 Shurong Han1
Shurong Han1 Jianjun Xiang
Jianjun Xiang- 1International Business School, Shaanxi Normal University, Xi’an, China
- 2Department of Preventive Medicine, School of Public Health, Fujian Medical University, Fuzhou, China
Background: It has become an alarming issue that older adults in China are facing mental health issues, causing severe depression. In this context, intergenerational care, in which grandparents care for young children instead of the young parents, is gaining importance. This study aims to explore the correlation between intergenerational care and depression among older adults, seeking alternative approaches to enhancing their quality of life. This study concludes that intergenerational care is an effective strategy for promoting active aging.
Methods: This study used multiple linear regression, propensity score matching, and additional analysis of heterogeneity, mediation, and moderation effects, with data from the 2018 CHARLS survey.
Results: The results indicated a negative correlation between intergenerational care and depression among older adults. The correlation was stronger for females and younger older adults people. Additionally, social activities served as a mediator between intergenerational care and depression among older adults, and health satisfaction positively moderated this relationship.
Conclusion: This study posits that intergenerational care serves as an effective approach for promoting active aging. It emphasizes the necessity for supportive government policies and community-family collaborations to encourage intergenerational care and its beneficial impact on mental health among older adults.
1 Introduction
By the year 2021, the population of Chinese citizens aged 60 or over had reached 267 million, making up a significant 18.9% of the total population. Based on the 2019 World Population Prospects Report by the United Nations Population Division, it is anticipated that China’s population aging rate will increase to 20.7% in 2035, and 26.1% in 2050 (1). This growing population of older adults people has caused heightened concerns about their health. As people age, their physical abilities deteriorate, and they must deal with new challenges associated with changing social roles and lifestyle changes. These changes can have a significant negative impact on their mental well-being, leading to feelings of anxiety, depression, and loneliness. In a survey conducted by the National Health and Wellness Commission, it was discovered that the prevalence of mental health issues among older adults in urban areas was 30.3%, while in rural areas, it was slightly lower at 26.8% (2). This alarming statistic suggests that the mental health of older adults in China is a serious issue that requires further attention. Depression is a common and noticeable manifestation of poor mental health.
Traditionally, older people have been seen as a group that requires assistance. However, as their health improves and their life expectancy increases, this perception of being reliant on others for care is gradually fading away. A significant approach to this is intergenerational care, which is a family upbringing model where younger parents are unable to provide sufficient care for their underage children due to various reasons, and their grandparents step in to raise, nurture, and educate them (3). As a result of East Asian cultural norms, the challenges faced by single-child families in childcare, and changes in family dynamics due to the rise in female workforce participation, intergenerational care has become a widespread choice for families (4). Intergenerational care is deeply entwined with the lives of older people, and its impact on female workforce participation and the market’s childcare service demand–supply balance can potentially increase fertility rates. However, its influence on the mental health of older adults themselves requires further investigation. In 2002, the World Health Organization introduced the concept of “active aging,” a policy framework aimed at enhancing the quality of life and providing older people with opportunities for health, participation, and security in the face of population aging in the 21st century (5). Therefore, exploring the connection between intergenerational care and the mental health of older people is crucial for advancing their well-being and promoting “active aging.”
The relationship between intergenerational care and the mental health of older people is a complex and contentious issue. There are currently two competing perspectives on this matter. One view, endorsed by the role tension theory, argues that intergenerational care negatively affects the mental health of older individuals. This theory posits that individuals in society are assigned various roles, each with different demands and expectations. As individuals attempt to juggle these diverse roles, they can experience role conflict, which can manifest as stress and strain, ultimately having a detrimental impact on their mental health (6). The strain imposed on older individuals by intergenerational care is accentuated by the physical and emotional toll it demands. This care often requires substantial effort, leaving older individuals overwhelmed due to their physical limitations (7, 8). Furthermore, the stress and dysfunctionality that often accompany family caregiving can have a particularly detrimental effect on older individuals’ mental health (9). The routine and mechanical nature of caregiving can lead to feelings of loneliness and boredom, which are known to negatively impact mental health (10). In addition, older individuals often prioritize the care of their grandchildren, thereby neglecting their own mental health, leading to a decline in their overall health (11). The psychological impacts of caregiving for older individuals can include depression and familial pressures (12). A study in the United States found that African American grandparent caregivers experience more depressive symptoms compared to their noncaregiving peers (13). Despite this, the relationship between the intensity of intergenerational care and the mental health of older individuals remains fluid. High-intensity caregiving can crowd out older individuals’ time and energy for self-care, negatively affecting both their physical and mental health (14, 15). On the other hand, some scholars suggest that high-intensity intergenerational care can reduce feelings of loneliness in older individuals, while low-intensity care can negatively affect their self-rated health (16).
The mental health of older individuals can be positively influenced by intergenerational care, which is supported by the role enhancement theory (17). This theory was developed by Sieber in 1974, building on the role tension theory. It posits that taking on multiple roles can not only cause role tension but also lead to benefits such as material resources and spiritual well-being. Intergenerational care can enable older individuals to increase their material and spiritual resources by assuming caregiving responsibilities. This practice can alleviate family stress associated with child care (18) and provides older individuals with more intergenerational support from their children (19). Moreover, providing intergenerational care allows older individuals to demonstrate their worth (20), find enjoyment and enrichment in their later years (21, 22), strengthen their family relationships (23), and enhance the bond between grandparents and grandchildren (24, 25). Zhao, J. found that reverse feeding, a form of intergenerational care where parents care for their children, can improve older individuals’ mental health (26). Furthermore, older individuals who assist their children with daily tasks can boost their abilities and sense of authority, which in turn can enhance their subjective well-being (27). The mental health of older individuals is significantly dependent on family companionship (28), and traditional Chinese culture advocates for older individuals to maintain productivity through caring for their grandchildren or household chores (29).
Cultural diversity across countries and ethnicities contributes to different motivations for older adults to engage in intergenerational care. Catherine and Merril examined the experiences of 1,058 grandparents with diverse ethnic backgrounds who had cared for their grandchildren in Los Angeles, United States. They discovered that the varying cultural backgrounds and lifestyles of these grandparents resulted in differences in their willingness to provide intergenerational care. This directly impacted the relationship between intergenerational care and their health status (30).
In China, a cultural context that values family and inheritance, older individuals tend to be more willing to take on intergenerational care as a way of perpetuating the family legacy (31). This sense of obligation in China often leads to a higher voluntary participation in intergenerational care among grandparents, with 51.7% of middle-aged and older Chinese individuals caring for their grandchildren (32). This compared to only 5.9% of middle-aged and older Korean individuals providing care to their grandchildren (33). This demonstrates that the act of providing intergenerational care is viewed more as a duty in China, while in Korea it is viewed as an optional act.
Moreover, there are multiple factors that influence the relationship between intergenerational care and older individuals’ depressive status, including gender, age, mobility, cognitive appraisal, time of care initiation, and source of care recipient (34–37). The gender division of labor theory suggests that men are typically associated with the public sphere and engaged in productive work, while women are associated with the private sphere and engaged in work related to human reproduction (38). Even in old age, men continue to be less involved in family matters. Wu Qi analyzed 180 questionnaires in Nantong, Jiangsu province, China, and found that the primary reason for rural older individuals to move to the city was to care for their grandchildren (39). Among the older individuals surveyed, women accounted for 80, and 90% of them were willing to take on the primary responsibility of caring for their grandchildren. The level of intergenerational care varies among older individuals of different ages. Younger older adults individuals are more actively involved in intergenerational care, whereas older individuals may no longer have grandchildren in need of care (40), and their physical condition as they age may also make them unable to provide intergenerational care. Therefore, intergenerational care varies based on gender and age, leading to differences in depressive status.
