 Johanna Carolina Sánchez-Castro1*
Johanna Carolina Sánchez-Castro1* Laura Pilz González1
Laura Pilz González1 Saidy Eliana Arias-Murcia2
Saidy Eliana Arias-Murcia2 Viviana Andrea Mahecha-Bermeo3
Viviana Andrea Mahecha-Bermeo3 Christiane Stock1
Christiane Stock1 Katherina Heinrichs1
Katherina Heinrichs1- 1Institute of Health and Nursing Science, Charité – Universitätsmedizin Berlin, Corporate Member of Freie Universität Berlin and Humboldt-Universität zu Berlin, Berlin, Germany
- 2Faculty of Nursing, Universidad El Bosque, Bogotá, Colombia
- 3Faculty of Humanities, Social Science and Education, Otto-von-Guericke-Universität Magdeburg, Magdeburg, Germany
Background and objective: Adolescents from Latin America and the Caribbean grow up in a context of social inequality, which diminishes their well-being and leads to impaired emotional-cognitive development. To understand the problem, it is important to synthesize the available research about it. This study aims to explore the knowledge about adolescents’ mental health in Latin America and the Caribbean exposed to social inequality.
Methods: A systematic scoping review was conducted encompassing a search in five databases (Medline, CINAHL, PsycINFO, Scopus, and LILACS) in June 2022. Articles of various typologies were included without time limit. After two rounds of screening, relevant data were manually extracted and synthesized into self-constructed themes using thematic analysis.
Results: Out of 8,825 retrieved records, 42 papers were included in the final review, with a predominance of quantitative approaches. The synthesis revealed two main analytical themes: (a) defining social inequality, wherein intersecting inequalities produce discrimination and determine conditions for social vulnerability; (b) social inequality and mental health, which highlights the association between socio-structural difficulties and emotional problems, amplifying vulnerability to mental ill health and poor mental health care.
Conclusion: The scientific evidence reveals that social inequality is related to impaired well-being and mental ill health on the one hand and a lack of access to mental health care on the other hand.
1 Introduction
Adolescents have different roles in society: on the one hand, they represent the development of countries as they will be the adults of tomorrow, so they are the workforce of the future and the caregivers of generations to come (1, 2). On the other hand, adolescence is portrayed as one of the most stressful phases in life (3, 4) because it is connected to many challenges, such as hormonal and physical changes (5, 6). In addition, the desire for independence, the establishment of an own identity, and/or the development of autonomy are also characteristics of this phase (6, 7).
In the construction of their different roles, adolescents are particularly sensitive to the social, economic, and cultural environment in which they grow up (8). Scientific evidence shows that the socioeconomic background of their countries affects adolescents’ life satisfaction and quality of life (9). As a result of an environment marked by poverty and discrimination, youths experience insecurity and hopelessness as well as the feeling of not having the necessary resources to fulfill their life projects (4, 10, 11). This social vulnerability, combined with the chaotic phase of adolescence, creates mental stress scenarios, and in this process, serious mental health problems may emerge (10, 12).
There is extensive evidence in the literature about how different aspects of social inequality are linked to mental health problems in adolescents. Studies conducted in Germany and Australia demonstrate that children and adolescents with low socioeconomic status (SES) and family difficulties have a higher risk of mental health problems (13, 14). Another study shows that adolescents in South Africa living in poverty face stressful situations that often lead to symptoms of depression and anxiety (15). In research involving Chinese adolescents, it was found that those with advantageous socioeconomic conditions such as social support and adequate financial resources show a better mental health status than less privileged adolescents (16).
In Latin America and the Caribbean, adolescents grow up in a context of social inequality, which affects people’s lives in different ways. One type of social inequality is economic inequality, which includes income and property (17, 18). Other forms of structural inequality hinder the fulfillment of human rights, the development of skills, educational and job-related opportunities, and autonomy (17, 18). Contexts marked by structural inequality – characterized by low income, unemployment, social exclusion as well as poor access to health services, education, and housing – undermine the quality of life and lead to discontent among the most vulnerable populations (17, 19). Especially among young people, inequality diminishes the possibilities to participate in society and to manage the transition to adulthood successfully, i.e., reaching their full potential and ultimately contributing to the improvement of society (1, 20). Thereby, social inequality allows for the violation of adolescents’ rights, especially in families with low SES (21).
So far, research on the association between social inequality and adolescents’ mental health has primarily focused on high-income countries (22, 23). Despite Latin America and the Caribbean being recognized as the region with the highest levels of inequality worldwide (24, 25), only one literature review has examined the association between socioeconomic inequality and mental disorders, covering the general population, including adults (26). This highlights a clear gap in the synthesis of the relationship between social inequality and mental health in adolescents from Latin America and the Caribbean.
Therefore, the present study aims to explore the available knowledge about the mental health of adolescents exposed to social inequality in Latin America and the Caribbean. It also aims at identifying the definitions of social inequality used in literature available on the topic. As a guide for reporting the results of this study, we used PRISMA Extension for Scoping Reviews (PRISMA-ScR) (27).
2 Methods
Due to the complexity and heterogeneity of the research topic and to account for the conceptual aim of this research, it was considered optimal to conduct a scoping review (28). We followed the six-stage scoping review framework proposed by the Joanna Briggs Institute (JBI) (28), which consists of the following stages: (1) identifying the research questions; (2) identifying potentially relevant studies; (3) study selection; (4) data extraction; (5) analysis of evidence; (6) presentation of the results. The detailed protocol of this study is available online (29).
2.1 Search strategy
The search structure was designed based on the PEO strategy (Population, Exposure, Outcome) (30). The population of interest is defined as adolescents born and living in Latin America and the Caribbean. Social inequality, serving as exposure, is defined as social difference in living conditions and essential services among different social groups, encompasses social exclusion, discrimination, power imbalances, migration or forced displacement, poverty, and violence (31). The outcome is the adolescents’ mental health, defined as the individual’s sense of well-being, self-efficacy, autonomy, and competence, along with the development of social relationships (32, 33).
The databases and keywords were determined with the support of an expert in Information Literacy Education/Systematic Reviews. We carried out searches in Medline (via OVID), CINAHL, PsycINFO, Scopus, and LILACS for articles resulting from primary research studies, systematic reviews, and reflection articles, including expert opinions on the subject in English, Spanish, and Portuguese. We did not limit our search by publication date. The search strings were adapted for the respective databases, but remained comparable. As an example, the full electronic search strategy for Medline is available in Appendix 1.
The following criteria were applied in selecting the literature included: 1. The aim of the study refers to adolescence, which extends from 10 to 19 years of age (34). However, we include samples exceeding this range as well as adult samples as long as the purpose of the study clearly relates to the situation of adolescents. 2. The study focuses on a population born and living in Latin America or the Caribbean. 3. The study explains or analyses the association of social inequality with adolescents’ mental health.
2.2 Study selection
All databases were searched on 30 June 2022. Afterwards, all records were imported into Endnote X9.3.3 (Clarivate Analytics) to find and eliminate duplicates. Subsequently, all remaining literature was uploaded to the online systematic review platform Rayyan Systems, Inc. for further screening, first title and abstract, then full-text. We employed a team approach in this stage: due to linguistic competence, two of the researchers screened the results in English and Spanish (JCSC and LPG) and two in Portuguese (SEAM and VAMB). Discrepancies between the reviewers were reconciled through direct discussion at each phase until consensus was achieved.
Further sources were identified through a backward literature search by reviewing the references cited in the articles included (28). The main researcher (JCSC) checked the additional titles for inclusion criteria, and those eligible were included in the data extraction and analysis phase. A team approach was not used for the screening of these articles as they came from papers already included in the review, which represented an indirect screening. In addition, previous discussions provided experience for single-author decision making at this stage.
2.3 Data extraction and analysis
Information from the included records was extracted into a charting table in Microsoft Excel by JCSC. The following data were extracted: author, year, country, type of article, aim, design, study population, method/data, assessed variables, limitations/bias, and key findings regarding the conceptualization of social inequality, mental health approach, and associations between social inequality and mental health in adolescents in Latin America and the Caribbean. Subsequently, the information in the charting table was summarized alongside the general information of the studies.
For the qualitative synthesis, a process of inductive thematic construction for scoping reviews was used, consisting of manually identifying and classifying relevant and recurring patterns in the extracted text segments. These patterns were then reorganized into themes, with descriptive sub-themes when necessary, by which we answer our research questions (35).
3 Results
3.1 Scope, nature, and distribution of literature
Figure 1 depicts the selection process (27, 36). The initial database search yielded 8,825 articles. After elimination of duplicates, 5,077 studies remained. The title and abstract screening resulted in 106 articles. A total of 101 articles was retrieved as full text, the respective screening resulted in the final count of 39 articles. Another three publications were added by manually scanning the references of the included publications. In the end, a total of 42 articles met the inclusion criteria.
