 Delong Wang
Delong Wang Ying Wang
Ying Wang Huifen Ma
Huifen Ma Shichao Zhao
Shichao Zhao
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health, 21 June 2024
Sec. Public Health Education and Promotion
Volume 12 - 2024 | https://doi.org/10.3389/fpubh.2024.1358269
This article is part of the Research TopicHealth Promotion in Schools, Universities, Workplaces, and CommunitiesView all 44 articles
Backgrounds: In the petrochemical industry, employees are exposed to various health hazards, which pose serious challenges to their health and hinder the sustainable development of the petrochemical industry. Investing in health has proved a potential strategy to enhance general health. However, global health investment is notably insufficient, mainly due to the public’s limited intention to invest in their health. While past research has identified various determinants of health investment intentions, the relationship between health literacy and health investment intention remains somewhat controversial and needs more empirical validation.
Objectives: This study aims to assess the level of health literacy and health investment intention among employees in one of China’s largest petrochemical companies and to explore the effect of health literacy on health investment intention.
Methods: A cross-sectional study was conducted in a petrochemical company. The valid sample size for this study was 39,911 respondents. Data were collected using a designed questionnaire, including socio-demographic information, questions about health investment intention, and the “2020 National Health Literacy Monitoring Questionnaire.” Several statistical analysis methods were employed, including descriptive analysis, Chi-square test, logistic regression, and multiple linear regression.
Results: The study disclosed an average health literacy score of 56.11 (SD = 10.34) among employees, with 52.1% surpassing the qualification threshold. The “Chronic Disease” dimension exhibited the lowest qualification rate at 33.0%. Furthermore, 71.5% of the employees expressed an intention to invest in health, yet a significant portion (34.5%) opted for the minimal investment choice, less than 2,000 RMB. Logistic regression analysis indicated a positive correlation between health literacy and health investment intention (OR = 1.474; p < 0.001). This association’s robustness was further indicated by multiple linear regression analyses (β = 0.086, p<0.001).
Conclusion: The employees’ health literacy significantly exceeds the national average for Chinese citizens, yet the qualified rate in the “Chronic Disease” dimension remains notably low. A majority of employees have the intention to invest in health, albeit modestly. Furthermore, while health literacy does positively influence health investment intention, this effect is somewhat limited. Accordingly, personalized Health education should be prioritized, with a focus on improving chronic disease knowledge and facilitating the internalization of health knowledge into health beliefs.
Occupational Health has become a crucial determinant of the development of the world economy and society, particularly in developing countries (1, 2). Worldwide, an estimated 1.53 million deaths and 76.1 million DALYs were attributable to the included occupational risk factors, accounting for 2.8% of deaths and 3.2% of DALYs from all causes (3). Specifically, in the petrochemical industry, employees are exposed to various health hazards, leading to significant health concerns (4, 5). These issues hinder the sustainable development of the petrochemical industry and, more importantly, pose serious challenges to the health and well-being of employees. Therefore, it is imperative to prioritize the health of petrochemical employees.
Health investment, encompassing preventive healthcare, nutrition, physical activity, etc. (6), presents a viable approach to enhancing overall health. Research substantiates that health investments effectively reduce disease risk, total medical expenditures, and health insurance costs (7). For example, Levi et al. (8) found that future healthcare expenses could be reduced by 6.2 dollars for every dollar invested in preventative healthcare. However, despite its recognized importance, the inadequacy of health investment is quite common. As an illustration, personal and household expenditures on preventive healthcare services constitute approximately 0.33% of the overall GDP and even less than 0.10% in developing countries (9).
The insufficient investment in health can primarily be attributed to the public’s limited intention to invest in their health (10). The health investment intention is influenced by a variety of factors, including economic factors like income and expected income (11, 12), social factors such as the degree of social trust and social networks (13), psychological factors including self-perceived disease risk and self-perceived hazards (14, 15), and individual characteristics like age, gender, education level and self-assessed health (16–18). However, previous research overlooks the influence of health literacy on health investment intention.
Health literacy is the degree to which individuals have the ability to find, understand, and use information and services to inform health-related decisions and actions for themselves and others (19). High health literacy is empirically linked to a range of positive health-related behaviors and outcomes (20), such as improved health decision-making (21), proper medication use (22), decreased mortality and morbidity (23, 24), and enhanced communication with healthcare providers (25). Notably, the improvement of health literacy is a key driver in prompting individuals’ awareness and engagement with preventive healthcare services (24, 26). Conversely, low health literacy is often associated with an increased dependence on treatment and emergency services over preventive measures (27).
The relationship between health literacy and health investment intention remains somewhat controversial. Theoretically, health literacy endows individuals with essential skills to comprehend health information, thereby empowering them to accurately evaluate their health needs and improve the quality of health-related decisions, which can potentially increase their health investment intention. However, empirical evidence suggests a paradox: while individuals often acknowledge the benefits of preventive healthcare, they frequently show reluctance to incur its costs (28). This observation raises questions about the straightforward link between high health literacy and increased health investment intention. To clarify the relationship, further empirical research is necessary.
This study investigates the health literacy and health investment intention of employees in a petrochemical company through a cross-sectional analysis. It aims to examine the relationship between the employees’ health literacy and health investment intention, thereby providing some implications to enhance both the occupational health of petrochemical employees and the health human capital of the petrochemical industry.
The comprehensive cross-sectional analysis of 39,911 employees in a major petrochemical company in China addresses a relatively under-explored area - the impact of health literacy on health investment decisions in a high-risk occupational setting, and aligns profoundly with the objectives of ‘Public Health Education and Promotion’. We provide empirical evidence supporting the positive correlation between health literacy and health investment intention, highlighting the importance of enhancing health literacy as a means to encourage proactive health investment behaviors. The study’s exploration of the general yet modest health investment intentions among employees also shows the complexities of translating health literacy into actual health-promoting behaviors. This finding reveals health education should not only focus on popularizing health knowledge but also on facilitating its practical application and internalization into health beliefs and actions. Additionally, the recommendations provided in the manuscript for personalized health education, focusing on chronic diseases and employing behavioral economics principles like ‘nudge’ strategies, are innovative and align well with the latest trends in health education and promotion.
This study employed a cross-sectional study design. Data were collected from one of China’s largest petrochemical companies. The sole inclusion criteria was that the respondent must be an in-service employee of the petrochemical company. The primary objective of this study is to examine the relationship between employees’ health literacy and their intentions to invest in health. We will test the following research hypotheses: Ha: Health literacy has a significant positive effect on health investment intentions. H0: Health literacy has no significant positive effect on health investment intentions. The secondary objective of this study is to investigate the current state of health literacy and health investment intentions among employees in a petrochemical company.
