 Beata Wieczorek-Wójcik
Beata Wieczorek-Wójcik Aleksandra Gaworska-Krzemińska
Aleksandra Gaworska-Krzemińska Aleksander Jerzy Owczarek
Aleksander Jerzy Owczarek Dorota Kilańska
Dorota Kilańska- 1Department of Nursing and Medical Rescue, Pomeranian University, Słupsk, Poland
- 2Institute of Nursing and Midwifery, Medical University of Gdańsk, Gdańsk, Poland
- 3Health Promotion and Obesity Management Unit, Department of Pathophysiology, Faculty of Medical Sciences, Medical University of Silesia, Katowice, Poland
- 4Department of Coordinated Care, Medical University of Lodz, Łódź, Poland
Objectives: Falls are associated with increased morbidity, mortality, prolonged hospitalization and an increase in the cost of treatment in hospitals. They contribute to the deterioration of fitness and quality of life, especially among older patients, thus posing a serious social and economic problem. They increase the risk of premature death. Falls are adverse, costly, and potentially preventable. The aim of the study was to analyze the cost-effectiveness of avoiding one fall by nurse care provided by the nurses with higher education, from the perspective of the health service provider.
Methods: The economic analysis included and compared only the cost of nurse intervention measured by the hours of care provided with higher education in non-surgical departments (40.5%) with higher time spend by nurses with higher education level an increase in the number of hours by 10% (50.5%) to avoid one fall. The time horizon for the study is 1 year (2021). Cost-effectiveness and Cost–benefit analysis were performed. All registered falls of all hospitalized patients were included in the study.
Results: In the analyzed was based on the case control study where, 7,305 patients were hospitalized, which amounted to 41,762 patient care days. Care was provided by 100 nurses, including 40 nurses with bachelor’s degrees and nurses with Master of Science in Nursing. Increasing the hours number of high-educated nurses care by 10% in non-surgical departments decreased the chance for falls by 9%; however, this dependence was statistically insignificant (OR = 1.09; 95% CI: 0.72–1.65; p = 0.65). After the intervention (a 10% increase in Bachelor’s Degrees/Master of Science in Nursing hours), the number of additional Bachelor’s Degrees/Master of Science hours was 6100.5, and the cost was USD 7630.4. The intervention eliminated four falls. The cost of preventing one fall is CER = USD 1697.1.
Conclusion: The results of these studies broaden the understanding of the relationship among nursing education, falls, and the economic outcomes of hospital care. According to the authors, the proposed intervention has an economic justification.
1 Introduction
“Delivering high value for patients must be the central and general goal of every health care organization” (1). The European Commission has consistently pursued the Value-based Health Care (VBHC) policy by recommending the extension of the procurement criteria for selecting the providers of health services equal to or exceeding EUR 750,000, and adding the criterion of “best value for money” (2). The value of nursing care for the patient, the healthcare system, and the payer has been proven in many studies, demonstrating not only the costs of insufficient care but also the benefits of adequate nursing staffing (3–17). Adequate staffing and access to necessary resources are vital for nurses to deliver high-quality care, which is conducive to reducing long-term costs associated with poor patient outcomes. Additionally, allowing nurses to work to their full scopes of practice prevents the waste of valuable human capital, particularly in a profession dominated by women, where their skills are often underused (18).
Value-based Health Care is becoming a priority for healthcare management (19). Productivity and sustainability are essential parts of VBHC, where patient experience and safety are quality indicators. Suitable Development Goals (SDGs) include “Good Health and Well-Being.” In order to attain the Good Health goal, it is essential to provide the extent of nursing care that is necessary to achieve a positive health outcome. Achieving positive health outcome is possible through nursing services that contribute to shortening the length of hospital stay and improving the patient’s health status, thus adding health to years (20). Over the past 30 years, the relationship between structural nursing-sensitive indicators and patient outcomes (e.g., falls or lack thereof) has been repeatedly proven (21–23). However, few studies demonstrate the value of nursing care at the process level in influencing health outcomes (21, 22, 24). Delivering high-quality care means providing appropriate care to the right patient, in the right way, at the right time (25), in safe and comfortable working conditions, with positive treatment outcomes achieved for patients (26). The quality of nursing care (27) and patient safety (28, 29) are influenced by workload, which may be affected by a lack of resources. Studies have confirmed that the current minimum nurse staffing standards do not guarantee the desired level of quality in medical services or the implementation of accepted care standards (30). It has also been proven that having an adequate number of nurses is not enough; their qualifications are also crucial for ensuring good quality care (25, 28, 31). Employing better educated nurses appears to make a substantial positive impact on patient outcomes, patient experience, and hospital costs (32). The consequences of the fall include not only pain and suffering (patient perspective), but also translate to prolonged hospital stay (from the hospital’s perspective), and consequently, high costs of treatment and care and increased demand for care (from the payer’s perspective) (33–36). Falls are associated with increased morbidity, mortality (patient perspective), and prolonged hospitalization (patient, payer, and hospital perspective) (37) and an increase in the cost of treatment in hospitals (payer perspective) (16). They contribute to the deterioration of fitness and quality of life (patient perspective) (38), especially among older patients (39) thus posing a serious social and economic problem (40). They increase the risk of premature death (40). In Polish hospitals, the most common adverse events related to nursing care include nosocomial infections, pressure ulcers, falls, and incorrect assessment of the patient’s condition or failure to detect symptoms signaling a deteriorating condition while conducting the assessment of the patient’s condition (41). The costs of preventing falls have been analyzed, and factors that can eliminate them are known; they include improving the quality of care by ensuring an adequate number of nurses to meet patients’ needs (42). Such data are not available in Poland. Moreover, unlike in other countries, hospitals in Poland do not maintain fall registries (43). Additionally, it should be emphasized that the standard practice is to meet the minimum staffing norms for nurses, which do not correspond to quality care indicators. The relationship between staffing levels, qualifications, and falls is not known. A review of the literature did not reveal any publications analyzing these variables, and cost analyses are also lacking (44).
There is a link between higher education of nurses (Bachelor’s Degrees—BSN/Master of Science—MScN) with a reduction in fall rate (45). Many international studies have also confirmed the link between nurse qualifications and: (a) patient outcomes (mortality and satisfaction)—24 studies; (b) knowledge and skills, commitment and job satisfaction, status improvement, and self-confidence—54 studies; (c) organizational benefits including staff stability, health care perception, and care costs—six studies (46). It has been proven that the higher the number of nurses with a BSc or MScN degree, the lower the fall rate per 1,000 patient-days (47). Additionally, a higher Nursing Hours per Patient Day (NHPPD) provided by nurses to severely ill patients is associated with a lower fall rate and more accurate assessments of the patient’s health status (12). Better education and training of nurses in surgical and non-surgical departments are essential in meeting customer expectations and maintaining patient care outcomes (48), and they are critical in achieving value for the patient.
National Health Fund do not indicate the proportion of nurses with higher education to other nursing staff. Training programs for nurses focus on increasing self-confidence, knowledge, critical thinking skills and improving interpersonal skills. Unfortunately, nursing leaders have yet to shape the quality of nursing care based on services selected for their quality-to-price ratio.
The current direction of change in Poland is also slowly toward paying for treatment results rather than procedures (49). As nursing leaders, we see that missed nursing care is endemic across all sectors, and falls are a proven consequence of that issue (50). During the hospital care, falls affect patient mobility and mean more staff involvement in care delivery (38) also due to pressure ulcers, new infections and patient mortality (51, 52).
Falls are among the most common adverse events associated with nursing care. Falls are one of the indicator of the nursing indicators sensitive to nursing care (e.g., C-HOBIC) (6, 53) and recognized in nursing quality indicator systems, such as Nursing Quality Indicators for Reporting and Evaluation® (NQuIRE®) (54). Only a few nursing-sensitive indicators are recognized and used worldwide; they are measured at the structural, process, or outcome levels (22). However, most existing indicators are measured at the structural level (e.g., nursing staff) (55) or at the outcome level (e.g., mortality and adverse events such as urinary tract infections and pressure ulcers) (55–59). In contrast, nursing-sensitive indicators at the process level (e.g., mobility—falls, nutritional support, and vital sign measurements) are rarely used routinely (22, 60), although the failure to meet nursing-sensitive process indicators, sometimes referred to as missed nursing care (50, 61) or nursing care neglect (60), poses a serious problem in healthcare (62, 63). Databases play an important role in ensuring high and consistent quality of healthcare by continuously monitoring treatment, care, and rehabilitation for clinical quality (32, 64). They are increasingly used in healthcare planning and in setting priorities to improve patient outcomes. However, there is often a lack of knowledge about effective reporting and measurement of nursing activities (65). The Quality Act, adopted in Poland in 2023 for the first time in the history of healthcare (66) does not include Nursing Sensitive Indicators including recorded falls despite their proven significance (67).
