 Narges Neyazi
Narges Neyazi Ali Mohammad Mosadeghrad3*
Ali Mohammad Mosadeghrad3* Mahnaz Afshari
Mahnaz Afshari Parvaneh Isfahani
Parvaneh Isfahani- 1International Campus, School of Public Health, Tehran University of Medical Sciences, Tehran, Iran
- 2Health System Development, World Health Organization Country Office, Kabul, Afghanistan
- 3Health Information Management Research Center, School of Public Health, Tehran University of Medical Sciences, Tehran, Iran
- 4Social Determinants of Health Research Center, Saveh University of Medical Sciences, Saveh, Iran
- 5School of Public Health, Zabol University of Medical Sciences, Zabol, Iran
Non-communicable diseases (NCDs) and their risk factors are the leading cause of death worldwide and contribute to 74.3% of deaths globally in 2019. The burden of NCDs is escalating in Afghanistan. Currently, every seconds, people in Afghanistan are dying of NCDs. Addressing this challenge in Afghanistan needs effective and practical interventions. This study aimed to identify the strategies developed and implemented in countries with low non-communicable premature death. To conduct a scoping review, we followed the six-step Arksey and O'Malley protocol and searched for eligible articles on eight international databases and the gray literature. The study followed the Preferred Reporting Items for Systematic review and Meta-Analysis (PRISMA) guidelines. The inclusion criteria were English documents and evidence produced up to 30 November 2021 for the control of NCDs. We excluded incomplete texts, duplicates, and dissertations due to lack of access. We used EndNote X9 and MaxQDA software for data management and analysis. We conducted content analysis for this study. A total of 122 documents developed between 1984 and 2021 met the inclusion criteria. We identified 35 strategies from which the most used strategies were related to unhealthy diets and smoking cessation programs. Canada (26.4%), Korea (19.8%), and the United Kingdom (19%) have the most publications on the control and prevention of NCDs among the countries included in the study. Most strategies were implemented over 2 years (41%). This study recommends specific interventions to control and prevent NCDs for the main risk factors of tobacco use, unhealthy diet, physical inactivity, and the main non-communicable diseases such as heart diseases, cancers, diabetes, and chronic obstructive pulmonary diseases. Afghanistan Ministry of Public Health, the WHO country office, and other involved stakeholders can use the findings of this review to design and implement strategies for controlling and preventing NCDs in Afghanistan. International organizations such as the World Health Organization, United Nations Agencies, the World Bank, and other involving communities should invest in strengthening good health governance in Afghanistan. The Afghan Government should focus on promoting and funding health literacy among the public and self-care to control and prevent NCDs.
1. Introduction
Non-communicable diseases (NCDs) are the major cause of death worldwide. The four prominent diseases are cardiovascular diseases, cancers, diabetes, and chronic obstructive pulmonary diseases (COPD) (1). NCDs and their common risk factors were the cause of 74.3% of deaths globally in 2019 (2). Importantly, three-quarters of these deaths and 80% of premature deaths occurred in low- and middle-income countries (LMICs) (3). Four risk factors are the common contributors to these diseases: smoking, harmful use of alcohol, physical inactivity, and unhealthy diet (4). As these factors can be influenced and contribute to reducing premature death, it is of utmost importance to focus on measures to reduce them.
Afghanistan is classified as a low-income country in which the health indicators have the worst situation after some African countries such as Sierra Leone, Central African Republic, Chad, Guinea-Bissau, and Nigeria in the world (5). This country was positioned at 169 out of 188 in the low development category (6). The total population of Afghanistan is 32,527,000 and the country's size is 625,864 km2. More than half of Afghanistan's population is male (51.3%) (7) and the median age is 18.4 years (8). National health services is managed by the Ministry of Public Health (MoPH) financed by donors and the government, and services are delivered based on two packages: Basic Packages of Health Services (BPHS) and Essential Package of Hospital Services (EPHS). These two packages were the main reforms that happened in Afghanistan's health system and had considerable effects on the health situation and indicators in Afghanistan. BPHS included the most needed services at the health posts and health center levels of the health system up to district hospitals. EPHS provides guidance to enable hospitals to function more effectively as part of the health system (9).
The burden of NCDs is escalating in Afghanistan. Based on the Afghanistan Non-Communicable Diseases and Injuries (NCDI) Poverty Commission 2018 Report, 23.6% of Disability-Adjusted Life Years (DALY) burden is attributed to cardiovascular diseases, and the next diseases with high DALY burden are neoplasms (8.9%), chronic respiratory diseases (5.2%), digestive diseases (5.1%), and diabetes mellitus (4.3%) (10). The primary studies about the burden of major NCDs are limited in Afghanistan, so the specific etiology is also unclear. However, mortality trends also show the burden of NCDs. Afghanistan Mortality Survey (AMS) 2010 revealed that about 46% of mortality in Afghanistan is mainly due to cardiovascular diseases (female 17.9% and male 14%), cancer (female 8.3% and male 7.3%), diabetes mellitus (female 2.7% and male 3.7%), respiratory disease (female 2.3% and male 1.9%), and injuries. It means that every two Afghans are dying from NCDs in Afghanistan and based on the Afghanistan NCDI poverty commission 2018 report, 56.6% of NCDs DALYs and the probability of premature mortality from target NCDs is 30% in Afghanistan (3). However, it is mentionable that the mortality data are related to the pre-COVID era, and huge shifts are expected in many countries in the share of communicable diseases and NCDs since the emergence of COVID-19. Despite its high burden, NCDs have ranked very low among government and donor priorities. The MoPH recently developed a national strategy for the prevention and control of NCDs 2015–2020 (11) and is currently working on the second strategy for 2022–2027. NCD-related health service delivery is still limited by the Afghanistan health system. The public sector lacks institutions with technical expertise for major NCDs. In this context, the private sector (not-for-profit and for-profit providers and contractors) is the prominent source of outpatient services. The for-profit sector provides mainly curative care. The national NCDs surveillance system, which is crucial for informed policy and strategy, has not been established yet. The mechanism for death registration and the qualification of the cause of death information does not exist (12). In addition, Afghanistan's health system is mainly financed by private out-of-pocket payments (77%) and development partners (13). Although several health strategies were developed for Afghanistan, there is no focus on NCDs, which is a major shortcoming as NCDs are increasing rapidly in Afghanistan.
