 Łukasz Rypicz
Łukasz Rypicz Izabela Witczak1
Izabela Witczak1 Mária Šupínová
Mária Šupínová- 1Department of Population Health, Division of Public Health, Faculty of Health Sciences, Medical University, Wroclaw, Poland
- 2Faculty of Health Sciences, Catholic University in Ružomberok, Ružomberok, Slovakia
- 3Department of Biomedical, Industrial, and Human Factors Engineering, Wright State University, Dayton, OH, United States
- 4Department of Nursing, Faculty of Health Studies, Jan Evangelista Purkyne University in Ústí nad Labem, Ústí nad Labem, Czechia
Background: Alarms are crucial in informing Healthcare Workers (HCWs) about critical patient needs, but unmanaged frequency and noise of alarms can de-sensitize medical staff and compromise patient safety. Alarm fatigue is identified as the major cause of the clinical alarm management problem. It occurs when the medical staff is overwhelmed by the number of clinical alarms.
Methods: The survey was conducted online using Google’s form-making tools from June to July 2023. There were three parts to the survey used in the study: a socio-demographic metric, the Alarm Fatigue Assessment Questionnaire (AFAQ), and The Pittsburgh Sleep Quality Index (PSQI). A significance level of 0.05 was used in the analysis.
Results: The survey included 756 medical professionals from three European countries (Slovakia, the Czech Republic and Poland). The participants in the study were 42 years old on average, and they had 12 years of work experience. 603 out of 756 survey participants had poor sleep quality, 147 had good sleep quality, and 6 did not provide an answer. This study analyzed the alarm fatigue levels of respondents in every country. In the Czech Republic, Poland and Slovakia, a statistically significant association (p = 0.039, p = 0.001, p < 0.001) was found between alarm fatigue and sleep quality in medical staff.
Conclusion: Based on our study, alarm fatigue and sleep quality of HCWs are correlated. Therefore, alarm fatigue and sleep hygiene should be monitored.
Highlights
• Medical device alarms are a major problem for medical personnel, leading to fatigue.
• Medical personnel’s well-being can be negatively impacted by alarm fatigue.
• The lack of measuring tools makes it hard to monitor alarm fatigue.
Introduction
Alarms are crucial for letting Healthcare Workers (HCWs) know about critical patient needs, but if alarms are not managed properly, the frequency and noise can de-sensitize medical staff and compromise patient safety (1). Alarm fatigue is a significant issue in healthcare that can be caused by improper alarm management (2, 3). Alarm fatigue is a result of staff being overwhelmed by the number of clinical alarms (2, 4, 5). Alarm fatigue is a safety issue for patients because it can cause alarm desensitization, which can result in delayed or no response from HCWs (4–6). This has led to the Emergency Care Research Institute (ECRI) recognizing alarm fatigue as a significant health technology risk for several years (7).
Determining the number of adverse events caused by alarm fatigue is a challenge, and it is expected that the number is underestimated (8). The reason is that studies report alarm fatigue qualitatively in various ways, including noise level and sensory overload (9–11). Mismanagement and disregarding alarms have resulted in significant deaths, even with current undercounted data. The FDA discovered that alarm mismanagement caused 566 deaths in the US from 2005 to 2010 (4, 12).
Moreover, alarm fatigue has a negative impact on HCWs’ well-being and performance (13, 14).
While providing care, HCWs utilize a variety of medical equipment (15). As a result, they are exposed to multiple alarms, which puts them at risk of alarm fatigue (14). Alarm fatigue increases the risk of burnout, which can lead to mental health issues, such as anxiety and depression (16, 17).
Also, if healthcare workers are exposed to alarms excessively, they may experience hearing irritation, sleep disturbances, and headaches (18). Sleep disturbances are a public health challenge given the importance of sleep for the human body (19). The human body can recover from a day of work during sleep. It is essential to study the quality of sleep and the mechanisms for improving it (20). Due to the high mental workload at work and shift work, HCWs frequently experience sleep problems.
