
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
BRIEF RESEARCH REPORT article
Front. Public Health, 10 April 2024
Sec. Infectious Diseases: Epidemiology and Prevention
Volume 12 - 2024 | https://doi.org/10.3389/fpubh.2024.1324336
This article is part of the Research TopicUnsolved Challenges in Hepatitis B and Hepatitis C: Host-Virus Interaction, Molecular Pathogenesis and Treatment StrategiesView all 7 articles
 Anna Pocurull1,2
Anna Pocurull1,2 Cristina Collazos1Anna Miralpeix1Laura Tapias1Tao Wang1
Cristina Collazos1Anna Miralpeix1Laura Tapias1Tao Wang1 María Jose Moreta1Zoe Mariño1,2
María Jose Moreta1Zoe Mariño1,2 Sabela Lens1,2*
Sabela Lens1,2* Xavier Forns1,2
Xavier Forns1,2Introduction: Hepatitis B infection (HBV) is prevalent in China. Due to language barriers and cultural differences, it is not always straightforward to evaluate disease knowledge in liver clinics. We aimed to assess the awareness on HBV and its mechanisms of transmission in HBV-infected Chinese patients and their household contacts.
Methods: HBV-infected Chinese patients and their contacts were interviewed by a native Chinese nurse regarding their knowledge on HBV transmission mechanisms, use of preventive measures and vaccination status. Non-Chinese HBV-infected patients and their household contacts served as a control group.
Results: In total 182 patients and 398 contacts participated with 85 (47%) patients and 240 (60%) contacts being from China. Language barrier was reported in 80% of Chinese patients and 44% of their contacts. Knowledge on parenteral and sexual HBV transmission was high in all patients (~90%) but Chinese were more aware of vertical transmission than controls (94% vs. 68%; p < 0.01). Regarding the use of preventive measures, Chinese patients were more forewarned in their use to avoid parenteral transmission (93% vs. 74%, p < 0.01). When assessing household contacts, Chinese used preventive measures more frequently than controls for parenteral and sexual transmission (79% vs. 65 and 81% vs. 48%, p < 0.05). Vaccination coverage was slightly lower in Chinese contacts compared to controls (78% vs. 86%, p = 0.05).
Conclusion: Despite relevant language barriers, Chinese patients are well informed on the mechanisms of HBV transmission. Cultural differences may explain a higher use of preventive measures among the Chinese population. HBV vaccination of household contacts should be reinforced in both groups.
Hepatitis B is a potentially life-threatening liver infection and a major global health problem (1, 2). In highly endemic areas, hepatitis B virus (HBV) is most commonly spread by perinatal transmission or through parenteral transmission (exposure to infected blood) (3, 4), while in less endemic areas is commonly spread sexually (5–8). Familiar transmission has also been described (9, 10), most likely due to the sharing of contaminated materials (11). The widespread use of hepatitis B vaccine in infants has considerably reduced the incidence of new chronic infections.
Due to the high prevalence of HBV infection in individuals from Asian origin (12), they represent a significant proportion of patients followed in Liver Disease Units in Spain. The Chinese community in Barcelona has grown considerably in the last 20 years and the last official data (2021) (13) indicate that more than 22.000 Chinese people are censored in the city. Importantly, around one third live in the area of influence of our University Hospital. Access to Health-Care services is not optimal in this population; indeed it is quite frequent that the first contact of Chinese individuals with the Health System is during pregnancy (when HBsAg is screened) (14). Given the relevant language barriers and cultural differences, we hypothesized that Chinese HBV-infected patients and their relatives might be less aware on the mechanisms of HBV transmission and vaccine coverage.
Our aim was to measure the awareness on hepatitis B mechanisms of transmission in HBV-infected Chinese patients and household contacts, and to assess their vaccination status.
This is an observational case–control study. All patients with a diagnosis of chronic hepatitis B of Chinese origin followed at our Liver Unit from 2020 to 2022 were invited to participate. A similar number of non-Chinese HBV-infected patients were used as a control group. The only exclusion criteria was refusal to participate in the study. The following variables were recorded for each patient: age, sex, initial HBV diagnosis, current antiviral therapy, HBV-DNA levels, last transient elastography value and the presence of cirrhosis.