In the first decade of the 21st century, many scientists and international organizations called for a global response to NCDs to control the global crisis (14). The initial efforts to control the NCDs pandemic started by WHO in 2010 by publishing “the Package for Essential Non-communicable (PEN) Diseases interventions for primary healthcare in low-resource settings” (15). It was followed by a high-level United Nations meeting in September 2011 that endorsed a declaration on the prevention and control of NCDs with a special focus on the challenges of developing countries (16, 17). These efforts were continued by a series of publications such as the WHO NCDs global monitoring framework; a report of WHO on the NCDs country profile; a global action plan for the prevention and control of NCDs 2013–2020; WHO regional action plan for prevention and control of NCDs; resolutions WHA63.14: restriction on marketing of foods and non-alcoholic beverages to children; global code of practice on the marketing of unhealthy food and beverages to children 2012; 2017 WHO Cancer Resolution; WHO mental health action plan 2013–2020; and Montevideo roadmap 2018–2030 on NCDs as a sustainable development priority (18). This shows the presence of many guidelines, roadmaps, and plans developed internationally which can be used by any individual country. However, in a literature review, we found two documents on controlling and preventing NCDs in Afghanistan which is as follows: the national strategy to control and prevent non-communicable diseases in Afghanistan (2015–2020) and the Afghanistan NCDI poverty commission report (2018).
International programs led to aging and longer life expectancy by addressing infectious diseases. The world bank data show that the life expectancy at birth increased from 52.5 years in 1960 to 72.7 years in 2019 globally (19). It resulted in an increased number of elderly people with NCDs, especially in low- and middle-income countries (LMICs) after a high incidence in higher-income countries. Currently, LMICs have 80% of the NCDs burden, especially in Southeast Asia and Eastern Mediterranean regions (20). NCDs also affect the economies of nations by lowering earning capacity, reducing productivity, and increasing household expenditures (21, 22).
Addressing this global challenge needs effective interventions which contribute to decreasing morbidity, premature death, and disability at the global level (20, 22). The World Health Assembly adopted a comprehensive set of indicators in 2013 as a global monitoring framework for NCDs. Since then, WHO published three sets of monitoring progress reports showing member states' status on achieving the specified targets. The reports indicate that some countries have considerable progress toward controlling and preventing NCDs. Nevertheless, many others including Afghanistan do not meet the targets. Based on the reports, Afghanistan has only conducted a national STEP survey in 2018, and there are national integrated NCD policy/strategy/action plans, smoke-free policies, and regulation on bans on advertising, promotion, and sponsorship of tobacco products. In addition, there are measures to restrict the harmful use of alcohol and policies and measures to restrict the marketing of breast-milk substitutes. Based on this progress report, the following targets are not achieved by Afghanistan: determining the national NCD targets and indicators, generating mortality data on NCDs, increasing excise taxes and prices on tobacco products, using large graphic health warnings/plain packaging on tobacco products, conducting mass media campaigns to reduce the tobacco demand, developing and implementing the strategies toward unhealthy diet reduction, addressing physical inactivity in the community, development of a guideline for the management of major NCDs, and using preventing measures for heart attacks and strokes. However, the countries which have good progress with cost-effective and feasible interventions can be a benchmark for other countries (23–25).
So, we used the NCDs progress monitor report 2020 to identify countries with a percentage of death from NCDs higher than 70% and a probability of premature mortality from target NCDs <14%. It means that these countries designed and implemented effective strategies for preventing and controlling NCDs despite their high mortality rate. We also tried to select countries from each region of the World Health Organization (African region, region of the Americas, South-East Asian region, European region, and Eastern Mediterranean region). This study aimed to identify the promising strategies to control and prevent NCDs which have already been implemented in 15 high- and middle-income countries from all over the world through a scoping review and propose the strategies which are appropriate to Afghanistan context compared to the recommended best buys interventions report of WHO (26). In this report, WHO proposed 16 interventions considered the most cost-effective and feasible for implementation in low- and middle-income countries (LMICs) with an average cost-effectiveness ratio of ≤1$100/DALY applicable in LMICs.
2. Methods
We conducted a scoping review from September to December 2021. Scoping review studies examine the nature, range, and extent of research activities, determine gaps in the literature, and summarize the research findings (27). We used the six-step Arksey and O'Malley protocol for this study based on the following: 1, identifying the research question; 2, searching for relevant studies; 3, selecting studies; 4, charting the data; 5, collating, summarizing, and reporting the results; and 6, consulting with stakeholders to inform or validate findings of the study (28).