This study aims to demonstrate whether there is a relationship between alarm fatigue and the sleep quality of medical staff. The survey study was conducted in Poland, Slovakia, and the Czech Republic, three countries. These countries were selected based on their cultural and work organization similarities, as well as their geographical proximity.
Methods
Study design
After obtaining the Bioethics Committee’s approval, the survey was conducted in three European countries: Poland, Slovakia, and the Czech Republic from June to July 2023. The survey was conducted online using Google’s form-making tools. Each country that participated was given a survey translated into their language. A designated person in each country distributed survey links to practicing medical staff through professional groups such as social media, medical associations, and scientific societies.
After collecting the data, a database was created and analyzed.
This study is exploratory and examines a chosen sample that is not representative of the entire medical staff population. Although it was desirable, the lack of time and resources prevented us from inviting more participants.
The study is intended to focus on medics such as nurses, midwives, doctors, and paramedics who work in departments where medical devices that are alarming are present. These departments are anesthesiology, intensive care unit, cardiac intensive care unit, and recovery room. There were 756 participants in the study, with 455 from Slovakia, 184 from the Czech Republic, and 117 from Poland.
Research tools
In the study, the survey questionnaire had three parts:
a. A socio-demographic metric;
b. The Alarm Fatigue Assessment Questionnaire (AFAQ) (21);
c. The Pittsburgh Sleep Quality Index (PSQI) (22).
The Alarm Fatigue Assessment Questionnaire (AFAQ) is used to assess alarm fatigue among respondents. The questionnaire score can be anywhere from 20 to 100 points, and a higher number indicates more alarm fatigue. The AFAQ lacks standardized criteria to determine which scores are indicative of high or low alarm fatigue. However, it’s possible to calculate the average score for each question and interpret it. In this study we used the following criteria: 1 means that the feeling of fatigue never occurs, 2 means that it rarely occurs, 3 means that it sometimes occurs, 4 means that it often occurs and 5 means that it always occurs. The AFAQ questionnaire is developed based on Torabizadeh et al. study in Polish language (23).
Following that, the tool was translated into Czech and Slovak. To evaluate the tool’s internal consistency, a Cronbach’s alpha coefficient was calculated. The questionnaire in the Czech version had a Cronbach alpha coefficient of 0.822, and the Slovak version had a Cronbach alpha coefficient of 0.795. A Cronbach’s alpha above 0.7 to 0.8 is acceptable, while 0.8 to 0.9 is good.
The PSQI questionnaire is employed to assess the quality of sleep of participants. Higher scores indicate a lower quality of sleep. In accordance with the key for this scale, the PSQI scores were analyzed, with 0–5 points being indicative of good sleep quality and 6–21 points being indicative of poor sleep quality. In this study we used Polish (24), Czech (25) and Slovak (26) versions of the PSQI.
Statistical analyses
The distributions of quantitative variables were summarized by using means, standard deviations, medians, and quartiles. Furthermore, the percentage of occurrence was utilized to summarize the distributions of qualitative variables. The chi-squared test was used to compare qualitative variables between groups, with Yates’ correction applied for 2×2 tables. Fisher’s exact test was used to analyze small sample sizes in contingency tables. Quantitative variables between two groups were compared using the Mann–Whitney and Kruskal-Wallis tests for multiple groups. Moreover, the correlation between two quantitative variables was assessed using Spearman’s coefficient of correlation. The significance level for all statistical tests was set to 0.05. The R 4.3.1 program was used for analysis (27).
Ethics
The study was executed according to the principles of the Declaration of Helsinki and the guidelines of Good Clinical Practice (28). At the top of the survey, there was a section where written consent and study information was provided. The participant identities were not linked to the collected data, and they were free to terminate their participation at any time. The independent Bioethics Committee of Wroclaw Medical University approved the research project (KB 156/2023).
