 Anusha Ban1*
Anusha Ban1* Ashish Shrestha1Carissa Van den Berk-Clark2Janice Ballard3Richard Logan Jr4Tripp Logan Sr4
Ashish Shrestha1Carissa Van den Berk-Clark2Janice Ballard3Richard Logan Jr4Tripp Logan Sr4 Anne Francioni5
Anne Francioni5 Megan Murray6
Megan Murray6 Elizabeth A. Baker1
Elizabeth A. Baker1- 1College for Public Health and Social Justice, Saint Louis University, Saint Louis, MO, United States
- 2Department of Family & Community Medicine, Saint Louis University, Saint Louis, MO, United States
- 3One Heart Many Hands, Caruthersville, MO, United States
- 4L and S Pharmacy, Charleston, MO, United States
- 5Whole Kids Outreach, Ellington, MO, United States
- 6Southeastern Missouri Area Health Education Center, Poplar Bluff, MO, United States
Public health emergencies, such as the COVID-19 pandemic, elucidate the strengths, weaknesses, and significant gaps in infrastructure, compatibility and consistency in communication systems, as well as the quality of collaborative relationships, and provider and workforce capacity. They also expose longstanding patterns of mistrust in the government and healthcare systems, and inadequacy in socio-economic infrastructures. These issues resulted in higher COVID-19 infection and mortality rates, and lower vaccination rates in many rural counties across the nation, including Missouri. In response to these challenges, the COVID-19 Response Network was formed in the Southeast corner of the state. The Network was a community-academic partnership that brought together community and faith-based leaders, academicians, healthcare providers and administrators, public health practitioners, and pharmacists to facilitate collaboration on education and outreach efforts aimed at reducing vaccine inequity in the 16-county project area. Importantly, the Network also included Community Health Workers (CHWs) who worked with these different agencies and organizations and were at the heart of implementing Network activities. The intent of this study was to assess their perspectives on the factors that influenced community engagement and communication strategies, and increased vaccine uptake in rural Missouri. Qualitative methods, including in-depth interviews, were used to explore the professional and personal experiences of CHWs working at the grassroots level during an ongoing pandemic. Narrative analysis revealed effective communication and engagement strategies for increasing vaccine uptake in rural communities. For instance, fear-based messaging was perceived as coercive and met with resistance. In contrast, messages that shared personal experiences and catered to the human need to protect their loved ones were more effective. Trust in the source of information was critical. This study highlights the significance of exploring and leveraging the capacities of trusted community members like CHWs to increase the effectiveness of public health interventions in rural communities.
Introduction
The Coronavirus Disease 2019 (COVID-19) presented unprecedented challenges to the State of Missouri, the US, and the entire world. Within rural counties of Missouri, including the study site, COVID-19 highlighted what we already knew about deficiencies in clinical, public health, and economic infrastructures, and magnified existing racial and economic inequities and distrust in the government and the healthcare system. COVID-19 safety measures such as wearing masks, testing, social distancing, and vaccination were controversial and politicized across these rural counties (1). Given these circumstances, rural Missouri experienced a higher COVID-19 mortality rate per 100,000 population (94.2) compared to both statewide (87.3) and urban rates (83.2) (2).
It is within the above context that the COVID-19 Response Network was formed to serve a 16-county rural area in the Southeast region of Missouri including Butler, Cape Girardeau, Carter, Dunklin, Howell, Iron, Madison, Mississippi, New Madrid, Oregon, Pemiscot, Ripley, Scott, Shannon, Stoddard, and Wayne counties. These counties have relatively low levels of racial and ethnic diversity. For example, while around 27.5% of Pemiscot County is comprised of African American persons other counties such as Carter, Ripley, Oregon have less than 0.5% of their population self-identifying as African American (3). Similarly, there are few individuals who self-identify as Hispanic/Latinx communities living in this 16-county area (Dunklin County being the highest at 7.2%) (3). Despite this, Black/African American persons living in rural areas were 80% more likely to die from COVID-19 than White persons living in rural areas (1).
