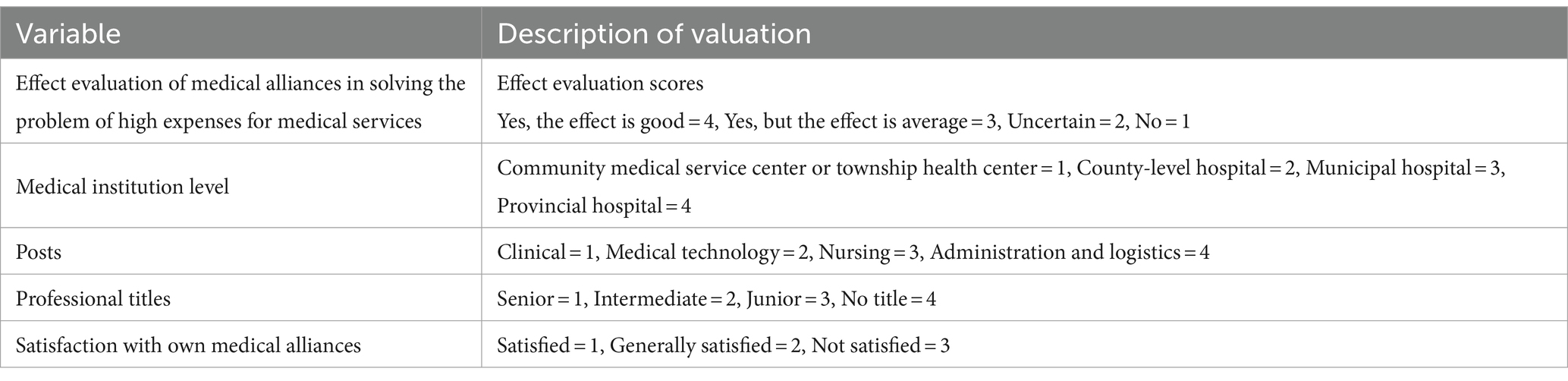
Table 4. Variable assignment table.
This analysis revealed the statistical significance of the determination coefficient (F = 293.899, p < 0.001), showed that the model was statistically significant. Posts, Medical institution level and satisfaction with their medical alliances influenced the respondents’ evaluation of the effect of medical alliances in resolving the problem of high expenses for medical services (Table 5).
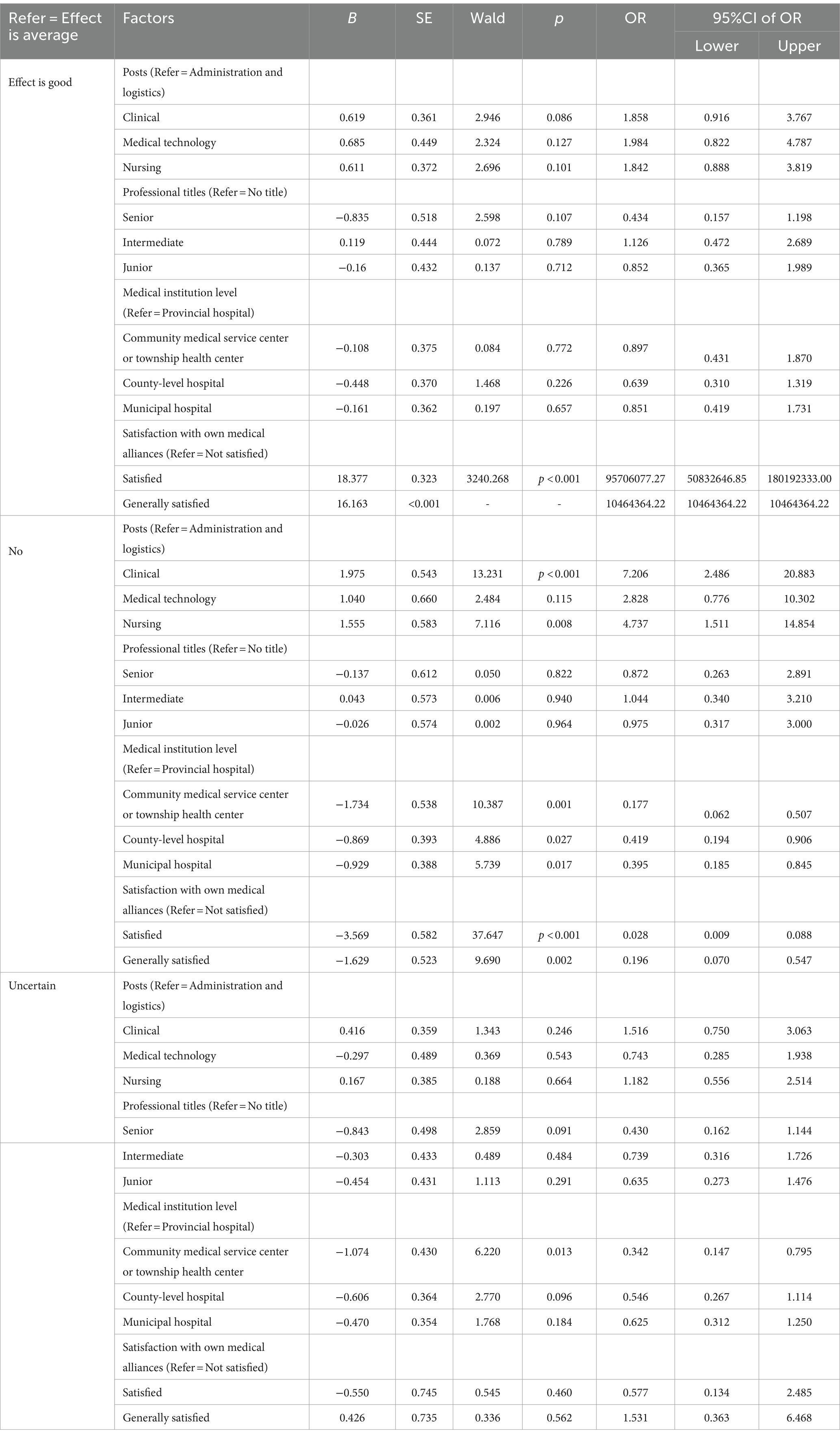
Table 5. Results of multiple regression analysis.
As shown in Figure 1, multiple correspondence analyses showed that medical staff not satisfied with the medical alliances tended to evaluate them as having no effect. Those satisfied with the medical alliances and community medical service or township health centers tended to evaluate the alliances as having a good effect. Moreover, those staffs from county-level hospitals, Medical technology, Nursing tended to evaluate them as having an average effect, and those generally satisfied with the medical alliances tended to be uncertain about the effect.
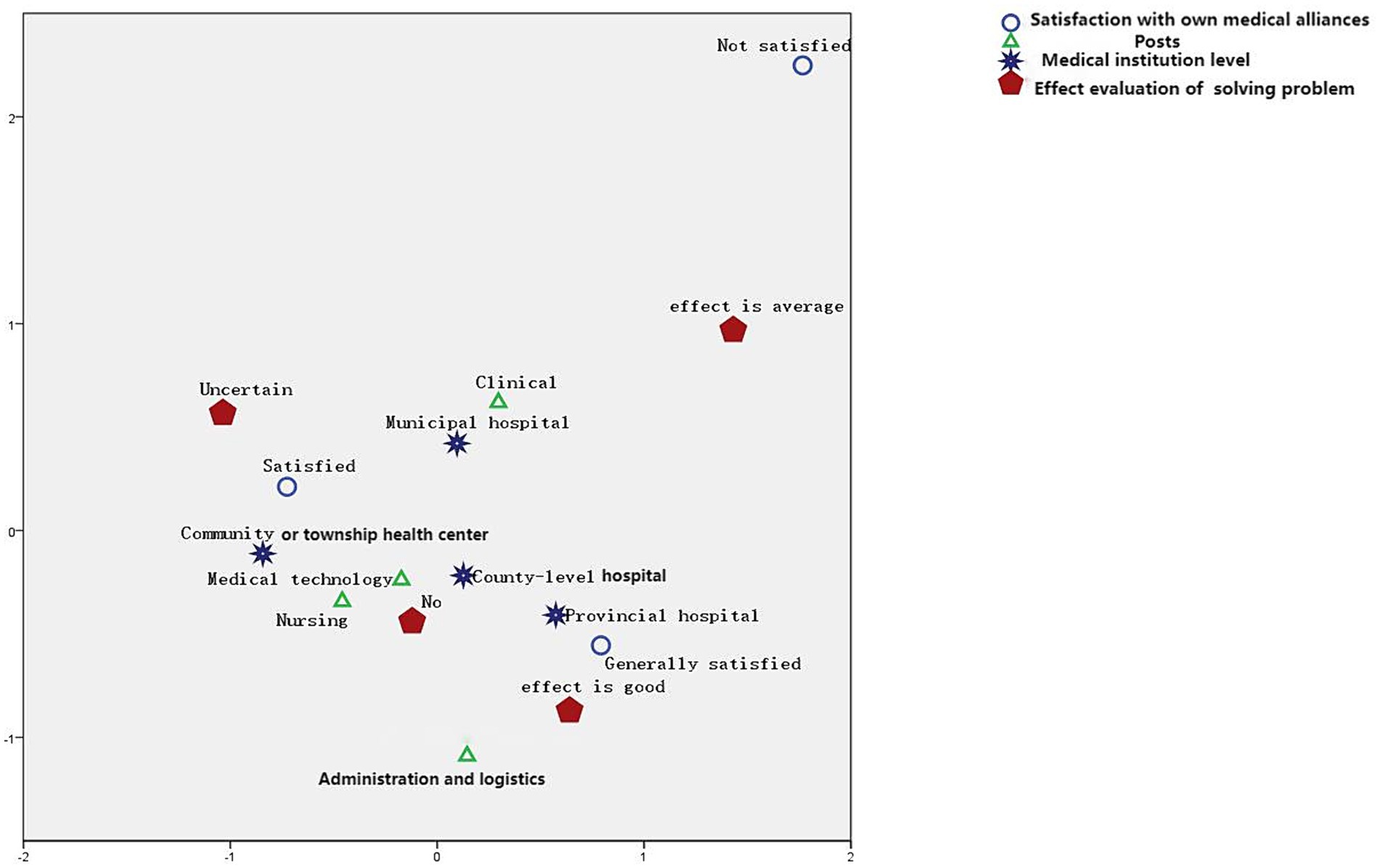
Figure 1. Results of multiple correspondence analysis.
We asked the respondents to suggest further measures to improve the construction of medical alliances. For this, we included relevant multiple-choice questions in the questionnaire. As shown in Figure 2, the medical staff believed that the three most important aspects to improving the formation of medical alliances are the coordination of the interests of the medical staff at different levels of medical institutions, smoothening of two-way referral channels, and strengthening of the construction of health information platforms.

Figure 2. Suggestions of medical staff for the establishment of a medical alliance.
4 Discussion
4.1 Overall evaluation of medical staff on medical alliances
