 Biruk Beletew Abate1,2*
Biruk Beletew Abate1,2* Ashenafi Kibret Sendekie3,4
Ashenafi Kibret Sendekie3,4 Mulat Ayele2
Mulat Ayele2 Eyob Shitie Lake2
Eyob Shitie Lake2 Tilahun Wodaynew2
Tilahun Wodaynew2 Befkad Derese Tilahun2
Befkad Derese Tilahun2 Molla Azmeraw2
Molla Azmeraw2 Tesfaye Engdaw Habtie2
Tesfaye Engdaw Habtie2 Muluemebet Kassa2
Muluemebet Kassa2 Melesse Abiye Munie2
Melesse Abiye Munie2 Dessie Temesgen2
Dessie Temesgen2 Abebe Merchaw2
Abebe Merchaw2 Addis Wondimagegn Alamaw2
Addis Wondimagegn Alamaw2 Alemu Birara Zemariam2
Alemu Birara Zemariam2 Tegene Atamenta Kitaw2
Tegene Atamenta Kitaw2 Amare Kassaw5
Amare Kassaw5 Ayelign Mengesha Kassie2,6
Ayelign Mengesha Kassie2,6 Gizachew Yilak2Mulat Awoke Kassa2
Gizachew Yilak2Mulat Awoke Kassa2 Gebremeskel Abebe Kibret2
Gebremeskel Abebe Kibret2 Muluken Chanie Agimas7
Muluken Chanie Agimas7 Fasikaw Kebede Bizuneh2
Fasikaw Kebede Bizuneh2 Molalign Aligaz Adisu2Bogale Molla Woreta2Kefyalew Addis Alene8,9
Molalign Aligaz Adisu2Bogale Molla Woreta2Kefyalew Addis Alene8,9- 1School of Population Health, Curtin University, Bentley, WA, Australia
- 2College of Medicine and Health Sciences, Woldia University, Woldia, Ethiopia
- 3Curtin Medical School, Faculty of Health Sciences, Curtin University, Bentley, WA, Australia
- 4Department of Clinical Pharmacy, College of Medicine and Health Sciences, University of Gondar, Gondar, Ethiopia
- 5Department of Nursing, College of Health Science, Debre Tabor University, Gondar, Ethiopia
- 6School of Public Health, The University of Queensland, Brisbane, QLD, Australia
- 7Department of Epidemiology and Biostatistics, Institute of Public Health, College of Medicine and Health Sciences, University of Gondar, Gondar, Ethiopia
- 8Faculty of Health Sciences, Curtin University, Bentley, WA, Australia
- 9Geospatial and Tuberculosis Research Team, Telethon Kids Institute, Nedlands, WA, Australia
Background: Fertility rates are key indicators of population health and demographic change, influencing economic development, healthcare planning, and social policies. Understanding subnational variation in fertility rate is important for effective geographical targeting and policy prioritization. This study aimed to identify geographic variation, trends, and determinants of fertility rates in Ethiopia over the past two decades.
Methods: We estimated total fertility rates (TFRs) and age-specific fertility rates (ASFRs) using five nationally representative cross-sectional Demographic and Health Surveys collected in Ethiopia between 2000 and 2019. ASFRs represent the number of live births per 1,000 women aged 15 to 49 during the 3 years before each survey, while TFRs indicate the average number of children a woman would have by the end of her reproductive years, calculated as the sum of ASFRs over five-year intervals. We developed model-based geostatistics by incorporating demographic and healthcare access data with spatial random fields to produce high-resolution fertility rate maps. These results were then aggregated to produce fertility rate estimates at local, sub-national, and national levels in Ethiopia.
Results: The national TFR gradually declined from 4.8 live births in 2000 to 4.2 live births in 2019, but it is still above the replacement level of 2.1 children per woman. There were sub-national and local variations in TFR, ranging from 5.7 live births in Somalia and 5.3 Oromia regions to 2.7 live births in Addis Ababa and 3.6 live births Dire Dawa cities. Geographical areas with high TFR were mostly associated with a high proportion of Muslim women and low access to health facilities.
Conclusion: Despite a decline in fertility rates among women of reproductive age over the past two decades, marked spatial variation persists at sub-national and local levels in Ethiopia, with demographic factors determining the spatial distribution and rate of decline, highlighting the need for tailored programs and strategies in high-fertility areas to increase access to family planning.
Introduction
Fertility rates are critical indicators of population health and demographic change, influencing economic development, healthcare planning, and social policies. They provide essential information about the population’s capacity to reproduce and its growth potential, shaping the age structure and demographic dynamics of a country (1). Understanding fertility rates is crucial not only for predicting future population trends but also for informing policy decisions that aim to enhance economic development, optimize healthcare services, and address social needs (2).
Globally, total fertility rates (TFRs) have declined over the past century, but the pace and timing of this decline have varied significantly across countries. High-income countries have generally experienced more rapid declines in fertility rates, while low-income countries have seen more stagnant or even increasing rates (3). Despite the overall decline in TFRs, the world’s population continues to grow, with a global population reaching 8.0 billion in 2023 and projected to hit 9.7 billion by 2050 (2). Developing countries tend to have higher fertility rates compared to developed countries (4). For example, Sub-Saharan Africa has an average of 5.1 births per woman, nearly double the rates of South Asia (2.8) and Latin America and the Caribbean (2.2) (5, 6).
Ethiopia has experienced considerable changes in its fertility rates over the past two decades. National data indicate a steady increase in fertility rates, yet this overall trend masks significant subnational variations. After an increase in fertility during the 1960s and 70s, a gradual decline began in the 1980s and 90s (7), resulting in a significant decrease in TFR from 5.5 children per woman in 2000 to 4.6 in 2016 (1). However, substantial regional disparities persist within Ethiopia. In 2016, Addis Ababa had the lowest TFR at 1.8 children per woman, while Somali region had the highest rate at 7.2 children per woman (1). Geographical variations in fertility rates are influenced by a complex interplay of demographic, socioeconomic, and cultural factors. Understanding the geographical distribution and the determinants of fertility rates can help policymakers develop targeted interventions to address specific needs, promote balanced population growth, and improve reproductive health outcomes. This study aimed to investigate the spatial distribution, trends, and determinants of fertility rates in Ethiopia over the past two decades using advanced spatial analysis techniques. The findings provided high-resolution maps of fertility rates that can guide policy decisions and resource allocation, contributing to more effective and equitable health and development strategies in Ethiopia.
