 Johanna Einhorn
Johanna Einhorn Michaela James
Michaela James Natasha Kennedy1
Natasha Kennedy1 Emily Marchant
Emily Marchant- 1National Centre for Population Health and Wellbeing Research, Data Science Building, Swansea University, Swansea, United Kingdom
- 2Department of Education and Childhood Studies, School of Social Sciences, Swansea University, Swansea, United Kingdom
Introduction: This study examines the changes in childhood self-reported health and wellbeing between 2014 and 2022.
Methods: An annual survey delivered by HAPPEN-Wales, in collaboration with 500 primary schools, captured self-reported data on physical health, dietary habits, mental health, and overall wellbeing for children aged 8–11 years.
Results: The findings reveal a decline in physical health between 2014 and 2022, as evidenced by reduced abilities in swimming and cycling. For example, 68% of children (95%CI: 67%–69%) reported being able to swim 25m in 2022, compared to 85% (95% CI: 83%–87%) in 2018. Additionally, unhealthy eating habits, such as decreased fruit and vegetable consumption and increased consumption of sugary snacks, have become more prevalent. Mental health issues, including emotional and behavioural difficulties, have also increased, with emotional difficulties affecting 13%–15% of children in 2017–2018 and now impacting 29% of children in 2021–2022. Moreover, indicators of wellbeing, autonomy, and competence have declined.
Discussion: Importantly, this trend of declining health and wellbeing predates the onset of the Covid-19 pandemic, suggesting that it is not solely attributed to the pandemic’s effects. The health of primary school children has been on a declining trajectory since 2018/2019 and has continued to decline through the COVID recovery period. The study suggests that these trends are unlikely to improve without targeted intervention and policy focus.
1 Introduction
The foundation of adulthood is laid in childhood, where experiences shape life achievements, mental health, and overall wellbeing (1). It is noted that 50% of mental health problems are established by the age of 14 (2), and stressors in childhood can influence brain development (3). Thus, the physical and mental health, as well as the overall wellbeing and self-confidence, of the nation’s school-aged children is vital to the health of the next generation.
The incidence of mental health disorders in childhood is increasing; global research indicates that mental health problems such as anxiety, depression, and behavioral problems increased among children between 2014 to 2020 (4). Observations of data from the United Kingdom (UK) revealed that mental health conditions rose from 1 in 9 to 1 in 6 between 2017 to 2021 (5). Moreover, trends observed in England and Wales have reported a decline in wellbeing, especially as children age and particularly in girls (6–8). In addition, recent evidence indicates a deterioration in children’s physical health. A study from England demonstrated an increase in children’s Body Mass Index (BMI) along with a decline in general fitness observed in 2020 (9). This has resulted in an increase in obesity rates since 2017 (8).
Legislative measures, such as the Wellbeing of Future Generations Act (WFGA) (10) in Wales, as well as policies concerning physical activity and play (e.g., Children and Families (Wales) Measure 2010, and the Play Sufficiency Duty (11)), have raised awareness of the need to improve the health and wellbeing of young people. The Covid-19 pandemic has potentially contributed to a decline in health and wellbeing, as access to socialization, support, and physical activity has been reduced due to school closures aimed at preventing virus transmission (12–14). Persistently elevated levels of mental health disorders in 2021 indicate that the full impact of the pandemic remains unaddressed or that overall health outcomes are trending downward (8).
Furthermore, amidst the Covid-19 pandemic, children have been exposed to a risk of contracting and transmitting the virus, as well as experiencing the associated health consequences. They have also faced elevated risks of reduced access to medical care, poverty, and social isolation due to COVID-19 restrictions (15). These challenges have arisen in conjunction with the United Kingdom’s departure from the European Union (16) and the current “cost of living crisis” (17, 18), subsequently presenting significant obstacles for children and society’s support systems.
This research aims to explore childhood trends between 2014 and 2022; examining changes in childhood experiences and how growing up during periods of political upheaval and crisis (e.g., the COVID-19 pandemic) has affected the health and wellbeing of children. This study employs data from a self-report survey administered by HAPPEN (Health and Attainment of Pupils in Primary EducatioN)-Wales to 36,951 children aged 8–11 across Wales. The survey covers aspects such as general health, physical activity, sleep, dietary habits, wellbeing, social contacts, mental health, and their experience of growing up.
2 Materials and methods
2.1 Study design
This study employs data collected by HAPPEN-Wales between 2014 and 2022. HAPPEN-Wales was officially established at Swansea University in 2015 and has been co-produced alongside school senior leaders, teachers, and pupils. Prior to this HAPPEN data was collected via ‘Fitness Fun Days’. Senior leaders advocated for collaboration and a joined-up approach to prioritizing health and wellbeing within the school setting (19) to bring together education, health, and research in line with the Curriculum for Wales proposals for health and wellbeing Wales, implemented in primary schools from September 2022.
Participating schools engage with the initiative by completing an online self-report survey with their pupils aged 8–11 years (years 4, 5, and 6). The survey encompasses various dimensions of health and wellbeing, including nutrition, physical activity, sleep, mental health, and concentration (20). The survey is included as Supplementary file S1. The modified version circulated during COVID-19 can be observed in Supplementary file S2. The latest version of the survey was granted ethical approval in November 2022 by Swansea University’s Medical School (2017-0033I).
2.2 Participants
HAPPEN is a pan-Wales infrastructure that delivers an online health and wellbeing survey to schools. To recruit, all primary schools in Wales are contacted via direct email, social media campaigns (including paid advertisements on Facebook and Twitter), and promotion through key stakeholders (e.g., regional education consortia) throughout the academic year. Schools that agree to participate are provided with information sheets to be shared with parents/guardians, who are given the opportunity to opt their child out of the survey. This opt-out approach to recruiting participants was implemented to establish a representative sample that encompasses the diverse population of children across Wales. Child information sheets are distributed, and assent is obtained at the start of the survey. Typically, the survey is completed in school as part of a lesson, supervised by a teacher. The exception for this is during 2020, where the survey was adapted and completed at home during Covid-19 enforced school closures (14). Prior to 2018, data were collected in South Wales specifically before HAPPEN expanded pan-Wales from 2018.
