 Yannick Munyeku-Bazitama1,2,3*
Yannick Munyeku-Bazitama1,2,3* Patient Okitale-Talunda3Justus Nsio-Mbeta4
Patient Okitale-Talunda3Justus Nsio-Mbeta4 Patrick Mpingabo-Ilunga3Paul Tshiminyi-Munkamba1Aimé Umba-Phuati5Jacques Kimfuta5Ferdinand Ango-Phukuta5Goethe Makindu5Raymond Mufwaya-Nsene6
Patrick Mpingabo-Ilunga3Paul Tshiminyi-Munkamba1Aimé Umba-Phuati5Jacques Kimfuta5Ferdinand Ango-Phukuta5Goethe Makindu5Raymond Mufwaya-Nsene6 Ryoko Asari6,7Saeda Makimoto6Steve Ahuka-Mundeke1,3
Ryoko Asari6,7Saeda Makimoto6Steve Ahuka-Mundeke1,3 Mitsuo Isono6Sheila Makiala-Mandanda1,3*Jean-Jacques Muyembe-Tamfum1,3
Mitsuo Isono6Sheila Makiala-Mandanda1,3*Jean-Jacques Muyembe-Tamfum1,3- 1Département de Virologie, Institut National de Recherche Biomédicale, Kinshasa, Democratic Republic of the Congo
- 2Division of Global Epidemiology, International Institute for Zoonosis Control, Hokkaido University, Sapporo, Japan
- 3Département de Biologie Médicale, Faculté de Médecine, Université de Kinshasa, Kinshasa, Democratic Republic of the Congo
- 4Direction de Surveillance Epidémiologique, Ministère de la Santé, Hygiène et Prévention, Kinshasa, Democratic Republic of the Congo
- 5Division Provinciale de Santé du Kongo Central, Matadi, Democratic Republic of the Congo
- 6Japan International Cooperation Agency, Tokyo, Japan
- 7Departments of Virology and Parasitology, Graduate School of Medicine, Osaka Metropolitan University, Osaka, Japan
Background: Several governments from African countries, including the Democratic Republic of the Congo (DRC), implemented stringent public health measures to curb COVID-19 transmission in the early phases of the pandemic. While these restrictive measures are believed to have contributed to lowering case incidence and related mortality in DRC, data on the population’s knowledge and adherence are limited. This study aimed to assess the knowledge, perception, attitudes, and practices of COVID-19 preventive measures and associated factors among adult residents of Matadi, thereby generating evidence for a strategy adjustment as the COVID-19 response is transitioning from emergency to control status.
Methods: We used data from a population-based cross-sectional study conducted in October 2021. Consenting participants were enrolled through a multi-stage cluster sampling approach and administered a pre-tested structured questionnaire using a mobile application (Epicollect 5). We analyzed adult participants’ data using STATA 15.1. Univariable and multivariable analyses were applied to identify factors associated with good knowledge, good perception, positive attitude and good practice.
Results: We included 1,269 adult respondents for the secondary analysis. One respondent in six was female. The median age was 36 years (IQR 24–50). Most respondents (76.5%) had good knowledge. Respondents aged 40–49 years and those with vocational education level were 1.7 time (AOR 1.75, 95% CI 1.07–2.87) and twice as likely (AOR 2.06, 95% CI 1.01–4.21) to have good knowledge. Preventive measures were perceived as efficient by 45% of respondents. Good perception was associated with education level, profession, average household monthly income and good knowledge. Only 40% of respondents had a positive attitude. A positive attitude was associated with age, education level, and good knowledge. Respondents having good practice represented 5.8%. Good practice was associated with good knowledge, attitude and perception.
Conclusion: Most respondents were knowledgeable, had a good perception of government-related COVID-19 preventive measures, a moderately positive attitude and an extremely low level of good practice. Current COVID-19 preventive strategies, including vaccination rollout, need adjustment into high-efficiency, context-based and risk group-specific interventions. Evidence generated by this study will improve preparedness and response to future outbreaks.
Introduction
The coronavirus disease (COVID-19) is an emerging disease caused by the severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) (1). As of November 9, 2023, 771,679,618 cases were reported worldwide, including 6,977,023 deaths (2). COVID-19 was declared a global pandemic by the World Health Organization (WHO) in March 2020 (2). Thereafter, several models predicted COVID-19 incidence and mortality would be higher in Africa given the numerous challenges faced by the healthcare systems of most African countries (3). In addition, COVID-19 vaccines, considered from the earliest phases of the pandemic as essential tools for pandemic control, were hardly available to African countries due to poor research and development capacities and vaccine nationalism (4, 5). Governments from several African countries opted for more feasible and less costly preventive measures based on previous experiences dealing with infectious disease outbreaks such as Ebola Virus Disease (6). Therefore, most governments implemented stringent public health measures to contain COVID-19 and curb transmission during the early phases of the pandemic. These measures included partial or complete lockdowns with the closure of international airports, schools and congregation points, curfew, prohibition of mass gatherings, downsizing public and private transport, and non-pharmaceutical interventions (3). The latter included mainly physical distancing, facemask wearing, avoiding crowded areas, frequent handwashing with soap, ventilation of indoor spaces, and teleworking to some extent (7). Altogether, these measures have contributed to lowering COVID-19 case incidence during the early phases of the pandemic in Africa (3). Later, these measures were progressively lifted because of their negative impact on the economy and trade. As a result, SARS-CoV-2 extensively spread, especially with the emergence of highly contagious SARS-CoV-2 variants (8, 9). Particularly, in the Democratic Republic of the Congo (DRC), the lightning of stringent public health measures after the first wave and the spread of the SARS-CoV-2 Beta variant (B.1.351) during the second wave led to a 4-fold increase in seroprevalence between the first and the second epidemic waves (16.6% vs. 76.5%) (10). While implementing restrictive COVID-19 preventive measures seems to have contributed to lowering the incidence of severe COVID-19 and related mortality in DRC (11), data on the population’s adherence to these government measures is scanty (12, 13). Adherence to preventive measures is affected by the population’s knowledge, attitudes, practice and perception (KAPP) (14, 15). Thus, understanding the population’s KAPP helps to identify gaps in the implementation of public health interventions, factors associated with poor adherence, and groups requiring more specific approaches. As the COVID-19 epidemic evolves, there is a critical need to adjust public health interventions into tailored preventive and control measures so as to prepare for future outbreaks.
In DRC, most COVID-19 studies have been conducted in Kinshasa (10, 12, 16, 17), the capital and epidemic epicenter, leaving behind cities such as Matadi in the neighboring Kongo Central province, which has sustained economic exchanges with Kinshasa. Despite the geographical proximity and trade between these two cities, the KAPPs of their respective populations regarding government preventive measures may differ. Matadi residents, including some rural communities, may consider themselves less at risk of infection and adhere less to government preventive measures. Therefore, developing mitigation strategies in Matadi based on evidence generated from Kinshasa could hamper efforts to control the epidemic in the context of limited available resources. This study aimed to assess the knowledge, attitudes, practices, and perception of government-related COVID-19 preventive measures among adult residents of Matadi and to provide insights into associated factors that should be considered to adjust the local response strategies and develop future ones.
Methods
Study design and setting
We used data from a population-based cross-sectional study conducted in Matadi from 16 October to 24 October 2021, after the third wave of the COVID-19 epidemic (11). The primary study aimed at measuring SARS-CoV-2 infection seroprevalence and associated factors. Matadi is the main seaport city of DRC and the political capital of the Kongo Central Province. It is located 352 km from Kinshasa and has an estimated population of 402,397 living in two health districts: Matadi (55%) and Nzanza (45%) (18, 19).
Study population and sample size
The minimum required sample size for the primary study was calculated considering an expected seroprevalence of at least 15%, a precision of 1%, a design effect of 2, and a nonresponse rate of 30% (11). A total of 2,241 participants were enrolled, including 1,602 adult participants (≥18 years of age), using a multi-stage cluster sampling as described elsewhere (11). Only 1,269 (79.2%) of all adult participants agreed to answer questions on government-related COVID-19 preventive measures and were considered for secondary data analysis. The minimum required sample size for the secondary analysis was 384 based on an estimated 50% proportion of adult residents having good knowledge, good perception, positive attitude and good practice toward COVID-19 preventive measures.
Data collection
A structured pre-tested questionnaire was administered to participants using a mobile application (Epicollect 5, Imperial College, London) as part of the primary study. The questionnaire was adapted following recommendations from WHO, the Ministry of Health, and a survey conducted in Kinshasa (12, 20). It included socio-demographic characteristics, current and past medical history, COVID-19 vaccination history, exposure to SARS-CoV-2, and COVID-19-related behavioral characteristics. Additionally, we collected data on participants’ knowledge, attitudes, practices, and perception of government-related COVID-19 control measures on which this secondary data analysis focused. The questionnaire was translated into local languages and administered by trained and experienced surveyors.