The mental health of older individuals is positively linked to social support (41), as suggested by the social companionship model, which posits that social support is derived from a person’s social network, which may vary throughout life depending on their circumstances (42). The presence of a supportive social network is vital for the physical and mental health of individuals, especially older adults, as it reduces stress and the likelihood of disabilities. The positive impact of social networks on the mental health of older adults has been extensively studied (43, 44), and it has been observed that individuals with fewer social connections are more susceptible to depression (45). Social activities, an integral part of social support, have been proposed as a way to increase the frequency and likelihood of social engagement in older adults, potentially impacting their mental state.
Previous research has highlighted that the impact of intergenerational care on health outcomes is largely contingent upon the preferences and satisfaction of the caregiver (46). This satisfaction, in turn, represents an overall evaluation of both physical and mental well-being. Thus, differences in self-evaluations of health can influence the perceived benefits of intergenerational care, either enhancing activities and cognitive functions (47), or potentially causing discomfort and role overload (48). These disparities in health satisfaction may subsequently alter older adults’ subjective perceptions of intergenerational care and subsequently influence its association with mental health.
Despite these significant insights, there are several limitations to consider. In particular, many studies have not taken into account selection bias, an issue that causes endogeneity. Therefore, in this study, we used propensity score matching to address this concern. Additionally, while caregivers may exhibit individual differences, there has been relatively little research examining gender and age disparities in intergenerational care. Therefore, our research will aim to fill this gap. Furthermore, previous studies have not thoroughly explored the intermediate mechanisms by which intergenerational care influences mental health. Hence, our study will aim to investigate the potential impact of social activities and health satisfaction on the relationship between intergenerational care and depression. Guided by these considerations, we propose the following hypotheses:
H1: Depression among older adults is negatively associated with intergenerational care.
H2: The relationship between intergenerational care and depression varies among older adults of different genders and ages.
H3: Social activities mediate the relationship between intergenerational care and depression among older adults.
H4: Satisfaction with one's own health positively moderates the relationship between intergenerational care and depression among older adults.
2 Materials and methods
The data used in this study were collected by the National Development Research Institute of Peking University and the China Social Science Survey Center through the China Health and Retirement Longitudinal Survey (CHARLS). The survey collects data in four waves, spanning from 2011 to 2018. These data cover approximately 150 county-level units, 450 village-level units, and 10,000 households. In our study, we used the latest data from 2018. CHARLS makes its data publicly available to the academic community 1 year after collection, meaning that the data we used were not collected by us and no ethical approval was required. The survey provides comprehensive information on demographics, households, health status and functioning, cognition and depression, healthcare and insurance, and pensions.
The main focus of this study was the analysis of a sample of individuals aged 60 years and above, specifically focusing on older adults, a population defined as individuals over the age of 60 according to the Law on the Protection of the Rights and Interests of older adults. Once the relevant observations with missing data were excluded, the final sample was comprised of 3,701 female and 3,890 male older adults.
The dependent variable for this study was the mental health of older adults, specifically depression. This was measured using a questionnaire, which asked 10 questions about depression, each offering four possible responses: “Rarely or not at all (<1 day),” “Not very much (1–2 days),” “Sometimes or about half the time (3–4 days),” and “Most of the time (5–7 days).” The questions “I am hopeful about the future” and “I am happy” were reverse-coded, with scores of 3, 2, 1, and 0 assigned, while the remaining eight questions were positively scored, with scores of 0, 1, 2, and 3 assigned. The scores of these 10 questions were then summed to create a score indicating the level of depression among older adults, which ranged from 0 to 30.
The intergenerational care variable was binary, indicating whether or not respondents had spent time caring for their grandchildren in the past year. The survey asked if the participants had spent time taking care of their grandchildren in the past year, and this was selected for 3,131 caregivers. The survey also asked for the specific time when they provided intergenerational care last year. This article calculated the total time of intergenerational care by adding up the time spent caring for different grandchildren. Therefore, if an older adults person cares for multiple grandchildren, the intergenerational care time is the total amount of time provided for multiple periods of intergenerational care. The intergenerational care time was measured as a continuous variable, ranging from 0.5 weeks to 208 weeks. The smaller the value, the shorter the time spent providing intergenerational care.
For the intermediate variable, social activity, we determined the participant’s level of social activity by looking at their answer to the CHARLS question: “Have you done any of the following social activities in the past month (multiple choices possible)?” If they participated in one or more of the 11 social activities, we assigned them a value of “1 = social activities”; if they did not participate in any of the activities, we assigned them a value of “0 = no social activities.”
For the adjustment variable, health satisfaction, we measured how satisfied participants were with their health by looking at their answer to the CHARLS question: “How satisfied are you with your health?” We used a 3-point scale and defined “0 = unsatisfied” as not very satisfied or not at all satisfied, “1 = satisfied” as completely satisfied, very satisfied, or somewhat satisfied, and “2 = not sure” as unsure or neutral.
In addition to the intermediate and adjustment variables, we also considered other factors that could affect participants’ responses. These included demographic factors such as gender, age, education level, marital status, living arrangement, and financial support from father to son or from son to father, and relational factors such as satisfaction with the relationship with children. All of these factors were derived from the questionnaire’s corresponding question and answer items. For some of these factors, we combined variables based on previous studies to create new variables. Table 1 provides detailed definitions and assignments of these control variables.

Table 1. Variable descriptions.
3 Results
3.1 Descriptive statistics
Table 2 presents the descriptive statistics for the main variables, based on a sample size of 7,591. The sample consisted of 51.24% males, with a relatively balanced ratio of males to females. The average age was 68.2 years, with 83.44% of the sample aged between 60 and 75 years. The level of education was uneven, with the majority of older people having received only primary education or less and only 4.27% having received higher education. Among the older people, 82.56% had a spouse, with 66.59% not living with their children. The percentage of children providing financial support for their father was 63.39%, while the percentage of fathers providing financial support for their children was only 30.73%. The majority of older people were satisfied with their relationship with their children, with only 4.47% expressing not very satisfied or not at all satisfied. Older people showed some variation in their satisfaction with their health, with 73.48% expressing satisfaction. Participation in social activities was evenly distributed, with 50.78% of older people engaging in social activities. The mean score for depression among older people was 8.713. Intergenerational care was common in the sample, with 43.97% of older people providing intergenerational care for their grandchildren and 56.03% not providing intergenerational care.

Table 2. Descriptive statistics results.
Additionally, this article divided the sample into two groups: those without intergenerational care and those with intergenerational care, and conducted intergroup difference tests (Table 3). The t-test was used to compare the mean differences between the two groups for depression and age, while chi-square tests were used for the rest of the variables. Significant intergroup differences were found for all variables except financial support from son to father and satisfaction with the relationship with children.
