
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Public Health , 02 October 2024
Sec. Public Health Education and Promotion
Volume 12 - 2024 | https://doi.org/10.3389/fpubh.2024.1344907
 Ana Renda1,2,3,4*
Ana Renda1,2,3,4* Heidi Turon1,2,4,5Michelle Lim6Luke Wolfenden1,2,4,5Sam McCrabb1,2,4,5
Heidi Turon1,2,4,5Michelle Lim6Luke Wolfenden1,2,4,5Sam McCrabb1,2,4,5 Seán R. O’Connor7,8Meghan Finch1,2,4Natasha Smith8Navdeep Goraya9Cheryce L. Harrison6
Seán R. O’Connor7,8Meghan Finch1,2,4Natasha Smith8Navdeep Goraya9Cheryce L. Harrison6 Shaan Naughton10
Shaan Naughton10 Alice Grady1,2,4,5
Alice Grady1,2,4,5 Rebecca Hodder1,2,4,5
Rebecca Hodder1,2,4,5 Kathryn Reilly1,4,5Serene Yoong2,5,10
Kathryn Reilly1,4,5Serene Yoong2,5,10Background: There is a large number of research studies about the prevention of non-communicable diseases (NCD), with findings taking several years to be translated into practice. One reason for this lack of translation is a limited understanding of how to best disseminate NCD research findings to user-groups in a way that is salient and useful. An understanding of barriers and facilitators to dissemination is key to informing the development of strategies to increase dissemination. Therefore, this review aims to identify and synthesise the barriers and facilitators to dissemination of NCD research findings.
Methods: A mixed studies systematic review was performed following JBI (formerly known as Joanna Briggs Institute) methodology. The search included articles from January 2000 until May 2021. We conducted a comprehensive search of bibliographic and grey literature of five databases to identify eligible studies. Studies were included if they involved end-users of public health research that were decision-makers in their setting and examined barriers/facilitators to disseminating research findings. Two pairs of reviewers mapped data from included studies against the Framework of Knowledge Translation (FKT) and used a convergent approach to synthesise the data.
Results: The database search yielded 27,192 reports. Following screening and full text review, 15 studies (ten qualitative, one quantitative and four mixed methods) were included. Studies were conducted in 12 mostly high-income countries, with a total of 871 participants. We identified 12 barriers and 14 facilitators mapped to five elements of the FKT. Barriers related to: (i) the user-group (n = 3) such as not perceiving health as important and (ii) the dissemination strategies (n = 3) such as lack of understanding of content of guidelines. Several facilitators related to dissemination strategies (n = 5) such as using different channels of communication. Facilitators also related to the user-group (n = 4) such as the user-groups’ interest in health and research.
Conclusion: Researchers and government organisations should consider these factors when identifying ways to disseminate research findings to decision-maker audiences. Future research should aim to build the evidence base on different strategies to overcome these barriers.
Systematic review registration: The protocol of this review was deposited in Open Science Framework (https://doi.org/10.17605/OSF.IO/5QSGD).
Non-communicable diseases (NCD) are a major public health concern, responsible for 71% of all deaths globally (1). NCD can be defined as “[…] a group of diseases linked by common risk factors, determinants, aetiologies, and pathologies, which can cause a variety of organ and organ system damage […] and are caused by the duration and dosage of exposure to anthropogenic risk factors, usually over several decades” (2, 3). In 2019, NCD accounted for approximately 1.6 billion disability-adjusted life years (DALY) lost worldwide, where one DALY equals one lost year of healthy life (4). The burden of NCD are highest among those aged 50–74 age group, with cardiovascular diseases, diabetes mellitus, chronic obstructive pulmonary disease, and various cancers being the leading causes of mortality (3). The primary modifiable risk factors contributing to the burden from NCD include physical inactivity, exposure to tobacco use, unhealthy diets and high consumption of alcohol (5–9). These risk factors can be targeted to reduce the incidence of NCD (10).
In past decades, public health research has resulted in evidence-based guidelines and plans that can inform public health policy and practice to reduce the risk of NCD by targeting their risk factors (11). Ensuring that this research evidence is used to inform public health policy is key to guarantee the benefits of research reaching the population. Governments and organisations report using different types of evidence in policy and practice decisions, however, various barriers to the use of evidence by policymakers have been identified (12). These include a lack of availability of research, lack of relevant research, poor dissemination and lack of managerial support (12, 13). As a result, newly published research or guidelines are often not translated into practice and, when they are, often taking a significant amount of time to influence policy and practice (14).
Despite guidance being available to support targeted dissemination of research, public health researchers do not disseminate research findings effectively to non-academic audiences (15). Understanding barriers to the dissemination process by public health researchers helps with better producing and disseminating NCD research. Dissemination is different from passive transfer of knowledge or diffusion, where the information spreads unintentionally (16). To improve research dissemination, it is important to comprehensively understand factors that promote or impede the dissemination process. Glasgow and colleagues have suggested that to enhance the integration of research into practice, barriers to dissemination need to be anticipated and be used to develop dissemination strategies (17). For the purpose of this review, we will be using the following adapted dissemination definition by Rabin and colleagues: “an active approach of spreading evidence-based research findings to the target audience via determined channels using planned strategies” (18).
The study of disseminating health research is not new (19); however, it is widely recognised that it is underdeveloped when compared to literature surrounding implementation science (16, 20–22). In contrast to implementation science, there is also a lack of consensus on a definition for dissemination research, limited understanding of dissemination determinants and outcomes and an almost absence of research on dissemination strategies (16, 23). One of the reasons for this is that the literature does not draw out dissemination as separate from implementation, often conflating the two. This review focuses on extending the evidence base related specifically to dissemination only (i.e., the process of getting research evidence to end-users in a way that supports practice and decisions making).
To the best of our knowledge, there is limited evidence that identifies factors that hinder or enable dissemination of public health research findings, and no previous systematic reviews synthesising the key factors that influence the dissemination of NCD research evidence specifically. Therefore, we sought to undertake a systematic review of barriers and facilitators using the Framework for Knowledge Translation (FKT) by Jacobson and colleagues as a guiding frame for synthesis (24). The FKT is a particularly useful framework describing five themes by which knowledge translation is affected: (1) the user group, (2) the issue, (3) the research, (4) the researcher-user relationship, and (5) dissemination strategies. The literature on dissemination science provides multiple frameworks and models that allow the examination of dissemination processes, agents, levels, and interactions (16, 25, 26). We opted to select the FKT for the following reasons, (a) it is dissemination only framework, and (b) comprehensively outlines the process for dissemination and the factors influencing each process (25).
This review aims to answer the following research question: What are the barriers and facilitators that disseminators (i.e., source) of research findings face when actively transferring research (i.e., dissemination) related to the prevention of NCD, from an end-user perspective.
Following the JBI (formerly known as Joanna Briggs Institute) methodology, we defined and described the Population, phenomena of Interest and Context (PICo) below.
We considered studies where the dissemination of NCD research was directed to end-users of public health research that were decision-makers in their setting. We have defined end-users as: public health practitioners who are healthcare providers in the community, community members who are not health care providers but who have the authority to decide whether health programs should be implemented (i.e., school principals, regional school managers), public health researchers and academics, research funders (i.e., government, private industry, foundations, professional organisations), regulatory bodies (i.e., government departments that manage and provide recommendations or standards relevant to public health), industry members, and policymakers (i.e., government health entities responsible for overseeing, developing, implementing and evaluating public health policy and strategies). We included studies where there were different types of participants if data pertaining to participants meeting the eligibility criteria was reported separately. For example, if the sample included researchers, healthcare providers and parents, we only took into consideration data from researchers and healthcare providers. Studies targeting community members such as patients, parents, children, and the older adult were excluded as these are not considered decision-makers in their setting. The terminology defining end-users can vary among the literature and in the FKT, therefore for the purpose of this review, end-user and user-group are both used to refer to the population sample.
This review includes studies that explored the barriers and facilitators to the dissemination of NCD research findings by researchers or organisations responsible for disseminating research. For this study, the definition of a barrier was adapted from Bach-Mortensen et al. (27) as any factors that obstruct the dissemination of evidence-based findings and the adapted definition of a facilitator is any factor that enables the dissemination of evidence-based findings (27).
For implementation research, context “is the set of circumstances or unique factors that surround a particular implementation effort” (28). Dissemination science can be key to helping research reach NCD policymakers and practitioners, however, it has been conventionally studied conjointly with implementation science, known as dissemination and implementation science or ‘D&I’. Recent evidence suggests that dissemination is a distinct construct from implementation and therefore systematic efforts to study this process are warranted (16, 20).
