
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health , 27 March 2024
Sec. Public Health Education and Promotion
Volume 12 - 2024 | https://doi.org/10.3389/fpubh.2024.1359363
This article is part of the Research Topic Community Health Workers: Describing the Breadth of Interventions and Contexts Across the World View all 18 articles
 Emilie Mosnier1,2*
Emilie Mosnier1,2* Maxime Hoyer1Fernanda Artigas3Hippolyte Regnault1
Maxime Hoyer1Fernanda Artigas3Hippolyte Regnault1 Elodie Richard4David Michels5,6Marine Mosnier3Grâce Inegbeze3Manuela Salcedo Robledo5
Elodie Richard4David Michels5,6Marine Mosnier3Grâce Inegbeze3Manuela Salcedo Robledo5 Bruno Spire1,5
Bruno Spire1,5 Stéphanie Vandentorren4Marc Lescaudron3
Stéphanie Vandentorren4Marc Lescaudron3 Carole Eldin7
Carole Eldin7 Perrine Roux1
Perrine Roux1Introduction: Given the high infection rate of sexually transmitted infections (STI) among migrant women sex workers (WSWs), it is necessary to understand how to improve prevention, information and care for this vulnerable population. Community health workers (CHWs), by linking community to health services, are positioned to improve health outcomes in migrant communities. This article aims to describe a pilot innovative intervention performed by CHWs to improve sexual health in migrant WSWs.
Methods: This one-year intervention study used a respondent-driven sampling (RDS) to recruit a representative cohort of migrant WSWs in Marseille, France. Four CHWs were recruited from different communities and participated in all stages of the research. They performed individual and group interventions of prevention, support in care and empowerment. Data on participant characteristics, type of intervention and adherence to the intervention were reported via questionnaires given to participants. Simultaneously, semi-structured interviews and informal interviews of migrant WSW, CHWs and care providers were carried out.
Results: A total of 132 migrant WSWs were included in the cohort. Very few of them knew about PrEP (12%) or already used HIV post-exposure treatment (9%). Migrant WSWs were often victims of rape or racism, 15 and 21%, respectively. In two-thirds of cases the level of health literacy was low. Participants suffered from a combination of vulnerability factors: difficulties with access to social rights, food or housing. Only 13% reported having benefited from medical follow-up or assistance by an NGO in the 3 months prior to the program. By 3 months, more than one third of the participants had been tested for HIV (35%) and 63% knew about PrEP. A total retention rate of 70% was reported in the cohort after 6 months.
Conclusion: CHWs enabled to improve care access for migrant WSWs by improving the collaboration between care and social actors at a local level. Through these “bring-back-to” interventions for this hard-to-reach population, CHWs enabled an optimization of the care pathway. Our results also highlight the importance of a population-based approach for individual and group support of empowerment interventions in order to strengthen their capacity for action.
In Europe, the epidemic of HIV and sexually transmitted infections (STI) remains particularly active among migrants, who, along with men who have sex with men (MSM), are the populations who are the most vulnerable to these infections (1). Migrants, particularly those from sub-Saharan Africa, represent a significant proportion of people living with HIV in France (PLHIV). Although prevalence in their country of origin is high, a large proportion of these people contract HIV in France due to poor living conditions (2). Moreover, foreign-born PLHIV are also at risk of late detection (3). Finally, foreign-born PLHIV are characterized by a high proportion of women because they combine intersectional risks such as gender inequality, racism, insecurity and violence (4). All these data underline the importance of specific, optimized screening and prevention strategies.
Despite this context, there is a poor perception of risk and consequently little demand for PrEP among migrants (5). The main difficulties encountered by migrant women are unfamiliarity with prevention tools, difficulties in follow-up and in access to social rights. Other specificities that are insufficiently taken into account, such as problems related to contraception, pregnancy, relationships with partners, etc. require holistic approaches (5).
Woman sex workers (WSWs) also represent one of the key populations for controlling the HIV epidemic, due to them having a combination of social, economic and cultural risk factors (6, 7). Several approaches have been tested to reduce HIV incidence in this population. Usually, access to condoms is at the heart of HIV prevention measures. However, these prevention methods are only partially effective (8, 9). In fact, as has been demonstrated, WSWs are not necessarily in a position to impose this type of prevention, particularly for their regular partners (10). WSWs are also more frequently victims of violence which makes the use of this prevention tool difficult (10, 11).
The ANRS-PARCOURS study showed that migrants experience a long period of insecurity upon arrival in France (2). In the PARCOURS study, factors linked to the likelihood of migrant women resorting to transactional relationships included the lack of housing and of residence permits (12). Thus, the factors of precariousness (housing, food, right to work, etc.) among migrant women are at the origin of SW activity. While community-based risk reduction programs for MSM have been successful, particularly in terms of levels of knowledge and access to PrEP, the same cannot be said for migrant populations (13).
All these factors point to the growing importance of community health programs in public health strategies. The development of these programs and the need for health mediation and Community Health Workers (CHWs) are now widely recognized, both nationally and internationally (14, 15). Community health is thus an integral part of public health, representing a strategy within health promotion approaches. Its specific feature is that it is population-based rather than individual-based, and promotes and implements a holistic vision of health on a fine territorial level. In practice, benefits are expected at individual, community and institutional levels. The power of these programs lies in the fact that they aim to empower people and communities. However, evaluation and scaling up of community health initiatives are hampered by the length of time needed to measure their effects, and by the fact that they are often adapted to a specific context and not easily replicated or synchronized (16). In order to understand better the different levels at which community health interventions can act, detailed intervention descriptions are needed.
This article aims to describe, via a cohort conducted as part of a pilot intervention to improve sexual health in migrant WSWs, the characteristics of this population and the actions implemented by CHWs.
This cohort, with a mixed method descriptive analysis, is an ancillary study of the FASSETS program (Favoriser l’Accés à la Santé SExuelle des Travailleuses du Sexe). The program protocol has already been published (17). The cohort was set up using Respondent-Driven Sampling (RDS). A 6-month follow-up was set up with a quantitative and qualitative evaluation. CHWs carried out the interventions throughout the follow-up period.
The FASSETS study is a community-based participatory study. Community-based participatory research is an approach to research that involves a collective, reflective and systematic study in which the researcher and community stakeholders are involved in all stages of the research process with the aim of improving practices (18). This approach promotes shared control over individual and collective health and social conditions (19, 20). The FASSETS project was initially developed around two community-based non-governmental organizations (NGOs): AIDES and The Truth, which provide community-based sexual and reproductive health interventions for migrant sex workers. These NGOs include CHWs from the communities involved in the research. In line with the principles of community-based participatory research, this study involved the creation of partnerships, regular exchanges between partners and community organizations/groups, and the sharing of experiences between researchers, CHWs and the community of migrant WSWs.
The study sites included all of the medical and social care sites, including outreach activities, for migrant WSWs in Marseille, as well as the inclusion and follow-up site specific to the FASSETS study.