With higher rates of poverty (15.9%) compared to the urban areas of the state (10.9%) (4) these rural counties rank very high or high on the Centers for Disease Control and Prevention (CDC)‘s Social Vulnerability Index (SVI) (Mean SVI = 0.69 ± 0.26) as well. This measure includes socioeconomic, population, and housing/transportation vulnerability measures with scores ranging from 0 representing lowest vulnerability to 1 representing highest vulnerability (5). These counties have also been designated as health professional shortage areas. For example, the range of primary care providers per 100,000 population in these southeast counties of the state range from 0 providers per 100,000 population in counties like Shannon and Oregon to 90–100 providers per 100,000 population in counties like Cape Girardeau and Butler (6). Having fewer primary care providers per capita has been linked to lower life expectancies (7). Furthermore, the county rankings and roadmaps indicate that these rural counties also experience some of the worst health outcomes and behaviors in the state (8).
During the pandemic additional measures of vulnerability were also utilized, for example the COVID-19Vaccine Coverage Index (CVAC) measured how well a community could handle the repercussions of a COVID-19 outbreak and was based on a community’s access to health care, affordable housing, transportation, childcare, and safe and secure employment (9). The CVAC Index values range from 0 (least vulnerable) to 1 (most vulnerable) and it is categorized as follows: Very Low (0.0–0.19), Low (0.20–0.39); Moderate (0.40–0.59); High (0.60–0.79); and Very High (0.80–1.0). Most counties in these rural counties of Missouri were found to have high or very high vulnerability to handle a COVID-19 outbreak (Minimum: Maximum: Mean CVAC = 0.64 ± 0.06) (9).
Establishing a community-academic network
It is within this context that the COVID-19 Response Network was developed. It brought together community and faith-based leaders, primary and mental healthcare providers, pharmacists, academic institutions, and CHWs affiliated with different community - based agencies. The Network met virtually (via Zoom) weekly prior to and throughout the project period (March 2020 through August 2022). During these meetings, community, and academic facilitators shared data on COVID-19 for the region, the state of Missouri, and the US, as well as resources available (financial, material and informational) in and beyond the state to mitigate the challenges raised by the pandemic. The meeting participants contributed by sharing resources available through their organizations and in the community with other participants along with information about COVID-19 related events and locations where education, awareness, and vaccination activities would be performed. These joint efforts also led to a number of diverse COVID-19 Response Network actions including mobile food banks; the creation and distribution of health infographics tailored specifically for the community; and the organization of vaccination events in collaboration with local community pharmacies (8).
Purpose of the study
The intent of this study was to assess community health worker perspectives on the factors that influenced community engagement and communication strategies, and increased vaccine uptake in rural MO. This paper focuses on the experiences and perspectives of CHWs regarding community engagement during the COVID-19 pandemic, specifically documenting the communication strategies that enabled them to be successful at providing education regarding COVID-19 and encouraging vaccine uptake in the rural counties of Missouri. The study aims to further provide insights into the potential of CHWs to contribute to the health-seeking behaviors of individuals living in rural areas of the US.
Methods
Study population
A total of 65 CHWs from three different partner organizations were mobilized to conduct community outreach events in multiple counties within the Southeast region of Missouri. A little over half of the CHWs (55%) were employed by the partnering pharmacies, and the other half were employed by community-based organizations. Most of these CHWs (89.2%) were females and 20% were between the ages of 18–25, while around 77% were over the age of 25. Efforts were made to hire CHWs that represented the most vulnerable populations in our 16-county area. Sixty-nine percent of our CHWs lived in the same community or in one of the communities where they worked. Majority of the CHWs identified themselves as White (77%), while 17% of them identified themselves as Black or African American. This racial breakdown suggests an overrepresentation of African American given the demographic background of our study area. Almost all (95%) CHWs involved had completed a GED or a high school diploma. Additionally, 43 % of the CHWs reported having worked prior to the pandemic as CHWs in various capacities such as outreach coordinator, community liaison, healthcare and social services navigator, health educator, as well as community health worker.
Of the total sample of 65 CHWs, a sub sample of 11 were recruited through stratified (by organization that employed them) convenience sampling to participate in a semi-structured qualitative interview. Their demographic characteristics mirrored that of the 65 CHWs in general (e.g., 77% white, 90% female). Similarly, among the eleven study participants, eight of them self-identified as white and the remaining as African American.
Study design
This observational study used designed to capture the unique reflections of CHWs while conducting community-based educational outreach events to improve the uptake of COVID-19 vaccines within the 16-county area of Missouri. Hence, it employed a narrative qualitative approach to understand both the personal and professional insights gained through the efforts made to promote vaccination uptake. Quantitative data were used to capture CHW demographics, the number of educational events, and vaccines delivered.