Prior to initiating the formal investigation, a preliminary survey was carried out among selected employees within a subsidiary, which aimed to provide a comprehensive evaluation of the questionnaire’s design. The survey respondents, comprising employees with diverse educational backgrounds, provided feedback that demonstrated a clear understanding of the questionnaire’s design and layout.
In the formal investigation phase, the survey questionnaire was deployed on the company’s internal website from April 1, 2022, and remained accessible for a period of 1 week. During this time, employees were afforded the opportunity to voluntarily complete the questionnaire at any time and from any location. The duration to complete the questionnaire was limited to 5 to 20 min. Out of an approximate total of 108,000 employees, 45,024 individuals voluntarily participated in the survey. To maintain the integrity of the responses and discourage dishonesty, respondents were limited to switching away from the questionnaire screen no more than twice during completion. Out of the 45,024 questionnaires returned, 5,113 were disqualified due to cheating, yielding an effective response rate of 88.64%. Consequently, the valid sample size for this study amounted to 39,911 respondents. This study adhered to the guidelines of the Declaration of Helsinki and received approval from the Ethics Committee of Traditional Chinese Medicine Hospital in Dongying District (No. ZYY-LL-006).
The questionnaire used in this study includes three sections.
1. Socio-demographic information: This section gathers data on respondents’ gender, age, income, marital status, education level, occupation, and presence of any chronic diseases. Table 1 shows the variable assignment table.
2. Health Investment Intention: It is measured using two questions. The first question is, “When you are in good health, are you willing to invest in your health? (Such as: pay for health care products, pay for health insurance, pay for health management costs)” with responses coded as a binary variable: “unwilling = 0, willing = 1.” As the construct of health investment intention is concrete, employing a single-item “global” measure is more concise, efficient and allows respondents to comprehensively consider all facets of the concept and their personal preferences (29). The second question is, “How much are you willing to pay annually to invest in your health” with responses coded as a multiple categorical variable: “0 yuan = 0, ≤2,000 yuan = 1, 2,000–5,000 yuan = 2, 5,000–10,000 yuan = 3, >10,000 yuan = 4.” For statistical analysis, it is treated as a continuous variable in the linear regression model.
3. Health Literacy: The study employs the “2020 National Health Literacy Monitoring Questionnaire,” developed by the National Health Commission of China, to measure health literacy. This questionnaire includes three aspects: Basic Knowledge and Attitudes, Health-Related Skills, and Healthy Behaviors and Lifestyles. Further, it can also be divided into six dimensions: Scientific Views of Health, Health Information, Infectious Disease, Chronic Disease, Safety and First Aid, and Primary Medical Care. The questionnaire’s maximum score is 73, with respondents answering over 80% of the questions correctly considered qualified. In the statistical analysis, the total scores were treated as a continuous variable in the linear regression model, while the qualification status was used as a binary variable in the logistic regression model.
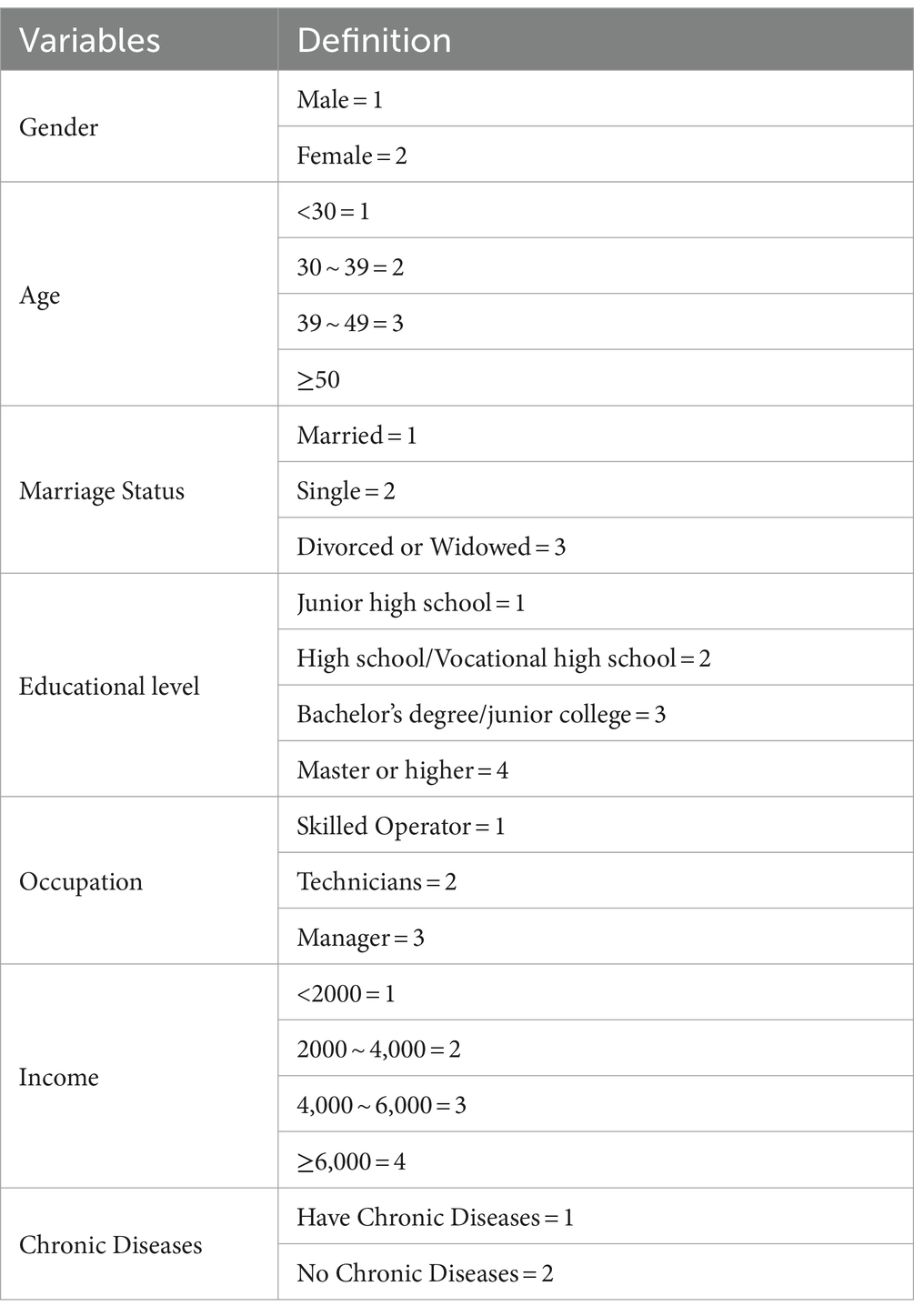
Table 1. Variable assignment table.