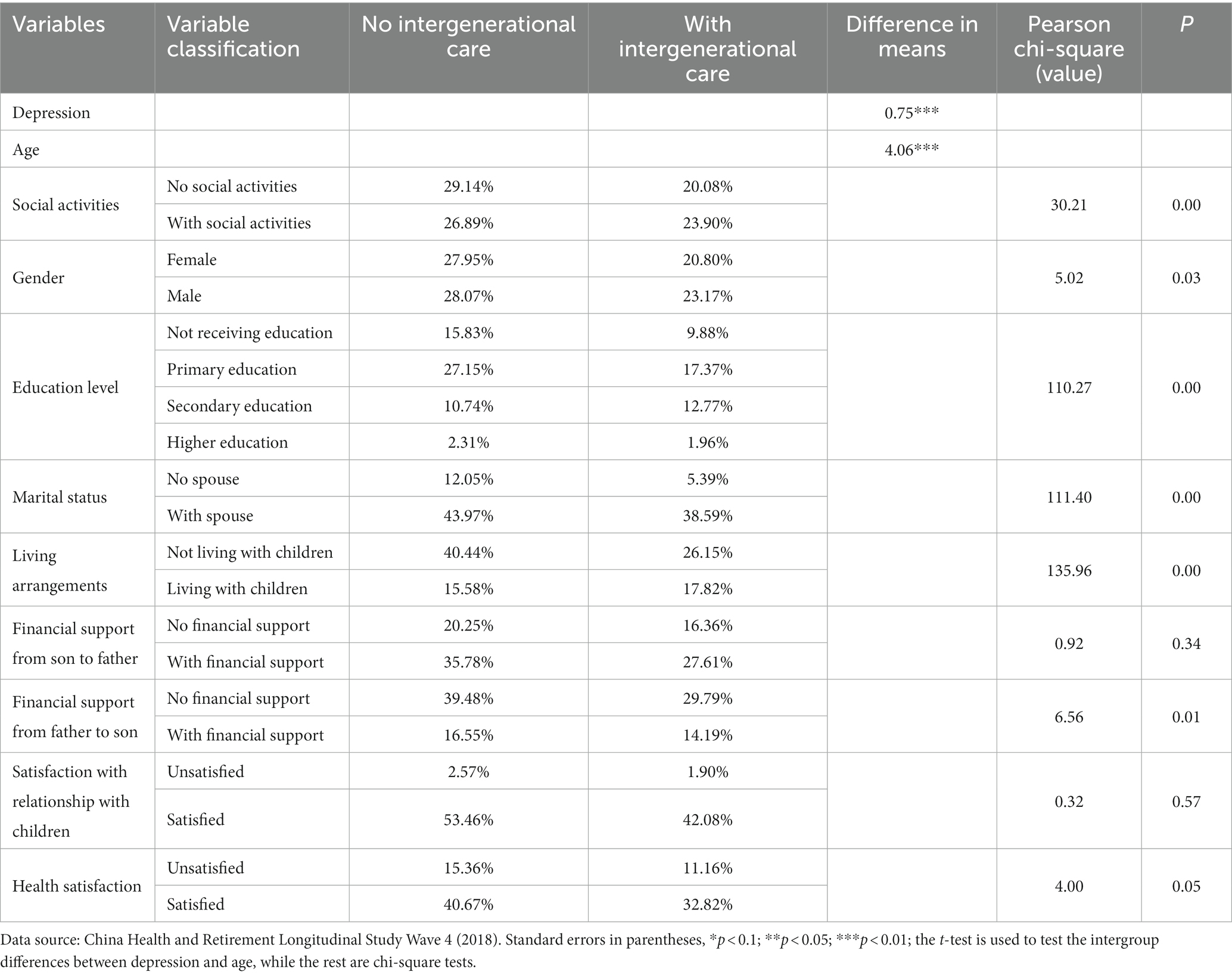
Table 3. Intergroup difference test.
3.2 Regression analysis
A multiple linear regression model (OLS) was used to explore the correlation between intergenerational care and the depressive status of older people. In the analysis below, age was standardized. In Model 1, the relationship between a range of control variables and depression was examined. These included gender, age, education level, marital status, living arrangements, and financial support from children to their parents. The study found that male older people, those who were older, had a higher level of education, were married, lived with their children, received financial support from their children to their parents, and were satisfied with their relationship with their children had varying levels of depression. Furthermore, the study found that those who received no financial support from their children to their parents, received financial support from their parents to their children, or were satisfied with their relationship with their children had better mental health status. The study further found that older, better educated older people were more self-adjusted, more tolerant of life, and more capable of relieving tension and stress. Those who were married, lived with their children, or were satisfied with their relationship with their children had a higher level of family well-being and had more options to relieve negative emotions. Finally, those who could provide financial support for their children but did not need financial support from their children were more confident and free.
Model 2 of the study analyzed the correlation between intergenerational care and depression, with a regression coefficient of −0.333 (p < 0.05). Model 3 explored the relationship between intergenerational care time and depression, with a regression coefficient of 0.006 (p < 0.1). The study found that providing intergenerational care was associated with lower levels of depression, but that a moderate care time was needed to maintain positive mental health.
The analysis of the data in Table 4 supported the hypothesis that depression among older people is negatively related to intergenerational care, which supports the H1 hypothesis.
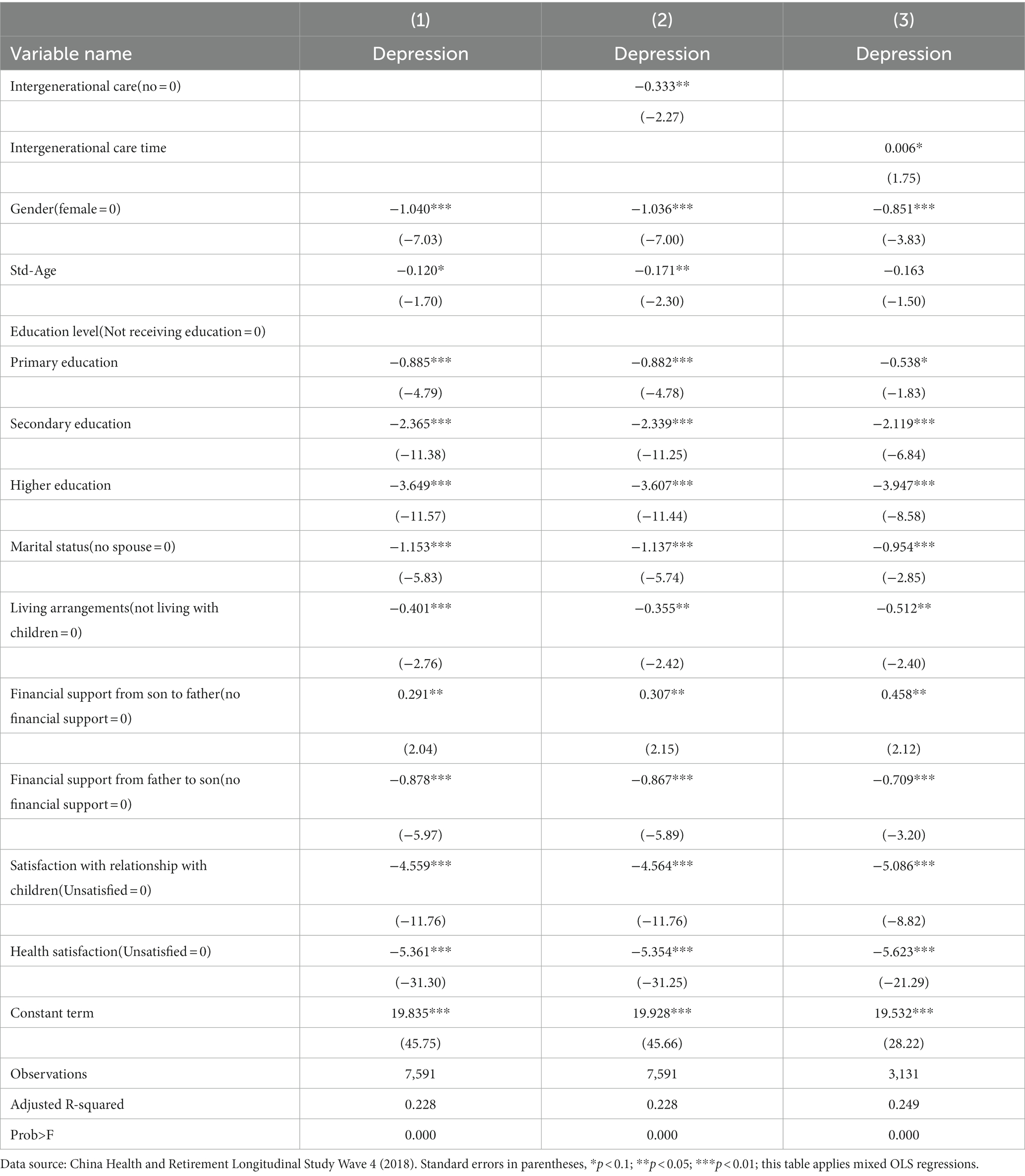
Table 4. Regression results of intergenerational care and intergenerational care time on depression of older people.