All patients and their household contacts were contacted telephonically by personnel of the study (LT, TW) to undergo an interview. To avoid potential language and cultural barriers a Chinese nurse (TW) contacted Chinese patients and their contacts. In case a patient/household contact did not speak Mandarin, family members helped in the translation. For patients, the interview included a question on their level of Spanish, level of education, knowledge on the mechanisms of HBV transmission (parenteral, sexual, vertical) and use of preventive measures for HBV transmission (Supplementary Table S1). For household contacts the interview included demographic data, familiar relationship with the patient, level of Spanish, knowledge on the mechanisms of HBV transmission (parenteral, sexual, vertical), the use of preventive measures and the status of HBV vaccination (Supplementary Table S1). The question regarding the use of preventive measures for sexual transmission was only asked to patients’ partners. Children below age 14 were not interviewed, and only their vaccination status was recorded.
Relative frequency is expressed in percentage. Quantitative variables are depicted as median (percentiles 25 and 75).
Regarding qualitative variables, differences between groups were calculated by the Chi-square test. For quantitative variables, differences between groups were calculated by Student’s t-test. Multivariate analysis was conducted using logistic regression, including variables exhibiting a p value <0.1 in the univariate analysis. Individuals who did not provide an answer were not included in the analysis. A p-value <0.05 was considered statistically significant. All computations were carried out in IBM SPSS Statistics version 21.0 (IBM, Chicago, USA).