This study utilized several statistical analysis methods, including descriptive analysis, Chi-square test, logistic regression, and multiple linear regression. The Chi-square test is applied to identify differences in health investment intentions among different groups. Logistic regression is employed to assess the effect of health literacy on health investment intention. Additionally, multiple linear regression is used to confirm the consistency and robustness of this relationship. All statistical analyses are performed using SPSS 22.0 (30). Results will be considered statistically significant if rejecting Alpha at p < 0.05.
The socio-demographic characteristics of the respondents are shown in Table 2. The majority of the respondents (74.8%) fell within the young to middle-aged category, aged 30–49. Over half of the employees (55.4%) held a bachelor’s degree or higher. Skilled operators constituted the majority (60.2%) of the respondents. Notably, the average monthly household disposable income for the vast majority (91.0%) was below 6,000 yuan. Most of the employees (72.1%) had at least one chronic disease.
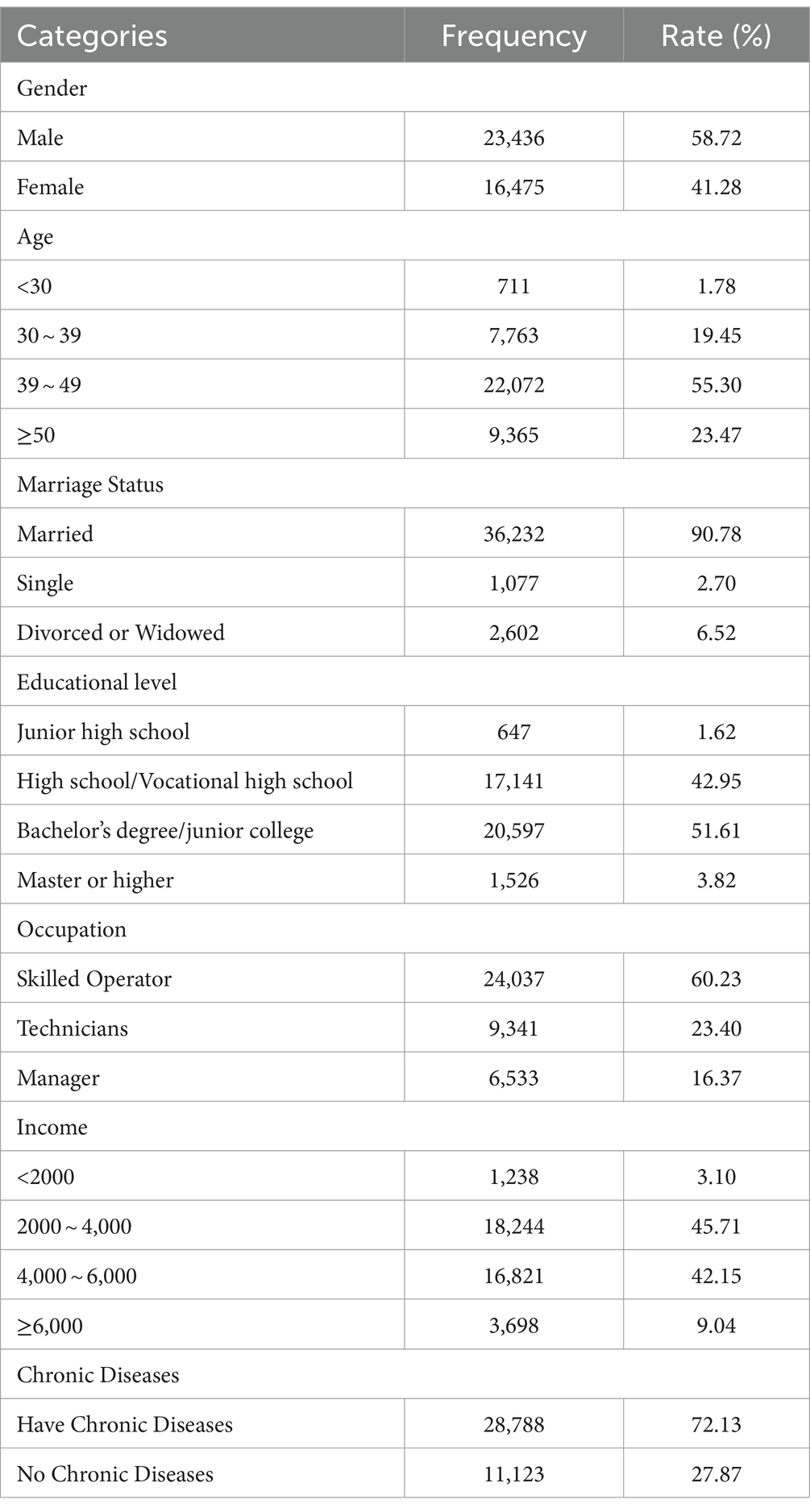
Table 2. Basic information of the petrochemical employees.
Among the surveyed employees, 52.1% (20,782 individuals) met the qualification criteria, with an average score of 56.11. The scores and qualification rate across three aspects and six dimensions of health literacy are shown in Table 3. Notably, the Chronic Disease dimension exhibited the lowest qualification rate at 33.0%.
