 Liangyuan Zhang
Liangyuan Zhang Jianzhou Yang
Jianzhou Yang Rila Su
Rila Su Xinquan Lan
Xinquan Lan Moxin Song1,2
Moxin Song1,2 Junjie Xu
Junjie Xu- 1Clinical Research Academy, Peking University Shenzhen Hospital, Shenzhen, China
- 2Department of Epidemiology, China Medical University, Shenyang, Liaoning, China
- 3Department of Public Health and Preventive Medicine, Changzhi Medical College, Changzhi, Shanxi, China
- 4Cancer Center of Inner Mongolia People's Hospital, Hohhot, Inner Mongolia, China
- 5Johns Hopkins Bloomberg School of Public Health, Baltimore, MD, United States
- 6Department of Oncology, Peking University Shenzhen Hospital, Shenzhen, China
Background: Despite the elevated COVID-19 risk for older adults with cancer, vaccine hesitancy poses a significant barrier to their immunization. Intriguingly, there is limited research on the prevalence of willingness to receive the second booster dose and associated determinants in older adults with cancer.
Objective: Our objective was to ascertain the level of awareness about COVID-19 vaccines and to uncover the factors influencing the willingness to receive the second booster among Chinese cancer patients aged 65 years and over.
Methods: To achieve our objective, we conducted a multicenter cross-sectional study in four tertiary hospitals from four provinces of China. This involved using a Health Belief Model (HBM) based self-administered questionnaire and medical records. Subsequently, we employed multivariable logistic regression to identify factors influencing the second COVID-19 booster vaccine willingness.
Results: Our results showed that among 893 eligible participants, 279 (31.24%) were aged 65 years and over, and 614 (68.76%) were younger. Interestingly, the willingness to receive the second COVID-19 booster vaccine was 34.1% (95/279) (OR: 1.043, 95% CI: 0.858, 1.267) in participants aged 65 years and over, which was similar to participants aged under 65 years (34.1% vs. 35.5%, p = 0.673). Furthermore, our findings revealed that a positive attitude toward the booster and recommendations from healthcare providers and family members were positively associated with vaccine willingness. Conversely, perceptions of negative impacts on cancer control and vaccine accessibility regarding the second COVID-19 booster were inversely related to the outcome event (all p < 0.05).
Conclusion: Our study concludes with the finding of a low willingness toward the second COVID-19 booster in Chinese cancer patients, particularly in the older adults, a fact which warrants attention. This reluctance raises their risk of infection and potential for severe outcomes. Consequently, we recommend using media and community outreach to dispel misconceptions, promote the booster’s benefits, and encourage vaccine discussions with healthcare providers and family members.
1 Introduction
COVID-19, an infectious disease instigated by the SARS-CoV-2 virus, rapidly escalated into a worldwide pandemic since its debut in December 2019 (1). Preliminary research suggests that cancer patients and senior citizens, two key demographics, face a heightened risk of severe disease and mortality following infection with COVID-19, compared to the general population (2–4). An alarming 86.8% of COVID-19-related fatalities among 13 European nations were individuals aged 70 years and over (5). Likewise, the global prevalence of cancer in COVID-19 patients stood at 4.63%, yet a staggering 43.26% of cancer patients infected with COVID-19 suffered from severe disease manifestations (6). These figures underscore the critical need for implementing effective preventative measures, such as vaccination, to tackle the health threats posed by COVID-19 (7). Building on this, COVID-19 vaccines have demonstrated considerable efficacy in halting disease transmission, positioning themselves as one of the most cost-effective strategies to manage the pandemic (7, 8). Nonetheless, evidence points toward a gradual decrease in vaccine effectiveness against SARS-CoV-2 following the primary immunization schedule (9–11). Notably, this decline is more conspicuous among cancer patients and the older adults relative to their healthier counterparts (12–14). Contemporary evidence indicates that a second booster dose can enhance the immunogenicity of COVID-19 vaccines in these crucial groups, thereby augmenting vaccine effectiveness and reducing risks of infection, severe illness, hospitalization, and death (15, 16). To further substantiate this, the United States Food and Drug Administration (FDA) and China’s Bureau of Disease Control and Prevention endorse an additional booster dose for immunocompromised individuals, including the older adults and adults suffering from severe underlying conditions such as cancer, after completing the primary three-dose COVID-19 vaccination regimen (12, 17).
However, despite these facts, a considerable impediment to the universal willingness of the COVID-19 s booster dose is vaccine reluctance among cancer patients. Previous studies disclose that 56.4% of cancer patients display apprehension toward the second booster dose (18), attributing their concerns to potential adverse impacts on their cancer prognosis, uncertainty surrounding the vaccine’s interaction with their ongoing treatment, and fear of vaccine-related side effects (18–20). Simultaneously, in Hong Kong, China, 52.4% of the older adults displayed hesitancy toward the second booster, primarily due to worries over vaccine safety and efficacy, vaccine accessibility, perceived susceptibility to the disease, and perceived benefits of vaccination (21, 22). While prior research has probed vaccine hesitancy in both cancer patients and the older adults, the intersection of these two demographics remains a relatively unexplored territory.
Acknowledging the knowledge gap in research focused on the factors influencing vaccine hesitancy toward the COVID-19 s booster dose among older cancer patients, our study aims to understand the cognitive perceptions and willingness to vaccinate within this demographic. This understanding is crucial for health authorities to formulate targeted interventions, potentially enhancing vaccination rates in this vulnerable group. The Health Belief Model (HBM), a well-established psychological model that explains health-related behaviors. This theoretical framework allows us to explore how components of HBM, such as perceived susceptibility, benefits, barriers, and cues to action, are associated with vaccine willingness in this particular group (23).
Moreover, much of the research on vaccine willingness has predominantly been conducted in single-center settings, which restricts the representativeness and generalizability of their findings. This limitation can hinder their usefulness for understanding the factors influencing vaccination willingness for the second booster dose. Therefore, in light of these limitations, the current study utilizes a multicenter cross-sectional survey to examine the prevalence and factors influencing vaccination willingness for the COVID-19 s booster dose among older and non-older adults with cancer. By doing so, this research aspires to provide a solid scientific basis for the development of effective vaccination strategies to enhance vaccination rates among these vulnerable groups.
2 Materials and methods
2.1 Study design
Utilizing a multi-center, cross-sectional design, this study was carried out from April to June 2022 across four prominent tertiary healthcare institutions in three distinct regions of China. These encompassed Shanxi Heping Hospital (affiliated with Changzhi Medical College), Inner Mongolia People’s Hospital in North China, the First Affiliated Hospital of Xinjiang Medical University in Northwest China, and Guangdong Peking University Shenzhen Hospital in South China. The study design employed cluster sampling, wherein each of the four regional hospitals functioned as individual units for selection.