2.3 Data collection
The data were collected between September 2014 and December 2022. All children in Wales aged 8–11 are eligible to participate in the survey. The process of data coding involved four researchers. The first researcher (MJ/EM) downloaded the raw data, cleaned the data, and generated a unique participant ID number before removing identifiable information. This process protects participants’ anonymity. Raw data was coded using STATA (version 16) (21) to produce a dataset for the purpose of analyses. A second researcher (JE) conducted analysis of the data with a third (NK) validating the initial analysis.
2.4 Analysis
For data analysis and statistics procedures, the R software (version 4.2.2) (22) was used, employing the packages “lubridate,” “MASS,” and “tidy verse.” From the survey, the variable “date participated” was extracted for use as the explanatory variable. The examined variables encompassed a range of factors, including the quantity of fruit and vegetables consumed, frequency of fatigue experienced per week, duration of screen time per week, proficiency in riding a bike without stabilizers, ability to swim 25 metres unassisted, self-reported happiness level with friends on a scale of 1–10, self-perceived competence level, level of worry experienced, emotional and behavioral difficulty scores derived from the Me and My Feelings questionnaire, self-perceived safety of the child’s area on a scale of 1–10, agreement on the importance of physical activity, number of friends seen in the past week, and presence of cold symptoms within the previous week. Additionally, demographic variables such as “age,” “gender,” “WIMD2019Quartile,” and “ChildIndex2011Quintile” were included as variables and covariates (Supplementary file S3).
The dependent variables were sorted into four categories. The first category describes variables with binary responses (yes or no). The second category encompassed variables with a concrete numerical answer such as “How many portions of fruits or vegetables did you eat yesterday.” The third category consisted of variables with a categorical scale ranging from 0 to 4, where each category represented a distinct response. The final category involved variables with a scale of one to 10. Only complete data were included in the analysis.
For variables from category one, the percentage of children answering ‘yes’ per month and year was calculated. For variables from the second, third, and fourth category the percentage of children choosing a specific category was determined on a monthly and yearly basis. In cases where “I do not know” or “I am not sure” were selected as answers, these responses were treated as missing data rather than separate categories due to the small number of cases. Additionally, for all results 95% confidence intervals were calculated. Regression analysis adjusting for age, gender and deprivation was used to examine change in health before and after 2020 (as a time marker of the Covid-19 pandemic) using interrupted time series.
3 Results
This study uses data from a total of 36,951 children from 2014 to 2022. Of this number, 47% were boys, 49% were girls and 3% preferred not to say. The average age of children was 9.35 years. In terms of deprivation levels, 15% of participants were classified in the most deprived quartile (1), 12% in quartile 2, 14% in quartile 3, and 7% in quartile 4 (least deprived). 38% of participants did not have deprivation associated data. Overall findings can be observed in Table 1.
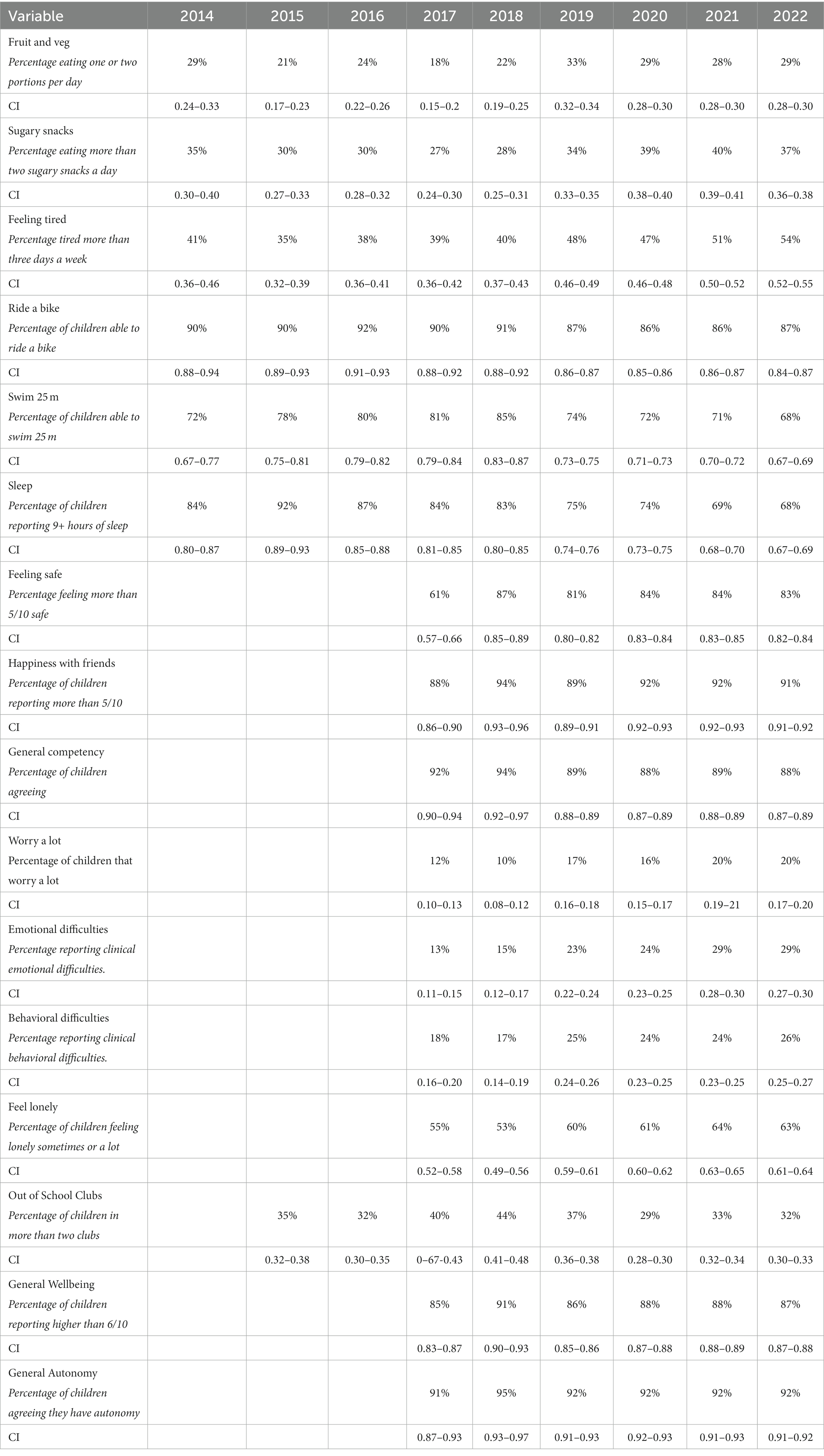
Table 1. Overall findings in children’s self-reported health and wellbeing from 2014 to 2022.
