 Edlayne Larissa Gretter Machado Pereira1
Edlayne Larissa Gretter Machado Pereira1 Isabella Braghin Ferreira1
Isabella Braghin Ferreira1 Roberta Brinholi Victorino2
Roberta Brinholi Victorino2 Susana Angélica Zevallos Lescano3
Susana Angélica Zevallos Lescano3 Rogério Giuffrida1
Rogério Giuffrida1 Louise Bach Kmetiuk4
Louise Bach Kmetiuk4 Alexander Welker Biondo5*
Alexander Welker Biondo5* Vamilton Alvares Santarém1
Vamilton Alvares Santarém1- 1Graduate College in Animal Sciences, University of Western São Paulo (UNOESTE), São Paulo, Brazil
- 2Medical School, University of Western São Paulo (UNOESTE), São Paulo, Brazil
- 3Institute of Tropical Medicine of São Paulo, University of São Paulo, São Paulo, Brazil
- 4Zoonoses Surveillance Unit, Municipal Secretary of Health, Curitiba, Brazil
- 5Graduate College of Cell and Molecular Biology, Federal University of Paraná (UFPR), Curitiba, Brazil
Introduction: Despite human toxoplasmosis and toxocariasis having been listed among the top six most neglected parasitic zoonoses worldwide, presenting similar associated risk factors and transmission routes, few studies have been conducted in pregnant women and the consequences of concurrent infection remain to be fully established. Accordingly, the present study has serologically assessed the co-infection and associated risk factors for Toxoplasma gondii and Toxocara spp. in pregnant women, assisted by the public Unified National Health System (SUS) in southeastern Brazil.
Materials and Methods: Blood samples were collected and tested for IgG antibodies against Toxoplasma gondii by chemiluminescence immunoassay and against Toxocara spp. by enzyme-linked immunosorbent assay (ELISA). An epidemiological questionnaire was applied to gather socioeconomic information to assess the risk factors associated with seropositivity to toxocariasis/toxoplasmosis by univariate analysis followed by logistic regression.
Results: Overall, seropositivity was 69/280 (24.6, 95% CI: 19.96–30.01) for T. gondii and 56/280 (20.0, 95% CI: 15.73–25.08) for Toxocara spp. Co-infection was observed in 25/280 (8.9, 95% CI: 6.12–12.85) pregnant women, with increased odds (OR: 3.3, CI 95%: 1.77–6.14, p = 0.0002). Logistic regression revealed that a higher educational level (high school or college) significantly reduced the likelihood of co-infection seropositivity, owning cats increased the odds of toxocariasis, and older pregnant women presented significantly higher T. gondii seropositivity.
Conclusion: Co-infection herein highlights the importance of educational programs in the prevention of toxocariasis and toxoplasmosis in pregnant women and other high-risk populations.
1 Introduction
Toxoplasmosis and toxocariasis, caused by the Toxoplasma gondii protozoan and Toxocara spp. nematodes, respectively, have been important parasitic zoonoses of public health concern (1). Both diseases have been highly associated with low socioeconomic conditions (2, 3), with a global overall prevalence of 19% for toxocariasis (4) and 36% for toxoplasmosis (5). Pregnant women have also been highly affected by both infections, with global seroprevalence of 1.9 and 32.9% for anti-T. gondii IgM and IgG, respectively (6), and toxocariasis prevalence of 6.4% worldwide, 7.4% in Brasília, central-western Brazil (7), 9.2% in the Shandong Province, eastern China (8), 14.5% in Caribbean countries (9), 17.2% in Athens and nearby Piraeus, Greece (10), and 21.2% in the Ilam Province, western Iran (11).
Although toxoplasmosis may be asymptomatic in approximately 50% of healthy immunocompetent adults, severe infection with devastating sequelae has been reported in immunocompromised individuals and neonates (12). Thus, pregnant women have been considered the most vulnerable group in need of healthcare attention to prevent and monitor toxoplasmosis infection (5). In addition, transplacental transmission of T. gondii may lead to fetal miscarriage or stillbirth, severe disease in living infants (3), and permanent injuries including neurological damage and blindness (13).
Toxocariasis agents have also been asymptomatic in most human infections, but serious health consequences (14) may occur, including hepatic (15), pulmonary (16), cardiac (17), and urinary (18) lesions in the visceral form, ocular impairment or vision loss (19, 20), and neurological disorders (21, 22). Although rare, congenital transmission of Toxocara spp. was reported to cause ocular lesions in a premature child in Argentina (23) and strabismus in a 5-week-old infant in the USA (24). Vertical transmission has been experimentally reproduced in a murine model for both Toxocara canis (25) and Toxocara cati (26).
Toxoplasmosis and toxocariasis have shared several associated risk factors, particularly due to low socioeconomic aspects (27). In addition to similar human organ targeting, both pathogens have been directly transmitted to the human hosts through the intake of raw or undercooked meat or viscera from intermediate hosts of T. gondii or paratenic hosts of Toxocara spp. (28) and through the ingestion of T. gondii sporulated oocysts (29) or infective Toxocara spp. eggs from soil, vegetables, and water (30, 31).
Despite the similarities of infection, transmission, and associated risks of toxoplasmosis and toxocariasis for pregnant women, the prevalence and impact of co-infection remain to be fully established. Accordingly, the present study has simultaneously assessed infection by T. gondii and Toxocara spp. and the risk factors associated with seropositivity in pregnant women assisted by the Public Health System in southeastern Brazil.
2 Materials and methods
2.1 Ethics statement
The present study was approved for research with human beings by the Ethics Committee at the University of Western São Paulo (UNOESTE), corroborated by the Brazilian National Health Council (protocol number 52817021.0.0000.5515).
For blood and data collection including socioepidemiological and socioeconomic information, individuals were informed about the survey and personal confidentiality. Participants formalized the authorization by signing a Free and Informed Consent Term (FICT), in compliance with the Brazilian National Health Council.
2.2 Study design
The present study was a cross-sectional serosurvey of anti-Toxocara spp. and anti-T. gondii antibodies (IgG) and the associated risk factors in pregnant women, assisted by the public Unified National Health System in southeastern Brazil.
2.3 Timeline and study area
The study was conducted from March to October 2022 in the city of Presidente Prudente, São Paulo state, southeastern Brazil, ranked 136th nationwide (top 2.4%) for population, with approximately 225,000 habitants, 146th (top 2.6%) for Gross Domestic Product - GDP, and 25th (top 0.4%) for Human Development Index - HDI (0.806), out of 5,570 Brazilian cities (32). Nonetheless, approximately 30% of inhabitants lived on half the minimum monthly wage (approximately US$ 245) at the time.
2.4 Sample size
The parameters to estimate the sample size were calculated based on a previous prevalence study of toxoplasmosis and toxocariasis in 280 pregnant women from southeastern Brazil, with the assumption of an expected co-infection rate of 3.2%, a 95% confidence interval, and 10% losses (33).
