 Marco A. Zonta1
Marco A. Zonta1 Anne Liljander2Karina B. Roque3Arne Schillert2
Anne Liljander2Karina B. Roque3Arne Schillert2 Marco Kai2*Flávia A. dos Santo1Giulia Pinheiro de Freitas1
Marco Kai2*Flávia A. dos Santo1Giulia Pinheiro de Freitas1 Michel Soane4
Michel Soane4 Markus Cavalar2Gustavo Janaudis1
Markus Cavalar2Gustavo Janaudis1 Marina Tiemi Shio3
Marina Tiemi Shio3- 1Inside Diagnosis, Research and Development S.A., São Paulo, Brazil
- 2Institute of Experimental Immunology, Affiliated to EUROIMMUN Medizinische Labordiagnostika AG, Lübeck, Germany
- 3Post Graduation Program in Health Sciences, Santo Amaro University, São Paulo, Brazil
- 4EUROIMMUN Brasil – EUROInstitute, São Caetano do Sul, Brazil
Introduction: Sexually transmitted infections (STIs) cause considerable morbidity worldwide and, depending on the specific pathogen, may lead to serious complications in the female reproductive tract. Incarcerated women are particularly vulnerable to health problems with a disproportionate high rate of STIs, including infections with human papillomavirus (HPV).
Methods: Here, cervical swab samples collected from 299 women (18 to 64 years) living in one of the women’s prisons of São Paulo, Brazil were submitted for liquid-based cytology to determine the prevalence of precancerous lesions. Furthermore, direct detection of 30 genital HPV genotypes (18 high-risk and 12 low-risk types) and 11 additional STIs (Chlamydia trachomatis, Neisseria gonorrhoeae, Herpes simplex virus 1 and 2, Haemophilus ducreyi, Mycoplasma genitalium and hominis, Treponema pallidum, Trichomonas vaginalis, Ureaplasma parvum and urealyticum) were performed by molecular typing using two PCR-based DNA microarray systems, i.e., EUROArray HPV and EUROArray STI (EUROIMMUN), respectively.
Results: The overall prevalence of cytological abnormalities was 5.8%, including five women with low-grade and five women with high-grade squamous intraepithelial lesions. The overall prevalence of HPV was 62.2, and 87.1% of the HPV-positive women were infected with oncogenic high-risk (HR) HPV types. HPV types 16 (24.1%), 33 and 52 (both 10.4%) were the most frequently detected. The prevalence of the other STIs was 72.8%. Up to four different pathogens were found in the infected women, the most frequent being Ureaplasma parvum (45.3%), Mycoplasma hominis (36.2%) and Trichomonas vaginalis (24.8%).
Conclusion: The high number of HR-HPV infections and other STIs described here highlights the fact that the Brazilian female prison population requires more attention in the country’s health policies. The implementation of screening programs and treatment measures might contribute to a decrease in the incidence of STIs and cervical cancer in this vulnerable population. However, for such measures to be effective, further studies are needed to investigate the best practice to get more women to engage in in-prison prevention programs, e.g., through offering further sexual health education and self-sampling.
1 Introduction
Sexually transmitted infections (STIs) are among the most common acute conditions causing considerable morbidity worldwide. The disease prevalence is particularly high in sexually active women of childbearing age residing in low- and middle-income countries (1), where access to testing and disease management is often limited. Many bacterial STIs such as gonorrhea (Neisseria gonorrhoeae), chlamydia (Chlamydia trachomatis), and syphilis (Treponema pallidum subsp. pallidum), as well as viral infections with, e. g., human papillomavirus (HPV), are often asymptomatic and can therefore go undetected for long time periods. If left untreated, some STIs can lead to serious consequences in the female reproductive tract, including the development of pelvic inflammatory disease (PID), ectopic pregnancy and tubal infertility (2–4). Concurrent infections with sexually transmitted pathogens such as parasitic Trichomonas vaginalis have also been associated with an increased risk of sexual acquisition and subsequent transmission of HIV (5). Furthermore, prenatal infections with Ureaplasma spp., N. gonorrhoeae and C. trachomatis can induce complications such as miscarriage, premature labour, low birth weight and neonatal pneumonia (6–8). Moreover, persistent infections with oncogenic high-risk (HR) human papilloma virus (HPV) types have been associated with the development of precancerous lesions and cervical malignancies, with viral detection in 95% of the cervical cancer cases worldwide, predominantly HR-HPV types 16, 18, and 35 (9, 10). In addition to behavioural co-factors such as parity, smoking and long-term use of oral contraceptives, co-infections with other STIs have also been associated with the progression from cervical HPV infection to cellular abnormalities and invasive cancer (11, 12).
Cervical cancer screening programs are an efficient tool to reduce the number of disease cases, and similarly, HPV vaccination plays a crucial role. Studies have shown that in middle-income countries like Brazil, vaccinating pre-adolescent girls is cost-effective, especially if high vaccination coverage rates can be achieved (13). HPV vaccination was incorporated into the Brazilian Unified Health System in 2014, where it initially was offered to girls from 9 to 11 years of age free of charge. The current recommendation is gender neutral and includes vaccination of children and adolescent between 9 and 14 years old and immunosuppressed people up to 45 years old (14). However, despite this, cervical cancer consistently remains one of the most frequent cancers in Brazilian women, ranking 4th in 2018 (15). The high incidence and mortality could be partly attributable to regional differences in the coverage of preventive screening (16) as well as vaccination (17).
Due to risk behaviors such as substance and alcohol abuse, multiple sex partners, commercial sex work and unprotected sex, incarcerated women represent a particularly vulnerable population for development of gynecological problems (18–20). Higher rates of STIs, HPV infections, precancerous lesions and cervical cancer have been reported among incarcerated women compared to women in the general population (20, 21). Older adult imprisoned women are also at a substantially higher risk of developing cervical cancer (22). Brazil has one of the largest populations of incarcerated women in the world (23). Only between the years 2000 and 2016 the number of imprisoned women increased by over 650% (24). This is much due to harshening penalties for small-scale drug trafficking, a task often performed by women to earn some income for their livelihood and that of their families. Women are often the main or only provider for their children and approximately 60% of the incarcerated women are mothers (25). Although incarcerated individuals should have access to health care services of the same standard as available in the community (26), this is unfortunately not always the case in Brazil (24, 27). Furthermore, official epidemiological data regarding notifiable infectious diseases in prison environments are scarce and most published data is focused on tuberculosis and HIV/AIDS (27). Thus, additional studies addressing the prevalence of other diseases e. g., STIs are warranted. One study demonstrated large differences in the access to cervical screening tests and treatment in female penitentiaries across the state of Mato Grosso do Sul, with only approximately 50% of the women reporting having received a Papanicolaou test (Pap test) during their incarceration (28). Furthermore, the prevalence of HPV infection in the female prison population in the city of São Paulo, Brazil was high, as indicated by a 44% prevalence rate of HR-HPV types (HPV 16, 18, 33 and 39) determined by molecular testing (29). In addition, some studies have reported high rates of STIs in women in Brazilian prisons (19, 30, 31). Characterizing the disease burden, both asymptomatic and symptomatic infections in these high risk populations, living under unhygienic conditions, in often overcrowded prisons and with limited access to basic health care (32), is of great importance. Not only for providing adequate treatment, thus improving the sexual and reproductive health of these vulnerable women, but also from a public health perspective by limiting disease transmission inside and outside the prison.
In this study, the prevalence of precancerous lesions, 30 HPV genotypes and 11 additional STIs was determined in cervical swab samples collected from incarcerated women at one of the women’s prisons in São Paulo, Brazil.
2 Materials and methods
2.1 Study population
This cross-sectional screening was conducted between June 2015 and February 2016 at one of the women’s prisons of the city of São Paulo, Brazil. At the time of the study, the prison health service team consisted of a full-time nurse and a medical doctor visiting the prison once per week. Cytology based screening for cervical cancer has been available (upon request) since 2011 through a women’s health program, initiated by the principal investigator of this study (Dr Zonta). No HPV testing was performed and any additional testing, e.g., for STIs was symptom-based. At the time of the study approximately 2,680 women were living in the correctional facility. Prior to the study, a series of group meetings were held where the women were informed about HPV in general, viral transmission routes and its association with cervical cancer. Newly arriving women were informed in a catch-up meeting held 1 week before the start of the study. All non-pregnant women aged ≥18 years were invited to participate in the screening.