Data collection and analysis
Members of the community and academic members of the research team reached out to CHWs via email, and provided an information statement about the study, requesting their participation. The interview protocol focused on the context within which CHWs conducted their work, community perceptions about COVID-19 and the vaccine, strategies and messages used for educational outreach, and CHW impact on a community as well as systemic level. Interviews were conducted and recorded via zoom after receiving the verbal consent of the participant. Transcription was completed using Zoom application’s written transcription option, and these written transcripts were compared to audio recordings by the team’s research assistants to ensure accuracy. All 11 transcripts were then analyzed using an inductive approach, beginning with open coding followed by a focused coding technique in which multiple members of the research team independently assigned codes to transcripts based on the interview topics, discussed disagreements, and came to a consensus on the best way to address discrepancies to ensuring intercoder reliability. After initial coding, codes were then arranged into thematic clusters with summary paragraphs synthesizing key elements from each thematic cluster, along with supporting quotations from the interviews.
Through shared online forms (Qualtrics), partner organizations collected quantitative data to identify CHW demographics, the number of educational events, and vaccines delivered.
Results
Through the interviews, CHWs provided an insight into the context within which they worked. They shared experiences related to the different strategies employed to navigate through that context and reach community people where they are. These experiences and insights have been documented in the CHW’s original words and have been presented below in four major thematic clusters: context, content, strategies, and trust.
Context within which the CHWs conducted their work
CHWs stated that most of the community members were not initially concerned about the pandemic as they had ‘bigger issues’ they needed to focus on, and many individuals in the community did not believe that COVID-19 was “real” (1a, 1b). CHWs also noted that initially when the vaccine came out, many people were ‘anxious and scared’ about getting the vaccine, and some families and community members had their ‘mind set against’ it (1c, 1d).
According to the CHWs, they experienced some pushback from the community members during community events, which they believed might have been due to misinformation about COVID-19 and the vaccine (1e). Furthermore, they noted that differences in political ideologies influenced community perspectives about the pandemic and the vaccines (1f). They indicated that social media platforms (including Facebook, Instagram, and TikTok) was their ‘worst enemy’ and the ‘biggest backset’ exacerbating much of the misinformation and polarization (1g).
CHWs also noted that lack of social support for getting vaccinated, or social norms against vaccination, made it difficult for some community members to get vaccinated (1h, 1i). Moreover, CHWs stated that families often created what could be called a “cultural block” within the communities which made it difficult for families to receive and accept information (1j). Some CHWs also raised similar concerns about the impact of the medical and social service organizations on community members’ decisions to get the COVID-19 vaccines. They noted that some medical professionals in these rural communities told their patients that they were against vaccinations (1k).
Content: messaging for rural communities
Given this context, CHWs noted that certain messages were particularly effective in increasing vaccine uptake among community members. For example, CHWs spoke about how sharing their own personal values and experiences with COVID-19 and the vaccines helped to shift community members’ mindsets, encouraging them to receive vaccines against COVID-19 (2a, 2b).
CHWs also indicated that family members, peers and people in their lives played a critical role in motivating their decision to vaccinate themselves (2c); the key driver being the desire to protect vulnerable family members. CHWs stated that recounting these personal stories about the process of accepting the vaccines at outreach events as a messaging strategy resonated with community members and helped them to understand the importance of the vaccine and even change their perspectives towards vaccines (2d, 2e). Sharing clear and easy to understand statistics about hospitalization and loss of life due to COVID-19 also played a critical role in motivating community members to obtain vaccines (2f, 2 g).
In addition, working in a diverse community setting with differing levels of understanding required CHWs to tailor the information provided in deference to the individuals or groups they interacted with (2h). For instance, catering to people’s beliefs or faith, was helpful in getting through to some groups (2i).
Strategies for engaging rural communities
Using neutral, non-coercive strategies and handing over the power to decide
CHWs indicated that their success was not just due to what they said to community members, but how they said it. They recognized the importance of being mindful of how the information is provided, starting from the moment they approached an individual (3.1a). They emphasized the importance of framing messages in ways that were appropriate for their communities. CHWs also noted that the level of credibility of the individual delivering the information was seen as equally important (3.1b) Apart from credibility, CHWs emphasized that treating people with respect, being polite, and greeting them with a welcoming attitude made community individuals receptive to the information provided (3.1c). Using appropriate, non-coercive words (3.1d, 3.1e) to offer information on COVID-19 and the vaccine against it was effective in creating an open dialog that people could return to. CHWs who sought to provide community members with options and a sense of control over their own decisions (3.1f, 3.1g) were met with less resistance (3.1 h). Furthermore, taking a “neutral standpoint” (3.1i) when providing necessary educational information on COVID-19 and vaccines helped CHWs address misinformation (3.1j) and enabled community members to make informed choices.