2.5 Blood sample collection and epidemiological information
All women who participated in the present survey voluntarily answered an epidemiological questionnaire and had blood samples collected to assess the presence of anti-T. gondii and anti-Toxocara spp. antibodies. Official consent forms were signed by adult pregnant women and the legal guardians of underage adolescents younger than 18 years old, as required by current Brazilian laws.
Blood sampling was performed by certified nurses from two prenatal reference centers at the City Secretary of Health of Presidente Prudente. A total of 10 mL was collected by venipuncture, placed into a tube with serum separator gel, and centrifuged at 800 × g for 5 min; the serum was then separated and kept at −20°C until laboratory processing.
The applied questionnaire gathered socioepidemiological and socioeconomic information to assess the associated risk factors for toxocariasis and toxoplasmosis (Table 1).
Table 1. Gathered information for assessing the potential exposure and associated risk factors for toxocariasis and toxoplasmosis.
Subjects were excluded from the present study if they failed to present a medical request for prenatal blood examination or refused to voluntarily sign the FICT provided by the researchers.
2.6 Serological tests
Detection of anti-Toxoplasma gondii antibodies (IgG) was performed during prenatal care by chemiluminescence microparticle immunoassay using a commercial kit test (Ortho-Clinical Diagnostics, Illkirch-Graffenstaden, France), performed in two city reference centers for the prenatal diagnosis of toxoplasmosis. Anti-Toxocara spp. antibodies (IgG) were detected using an in-house indirect enzyme-linked immunosorbent assay (ELISA) through antigen excretion and secretion (TES) of Toxocara canis, following a protocol of pre-adsorption with Ascaris suum antigen (34) of each tested sample to minimize the potential cross-reactivity by exposure to Ascaris spp. A serum previously shown to be non-reactive (negative control) and a known reactive serum (positive control) were tested along with research samples on each plate. Absorbance was read at 492 nm, and antibody levels were expressed as reactivity indexes (RI), which were calculated as the ratio between the absorbance values of each sample and the cut-off value of the ELISA test. Testing of anti-Toxocara spp. antibodies was carried out at the Institute of Tropical Medicine of São Paulo, São Paulo state, Brazil.
2.7 Statistical analysis
All the statistical analyses were performed using R software (35). Seropositivity to toxocariasis and toxoplasmosis were independently compared using Pearson’s chi-square test. To access risk factors related to seropositivity, outcome data were initially categorized (variables shown in Table 1) and submitted to the univariate analysis (Pearson Chi-Squared Test or Fisher’s exact test). Variables presenting statistical significance lower than 0.20 in the univariate model were included in multivariate analyses (logistical regression) to assess the contribution of the risk/protective factors studied to the likelihood of seropositivity. To improve the final model, the predictor variables were tested for collinearity and the presence of influential values. From the regression coefficients for each predictor variable, odds ratio values were estimated per point and with a 95% confidence interval. The best-fitting model was considered the one that included significantly associated variables (p-value < 0.05) and minimized the Akaike Information Criterion (AIC) value. A significant level of 5% was adopted for all statistical tests.
3 Results
3.1 Characteristics of the studied population
The ages of pregnant women in the present study ranged from 15 to 43 years (median = 26); most were adults (267/280, 95.4%) and 13 were underage individuals (less than 18 years old). The majority of women (177/280, 63.0%) reported a family monthly income of up to 2 minimum wages, while more than half of adult women (145/267, 54.3%) declared having a work occupation. Pregnant women mostly (194/280, 69.3%) self-declared a history of previous pregnancy.
3.2 Prevalence and concurrent infection to Toxoplasma gondii and Toxocara spp.
Overall seropositivity (IgG) was observed in 69/280 (24.6, 95% CI: 19.96–30.01) women to T. gondii, and in 56/280 (20.0, 95% CI: 15.73–25.08) women to Toxocara spp., resulting in a 1.23 ratio. Concomitant seropositivity was verified in 25/280 (8.9, 95% CI: 6.12–12.85) individuals, with a high statistically significant association between Toxocara spp. and T. gondii seropositivity (OR: 3.3, CI 95%: 1.77–6.14, p = 0.0002).
3.3 Risk factors for Toxocara spp. infection and for Toxoplasma gondii infection
Risk factors associated with seropositivity to anti-Toxocara spp. antibodies (IgG) were gathered and analyzed (Table 2). Logistic regression (multivariate analysis) revealed that having a high school (OR: 0.26, p < 0.001) or college (OR: 0.23, p = 0.005) degree and the presence of a sewage system at home (OR: 0.08, p = 0.036) were protective factors, while owning cats was a risk factor and increased the odds (OR: 2.3, p = 0.033) of toxocariasis in pregnant women.