The study was approved by Hospital Clínic Barcelona Ethics Committee (HCB/2021/0752) and informed consent was obtained from all the participants and from the legal guardians of the participants who were below 18 years of age. The consent was written in Chinese for patients of this origin. An oral authorization from all patients was obtained to allow us to contact their relatives, who also gave oral approval to be interviewed. All data was registered anonymously.
From 142 HBV-infected Chinese patients with records in our database, 2 did not give their consent to participate and 55 were not reached after 3 phone call attempts in different days. Thus, 85 Chinese patients were finally included in the study.
In the control group, from the initial 142 consecutive HBV-infected Caucasian patients 3 declined to participate, 6 were dead and 36 were not reached after 3 phone call attempts. Thus, 97 non-Chinese patients were finally included in the study.
The main characteristics of the patient cohorts are depicted in Table 1. Age did not differ between the two groups, but female sex was significantly higher in the Chinese cohort. In both groups, the most common diagnosis was HBeAg-negative Chronic Hepatitis B infection (around 50%). The proportion of patients under NAs (nucleos(t)ide analogs) therapy was significantly greater for Chinese (48%) compared to control (36%). HBV-DNA was detectable in 50% of patients, similar between groups.
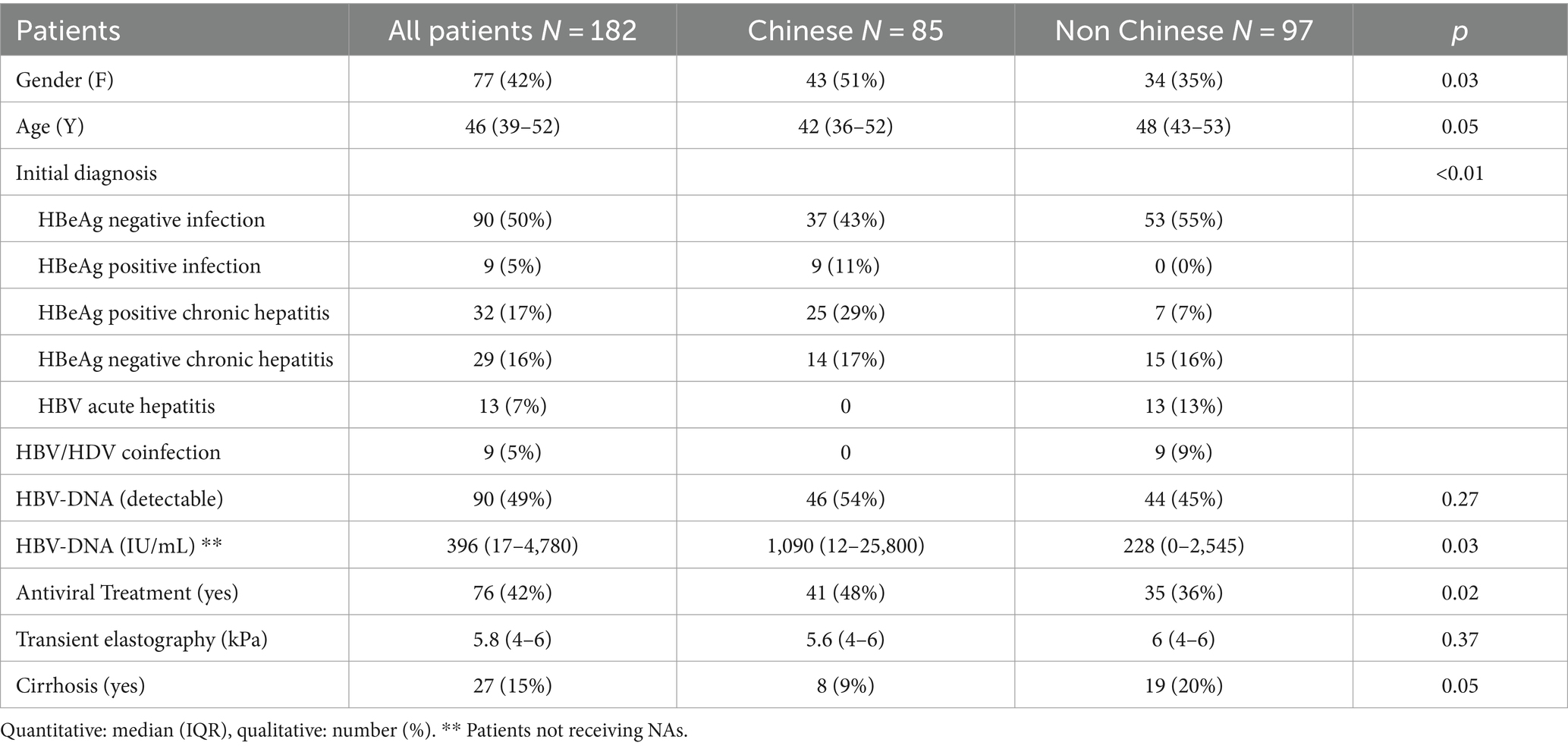
Table 1. Baseline characteristics of patients.