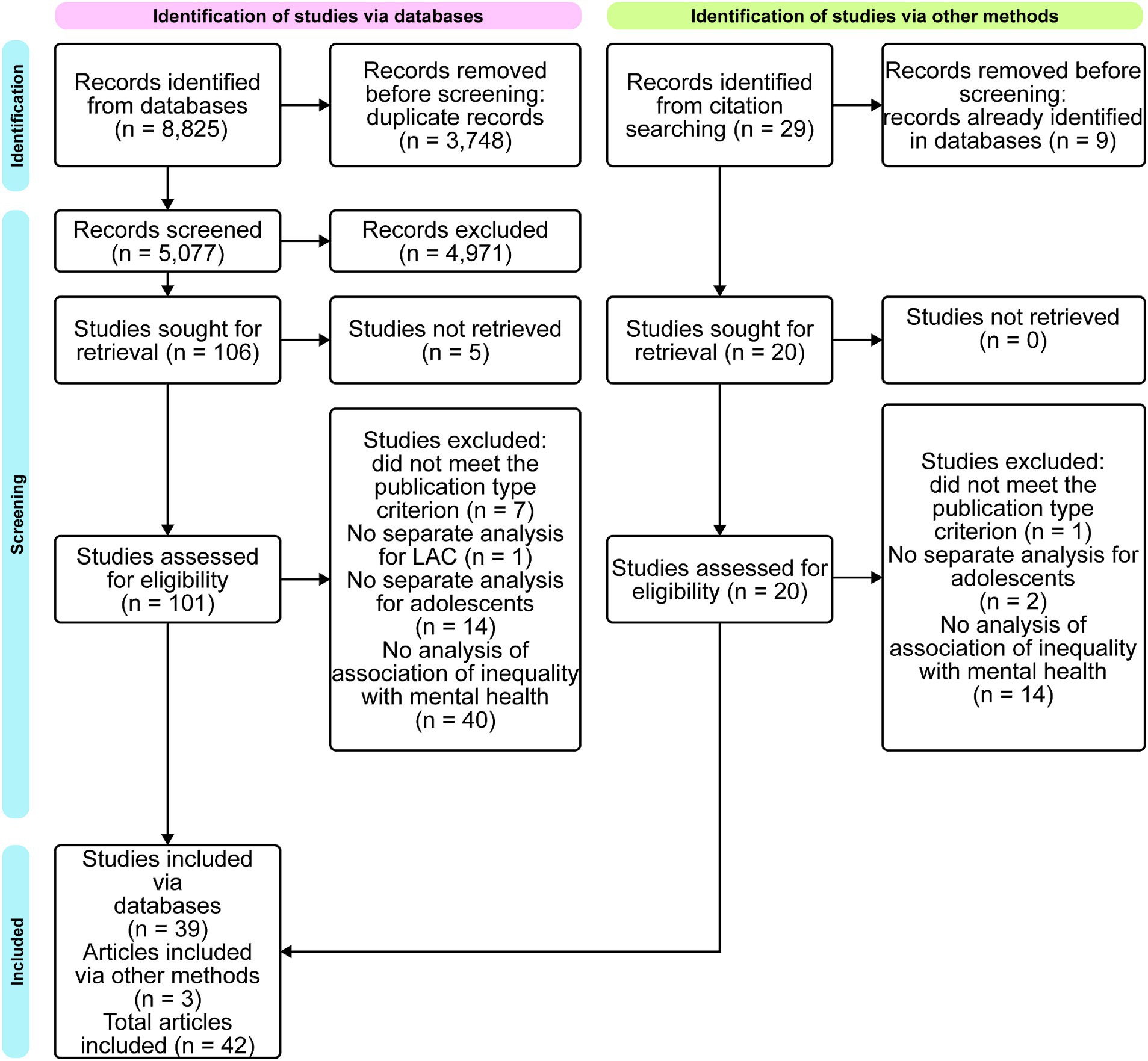
Figure 1. Flow diagram of selection process (designed on miro.com).
Supplementary Table S2 provides the characteristics of the 42 articles included. The articles were published between 1989 and 2022. When classifying the year of publication by decades, a greater number of publications was found in the period from 2011 to 2020 (n = 23). The majority of studies were conducted in Brazil (n = 19), with the remaining articles written by authors in Colombia (n = 5), Mexico (n = 5), Chile (n = 4), Ecuador (n = 4), Nicaragua (n = 2), Peru (n = 2), and one study included two countries, Colombia and Mexico. The predominant language was English (n = 28), followed by Spanish (n = 8) and Portuguese (n = 6). We identified 39 original articles, one letter to the editor, one description of the implementation of a health care project, and one review of the scientific literature. Among the original articles, most used a quantitative design (n = 29), 27 were cross-sectional studies, one cohort study, and one panel study. A total of eight studies were conducted qualitatively, and two followed a mixed methods design.
3.2 Thematic findings
As a result of the thematic analysis, two main themes emerged: 1. Defining social inequality; 2. Social inequality and mental health. For the second theme, the construction of sub-themes “social inequality threatening well-being,” “social inequality and mental ill health,” and “mental health care in social inequality environments” was significant to deepen its description.
3.2.1 Theme 1: Defining social inequality
Across the 42 studies included, we identified varied approaches in defining social inequality. The concepts mapped in this theme are presented in Figure 2. Social inequality seems to emerge from the interplay of ethnicity/race, migration, gender, and class. These are social categories that play a decisive role in shaping the social environment.
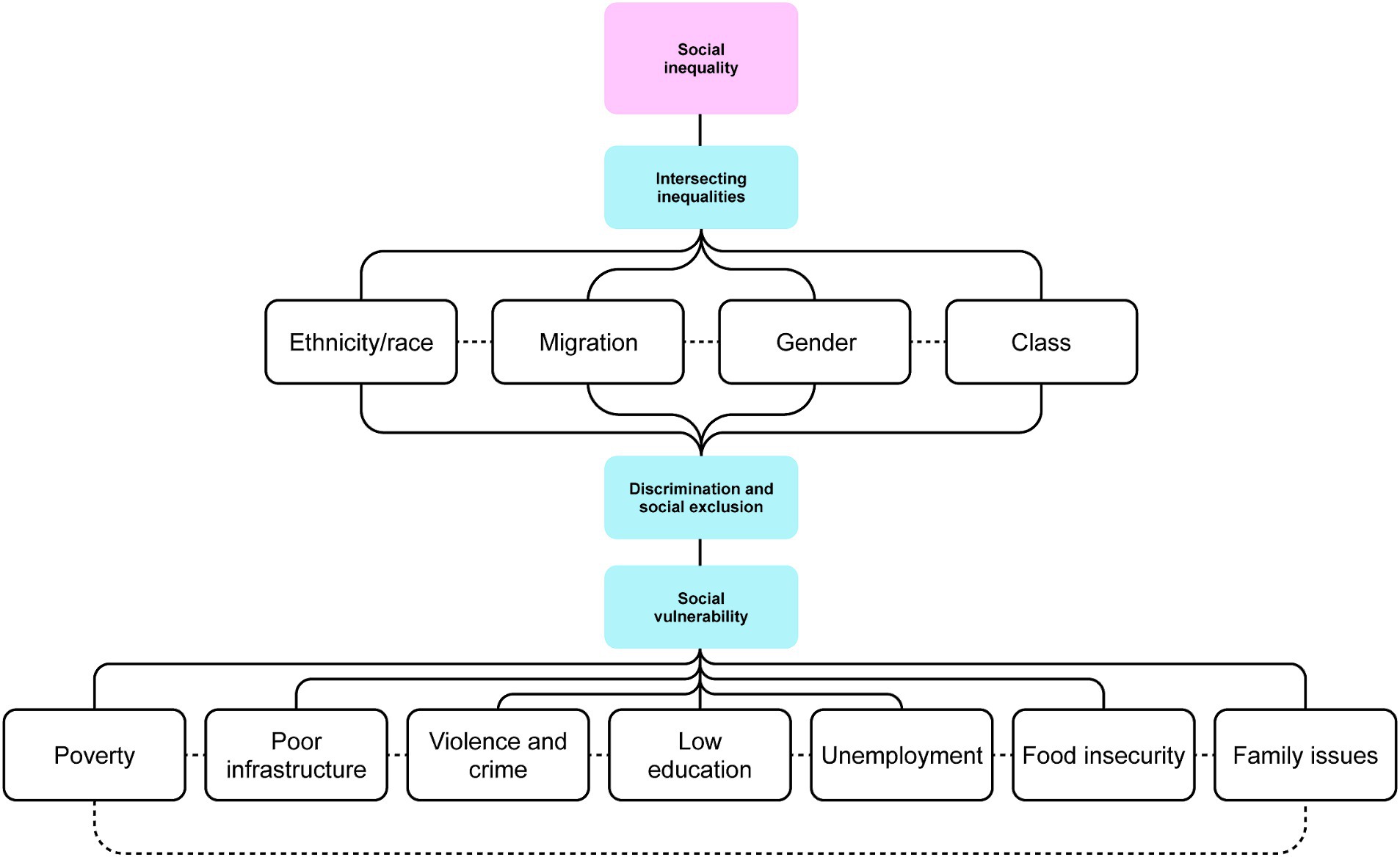
Figure 2. Theme 1: Defining social inequality (designed on miro.com).
Regarding ethnicity/race, it is described how populations with ethnic-racial background often experienced inequitable treatment (37, 38). One of the articles reports people being mostly white in the central areas of the cities, where socioeconomic conditions were favorable (better parental education and formal employment) (39). However, in populations of African descendants, lower levels of structured education and low income were prominent (40).
Another relevant phenomenon was migration due to various reasons, e.g., forced migration related to conflict and war, rural–urban migration, international migration that might be south–south among Latin American and Caribbean countries (between countries or regions located in the global South, involves people moving from one developing country to another) or south–north (from less economically developed regions to more economically developed countries) (41–45). Migrant population usually concentrated in the peripheral neighborhoods embodied by social vulnerability (42, 45).
Few studies investigated the role of gender in perpetuating social inequality. This research sheds light on traditional patriarchal norms (sometimes based on religious belief), exposing women to greater social and financial vulnerability (46, 47). When gender inequalities were conjoined with socioeconomic stratification (class), compelling evidence of social inequality emerged. For instance, among groups of economically disadvantaged adolescents who were obliged to work, female adolescents were usually engaged in unpaid activities such as stay-at-home care for younger siblings and household chores, while male adolescents were engaged in paid work (46, 47).
In several studies, the concept of SES was used to classify the participants according to their class, for example, based on goods and assets of the family, and/or schooling of the head of the household (37, 45, 48–56). The type of school such as municipal or subsidized school and paid school was also used to define the SES (57). In these papers, this classification was based on the location of the schools or households like low-, middle-, or high-income areas (58, 59).