3.1 Physical health
For this study, physical health includes physical competency measures of the ability to swim, ability to ride a bike, understanding of the benefits of physical activity, diet, and tiredness and sleep (Table 1). The ability to swim was measured by the percentage of children self-reporting they were able to swim 25 m. This decreased rapidly in the last few years and has not recovered (Figure 1). Currently, only 68% (95% CI: 67–69%) of children reported to be able to swim 25 m in 2022, compared to 85% (95% CI: 83–87%) in 2018.
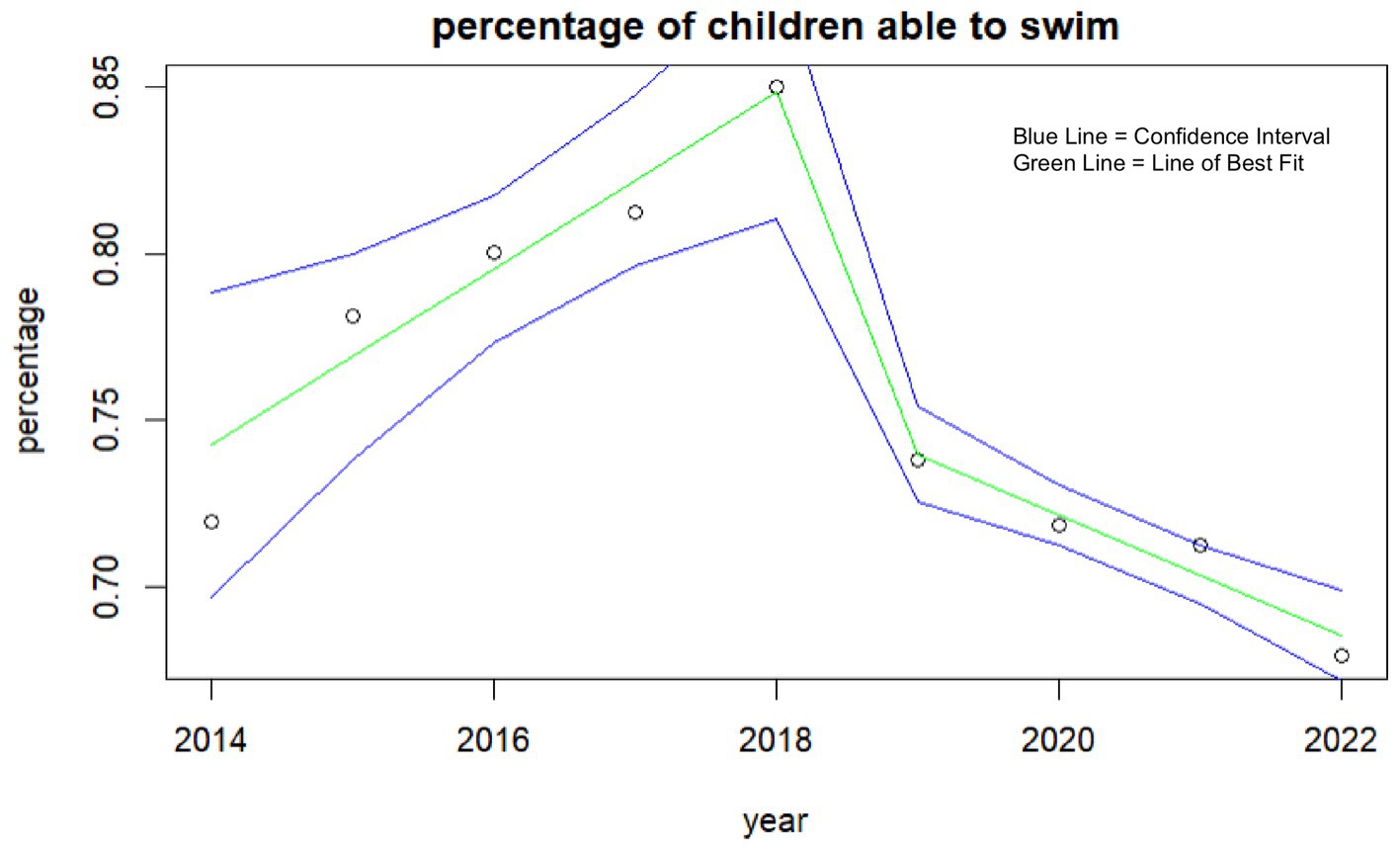
Figure 1. Percentage of children self-reporting the ability to swim each year.