2.2 Participants
The eligibility criteria for participants included: (1) being 18 years or older; (2) being cancer patients admitted to any of the four participating hospitals during the study period; and (3) displaying a willingness to participate in the study by providing signed informed consent. Exclusions were made for individuals diagnosed with lymphoma, leukemia, or mental illness, those under medication for mental disorders, and patients having communication difficulties with researchers (Figure 1).
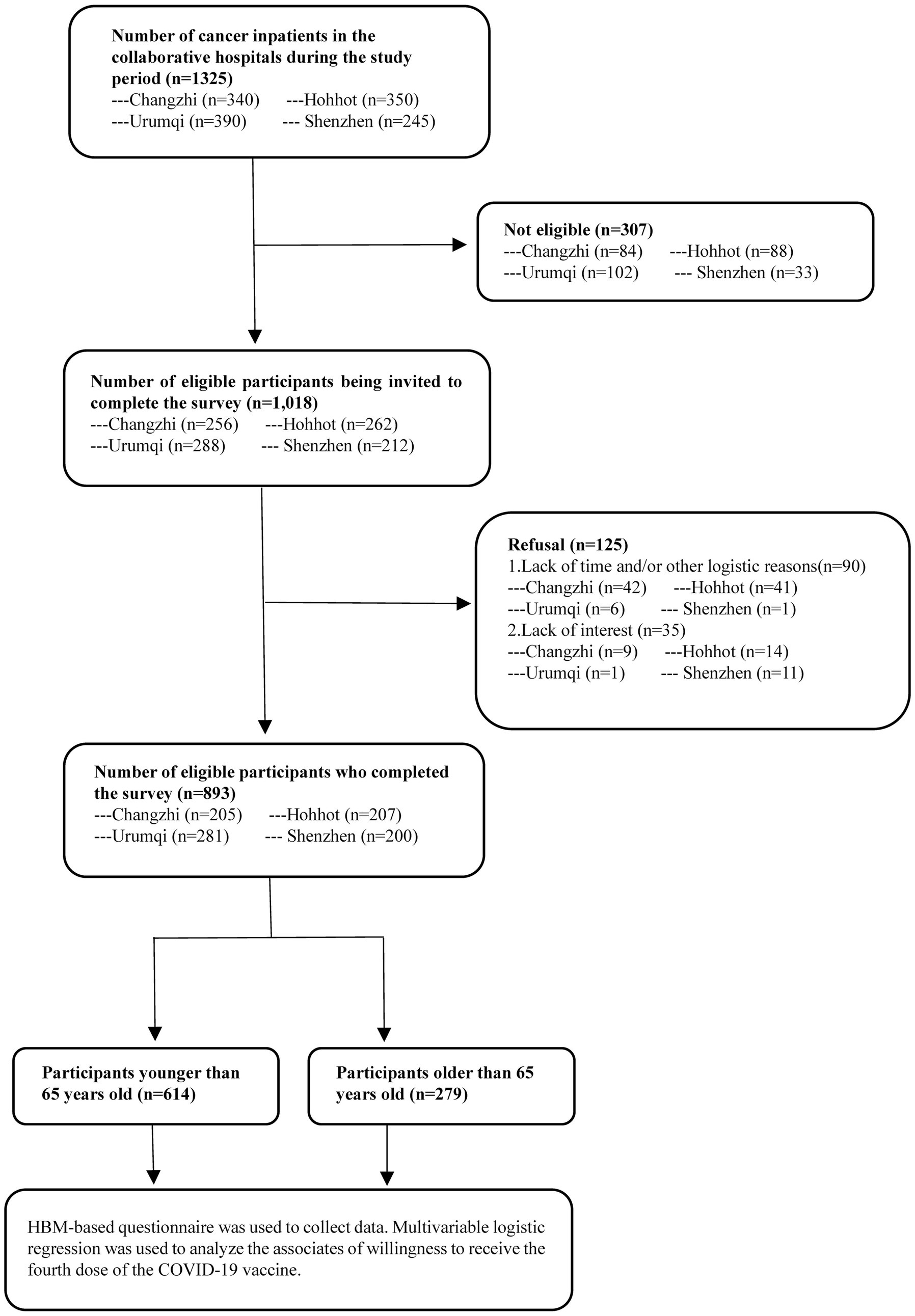
Figure 1. The data collection procedures of this study.
2.3 Data collection
Data was collected by medical staff from each participating hospital who were tasked with patient recruitment and screening within their respective oncology departments. Patients meeting the specified inclusion and exclusion criteria were selected via field interviewer questionnaire surveys. After acquiring informed consent, these participants completed self-administered questionnaires on the Jinshuju platform. All procedures strictly adhered to the Declaration of Helsinki’s principles, with ethical approval granted by the Institutional Review Board of Changzhi Medical College. The questionnaire-based surveys commenced only after receiving participants’ written informed consent.
2.4 Methods
2.4.1 Design and content of the questionnaire
A team of epidemiologists, statisticians, behavioral health experts, health psychologists, and oncologists collaboratively crafted the survey questionnaire. The reliability and validity of the questionnaire were ensured via a pilot study. The individual-level variables segment of the survey drew upon the Health Belief Model (HBM), a recognized framework for studying vaccination beliefs and intentions. The survey was divided into categories covering: (1) demographic and background characteristics; (2) receipt of the first COVID-19 vaccine booster; (3) willingness to receive the second booster; (4) individual-level variables such as attitudes and perceptions toward COVID-19 vaccine boosters; (5) comprehension of the booster vaccination’s potential impact on cancer treatment; (6) vaccination fatigue; and (7) frequency of contemplating the validity of specific pandemic information. The main outcome measure was the participants’ willingness to receive the second booster dose of the COVID-19 vaccine, measured on a Likert scale (24), spanning from “strongly disagree” to “strongly agree.” For analysis purposes, responses were subsequently categorized into “unwilling to vaccinate” or “uncertain about vaccination” groups as vaccine hesitancy, following the approach adopted by Kimberly A Fisher (25).
2.4.2 Sample size calculation
The sample size was calculated using a simple random sampling formula with a significance level α of 0.05, yielding Z1-α/2 = 1.96, and an allowable error δ of 0.05. We anticipated that the estimated booster dose rate for COVID-19 vaccines among cancer patients aged 65 years and over would be around 50%. The design effect (deff) was used for further sample size computation, considering the cluster sampling strategy. As per prior research (26), the deff value was set at 1.5. The initial sample size of 576, when accounting for a non-response rate of 20%, necessitated a minimum sample size of 720 respondents.
2.4.3 Statistical analysis
We used descriptive statistics, the χ2 test, and Fisher’s exact test to probe associations between study outcomes and various explanatory variables. The treatment of missing data was as follows: variables with more than 30% missing data were omitted from the analysis, while for variables with less than 30% missing data, imputation techniques such as autoregressive modeling or mean imputation were applied. Autoregressive modeling is used for time-related missing data patterns, while mean imputation is used for randomly missing data.