Methods
Study settings
The study was conducted in Ethiopia, the second-most populous country in Africa with an estimated population size of more than 120 million people in 2022 and a surface area of approximately 1.1 million square kilometers. There are marked differences in population density, socioeconomic conditions, and geographical features across the country. More than 84% of the population resides in rural parts of the country with low healthcare access including contraceptive services. The country has three administrative levels including region, zone, and districts.
Data source
Data for total fertility rate (TFR) and age-specific fertility rate (ASFR) were obtained from the Ethiopian Demographic and Health Survey (EDHS), which consists of five nationally representative cross-sectional surveys conducted in 2000, 2005, 2011, 2016, and 2019. ASFR represents the number of live births to women aged 15 to 49 during the 3 years before each survey. The TFR indicates the average number of children a woman would have by the end of her reproductive years, calculated as the sum of ASFRs over five-year intervals. ASFR and TFR were used because they provide a comprehensive understanding of fertility patterns across different age groups and the overall reproductive behavior of women, making them more informative and accurate compared to single-point estimates of fertility.
The EDHS used a two-stage cluster sampling design with stratification into urban and rural areas. In the initial phase of the selection process, primary sampling units, often census areas, were chosen based on their size, ensuring that larger areas had a higher chance of being selected within each group. Next, a list of households was created within these selected areas, and a set number of households were picked using a systematic method where each had an equal chance of being chosen. Because of this selection method, sampling weights were applied during the analysis to account for any differences in sampling rates among various groups, ensuring that the results were accurate and representative. After data cleaning and applying sampling weights, the final analytic sample included 37,251 women of reproductive age (15–49 years). The EDHS contains geographic information with latitude and longitude coordinates for each surveyed clusters (enumeration areas), enabling spatial analysis and mapping of fertility rate at subnational levels. In total, we gathered data from 2,618 unique locations for women aged 15–49 years between 2000 and 2019.
Covariate data
In addition to demographic data gathered through the EDHS, we also compiled environmental covariate data from publicly available sources that we extracted to EDHS cluster locations. Because these locations are displaced, we averaged geospatial covariates to 2 km and 5 km buffers for urban and rural locations, respectively. Covariates were limited to those for which country-wide representative data were available at a high resolution and that are plausibly associated with fertility rate. Data on travel time to the nearest city were obtained from Malaria Atlas Project (MAP) (8). Altitude data were obtained from the Shuttle Radar Topography Mission (SRTM) (9). Population density, estimated as the number of people per grid, was obtained from WorldPop (10). Distance to the nearest health facilities was also obtained from MAP. Data on religion were obtained from the EDHS, and to estimate the proportion of Muslim women at a high resolution, we employed Bayesian Kriging interpolation techniques (11, 12). To do this we first defined the Kriging model, applied Bayesian inference for parameter estimation, integrated the covariate, and used Bayesian methods to update the model with the data, allowing us to explore the impact of the proportion of Muslims on the fertility rates. This advanced statistical method allowed us to create detailed maps showing the distribution of Muslim women across various regions, providing a more accurate depiction of religious demographics to include in our spatial model. The covariate maps used in our models are provided in the supplementary information. Before fitting multivariable models, we checked for multi-collinearity between covariates using a variance correlation matrix.
Geoprocessing
As the raster of the covariates were at different resolutions, we standardized them to a common resolution of approximately 1 × 1 km. We achieved this by performing resampling and aggregation as pre-processing steps before combining the data, following previously described methods (13–15). All variables were resampled and clipped to the extent of Ethiopia. This approach allowed us to align all the covariate data at the desired resolution.
Geospatial analysis
Bayesian geostatistical models were fitted to analyze Ethiopia’s total fertility rate and age-specific fertility rate, utilizing integrated nested Laplace approximation (INLA) for model inference and prediction. INLA applies the Stochastic Partial Differential Equation (SPDE) method to account for spatial interaction effects, estimating a continuous Gaussian Markov Random Field (GMRF) with spatial correlations between locations defined by the Matérn correlation function. The Matérn correlation function is a popular spatial model in geostatistics and Kriging. It determines how the correlation between points declines with distance, using parameters for smoothness and range, and can accommodate various levels of spatial smoothness (16). The Bayesian models were created by estimating a Gaussian generalized additive model (GAM) with and without spatially correlated random effects. The Gaussian GAM is defined as follows:
Results
We analyzed 2,618 nationally representative survey clusters from the EDHS for the period 2010–2019. Figure 1 describes the national-level trends of the TFR in Ethiopia from 2000 to 2019. The TFR was 4.8 live births per woman in 2000, and over two decades, it decreased by 12.5% to 4.2 live births per woman by 2019, showing a gradual decline while remaining above the replacement level of 2.1 children per woman. The ASFR was 0.96 in 2000 and decreased to 0.84 in 2019. The temporal trends in the decline of live births per woman mask significant heterogeneity at the subnational level. Figure 2 shows that TFR in Ethiopia from 2000 to 2019 consistently higher in rural areas compared to urban areas.