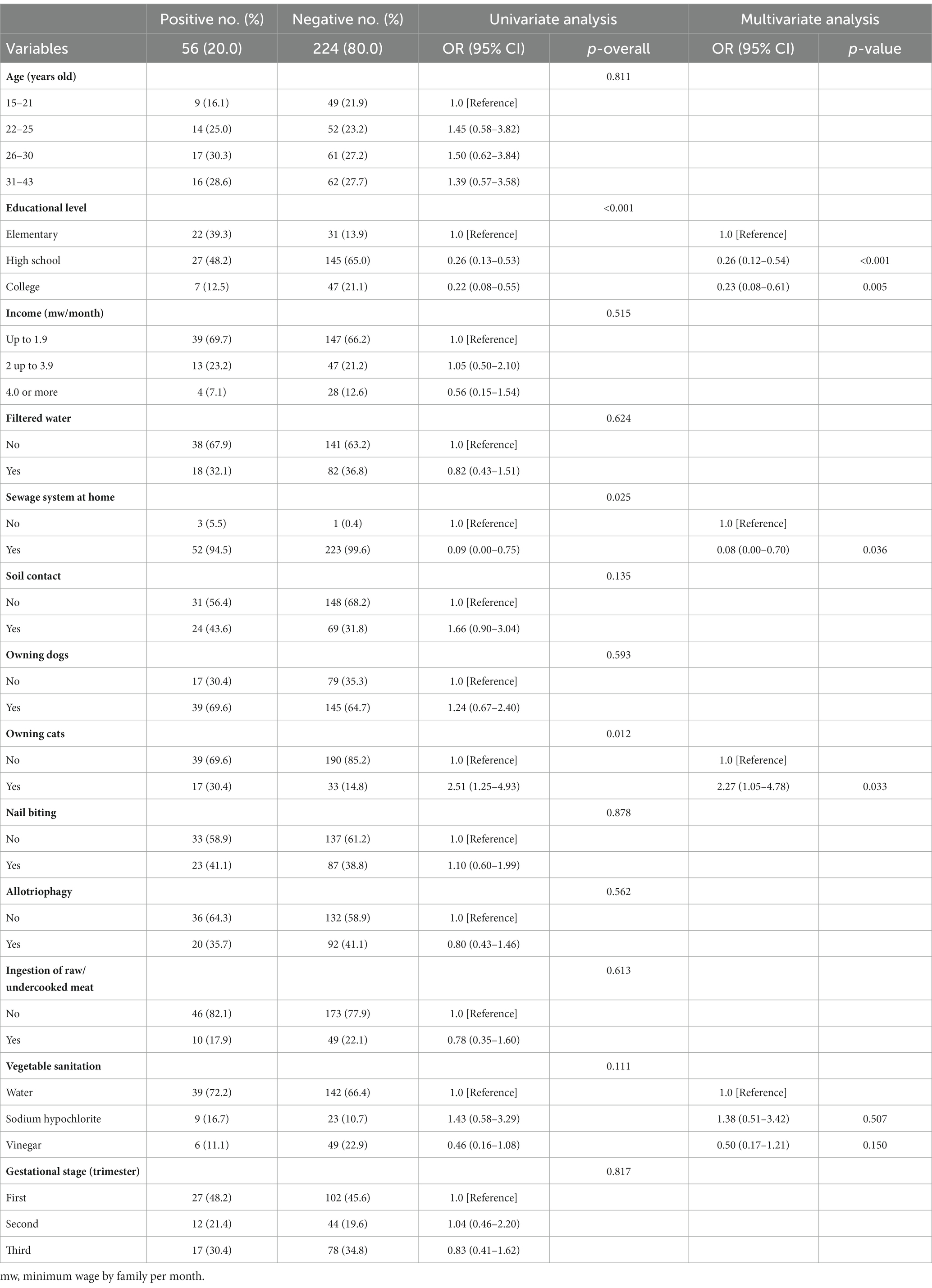
Table 2. Association of the presence of anti-Toxocara spp. antibodies (IgG) with characteristics of pregnant women (N = 280) assisted by the Public Health System in southeastern Brazil, by univariate and logistic multivariate regression analysis.
The final multivariate model for T. gondii seropositivity was calculated and presented (Table 3). Having a high school (OR: 0.44, p < 0.016) or college (OR: 0.17, p < 0.001) degree was a statistically significant protective factor for toxoplasmosis. In addition, the odds of T. gondii seropositivity were directly proportional to the age of pregnant women, considering the ages of 15 to 21 as a reference.
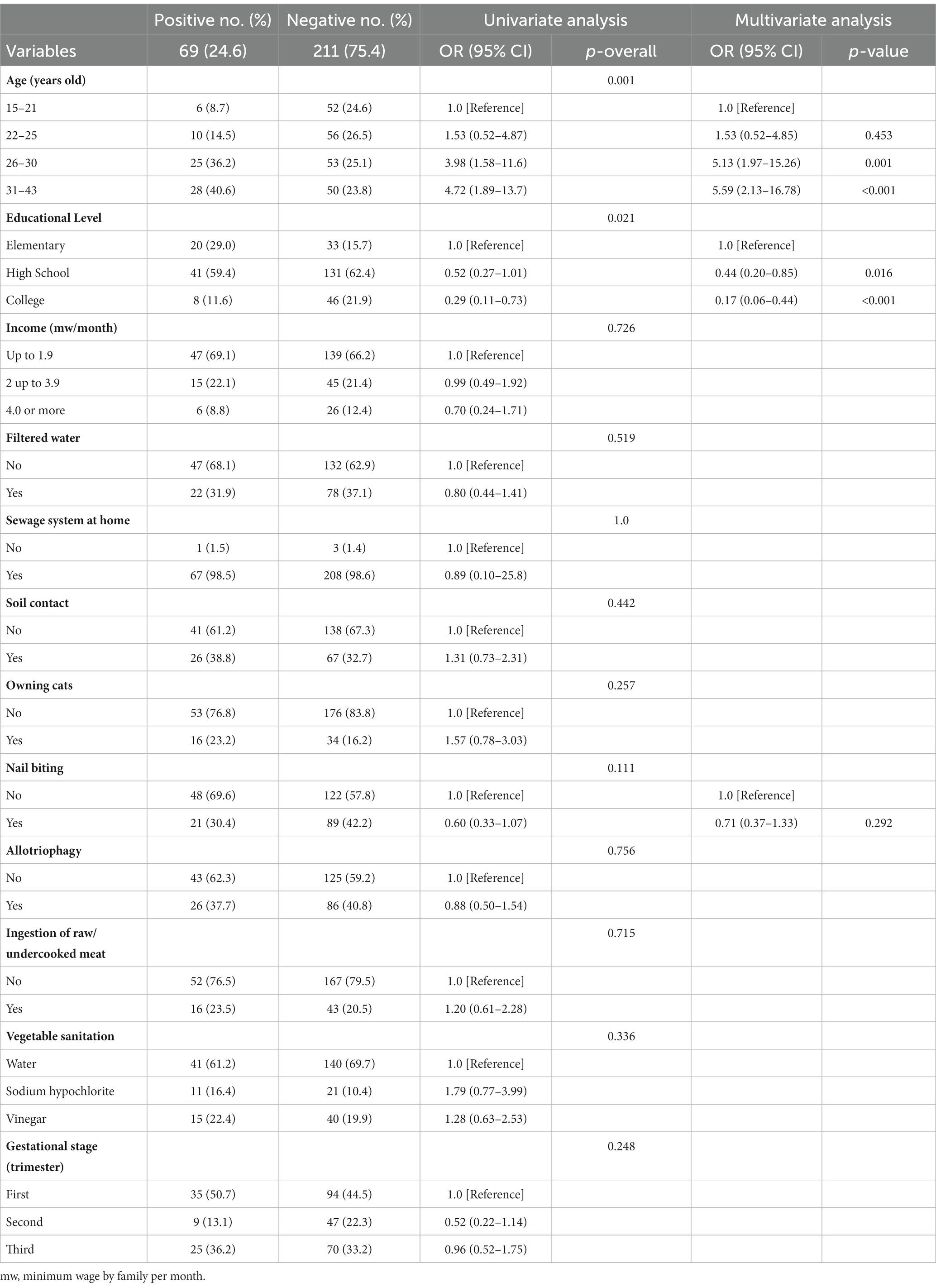
Table 3. Association between the presence of anti-Toxoplasma gondii antibodies (IgG) and characteristics of pregnant women (N = 280) assisted by the Public Health System in southeastern Brazil, by univariate and logistic multivariate regression analysis.