The recruitment and scheduling of the women, the follow-up of collection procedures and organization of the site during the activities was supervised by the principal investigator of this study, while the sample collection was performed and overseen by members of the prison health service team. Written informed consent was obtained from all participants before their inclusion in the study. The women, who accepted to participate were interviewed using a self-administered paper-based questionnaire that included closed-ended questions on sociodemographic factors and sexual behaviour. A member of the research team was available if the women had any inquiries or if they had any difficulties in understanding any of the questions.
The results from the analyses were forwarded to the medical clinic at the prison. If any abnormalities were detected the women were referred to the public hospital for further examinations and treatment if needed.
The study was approved by the Ethics Committee of Santo Amaro University – SP (Plataforma Brasil – CAAE: 61414216.4.0000.0081).
2.2 Sampling procedures, cervical cytology, HPV genotyping and STI screening
Cervical material was collected from ecto- and endocervical regions using a standard cytobrush (Kolplast™ C I Ltda, Brazil). The sample brush was conserved in a liquid-based cytology medium (CellPreserv – Kolplast™ C I Ltda, Brazil). All samples were sent to the cytology laboratory at the Santo Amaro University for processing. Cervical cell suspensions were fixed and processed using a KLP 2000 slide processor (Kolplast™ C I Ltda, Brazil) according to the manufacturer’s instructions. Following Papanicolaou (Pap) staining, the slides were analysed and classified according to the 2001 Bethesda system.
The remaining medium was stored at – 20 °C until molecular analyses. DNA was extracted from 1 mL medium using the QIAamp DNA Mini Kit (QIAGEN, Germany) according to the manufacturer’s instructions.
HPV genotyping was performed using a PCR-based DNA microarray system (EUROArray HPV, EUROIMMUN Medizinische Labordiagnostika AG, Germany). This full HPV genotyping system allows for the simultaneous detection and differentiation of 18 high-risk (HR) types (16, 18, 26, 31, 33, 35, 39, 45, 51, 52, 53, 56, 58, 59, 66, 68, 73 and 82) and 12 low-risk (LR) types (6, 11, 40, 42, 43, 44, 54, 61, 70, 72, 81 and 89).
The STI prevalence was determined using a similar DNA microarray system, EUROArray STI (EUROIMMUN, Germany). The array allows for simultaneous detection of 11 pathogens: Chlamydia trachomatis, Herpes simplex viruses 1 and 2 (HSV-1 and HSV-2), Haemophilus ducreyi, Mycoplasma genitalium, Mycoplasma hominis, Neisseria gonorrhoeae, Treponema pallidum, Trichomonas vaginalis, Ureaplasma parvum and Ureaplasma urealyticum. Both arrays (HPV and STI) were performed and evaluated according to the instructions provided by the manufacturer.
2.3 Statistical analysis
Sociodemographic and variables related to sexual activity and history, which are associated with HPV status (pos / neg) or the infection diversity (1 vs. >1 HPV type) were selected using group least absolute shrinkage and selection operator (LASSO) analyses (33, 34). Selected group variables were subsequently included in multivariate logistic regression models. The significance level for all analyses was set as α = 0.05. Comparisons of the STI prevalences between HPV-positive and negative women were performed using Pearson’s Chi-squared test. All statistical analyses were performed using R, version 4.0.2 (35). For the group LASSO analysis, the R package grpreg version 3.3.0 was used (36).
3 Results
3.1 Characteristics of the participants
In total, 299 incarcerated women agreed to participate in the study and the results are based on data from all women, unless stated otherwise (the number of women answering the individual questions is indicated in brackets). The participants’ ages ranged from 18 to 64 years (mean = 31.8 years). The literacy rate among the 297 responding women was 100%. In total, 79.8% (225 / 282) women reported having a profession. More than half of the women (57.4%, 171 / 298) stated that they were not engaged in a formal relationship (i.e., being single) and most of them (81.9%, 245 / 299) were below the age of 18 at the time of their first sexual intercourse. In total, 57.5% (168 / 292) of the women reported having had between one to five- life-time sexual partners. Moreover, most of the interviewed women reported having been pregnant more than two times (66.2%, 198 / 299). Furthermore, 82.3% (246 / 299) women had children; more than half of them (57.5%, 172 / 299) had one to three children while 24.8% (74 / 299) had four or more children (Table 1).
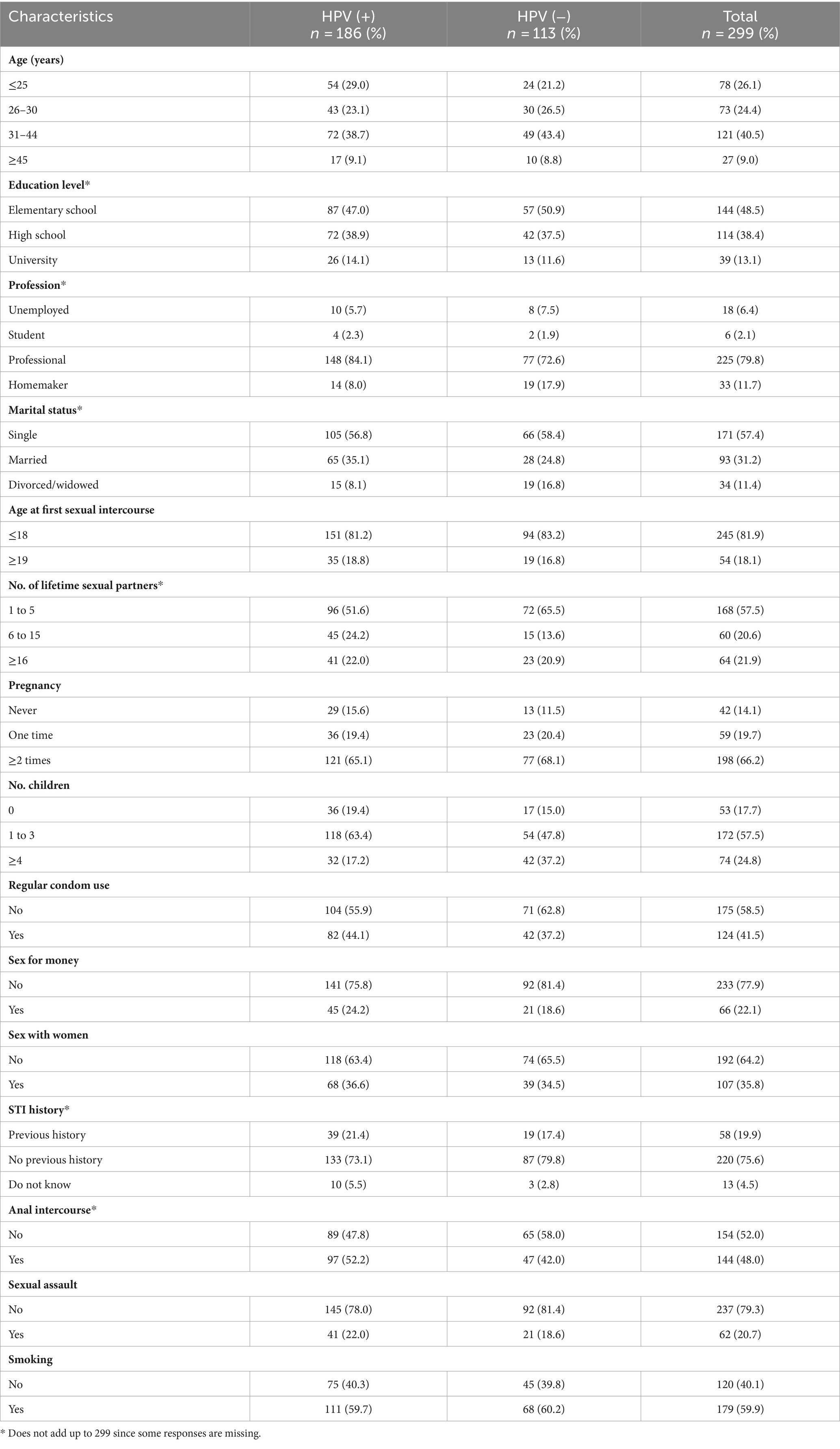
Table 1. Sociodemographic and sexual characteristics of the incarcerated women in São Paulo, Brazil.