3.3 Robustness test
To examine the connection between intergenerational care and older people’s depressive status, we considered factors such as gender, self-care ability, financial standing, and social insurance status, all of which play a role in the provision of intergenerational care (49, 50). However, the complex relationship between these factors and depressive status can make it difficult to isolate the ‘pure’ relationship between the two. This study aims to address this issue by using multiple regressions, but recognizes that it may be challenging to ensure a linear relationship between control variables and the depressive status of older people. Moreover, it is possible that intergenerational care and depressive status may be inherently related, meaning that individuals with lower levels of depression may be more likely to provide care to others. To control for this, we employ the propensity score matching technique proposed by Rosenbaum and Rubin (51) as a robustness check. We first identify the factors influencing the provision of intergenerational care for older people. Next, we calculate propensity scores using the probit model. Finally, we match the sample based on these propensity scores, ensuring that the characteristics of older people who participate in intergenerational care are as similar as possible to those who do not participate. We use kernel matching and radius matching methods to ensure the reliability of our results.
3.3.1 Balance test
Post-matching, a balance test confirms the optimal balancing of intergenerational care participation across both groups through its standardized deviations. As shown in Table 5, these values fall below 10 after matching, indicating a substantial decrease. All t-test results uphold the initial null hypothesis of no significance in group disparities, demonstrating the efficacy of the matching process in achieving balance.
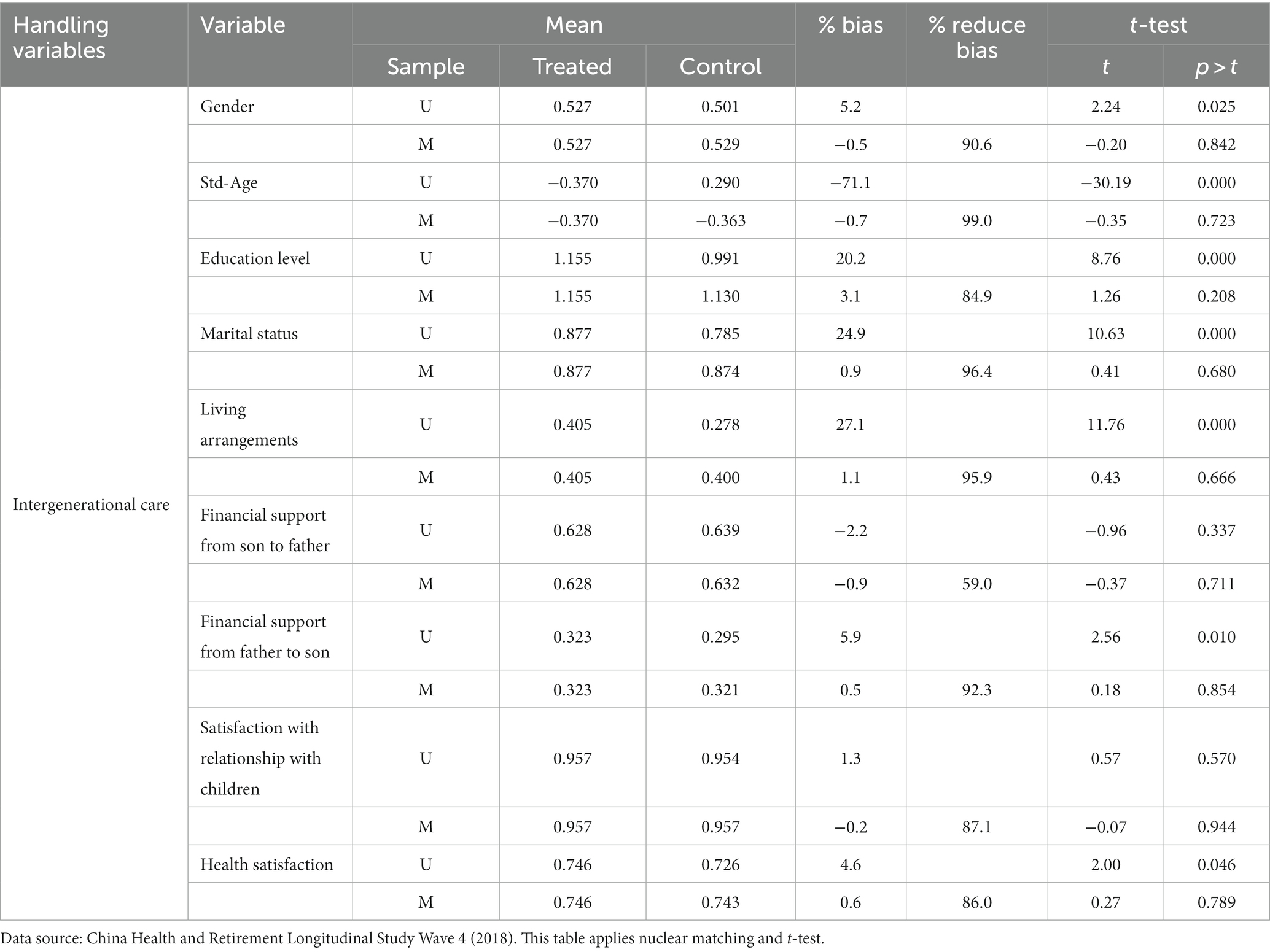
Table 5. Matching variables balance test.
3.3.2 Regression based on PSM matched data
In Table 6, our OLS model demonstrates a significant—and robust—negative correlation between intergenerational care and older adults’ depression levels. This result was observed both in the Kernel matching analysis and the Radius matching analysis.
