
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health, 20 March 2024
Sec. Children and Health
Volume 12 - 2024 | https://doi.org/10.3389/fpubh.2024.1339860
 Fidanka Vasileva1,2
Fidanka Vasileva1,2 Gemma Carreras-Badosa1
Gemma Carreras-Badosa1 Judit Bassols3
Judit Bassols3 Juan Serrano-Ferrer2Raquel Font-Lladó2,4
Juan Serrano-Ferrer2Raquel Font-Lladó2,4 Victor López-Ros5Inés Osiniri6Jose-Maria Martínez-Calcerrada7Marta San Millán2,8
Victor López-Ros5Inés Osiniri6Jose-Maria Martínez-Calcerrada7Marta San Millán2,8 Abel López-Bermejo1,9,10*†
Abel López-Bermejo1,9,10*† Anna Prats-Puig2,8
Anna Prats-Puig2,8Background: Physical activity (PA) is beneficial for the overall health. Objectives are: (1) To compare metabolic (MRM) and cardiovascular-risk-markers (CRM) in children according to their PA-level; (2) to explore the associations of MRM and CRM with PA and sedentary time (ST); and (3) to identify the associations between MRM and CRM in less (LA) and more active (MA) children.
Methods: A total of 238 apparently healthy school-aged children were enrolled (132 boys/106 girls; 9.1 ± 1.8 years) and body mass index standard deviation score (BMI SDS) and blood pressure were assessed. Fasting venous blood sampling was performed to assess insulin resistance (HOMA-IR) and high-sensitivity-C-reactive protein (hsCRP). Epicardial fat, interventricular septal and left ventricular posterior wall thicknesses were assessed by high-resolution ultrasonography. PA and ST were assessed by enKid-questionnaire. Children were classified based on enKid-score as being LA and MA (below and above 50th percentile for PA).
Results: MA-children had lower values for: BMI SDS, diastolic-to-systolic blood pressure ratio, HOMA-IR and hsCRP (7.02 to 61.5% lower, p = 0.040 to p < 0.0001) compared to LA-children. MRM and CRM were positively associated with ST (p = 0.003 to p < 0.001), and negatively associated with PA (p = 0.044 to p < 0.001). Finally, MRM were positively associated with CRM (p = 0.008 to p < 0.0001). Interestingly, the latter associations were observed in LA-children but were not present in MA-children.
Conclusion: More PA is associated with better cardio-metabolic profile in school-aged children. PA seems to modulate the associations between MRM and CRM, thus reinforcing the idea that fostering PA in children may lower the risk for development of a cardio-metabolic disease.
Physical activity (PA) is any movement produced by the skeletal muscles that raises energy expenditure above resting metabolic rate, and is performed to improve or maintain the components of physical fitness and health (1). Since PA is widely recognized as a primary contributor to overall health protection (2), the World Health Organization recommends ≥1 h/day of PA (3). In parallel, inactivity and sedentary time should be reduced because they promote obesity and diabetes (3). Sedentary time is characterized by any sitting, reclining, or lying posture with an energy expenditure ≤1.5 metabolic equivalents (4).
Nowadays, there is a growing prevalence of metabolic disorders in children that may place a child at a high risk of developing a cardiovascular disease (CVD) later in life. CVD are the most common cause of death globally, accounting for 17.8 million deaths worldwide (5). For instance, known metabolic risk markers such as insulin resistance (HOMA-IR) and high sensitivity C-reactive protein (hsCRP) are considered to induce detrimental effect on cardio-metabolic health (6). Increased HOMA-IR, together with increased total body adiposity and fat accumulation were related to increased epicardial fat (EF) in adult population (5, 7). Additionally, hsCRP was related to cardiac remodeling and diastolic dysfunction in hypertensive patients (8). Similar associations have been identified in children with insulin resistance, hypertension and CVD (9–11). However, to the best of our knowledge, no previous studies explored these associations in relation to PA in healthy children.
High blood pressure, especially diastolic-to-systolic blood pressure ratio (D/S BP ratio) has been proposed as a relevant cardiovascular risk marker because of its relation to systemic vascular resistance (12). EF, interventricular septal thickness (IVST) and left ventricular posterior wall thickness (LVPWT) are heart-related cardiovascular risk markers, and potential therapeutic targets for maintenance of cardiovascular health (13–15). Previous studies have shown that EF causes local inflammation and has direct effects on coronary atherosclerosis (13), while IVST and LVPWT predict all-cause death in patients with coronary artery disease (14), and cardiac events (15), respectively.
Since PA has been reported to be beneficial for the overall health (2), we hypothesize that there will be differences in the cardio-metabolic profile of the children according to their level of PA, and that more PA may relate to a better cardio-metabolic profile. Therefore, our objectives are: (1) To compare metabolic and cardiovascular risk markers in children according to the level of PA; (2) to explore the associations of metabolic and cardiovascular risk markers with PA and sedentary time; and (3) to identify the associations between metabolic and cardiovascular risk markers in less and more active children (below and above 50th percentile for PA).
A total of 238 apparently healthy school-aged children (106 girls/132 boys; 9.19 ± 1.80 years) were recruited in primary health centers in Girona (Northeastern Spain). Inclusion criteria were: age between 5 and 12 years. Exclusion criteria were: (1) major congenital abnormalities; (2) chronic illness or chronic use of medication; (3) acute illness or use of medication in the last 2 weeks preceding potential enrolment; (4) abnormal blood counts, (5) abnormal liver, kidney or thyroid functions; and (6) hsCRP levels higher than 10 mg/L indicating an acute infection or inflammatory process (16). The research was approved by the Institutional Review Board of Dr. Josep Trueta Hospital, Girona, Spain (CEIC: 2010.056). Signed consent was obtained from the parents of all children included in the study.
Body mass was measured wearing light clothes with a calibrated scale and height was measured with a Harpenden stadiometer. Body mass index (BMI) was calculated as body mass in kilograms divided by the square of height in meters. Age- and sex-adjusted standard deviation scores (SDS) for body mass, height and BMI were calculated using regional normative data (17). Venous blood sampling was performed in a fasting state in the morning (between 8.00 and 9.00 AM). Serum insulin was measured by immunochemiluminiscence (IMMULITE 2000, Diagnostic Products Corporation). Lower detection limit was 0.4 mIU/L and intra- and inter-assay coefficients of variability were less than 10%. Serum glucose was analysed by the hexokinase method (Cobas C; Roche Diagnostics, Indianapolis, US). Lower detection limit was 2.0 mg/dL and intra- and inter-assay coefficients of variability were less than 3%. HOMA-IR was estimated from fasting insulin and glucose concentrations using the homeostasis model assessment [HOMA-IR = (fasting insulin in mU/L) x (fasting glucose in mg/dL)/405]. Serum levels of hsCRP were measured using the ultrasensitive latex immunoassay CRP Vario (Sentinel Diagnostics, Abbott Diagnostics Europe, Milan, Italy). Lower detection limit was 0.2 mg/L and intra- and inter-assay coefficients of variability were less than 3%.