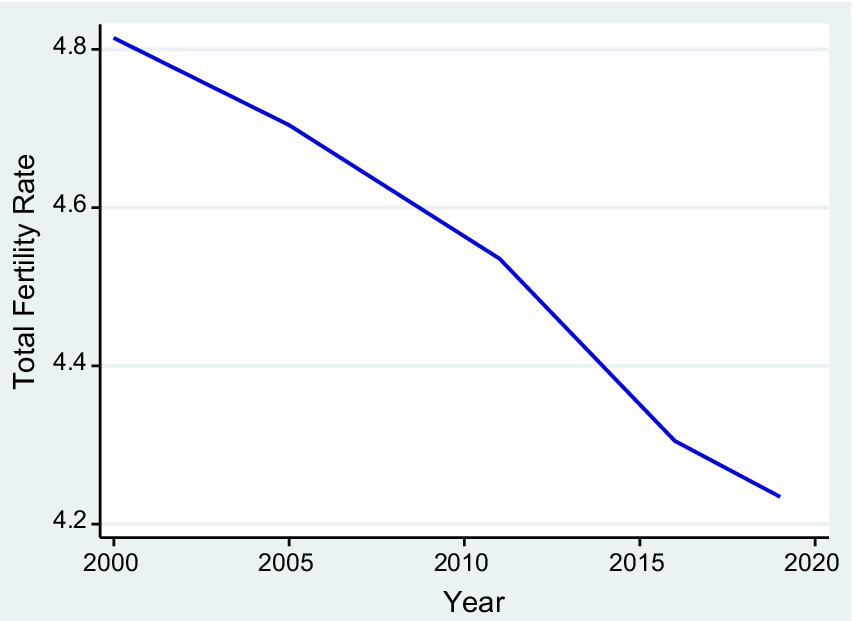
Figure 1. Average national-level trends of total fertility rates in Ethiopia.
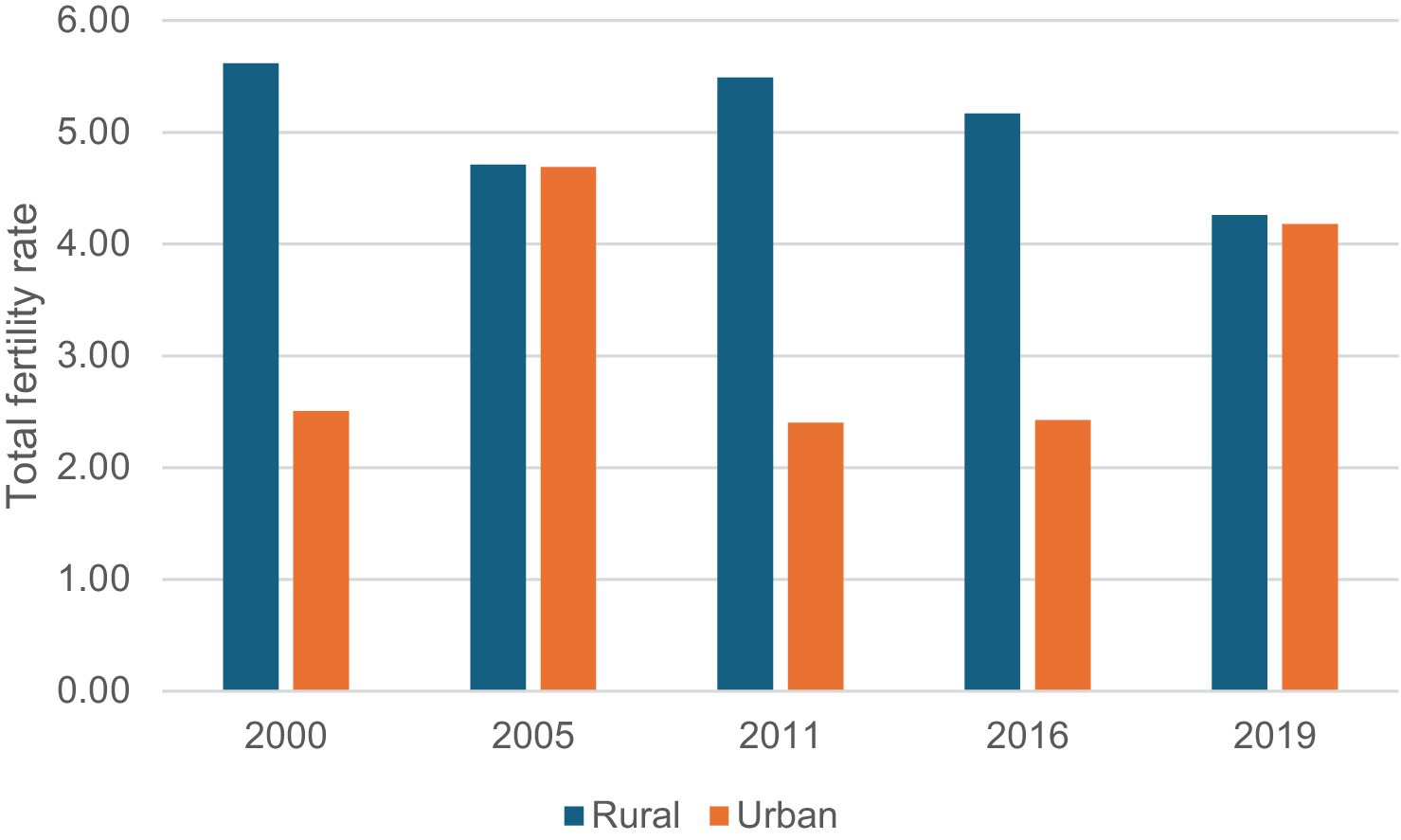
Figure 2. Total fertility rate by rural and urban across all surveys.
Spatial distribution of fertility rate in Ethiopia
Substantial spatial variations in TFR were observed at regional, zonal, district and pixel levels in Ethiopia. Regional variations in TFR ranged from 5.7 live births in the Somali region and 5.3 in Oromia to 2.7 in Addis Ababa and 3.6 in Dire Dawa (Figure 3). At the zone level, total fertility rates ranged from 3.3 to 7.3 live births, and age-specific fertility rates ranged from 0.08 to 1.7 live births (Figure 4). At the district level, total fertility rates varied from 1.6 to 7.5 live births, with age-specific rates between 0.33 and 1.5 live births (Figure 5). At the pixel level, total fertility rates ranged from 0.3 to 8.6 live births, and age-specific rates also ranged from 0.33 to 1.5 live births (Figure 6).