A total of 398 household contacts were telephonically interviewed, 60% Chinese and 40% Caucasian.
Among Chinese patients 68 of 85 (80%) acknowledged major limitations in the understanding of Spanish. The level of education was significantly higher in the control group than in Chinese patients (Table 2).
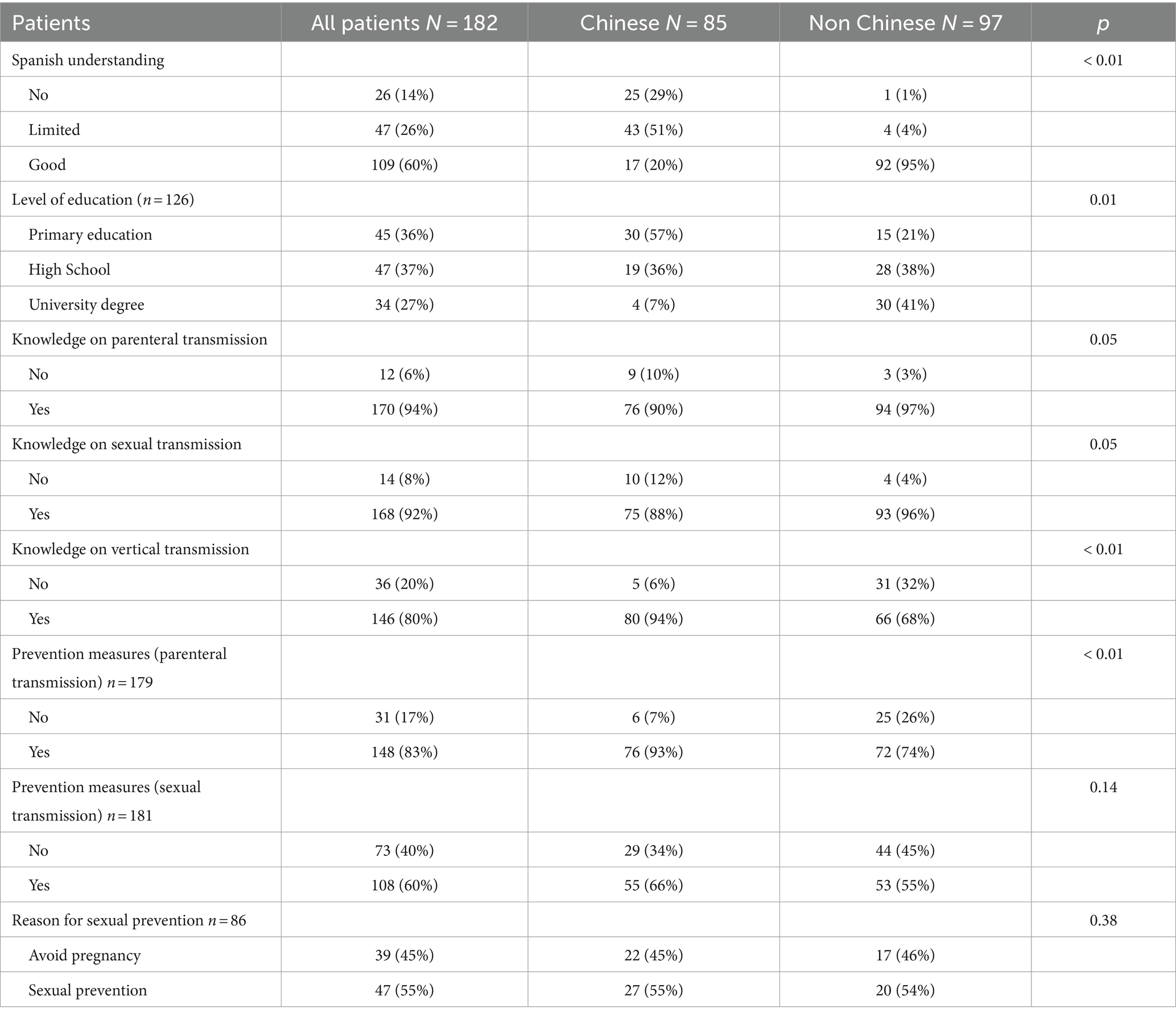
Table 2. Knowledge and attitude regarding HBV transmission and comparison between Chinese vs. non-Chinese patients.
Overall awareness on parenteral and sexual HBV transmission was good (~90%), with better results in the control group compared to Chinese patients, but not reaching statistical significance (p = 0.05 for both variables). Males were more aware on sexual transmission than females (97% vs. 86%) (Table 3) and male sex was the only variable independently associated with a better knowledge on HBV sexual transmission (OR 5.02 CI 95% 1.3–18.9; p = 0.02) (Supplementary Table S2).
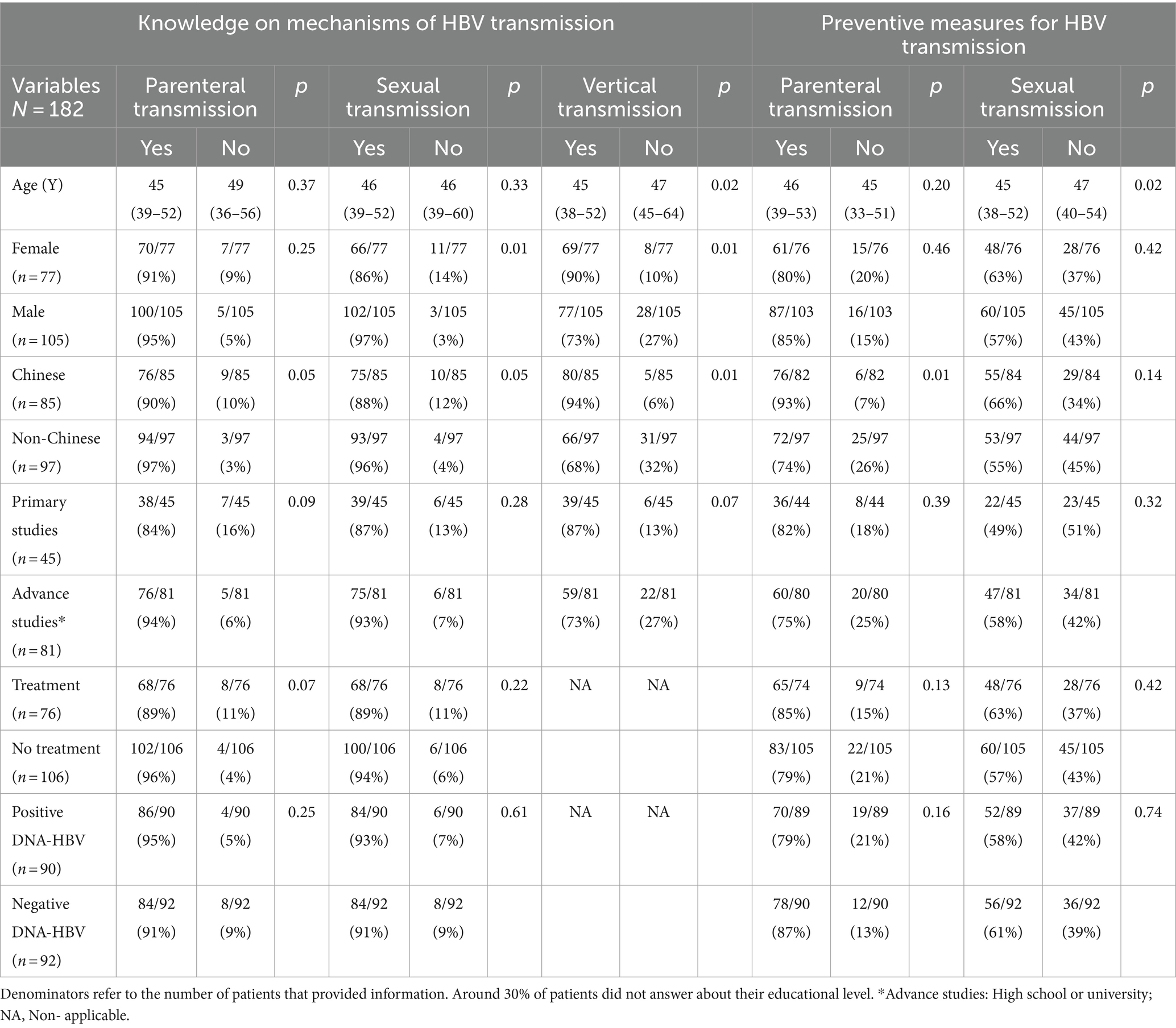
Table 3. Knowledge of transmission routes and preventive measures according to clinical, demographic, and virological characteristics in patients.
Awareness on HBV vertical transmission was significantly better in Chinese patients (94%) compared to controls (68%, p < 0.01). Younger age and female sex were also associated with a better knowledge on vertical transmission (Table 3), but the only variable independently related to knowledge on vertical transmission by multivariate analysis was Chinese origin (OR 4.9 CI 95% 1.5–16.2, p = 0.01) (Supplementary Table S2).