The study results indicated that 50.00% of the medical staff respondents considered the medical alliances to have an average overall effect on establishing HDT. Only 28.73% of the medical staff believed that the medical alliances could solve the problem of high expenses for medical services and that their effect was good. In addition, 40.10% of medical staff were not satisfied with the medical alliances. Moreover, the medical staff in medical alliances generally believed that the effect of medical alliances on HDTs is average, and they are not very satisfied with the medical alliance. As medical alliances in Fujian Province are still in their initial stages, their effect has not been highlighted. Meanwhile, some studies note a few shortcomings in all aspects of the implementation process of medical alliances, which results in a lack of satisfaction from the medical staff (9). This study highlighted the effect of medical alliances in promoting hierarchical diagnosis and treatment in details from the perspective of medical staff, compared with previous studies. Therefore, it is suggested that more efforts should be made to publicize and train medical staff regarding medical alliances, completely mobilize their enthusiasm for participation, enable them to understand and support the medical care mode of medical alliances, and gradually internalize the medical alliance mode into a sense of empathy and identity (10).
4.2 Comparative analysis of different medical staff evaluations of medical alliances in promoting HDT
The study results showed significant differences in the effect evaluation of medical alliances in promoting the establishment of HDTs with different levels of satisfaction (p < 0.05). Only 4.12% of medical staff who were satisfied with the medical alliances considered the alliances to have no effect. In contrast, 86.21% of medical staff who were not satisfied with the medical alliances considered the alliances to have no effect.