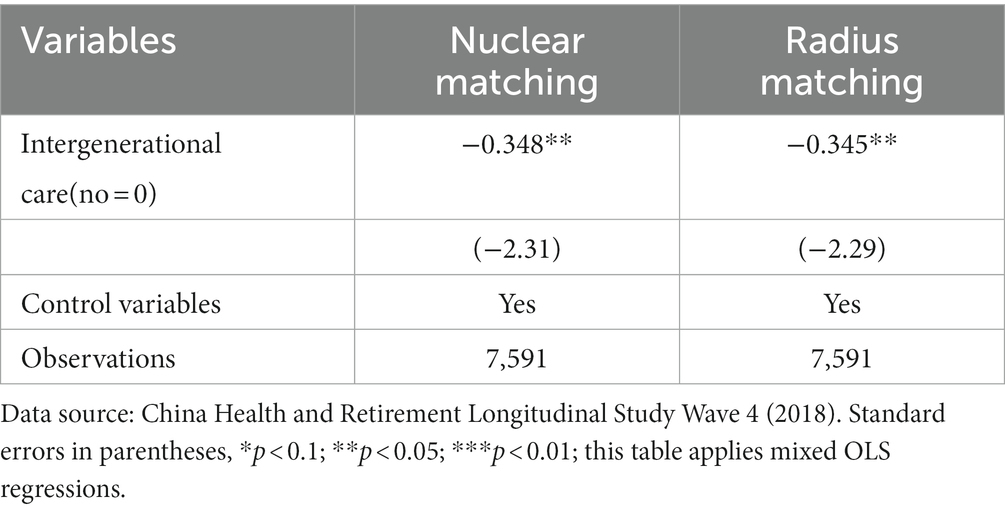
Table 6. Intergenerational care and depression of older people based on PSM matched data.
3.4 Heterogeneity analysis
3.4.1 Gender heterogeneity analysis
To scrutinize potential gendered disparities regarding the connection between intergenerational care and depression of older adults, the sample was partitioned into male and female subsets. Notably, evidence strongly supported the negative correlation between caregiving and depression among female seniors (−0.586; p < 0.01). By contrast, such association proved non-significant for male seniors.
3.4.2 Age heterogeneity analysis
We employed a sample divided into two sub-samples based on age, specifically targeting lower-aged older adults (60–75 years old) and higher-aged older adults (75 years old and above). This enabled us to analyze the possible age differences in the relationship between intergenerational care and the depressive status of older people. The results indicated that there is a significant negative relationship between intergenerational care and the depressive status of lower-aged older adults (60–75 years old), with a regression coefficient of −0.275 (p < 0.1). In contrast, the relationship between intergenerational care and the depressive status of higher-aged older adults (75 years old and above) was not found to be significant.
From Table 7, it is evident that there are diverse relationships between intergenerational care and the depression of older people, with these relationships varying according to gender and age. This provides support for hypothesis H2.
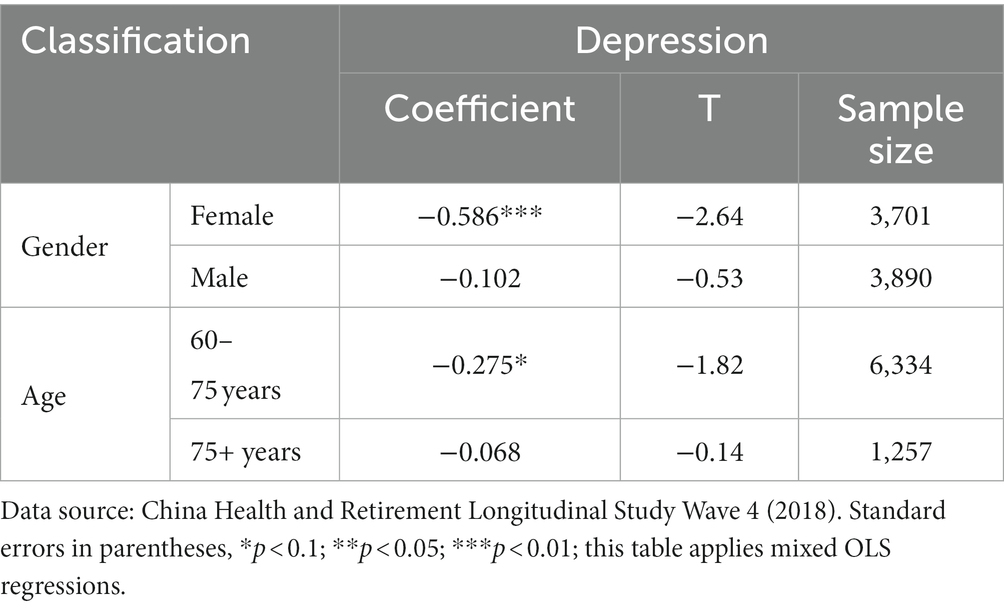
Table 7. Heterogeneity analysis of intergenerational care status on older people’s depression.
3.5 Analysis of correlation mechanisms
The previous section empirically examined the relationships between intergenerational care and depression of older adults, while the current section aims to delve into the mechanisms behind these relationships.
3.5.1 Mediating effect
To examine whether social activity mediates the association between intergenerational care and older individuals’ depression, this paper utilized commonly utilized operational recommendations to identify the relationship between intergenerational care and social activity through multiple linear regression, and then further explored the theoretical underpinnings of the connection between social activity and depressive states in older adults. Model 1 in Table 8 indicates that the provision of intergenerational care significantly escalated the level of social activity in older individuals. According to activity theory, mental health in older people positively correlates with social activity (52). Activity theory suggests that “participation in social activities” plays a pivotal role in the lives of older individuals, and independent engagement in interpersonal activities can efficiently prevent the adverse effects of life-altering events such as aging, physical decline, and changes in social status, and afford older individuals more energy to live a positive and active social life (53). Continuing to undertake the social responsibilities and roles in their earlier life stages can aid them in managing negative psychological emotions (54). Therefore, intergenerational care significantly reduced depression and enhanced psychological well-being of older individuals by augmenting their social activities, and social activities acted as a mediating pathway for the relationship between intergenerational care and the depressive status of older adults, thus supporting hypothesis H3.