In social environments where ethnicity/race, migration, gender, and/or class intersecting inequalities emerge, the affected population became marginalized, facing exclusion from state provisions and broader societal engagement (50, 60, 61). Notably, impoverished adolescents were distinctively affected by discrimination, social exclusion, and impediments in the realization of fundamental human rights (37, 61–65).
Furthermore, individuals facing intersecting inequalities were susceptible to social vulnerability, which manifests through challenging life circumstances (20, 40, 46, 60, 62, 64–70). Several articles highlight poverty as one of the most significant determinants of social vulnerability. Poverty has been widely associated with income shortfall. More recently, this concept has been expanded to the consumption of goods and services (71). However, the essential definition of poverty recognizes it as a fundamental life condition that affects social, economic, and environmental relations and determines the degree of social inequality (20, 39, 40, 47, 54, 57–59, 61, 62, 65, 68, 71–74).
Moreover, a number of studies have reported that poor infrastructure is characteristic for social vulnerability. Two studies point out that neighborhoods dominated by low social status presented hazardous life circumstances which included residences in a precarious state of repair and with insufficient rooms and thus hindering privacy, lack of piped water, sewage, and electricity as well as inadequate garbage collection (68, 75). Poor infrastructure is also related to lack of public transportation, besides leisure, education and health centers (39, 47, 58). Furthermore, in 11 articles, disadvantaged neighborhoods were characterized by high levels of insecurity (violence and accidents), drug trafficking, urban crime, police raids, assaults, robberies, and shootouts (20, 39, 42, 58, 59, 62, 63, 65, 67, 70, 76).
Social vulnerability was further manifested in the disparities in educational attainment among individuals from low, middle, and higher socioeconomic classes (39). The access to education among poor adolescents is erratic, reflected in their low school enrolment (20, 42, 46, 62, 65, 70, 71). This phenomenon also occurs in the parental (household head) generation among disadvantaged groups (40, 58, 66).
Similarly, numerous studies reported that caregivers’ loss of employment or engagement in low-status occupations, particularly within informal, illegal, or low-paying sectors, contributed to an increase in the family’s social vulnerability (20, 39, 40, 42, 58, 66, 70, 72). Furthermore, the need of increasing family income could push young individuals into premature employment, which could be harmful because it interferes with their education and personal development (46, 65, 76). Unemployment and economic risk lead to food insecurity and insufficiency and thus, to adolescents suffering from hunger (20, 43, 58).
Social vulnerability is also reflected in family issues. Three author teams identified family disruption as an indicator of socioeconomic disadvantage (40, 47, 67). Across 11 articles, social vulnerability within the family setting is described through various factors, including parental conflict and divorce, the presence of a stepfather, extended family or single-parent family, or mother-only households (39, 40, 42, 47, 58, 66). Two-parent families were expected to provide much more stability, with changes in the family structure considered as a risk factor (39, 58). Fragile families are also characterized by domestic violence and familial addiction (62, 63). In Latin America and the Caribbean, the breakdown of the family structure is common due to international migration, when adults leave their country of origin in search of employment and resources, leaving their children behind in the care of grandparents or other relatives (41, 44).
3.2.2 Theme 2: Social inequality and mental health
Across various studies, there was evidence that social inequality was negatively related to adolescents’ mental health. The concepts mapped in this theme are presented in Figure 3. Sub-themes were 1. Social inequality threatening well-being: how social inequality is related to the positive mental health approach, emphasizing concepts like well-being and quality of life. 2. Social inequality and mental ill health: focusing on a clinical standpoint, analyzing symptoms and/or mental health disorders that are prevalent among adolescents experiencing social inequalities. 3. Mental health care in social inequality environments: the lack of access to mental health care for adolescents facing social inequality.
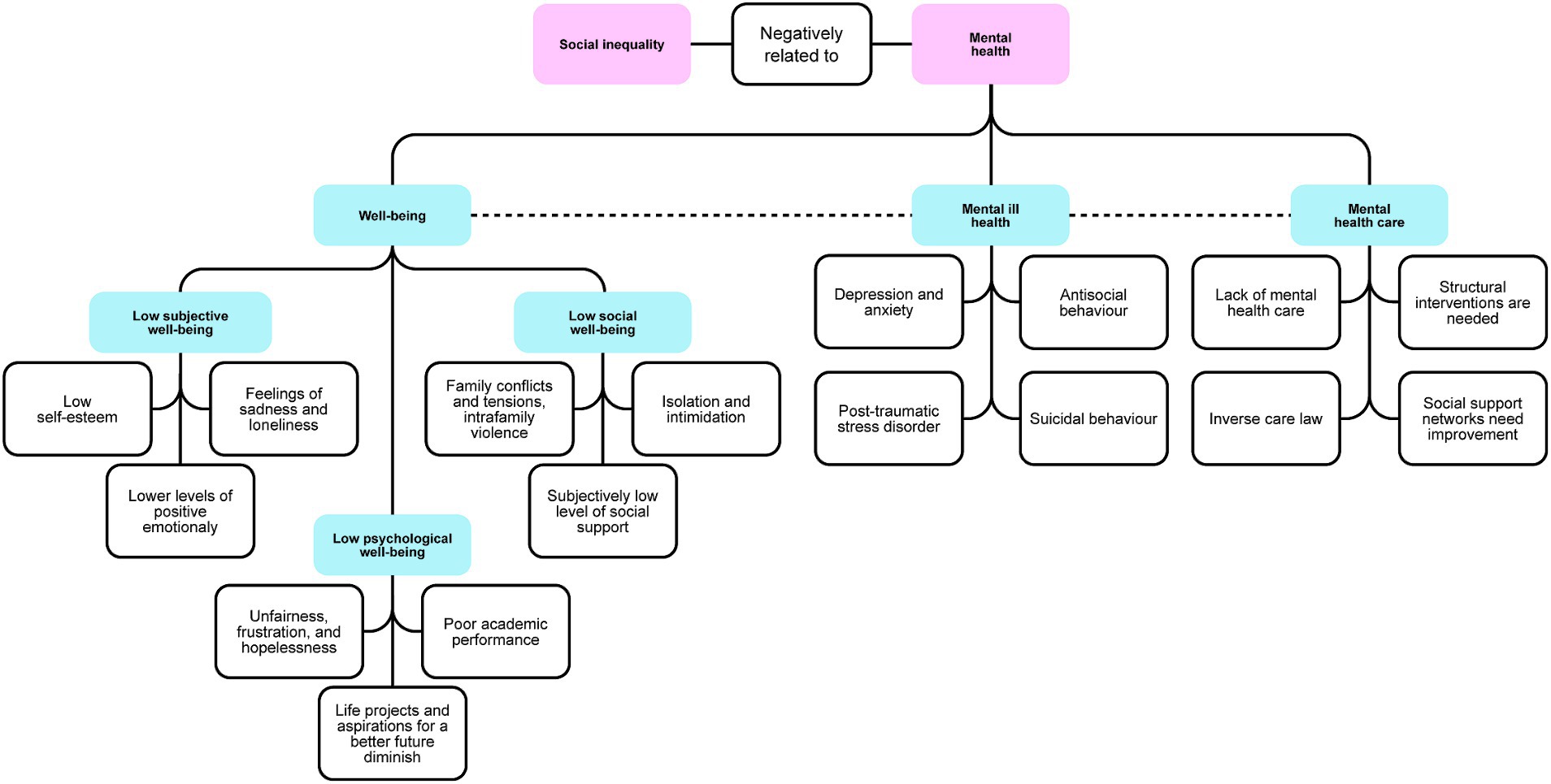
Figure 3. Theme 2: Social inequality and mental health (designed on miro.com).
3.2.2.1 Social inequality threatening well-being
A number of studies reported that well-being was a key component of mental health and was based on the degree that each individual assesses their life circumstances, depending on the possibility to cope with and assimilate life events (49, 59, 65). There are three types of well-being: subjective well-being, psychological or eudaemonic well-being, and social well-being (70). Here, we map the diverse ways in which social inequality poses challenges to overall well-being, encompassing the intricate interplay between the abovementioned types.
Some evidence showed that the higher the social inequality, the lower the well-being (49, 59, 65, 71, 73). We found research on how intersecting inequality relates to mental health. Two studies described how discrimination based on ethnicity/race generates negative emotional responses, thereby raising difficulties for the proper development of mental health (37, 38). In particular, two papers reported how adolescents who were left behind after their parents’ migration reported feelings of sadness, loneliness, and behavioral problems (41, 44). Moreover, patriarchal norms affected the communication and expression of feelings among female adolescents, especially in relation to sexuality, creating feelings of inferiority in young women (47). In this regard, a synergy could be seen between gender and SES, with women from schools in poorer social conditions having less self-esteem and stronger feelings of anxiety and sadness (57). In addition, adolescents’ quality of life was reduced by high levels of emotional stress resulting from the lack of social and economic resources, representing early adversity for youths (42, 52, 53, 55, 56, 59, 65, 71, 74). The result was social vulnerability characterized by stressful events and lower levels of positive emotionality (40, 53, 58, 74). Social vulnerability was associated with aggressive behavior (20, 65, 67) with the affected adolescents becoming victims or aggressors, perpetuating the vicious circle of violence (59).
Furthermore, increased poverty and perceived social exclusion were associated with lower self-esteem, perception of having less social support, and feelings of isolation and intimidation (37, 38, 58, 65) as well as feelings of unfairness, frustration, disrespect, anger, and hopelessness (42, 59, 69). In general, lack of opportunities and sometimes also of information hindered adolescents to follow their life projects and aspirations for a better future (better conditions than those of their caregivers) (65, 68, 71).
Besides, well-being was constantly threatened in hostile environments characterized by high levels of insecurity, violence, and crime as well as precarious infrastructure such as substandard housing, inadequate sanitation, and low quality of local services (48, 65, 67, 72, 77). Having computer or internet access was essential to perform academic activities, but not available to disadvantaged adolescents, leading to daily stress (50).