This review considered quantitative, qualitative and mixed methods studies, as long as they investigated barriers and facilitators to dissemination of public health research related to NCD. We excluded systematic reviews, randomised controlled trials, protocols, commentaries, editorials, comments/reviews of another paper, book reviews, narrative/literature reviews, letters to the editor, papers describing measures and conference abstracts. We included studies published in any language from January 2000, as we anticipate that the evidence surrounding dissemination is likely to have more formally emerged since then (18, 29).
This review was conducted and reported according to the JBI convergent integrated approach for mixed methods systematic reviews (30). For this review, we chose a mixed methods approach integrating data from qualitative, quantitative and mixed methods studies as this provides a more complete understanding of the type, breadth and depth of barriers and facilitators that are emerging through different research approaches such as exploratory, explanatory or convergent (31). In the latter, equal priority is given to the different types of data and results are merged (32). For example, qualitative data might add contextual information or illustrations to a numerical answer or quantitative data can provide frequency, magnitude and effects of factors regarding the existence of particular barriers and/or facilitators (32, 33). A protocol for this review has been prospectively deposited in Open Science Framework (OSF) 10.17605/OSF.IO/5QSGD.
A search strategy was developed in conjunction with a university health research librarian. The search included articles from January 2000 until May 2021.
We conducted a comprehensive search of bibliographic and grey literature databases to identify eligible studies. We searched several databases including Medline, Psycinfo, and EBSCO Search Ultimate (focus on health, communications and business/marketing databases). A list of keywords for Medline and PsycInfo are found in Supplementary Data Sheet S1. Based on previous recommendations (34), the top 200 search results in Google and Google Scholar were also screened for articles and the terms dissemination and public health were used. We searched the reference lists of relevant reviews to locate additional primary studies.
Search findings were uploaded to Covidence (35) and one team member removed duplicates (HT). Pairs of team members (HT, NS, SO’C, SN, EW, SMc, AR, CH, SY) screened titles and abstracts for relevance independently. Where conflict between reviewers could not be resolved, a third reviewer (i.e., a senior researcher) decided on inclusion (SY). Full text articles of relevant studies were retrieved and reviewed independently by pairs of reviewers (MF, HT, AR, NS, SY), with a third reviewer where conflicts arose (SY). Studies that met the inclusion criteria were included in the review.
For all included studies, pairs of team members appraised them individually using JBI critical appraisal tools for qualitative, analytical cross-sectional, case controls, case reports (36) (AR, ML, NG). For mixed methods studies, we used the mixed methods appraisal tool (MMAT) (37). We included all studies regardless of their quality.
Following JBI methodology, we conducted data extraction using an adapted version of the JBI template explicitly deemed by authors and extracted by independent pairs of researchers (AR, ML, NG). We extracted the suggested fields (author, year, methodology, methods, number and characteristics of participants, aim/objective of study, phenomena of interest and setting and other context-related information) and the five elements of the FKT: the user-group, the issue, the research, the researcher-user relationship and dissemination strategies (24). These five elements are considered the themes of our review. We defined them and included the definitions in Supplementary Data Sheet S2. We chose the FKT as it is a dissemination-only framework, it provides construct flexibility and it addresses the complexity of knowledge dissemination across the socio-ecologic framework (25).
We then extracted verbatim qualitative and quantitative data into each of the themes. To reduce the need to interpret findings, we extracted those findings that were deemed as either barriers or facilitators to dissemination in included studies. However, there were occasions where the review team met to decide whether a factor was a barrier or facilitator when it was not explicitly reported.
Consistent with the JBI methodology, we assessed for quality of individual findings using a scale of: (1) Unequivocal (“findings accompanied by an illustration that is beyond reasonable doubt and therefore not open to challenge”), (2) Credible (“findings accompanied by an illustration lacking clear association with it and therefore open to challenge”), (3) Not supported (“when 1 nor 2 apply and when most notable findings are not supported by the data. Should not be included in synthesis to inform practice”) (see Supplementary Data Sheet S3 for not supported findings which are not included in the synthesis), and (4) not applicable—qualitized finding (see Supplementary Data Sheet S4).
After extracting data, two reviewers independently “qualitized” the quantitative evidence by converting it to a narrated version of the finding. This method was preferred above converting qualitative into quantitative findings as it is difficult to attribute a numeric value to a qualitative finding (38). As there is no step-by-step guidance to data transformation suggested by JBI, two team members (AR, ML) independently transformed each quantitative finding into a ‘qualitized’ finding, met to discuss disagreements, and consolidated the findings (Supplementary Data Sheets S5, S6).
After the findings were transformed, we inductively performed thematic analysis based on suggested methodologies (39–41), where two reviewers (AR, ML) created codes of all findings per theme of the FKT independently. The team members met to discuss the coding until reaching agreement. For example, we coded the findings extracted from “the research” theme and met to discuss discrepancies. Then, we inductively converted the codes into sub-themes through thematic analysis (40, 42). Finally, we discussed the refining of sub-themes with members of the team until reaching agreement. Figure 1 illustrates this process. Themes, sub-themes and codes were summarised through a narrative description and in a table format in the results section.
Figure 1. Data synthesis and integration process.
The initial search yielded 27,192 results. Of these, 20,343 were retained after removing duplicates. After title and abstract screening, 658 reports were retained for full-text screening and those that did not meet the criteria were excluded due to wrong study design (n = 105), wrong population (n = 117), wrong outcomes (n = 88), wrong aim (n = 26), wrong intervention (n = 288), duplicates (n = 3), full-text not found (n = 1). Further, 1 report was not retrieved as its full-text version could not be accessed despite repeated attempts. We included a total of 15 full-text articles as shown in the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram in Figure 2 (43). Table 1 shows the characteristics of studies included.
Figure 2. PRISMA flowchart. From: Page et al. (43).
Table 1. Characteristics of included studies.
There was a total of 10 qualitative (five interpretive, three grounded theory, one multiple case approach and one case study), one quantitative (one cross-sectional) and four mixed-methods studies. They were conducted in Canada (n = 7), United States (n = 5), Europe (n = 1), Fiji (n = 1) and Australia (n = 1). A total of 871 participants were included in the 15 studies. Studies included physical activity (n = 5) (44–48), mental health (n = 3) (49–51), occupational cancer prevention (n = 1) (52), multicomponent aiming to prevent cancer (n = 1) (53), obesity (n = 1) (54), and alcohol and drug abuse prevention (n = 2) (55, 56); and multicomponent promoting healthy behaviours (n = 2) (57, 58). One study was published in 2001 (56), 2008 (50), 2009 (49), 2015 (57), 2017 (46), 2018 (58), and 2019 (52), two in 2007 (48, 55) and in 2016 (44, 51), and three in 2013 (45, 47, 54).
We assessed the methodological quality of 10 qualitative articles using the JBI critical appraisal tool for qualitative research (59). All studies addressed the congruity of the research methodology and the research question, and 90% of studies addressed the congruity of the research methodology with the methods to collect data, the representation and analysis of data, and the interpretation of results. However, seven out of ten studies did not clearly state their philosophical perspective and seven others did not clearly declare their cultural or theoretical orientation. It was therefore difficult to understand the authors’ philosophical, cultural and theoretical perspective in each study and how this could affect interpretation of findings (59). The quality of the case study could not be appraised on all items on checklist due to the reporting style (56). The JBI critical appraisal tool was used to assess the cross-sectional study (60). This study met five out of the eight criteria, however, did not meet criteria for reporting on confounding factors and validity of measures (see Tables 2, 3). Four mixed-methods studies were appraised using the MMAT, three achieved high quality in the integration of both methodologies. All studies showed high quality in conducting the qualitative section of the studies. However, in the quantitative section of three studies, authors did not report on the representativeness of the target population (see Table 4).
Table 2. Assessment of methodological quality of qualitative studies using the JBI critical appraisal tool.