Results
Females made up the majority of the study participants (94.05% female, 5.95% male). The majority of respondents were nurses (90.21%, p = 0.001) and had a mean age of 42 years, with approximately 12 years of work experience. In all three countries, the demographics of the respondents were the same. When taking the survey, the majority of those surveyed, which is 60.32% (p < 0.001), were already in a relationship. Nearly all the respondents had equivalent levels of education, with approximately 30% possessing a secondary education that includes a bachelor’s and a master’s degree. Polish participants had the lowest percentage of HCWs with secondary education (p < 0.001) compared to Czech and Slovakia. The reason for this is that nurses have not been educated at the secondary level for several decades. Currently, nursing education is offered at the bachelor’s and master’s levels. A total of 72.75 percent (72.75%, p = 0.001) work 12-h shifts and have a monthly workload of 160–240 h. The workload is consistent across all countries (p = 0.001). Our study shows that 46.15% of Polish healthcare workers work in two locations, which is the highest percentage among survived countries. Table 1 exhibits detailed socio-demographic information.
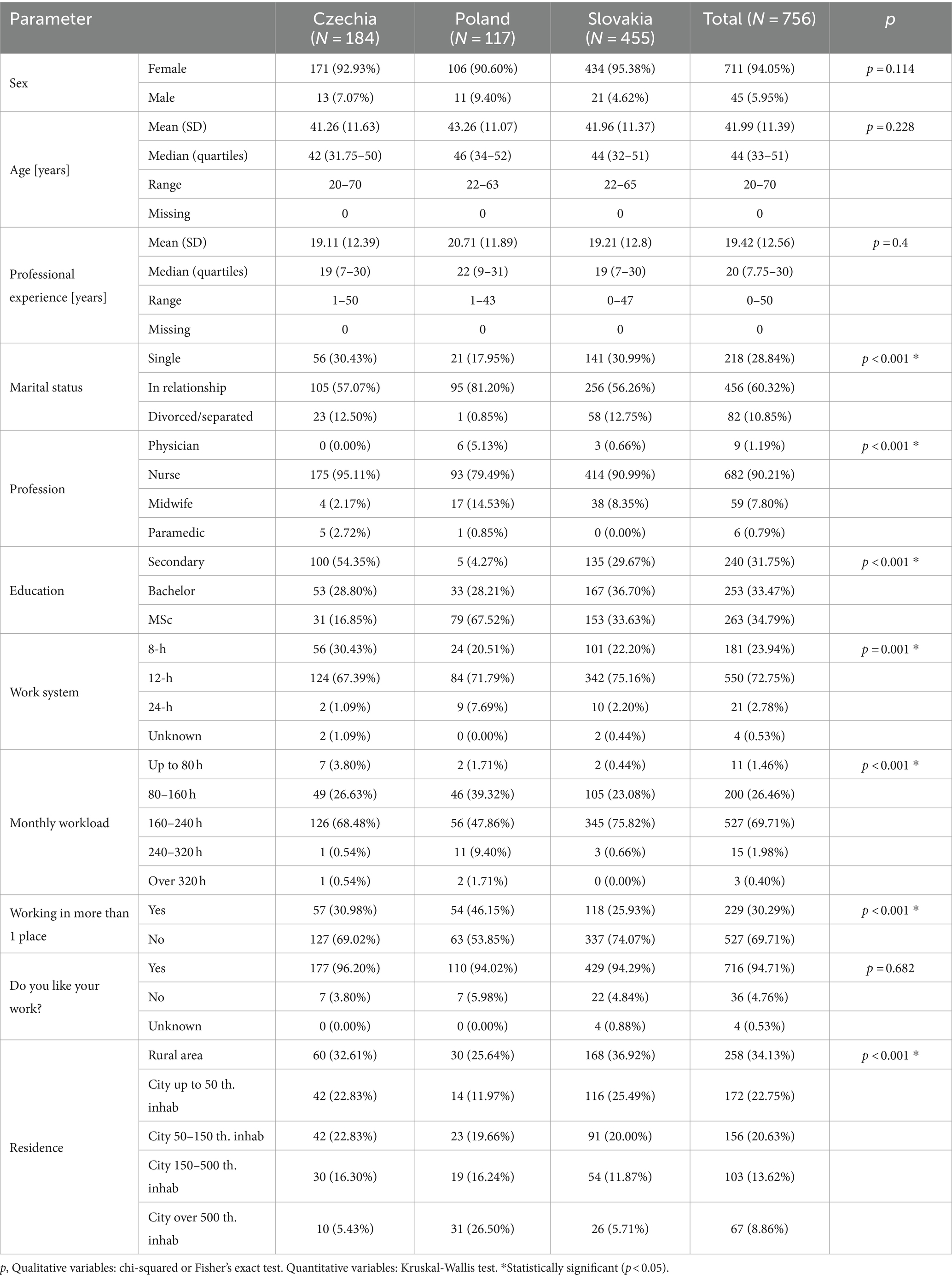
Table 1. Socio-demographic characteristics of the study group.