Key variables and assessment
Outcome variables
Knowledge of government-related COVID-19 preventive measures
To assess knowledge of government-related COVID-19 preventive measures, study participants were asked whether they knew the following seven measures: curfew, mandatory mask-wearing, quarantine, lockdown, public spaces closure, mass gathering prohibition and limitation of public transportation use. For each assessed measure, one point was assigned when a participant knew the assessed measure, while 0 point was assigned when the measure was unknown or the participant was unsure.
Perception of government-related preventive measures efficiency
Participants’ perception of government-related COVID-19 preventive measures’ efficiency was assessed using four response options, namely “not efficient”, “not sure or undecided”, “somewhat efficient”, “efficient”.
Attitudes toward COVID-19
Participants’ attitude toward COVID-19 was measured by their willingness to get the vaccine and get tested in case they experience flu-like symptoms. We used a zero to four-point Likert scale to assess each component of participants’ attitudes with the following scoring: 0 (not willing), 1 (somewhat not willing), 2 (undecided), 3 (somewhat willing), and 4 (willing).
Practice of government-related COVID-19 preventive measures
To measure the practice of government-related COVID-19 preventive measures, study participants were asked whether they practiced the following nine measures: wearing a facemask, wearing gloves, washing hands with soap, washing hands for at least 20 s, staying at home, avoiding crowded spaces, keeping 1.5 m distance, washing clothes upon returning home, and reducing public transportation use. For each measure, one point was assigned when a participant practiced the measure, while 0 was assigned when he did not.
Explanatory variables
Seven explanatory variables were considered in this secondary data analysis: sex, health district, age, education, household average monthly income, occupation, and religion.
Statistical analyses
We used STATA 15.1 (Stata Corp LLC, College Station, TX, United States) for data analysis. Proportions were used to summarize categorical variables while the median with the interquartile range was used to summarize continuous variables. The knowledge, attitude, and practice were summarized by transforming the point scale to percentages and categorized using Bloom’s cut-off-points as good/positive (80–100%), moderate/neutral (60–70%), and poor/negative (less than 60%) (14). Associations between outcomes and explanatory variables were assessed using logistic regression.
For logistic regression analyses, knowledge, attitude and practice were further categorized into two groups by considering percentages above 60 as good/positive and percentages below 60 as poor/negative. Similarly, the perception was classified as good if a respondent thought that COVID-19 preventive measures efficiently limited the disease spread.
Differences between groups were assessed using the Fisher’s Exact test or the paired t-test. We considered a p-value of <0.05 statistically significant.
Results
Sociodemographic characteristics
Overall, 1,269 adult participants from 444 households were included in the secondary data analysis, of which 57.8% (733/1,269) were recruited from the Matadi health district and 42.2% (536/1,269) from the Nzanza health district. One participant out of six was female (61.0%). The median age was 36 (interquartile range 24–50). Participants aged 18 to 28 represented one-third of the respondents (34.4%). More than half participants (54.2%) had achieved secondary education, whereas 5.9% had no formal education and nearly one-fifth (19.6%) had university-level education. Most participants (91.7%) lived in households with a monthly average income between US $ 1 and 250. Nearly nine participants in 10 (87.5%) were Christian (Table 1).
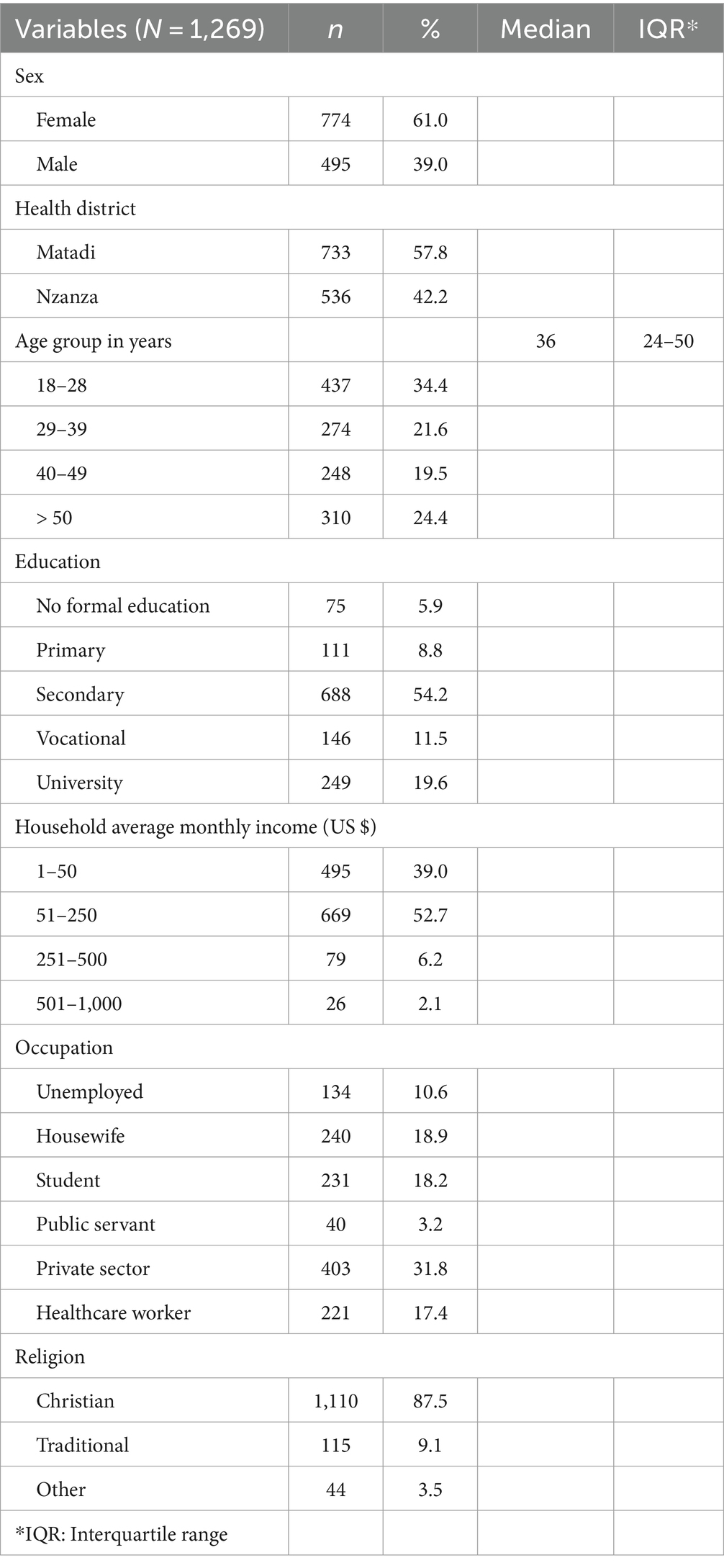
Table 1. Sociodemographic characteristics of study participants.
Knowledge of government-related COVID-19 preventive measures
Three respondents in four (75.6%) had good knowledge. In contrast, nearly one-fifth (19.8%) had poor knowledge and 4.6% had average knowledge. Most respondents heard about the COVID-19 vaccine (76.8%) and only 36.3% knew the location of the nearest COVID-19 testing center. Regarding specific knowledge questions, at least 80% of respondents knew COVID-19 preventive measures recommended by the government, though nearly four respondents in 10 (38.9%) did not recognize lockdown as one of these measures (Table 2).