The study population included: (i) the 4 CHWs from Nigeria, Eastern Europe, Brazil and North Africa (two of the four are peer workers), (ii) the partners: health institutions and organizations involved in sexual health care in Marseille (Planning familial, Amicale du Nid, CEGIDD, AIDES, Autres Regards, COREVIH, ARS etc.) and (iii) the migrant WSWs accompanied by the FASSETS mediators.
As migrant WSWs are a hidden population, the FASSETS study used the Respondent-Driven Sampling method to obtain a cohort as representative as possible of the different migrant WSW communities, whether or not they were already in the care system (21). There were 10 seeds in total, of different ages and belonging to cis or transgender women’s communities, who were from sub-Saharan Africa, North Africa, South America and Eastern Europe communities.
The criteria for inclusion in the FASSETS cohort were: (i) cis or transgender women over 18 years of age, (ii) having provided sexual services in exchange for a service or monetary compensation during the last 12 months, (iii) born abroad, (iv) working, living or regularly passing through Marseille and (v) having signed a free and informed consent to take part in this study. Non-mastery of the French language was not a criterion for exclusion. Questionnaires and follow-up were conducted by CHWs in the participants’ native language.
The FASSETS CHWs were previously trained in the survey technique by researchers and infectious disease physicians. They collected quantitative data from the migrant WSWs using a standardized tablet questionnaire. The interview method was face-to-face with CHWs in the participant’s native language for the first questionnaire and the two following ones. Additional follow-up by CHWs could be face-to-face, by telephone or via social networks, depending on needs. They also listed all the actions carried out and how they were implemented. Members of the project team worked with a team of sociologists to collect qualitative data from the WSWs. Data on partners was collected by questionnaires and focus groups.
Variables were collected through standardized questionnaires and included demographic characteristics, sex work characteristics, behavioral characteristics (alcohol use, drug use), medical history, level of health literacy and needs in sexual health. Perceived stress was measured using the Perceived Stress Scale (PSS) (22). A committee of experts from outside the study reviewed the questionnaire. Questions and variables were standardized on previous PARCOURS studies, on precariousness scales and on the conceptual framework for describing CHW activities previously validated in the literature (12, 23, 24).
For this ancillary study, only data collected between April (the start of the study) and November 2022 were analyzed.
Categorical variables were compared using Fisher’s exact test. Means were compared using Student’s t-test. The association between lost to follow-up and explanatory variables were assessed using univariate analysis. All p < 0.05 were considered statistically significant. Statistical analysis was carried out using R software (R Foundation for Statistical Computing, 3.3.1-Studio).
An inductive approach was used, particularly adapted to exploratory research. Questions were focused on the needs and representation of sexual health and care among migrant WSWs. Health care providers, CHWs and migrant WSWs were interviewed. Migrant WSWs were encouraged to share specific experiences such as stories from their own lives to generate conversation. A revision workshop was organized where researchers provided a summary of the data collected to the participants in order to get their feedback and confirmation of results. The interviews and notes of these exchanges were transcribed and were subjected to manual thematic coding. A total of 13 semi-structured and 12 informal interviews were performed.
Qualitative and quantitative data were collected and analyzed, respectively, and simultaneously, followed by a triangulation of qualitative and quantitative data to interpret the results.
The protocol received approval from French Ethics Committee in October 2021 (no. 2021—A01746-35).
A total of 132 participants were included in the study. Table 1 provides population estimates of socio-demographic characteristics. More than half could not write (n = 85/132, 65%) and the level of health literacy was low (Table 1).
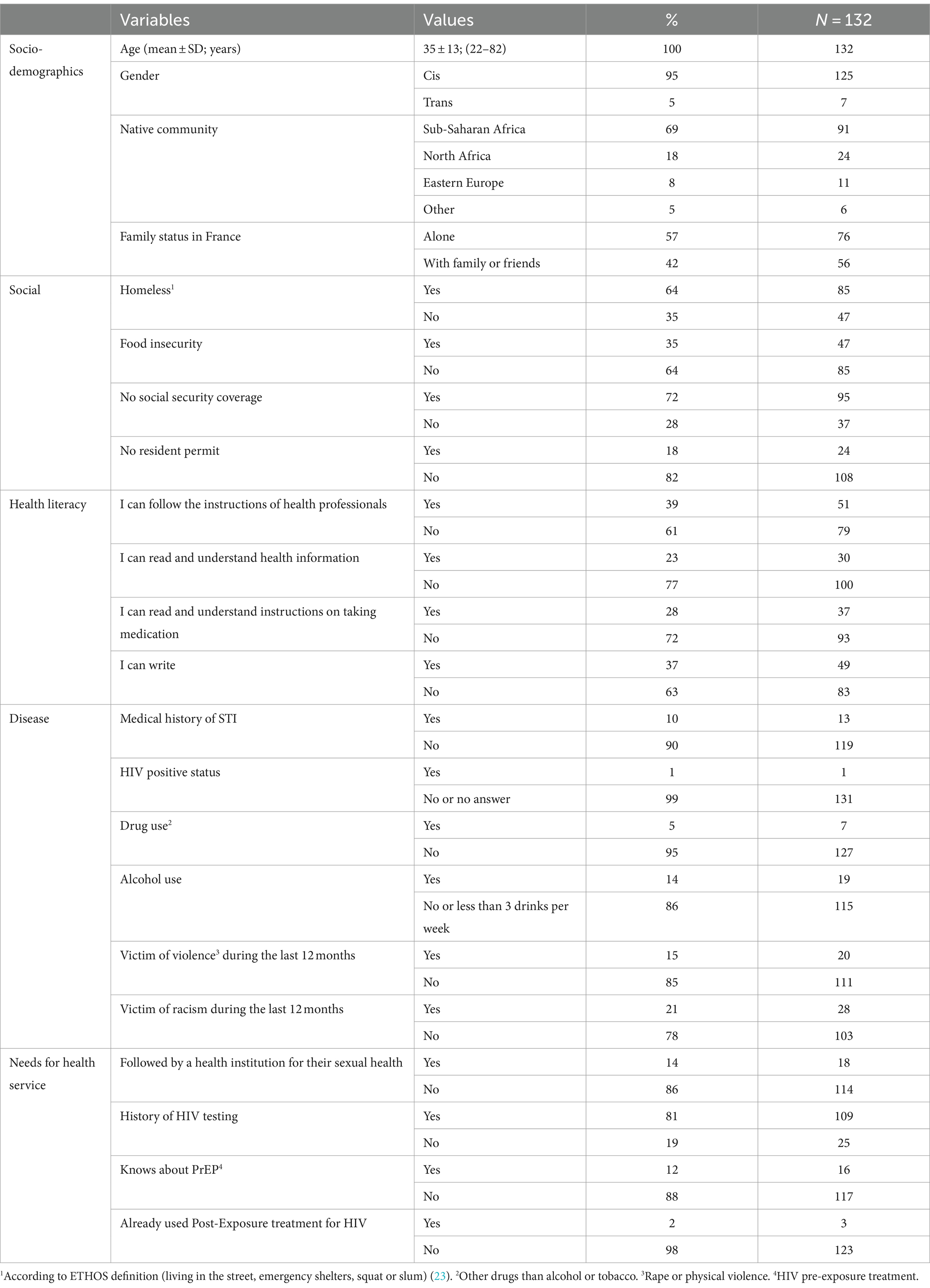
Table 1. Socio-demographic, social, disease and needs of health service variables and indexes.