The survey found that 603 out of 756 survey participants (79.76%) had low quality sleep (6–21 PSQI points), while 147 out of 756 participants had good sleep quality (0–5 PSQI points) and 6 participants did not answer this question. Slovakia and Poland had significantly higher sleep problems than the Czech Republic (p < 0.05), and the PSQI scores for Poland and Slovakia were relatively similar (Table 2). All three countries scored above 5 points, which suggests that healthcare workers in all three countries are experiencing poor sleep quality.
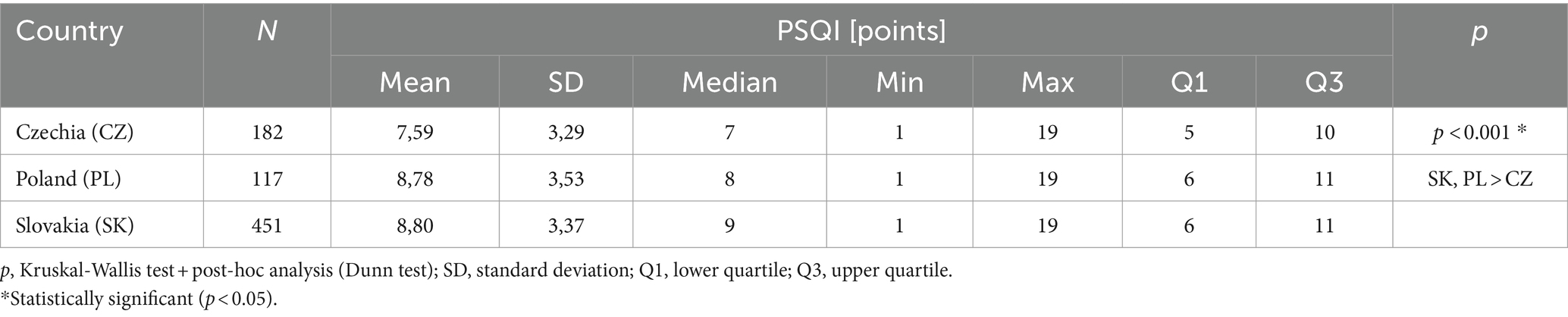
Table 2. Overall sleep quality score for each country.
Alarm fatigue levels were calculated for participants in every country in this study. The statistical differences between countries are significant (p < 0.05). Alarm fatigue caused by medical devices was significantly higher in Slovakia and Poland than in the Czech Republic (Table 3). Alarm fatigue and sleep problems are positively correlated (Table 4). All three countries had statistically significant positive correlations, with the correlation coefficients being 0.171 (p = 0.039) in the Czech Republic, 0.303 (p = 0.001) in Poland, and 0.228 (p < 0.001) in Slovakia. The importance of this result for further exploration is that it supports the idea that medical devices that emit audible alarms have an impact on the sleep quality of medical staff. Furthermore, the association between socio-demographic data and alarm fatigue was investigated. Alarm fatigue has been found to have a statistically significant relationship (p < 0.05) with age and length of service. Poland, Czech Republic, and Slovakia show a correlation coefficient of −0.28; −0.378; −0.156, which indicates that more years of practice result in a reduction in alarm fatigue experience. The prevalence of alarm fatigue in older adult HCWs is lower than it is in younger individuals, as assessed by Spearman’s correlation coefficients for Poland, Czech Republic, and Slovakia: −0.274, −0.362, −0.169. Alarm fatigue was found to be significantly greater in those working 12-h shifts than in those working 8-h shifts only in the Czech study group (p < 0.05). There was no statistical significance observed for other demographic variables and alarm fatigue.