We investigated the strategies to prevent and control NCDs in the selected countries. We carried out this study by searching eight international databases (PubMed through MED-LINE, Web of Science, Scopus, Science Direct, Springer, Wiley, Emerald, and ProQuest) and searching Google Scholar for literature published up to 30 November 2021. Moreover, we reviewed reports from WHO and the World Bank. We used three key terms to search the strategies (NCDs, reduction, and strategies). In addition to the key terms, we used Medical Subject Headings (MeSH) terms. Table 1 shows the search strategy in the selected international databases.
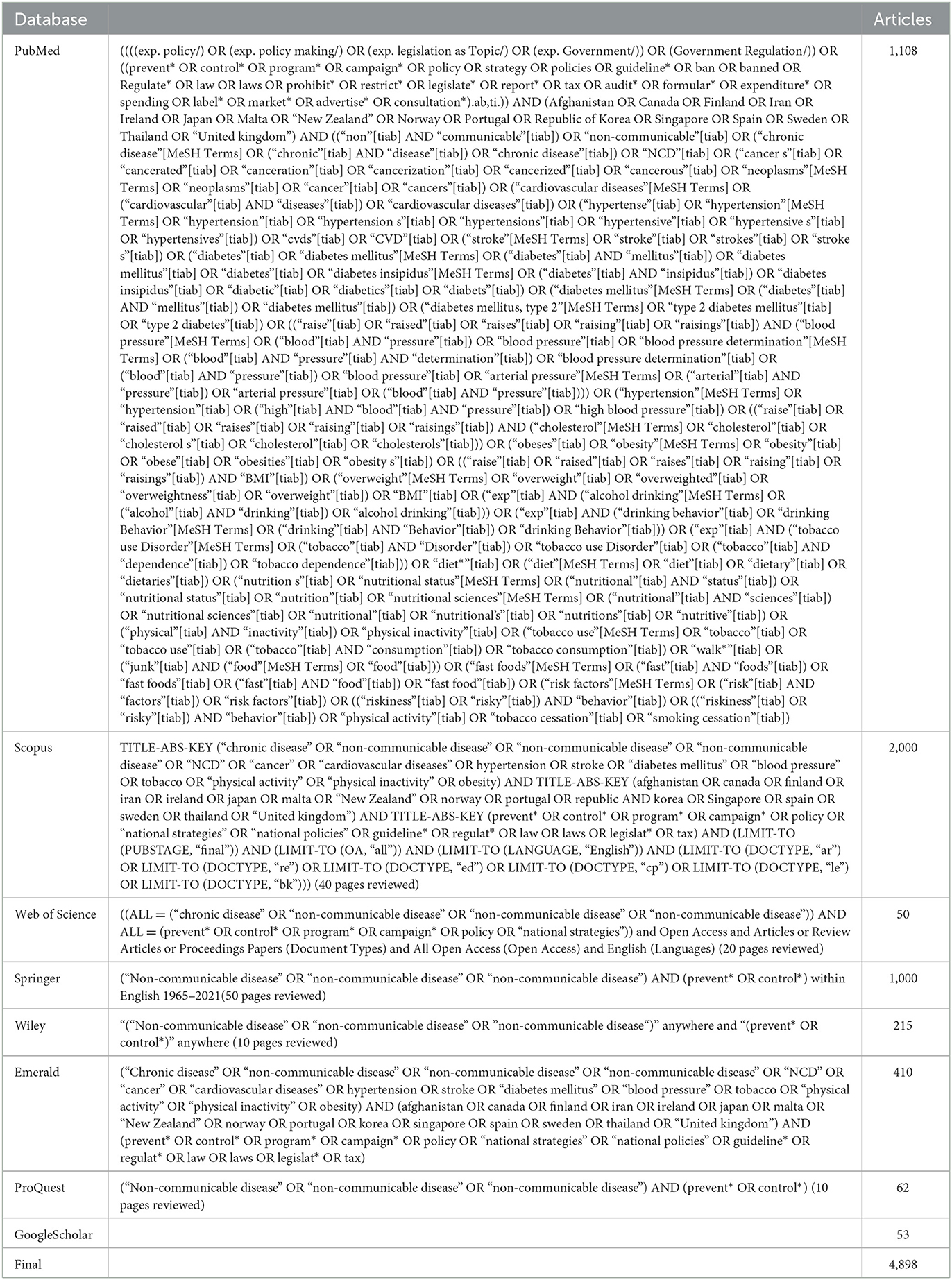
Table 1. Search strategy terms in selected databases.
The inclusion criteria were English documents and evidence produced up to 30 November 2021 for the control of NCDs in selected countries (Iran, Malta, Thailand, Spain, Sweden, Singapore, United Kingdom, Republic of Korea, Portugal, Norway, New Zealand, Japan, Ireland, Finland, and Canada). These countries had a percentage of death from NCDs higher than 70% and the probability of premature mortality from target NCDs <14%. It means these countries designed and implemented effective strategies for preventing and controlling NCDs despite their high mortality rate. We excluded incomplete texts, duplications, and dissertations (due to lack of access).
We used the NCDs country profile 2018 developed by WHO to find out the countries with the best policies, protocols, and measures. Importantly, these documents were used to track the progress of Member States toward achieving the global targets for NCDs to be reached by 2025. Three researchers independently extracted and created summary sheets in Microsoft Excel. The unobtainable data were recorded as missing data. One of these researchers compared the collected data after data extraction and made a single data sheet for analysis.