Regarding the use of preventive measures to avoid parenteral HBV transmission (sharing scissors, toothbrush, or manipulation of infected patients’ wounds) being Chinese was the only variable associated with its use (93% for Chinese vs. 74% for controls, p < 0.01); we did not find any relationship with age, sex, or being on NAs therapy. Concerning preventive measures to avoid sexual HBV transmission, only a younger age was associated with a significantly higher use of preventive measures (Table 3). It is important to notice, however, that prevention of pregnancy was the reason for using barrier methods in ~50% of patients (Table 2).
For household contacts, the proportion of individuals with major limitations in the understanding of Spanish decreased to 44%.
As expected, most (96%) household contacts who answered the survey knew about HBV infection of the index patient. Among them, awareness on parenteral and sexual transmission was excellent among control individuals (96 and 95%, respectively) and fair among Chinese (86 and 81%, respectively); these differences reached statistical significance (Supplementary Table S3). Both groups had a similar awareness on HBV vertical transmission (>80%). Younger age was found to be associated with increased awareness of vertical transmission (Supplementary Table S4).
As we found in patients, the use of preventive measures to avoid parenteral HBV transmission was significantly higher in Chinese household contacts (Supplementary Tables S3, S4), being the only variable associated with its use. Concerning preventive measures to avoid sexual HBV transmission, we only interviewed patients’ partners. We found a significantly higher use of preventive methods in Chinese (81%) than in control partners (48%, p < 0.01) (Supplementary Table S3).