“Meeting people where they are” (literally and figuratively) and being polite often helped CHWs to develop trust and rapport with community members (3.1k). In their experience, it was equally important to use easy to understand plain language (3.1l) and visually appealing educational aids such as flyers and audiovisual aids (3.1m, 3.1n). Whatever the mix of strategies for engagement, they also highlighted that to be effective they needed to interact with people in ways that left the door open, allowing for follow up conversations (3.1o, 3.1p). Using educational materials to facilitate a two-way conversation as opposed to a one-way narration of information was met with more ‘acceptance’ by the community members (3.1q).
Using insistent, forceful language, fear-based messaging was ineffective
Trying to force families to get vaccinated was seen as ineffective and in certain cases worsened existing doubts and fears people had about vaccinations. One example where insistent language was used, the individual decided not to get vaccinated, and this also had a detrimental ‘domino effect’ resulting in them discouraging vaccinations for their children as well (3.2a).
Instances where fear-based messaging was used or when the CHWs just told people to get vaccinated without providing educational information reportedly created increased resistance (3.2b). While most CHWs found using different forms of Supplementary educational materials helpful (3.2c), some noted that many community members also preferred to engage in conversations rather than reading information from a piece of paper or having someone read information to them but was important to have it available (3.2d).
Strength in partnership
CHWs shared the positive changes brought about through the outreach efforts conducted in collaboration with community pharmacists and other community-based organizations. They noted that along with the efforts to promote preventive strategies against COVID-19 CHWs also responded to any needs or challenges presented during the pandemic as a ‘united front’ (3.3c). Particularly the collaborative relationship established with pharmacists was quoted to be a ‘big change’ which did not exist prior to the formation of the Network (3.3b) and continued to last beyond the completion of the project (3.3a). Apart from this, partnership with other organizations led to increased accessibility to more resources and provided CHWs with the ability to refer community members to relevant resources and services when necessary (3.3d).
Meeting community members where they are
CHWs relied heavily on partnerships with community organizations to increase their capacity to intervene in person. One of the most used approaches was to be a part of existing community events. Conducting outreach events at locations frequented by community members enabled CHWs to reach people “where they are.” CHWs also organized their own social events such as ‘luncheons’, ‘pageants’ etc. that offered a combination of entertainment, information, and service (opportunity to vaccinate) that not only ‘attracted’ people but was also a successful engagement strategy for encouraging vaccine uptake (3.4a, 3.4b). CHWs also noted that apart from the content and its delivery, it was necessary to be mindful of ‘who’ was present at the event, and who was providing the information at the event. Having pharmacists provide technical information within the context of such events further increased the positive impact of the information provided (3.4c). This was even more profound when CHWs went into communities they were not familiar with, and the trust factor had not yet been established (3.4d). A big part of meeting community members where they are, and the community outreach efforts conducted by the CHWs was the ability to have ‘face-to-face’ conversations which were noted to be a more effective medium of communication compared to phone calls (3.4d, 3.4e).
Trust was the key factor
In addition to having the right message and medium, when asked about how the community received them, CHWs felt that a key to their success was that the community trusted them regarding the information they provided on COVID-19 and the vaccines, which helped community members make their own decision. A major factor contributing to the community’s trust in the CHWs was related to them already being known and ‘embedded’ within the community (4c). As a result, community members felt ‘comfortable’ expressing their views to these CHWs (4a, 4b, 4d). Importantly, as noted earlier, the majority (69%) of the CHWs lived in the same community where they were working as a CHW for this project. The trust factor extended beyond CHWs to the broader community, as observing fellow community members getting vaccinated or learning about their vaccination decisions through social media played a significant role in influencing individuals’ own decisions regarding vaccination (4e, 4f) (Tables 1–4).

Table 1. Community context.