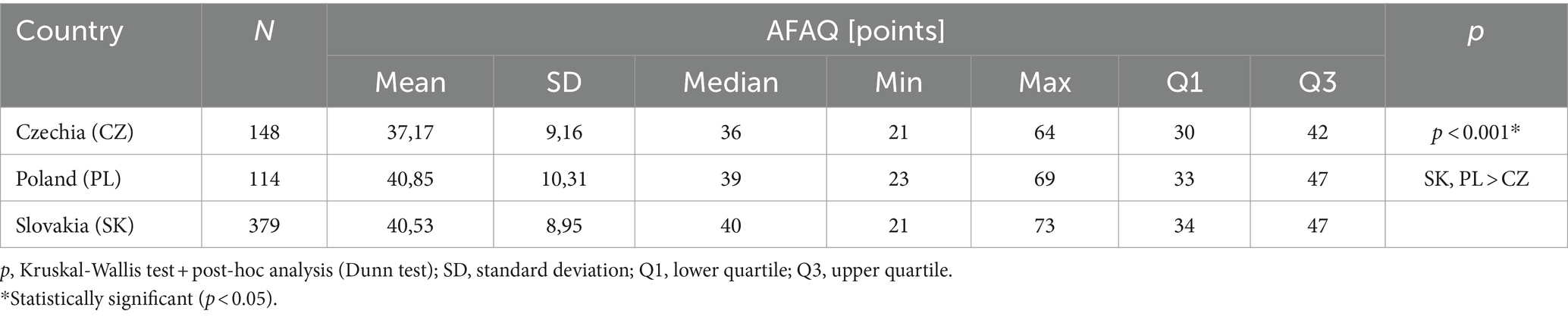
Table 3. Overall alarm fatigue score for each country.

Table 4. Relationship between sleep quality and fatigue alarms by country.
Discussion
Healthcare workers’ well-being and patient safety depend on their sleep quality. This article explores the relationship between alarm fatigue and the quality of sleep of healthcare workers. Sleep hygiene can lead to an increase in job satisfaction for healthcare staff and, ultimately, a healthier and more resilient healthcare system. Alarm fatigue is a result of HCWs being overexposed to alarms, which can lead to indifference and potentially death or permanent injuries for patients (15, 29). The impact of medical device alarms on patient and staff safety has become a growing concern in healthcare facilities.
According to Bourjet al., Alarm fatigue and its consequences are affecting all medical personnel (30).
The effects of alarm fatigue on the well-being of healthcare workers have only been investigated in a few studies at present. Our study shows that alarm fatigue is a common occurrence among medical staff because they are exposed to medical alarms for a long time at work. Alarm fatigue issues are present in all participating countries in our study, which is concerning. Alarm fatigue was more intense in Poland and Slovakia than in the Czech Republic, among the three participating countries in this study.
Healthcare workers are increasingly mentioning that alarm fatigue has a negative impact on sleep quality when discussing its impact on their well-being. Curry et al. showed that sleep disturbance occurs due to alarm fatigue (31). The study discovered that alarm fatigue has a negative impact on the quality of sleep of medical staff. Similarly, Kaylor et al. conducted a study to investigate alarm fatigue and sleep quality in caregivers of children with diabetes who continuously monitor glucose levels. The quality of sleep for caregivers is negatively impacted by alarm fatigue, as evidenced by the results (32).