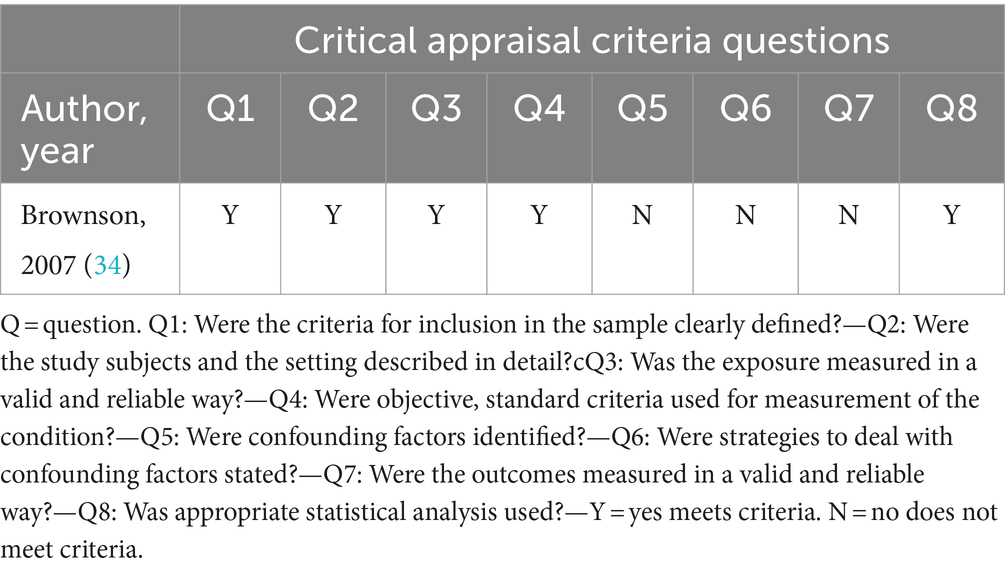
Table 3. Assessment of methodological quality of cross-sectional studies using the JBI critical appraisal tool.
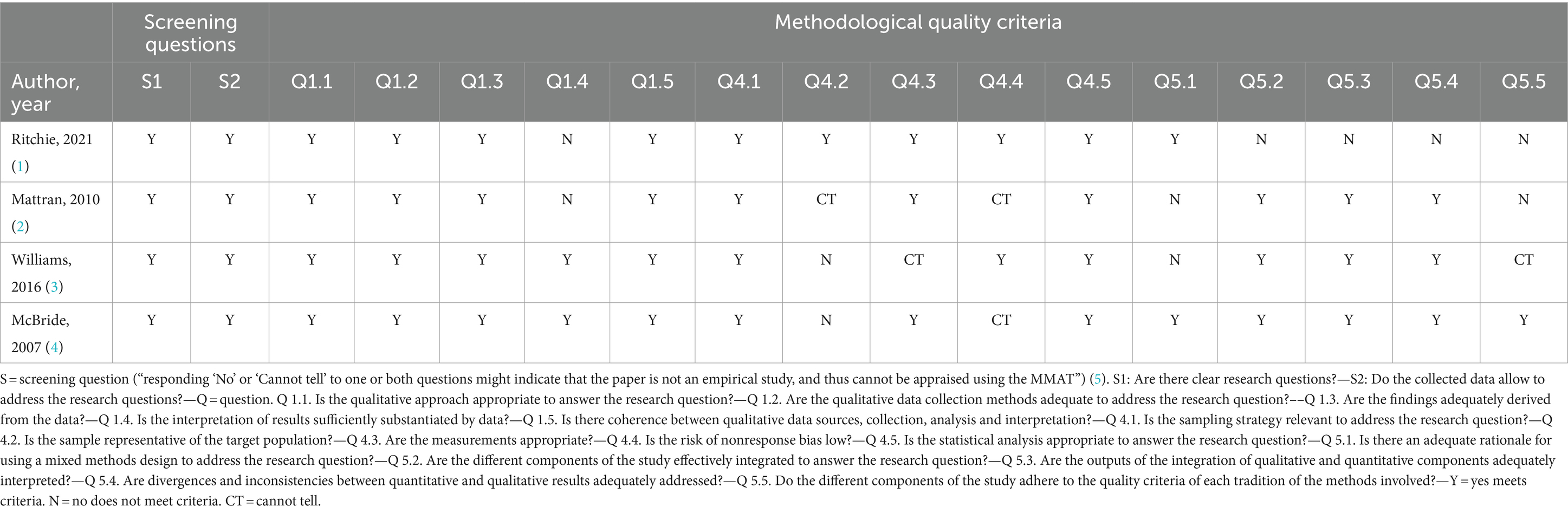
Table 4. Assessment of methodological quality of mixed methods studies using the MMAT.
Following the synthesis, we identified 12 barriers and 14 facilitators mapped to five elements of the FKT (see Tables 5, 6 for summary of findings. See Supplementary Data Sheet S2 for definitions). The themes with the most synthesised barriers were ‘user-group’ and ‘dissemination strategies’. The ‘the user-group’ theme included four studies describing three barriers and ‘dissemination strategies’ included six studies describing three barriers. The theme with the most synthesised facilitators was ‘dissemination strategies’, had six studies identifying three facilitators. The ‘research’ theme included two barriers synthesised from four studies and two facilitators synthesised from four studies. The ‘researchers-user relationship’ theme has two barriers synthesised from two studies and two facilitators synthesised from two studies. Lastly, two barriers were synthesised from two studies and one facilitator from one study that was mapped to ‘the issue’ theme. The remainder of the section details the review findings per element of the framework.
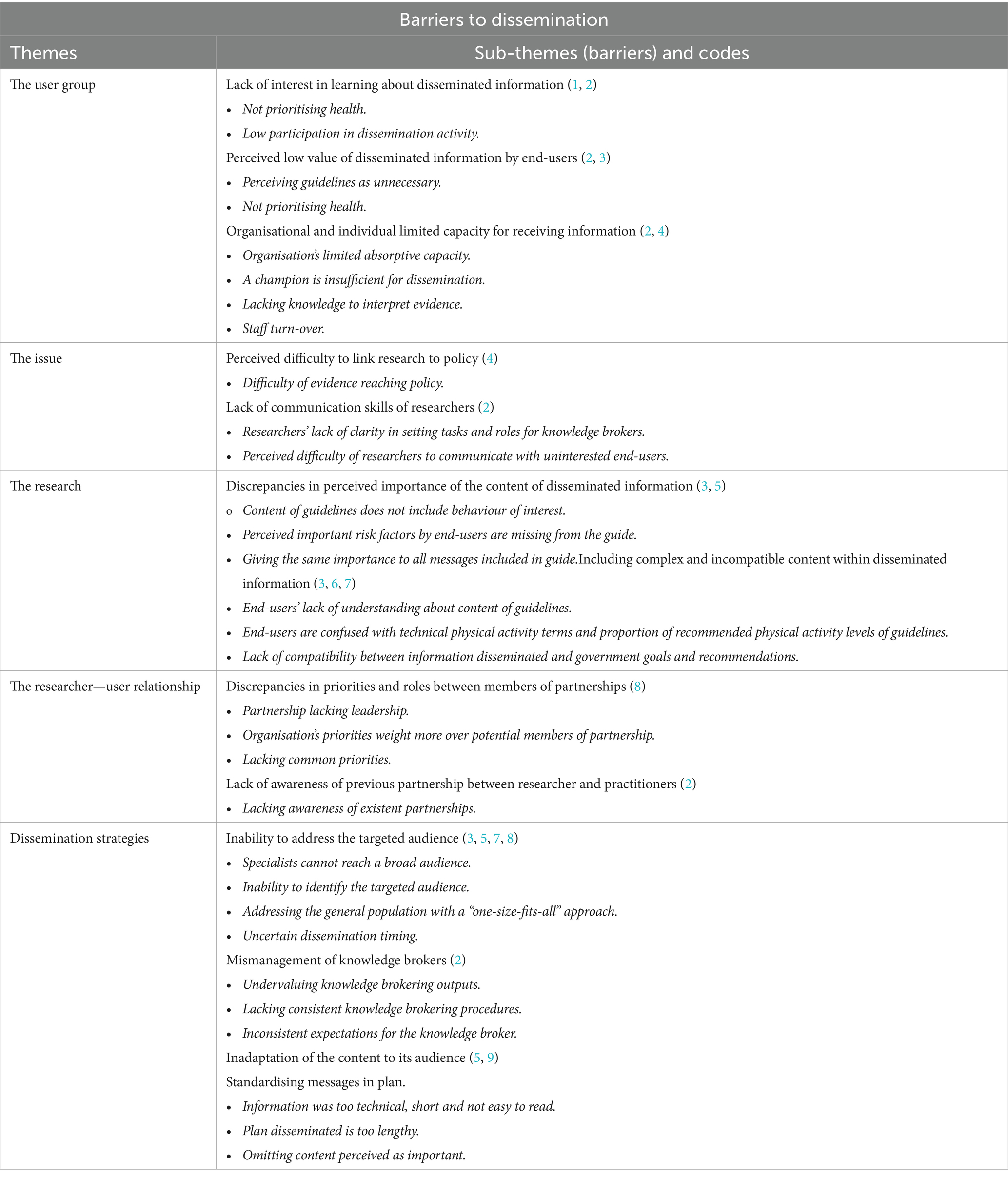
Table 5. Barriers to dissemination related to the framework for knowledge translation.