Furthermore, the study results showed that medical institution level, posts and satisfaction with the medical alliances affected the effect evaluation of medical alliances in solving the problem of high expenses for medical services. Medical staff not satisfied with the medical alliances tended to perceive no effect. Those satisfied with the medical alliances and community medical services or township health centers tended to perceive a good effect. In contrast, those staffs from county-level hospitals, Medical technology, Nursing tended to evaluate them as having an average effect, and those who were generally satisfied with the medical alliances tended to be uncertain about the effect.
Despite the level of awareness about the medical alliance policy or the evaluation of the overall effect of the medical alliance, those in primary hospitals are much more satisfied than those in tertiary hospitals (such as provincial and municipal hospitals), which is consistent with the results of similar studies [i.e., (11–13)]. This may be because the current policy of China’s medical alliance is to adjust and optimize the structural layout of medical resources and promote the sinking of high-quality resources to enhance the service capacity of primary medical institutions and promote HDT (14). Therefore, the formulation of policies and related work is more focused on primary medical institutions, and the interests of primary hospitals are more guaranteed. By contrast, tertiary hospitals must pay for more workforce, materials, and additional financial resources to support primary hospitals. After the hierarchical diagnosis and treatment system is implemented, the economic benefits of tertiary hospitals may be greatly impacted. The workload of medical staff has increased dramatically, leading to more negative performance and lower satisfaction (15). Studies have shown that after the implementation of the HDT, 71.7% of the medical staff believed that the burden of work had increased and that the performance pay did not undergo a reasonable dynamic adjustment (16). The study analyzed different medical staff evaluations of medical alliances in promoting HDT using stakeholders theory from the distribution of benefits, workload changes, medical policies, among others. The results further supplement and refine the existing literature.