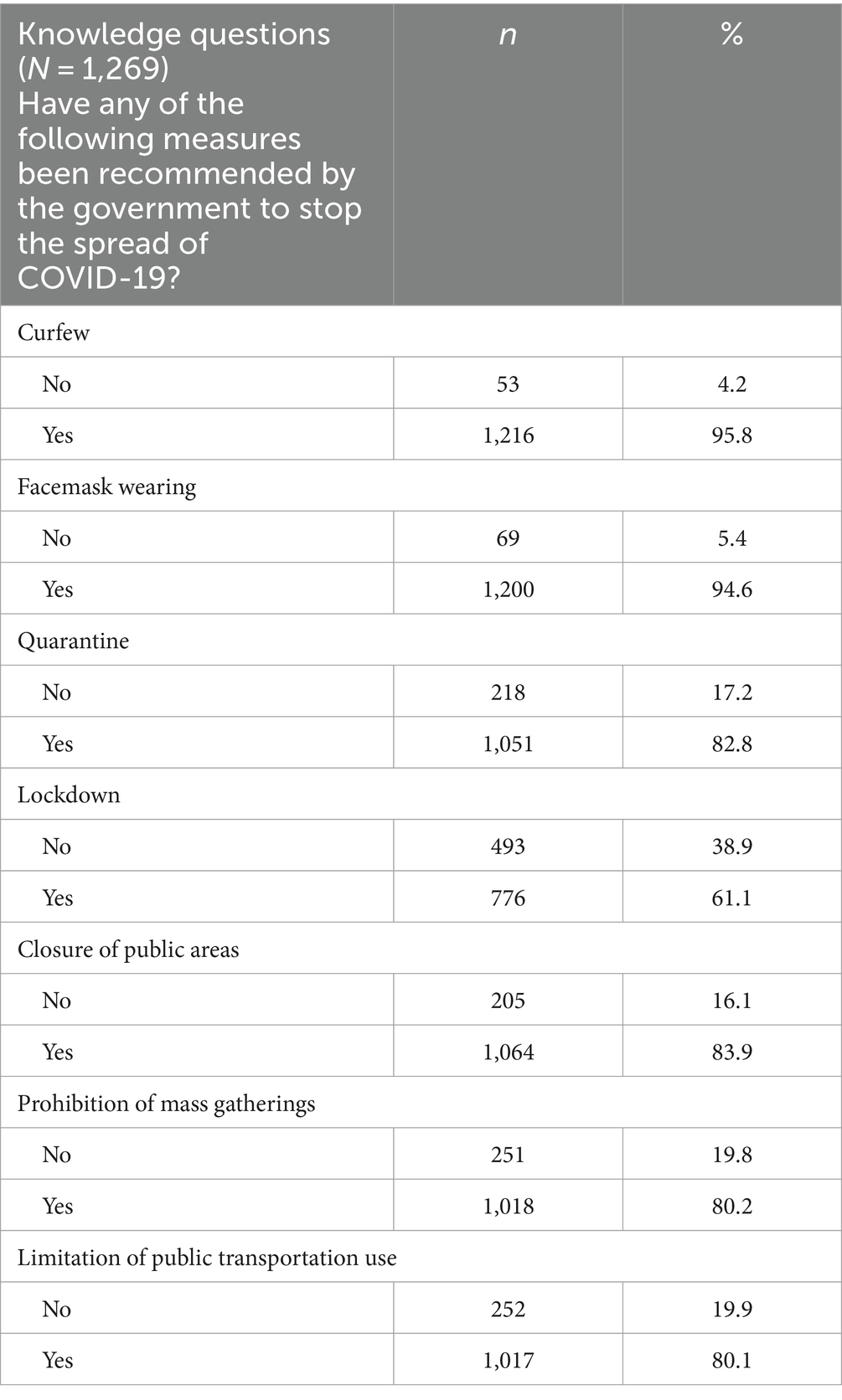
Table 2. Participants’ knowledge of government-related COVID-19 preventive measures.
The multivariable analysis of data revealed that being 40–49 years of age and having a vocational education were associated with good knowledge. Respondents 40–49 years of age had 75% increased odds of having a good knowledge than those 18–28 years of age (AOR 1.75, 95% CI 1.07–2.87, p = 0.025). Similarly, the odds of having good knowledge were twice as high among respondents with a vocational education than those with no formal education (AOR 2.06, 95% CI 1.01–4.21, p = 0.047; Table 3).

Table 3. Factors associated with participants’ knowledge of government-related COVID-19 preventive measures.
Perception of government-related COVID-19 preventive measures efficiency
Overall, 45.0% of respondents perceived the government’s COVID-19 preventive measures as efficient in limiting the spread of COVID-19 in DRC. Nearly 39% of respondents perceived these measures as somewhat efficient, 10.9% were unsure, and 5.2% thought they were inefficient. Respondents from the Nzanza health district were 43% less likely to perceive COVID-19 preventive measures as efficient than respondents from the Matadi health district (AOR 0.57, 95% CI 0.44–0.74, p = 0.000; Table 4). Similarly, respondents with primary, secondary, vocational, and university education were, respectively, 53% (AOR 0.47, 95% CI 0.25–0.90, p = 0.023), 56% (AOR 0.44, 95% CI 0.26–0.77, p = 0.004), 78% (AOR 0.22, 95% CI 0.11–0.42, p = 0.000) and 57% (AOR 0.43, 95% CI 0.24–0.79, p = 0.006) less likely to perceive COVID-19 preventive measures as efficient than respondents with no formal education. However, we observed a trend toward increased odds of perceiving preventive measures as efficient with household average monthly income. Respondents from households with an average monthly income of US $ 51–250, US $ 251–500, and US $ 501–1,000 were, respectively, 1.7 (AOR 1.74, 95% CI 1.35–2.24, p = 0.000), 3.8 (AOR 3.89, 95% CI 2.29–6.64, p = 0.000), and 54.2 times (AOR 54.2, 95% CI 7.12–413, p = 0.000) more likely to perceive COVID-19 preventive measures as efficient than respondents from households with an average monthly income of US $ 1–50 (Table 4). Similarly, respondents with good knowledge were twice as likely to perceive preventive measures as efficient (AOR 2.49, 95% CI 1.82–3.43, p = 0.000). Regarding respondents’ occupation, students (AOR 1.79, 95% CI 1.07–3.01, p = 0.026) and public servants (AOR 2.28, 95% CI 1.06–4.93, p = 0.035) were more likely to perceive COVID-19 preventive measures as efficient than unemployed respondents.
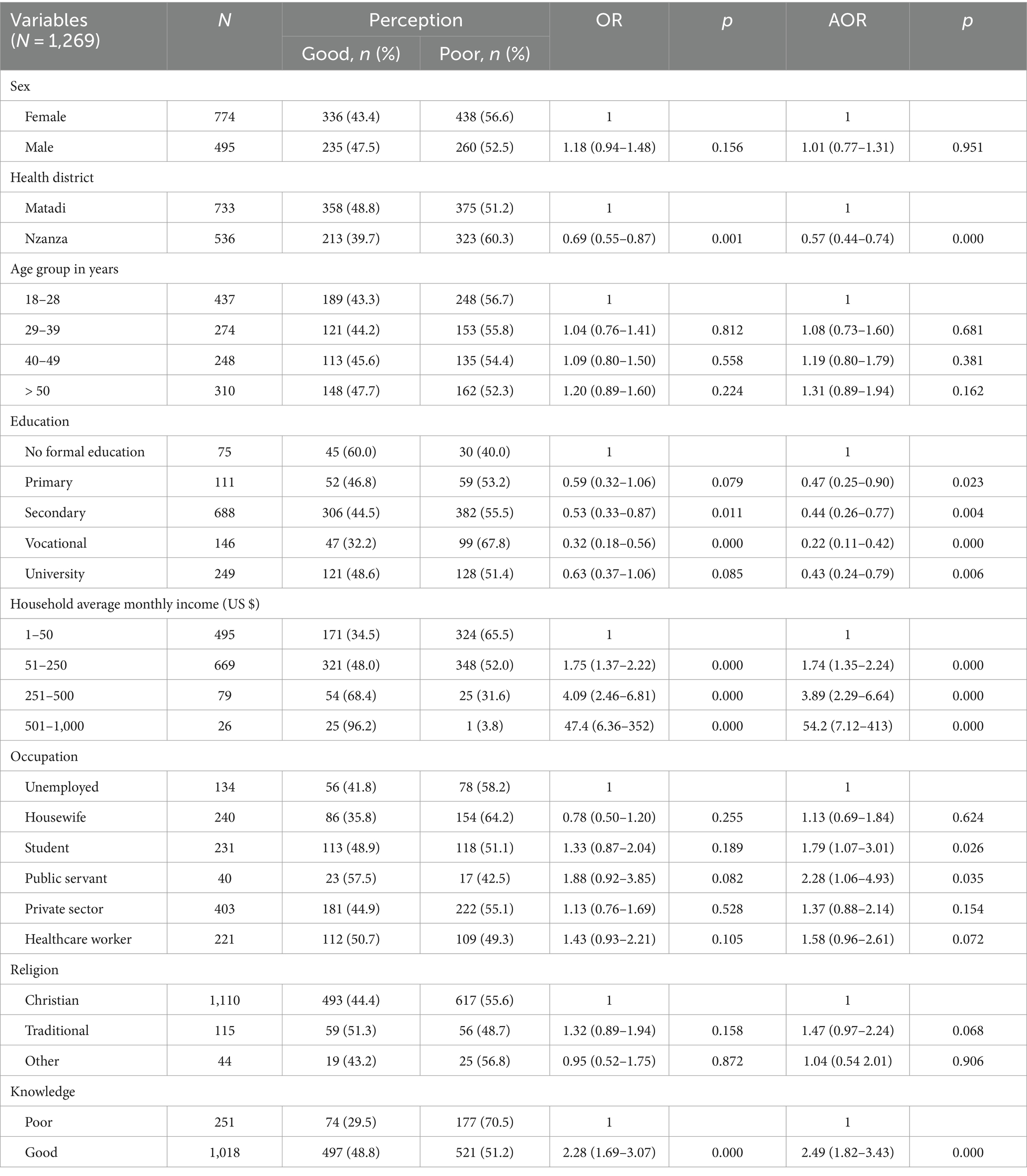
Table 4. Factors associated with participants’ perception of government-related COVID-19 preventive measures efficiency.