We followed the Preferred Reporting Items for Systematic review and Meta-Analysis (PRISMA) guidelines (29). The initial search resulted in 4,898 articles. We used EndNote X9 software to exclude duplications and irrelevant studies and organize the references. We removed 18 duplicated papers. After screening for relevant titles, we excluded 3,846 studies and selected 1,034 studies for abstract screening. We removed 779 articles after reviewing their abstracts. These studies did not include any strategies for preventing and controlling NCDs and their risk factors. We removed 141 additional articles after examining the full texts. Finally, we found 114 documents eligible for inclusion in this scoping review. We manually searched the reference lists of the 114 articles and added eight studies to eligible articles. Figure 1 demonstrates the search process.
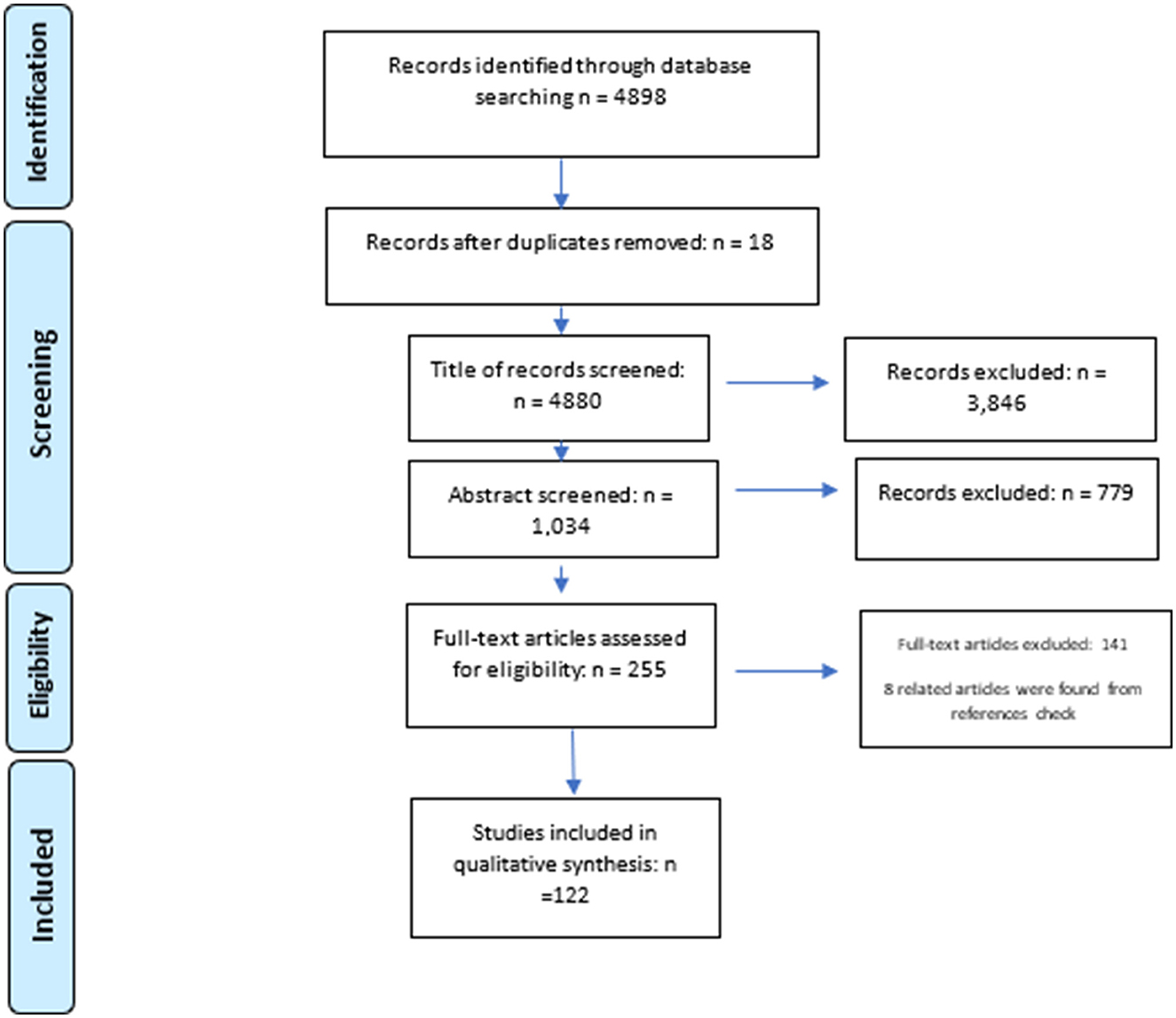
Figure 1. PRISMA flow diagram depicting the study selection process.
The researchers designed a data-gathering form based on the study's objective. They used the content analysis method for data analysis via MaxQDA software. Content analysis as a research method is a systematic and objective means of describing and exploring phenomena. It is also known as a method of analyzing documents. Through content analysis, we can categorize the words and phrases into similar groups which have similar meanings and generate ideas (30).
We used the major NCDs and their risk factors as themes (cardiovascular diseases, cancer, diabetes, hypertension, tobacco use, unhealthy diets, harmful use of alcohol, and physical inactivity/obesity). We also generated a separate theme for studies that target multiple of these diseases and risk factors as integrated strategies, as most of the strategic plans of these countries addressed most/all the NCDs and their risk factors, but the published papers usually addressed only one or two of these diseases or their risk factors. Then, we extracted the strategies from the studies and categorized them under related themes.