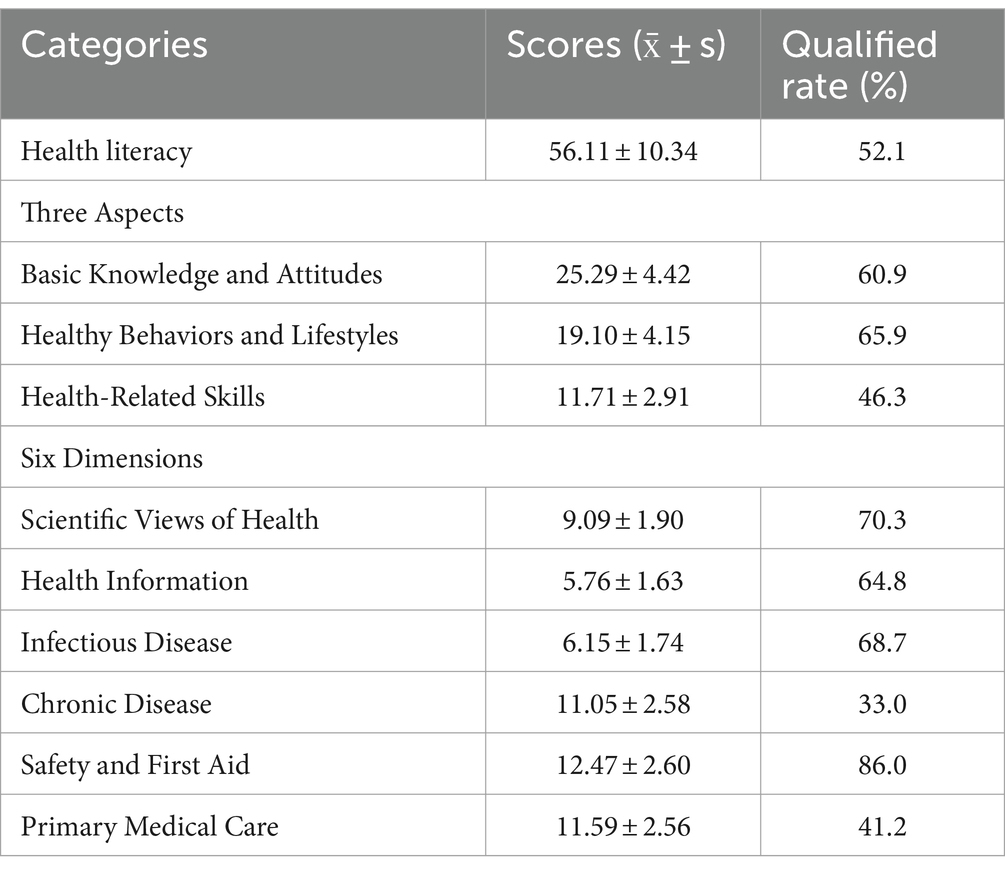
Table 3. Qualified rate and scores of health literacy.
In terms of health investment intention, the results indicated a majority of employees (71.5%) intended to invest in their health. Nonetheless, a notable proportion (34.5%) preferred the minimum investment option, under 2,000 RMB, as detailed in Table 4.
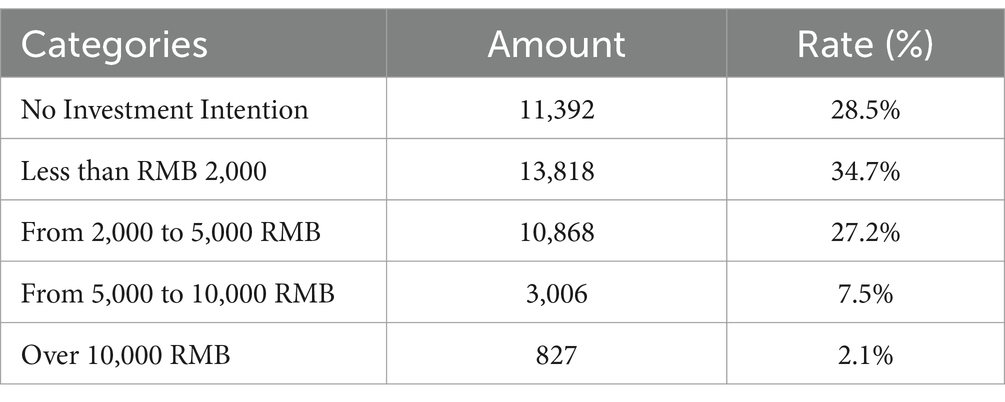
Table 4. Amount and rate of health investment intention.
After the chi-square test, it was found that there is a significant correlation between the qualified condition of health literacy, the health investment intentions, and socio-demographic variables such as gender, age, marital status, educational level, occupational type, income, and the presence of chronic diseases (p < 0.05), as detailed in Table 5.
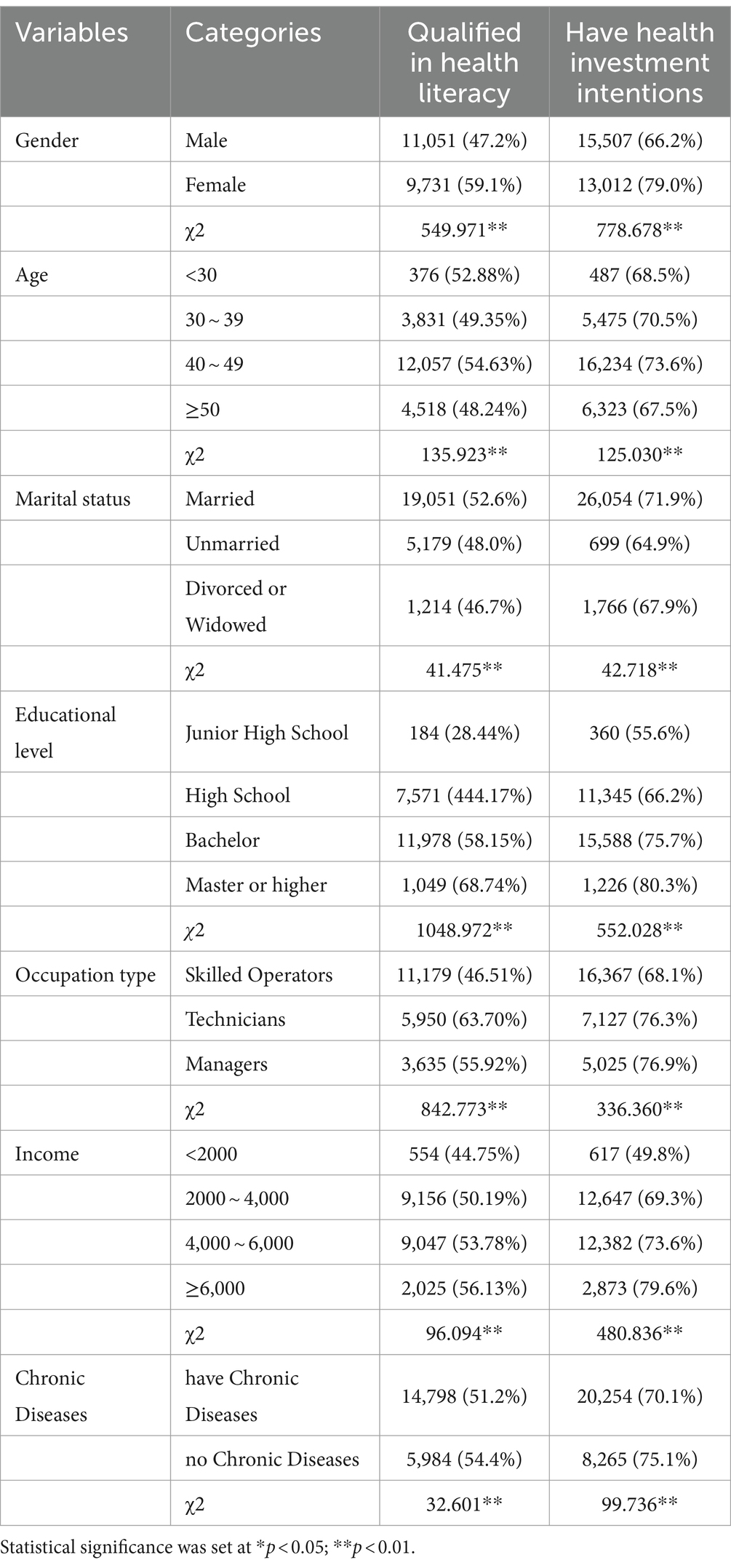
Table 5. Socio-demographic differences in health literacy and health investment intention.