Attitude toward COVID-19
Almost 40% of respondents had a positive attitude, while 36.6% had a negative attitude, and 23.5% had a neutral attitude toward the assessed COVID-19 preventive measures. More than half of respondents (54.5%) were willing to get a COVID-19 test if they experienced flu-like symptoms, while only 40.2% were willing to get the COVID-19 vaccine (Table 5). We found a trend toward increased odds of positive attitude regarding COVID-19 preventive measures with age. Respondents aged 29–39 years, 40–49 years, and more than 50 years were, respectively, 1.5 (AOR 1.50, 95% CI 1.04–2.19, p = 0.031), 2.1 (AOR 2.07, 95% CI 1.39–3.08, p = 0.000) and 2.4 times (AOR 2.38, 95% CI 1.62–3.50, p = 0.000) more likely to have a positive attitude than those 18–28 years of age (Table 6). Similarly, respondents with good knowledge were 55% more likely to have a good attitude (AOR 1.55, 95% CI 1.15–2.08, p = 0.003). However, respondents with primary or vocational education were less likely to have a positive attitude than respondents with no formal education. They had, respectively, 54 and 59% decreased odds of positive attitude (AOR 0.46, 95% CI 0.24–0.91, p = 0.025 and AOR 0.41, 95% CI 0.21–0.80, p = 0.009).
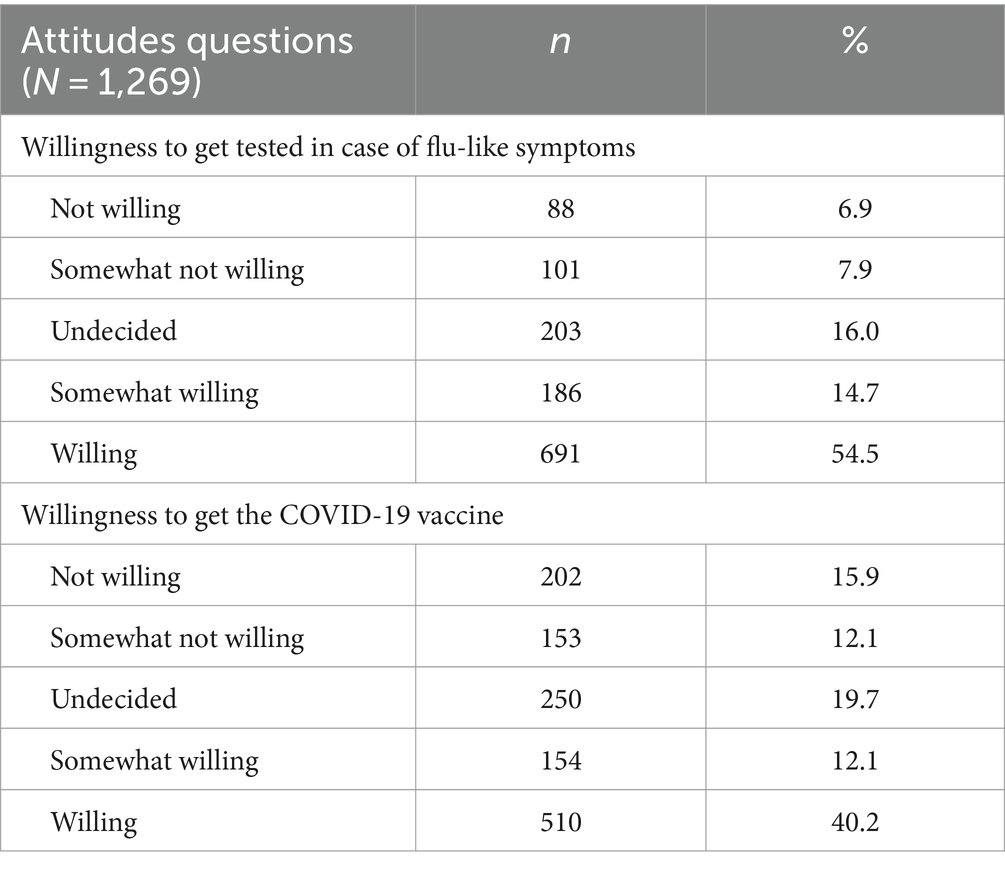
Table 5. Participants’ attitudes toward COVID-19 preventive measures.
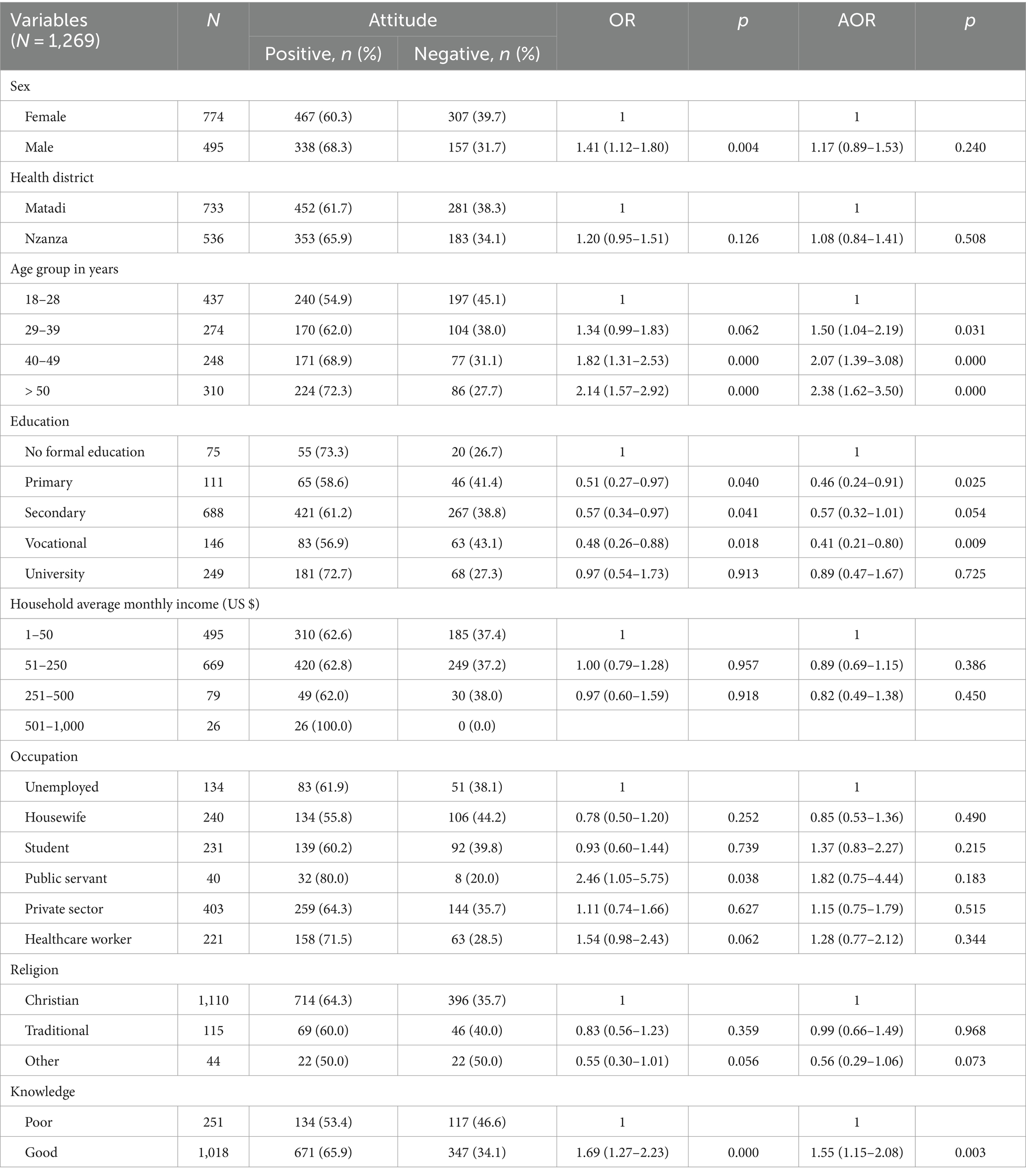
Table 6. Factors associated with participants’ attitude toward COVID-19 preventive measures.
Practice of government-related COVID-19 preventive measures
Most respondents (80.8%) had poor practice, whereas only 5.8% had good practice of COVID-19 preventive measures when the survey was conducted. Compared to early phases of the pandemic, facemask wearing was still the most practiced preventive measure at the time of data collection despite a slight decrease. The proportion of respondents practicing measures such as staying at home, avoiding crowded spaces, keeping a 1.5 m distance, washing clothes upon returning home, or reducing the use of public transportation decreased by nearly half at the time of data collection than during early phases of the pandemic (Table 7). The mean practice score during the survey period (3.22 ± 2.28) was lower as opposed to earlier phases of the pandemic (4.63 ± 2.51), with a statistically significant decrease in score of 1.40 (95% CI 1.25–1.55, p < 0.000).