The majority of migrant WSWs were socially very vulnerable. In over half of the cases they were homeless, and they reported food insecurity or having no social security coverage or resident permit (Table 1).
During the previous 12 months a significant number of participants reported having suffered from violence and racism (Table 1).
The majority of participants (87%, n = 114) said that they had had no contact with NGOs or institutional care structures for their sexual health within the last 3 months.
Most Migrant WSW had children (87%, n = 115) with a mean of 2.12 children. They had been in France for an average of 7.8 years (SD = 10.1).
A total of 56% (n = 56) of participants assessed had a low level of stress, 32% (n = 30) a moderate level, and 12% (n = 11) a high level of perceived stress according the PSS.
The RDS reported a near-perfect homophily of the communities network (Figure 1). A total of 10 seeds were used. The RDS was stopped at the third wave for reasons of human resource capacity (CHWs) to monitor the recruited cohort correctly.
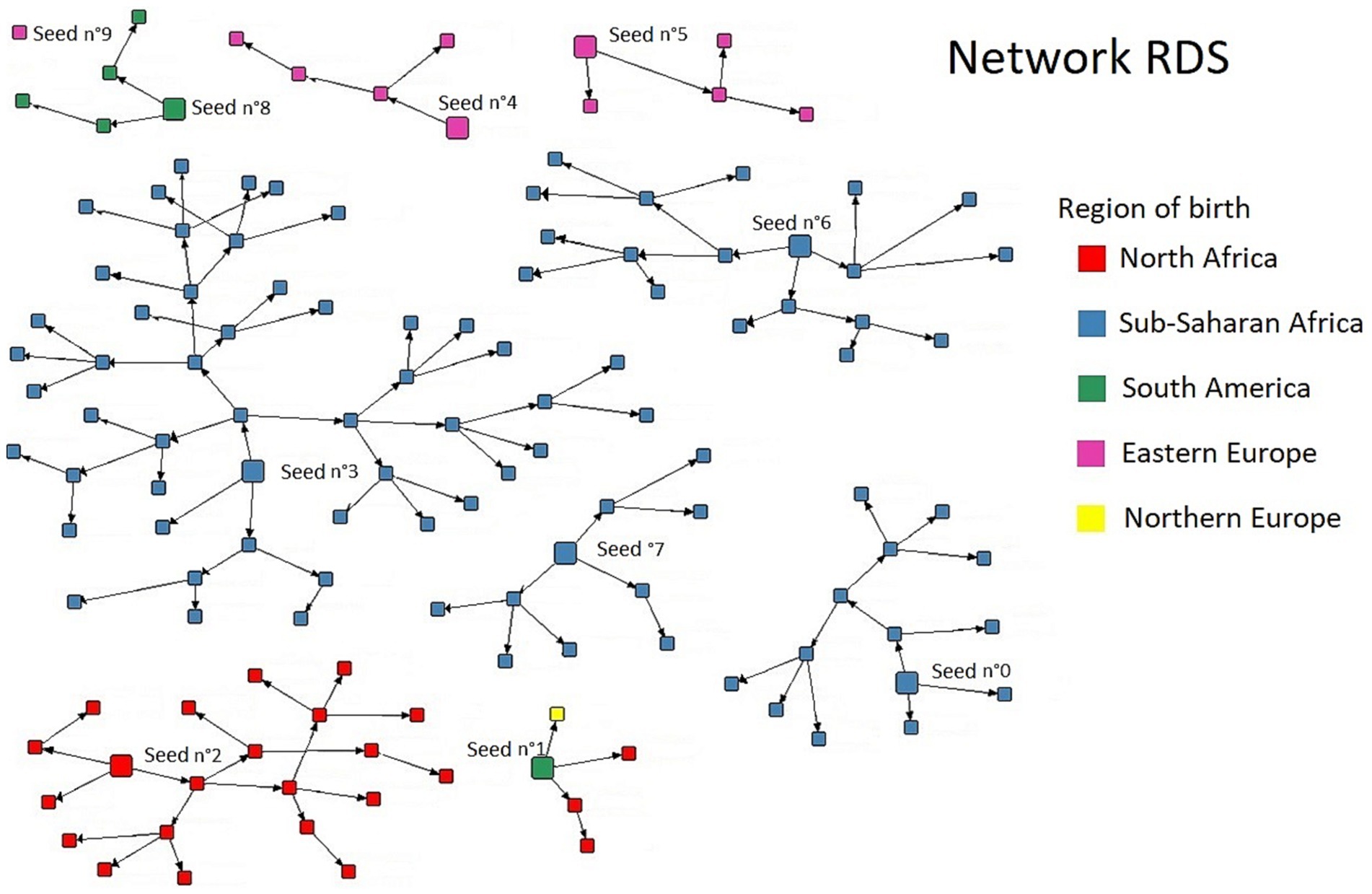
Figure 1. Result of the respondent-driven sampling in migrant WSWs.
A total of 4 CHWs were recruited from the various regions of origin of the migrant WSWs. Two of them were peer workers. All were women and one of them was transgender. CHWs activities are very varied, an example of a CHW’s activities is shown in Table 2.