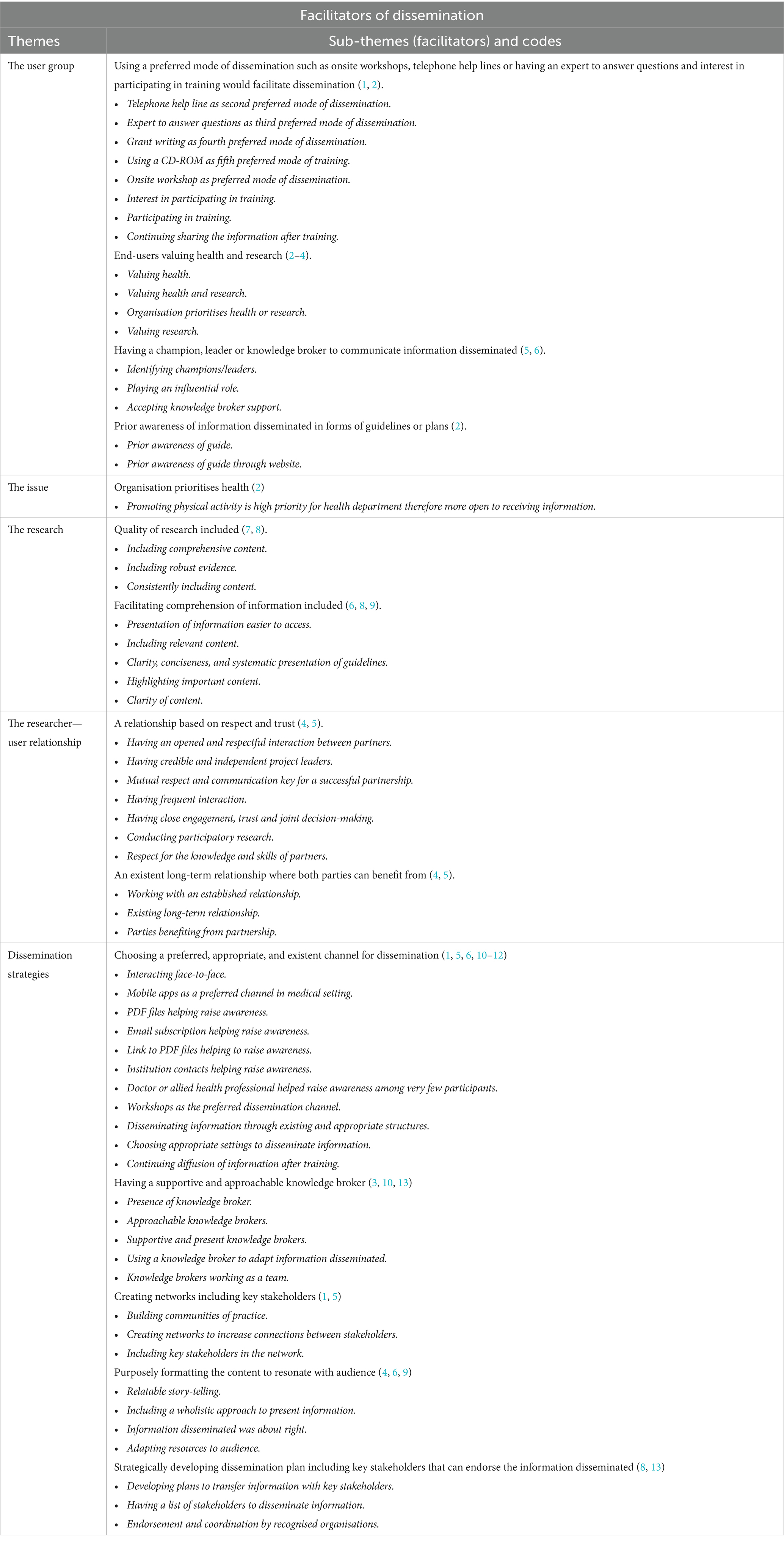
Table 6. Facilitators of dissemination related to the framework for knowledge translation.
The user groups targeted are outlined in Table 1 and included school principals (i.e., headmaster, school director), program managers and health professionals. Within the user-group framework theme, three sub-themes emerged as barriers. This is centred around the lack of perceived value of evidence-based guidelines. For example, one participant said “I do not need these guidelines. I’ve been doing this in my whole career. This is not rocket science, this to me is common sense” (44). Additionally, some user-groups may not view health as a priority for their particular setting (e.g., schools) (58). Limited capacity and inconsistency of staff (i.e., staff turnover) also hinders dissemination as information may not reach the appropriate user-groups (58).
A factor that facilitated dissemination under the user-group theme was preference for different types of communication channels (e.g., workshops or face-to-face communication). Some studies found that participants value health information as they are willing to accept health related research. Having a champion, leader or knowledge broker also facilitates dissemination (58). For example, in one study a participant reported that “you need a specific individual identified as your dissemination manager and that individual helps working with the researchers all the way through from the start to the end of the project” (49). A knowledge broker can be considered as “‘knowledge managers’, ‘linkage agents’, and ‘capacity builders’” (61).
Two barriers emerged within this theme. One study reported a barrier related to the perceived difficulty of research reaching policy. For example, one participant noted: “Less is linked back to policy… I think [research information] gets lost and stays at the clinical or at the scientific level. And they do a good job, moving that information around at that tier. It has a very hard time coming through the glass ceiling though, into the policy world” (participant 7) (49). Another study reported the lack of communication skills of researchers.
Only facilitator identified within this theme was that if the organisation prioritises health, it increases the possibilities to improve the dissemination process.
Barriers related to the research were most frequently explored at the end of the dissemination phase. Participants reported that there was missing content that they perceived as important, or that the messages included in plan were considered with the same degree of importance which hinders dissemination. Also, the information disseminated included complex and incompatible content. For example, a participant noted that “there seems to be a disconnect with maybe some of the federal policy recommendations and the Physical Activity Plan…. I think that the other federal organizations could do a better job of supporting that at the national level” (45).
Participants reported that the presentation of the research, guidelines or plans was important, citing the comprehensiveness, conciseness or the clarity of the content serve as facilitators. For example, a paediatrician highlights that guidelines need to include all health habits, including key components of the message: “I think it’s important to balance both sides of the equation … If you do not sleep, well you do not have as much energy to expend or to conduct the activities of your day. I think you are less likely to engage in physical activity. We know that there are links between sedentary behaviour, sleep, and obesity risk as well. So a lot of the outcomes that you are targeting with this [guideline] are going to be affected by sleep as well. So it all kind of fits together as one big puzzle” (44).
Two subthemes were identified as barriers related to the researcher-user relationship. Discrepancies in priorities and roles could impact the relationship between researchers and practitioners. For example, a practitioner reported: “It is more like oil and water. It can exist in the same bucket but you never fully integrate.” “There was definitely a bit of a bump, bumping along you know, when you realized that you do not share a lot of the same vocabulary and you do not share a lot of the same working priorities and all those kind of things” (52). Also, they reported a lack of awareness of previous partnership between researcher and practitioners.
Two subthemes were identified as facilitators. Having an established relationship based on respect and trust helps dissemination. For example, “Going into [the project] we pretty much had established the relationship in my view. I was very familiar with your work, with the type of people that you were, your passion for it… Of course we are going to at every opportunity partner with you guys” (p270) (52). Also, having a partnership provides mutual benefits to disseminate information (54). Lastly, the elements of participatory research might facilitate dissemination. As one participant reported: “More of the work I have done in the last five years has been involved in participatory research where the researcher knows us, knows the Centre, still has some of the distance to be able to do some of their work, but I think some of the distance in traditional research is artificial, and I think it gets in the way of some of the knowledge transfer. So I think the fact that I have colleagues that I work with and trust, and know me… has made a huge difference” (participant 15) (49).