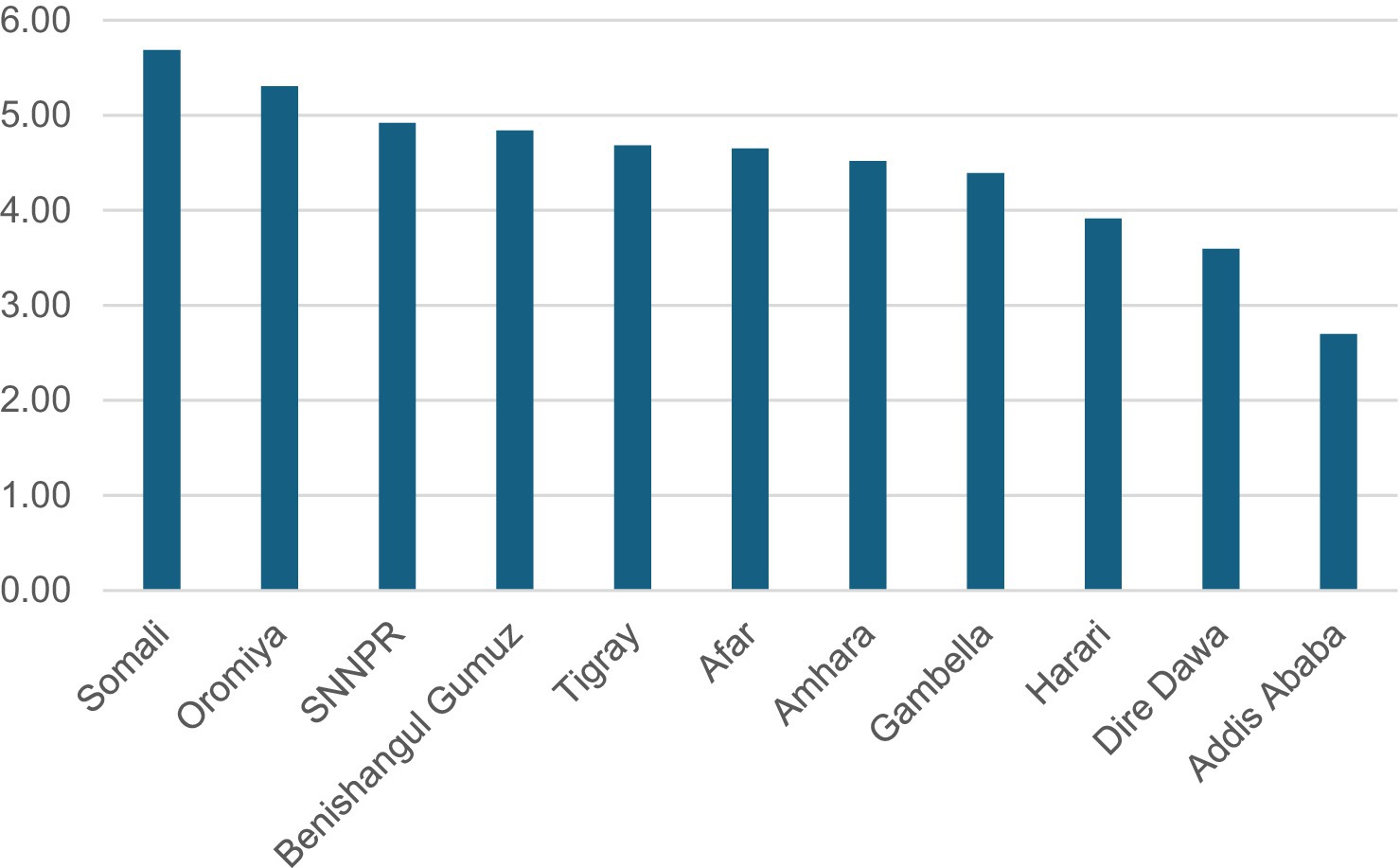
Figure 3. Total fertility rates by regions in Ethiopia.
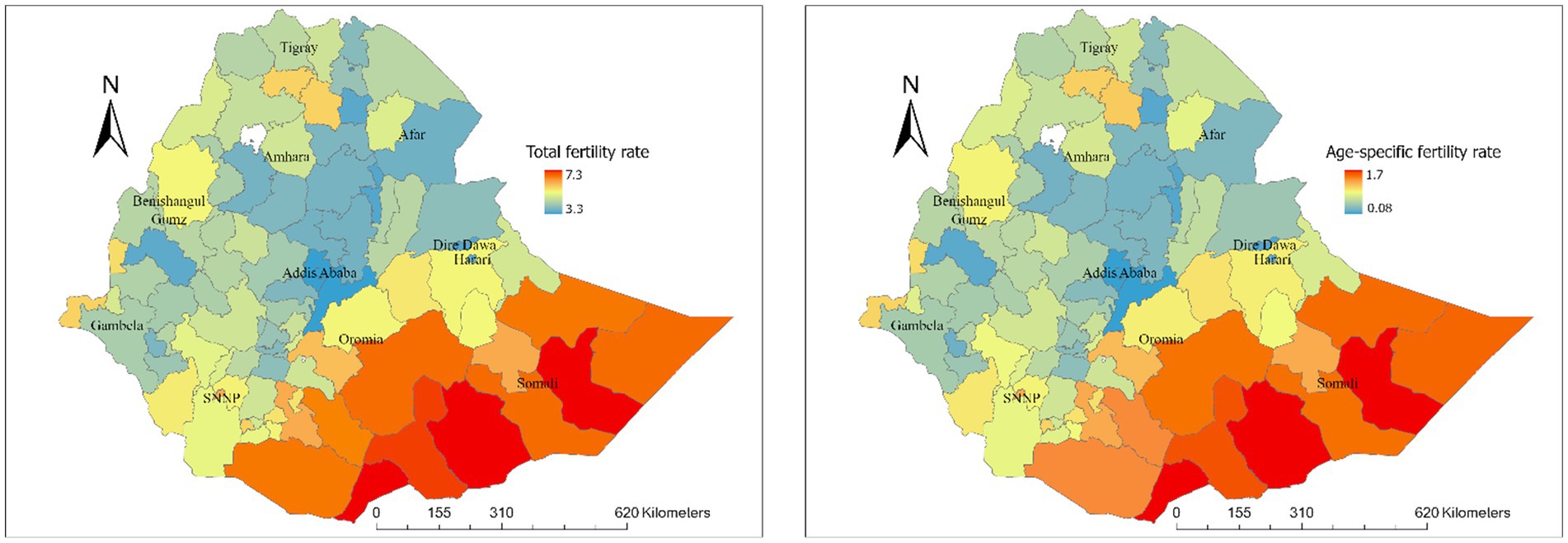
Figure 4. Total and age-specific fertility rate by zone level in Ethiopia.