According to published data, fall incidence rates range from 1.3 to 8.9 per 1,000 patient days (15, 17, 68). There was some tendency for units in larger hospitals to have lower unassisted fall rates. For medical–surgical units, the estimated average fall rate was 10% (95% CI: 5–16%) higher in teaching hospitals (17). Falls are among the main quality of care indicators that are sensitive to nursing care (47). Many of them can be prevented through proper and safe care (69). Healthcare spending in Poland is among the lowest in the EU (70), resulting in prioritizing the low value of services and saving on nursing care. In Poland, nursing care is generally considered a cost. Studies have shown that nurse care costs account for only 25.5–30.1% of the yearly hospital budget (71). Increasing the number of nurses in the healthcare system has impact on the Gross Domestic Product (GDP) growth—the magnitude of the effect of nurse staffing on GDP is 1.52 in Poland, which is among the highest in Europe (72). The procurement criteria of the Polish (19). This paper presents a health technology assessment (HTA) to determine the value of BSN/MScN care.
The aim of the study was to analyze the cost-effectiveness of avoiding one fall by increasing the percentage of nurses with higher education.
2 Materials and methods
The clinical assessment of the impact of BSN/MScN care in medical departments on the incidence of falls was carried out in a case–control (retrospective) study. The analysis concerned patients hospitalized in the period from January 1, 2021 to December 31, 2021 in the following departments: cardiology, neurology, internal disease, and pulmonary diseases, who suffered a fall.
The study site was the Specialist Hospital in Wejherowo [Szpital Specjalistyczny w Wejherowie], one of the four Pomeranian Hospitals in the Pomeranian Region. The hospital provides specialized care at the third reference level of the hospital network for 20% of the region’s population, offering several unique services and certain specialized medical facilities, including specialized cardiac surgery, cardiology, neurology, and orthopedic procedures, as well as an Emergency Department (ED) and intensive care. In 2021, 34,167 patients were hospitalized (90,853 patient-days) in seven medical wards, and 12,472 surgeries were performed, accounting for 21% of the hospital’s patients, with 55% of patients admitted in the urgent (unplanned) mode through the ED.
2.1 Study design and setting
Cost-effectiveness Analysis (CEA) and Cost Benefit Analysis (CBA) was evaluated based on the clinical case study. The analysis scopes were established based on the following: assumptions:
a. population—patients (women and men) over 18 years of age, hospitalized in internal disease, cardiology, neurology, and pulmonary disease during a 12-month period;
b. intervention: a 10% increase in the number of hours of care provided by BSN/MScN nurses up to 50.5%;
c. comparator: current working hours of nurses with higher education (40.5%);
d. outcome: all fall patients, regardless of whether they were injured during the fall; patients and direct cost per care per prevented fall (CER).
The study compared the cost of the current number of hours of care provided by nurses with higher education in non-surgical departments (40.5%) and an increase in the number of her hours by 10% (50.5%) to avoid one fall (the perspective of the provider).
To calculate the cost of avoiding one fall (from the hospital’s perspective), the cost of increasing the proportion of BSN/MScN nurses by 10% was compared with the current standard level of care. The comparison between standard care and the 10% BSN/MScN intervention was based on previous analyses conducted at the studied hospital, which indicated a relationship between the percentage of BSN/MScN nurses and falls in non-surgical wards, when the proportion of BSN/MScN is increased by 10%, and it was arbitrarily determined that the 10% intervention would be used for the calculations in this study. The inclusion criterion for the non-surgical wards in the study was based on the fact that there was no demonstrated relationship between NHPPD and higher education levels in surgical wards (73). The time horizon for the study is 1 year (2021). The study was designed according to the CHEERS protocol (74).
2.2 Collection of data
The data used in the analysis comes from actual calculations and hospital data. The parameters used in the analysis include (1) the actual number of patient and patient days in 2021 (number of patient days is the number of patients admitted to hospital multiplied by the number of days spent in hospital), for which we calculated fall incidence per 1,000 patient days; The study included patients from four non-surgical departments, including 7,305 patients who were hospitalized, which constituted 41,762 patient days. (2) the number of hours provided by nurses, including nurses with higher education, which was monitored daily and recorded in Excel; (3) the average cost of an hour of work performed by nurses with secondary and higher education as of 2021; and (4) the number of falls. The definition of a fall was: an event that resulted in a person unintentionally landing on the ground, floor or other lower level (75). Data on falls were collected in Electronical Health Record (EHR)—EPR: CLININET. Upon admission to the hospital, each patient had his or her risk of falls assessed according to the MORSE scale (used since 2012). The variables assessed were summed, then the system calculated a risk score for each patient. The variables assessed (five risk factors) were: history of falls, multi-morbidities, mobility support, mobility assessment, mental state. The falls register is maintained by the falls team, using a daily reporting system. The analysis of falls concerned monthly and annual periods; the incidence of falls was calculated per 1,000 person-days in the analyzed departments.
2.3 Data analysis
The CEA and CBA analysis is based on the assumption that patients will receive additional hours of care provided by nurses with a BSN/MScN title. The cost of nurses’ salaries was calculated in PLN, and then converted into USD according to the average National Bank of Poland (NBP) exchange rate from 2021 (4.1051). The cost of 1 h of care provided by a nurse with a BSN/MScN degree was calculated by dividing the total salary of nurses with higher education by the actual number of hours of nurses with a BSN/MScN degree. The cost of 1 h of work of a general nurse (i.e., without higher education) was calculated analogically. The intervention involved increasing the number of hours of nurses with higher education, which means an increase in the level of education, and not the employment of nurses, so we calculated the incremental cost (other costs will still be valid after the intervention).
The cost of a BSN/MScN nurse’s working hour was calculated according to the Cookson methodology, i.e., by subtracting the cost of an hour of a nurse without a higher education from the cost of an hour of a graduate nurse. Other costs of care were assumed to be non-differentiating.
In the cost-effectiveness analysis, two measures of health effect were adopted: (1) a fall that can be prevented; (2) the falls that occurred during hospitalization were monitored daily and recorded in Excel. The next step involved calculating the number of falls that could be avoided by increasing the number of BSN/MScN nurses’ working hours by 10%. The result was obtained by dividing the cost of additional hours of BSN/MScN nurses by the number of avoidable falls. To calculate the number of avoidable falls we used the coefficient from previous study. This study showed correlation between education level and falls (backward stepwise regression result). However, there was no relationship between the number of Nursing Hours per Patient Day (NHPPD) and the severity of patients’ condition, and the incidence of falls (73). It was proved the relationship between the organizational change consisting in increasing the number of nurses with higher education by 10% and adverse events in hospitalized patients: deaths—971; rehospitalizations—2,129; bedsores—334; falls—198; pneumonia—143; urinary tract infections—159; and re-operations—153 and hospitalization time. This study included 44,809 patients. The more patients in Cat. III according to PCS, the more frequent the occurrence of falls in surgical departments. An increase in the percentage of patients in PCS category III by 10% = an increase in the incidence of falls by 0.158 per 1,000 patient days [0.0158 (0.0044) p < 0.01]; the more nurses with higher education, the less frequent the occurrence of falls in medical departments. A 10% increase in the percentage of nurses reduces the incidence of falls by 0.737 per 1,000 patient days [−0.0737 (0.0285) p < 0.05]; the more nurses with higher education, the fewer rehospitalizations in surgical and medical departments. An increase in the percentage of nurses by 10% causes a decrease in the incidence of rehospitalization by 24.74 per 1,000 patient days [−2.474 (0.570) p < 0.01] and 8.79 per 1,000 patient days [−0.879 (0.283) p < 0.05]; the more nurses with higher education, the fewer deaths in surgical and medical departments. An increase in the percentage of nurses by 10% causes a decrease in mortality by 3.25 per 1,000 patient days [−0.3250 (0.0448) p < 0.001] and 7.53 per 1,000 patient days [−0.7529 (0.1385) p < 0.001]. Moreover, in the case of medical departments, the mortality rate decreases with an increase in the nursing care rate [−6.8171 (2.3547) p < 0.05] (73). The cost of obtaining a unit of effect which is the cost of avoiding one fall (CER—The cost-effectiveness ratio) refers to the ratio of the cost of the intervention consisting in increasing the number of hours of BSN/MScN nurses by 10% to the health benefit of avoiding a fall was calculated by dividing the cost of additional hours of nurses with higher education by, respectively, the number of avoidable falls.
A cost–benefit analysis (CBA) was conducted in order to verify the cost-effectiveness threshold of the 10% increase in the number of hours of care provided by nurses with higher education and fall prevention from the perspective of the hospital. The number of falls avoidable by increasing the hours of nurses with higher education in non-surgical departments by 10% was the benefit, which was the benefit calculated for the analyzed departments. The next step was to establish the monetary benefit of avoidable falls by calculating the estimated value of nurses’ salaries (including projected growth) according to data from the available literature (25.5%) (76). This value was applied to the hospital budget calculated on the basis of the cost per day of hospitalization according to the hospital price list and then converted into avoidable falls. The CBA analysis was used to verify the cost-effectiveness of increasing the number of hours of care provided by BSN/MScN nurses. The gross monetary benefit was calculated by multiplying the percentage of nurses’ salaries in the hospital budget by the number of avoidable falls. We calculated how much needs be to spent in zloty (1 PLN ≈ 0.243 USD) to save 1 PLN. This analysis was carried out using cost–benefit ratio (CBR) and cost–benefit ratio (BCR). The result obtained in PLN was converted into USD.