Three barriers related to dissemination strategies were found. One common barrier encountered was the inadaptation of the content to the audience. One study reported that the format of the training package was difficult to understand. For example, one participant reported, “I got a little lost with the tables explaining the characteristics of CER [comparative effectiveness research] studies of motivational interviewing. A paragraph would have been satisfactory’. Another participant reported, ‘Characteristics of the CER studies (the tables), I’d rather just a summary of what the studies found’. The participants felt the inclusion of research evidence is important, but should be used sparingly” (51). However, two studies reported that specific characteristics of the content of the disseminated information, e.g., guidelines, would help its dissemination.
Another barrier found was the mismanagement of knowledge brokers and their outputs. These were illustrated particularly when researchers lacked knowledge of how to use the information generated by the knowledge brokers. For example, “We were coming up with this more or less as we went along. And it becomes an afterthought sometimes, to say, “we have got all these notes but how are we storing them, how are we presenting them to people, how are we making them user friendly?” And the answer was we were not doing a very good job of that (project manager) (58). On the other hand, having supportive and approachable knowledge broker was a key sub-theme (50, 54, 58).
Strategically developing a dissemination plan including stakeholders that can endorse the information disseminated acts as a facilitator (50, 53). For example, “Think the whole chain out—what do you really want to achieve with your message to a policy maker? You must think the whole chain through and not only be clever in putting it, making a summary on one page, or to send it in terms of guidelines, you have to think all the way up to what you want to achieve at the end. And think those steps out and take action on all of them” (participant 13). “I think first of all it needs to be something that is clearly developed. It has to have who it is aimed at, who it is targeted at, what are the goals and the objectives” (participant 12) (page 6) (49).
Another key finding is to choose a preferred and appropriate channel for dissemination. Face-to-face workshops, organisation contacts, word-of-mouth, media, pdf files, email subscriptions and websites were cited in various studies as means of facilitating dissemination (47, 49, 51, 54, 55). This finding is related to the sub-theme in the user-group. Further, included studies report that using existing communication channels to disseminate information included in guidelines will increase dissemination. For example, one participant (Physical Activity Communicator) explained, “In the webinars that we do, we could leverage the new guidelines, and definitely through our communications we can start some conversations around these guidelines” (page 141) (46). Another facilitator is purposely formatting the content to resonate with audience. For example, researchers when they communicate to policy-makers have said, “research really helps inform what our policy position would be. But even when you have the research, you still have the personal story. You know, the real-life example of it. It’s really important to help when you are talking to policymakers, especially… Like when you can bring it to life by having a real story to say, ‘This is why this is really important to make this policy change” (page 271) (52).
Lastly, a key facilitator was to develop networking opportunities between researchers and practitioners by including key actors in the communication chain (49, 54). A study cited that participants were struggling to reach certain stakeholders, and thanks to networking, information can be disseminated: “[Now] I am thankful with the networking that TROPIC started as we meet and [know] the people that we [usually struggled] to see within the Ministry and those outside the Ministry and is not a challenge any more.”
This systematic review is the first, to our knowledge, to provide a comprehensive summary of the barriers and facilitators that affect the dissemination of NCD prevention related research to public health decision makers. It describes these findings using the five elements of the Framework for Knowledge Translation. One of the primary findings of the review is that using end-user preferred channels for dissemination, and identifying ways to integrate these with existing dissemination pathways would facilitate the dissemination of research findings. This finding is related to both user-groups and dissemination strategies. For example, one strategy to disseminate new guidelines or research would be to include this information into physical activity forums/conferences where physical activity related information is already being communicated to the workforce (46). Consistent with a review of dissemination frameworks by Baumann and colleagues, and Brownson’s Model for Dissemination of Research, the channel or medium of communication is considered a key determinant of dissemination success (16, 22). Our review found that the user-group preferred onsite workshops, telephone help lines or having an expert to answer questions to facilitate dissemination. Despite this, evidence shows that researchers tend to predominately use publications or academic conferences to disseminate their findings (62). Future controlled research examining the impact of different dissemination channels as a dissemination strategy is needed, in light of limited existing empirical research (63). Another important finding of the review is the role of knowledge brokers or champions and noted the potential usefulness when they are integrated within the end-user agencies. Our findings show that having an influential champion/individual may be a useful dissemination strategy by being a trusted, present, supportive and approachable source of information. Knowledge brokers can support end-users to change knowledge and skills and tailor knowledge products to be relevant to end-users’ needs and values (61). As Jacobson suggests, research that is related to the end-users’ beliefs and values will resonate with them and more likely lead to the adoption of the disseminated research (24). However, knowledge brokers could be seen as a barrier if their roles are not well defined (58).
Finally, the review highlights the importance of relationships between researchers and user-groups to support dissemination success. This is consistent with research co-production and integrated knowledge translation where researchers and knowledge users work together to produce research relevant to knowledge users and enhance the sharing and use of findings (64). It is therefore unsurprising that developing and fostering trustworthy and respectful relationships between researchers and end-users may help support effective dissemination of research findings. This is supported by research that highlights the need to build personal networks, relationships and partnerships to facilitate dissemination and use end-users’ preferred communication methods (6, 20, 62, 65–67). Despite this, less than half (46%) of researchers use networking (68) and do not have a strategy to build relationships beforehand. Uphold and colleagues suggest researchers find it difficult to know how to best disseminate beyond professional conferences and publications (26% of participants) (69). There is a clear disconnection between researchers, the channels chosen, the relationship between researchers and the user-group, and the knowledge about the user-group preferred channels. Future research exploring the user-group preferred channels, and research that includes both researchers and user-groups are recommended. A suggested approach is using participatory research methods (e.g., participatory codesign or community-based participatory research) which by design involves all participants or partners (i.e., researchers, end-users, knowledge brokers) in the research process, and taking into consideration their preferences through continuous communication to facilitate dissemination of research findings (23, 70).
The use of a convergent mixed methods methodology which allowed for the examination of the research question through a quantitative and qualitative lens, which is best suited to provide a better understanding of factors affecting dissemination. We undertook the review consistent with best practice approaches and included a range of study designs to better provide a thorough and a contextual understanding of the factors affecting dissemination. We attempted to reduce issues related to conducting systematic reviews of barriers and facilitators (27), by including duplicate screening, factor identification, grading the factors, and data extraction.
There were a number of limitations with the review. Firstly, we encountered challenges with defining dissemination and differentiating dissemination from implementation science or from knowledge translation studies. To support selection of studies, we used a definition of dissemination that was frequently employed and widely accepted in the field. Prior to commencing screening and extraction, iterative discussions with senior researchers who are experts in the field of implementation science (SY, LW) were undertaken. This enabled the research team to develop clear criteria for distinguishing dissemination activities from implementation ones. This was used throughout the review process. We used a broad search strategy to capture all possible eligible studies, however it is possible that some studies may be missed given inconsistent terminology and indexing. Furthermore, although our focus has been solely on dissemination, there is a lack of evidence suggesting that dissemination alone improves implementation (63, 71). Secondly, although a rigorous data extraction process was undertaken, identifying barriers and facilitators proved challenging due to inconsistent reporting across studies. Several rounds of consultation within the team were conducted to reach agreement; however, certain findings may have been missed due to lack of clarity in reporting.
Lastly, studies reporting findings about public health as a broad discipline were excluded as they were outside the scope of the review. We acknowledge that the public health discipline includes communicable diseases such as Human Immunodeficiency Virus, COVID-19, influenza, and other viral or bacterial diseases, and there would have provided some insights into the barriers to dissemination. However, given the differences in the way research evidence is used and therefore disseminated between communicable and NCD (72), we sought to limit the review to focus only on prevention of NCD.
Our review found several barriers and facilitators that should be considered to enhance dissemination of NCD prevention research evidence. Firstly, the use of different communication channels, identifying effective, appropriate dissemination strategies and disseminators developing meaningful relationships with the user-group is recommended to facilitate an open and ongoing dialogue between the disseminators and the user-group. To further advance the science of dissemination, consistent terminology and definitions need to be applied to future research. The review by Baumann summarised the components of dissemination frameworks to guide future research, which include recommendations for a more consistent use of a dissemination definition, strategies and determinant constructs when conducting and reporting dissemination studies (17).