A binary logistic regression was conducted with health investment intention as the dependent variable and health literacy qualified condition as the independent variable, controlling socio-demographic factors such as gender, age, marital status, education, occupation, income, and chronic diseases. The results, shown in Table 6, indicate that all these factors significantly influence health investment intentions. Notably, respondents with qualified health literacy exhibited a higher health investment intention (OR = 1.474, p<0.05) compared to those with unqualified health literacy.
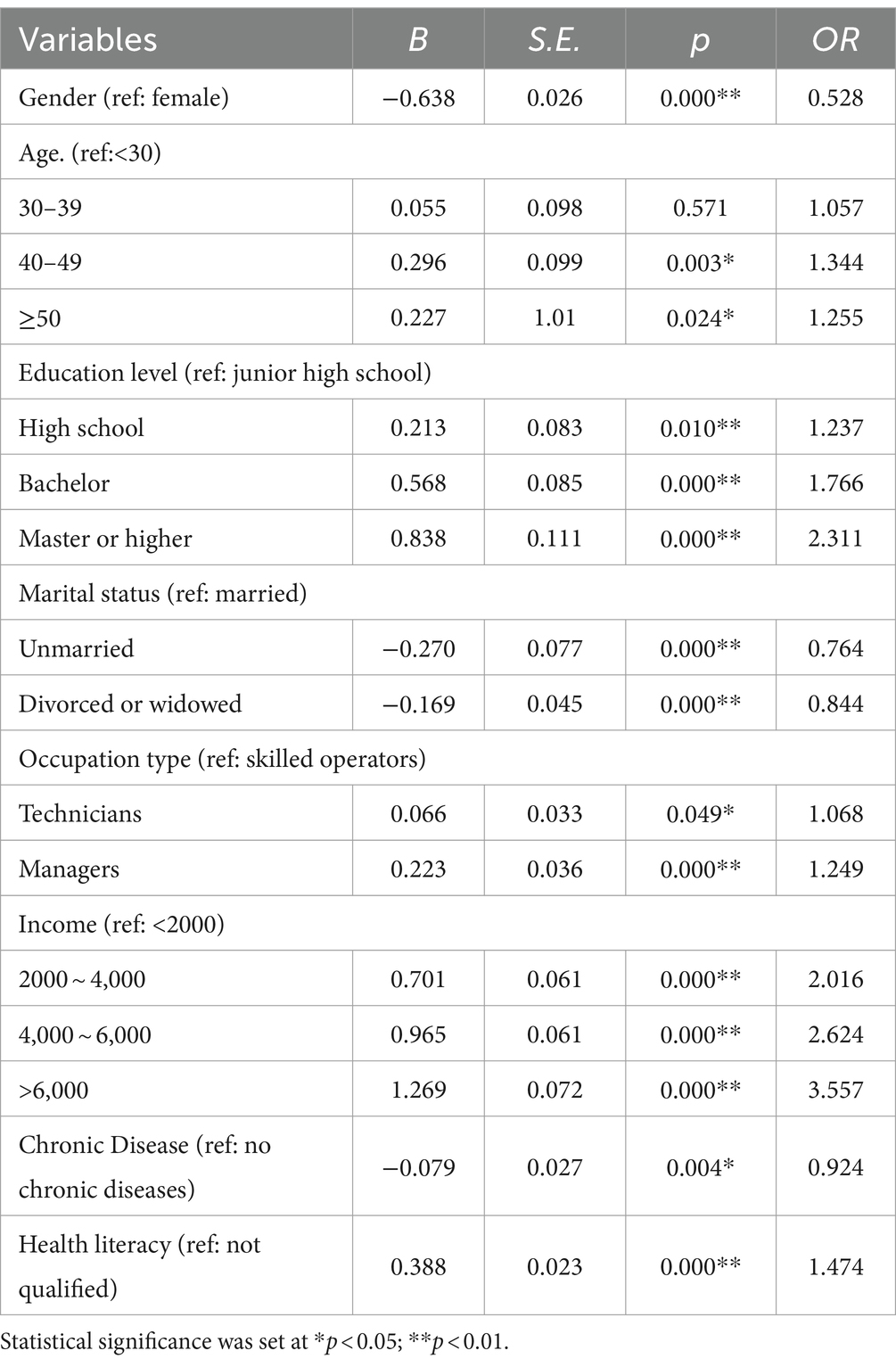
Table 6. Logistic regression model for influencing factors of health investment intention.
To further examine the robustness of the relationship between health literacy and health investment intention, the study employed alternative measures for both the independent and dependent variables and developed a multiple linear regression model. In this approach, health investment intention was quantified as a continuous variable, scaled from 0 to 4, to reflect the intensity of intention, and was used as the dependent variable. Health literacy score, instead of health literacy qualified condition, was used as the independent variable. The findings reveal that health literacy had a significantly positive effect (β = 0.086, p<0.05) on health investment intention. (Table 7).