3. Results
In this section, we present the characteristics of the identified studies and elaborate on the strategies under nine themes including tobacco use, healthy diet, harmful use of alcohol, physical inactivity/obesity, heart diseases, cancers, diabetes mellitus, hypertension, and integrated strategies, which address multiple of the mentioned factors.
3.1. Main characteristics of reviewed articles/documents
A total of 122 articles/documents have been identified that were developed during 1984–2021. Almost 60% of the studies have been conducted after 2017 (Figure 2).

Figure 2. Frequency distribution of published documents on NCDs strategy per year.
Canada (26.4%), Korea (19.8%), and the United Kingdom (19%) have the most publications on the control and prevention of NCDs among the countries included in the study (Figure 3).
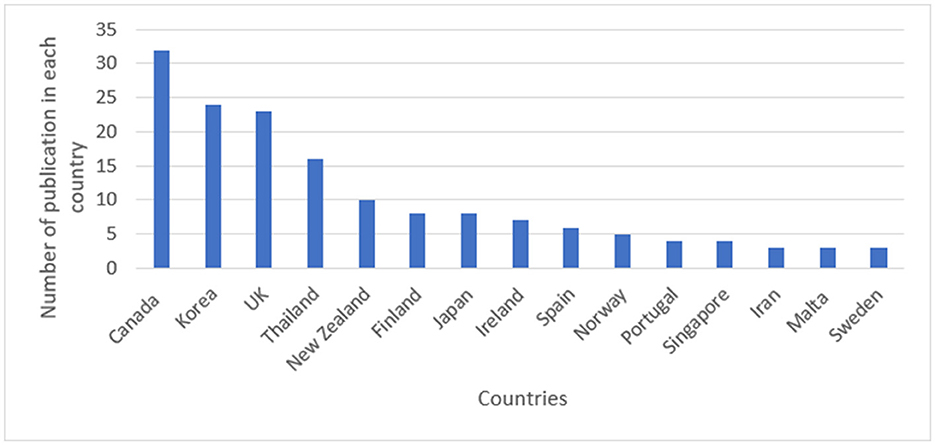
Figure 3. Frequency distribution of published documents on NCDs strategy per country.
Approximately 79.3% of the studies were original articles. The remaining (30.7%) were document reviews, action plans, and review articles. As Figures 4, 5 show, most of the studies were focused on how to control and prevent diabetes, heart disease, and tobacco use.
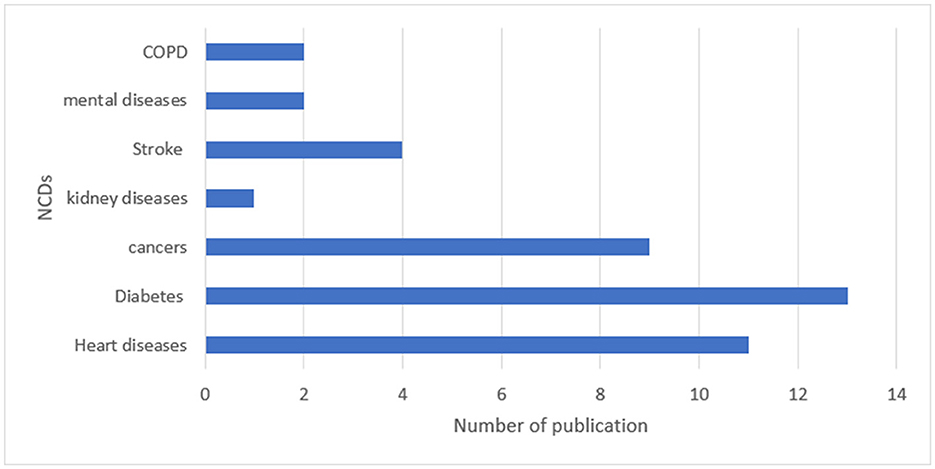
Figure 4. Frequency distribution of publications focused on NCDs.
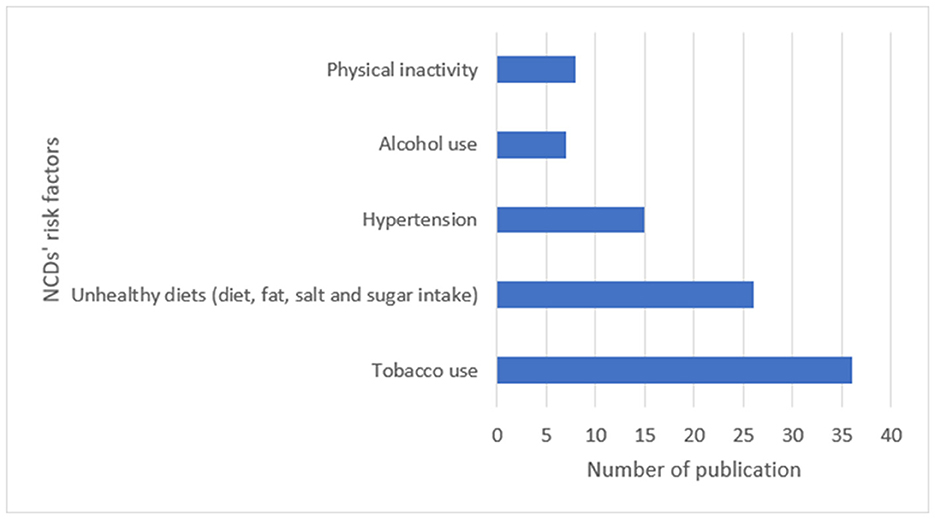
Figure 5. Frequency distribution of publications focused on risk factors.