Previous miscarriage was not associated with a positive serological result to toxocariasis (OR: 0.6, CI 95%: 0.287–1.258, p = 0.238) nor toxoplasmosis (OR: 0.7, CI 95%: 0.376–1.422, p = 0.449). The ROC curve presenting the model’s accuracy was constructed (Supplementary Figure S1), with 70.3% for toxocariasis and 71.0% for toxoplasmosis, which were considered fair (36).
4 Discussion
Seroprevalence of Toxocara spp. and Toxoplasma gondii was observed in the present study, with a significant concurrent infection in pregnant women living in low-income areas of southeastern Brazil.
The 20.0% (56/280) seropositivity to toxocariasis herein was higher than the 6.4% found in southern Brazil (33) and the 7.2% observed in central-western Brazil (7), both in pregnant women assisted by the Public Health System (SUS), but similar to the 20.7% observed in a different group of pregnant women in Presidente Prudente (37), the municipality of the present study. Although all these low-income populations were assisted by SUS and presented disadvantaged socioeconomic characteristics, differences in seroprevalence may reflect local infrastructure, habits, and hygiene. Nonetheless, the results herein are similar to the overall global 19.0% toxocariasis seropositivity, which has been associated with lower income levels (4).
The 24.6% (69/280) seropositivity to T. gondii herein is lower than that of other recent Brazilian studies (last 10 years) involving pregnant women attended by SUS, ranging from 51.7% in southern Brazil (38) to 68.4% in northern Brazil (39). Although such variation could be related to the technique used for IgG detection, eating habits and water sources may play a role in transmission, as already reported (13). In addition, such seropositivity divergence between the two pregnant populations may be influenced by the socio-economic and climatic differences. As the northern Tocantins state presents higher rainfall and temperature, favoring the disease cycle, and the southern Paraná shows a very similar climate to the study setting herein, the socio-economic disparities between these two regions may be the main reason for seropositivity differences.
In the present study, a statistically significant concurrent 8.9% seropositivity (25/280, OR: 3.3) to anti-T. gondii and anti-Toxocara spp. differed from previous pregnant women serosurveys, with 7.9% (22/280) in southern Brazil (33), 13.2% (31/235) in China (40), and 9.5% (36/378) in western Iran (41). Co-infection has been shown in pregnant women, as IgG antibodies against T. gondii posed a risk (OR: 2.2, 95% CI: 1.7–2.9) of Toxocara spp. seropositivity in a general population survey of 13,509 individuals between 2011 and 2014 (42). Co-infection has also been reported in children, ranging from 3.2% (17/544) (43) to 27.4% (113/412) (27) in southern Brazil.
Herein, the ratio between toxoplasmosis/toxocariasis seroprevalence (1.23) was higher than 1. It was very close to the 1.17 observed in China (40) and lower than the 4.2 in western Iran (41). This finding possibly indicates increased exposure of pregnant women to T. gondii herein. In Iran, seropositivity in pregnancy was associated with contact with cats (41). In the present study, aging was associated with increased odds of T. gondii seropositivity, as shown in older pregnant women in northeastern (44, 45), southern (46, 47), northern (48), and central-western Brazil (49), Iran (50), and Saudi Arabia (51). This phenomenon has been attributed to lifelong antibody persistence and detection (52), but other causes have been indicated such as prolonged exposure to etiological agents, transmission routes, and lack of public awareness about prevention (50). Although increased odds of Toxocara spp. seropositivity has also been related to antibody persistence following exposure (53), no association between age and seropositivity was observed herein. This outcome differs from a previous study in the same area, in which adolescents were 2.6-fold more likely to be seropositive for toxocariasis than adult pregnant women (37), showing soil contact as an associated risk factor for toxocariasis among pregnant adolescents, but not for pregnant adults.
In Brazil, previous studies have reported risk factors associated with T. gondii infection during pregnancy, such as previous contact with cats in northern (54), northeastern (45, 55), and southern states (46, 56); socioeconomical vulnerability (55, 57), washing vegetables with untreated water (57), dog ownership (57), and homemade water ice consumption in northeastern states (57); living in urban area (48), frequent consumption of vegetables (58), and meat handling in northern states (54); living in rural areas in southern states (38, 47, 59, 60); gardening activities, contact with soil (48, 61), and raw milk consumption in southern and northern states (56, 58); consumption of chicken and meat in northeastern and northern states (57, 58). However, few studies involving co-infection with both parasites in pregnant women have been conducted, limiting the discussion of comparative risk factors. Thus, further retrospective and review studies are necessary to characterize the ratio of co-infection in different pregnant populations.
The similar transmission route of T. gondii and Toxocara spp., including consumption of raw or undercooked meat and the ingestion of embryonated eggs of Toxocara spp. and oocysts of T. gondii, may explain the co-infection in pregnant women observed in southern Brazil (33). Herein, logistic regression revealed that having a higher educational level was a protective factor against toxoplasmosis and toxocariasis co-seropositivity, corroborating with other serosurveys for T. gondii in pregnant women in Brazil (38, 55, 62) and other countries, such as Benin, Africa (63). Pregnant women with a higher educational level were associated with having toxoplasmosis-related knowledge (62), which may increase their awareness and understanding of the importance of hygiene habits to prevent diseases, including toxoplasmosis (64). Although the presence of a sewage system at home herein was also found to be a protective factor for toxocariasis but not for toxoplasmosis, having no public sewer service was previously associated with an increased risk of toxoplasmosis in southern Brazil (65).
In addition, owning cats increased the odds (OR: 2.3) of toxocariasis seropositivity herein, while no influence had previously been reported in that area (37). Despite the pregnant population of both studies being similar, the divergent outcome between studies may have been influenced by the higher number of pregnant women who declared their ownership of cats herein (n = 50) and previously (n = 38), which may have made it difficult to find statistically significant differences due to the low number of positive individuals. Likewise, owning cats has been reported as a risk factor for toxoplasmosis in some (66–69) but not all (27, 45, 70) serosurveys worldwide. Although seropositivity to toxoplasmosis herein was not influenced by the presence of cats in the household, increased odds of Toxocara spp. seropositivity herein due to cat contact should be considered as a potential disease risk when keeping cats at home.
Pregnant women may be directly infected by T. gondii and Toxocara spp. through the consumption of raw or undercooked meat or viscera (28), with high odds (OR: 5.7) of toxoplasmosis observed in pregnant women in northeastern Brazil (67). Although no study has found such a risk for toxocariasis and approximately one-fifth of the pregnant women herein declared the habit of consuming undercooked or raw meat, no association with toxocariasis or toxoplasmosis seropositivity was found. As previously stated, Presidente Prudente has been ranked in the top 2.4% of cities for population nationwide, the top 2.6% for Gross Domestic Product, and the top 0.4% for Human Development Index, with low commercial meat disease risk, mostly slaughtered, traded, and handled under rigorous state and federal sanitary inspections (37).