To assess the impact of various factors on the intention to receive the second COVID-19 vaccine booster among older adults with cancer, our initial analysis involved univariate logistic regressions. These analyses evaluated the associations between demographic characteristics, specifically age groups, and booster uptake intentions. Participants were divided into two age groups: those aged 18–64 years and those aged 65 years and over. This stratification was in response to the revised focus on older adults with cancer. Significant variables (p < 0.1) from the univariate analysis were then included in a comprehensive multivariable logistic regression model. This model was tailored to assess the combined effect of all pertinent variables on the willingness to receive the booster dose in these distinct age groups. The approach facilitated a nuanced understanding of how each factor, particularly age, contributed to the decision-making process regarding vaccine uptake. Adjusted odds ratios (AORs) from the multivariable logistic regression provided insights into the relative importance and interplay of these variables in determining the willingness to receive the second booster dose among cancer patients, segmented by the two age groups. All data analyses were performed using IBM SPSS software (Version 25.0; IBM Corporation, Armonk, New York, USA), and statistical significance was determined using a two-sided p-value of less than 0.05.
3 Results
In this section, we present a summarized view of our key findings. Initially, we explore the background characteristics of the cancer inpatients, comparing demographic differences between age groups. Following this, we analyze factors influencing the willingness for the second COVID-19 booster dose, utilizing the Health Belief Model (HBM) as a framework. The focus will be on contrasting these factors among patients aged 65 years and over with those under 65 years.
3.1 Background characteristics
This section provides a detailed analysis of the demographic characteristics of the cancer patients in our study, as shown in Table 1.
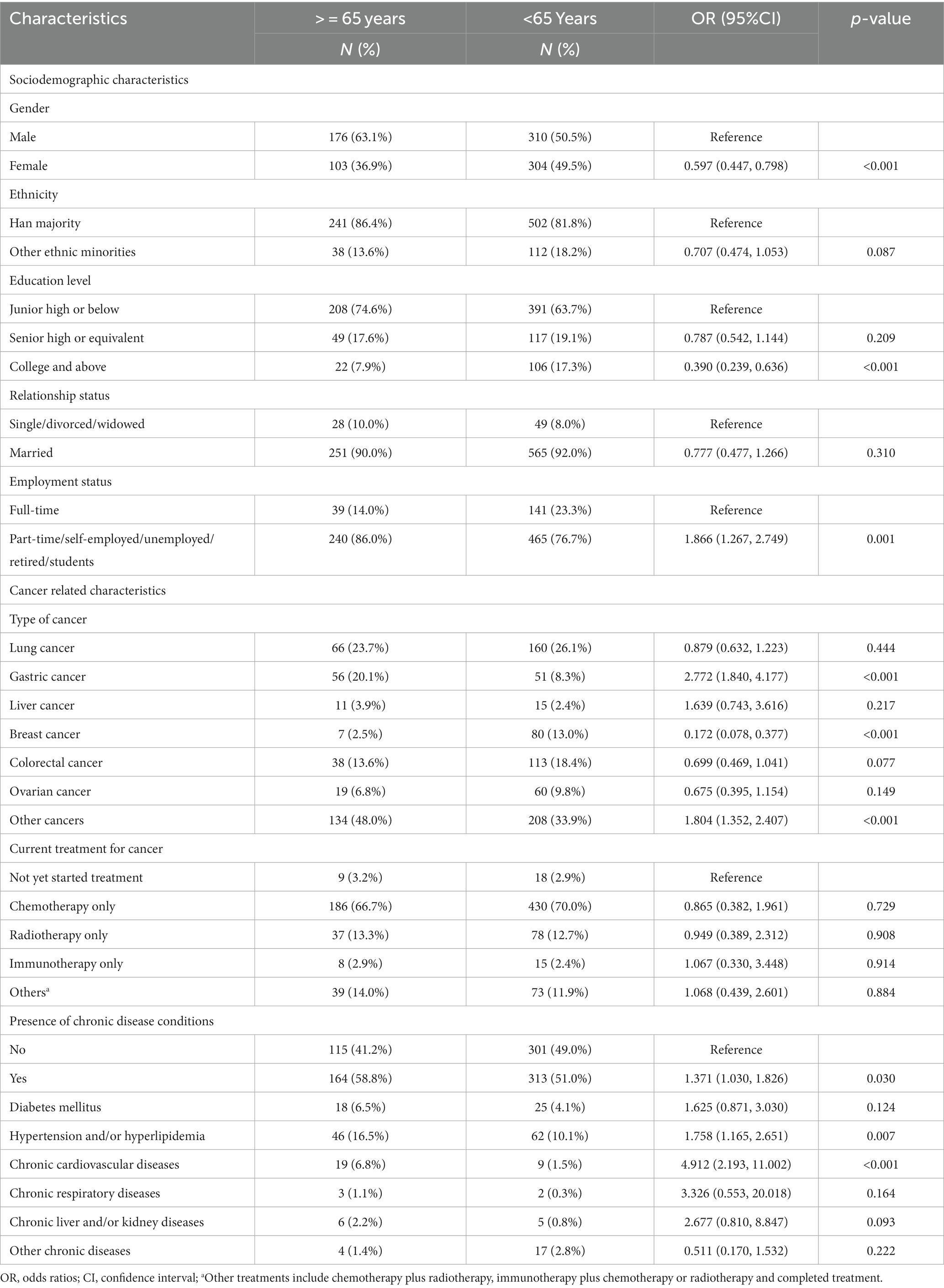
Table 1. Background characteristics of participants.
During the research period, 1,325 cancer inpatients were recruited from four survey sites, of which 1,018 cases (76.8%) met the inclusion criteria. After informed consent, 893 eligible participants completed the interview, among which 279 participants (31.2%) aged 65 years and over, and 614 participants (68.8%) under 65 years. Compared to the group aged less than 65, participants aged 65 years and over had a higher proportion of males (63.1% vs. 50.5%), gastric cancer (20.1% vs.8.3%), other cancers (48.0% vs. 33.9%), hypertension and hyperglycemia (16.5% vs. 10.1%) and chronic cardiovascular diseases (6.8% vs. 1.5%) (all p < 0.05). In contrast, older participants had a lower proportion with college or above education (7.9% vs. 17.3%), full-time employment (14.0% vs. 23.3%) and breast cancer (2.5% vs. 13.0%) compared to the younger group (all p < 0.05). Other characteristics did not show significant statistical differences between the two groups (p > 0.05) (Table 1).
3.2 HBM relevant variables to the willingness for the second dose of COVID-19 booster vaccination
This section analyzes how individual-level factors, based on the Health Belief Model, are connected to the willingness for the second dose of the COVID-19 booster vaccine, as shown in Table 2.