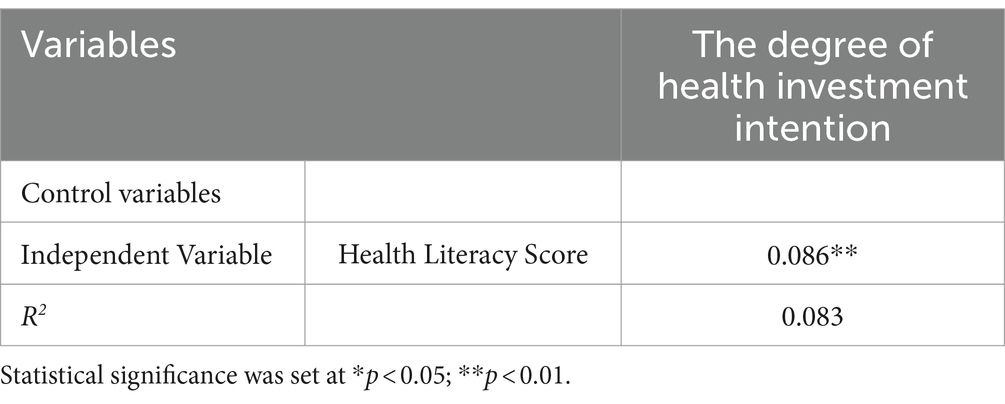
Table 7. Multiple regression model for the effect of health literacy on health investment intention.
It is crucial to improve occupational health among employees in the petrochemical industry. Previous studies have demonstrated health literacy and health investment intention significantly impact their health status. This study focuses on assessing the health literacy and health investment intentions of employees in a petrochemical company, aiming to clarify their relationship. The study reveals three key findings, which are outlined as follows.
First, the study showed that the qualified rate of health literacy among employees from the petrochemical company was 52.1%, surpassing the average level (23.15%) of Chinese citizens in 2021 (31). This discrepancy can be attributed to two reasons. On one hand, more than half of the employees (55.4%) in our study held a bachelor’s degree or above. Previous studies have confirmed higher educational levels often correlate with increased health literacy (32, 33). On the other hand, the company had implemented a long-term health education and promotion program before our investigation, which may play a crucial role in enhancing health literacy (34). Among different aspects and dimensions of health literacy, “Chronic Disease” (33.0%) demonstrated the lowest qualified rates, which might contribute significantly to the high incidence (72.1%) of chronic diseases among the employees since previous studies have indicated that limited health literacy regarding specific diseases can substantially increase their prevalence (24, 35).
Second, the results showed that 71.5% of the respondents had the intention to invest in their health, but the intended investment amounts were not high. Specifically, almost half of those who had health investment intention opted for the minimal investment bracket, under 2,000 RMB annually. The limited ability and motivation are two possible reasons for the limited amount of health investment. As for ability, low disposable income may be a constraint on higher health investment, since prior studies found those with low income frequently encounter financial hurdles in pursuing activities promoting health (36), such as maintaining a balanced diet, engaging in regular exercise, and avoiding high-risk activities (37, 38). In this study, 91% of respondents reported a household per capita disposable income below 6,000 RMB monthly. This figure is notably lower than the average monthly wage of 7,897 yuan reported in the Shandong Statistical Yearbook, which significantly restricts their ability to increase health investments ((39), p.7, Tables 1, 2). As for motivation, the intrinsic characteristics of health as a form of capital may diminish investment motivation. First, healthy human capital is acquired inborn, declines slowly, and diminishes imperceptibly, making individuals undervalue the potential disease susceptibility and seriousness (40, 41). Second, the return on investment of health human capital always has a certain delay, which will exacerbate the myopia effect and lead individuals to favor current utilities and undervalue perceived long-term health benefits (41). Additionally, the company offers both basic medical social insurance and supplementary medical insurance to all employees. Given the cost sharing mechanism between employer and employee in China’s social medical insurance, this provision may diminish the respondents’ intention to purchase commercial medical insurance, leading to a generally low level of health investment intention.
Third, a final but important finding of this study is that health literacy does positively influence health investment intention, though the strength of this effect is limited. The conversion of the standardized regression coefficient (β) to an effect size d of 0.2746, and the conversion of the Odds Ratio (OR) to an effect size d of 0.2139, both indicates that health literacy exerts a small effect (ranging from 0.2 to 0.4) on health investment intentions (42, 43). In our view, this observed limited effect may stem from two aspects. On one hand, health literacy may act as a distal variable, indirectly influencing health investment intention through other mediating variables (44). For example, health beliefs, being closer in the causal chain, might have a more direct impact on health investment intention and could mediate the effect of health literacy (45). On the other hand, the scale employed in this study focuses on evaluating employees’ specific health knowledge, thereby may not comprehensively capture the connotation of health literacy, though it is widely used in China. However, health literacy is a multifaceted concept that encompasses the ability to apply health information and critical thinking skills for informed health decisions (46). These facets, potentially more influential in shaping health investment intention, were not adequately represented in this study.
While this study yielded noteworthy findings, it is not without limitations. Firstly, the non-random sampling raises concerns about the generalizability of the conclusions. This study is limited by its single-institutional scope and cultural context, which constrain its generalizability to other occupational settings and population groups within the country. All participants were from a single petrochemical company that had implemented a health education and promotion program before the investigation, probably resulting in higher-than-average levels of health literacy among those surveyed. Furthermore, the company provides employees with both basic medical social insurance and supplementary medical insurance, which may contribute to a low level of health investment intention. The next phase of research should focus on addressing the limitation of inadequate sample representation by conducting comprehensive studies across entire populations and multiple countries. Secondly, potential selection bias may exist due to the response rate. More than half of the employees declined to participate, potentially introducing systematic bias into the conclusion. Thirdly, as previously mentioned, the health literacy measurement scale predominantly focused on assessing health knowledge, neglecting the assessment of the ability to apply health information and make informed health decisions, which may decrease the validation of measurement. Moreover, there are inherent measurement errors associated with using a single item to measure the health investment intention. It is advisable to develop multi-level measurement tools that can more accurately define health investment intention and its specific components in the future research. Finally, given the cross-sectional design of the study, it is unable to establish causality between health literacy and health investment intention. Additionally, the omission of certain confounding variables could introduce endogeneity issues into the analysis.
This study undertook a cross-sectional survey involving 39,911 employees from a petrochemical company to evaluate their health literacy and health investment intention, as well as to clarify the relationship between them. The results revealed that the employees’ health literacy significantly exceeds the national average for Chinese citizens, yet the qualified rate of Chronic Disease dimension is relatively low. A majority of employees have the intention to invest in health, albeit with a modest amount. Furthermore, the study demonstrates that while health literacy does positively influence health investment intention, this effect is somewhat limited.