Antiviral treatment (patients) or vaccination status (household contacts) did not influence the use of preventive measures (Supplementary Table S5).
When asked about their vaccination status, 74 (19%) household contacts reported not being fully vaccinated (three completed doses) (Supplementary Table S3). When comparing both groups, household contacts of Chinese patients had a slightly lower vaccination rate compared to controls (78% vs. 86%, p = 0.05). Importantly, when household contacts of Chinese patients were categorized by place of birth, the rate of vaccination was 96% if born in Spain compared to only 59% if born in China (p < 0.01).
HBV is a highly transmissible virus and thus, knowledge on the potential mechanisms of transmission and measures to prevent it are relevant. Our initial hypothesis was that in migrants from areas of high HBV prevalence, language barriers and cultural differences might difficult engagement into local healthcare and educational programs and consequently, decrease awareness on diagnosis and prevention of hepatitis B (15, 16).
Contrarily to our hypothesis, we found that Chinese patients were aware of the routes of HBV transmission. Differences between Chinese and control patients were slight regarding the parenteral and sexual routes, but patients from China had a significantly better knowledge on the potential vertical transmission of the virus. The different epidemiology of HBV infection in Asia (mainly transmitted from mother-to-child) compared to Europe (where HBV is mainly transmitted by the sexual route) is the most likely explanation, since origin (and not educational level or sex) was the only variable independently associated with vertical transmission awareness. Our data seem to be in accordance with data published by Huang et al. (17) and suggest that information on HBV transmission mechanisms in Chinese patients were acquired in China.
When the same questions were asked to household contacts, we found that awareness of parenteral and sexual transmission mirrored the pattern seen in patients, with a slightly (but significant) lower knowledge among Chinese individuals. Interestingly, the better knowledge on HBV vertical transmission of Chinese patients was lost for household contacts. Since half of them were born in Spain, the latter may just reflect the epidemiology of HBV infection in our country, with a prevalence below 1%, and practical absence of vertical transmission (18).
Regarding the use of preventive measures to avoid HBV transmission, we found that Chinese patients and their relatives were more prone to use them. This finding is against our initial hypothesis, since we believed that language barriers would negatively impact the use of preventive measures. One potential explanation might be that Asian population is well instructed in the use of barriers to avoid infections (not only those transmitted by the parenteral route but also by air). Moreover, stigma caused by HBV infection is still a problem in mainland China (19), where the infection is associated with fear of contagion (20). Thus, we believe that our findings mainly reflect different cultural backgrounds between Asia and Europe.
Vaccine coverage was overall good; however, when comparing HBV vaccination in relatives from Chinese and native patients, we found a lower (although not significant) vaccination rate in the first group. Nevertheless, when better dissecting the vaccination rates among household contacts of Chinese patients, we found a practical universal coverage in relatives born in Spain (where HBV vaccination is universal since 1991), compared to rates below 60% in those born in China. The latter reflects the lower vaccination coverage in China in the adult population (21). Thus, results from our study emphasize the need to (22) further promote vaccination among this group of individuals at risk.
The study has some limitations. First, a sample size was not estimated due to the lack of solid data in the literature to establish a hypothesis on the expected differences between Chinese and Non-Chinese patients. Second, around 30% of household contacts were not available for the interview, and we cannot exclude that this introduced a selection bias. Second, all collected data are self-reported and interviews were performed by phone, which might not be as accurate as face-to-face (21). Another limitation is that lack of validation of our questionnaire; however, we based our interview on well-known mechanisms of HBV transmission and followed the main items described by the Centers for Disease Control and Prevention (21). Finally, questions about potential misconception on HBV transmission, such as transmission by shaking hands or sharing food were not included in the questionnaire (17).
In summary, we found that, despite the presence of relevant language barriers, Chinese HBV-infected patients are well informed on the mechanisms of HBV transmission. Chinese patients and household contacts used preventive measures more frequently, which might be explained by cultural differences. An important finding was the low rate of HBV vaccination among household contacts born in China, which requires a targeted public health intervention.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving humans were approved by Ethics commitee Hospital Clínic Barcelona. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants’ legal guardians/next of kin. Written informed consent was obtained from the minor(s)’ legal guardian/next of kin for the publication of any potentially identifiable images or data included in this article.