Socially vulnerable families were more likely characterized by family conflicts and tensions, intra-familiar violence, illnesses, single-parent families, large families, and unemployment, which were considered as stressful situations impairing adolescents’ mental health and quality of life (50, 54, 56, 63, 67). Likewise, low levels of parental education and little or no paid work might impose stress and reduce the mental stability of adolescents (49, 65, 77).
These life circumstances played a central role in adolescents’ academic performance as well: in schools where students had better socioeconomic conditions, their cognitive and psychosocial skills were better developed than in schools located in poor areas, generally public schools (60, 65). Although one study reported that educational work with adolescents could help them improve their self-esteem as they felt valuable to their family and community (76), this was different when measured in relation with other work circumstances. For instance, adolescents who could not study because they have to work or those not in education, employment, or training (NEET) are affected by social vulnerability that puts their mental health at risk since they are unable to meet social expectations, and this generates feelings of dissatisfaction with life (66). In addition, when economic difficulties force the youngest members of the family to work, they suffer from the responsibility to provide for a family far too early (46).
The situation of street adolescents was complicated in its own way, since most of them fled from the negative situation at home, thinking that in the street they would find autonomy and freedom to fulfill their life expectations (61). However, they ended up facing the sense of having lost family protection, resulting in feelings of shame and loss, exclusion, discrimination, and violence (61). In addition, they tended to develop inappropriate behaviors such as taciturnity, hostility, and mistrust (63).
3.2.2.2 Social inequality and mental Ill health
Mental health was often investigated from a psychopathological perspective. The common terms used were “mental ill health,” “common mental disorders” or “psychiatric disorders” in the literature in English and its equivalent translation in the other two languages (39, 42, 52, 64, 69, 71). Here, we present different associations found between social inequality and mental health problems.
Several studies reported that socioeconomic adversities were associated with mental ill health (40, 42, 69, 74, 75). Less formal education and parental unemployment were found as strong predictors of high rates of mental disorders (40, 50, 71, 72, 74). While one group of researchers identified that a significant portion of depressed adolescents were associated with functional families (54), in most studies, disruptions in the family structure played an important role in the vulnerability of internalizing and externalizing problems (40, 43, 50, 71, 72). Although in one of the studies, no significant difference between inner city and outer city areas was found (39), living in structurally deprived neighborhoods or in under-served rural areas was shown to be associated with psychosocial deprivation and thus, with the vulnerability to develop mental illness in two other papers (72, 74). Research in adolescents identified as NEET showed that they have greater odds of mental ill health in connection with disengagement from social, educational and working life (66).
Poverty and social vulnerability were associated with depressive and anxiety symptoms (20, 40, 51, 64). This was the case in the children of ragpickers who reported how the constant presence of garbage in their homes caused a feeling of constant discomfort with their environment (72). Furthermore, young people who experienced racial discrimination showed higher rates of depression compared to those who never felt discriminated (37). Working adolescents showed higher levels of anxiety or depressive symptoms than those who did not (46). Food insecurity and hunger were also associated with depressive symptoms in adolescents (43).
Further important mental health issues among poor adolescents were social problems, aggressive behavior, and antisocial behavior (ASB) (20, 40, 51, 67). In most cases, male adolescents were more likely to externalize their problems (39). Family conflict, in particular when parents used physical punishment as disciplinary strategies, confers risk for aggressive behavior and other externalizing disorders (40, 67). In addition to the psychiatric diagnoses mentioned above, it is important to remark the high probability of developing post-traumatic stress disorder (PTSD) in street adolescents who experienced extreme inequality and thus, vulnerability (62).
Some studies reported how the effects of social vulnerability described above can also trigger suicidal behavior (47, 56, 58, 72). Being a child of a ragpicker, racial discrimination, hunger, and low parental/guardian involvement are risk factors for self-injury (37, 43, 72). In addition, the absence of social support networks can be a risk factor for suicidal behavior (56, 66). One research on the socioeconomic and political determinants of suicide in adolescent females showed an association of turbulent political situations, traditional patriarchal norms, and the weakening of religions with suicidal behavior (47).
3.2.2.3 Mental health care In social inequality environments
Few studies investigated how families, health system, society and governments recognize and attend to adolescents’ mental health. Two studies reported that sometimes mental health issues were denied, e.g., by parents who reported that their children’s complaints were somatic in nature (20, 75). Furthermore, mental health care was shown to often be lacking in poor areas (40, 57, 65, 71). Likewise, lower income populations with higher morbidity received less than the minimum amount of mental health care, while privileged populations received excessive assistance – this is known as “inverse care law” (40, 48, 56, 57).
Finally, it was reported that improving adolescents’ mental health required major efforts at different levels. First of all, structural and systematic interventions were needed to address inequality and social vulnerability (44, 52). At the same level, it was necessary to promote dignified and well-paid employment for caregivers as well as strategies to increase family cohesion (40, 44, 65, 67). The development of social support networks in which adolescents and their families can trust was highly recommended (42, 45, 65, 70). For instance, the construction of youth organizations that motivate them to optimize the utilization of leisure time and achieve social inclusion removing discrimination of all kinds (37, 42, 44, 45, 70).
4 Discussion
In this scoping review, we described the concept of social inequality based on intersecting inequalities and social vulnerability of adolescents as well as the resulting life circumstances in Latin America and the Caribbean. Furthermore, this scoping review shows that social inequality in different countries is associated with negative emotions related to the low well-being of adolescents, harms their self-esteem, hampers the life projects viability, and fosters feelings of isolation. It is also revealed that these contexts are related to the presence of mental illness and suicidal behavior. In addition, we highlight the lack of access to health promotion, prevention, and care services in mental health for young people experiencing social vulnerability.
4.1 Defining social inequality
Through the thematic analysis of the articles included in this review, we examined the broad and complex concept of social inequality, revealing how important it is for Latin American and Caribbean societies, since this is considered to be a region with highest rates of inequalities compared with other areas in the world (24, 25, 67). The unequal conditions in which people in the region live have caused social injustice and difficulties for the population to have opportunities maintaining their quality of life and achieving individual and collective well-being (78).
To understand the complexity of the concept of social inequality, we consider the approach of intersectionality, which has been used in previous research to analyze social inequality in Latin America, for example by Baquero Melo (79). This analytical framework acknowledges the diversity inherent in human experiences by contemplating the overlapped dimensions of ethnicity/race, migration, gender, and class (79). In this approach, it is recognized that these categories are inseparable (31). Previous studies have reported that adolescents in Latin America growing up in a context that presents them obstacles to different levels, resulting in the accumulation and reinforcement of inequality (79, 80).
Social inequality is also closely linked to discrimination, with certain populations experiencing unfair and unfavorable treatment based on characteristics such as low SES, ethnicity/race, migrant background, or gender identity (Erin (81, 82)). In Latin America and the Caribbean, research indicates that disadvantaged communities encounter limited access to opportunities and resources due to the prejudices and stigmatization present in society. This means that social inequality and discrimination creates a self-reinforcing cycle that hinders the comprehensive human development of these marginalized populations (17, 80, 81). In this way, a profound acknowledgment arises concerning the intensified infringement upon the fundamental rights of certain groups (25, 83).
We raise a warning regarding unfavorable life circumstances specifically concerning poverty, poor infrastructure, violence and crime, limited educational opportunities, unemployment, food insecurity, and family issues. These factors have been found to have detrimental associations with adolescents’ mental health (84). Furthermore, given the lack of evidence in rural areas in this scoping review, future primary studies should focus on examining social inequality in these regions. It is essential to consider the challenges posed by limited access to healthcare, education, and other vital services in rural territories. By addressing these issues, we can gain valuable insights into social disparities and develop targeted interventions to tackle these challenges effectively. This realization poses a significant challenge in developing effective public policies and attention programs addressing the needs of the most vulnerable populations. The aim is to dismantle the underlying structures of social inequality and thus, to ensure equitable access to human rights and better living conditions for all (17).
It is acknowledged that consolidating all countries in the region into a single study of social inequality may oversimplify matters, considering the distinct historical, social, political, and cultural processes unique to each nation. However, gaining a general overview of the situation remains valuable, as it aids in understanding the regional profile and furnishes the essential knowledge needed for formulating comprehensive public policies. Moreover, it presents an opportunity to advance research by exploring the specific characteristics of each country in future studies.
4.2 Social inequality and mental health
The associations outlined herein are contextualized within Latin America and the Caribbean, where historical processes of colonization contribute to racial hierarchies, discrimination, and the marginalization of diverse ethnic groups (85). Furthermore, traditional gender roles prevail, with men often being the authoritarian heads of households, while women are relegated to secondary positions (86). Additionally, economic and political shifts, frequently accompanied by violence and criminality, have shaped the socio-economic situation of whole peoples and, in many cases, have driven migration both within and beyond national borders (87). It is therefore essential to comprehend mental health as an experience influenced by all the social phenomena inherent to the region. From this perspective, we can identify processes aimed at enhancing the living conditions and health of adolescents residing in the area (88).
In this scoping review, three distinctive sub-themes regarding the association between social inequality and mental health have emerged, delineated based on the various aspects examined in the included studies. The first sub-theme is based on the well-being and positive mental health approach, studies from this perspective refer to mental health in terms of quality of life, life satisfaction, and social relationships, explaining that mental health goes beyond diagnosing illnesses and requires attention based on health promotion and psychosocial work (89).
Well-being appeared as the prevailing concept frequently employed to define positive mental health within the scope of the included articles. Moreover, we found diverse well-being dimensions that contribute to a more nuanced understanding of the relationship between social inequality and mental health. First, subjective well-being was most commonly used by researchers and has two essential components: (a) the affective or emotional component which includes a balance between positive and negative affectivity or emotional responses and (b) the cognitive component characterized by the evaluation of global satisfaction with life (48, 57, 59, 73, 76). This scoping review highlights a consistent pattern indicating that adolescents residing in contexts characterized by social inequality present diminished levels of subjective well-being. To assess this phenomenon various instruments were used, encompassing evaluations of quality of life, self-esteem, and life satisfaction. The evidence indicates that social vulnerability serves as a potent stressor, fundamentally linked to the experience of reduced positive emotionality and self-esteem among adolescents not only in Latin America and the Caribbean but other social inequality contexts around the world (4, 90).