3.2. Strategies to prevent and control NCDs
We identified 35 strategies in this study, which we categorized under nine themes presented in the Method section. The number of strategies under each theme is presented in Table 2.
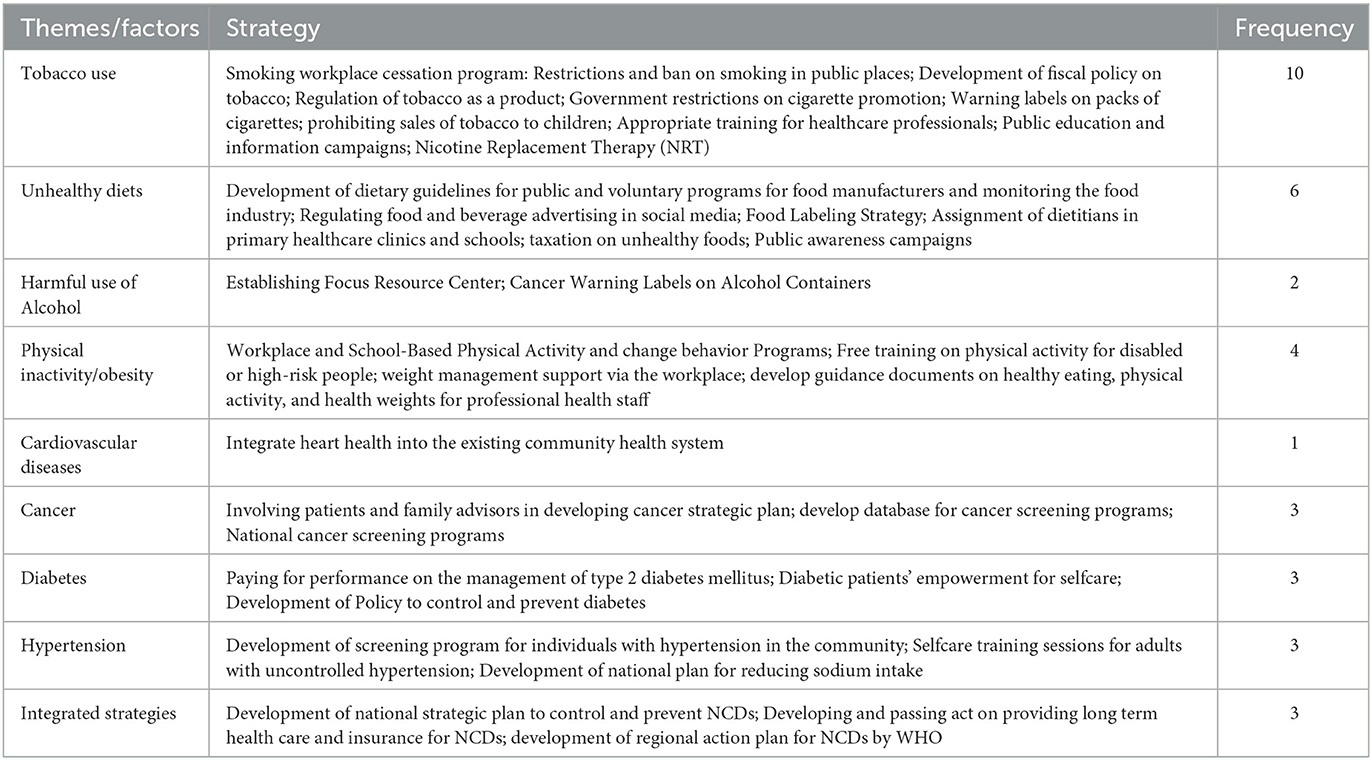
Table 2. Population-based strategies for the prevention and control of NCDs.
3.2.1. Tobacco use
Smoking cessation program is the most frequent strategy applied by most countries. Workplace smoking cessation program was applied in Korea, Thailand, and the United Kingdom. A workplace smoking cessation program in Korea effectively encouraged autonomous regulation and competence for workers. This program was based on self-determination theory using individual counseling and tailored text messaging for 12 weeks (31). Restriction and ban on smoking in public places are another strategy applied by some governments and was effective in declining smoking prevalence in federal jurisdictions of Canada (32–34), the United Kingdom (35, 36), Thailand (37, 38), and Korea (39, 40). However, a study in the United Kingdom showed low levels of clinician support for recommending e-cigarettes to patients with cancer (41).
Fiscal policies are used to reduce the demand for tobacco use by increasing cigarette prices and taxes on tobacco in many countries including Thailand, Malta, Portugal, Sweden, Ireland, Canada, and the United Kingdom (36, 41–43). Korean government imposed a 10% value-added and waste disposal tax of 7 Won on 20 cigarettes during 1994–2014. This policy led to more cutbacks on smoking among lower-income smokers than among higher-income smokers in Korea (40).
Ban on all tobacco advertisements or restriction on tobacco point of sale is the demand reduction measures applied in many countries (32, 36, 43–46). Canada passed the Smoke-Free Ontario Act (SFOA) in 2006 by which restrictions were applied on tobacco point of sale in any place. The government aimed to restrict youth access and smoking in enclosed workplaces and public places (35). Japan also banned tobacco advertisements on broadcast media on TV commercials aired between 5 am and 10:54 pm based on its tobacco policies in 2005 (45). In the United Kingdom, a committee on advertising practice has produced guidelines that balance the protection of minors and the promotion of new low-risk products to consumers (46).