Pregnancy may be the highest risk time to be infected with T. gondii, as transplacental infection may lead to a wide variety of manifestations including miscarriage, stillbirth, and severe disease in living infants, despite mostly children being asymptomatic at birth (3). In addition, transplacental toxocariasis has been reported in one premature (23) and one 5-week-old (24) baby with ocular lesions. However, no study in pregnant women has found an association between miscarriage history and toxocariasis seropositivity in Brazil (7, 37, 71), including the present study.
A limitation of the present study is that no differentiation between acute and chronic phases was made, as no IgM or antibody avidity tests were performed for either pathogen. Nonetheless, infant mortality associated with congenital toxoplasmosis has been a persistent public health problem in Brazil (72). A surveillance protocol for gestational toxoplasmosis has been recently established by the Brazilian Minister of Health, including systematic serodiagnosis, compulsory notification, and educational and preventive activities coordinated by the Unified Health System (73). Given that serological tests may result in the overestimation of prevalence via false positive results, a second test should be recommended for further confirmation in epidemiological investigations of toxoplasmosis. Accordingly, a meta-analysis revealed that a combination of tests may improve the sensitivity and provide improved accuracy (74). Finally, as knowledge of risk factors for toxoplasmosis and toxocariasis may be helpful during early pregnancy (44), such educational and preventive activities should be taken into consideration as public health policies.
5 Conclusion
In conclusion, significant co-infection observed herein reinforces the importance of educational programs aimed at the prevention of toxocariasis and toxoplasmosis, particularly in pregnant women at high risk of exposure.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author.
Ethics statement
The present study was approved for research with human beings by the Ethics Committee at the University of Western São Paulo (UNOESTE), corroborated by the Brazilian National Health Council (protocol number 52817021.0.0000.5515). The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants or/and their legal guardians/next of kin.
Author contributions
EP: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Validation, Visualization, Writing – original draft, Writing – review & editing. IF: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Writing – original draft, Writing – review & editing. RV: Data curation, Investigation, Writing – original draft, Writing – review & editing. SL: Formal analysis, Investigation, Methodology, Writing – original draft, Writing – review & editing. RG: Data curation, Formal analysis, Investigation, Software, Validation, Writing – original draft, Writing – review & editing. LK: Investigation, Writing – review & editing. AB: Funding acquisition, Investigation, Writing – review & editing. VS: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Acknowledgments
The authors would like to thank Lígia Maria Delfino Caldeira and the crew of the Clinical Analysis Laboratory Dr. João Carlos Grigoli at Unoeste and the Mastellini Laboratory for their help with the samplings. They are also grateful to all participants who voluntarily took part in the present study. The authors also thank the Brazilian Higher Education Improvement Coordination (CAPES) for sponsoring the PhD fellowship (code 001) of IF.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2024.1340434/full#supplementary-material
References
1. CDC. Centers for Disease Control and Prevention. Parasites - Toxocariasis (also known as Roundworm Infect). (2023). Available at: https://www.cdc.gov/parasites/toxocariasis/index.html (Accessed August 30, 2023).
2. Chen, J, Liu, Q, Liu, G-H, Zheng, W-B, Hong, S-J, Sugiyama, H, et al. Toxocariasis: a silent threat with a progressive public health impact. Infect Dis Poverty. (2018) 7:59. doi: 10.1186/s40249-018-0437-0
3. Dubey, JP, Murata, FHA, Cerqueira-Cézar, CK, Kwok, OCH, and Villena, I. Congenital toxoplasmosis in humans: an update of worldwide rate of congenital infections. Parasitology. (2021) 148:1406–16. doi: 10.1017/S0031182021001013
4. Rostami, A, Riahi, SM, Holland, CV, Taghipour, A, Khalili-Fomeshi, M, Fakhri, Y, et al. Seroprevalence estimates for toxocariasis in people worldwide: A systematic review and meta-analysis. PLoS Negl Trop Dis. (2019) 13:e0007809. doi: 10.1371/journal.pntd.0007809
5. Rahmanian, V, Rahmanian, K, Jahromi, A, and Bokaie, S. Seroprevalence of Toxoplasma gondii infection: An umbrella review of updated systematic reviews and meta-analyses. J Fam Med Prim Care. (2020) 9:3848–55. doi: 10.4103/jfmpc.jfmpc_753_20
6. Bigna, JJ, Tochie, JN, Tounouga, DN, Bekolo, AO, Ymele, NS, Youda, EL, et al. Global, regional, and country seroprevalence of Toxoplasma gondii in pregnant women: a systematic review, modelling and meta-analysis. Sci Rep. (2020) 10:12102. doi: 10.1038/s41598-020-69078-9
7. Pereira, LC, Elefant, GR, Nóbrega, YM, Vital, T, Nitz, N, Gandolfi, L, et al. Toxocara spp. seroprevalence in pregnant women in Brasília, Brazil. Rev Soc Bras Med Trop. (2016) 49:641–3. doi: 10.1590/0037-8682-0106-2016
8. Cong, W, Zhang, X-X, Zhou, N, Yu, C-Z, Chen, J, Wang, X-Y, et al. Toxocara seroprevalence among clinically healthy individuals, pregnant women and psychiatric patients and associated risk factors in Shandong Province, eastern China. PLoS Negl Trop Dis. (2014) 8:e3082. doi: 10.1371/journal.pntd.0003082
9. Guo, F, Forde, MS, Werre, SR, Krecek, RC, and Zhu, G. Seroprevalence of five parasitic pathogens in pregnant women in ten Caribbean countries. Parasitol Res. (2017) 116:347–58. doi: 10.1007/s00436-016-5297-6
10. Papavasilopoulos, V, Bonatsos, G, Elefsiniotis, I, Birbas, C, Panagopoulos, P, and Trakakis, E. Seroepidemiological investigation of Toxocara canis in a female Greek pregnant population in the area of Athens. Clin Exp Obstet Gynecol. (2016) 43:384–7. doi: 10.12891/ceog2100.2016
11. Raissi, V, Sohrabi, Z, Getso, M, Raiesi, O, Hashemi Hafshejani, S, Shabandoust, H, et al. Risk factors and prevalence of toxocariasis in pregnant women and diabetic patients compared to healthy adults in Ilam province, western Iran. Exp Clin Sci J. (2018) 17:983–8. doi: 10.17179/excli2018-1630
12. Kota, AS, and Shabbir, N. Congenital Toxoplasmosis. Treasure Island, FL: StatPearls Publishing (2023) Available at: https://www.ncbi.nlm.nih.gov/books/NBK545228/.