The second dimension is psychological or eudaemonic well-being. Adolescents facing conditions of poverty, poor infrastructure, limited educational opportunities, and unemployment confront significant challenges in fostering hope for the future and realizing their personal aspirations (68, 70). This is comparable to adolescents from other regions in the world. For example, a study among adolescents from families with financial difficulties in China found that adolescents’ future orientation is under threat (91). The results of this scoping review in a Latin American context supported it. In the included literature there is evidence on how the scarcity of socioeconomic resources and the adversities stemming from the intersecting inequalities of ethnicity/race, migration, gender, and class can impede the adolescents’ autonomy and freedom of choice concerning life goals or finding their own way for investing an effort (61, 70).
Thirdly, social well-being refers to the capacity to be part of society and to build social networks (70). The institutions of family, community, school, the state, informal support networks, and the relationships formed between their members are a key component of well-being and the fulfillment of human needs (61, 68). For adolescents, family is one of the most important protective factors for mental health through the dimensions of cohesion, affectivity, hierarchies or roles, communication, decision making, and conflict resolution (40, 43, 54). Family marks an important influence on the development of the individual’s personality (40, 44, 75). Consequently, households with adolescents experiencing family disintegration, domestic violence, economic hardships, and insufficient resources to fulfill fundamental nutritional and housing requirements pose a significant concern, not only for social well-being but also due to their connection with other dimensions of well-being. These adversities are closely linked to diminished levels of self-esteem, self-efficacy, and self-concept (92).
It is imperative to underscore the profound challenges faced by populations affected by intersectional discrimination. According to numerous research studies, these discriminatory experiences are strongly associated with negative feelings that significantly jeopardize mental well-being (38, 93, 94).
The second sub-theme was identified through an illness-centered approach, which concerns about manifestations of mental health disruptions, symptoms, and disorders (89). Numerous investigations have delved into mental health from a psychopathological standpoint. The terminologies employed in the included studies encompassed mental ill health, common mental disorders, or psychiatric disorders (39, 42, 52, 64, 69, 71). We opted to label our sub-theme as mental ill health to cover comprehensive evidence concerning mental diagnostics and problematic behaviors. Moreover, the concept of internalizing and externalizing problems was also used. Internalizing problems comprises symptoms of anxiety and depression, i.e., those problems are directed toward oneself (40, 46, 74). Externalizing problems comprise breaking of rules, disruptive, delinquent, ASB, and/or aggressive behavior, mainly toward others (20, 40, 46, 74).
The predominant mental disorders observed in adolescents are depression (43, 51, 53, 57) and anxiety (57, 66, 74). Through this scoping review, we have established an association between social inequality and the prevalence of these mental illnesses among adolescents in Latin America. This association is grounded in the understanding that socioeconomic adversity and discrimination give rise to concerns and stressors that adversely compromise well-being, thereby acting as significant risk factors for the onset of these disorders (11, 12, 95, 96).
The literature reviewed also found an association between social inequality and discrimination with ASB, a heterogeneous concept that encompasses behaviors as diverse as physical fighting, vandalism, stealing, status violation, and disobedience to adults. This association had also been considered by other authors, who reported that ASB in children and adolescents was associated with low SES (97).
Although not among the most prevalent mental health conditions in adolescents, this scoping review identified relevant information concerning the association between PTSD and social inequality experienced by street adolescents (62). PTSD appears when individuals or populations are exposed to highly distressing and traumatic events, such as violence or natural disasters, which jeopardize their physical and emotional well-being (98). Adolescents experiencing social inequality, characterized by highly unfavorable conditions, such as armed conflicts, extreme poverty, or gender-based violence, are at high risk for adverse mental health outcomes and the development of PTSD (98–100).
Finally, the included literature also assessed suicidal behavior among adolescents, which can be associated with psychological, especially affective, disorders (43, 47, 72) and comprises intentional self-harm, suicidal ideation (with or without planning), attempted suicide, and completed suicide (37, 43, 56, 58, 66). During adolescence, the influence of socioeconomic contexts can potentially contribute to inadequate emotional regulation and ineffective coping with stressful situations stemming from social inequality and discrimination. These factors may be associated with deliberate self-harm tendencies (96).
The third sub-theme that emerged from the thematic analysis refers to mental health care for populations facing social inequality. This aspect assumes crucial significance as it highlights how individuals in the most challenging life circumstances often confront scarcity of resources to effectively address their mental health (84, 95). However, this sub-theme addressed the type of interventions that would improve the mental health of adolescents in Latin America and the Caribbean, which respond to the development of strategies that firstly address the underlying causes of social inequality, such as social programs and poverty reduction programs (92, 101). Secondly, it is essential to build community spaces that seek to promote the well-being and quality of life of adolescents, with a focus on primary health care and mental health promotion (102, 103).
5 Strengths and limitations
The scoping review approach was convenient in our study because the available scientific literature was extensive. Hence, through this methodology, it was possible to map the information and include various aspects needed to answer the research question and understand how social inequality is associated with mental health. The methodology employed, based on JBI guidelines (28), facilitated the systematic development of each of the six research steps and provided an overview of the available literature on the topic of interest. It is noteworthy that within this methodological framework, risk of bias assessment and critical appraisal are not mandatory, as the primary aim is not to critically synthesize the evidence. Consequently, this scoping review does not comprise critical appraisal. Instead, evaluation of the studies focused on their relevance to the research aim in accordance with the inclusion criteria outlined at the outset. Furthermore, two authors of this study (JCSC and SEAM) are trained by JBI in the development of scoping reviews. Although the main author (JSCS) only has knowledge of Spanish and English, the fact that two authors (SEAM and VAMB) are fluent in Portuguese made it possible to break down the language barrier and broaden the scope of the review. Another strength of the methodology was the involvement of an expert in Information Literacy Education/Systematic Reviews in the construction of the search strategy.
However, it is important to highlight the limitations of this review. Firstly, in formulating the search strategy, terms such as “ethnicity/race”, “migration”, and “gender”, along with closely related terms, were omitted. This decision was made because including these terms redirected the results to issues not within the scope of this review. Consequently, only broader terms such as “social segregation”, “social exclusion”, and “social discrimination”, among others, were included. So most of the available information on intersecting social inequality refers to socioeconomic stratification/class. Thus, it is considered relevant to recognize and expand knowledge about the influence of these three variables related to social inequality and adolescent mental health. While our search strategy includes research from a wide range of countries in the Latin America and the Caribbean (n = 42), the final review revealed that the reported research originated from only seven countries (Brazil, Chile, Colombia, Ecuador, Mexico, Nicaragua, and Peru), with none of them considered part of the Caribbean. This highlights the lack of research in the field of social inequality and adolescent’s mental health in the Caribbean region, potentially attributed to limited resources or the stigma surrounding mental health in the area (104, 105). This study underscores the necessity for increased focus on primary research addressing this topic in Caribbean countries. The limited representation of countries may introduce potential bias and restrict the generalizability of our findings to other countries within the region.
The data extraction sheet was designed by one author (JCSC) and discussed among the team (SEAM, VAMB, and KH) before starting the extraction step. The data extraction process was carried out by only one author (JCSC). However, the information extracted from the Portuguese articles was verified by the fluent Portuguese authors (SEAM and VAMB). The thematic analysis was developed by one author (JCSC) and then discussed with three authors (LPG, SEAM, and VAMB) in order to arrive at the refined themes and sub-themes presented in this study. While relying on a single researcher for data extraction and thematic analysis facilitates focused exploration, it may limit diverse insights and overlook data nuances (106). Collaborative analysis involving multiple perspectives might have mitigated these limitations, fostering a more holistic and robust understanding of the data.
6 Conclusion
This scoping review represents an overview of the social inequality experienced by adolescents in Latin America and its relationship with mental health outcomes. Scientific literature establishes that social inequality operates at the intersection of ethnicity/race, migration, gender, and socioeconomic class. These dimensions, along with experiences of discrimination and social vulnerability, contribute to the perpetuation of inequality. This review reveals an association between social inequality and adverse mental health outcomes in adolescents. Adolescents exposed to intersecting inequalities reported low levels of well-being as well as higher levels of mental ill health and difficulties accessing mental health care.
In light of these compelling findings, we issue a resounding call to action to academia, government agencies, the private sector, and health systems across the region to develop strategic interventions that address the structural challenges of social inequality. By enhancing living conditions and improving the root causes threatening the well-being and mental health of young people, we can foster a more equitable and healthier adolescence.
Author contributions
JSCS: Conceptualization, Investigation, Formal Analysis, Writing – original draft, Writing – review & editing. LPG: Conceptualization, Investigation, Writing – original draft, Writing – review & editing. SEAM: Investigation, Writing – original draft, Writing – review & editing. VM-B: Investigation, Writing – review & editing. CS: Conceptualization, Writing – review & editing. KH: Conceptualization, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Acknowledgments
We thank to Corinna Dressler, PhD; Medical Library Charité – Universitätsmedizin Berlin for her support and advice in the development of the search strategy. Support by the German Academic Exchange Service (DAAD, doctoral scholarship for JCSC) is gratefully acknowledged.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2024.1342361/full#supplementary-material
References
1. Bergstrom, K, and Özler, B. Improving the well-being of adolescent girls in developing countries. Policy research working paper 9827’. World Bank Group. (2021). Available at: https://openknowledge.worldbank.org/server/api/core/bitstreams/d6340e66-f894-5c64-9026-b09ef6a9434a/content (Accessed June 14, 2023).