GDP per capita was 37,800 USD in 2021 in Poland. The calculations aimed to determine how much we need to spend in zloty (1 PLN ≈ 0.243 USD) to save 1 PLN. The result obtained in PLN was converted into USD.
The study was approved by the Bioethics Committee of the Medical University of Gdansk under approval no. NKBBN/573/2022.
3 Results
In the analyzed period, 7,305 patients were hospitalized, which amounted to 41,762 patient days. The total number of beds in the analyzed non-surgical departments, i.e., pulmonary diseases, internal diseases, neurology, and cardiology, was 158. The average bed occupancy was 85.5%, and the average hospitalization time was 4.8 days. The mean cost of hospitalization based on the price list was USD 2,309 per patient (77).
Care was provided by 100 nurses, including 40 BSN/MScN nurses. The total number of hours of nursing care was 151,286 h, and the number of BSN/MScN nurse hours was 61004.9 (40.5%) before the intervention. After the intervention, the number of BSN/MScN nurse hours was 67105.4. The cost of BNS/MNS nurses’ hours was USD 548611.3 before and USD 556241.7 after the intervention. The difference in total salaries was USD 7907.8.
3.1 Participants’ characteristics
In the analyzed period 7,305 patients were hospitalized, which amounted to 41,762 patient days. In the study population, the number of women was—3117 (42.7%)—and the number of men was 4,188 (57.3%). The average age of patients in the general population was 64.2 years, including women—66.2 and men—63.2. The patient population who suffered a fall (64 patients) included 25 women (39%) and 39 men (61%). Main diagnosis according to ICD-10: Cancer—9 (14.1%);1 Stroke—11 (17.2%);2 Sepsis—6 (9.4%);3 Other disease nervous systems—8 (12.5%);4 Other respiratory diseases—5 (7.8%);5 Heart failure (N17.9)—2 (3.1%); Heart attack—3 (4.7%);6 Heart failure—2 (3.1%); COVID 19–3 (4.7%) (U07.1); Gastrointestinal disease—5 (7.8%);7 Kidney failure (N17.9)—4 (6.2%). The profile of patients who suffered a fall (including those who fell) in the analyzed period was compared according to ICD-10 and 80% of the most common causes of hospitalization were identified. A description of the clinical characteristics of the entire population is provided in Appendix to the article (Table 1).
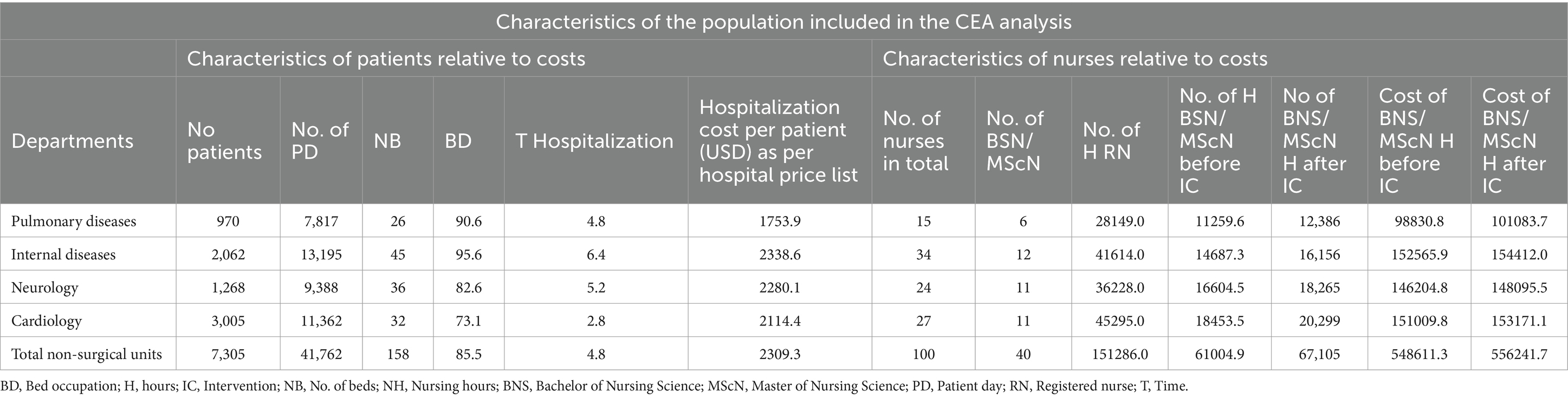
Table 1. A characteristics of nurses included in the CEA analysis.
3.2 Falls analysis
In the analyzed non-surgical departments, there were 64 falls in 2021. An increase in the percentage of BSN/MScN nurses from 40.5 to 50.5% in non-surgical departments decreased the incidence of falls by 9%; however, this dependence was statistically insignificant (OR = 1.09; 95% CI: 0.72–1.65; p = 0.65). The most significant number of falls was recorded in the internal diseases department, while the cardiology department had the smallest one (73). As a result of the 10% increase in the working hours of BSN/MScN nurses, the number of falls decreased by 1 in each of the analyzed departments. The pre-intervention incidence of falls was 1.5 (BSN/MScN ratio = 40.5%), and the post-intervention rate was 1.4 (BSN/MScN ratio = 50.5%) per 1,000 patient days. The incremental change is 0.1 (Table 2).
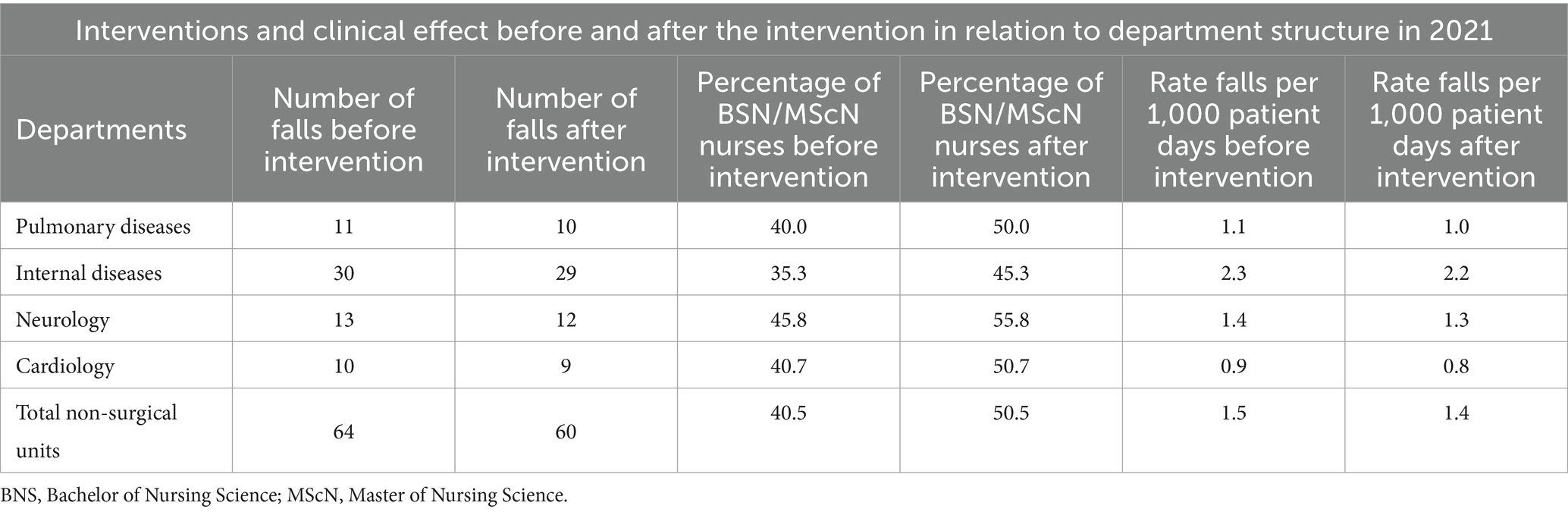
Table 2. Clinical effect of the intervention.
3.3 Intervention effects
After the intervention (a 10% increase in BSN/MScN hours), the number of additional BSN/MScN hours was 6100.5, and the cost was USD 7630.4. In Poland, the cost-effectiveness of technology is determined at the level of three times the value of GDP, which was 166,758 in 2021 (78). The intervention eliminated four falls. The cost of preventing one fall CER = USD 1697.1 (Table 3).