Secondly, our review highlights the lack of empirical research examining the dissemination process, despite its importance (63). Future empirical studies assessing dissemination determinants and strategies are needed. Studies similar to one conducted by Tabak and colleagues, which identified factors related to researchers’ efforts to disseminate findings, are encouraged. They found that having experience in practice or policy settings, as well as being a university researcher affiliated with a Prevention Research Centre, were the strongest predictors of effective dissemination (65). Furthermore, there is a need to assess the impact of dissemination strategies when applied to different contexts and audiences to overcome reported barriers. A recent scoping review by Turon and colleagues highlight the need for experimental studies comparing different dissemination strategies for effective dissemination (63). We encourage future studies to trial the dissemination of research findings with adapted content (i.e., what it contains and how it is presented) among a targeted sample, to understand the potential effect on dissemination outcomes.
Thirdly, dissemination strategies should consider audience preferences for communication channels, information format and content, and focus on addressing identified barriers, such as the lack of researchers’ communication skills and the lack of comprehensiveness of disseminated guidelines. Importantly, our review highlighted that relationships between researchers and end-users are key to support effective dissemination. Integrated research-practice roles have been identified as a way to support the translation of research and to build strong, meaningful partnerships between researchers and practitioners (73).
Lastly, the context in which dissemination occurs is likely to significantly influence its success. Therefore, we recommend conducting research aimed at understanding the current political, policy, economic context before disseminating research findings. This could be achieved through mixed methods studies that incorporate contextual information, thus informing future dissemination efforts. This recommendation is further supported by a recent review by Escoffery and colleagues which identified a lack of consensus on the definition of context and scarce empirical evidence testing context constructs in dissemination and implementation science (74).
Our systematic review identified that several unique barriers exist for disseminators, regarding their relationship with user-groups, and for the user-groups alone. Despite this, there are numerous facilitators that could be considered when planning to disseminate, such as having a dissemination plan prior to disseminating, improving and adapting the content to the audience and forming a respectful and trustworthy relationship with the intended audience. Future research on this topic should aim to reduce barriers and identify dissemination strategies that will increase uptake of NCD findings.
AR: Writing – review & editing, Writing – original draft, Visualization, Project administration, Methodology, Investigation, Formal analysis, Data curation, Conceptualization. HT: Writing – review & editing, Validation, Methodology, Data curation. ML: Writing – review & editing, Formal analysis, Data curation. LW: Writing – review & editing, Validation, Supervision, Methodology, Funding acquisition, Conceptualization. SM: Writing – review & editing, Investigation, Data curation. SO’C: Writing – review & editing, Methodology, Data curation. MF: Writing – review & editing, Methodology, Data curation. NS: Writing – review & editing, Methodology, Investigation, Data curation. NG: Writing – review & editing, Validation, Methodology, Investigation, Formal analysis, Data curation. CH: Writing – review & editing, Methodology, Investigation, Data curation. SN: Writing – review & editing, Methodology, Investigation, Data curation. AG: Writing – review & editing, Supervision. RH: Writing – review & editing, Supervision. KR: Writing – review & editing, Supervision. SY: Writing – review & editing, Writing – original draft, Supervision, Methodology, Investigation, Funding acquisition, Formal analysis, Conceptualization.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. The project described was funded by the National Health and Medical Research Council (NHMRC) Centre for Research Excellence (CRE)—National Centre of Implementation Science (NCOIS) grant (APP1153479), and a NSW Cancer Council Program grant (G1500708). This research was supported by a PhD scholarship (Australian research training program) linked to the NCOIS, a University of Newcastle Prevention Research Centre Health Behaviour Small Grant Funding and Research Student Funds. LW is supported by an NHMRC Investigator Grant (G1901360) and NSW Cardiovascular Research Capacity Program grant number H20/28248. SN is supported by the NHMRC funded CRE in Food Retail Environments for Health (RE-FRESH) (APP1152968). SO’C was supported by the Irish Health Research Board and the HSC Public Health Agency (grant number CBES-2018-001) in association with Evidence Synthesis Ireland/Cochrane Ireland. CH is supported by a NHMRC CRE Health in Preconception and Pregnancy Senior Postdoctoral Fellowship (APP1171142). SY was supported by a Heart Foundation Future Leader Fellowship (ref no: 106654) from the National Heart Foundation of Australia. AG is supported by a Heart Foundation Postdoctoral Fellowship (102518). The opinions, analysis, and conclusions in this paper are those of the authors and should not be attributed to the NHMRC.
We thank Jessica Birchall, University of Newcastle Librarian for her support in conducting the search.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2024.1344907/full#supplementary-material
NCD, Non-communicable diseases; JBI, formerly known as Joanna Briggs Institute; FKT, Framework of Knowledge Translation; DALY, Disability-adjusted life years; PICo, Population, phenomena of Interest and Context; OSF, Open Science Framework; MMAT, Mixed methods appraisal tool; PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
1. Bennett, JE, Stevens, GA, Mathers, CD, Bonita, R, Rehm, J, Kruk, ME, et al. NCD countdown 2030: worldwide trends in non-communicable disease mortality and progress towards sustainable development goal target 3.4. Lancet. (2018) 392:1072–88. doi: 10.1016/S0140-6736(18)31992-5
2. Lincoln, P. Renaming non-communicable diseases. Lancet Glob Heal. (2017) 5:e654. doi: 10.1016/S2214-109X(17)30219-X
3. Abbafati, C, Abbas, KM, Abbasi-Kangevari, M, Abd-Allah, F, Abdelalim, A, Abdollahi, M, et al. Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: a systematic analysis for the global burden of disease study 2019. Lancet. (2020) 396:1204–22. doi: 10.1016/S0140-6736(20)30925-9
4. Institute for Health Metrics and Evaluation (IHME) . Global burden of disease study 2019 (GBD 2019) results [internet]. Global burden of disease collaborative network. (2021). Available at: http://ghdx.healthdata.org/gbd-results-tool
5. Soerjomataram, I, and Bray, F. Planning for tomorrow: global cancer incidence and the role of prevention 2020–2070. Nat Rev Clin Oncol. (2020) 18:663–72. doi: 10.1038/s41571-021-00514-z
6. Roth, GA, Mensah, GA, Johnson, CO, Addolorato, G, Ammirati, E, Baddour, LM, et al. Global burden of cardiovascular diseases and risk factors, 1990-2019: update from the GBD 2019 study. J Am Coll Cardiol. (2020) 76:2982–3021. doi: 10.1016/j.jacc.2020.11.010
7. Toi, PL, Anothaisintawee, T, Chaikledkaew, U, Briones, JR, Reutrakul, S, and Thakkinstian, A. Preventive role of diet interventions and dietary factors in type 2 diabetes mellitus: an umbrella review. Nutrients. (2020) 12:1–17. doi: 10.3390/nu12092722
8. Lee, IM, Shiroma, EJ, Lobelo, F, Puska, P, Blair, SN, Katzmarzyk, PT, et al. Impact of physical inactivity on major non-communicable diseases worldwide: an analysis of burden of disease. Lancet. (2012) 380:219–29. doi: 10.1016/S0140-6736(12)61031-9