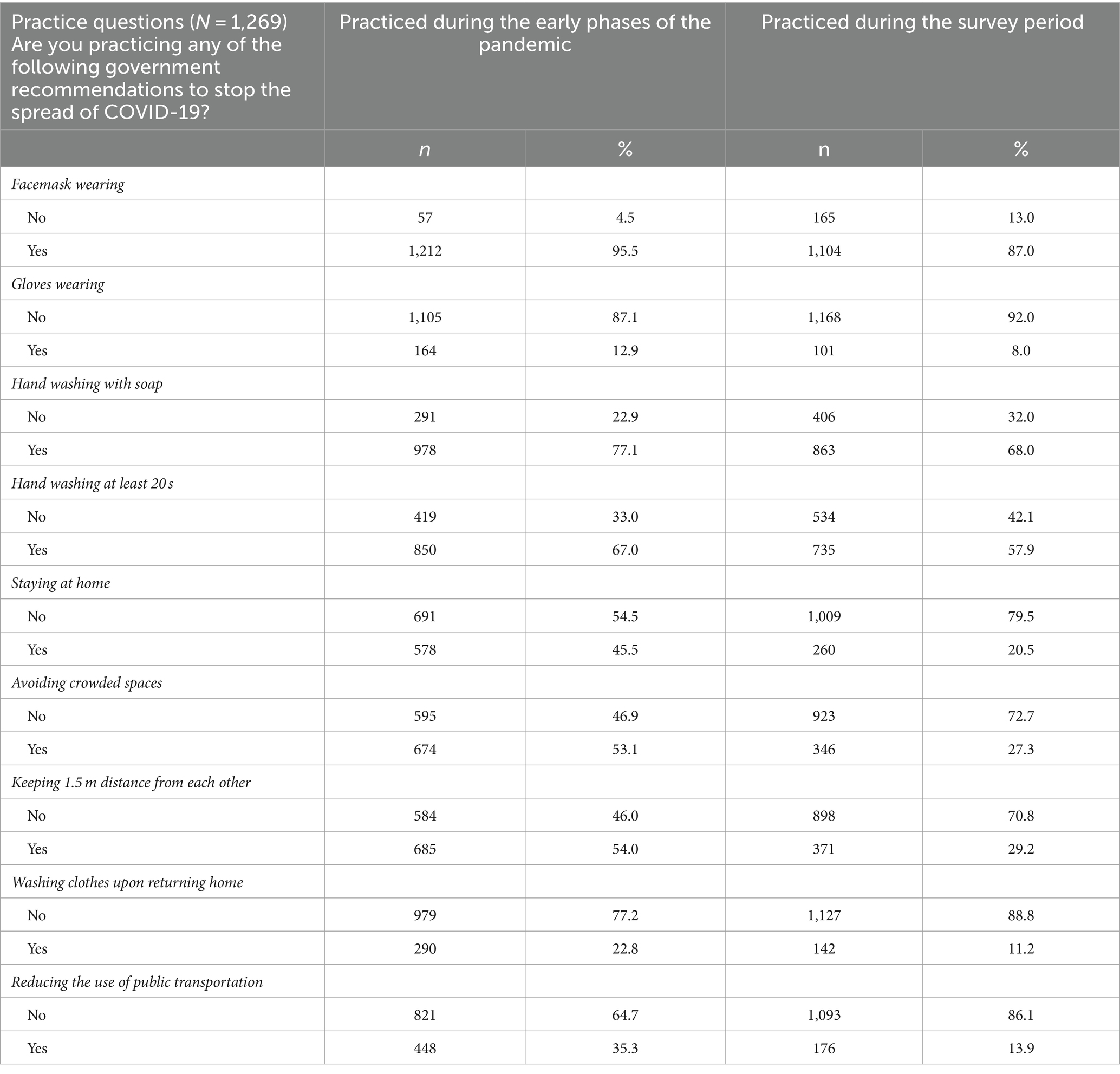
Table 7. Participants’ practice of government-related COVID-19 preventive measures.
Regarding COVID-19 vaccination status, only 18/1,269 (1.4%) respondents had received at least one dose of vaccine, most of whom were healthcare workers 8/18 (44.4%).
The multivariable analysis showed that respondents from the Nzanza health district were 43% less likely to practice COVID-19 preventive measures than those from the Matadi health district (AOR 0.57, 95% CI 0.41–0.81, p = 0.002; Table 8). Similarly, students were 53% less likely to practice COVID-19 preventive measures than unemployed respondents (AOR 0.47, 95% CI 0.24–0.95, p = 0.034). On the contrary, respondents with primary education were twice as likely to practice COVID-19 preventive measures than those without formal education (AOR 2.77, 95% CI 1.21–6.38, p = 0.016). Respondents living in households with an average monthly income of US $ 51–250 were nearly twice as likely to practice COVID-19 preventive measures than respondents from households with an average monthly income of US $ 1–50 (AOR 1.79, 95% CI 1.28–2.52, p = 0.001).
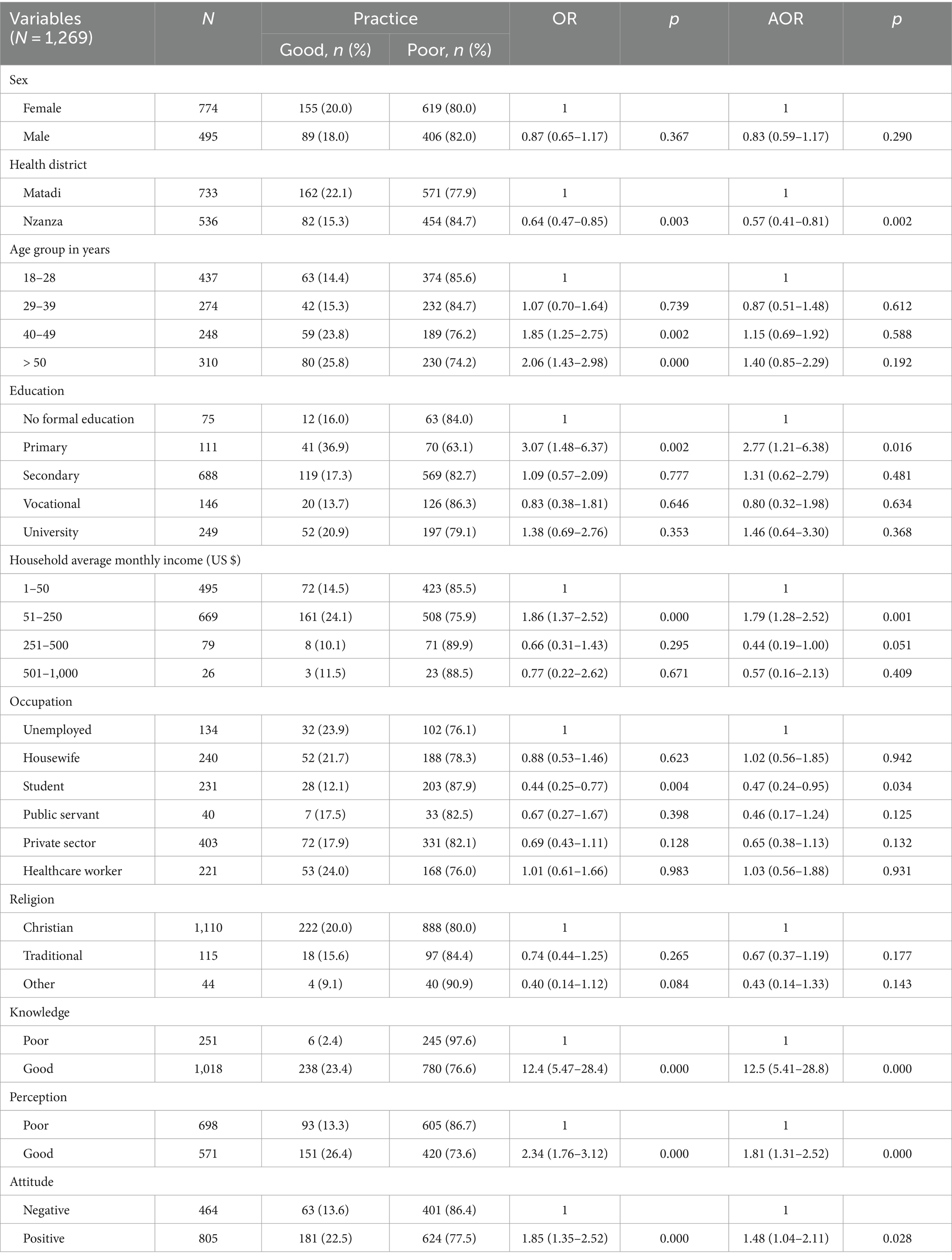
Table 8. Factors associated with participants’ practice of COVID-19 preventive measures.
Regarding the influence of knowledge, attitude, and perception on practice, respondents with good knowledge, positive attitude or good perception were, respectively, 12.5 (AOR 12.5, 95% CI 5.41–28.8, p = 0.000), 1.5 (AOR 1.48, 95% CI 1.04–2.11, p = 0.028), and 1.8 (AOR 1.81, 95% CI 1.31–2.52, p = 0.000) times more likely to practice COVID-19 preventive measures than respondents with poor knowledge, negative attitude or poor perception (Table 8).