The reduction of alarm fatigue can be achieved with effective management of medical device alarms (33). It is crucial to prioritize this issue as prolonged exposure to this psychosocial risk factor can lead to decreased quality of life, depression, job burnout, or cardiovascular problems among HCWs, as well as patient safety risks (34–37). There is no question that this is an area of research that needs further examination due to its direct impact on the safety of patients and healthcare workers and education is crucial to solving this issue.
Conclusion
Healthcare systems worldwide are facing a challenge due to the shortage of healthcare workers. The current shortage can be worsened by the presence of psychosocial stressors in hospitals and clinics, causing absenteeism and resignations. Medical staff shortages can result in negative outcomes and pose a potential risk to both patient safety and the well-being of medical staff.
Medical alarms have the potential to cause significant stress for medical staff, which can further exacerbate the situation. Excessive exposure to alarms can lead to fatigue and decreased sleep quality. Long-term fatigue caused by sleep disturbances can pose significant health and patient safety risks. Just like other psychosocial risk factors, the exposure to medical alarms requires effective monitoring and management in hospitals and clinics.
Based on our study, alarm fatigue and sleep quality of HCWs are correlated and the Alarm Fatigue Assessment Questionnaire (AFAQ) and The Pittsburgh Sleep Quality Index (PSQI) can be employed to measure alarm fatigue and evaluate sleep hygiene. Medical staff and patients can be more satisfied and safer by continuing monitoring for alarm fatigue.
Study limitations
It’s worth noting that despite the invitation to all health professionals (doctors, paramedics, and nurses/midwives) to participate in the study, nurses received the highest response rate. Therefore, the study group cannot represent all health professions due to the low response rate of other professions when compared to nurses. Given the significant proportion of respondents being women, it is important to consider gender as a limitation. Continuing research in this stream should consider aspects such as non-sound alerts, setting and adjusting limits on alarms, the impact of OSA and obesity on sleep quality, and the prevalence of hearing problems in staff versus responding to alarms.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Author contributions
ŁR: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. IW: Formal analysis, Writing – original draft. MŠ: Resources, Software, Validation, Writing – original draft. HS: Writing – original draft, Writing – review & editing. OJ: Methodology, Resources, Writing – original draft.
Funding
The author(s) declare financial support was received for the research and/or publication of this article. This study received internal resources funding from: REZD.2 507.24.003. This study was carried out as part of a project implemented at the Wroclaw Medical University, project number SUBK.E260.23.002.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Correction note
A correction has been made to this article. Details can be found at: 10.3389/fpubh.2025.1729764.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Tanner, T. The problem of alarm fatigue. Nurs Womens Health. (2013) 17:153–7. doi: 10.1111/1751-486X.12025
2. Graham, KC, and Cvach, M. Monitor alarm fatigue: standardizing use of physiological monitors and decreasing nuisance alarms. Am J Crit Care. (2010) 19:28–34. doi: 10.4037/ajcc2010651
3. Harris, PR, Zègre-Hemsey, JK, Schindler, D, Bai, Y, Pelter, MM, and Hu, X. Patient characteristics associated with false arrhythmia alarms in intensive care. Ther Clin Risk Manag. (2017) 13:499–513. doi: 10.2147/TCRM.S126191
4. Cvach, M. Monitor alarm fatigue: an integrative review. Med Device Res Rep. (2012) 46:268–77. doi: 10.2345/0899-8205-46.4.268
5. Solet, JM, and Barach, PR. Managing alarm fatigue in cardiac care. Prog Pediatr Cardiol. (2012) 33:85–90. doi: 10.1016/j.ppedcard.2011.12.014
6. Sendelbach, S, and Funk, M. Alarm FatigueA patient safety concern. AACN Adv Crit Care. (2013) 24:378–86. doi: 10.4037/NCI.0b013e3182a903f9
7. Sowan, AK, Staggers, N, Reed, CC, Austin, T, Chen, Q, Xu, S, et al. State of science in alarm system safety: implications for researchers, vendors, and clinical leaders. Med Device Res Rep. (2022) 56:19–28. doi: 10.2345/0899-8205-56.1.19
8. Commission TJ. (2013). Sentinel event alert: Medical device alarm safety in hospitals. Available at: www.jointcommission.org
9. Claudio, D, Deb, S, and Diegel, E. A framework to assess alarm fatigue indicators in critical care staff. Crit Care Explor. (2021) 3:E0464. doi: 10.1097/CCE.0000000000000464
10. Pishori, T. (2012). A stochastic simulation model of alarm response strategies on a telemetry floor [Master’s Theses].