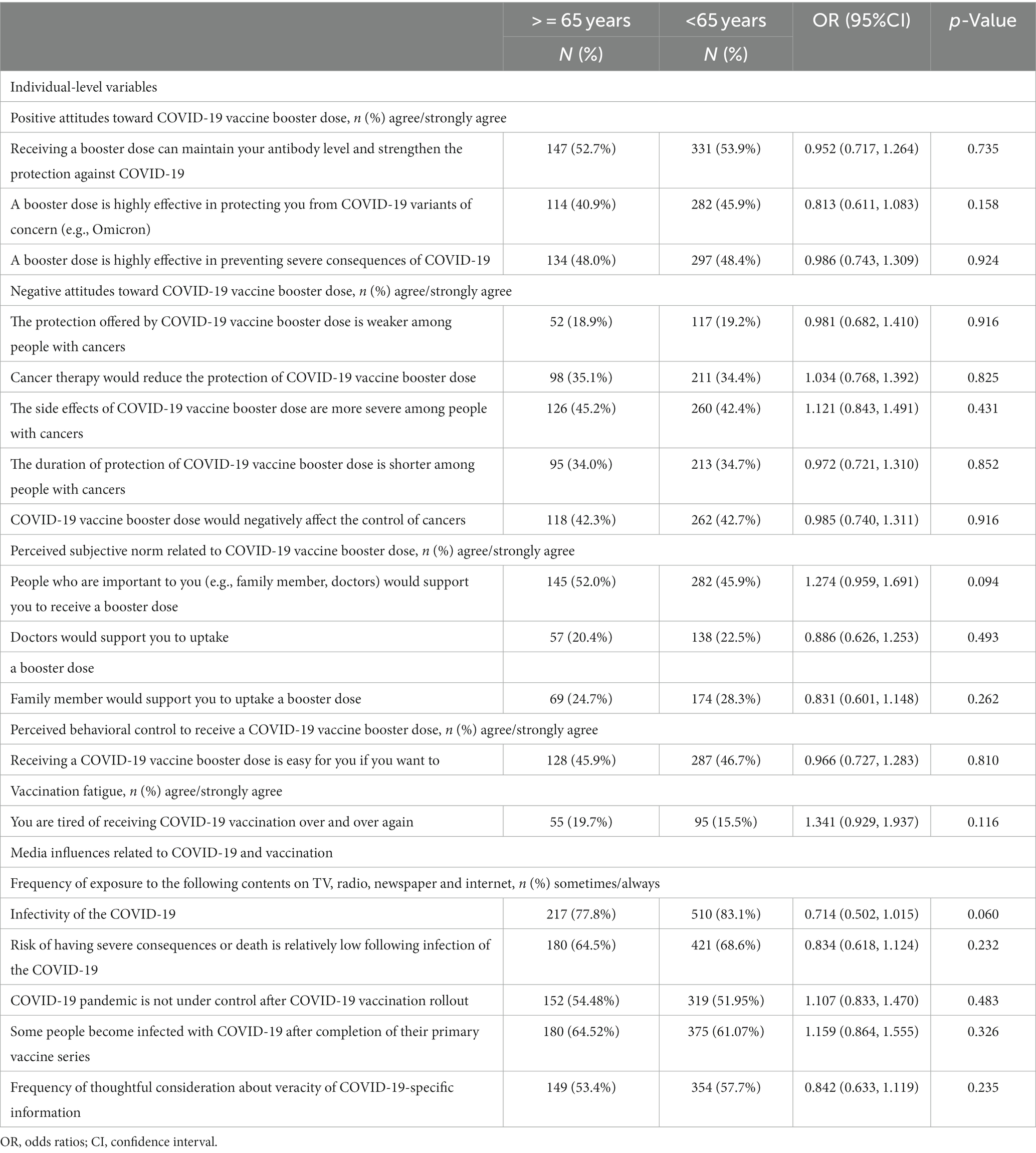
Table 2. The HBM relevant variables for the willingness to receive the second dose of COVID-19 booster vaccination.
There were also no significant differences in individual-level variables concerning the COVID-19 vaccine booster dose, such as positive attitudes, negative attitudes, perceived subjective norm, vaccination fatigue, consideration about the veracity of COVID-19 specific information and the Media influences related to COVID-19 and vaccination (p > 0.05) (Table 2).
3.3 Willingness for the second dose of COVID-19 booster vaccination and associated factors among patients aged 65 years and over
In this section, we examine the factors that affect the willingness of patients aged 65 years and over to get the second dose of the COVID-19 booster vaccine. Detailed results can be found in Table 3.
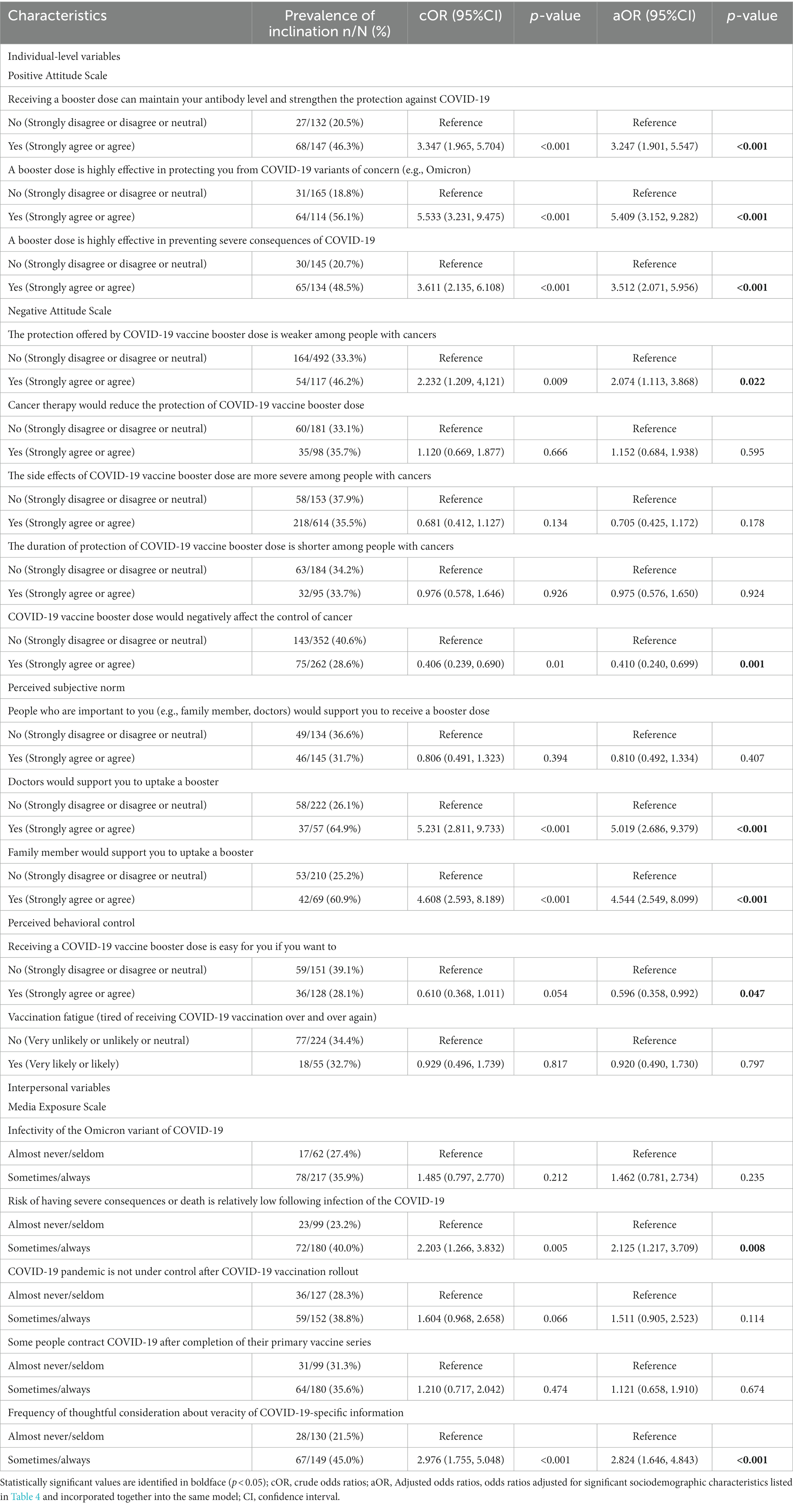
Table 3. Willingness for the second dose of COVID-19 booster vaccination and associated factors among patients aged 65 years and over (N = 279).