Blood pressure was measured in a supine position on the right arm by means of an electronic oscillometer (Dinamap ProCare 100, GE Healthcare) with cuff size appropriate for the arm circumference. The average of three measurements was considered. Heart-related cardiovascular risk markers (EF, IVST and LVPWT) were measured using a high-resolution ultrasonography (MyLabTM25, Esaote, Firenze, Italy). To assess EF, IVST and LVPWT children were placed in the left lateral decubitus position according to the recommendations of the American Society of Echocardiography (18). Linear 7.5–12 MHz transducer was used for EF and a convex 3.5–5 MHz transducer was used for IVST and LVPWT. The measurements were taken from the parasternal long-axis views. Three consecutive measurements were performed and the calculated mean was considered for analysis. All measurements were taken on a separate visit and were performed by the same observer (a sonographer specialized in pediatric ecography) who was unaware of the clinical characteristics of the participants. Intra-observer coefficient of variation for ultrasound measurements was less than 6%.
PA and sedentary time were assessed by the enKid questionnaire that was filled out by the children’s parents (19). This self-reported questionnaire offers a broad, general perspective on children’s PA but it is practical, cost-effective and easy to apply, thus being convenient for PA assessment, especially in research including pediatric population (20). To analyze data, the following categories were created: (1) PA – hours per day spent playing alone, playing with others, and activities such as riding a bike, rollerblading, skateboarding, swimming, playing football, basketball, handball, volleyball etc. (2) sedentary time – hours per day in a seated position (screen time activities, listening to music, reading and studying).
Statistical analyses were performed using SPSS version 22.0 (SPSS Inc., Chicago, IL, United States). The normality of the data distribution was tested by the Kolmogorov–Smirnov test. Non-normally distributed variables were logarithmically transformed to improve the distribution symmetry. Subsequently, PA percentiles were created in order to classify children as more (above 50th percentile) and less (below 50th percentile) physically active. We employed this approach mainly because it provides balanced allocation by dividing the dataset into two equal parts, ensuring a reference threshold which is sample-specific, making it a suitable and convenient method for group formation in research (21). In this line, the use of percentiles is widely and commonly accepted in research with children, adolescents, adults and older population (21–28). Differences in metabolic and cardiovascular risk markers between more and less physically active children were examined with a Student’s t-test. It was followed by analysis of covariance to correct for potential confounding variables (age, sex and BMI). The associations of PA and sedentary time with metabolic and cardiovascular risk markers, as well as the associations between metabolic and cardiovascular risk markers, were analyzed by Pearson correlations. It was followed by a linear regression analysis (enter method) to correct for potential confounding variables (age, sex and BMI). Significance level was set at 0.05.
Descriptive characteristics, as well as a comparison of the cardio-metabolic profile according to the level of PA of the children are presented in Table 1. Based on the results, more physically active children had lower values for BMI SDS (27.51% less, p = 0.040), insulin (30.72% less, p = 0.013), HOMA-IR (34.15% less, p < 0.001), hsCRP (61.54 less, p < 0.001) and D/S BP ratio (7.02% less, p < 0.0001) compared to less physically active children. Worthy to note is that we identified sex differences among the groups of more and less physically active children, thus we corrected the observed differences for any potential confounding variables such as age, sex and BMI. Interestingly, all differences remained significant in analysis of covariance correcting for the previously mentioned confounding variables (Table 1).
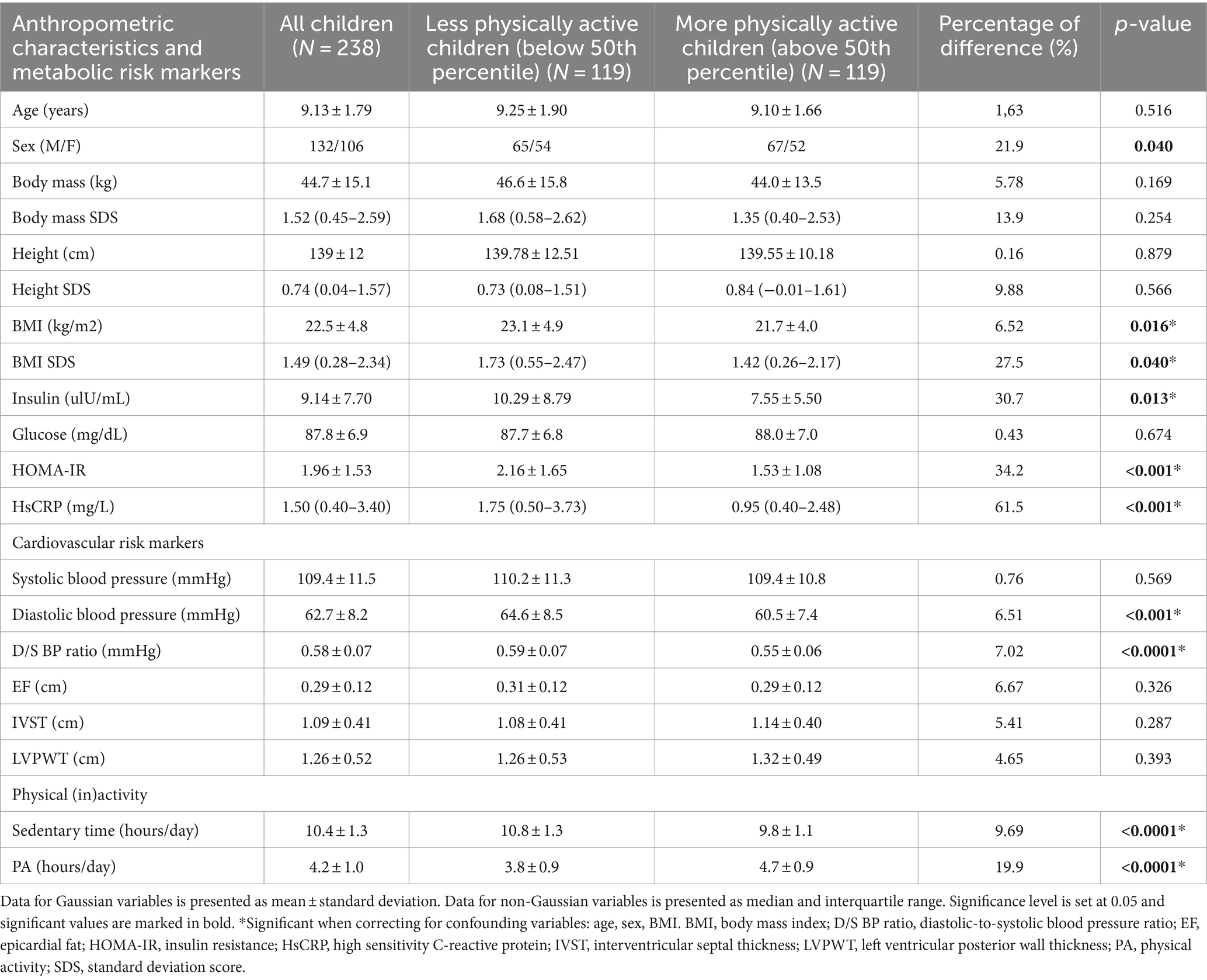
Table 1. Descriptive characteristics of the studied population and comparison of the cardio-metabolic profile between more and less physically active children.