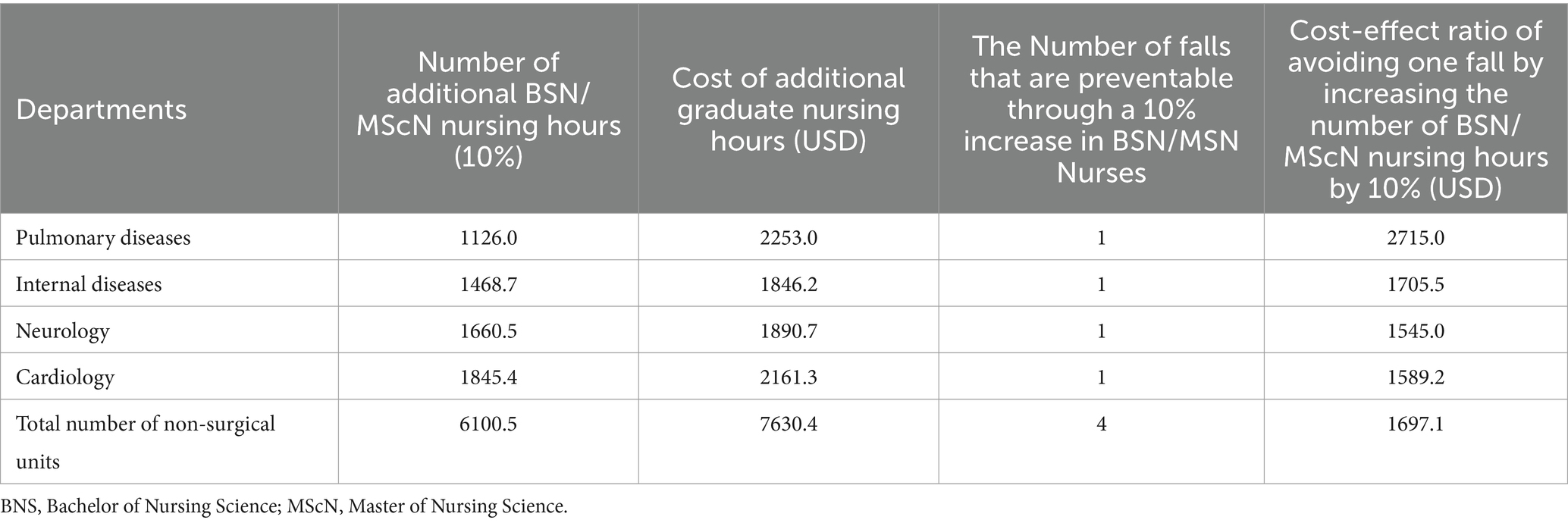
Table 3. Cost-effect ratio (CER).
3.4 Sensitivity analysis
The aim of the analysis was to estimate the extent to which the planned intervention was at risk of inconsistency with the economic forecast. To this end, we changed the number of hours of BSN/MScN nurses, the cost of an hour of BSN/MScN nursing, the number of avoidable falls. A one-way sensitivity analysis was conducted with each parameter tested separately (Table 4).

Table 4. The parameter values used as the baseline for the sensitivity analysis and lower and upper values.
In the sensitivity analysis, the calculated value of the variable for a 10% increase in BSN/MScN nursing hours had a standard deviation of 5%, which was arbitrarily assigned to the parameters of additional BSN/MScN nursing hours and the cost per hour of BSN/MScN nursing care. For avoidable falls, the variable value was calculated at 7%, representing the standard deviation in the quarter with the highest number of falls.
Simulation of the optimistic and pessimistic scenarios indicates the possible effects of a 10% increase in BSN/MScN nursing hours (Figure 1).
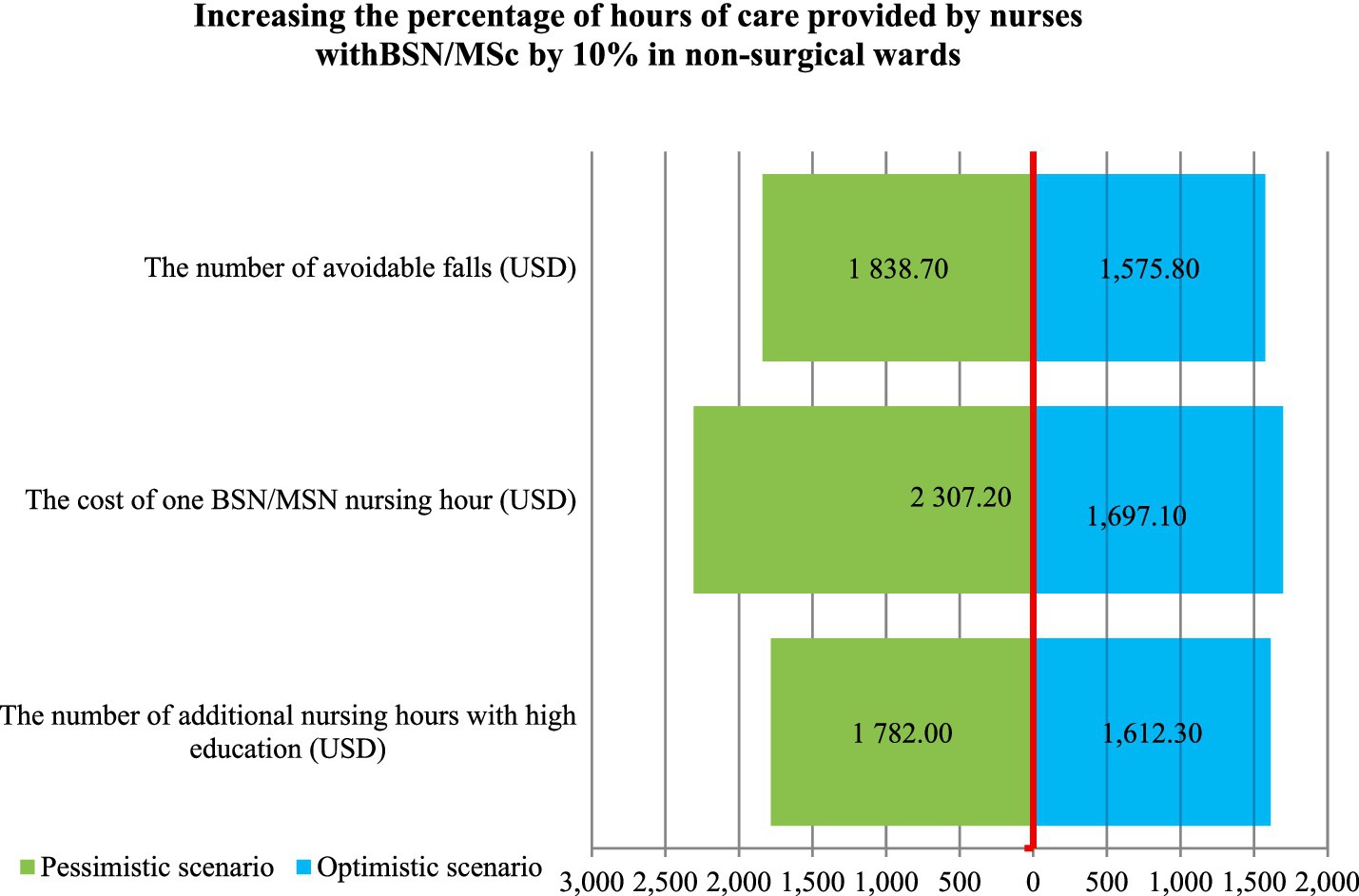
Figure 1. The sensivity analysis.
For the variable of BSN/MScN hours, we tested a 50.5% increase in BSN/MScN hours over the intervention, in comparison with the arbitrarily assigned increase by 5% (SD = 5%). In the pessimistic scenario, SD was subtracted from the number of BSN/MScN hours. In the optimistic scenario, SD was added to the baseline number of BSN/MScN hours.
In the pessimistic scenario for the “cost of 1 h of BSN/MScN” variable, arbitrarily assigned standard deviation SD = 5% was added to the cost of a BSN/MScN nursing hour. The analysis did not include a reduction in wages.
In the pessimistic scenario for the “avoidable falls in 2021” variable, we selected the quarter with the lowest number of falls. On this basis, the number of avoidable falls was calculated.
In the optimistic scenario, the quarter of 2021 with the highest number of falls was selected, and the number of avoidable falls was calculated. In both scenarios, SD = 7%.
The sensitivity analysis shows that with a 10% increase in the number of BSN/MScN nursing hours (6100.5 h), the cost of avoiding one fall is 1697.1 USD. In the optimistic scenario, the number of BSN/MScN nurses’ hours is reduced by 5% (to 5795.5 h) and CER drops to 1612.3 USD. In the pessimistic scenario, an increase in the number of hours of BSN/MScN nurses by 5% (up to 6405.5 h) results in an increase in CER = 1782.0 USD. In the pessimistic scenario, a 5% increase in the cost of a BSN/MScN hour (USD9.4) results in an increase in CER = 2307.2 USD. A reduced cost of a BSN/MScN hour was not analyzed.
In the optimistic scenario, if the number of falls increases to 68 (SD = 7%), CER decreases to 1575.8 USD and in a pessimistic scenario, the number of falls decreases to 60 (7%) and CER increases to 1838.7 USD.
According to the sensitivity analysis, the biggest threat to the cost-effectiveness of the 10% increase in the number of BSN/MScN nursing hours is the increase in the cost of BSN/MScN nurse hours. For the remaining parameters, the result does not change significantly, meaning it is not sensitive to the parameter.