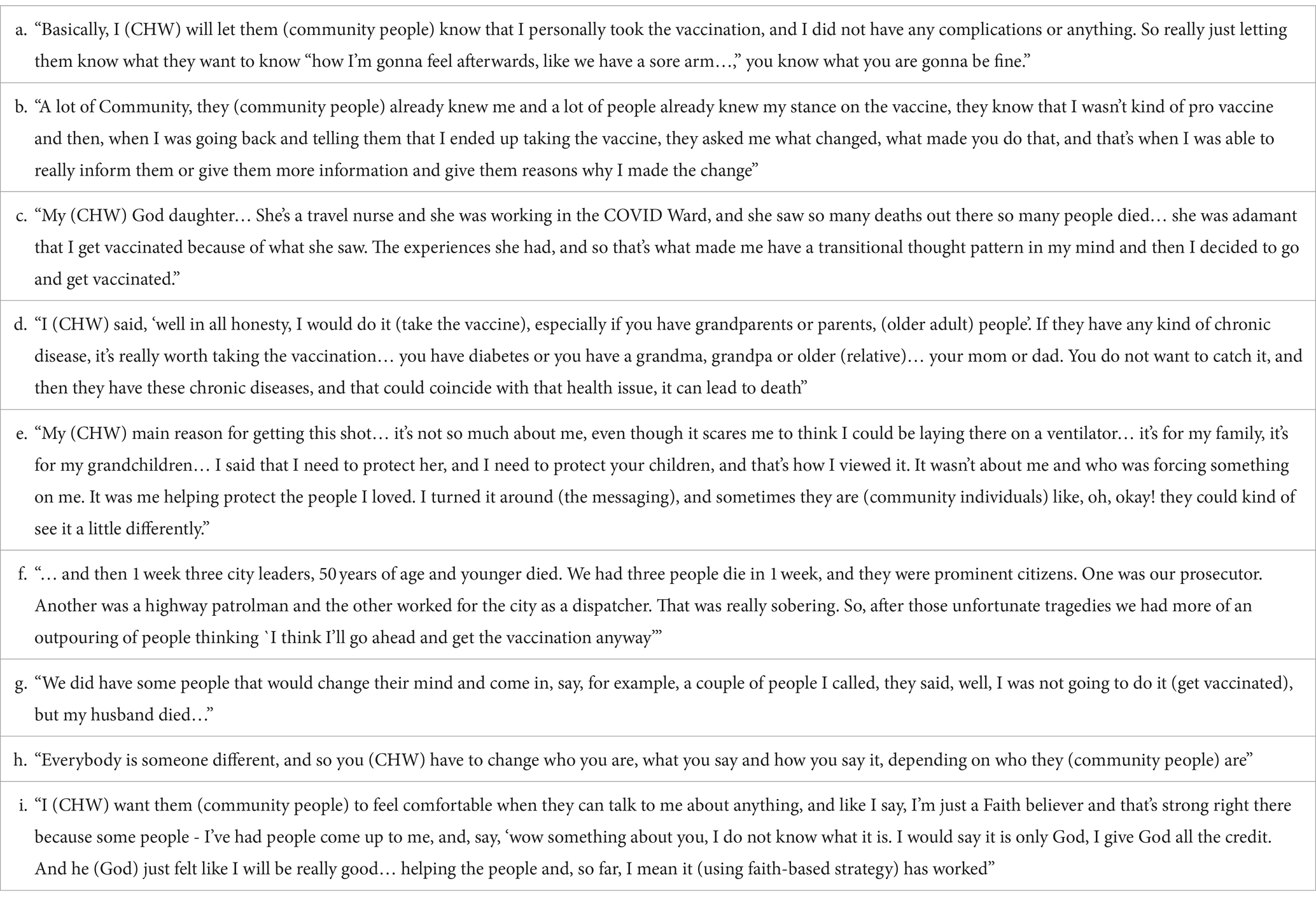
Table 2. Messaging for rural communities.

Table 3. Strategies.