9. Afshin, A, Sur, PJ, Fay, KA, Cornaby, L, Ferrara, G, Salama, JS, et al. Health effects of dietary risks in 195 countries, 1990–2017: a systematic analysis for the global burden of disease study 2017. Lancet. (2017) 393:1958–72. doi: 10.1016/S0140-6736(19)30041-8
10. Peters, R, Ee, N, Peters, J, Beckett, N, Booth, A, Rockwood, K, et al. Common risk factors for major noncommunicable disease, a systematic overview of reviews and commentary: the implied potential for targeted risk reduction. Ther Adv Chronic Dis. (2019) 10:204062231988039–14. doi: 10.1177/2040622319880392
11. World Health Organization. Global action plan for the prevention and control of noncommunicable diseases 2013–2020. World Health Organization (2013). Available at: https://iris.who.int/handle/10665/94384
12. Oliver, K, Innvar, S, Lorenc, T, Woodman, J, and Thomas, J. A systematic review of barriers to and facilitators of the use of evidence by policymakers. BMC Health Serv Res. (2014) 14:1–12. doi: 10.1186/1472-6963-14-2
13. Oliver, KA, and de Vocht, F. Defining “evidence” in public health: a survey of policymakers’ uses and preferences. Eur J Pub Health. (2017) 27:112–7. doi: 10.1093/eurpub/ckv082
14. Morris, ZS, Wooding, S, and Grant, J. The answer is 17 years, what is the question: understanding time lags in translational research. J R Soc Med. (2011) 104:510–20. doi: 10.1258/jrsm.2011.110180
15. Brownson, RC, Fielding, JE, and Green, LW. Building capacity for evidence-based public health: reconciling the pulls of practice and the push of research. Annu Rev Public Health. (2018) 39:27–53. doi: 10.1146/annurev-publhealth-040617-014746
16. Baumann, AA, Hooley, C, Kryzer, E, Morshed, AB, Gutner, CA, Malone, S, et al. A scoping review of frameworks in empirical studies and a review of dissemination frameworks. Implement Sci. (2022) 17:53–15. doi: 10.1186/s13012-022-01225-4
17. Glasgow, RE, and Emmons, KM. How can we increase translation of research into practice? Types of evidence needed. Annu Rev Public Health. (2007) 28:413–33. doi: 10.1146/annurev.publhealth.28.021406.144145
18. Rabin, BA, Glasgow, RE, Kerner, JF, Klump, MP, and Brownson, RC. Dissemination and implementation research on community-based Cancer prevention. A systematic review. Am J Prev Med. (2010) 38:443–56. doi: 10.1016/j.amepre.2009.12.035
19. Kerner, J, Rimer, B, and Emmons, K. Introduction to the special section on dissemination—dissemination research and research dissemination: how can we close the gap? Health Psychol. (2005) 24:443–6. doi: 10.1037/0278-6133.24.5.443
20. Purtle, J, Nelson, KL, Bruns, EJ, and Hoagwood, KE. Dissemination strategies to accelerate the policy impact of Children’s mental health services research. Psychiatr Serv. (2020) 71:1170–8. doi: 10.1176/appi.ps.201900527
21. Ashcraft, LE, Quinn, DA, and Brownson, RC. Strategies for effective dissemination of research to United States policymakers: a systematic review. Implement Sci. (2020) 15:1–17. doi: 10.1186/s13012-020-01046-3
22. Brownson, RC, Eyler, AA, Harris, JK, Moore, JB, and Tabak, RG. Getting the word out: new approaches for disseminating public health science. J Public Heal Manag Pract. (2018) 24:102–11. doi: 10.1097/PHH.0000000000000673
23. Kwan, BM, Brownson, RC, Glasgow, RE, Morrato, EH, and Luke, DA. Designing for dissemination and sustainability to promote equitable impacts on health. Annu Rev Public Health. (2022) 43:331–53. doi: 10.1146/annurev-publhealth-052220-112457
24. Jacobson, N, Butterill, D, and Goering, P. Development of a framework for knowledge translation: understanding user context. J Heal Serv Res Policy. (2003) 8:94–9. doi: 10.1258/135581903321466067
25. Tabak, RG, Khoong, EC, Chambers, DA, and Brownson, RC. Bridging research and practice: models for dissemination and implementation research. Am J Prev Med [Internet]. (2012) 43:337–50. doi: 10.1016/j.amepre.2012.05.024
26. Rabin, BA, Swanson, K, Glasgow, RE, Ford, B, Huebschmann, A, Marsh, R, et al. Dissemination & implementation models in health [internet]. (2024) (Accessed Mar 27, 2024). Available at: https://dissemination-implementation.org/
27. Bach-Mortensen, AM, and Verboom, B. Barriers and facilitators systematic reviews in health: a methodological review and recommendations for reviewers. Res Synth Methods. (2020) 11:743–59. doi: 10.1002/jrsm.1447
28. Damschroder, LJ, Aron, DC, Keith, RE, Kirsh, SR, Alexander, JA, and Lowery, JC. Fostering implementation of health services research findings into practice: a consolidated framework for advancing implementation science. Implement Sci. (2009) 4:1–15. doi: 10.1186/1748-5908-4-50
29. Larocca, R, Yost, J, Dobbins, M, Ciliska, D, and Butt, M. The effectiveness of knowledge translation strategies used in public health: a systematic review. BMC Public Health. (2012) 12:1–15. doi: 10.1186/1471-2458-12-751
30. Stern, C, Lizarondo, L, Carrier, J, Godfrey, C, Rieger, K, Salmond, S, et al. Methodological guidance for the conduct of mixed methods systematic reviews. JBI Evid Synth. (2020) 18:2108–18. doi: 10.11124/JBISRIR-D-19-00169
31. Bressan, V, Bagnasco, A, Aleo, G, Timmins, F, Barisone, M, Bianchi, M, et al. Mixed-methods research in nursing—a critical review. J Clin Nurs. (2016) 26:2878–90. doi: 10.1111/jocn.13631
32. Doyle, L, and Brady, AM. An overview of mixed methods research—revisited. J Res Nurs. (2016) 21:623–35. doi: 10.1177/1744987116674257
33. Pluye, P, and Hong, QN. Combining the power of stories and the power of numbers: mixed methods research and mixed studies reviews. Annu Rev Public Health. (2014) 35:29–45. doi: 10.1146/annurev-publhealth-032013-182440
34. Haddaway, NR, Collins, AM, Coughlin, D, and Kirk, S. The role of google scholar in evidence reviews and its applicability to grey literature searching. PLoS One. (2015) 10:1–17. doi: 10.1371/journal.pone.0138237
35. Veritas Health Innovation . Covidence systematic review software. Melbourne, Australia; Available at: www.covidence.org
36. Aromataris, E, Lockwood, C, Porritt, K, Pilla, B, and Jordan, Z. (eds.). JBI manual for evidence synthesis. JBI (2024). Available at: https://synthesismanual.jbi.global
37. Hong, QN, Gonzalez-Reyes, A, and Pluye, P. Improving the usefulness of a tool for appraising the quality of qualitative, quantitative and mixed methods studies, the mixed methods appraisal tool (MMAT). J Eval Clin Pract. (2018) 24:459–67. doi: 10.1111/jep.12884
38. Hong, QN, Pluye, P, Bujold, M, and Wassef, M. Convergent and sequential synthesis designs: implications for conducting and reporting systematic reviews of qualitative and quantitative evidence. Syst Rev. (2017) 6:61. doi: 10.1186/s13643-017-0454-2
39. Braun, V, and Clarke, V. One size fits all? What counts as quality practice in (reflexive) thematic analysis? Qual Res Psychol. (2021) 18:328–52. doi: 10.1080/14780887.2020.1769238
40. Braun, V, and Clarke, V. Using thematic analysis in psychology. Qual Res Psychol. (2006) 3:77–101. doi: 10.1191/1478088706qp063oa
41. Thomas, J, and Harden, A. Methods for the thematic synthesis of qualitative research in systematic reviews. BMC Med Res Methodol. (2008) 8:1–10. doi: 10.1186/1471-2288-8-45
42. Braun, V, and Clarke, V. Can I use TA? Should I use TA? Should I not use TA? Comparing reflexive thematic analysis and other pattern-based qualitative analytic approaches. Couns Psychother Res. (2021) 21:37–47. doi: 10.1002/capr.12360
43. Page, MJ, McKenzie, JE, Bossuyt, PM, Boutron, I, Hoffmann, TC, Mulrow, CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. (2021) 372:n71. doi: 10.1136/bmj.n71
44. Faulkner, G, White, L, Riazi, N, Latimer-Cheung, AE, and Tremblay, MS. Canadian 24-hour movement guidelines for children and youth: exploring the perceptions of stakeholders regarding their acceptability, barriers to uptake, and dissemination. Appl Physiol Nutr Metab. (2016) 41:S303–10. doi: 10.1139/apnm-2016-0100
45. Evenson, KR, Satinsky, SB, Valko, C, Gustat, J, Healy, I, Litt, JS, et al. In-depth interviews with state public health practitioners on the United States National Physical Activity Plan. Int J Behav Nutr Phys Act. (2013) 10:1–9. doi: 10.1186/1479-5868-10-72