From the provider’s perspective, the cost and benefit analysis demonstrated that increasing the number of BSN/MScN nurses by 10% is a cost-effective means of eliminating missed care resulting in falls. The cost–benefit ratio is 0.1. This means that every zloty invested in eliminating missed care (increasing nursing care) brings a profit of 0.1 PLN. The cost–benefit ratio is 14. This means that the benefit of every zloty invested in increasing nursing care is14 PLN (3.3 USD).
In every respect, the analysis indicates that the net benefit is positive (benefits outweigh costs), so the intervention should be implemented (Table 5).
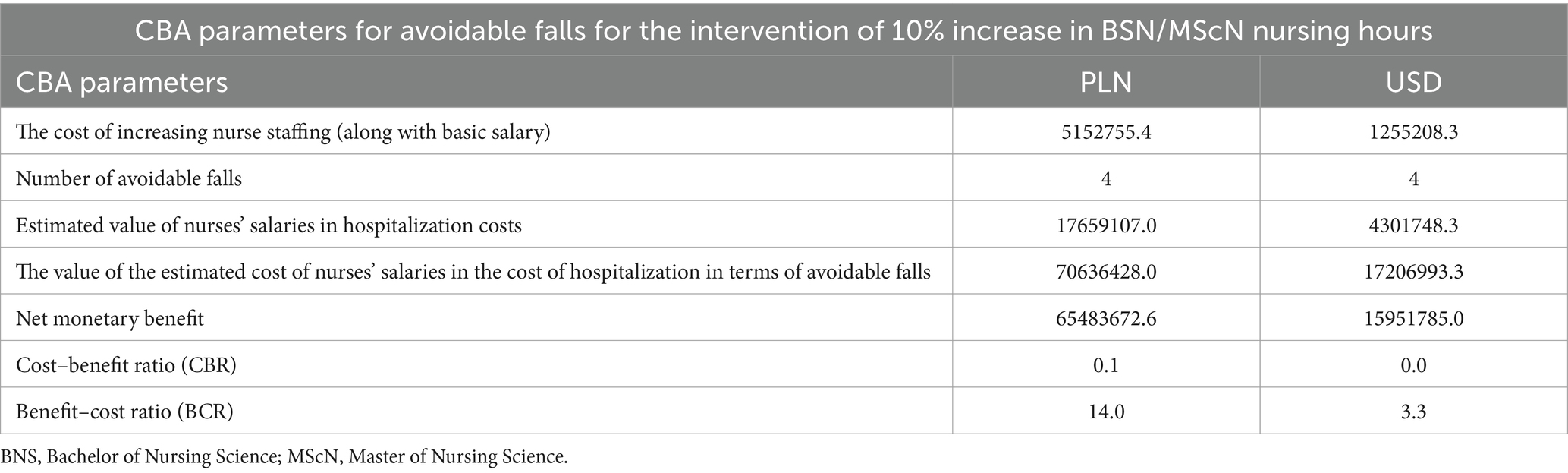
Table 5. The cost–benefit analysis (CBA).
4 Discussion
The CEA we conducted evaluates the cost-effectiveness of a 10% increase in BSN/MScN hours to achieve the clinical effect of avoiding one fall The incremental cost of avoiding one fall (CER) by increasing the number of BSN/MScN nurses by 10% is USD 1697.1. The cost of additional BSN/MScN hours in non-surgical departments in 2021 it is USD 1.00 per hospitalized patient.
The study population included adult patients (7,305) from four specialized hospital departments in 2021. The intervention involved a 10% increase in the number of BSN/MSN hours compared to the standard level of BSN/MScN hours (40.5%). The intended health effect was to reduce the number of falls during hospitalization by eliminating missed care associated with insufficient BSN/MScN staffing. The cost-effectiveness analysis was carried out from the provider’s perspective, i.e., the hospital. We calculated the unit cost of an hour of nursing care and the cost of an hour of care provided by BSN/MScN nurses. The analysis involved the falls that occurred in 2021, and then we calculated avoidable falls.
In the next step, we calculated the unit cost of the effect the avoidable fall (CER). The analysis adopted two scenarios of data variability: pessimistic and optimistic. The sensitivity analysis model considered variables such as the number of hours of BSN/MScN care, the cost of hour BSN/MScN care, and the number of avoidable falls.
The results showed that the calculated cost of avoiding a single fall through the intervention was USD 1697.1, comparable to Cookson’s analysis (1907.5 USD = 1,412 GBP) (79). Similar results were obtained for the BSN/MScN hour cost variable, whose cost amounted to 2,307 USD—more than the increase in the number of BSN/MScN hours variable. In Cookson’s study, that cost was USD 3394.8 (GBP2513) and was > USD 1487.3. The results obtained for the “increase in the number of avoidable falls” variable were also close to Cookson’s results. In the presented study, CER was USD 1,576, compared to USD 1,634.6 (GBP 1,210) in Cookson’s study. A reduction in the number of falls was associated with an increase in CER = 1839 USD. In contrast, Cookson’s analysis indicated USD 2,410 (GBP 1,784).
The incidence rate for falls per 1,000 patient days estimated for the representative Polish population is significantly lower than in the Cookson study. The fall incidence rate was 1.5 per 1,000 patient days, and after a 10% increase in BSN/MScN hours, the incidence rate decreased by 1.4. The Incremental Change was 0.1. This means that four falls were prevented. In Cookson’s study, the fall incidence rate was higher before the intervention—14.62 per 1,000 patient days and higher after the intervention—12.22, in relation to nation-wide rates. The incremental change was 2.40. This meant that 22 falls were prevented. The difference in the number of falls that were prevented was 18. However, the average national fall rate per 100 patient-days in the United Kingdom, to which Cookson’s study referred, was 4.8 (80). According to Cookson, this indicates that in their own studies, the average hospitalization time is short and the risk is lower because it is measured only during hospitalization, which was 4.8 days.
Cookson’s research shows that increasing the percentage of BSN/MScN nurses above 60% results in fewer falls, and improving nurses’ education to reduce falls is cost-effective (79). In contrast, our own study proved that 50.5% is the percentage of graduate nurses which is cost-effective and results in a decrease in the number of falls.
The 10% increase in the number of hours proved to be both clinically effective and cost-effective in the conducted analysis. Each zloty (1 PLN) invested eliminating avoidable falls generates the benefit of PLN 14 PLN (3.3 USD).
There are no studies evaluating the cost-effectiveness of interventions for fall prevention in Poland. In the United States, “patient monitoring” intervention was studied from that perspective. It contributed to reducing the costs down to USD 5895 per fall (ICER) (16). Patient monitoring means eliminating missed care and, as a result, the risk of falls. The presented study operates on the assumption that the “increase in % of BSN/MScN nurses” intervention can also allow for more effective and efficient “monitoring of patients” and thus reduce the number of falls.
The cost of falls in Poland is also unknown. In the United States, the mean fall cost is estimated at USD 7,718 (79).
Poland has requirements concerning minimum employment standards, but the BSN/MSN level is not regulated (81).
Other fall prevention strategies are also researched, e.g., changing nursing staffing levels and assessing the cost-effectiveness of this intervention (45). ICER cost for direct fall care in the United Kingdom was estimated at USD 106.7 (79 GPD) per fall (45). In this study, the cost of effective prevention of one fall (CER) is USD 1,697.1. Thus, it can be concluded that this intervention can prevent generating costs associated with the treatment of complications and eliminate prolonged hospitalization, rehospitalization, rehabilitation and other permanent health effects for patients. Moreover, in Poland, the costs of care for post-fall patients are not separately monitored or shown in statistics as a separate cost of hospitalization. The costs of post-fall direct care and prolonged hospitalization are not specified.
The CEA analysis provides evidence that additional BSN/MScN hours contribute to eliminating avoidable falls. The intervention consisting in increasing care in order to eliminate missed care is cost-effective from both the provider Increasing the hours of nurses with higher education, based on a case–control study, reduces falls by 9%—the intervention is cost-effective. From the perspective of the hospital, in turn, the profitability depends on the profitability threshold established in the hospital. Staff salary is within 60% of the costs (82), and the cost of nurses is only 25.5–30.1% of the hospital budget per year (71). If we accept that nurses’ salaries are 25.5% of the total hospital budget, increasing the percentage of graduate nurses to 50.5% should be acceptable according to HB HTA. In addition, the salary increase due to a 10% increase in BSN/MScN hours is only 1 USD per patient (2021).
The level of nurses’ education plays a vital role in developing awareness and integrating professional values in practice (83). Nurse education is also associated with reduced mortality and rehospitalization of patients (84, 85). Also, knowledge validation through nursing certification has an impact on specific outcomes, such as patient falls and healthcare-related infections (86).
In compliance with the best-quality-to-price ratio procurement criterion, which is recommended in the EU for reimbursement of benefits (2), it is worth adding the criterion of 50.5% BSN/MScN to the criteria for ordering nursing care-related health services in Poland.
Due to the limited number of studies on the cost-effectiveness of fall prevention, further research should be expanded based on a larger population of patients and various hospital profiles to obtain more reliable results in the future.