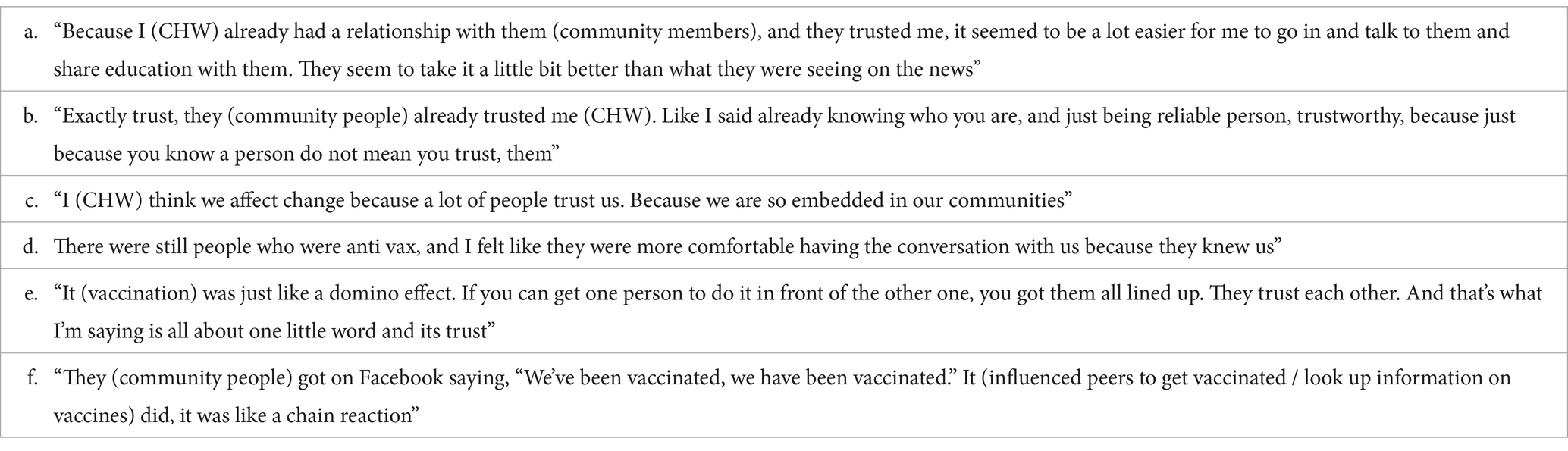
Table 4. Trust was the key factor.
Discussion
This paper provides insight into the functioning of CHWs within an initiative implemented in rural Missouri through a community-academic partnership (10). The central role of CHWs in conducting various outreach events facilitated collaboration among local partner organizations, pharmacies, and community leaders. This further allowed their impact to go beyond providing information to the community members and increasing vaccine uptake. The efficacy of face-to-face conversation was a reoccurring theme among the CHWs. Apart from making people aware of facts about COVID-19 and providing them with authentic sources of information, the CHWs were also able to empower communities to fact-check information for themselves as well as connect people to resources such as transportation.
Our findings also indicate that CHWs have the potential to contribute to the health seeking behavior of their communities. Health seeking behavior includes recognizing that there is a concern significant enough to require seeking an appropriate remedy for it (11). However, evidence suggests that care seeking is a complex process influenced by many factors preceding the actual act of decision-making (12), and requiring contextual analysis. Social determinants of health often act as barriers and enablers to treatment decision making and health outcomes. CHWs that were a part of this community academic network were more equipped at understanding these contextual barriers as they were a part of the communities they were serving, and more importantly had their trust. This allowed them to address their health-related needs and placed them in a position to create structural and systems changes to begin to address associated social determinants. As noted by the CHWs, when engaging communities, health workers need to be aware of the social and political context within which this decision-making occurs. When governmental entities, public health, clinical and social services have acted in ways that indicate that they have not had the communities’ interests in mind, communities lose trust in these institutions and will view any new health requests, mandates, and suggestions through this lens of mistrust (13).
Our study strongly indicated that rural communities viewed COVID-19 messages and data through a contextual lens. CHWs were able to bridge what was often a lack of trust and dismantle the barriers because they were a part of the communities they served, they established relationships with the community, and they developed unique ways to engage with communities using locally appropriate strategies. This suggests that we need to consider the messages we provide, the way we provide them, who is providing the message and the current and historical relationships that the individual and/or community has with providers and the organizations they represent. Study findings strongly recommend that community health actions draw on the capacities of trusted members of the community for planning and implementing future educational interventions.
There is already a substantial body of evidence demonstrating the disparate burden of the adverse impact of COVID-19 on underserved and under-resourced communities (14, 15). In terms of process of engaging with such communities, the CHWs highlighted the need to meet people where they were and provide information in multiple ways and at multiple times; taking time to realize that health education needs to be a process of engagement and building trust, recognizing the historical and cultural perspectives of communities, not just telling people what to do. Although, CHWs saw the negative impact of social media on vaccine uptake, quoting it to be their ‘worst enemy’, in considering what information to provide, the CWHs emphasized the importance of providing community members with reliable and credible sources of information, in person and online, in ways that facilitated dialog and encouraged reflection and questions.