Of the interviewed women, 41.5% (124 / 299) reported that they always used condoms when having sex, 22.1% (66 / 299) stated that they have had sex in exchange for money and 35.8% (107 / 299) of the women have had sex with other women. In total, 75.6% (220 / 291) women reported that they have had no previous STIs, 19.9% stated that they have had STIs, while 4.5% did not know their history of infection. Nearly half (48.0%, 144 / 298) of the responding women reported having had anal sex. One out of five women (20.7%, 62 / 299) reported having been sexually assaulted. In total, 59.9% (179 / 299) of the women used tobacco (Table 1). A low percentage of the women consumed alcohol (2.3%) and none of the women were vaccinated against HPV.
3.2 Cytological examination
In the 277 cervical smear samples considered satisfactory for cytopathological examination, the overall prevalence of precancerous lesions was 5.8% (16 / 277), including six samples (2.2%) with atypical squamous cells of undetermined significance (ASC-US), five samples (1.8%) with low-grade squamous intraepithelial lesions (LSIL) and five samples (1.8%) with high-grade squamous intraepithelial lesions (HSIL). The age of the women presenting with precancerous lesions ranged between 20 and 49 years (mean 29.8 years). Of the 261 / 277 samples (94.2%) that were negative for cytological abnormalities, 32 were classified as normal, i.e., showed no reactive alterations in cellular morphology, while the rest (n = 229) were classified as reactive, compatible with cervical inflammation.
3.3 HPV infection prevalence and genotype
Of the investigated women, 62.2% (186 / 299) were positive for any HPV type. The overall prevalence of HR-HPV types, either as single infection or in combination with other HR types or with LR-HPV types, was 54.2% (162/299). Among the women that tested positive for HPV, 53.8% (100 / 186) were infected with two or more HPV types (range 2 to 9 types, Figure 1). In total, 29 different types were detected, with HPV 16 (24.1%), HPV 33 (10.4%), HPV 52 (10.4%), HPV 42 (8.7%) and HPV 18 (8.0%) being the most prevalent types (Figure 2). Seven women were infected with both HPV 16 and 18. Of the 16 women presenting with any precancerous lesion (ASC-US, LSIL or HSIL), 14 had detectable HPV infections. Of these women, 11 were infected with HR-HPV types (71.4%), while all women presenting with LSIL or HSIL were infected with HR-HPV types (Table 2). The prevalence of multiple infections in the latter group was 77.8%. One woman with ASC-US and one woman with HSIL had no detectable HPV infection.
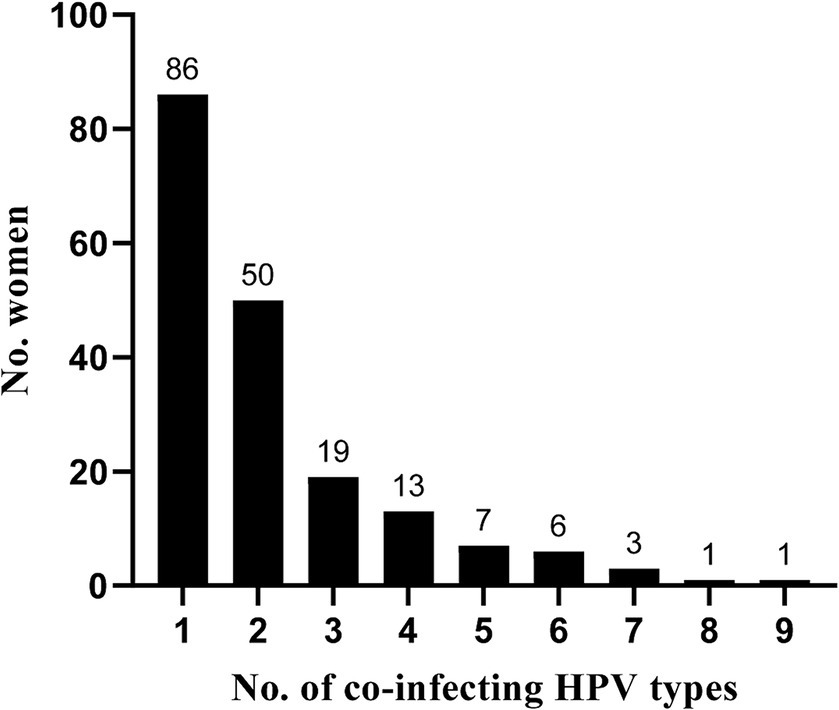
Figure 1. Number of co-infecting HPV types among the incarcerated women in São Paulo, Brazil.
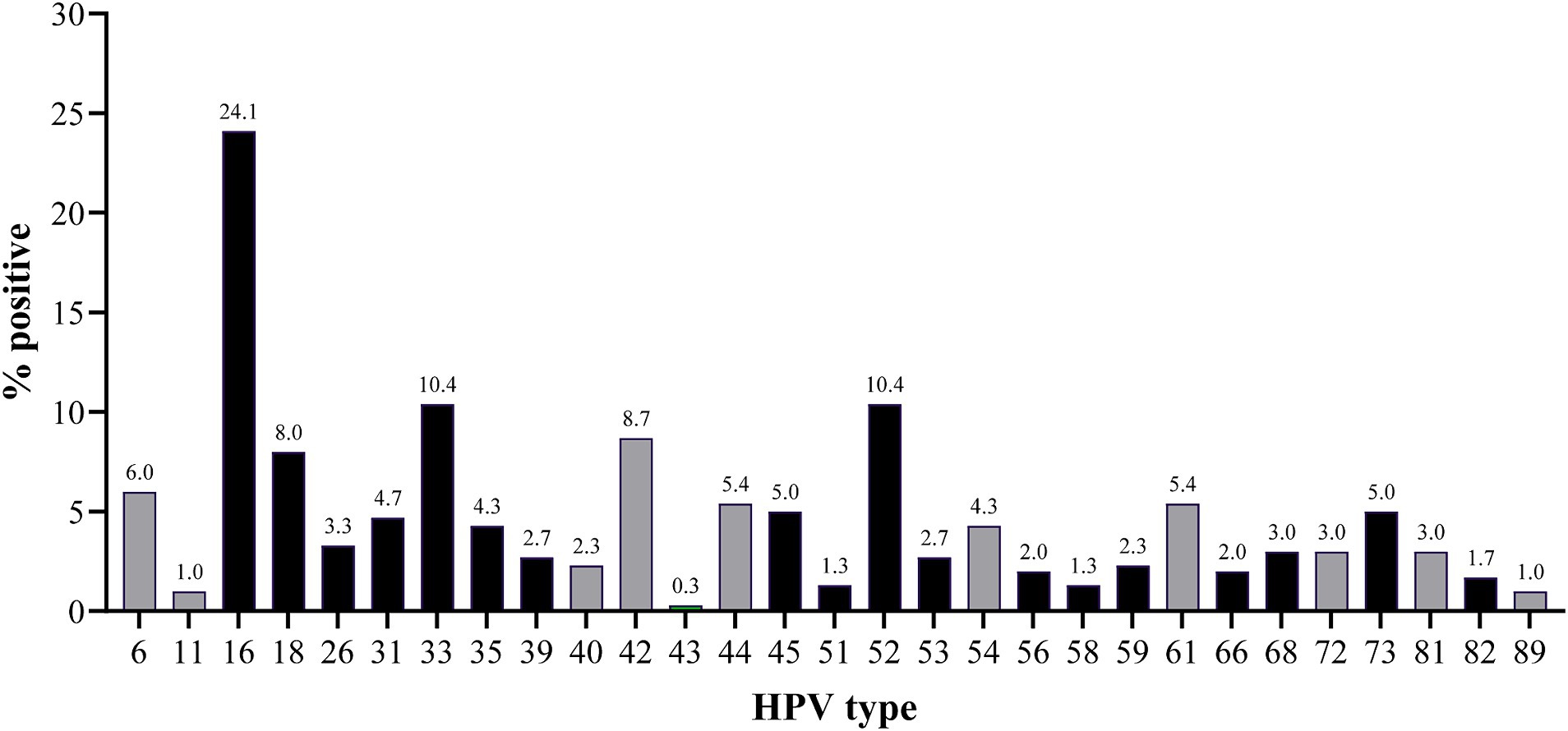
Figure 2. Frequency of the different HPV types in the incarcerated women in São Paulo, Brazil. HR-HPV and LR-HPV types are indicated in black and grey, respectively.