Patients aged 65 years and over demonstrated a higher initial COVID-19 booster vaccination uptake proportion than those under 65 years (76.3% vs. 68.1%, p = 0.012), yet there was no significant difference shown in the willingness for a second booster among these two cancer patient groups (34.1% vs. 35.5%, p > 0.05). However, significant differences in the willingness for a second booster of the vaccine were found at the four survey sites (Shanxi site: 22.7%, Inner Mongolia site: 15.7%, Xinjiang site: 53.7%, Guangdong: 12.5%, p < 0.05).
Univariate analysis revealed a positive association between patients aged over 65 years from other ethnic minorities and the willingness for the fourth COVID-19 vaccine booster vaccination (Table 4).
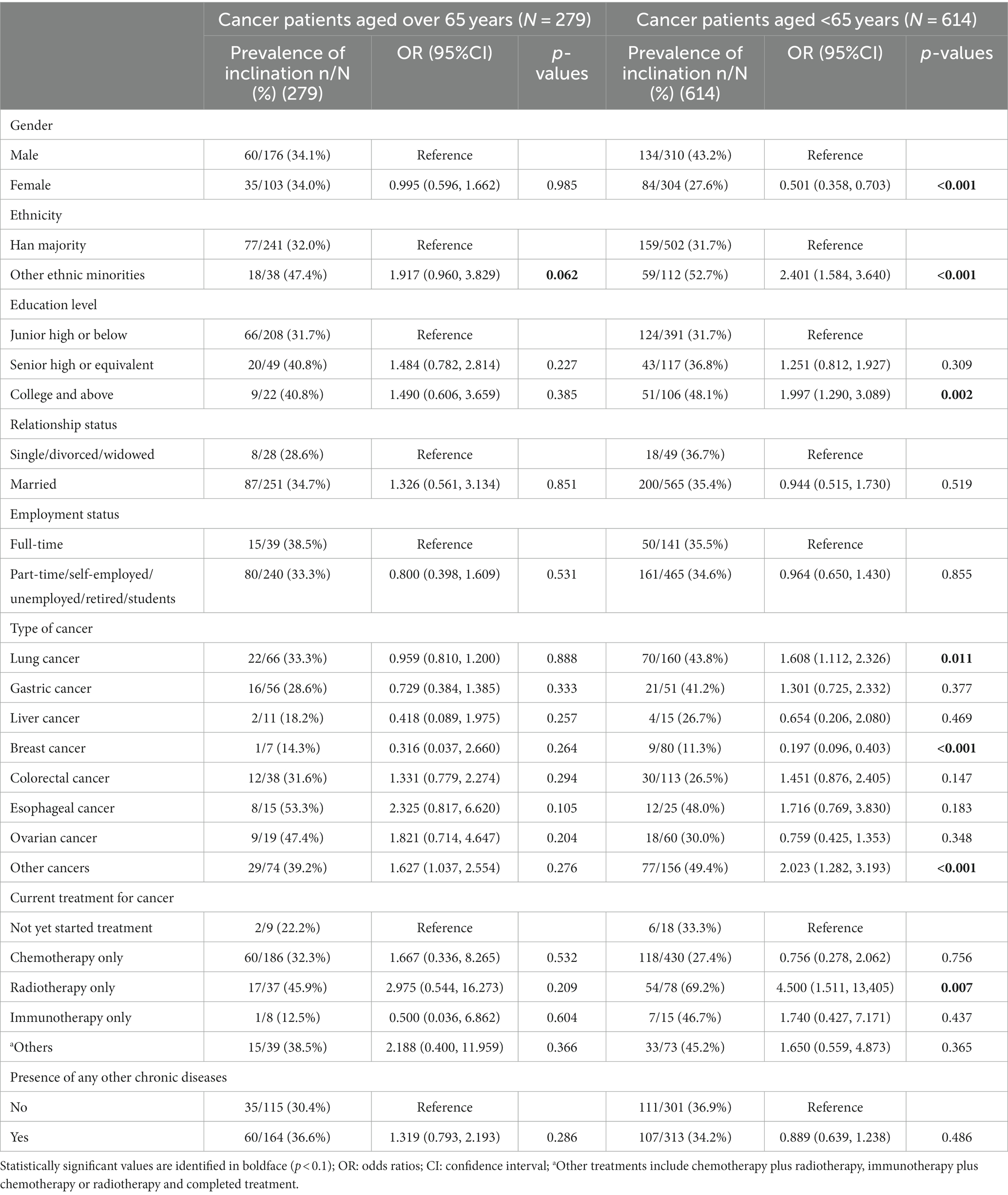
Table 4. Associations between background characteristics and the willingness of the second COVID-19 vaccine booster vaccination (N = 893).
The multivariable logistic regression was used to adjust for significant background variables (p < 0.1) and to incorporate them into the same model. Post adjustment for the ethnic minorities factor, several variables, such as positive attitudes about the vaccine’s effectiveness in maintaining antibody levels (AOR: 3.247, 95% CI: 1.901, 5.547), protection against COVID-19 variants (AOR: 5.409, 95% CI: 3.152, 9.282), and prevention of severe COVID-19 consequences (AOR: 3.512, 95% CI: 2.071, 5.956), correlated with a higher willingness for the booster dose. Negative attitudes about the booster’s efficacy in cancer patients also influenced the inclination for the booster dose, such as the protection of booster dose is weaker among cancers (AOR: 2.074, 95% CI: 1.113, 3.868) while control of cancers is negatively affected among cancer patients (AOR: 0.410, 95% CI: 0.240, 0.699) (Table 3).