Based on the aforementioned conclusions, the study proposes several recommendations. First, health education and promotion should focus on improving the employees’ health knowledge regarding chronic disease. Personalized health education, informed by the outcomes of employees’ physical examinations, should be implemented, emphasizing specific aspects like prevention, early detection, management, and treatment of chronic diseases. Moreover, these programs should incorporate interactive training methods, such as group discussions and question-and-answer sessions, to increase employee engagement and learning efficacy.
Second, health education should focus not only on spreading health knowledge but also on facilitating its internalization into health beliefs. Employing ‘nudge’ strategies from behavioral economics could help overcome psychological barriers. For example, according to the principle of loss aversion, where individuals generally prefer avoiding losses over acquiring similar gains, health education could be more effective in underscoring the negative consequences (such as illness, increased medical costs, and reduced quality of life) of unhealthy behaviors through concrete examples, rather than merely focusing on the benefits of healthy practices.
Finally, it is imperative for both the company and government to enhance the financial capacity of employees, as income is a pivotal determinant of their ability to invest in health, either through direct or indirect means. The company could establish a dedicated health investment fund aimed at offsetting the costs of preventive healthcare for employees. This fund would cover expenses related to regular health check-ups, vaccinations, and wellness programs. Concurrently, governments could offer incentives to encourage healthy behaviors in the workforce, such as tax benefits for participating in health programs, financial aid for obtaining health insurance, and subsidies for health-promoting activities. Implementing these strategies would not only improve the health outcomes of employees but also potentially reduce long-term healthcare costs.
The raw data supporting the conclusions of this article will be made available by the authors upon reasonable request and with permission of the data owners.
This study adhered to the guidelines of the Declaration of Helsinki and received approval from the Ethics Committee of Traditional Chinese Medicine Hospital in Dongying District (No. ZYY-LL-006). The participants provided their written informed consent to participate in this study.
DW: Writing – review & editing, Writing – original draft. YW: Writing – review & editing, Investigation, Data curation. HM: Writing – review & editing, Validation, Supervision. SZ: Writing – review & editing, Writing – original draft, Methodology, Investigation, Funding acquisition, Data curation.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. The research was supported by National Natural Science Foundation of China (No. 72204150).
The authors would like to deeply appreciate the officials from the occupational health sector in the petrochemical company and all participants’ invaluable contributions to this study.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Takala, J, Hämäläinen, P, Saarela, KL, Yun, LY, Manickam, K, Jin, TW, et al. Global estimates of the burden of injury and illness at work in 2012. J Occup Environ Hyg. (2014) 11:326–37. doi: 10.1080/15459624.2013.863131
2. Zhang, X, Wang, Z, and Li, T. The current status of occupational health in China. Environ Health Prev Med. (2010) 15:263–70. doi: 10.1007/s12199-010-0145-2
3. GBD 2016 Occupational Risk Factors Collaborators. Global and regional burden of disease and injury in 2016 arising from occupational exposures: a systematic analysis for the global burden of disease study 2016. Occup Environ Med. (2020) 77:133–41. doi: 10.1136/oemed-2019-106008
4. Benson, C, Dimopoulos, C, Argyropoulos, CD, Varianou Mikellidou, C, and Boustras, G. Assessing the common occupational health hazards and their health risks among oil and gas workers. Saf Sci. (2021) 140:105284. doi: 10.1016/j.ssci.2021.105284
5. Gardner, RON. Overview and characteristics of some occupational exposures and health risks on offshore oil and gas installations. Ann Occup Hyg. (2003) 47:201–10. doi: 10.1093/annhyg/meg028
6. Cropper, ML. Health, investment in health, and occupational choice. J Polit Econ. (1977) 85:1273–94. doi: 10.1086/260637
7. Murphy, KM, and Topel, RH. The economic value of medical research. Obstet Gynecol. (2003) 15:125–46. doi: 10.1097/00006250-200205000-00027
8. Levi, J. Prevention for a healthier America. Health Aff. (2012) 2012:17428. doi: 10.1377/forefront.20120301.017428
9. Friedman, W, and Wilson, N. Money, masculinity, and men’s health: Experimental evidence on demand for a preventive health input. Houston, Texas: University of Houston Working Paper (2018).
10. Ajzen, I. The theory of planned behavior. Organ Behav Hum Decis Process. (1991) 50:179–211. doi: 10.1016/0749-5978(91)90020-T
11. Du, J, and Yagihashi, T. Health capital investment and time spent on health-related activities. Rev Econ Househ. (2017) 15:1215–48. doi: 10.1007/s11150-017-9378-9
12. Javan-Noughabi, J, Kavosi, Z, Faramarzi, A, and Khammarnia, M. Identification determinant factors on willingness to pay for health services in Iran. Heal Econ Rev. (2017) 7:40–6. doi: 10.1186/s13561-017-0179-x
13. Wang, W, Jin, J, He, R, Gong, H, and Tian, Y. Farmers’ willingness to pay for health risk reductions of pesticide use in China: a contingent valuation study. Int J Environ Res Public Health. (2018) 15:625. doi: 10.3390/ijerph15040625
14. Basu, R. Willingness-to-pay to prevent Alzheimer’s disease: a contingent valuation approach. Int J Health Care Finance Econ. (2013) 13:233–45. doi: 10.1007/s10754-013-9129-2
15. Milligan, MA, Bohara, AK, and Pagán, JA. Assessing willingness to pay for cancer prevention. Int J Health Care Finance Econ. (2010) 10:301–14. doi: 10.1007/s10754-010-9082-2
16. Chen, F, Xu, X-L, Yang, Z, Tan, H-W, and Zhang, L. The willingness-to-pay for general practitioners in contractual service and influencing factors among empty nesters in Chongqing, China. Int J Environ Res Public Health. (2015) 12:9330–41. doi: 10.3390/ijerph120809330
17. Wu, Y, Dong, H, Duan, S, Liu, X, Ye, C, You, H, et al. Study on willingness to participate and willingness to pay for hypothetical industrial injury insurance scheme. Zhonghua Lao Dong Wei Sheng Zhi Ye Bing Za Zhi. (2014) 32:732–41. doi: 10.3760/cma.j.issn.1001-9391.2014.10.004
18. Wang, Q, Zhou, Y, Ding, X, and Ying, X. Demand for long-term care insurance in China. Int J Environ Res Public Health. (2017) 15:6. doi: 10.3390/ijerph15010006
19. U.S. Department of Health and Human Services. (2020). Healthy people 2030 health literacy definitions. Available at: https://health.gov/our-work/healthy-people/healthy-people-2030/health-literacy-healthy-people-2030.