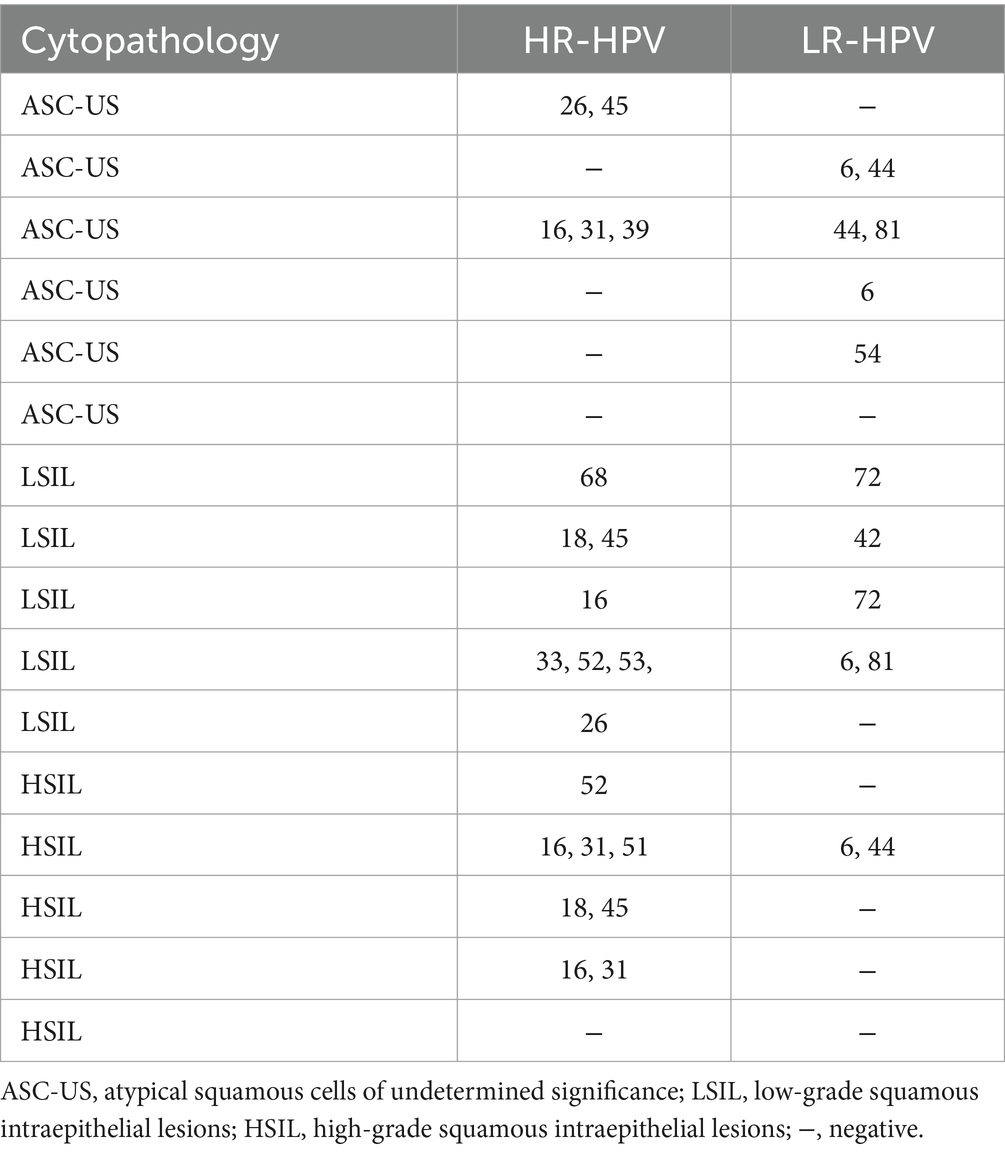
Table 2. Frequency of the different HPV types in the incarcerated women in São Paulo, Brazil.
3.4 Prevalence of sexually transmitted infections
In total 217 / 298 (72.8%) women were positive for one or more STIs. One woman had an invalid result in the testing and was excluded from the analysis. Of the positive women, a comparable percentage was infected with one (51.6%) or at least two infecting microorganisms (48.4%). U. parvum and M. hominis were the most frequently detected infective agents with 45.3% (135/298) and 36.2% (108/298) of the women being infected, respectively. T. vaginalis was identified in 24.8% (74/298) of the women. The prevalence of the other eight STIs was low (0 to 5%) (Figure 3; Supplementary Table S1).
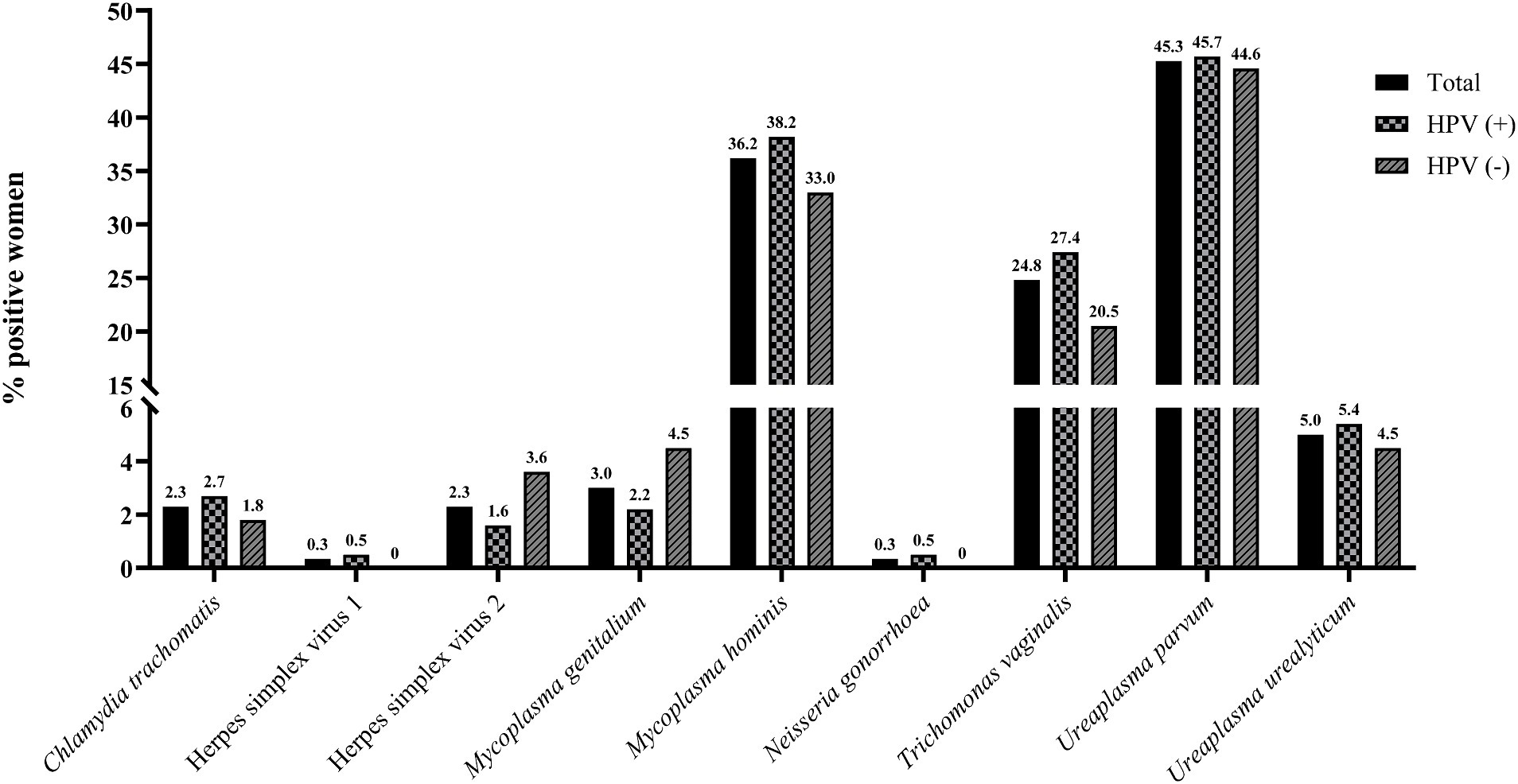
Figure 3. Prevalence of STIs among the imprisoned women. The y-axis has been segmented in order to display all results. STIs for which all women were negative for have been excluded.