13. Ahmed, M, Sood, A, and Gupta, J. Toxoplasmosis in pregnancy. Eur J Obstet Gynecol Reprod Biol. (2020) 255:44–50. doi: 10.1016/j.ejogrb.2020.10.003
14. Ma, G, Holland, CV, Wang, T, Hofmann, A, Fan, C-K, Maizels, RM, et al. Human toxocariasis. Lancet Infect Dis. (2018) 18:e14–24. doi: 10.1016/S1473-3099(17)30331-6
15. Gakosso, LGC, Baadi, F, Abakka, FZ, Basraoui, D, and Jalal, H. The visceral larva migrans caused by Toxocara canis: a case report. Pan Afr Med J. (2020) 36:150–5. doi: 10.11604/PAMJ.2020.36.150.24176
16. Kakimoto, M, Murata, M, Mitsumoto-Kaseida, F, Ogawa, E, Matsumoto, Y, Kusaga, A, et al. Toxocariasis suspected of having infiltrated directly from the liver to the lung through the diaphragm. Intern Med. (2019) 58:2737–41. doi: 10.2169/internalmedicine.2716-19
17. Ramos-López, N, Pérez-García, CN, Ferrera, C, Olmos, C, Paz-Arias, P, Boianelli, D, et al. Eosinophilic myocarditis due to Toxocara infection. Hell J Cardiol. (2022) 68:74–5. doi: 10.1016/j.hjc.2022.05.009
18. Ardekani, A, Roshanshad, A, Hosseini, SA, Magnaval, JF, Abdollahi, A, and Rostami, A. Toxocariasis-associated urinary system diseases: a systematic review of reported cases. Trans R Soc Trop Med Hyg. (2022) 116:668–72. doi: 10.1093/TRSTMH/TRAB177
19. Fata, A, Hosseini, SM, Woo, SJ, Woo, SJ, Zibaei, M, Berenji, F, et al. Frequency of Toxocara antibodies in patients clinically suspected to ocular toxocariasis, northeast of Iran. Iran J Parasitol. (2021) 16:305–11. doi: 10.18502/ijpa.v16i2.6312
20. Zibaei, M, Mahdavi, FS, Firoozeh, F, Hasani, H, and Bahadory, S. Ocular toxocariasis associated with blurred vision and visual impairment: Report of four cases. Iran J Parasitol. (2022) 17:118–23. doi: 10.18502/ijpa.v17i1.9034
21. Faure, G, Goulenok, T, Lariven, S, Dossier, A, Henry-Feugeas, M-C, Argy, N, et al. Eosinophilic meningomyelitis caused by Toxocara spp. in a migrant coming from La Reunion. J Travel Med. (2021) 28:taab075. doi: 10.1093/jtm/taab075
22. Chatzikonstantinou, S, Polymeropoulos, K, Stavrati, A, Konstantinidis, G, and Kazis, D. Toxocara canis infection manifesting as cerebral vasculitis: a case report. Neurol Sci. (2022) 43:4583–6. doi: 10.1007/s10072-022-06052-5
23. Maffrand, R, Ávila-Vázquez, M, Princich, D, and Alasia, P. Toxocariasis ocular congénita en un recién nacido prematuro. An Pediatría. (2006) 64:599–600. doi: 10.1157/13089931
24. Or, C, David, JA, Singh, M, Eustis, HS, Mazzulla, DA, Hypes, S, et al. A rare case of congenitally acquired ocular toxocariasis in a five week old infant. Ocul Immunol Inflamm. (2021) 29:1277–9. doi: 10.1080/09273948.2020.1866619
25. Schoenardie, ER, Scaini, CJ, Pepe, MS, Borsuk, S, de Avila, LF, Villela, M, et al. Vertical transmission of Toxocara canis in successive generations of mice. Brazilian. J Vet Parasitol. (2013) 22:623–6. doi: 10.1590/S1984-29612013000400030
26. Okada, N, Ooi, H-K, and Taira, K. Toxocara cati larval migration to mouse fetuses through transplacental infection. Vet Parasitol. (2021) 290:109350. doi: 10.1016/j.vetpar.2021.109350
27. Cabral Monica, T, Evers, F, Souza Lima Nino, B, Pinto-Ferreira, F, Breganó, JW, Ragassi Urbano, M, et al. Socioeconomic factors associated with infection by Toxoplasma gondii and Toxocara canis in children. Transbound Emerg Dis. (2022) 69:1589–95. doi: 10.1111/tbed.14129
28. Omonijo, AO, and Mukaratirwa, S. Knowledge and practices on consumption of free-range chickens in selected rural communities of KwaZulu-Natal, South Africa, with focus on zoonotic transmission of Toxoplasma gondii and Toxocara spp. Trop Anim Health Prod. (2022) 55:9. doi: 10.1007/s11250-022-03393-3
29. CDC. Centers for Disease Control and Prevention. Parasites - Toxoplasmosis (Toxoplasma Infect). (2018). Available at: https://www.cdc.gov/parasites/toxoplasmosis/epi.html (Accessed August 8, 2023).
30. Adeel, AA. Seroepidemiology of human toxocariasis in North Africa. Adv Parasitol. (2020) 109:501–34. doi: 10.1016/bs.apar.2020.01.023
31. Healy, SR, Morgan, ER, Prada, JM, and Betson, M. First report demonstrating the presence of Toxocara spp. eggs on vegetables grown in community gardens in Europe. Food Waterborne Parasitol. (2022) 27:e00158. doi: 10.1016/j.fawpar.2022.e00158
32. IBGE. Instituto Brasileiro de Geografia e Estatística. Pres Prudente. (2023). Available at: https://cidades.ibge.gov.br/brasil/sp/presidente-prudente/panorama.
33. Santos, PC, Telmo, PL, Lehmann, LM, Mattos, GT, Klafke, GB, Lorenzi, C, et al. Risk and other factors associated with toxoplasmosis and toxocariasis in pregnant women from southern Brazil. J Helminthol. (2017) 91:534–8. doi: 10.1017/S0022149X16000481
34. Elefant, GR, Shimizu, SH, Sanchez, MCA, Jacob, CMA, and Ferreira, AW. A serological follow-up of toxocariasis patients after chemotherapy based on the detection of IgG, IgA, and IgE antibodies by enzyme-linked immunosorbent assay. J Clin Lab Anal. (2006) 20:164–72. doi: 10.1002/jcla.20126
35. R Core Team. The R Project for Statistical Computing. (2023). Available at: https://www.r-project.org/ (Accessed July 21, 2023).