Bivariate associations of metabolic and cardiovascular risk markers with PA and sedentary time are presented in Table 2 and Figure 1. On the one hand, PA was negatively associated with HOMA-IR (r = −0.142, p = 0.044), EF (r = −0.133, p = 0.040) (Table 2), hsCRP (r = −0.157, p = 0.016) and D/S BP ratio (r = −0.211, p < 0.001) (Figure 1A). On the other hand, sedentary time was positively associated with insulin (r = 0.221, p < 0.001), HOMA-IR (r = 0.210, p = 0.003), EF (r = 0.197, p < 0.002) (Table 2), hsCRP (r = 0.227, p < 0.001) and D/S BP ratio (r = 0.202, p = 0.002) (Figure 1B). Worthy to note is that the negative association of D/S BP ratio with PA, as well as its positive association with sedentary time, remained significant after correcting for age, sex and BMI (Figure 1). The positive association between sedentary time and hsCRP also remained significant after correcting for age, sex and BMI (Figure 1B).
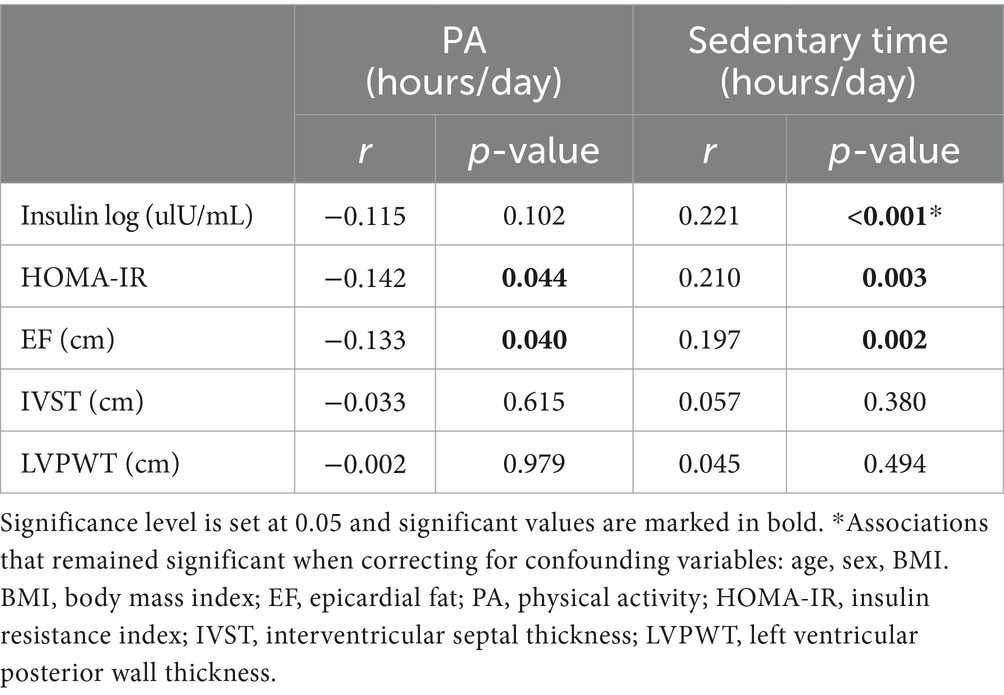
Table 2. Bivariate associations of metabolic and cardiovascular risk markers with PA and sedentary time in school-aged children (N = 238).
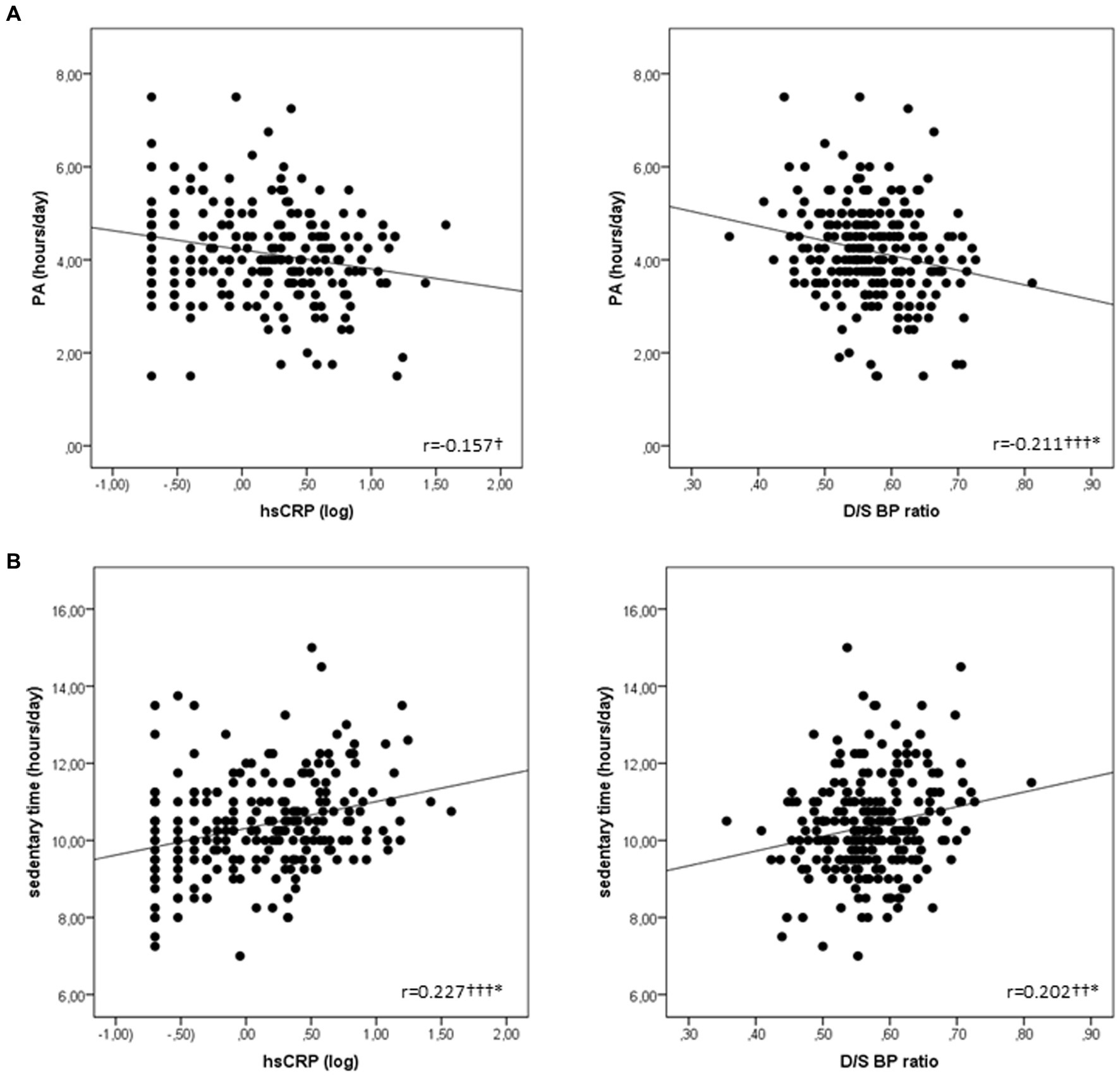
Figure 1. Scatterplots representing the associations of: (A) PA with hsCRP and D/S BP ratio; and (B) Sedentary time with hsCRP and D/S BP ratio. Significance level is set at 0.05 and significant values are marked as follows: p < 0.05†, p < 0.01†† and p < 0.001†††. *Associations that remained significant when correcting for confounding variables: age, sex and BMI. BMI, body mass index; D/S BP ratio, diastolic-to-systolic blood pressure ratio; hsCRP, high sensitivity C-reactive protein; PA, physical activity.