3.5 Factors associated with HPV status and cytopathology
Using a group LASSO analysis, six variables were identified as key determinants for the HPV status (pos /neg): profession, number of pregnancies and number of children, current STI status (pos /neg), condom use and sexual assault. However, none of the factors were significantly associated with the HPV status in the multivariate logistic regression model (Table 3). A similar LASSO analysis identified the following determinants of infection diversity (1 vs. > 1 infecting HPV type): age category, profession, marital status, age at first sexual intercourse, number of lifetime sexual partners, condom use and sexual assault. However, similarly to the HPV status, no individual variables were significantly associated with infection diversity (Supplementary Table S2).
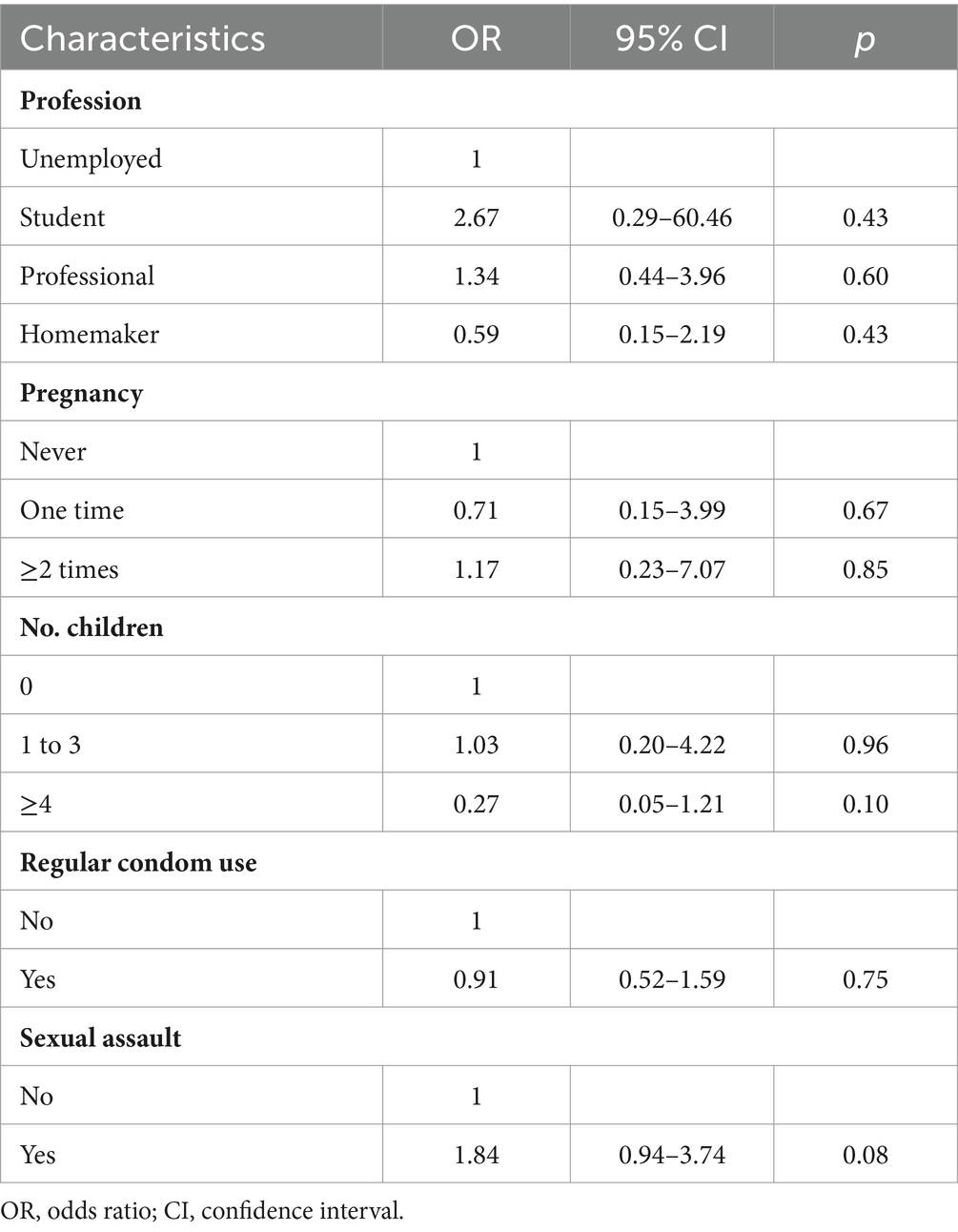
Table 3. Multivariate analysis of factors associated with HPV status among the incarcerated women in São Paulo, Brazil.
Notably, infections with M. hominis were more frequent in HPV-positive than HPV-negative women, 38.2% (71/186) vs. 33.0% (37/112), while infections with HSV-2 were more frequent in HPV-negative women (Figure 3; Supplementary Table S1). Furthermore, T. vaginalis infections were more common in women that were positive for HPV (27.4% [51/186] vs. 20.5% [23/112]) and in women presenting with cervical abnormalities (ASC-US, LSIL and HSIL) compared to the other women (50.0% [8/16] vs. 23.1% [65/282]). However, the differences were not significant (Supplementary Table S1).
4 Discussion
Incarcerated women are a group that is particularly vulnerable to health problems, with a disproportionate high rate of infectious diseases, in particular sexually transmitted infections (STIs) such as HPV (21). This fact may be related to risk factors occurring prior to imprisonment, such as low socioeconomic status and high-risk sexual behaviour, but may also be due to unprotected sexual activities and limited access to healthcare and prevention measures during incarceration. Besides increasing the risk of gynecological conditions such as PID, infertility and cervical cancer (21), untreated STIs might also be transmitted to susceptible partners. Therefore, targeted measures of STI screening and treatment in prisons can help to improve women prisoner’s health and stop the chain of disease transmission. In fact, previous studies have demonstrated that correctional facilities are important sites for STI screening and treatment implementation (37, 38) and in addition to T. pallidum testing for pregnant women (39), routine screening of female detainees for, e.g., C. trachomatis, T. vaginalis and N. gonorrhoeae has been recommended (40, 41). Besides improving the wellbeing of the individual, such measures might have positive impact on the community prevalence of STIs (42). Assessing the prevalence of HPV and other STIs in these high-risk populations is pivotal for such implementation programs. Here, the prevalence of precancerous lesions, HPV and 11 other STIs was investigated in a group of incarcerated women in one of the women’s prisons of the city of São Paulo, Brazil. In this study, 5.8% of the women presented with cytological abnormalities. Furthermore, 62.2% of the women were positive for any HPV type.
The HPV prevalence was higher than that recently reported in a meta-analysis of studies in Brazilian women with and without cytology, which showed an overall prevalence of 25.4% (43). It is also substantially higher than what has been described in studies investigating women in São Paulo (20.2 and 48.6% HPV positive) and women with normal cytology in Brazil (6.7% HPV positive) (44).