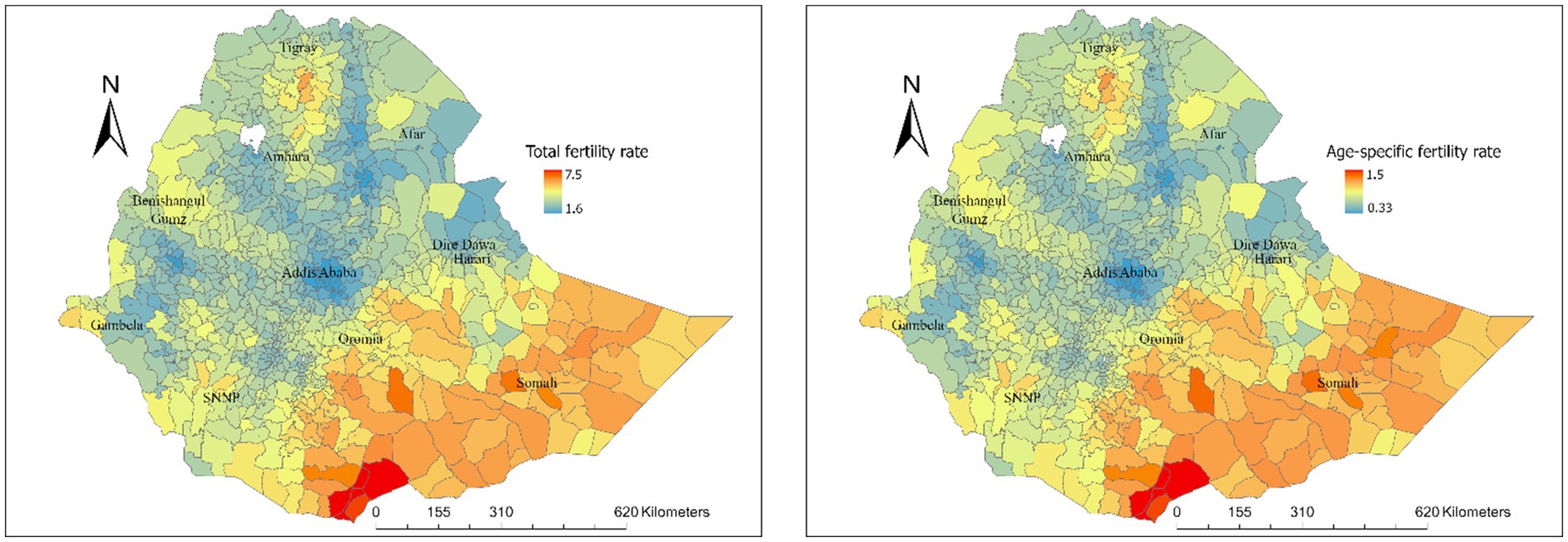
Figure 5. Total and age-specific fertility rate by district level in Ethiopia.
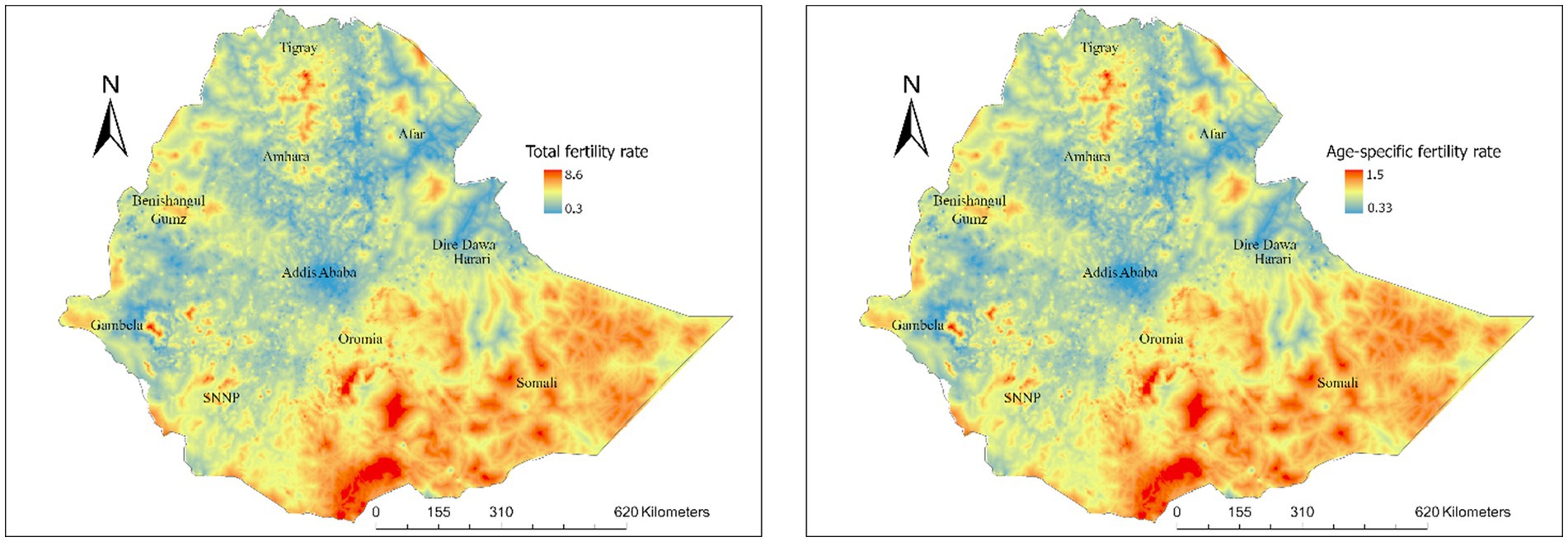
Figure 6. Total and age-specific fertility rate at pixel level in Ethiopia.