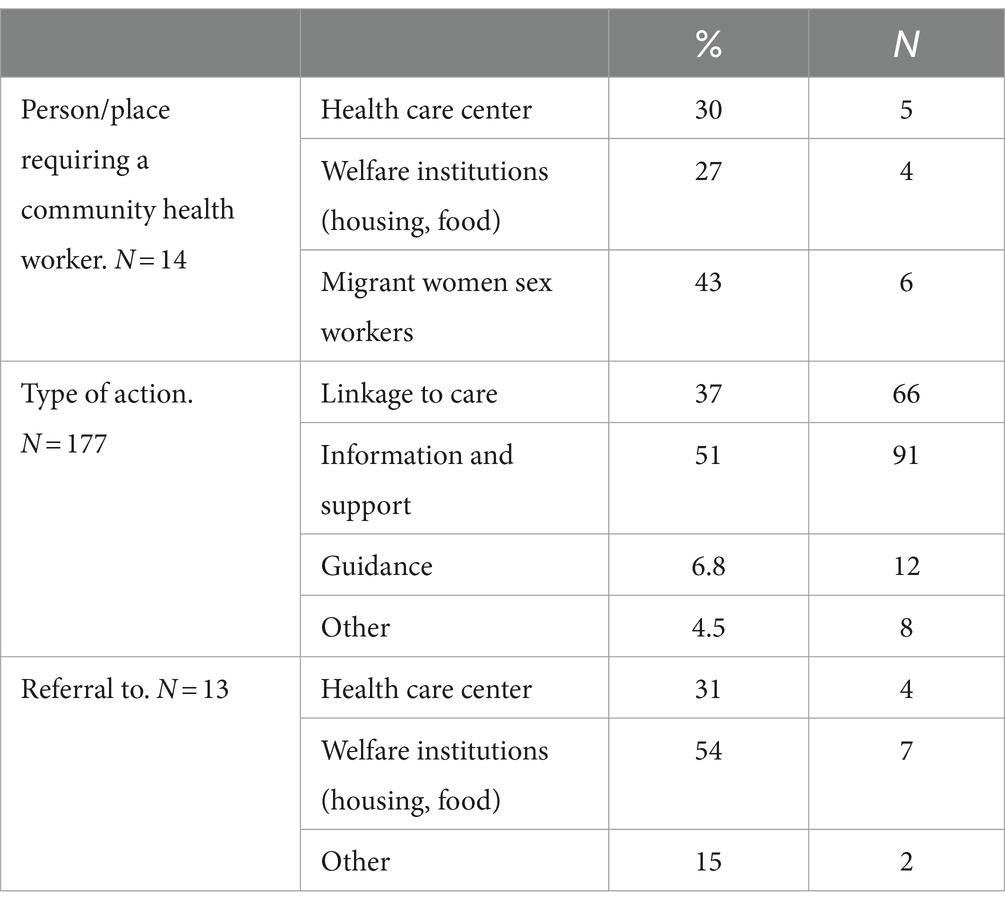
Table 2. Example of the activity of one community health worker from April 2022 to November 2022.
The actions implemented by CHWs to improve the sexual health of migrant WSWs take place at different levels (Table 3; Figure 2). At an individual level, it is necessary to perceive the person’s health needs (all the more difficult in the presence of discrimination or a competitiveness of needs, notably here with access to social rights, food and family needs), then to improve levels of knowledge in sexual health and facilitate access to care. Taking into account past experiences, vicarious experiences, medical history and perceptions also play a role in the migrant WSWs’ self-efficacy and capacity to act. The CHWs also work on a collective and social level to gain recognition of the participants’ specificities, notably when setting up care pathways dedicated to women (adaptation of the care system) or their advocacy actions (Figures 2, 3).
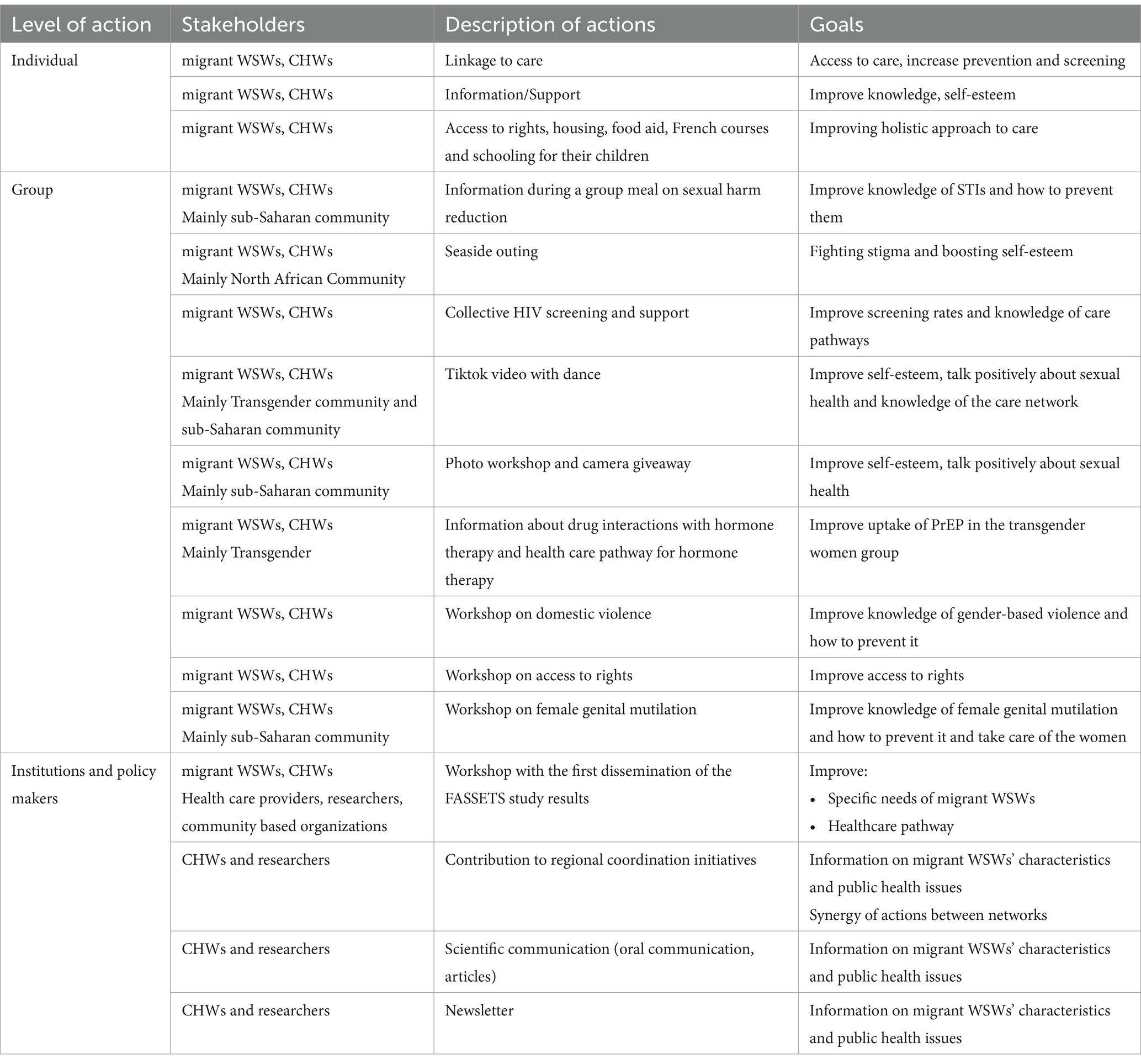
Table 3. Description of actions carried out among and with migrant women sex workers.