AP: Conceptualization, Data curation, Formal analysis, Methodology, Validation, Visualization, Writing – original draft. CC: Data curation, Validation, Visualization, Writing – review & editing. AM: Data curation, Validation, Visualization, Writing – review & editing. LT: Validation, Visualization, Data curation, Writing – review & editing. TW: Data curation, Validation, Visualization, Writing – review & editing. MM: Data curation, Validation, Visualization, Writing – review & editing. ZM: Data curation, Investigation, Methodology, Validation, Visualization, Writing – review & editing. SL: Data curation, Investigation, Methodology, Supervision, Validation, Visualization, Writing – review & editing. XF: Data curation, Formal analysis, Funding acquisition, Project administration, Resources, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. XF has received support from Secretaria d’Universitats i Recerca del Departament d’Economia i Coneixement (grant 2021_SGR_01322) and CERCA Programme/Generalitat de Catalunya. SL has received funding from ISCIII (PI20/00609), from Asociación Española para el Estudio del Hígado (AEEH) and Societat Catalana de Digestologia (SCD). AP has received support from the Rio Hortega program (fellowship CM21/00081) of the Instituto de Salud Carlos III and an initiation research grant from SCD.
XF has acted as advisor for Gilead. SL and ZM has received fees for lectures and consulting from Gilead, Abbvie, Orphalan, Alexion and Deep Genomics, and a research grant from Gilead.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2024.1324336/full#supplementary-material
1. Shepard, CW, Simard, EP, Finelli, L, Fiore, AE, and Bell, BP. Hepatitis B virus infection: epidemiology and vaccination. Epidemiol Rev. (2006) 28:112–25. doi: 10.1093/epirev/mxj009
2. World Health Organization. (2007). Global hepatitis report. Available at:https://www.who.int/publications/i/item/9789241565455
3. van Damme, P, Cramm, M, van der Auwera, JC, Meheus, A, and Vranckx, R. Horizontal transmission of hepatitis B virus. Lancet. (1995) 345:27–9. doi: 10.1016/S0140-6736(95)91155-3
4. Yao, GB. Importance of perinatal versus horizontal transmission of hepatitis B virus infection in China. Gut. (1996) 38:S39–42. doi: 10.1136/gut.38.Suppl_2.S39
5. Maddrey, WC. Hepatitis B: an important public health issue. J Med Virol. (2000) 61:362–6. doi: 10.1002/1096-9071(200007)61:3<362::AID-JMV14>3.0.CO;2-I
6. Francis, DPHTS, et al. The prevention of hepatitis B with vaccine. Report of the centers for disease control multi-center efficacy trial among homosexual men. Ann Intern Med. (1982) 97:362–6. doi: 10.7326/0003-4819-97-3-362
7. Mele, A, Franco, E, Caprilli, F, Gentili, G, Stazi, MA, Zaratti, L, et al. Hepatitis B and Delta virus infection among heterosexuals, homosexuals and bisexual men. Eur J Epidemiol. (1988) 4:488–91. doi: 10.1007/BF00146404
8. Szmuness, WMIPA, Much, I, Prince, AM, Hoofnagle, JH, Cherubin, CE, Harley, EJ, et al. On the role of sexual behavior in the spread of hepatitis B infection. Ann Intern Med. (1975) 83:489–95. doi: 10.7326/0003-4819-83-4-489
9. Erol, S, Ozkurt, Z, Ertek, M, and Tasyaran, MA. Intrafamilial transmission of hepatitis B virus in the eastern Anatolian region of Turkey. Eur J Gastroenterol Hepatol. (2003) 15:345–9. doi: 10.1097/00042737-200304000-00002
10. Oon, CJ, Chen, WN, Goo, KS, and Goh, KT. Intra-familial evidence of horizontal transmission of hepatitis B virus surface antigen mutant G145R. J Infect. (2000) 41:260–4. doi: 10.1053/jinf.2000.0751
11. van der Eijk, AA, Niesters, HGM, Götz, HM, Janssen, HLA, Schalm, SW, Osterhaus, ADME, et al. Paired measurements of quantitative hepatitis B virus DNA in saliva and serum of chronic hepatitis B patients: implications for saliva as infectious agent. J Clin Virol. (2004) 29:92–4. doi: 10.1016/S1386-6532(03)00092-1
12. Chen, Y, Xie, C, Zhang, Y, Li, Y, Ehrhardt, S, Thio, CL, et al. Knowledge regarding hepatitis B mother-to-child transmission among healthcare workers in South China. J Viral Hepat. (2018) 25:561–70. doi: 10.1111/jvh.12839
13. Ajuntament de Barcelona. (2021). Estadística i difusió de dades. Available at:https://ajuntament.barcelona.cat/estadistica/catala/Estadistiques_per_temes/Poblacio_i_demografia/Documents_relacionats/pobest/a2021/part1/nt46.htm.