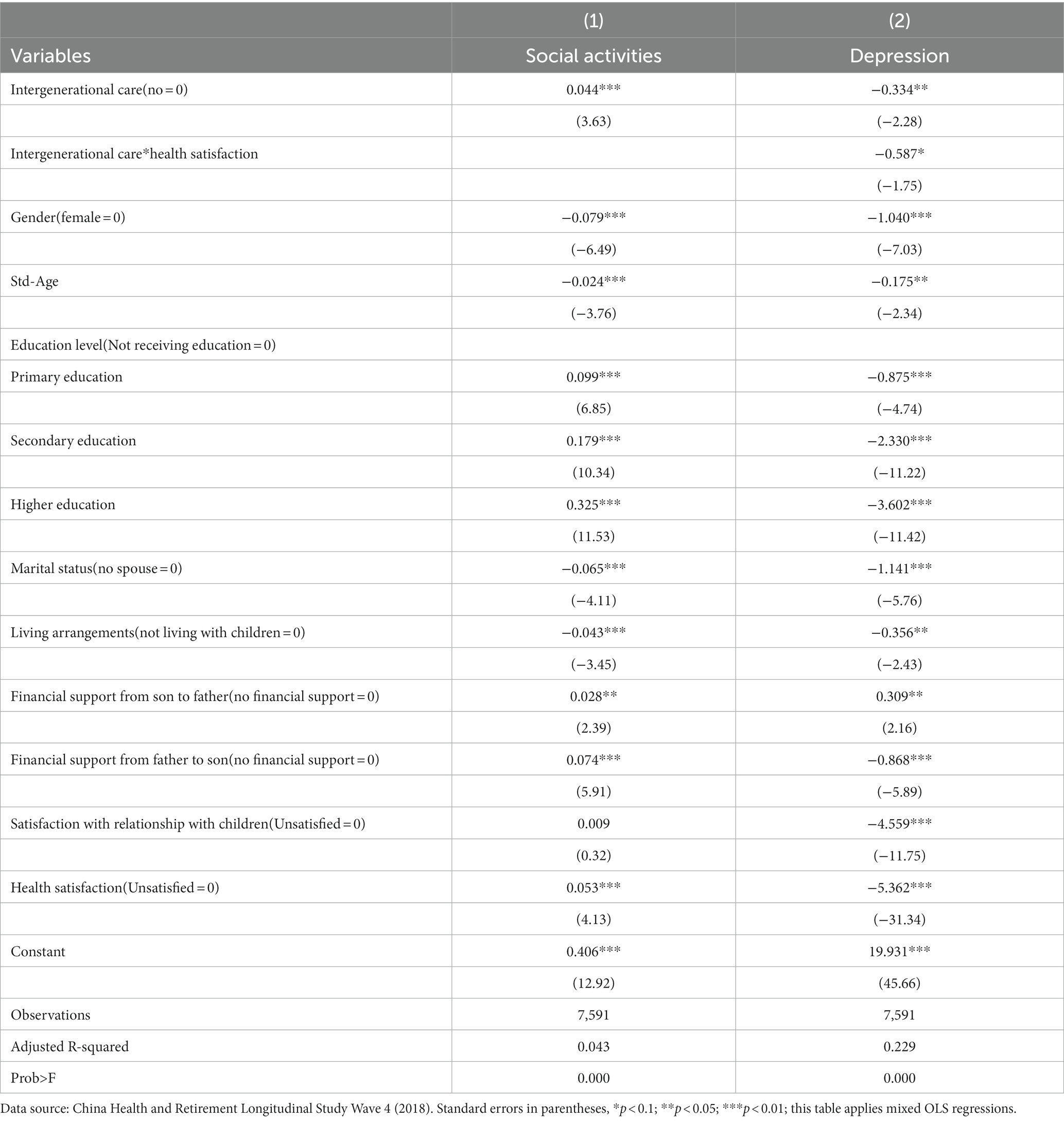
Table 8. Mediating effect of social activities and moderating effect of health satisfaction.
3.5.2 Moderating effect
In order to investigate the impact of health satisfaction on the relationship between intergenerational care and depression in older adults, the current study estimated the interaction coefficients between health satisfaction and intergenerational care. The findings from Table 8 indicate that Model 2 revealed significant negative interaction terms when considering the two indicators of intergenerational care and health satisfaction combined. This finding suggests that health satisfaction possesses a positive moderating effect on the relationship between intergenerational care and depression. As such, it was found that the higher the level of health satisfaction, the more effective intergenerational care was in reducing depression symptoms. Individuals who reported higher levels of health satisfaction were more likely to utilize intergenerational care as a method of valuing their family ties and resources, thus enhancing the relationship between intergenerational care and depressive status. Conversely, those with lower levels of health satisfaction were more likely to perceive intergenerational care as a drain on energy, thus reducing the relationship between intergenerational care and depressive status. Overall, these results provide support for Hypothesis 4, which proposes that health satisfaction plays a critical role in modifying the relationship between intergenerational care and depression in older adults.
4 Discussion
This paper shows that caring for grandchildren is prevalent among older individuals in China. It highlights that more attention should be paid to the practice of intergenerational care, which not only brings families closer together but also promotes active aging (4). Furthermore, with the introduction of the three-child policy in China and the increase in women’s employment rates, older individuals caring for their grandchildren has become an effective approach to bridge the childcare gap. Notably, intergenerational care not only taps the human resources of older individuals but also presents significant opportunities for their participation in the socio-economic and family development.
Furthermore, intergenerational care can be more than just “altruistic.” Through the involvement of older people in child care, it alleviates a great deal of the burden on their children. In return, children may provide additional financial, daily, and emotional support to their parents. This financial support can alleviate the financial stress that older people may face due to reduced income post-retirement. Daily care can address the basic difficulties that older people may encounter, particularly in cases of illness, providing them with a sense of security. Emotional support can directly alleviate the loneliness that older people may feel, providing them with positive emotional values through interpersonal interaction and emotional communication. As a result, their mental health can improve, as their stress and depression are relieved.
Nevertheless, it is crucial to remember that intergenerational care should be a moderate practice. When the frequency and duration of intergenerational care are well-balanced, it not only can allow older people to take pleasure in caring for their grandchildren, but also prevent them from feeling drained.
In China, due to the traditional gender roles, women are often seen as the primary caregivers in their family, and hence older women are most commonly assigned the responsibility of intergenerational care. In most instances, grandchildren tend to have a closer bond with their grandmothers than with their grandfathers (55). This fondness for their grandchildren further encourages female older adults to become more involved in intergenerational care. As the main caregivers, older women derive joy and personal worth from intergenerational care (56), which in turn, can effectively alleviate depression. However, the connection between intergenerational care and depression is not as significant for grandfathers. For instance, it may be more beneficial for grandfathers to focus their energy on other aspects, such as managing household affairs. Through effective division of labor, the grandparents can alleviate their own stress and provide support for each other, thus promoting their overall mental health.
For younger older individuals, engaging in intergenerational care can provide them with a sense of fulfillment, and can occupy a significant portion of their lives. There is a strong correlation between intergenerational care and their psychological well-being, and appropriate frequency and duration of intergenerational care can provide them with a sense of satisfaction. However, for higher-aged older adults, who may not have the physical capabilities to care for their grandchildren, shifting this responsibility can be overwhelming. Considering the age difference and the physical condition of these individuals, it is important to avoid providing intergenerational care or reduce their care time.
This article examines the mechanisms of intergenerational care and its impact on older people’s depressive status. Social activities play an intermediary role in the relationship between intergenerational care and older people’s depression. Participation in social activities not only maintains social networks, but also enables older people to engage in community exchanges by providing care to their grandchildren. These social interactions can bring them closer to their neighbors, friends, family, and broaden their social and life circles, thereby reducing the likelihood of social isolation. Additionally, a positive relationship exists between health satisfaction and intergenerational care for older people. For those with high levels of health satisfaction, intergenerational care can serve as a pathway to personal fulfillment and the positive effect on their mental health becomes more evident.
Intergenerational care is not unique to China. Professor Buchanan, a representative from Oxford University’s Department of Social Policy, mentioned in the introduction to the 2018 special issue titled “Twenty first century grandparents” that grandparents globally have assumed a more significant role in raising and educating their grandchildren in the last decade (57). Additionally, based on the data from the Australian Bureau of Statistics Time Use Survey of 2006, Craig and Jenkins found that approximately 60% of Australian grandparents surveyed indicated their involvement in caring for their grandchildren (58). In the United States, Guzman reported based on data from two large national surveys (NSFH and NHES) from 1992 to 1994 that 47% of American grandparents were involved in intergenerational care, a significant increase from before the 1990s, as evident by a surge in the number of grandparents living with their grandchildren (59). The differences in intergenerational care among countries around the world are primarily due to specific institutional conditions, cultural rules, and family circumstances. However, the research based on Chinese data on the relationship between intergenerational care and depression in older adults provides insights for promoting the mental health of older people. It was found that promoting intergenerational care for older people can help alleviate depression, and social activities can play a positive role in facilitating this care. Gender and age differences should be considered when providing intergenerational care.