Bivariate associations between metabolic and cardiovascular risk markers are presented in Table 3 and Figure 2. D/S BP ratio was positively associated with insulin (r = 0.196, p = 0.005) and HOMA-IR (r = 0.185, p = 0.008) in the studied children (Table 3). Furthermore, IVST and LVPWT were positively associated with hsCRP (r = 0.171, p = 0.008 and r = 0.186, p = 0.004) (Table 3), while EF was positively associated with insulin (r = 0.292, p < 0.0001) and hsCRP (r = 0.298, p < 0.0001) (Figure 2) in the same children. Interestingly, when we analyzed the same associations in groups according to the level of PA of the children, all previously mentioned associations were present only in less physically active children (r = 0.179 to r = 0.367, p = 0.049 to p < 0.0001), while they were not observed in more physically active children (Table 3 and Figure 2). Worthy to note is that the positive associations of EF with insulin and hsCRP remained significant after correcting for age, sex and BMI in the studied children, especially in less physically active children (Figure 2).
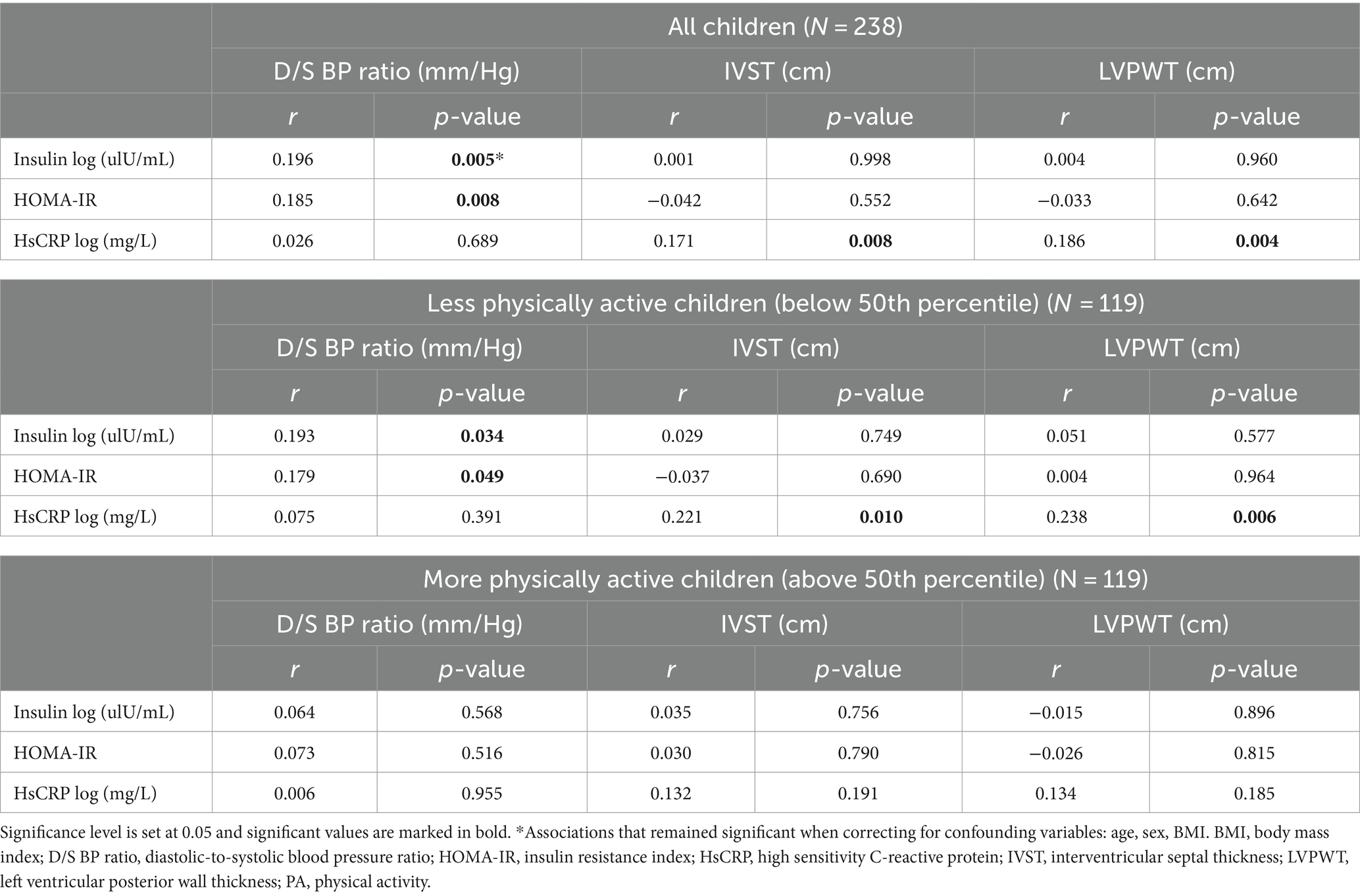
Table 3. Bivariate associations between metabolic and cardiovascular risk markers in apparently healthy school-aged children according to the level of PA.
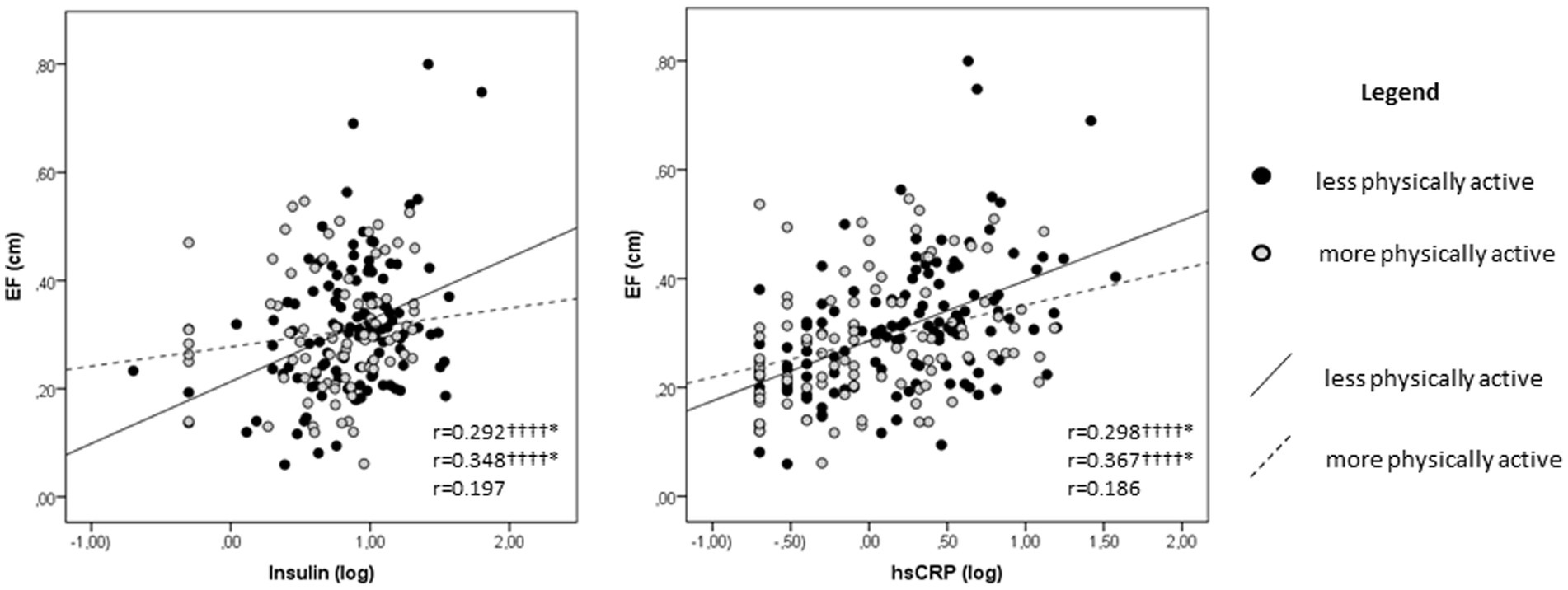
Figure 2. Scatterplots representing the associations of EF with insulin and hsCRP. Pearson’s correlation coefficients are presented in the following order from top to bottom: all studied children, less physically active children and more physically active children. Significance level is set at 0.05 and significant values are marked as follows: p < 0.0001††††. *Associations that remained significant when correcting for confounding variables: age, sex and BMI. BMI, body mass index; EF, epicardial fat; hsCRP, high sensitivity C-reactive protein.