11. Wallis, L. Alarm fatigue linked to Patient’s death. Am J Nurs. (2010) 110:16. doi: 10.1097/01.NAJ.0000383917.98063.bd
12. White, K. Translation of evidence into nursing and health care. Second Springer. (2016):419–30. doi: 10.1891/9780826117830
13. Deb, S, and Claudio, D. Alarm fatigue and its influence on staff performance. IIE Trans Healthc Syst Eng. (2015) 5:183–96. doi: 10.1080/19488300.2015.1062065
14. Storm, J, and Chen, HC. The relationships among alarm fatigue, compassion fatigue, burnout and compassion satisfaction in critical care and step-down nurses. J Clin Nurs. (2021) 30:443–53. doi: 10.1111/jocn.15555
15. Johnson, KR, Hagadorn, JI, and Sink, DW. Alarm safety and alarm fatigue. Clin Perinatol. (2017) 44:713–28. doi: 10.1016/j.clp.2017.05.005
16. Ding, S, Huang, X, Sun, R, Yang, L, Yang, X, Li, X, et al. The relationship between alarm fatigue and burnout among critical care nurses: a cross-sectional study. Nurs Crit Care. (2023) 28:940–7. doi: 10.1111/nicc.12899
17. Søvold, LE, Naslund, JA, Kousoulis, AA, Saxena, S, Qoronfleh, MW, Grobler, C, et al. Prioritizing the mental health and well-being of healthcare workers: an urgent global public health priority. Front Public Health. (2021) 9:679397. doi: 10.3389/fpubh.2021.679397
18. Movahedi, A, Sadooghiasl, A, Ahmadi, F, and Vaismoradi, M. A grounded theory study of alarm fatigue among nurses in intensive care units. Aust Crit Care. (2022) 36:980–8. doi: 10.1016/j.aucc.2022.12.004
19. Nelson, KL, Davis, JE, and Corbett, CF. Sleep quality: an evolutionary concept analysis. Nurs Forum. (2022) 57:144–51. doi: 10.1111/nuf.12659
20. Scott, AJ, Webb, TL, Martyn-St James, M, Rowse, G, and Weich, S. Improving sleep quality leads to better mental health: a meta-analysis of randomised controlled trials. Sleep Med Rev. (2021) 60:101556. doi: 10.1016/j.smrv.2021.101556
21. Rypicz, Ł, Rozensztrauch, A, Fedorowicz, O, Włodarczyk, A, Zató Nska, K, Juárez-Vela, R, et al. Polish adaptation of the alarm fatigue assessment questionnaire as an element of improving patient safety. Int J Environ Res Public Health. (2023) 20:1734. doi: 10.3390/ijerph20031734
22. Buysse, DJ, Reynolds, CF, Monk, TH, Berman, SR, and Kupfer, DJ. The Pittsburgh sleep quality index: a new instrument for psychiatric practice and research. Psychiatry Res. (1989) 28:193–213. doi: 10.1016/0165-1781(89)90047-4
23. Torabizadeh, C, Yousefinya, A, Zand, F, Mahnaz, R, and Mohammad, F. A nurses’ alarm fatigue questionnaire: development and psychometric properties. J Clin Monit Comput. (2017) 31:1305–1312. doi: 10.1007/s10877-016-9958-x
24. Staniszewska, A, Mąka, A, Religioni, U, and Olejniczak, D. Sleep disturbances among patients with epilepsy. Neuropsychiatr Dis Treat. (2017) 13:1797–803. doi: 10.2147/NDT.S136868
25. Manková, D, Dudysová, D, Novák, J, Fárková, E, Janků, K, Kliková, M, et al. Reliability and validity of the Czech version of the Pittsburgh sleep quality index in patients with sleep disorders and healthy controls. Biomed Res Int. (2021) 2021:1–9. doi: 10.1155/2021/5576348
26. Kmetec, S, Fekonja, Z, Davey, A, Mlinar Reljić, N, and Lorber, M. Development of a slovenian version of the Pittsburgh sleep quality index (PSQI-SLO) for use with older adults. Int J Older People Nursing. (2022) 17:12411. doi: 10.1111/opn.12411
27. R Core Team. R: A language and environment for statistical computing. Vienna, Austria: R Foundation for Statistical Computing (2023).