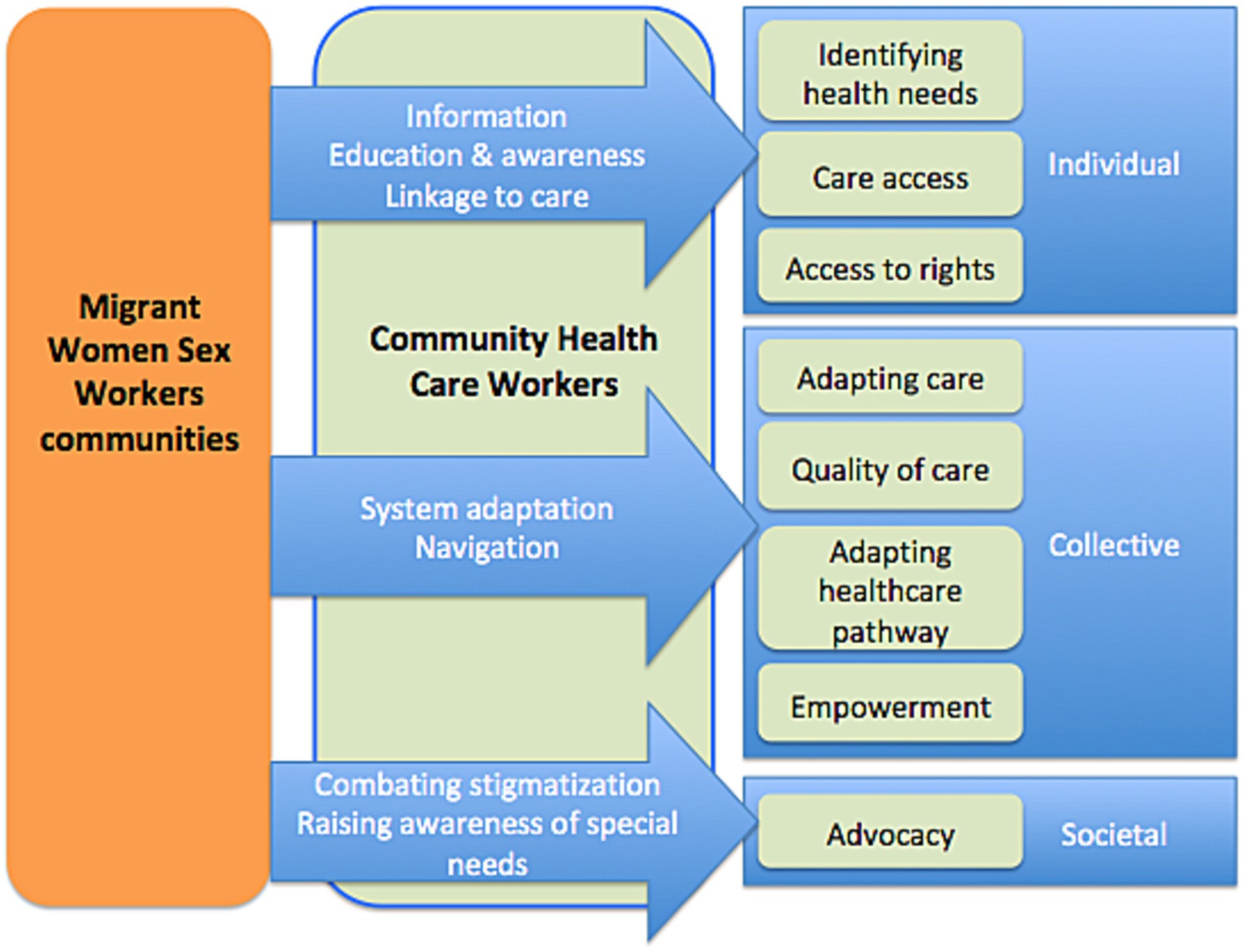
Figure 2. Type and level of community health workers health actions with migrant women sex workers.

Figure 3. Example of an empowerment group for Nigerian women on sexual health and information about PrEP.
It is clear from these actions (Table 3) that the CHWs enable the needs formulated by the MWSWs to be incorporated into collective actions and have an impact on institutions (Figure 2).
CHWs take into account the complex intersections between structural barriers affecting migrant WSWs and their gender, education, race, and socio-economic status. Based on the needs expressed by migrant WSWs, CHWs not only optimize access to care but also impact it by encouraging adaptations (Figure 2).
The results of the interviews showed that cisgender women differ from transgender women (TGW) in their perception of the sexual health risks to which they are exposed, in their knowledge of prevention tools and in the expression of their needs to the medical-social sector.
“Normally South American [trans] girls are mainly looking for access to care, health, help with their papers, it’s stuff… frankly it’s light… when they arrive at the association they know what they’re looking for, what they want… it’s different from Nigerian girls where you have to unpack the whole package to try and find out what they want…” (CHW, sex workers NGO).
For the NGOs, TGW are more receptive to sexual health issues. According to health care workers, migrant TGW feel much more “at risk” of contracting HIV and other STIs than migrant cisgender women.
There are also community-specific characteristics, particularly among Nigerian women, related to the violence and trauma of migration.
“As I was telling you earlier, there's normal prostitution and forced prostitution… and right now we’re taking much more care of Nigerian girls than other WSWs at the association… 70% of our active file I think. As these are girls who have experienced rape, exploitation… they don’t see prostitution as work…” (Health mediator, association for sex workers).
The migrant WSWs interviewed frequently told stories of rape, particularly during their migration pathway. Most of the Nigerian women reported psychosomatic trauma, and said they were not treated for post-traumatic stress disorder due to a lack of English-speaking psychologists, who also refused to treat migrants without documents. Migrant WSWs from North Africa, who have been living in France for longer, reported a particular need to fight stigmatization and build social ties. Eastern European migrant WSWs reported frequent trips back to their home countries to see their families and often their children, limiting their follow-up in care facilities.
Participants, particularly those of sub-Saharan origin, also often mentioned the notion of excision and lack of knowledge of their own body.
“Most don’t know if they have been or not” (Health care worker talking about genital mutilation/cutting).
Upon inclusion, 28% (n = 37/132) of migrant WSWs felt that the CHWs could not help them with their sexual health. Moreover, the vast majority of migrant WSWs (69%, n = 93/132) provided no help to their peers to improve their sexual health.
At 3 months, 63% (n = 60/95) of participants knew about PrEP. A total of 21% of migrant WSWs were referred to care for their sexual health needs. More than one third of participants had been tested for HIV (34%, n = 33/95).
At 6 months of follow-up, 45% (n = 42/93) of migrant WSWs declared having asked the CHWs for help with their care.
At 3 and 6 months of follow-up by the CHWs, the cohort retention rates were 72 and 70%, respectively.
This study used a community-based recruitment and follow-up method. The main results from the migrant population showed relatively closed networks and community-specific needs. CHWs were able to set up multi-level actions with the migrant WSWs, while adapting to the local healthcare offer and the needs of each community.