Higher HPV prevalence in imprisoned women has been described previously (21). The overall prevalence of HR-HPV types was 54.2%, corresponding to a percentage of 87.1 in HPV-positive women only. These frequencies are substantially higher than those reported for the general female population (17.7%) in Brazil (43). Such high HPV and HR-HPV prevalences have also been described in other risk groups, such as women with HIV (45) and commercial sex workers (46). It should be noted that the HIV status of the women investigated in this study is not known. The high prevalence of HPV, in particular HR-HPV types detected in this study, highlights the importance of offering tailored screening programs in correctional institutions in order to ensure access to testing and, if needed, medical treatment. Furthermore, incarceration could also present a unique opportunity to offer HPV vaccination of eligible women. While the attitudes and barriers to receiving in-prison vaccinations were not investigated here, previous studies have shown a willingness among the female inmates to receive immunizations during incarceration (47, 48).
Extended HPV genotyping is an important tool for risk determination in cervical cancer screening programs as well as verifying the effectiveness of vaccination programs against infection (49–51). Here, a DNA array enabling simultaneous differentiation of 30 HPV types was used. All types but one (HPV 70) were detected, with HPV 16 (24.1%), HPV 33 (10.4%), HPV 52 (10.4%), HPV 42 (8.7%) and HPV 18 (8.0%) being the most frequently detected (Figure 2). Except for HPV 42, all these types are HR-HPV types and are associated with cumulative risks for precancerous lesions by year seven, ranging between >20% for HPV 16 and > 5% for HPV 33 and HPV 52 (50). The HPV types reported here were also the most frequently found types in Brazilian women with and without cytology (52).
Infections with multiple HPV types were detected in 53.8% of the HPV-positive women and in 77.8% of the women presenting with precancerous lesions (LSIL and HSIL). The role of HPV co-infections in the development and progression of such lesions and cervical cancer is unclear. Previous studies have suggested that concurrent infections with multiple HPV types are associated with an increased risk of precancerous lesions (53–55), while other studies have found no increased risk associated with multiple infections (56). The risk of cervical cancer or its precursors is, however, elevated in women with other co-infecting agents such as C. trachomatis, HSV and T. vaginalis (11, 57). Likewise, cervical inflammation has been suggested to be a contributing factor to HSIL (58). Of the women investigated here, 82.7% showed signs of inflammation in their cervical samples. Furthermore, 72.8% were infected with one or more STIs. U. parvum and M. hominis were commonly detected. Both bacteria frequently occur in the female lower genital tract and are associated with HPV infections (59, 60). Here, a higher prevalence was also found in HPV-positive women. The difference between HPV-positive and -negative women was, however, not significant.
Similarly, to what has previously been reported (57), the prevalence of T. vaginalis was higher in HPV-positive women (27.4% vs. 20.5%), in particular in women displaying cervical abnormalities (50.0% vs. 23.1%). However, in contrast to what was reported previously (59, 61), infections with HSV-2 and M. genitalium were more frequent in HPV-negative women (Figure 3; Supplementary Table S1). The difference between HPV-positive and -negative women was, however, not significant. Furthermore, although many women with risk profiles, i.e., many sexual partners (in total 42.5% had more than 6 lifetime partners), low age at first sex (81.9%), numerous pregnancies and several children, were included, no significant associations were found between the HPV status and the sociodemographic factors identified as key determinants in the group LASSO analysis (Table 3).
4.1 Study limitation
Sample size was considered a limitation of this study. The authors can only speculate regarding the reasons why so few women were willing to participate. However, intimate gynecological examinations have the potential for causing embarrassment, anxiety, and discomfort, making women reluctant. For future studies, vaginal self-sampling should be offered to overcome the emotional and practical barriers to potentially increase the participation in cervical screening. The authors therefore acknowledge that the results presented here represent a small group of the sexually active incarcerated women in Brazil. Furthermore, the questionnaire used in this study exhibited limitations in its level of detail, which hindered the identification of statistically significant factors associated with HPV status. In addition, although symptomatic and asymptomatic viral shedding is common for both HSV-1 and HSV-2, the prevalence of these infections is likely to have been underestimated when only applying direct detection and not serology.
5 Conclusion
There has been a sharp increase in the incarceration rate of females in Brazil between 2000 and 2016, mainly driven by a harshening in the sentencing for minor drug-trafficking offences. Since women in prison are more likely to engage in risk behaviors such as having multiple sex partners, commercial sex work and unprotected sex, they are particularly susceptible to gynecological problems. Furthermore, over-crowding and a lack of basic healthcare contributes to their already precarious situation. Imprisonment presents a distinct opportunity to offer preventive services that these at-risk women might otherwise lack access to. Health measures that could be of particular importance to incarcerated women include cervical cancer screening and infectious disease testing and immunization (STIs). The data generated here demonstrates that the burden of infectious diseases, i.e., HPV and other STIs is high among incarcerated women in São Paulo, Brazil. Moreover, not only are these infections often asymptomatic, but also transmissible, further highlighting the important public health role that a prison could serve in the detection and management of these diseases. Given the right support, prisons could potentially also provide HPV vaccinations to eligible women, thus further reducing the morbidity and mortality from cervical and other HPV-related cancers. However, for such measures to be effective, further studies are needed to investigate the best practice to get more women to engage in in-prison prevention programs, e.g., through offering further sexual health education and self-sampling.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Ethics Committee of Santo Amaro University – SP (Plataforma Brasil – CAAE: 61414216.4.0000.0081). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
MZ: Conceptualization, Formal analysis, Investigation, Supervision, Writing – original draft, Writing – review & editing. AL: Data curation, Formal analysis, Visualization, Writing – original draft, Writing – review & editing. KR: Formal analysis, Writing – review & editing. AS: Data curation, Formal analysis, Writing – review & editing. MK: Formal analysis, Writing – original draft, Writing – review & editing. FS: Data curation, Writing – review & editing. GF: Data curation, Resources, Writing – review & editing. MiS: Data curation, Writing – review & editing. MC: Resources, Writing – review & editing. GJ: Resources, Writing – review & editing. MaS: Data curation, Investigation, Visualization, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. A Scientific Initiation scholarship was offered by the CNPq program to KR.
Acknowledgments
We are grateful to Sandra Saschenbrecker and Sandy Marckstadt for reviewing the manuscript.