46. Riazi, N, Ramanathan, S, O’Neill, M, Tremblay, MS, and Faulkner, G. Canadian 24-hour movement guidelines for the early years (0-4 years): exploring the perceptions of stakeholders and end users regarding their acceptability, barriers to uptake, and dissemination. BMC Public Health. (2017) 17:841. doi: 10.1186/s12889-017-4853-z
47. Mattran, K, Harris, C, Jernigan, J, and Fulton, J. Evaluating the awareness, access, and use of the state indicator report on physical activity, 2010. J Phys Act Health. (2013) 10:863–70. doi: 10.1123/jpah.10.6.863
48. Brownson, RC, Ballew, P, Dieffenderfer, B, Haire-Joshu, D, Heath, GW, Kreuter, MW, et al. Evidence-based interventions to promote physical activity. What contributes to dissemination by state health departments. Am J Prev Med. (2007) 33:S66–78. doi: 10.1016/j.amepre.2007.03.011
49. Mitton, C, Adair, CE, McKenzie, E, Patten, S, Waye-Perry, B, and Smith, N. Designing a knowledge transfer and exchange strategy for the Alberta depression initiative: contributions of qualitative research with key stakeholders. Int J Ment Health Syst. (2009) 3:11–20. doi: 10.1186/1752-4458-3-11
50. Boydell, KM, Stasiulis, E, Barwick, M, Greenberg, N, and Pong, R. Challenges of knowledge translation in rural communities: The case of rural children’s mental health. Can J Community Ment Heal. (2008) 27:49–63. doi: 10.7870/cjcmh-2008-0004
51. Williams, JR, Caceda-Castro, LE, Dusablon, T, and Stipa, M. Design, development, and evaluation of printed educational materials for evidence-based practice dissemination. Int J Evid Based Healthc. (2016) 14:84–94. doi: 10.1097/XEB.0000000000000072
52. Haynes, E, Holness, DL, Tenkate, T, Strahlendorf, P, and Kramer, DM. With a little help from our friends: collaborative research partnerships in three workplace-based occupational disease research projects. Work. (2019) 62:261–78. doi: 10.3233/WOR-192861
53. Ritchie, D, Mallafré-Larrosa, M, Ferro, G, Schüz, J, and Espina, C. Evaluation of the impact of the European code against Cancer on awareness and attitudes towards cancer prevention at the population and health promoters’ levels. Cancer Epidemiol. (2021) 71:101898. doi: 10.1016/j.canep.2021.101898
54. Waqa, G, Mavoa, H, Snowdon, W, Moodie, M, Nadakuitavuki, R, Mc Cabe, M, et al. Participants’ perceptions of a knowledge-brokering strategy to facilitate evidence-informed policy-making in Fiji. BMC Public Health. (2013) 13:1–9. doi: 10.1186/1471-2458-13-725
55. McBride, NT, Farringdon, FH, and Kennedy, CA. Research to practice—formal dissemination of the school health and alcohol harm reduction project (SHAHRP) in Australia. Drug Alcohol Rev. (2007) 26:665–72. doi: 10.1080/09595230701613510
56. Hoelscher, DM, Kelder, SH, Murray, N, Cribb, PW, Conroy, J, and Parcel, GS. Dissemination and adoption of the child and adolescent trial for cardiovascular health (CATCH): a case study in Texas. J Public Heal Manag Pract. (2001) 7:90–100. doi: 10.1097/00124784-200107020-00012
57. Dagenais, C, Laurendeau, MC, and Briand-Lamarche, M. Knowledge brokering in public health: a critical analysis of the results of a qualitative evaluation. Eval Program Plann. (2015) 53:10–7. doi: 10.1016/j.evalprogplan.2015.07.003
58. Brown, KM, Elliott, SJ, Robertson-Wilson, J, Vine, MM, and Leatherdale, ST. “Now what?” perceived factors influencing knowledge exchange in school Health Research. Health Promot Pract. (2018) 19:590–600. doi: 10.1177/1524839917732037
59. Lockwood, C, Munn, Z, and Porritt, K. Qualitative research synthesis: methodological guidance for systematic reviewers utilizing meta-aggregation. Int J Evid Based Healthc. (2015) 13:179–87. doi: 10.1097/XEB.0000000000000062
60. Moola, S, Munn, Z, Tufanaru, C, Aromataris, E, Sears, K, Sfetcu, R, et al. Systematic reviews of etiology and risk. In: E Aromataris, C Lockwood, K Porritt, B Pilla, and Z Jordan, editors. JBI manual for evidence synthesis. JBI (2020). Available at: https://synthesismanual.jbi.global
61. Bornbaum, CC, Kornas, K, Peirson, L, and Rosella, LC. Exploring the function and effectiveness of knowledge brokers as facilitators of knowledge translation in health-related settings: a systematic review and thematic analysis (2015) 10:1–12. doi: 10.1186/s13012-015-0351-9,
62. McVay, AB, Stamatakis, KA, Jacobs, JA, Tabak, RG, and Brownson, RC. The role of researchers in disseminating evidence to public health practice settings: a cross-sectional study. Heal Res Policy Syst. (2016) 14:1–10. doi: 10.1186/s12961-016-0113-4
63. Turon, H, Wolfenden, L, Finch, M, McCrabb, S, Naughton, S, O’Connor, SR, et al. Dissemination of public health research to prevent non-communicable diseases: a scoping review. BMC Public Health. (2023) 23:757. doi: 10.1186/s12889-023-15622-x
64. Lawrence, LM, Bishop, A, and Curran, J. Integrated knowledge translation with public health policy makers: a scoping review. Healthc Policy. (2019) 14:55–77. doi: 10.12927/hcpol.2019.25792
65. Tabak, RG, Stamatakis, KA, Jacobs, JA, and Brownson, RC. What predicts dissemination efforts among public health researchers in the United States? Public Health Rep. (2014) 129:361–8. doi: 10.1177/003335491412900411
66. Dearing, JW, and Kreuter, MW. Designing for diffusion: how can we increase uptake of cancer communication innovations? Patient Educ Couns. (2010) 81:S100–10. doi: 10.1016/j.pec.2010.10.013
67. Koorts, H, Naylor, PJ, Laws, R, Love, P, Maple, JL, and Van Nassau, F. What hinders and helps academics to conduct dissemination and implementation (D & I) research in the field of nutrition and physical activity? An international perspective. Int J Behav Nutr Phys Act. (2020) 17:1–12.
68. Wilson, PM, Petticrew, M, Calnan, MW, and Nazareth, I. Does dissemination extend beyond publication: a survey of a cross section of public funded research in the UK. Implement Sci. (2010) 5:1–8. doi: 10.1186/1748-5908-5-61
69. Uphold, HS, Drahota, A, Bustos, TE, Crawford, MK, and Buchalski, Z. “There’s no money in community dissemination”: a mixed methods analysis of researcher dissemination-as-usual. J Clin Transl Sci. (2022) 6:e105. doi: 10.1017/cts.2022.437
70. Ramanadhan, S, Davis, MM, Armstrong, R, Baquero, B, Ko, LK, Leng, JC, et al. Participatory implementation science to increase the impact of evidence-based cancer prevention and control. Cancer Causes Control. (2018) 29:363–9. doi: 10.1007/s10552-018-1008-1
71. Chapman, E, Pantoja, T, Kuchenmüller, T, Sharma, T, and Terry, RF. Assessing the impact of knowledge communication and dissemination strategies targeted at health policy-makers and managers: an overview of systematic reviews. Heal Res Policy Syst. (2021) 19:140. doi: 10.1186/s12961-021-00780-4
72. Bosu, WK. Learning lessons from operational research in infectious diseases: can the same model be used for noncommunicable diseases in developing countries? Adv Med Educ Pract. (2014) 5:469–82. doi: 10.2147/AMEP.S47412
73. Wolfenden, L, Yoong, SL, Williams, CM, Grimshaw, J, Durrheim, DN, Gillham, K, et al. Embedding researchers in health service organizations improves research translation and health service performance: the Australian hunter New England population health example. J Clin Epidemiol [Internet]. (2017) 85:3–11. doi: 10.1016/j.jclinepi.2017.03.007
Keywords: dissemination, public health, non-communicable diseases, implementation science, barriers and facilitators
Citation: Renda A, Turon H, Lim M, Wolfenden L, McCrabb S, O’Connor SR, Finch M, Smith N, Goraya N, Harrison CL, Naughton S, Grady A, Hodder R, Reilly K and Yoong S (2024) Barriers and facilitators to dissemination of non-communicable diseases research: a mixed studies systematic review. Front. Public Health. 12:1344907. doi: 10.3389/fpubh.2024.1344907
Edited by:
Iffat Elbarazi, United Arab Emirates University, United Arab EmiratesReviewed by:
Laura Balis, Gretchen Swanson Center for Nutrition, United StatesCopyright © 2024 Renda, Turon, Lim, Wolfenden, McCrabb, O’Connor, Finch, Smith, Goraya, Harrison, Naughton, Grady, Hodder, Reilly and Yoong. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ana Renda, QW5hLlJlbmRhQGhlYWx0aC5uc3cuZ292LmF1
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.