4.1 Application in practice
The initiated studies could be used to design research in other hospitals and contribute to starting a discussion aimed at creating a national database of nursing-sensitive indicators to support healthcare policy development. The publication of the research results should lead to a proposal from nursing organizations to the Ministry of Health to include nursing-sensitive quality indicators in the executive regulations of the Quality Act and to design a data collection system for the discussed events through a platform containing medical records.
The study results could serve as a basis for discussions on how to finance healthcare services, which should be dependent on hospital care outcomes measured by quality indicators, as is the case in other countries, e.g., C-HOBIC (Standardized Information to Support Clinical Practice and Quality Patient Care), NQuIRE® (Nursing Quality Indicators for Reporting and Evaluation®) (54).
When managing databases of nursing-sensitive indicators, the quality and outcomes assessment model according to Donabedian (15, 87).
4.2 Limitations
The implementation of the intervention will depend on the willingness of the NHS to pay for the value for the patient (VBHC), which is the proven level of BSN/MScN in the study, which is necessary to eliminate missed care for falls. There is no access to data on the cost of falls (the cost of hospitalization for a femoral neck fracture from a hospital and social perspective), which could indicate the additional value of the proposed intervention. The presented results may be conducive to revising the AOTMiT (Polish Agency for Health Technology Assessment and Tariff System) service tariff, which will take into account the cost-effectiveness of BSN/MScN staffing. AOTMiT is expected to announce new estimates for all types of health services and update salaries in health care, including nurses’ salaries in 2024 (88). The lack of national records of adverse events in Poland prevents multicenter analyses, so this study is based on a single hospital. Another limitation is that not all costs were included in the analysis, the analysis only concerns interventions to increase care by nurses with higher education, other costs of the service provider were not counted.
Data availability statement
The datasets presented in this article are not readily available because the data are property of the hospital and have been made available to the researchers only for the purposes of the project. Resources contain non-anonymized data. Requests to access the datasets should be directed to YmVhdGEud2llY3pvcmVrLXdvamNpa0BhcHNsLmVkdS5wbA==.
Ethics statement
The study was approved by the Bioethics Committee of the Medical University of Gdansk under approval no. NKBBN/573/2022. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required from the participants or the participants’ legal guardians/next of kin in accordance with the national legislation and institutional requirements.
Author contributions
BW-W: Writing – original draft, Writing – review & editing. AG-K: Writing – original draft, Writing – review & editing. AO: Writing – original draft, Writing – review & editing. DK: Writing – original draft, Writing – review & editing.
Acknowledgments
We would like to thank Magdalena Władysiuk for consulting the research results and their interpretation in accordance with the HTA methodology.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Footnotes
1. ^C34.2, C78.7, D38.6, D38.3.
2. ^I63.0, I63.5, I64, I64.4, I63.3.
3. ^A41.5, A41.8, A40.1.
4. ^M51 0.1, G62.2, G98, G93.4, G40.3.
5. ^J44.8, J96.1, J26.9, J96.0, J15.8.
6. ^I29.9, I21.3, I25.0.
7. ^K51.9, A04.7.
References
1. Porter, M, and Teisberg-Olmsted, E. Redefining Health Care: Creating Value-Based Competition on Results. Brighton, Massachusetts: Harvard Business School Press (2006).
2. The European Parliament and The Council of the European Union (2014). Directive of the European Parliament the council on public procurement and repealing directive 2004/18/EC no. item 2014/24/EU. Official Journal of the European Union. Brussels: European Parliament. Available online at: https://moz-extension://b5a04a5d-aca7-445e-a01d-73abc565cf29/enhanced-reader.html?openApp&pdf=https%3A%2F%2Feur-lex.europa.eu%2Flegal-content%2FEN%2FTXT%2FPDF%2F%3Furi%3DCELEX%3A32014L0024%26from%3DPL (Accessed February 21, 2023).
3. Jones, CB . The costs of nurse turnover, part 2: application of the nursing turnover cost calculation methodology. J Nurs Adm. (2005) 35:41–9. doi: 10.1097/00005110-200501000-00014
4. Klazinga, N. (2021). The economics of patient safety: safety in the workplace. OECD, Paris. Available online at: https://www.oecd.org/health/OECD-Work-on-Patient-Safety-Brochure-2019.pdf (August 16, 2024).
5. Auraaen, A, Slawomirski, L, and Klazinga, N (2016). The economics of patient safety in primary and ambulatory care: Flying blind. Paris. Available online at: https://www.oecd-ilibrary.org/docserver/baf425ad-en.pdf?expires=1722715677&id=id&accname=guest&checksum=887DAF3A93B3599C5AB186C19C44CB69
6. Xu, X (2015). Identification of nursing-sensitive indicators for nursing quality monitoring and reporting in an Australian context. College of Health and Biomedicine, St Albans. Available online at: https://moz-extension://0be4eb28-a4c9-40b3-ad3b-d9ee4ab3d3fb/enhanced-reader.html?openApp&pdf=https%3A%2F%2Fvuir.vu.edu.au%2F29788%2F3%2FXU%2520Xiaoquan-thesis_nosignature.pdf (Accessed February 21, 2023).
7. Mäki-Turja-Rostedt, S, Stolt, M, Leino-Kilpi, H, and Haavisto, E. Preventive interventions for pressure ulcers in long-term older people care facilities: a systematic review. J Clin Nurs. (2019) 28:2420–42. doi: 10.1111/jocn.14767
8. Magny, E, Vallet, H, Cohen-Bittan, J, Raux, M, Meziere, A, Verny, M, et al. Pressure ulcers are associated with 6-month mortality in elderly patients with hip fracture managed in orthogeriatric care pathway. Arch Osteoporos. (2017) 12:77. doi: 10.1007/s11657-017-0365-9
9. Jessup, RL, Tacey, M, Glynn, M, Kirk, M, and McKeown, L. Evaluation of the effectiveness of a comprehensive care plan to reduce hospital acquired complications in an Australian hospital: protocol for a mixed-method preimplementation and postimplementation study. BMJ Open. (2020) 10:e034121. doi: 10.1136/BMJOPEN-2019-034121
10. Registered Nurses Association of Ontario (2006). Nursing quality indicators for reporting and evaluation®. Best practice guideline program. Available online at: https://rnao.ca/bpg/initiatives/nquire (Accessed August 18, 2024).
11. Lake, ET, Shang, J, Klaus, S, and Dunton, NE. Patient falls: association with hospital magnet status and nursing unit staffing. Res Nurs Health. (2010) 33:413–25. doi: 10.1002/nur.20399
12. Staggs, VS, Knight, JE, and Dunton, N. Understanding unassisted falls: effects of nurse staffing level and nursing staff characteristics. J Nurs Care Qual. (2012) 27:194–9. doi: 10.1097/NCQ.0b013e318241da2d
13. Correa, AD, Marques, IAB, Martinez, MC, Laurino, PS, Leão, ER, and Chimentão, DMN. The implementation of a hospital’s fall management protocol: results of a four-year follow-up. Rev Esc Enferm USP. (2012) 46:67–74. doi: 10.1590/S0080-62342012000100009
14. Irvine, L, Conroy, SP, Sach, T, Gladman, JRF, Harwood, RH, Kendrick, D, et al. Cost-effectiveness of a day hospital falls prevention programme for screened community-dwelling older people at high risk of falls. Age Ageing. (2010) 39:710–6. doi: 10.1093/ageing/afq108
15. Dunton, N, Gajewski, B, Taunton, RL, and Moore, J. Nurse staffing and patient falls on acute care hospital units. Nurs Outlook. (2004) 52:53–9. doi: 10.1016/j.outlook.2003.11.006
16. Spetz, J, Jacobs, J, and Hatler, C. Cost effectiveness of a medical vigilance system to reduce patient falls. Nurs Econ. (2007) 25:333–352.
17. Staggs, VS, and Dunton, N. Associations between rates of unassisted inpatient falls and levels of registered and non-registered nurse staffing. Int J Qual Health Care. (2014) 26:87–92. doi: 10.1093/intqhc/mzt080
18. Limani, D. (2023). Nurses and midwives: overworked, underpaid, undervalued? International Labour Organisation. Available online at: https://ilostat.ilo.org/blog/nurses-and-midwives-overworked-underpaid-undervalued/ (Accessed August 8, 2024).
19. Ministry of Health (2021). Healthy Future. Strategic framework for the development of the health care system for 2021-2027, with a perspective until 2030. (Zdrowa Przyszłość. Ramy strategiczne rozwoju systemu ochrony zdrowia na lata 2021–2027, z perspektywą do 2030). Ministry of Health, Warsaw. Available online at: https://moz-extension://744bb243-1f19-4d5d-acd2-9fa501785ea2/enhanced-reader.html?openApp&pdf=https%3A%2F%2Fwww.gov.pl%2Fattachment%2F4a9bd160-e052-4a52-8fd4-b7c546d556f8 (Accessed April 22, 2022).
20. Rozalska-Walaszek, I, Lesiuk, W, Aftyka, A, and Lesiuk, L. Nursing care of a premature newborn hospitalized in the neonatal intensive care unit. Nurs Probl. (2012) 20:409–15.