5 Conclusion
The significance of intergenerational care for older people should be properly understood by society, families, and individuals, and multiple social actors should be fully mobilized to maximize the benefits of intergenerational care. This includes promoting the involvement of grandparents in caring for their grandchildren, the government’s support for such intergenerational care, the promotion of community activities that offer opportunities for intergenerational interaction, the improvement of mental health services for older people providing intergenerational care, and the moderation of intergenerational care duration and frequency. In doing so, we can promote the concept of active aging, which acknowledges the potential productivity and happiness of older people.
6 Limitations
This research study possesses several limitations that should be acknowledged. Firstly, due to constraints related to time and sample loss, the data used in this study were collected from one period. However, as survey questionnaires have time constraints in tracking information, it is possible that some previous caregivers were missed. Furthermore, social desirability and recall bias may result in measurement errors. Secondly, the study solely examined the relationship between intergenerational care and depression in older individuals, without concluding a causal link. Depression is a complex phenomenon, which can be affected by numerous conditions; this study has merely focused on one. Thirdly, the participants in our interviews were from China, and caution is advised when attempting to generalize the results to other countries.
Data availability statement
Publicly available datasets were analyzed in this study. This data can be found here: http://charls.pku.edu.cn/.
Author contributions
SH: Data curation, Investigation, Supervision, Writing – original draft. JG: Formal analysis, Investigation, Visualization, Writing – original draft. JX: Methodology, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Acknowledgments
We are immensely grateful to the editor and reviewers for their insightful and constructive comments that have significantly enhanced the quality and value of this paper.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Wang, Z . World population growth slows as humanity enters an era of low growth–world population prospects 2019 symposium held in Beijing. Popul Health. (2019) 7:14–5.
2. Hou, JM, Zhang, PD, and Zhou, WJ. The impact of intergenerational support on the mental health status of the Chinese older population. J Popul. (2021) 43:88–98. doi: 10.16405/j.cnki.1004-129X.2021.05.008
3. Ma, L, and Pan, H. Research on intergenerational care: a review and outlook. Henan Soc Sci. (2019) 27:106–11.
4. Wu, H . The impact of caring for grandchildren on the older adult support of urban first-generation elder only child parents. Soc Sci. (2019) 4:71–80. doi: 10.13644/j.cnki.cn31-1112.2019.04.007
5. Wang, G . A study on the impact of intergenerational care on active aging. China: Shandong University of Finance and Economics (2022).
7. Xiao, Y . The impact of intergenerational caregiving on the health status of older people - an empirical study based on CHARLS. Soc Secur Res. (2017) 50:33–9. doi: 10.3969/j.issn.1674-4802.2017.01.004
8. Song, L, and Feng, X. Intergenerational parenting: an analytical framework with grandparents as a perspective. J Shaanxi Normal Univ. (2018) 1:83–9. doi: 10.15983/j.cnki.sxss.2018.0123
9. Musil, CM, Gordon, NL, Warner, CB, Zauszniewski, JA, Standing, T, and Wykle, M. Grandmothers and caregiving to grandchildren: continuity, change, and outcomes over 24 months. The Gerontologist. (2011) 51:86–100. doi: 10.1093/geront/gnq061
10. Peterson, TL . Open house as a tool to connect schools to grandparents raising grandchildren. Child Sch. (2017) 39:25–32. doi: 10.1093/cs/cdw043
11. Lo, M, and Liu, YH. Quality of life among older grandparent caregivers: a pilot study. J Adv Nurs. (2009) 65:1475–84. doi: 10.1111/j.1365-2648.2009.05000.x
12. Baker, LA, and Silverstein, M. Depressive symptoms among grandparents raising grandchildren: the impact of participation in multiple roles. J Inter Relations. (2008) 6:285–304. doi: 10.1080/15350770802157802
13. Fuller-Thomson, E, and Minkler, M. African American grandparents raising grandchildren: a national profile of demographic and health characteristics. Health Soc Work. (2000) 25:109–18. doi: 10.1093/hsw/25.2.109
14. Han, B, and Wang, S. Effects of caring for grandchildren on the health of middle-aged and older adults. Popul Res. (2019) 43:85–96.
15. Song, L, Yang, L, and Peng, X. An empirical study of intergenerational caregiving and health outcomes among older adults in China and policy considerations. J Popul. (2020) 42:55–69. doi: 10.16405/j.cnki.1004-129X.2020.01.005
16. Huang, G, Du, P, and Chen, G. Exploring the impact of intergenerational care on the health of older people in China. Popul Dev. (2016) 22:93–100. doi: 10.3969/j.issn.1674-1668.2016.06.010
17. Tsai, FJ, Motamed, S, and Rougemont, A. The protective effect of taking care of grandchildren on elders’ mental health? Associations between changing patterns of intergenerational exchanges and the reduction of elders’ loneliness and depression between 1993 and 2007 in Taiwan. BMC Public Health. (2013) 13:567. doi: 10.1186/1471-2458-13-567
18. Kanji, S . Grandparent care: a key factor in mothers' labour force participation in the UK. J Soc Policy. (2018) 47:523–42. doi: 10.1017/S004727941700071X
19. Song, L, Li, L, and Li, S. A study on the impact of older people caring for their grandchildren on intergenerational conflict in rural families. Psychol Sci. (2016) 39:1137–43. doi: 10.16719/j.cnki.1671-6981.20160518
20. Zhang, W, and Chen, M. Psychological distress of older Chinese: exploring the roles of activities, social support, and subjective social status. J Cross Cult Gerontol. (2014) 29:37–51. doi: 10.1007/s10823-013-9219-0
21. Cheng, Z, Ye, X, and Chen, G. A study on the association between intergenerational care, living arrangement and depressive status among middle-aged and older adults. Popul Dev. (2017) 23:70–9. doi: 10.3969/j.issn.1674-1668.2017.02.008
22. Grundy, EM, Albala, C, Allen, E, Dangour, AD, Elbourne, D, and Uauy, R. Grandparenting and psychosocial health among older Chileans: a longitudinal analysis. Aging Ment Health. (2012) 16:1047–57. doi: 10.1080/13607863.2012.692766
23. Shen, L, and Zhang, Z. Intergenerational caregiving and the mental health of middle-aged and older adults: the mediating role of family closeness. Psychol Behav Res. (2020) 18:234–40. doi: 10.3969/j.issn.1672-0628.2020.02.013
24. Zhang, J . The relationship between perceived physical health and death anxiety in intergenerational parenting grandparents: The mediating effect of life meaning. China: Sichuan Normal University (2018).