Factors associated with total and age-specific fertility rate
Table 1 shows the factors associated with the TFR and ASFR derived from the Bayesian geostatistical model. Distance to the city was positively associated with both total fertility rate (β: 0.42; 95% CrI: 0.23, 0.62) and age-specific fertility rate (β: 0.08: 95% CrI: 0.04, 0.12). The proportion of Muslim women was also positively associated with both the total fertility rate (β: 0.37: 95% CrI: 0.32, 0.42) and age-specific fertility rates (β: 0.07; 95% CrI: 0.06, 0.08). In contrast, the population density was negatively associated with both total fertility rate (β: −0.01; 95% CrI: −0.02, −0.01), and age-specific fertility rates (β: −0.003; 95% CrI: −0.004, −0.002) indicating lower fertility rates in more densely populated areas (Figure S2).
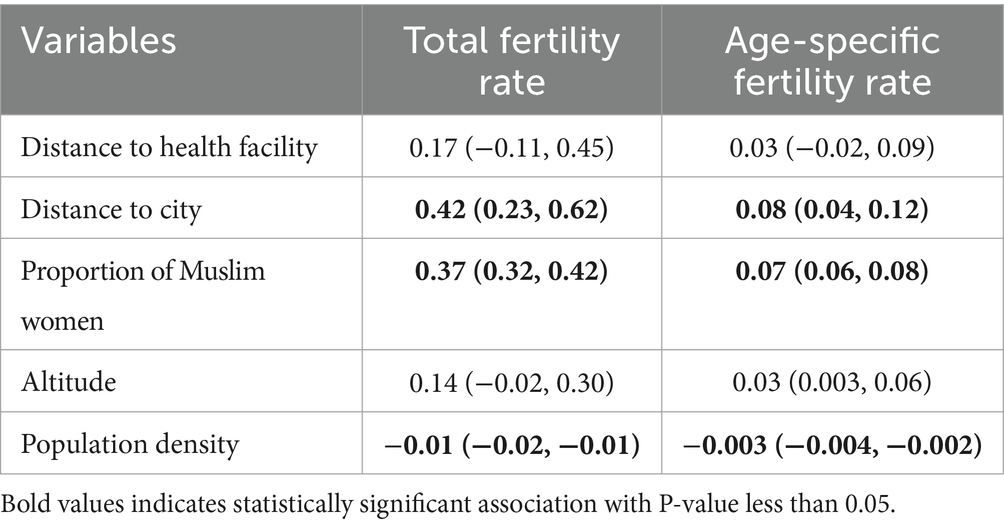
Table 1. Factors associated with total fertility rate and age-specific fertility rate.
Discussion
This study applied an advanced geospatial analysis approach to map fertility rates at national, sub-national, and local levels in Ethiopia between 2000 and 2019. The fertility rates in Ethiopia have shown a consistent decline over the last two decades, though they remain above the replacement level. The declining trend might be attributed to urbanization, increased focus on women’s education, and improved healthcare access, which typically result in delayed marriages and higher contraceptive use. Contraceptive coverage in Ethiopia increased from 8.1% in 2000 to 41.4% in 2019. This declined trend is consistent with findings from other studies conducted in Uganda (17) and Europe (18). Evidence also showed a low fertility in some Asian countries such as Singapore, Japan, and China, where government policies aimed at population control, like ‘one-child policy’, have been implemented (19).
Despite a gradual decline in fertility rates at the national level, substantial regional disparities have been observed, with rates ranging from 5.7 live births per woman in the Somalia region and 5.3 in Oromia to 3.6 Dire Dawa city and 2.7 in Addis Ababa. This regional discrepancy might be due to unequal access and utilization of family planning services, with high contraceptive use in major cities like Addis Ababa (20). Studies show a strong correlation between contraceptive use and fertility decline (21). The increased contraceptive use in Addis Ababa city and other regions such as Amhara region may be part of government efforts to manage population growth through targeted strategies (22). Ensuring equitable access to family planning services and addressing regional socioeconomic disparities is crucial for achieving a consistent decline in fertility rates nationwide.
Out study also showed that women in rural areas are more likely to have higher fertility rates compared to their urban counterparts (23). Previous studies conducted in Sub-Saharan Africa (SSA) also indicate significant disparities in fertility rates between urban and rural areas (24, 25). This disparity may be due to easier access to contraception and higher educational attainment in urban areas (26–30). Additionally, women in rural areas tend to marry earlier, with an average marriage age of 16.1 years compared to 19.4 years in urban areas (31). These findings suggest that improving access to family planning services and education in rural areas could help reduce fertility rates and address regional disparities.
Furthermore, the fertility rate also varied by religion, with areas having a high proportion of Muslim women exhibiting higher fertility rates. This variation may be influenced by cultural norms and practices regarding family size and contraceptive use within different religious groups (32, 33). These findings showed the importance of considering religious and cultural contexts when designing and implementing family planning programs. Tailored interventions that respect and address specific cultural and religious beliefs are crucial for effectively managing fertility rates and promoting reproductive health across diverse communities.
Another important finding of our study is the positive association between distance to the city and fertility rates. Women living further from urban centers tend to have higher fertility rates, likely due to limited access to healthcare facilities, family planning services, and educational opportunities, which are more readily available in cities. This relationship is further explained by the increased costs of transportation as travel time to the nearest cities increases. In low-income African countries, research has consistently shown a significant link between geographic accessibility to healthcare facilities and the utilization of maternal and child health services (34). Urban areas often provide better economic opportunities and social services, leading to delayed marriages and smaller family sizes. This finding shows the necessity for improved infrastructure and service delivery in rural areas to bridge the gap between urban and rural fertility rates. Enhancing accessibility to healthcare and education in remote regions is essential for addressing these disparities and promoting equitable reproductive health outcomes across the country (35–37). This study has significant implications for policymakers and health program designers, emphasizing the need for geographically targeted and integrated fertility control programs that address ecological and religious disparities.