The RDS network results of our study showed a significant compartmentalization of the migrant WSWs network. These sub-networks are structured around communities of belonging linked to the migrant WSWs country and geographic region of origin. Indeed, these results show the importance of community mediation actions investing in these sub-networks. Few studies exist about the characteristics of interactions between sex workers (25). Some studies provide some information about exchanges of social support and others resources between partners, clients, peers or co-workers (26, 27), but data is lacking on the organization and quality of the relationships described. Indeed, trust between migrant WSWs and CHWs is a key element in the linkage to care. Here we show that groups are compartmentalized, have different needs and require specific actions. The TGW community seemed, in our program, to have a better understanding of STI prevention issues than cisgender migrant women. One hypothesis is that they benefit more from the LGBTQ+ community network and targeted communication campaigns. TGWs may also benefit from information and support via LGBTQ+ Social Network apps (28). Furthermore, other studies comparing cis and transgender black women have shown that beyond gender, it is access to employment that is linked to prevention practices (29). Unfortunately, we can also confirm, notably in the sub-Saharan community, the high rate of post-traumatic stress disorder linked to the violence experienced during the migration pathway, and its consequences in terms of mental health (30, 31).
CHWs seem to be able to adapt actions to needs at individual and collective levels. They also enable institutions to adapt themselves in terms of care provision or recognition of specific community health needs. This study is exploratory but seems to show an impact even after 3 months on knowledge and screening practices. These results need to be confirmed with longer follow-up times and larger groups.
These results also showed women with a combination of vulnerability factors: lack of housing, multiple forms of violence and food insecurity. This calls for a complex, holistic approach on multiple levels. Indeed, the WHO is increasingly recommending integrated approaches for STI prevention and care (32). Levels of insecurity are high and probably lead to significant risk-taking (2). The participants have to meet their own needs as well as those of their families, and studies have shown that the presence of dependent children exacerbates the need for money and sexual risk-taking (33). There is a competitiveness of needs, with those of the children always taking precedence over those of the mother. Illegal status on the territory, lack of housing, multiple forms of violence and food insecurity mean that migrant WSWs need an approach that prioritizes their urgent needs. Numerous studies and “housing first” programs have shown that, in order to be effective, all preventive and therapeutic actions must first ensure the safety of the beneficiaries (34). Given the complexity of needs, CHWs could help optimize access to local resources, but this would clearly not be sufficient in a context of chronic lack of accommodation and food aid in France for the most vulnerable (35).
Community health work involves information-, education-, and communication-based activities, as well as health system navigation activities, and includes activities to involve professionals, stakeholders and communities. Health mediation is thus both a promising intervention (“one whose effectiveness has not been evaluated by research, but for which a solid normative evaluation induces a presumption of relevant results” (36)) and a complex one to study, in that it combines varied practices that require constant adaptation to a socially shifting context. Our results show that community health interventions with empowerment actions are part of an ecological concept that applies to interactive change at several levels: the individual, the organization and the community (37). Working on mediation issues therefore implies studying not only individual changes, but also changes in the social setting itself. In fact, to our knowledge, with the exception of some pioneering studies (38, 39), no study has been able to demonstrate its effectiveness by taking into account the conditions of the effect of mediation on health, because this evaluation requires integrating all this complexity. In fact, as mentioned above, healthcare mediation practices are multi-faceted, constantly adapting and multi-level (24). They make up an interventional system centered around the individual (40). Following this systemic approach, Richard et al. (20) proposed to map the theoretical conditions of feasibility and success of health mediation to promote the use of health services within a conceptual framework characterizing their potential interrelationships, which it would be interesting to map out in real life.
This study provides community data from a hidden key population, who are without linkage to care. Indeed, migrant WSWs do not receive care in the usual screening centers in the study region (41). Specific information on these communities is required to control the STI epidemic. More and more studies and programs are using RDS to reach these populations and enable specific interventions (42, 43). Furthermore, our findings demonstrated that migrant WSWs were able to recruit others, regardless of the level of education or vulnerability, showing how RDS could reach participants, even those with an illegal status and not followed by the NGOs network, within a short recruitment period. To our knowledge, this is the first RDS study in France on sex workers or on migrants. However, other RDS studies have been successfully carried out in other countries among sex worker populations (44, 45).
Some limitations have to be acknowledged. The study’s findings may lack generalizability due to its specific focus on Marseille and a relatively small sample size. Sampling bias and the absence of a control group limit the ability to establish a causal relationship between community health worker interventions and observed outcomes. The small size of the study population precluded extensive multivariate analysis, especially of subgroups. The short six-month follow-up period may not capture sustained changes over time. Additionally, reliance on self-reported data introduces the potential for recall and social desirability biases. However, this is important exploratory research within a difficult-to-reach population, which will allow us to set up more specific interventional studies.
In conclusion, CHWs can carry out complex and comprehensive interventions with migrant WSWs. This key population has multiple vulnerability factors and requires a holistic approach that takes into account different levels of network: the women’s family (especially their children), their community of origin to which they seem extremely connected, and the local care network to which they have little access despite their substantial needs. Other studies are required, using specific methodologies, to evaluate CHW actions, their acceptability, their cost effectiveness, and their impact on the health of beneficiaries and on public health. Finally, these actions carried out by harm-reduction CHWs should be accompanied by public policy measures to help secure the most vulnerable people, at the very least in terms of protection from stigma, discrimination and violence, and by providing emergency accommodation and food aid.
The original contributions presented in the study are included in the article/supplementary materials, further inquiries can be directed to the corresponding author.
The studies involving humans were approved by French Ethics Committee in October 2021 (no. 2021—A01746-35). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study. Written informed consent was obtained from the individual(s) for the publication of any identifiable images or data included in this article.
EM: Writing – original draft, Writing – review & editing, Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization. MH: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Software, Writing – original draft, Writing – review & editing, Supervision. FA: Conceptualization, Data curation, Funding acquisition, Investigation, Methodology, Project administration, Resources, Validation, Visualization, Writing – original draft, Writing – review & editing. HR: Data curation, Methodology, Validation, Writing – review & editing. ER: Conceptualization, Methodology, Validation, Writing – review & editing. DM: Conceptualization, Methodology, Validation, Writing – review & editing. MM: Conceptualization, Data curation, Funding acquisition, Investigation, Methodology, Project administration, Validation, Writing – review & editing. GI: Data curation, Investigation, Project administration, Validation, Writing – review & editing. MR: Conceptualization, Data curation, Project administration, Writing – review & editing. BS: Conceptualization, Methodology, Supervision, Writing – review & editing. SV: Conceptualization, Investigation, Methodology, Supervision, Writing – review & editing. ML: Data curation, Funding acquisition, Project administration, Resources, Validation, Writing – review & editing. CE: Conceptualization, Formal analysis, Investigation, Methodology, Project administration, Supervision, Writing – review & editing. PR: Writing – original draft, Writing – review & editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This work was supported by Sidaction grant number [2020-2-AEQ-12890], by the city of Marseille and by ViiV Healthcare.
The authors thank all participants, The Operational Team and NGOs and Especially Prospective Coopération, l’Amicale du Nid, Autres Regards, AIDES and the truth for their support and help.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. European Centre for Disease Prevention and Control, World Health Organization . HIV/AIDS Surveillance in Europe 2020: 2019 Data. LU: Publications Office (2020).