Main findings of this study indicate that school-aged children who are more physically active have a better cardio-metabolic profile than those who are less physically active. Metabolic and cardiovascular risk markers are negatively related to PA and positively related to sedentary time in these children. Finally, metabolic risk markers were positively related to cardiovascular risk markers in the same children. Interestingly, PA seems to modulate the latter associations in a volume-dependent manner, as they were identified in less physically active children and were not present in more physically active children.
Children who are more physically active have lower insulin, HOMA-IR, hsCRP and D/S BP ratio, than less physically active children. This outcome allows us to accept the postulated hypothesis of the present study. Even if previous studies did not focus on comparing the metabolic and cardiovascular profile in healthy children depending on their PA levels, existing evidence in adult population is in line with our findings (29). For instance, previous studies reported that HOMA-IR, hsCRP and blood pressure were significantly lower in adults who perform a minimum of 150 min/week of PA, in comparison to those who performed less PA (29, 30). A recent meta-analysis confirmed that increased blood pressure in childhood is associated with higher risk for CVD and mortality in adulthood (31). However, subjects with increased blood pressure during childhood, but normal blood pressure during adolescence, were not at risk for developing a CVD (31). This evidence raises the need to develop an effective non-medication based strategy to reduce blood pressure in pre-pubertal children, with the aim to prevent CVD in adulthood. Results obtained in our study indicate that PA may be such strategy even in apparently healthy children, which emphasizes the importance for children to be physically active in order to maintain their cardiovascular health. As it has been previously suggested, PA may confer beneficial effects on metabolic and cardiovascular health by enhancing insulin sensitivity in the muscles and the liver (30). Moreover, PA helps reducing the amount of adipose tissue, which may prevent from obesity-driven insulin resistance and inflammation (30). In addition, our results reinforce the idea of benefits on cardiovascular health depending on the PA levels, which may be explained by a higher increase in the blood flow and a higher reduction in the vascular resistance due to the demand induced by higher PA levels (32).
Present findings also indicate that HOMA-IR, hsCRP, D/S BP ratio and EF are related to sedentary time in school-aged children. On the other hand, all these metabolic and cardiovascular risk markers were inversely related to PA. In line with the associations of metabolic and cardiovascular risk markers with PA and sedentary time in our study, previous evidence suggest that sedentary time is associated with altered metabolic profile (33), while PA was inversely related to BMI, fat percentage and HOMA-IR, thus lowering the risk for obesity in children (34). Additionally, higher levels of PA were related to lower hsCRP concentration (35). In the same line, cardiovascular markers were also negatively associated with PA. More precisely, the associations between D/S BP ratio and PA obtained in the present study are in accordance with previous reports suggesting that a lowered risk for hypertension was related to more PA and less sedentary time (36). In general, PA is associated with a lower heart rate on a long-term scale that could allow for sufficient time for diastolic left ventricular filling and coronary flow, therefore improving arterial compliance and lowering blood pressure (30, 37). Furthermore, it is worthy to emphasize that the World Hypertension League and the European Society of Hypertension recommended regular PA across the lifespan (including childhood) because of its well-established antihypertensive effects, as well as its favorable impact on other modifiable CVD risk factors (38). Moreover, they highlighted an inverse dose–response relationship between PA levels and CVD, i.e., the incidence of stroke, coronary artery disease and overall mortality (38). Finally, EF was negatively related to PA in our study suggesting that more PA will potentially contribute to less EF. To the best of our knowledge, no previous studies in healthy children have explored this association. However, in line with our findings, PA was related to lower visceral fat in Japanese female adults (39). One possible physiological mechanism explaining the inverse association between EF and PA may be the lipid mobilization triggered by increased catecholamine production during PA, leading to increased lipolysis rate in the EF cells (39).
Metabolic risk markers were related to cardiovascular risk markers in the present study, leading to the premise that any metabolic alterations in these children may potentially induce alterations in their cardiovascular health as well. Even though studies reporting associations between metabolic and cardiovascular risk markers in healthy children are scarce, previous studies have obtained similar results in adults (5, 7, 40), and in children at risk for developing a cardiovascular disease (9–11). For instance, increased body mass, insulin concentration and higher HOMA-IR in children with obesity were related to higher EF (9, 41). Increased hsCRP in hemodialysis patients was related to higher IVST (42), while higher BMI in children with hypertrophic cardiomyopathy was related to higher LVPWT (11). As discussed previously, studies in healthy children exploring the associations of metabolic risk markers with IVST and LVPWT, and in relation to PA, are missing to the best of our knowledge. However, we suggest that the associations between metabolic and cardiovascular risk markers identified in healthy children may be a result of the interplay between multiple underlying mechanisms. Higher insulin levels may lead to reduction of the sodium excretion rate and increased blood pressure (43). In addition, higher insulin levels may also promote fatty acid synthesis (44) which may end up in excessive lipid accumulation, therefore directly contributing to the formation of ectopic fat (45), such in this case - EF. Furthermore, hsCRP stimulates the production of adhesion molecules that enhance the infiltration of monocytes and lymphocytes resulting in fibrosis and cardiac remodeling (8), such as increased IVST and LVPWT. It is worthwhile to note that the results in our study were obtained in apparently healthy school-aged children, and thus indicate the importance of the early assessment of metabolic and cardiovascular profile in children.