20. Nutbeam, D, and Lloyd, JE. Understanding and responding to health literacy as a social determinant of health. Annu Rev Public Health. (2021) 42:159–73. doi: 10.1146/annurev-publhealth-090419-102529
21. Mancuso, CA, and Rincon, M. Asthma patients' assessments of health care and medical decision making: the role of health literacy. J Asthma. (2006) 43:41–4. doi: 10.1080/02770900500447052
22. Mayo-Gamble, TL, and Mouton, C. Examining the association between health literacy and medication adherence among older adults. Health Commun. (2018) 33:1124–30. doi: 10.1080/10410236.2017.1331311
23. Smith, SG, Jackson, SE, Kobayashi, LC, and Steptoe, A. Social isolation, health literacy, and mortality risk: findings from the English longitudinal study of ageing. Health Psychol. (2018) 37:160–9. doi: 10.1037/hea0000541
24. Samoil, D, Kim, J, Fox, C, and Papadakos, JK. The importance of health literacy on clinical cancer outcomes: a scoping review. Ann Cancer Epidemiol. (2021) 5:30. doi: 10.21037/ace-20-30
25. Verkissen, MN, Ezendam, NPM, Fransen, MP, Essink-Bot, M-L, Aarts, MJ, Nicolaije, KAH, et al. The role of health literacy in perceived information provision and satisfaction among women with ovarian tumors: a study from the population-based PROFILES registry. Patient Educ Couns. (2014) 95:421–8. doi: 10.1016/j.pec.2014.03.008
26. Fleary, SA, Joseph, P, and Pappagianopoulos, JE. Adolescent health literacy and health behaviors: a systematic review. J Adolesc. (2018) 62:116–27. doi: 10.1016/j.adolescence.2017.11.010
27. Scott, TL, Gazmararian, JA, Williams, MV, and Baker, DW. Health literacy and preventive health care use among Medicare enrollees in a managed care organization. Med Care. (2002) 40:395–404. doi: 10.1097/00005650-200205000-00005
28. Corso, PS, Hammitt, JK, Graham, JD, Dicker, RC, and Goldie, SJ. Assessing preferences for prevention versus treatment using willingness to pay. Med Decis Mak. (2002) 22:S92–S101. doi: 10.1177/027298902237713
29. Diamantopoulos, A, Sarstedt, M, Fuchs, C, Wilczynski, P, and Kaiser, S. Guidelines for choosing between multi-item and single-item scales for construct measurement: a predictive validity perspective. J Acad Mark Sci. (2012) 40:434–49. doi: 10.1007/s11747-011-0300-3
31. Li, Y, Lv, X, Liang, J, Dong, H, and Chen, C. The development and progress of health literacy in China. Front Public Health. (2022) 10:1034907. doi: 10.3389/fpubh.2022.1034907
32. Baker, DW. The meaning and the measure of health literacy. J Gen Intern Med. (2006) 21:878–83. doi: 10.1111/j.1525-1497.2006.00540.x
33. Neill, BO, Gonçalves, D, Ricci-Cabello, I, Ziebland, S, and Valderas, J. An overview of self-administered health literacy instruments. PLoS One. (2014) 9:e109110. doi: 10.1371/journal.pone.0109110
34. Nutbeam, D. Health literacy as a public health goal: a challenge for contemporary health education and communication strategies into the 21st century. Health Promot Int. (2000) 15:259–67. doi: 10.1093/heapro/15.3.259
35. Fraser, SDS, Roderick, PJ, Casey, M, Taal, MW, Yuen, HM, and Nutbeam, D. Prevalence and associations of limited health literacy in chronic kidney disease: a systematic review. Nephrol Dial Transplant. (2013) 28:129–37. doi: 10.1093/ndt/gfs371
36. Pampel, FC, Krueger, PM, and Denney, JT. Socioeconomic disparities in health behaviors. Annu Rev Sociol. (2010) 36:349–70. doi: 10.1146/annurev.soc.012809.102529
37. Baker, DW, Sudano, JJ, Albert, JM, Borawski, EA, and Dor, A. Lack of health insurance and decline in overall health in late middle age. N Engl J Med. (2001) 345:1106–12. doi: 10.1056/NEJMsa002887
38. Darmon, N, and Drewnowski, A. Does social class predict diet quality? Am J Clin Nutr. (2008) 87:1107–17. doi: 10.1093/ajcn/87.5.1107
39. Shandong Provincial Bureau of Statistics. (2023). Shandong Statistical Yearbook—2022. Available at: http://tjj.shandong.gov.cn/tjnj/nj2022/zk/zk/indexch.htm
40. Grossman, M. The demand for health: A theoretical and empirical investigation. New York, NY: Columbia University Press (2017).
41. Halliday, TJ, He, H, Ning, L, and Zhang, H. Health investment over the life-cycle. Macroecon Dyn. (2019) 23:178–215. doi: 10.1017/S1365100516001152
42. Cohen, J. Statistical power analysis for the behavioral sciences. Hillsdale, NJ: Erlbaum (1988).
43. Lenhard, W., and Lenhard, A. (2022). Computation of effect sizes. Available at: https://www.psychometrica.de/effect_size.html.
44. Fishbein, M. The role of theory in HIV prevention. AIDS Care. (2000) 12:273–8. doi: 10.1080/09540120050042918
45. Prochaska, JO, and Velicer, WF. The transtheoretical model of health behavior change. Am J Health Promot. (1997) 12:38–48. doi: 10.4278/0890-1171-12.1.38
Keywords: health literacy, health investment intention, petrochemical industry, health education, occupational health
Citation: Wang D, Wang Y, Ma H and Zhao S (2024) The effect of health literacy on health investment intention: a cross-sectional study among petrochemical employees in China. Front. Public Health. 12:1358269. doi: 10.3389/fpubh.2024.1358269
Edited by:
Teresa Vilaça, University of Minho, PortugalReviewed by:
Satish Chandrasekhar Nair, Tawam Hospital, United Arab EmiratesCopyright © 2024 Wang, Wang, Ma and Zhao. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Shichao Zhao, emhhb3poYW8xOTg4MzIwQDE2My5jb20=; Huifen Ma, bWFodWlmZW4yMUAxMjYuY29t
†These authors have contributed equally to this work and share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.