Conflict of interest
AL, AS, MiS, MK, and MC are employees of EUROIMMUN.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2024.1353845/full#supplementary-material
References
1. Rowley, J, Vander Hoorn, S, Korenromp, E, Low, N, Unemo, M, Abu-Raddad, LJ, et al. Chlamydia, gonorrhoea, trichomoniasis and syphilis: global prevalence and incidence estimates, 2016. Bull World Health Organ. (2019) 97:548–562P. doi: 10.2471/BLT.18.228486
2. Lobão, TN, Campos, GB, Selis, NN, Amorim, AT, Souza, SG, Mafra, SS, et al. Ureaplasma urealyticum and U. parvum in sexually active women attending public health clinics in Brazil. Epidemiol Infect. (2017) 145:2341–51. doi: 10.1017/S0950268817001145
3. Saridogan, E. Role of general gynaecologists in the prevention of infertility. Best Pract Res Clin Obstet Gynaecol. (2019) 59:132–6. doi: 10.1016/j.bpobgyn.2019.01.014
4. Zacharis, K, Messini, CI, Anifandis, G, Koukoulis, G, Satra, M, and Daponte, A. Human papilloma virus (HPV) and fertilization: a mini review. Medicina (Kaunas). (2018) 54:50. doi: 10.3390/medicina54040050
5. Ward, H, and Ronn, M. Contribution of sexually transmitted infections to the sexual transmission of HIV. Curr Opin HIV AIDS. (2010) 5:305–10. doi: 10.1097/COH.0b013e32833a8844
6. Horne, AW, Wheelhouse, N, Horner, PJ, and Duncan, WC. Association of Past Chlamydia trachomatis infection with miscarriage. JAMA Netw Open. (2020) 3:e2018799. doi: 10.1001/jamanetworkopen.2020.18799
7. Sprong, KE, Mabenge, M, Wright, CA, and Govender, S. Ureaplasma species and preterm birth: current perspectives. Crit Rev Microbiol. (2020) 46:169–81. doi: 10.1080/1040841X.2020.1736986
8. Vallely, LM, Egli-Gany, D, Wand, H, Pomat, WS, Homer, CSE, Guy, R, et al. Adverse pregnancy and neonatal outcomes associated with Neisseria gonorrhoeae: systematic review and meta-analysis. Sex Transm Infect. (2021) 97:104–11. doi: 10.1136/sextrans-2020-054653
9. Bosch, FX, Lorincz, A, Munoz, N, Meijer, CJLM, and Shah, KV. The causal relation between human papillomavirus and cervical cancer. J Clin Pathol. (2002) 55:244–65. doi: 10.1136/jcp.55.4.244
10. El-Zein, M, Richardson, L, and Franco, EL. Cervical cancer screening of HPV vaccinated populations: cytology, molecular testing, both or none. J Clin Virol. (2016) 76:S62–8. doi: 10.1016/j.jcv.2015.11.020
11. Almonte, M, Albero, G, Molano, M, Carcamo, C, García, PJ, and Pérez, G. Risk factors for human papillomavirus exposure and co-factors for cervical cancer in Latin America and the Caribbean. Vaccine. (2008) 26:L16–36. doi: 10.1016/j.vaccine.2008.06.008
12. Castellsague, X, Bosch, FX, and Munoz, N. Environmental co-factors in HPV carcinogenesis. Virus Res. (2002) 89:191–9. doi: 10.1016/S0168-1702(02)00188-0
13. Vanni, T, Mendes Luz, P, Foss, A, Mesa-Frias, M, and Legood, R. Economic modelling assessment of the HPV quadrivalent vaccine in Brazil: a dynamic individual-based approach. Vaccine. (2012). 30:4866–4871. doi: 10.1016/j.vaccine.2012.04.087
14. Filho, DST, Rocha, CMR, Bacha, E, Andrade, ANM, Pereira, DDP, Nunes, LM, et al. Current HPV Vaccination strategies in Brazil. Health. (2023). 15:107–121. doi: 10.4236/health.2023.152009
15. (IARC) IAfRoC. (2022) Brazil- global Cancer observatory 1–2. Available at: https://gco.iarc.who.int/media/globocan/factsheets/populations/76-brazil-fact-sheet.pdf
16. Costa, RFA, Longatto-Filho, A, de Lima Vazquez, F, Pinheiro, C, Zeferino, LC, and Fregnani, JHTG. Trend analysis of the quality indicators for the Brazilian cervical cancer screening programme by region and state from 2006 to 2013. BMC Cancer. (2018) 18:126. doi: 10.1186/s12885-018-4047-9
17. Mendes Lobão, W, Duarte, FG, Burns, JD, de Souza Teles Santos, CA, Chagas de Almeida, MC, Reingold, A, et al. Low coverage of HPV vaccination in the national immunization programme in Brazil: parental vaccine refusal or barriers in health-service based vaccine delivery? PLoS One. (2018) 13:e0206726. doi: 10.1371/journal.pone.0206726
18. Caviness, CM, Anderson, BJ, and Stein, MD. Prevalence and predictors of sexually transmitted infections in hazardously-drinking incarcerated women. Women Health. (2012) 52:119–34. doi: 10.1080/03630242.2011.649396
19. Ferreira de Sá Queiroz, JH, Pompilio, MA, Esther da Silva, K, Coimbra Motta de Castro, AR, Omizolo de Souza, R, Correa, ME, et al. High prevalence of Treponema pallidum infection in Brazilian prisoners. Am J Trop Med Hyg. (2017) 97:1078–84. doi: 10.4269/ajtmh.17-0098
20. van den Bergh, B. Women’s health and the prison setting WHO/Europe, Prisons and Health, 2014 (2014).
21. Escobar, N, and Plugge, E. Prevalence of human papillomavirus infection, cervical intraepithelial neoplasia and cervical cancer in imprisoned women worldwide: a systematic review and meta-analysis. J Epidemiol Community Health. (2020) 74:95–102. doi: 10.1136/jech-2019-212557
22. Binswanger, IA, Krueger, PM, and Steiner, JF. Prevalence of chronic medical conditions among jail and prison inmates in the USA compared with the general population. J Epidemiol Community Health. (2009) 63:912–9. doi: 10.1136/jech.2009.090662
23. Roy, W. (2017) World female imprisonment list fourth edition women and girls in penal institutions, including pre-trial detainees/remand prisoners world prison brief. Available at: https://www.prisonstudies.org/news/world-female-imprisonment-list-fourth-edition
24. de Araújo, PF, Kerr, L, Kendall, C, Rutherford, GW, Seal, DW, da Justa Pires Neto, R, et al. Behind bars: the burden of being a woman in Brazilian prisons. BMC Int Health Hum Rights. (2020) 20:28. doi: 10.1186/s12914-020-00247-7
25. Silva, MVM. (2019) Relatorio Tematico Sobre Mulheres Privadas De Liberdade – Junho de 2017. Available at: https://www.gov.br/senappen/pt-br/assuntos/noticias/depen-divulga-infopen-mulheres-de-junho-de-2017
26. UN General Assembly. United Nations standard minimum rules for the treatment of prisoners (the Nelson Mandela rules): resolution / adopted by the general Assembly UN General Assembly (2016).
27. Job Neto, F, Miranda, RB, Coelho, RA, Gonçalves, CP, Zandonade, E, and Miranda, AE. Health morbidity in Brazilian prisons: a time trends study from national databases. BMJ Open. (2019) 9:e026853. doi: 10.1136/bmjopen-2018-026853
28. da Silva, ERP, de Souza, AS, de Souza, TGB, Tsuha, DH, and Barbieri, AR. Screening for cervical cancer in imprisoned women in Brazil. PLoS One. (2017) 12:e0187873. doi: 10.1371/journal.pone.0187873
29. Zonta, M, Monteiro, J, Santos, G Jr, Paruci, P, Hyppolyto, P, and Pignatari, AC. Lesões cervicais e infecção pelo papilomavírus humano no sistema prisional da cidade de São Paulo, Brasil cervical lesions and human papillomavirus infection in women at a prisional system in São Paulo city, Brazil. Rev Bras Anal Clin. (2011) 43:301–5.
30. Batista, M, Paulino, MR, Castro, KS, Gueiros, LAM, Leão, JC, and Carvalho, AAT. High prevalence of syphilis in a female prison unit in northeastern Brazil. Einstein (São Paulo). (2020) 18:eAO4978. doi: 10.31744/einstein_journal/2020AO4978
31. Miranda, AE, Vargas, PM, St Louis, ME, and Viana, MC. Sexually transmitted diseases among female prisoners in Brazil: prevalence and risk factors. Sex Transm Dis. (2000) 27:491–5. doi: 10.1097/00007435-200010000-00001
32. Soares, MMF, and Bueno, PM. Demography, vulnerabilities and right to health to Brazilian prison population. Ciênc Saúde Colet. (2016) 21:1999–2010. doi: 10.1590/1413-81232015217.24102015
33. Tibshirani, R. Regression shrinkage and selection via the Lasso. J R Stat Soc. (1996) 58:267–88. doi: 10.1111/j.2517-6161.1996.tb02080.x
34. Yuan, M. Model selection and estimation in regression with grouped variables. J R Stat Soc Series B Stat Methodol. (2006) 68:49–67. doi: 10.1111/j.1467-9868.2005.00532.x
35. R CT. A language and environment for statistical computing. Vienna, Austria: R Foundation for Statistical Computing (2020) Available at: https://www.R-project.org/.