4.3 Strengthen the construction of medical alliances in various ways
The study results suggest that the three most important aspects of establishing a formal medical alliance are coordination of the interests of the medical staff at different levels of medical institutions, smoothening of two-way referral channels, and strengthening of the construction of health information platforms. Among them, the coordination of the interests of medical staff in medical institutions at all levels is the most essential.
This aspect necessitates the establishment of a restriction mechanism where risks and benefits are shared within the medical alliance. Otherwise, it is difficult to realize the adjustment and integration of resources (17). Furthermore, to improve satisfaction among medical staff, the administration should meet the interests and demands of medical staff and further promote the development of the medical alliance. The interests of medical staff in medical institutions at all levels should be coordinated through risk and benefit sharing. This aims to reduce the impact on the interests of medical staff brought about by the implementation of the medical alliance and help enable the medical staff to cooperate with and support the establishment of the medical alliance mode.
A two-way referral is an important aspect of the work of a medical alliance. Currently, medical alliances lack referral “green channel” services (18), which are critical and form a bridge in implementing two-way referrals. Therefore, to realize two-way referral, it is necessary to establish a smooth and convenient referral channel. A green channel for referral can be established, and special personnel can be appointed to be in charge of arranging and coordinating appointments to clarify the referral principle, indications of patients requiring referrals, and the referral process. Furthermore, quality control indexes of two-way referrals should be perfected to reduce referral resistance and ensure the standardization and effective operation of two-way referrals.
The construction of a health information platform is an essential measure for the development of medical alliances. According to the survey data, the frequency of various activities in medical alliances is uneven, and routine activities such as expert visits and further studies are carried out frequently. Moreover, remote consultation and mutual recognition of examination results require further enhancement (19). Therefore, modern information technology should be adopted to improve the medical alliances’ resource integration and resource sharing. This allows for the broadening of the information cooperation channels between medical alliances and a regional information-sharing platform centered on the regional laboratory center, imaging center, pathology center, residents’ electronic health records, and electronic medical records (20) to realize the effective operation and scientific management of the medical alliances.
Building on existing literature, this study put forward targeted and practical policy recommendations to strengthen the construction of medical alliances in various ways. By doing so, it established the need for policy changes that could positively influence healthcare in society.
The study’s limitation is its small sample size; only 616 medical staff personnel in Fujian Province were interviewed. In addition, the questionnaire content can be further enriched.
5 Conclusion
Compared to current research, our study makes a significant contribution to the literature because it highlights the effect of medical alliances in promoting HDT. In summary, medical professionals at primary hospitals evaluated medical alliances’ promotion of HDT much better than those at tertiary hospitals. Given that primary medical institutions are more inclined toward the formulation of policies and related work, the interests of primary hospitals can be guaranteed. Moreover, tertiary hospitals must supply more workforce, material, and financial resources to support primary hospitals. Therefore, it is necessary to coordinate the interests of the medical staff at different levels of medical institutions.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by all methods were conducted in accordance with relevant guidelines and regulations. Ethical clearance (2022KY137) was granted by the ethics committee of Fujian Medical University Union Hospital. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required from the participants or the participants’ legal guardians/next of kin in accordance with the national legislation and institutional requirements.
Author contributions
ZZ: Conceptualization, Data curation, Investigation, Methodology, Software, Writing – original draft. XX: Conceptualization, Data curation, Investigation, Supervision, Writing – original draft. QW: Methodology, Project administration, Supervision, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This research was funded by Fujian Province Social Science Foundation Project in 2023 (FJ2023BF030).
Acknowledgments
We would like to express our sincere thanks to all those who extended their support during the course of our research and in the writing of this paper. Our warm gratitude also goes to friends who provided much encouragement and support.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Zhong, W . Adhere to regional linkage to promote medical groups from planning to high-quality development. Jiangsu Healthcare Admin. (2018) 12:1354–8.
2. Yong, B, Shui, X, and Xueli, D. Discussion on the trend of medical reform in China based on the development trend of international regional medical alliance. Chin J Gen Pract. (2013) 11:1827–8.