Our study has some limitations. One limitation is the reliance on cross-sectional data from the EDHS, which may not fully capture the temporal dynamics of fertility trends and their determinants. The relatively smaller sample size in the EDHS 2019 dataset may have slightly affected the comparability of findings. Additionally, the study also does not account for potential confounding factors such as cultural practices, economic variations, and local policy differences that might influence fertility rates independently of geographic factors. Furthermore, Ethiopia’s challenging topography and infrastructure limitations might affect the accuracy of spatial data, leading to potential misclassification of accessibility levels.
Conclusion
The fertility rate among women of reproductive age in Ethiopia gradually declined from 2000 to 2019, yet significant spatial disparities persist at regional and local levels, influenced by demographic factors. Tailored programs and strategies are essential in high-fertility areas to improve access to family planning and address unequal fertility trends across different regions, religions, residential settings. Further research is needed to identify independent factors influencing fertility rates and to understand regional and religious disparities, incorporating social, economic, and other characteristics at both national and subnational levels.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author.
Ethics statement
This study is a secondary data analysis from the EDHS data, so it does not require ethical approval. For conducting this study, online registration and request for measure DHS were conducted. The dataset was downloaded from the DHS online archive from the MEASURE DHS dataset for free after getting approval to access the data.
Author contributions
BA: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. MuA: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. EL: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. TW: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. BT: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. MoA: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. TH: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. MK: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. MM: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. DT: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. AM: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. AA: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. AZ: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. TK: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. AK: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. AMK: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. GY: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. MAK: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. GK: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. MCA: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. FB: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. MAA: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. BW: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. AS: Writing – original draft, Writing – review & editing, Data curation, Methodology, Supervision, Conceptualization, Formal analysis, Project administration, Validation, Investigation, Funding acquisition, Resources, Visualization, Software. KA: Writing – original draft, Writing – review & editing, Data curation, Methodology, Supervision, Conceptualization, Formal analysis, Project administration, Validation, Investigation, Funding acquisition, Resources, Visualization, Software.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2024.1363284/full#supplementary-material
References
1. Csa, ICentral statistical agencyICF . Ethiopia demographic and health survey. Addis Ababa, Ethiopia and Calverton, Maryland, USA: (2016). Available at: https://www.dhsprogram.com/pubs/pdf/FR328/FR328.pdf
2. United Nations . Population. Available at: https://www.un.org/en/global-issues/population. Accessed on 10 June 2024.
3. Max Roser and Hannah Ritchie (2023). “Two centuries of rapid global population growth will come to an end” Published online at OurWorldInData.org. Retrieved from: 'https://ourworldindata.org/world-population-growth-past-future' [Accessed on June 2024].
4. Asmamaw, DB, Negash, WD, Aragaw, FM, Belay, DG, Asratie, MH, Endawkie, A, et al. Spatial distribution, magnitude, and predictors of high fertility status among reproductive age women in Ethiopia: further analysis of 2016 Ethiopia demographic and health survey. PLoS One. (2023) 18:e0290960. doi: 10.1371/journal.pone.0290960
5. Reda, MG, Bune, GT, and Shaka, MF. Research article epidemiology of high fertility status among women of reproductive age in Wonago District, Gedeo zone, Southern Ethiopia: A Community-Based Cross-Sectional Study. Int J Reproduct Med. (2020) 2020:1–8. doi: 10.1155/2020/2915628
6. Njoku, CO, Abeshi, SE, and Emechebe, CI. Grand multiparity: obstetric outcome in comparison with multiparous women in a developing country. Open J Obstetrics and Gynecol. (2017) 7:707–18. doi: 10.4236/ojog.2017.77071
7. World Health O . Trends in maternal mortality: 1990–2015: Estimates from WHO, UNICEF, UNFPA, World Bank Group, and the United Nations population Division. Geneva: World Health Organization (2015).
8. Weiss, DJ, Nelson, A, Gibson, H, Temperley, W, Peedell, S, Lieber, A, et al. A global map of travel time to cities to assess inequalities in accessibility in 2015. Nature. (2018) 553:333–6. doi: 10.1038/nature25181
9. Farr, TG, and Kobrick, M. Shuttle radar topography Mission produces a wealth of data. EOS Trans Am Geophys Union. (2000) 81:583–5. doi: 10.1029/EO081i048p00583
10. Tatem, AJ . WorldPop, open data for spatial demography. Scientific data. (2017) 4:170004–4. doi: 10.1038/sdata.2017.4
11. Pilz, J, and Spöck, G. Why do we need and how should we implement Bayesian kriging methods. Stoch Env Res Risk A. (2008) 22:621–32. doi: 10.1007/s00477-007-0165-7
13. Dwyer-Lindgren, L, Cork, MA, Sligar, A, Steuben, KM, Wilson, KF, Provost, NR, et al. Mapping HIV prevalence in sub-Saharan Africa between 2000 and 2017. Nature. (2019) 570:189–93. doi: 10.1038/s41586-019-1200-9
14. Battle, KE, Lucas, TC, Nguyen, M, Howes, RE, Nandi, AK, Twohig, KA, et al. Mapping the global endemicity and clinical burden of plasmodium vivax, 2000–17: a spatial and temporal modelling study. Lancet. (2019) 394:332–43. doi: 10.1016/S0140-6736(19)31096-7
15. Alene, KA, Python, A, Weiss, DJ, Elagali, A, Wagaw, ZA, Kumsa, A, et al. Mapping tuberculosis prevalence in Ethiopia using geospatial meta-analysis. Int J Epidemiol. (2023) 52:1124–36. doi: 10.1093/ije/dyad052
16. Gneiting, T, Kleiber, W, and Schlather, M. Matérn cross-covariance functions for multivariate random fields. J Am Stat Assoc. (2010) 105:1167–77. doi: 10.1198/jasa.2010.tm09420
17. Ariho, P, Kabagenyi, A, and Nzabona, A. Determinants of change in fertility pattern among women in Uganda during the period 2006–2011. Fertility Res Prac. (2018) 4:1–11. doi: 10.1186/s40738-018-0049-1
18. Lutz, W . Determinants of low fertility and ageing prospects for Europe. Family issues between gender and generations seminar report, produced by the European observatory on family matters at the Austrian Institute for Family Studies. Vienna, Austria Luxembourg: Office for Official Publications of the European Communities (2000).