Discussion
We conducted a cross-sectional study to assess the knowledge and perception of government-related COVID-19 preventive measures, attitudes, and practices among adult residents of Matadi and to determine associated factors. Our results indicate that 75.6% of respondents had good knowledge of the assessed COVID-19 preventive measures. Studies conducted in Ethiopia and Uganda earlier during the pandemic reported similar results (14, 21, 22). However, this finding is slightly lower than one could expect since the study was conducted by the end of the third epidemic wave after several awareness campaigns on COVID-19 prevention were implemented by the local COVID-19 response team. A high proportion of respondents (76.8%) had heard about the COVID-19 vaccine nearly 5 months after the vaccination campaign started, highlighting the effectiveness of awareness campaigns on vaccines as a pillar for COVID-19 prevention. Conversely, only 36.3% of respondents knew the nearest COVID-19 testing center. This result underscores the poor health service utilization resulting from limited testing capacities, the stigma and misconception about COVID-19.
The likelihood of good knowledge of preventive measures increased with age, especially for respondents aged 40–49. This is consistent with studies conducted in Ethiopia, Spain, and Uganda, where older age was associated with good knowledge (14, 21–23). Respondents aged at least 40 are more likely to be exposed to information and have the adequate background to process it, partly because they might have experienced or heard of previous outbreaks. Similarly, the likelihood of good knowledge increased with education level, especially for respondents with vocational training. Several studies have reported a similar trend (13, 14, 21, 22). People with high education level know how critical information is and are more exposed to information through various channels (e.g., social media, websites, community events) either passively or actively.
Government-related preventive measures were perceived as efficient by 45.0% of respondents. Similar results have been reported in other countries, with slight variations depending on the level of trust in governments and public hospitals (24–26). However, in our study, the more respondents were educated, the less likely they perceived government measures as efficient. A study in 12 Latin American countries reported consistent results (27). The odds of perceiving preventive measures as efficient increased with the household average monthly income and being a student or public servant. Similarly, a multi-country study found that individuals from higher socioeconomic or educational status were less likely to have misperceptions about COVID-19 and government-related interventions (28). Our study population’s sociodemographic and cultural characteristics can explain the observed differences. Several approaches may improve the population’s perception, such as delivering clear, simple, positive, and consistent preventive messages using visual aids and several channels to reach a wider audience.
Regarding attitudes toward preventive measures, only 40% of respondents had a positive attitude. Similar results have been reported in DRC and Ethiopia (13, 15). Conversely, other studies in Ethiopia and Uganda reported nearly twice the proportion of respondents with a positive attitude (21, 22). Differences could be explained by respondents’ relatively higher education level and the study period. Studies reporting higher proportions of positive attitudes were conducted earlier during the pandemic when stringent public health measures were in place, and the fear of getting infected was high. Our study was conducted after three epidemic waves were recorded in DRC, with decreasing case fatality rates and thus decreasing perception of risk (29). There was a trend of reduced odds of positive attitude with education level especially for respondents with primary or vocational education. This is in line with a previous study conducted in DRC, which reported lower adherence to preventive measures among respondents with low education levels (13). These groups should be particularly targeted with tailored messages convened by peers. As reported by other studies, we found a trend toward increasing odds of positive attitude with age (15, 30). As for knowledge, the older the respondent gets, the more he is exposed to information, and the more likely his attitude will be positive.
Respondents willing to get COVID-19 vaccinated represented 54.5%. A previous study conducted a year earlier in seven provinces of the DRC reported COVID-19 vaccine acceptance rates of 55.9 and 52.0%, respectively, for all study sites and the Kongo Central province (16). Vaccine acceptance rates seemed not to have changed as the fear arising from the lack of local data on safety, rumors and conspiracy theories continued to prevail. In contrast, a longitudinal study across four waves in South Africa revealed that only 6.6% of respondents remained firmly vaccine-hesitant between survey waves (31). The large-scale vaccine rollout in health care workers contributed to sustaining respondents’ willingness to get vaccinated across survey waves despite blood clotting issues reported after the vaccination rollout (31). Our survey was conducted about 2 months after the launch of the vaccination campaign in Matadi, which started with healthcare workers as a strategy to increase population trust while protecting frontline workers. In fact, only 1.4% (18/1,269) of respondents had received at least one dose of the COVID-19 vaccine, with healthcare workers representing 44% (8/18). However, by the end of 2022, less than 4% of the DRC population had been fully vaccinated (32). Vaccine hesitancy, external aid-dependent supply, and logistic challenges have contributed to sustaining poor vaccination coverage (32). Additionally, population perception of risk has decreased over epidemic waves due to decreasing case fatality from 5.1% during the first wave to 0.9% during the fourth wave (29). Context-specific risk communication and community engagement strategies are needed for effective vaccine rollout or any other epidemic control intervention. Research and development capacities should be strengthened in African countries to cope with dependency on external supply and provide critical products that will be financially accessible and socially accepted.
Eight respondents out of 10 (80.8%) poorly practiced preventive measures. Higher proportions of respondents with better practice patterns have been reported in several studies (14, 15, 21, 22, 30). Studies reporting better practice patterns were conducted earlier during the pandemic when stringent preventive measures were in place and enforced by the law. In fact, compared to the pandemic’s early phases, our study’s mean practice score significantly decreased by 1.40. Furthermore, the proportion of respondents still practicing the assessed preventive measures decreased by half compared to the early phases of the pandemic, except for facemask wearing that nearly nine respondents out of 10 still practiced after the third epidemic wave. This finding could also reflect the progressively decreasing availability and accessibility to critical prevention resources such as masks, hand sanitizers, vaccines or testing kits. Surprisingly, respondents with a primary education level were twice as likely to practice preventive measures. Although some studies have reported an association between a higher level of education and higher odds of preventive measures practice (33, 34), a study conducted in Spain found results consistent with ours (23). Respondents with higher education may have been overloaded with information about COVID-19, causing pandemic fatigue and decreasing interest in practicing preventive measures. Therefore, preventive messages should be adapted over time to account for the long-lasting epidemic’s social and mental impact. We found that students were 53% less likely to practice preventive measures than unemployed respondents. Younger individuals and students have been disproportionately affected by COVID-19 through its impact on their daily lives and social interactions (35, 36). The frustration and psychological distress arising from prolonged restrictive measures may have contributed to decreasing their adherence to preventive measures in the long run. Youth-friendly support programs could address this issue and increase adherence to preventive measures during future epidemics. Respondents with a good knowledge of preventive measures were 12 times more likely to practice them. Similarly, respondents with a good attitude toward preventive measures were 48% more likely to practice them. This finding is in keeping with results from other studies reporting good knowledge and good attitude as determinants of good practice (15, 22, 23).
Our results revealed that although most respondents had good knowledge of COVID-19 preventive measures, they did not perceive them as efficient in controlling the disease spread, resulting in negative attitudes and poor practices. Noncompliers were mainly young, educated and with a lower socio-economic status. Noncompliance with COVID-19 preventive measures is a multifaceted concept with social, economic, psychological and political determinants. As previously reported, participants in this study failed to comply with recommendations, most likely due to pandemic fatigue and the exacerbation of pre-existing socioeconomic inequities and disparities (37). The latter may not have facilitated the emergence of social identity and accountability necessary for a collective response (38). Moreover, most respondents had lowered perceptions of risk because of the decreasing case fatality over epidemic waves and distrust of the government as a result of growing beliefs in conspiracy theories, especially on COVID-19 vaccines (38, 39). Finally, the decreasing availability and accessibility to critical tools and interventions for compliance (face masks, hand sanitizers, etc.) might have strengthened skepticism among residents. These determinants should be considered to enhance compliance and develop tailored and efficient countermeasures for future emergencies.
Our study has the merit of a robust sampling frame that yielded a large and representative sample of adult residents from Matadi. As such, it provides evidence supporting the need for adjusting current and future epidemic control strategies. However, respondents’ knowledge, attitude, practice, and perception patterns may have been rapidly evolving during the pandemic course, making the study’s cross-sectional design not optimal to capture trends over time and further elucidate the cause-effect relationship between the assessed variables. There may have been respondent bias through either exaggeration of answers or information retainment, especially for government-related questions. Finally, although logistic regression could accurately predict factors associated with good knowledge, positive attitude, good practice and good perception, other more robust machine learning techniques could have generated predictors of compliance to government preventive measures with more accuracy and precision as reported by some studies (40–43).
Conclusion
Our study has shown that by the end of the third COVID-19 epidemic wave, Matadi residents had a high level of knowledge, a good perception of government-related COVID-19 preventive measures, a moderately positive attitude and an extremely low level of good practice. Age, education level, health district, profession, average household monthly income, good knowledge, positive attitude, and good perception were identified as main determinants. Despite the moderate adherence to vaccination as a pilar for COVID-19 control, vaccine uptake was extremely low. These results underscore the need to develop and implement context-based and risk group-specific communication and community engagement strategies to respond more efficiently to future outbreaks. These strategies should include refining messages considering emotions, values, and beliefs, fostering discussions and community activities such as showcasing positive role models. As the COVID-19 response is moving from emergency to control, and variants of concern with the potential of resisting previously acquired protection are still emerging, tailored and targeted interventions are needed more than ever to sustain the current disease control. Lessons learned from the current epidemic will improve preparedness and response to future outbreaks.