3. Rui, Z, and Qiang, F. A study on the job satisfaction of healthcare staff in public hospital under the reform of hierarchical medical system. Chin Hosp Manag. (2022) 42:19–22.
4. Mingjun, C, Jixiang, C, and Lvlin, Z. Analysis of cognitive status and impact factors of medical staff on hierarchical medical system - taking Zhenjiang as an example. Chin Health Service Manag. (2019) 36:579–82.
5. Kitsios, F, and Kamariotou, M. Job satisfaction behind motivation: an empirical study in public health workers. Heliyon. (2021) 7:e06857. doi: 10.1016/j.heliyon.2021.e06857
6. Hotchkiss, DR, Banteyerga, H, and Tharaney, M. Job satisfaction and motivation among public sector health workers: evidence from Ethiopia. Hum Resour Health. (2015) 13:83. doi: 10.1186/s12960-015-0083-6
7. Haibin, L, and Guosheng, F. A study on the cognition of doctors and patients on referral in a tertiary grade a hospital. Chin Hosp. (2017) 21:41–3. doi: 10.3969/j.issn.1671-0592.2017.04.011
8. Peihong, L, and Bin, T. A study on the current situation and countermeasures of two-way referral in a community health service center in shanghai. Med Pharm J. (2015) 24:13–6.
9. Qimin, H, Dengxiao, H, Guo, Y, Yingying, G, and Yafang, L. Medical alliance - the beneficial exploration of the Chinese-style managed medical treatment mode. J Shanghai Jiaotong Univ. (2010) 30:919–24. doi: 10.3969/j.issn.1674-8115.2010.08.012
10. Xiao, Y, and Ruan, X. Practice and thoughts of regional medical consortia in Hubei Province. Chin Hosp Manag. (2012) 32:12–3.
11. Qian, L, Fen, RL, Pei, NS, Qiuqiao, W, Jian, L, and Xin, Y. Analysis on current situation of the enthusiasm of medical staffs in a medical association. Beijing Med Soc. (2016) 29:43–6.
12. Yan, Z, and Yanbo, Q. Investigation and analysis of medical staff's cognition of medical consortium in Heilongjiang Province. Chinese health. Serv Manag. (2019) 36:654–6.
13. Yifan, Z, Zhenni, L, Baoling, W, and Hanxiang, G. Investigation on the attitude and influencing factors of medical staff in medical associations to hierarchical diagnosis and treatment. Chin Med. (2019) 32:893–8.
14. Hongliang, Z, Chunxia, M, Jie, Z, Xu, D, and Shihong, Z. Analysis on knowledge and its influencing factors of medical staff in medical union. Health Eco Res. (2020) 37:21–4. doi: 10.16766/j.cnki.issn.1674-4152.2013.12.008
15. Jing, W . Analysis of working status of medical staffs in medical alliance: a case study of a hospital in a city. Chin Health Ind. (2017) 36:189–90. doi: 10.16659/j.cnki.1672-5654.2017.36.189
16. Ling, W, Kun, Z, Rui, Z, and Aizhong, L. Cognitive status and impact of tiered medical care system implementation on medical staff. Chin J Health Pol. (2018) 11:53–7.
17. Licheng, Y, Linhui, B, Yijuan, T, and Yang, Z. Discussion on the construction of two-way referral mechanism under the mode of medical alliance. Chin Hosp. (2015) 19:33–5. doi: 10.3969/j.issn.1671-0592.2015.07.014
18. Yiqun, Z, Peihao, Y, Siyi, S, and Yingmei, L. Discussion on knowledge, belief and practice of medical staffs on in the west of Putuo District, Shanghai. Chin Health Stand Manag. (2018) 9:20–3.
19. Chao, L, Fangqin, J, and Zhuoyun, W. Study on the cognition of medical staffs in Anhui Province on construction of medical alliance. Chin Hosp Manag. (2016) 36:42–5.
Keywords: medical staff, medical alliance, hierarchical diagnosis and treatment, effect evaluation, medical reform
Citation: Zhao Z, Xie X and Wu Q (2024) Medical staff evaluation on ‘the effect of medical alliance policy on hierarchical diagnosis and treatment’. Front. Public Health. 12:1366100. doi: 10.3389/fpubh.2024.1366100
Edited by:
Mingsheng Chen, Nanjing Medical University, ChinaReviewed by:
Yanbing Zeng, Capital Medical University, ChinaZhongming Chen, Weifang Medical University, China
Copyright © 2024 Zhao, Xie and Wu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Qinde Wu, cWR3dTg4QDEyNi5jb20=
†These authors have contributed equally to this work