25. Christiansen, GS . The association between grandparenthood and mortality. Soc Sci Med. (2014) 118:89–96. doi: 10.1016/j.socscimed.2014.07.061
26. Lee, GR, Netzer, JK, and Coward, RT. Depression among older parents: the role of intergenerational exchange. J Marriage Fam. (1995) 57:823–33. doi: 10.2307/353935
27. Zhao, J, Guan, W, and Wang, J. The impact of "reverse feedback" on the mental health of older people. J Jinan. (2022) 44:39–55. doi: 10.3969/j.issn.1000-5072.2022.02.004
28. Fang, H, Lei, Z, Lin, L, Zhang, P, and Zhou, M. Family companionship and older suicide: evidence from the Chinese lunar new year. J Dev Econ. (2023) 162:103055. doi: 10.1016/j.jdeveco.2023.103055
29. Chen, X, and Silverstein, M. Intergenerational social support and the psychological well-being of older parents in China. Res Aging. (2000) 22:43–65. doi: 10.1177/0164027500221003
30. Catherine, G, and Merril, S. Grandmothers raising grandchildren: family structure and well-being in culturally diverse families. Gerontologist. (2002) 42:676–89. doi: 10.1093/geront/42.5.676
31. Zhang, Y, and Liu, J. Analysis of the impact of intergenerational care on the physical and mental health of the older adult and the mechanism--an empirical analysis based on the 2014 data of the China social tracking survey of the older adult. Agric Technol Econ. (2022) 324:117–31. doi: 10.13246/j.cnki.jae.2022.04.007
32. Wang, Y . A study on the impact of intergenerational care for grandchildren on the psychological health of middle-aged and older people. Sci Dec Making. (2018) 254:47–68. doi: 10.3773/j.issn.1006-4885.2018.09.047
33. Ko, PC, and Hank, K. Grandparents caring for grandchildren in China and Korea: findings from CHARLS and KLoSA. J Gerontol B Psychol Sci Soc Sci. (2014) 69:646–51. doi: 10.1093/geronb/gbt129
34. Jin, X, and Liu, Y. The impact of caring for grandchildren on the life satisfaction of the older adult - a study based on mobile and non-mobile older people. J Southeast Univ. (2017) 19:119–129+148. doi: 10.13916/j.cnki.issn1671-511x.2017.02.016
35. Ku, L, Stearns, SC, van Houtven, CH, Lee, SYD, Dilworth-Anderson, P, and Konrad, TR. Impact of caring for grandchildren on the health of grandparents in Taiwan. J Gerontol B. (2013) 68:1009–21. doi: 10.1093/geronb/gbt090
36. Song, L, Li, S, and Li, L. A study on the impact of providing care for grandchildren on the psychological health of rural older people. Popul Dev. (2008) 78:10–8.
37. Sun, J, and Ji, Y. The impact of caring for grandchildren on attitudes toward aging among Chinese older adults. Popul Dev. (2016) 22:79–86. doi: 10.3969/j.issn.1674-1668.2016.04.010
38. Tong, X . The production and reproduction of unequal gender relations: an analysis of domestic violence in China. Sociol Res. (2000) 1:102–11. doi: 10.19934/j.cnki.shxyj.2000.01.009
39. Wu, Q . A survey on the living conditions of "migratory bird" older people from rural areas who have moved to the city to take care of their grandchildren - an exploratory study. South Popul. (2014) 29:51–61. doi: 10.3969/j.issn.1004-1613.2014.03.007
40. Wu, J . A study on the impact of moderate intergenerational care on the psychological health of female older adult. Chengdu, China: Sichuan Academy of Social Sciences (2021).
41. Cohen, S, and Wills, TA. Stress, social support, and the buffering hypothesis. Psychol Bull. (1985) 98:310–57. doi: 10.1037/0033-2909.98.2.310
42. Kahn, RL, and Antonucci, TC. Convoys over the life course: attachment, role, and social support. Life Span Dev Behav. (1980) 3:253–86.
43. Chan, YK, and Lee, RPL. Network size, social support and happiness in later life: a comparative study of Beijing and Hong Kong. J Happiness Stud. (2006) 7:87–112. doi: 10.1007/s10902-005-1915-1
44. Singh, L, Singh, PK, and Arokiasamy, P. Social network and mental health among older adults in rural Uttar Pradesh, India; a cross-sectional study. J Cross Cult Gerontol. (2016) 31:173–92. doi: 10.1007/s10823-016-9286-0
45. Domènech-Abella, J, Lara, E, Rubio-Valera, M, Olaya, B, Moneta, MV, Rico-Uribe, LA, et al. Loneliness and depression in the elderly: the role of social network. Soc Psychiatry Epidemiol. (2017) 52:381–90. doi: 10.1007/s00127-017-1339-3
46. Bert, H, and Kaminskip, L. Grandparents raising their grandchildren: a review of the literature and suggestions for practice. Gerontologist. (2005) 45:262–9. doi: 10.1093/geront/45.2.262
47. Chen, F, and Liu, G. The health implications of grandparents caring for grandchildren in China. J Gerontol. (2012) 67B:99–112. doi: 10.1093/geronb/gbr132
48. Balukonis, J, Melkus, GD, and Chyun, D. Grandparenthood status and health outcomes in midlife African American women with type 2 diabetes. Ethn Dis. (2008) 18:141–6. Available at: https://www.jstor.org/stable/48667323
49. Peng, Z, Zou, H, and He, Q. Social childcare resources, intergenerational care and labor participation of middle-aged and older adults. Finance Econ Sci. (2019) 12:53–66.
50. Zou, H, Peng, Z, and Luan, B. Intergenerational caregiving and female labor supply-an analysis of the comprehensive two-child and delayed retirement paradox in a caregiving perspective. Econ Dyn. (2018) 7:37–52.
51. Rosenbaum, PR, and Rubin, DB. Constructing a control group using multivariate matched sampling methods that incorporate the propensityscore. Am Stat. (1985) 39:33–8. doi: 10.1080/00031305.1985.10479383
52. Zhang, X . Research on the current policy problems and countermeasures of community-based older adult care in China. Law Soc. (2020) 34:110–1. doi: 10.19387/j.cnki.1009-0592.2020.12.053
53. Zhu, S, and Sun, C. Research on activity theory-based older adult-friendly community older adult service platform for migrant older adult. Packag Eng. (2022) 43:129–38. doi: 10.19554/j.cnki.1001-3563.2022.14.015
54. Yang, M, Li, Z, and Li, L. Internet use and the mental health of older adults - a two-level digital inequality perspective. Popul Dev. (2022) 28:132–47.
55. Bernhold, QS, and Giles, H. Paternal grandmothers benefit the most from expressing affection to grandchildren: an extension of evolutionary and sociological research. J Soc Pers Relat. (2019) 36:514–34. doi: 10.1177/0265407517734657
56. Dolbin-macnab, M, Jarrott, S, Moore, L, O'hora, K, De Chavonnes Vrugt, M, and Erasmus, M. Dumela Mma: an examination of resilience among south African grandmothers raising grandchildren. Ageing Soc. (2016) 36:2182–212. doi: 10.1017/S0144686X15001014
57. Buchanan, A, and Rotkirch, A. Twenty-first century grandparents: global perspectives on changing roles and consequences. Contemp Soc Sci. (2018) 13:131–44. doi: 10.1080/21582041.2018.1467034
58. Craig, L, and Jenkins, B. Grandparental childcare in Australia: gender differences in the correlates of providing regular grandparental care while parents work. Community Work Fam. (2015) 19:281–301. doi: 10.1080/13668803.2015.1027176
Keywords: intergenerational care, depression, older people, propensity score matching, heterogeneity
Citation: Han S, Guo J and Xiang J (2024) Is intergenerational care associated with depression in older adults? Front. Public Health. 12:1325049. doi: 10.3389/fpubh.2024.1325049
Edited by:
Vahid Rashedi, University of Social Welfare and Rehabilitation Sciences, IranReviewed by:
Lambert Zixin Li, Stanford University, United Statesİsmail Toygar, Mugla University, Türkiye
Patricia M. Alt, Towson University, United States
Karolina Kopacz, Medical University of Lodz, Poland
Copyright © 2024 Han, Guo and Xiang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jianjun Xiang, amlhbmp1bi54aWFuZ0BmbXUuZWR1LmNu