28. World Medical Association. World Medical Association Declaration of Helsinki: ethical principles for medical research involving human subjects. JAMA. (2013) 310:2191–4. doi: 10.1001/jama.2013.281053
29. Voepel-Lewis, T, Parker, ML, Burke, CN, Hemberg, J, Perlin, L, Kai, S, et al. Pulse oximetry desaturation alarms on a general postoperative adult unit: a prospective observational study of nurse response time. Int J Nurs Stud. (2013) 50:1351–8. doi: 10.1016/j.ijnurstu.2013.02.006
30. Bourji, H, Sabbah, H, al’Jamil, A, Khamis, R, Sabbah, S, Droubi, N, et al. Evaluating the alarm fatigue and its associated factors among clinicians in critical care units. European journal of. CLINICMED. (2020) 1:1. doi: 10.24018/clinicmed.2020.1.1.8
31. Curry, JP, and Jungquist, CR. A critical assessment of monitoring practices, patient deterioration, and alarm fatigue on inpatient wards: A review. Patient Safety in Surgery, vol. 8. London: BioMed Central Ltd. (2014). 29 p.
32. Kaylor, MB, and Morrow, L. Alarm fatigue and sleep deprivation in carers of children using continuous glucose monitors. Diabetes Care for Children & Young People (2022) 11:[Early view publication].
33. Bi, J, Yin, X, Li, H, Gao, R, Zhang, Q, Zhong, T, et al. Effects of monitor alarm management training on nurses’ alarm fatigue: a randomised controlled trial. J Clin Nurs [Internet]. (2020) 29:4203–16. doi: 10.1111/jocn.15452
34. Ruskin, KJ, and Hueske-Kraus, D. Alarm fatigue: impacts on patient safety. Curr Opin Anesthesiol. (2015) 28:685–90. doi: 10.1097/ACO.0000000000000260
35. Nguyen, J, Davis, K, Guglielmello, G, and Stawicki, SP. Combating alarm fatigue: the quest for more accurate and safer clinical monitoring equipment In: SP Stawicki and MS Firstenberg, editors. Vignettes in patient safety. Rijeka: IntechOpen (2019). 6.
36. Nyarko, BA, Yin, Z, Chai, X, and Yue, L. Nurses’ alarm fatigue, influencing factors, and its relationship with burnout in the critical care units: a cross-sectional study. Aust Crit Care. (2023) 37:273–80. doi: 10.1016/j.aucc.2023.06.010
Keywords: alarm fatigue, sleep, healthcare worker, well-being, safety, ergonomics
Citation: Rypicz Ł, Witczak I, Šupínová M, Salehi HP and Jarabicová O (2024) Alarm fatigue and sleep quality in medical staff—a Polish-Czech-Slovak study on workplace ergonomics. Front. Public Health. 12:1345396. doi: 10.3389/fpubh.2024.1345396
Edited by:
Marcus Stueck, International Biocentric Research Academy (IBRA), GermanyReviewed by:
Fatemeh Salmani, Islamic Azad University of Najafabad, IranSai Praveen Haranath, Apollo Hospitals, India
Copyright © 2024 Rypicz, Witczak, Šupínová, Salehi and Jarabicová. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Łukasz Rypicz, bHVrYXN6LnJ5cGljekB1bXcuZWR1LnBs