21. Burston, S, Chaboyer, W, and Gillespie, B. Nurse-sensitive indicators suitable to reflect nursing care quality: a review and discussion of issues. J Clin Nurs. (2014) 23:1785–95. doi: 10.1111/jocn.12337
22. Oner, B, Zengul, FD, Oner, N, Ivankova, NV, Karadag, A, and Patrician, PA. Introduction nursing-sensitive indicators for nursing care: a systematic review (1997-2017). Nurs Open. (2021) 8:1005–22. doi: 10.1002/nop2.654
23. Twigg, DE, Myers, H, Duffield, C, Giles, M, and Evans, G. Is there an economic case for investing in nursing care—what does the literature tell us? J Adv Nurs. (2015) 71:975–90. doi: 10.1111/jan.12577
24. Kristensen, N, Nymann, C, and Konradsen, H. Implementing research results in clinical practice-the experiences of healthcare professionals. BMC Health Serv Res. (2016) 16:2–10. doi: 10.1186/s12913-016-1292-y
25. VanFosson, CA, Jones, TL, and Yoder, LH. Unfinished nursing care: an important performance measure for nursing care systems. Nurs Outlook. (2016) 64:124–36. doi: 10.1016/j.outlook.2015.12.010
27. Conishi, RMY, and Gaidzinski, RR. Nursing Activities Score (NAS) como instrumento para medir carga de trabalho de enfermagem em UTI adulto. Rev Esc Enferm USP. (2007) 41:346–54. doi: 10.1590/S0080-62342007000300002
28. Carvalho De Oliveira, A, De Carvalho, E, Aguiar, A, Carlos Garcia, P, De, L, and Nogueira, S. Nursing workload and occurrence of adverse events in intensive care: a systematic review. Rev Esc Enferm USP. (2016) 50:679–89. doi: 10.1590/S0080-623420160000500020
29. Gibbon, B, and Crane, J. The impact of “missed care” on the professional socialisation of nursing students: a qualitative research study. Nurse Educ Today. (2018) 66:19–24. doi: 10.1016/j.nedt.2018.04.002
30. Uchmanowicz, I, and Gotlib, J. What is rationing of nursing care? Mod Nurs Health Care. (2018) 7:46–8.
31. Majda, A, Majkut, M, Wróbel, A, Kurowska, A, Wojcieszek, A, Kołodziej, K, et al. Perceptions of clinical adverse event reporting by nurses and midwives. Health. (2024) 12:2–13. doi: 10.3390/healthcare12040460
32. Coster, S, Watkins, M, and Norman, IJ. What is the impact of professional nursing on patients’ outcomes globally? An overview of research evidence. Int J Nurs Stud. (2018) 78:76–83. doi: 10.1016/j.ijnurstu.2017.10.009
33. Stevens, JA, Corso, PS, Finkelstein, EA, and Miller, TR. The costs of fatal and non-fatal falls among older adults. Inj Prev. (2006) 12:290–5. doi: 10.1136/ip.2005.011015
34. Joint Commission Accredited Organizations and Interested Health Care Professionals (2015). Sentinel event alert 55: preventing falls and fall related injuries in health care facilities. A complimentary publication of The Joint Commission Issue 55. Available online at: www.jointcommission.org
35. Haddad, YK, Bergen, G, and Florence, CS. Estimating the economic burden related to older adult falls by state. J Public Health Manag Pract. (2019) 25:E17–24. doi: 10.1097/PHH.0000000000000816
36. Edbom-Kolarz, A, and Marcinkowski, JT (2011). Upadki osób starszych-przyczyny, następstwa, profilaktyka. Available online at: https://www.h-ph.pl/hyg.php (Accessed February 21, 2023).
37. Long, Y, Wang, T, Xu, X, Ran, G, Zhang, H, Dong, Q, et al. Risk factors and outcomes of extended length of stay in older adults with intertrochanteric fracture surgery: a retrospective cohort study of 2132 patients. J Clin Med. (2022) 11. doi: 10.3390/jcm11247366
38. Willis, E, and Brady, C. The impact of “missed nursing care” or “care not done” on adults in health care: a rapid review for the consensus development project. Nurs Open. (2022) 9:862–71. doi: 10.1002/nop2.942
39. World Health Organization (WHO) (2023). Step Safely: Strategies for preventing and managing falls across the life-course. Available online at: https://www.who.int/publications/i/item/978924002191-4 (Accessed February 21, 2023).
40. Burns, ER, Stevens, JA, and Lee, R. The direct costs of fatal and non-fatal falls among older adults—United States. J Saf Res. (2016) 1:99–103. doi: 10.1016/j.jsr.2016.05.001
41. Piątek, A (2013). “Adverse events in the professional practice of nurses” in The image of a nurse and midwife against the background of new challenges in Polish and European nursing. ed. The Main Chamber of Nurses and Midwives, The Main Chamber of Nurses and Midwives, Warsaw. 213–222.
42. Encinosa, WE, and Hellinger, FJ. The impact of medical errors on ninety-day costs and outcomes: an examination of surgical patients. Health Serv Res. (2008) 43:2067–85. doi: 10.1111/j.1475-6773.2008.00882.x
43. Montalvo, I . (2008). The National Database of Nursing Quality IndicatorsTM (NDNQI®). Online J Issues Nurs. 12. doi: 10.3912/OJIN.VOL12NO03MAN02
44. Asmirajanti, M, and Sukma, MC. Nurse implementation in preventing the risk of fall in hospital: literature review. Malays J Public Health Med. (2022) 22:80–9. doi: 10.37268/mjphm/vol.22/no.3/art.1619
45. Cookson, G, and Mc Govern, A (2014). The cost-effectiveness of nurse staffing and skill mix on nurse sensitive outcomes. A report for the National Institute for health and care excellence. A report for the National Institute for health and care excellence. London. Available online at: https://moz-extension://b5a04a5d-aca7-445e-a01d-73abc565cf29/enhanced-reader.html?openApp&pdf=https%3A%2F%2Fwww.nice.org.uk%2Fguidance%2Fsg1%2Fdocuments%2Fsafe-staffing-guideline-consultation9 (Accessed March 11, 2023).
46. Whitehead, L, Ghosh, M, Walker, DK, Bloxsome, D, Vafeas, C, and Wilkinson, A. The relationship between specialty nurse certification and patient, nurse and organizational outcomes: a systematic review. Int J Nurs Stud. (2019) 93:1–11. doi: 10.1016/j.ijnurstu.2019.02.001
47. Griffiths, P, Ball, J, Drennan, J, James, L, Jones, J, Recio, A, et al. (2014). The association between patient safety outcomes and nurse/healthcare assistant skill mix and staffing levels and factors that may influence staffing requirements.
48. Abdul Rahman, H, Jarrar, M, and Don, MS. Nurse level of education, quality of care and patient safety in the medical and surgical wards in Malaysian private Hospitals: a cross-sectional study. Global J Health Sci. (2015) 7:331–7. doi: 10.5539/gjhs.v7n6p331
49. Niedzielski, A. (2019). Kierunek zmian to płacenie nie za procedury, ale za wyniki leczenia. Polityka Zdrowotna. Available online at: https://politykazdrowotna.com/artykul/a-niedzielski-kierunek-zmian-to-placenie-nie-za-procedury-ale-za-wyniki-leczenia/832206 (Accessed February 21, 2023)
50. Kalisch, BJ . Missed nursing care: a qualitative study. J Nurs Care Qual. (2006) 21:306–13. doi: 10.1097/00001786-200610000-00006
51. Kalisch, BJ, and Xie, B. Errors of omission: missed nursing care. West J Nurs Res. (2014) 36:875–90. doi: 10.1177/0193945914531859
52. Wieczorek-Wojcik, B, Gaworska-Krzemińska, A, Owczarek, AJ, and Kilańska, D. In-hospital mortality as the side effect of missed care. J Nurs Manag. (2020) 28:2240–6. doi: 10.1111/jonm.12965
53. Hannah, KJ, White, PA, Nagle, LM, and Pringle, DM. Standardizing nursing information in Canada for inclusion in electronic health records: C-HOBIC. J Am Med Inform Assoc. (2009) 16:524–30. doi: 10.1197/jamia.M2974
54. RNAO Nursing Quality Indicators for Reporting and Evaluation® (NQuIRE®). (2012) RNAO.ca [Internet]. Available at: https://rnao.ca/bpg/initiatives/nquire (Accessed March 11, 2023).
55. Hoque, R, and Sorwar, G. Understanding factors influencing the adoption of mHealth by the elderly: an extension of the UTAUT model. Int J Med Inform. (2017) 101:75–84. doi: 10.1016/j.ijmedinf.2017.02.002
56. Richards, DA, Hanssen, TA, and Borglin, G. The second triennial systematic literature review of European nursing research: impact on patient outcomes and implications for evidence-based practice. Worldviews Evid-Based Nurs. (2018) 15:333–43. doi: 10.1111/wvn.12320
57. Ministry of Health (2023). Regulation of the Council of Ministers No. Item 2023/1692. (Ustawa z dnia 16 czerwca 2023 r. o jakości w opiece zdrowotnej i bezpieczeństwie pacjenta).The Sejm Warsaw. p. 1–22. Available online at: https://isap.sejm.gov.pl/isap.nsf/download.xsp/WDU20230001692/T/D20231692L.pdf (Accessed August 1, 2024).