This analysis also shows an association between the ability to ride a bike and the number of friends children are having over their houses with those with more friends more likely to be able to ride a bike. This positive association suggests having more friends can influence skills and abilities at an early age. As well as this, a negative association is observed between the ability to ride a bike and tiredness; higher tiredness was reported in those who cannot ride a bike.
The data shows an overall increase of tiredness among all children (Figure 2). From 41% of children feeling tired more than 3 days a week in 2014 (95%CI: 36–46%) this is relatively unchanged until 2019 where the mean increases to 51% (95%CI: 50–52%) and 54% (95%CI: 53–55%) in 2022. One-way ANOVA analysis shows an interaction between tiredness and the number of sugary snacks consumed with increases in tiredness seen as sugary snack consumption increases [f (4,35,325) = 174.96, p = 0.000].
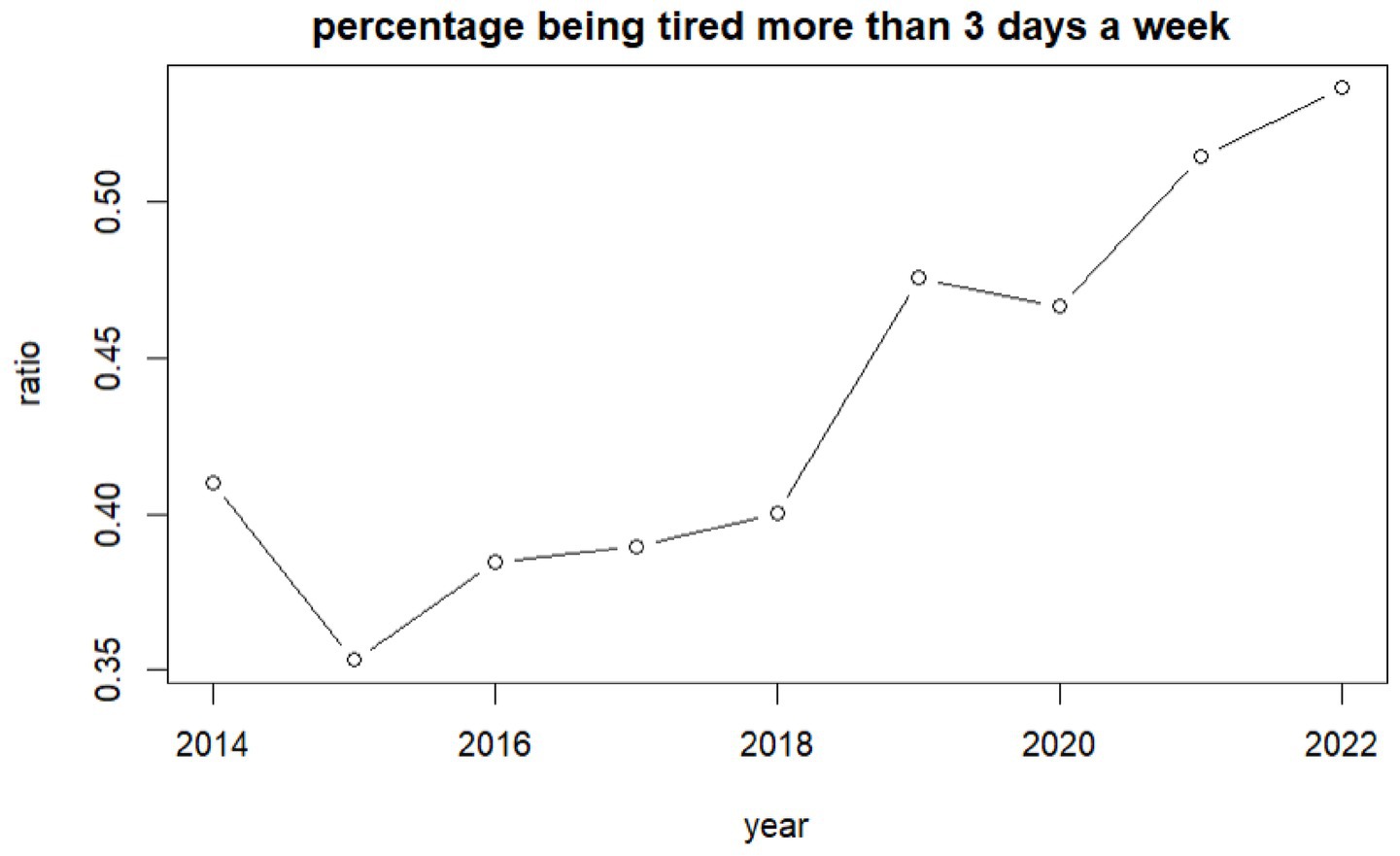
Figure 2. Percentage of children self-reporting feeling tired more than 3 days a week per year.
The average number of sugary snacks children consumed per day increased rapidly in 2020, following an upward trend that commenced in 2018. In 2018, 28% (95%CI: 25–32%) of children were consuming more than two sugary snacks, increasing to 34% (95%CI: 33–35%) in 2019. By 2020, it had further escalated to 39% (95%CI: 38–40%), maintaining this level thereafter. Regression analysis shows a significant increasing trend [f (1,35,701) = 157.89, p = 0.0001].
In terms of sleep, trends show a decrease in the number of children having 9+ hours of sleep per night. In 2015, 92% (95%CI: 89–93%) of children reported achieving this outcome, compared to 68% (95%CI: 67–69%) in 2022. This negative trend could have a significant impact on children’s health and wellbeing.
3.2 Mental health and wellbeing
The percentage of children reporting emotional difficulties increased from 13% (95%CI: 11–15%) in 2017 to 23% (95%CI: 23–25%) in 2019 and to 29% (95%CI: 27–30%) in 2022 (Figure 3). Higher values represent higher difficulties. One-way ANOVA analysis indicates differences between genders with boys reporting lower emotional difficulties than girls [f = (2,232,092) = 66.20, p = 0.000]. The highest difficulties are children who preferred not to state their gender. The effect size, as measured by eta-squared, was small but statistically significant (n2 = 0.0041) suggesting that variance in emotional difficulty could be attributed to differences between gender. Behavioral difficulties increased in general, especially in girls. The percentage of children reporting behavioral difficulties increased from 18% (95%CI: 16–20%) in 2017 to 25% (95%CI: 24–26%) in 2019 (Figure 4).