Finally, it is also important to mention that the positive associations of D/S BP ratio with insulin and HOMA-IR, the positive associations of hsCRP with IVST and LVPWT, and the positive associations of EF with insulin and hsCRP identified in less physically active children, were not observed in more physically active children at the present study. More precisely, our results are indicative on a potential modulatory role of PA on the associations between the metabolic and cardiovascular risk markers because none of the associations identified in less physically active children was present in more physically active children. Moreover, current findings are pointing toward a dose-dependent modulatory effect of PA, propounding the idea that PA may modulate cardio-metabolic health in these children in a volume-dependent manner. Even though studies in healthy children that report volume-dependent PA-induced cardio-metabolic health benefits are scarce, in support to our findings previous studies in adult hypertensive population reported that higher PA levels provided superior cardio-metabolic benefits (38, 46). Additionally, the authors of the previous works argued that higher PA levels did not show any adverse effects among individuals diagnosed with hypertension, contradicting and disproving the hypothesis that there might be a threshold beyond which high PA levels could become harmful or counterproductive, especially for individuals with hypertension (38, 46). Remarkably, they demonstrated that higher PA levels are superior in reducing the risk for CVD and may serve as a beneficial approach in reducing the mortality rates among hypertensive population (38, 46). Indeed, prior findings in adult hypertensive population are in line with the findings of the present study in apparently healthy school-aged children. Therefore, taking in consideration previous and current findings, we suggest that encouraging higher levels of PA, even from pediatric age, could contribute to improved cardio-metabolic health outcomes in children, and potentially prevent the development of CVD in the future (38, 46).
More PA is associated with a better cardio-metabolic profile in school-aged children. PA appears to modulate the associations between metabolic and cardiovascular risk markers in a volume-dependent manner, thus reinforcing the idea that fostering PA in children and encouraging an active lifestyle from an early age, could potentially reduce the risk for future cardio-metabolic diseases and improve overall health outcomes in adulthood.
Present findings will potentially promote and inspire practicing more PA in order to evoke cardio-protective effects and maintain cardio-metabolic health in children. Also they may help the professional in exercise medicine, the coach and even the physical education teacher in the schools, to design appropriate PA interventions that will promote health and contribute to disease prevention in school-aged children. Also, these findings may raise the need for implementation of additional PA programs within schools that will result in higher PA levels, thus promoting a healthier lifestyle from a young age. Additionally, they may potentially encourage modifications in the physical education curriculum, advocating for the incorporation of more physical education classes, as well as more active breaks during the other classes with the aim to reduce the sedentary time.
Furthermore, current findings may raise awareness among parents about the importance of PA for children’s health and encourage them to guide and support their children to engage in PA beyond school hours. Community caregivers may be inspired to develop safe and accessible play areas in neighborhoods, parks, or public spaces to facilitate outdoor activities and playtime for children.
The major limitation of this study is the lack of accelerometer data in addition to the PA questionnaire in order to assess PA. Accelerometers may provide thorough assessment of PA, including information on PA intensity, offering a more detailed outlook than the self-reported questionnaires. However, the use of validated self-reporting instruments such as questionnaires is widely accepted in research as well as by medical communities, since they are practical, cost-effective and easy to apply, especially when dealing with large populations or specific demographics like children (20). Even though the self-reported questionnaires are commonly used in research due to their convenience, it is important to acknowledge their limitation to capture detailed information such as PA intensity, and point out the necessity for considering this in future research. Therefore, future studies should focus on clarifying the effects of light, moderate and vigorous PA on cardio-metabolic health. The impact of various PA intensities on cardio-metabolic health will potentially contribute in establishing intensity thresholds that are necessary to achieve prominent health benefits. This information is valuable for guiding public health recommendations and personalized exercise prescriptions. In addition, understanding the effects of different PA intensities on specific cardio-metabolic health indicators, may contribute to the development of personalized exercise programs for individuals with specific health conditions. Finally, the acquired knowledge can be translated into tailored recommendations, strategies and exercise interventions with the aim to improve public health and reduce the burden of cardio-metabolic diseases.
Furthermore, future interventional studies should also compare the effects of different types of physical exercise (e.g., aerobic, anaerobic, mixed interventions) on cardio-metabolic health. These studies could clarify further the physiological responses to varying exercise regimens. This may contribute significantly in optimizing exercise prescriptions designed to maintain and improve cardio-metabolic-health. In addition, the acquired knowledge may raise the need for further studies that will implement specifically tailored PA interventions in school settings, with the aim to assess their impact on improving cardio-metabolic health in children.
Another limitation of the present study is the cross-sectional design which does not allow inference on causality to be done. Alternatively, longitudinal follow-up studies track participants over time and may offer insights into the causality of sustained PA and the long-term cardio-metabolic health benefits. Thus, further longitudinal studies should be designed to observe changes in PA patterns, and elucidate the underlying mechanisms for the long-term benefits that may be induced by PA.
Future experimental and genome-wide studies should investigate the epigenetic modifications potentially induced by PA in children, and how these modifications may impact their cardio-metabolic health. By pursuing these research avenues, researchers can uncover the epigenetic mechanisms underlying the relationship between PA and cardio-metabolic health, and potentially develop interventions that will evoke the desired modifications to maximize cardio-metabolic health outcomes.
Finally, further comparative studies should aim to explore potential sex-specific differences in PA-induced cardio-metabolic health benefits. Future research employing larger sample size should focus on comparing the effects of PA on cardio-metabolic health in males and females separately in order to understand potential sex-specific implications.
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
The studies involving humans were approved by Institutional Review Board of Dr. Josep Trueta Hospital, Girona, Spain. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants’ legal guardians/next of kin.
FV: Conceptualization, Formal analysis, Investigation, Methodology, Software, Writing – original draft. GC-B: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Software, Writing – review & editing. JB: Data curation, Funding acquisition, Project administration, Writing – review & editing. JS-F: Formal analysis, Methodology, Software, Writing – review & editing. RF-L: Methodology, Software, Supervision, Writing – review & editing. VL-R: Methodology, Software, Writing – review & editing. IO: Data curation, Methodology, Software, Writing – review & editing. JM-C: Data curation, Methodology, Software, Writing – review & editing. MS: Methodology, Writing – review & editing. AL-B: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Supervision, Writing – review & editing. AP-P: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Software, Supervision, Writing – review & editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This study was supported by grants from the Ministry of Science and Innovation, Carlos III Health Institute, Madrid, Spain (PI20/00399 to JB and PI19/00451 to AL-B), projects co-funded by FEDER (European Fund for regional development). FV holds a fellowship from the Secretariat for Universities and Research of the Ministry of Business and Knowledge of the Government of Catalonia and the European Social Fund (2022FI_B1 00074). GC-B is an Investigator of the Sara Borrell Fund for Scientific Research from Carlos III National Institute of Health (CD19-00172). JB is an investigator of the Miguel Servet Fund from Carlos III National Institute of Health (CPII17/00013). AL-B is an investigator of the I3 Fund for Scientific Research (Ministry of Science and Innovation, Spain).
Authors are grateful to all children and parents who took part in the study.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Pescatello, LS, Arena, R, Riebe, D, and Thomsen, PD. ACSM’s Guidelines for exercise testing and prescription. 9th ed. Philadelphia: Wolters Kluwer Health/Lippincott Williams & Wilkins (2014).