Additionally, the support of doctors and family member promoted higher uptake willingness of booster dose (AOR: 5.019, 95% CI: 2.686, 9.379 and AOR: 4.544, 95% CI: 2.549, 8.099). However, perceived behavioral control such as accessibility of vaccines hindered the uptake willingness of the booster dose (AOR: 0.596, 95% CI: 0.358, 0.992). Furthermore, the media exposure scale about the low fatality and severity of variations and frequent consideration about the veracity of COVID-19 specific information significantly promoted higher willingness uptake of the booster dose (AOR: 2.125, 95% CI: 1.217, 3.709 and AOR: 2.824, 95% CI: 1.646, 4.843) (Table 3).
3.4 Willingness for the second dose of COVID-19 booster vaccination and associated factors among patients under 65 years.
In this section, we examine the factors that affect the willingness of patients under 65 years to get the second dose of the COVID-19 booster vaccine. Detailed results can be found in Table 5.
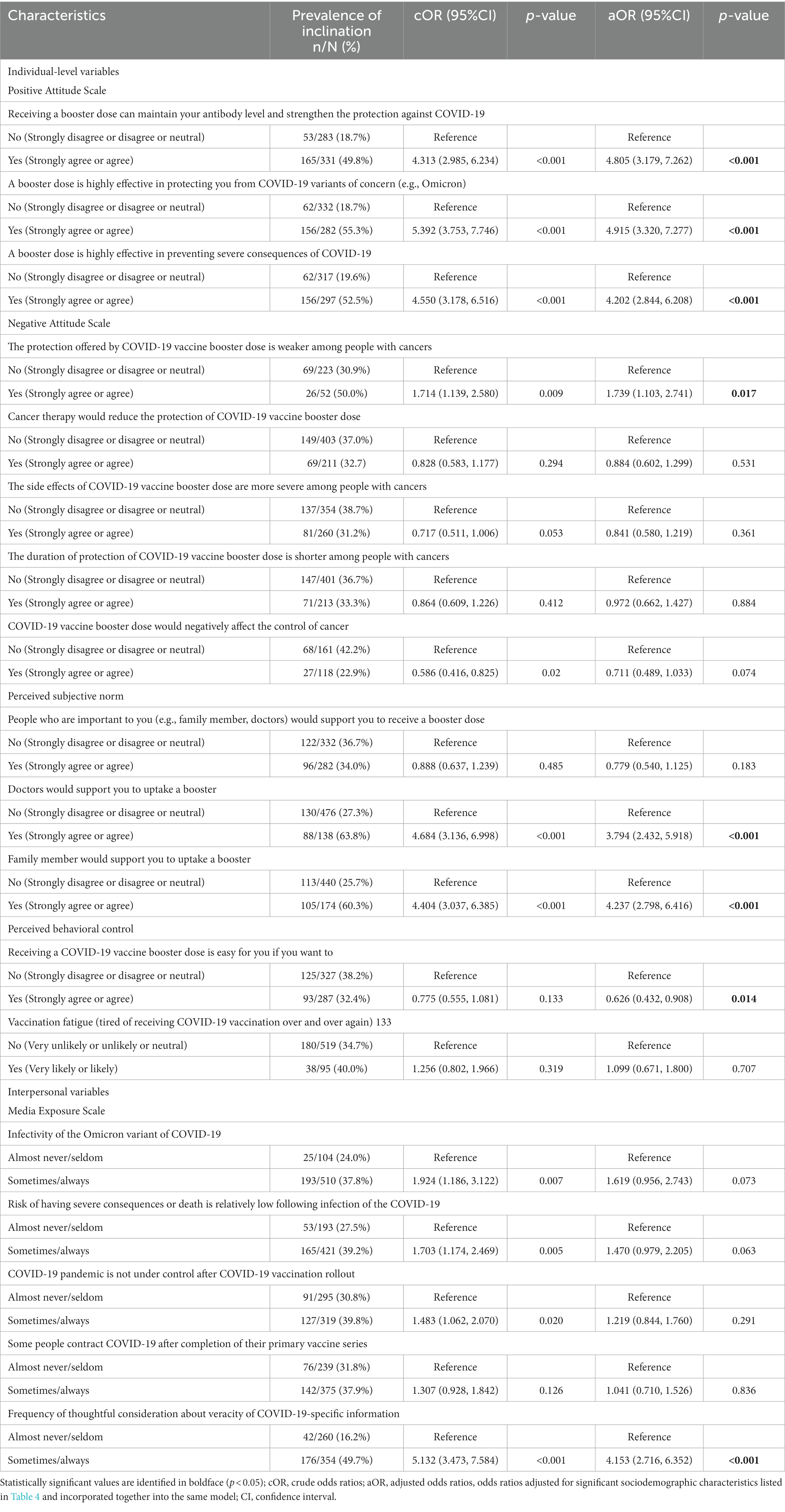
Table 5. Willingness for the second dose of COVID-19 Booster vaccination and associated factors among patients under 65 years (N = 614).
In the under 65 years group, certain demographic factors, including other ethnicities, having a college or higher education, specific types of cancer, and current treatment regimen, positively associated with the willingness for the booster. Conversely, being female and having breast cancer negatively associated with the propensity for the booster (Table 4).
The multivariable logistic regression, adjusted for these significant factors (p < 0.1) and to incorporate them into the same model, revealed similar associations as seen in the older age group, including attitudes about the vaccine’s effectiveness, the support of doctors and family member (AOR: 5.019, 95% CI: 2.686, 9.379 and AOR: 4.544, 95% CI: 2.549, 8.099), and frequent consideration about the veracity of COVID-19 specific information (AOR: 4.153, 95% CI: 2.716, 6.352). Vaccine accessibility negatively correlated with the propensity for the second booster dose (AOR: 0.626, 95% CI: 0.432, 0.908) (Table 5).
4 Discussion
Our multi-center cross-sectional study examined the levels of vaccine hesitancy and its related factors among older adults with cancer in China concerning the second COVID-19 booster dose. Our findings revealed a markedly low inclination to receive the second booster, with only one-third of Chinese older adults with cancer expressing such a willingness. Key determinants of this hesitancy included the perceived COVID-19 threat, perceived benefits, self-efficacy, and cues to action. This study not only fills a gap in existing research but also lays the foundation for the development of targeted strategies to mitigate hesitancy and boost vaccination coverage rates within this highly vulnerable population.