This is consistent with previous work that has noted that individuals who had questions about COVID-19 vaccines and used the internet as their main source of information about vaccines were less likely to obtain the vaccine (16). Some have suggested that this may be associated with the fact that search engines are designed to reflect individuals’ patterns of inquiry, thus if one finds one source that is critical of the vaccine, their future searches are likely to bring them to similarly framed sources. In this way the internet may actually be narrowing rather than broadening access to information (17). CHWs found that the best way to counter the negative impacts of these websites was to encourage people to begin to confirm information for themselves, providing them with online news sources and authentic websites that might help expand their views (and their future searches), rather than just deepen one perspective. As health educators, we need to recognize and encourage the agency of communities in improving their own health and the need to create the conditions within which they can do so. We need to recognize the potential for benefit from technology but temper it with providing it with both strategies for vetting information on the web and interpersonal interactions.
The CHWs also identified that having CHWs working with and across agencies enhanced coordination among agencies and enhanced the ways that agencies were able to listen to community needs, opening the door to addressing social determinants of health, through lasting partnerships, not just providing direct care.
Limitations
Study findings are consistent with previous work in the field that suggests that vaccine uptake is influenced by the degree to which individuals understand the reasons for obtaining a vaccine, agree to getting the vaccine, and are moved toward obtaining a vaccine (awareness, acceptance, and activation) (18). However, within the context of our project, COVID-19 vaccines were brought to community sites, where people were otherwise gathered, and were offered for free. This reduces the generalizability of our findings, given that they do not highlight two other critical determinants of vaccine uptake, affordability and accessibility.
Conclusion
CHWs are a vital health care resource within our communities. Their knowledge, experiences, and pre-established relationships with community members facilitate program implementation and improve health outcomes in the community. Within rural communities, where healthcare systems are often inadequate, our work suggests that CHWs can also contribute to collaboration among community organizations, social service agencies, and health care providers (including pharmacies) and enhance their ability to positively impact health outcomes.
Data availability statement
Aggregate, deidentified data will be made available, without undue reservation. However raw qualitative data cannot be provided without compromising the confidentiality of our participants. Further inquiries can be directed to the corresponding author.
Ethics statement
The studies involving humans were approved by Saint Louis University Institutional Review Board. The studies were conducted in accordance with the local legislation and institutional requirements. Given the nature of the study, the IRB determined that written consent was not necessary and instead participants provided verbal informed consent to participate in this study and for the publication of aggregate, deidentified data.
Author contributions
AB: Conceptualization, Data curation, Investigation, Methodology, Writing – original draft, Project administration. AS: Writing – review & editing, Data curation. CV: Conceptualization, Funding acquisition, Investigation, Project administration, Supervision, Writing – review & editing. JB: Conceptualization, Funding acquisition, Project administration, Writing – review & editing. RL: Project administration, Resources, Writing – review & editing, Data curation. TL: Project administration, Resources, Writing – review & editing, Data curation. AF: Project administration, Project administration, Data curation. MM: Project administration, Resources, Writing – review & editing. EB: Conceptualization, Funding acquisition, Investigation, Project administration, Resources, Supervision, Writing – original draft, Data curation, Formal analysis.
Funding
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. Support for this project was provided by a grant from the Robert Wood Johnson Foundation Interdisciplinary Research Leaders program. Interdisciplinary Research Leaders is a national program of the Robert Wood Johnson Foundation led by the University of Minnesota. The views expressed here do not necessarily reflect those of the Foundation or the University of Minnesota. This project was also supported by the Health Resources and Services Administration (HRSA: U3SHS42192‐01‐00) of the U.S. Department of Health and Human Services (HHS) and Saint Louis University (SLU) Drs. Mary Susan and Robert Heaney Primary Care Research Fund. The contents are those of the author(s) and do not necessarily represent the official views of, nor an endorsement, by SLU, HRSA, HHS, or the U.S. Government. For more information, please visit HRSA.gov.