2. Fatusi, AO, and Hindin, MJ. Adolescents and youth in developing countries: health and development issues in context. J Adolesc. (2010) 33:499–508. doi: 10.1016/j.adolescence.2010.05.019
3. Assis, SG, Avanci, JQ, Silva, CMFP, Malaquias, JV, Santos, NC, and Oliveira, RVC. A representação social do ser adolescente: um passo decisivo na promoção da saúde [The social representation of being an adolescent: A decisive step in health promotion]. Ciênc Saúde Colet. (2003) 8:669–79. doi: 10.1590/S1413-81232003000300002
4. Safipour, J, Schopflocher, D, Higginbottom, G, and Emami, A. Socioeconomic factors and mental health of Swedish adolescents – a cross-sectional study among Stockholm high-school students aged 15–19 years. Vulnerable Child Youth Stud. (2013) 8:120–34. doi: 10.1080/17450128.2012.708462
5. Jaworska, N, and MacQueen, G. Adolescence as a unique developmental period. J Psychiatry Neurosci. (2015) 40:291–3. doi: 10.1503/jpn.150268
6. Sisk, LM, and Gee, DG. Stress and adolescence: vulnerability and opportunity during a sensitive window of development. Curr Opin Psychol. (2022) 44:286–92. doi: 10.1016/j.copsyc.2021.10.005
8. Devonald, M, Jones, N, and Youssef, S. “We have no Hope for anything”: exploring interconnected economic, social and environmental risks to adolescents in Lebanon. Sustain For. (2022) 14:2001. doi: 10.3390/su14042001
9. Frasquilho, D, Matos, MG, Salonna, F, Guerreiro, D, Storti, CC, Gaspar, T, et al. Mental health outcomes in times of economic recession: a systematic literature review. BMC Public Health. (2016) 16:115. doi: 10.1186/s12889-016-2720-y
10. Nepomuceno, BB, Cardoso, AAV, Ximenes, VM, Barros, JPP, and Leite, JF. Mental health, well-being, and poverty: a study in urban and rural communities in northeastern Brazil. J Prev Interv Community. (2016) 44:63–75. doi: 10.1080/10852352.2016.1102590
11. Reynolds, AD, and Crea, TM. Household stress and adolescent behaviours in urban families: the mediating roles of parent mental health and social supports. Child Fam Soc Work. (2016) 21:568–80. doi: 10.1111/cfs.12181
12. Vilhjalmsdottir, A, Gardarsdottir, RB, Bernburg, JG, and Sigfusdottir, ID. Neighborhood income inequality, social capital and emotional distress among adolescents: a population-based study. J Adolesc. (2016) 51:92–102. doi: 10.1016/j.adolescence.2016.06.004
13. Afroz, N, Kabir, E, and Alam, K. A latent class analysis of the socio-demographic factors and associations with mental and behavioral disorders among Australian children and adolescents. PLoS One. (2023) 18:e0285940. doi: 10.1371/journal.pone.0285940
14. Reiss, F, Meyrose, AK, Otto, C, Lampert, T, Klasen, F, and Ravens-Sieberer, U. Socioeconomic status, stressful life situations and mental health problems in children and adolescents: results of the German BELLA cohort-study. PLoS One. (2019) 14:e0213700–16. doi: 10.1371/journal.pone.0213700
15. Harrison, C, Loxton, H, and Somhlaba, NZ. Stress and coping: considering the influence of psychological strengths on the mental health of at-risk south African adolescents. Child Care Pract. (2021) 27:72–86. doi: 10.1080/13575279.2019.1604492
16. Guo, C, Tomson, G, Keller, C, and Söderqvist, F. Prevalence and correlates of positive mental health in Chinese adolescents. BMC Public Health. (2018) 18:263. doi: 10.1186/s12889-018-5133-2
17. Abramo, L, Cecchini, S, and Ullmann, H. Addressing health inequalities in Latin America: the role of social protection. Cienc. Saude Coletiva. (2020) 25:1587–98. doi: 10.1590/1413-81232020255.32802019
18. Economic Commission for Latin America and the Caribbean. The inefficiency of inequality. Santiago: United Nations publication (2018).
19. Lustig, N. ‘Desigualdad y descontento social en América Latina [Inequality and social discontent in Latin America]’. Nueva Sociedad | Democracia y política en América Latina. (2020). Available at: https://nuso.org/articulo/desigualdad-y-descontento-social-en-america-latina/ (Accessed September 14, 2022).
20. Lemos Couto, IS, Monzani da Rocha, M, and Botelho, AC. Prevalence of behavioral problems in adolescents in social vulnerability: assessment from a parental perspective. Paidéia. (2020) 30:3039. doi: 10.1590/1982-4327e3039
21. Souza, LB, Aragão, FBA, Cunha, JHS, and Fiorati, RC. Intersectoral actions in decreasing social inequities faced by children and adolescents. Rev Lat Am Enfermagem. (2021) 29:e3427. doi: 10.1590/1518-8345.4162.3427
22. Letourneau, NL, Duffett-Leger, L, Levac, L, Watson, B, and Young-Morris, C. Socioeconomic status and child development: a meta-analysis. J Emot Behav Disord. (2013) 21:211–24. doi: 10.1177/1063426611421007
23. Reiss, F. Socioeconomic inequalities and mental health problems in children and adolescents: a systematic review. Soc Sci Med. (2013) 90:24–31. doi: 10.1016/j.socscimed.2013.04.026
24. Amarante, V, Galván, M, and Mancero, X. Inequality in Latin America: a global measurement’. CEPAL Rev. (2016) 2016:25–44. doi: 10.18356/a7337ed5-en
25. Busso, M, and Messina, J. ‘The inequality crisis: Latin America and the Caribbean at the crossroads’. Inter-American Development Bank. (2020). Available at: https://publications.iadb.org/en/node/28743 (Accessed September 14, 2022).
26. Ortiz-Hernández, L, López-Moreno, S, and Borges, G. Desigualdad socioeconómica y salud mental: Revisión de la literatura latinoamericana [socioeconomic inequality and mental health: a review of the Latin American literature]. Cad Saude Publica. (2007) 23:1255–72. doi: 10.1590/S0102-311X2007000600002
27. Tricco, AC, Lillie, E, Zarin, W, O’Brien, KK, Colquhoun, H, Levac, D, et al. PRISMA extension for scoping reviews (PRISMA-ScR): checklist and explanation. Ann Intern Med. (2018) 169:467–73. doi: 10.7326/M18-0850
28. Peters, M, Godfrey, C, McInerney, P, Munn, Z, Tricco, A, and Khalil, H. ‘Chapter 11: scoping reviews. in JBI manual for evidence synthesis, eds. E. Aromataris and Z. Munn (eds) JBI. (2020). Available at: https://synthesismanual.jbi.global (Accessed June 29, 2022).
29. Sánchez Castro, JC, Pilz González, L, Stock, C, and Heinrichs, K. Mental health among adolescents exposed to social inequality in Latin America and the Caribbean: a scoping review protocol. Figshare. (2022) 2022:4286. doi: 10.6084/m9.figshare.21614286.v1
30. Munn, Z, Stern, C, Aromataris, E, Lockwood, C, and Jordan, Z. What kind of systematic review should I conduct? A proposed typology and guidance for systematic reviewers in the medical and health sciences. BMC Med Res Methodol. (2018) 18:5. doi: 10.1186/s12874-017-0468-4
31. Therborn, G. The killing fields of inequality. Int J Health Serv. (2012) 42:579–89. doi: 10.2190/HS.42.4.a
32. Restrepo, ODA, and Jaramillo, EJC. Concepciones de salud mental en el campo de la salud pública [Conceptions of mental health in the field of public health]. Rev Facult Nacl Salud Pública. (2012) 30:202–11. doi: 10.17533/udea.rfnsp.10764
33. Ruiz Eslava, L. La salud mental vista desde la medicina social latinoamericana [Mental health as seen from the perspective of Latin American social medicine]. Rev Investig Seguridad Soc Salud. (2009) 11:131–42. doi: 10.13140/RG.2.2.23757.87520
34. World Health Organization. Health for the world’s adolescents: A second chance in the second decade. Geneva: World Health Organization (2014).
35. Levac, D, Colquhoun, H, and O’Brien, KK. Scoping studies: advancing the methodology. Implement Sci. (2010) 5:69. doi: 10.1186/1748-5908-5-69
36. Page, MJ, Moher, D, Bossuyt, PM, Boutron, I, Hoffmann, TC, Mulrow, CD, et al. PRISMA 2020 explanation and elaboration: updated guidance and exemplars for reporting systematic reviews. BMJ. (2021) 372:160. doi: 10.1136/bmj.n160
37. Santana, V, Almeida-Filho, N, Roberts, R, and Cooper, SP. Skin colour, perception of racism and depression among adolescents in urban Brazil. Child Adolesc Mental Health. (2007) 12:125–31. doi: 10.1111/j.1475-3588.2007.00447.x
38. Sladek, MR, Umaña-Taylor, AJ, Oh, G, Spang, MB, Tirado, LMU, Vega, LMT, et al. Ethnic-racial discrimination experiences and ethnic-racial identity predict adolescents’ psychosocial adjustment: evidence for a compensatory risk-resilience model. Int J Behav Dev. (2020) 44:433–40. doi: 10.1177/0165025420912013
39. Cucchiaro, G, and Dalgalarrondo, P. Mental health and quality of life in pre-and early adolescents: a school-based study in two contrasting urban areas. Rev Bras Psiquiatr. (2007) 29:213–21. doi: 10.1590/S1516-44462007000300005
40. Sherman, BJ, Duarte, CS, and Verdeli, H. Internalizing and externalizing problems in adolescents from Bahia, Brazil. Int J Ment Health. (2011) 40:55–76. doi: 10.2753/IMH0020-7411400304
41. Doesschate, TT, Quizhpe Peralta, A, Cañar Lojano, H, Fajardo, V, Flores, N, and Guachún, M. Psychological and behavioral problems among left-behind adolescents: the case of Ecuador. Rev Fac Cienc Méd Univ Cuenca. (2012) 30:16–29.