Data availability statement
The data analyzed in this study is subject to the following licenses/restrictions: Data are available from the corresponding author upon reasonable request and approval by the Kinshasa School of Public Health Ethics Committee. Requests to access these datasets should be directed to SM-M, c2hlbWFraWFsYUB5YWhvby5mcg==.
Ethics statement
The studies involving humans were approved by Kinshasa School of Public Health Ethics Committee. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
YM-B: Conceptualization, Data curation, Formal analysis, Funding acquisition, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. PO-T: Investigation, Resources, Writing – original draft, Writing – review & editing. JN-M: Conceptualization, Data curation, Funding acquisition, Investigation, Methodology, Project administration, Resources, Supervision, Writing – original draft, Writing – review & editing. PM-I: Conceptualization, Funding acquisition, Methodology, Writing – original draft, Writing – review & editing. PT-M: Investigation, Resources, Writing – original draft, Writing – review & editing. AU-P: Investigation, Methodology, Resources, Supervision, Writing – original draft, Writing – review & editing. JK: Conceptualization, Resources, Supervision, Writing – original draft, Writing – review & editing. FA-P: Investigation, Methodology, Resources, Supervision, Writing – original draft, Writing – review & editing. GM: Conceptualization, Methodology, Resources, Writing – original draft, Writing – review & editing. RM-N: Conceptualization, Funding acquisition, Investigation, Methodology, Project administration, Resources, Writing – original draft, Writing – review & editing. RA: Conceptualization, Funding acquisition, Methodology, Project administration, Resources, Writing – original draft, Writing – review & editing. SM: Funding acquisition, Methodology, Project administration, Resources, Writing – original draft, Writing – review & editing, Conceptualization. SA-M: Writing – original draft, Writing – review & editing, Project administration, Funding acquisition, Conceptualization. MI: Conceptualization, Funding acquisition, Methodology, Project administration, Resources, Supervision, Writing – original draft, Writing – review & editing. SM-M: Conceptualization, Data curation, Funding acquisition, Investigation, Methodology, Project administration, Resources, Supervision, Validation, Writing – original draft, Writing – review & editing. J-JM-T: Conceptualization, Funding acquisition, Methodology, Project administration, Resources, Supervision, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. This work was conducted under the COVID-19 research project of the Japan International Cooperation Agency Ogata Sadako Research Institute for Peace and Development.
Acknowledgments
We thank all study participants and the Division Provinciale de Santé du Kongo Central. We are also grateful to field supervisors and surveyors for their valuable contribution to data acquisition.
Conflict of interest
The authors declare no conflict of interest. Authors affiliated with the funding agency facilitated the funding process and the provision of study material. They were involved in the study design, data collection, and interpretation under the leadership of an independent principal investigator from the Democratic Republic of the Congo Ministry of Health.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Abbreviations
COVID-19, Coronavirus disease 2019; SARS-CoV-2, Severe Acute Respiratory Syndrome Coronavirus 2; DRC, Democratic Republic of the Congo; KAPP, Knowledge, Attitude, Practice, and Perception; AOR, Adjusted Odd Ratio; 95% CI, 95% confidence interval
References
1. Khan, S, Siddique, R, Bai, Q, Shabana, LY, Xue, M, Nabi, G, et al. (COVID-19): causative agent, mental health concerns, and potential management options. J Infect Public Health. (2019) 13:1840–4. doi: 10.1016/j.jiph.2020.07.010
2. WHO Coronavirus (COVID-19) Dashboard . WHO coronavirus (COVID-19) dashboard with vaccination data. (2023). Available at: https://covid19.who.int/ (Accessed March 9, 2023).
3. Bwire, G, Ario, AR, Eyu, P, Ocom, F, Wamala, JF, Kusi, KA, et al. The COVID-19 pandemic in the African continent. BMC Med. (2022) 20:1–23. doi: 10.1186/s12916-022-02367-4
4. Hafner, M, Yerushalmi, E, Fays, C, Dufresne, E, and Van Stolk, C. COVID-19 and the cost of vaccine nationalism. RAND Corp. (2020) 2020:769. doi: 10.7249/RRA769-1
5. Riaz, MMA, Ahmad, U, Mohan, A, dos Santos Costa, AC, Khan, H, Babar, MS, et al. Global impact of vaccine nationalism during COVID-19 pandemic. Trop Med Health. (2021) 49:101. doi: 10.1186/s41182-021-00394-0
6. Udoakang, A, Oboh, M, Henry-Ajala, A, Anyigba, C, Omoleke, S, Amambua-Ngwa, A, et al. Low COVID-19 impact in Africa: the multifactorial Nexus. Open Res Africa. (2021) 4:47. doi: 10.12688/AASOPENRES.13261.1
7. Xylogiannopoulos, KF, Karampelas, P, and Alhajj, R. COVID-19 pandemic spread against countries’ non-pharmaceutical interventions responses: a data-mining driven comparative study. BMC Public Health. 21:1607. doi: 10.1186/s12889-021-11251-4
8. Teachout, M, and Zipfel, C. The economic impact of COVID-19 lockdowns in sub-Saharan Africa: Policy brief. (2020). Available at: https://www.wider.unu.edu/publication/estimates-impact-covid-19-global-poverty (Accessed March 8, 2023).
9. Anyanwu, JC, and Salami, AO. The impact of COVID-19 on African economies: an introduction. Afr Dev Rev. (2021) 33:S1. doi: 10.1111/1467-8268.12531
10. Munyeku-Bazitama, Y, Folefack, GT, Yambayamba, MK, Tshiminyi, PM, Kazenza, BM, Otshudiema, JO, et al. High SARS-CoV-2 seroprevalence after second wave (October 2020–April 2021), Democratic Republic of the Congo. Emerg Infect Dis. (2023) 29:89–97. doi: 10.3201/eid2901.221009
11. Munyeku-Bazitama, Y, Okitale-Talunda, P, Mpingabo-Ilunga, P, Yambayamba, MK, Tshiminyi, PM, Umba-Phuati, A, et al. High severe acute respiratory syndrome coronavirus 2 antibody prevalence after the third epidemic wave (may–October 2021) in Matadi, Democratic Republic of the Congo. Open Forum Infect Dis. (2023) 10:23. doi: 10.1093/ofid/ofad023
12. Akilimali, PZ, Mashinda, DK, Lulebo, AM, Mafuta, EM, Onyamboko, MA, and Tran, NT. The emergence of COVID-19 in the Democratic Republic of Congo: community knowledge, attitudes, and practices in Kinshasa. PLoS One. (2022) 17:e0265538. doi: 10.1371/journal.pone.0265538
13. Ditekemena, JD, Nkamba, DM, Muhindo, HM, Siewe, JNF, Luhata, C, Van Den Bergh, R, et al. Factors associated with adherence to COVID-19 prevention measures in the Democratic Republic of the Congo (DRC): results of an online survey. BMJ Open. (2021) 11:e043356. doi: 10.1136/bmjopen-2020-043356
14. Feleke, BT, Wale, MZ, and Yirsaw, MT. Knowledge, attitude and preventive practice towards COVID-19 and associated factors among outpatient service visitors at Debre Markos compressive specialized hospital, north-West Ethiopia, 2020. PLoS One. (2021) 16:e0251708. doi: 10.1371/journal.pone.0251708
15. Bukata, IT, Dadi, LS, Ayana, AM, Mengistu, D, Yewal, D, Gizaw, TS, et al. Knowledge, attitudes, and practice toward prevention of COVID-19 among Jimma town residents: a community-based cross-sectional study. Front Public Heal. (2022) 10:942. doi: 10.3389/fpubh.2022.822116
16. Ditekemena, JD, Nkamba, DM, Mutwadi, A, Mavoko, HM, Siewe Fodjo, JN, Luhata, C, et al. COVID-19 vaccine acceptance in the Democratic Republic of Congo: a cross-sectional survey. Vaccine. (2021) 9:153. doi: 10.3390/vaccines9020153
17. Nkuba, AN, Makiala, SM, Guichet, E, Tshiminyi, PM, Bazitama, YM, Yambayamba, MK, et al. High prevalence of anti–severe acute respiratory syndrome coronavirus 2 (anti–SARS-CoV-2) antibodies after the first wave of coronavirus disease 2019 (COVID-19) in Kinshasa, Democratic Republic of the Congo: results of a cross-sectional household-based Su. Clin Infect Dis. (2022) 74:882–90. doi: 10.1093/cid/ciab515
18. United Nations Office for the Coordination of Humanitarian Affaires . RDC - Statistiques des populations par zones de santé - humanitarian data exchange. (2022). Available at: https://data.humdata.org/dataset/rdc-statistiques-des-populations (Accessed July 4, 2022).
19. World Population Review . Matadi population 2022 (demographics, maps, graphs). (2022). Available at: https://worldpopulationreview.com/world-cities/matadi-population (Accessed July 8, 2022).