Conflict of interest
Authors RL and TL are employed by company L and S Pharmacy.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2024.1286177/full#supplementary-material
References
1. Callaghan, T, Lueck, JA, Trujillo, KL, and Ferdinand, AO. Rural and urban differences in COVID-19 prevention behaviors. J Rural Health. (2021) 37:287–95. doi: 10.1111/jrh.12556
2. Sara, D, Barbara, B, and Aleesha, J (2021). Missouri Office of Rural Health’s Biennial Report 2020–2021. Jefferson city. Available at: https://health.mo.gov/living/families/ruralhealth/publications.php
3. MISSOURI (2020). Census. Available at: https://www.census.gov/library/stories/state-by-state/missouri-population-change-between-census-decade.html
4. Rural health for Missouri Overview. Rural Health Information Hub. Available at: https://www.ruralhealthinfo.org/states/missouri
5. SVI. CDC/ATSDR Social Vulnerability Index (SVI). Available at: https://www.atsdr.cdc.gov/placeandhealth/svi/index.html
6. Area Health Resources Files. Available at: https://data.hrsa.gov/topics/health-workforce/ahrf
7. Basu, S, Berkowitz, SA, Phillips, RL, Bitton, A, Landon, BE, and Phillips, RS. Association of Primary Care Physician Supply with Population Mortality in the United States, 2005-2015. JAMA Intern Med. (2019) 179:506. doi: 10.1001/jamainternmed.2018.7624
8. Missouri. County Health Rankings & Roadmaps. Available at: https://www.countyhealthrankings.org/explore-health-rankings/missouri?year=2023
9. Vaccine Hesitancy for COVID-19. Data | Centers for Disease Control and Prevention. Available at: https://data.cdc.gov/stories/s/Vaccine-Hesitancy-for-COVID-19/cnd2-a6zw/
10. Spalluto, LB, Thomas, D, Beard, KR, Campbell, T, Audet, CM, McBride Murry, V, et al. A community academic partnership to reduce healthcare disparities in diagnostic imaging. J Am Coll Radiol. (2019) 16:649–56. doi: 10.1016/j.jacr.2018.12.033
11. Oberoi, S, Chaudhary, N, Patnaik, S, and Singh, A. Understanding health seeking behavior. J Family Med Prim Care. (2016) 5:463. doi: 10.4103/2249-4863.192376
12. Poortaghi, S, Raiesifar, A, Bozorgzad, P, Golzari, SEJ, Parvizy, S, and Rafii, F. Evolutionary concept analysis of health seeking behavior in nursing: a systematic review. BMC Health Serv Res. (2015) 15:523. doi: 10.1186/s12913-015-1181-9
13. López-Cevallos, DF, Harvey, SM, and Warren, JT. Medical mistrust, perceived discrimination, and satisfaction with health care among young-adult rural Latinos. J Rural Health. (2014) 30:344–51. doi: 10.1111/jrh.12063
14. Millett, GA, Jones, AT, Benkeser, D, Baral, S, Mercer, L, Beyrer, C, et al. Assessing differential impacts of COVID-19 on black communities. Ann Epidemiol. (2020) 47:37–44. doi: 10.1016/j.annepidem.2020.05.003
15. Adhikari, S, Pantaleo, NP, Feldman, JM, Ogedegbe, O, Thorpe, L, and Troxel, AB. Assessment of community-level disparities in coronavirus disease 2019 (COVID-19) infections and deaths in large US metropolitan areas. JAMA Netw Open. (2020) 3:e2016938. doi: 10.1001/jamanetworkopen.2020.16938
16. Bridgman, A, Merkley, E, Loewen, PJ, Owen, T, Ruths, D, Teichmann, L, et al. (2020). The causes and consequences of COVID-19 misperceptions: understanding the role of news and social media. Harvard Kennedy School Misinformation Review. Available at: https://misinforeview.hks.harvard.edu/article/the-causes-and-consequences-of-covid-19-misperceptions-understanding-the-role-of-news-and-social-media/
17. Marshall, GS. Vaccine hesitancy, history, and human nature: the 2018 Stanley a. Plotkin lecture. J Pediatric Infect Dis Soc. (2019) 8:1–8. doi: 10.1093/jpids/piy082
Keywords: community health workers, rural health, COVID-19, vaccine equity, community engagement
Citation: Ban A, Shrestha A, Van den Berk-Clark C, Ballard J, Logan R Jr, Logan T Sr, Francioni A, Murray M and Baker EA (2024) Through the eyes of community health workers: what was needed to increase COVID-19 vaccine uptake in the Missouri Southeast region. Front. Public Health. 12:1286177. doi: 10.3389/fpubh.2024.1286177
Edited by:
Tomas Nuno, University of Arizona, United StatesReviewed by:
Tony Kuo, University of California, Los Angeles, United StatesJoseph Odhiambo Onyango, Strathmore University, Kenya
Copyright © 2024 Ban, Shrestha, Van den Berk-Clark, Ballard, Logan, Logan, Francioni, Murray and Baker. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Anusha Ban, YW51c2hhLmJhbkBzbHUuZWR1