42. Harpham, T, Grant, E, and Rodriguez, C. Mental health and social capital in Cali, Colombia. Soc Sci Med. (2004) 58:2267–77. doi: 10.1016/j.socscimed.2003.08.013
43. Romo, ML, Abril-Ulloa, V, and Kelvin, EA. The relationship between hunger and mental health outcomes among school-going Ecuadorian adolescents. Soc Psychiatry Psychiatr Epidemiol. (2016) 51:827–37. doi: 10.1007/s00127-016-1204-9
44. Saad, E, Saad, J, Cueva, E, and Hinostroza, W. Causas socioeconómicas de la migración en el Ecuador y su impacto en la adolescencia [Socio-economic causes of migration in Ecuador and its impact on adolescence]. Rev Tecnol ESPOL. (2004) 17:281–99.
45. Webb, A, and Alvarez, P. Counteracting victimization in unequal educational contexts: Latin American migrants, friendship dynamics in Chilean schools. Equity Excell Educ. (2018) 51:416–30. doi: 10.1080/10665684.2019.1582377
46. Bordin, IA, Pires, IH, and Paula, CS. Lifetime paid work and mental health problems among poor urban 9-to-13-year-old children in Brazil. Sci World J. (2013) 2013:1–7. doi: 10.1155/2013/815218
47. Herrera, A, Dahlblom, K, Dahlgren, L, and Kullgren, G. Pathways to suicidal behaviour among adolescent girls in Nicaragua. Soc Sci Med. (2006) 62:805–14. doi: 10.1016/j.socscimed.2005.06.055
48. Alfaro-Inzunza, J, Ramírez-Casas Del Valle, L, and Varela, JJ. Notions of life satisfaction and dissatisfaction in children and adolescents of low socioeconomic status in Chile. Child Indic Res. (2019) 12:1897–913. doi: 10.1007/s12187-018-9618-4
49. Silva, RA, Horta, BL, Pontes, LM, Faria, AD, Souza, LDM, Cruzeiro, ALS, et al. Bem-estar psicológico e adolescência: fatores associados [Psychological well-being and adolescence: associated factors]. Cad Saude Publica. (2007) 23:1113–8. doi: 10.1590/S0102-311X2007000500013
50. Barcelata Eguiarte, BE, Durán Patiño, C, and Lucio Gómez-Maqueo, E. Valoración subjetiva de los sucesos de Vida estresantes en dos grupos de adolescentes de zonas marginadas [Subjective assessment of stressful life events in two groups of adolescents from low-income neighborhoods]. Salud Ment. (2012) 35:513–20.
51. Souza, LD d M, Silva, RS, Godoy, RV, Cruzeiro, ALS, Faria, AD, Pinheiro, RT, et al. Sintomatologia depressiva em adolescentes iniciais: estudo de base populacional [Depressive symptomatology in early adolescents: population-based study]. J Bras Psiquiatr. (2008) 57:261–6. doi: 10.1590/S0047-20852008000400006
52. Gajaria, A, Ravindran, AV, Castrillo, ME, Herrera Rodríguez, A, and Zaheer, J. Mental health of transitional aged youth in Nicaragua: perceptions and experiences of educators. Glob Public Health. (2020) 15:151–60. doi: 10.1080/17441692.2019.1648535
53. González-Forteza, C, Villatoro, J, Pick, S, and Collado, ME. El estrés psicosocial y su relación con las respuestas de enfrentamiento y el malestar emocional en una muestra representativa de adolescentes al sur de la ciudad de México: análisis según su nivel socioeconómico [Psychosocial stress and its relation with coping responses and emotional distress in a representative sample of adolescents of Mexico City: An analysis according to their socioeconomic level]. Salud Ment. (1998) 21:37–45.
54. Hinostroza-Gastelú, L, Huashuayo-Vega, C, Navarro-Gómez, S, Torres-Deza, C, and Matos-Retamoso, L. Dinámica familiar y manifestaciones de depresión en escolares de 13 a 15 años de edad [Family dynamics and manifestations of depression in 13-15 year-old schoolchildren]. Rev Enferm Herediana. (2011) 4:12–9.
55. Lucio, E, León, I, Durán, C, Bravo, E, and Velasco, E. Los sucesos de vida en dos grupos de adolescentes de diferente nivel socioeconómico [Life events in two groups of adolescents from different socio-economic backgrounds.]. Salud Ment. (2001) 24:17–24.
56. Serrano-Ruiz, CP, and Olave-Chaves, JA. Factores de riesgo asociados con la aparición de conductas suicidas en adolescentes [Risk factors associated with the appearance of suicidal behavior in adolescents]. MedUNAB. (2017) 20:139–47. doi: 10.29375/01237047.2272
57. Alvarado, R, Vera, CA, Román, E, Sayago, S, Soto, I, Pinto, R, et al. Descripción de desigualdades en dimensiones psicosociales y de salud mental en grupo de jóvenes estudiantes [Description of inequalities in psychosocial and mental health dimensions in a group of young students.]. Cuadernos Méd Soc. (2001) 42:14–21.
58. Raffaelli, M, Koller, SH, Cerqueira-Santos, E, and de Morais, NA. Developmental risks and psychosocial adjustment among low-income Brazilian youth. Dev Psychopathol. (2007) 19:565–84. doi: 10.1017/S0954579407070277
59. Varela, JJ, Fábrega, J, Carrillo, G, Benavente, M, Alfaro, J, and Rodríguez, C. Bullying and subjective well-being: a hierarchical socioeconomical status analysis of Chilean adolescents. Child Youth Serv Rev. (2020) 118:105398. doi: 10.1016/j.childyouth.2020.105398
60. Barros de Souza, L, Panúncio-Pinto, MP, and Fiorati, RC. Crianças e adolescentes em vulnerabilidade social: bem-estar, saúde mental e participação em educação [Children and adolescents in social vulnerability: well-being, mental health, and participation in education]. Cad Bras Ter Ocup. (2019) 27:251–69. doi: 10.4322/2526-8910.ctoao1812
61. Butler, UM. Freedom, revolt and “citizenship”: three pillars of identity for youngsters living on the streets of Rio de Janeiro. Childhood. (2009) 16:11–29. doi: 10.1177/0907568208101688
62. Pluck, G, Banda-Cruz, DR, Andrade-Guimaraes, MV, Ricaurte-Diaz, S, and Borja-Alvarez, T. Post-traumatic stress disorder and intellectual function of socioeconomically deprived “street children” in Quito, Ecuador. Int J Ment Heal Addict. (2015) 13:215–24. doi: 10.1007/s11469-014-9523-0
63. Scivoletto, S, da Silva, TF, and Rosenheck, RA. Child psychiatry takes to the streets: a developmental partnership between a university institute and children and adolescents from the streets of São Paulo, Brazil. Child Abuse Negl. (2011) 35:89–95. doi: 10.1016/j.chiabu.2010.11.003
64. Da Silva, TF, Cunha, PJ, and Scivoletto, S. High rates of psychiatric disorders in a sample of Brazilian children and adolescents living under social vulnerability—urgent public policies implications. Rev Bras Psiquiatr. (2010) 32:195–6. doi: 10.1590/S1516-44462010000200018
65. Viñas, F, Casas, F, Abreu, DP, Alcantara, SC, and Montserrat, C. Social disadvantage, subjective well-being and coping strategies in childhood: the case of northeastern Brazil. Child Youth Serv Rev. (2019) 97:14–21. doi: 10.1016/j.childyouth.2017.06.012
66. Benjet, C, Hernández-Montoya, D, Borges, G, Méndez, E, Medina-Mora, ME, and Aguilar-Gaxiola, S. Youth who neither study nor work: mental health, education, and employment. Salud Publica Mexico. (2012) 54:410–7. doi: 10.1590/S0036-36342012000400011
67. Curto, BM, Paula, CS, do Nascimento, R, Murray, J, and Bordin, IA. Environmental factors associated with adolescent antisocial behavior in a poor urban community in Brazil. Soc Psychiatry Psychiatr Epidemiol. (2011) 46:1221–31. doi: 10.1007/s00127-010-0291-2
68. Graham, C, and Pozuelo, JR. Do high aspirations lead to better outcomes? Evidence from a longitudinal survey of adolescents in Peru. J Popul Econ. (2022) 36:1099–137. doi: 10.1007/s00148-021-00881-y
69. Harpham, T, Snoxell, S, Grant, E, and Rodriguez, C. Common mental disorders in a young urban population in Colombia. Br J Psychiatry. (2005) 187:161–7. doi: 10.1192/bjp.187.2.161
70. Quintero-Jurado, J, and Ossa-Henao, Y. Agrupaciones comunitarias juveniles: Promoción de la salud mental y desarrollo de capacidades [community youth groups: mental mealth promotion and capacity building]. Trends Psychol. (2018) 26:1605–18. doi: 10.9788/TP2018.3-17En
71. Zimmerman, A, Lund, C, Araya, R, Hessel, P, Sanchez, J, Garman, E, et al. The relationship between multidimensional poverty, income poverty and youth depressive symptoms: cross-sectional evidence from Mexico, South Africa and Colombia. BMJ Glob Health. (2022) 7:e006960. doi: 10.1136/bmjgh-2021-006960
72. Etcheverry, GB, Pereira, EF, and Cordeiro, ML. Depressive symptoms and suicidal ideation in adolescents accompanying a parent in recyclable trash collection. Span J Psychol. (2014) 17:E13. doi: 10.1017/sjp.2014.13
73. Hallal, PC, Dumith, SC, Bertoldi, AD, Scalco, DL, Menezes, AMB, and Araújo, CL. Well-being in adolescents: the 11-year follow-up of the 1993 Pelotas (Brazil) birth cohort study. Cad Saude Publica. (2010) 26:1887–94. doi: 10.1590/S0102-311X2010001000004
74. Palomar-Lever, J, and Victorio-Estrada, A. Factors associated with psychological maladjustment of Mexican adolescents living in poverty. J Child Family Stud. (2016) 25:3511–22. doi: 10.1007/s10826-016-0523-5
75. Guenes De Oliveira, MF, and Meirelles Monteiro, E. Necessidades psicossociais do menor de baixa renda, na faixa etária de 10 a 15 anos [Psychosocial needs of low-income children aged 10-15 years old]. Rev Bras Enferm. (1989) 42:14–21. doi: 10.1590/S0034-71671989000100003
76. Arteche, AX, and Ruschel Bandeira, DR. Bem-estar subjetivo: um estudo com adolescentes trabalhadores [Subjective well-being: a study with working adolescents]. Psico USF. (2003) 8:193–201. doi: 10.1590/S1413-82712003000200011
77. Fukuda, CC, Araújo Garcia, K, and Matos Do Amparo, D. Concepções de saúde mental a partir da análise do desenho de adolescentes [Conceptions of mental health from the analysis of adolescents’ drawing]. Estud Psicol. (2012) 17:207–14. doi: 10.1590/S1413-294X2012000200003
78. Quijada, Y, Villagrán, L, Vaccari Jiménez, P, Reyes, C, and Gallardo, LD. Social inequality and mental health in Chile, Ecuador, and Colombia. Lat Am Perspect. (2019) 46:92–108. doi: 10.1177/0094582X18803682
79. Baquero Melo, J. Desigualdades superpuestas, capas de desigualdad e interseccionalidad: Consideraciones analíticas y aplicación al Caso colombiano [Overlapping inequalities, layers of inequality and intersectionality: analytical considerations and application to the Colombian case]. Anál Polít. (2017) 30:59–75. doi: 10.15446/anpol.v30n89.66217
80. Layton, ML, and Smith, AE. Is it race, class, or gender? The sources of perceived discrimination in Brazil. Latin Am Polit Soc. (2017) 59:52–73. doi: 10.1111/laps.12010
81. Beck, E. The uneven impacts of violence against women reform in Guatemala: intersecting inequalities and the patchwork state. Lat Am Res Rev. (2021) 56:20–35. doi: 10.25222/larr.636
82. Stensrud, AB. Settlers and squatters: the production of social inequalities in the Peruvian Desert In: M Ystanes and IÅ Strønen, editors. The social life of economic inequalities in contemporary Latin America: Decades of change. Cham: Springer International Publishing (2018). 231–52.