Interestingly, we found no significant difference in the willingness to receive the second booster between older and non-older adults with cancer (34.1% vs. 35.5%, p = 0.673). This finding underscores the importance of addressing vaccination hesitancy across all age groups among cancer patients, as both these groups demonstrated lower willingness compared to previous studies in Hong Kong, China, and the United States (22, 27). However, given that cancer patients over 65 years have a higher risk of COVID-19 infection and death than younger cancer patients, more attention should be paid to promoting the second dose of COVID-19 vaccine for cancer patients over 65 years. However, the notable disparities in vaccine willingness observed among cancer patients residing in distinct regions necessitate targeted efforts in health education to address lower willingness rates in these areas.
Given the elevated vulnerability of both older adults and cancer patients to COVID-19 complications, it is crucial to confront hesitancy toward the second booster. According to our findings, one of the major determinants of this hesitancy was the fear that the vaccine could interfere with cancer treatment. This fear was more prevalent among older adults with cancer aged 65 years and over, and absent in the under-65 years group. This may be due to the fact that older adults with cancer over 65 years are relatively inconvenient to obtain external information through the Internet, smartphone and other means. Therefore, China needs to increase publicity and education on related concerns of older adults with cancer to eliminate their doubts when carrying out the second booster injection of COVID-19 vaccine for groups with underlying diseases.
Unexpectedly, we found that both older and non-older adults with cancer who perceived the booster as ineffective exhibited a higher willingness to get vaccinated. This paradox may be linked to a heightened awareness of COVID-19’s severity, leading to vaccine skepticism yet willingness. This hypothesis, however, requires further exploration.
Contrary to our expectations, our study found that easier access to vaccination was associated with diminished willingness to vaccinate. This may be explained by the “Veblen effect” (28), whereby easily attainable commodities are perceived as less valuable. Despite this, it remains crucial to improve vaccine accessibility among cancer patients.
We discovered that the attitudes toward booster shots, as well as recommendations from healthcare providers and family members, were positively correlated with the vaccine willingness among cancer patient participants. These findings suggest that garnering support from relatives, healthcare professionals, and the broader community is pivotal in promoting the uptake of the second dose of the COVID-19 booster vaccine among Chinese cancer patients.
This study boasts two main strengths. Firstly, its design as a multi-center cross-sectional survey ensures a broader representation of respondents compared to a single-center study. Secondly, our research undertook a side-by-side comparison of the willingness of cancer patients, both over and under 65 years of age, to receive the second COVID-19 vaccine booster dose. This comparison, along with an analysis of associated factors, offers valuable insights for guiding current vaccination promotion and education efforts targeted at the Chinese population. This study does have limitations. Firstly, the survey was conducted in the specific context of China’s epidemic strategy, so patient views and behaviors could change with evolving policies. Secondly, the focus on hospitalized cancer patients in four specific prominent tertiary healthcare institutions may limit the broader applicability of our findings to all cancer patients in China. Lastly, the cross-sectional nature of our study does not allow for causal inferences. Future research should be expanded to encompass a broader sample of the population, including diverse regional environments or a more extensive group of non-hospitalized cancer patients, and adapt to continuously evolving strategies to achieve more comprehensive applicability.
In conclusion, given the pronounced lack of willingness for the second COVID-19 vaccine booster shot among cancer patients, health departments must intensify their efforts. Strategies should aim to increase understanding of the severity of COVID-19 and the benefits of vaccination, especially among 65 years and over older adults with cancer. Differentiated approaches for patients of varying ages, while ensuring vaccine accessibility, are crucial. Further exploration should focus on the vaccine’s potential impact on cancer treatment and include non-hospitalized patients.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Institutional Review Board (or Ethics Committee) of Institutional Review Board of Changzhi Medical College (protocol code RT2022027). The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants' legal guardians/next of kin.
Author contributions
LiZ: Formal analysis, Software, Writing – original draft, Writing – review & editing. JY: Data curation, Project administration, Resources, Supervision, Writing – review & editing. RS: Data curation, Project administration, Resources, Supervision, Writing – review & editing. XL: Data curation, Supervision, Writing – review & editing. MS: Data curation, Supervision, Writing – review & editing. LeZ: Conceptualization, Methodology, Supervision, Writing – review & editing. JX: Conceptualization, Formal analysis, Funding acquisition, Methodology, Project administration, Supervision, Writing – review & editing, Writing – original draft.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This research was funded by the Shenzhen Science and Technology Innovation Committee Project, grant number JCYJ20220818102817038, Shenzhen’s Sanming Project, grant number SZSM201612061 and was funded by the Scientific Research Foundation of Peking University Shenzhen Hospital, grant number KYQD2022216.
Acknowledgments
The authors alone are responsible for the views expressed in this article and they do not necessarily represent the views, decisions, or policies of the institutions with which they are affiliated.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Organization WH. Coronavirus disease (COVID-19) pandemic. (2023). Available at: https://www.who.int/emergencies/diseases/novel-coronavirus-2019.
2. De Joode, K, Dumoulin, D, Tol, J, Westgeest, H, Beerepoot, L, Van den Berkmortel, F, et al. Dutch oncology COVID-19 consortium (DOCC): outcome of COVID-19 in patients with cancer in a nationwide cohort study. Ann Oncol. (2020) 31:S1207–8. doi: 10.1016/j.annonc.2020.08.2320
3. Prevention CDC. Medical conditions. (2023). Available at: https://www.cdc.gov/coronavirus/2019-ncov/need-extra-precautions/people-with-medical-conditions.html.