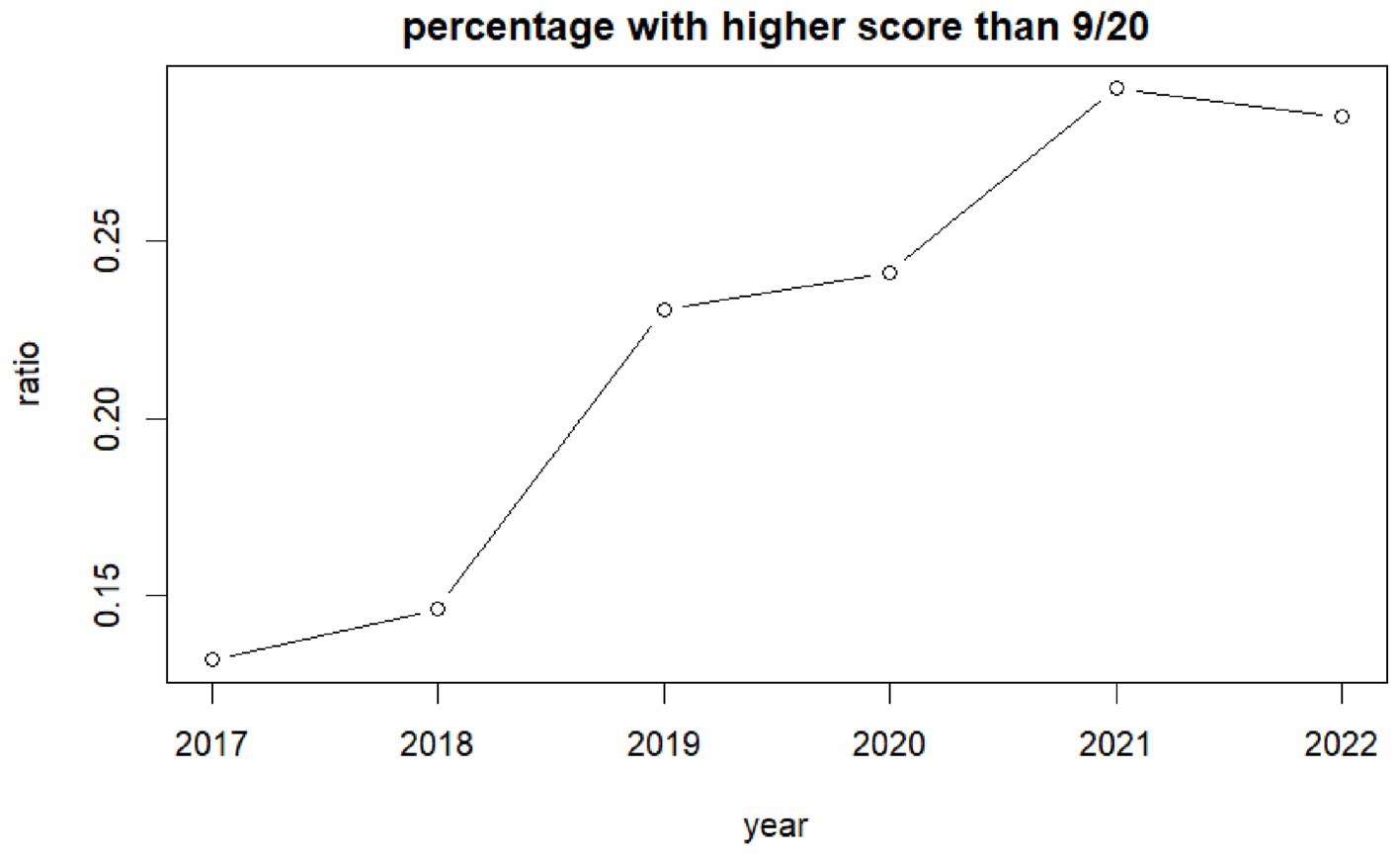
Figure 3. Ratio children self-reporting high emotional difficulties per year.