2. Desgrees-du-Lou, A, Pannetier, J, Ravalihasy, A, Le Guen, M, Gosselin, A, Panjo, H, et al. Is hardship during migration a determinant of HIV infection? Results from the ANRS PARCOURS study of sub-Saharan African migrants in France. AIDS. (2016) 30:645–56. doi: 10.1097/QAD.0000000000000957
3. De Monteynard, L-A . Infection Par le VIH Chez les Patients Migrants Suivis en France. [PhD Thesis], vol. 6. Paris:theses.hal.science (2016).
4. Cazein, F, Lot, F, Pillonel, J, Le Strat, Y, Sommen, C, Pinget, R, et al. Découvertes de séropositivité VIH et de sida, France, 2003-2013. Bull Epidémiol Hebd. (2015) 9:152Á61.
5. Hadj, L, Desgrées du Loû, A, Dupont, J, and Nguyen, V-K. Acceptabilité et freins chez les populations africaines et caribéennes vivant en Ile-de-France d’une nouvelle offre de prévention du VIH: le Truvada en prophylaxie pré-exposition (PrEP): une enquête exploratoire. Bulletin Epidemiologique Hebdomadaire. (2017) 6:110–4.
6. Baral, S, Beyrer, C, Muessig, K, Poteat, T, Wirtz, AL, Decker, MR, et al. Burden of HIV among female sex workers in low-income and middle-income countries: a systematic review and meta-analysis. Lancet Infect Dis. (2012) 12:538–49. doi: 10.1016/S1473-3099(12)70066-X
7. Scorgie, F, Chersich, MF, Ntaganira, I, Gerbase, A, Lule, F, and Lo, Y-R. Socio-demographic characteristics and behavioral risk factors of female sex workers in sub-saharan Africa: a systematic review. AIDS Behav. (2012) 16:920–33. doi: 10.1007/s10461-011-9985-z
8. Weller, S, and Davis, K. Condom effectiveness in reducing heterosexual HIV transmission. Cochrane Database Syst Rev. (2002) 2012:CD003255. doi: 10.1002/14651858.CD003255
9. Wilson, AL . A systematic review and Meta-analysis of the efficacy and safety of intermittent preventive treatment of malaria in children (IPTc). PLoS One. (2011) 6:e16976. doi: 10.1371/journal.pone.0016976
10. Parriault, M-C, Basurko, C, Melle, AV, Gaubert-Maréchal, E, Rogier, S, Couppié, P, et al. Predictive factors of unprotected sex for female sex workers: first study in French Guiana, the French territory with the highest HIV prevalence. Int J STD AIDS. (2015) 26:542–8. doi: 10.1177/0956462414545794
11. Parriault, M-C, van Melle, A, Basurko, C, Gaubert-Marechal, E, Macena, RHM, Rogier, S, et al. HIV-testing among female sex workers on the border between Brazil and French Guiana: the need for targeted interventions. Cad Saude Publica. (2015) 31:1615–22. doi: 10.1590/0102-311X00138514
12. Desgrées du, LA, Pannetier, J, Ravalihasy, A, Gosselin, A, Supervie, V, Panjo, H, et al. Migrants subsahariens suivis pour le VIH en France: combien ont été infectés après la migration?: estimation dans l’étude ANRS-Parcours. Bull Epidémiol Hebd. (2015) 40:752–8.
13. Puppo, C, Spire, B, Morel, S, Génin, M, Béniguel, L, Costagliola, D, et al. How PrEP users constitute a community in the MSM population through their specific experience and management of stigmatization. The example of the French ANRS-PREVENIR study. AIDS Care. (2020) 32:32–9. doi: 10.1080/09540121.2020.1742863
14. de Santé, HA . La Médiation en Santé Pour les Personnes Éloignées des Systèmes de Prévention et de Soins. Référentiel de Compétences, Formations et Bonnes Pratiques, Rapport Final Haute Autorité de Santé (HAS) (2017)
15. Sarriot, E, Davis, T, Morrow, M, Kabore, T, and Perry, H. Motivation and performance of community health workers: nothing new under the Sun, and yet …. Glob Health Sci Pract. (2021) 9:716–24. doi: 10.9745/GHSP-D-21-00627
16. Cometto, G, Ford, N, Pfaffman-Zambruni, J, Akl, EA, Lehmann, U, McPake, B, et al. Health policy and system support to optimise community health worker programmes: an abridged WHO guideline. Lancet glob. Health. (2018) 6:e1397–404. doi: 10.1016/S2214-109X(18)30482-0
17. Mosnier, E, Artigas, F, Richard, E, Hoyer, M, Michels, D, Vandentorren, S, et al. Effectiveness of a community empowerment intervention to improve access to pre-exposure prophylaxis in migrant women sex workers: protocol for a mixed methods implementation study. JMIR Res Protoc. (2023) 12:e42844. doi: 10.2196/42844
18. Ridde, V . Suggestions d’ameliorations d’un cadre conceptuel de l’evaluation participative. Can J Program Eval. (2006) 21:1–23. doi: 10.3138/cjpe.21.001
19. Baum, F, MacDougall, C, and Smith, D. Participatory action research. J Epidemiol Community Health. (2006) 60:854–7. doi: 10.1136/jech.2004.028662
20. Tremblay, M-C, Martin, DH, McComber, AM, McGregor, A, and Macaulay, AC. Understanding community-based participatory research through a social movement framework: a case study of the Kahnawake schools diabetes prevention project. BMC Public Health. (2018) 18:487. doi: 10.1186/s12889-018-5412-y
21. Malekinejad, M, Johnston, LG, Kendall, C, Kerr, LR, Rifkin, MR, and Rutherford, GW. Using respondent-driven sampling methodology for HIV biological and behavioral surveillance in international settings: a systematic review. AIDS Behav. (2008) 12:S105–30. doi: 10.1007/s10461-008-9421-1
22. Yılmaz Koğar, E, and Koğar, H. A systematic review and meta-analytic confirmatory factor analysis of the perceived stress scale (PSS-10 and PSS-14). Stress Health. (2023) 40:e3285. doi: 10.1002/smi.3285
23. ETHOS . Typology on Homelessness and Housing Exclusion. (2017). Available at: https://www.feantsa.org/en/toolkit/2005/04/01/ethos-typology-on-homelessness-and-housing-exclusion (Accessed March 15, 2021)
24. Richard, E, Vandentorren, S, and Cambon, L. Conditions for the success and the feasibility of health mediation for healthcare use by underserved populations: a scoping review. BMJ Open. (2022) 12:e062051. doi: 10.1136/bmjopen-2022-062051
25. Shushtari, ZJ, Hosseini, SA, Sajjadi, H, Salimi, Y, Latkin, C, and Snijders, TAB. Social network and HIV risk behaviors in female sex workers: a systematic review. BMC Public Health. (2018) 18:1020. doi: 10.1186/s12889-018-5944-1
26. Chen, Y, Latkin, C, Celentano, DD, Yang, X, Li, X, Xia, G, et al. Delineating interpersonal communication networks: a study of the diffusion of an intervention among female entertainment workers in Shanghai, China. AIDS Behav. (2012) 16:2004–14. doi: 10.1007/s10461-012-0214-1
27. Reisner, SL, Mimiaga, MJ, Bland, S, Mayer, KH, Perkovich, B, and Safren, SA. HIV risk and social networks among male-to-female transgender sex workers in Boston. Massachusetts J Assoc Nurses AIDS Care. (2009) 20:373–86. doi: 10.1016/j.jana.2009.06.003
28. Sun, CJ, Sutfin, E, Bachmann, LH, Stowers, J, and Rhodes, SD. Comparing men who have sex with men and transgender women who use Grindr, other similar social and sexual networking apps, or no social and sexual networking apps: implications for recruitment and health promotion. J AIDS Clin Res. (2018) 9:757. doi: 10.4172/2155-6113.1000757
29. Rutledge, JD, Anderson-Carpenter, K, and Puckett, J. HIV testing and associated characteristics among black cisgender and transgender women in the United States. J Healthc Sci Humanit. (2021) 11:149–62.