Warning labels on packs of cigarettes including text or graphic pictorial messages are used to decrease the prevalence of smoking in many countries. The United Kingdom also passed a regulation in 2009 to control label packaging according to the chemical of cigarettes (47). This country also passed another tobacco plain packaging legislation to reduce the brand equity and diminish the industry's long industry (48). An experimental study examined the effect of warning labels on cigarette packs in Korea between 2010 and 2012. The findings of that study support the efficacy of graphic pictorial warnings across diverse geographical and cultural contexts and support sharing health warning images across jurisdictions (49). New Zealand and Korea also used graphic pictorial warning labels (PWLs) on cigarette packs to increase non-smoking intention among adolescents (49–51). Japan also included a warning label “Be careful not to smoke too much, as smoking may be harmful to your health” on the pack of cigarettes in its tobacco policies (46).
The United Kingdom used legislation to prohibit tobacco sales to children (52) or set a committee to develop guidelines that balance the protection of minors and the promotion of new low-risk products to consumers (53). High school students were trained in a 1-h orientation program about tobacco use and the challenges of its use in a field randomized controlled trial in Iran. In addition, measures were taken to ban tobacco sales in the proximity of schools and sale to high school students (52). As part of a nationwide school-based smoking prevention program, Korea conducted a study among students aged 10–18 years in 2020. The study highlights how the school environment is associated with adolescent smoking behavior, and the effects programs and norms differ with gender. The findings of this study suggested the need to develop strategies to enhance school-based tobacco control programs and the school norm considering gender differences (54). Korea then designed a nationwide school-based smoking prevention program for students from grades 1 to 12 in 2021. This program aims to achieve a tobacco-free generation in Korea (55). In addition, through a randomized control trial study, 160 smokers from the 10th to 12th grades in Korea were included in a teen tobacco use cessation program in 2019 (56).
Providing appropriate training for health workers was another strategy for controlling tobacco use. Department of family medicine in the college of medicine at Korea Hanyang university provided a 1-year program for fourth year medical students in which they attended a role play or standardized patient's module of smoking- cessation counseling training for medical students. As a result of the program, medical students were equipped with enough knowledge to deal with a smoker willing to quit (56). Public education and information campaigns and Nicotine Replacement Therapy (NRT) are other interventions used in the European Union (35).
3.2.2. Healthy diet
New Zealand developed guidelines that recommended a dietary pattern emphasizing a variety of nutritious and limiting energy-dense and nutrient-poor food products for the public (57). Some countries such as the United Kingdom, New Zealand, and Canada also designed voluntary programs for processed food manufacturers, retailers, and caterers to reduce salt intake in the general population (58, 59). Canada passed the Consumer Protection Act in 1980; and then it restricted the commercial marketing of unhealthy foods to children (60). A study in the United Kingdom assessed the adolescents' awareness of marketing for foods high in fat, salt, or sugar (HFSS), and the association between the past month's awareness and weekly HFSS food consumption. The authors found a causal relationship between marketing awareness and consumption and proposed to the United Kingdom government for further restrictions to reduce HFSS consumption (61). The government of Canada also tried to promote healthy diets and lifestyles in all child-directed activities (completely refrain from marketing products to children or to only market products that satisfy the CAI's Uniform Nutrition Criteria) (62, 63).
The front-of-pack labeling strategy was also reported in Canada and Portugal. Simplified nutrition information is an effective population-wide intervention to improve NCD outcomes. It leads to making the healthier and easier choice for consumers and encouraging manufacturers' reformulation of their food products toward offerings of higher nutritional quality (64, 65). A study in Canada shows the strength of using free sugar DV labeling to discourage the selection of products with excess free sugars (66). Boon et al. (67) reported that most Canadian consumers now use National Health Products to make informed consumer decision-making to choose healthy foods. A study in the United Kingdom showed that modest dietary improvements in the United Kingdom could avert approximately 12,000 CVD deaths annually and more substantial improvements could avert about 30,000 CVD deaths annually (68). Assignment of dietitians in primary healthcare clinics and schools is one of the strategies to promote a healthy diet in the community. Another study in New Zealand investigated the effectiveness of dietetic intervention in primary healthcare on health and wider economic outcomes. The study concluded that dietitians in primary healthcare can improve patients' health and quality of life. Increasing the number of dietitians working in primary healthcare has the potential to make quality nutrition care accessible and affordable for more New Zealanders (69). Face-to-face lifestyle counseling sessions were provided to the adult in the families in a study in European Countries during the first year of intervention; while during the second year, the intervention was implemented via personalized SMS messages. The program resulted in the improvement of certain lifestyle behaviors in parents from high-risk families (70). The Korea Institute of Child Care and Education designed a similar program in Korea. A 10-week nutrition intervention was performed by a team of nutrition professionals with the cooperation of 14 class teachers at the seven daycare centers and kindergartens in 2016. This program improved young children's eating behaviors and nutrition status (71). Taxation of sugary drinks and education and awareness of consumers, industry, and health professionals are other strategies suggested in some studies (59, 60, 62).