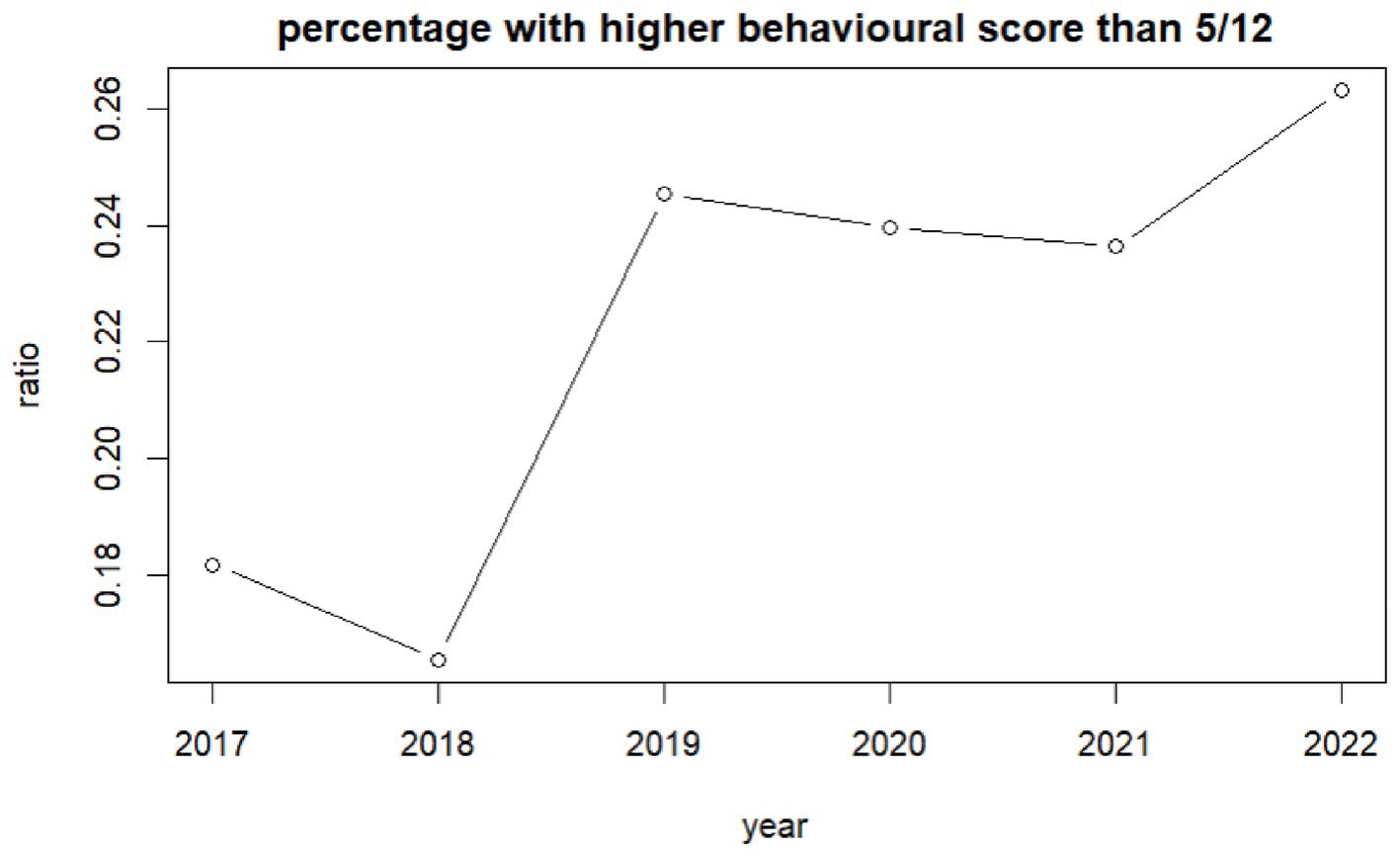
Figure 4. Ratio of children self-reporting high behavioural difficulties per year.
Since 2017 children reporting they worry a lot has increased from 17% (95%CI: 16–18%) in 2017 to 20% (95%CI: 17–20%) in 2022. Regression analysis shows a significant inclining trend [f (1,33,360) = 184.90, p < 0.0001].
3.3 Socialization
Since 2019, the number of children feeling lonely increased from 55% (95%CI: 52–58%) to 63% (95%CI: 61–64%) in 2022. Additionally, one-way ANOVA analysis shows an interaction between increased loneliness and a higher number of sugary snacks consumed [f (4,32,742) = 12.39, p = 0.0000].
4 Discussion
The aim of this research was to explore childhood trends over the last 8 years; examining the changes in childhood health and wellbeing. The health and wellbeing of children has been declining globally and data has indicated that mental health conditions are rising. The Covid-19 pandemic and its associated restrictions have potentially impacted this further. This, alongside points of political and societal upheaval in the United Kingdom (e.g., Brexit and the ‘cost of living’ crisis) have presented challenges for society. These instances have brought with them uncertainty about finances, healthcare, employment, and education which has significant impacts on health and wellbeing. For children, living with adults facing these uncertainties will have an impact due to changes in diet, activity provision, and general societal and cultural dynamics.
This study has identified some key findings in children’s health and wellbeing from 2014 to 2022, with a notable emphasis on the significant declines observed across several areas. Health and wellbeing have been declining for some time, even prior to Covid-19, suggesting that the pandemic has not been the cause of poor health and wellbeing, but has contributed further to the decline.
4.1 Physical health
The physical health of children has exhibited no improvement since 2014, accompanied by a decline in reported swimming and cycling abilities. These physical skills are essential for developing physical literacy and fundamental movement skills (23), these are often developed during early childhood years. Swimming is often promoted during early years as an avenue of teaching and developing these skills (24). However, funding cuts in Wales in 2019, which forced changes to swimming provision for children (25), and the subsequent closure of swimming facilities during the pandemic to prevent transmission, have exacerbated this issue. Notably, self-reported swimming ability significantly declined the year prior to the pandemic, highlighting the role of funding redirection and the subsequent lack of accessibility on children’s perception of their physical literacy. Moreover, deprived children are more likely to report not being able to swim, further demonstrating the potential role of the funding cuts in widening inequalities.
Dietary habits have also not improved over time, with no improvements observed in sugar, fruit, and vegetable consumption. Sugar consumption increased rapidly in 2020, coinciding with the Covid-19 pandemic, which caused an increased time at spent home rather than attending school, potentially encouraging less-favorable diets with interruptions to regular, enforced mealtimes during the school day. These observations have been reflected in other studies (14, 26). Fruit and vegetable intake has also not improved over time, with nearly a third of children in this study reporting eating zero or one portion a day. Other studies noted that more deprived children ate fewer portions of fruit and vegetables during the pandemic (14), and free school meals, a key policy that helps reduce dietary inequalities, remained inaccessible to almost half of all children on free school meals during pandemic restrictions (27).
The combination of fewer physical skills, a lack of understanding of the benefits of physical activity, and a rise in sugary snack consumption could lead to an increase in sedentary behavior, obesity, and related negative health behaviors among this generation of children, potentially increasing the risk of a range of non-communicable diseases such as diabetes. Another key finding from this study is the reduction in self-reported sleep which will underpin tiredness but will also impact children’s health and wellbeing much more widely, for example, being motivated to be physically active when already tired. It is important to note that all the above variables were already showing a decreasing trend in 2019 before the pandemic, indicating that the pandemic is not the only risk factor to children’s health and wellbeing. Therefore, the assumption that the situation will naturally recover with restrictions easing cannot be made.