36. Breheny, P, and Huang, J. Group descent algorithms for nonconvex penalized linear and logistic regression models with grouped predictors. Stat Comput. (2015) 25:173–87. doi: 10.1007/s11222-013-9424-2
37. Varan, AK, Mercer, DW, Stein, MS, and Spaulding, AC. Hepatitis C Seroprevalence among prison inmates since 2001: still high but declining. Public Health Re. (2014). 129:187–195. doi: 10.1177/003335491412900213
38. Seligson, AL, Parvez, FM, Lim, S, Singh, T, Mavinkurve, M, Harris, TG, et al. Public health and vulnerable population: morbidity and mortality among people ever incarcerated in New York City jails, 2001 to 2005. J. Correct. Health Care. (2017). 23:421–436. doi: 10.1177/1078345817727527
39. Biswas, HH, Chew, NG RA, Murray, EL, Chow, JM, Stoltey, JE, Watt, JP, et al. Characteristics associated with delivery of an infant with congenital Syphilis and missed opportunities for prevention-California, 2012 to 2014. Sex. Transm. Dis. (2018). 45:435–441. doi: 10.1097/OLQ.0000000000000782
40. Javanbakht, M, Stirland, A, Stahlman, S, Smith, LV, Chien, M, Torres, R, et al. Prevalence and factors associated with Trichomonas vaginalis infection among high-risk women in Los Angeles. Sex. Transm. Dis. 40:804–807. doi: 10.1097/OLQ.0000000000000026
41. Oshin, E, Eissa, MA, Benjamins, LJ, Baratt, MS, and Beyda, RM. Trichomonas vaginalis infections among youth in detention in the southeastern United States. J. Pediatr. Adolesc. Gynecol. (2022). 35:368–370. doi: 10.1016/j.jpag.2021.09.006
42. Nijhawan, AE. Infectious diseases and the criminal justice system: a public health perspective. Am. J. Med. Sci. (2016). 352:399–407. doi: 10.1016/j.amjms.2016.05.020
43. Colpani, V, Soares Falcetta, F, Bacelo Bidinotto, A, Kops, NL, Falavigna, M, Serpa Hammes, L, et al. Prevalence of human papillomavirus (HPV) in Brazil: a systematic review and meta-analysis. PLoS One. (2020) 15:e0229154. doi: 10.1371/journal.pone.0229154
44. da Silva, MC, Martins, HP, de Souza, JL, Tognim, MCB, Svidzinski, TIE, Teixeira, JJV, et al. Prevalence of HPV infection and genotypes in women with normal cervical cytology in the state of Parana, Brazil. Arch Gynecol Obstet. (2012) 286:1015–22. doi: 10.1007/s00404-012-2399-y
45. Correa, CM, Teixeira, NC, Araujo, AC, Carvalho Nde, O, Castillo, DM, Campos, RR, et al. Prevalence and multiplicity of HPV in HIV women in Minas Gerais. Rev Assoc Med Bras (1992). (2011) 57:425–30. doi: 10.1590/S0104-42302011000400017
46. Farahmand, M, Moghoofei, M, Dorost, A, Abbasi, S, Monavari, SH, Kiani, SJ, et al. Prevalence and genotype distribution of genital human papillomavirus infection in female sex workers in the world: a systematic review and meta-analysis. BMC Public Health. (2020) 20:1455. doi: 10.1186/s12889-020-09570-z
47. Moore, A, Cox-Martin, M, Dempsey, AF, Berenbaum Szanton, K, and Binswanger, IA. HPV vaccination in correctional care: knowledge, attitudes, and barriers among incarcerated women. J. Correct. Health Care.(2019). 25:219–230. doi: 10.1177/1078345819853286
48. Emerson, A, Allison, M, Saldana, L, Kelly, PJ, and Ramaswamy, M. Collaborating to offer HPV vaccinations in jails: results from a pre-implementation study in four states. BMC Health Serv. Res. (2021). 21:309. doi: 10.1186/s12913-021-06315-5
49. Bonde, JH, Sandri, MT, Gary, DS, and Andrews, JC. Clinical utility of human papillomavirus genotyping in cervical Cancer screening: a systematic review. J Low Genit Tract Dis. (2020) 24:1–13. doi: 10.1097/LGT.0000000000000494
50. Demarco, M, Hyun, N, Carter-Pokras, O, Raine-Bennett, TR, Cheung, L, Chen, X, et al. A study of type-specific HPV natural history and implications for contemporary cervical cancer screening programs. EClinicalMedicine. (2020) 22:100293. doi: 10.1016/j.eclinm.2020.100293
51. Loenenbach, A, Schönfeld, V, Takla, A, Wiese-Posselt, M, Marquis, A, Thies, S, et al. Human papillomavirus prevalence and vaccine effectiveness in young women in Germany, 2017/2018: results from a nationwide study. Front Public Health. (2023) 11:1204101. doi: 10.3389/fpubh.2023.1204101
52. Martins, TR, Mendes de Oliveira, C, Rosa, LR, de Campos Centrone, C, Rodrigues, CLR, Villa, LL, et al. HPV genotype distribution in Brazilian women with and without cervical lesions: correlation to cytological data. Virol J. (2016) 13:138. doi: 10.1186/s12985-016-0594-3
53. Chaturvedi, AK, Katki, HA, Hildesheim, A, Rodríguez, AC, Quint, W, Schiffman, M, et al. Human papillomavirus infection with multiple types: pattern of coinfection and risk of cervical disease. J Infect Dis. (2011) 203:910–20. doi: 10.1093/infdis/jiq139
54. de Brot, L, Pellegrini, B, Moretti, ST, Carraro, DM, Soares, FA, Rocha, RM, et al. Infections with multiple high-risk HPV types are associated with high-grade and persistent low-grade intraepithelial lesions of the cervix. Cancer Cytopathol. (2017) 125:138–43. doi: 10.1002/cncy.21789
55. Schmitt, M, Depuydt, C, Benoy, I, Bogers, J, Antoine, J, Arbyn, M, et al. Multiple human papillomavirus infections with high viral loads are associated with cervical lesions but do not differentiate grades of cervical abnormalities. J Clin Microbiol. (2013) 51:1458–64. doi: 10.1128/JCM.00087-13
56. Muñoz, N, Bosch, FX, de Sanjosé, S, Herrero, R, Castellsagué, X, Shah, KV, et al. Epidemiologic classification of human papillomavirus types associated with cervical cancer. N Engl J Med. (2003) 348:518–27. doi: 10.1056/NEJMoa021641
57. Belfort, IKP, Cunha, APA, Mendes, FPB, Galvão-Moreira, LV, Lemos, RG, de Lima Costa, LH, et al. Trichomonas vaginalis as a risk factor for human papillomavirus: a study with women undergoing cervical cancer screening in a northeast region of Brazil. BMC Womens Health. (2021) 21:174. doi: 10.1186/s12905-021-01320-6
58. Castle, PE, Hillier, SL, Rabe, LK, Hildesheim, A, Herrero, R, Bratti, MC, et al. An association of cervical inflammation with high-grade cervical neoplasia in women infected with oncogenic human papillomavirus (HPV). Cancer Epidemiol Biomarkers Prev. (2001) 10:1021–7.
59. Klein, C, Samwel, K, Kahesa, C, Mwaiselage, J, West, JT, Wood, C, et al. Mycoplasma co-infection is associated with cervical Cancer risk. Cancers (Basel). (2020) 12:1093. doi: 10.3390/cancers12051093
60. Liu, J, Liu, W, Liu, Y, Zhou, X, Zhang, Z, and Sun, Z. Prevalence of microorganisms co-infections in human papillomaviruses infected women in northern China. Arch Gynecol Obstet. (2016) 293:595–602. doi: 10.1007/s00404-015-3826-7
61. Bahena-Román, M, Sánchez-Alemán, MA, Contreras-Ochoa, CO, Lagunas-Martínez, A, Olamendi-Portugal, M, López-Estrada, G, et al. Prevalence of active infection by herpes simplex virus type 2 in patients with high-risk human papillomavirus infection: a cross-sectional study. J Med Virol. (2020) 92:1246–52. doi: 10.1002/jmv.25668
Keywords: sexually transmitted infections, HPV, epidemiology, women’s health, prison, Brazil
Citation: Zonta MA, Liljander A, Roque KB, Schillert A, Kai M, dos Santo FA, de Freitas GP, Soane M, Cavalar M, Janaudis G and Shio MT (2024) Prevalence of sexually transmitted infections and human papillomavirus in cervical samples from incarcerated women in São Paulo, Brazil: a retrospective single-center study. Front. Public Health. 12:1353845. doi: 10.3389/fpubh.2024.1353845
Edited by:
Adwoa Asante-Poku, University of Ghana, GhanaReviewed by:
Usman Ayub Awan, Vanderbilt University Medical Center, United StatesLuiz Fernando Almeida Machado, Federal University of Pará, Brazil
Copyright © 2024 Zonta, Liljander, Roque, Schillert, Kai, dos Santo, de Freitas, Soane, Cavalar, Janaudis and Shio. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Marco Kai, bS5rYWlAZXVyb2ltbXVuLmRl