19. Shin, I . Change and prediction of income and fertility rates across countries. Cogent Econ Finance. (2016) 4:1119367. doi: 10.1080/23322039.2015.1119367
20. Gubhaju, B . Fertility decline in Asia: opportunities and challenges. Jpn J Popul. (2007) 5:19–42.
21. Merid, MW, Kibret, AA, Alem, AZ, Asratie, MH, Aragaw, FM, Chilot, D, et al. Spatial variations and multi-level determinants of modern contraceptive utilization among young women (15–24 years) in Ethiopia: spatial and multi-level analysis of mini-EDHS 2019. Contraception Reprod Med. (2023) 8:26. doi: 10.1186/s40834-023-00224-0
22. UNICEF . UNICEF-Ethiopia-2018-Amhara-regional-state-budget-brief.Pdf. Available at: https://www.unicef.org/esa/sites/unicef.org.esa/files/2019-05/UNICEF-Ethiopia-2018-Amhara-Regional-State-Budget-Brief.pdf. (2019). (Accessed on June 10, 2024).
23. Alaba, OO, Olubusoye, OE, and Olaomi, J. Spatial patterns and determinants of fertility levels among women of childbearing age in Nigeria. S Afr Fam Pract. (2017) 59:143–7. doi: 10.1080/20786190.2017.1292693
24. Shapiro, D, and Tenikue, M. Women’s education, infant and child mortality, and fertility decline in urban and rural sub-Saharan Africa. Demogr Res. (2017) 37:669–708. doi: 10.4054/DemRes.2017.37.21
25. Lerch, M . Regional variations in the rural-urban fertility gradient in the global south. PLoS One. (2019) 14:e0219624. doi: 10.1371/journal.pone.0219624
26. Bizuneh, FK, Bizuneh, TK, Masresha, SA, and Yayeh, BM. Individual and community level factors for modern contraceptives utilization among reproductive aged women in Amhara region, mixed effect multi-level modeling, data from Mini-EDHS, 2019. Contraception Reprod Med. (2023) 8:56. doi: 10.1186/s40834-023-00256-6
27. Tsegaye, NB . Fertility intention among married women in Ethiopia: a multilevel analysis of Ethiopian demographic health survey 2016. Contraception Reprod Med. (2023) 8:6. doi: 10.1186/s40834-022-00201-z
28. Kulu, H . Why do fertility levels vary between urban and rural areas? Reg Stud. (2013) 47:895–912. doi: 10.1080/00343404.2011.581276
29. Rele, JR, and Kanitkar, T. Residence background and fertility in greater Bombay. Popul Stud. (1974) 28:299–308. doi: 10.1080/00324728.1974.10405181
30. Choi, H, Cho, Y, Paek, H-J, Hong, W, Ko, W, Balew, G, et al. Determinants of fertility in Ethiopia: a National Survey in 2017. 보건학논집. (2018) 55:31–40. doi: 10.1021/JP508162PCorpus
31. Gizachew Balew, J, Cho, Y, Tammy Kim, C, and Ko, W. Structural determinants in family planning service utilization in Ethiopia: EDHS 2011 analysis. Biomed Res Int. (2015):1–17. doi: 10.1155/2015/495745
32. Tigabu, S, Demelew, T, Seid, A, Sime, B, and Manyazewal, T. Socioeconomic and religious differentials in contraceptive uptake in western Ethiopia: a mixed-methods phenomenological study. BMC Womens Health. (2018) 18:1–10. doi: 10.1186/s12905-018-0580-6
33. Tiruneh, FN, Chuang, K-Y, Ntenda, PA, and Chuang, Y-C. Factors associated with contraceptive use and intention to use contraceptives among married women in Ethiopia. Women Health. (2016) 56:1–22. doi: 10.1080/03630242.2015.1074640
34. Lohela, TJ, Campbell, OM, and Gabrysch, S. Distance to care, facility delivery and early neonatal mortality in Malawi and Zambia. PLoS One. (2012) 7:e52110. doi: 10.1371/journal.pone.0052110
35. Tegegne, TK, Chojenta, C, Getachew, T, Smith, R, and Loxton, D. Antenatal care use in Ethiopia: a spatial and multilevel analysis. BMC Pregnancy Childbirth. (2019) 19:1–16. doi: 10.1186/s12884-019-2550-x
36. Tadele, N, and Lamaro, T. Utilization of institutional delivery service and associated factors in bench Maji zone, Southwest Ethiopia: community based, cross sectional study. BMC Health Serv Res. (2017) 17:1–10. doi: 10.1186/s12913-017-2057-y
Keywords: mapping, fertility rate, spatial analysis, trends, Ethiopia
Citation: Abate BB, Sendekie AK, Ayele M, Lake ES, Wodaynew T, Tilahun BD, Azmeraw M, Habtie TE, Kassa M, Munie MA, Temesgen D, Merchaw A, Alamaw AW, Zemariam AB, Kitaw TA, Kassaw A, Kassie AM, Yilak G, Kassa MA, Kibret GA, Agimas MC, Bizuneh FK, Adisu MA, Woreta BM and Alene KA (2024) Mapping fertility rates at national, sub-national, and local levels in Ethiopia between 2000 and 2019. Front. Public Health. 12:1363284. doi: 10.3389/fpubh.2024.1363284
Edited by:
Maria Rosario O. Martins, New University of Lisbon, PortugalReviewed by:
Isabel Natário, NOVA University of Lisbon, PortugalErick Kiprotich Yegon, Jomo Kenyatta University of Agriculture and Technology, Kenya
Copyright © 2024 Abate, Sendekie, Ayele, Lake, Wodaynew, Tilahun, Azmeraw, Habtie, Kassa, Munie, Temesgen, Merchaw, Alamaw, Zemariam, Kitaw, Kassaw, Kassie, Yilak, Kassa, Kibret, Agimas, Bizuneh, Adisu, Woreta and Alene. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Biruk Beletew Abate, YmlydWtrZWxlbWJAZ21haWwuY29t