4. Dai, MY, Liu, DB, Liu, M, Zhou, FX, Li, GL, Chen, Z, et al. Patients with Cancer appear more vulnerable to SARS-CoV-2: a multicenter study during the COVID-19 outbreak. Cancer Discov. (2020) 10:783–91. doi: 10.1158/2159-8290.Cd-20-0422
5. Cohen, JF, Korevaar, DA, Matczak, S, Chalumeau, M, Allali, S, and Toubiana, J. COVID-19-related fatalities and intensive-care-unit admissions by age groups in Europe: a Meta-analysis. Front Med. (2021) 7:7. doi: 10.3389/fmed.2020.560685
6. Sitanggang, JS, Siregar, KB, Sitanggang, HH, and Sprinse, VN. Prevalence and characteristics of cancer patients with COVID-19: a meta-analysis study. F1000Research. (2021) 10:975. doi: 10.12688/f1000research.53539.1
7. Fiolet, T, Kherabi, Y, MacDonald, CJ, Ghosn, J, and Peiffer-Smadja, N. Comparing COVID-19 vaccines for their characteristics, efficacy and effectiveness against SARS-CoV-2 and variants of concern: a narrative review. Clin Microbiol Infect. (2022) 28:202–21. doi: 10.1016/j.cmi.2021.10.005
8. Kirson, N, Swallow, E, Lu, J, Mesa-Frias, M, Bookhart, B, Maynard, J, et al. The societal economic value of COVID-19 vaccines in the United States. J Med Econ. (2022) 25:119–28. doi: 10.1080/13696998.2022.2026118
9. Menni, C, May, A, Polidori, L, Louca, P, Wolf, J, Capdevila, J, et al. COVID-19 vaccine waning and effectiveness and side-effects of boosters: a prospective community study from the ZOE COVID study. Lancet Infect Dis. (2022) 22:1002–10. doi: 10.1016/s1473-3099(22)00146-3
10. Petrie, JG, King, JP, McClure, DL, Rolfes, MA, Meece, JK, Pattinson, D, et al. Effectiveness of first and second COVID-19 mRNA vaccine monovalent booster doses during a period of circulation of omicron variant sublineages: December 2021–July 2022. Influenza Other Respir Viruses. (2023) 17:e13104. doi: 10.1111/irv.13104
11. Kurita, J, Sugawara, T, and Ohkusa, Y. Waning COVID-19 vaccine effectiveness in Japan. Drug Discov Ther. (2022) 16:30–6. doi: 10.5582/ddt.2022.01000
12. Tanne, JH. Covid-19: Americans who are over 50 or immunocompromised are advised to have second booster. BMJ. (2022) 376:o842. doi: 10.1136/bmj.o842
13. Wise, J. Covid-19: vaccine effectiveness wanes more rapidly for cancer patients, study finds. BMJ. (2022) 377:o1305. doi: 10.1136/bmj.o1305
14. Andrews, N, Tessier, E, Stowe, J, Gower, C, Kirsebom, F, Simmons, R, et al. Duration of protection against mild and severe disease by Covid-19 vaccines. N Engl J Med. (2022) 386:340–50. doi: 10.1056/NEJMoa2115481
15. Grewal, R, Kitchen, SA, Nguyen, L, Buchan, SA, Wilson, SE, Costa, AP, et al. Effectiveness of a fourth dose of covid-19 mRNA vaccine against the omicron variant among long term care residents in Ontario, Canada: test negative design study. BMJ. (2022) 378:e071502. doi: 10.1136/bmj-2022-071502
16. Park, SK, Choe, YJ, Jang, EJ, Kim, RK, Lim, D-S, Yi, S, et al. Effectiveness of a fourth dose of COVID-19 mRNA vaccine in the older adults population during the omicron BA.2 and BA.5 circulation: a Nationwide cohort study in Korea (K-COVE). Open Forum Infect Dis. (2023) 10:ofad109. doi: 10.1093/ofid/ofad109
17. CDC C. FAQs on COVID-19 vaccination for seniors. (2022). Available at: https://en.chinacdc.cn/special/COVID19_Response/health_tips/202205/t20220516_259192.html.
18. Wang, YX, Zhang, L, Chen, SY, Lan, XQ, Song, MX, Su, RL, et al. Hesitancy to receive the booster doses of COVID-19 vaccine among Cancer patients in China: a multicenter cross-sectional survey - four PLADs, China, 2022. China Cdc Weekly. (2023) 5:223–8. doi: 10.46234/ccdcw2023.041
19. Chan, WL, Ho, YHT, Wong, CKH, Choi, HCW, Lam, KO, Yuen, KK, et al. Acceptance of COVID-19 vaccination in Cancer patients in Hong Kong: approaches to improve the vaccination rate. Vaccine. (2021) 9:792. doi: 10.3390/vaccines9070792
20. Hathaway, CA, Siegel, EM, Gonzalez, BD, Oswald, LB, Peoples, AR, Ulrich, CM, et al. Individual-level factors associated with COVID-19 vaccine acceptance among US patients with cancer. Vaccine. (2022) 40:6649–57. doi: 10.1016/j.vaccine.2022.09.063
21. Qin, CY, Yan, WX, Tao, LY, Liu, M, and Liu, J. The association between risk perception and hesitancy toward the booster dose of COVID-19 vaccine among people aged 60 years and older in China. Vaccine. (2022) 10:1112. doi: 10.3390/vaccines10071112
22. Chan, PSF, Lee, MLT, Fang, Y, Yu, FY, Ye, DH, Chen, SY, et al. Hesitancy to receive the second COVID-19 vaccine booster dose among older adults in Hong Kong: a random telephone survey. Vaccine. (2023) 11:392. doi: 10.3390/vaccines11020392
23. Qin, CY, Yan, WX, Du, M, Liu, Q, Tao, LY, Liu, M, et al. Acceptance of the COVID-19 vaccine booster dose and associated factors among the older adults in China based on the health belief model (HBM): a national cross-sectional study. Front Public Health. (2022) 10:10. doi: 10.3389/fpubh.2022.986916
24. Larson, HJ, de Figueiredo, A, Zhao, XH, Schulz, WS, Verger, P, Johnston, IG, et al. The state of vaccine confidence 2016: global insights through a 67-country survey. EBioMedicine. (2016) 12:295–301. doi: 10.1016/j.ebiom.2016.08.042
25. Fisher, KA, Bloomstone, SJ, Walder, J, Crawford, S, Fouayzi, H, and Mazor, KM. Attitudes toward a potential SARS-CoV-2 vaccine a survey of US adults. Ann Intern Med. (2020) 173:964–73. doi: 10.7326/m20-3569
26. Abouzid, M, Ahmed, AA, El-Sherif, DM, Alonazi, WB, Eatmann, AI, Alshehri, MM, et al. Attitudes toward receiving COVID-19 booster dose in the Middle East and North Africa (MENA) region: a cross-sectional study of 3041 fully vaccinated participants. Vaccine. (2022) 10:1270. doi: 10.3390/vaccines10081270
27. Waters, AR, Kepka, D, Ramsay, JM, Mann, K, Vaca Lopez, PL, Anderson, JS, et al. COVID-19 vaccine hesitancy among adolescent and young adult Cancer survivors. JNCI Cancer Spectrum. (2021) 5:Pkab049. doi: 10.1093/jncics/pkab049
28. SCHOOL MB. Veblen Effect. (2023). Available at: https://www.monash.edu/business/marketing/marketing-dictionary/v/veblen-effect.
Keywords: vaccine willingness, second booster of COVID-19 vaccine, cancer, older adults, hesitancy
Citation: Zhang L, Yang J, Su R, Lan X, Song M, Zhang L and Xu J (2024) Willingness to receive the second booster of COVID-19 vaccine among older adults with cancer: a stratified analysis in four provinces of China. Front. Public Health. 12:1298070. doi: 10.3389/fpubh.2024.1298070
Edited by:
Murugesan Velayutham, West Virginia University, United StatesReviewed by:
Hassan Fouayzi, University of Massachusetts Medical School, United StatesBita Fayaz, University of Pennsylvania, United States
Copyright © 2024 Zhang, Yang, Su, Lan, Song, Zhang and Xu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Junjie Xu, eGpqY211QDE2My5jb20=; Lei Zhang, QWlsaWZ1emwyNkAxNjMuY29t
†These authors have contributed equally to this work