2. Peplies, J, Börnhorst, C, Günther, K, Fraterman, A, Russo, P, Veidebaum, T, et al. Longitudinal associations of lifestyle factors and weight status with insulin resistance (HOMA-IR) in preadolescent children: the large prospective cohort study IDEFICS. Int J Behav Nutr Phys Act. (2016) 13:97. doi: 10.1186/S12966-016-0424-4
3. World Health Organization. WHO guidelines on physical activity and sedentary behaviour at a glance (2020). Available at: https://www.who.int/publications/i/item/9789240014886
4. Tremblay, MS, Aubert, S, Barnes, JD, Saunders, TJ, Carson, V, Latimer-Cheung, AE, et al. Sedentary behavior research network (SBRN) - terminology consensus project process and outcome. Int J Behav Nutr Phys Act. (2017) 14:75. doi: 10.1186/S12966-017-0525-8
5. Guembe, MJ, Fernandez-Lazaro, CI, Sayon-Orea, C, Toledo, E, and Moreno-Iribas, Cfor the RIVANA Study Investigators, et al. Risk for cardiovascular disease associated with metabolic syndrome and its components: a 13-year prospective study in the RIVANA cohort. Cardiovasc Diabetol. (2020) 19:195. doi: 10.1186/S12933-020-01166-6
6. Srikanthan, K, Feyh, A, Visweshwar, H, Shapiro, JI, and Sodhi, K. Systematic review of metabolic syndrome biomarkers: a panel for early detection, management, and risk stratification in the west Virginian population. Int J Med Sci. (2016) 13:25–38. doi: 10.7150/IJMS.13800
7. Rabkin, SW. The relationship between epicardial fat and indices of obesity and the metabolic syndrome: a systematic review and meta-analysis. Metab Syndr Relat Disord. (2014) 12:31–42. doi: 10.1089/MET.2013.0107
8. Seyfeli, E, Sarli, B, Saglam, H, Karatas, CY, Ozkan, E, and Ugurlu, M. The relationship between high-sensitivity C-reactive protein levels and left ventricular hypertrophy in patients with newly diagnosed hypertension. J Clin Hypertens. (2016) 18:679–84. doi: 10.1111/JCH.12734
9. Manco, M, Morandi, A, Marigliano, M, Rigotti, F, Manfredi, R, and Maffeis, C. Epicardial fat, abdominal adiposity and insulin resistance in obese pre-pubertal and early pubertal children. Atherosclerosis. (2013) 226:490–5. doi: 10.1016/J.ATHEROSCLEROSIS.2012.11.023
10. Sorof, JM, Alexandrov, AV, Cardwell, G, and Portman, RJ. Carotid artery intimal-medial thickness and left ventricular hypertrophy in children with elevated blood pressure. Pediatrics. (2003) 111:61–6. doi: 10.1542/PEDS.111.1.61
11. Balaji, S, DiLorenzo, MP, Fish, FA, Etheridge, SP, Aziz, PF, Russell, MW, et al. Impact of obesity on left ventricular thickness in children with hypertrophic cardiomyopathy. Pediatr Cardiol. (2019) 40:1253–7. doi: 10.1007/S00246-019-02145-9
12. Akaishi, T, Abe, M, Miki, T, Miki, M, Funamizu, Y, Ito, S, et al. Ratio of diastolic to systolic blood pressure represents renal resistive index. J Hum Hypertens. (2019) 34:512–9. doi: 10.1038/s41371-019-0264-1
13. Bertaso, AG, Bertol, D, Duncan, BB, and Foppa, M. Epicardial fat: definition, measurements and systematic review of main outcomes. Arq Bras Cardiol. (2013) 101:e18–28. doi: 10.5935/ABC.20130138
14. Huang, BT, Peng, Y, Liu, W, Zhang, C, Huang, FY, Wang, PJ, et al. Increased interventricular septum wall thickness predicts all-cause death in patients with coronary artery disease. Intern Med J. (2015) 45:275–83. doi: 10.1111/IMJ.12667
15. Walsh, TF, Dall’ Armellina, E, Chughtai, H, Morgan, TM, Ntim, W, Link, KM, et al. Adverse effect of increased left ventricular wall thickness on five year outcomes of patients with negative dobutamine stress. J Cardiovasc Magn Reson. (2009) 11:1–9. doi: 10.1186/1532-429X-11-25/TABLES/4
16. Mac Giollabhui, N, Ellman, LM, Coe, CL, Byrne, ML, Abramson, LY, and Alloy, LB. To exclude or not to exclude: considerations and recommendations for C-reactive protein values higher than 10 mg/L. Brain Behav Immun. (2020) 87:898–900. doi: 10.1016/J.BBI.2020.01.023
17. Carrascosa-Lezcano, A, Fernandez-Garcia, J, Ferandez-Longas, A, Lopez-Siguero, J, and Sanchez-Gonzales, E. Cross-sectional study of growth and development. 1st ed. Barcelona, Spain: Pfizer, S.A. (2008).
18. American Society of Echocardiography, American Society of Echocardiography – Organization of professionals committed to excellence in cardiovascular ultrasound. (2021). Available at: https://www.asecho.org/
19. Roman, B, Serra-Majem, L, Ribas-Barba, L, Pérez-Rodrigo, C, and Aranceta, J. How many children and adolescents in Spain comply with the recommendations on physical activity? J Sports Med Phys Fitness. (2008) 48:380–7.
20. Ainsworth, B, Cahalin, L, Buman, M, and Ross, R. The current state of physical activity assessment tools. Prog Cardiovasc Dis. (2015) 57:387–95. doi: 10.1016/J.PCAD.2014.10.005
21. Shieh, G. Comparison of alternative approaches for difference, noninferiority, and equivalence testing of normal percentiles. BMC Med Res Methodol. (2020) 20:59. doi: 10.1186/s12874-020-00933-z
22. Benavides, C, Benítez-Andrades, JA, Marqués-Sánchez, P, and Arias, N. eHealth intervention to improve health habits in the adolescent population: mixed methods study. JMIR Mhealth Uhealth. (2021) 9:e20217. doi: 10.2196/20217
23. Fairclough, SJ, Rowlands, AV, del Pozo Cruz, B, Crotti, M, Foweather, L, Graves, LEF, et al. Reference values for wrist-worn accelerometer physical activity metrics in England children and adolescents. Int J Behav Nutr Phys Act. (2023) 20:35. doi: 10.1186/s12966-023-01435-z
24. Belcher, BR, Wolf-Gughes, DL, Dooley, EE, Staudenmayer, J, Berrigan, D, Eberhardt, MS, et al. US population-referenced percentiles for wrist-worn accelerometer-derived activity. Med Sci Sports Exerc. (2021) 53:2455–64. doi: 10.1249/MSS.0000000000002726
25. Blagus, R, Jurak, G, Starc, G, and Leskošek, B. Centile reference curves of the SLOfit physical fitness tests for school-aged children and adolescents. J Strength Cond Res. (2023) 37:328–36. doi: 10.1519/JSC.0000000000004265
26. Santos, R, Mota, J, Santos, DA, Silva, AM, Baptista, F, and Sardinha, LB. Physical fitness percentiles for Portuguese children and adolescents aged 10-18 years. J Sports Sci. (2014) 32:1510–8. doi: 10.1080/02640414.2014.906046
27. Pereira, C, Fernandes, J, Raimundo, A, Biehl-Printes, C, Marmeleira, J, and Tomas-Carus, P. Increased physical activity and fitness above the 50(th) percentile avoid the threat of older adults becoming institutionalized: a cross-sectional pilot study. Rejuvenation Res. (2016) 19:13–20. doi: 10.1089/rej.2015.1669