4.2 Mental health and wellbeing
The mental health of children has not improved over time and displays a concerning trend. These findings are consistent with previous studies (6–8), and indicate an alarming picture of mental health and wellbeing among school-aged children. Effective and sustainable intervention is necessary to interrupt this trend, particularly for girls who exhibit higher rates of emotional and behavioral difficulties compared to boys. Research indicates that girls are more likely to experience difficulties than boys and this gender gap increases with age (28), underscoring the importance of addressing these trends.
Although this study highlights that this trend was apparent prior to the pandemic, it is possible that periods of isolation, restrictions, and interruption to normal routine have highlighted and exacerbated these issues. Research indicates that a proportion of young people reported the pandemic had worsened their mental health (29). The pandemic may have exacerbated these trends by increasing worry and uncertainty over young people’s futures, particularly in terms of schooling, where young people reported difficulties with online learning (30).
However, these trends were reported among young people in secondary school and higher education. These trends have been ongoing since 2019, where the most significant declines were observed in this study. It is plausible that younger children (aged 7–11) were happier and healthier during lockdowns, especially as this study notes some increases in wellbeing in 2020. This could have been because of increased time with parents, more opportunities for unstructured imaginative free time and play, or a less restrictive schedule (i.e., the school day) (14). It is critical that children of all ages are heard, with their wants and needs recorded and addressed, as they differ by age and gender. During the pandemic, younger children stated how much they valued the ability to play with their friends (something that was removed from them during the restrictions), while older children were concerned about future prospects and online learning (30). Addressing areas of support tailored to their specific needs is necessary to alleviate negative trends.
Friendships are vital to children’s social lives, providing them with early experiences of relationships and support beyond their families (31). This research suggests that children are not socializing with friends as much as they used to and feel lonelier, which may have been exacerbated by the pandemic and the shift to online interactions. However, children reported feeling lonely before the pandemic and again in 2021, indicating a need to facilitate socialization in settings where children spend time to promote their health and wellbeing. It is worth noting that children have different needs for their happiness, health, and wellbeing.
4.3 Limitations
This study employs a descriptive approach, utilizing a self-report methodology to investigate children’s perceptions of their childhood. The present paper exclusively presents the findings derived from survey participants. However, it is important to note that the study does not delve into the underlying reasons behind children’s responses or explore the factors contributing to changes in their perspectives.
5 Conclusion
In summary, the study indicates that the health and wellbeing of children had been deteriorating before the COVID-19 pandemic and has either stabilized or continued to decline following the pandemic. Thus, it cannot be assumed that the removal of restrictions and return to normal routines and school will automatically improve children’s health and wellbeing. Therefore, it is imperative to prioritise the development and implementation of effective and sustainable interventions, funding distribution and policy focus that address physical skills like swimming and cycling, promote confidence and autonomy in physical activity, and enhance overall wellbeing and socialization. It is also essential to recognize that the pandemic and its accompanying restrictions could exacerbate these issues, and broader political and societal challenges like Brexit and the “cost of living” crisis may further complicate matters.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Author contributions
JE: Conceptualization, Data curation, Investigation, Methodology, Project administration, Resources, Supervision, Validation, Writing – original draft, Writing – review & editing. MJ: Data curation, Formal analysis, Investigation, Methodology, Writing – original draft, Writing – review & editing. NK: Validation, Writing – review & editing. EM: Writing – review & editing. SB: Conceptualization, Funding acquisition, Investigation, Methodology, Project administration, Resources, Supervision, Validation, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This research was funded by the National Centre for Population Health and Wellbeing and ADR Wales, part of the ESRC funded ADR UK investment.
Acknowledgments
The research team would like to thank all pupils, teachers and schools who took part in facilitating, administering, and taking part in the HAPPEN Survey and for their support.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2024.1285687/full#supplementary-material
References
1. Daines, CL, Hansen, D, Novilla, MLB, and Crandall, AA. Effects of positive and negative childhood experiences on adult family health. BMC Public Health. (2021) 21:1–8. doi: 10.1186/s12889-021-10732-w
2. Mental Health Foundation. Children and young people: Statistics. (2023). Available at: https://www.mentalhealth.org.uk/explore-mental-health/statistics (Accessed March 18, 2023).
3. Lloyd, A, McKay, RT, and Furl, N. Individuals with adverse childhood experiences explore less and underweight reward feedback. Proc Natl Acad Sci USA. (2022) 119:1–8. doi: 10.1073/pnas.2109373119
4. Lebrun-Harris, LA, Ghandour, RM, Kogan, MD, and Warren, MD. Five-year trends in US Children’s health and well-being, 2016-2020. JAMA Pediatr. (2022) 176:e220056–20. doi: 10.1001/jamapediatrics.2022.0056
5. Grimm, F, Alcock, B, Butler, J, Fernandez Crespo, R, Davies, A, et al. Improving children and young people’s mental health services: Local data insights from England, Scotland and Wales. The Heal Found. (2022). 1–38.
6. NHS Digital. Mental health of children and young people in England 2022 - wave 3 follow up to the 2017 survey (2022). Available at: https://digital.nhs.uk/data-and-information/publications/statistical/mental-health-of-children-and-young-people-in-england/2022-follow-up-to-the-2017-survey#highlights (Accessed February 13, 2023.
7. Department for Education. State of the nation 2021: Children and young people’s wellbeing research report. (2022). Government Social Research. 1–11.