20. Bergeri, I, Lewis, HC, Subissi, L, Nardone, A, Valenciano, M, Cheng, B, et al. Early epidemiological investigations: World Health Organization UNITY protocols provide a standardized and timely international investigation framework during the COVID-19 pandemic. Influenza Other Respir Viruses. (2022) 16:7–13. doi: 10.1111/irv.12915
21. Ssebuufu, R, Sikakulya, FK, Mambo, SB, Wasingya, L, Nganza, SK, Ibrahim, B, et al. Knowledge, attitude, and self-reported practice toward measures for prevention of the spread of COVID-19 among Ugandans: a Nationwide online cross-sectional survey. Front Public Health. (2020) 8:731. doi: 10.3389/fpubh.2020.618731
22. Kedir, S, Yesse, M, Muze, M, Argaw, B, Dengo, M, Nesre, T, et al. Determinants of knowledge, attitude and practice towards preventive measures of COVID-19 among adult residencies in Silte zone, southern Ethiopia. Pan Afr Med J. (2022) 41:826. doi: 10.11604/pamj.2022.41.211.33826
23. González-Herrera, A, Rodríguez-Blázquez, C, Romay-Barja, M, Falcon-Romero, M, Ayala, A, and Forjaz, MJ. Age differences in knowledge, attitudes and preventive practices during the COVID-19 pandemic in Spain. Sci Rep. (2022) 12:1–8. doi: 10.1038/s41598-022-25353-5
24. Chu, Q, Gu, T, Li, A, Chen, J, Wang, H, Liu, N, et al. Perceived effectiveness of public health measures and positive attitudes during a pandemic: a large cross-sectional study in Shanghai. China BMJ Open. (2021) 11:e047231. doi: 10.1136/bmjopen-2020-047231
25. Georgieva, I, Lantta, T, Lickiewicz, J, Pekara, J, Wikman, S, Loseviča, M, et al. Perceived effectiveness, restrictiveness, and compliance with containment measures against the Covid-19 pandemic: an international comparative study in 11 countries. Int J Environ Res Public Health. (2021) 18:3806. doi: 10.3390/ijerph18073806
26. Mækelæ, MJ, Reggev, N, Dutra, N, Tamayo, RM, Silva-Sobrinho, RA, Klevjer, K, et al. Perceived efficacy of COVID-19 restrictions, reactions and their impact on mental health during the early phase of the outbreak in six countries. R Soc Open Sci. (2020) 7:200644. doi: 10.1098/rsos.200644
27. Mejia, CR, Liendo-Venegas, D, García-Gamboa, F, Mejía-Rodríguez, MA, and Valladares-Garrido, MJ. Factors associated with the perception of inadequate sanitary control in 12 Latin American countries during the COVID-19 pandemic. Front Public Health. (2022) 10:2272. doi: 10.3389/fpubh.2022.934087
28. Bhuiya, T, Klares, R, Conte, MA, and Cervia, JS. Predictors of misperceptions, risk perceptions, and personal risk perceptions about COVID-19 by country, education and income. J Investig Med. (2021) 69:1473–8. doi: 10.1136/jim-2021-001835
29. Otshudiema, JO, Folefack, GLT, Nsio, JM, Mbala-Kingebeni, P, Kakema, CH, Kosianza, JB, et al. Epidemiological comparison of four COVID-19 waves in the Democratic Republic of the Congo, march 2020–January 2022. J Epidemiol Glob Health. (2022) 12:316–27. doi: 10.1007/s44197-022-00052-6
30. Desalegn, Z, Deyessa, N, Teka, B, Shiferaw, W, Hailemariam, D, Addissie, A, et al. COVID-19 and the public response: knowledge, attitude and practice of the public in mitigating the pandemic in Addis Ababa. Ethiopia PLoS One. (2021) 16:e0244780. doi: 10.1371/journal.pone.0244780
31. Burger, R, Köhler, T, Golos, AM, Buttenheim, AM, English, R, Tameris, M, et al. Longitudinal changes in COVID-19 vaccination intent among south African adults: evidence from the NIDS-CRAM panel survey, February to May 2021. BMC Public Health. (2022) 22:422. doi: 10.1186/s12889-022-12826-5
32. Zola Matuvanga, T, Doshi, RH, Muya, A, Cikomola, A, Milabyo, A, Nasaka, P, et al. Challenges to COVID-19 vaccine introduction in the Democratic Republic of the Congo–a commentary. Hum Vaccin Immunother. (2022) 18:272. doi: 10.1080/21645515.2022.2127272
33. Bekele, F, Sheleme, T, Fekadu, G, and Bekele, K. Patterns and associated factors of COVID-19 knowledge, attitude, and practice among general population and health care workers: a systematic review. SAGE Open Med. (2020) 8:97072. doi: 10.1177/2050312120970721
34. Wake, AD . Knowledge, attitude, practice, and associated factors regarding the novel coronavirus disease 2019 (COVID-19) pandemic. Infect Drug Resist. (2020) 13:3817–32. doi: 10.2147/IDR.S275689
35. Devita, M, Di Rosa, E, Iannizzi, P, Bianconi, S, Contin, SA, Tiriolo, S, et al. Cognitive and psychological sequelae of COVID-19: age differences in facing the pandemic. Front. Psychiatry. (2021) 12:1461. doi: 10.3389/fpsyt.2021.711461
36. Romay-Barja, M, Pascual-Carrasco, M, De Tena-Dávila, MJ, Falcón, M, Rodriguez-Blazquez, C, Forjaz, MJ, et al. How patients with COVID-19 managed the disease at home during the first wave in Spain: a cross-sectional study. BMJ Open. (2021) 11:e048702. doi: 10.1136/bmjopen-2021-048702
37. Cowling, BJ, Ng, DMW, Ip, DKM, Liao, Q, Lam, WWT, Wu, JT, et al. Community psychological and behavioral responses through the first wave of the 2009 influenza a(H1N1) pandemic in Hong Kong. J Infect Dis. (2010) 202:867–76. doi: 10.1086/655811
38. Fancourt, D, Steptoe, A, and Wright, L. The cummings effect: politics, trust, and behaviours during the COVID-19 pandemic. Lancet. (2020) 396:464–5. doi: 10.1016/S0140-6736(20)31690-1
39. Uluşahin, Y, Mavor, K, and Reicher, S. A political psychology of the link between populist beliefs and compliance with COVID-19 containment measures. Front. Pol Sci. (2024) 6:798. doi: 10.3389/fpos.2024.1279798
40. Pavlović, T, Azevedo, F, De, K, Riaño-Moreno, JC, Maglić, M, Gkinopoulos, T, et al. Predicting attitudinal and behavioral responses to COVID-19 pandemic using machine learning. PNAS Nexus. (2022) 1:1–15. doi: 10.1093/pnasnexus/pgac093
41. Pradhan, AK, Mishra, D, Das, K, Obaidat, MS, and Kumar, M. A COVID-19 X-ray image classification model based on an enhanced convolutional neural network and hill climbing algorithms. Multimed Tools Appl. (2023) 82:14219–37. doi: 10.1007/s11042-022-13826-8
42. Raheja, S, Kasturia, S, Cheng, X, and Kumar, M. Machine learning-based diffusion model for prediction of coronavirus-19 outbreak. Neural Comput & Applic. (2023) 35:13755–74. doi: 10.1007/s00521-021-06376-x
Keywords: COVID-19, knowledge, attitudes, practices, perception, prevention, vaccine, noncompliance
Citation: Munyeku-Bazitama Y, Okitale-Talunda P, Nsio-Mbeta J, Mpingabo-Ilunga P, Tshiminyi-Munkamba P, Umba-Phuati A, Kimfuta J, Ango-Phukuta F, Makindu G, Mufwaya-Nsene R, Asari R, Makimoto S, Ahuka-Mundeke S, Isono M, Makiala-Mandanda S and Muyembe-Tamfum J-J (2024) Knowledge, attitudes, practices, and perception of COVID-19 preventive measures among adult residents of Matadi (Democratic Republic of the Congo) after the third epidemic wave. Front. Public Health. 12:1363717. doi: 10.3389/fpubh.2024.1363717
Edited by:
Sotirios Karampampas, University of Essex, United KingdomReviewed by:
Manoj Kumar, University of Wollongong in Dubai, United Arab EmiratesSteward Mudenda, University of Zambia, Zambia
Copyright © 2024 Munyeku-Bazitama, Okitale-Talunda, Nsio-Mbeta, Mpingabo-Ilunga, Tshiminyi-Munkamba, Umba-Phuati, Kimfuta, Ango-Phukuta, Makindu, Mufwaya-Nsene, Asari, Makimoto, Ahuka-Mundeke, Isono, Makiala-Mandanda and Muyembe-Tamfum. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Sheila Makiala-Mandanda, c2hlbWFraWFsYUB5YWhvby5mcg==; Yannick Munyeku-Bazitama, eW11bnlla3VAZ21haWwuY29t