36. Nahm, FS. Receiver operating characteristic curve: overview and practical use for clinicians. Korean J Anesthesiol. (2022) 75:25–36. doi: 10.4097/kja.21209
37. de Oliveira, AP, Lescano, SZ, Giuffrida, R, Kmetiuk, LB, Dos Santos, AP, Dangoudoubiyam, S, et al. Serosurvey of anti-Toxocara antibodies and risk factors in adolescent and adult pregnant women of southeastern Brazil. PLoS Negl Trop Dis. (2021) 15:e0009571. doi: 10.1371/journal.pntd.0009571
38. Lopes-Mori, FMR, Mitsuka-Breganó, R, Bittencourt, LHFB, Dias, RCF, Gonçalves, DD, Capobiango, JD, et al. Gestational toxoplasmosis in Paraná State, Brazil: prevalence of IgG antibodies and associated risk factors. Braz J Infect Dis. (2013) 17:405–9. doi: 10.1016/j.bjid.2012.12.003
39. Gontijo da Silva, M, Clare Vinaud, M, and de Castro, AM. Prevalence of toxoplasmosis in pregnant women and vertical transmission of Toxoplasma gondii in patients from basic units of health from Gurupi, Tocantins, Brazil, from 2012 to 2014. PLoS One. (2015) 10:e0141700. doi: 10.1371/journal.pone.0141700
40. Yu, S-L, and Qian, C-Y. Seroprevalence of Toxoplasma gondii and Toxocara infections among pregnant women in Hangzhou City. Zhongguo Xue Xi Chong Bing Fang Zhi Za Zhi. (2020) 32:534–6. doi: 10.16250/j.32.1374.2020169
41. Raissi, V, Taghipour, A, Navi, Z, Etemadi, S, Sohrabi, Z, Sohrabi, N, et al. Seroprevalence of Toxoplasma gondii and Toxocara spp. infections among pregnant women with and without previous abortions in the west of Iran. J Obstet Gynaecol Res. (2020) 46:382–8. doi: 10.1111/jog.14184
42. Liu, EW, Elder, ES, Rivera, HN, Kruszon-Moran, D, Handali, S, and Jones, JL. Concurrent Seroprevalence of antibodies to Toxoplasma gondii and Toxocara species in the United States, 2011–2014. Clin Infect Dis. (2019) 68:712–3. doi: 10.1093/cid/ciy729
43. Marchioro, AA, Colli, CM, Ferreira, ÉC, Viol, BM, Araújo, SM, and Falavigna-Guilherme, AL. Risk factors associated with toxoplasmosis and toxocariasis in populations of children from nine cities in southern Brazil. J Helminthol. (2015) 89:428–32. doi: 10.1017/S0022149X14000212
44. Avelar, MV, Martinez, VO, Moura, DLde, Barros, IA, Primo, AADS, Duarte, AO, et al. Association between seroprevalence of IgG anti-Toxoplasma gondii and risk factors for infection among pregnant women in Climério de Oliveira Maternity, Salvador, Bahia, Brazil. Rev Inst Med Trop Sao Paulo (2017) 59:e90. doi: 10.1590/s1678-9946201759090
45. Oliveira, GMSde, Simões, JM, Schaer, RE, Freire, SM, Nascimento, RJM, Pinheiro, AMC M, et al. Frequency and factors associated with Toxoplasma gondii infection in pregnant women and their pets in Ilhéus, Bahia, Brazil. Rev Soc Bras Med Trop (2019) 52: doi: 10.1590/0037-8682-0250-2019,:e20190250
46. de Moura, FL, Amendoeira, MRR, Bastos, OMP, Mattos, DPBG, Fonseca, ABM, Nicolau, JL, et al. Prevalence and risk factors for Toxoplasma gondii infection among pregnant and postpartum women attended at public healthcare facilities in the City of Niterói, State of Rio de Janeiro, Brazil. Rev Soc Bras Med Trop. (2013) 46:200–7. doi: 10.1590/0037-8682-1613-2013
47. Antinarelli, LMR, Silva, MR, Guimarães, RJPS, Terror, MS, Lima, PE, Ishii, JSC, et al. Rural residence remains a risk factor for Toxoplasma infection among pregnant women in a highly urbanized Brazilian area: a robust cross-sectional study. Trans R Soc Trop Med Hyg. (2021) 115:896–903. doi: 10.1093/trstmh/traa153
48. dos Anjos Pinheiro Bogoevich Morais, R, Lima do Carmo, E, Carneiro Bichara, CN, Ramos dos Santos, B, Silva da Silveira, KW, and Marins Póvoa, M. Seroprevalence and risk factors associated with T. gondii infection in pregnant individuals from a Brazilian Amazon municipality. Parasite Epidemiol Control. (2020) 9:e00133. doi: 10.1016/j.parepi.2020.e00133
49. Avelar, JB, Silva, MG, Rezende, HHA, Storchilo, HR, Amaral, WN, Xavier, IR, et al. Epidemiological factors associated with Toxoplasma gondii infection in postpartum women treated in the public healthcare system of Goiânia, State of Goiás, Brazil. Rev Soc Bras Med Trop. (2018) 51:57–62. doi: 10.1590/0037-8682-0112-2017
50. Mizani, A, Alipour, A, Sharif, M, Sarvi, S, Amouei, A, Shokri, A, et al. Toxoplasmosis seroprevalence in Iranian women and risk factors of the disease: a systematic review and meta-analysis. Trop Med Health. (2017) 45:7. doi: 10.1186/s41182-017-0048-7
51. Alzaheb, R. Seroprevalence of Toxoplasma gondii and its associated risk factors among women of reproductive age in Saudi Arabia: a systematic review and meta-analysis. Int J Women's Health. (2018) 10:537–44. doi: 10.2147/IJWH.S173640
52. Garnaud, C, Fricker-Hidalgo, H, Evengård, B, Álvarez-Martínez, MJ, Petersen, E, Kortbeek, LM, et al. Toxoplasma gondii-specific IgG avidity testing in pregnant women. Clin Microbiol Infect. (2020) 26:1155–60. doi: 10.1016/j.cmi.2020.04.014
53. Bradbury, RS, and Hobbs, CV. Toxocara seroprevalence in the USA and its impact for individuals and society. Adv Parasitol. (2020) 109:317–39. doi: 10.1016/bs.apar.2020.01.035
54. da Rocha, ÉM, Lopes, CWG, Ramos, RAN, and Alves, LC. Risk factors for Toxoplasma gondii infection among pregnant women from the State of Tocantins, Northern Brazil. Rev Soc Bras Med Trop. (2015) 48:773–5. doi: 10.1590/0037-8682-0074-2015
55. Barbosa, IR, de Carvalho Xavier Holanda, CM, and de Andrade-Neto, VF. Toxoplasmosis screening and risk factors amongst pregnant females in Natal, northeastern Brazil. Trans R Soc Trop Med Hyg. (2009) 103:377–82. doi: 10.1016/j.trstmh.2008.11.025
56. Higa, LT, Araújo, SM, Tsuneto, L, Castilho-Pelloso, M, Garcia, JL, Santana, RG, et al. A prospective study of Toxoplasma-positive pregnant women in southern Brazil: a health alert. Trans R Soc Trop Med Hyg. (2010) 104:400–5. doi: 10.1016/j.trstmh.2010.01.006