83. Abramo, L. La matriz de la desigualdad en América Latina: Avances y desafíos de cara al futuro [The matrix of inequality in Latin America: Progress and challenges ahead] In: D Filmus and L Rosso, editors. Las sendas abiertas en América Latina. Buenos Aires: CLACSO (2019). 99–136.
84. Kim, Y, Lee, S, Jung, H, Jaime, J, and Cubbin, C. Is neighborhood poverty harmful to every child? Neighborhood poverty, family poverty, and behavioral problems among young children. J Community Psychol. (2019) 47:594–610. doi: 10.1002/jcop.22140
85. Gomes da Conceicao, MCG. Biopolitics: slavery, racism and eugenics in Latin America. J Adv Res Soc Sci. (2020) 3:48–61. doi: 10.33422/jarss.v3i3.520
86. Mascayano, F, Tapia, T, Schilling, S, Alvarado, R, Tapia, E, Lips, W, et al. Stigma toward mental illness in Latin America and the Caribbean: a systematic review. Braz J Psychiatry. (2016) 38:73–85. doi: 10.1590/1516-4446-2015-1652
87. Almeida-Filho, N. Urbanization and mental health as a research problem in Latin America (with a focus on Brazil). Curr Opin Psychiatry. (2021) 34:293–8. doi: 10.1097/YCO.0000000000000695
88. Breilh, J. Critical epidemiology and the People’s health. New York: Oxford University Press (2021).
89. Titistar-Cruz, ED, Matabanchoy-Salazar, JM, and Ruíz-Bravo, OT. Dos enfoques de salud mental en docentes de Latinoamérica: una revisión sistemática [Two approaches to mental health in Latin American teachers: A systematic review]. Cult Educ Soc. (2022) 13:183–202. doi: 10.17981/cultedusoc.13.2.2022.10
90. Caicedo, M, and van Gameren, E. Desempleo y salud mental en la población de origen hispano en Estados Unidos: un análisis epidemiológico [unemployment and mental health in the Hispanic population in the United States: an epidemiological analysis]. Ciênc Saúde Colet. (2016) 21:955–66. doi: 10.1590/1413-81232015213.16592014
91. Chen, J, and Guo, X. Poverty stifles ambition: the role of self-efficacy and perceived social fairness in the future orientation of adolescents from financially disadvantaged families. Youth Soc. (2023) 56:263–82. doi: 10.1177/0044118X231163242
92. Karimli, L, Ssewamala, FM, and Neilands, TB. The impact of poverty-reduction intervention on child mental health mediated by family relations: findings from a cluster-randomized trial in Uganda. Soc Sci Med. (2023) 332:116102. doi: 10.1016/j.socscimed.2023.116102
93. Venegas León, CV, Pedrero Castillo, V, and Chepo Chepo, M. Discriminación racial y determinantes sociales de la salud en niños y niñas migrantes: revisión narrativa [Racial Discrimination and Social Determinants of Health in Migrant Children: A Narrative Review]. Rev Cien Salud Uninorte. (2023) 39:241–64. doi: 10.14482/sun.39.01.610.422
94. Régio, L, Barros, S, Ballan, C, Aguiar, C, Candido, BP, and Oliveira, MAF. El cuidado de niños y adolescentes negros con problemas de salud mental en la interseccionalidad entre género y raza [Caring for black children and adolescents with mental health problems in the intersectionality between gender and race]. Rev Lat Am Enfermagem. (2023) 31:e3941. doi: 10.1590/1518-8345.6058.3941
95. Ridley, M, Rao, G, Schilbach, F, and Patel, V. Poverty, depression, and anxiety: causal evidence and mechanisms. Science. (2020) 370:214. doi: 10.1126/science.aay0214
96. Robinson, K, Brocklesby, M, Garisch, JA, O’Connell, A, Langlands, R, Russell, L, et al. Socioeconomic deprivation and non-suicidal selfinjury in New Zealand adolescents: the mediating role of depression and anxiety. N Z J Psychol. (2017) 46:126–36.
97. Piotrowska, PJ, Stride, CB, Croft, SE, and Rowe, R. Socioeconomic status and antisocial behaviour among children and adolescents: a systematic review and meta-analysis. Clin Psychol Rev. (2015) 35:47–55. doi: 10.1016/j.cpr.2014.11.003
98. Juárez, F, and Guerra, Á. Características socioeconómicas y salud en personas pobres y desplazadas [Socio-economic characteristics and health in poor and displaced people]. Psicologia. (2011) 27:511–9. doi: 10.1590/S0102-37722011000400016
99. Jones, L, Hughes, M, and Unterstaller, U. Post-traumatic stress disorder (PTSD) in victims of domestic violence: a review of the research. Trauma Violence Abuse. (2001) 2:99–119. doi: 10.1177/1524838001002002001
100. Sarmiento Suárez, R. Trastorno de estrés postraumático, ansiedad y depresión en adolescentes expuestos al conflicto armado en Colombia 2005 - 2008 [Post-traumatic stress disorder, anxiety, and depression in adolescents exposed to the armed conflict in Colombia 2005 - 2008]. Medicina. (2016) 38:134–56.
101. Richter, M, and Dragano, N. Micro, macro, but what about meso? The institutional context of health inequalities. Int J Public Health. (2018) 63:163–4. doi: 10.1007/s00038-017-1064-4
102. Cuellar Rivas, LX. La Salud Mental, un verdadero problema de salud pública [Mental Health, a real public health problem]. Rev Colombiana Salud Libre. (2018) 13:5–8. doi: 10.18041/1900-7841/rcslibre.2018v13n1.4985
103. Stolkiner, AI, and Ardila Gómez, SE. Conceptualizando la salud mental en las prácticas: consideraciones desde el pensamiento de la medicina social/salud colectiva latinoamericanas [Conceptualising mental health in practice: considerations from Latin American social medicine/collective health thinking]. Vertex. (2012) 23:57–67.
104. Cloos, P. Health inequalities in the Caribbean: increasing opportunities and resources. Glob Health Promot. (2010) 17:73–6. doi: 10.1177/1757975909356626
105. Lacey, KK, Powell Sears, K, Crawford, TV, Matusko, N, and Jackson, JS. Relationship of social and economic factors to mental disorders among population-based samples of Jamaicans and Guyanese. BMJ Open. (2016) 6:e012870. doi: 10.1136/bmjopen-2016-012870
Keywords: adolescents, mental health, psychological phenomena, social discrimination, social inequality, social sciences, social vulnerability, well-being
Citation: Sánchez-Castro JC, Pilz González L, Arias-Murcia SE, Mahecha-Bermeo VA, Stock C and Heinrichs K (2024) Mental health among adolescents exposed to social inequality in Latin America and the Caribbean: a scoping review. Front. Public Health. 12:1342361. doi: 10.3389/fpubh.2024.1342361
Edited by:
Cyrille Delpierre, INSERM Public Health, FranceReviewed by:
Sagrario Gomez-Cantarino, University of Castilla La Mancha, SpainCara Booker, University of Essex, United Kingdom
Copyright © 2024 Sánchez-Castro, Pilz González, Arias-Murcia, Mahecha-Bermeo, Stock and Heinrichs. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Johanna Carolina Sánchez-Castro, am9oYW5uYS1jYXJvbGluYS5zYW5jaGV6LWNhc3Ryb0BjaGFyaXRlLmRl