8. Welsh Government. Wellbeing of Wales 2022: Children and young people’s wellbeing. Cardiff: Welsh Government. (2022).
9. Basterfield, L, Burn, NL, Galna, B, Batten, H, Goffe, L, Karoblyte, G, et al. Changes in children’s physical fitness, BMI and health-related quality of life after the first 2020 COVID-19 lockdown in England: a longitudinal study. J Sports Sci. (2022) 40:1088–96. doi: 10.1080/02640414.2022.2047504
12. Viner, RM, Russell, SJ, Croker, H, Packer, J, Ward, J, Stansfield, C, et al. School closure and management practices during coronavirus outbreaks including COVID-19: a rapid systematic review. Lancet Child Adolesc Heal. (2020) 4:397–404. doi: 10.1016/S2352-4642(20)30095-X
13. Viner, R, Russell, S, Saulle, R, Croker, H, Stansfield, C, Packer, J, et al. School closures during social lockdown and mental health, health behaviors, and well-being among children and adolescents during the first COVID-19 wave: a systematic review. JAMA Pediatr. (2022) 176:400–9. doi: 10.1001/jamapediatrics.2021.5840
14. James, M, Marchant, E, Defeyter, MA, Woodside, JV, and Brophy, S. Impact of school closures on the health and well-being of primary school children in Wales UK: a routine data linkage study using the HAPPEN Survey (2018-2020). BMJ Open. (2021). 11:1–9. doi: 10.1136/bmjopen-2021-051574
15. BBC children in need. Understanding the impact of the COVID-19 pandemic on children and young people. (2020). Available at: https://www.bbcchildreninneed.co.uk/wp-content/uploads/2020/11/CN1081-Impact-Report.pdf.
16. Fahy, N, Hervey, T, Dayan, M, Flear, M, Galsworthy, MJ, Greer, S, et al. Impact on the NHS and health of the UK’s trade and cooperation relationship with the EU, and beyond. Heal Econ Policy Law. (2022) 17:1–26. doi: 10.1017/S1744133122000044
17. Goddard, A. The cost of living crisis is another reminder that our health is shaped by our environment. BMJ. (2022) 1–1. doi: 10.1136/bmj.o1343
18. Mental Health Foundation. Mental health and the cost-of-living crisis report: another pandemic in the making? The Mental Health Foundation. (2022).
19. Todd, C, Christian, D, Davies, H, Rance, J, Stratton, G, Rapport, F, et al. Headteachers’ prior beliefs on child health and their engagement in school based health interventions: a qualitative study. BMC Res Notes. (2015) 8:1–10. doi: 10.1186/s13104-015-1091-2
20. Todd, C, Chistian, D, Tyler, R, Stratton, G, and Brophy, S. Developing HAPPEN (health and attainment of pupils involved in a primary education network): working in partnership to improve child health and education. Perspect Public Health. (2016) 136:115–6. doi: 10.1177/1757913916638231
22. R Core Team. R: A language and environment for statistical computing. Vienna, Austria: R Foundation for Statistical Computing (2021).
23. Whitehead, M. The definition of physical literacy. (2016). Available at: https://www.physical-literacy.org.uk/defining-physical-literacy/ (Accessed January 17, 2020).
24. Invernizzi, PL, Rigon, M, Signorini, G, Alberti, G, Raiola, G, and Bosio, A. Aquatic physical literacy: the effectiveness of applied pedagogy on parents’ and children’s perceptions of aquatic motor competence. Int J Environ Res Public Health. (2021) 18:10847. doi: 10.3390/ijerph182010847
25. Sport Wales. Sport Wales welsh government free swimming initiative (FSI) – A new approach. Sport Wales. (2018). 16–18.
26. Marchant, E, Todd, C, James, M, Crick, T, Dwyer, R, Kingdom, U, et al. Primary school staff reflections on school closures due to COVID-19 and recommendations for the future: a national qualitative survey. Plos One. (2020) 16:1–24. doi: 10.1371/journal.pone.0260396
27. Parnham, JC, Laverty, AA, Majeed, A, and Vamos, EP. Half of children entitled to free school meals did not have access to the scheme during COVID-19 lockdown in the UK. Public Health. (2020) 187:161 March:161–4–4. doi: 10.1016/j.puhe.2020.08.019
28. Jacques-Avinõ, C, López-Jiménez, T, Medina-Perucha, L, De Bont, J, Goncąlves, AQ, Duarte-Salles, T, et al. Gender-based approach on the social impact and mental health in Spain during COVID-19 lockdown: a cross-sectional study. BMJ Open. (2020) 10:e044617–09. doi: 10.1136/bmjopen-2020-044617
29. Waite, P, Pearcey, S, Shum, A, Raw, JAL, Patalay, P, and Creswell, C. How did the mental health symptoms of children and adolescents change over early lockdown during the COVID-19 pandemic in the UK? JCPP Adv. (2021) 1:1–10. doi: 10.1111/jcv2.12009
30. James, M, Jones, H, Baig, A, Marchant, E, Waites, T, Todd, C, et al. Factors influencing wellbeing in young people during COVID-19: a survey with 6291 young people in Wales. PLoS One. (2021). 1–17. doi: 10.1371/journal.pone.0260640
Keywords: children, social interaction, mental health, United Kingdom, survey, primary school, Wales
Citation: Einhorn J, James M, Kennedy N, Marchant E and Brophy S (2024) Changes in self-reported health and wellbeing outcomes in 36,951 primary school children from 2014 to 2022 in Wales: an analysis using annual survey data. Front. Public Health. 12:1285687. doi: 10.3389/fpubh.2024.1285687
Edited by:
Rafaela Rosário, University of Minho, PortugalReviewed by:
Wesley de Oliveira Vieira, Federal University of São Paulo, BrazilSharinaz Hassan, Curtin University, Australia
Copyright © 2024 Einhorn, James, Kennedy, Marchant and Brophy. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Michaela James, bS5sLmphbWVzQHN3YW5zZWEuYWMudWs=