30. Khouani, J, Blatrix, L, Tinland, A, Jego, M, Gentile, G, Fond, G, et al. Health status of recently arrived asylum seekers in their host country: results of a cross-sectional observational study. BMC Public Health. (2022) 22:1688. doi: 10.1186/s12889-022-14095-8
31. Khouani, J, Landrin, M, Boulakia, RC, Tahtah, S, Gentile, G, Desrues, A, et al. Incidence of sexual violence among recently arrived asylum-seeking women in France: a retrospective cohort study. Lancet Regional Health Europe. (2023) 34:100731. doi: 10.1016/j.lanepe.2023.100731
32. WHO . Consolidated Guidelines on HIV, Viral Hepatitis and STI Prevention, Diagnosis, Treatment and Care for Key Populations. Geneva, Switzerland: World Health Organization (2022).
33. Hao, C, Guida, J, Morisky, DE, and Liu, H. Family network, workplace network, and their influence on condom use: a qualitative study among older female sex Workers in China. J Sex Res. (2015) 52:924–35. doi: 10.1080/00224499.2014.973101
34. Baxter, AJ, Tweed, EJ, Katikireddi, SV, and Thomson, H. Effects of housing first approaches on health and well-being of adults who are homeless or at risk of homelessness: systematic review and meta-analysis of randomised controlled trials. J Epidemiol Community Health. (2019) 73:379–87. doi: 10.1136/jech-2018-210981
35. La Fondation Abbé Pierre . 28e Rapport Sur l’état du Mal-Logement en France 2023. (2023). Available at: https://www.fondation-abbe-pierre.fr/actualites/28e-rapport-sur-letat-du-mal-logement-en-france-2023
36. Lacouture, A. Etat de l’art des Dispositifs mis en Oeuvre à l’étranger pour Favoriser Auprès des Décideurs le Recours aux Données sur des Interventions Probantes ou Prometteuses dans le Champ de la Prévention ou de la Promotion de la Santé. EHESP Eole Des Hautes Etudes en Santé Publique (2016).
37. Wallerstein, N . Powerlessness, empowerment, and health: implications for health promotion programs. Am J Health Promot. (1992) 6:197–205. doi: 10.4278/0890-1171-6.3.197
38. Musso, S, and Delaquaize, H. Réinventer la roue? La difficile capitalisation des expériences de médiation en santé en France In: Convention Nationale 2016 Sidaction. HAL science Paris, France: Mairie de Paris; Sidaction (2016). 1–20.
39. DGS . Évaluation des Actions de Proximité des Médiateurs de Santé Publique et de Leur Formation dans le Cadre d’un Programme Expérimental mis en Oeuvre par l’IMEA. Direction Générale de la Santé (2006)
40. Cambon, L, Terral, P, and Alla, F. From intervention to interventional system: towards greater theorization in population health intervention research. BMC Public Health. (2019) 19:339. doi: 10.1186/s12889-019-6663-y
41. Eldin, C, Hoyer, M, Martinet, P, Saule, J, Villermy, P, Inegbeze, G, et al. There Is Still a Long Way to Go to Facilitate PrEP Use in Migrant Women Sex Workers. ESCMID congress 2022 (2023).
42. Nagot, N, D’Ottavi, M, Quillet, C, Debellefontaine, A, Castellani, J, Langendorfer, N, et al. Reaching hard-to-reach people who use drugs: a community-based strategy for the elimination of hepatitis C. Open Forum Infect Dis. (2022) 9:ofac181. doi: 10.1093/ofid/ofac181
43. Des Jarlais, D, Duong, HT, Pham Minh, K, Khuat, OHT, Nham, TTT, Arasteh, K, et al. Integrated respondent-driven sampling and peer support for persons who inject drugs in Haiphong, Vietnam: a case study with implications for interventions. AIDS Care. (2016) 28:1312–5. doi: 10.1080/09540121.2016.1178698
44. de Matos, MA, da França, DD, Carneiro, MADS, Martins, RMB, Kerr, LRFS, Caetano, KAA, et al. Viral hepatitis in female sex workers using the respondent-driven sampling. Rev Saude Publica. (2017) 51:65. doi: 10.1590/S1518-8787.2017051006540
45. Mbunda, T, Tarimo, EAM, Bakari, M, Sandström, E, and Kulane, A. Recruitment using respondent driven sampling, risk behaviors assessment and willingness of young female sex workers (18–25 years) in Dar Es Salaam, Tanzania to participate in HIV vaccine trials. BMC Public Health. (2019) 19:1537. doi: 10.1186/s12889-019-7822-x
Keywords: community health interventions, women sex workers, migrants, cohort, community-based participatory research, health promotion, community health workers
Citation: Mosnier E, Hoyer M, Artigas F, Regnault H, Richard E, Michels D, Mosnier M, Inegbeze G, Robledo MS, Spire B, Vandentorren S, Lescaudron M, Eldin C and Roux P (2024) Enhancing sexual health and empowerment among migrant women sex workers: a community health worker-led intervention in Marseille, France. Front. Public Health. 12:1359363. doi: 10.3389/fpubh.2024.1359363
Edited by:
Nicolas Vignier, Université Sorbonne Paris Nord, FranceReviewed by:
Emilien Jeannot, Centre Hospitalier Universitaire Vaudois (CHUV), SwitzerlandCopyright © 2024 Mosnier, Hoyer, Artigas, Regnault, Richard, Michels, Mosnier, Inegbeze, Robledo, Spire, Vandentorren, Lescaudron, Eldin and Roux. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Emilie Mosnier, ZW1pbGllLm1vc25pZXJAZ21haWwuY29t
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.