57. Sroka, S, Bartelheimer, N, Winter, A, Heukelbach, J, Ariza, L, Ribeiro, H, et al. Prevalence and risk factors of toxoplasmosis among pregnant women in Fortaleza, Northeastern Brazil. Am J Trop Med Hyg. (2010) 83:528–33. doi: 10.4269/ajtmh.2010.10-0082
58. da Silva, MG, Câmara, JT, Vinaud, MC, and de Castro, AM. Epidemiological factors associated with seropositivity for toxoplasmosis in pregnant women from Gurupi, State of Tocantins, Brazil. Rev Soc Bras Med Trop. (2014) 47:469–75. doi: 10.1590/0037-8682-0127-2014
59. Dias, RCF, Lopes-Mori, FMR, Mitsuka-Breganó, R, Dias, RAF, Tokano, DV, Reiche, EMV, et al. Factors associated to infection by Toxoplasma gondii in pregnant women attended in Basic Health Units in the city of Rolândia, Paraná, Brazil. Rev Inst Med Trop Sao Paulo. (2011) 53:185–91. doi: 10.1590/S0036-46652011000400002
60. Spalding, SM, Amendoeira, MRR, Klein, CH, and Ribeiro, LC. Serological screening and toxoplasmosis exposure factors among pregnant women in South of Brazil. Rev Soc Bras Med Trop. (2005) 38:173–7. doi: 10.1590/S0037-86822005000200009
61. Quadros, RM, Rocha, GC, Romagna, G, Oliveira, JP, Ribeiro, DM, and Marques, SMT. Toxoplasma gondii seropositivity and risk factors in pregnant women followed up by the Family Health Strategy. Rev Soc Bras Med Trop. (2015) 48:338–42. doi: 10.1590/0037-8682-0233-2014
62. Moura, FL, Goulart, PRM, Moura, APP, Souza, TS, Fonseca, ABM, Amendoeira, MRR, et al. Fatores associados ao conhecimento sobre a toxoplasmose entre gestantes atendidas na rede pública de saúde do município de Niterói, Rio de Janeiro, 2013-2015. Epidemiol e Serviços Saúde. (2016) 25:655–61. doi: 10.5123/S1679-49742016000300022
63. Dambrun, M, Dechavanne, C, Guigue, N, Briand, V, Candau, T, Fievet, N, et al. Retrospective study of toxoplasmosis prevalence in pregnant women in Benin and its relation with malaria. PLoS One. (2022) 17:e0262018. doi: 10.1371/journal.pone.0262018
64. Ait Hamou, S, and Laboudi, M. An analytical study on the awareness and practice relating toxoplasmosis among pregnant women in Casablanca, Morocco. BMC Public Health. (2021) 21:507. doi: 10.1186/s12889-021-10474-9
65. Benitez, A, Martins, FDC, Mareze, M, Santos, NJR, Ferreira, FP, Martins, CM, et al. Spatial and simultaneous representative seroprevalence of anti-Toxoplasma gondii antibodies in owners and their domiciled dogs in a major city of southern Brazil. PLoS One. (2017) 12:e0180906. doi: 10.1371/journal.pone.0180906
66. Teweldemedhin, M, Gebremichael, A, Geberkirstos, G, Hadush, H, Gebrewahid, T, Asgedom, SW, et al. Seroprevalence and risk factors of Toxoplasma gondii among pregnant women in Adwa district, northern Ethiopia. BMC Infect Dis. (2019) 19:327. doi: 10.1186/s12879-019-3936-0
67. Moura, IPDS, Ferreira, IP, Pontes, AN, and Bichara, CNC. Toxoplasmosis knowledge and preventive behavior among pregnant women in the city of Imperatriz, Maranhão, Brazil. Cien Saude Colet. (2019) 24:3933–46. doi: 10.1590/1413-812320182410.21702017
68. Mulugeta, S, Munshea, A, and Nibret, E. Seroprevalence of anti– Toxoplasma gondii antibodies and associated factors among pregnant women attending antenatal care at Debre Markos Referral Hospital, Northwest Ethiopia. Infect Dis Res Treat. (2020) 13:117863372094887. doi: 10.1177/1178633720948872
69. Hassanen, EAA, Makau, DN, Afifi, M, Al-Jabr, OA, Abdulrahman Alshahrani, M, Saif, A, et al. Interplay between cross sectional analysis of risk factors associated with Toxoplasma gondii infection in pregnant women and their domestic cats. Front Vet Sci. (2023) 10:1147614. doi: 10.3389/fvets.2023.1147614
70. Chandrasena, N, Herath, R, Rupasinghe, N, Samarasinghe, B, Samaranayake, H, Kastuririratne, A, et al. Toxoplasmosis awareness, seroprevalence and risk behavior among pregnant women in the Gampaha district, Sri Lanka. Pathog Glob Health. (2016) 110:62–7. doi: 10.1080/20477724.2016.1173325
71. Santos, PC, Lehmann, LM, Lorenzi, C, Hirsch, C, Telmo, PL, Mattos, GT, et al. The seropositivity of Toxocara spp. antibodies in pregnant women attented at the university hospital in Southern Brazil and the factors associated with infection. PLoS One. (2015) 10:e0131058. doi: 10.1371/journal.pone.0131058
72. Melo, MS, Cabrera, LAA, Lima, SVMA, dos Santos, AD, Oliveira, LMGB, de Oliveira, RC, et al. Temporal trend, spatial analysis and spatiotemporal clusters of infant mortality associated with congenital toxoplasmosis in Brazil: Time series from 2000 to 2020. Trop Med Int Heal. (2023) 28:476–85. doi: 10.1111/tmi.13877
73. Ministério da Saúde. Protocolo de notificação e investigação: Toxoplasmose gestacional e congênita (2018). 31 p Available at: https://bvsms.saude.gov.br/bvs/publicacoes/protocolo_notificacao_investigacao_toxoplasmose_gestacional_congenita.pdf.
Keywords: epidemiology, pregnancy, toxocariasis, toxoplasmosis, zoonoses
Citation: Pereira ELGM, Ferreira IB, Victorino RB, Lescano SAZ, Giuffrida R, Kmetiuk LB, Biondo AW and Santarém VA (2024) Serosurvey of Toxoplasma gondii and Toxocara spp. co-infection in pregnant women in low-income areas of Brazil. Front. Public Health. 12:1340434. doi: 10.3389/fpubh.2024.1340434
Edited by:
Daniel Diaz, National Autonomous University of Mexico, MexicoReviewed by:
Majid Pirestani, Tarbiat Modares University, IranAbdelbaset Eweda Abdelbaset, Hokkaido University, Japan
Copyright © 2024 Pereira, Ferreira, Victorino, Zevallos Lescano, Giuffrida, Kmetiuk, Biondo and Santarém. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Alexander Welker Biondo, YWJpb25kb0B1ZnByLmJy