58. Mainz, H, Odgaard, L, and Kristensen, PK. Nursing representatives in clinical quality databases and the presence of nursing-sensitive indicators of fundamental nursing care. J Adv Nurs. (2023) 79:1129–38. doi: 10.1111/jan.15400
59. Montalvo, I . The National Database of nursing quality indicators™ (NDNQI®). Online J Issues Nurs. (2008) 12. doi: 10.3912/OJIN.Vol12No03Man02
60. Gemeinsamer Bundesausschuss (2024). Richtlinie zur datengestützten einrichtungsübergreifenden Qualitätssicherung. Available online at: https://www.g-ba.de/richtlinien/105/
61. Andersson, J, Imberg, S, and Rosengren, K. Documentation of pressure ulcers in medical records at an internal medicine ward in university hospital in western Sweden. Nurs Open. (2023) 10:1794–802. doi: 10.1002/nop2.1439
62. Emilsson, L, Lindahl, B, Köster, M, Lambe, M, and Ludvigsson, JF. Review of 103 Swedish healthcare quality registries. J Intern Med. (2015) 277:94–136. doi: 10.1111/joim.12303
63. NHS (2019). The NHS Patient Safety Strategy Safer culture, safer systems, safer patients NHS England and NHS Improvement [Internet]. Available from: https://www.england.nhs.uk/patient-safety/the-nhs-patient-safety-strategy/ (Accessed August 2, 2024).
64. Griffiths, P, Recio-Saucedo, A, Dallora, C, Briggs, J, Maruotti, A, Meredith, P, et al. The association between nurse staffing and omissions in nursing care: a systematic review. J Adv Nurs. (2018) 74:1474–87. doi: 10.1111/jan.13564
65. White, EM, Aiken, LH, and McHugh, MD. Registered nurse burnout, job dissatisfaction, and missed Care in Nursing Homes. J Am Geriatr Soc. (2019) 67:2065–71. doi: 10.1111/jgs.16051
66. Francis, R (ed.) (2013). The mid Staffordshire NHS foundation trust public inquiry report of the mid Staffordshire NHS foundation trust public inquiry executive summary. London. Available online at: www.midstaffspublicinquiry.com (Accessed August 8, 2024).
67. Kristensen, PK, Falstie-Jensen, AM, Madsen, M, and Johnsen, SP. Patient-related healthcare disparities in the quality of acute hip fracture care: a 10-year nationwide population-based cohort study. BMJ Open. (2021) 11:51424. doi: 10.1136/bmjopen-2021-051424
68. Cafardi, SG, Miller, RD, Eng, T, Kandilov, AMG, Cromwell, J, and Mccall, N (2012). Readmissions due to hospital-acquired conditions (HACs): Multivariate modeling and under-coding analyses final report prepared for.
69. Grochans, E, Kardela, B, Starczewska, M, Szkup-Jabłońska, M, Jurczak, A, and Kuczyńska, M. The analysis of falls in patients hospitalized at geriatric ward. Hygeia Public Health. (2012) 47:360–364.
70. Eurostat (2022). Government expenditure on health. Available online at: https://ec.europa.eu/eurostat/statistics-explained/index.php?title=Government_expenditure_on_health (Accessed April 2, 2023).
71. Sanson, G, Welton, J, Vellone, E, Cocchieri, A, Maurici, M, Zega, M, et al. Enhancing the performance of predictive models for hospital mortality by adding nursing data. Int J Med Inform. (2019) 125:79–85. doi: 10.1016/j.ijmedinf.2019.02.009
72. Amiri, A, and Solankallio-Vahteri, T. Analyzing economic feasibility for investing in nursing care: evidence from panel data analysis in 35 OECD countries. Int J Nurs Sci. (2020) 7:13–20. doi: 10.1016/j.ijnss.2019.06.009
73. Wieczorek-Wójcik, B. (2016). The level of nursing staffing and the frequency and type of adverse events. Dissertation. Medical University of Gdańsk, Gdańsk.
74. Husereau, D, Drummond, M, Augustovski, F, De Bekker-Grob, E, Briggs, AH, Carswell, C, et al. Consolidated Health Economic Evaluation Reporting Standards (CHEERS 2022) statement: updated reporting guidance for health economic evaluations. BMJ. (2022) 2022:376. doi: 10.1136/bmj-2021-067975
75. World Health Organisation (2021). Falls. World Health Organisation. Available online at: https://www.who.int/news-room/fact-sheets/detail/falls (Accessed June 6, 2024).
76. Welton, JM . Hospital nursing workforce costs, wages, occupational mix, and resource utilization. J Nurs Adm. (2015) 45:S10–5. doi: 10.1097/NNA.0000000000000247
77. Pomeranian Hospitals (2023). Pomeranian Hospitals Price list. Available online at: https://www.szpitalepomorskie.eu/cennik/ (Accessed April 12, 2023).
78. AOTMIT (2021). Announcement of the president of the Agency for Health Technology Assessment and Tariff System on the amount of the threshold for the cost of obtaining an additional quality-adjusted year of life applicable from October 29, 2021—Agency for Health Technology Assessment and Tariff System. Available online at: https://www.aotm.gov.pl/aktualnosci/najnowsze/komunikat-prezesa-agencji-oceny-technologii-medycznych-i-taryfikacji-w-sprawie-obowiazujacej-od-dnia-29-pazdziernika-2021r-wysokosci-progu-kosztu-uzyskania-dodatkowego-roku-zycia-skorygowanego-o-jak/ (Accessed March 11, 2023).
79. McGovern, A. (2014). The cost-effectiveness of nurse staffing and skill mix on nurse sensitive outcomes professor Graham Cookson.
80. Healey, F, Pryce, A, and Joule, N (2007). “Slips, trips and falls in hospital” in The third report from the patient safety observatory. London.
81. Polish Federation of Hospitals (2022). Employment standards for nurses: the polish Federation of Hospitals wants changes. Medexpress.
82. Schwieters, J, and Harper, D. 7 steps toward gaining control of your labor costs: as healthcare organizations face shrinking revenues and rising expenses, one cost-saving solution could lie in addressing your facility’s labor costs. Healthcare Fin Manag. (2007) 61:76–81.
83. Sibandze, BT, and Scafide, KN. Among nurses, how does education level impact professional values? A systematic review. Int Nurs Rev. (2018) 65:65–77. doi: 10.1111/inr.12390
84. Wieczorek-Wójcik, B, Gaworska-Krzemińska, A, Owczarek, A, Wójcik, M, Orzechowska, M, and Kilańska, D. The influence of nurse education level on hospital readmissions—a cost-effectiveness analysis. Int J Environ Res Public Health. (2022) 19. doi: 10.3390/ijerph19074177
85. Wieczorek-Wójcik, B, Gaworska-Krzemíńska, A, Szynkiewicz, P, Wójcik, M, Orzechowska, M, and Kilańska, D. Cost-effectiveness analysis of improving nurses’ education level in the context of in-hospital mortality. Int J Environ Res Public Health. (2022) 19:996. doi: 10.3390/ijerph19020996
86. Coelho, P . Relationship between nurse certification and clinical patient outcomes: a systematic literature review. J Nurs Care Qual. (2020) 35:E1–5. doi: 10.1097/NCQ.0000000000000397
87. Donabedian, A . The role of outcomes in quality assessment and assurance. Qual Rev Bull. (1992) 18:356–60. doi: 10.1016/S0097-5990(16)30560-7
88. Nocuń, K., and Prawo, PL (2023). Healthcare pay rises from July 2023 (Podwyżki w ochronie zdrowia od lipca 2023 r.). Available online at: https://www.prawo.pl/zdrowie/podwyzki-w-ochronie-zdrowia-od-lipca-2023-r,518677.html (Accessed March 11, 2023).
Appendix
Appendix 1 A description of the clinical characteristics of the entire population of the study.

Keywords: cost-effectiveness analysis, cost-benefit analysis, accountable care organization, falls, patient outcome assessment, patient safety, nursing staff
Citation: Wieczorek-Wójcik B, Gaworska-Krzemińska A, Owczarek AJ and Kilańska D (2024) Economic evaluation of the prevention of falls resulting from missed care in polish hospitals. Front. Public Health. 12:1228471. doi: 10.3389/fpubh.2024.1228471
Edited by:
Jouhanna Menegaz, Santa Catarina State University, BrazilReviewed by:
Olga Ribeiro, Escola Superior de Enfermagem do Porto, PortugalCheng-Feng Wu, Hubei University of Economics, China
Copyright © 2024 Wieczorek-Wójcik, Gaworska-Krzemińska, Owczarek and Kilańska. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Dorota Kilańska, ZG9yb3RhLmtpbGFuc2thQGd1bWVkLmVkdS5wbA==