14. Badanta-Romero, B, Lucchetti, G, and Barrientos-Trigo, S. Access to healthcare among Chinese immigrants living in Seville, Spain. Gac Sanit. (2021) 35:145–52. doi: 10.1016/j.gaceta.2019.09.008
15. Huang, Z, Liu, T, Qin, Y, Chen, J, Ou, Z, and Min, X. A cross-sectional survey on the rate of awareness of hepatitis B virus (HBV) infection and the prevention of mother-to-child transmission among hepatitis B surface antigen (HBsAg)-positive pregnant women. Ann Transl Med. (2022) 10:773–3. doi: 10.21037/atm-22-2748
16. Sheng, QJ, Wang, SJ, Wu, YY, Dou, XG, and Ding, Y. Hepatitis B virus serosurvey and awareness of mother-to-child transmission among pregnant women in Shenyang, China. Medicine. (2018) 97:e10931. doi: 10.1097/MD.0000000000010931
17. Huang, J, Guan, ML, Balch, J, Wu, E, Rao, H, Lin, A, et al. Survey of hepatitis B knowledge and stigma among chronically infected patients and uninfected persons in Beijing, China. Liver Int. (2016) 36:1595–603. doi: 10.1111/liv.13168
18. Razavi-Shearer, D, Gamkrelidze, I, Nguyen, MH, Chen, DS, van Damme, P, Abbas, Z, et al. Global prevalence, treatment, and prevention of hepatitis B virus infection in 2016: a modelling study. Lancet Gastroenterol Hepatol. (2018) 3:383–403. doi: 10.1016/S2468-1253(18)30056-6
19. Liu, K. Hepatitis B infection in China: the stigma behind the stigmata. Liver Int. (2016) 36:1582–4. doi: 10.1111/liv.13189
20. Cotler, SJ, Cotler, S, Xie, H, Luc, BJ, Layden, TJ, and Wong, SS. Characterizing hepatitis B stigma in Chinese immigrants. J Viral Hepat. (2012) 19:147–52. doi: 10.1111/j.1365-2893.2011.01462.x
21. Bai, X, Chen, L, Liu, X, Tong, Y, Wang, L, Zhou, M, et al. Adult hepatitis B virus vaccination coverage in China from 2011 to 2021: a systematic review. Vaccines. (2022) 10:900. doi: 10.3390/vaccines10060900
22. Xiao, Y, Wallace, J, Ahad, M, van Gemert, C, Thompson, AJ, Doyle, J, et al. Assessing the feasibility, acceptability and impacts of an education program on hepatitis B testing uptake among ethnic Chinese in Australia: results of a randomised controlled pilot study. BMC Public Health. (2021) 21:1861. doi: 10.1186/s12889-021-11916-0
Keywords: chronic hepatitis B, language barrier, hepatitis B knowledge, cultural background, hepatitis B vaccination
Citation: Pocurull A, Collazos C, Miralpeix A, Tapias L, Wang T, Moreta MJ, Mariño Z, Lens S and Forns X (2024) Influence of language barrier and cultural background in hepatitis B disease knowledge in a Chinese community of Spain. Front. Public Health. 12:1324336. doi: 10.3389/fpubh.2024.1324336
Edited by:
Juarez Antonio Simões Quaresma, Federal University of Pará, BrazilReviewed by:
Maureen Dar Iang, Heidelberg University Hospital, GermanyCopyright © 2024 Pocurull, Collazos, Miralpeix, Tapias, Wang, Moreta, Mariño, Lens and Forns. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Sabela Lens, c2xlbnNAY2xpbmljLmNhdA==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.