28. Blom, WM, Westerhout, J, and Houben, GF. The 50th percentile of the general population single eating occasion intake of food is optimal for the calculation of action levels for precautionary allergen labelling. Food Chem Toxicol. (2023) 179:113953. doi: 10.1016/j.fct.2023.113953
29. Reddigan, JI, Ardern, CI, Riddell, MC, and Kuk, JL. Relation of physical activity to cardiovascular disease mortality and the influence of cardiometabolic risk factors. Am J Cardiol. (2011) 108:1426–31. doi: 10.1016/J.AMJCARD.2011.07.005
30. An, SJ, Jung, MH, Ihm, SH, Yang, Y, and Youn, HJ. Effect of physical activity on the cardiometabolic profiles of non-obese and obese subjects: results from the Korea National Health and nutritional examination survey. PLoS One. (2019) 14:e0208189. doi: 10.1371/JOURNAL.PONE.0208189
31. Yang, L, Magnussen, CG, Yang, L, Bovet, P, and Xi, B. Elevated blood pressure in childhood or adolescence and cardiovascular outcomes in adulthood: a systematic review. Hypertension. (2020) 75:948–55. doi: 10.1161/HYPERTENSIONAHA.119.14168
32. de Oliveira, CVC, Santos, AC, Brito, A, and so Socorro Brasileiro, M. Resistance exercise with different volumes: blood pressure response and forearm blood flow in the hypertensive elderly. Clin Interv Aging. (2014) 9:2151–8. doi: 10.2147/CIA.S53441
33. Leiva, AM, Martínez, MA, Cristi-Montero, C, Salas, C, Ramírez-Campillo, R, Díaz Martínez, X, et al. Sedentary lifestyle is associated with metabolic and cardiovascular risk factors independent of physical activity. Rev Med Chile. (2017) 145:458–67. doi: 10.4067/S0034-98872017000400006
34. Kehoe, SH, Krishnaveni, GV, Veena, S, Kiran, KN, Karat, SC, Dhubey, A, et al. Active children are less adipose and insulin resistant in early adolescence; evidence from the Mysore Parthenon cohort. BMC Pediatr. (2019) 19:1–12. doi: 10.1186/S12887-019-1855-2/TABLES/5
35. Bergström, G, Behre, CJ, and Schmidt, C. Moderate intensities of leisure-time physical activity are associated with lower levels of high-sensitivity C-reactive protein in healthy middle-aged men. Angiology. (2012) 63:412–5. doi: 10.1177/0003319711423386
36. Weres, A, Baran, J, Czenczek-Lewandowska, E, Leszczak, J, and Mazur, A. The association between steps per day and blood pressure in children. Sci Rep. (2022) 12:1422–7. doi: 10.1038/s41598-022-05497-0
37. Reule, S, and Drawz, PE. Heart rate and blood pressure: any possible implications for Management of Hypertension? Curr Hypertens Rep. (2012) 14:478–84. doi: 10.1007/S11906-012-0306-3
38. Charchar, FJ, Prestes, PR, Mills, C, Ching, SM, Neupane, D, Marques, FZ, et al. Lifestyle management of hypertension: International Society of Hypertension position paper endorsed by the world hypertension league and European Society of Hypertension. J Hypertens. (2024) 42:23–49. doi: 10.1097/HJH.0000000000003563
39. Ayabe, M, Kumahara, H, Morimura, K, Sakane, N, Ishii, K, and Tanaka, H. Accumulation of short bouts of non-exercise daily physical activity is associated with lower visceral fat in Japanese female adults. Int J Sports Med. (2013) 34:62–7. doi: 10.1055/S-0032-1314814
40. Manno, C, Campobasso, N, Nardecchia, A, Triggiani, V, Zupo, R, Gesualdo, L, et al. Relationship of Para- and perirenal fat and epicardial fat with metabolic parameters in overweight and obese subjects. Eat Weight Disord. (2019) 24:67–72. doi: 10.1007/S40519-018-0532-Z
41. Reyes, Y, Paoli, M, Camacho, N, Molina, Y, Santiago, J, and Lima-Martínez, MM. Epicardial adipose tissue thickness in children and adolescents with cardiometabolic risk factors. Endocrinol Nutr. (2016) 63:70–8. doi: 10.1016/J.ENDONU.2015.09.007
42. Kim, BS, Jeon, DS, Shin, MJ, Kim, YO, Song, HC, Lee, SH, et al. Persistent elevation of C-reactive protein may predict cardiac hypertrophy and dysfunction in patients maintained on hemodialysis. Am J Nephrol. (2005) 25:189–95. doi: 10.1159/000085585
43. Giglio, RV, Stoian, AP, Haluzik, M, Pafili, K, Patti, AM, Rizvi, AA, et al. Novel molecular markers of cardiovascular disease risk in type 2 diabetes mellitus. Biochim Biophys Acta Mol basis Dis. (2021) 1867:166148. doi: 10.1016/J.BBADIS.2021.166148
44. Hardy, OT, Czech, MP, and Corvera, S. What causes the insulin resistance underlying obesity? Curr Opin Endocrinol Diabetes Obes. (2012) 19:81–7. doi: 10.1097/MED.0B013E3283514E13
45. Trouwborst, I, Bowser, SM, Goossens, GH, and Blaak, EE. Ectopic fat accumulation in distinct insulin resistant phenotypes; targets for personalized nutritional interventions. Front Nutr. (2018) 5:77. doi: 10.3389/FNUT.2018.00077
46. Del Pozo, CB, Ahmadi, M, Inan-Eroglu, E, Huang, BH, and Stamatakis, E. Prospective associations of accelerometer-assessed physical activity with mortality and incidence of cardiovascular disease among adults with hypertension: the UK biobank study. J Am Heart Assoc. (2022) 11:e023290. doi: 10.1161/JAHA.121.023290
Keywords: epicardial fat, interventricular septal thickness, left ventricular posterior wall thickness, insulin resistance, C-reactive protein, physical activity, sedentary time, school-aged children
Citation: Vasileva F, Carreras-Badosa G, Bassols J, Serrano-Ferrer J, Font-Lladó R, López-Ros V, Osiniri I, Martínez-Calcerrada J-M, San Millán M, López-Bermejo A and Prats-Puig A (2024) Insulin resistance, C-reactive protein, diastolic to systolic blood pressure ratio and epicardial fat are related to sedentary time, and inversely related to physical activity in school-aged children. Front. Public Health. 12:1339860. doi: 10.3389/fpubh.2024.1339860
Edited by:
Alexandre A. da Silva, University of Mississippi Medical Center, United StatesReviewed by:
Mircea-Catalin Fortofoiu, University of Medicine and Pharmacy of Craiova, RomaniaCopyright © 2024 Vasileva, Carreras-Badosa, Bassols, Serrano-Ferrer, Font-Lladó, López-Ros, Osiniri, Martínez-Calcerrada, San Millán, López-Bermejo and Prats-Puig. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Abel López-Bermejo, YWxvcGV6YmVybWVqb0BpZGliZ2kub3Jn
†ORCID: Abel López-Bermejo https://orcid.org/0000-0002-5828-8911
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.