3.2.3. Harmful use of alcohol
Casswell et al. (72) in 2012 designed an instrument to assess the impact of alcohol control policies. He and his team then conducted the International Alcohol Control (IAC) study that assessed the impact of alcohol control policies on consumption and policy-related behaviors in New Zealand. The study contributed to the debate on appropriate policy responses to reduce alcohol-related harms (73). Canada established the Focus Resource Center from 2002 to 2008, which provided a wide range of services, including networking, training, consultation, and information dissemination, to 22 community programs throughout Ontario province. This intervention increased the capacity of health promoters through training, organizing, and collective efforts, and providing common services to control the harmful use of alcohol (74). Another initiative used in Canada is Cancer Warning Labels on Alcohol Containers. Placing cancer warnings on alcohol containers could make a pivotal difference in motivating both drinkers to consume less and regulators to introduce more effective policies to reduce the serious harms of alcohol consumption (75). A review study in 2017 found that screening and appropriate interventions for hazardous alcohol use and use disorders could lower blood pressure levels, but there is a lack and gap in implementing these measures in European primary healthcare. They provided some recommendations in this regard and proposed that implementing these recommendations should be in controlled settings with evaluation (76).
3.2.4. Physical inactivity/obesity
Many countries designed different interventions to promote physical activity and prevent obesity among the population. A 1-year badminton and table tennis program was designed in Korea for 120 high school students in 2018 (35 min/day, three times a week). School-based physical activity programs can positively affect adolescents' physical fitness which is expected to assist health and education professionals to plan or make decisions on strategies that can promote physical activities in schools (77). A cluster randomized controlled trial also targeted junior high school students in Thailand to modify their health beliefs toward obesity and physical activity. They first trained the students on obesity and its causes in children using cartoon animation, then they informed the students on the perceived benefit of the prevention of obesity, and finally, the students were trained on cues to action for the prevention of obesity. The researcher used a family-centered approach by visiting students' homes to stimulate awareness and change behavior based on family support (78).
Countries such as Canada, Iran, and Thailand provided free physical activity training for disabled or high-risk people. Thailand designed a lifestyle modification program for rural obese women for 16 weeks. It included nutritional counseling, health education, and exercise training, leading to a loss of weight of 10.2% from baseline (79). A weight reduction program was also designed in Thailand using Facebook in 2016. They posted exercise videos from an exercise expert over a Facebook private group and assessed the program via daily weight reporting and monthly personalized feedback. The result of the study proves that health education and support services through Facebook can be effectively used for weight reduction among students at a public university in Thailand (80). Iran also designed a randomized control trial including theory-based training intervention on physical activity and blood pressure in hypertensive patients for 1 year (81). Canada also provides financial support for disabled athletes nationally. This promoted physical activity and recreational sports through bilateral agreements with territories and provinces (82). In some countries such as the United Kingdom, organizations also provided weight management support via the workplace for their staff through a partnership scheme with Slimming World Organization for a 12-week duration. The program was especially effective for people with high BMIs (83, 84). In a loyalty scheme-based program in Ireland, rewards are provided to public sector employees to increase their physical activities (85). A scale-up and scale-out of gender-sensitized weight management and healthy living program in European countries such as Canada, New Zealand, and England recruited men aged 35–65 years who were at increased risk of future ill health because of their body size (BMI > 28 kg/m2). The participants in this program were provided a 12-week group of 90 min sessions in Football Fans in Training (FFIT) (86). Canada also provided guidance documents about healthy eating, physical activity, and healthy weights for professional staff employed by local health boards in 2010 (87) (Table 2).
3.2.5. Heart diseases
Heart Health Action Program was designed and implemented in Canada from 1990 to 1996 to integrate heart health into the existing community health system by the health promotion branch of the Ontario ministry of health (74). A study in the United Kingdom assessed the General Practitioners' (GPs) familiarity with and use of cardiovascular clinical prediction rules in 2014. Their target was a network of doctors in the United Kingdom with more than 238,000 members. They found that the GPs' knowledge and use of the CardioPulmonary Resuscitations (CPRs) technique changed substantially. They also recommended integrating CPRs into guidelines and practice software which might increase familiarity and use (88).
3.2.6. Cancers
Countries used different strategies to prevent and control cancer incidence among the population. Cancer Care Ontario developed its Cancer Plan IV in 2015–2019 while cancerous patients and family advisors were involved in planning. The engagement intended to ensure that the plan would be meaningful to patients and families and help to improve the quality of care and patient experience (88). Sweden and Finland developed a web-based application to provide access to a standardized, evidence-based database for Nordic Cancer screening. This database had performance and outcome indicators of cancer screening based on the up-to-date Nordic Cancer screening register data in 1980 which is used for quality assurance and improvement of cancer screening programs (89). The cervical cancer screening program was another strategy implemented in countries such as Korea, Thailand, and Norway (90, 91).
3.2.7. Diabetes mellitus
Ireland used a pay-for-performance system to manage type 2 diabetes mellitus. O'Connor et al. (92) showed substantial improvement in the process and quality of care in managing patients with type 2 diabetes mellitus in Ireland. Providing education to diabetic patients for self-management is also used in Korea and Thailand through face-to-face training sessions, text content, quizzes and video links, medication reminder, and emergency calls (93, 94). The Singapore Ministry of Health declared War on Diabetes (WoD) to rally a whole national effort to reduce the diabetes burden in the country in 2016. They developed a national policy to control and prevent diabetes. In 2021, a study showed that WoD policy generated a sense of unity and purpose across most policy actors. Policy actors were cognizant of the thrust of the policy and have begun to make shifts to align their interests with the government policy (95).
3.2.8. Hypertension
Self-care training sessions for adults with uncontrolled hypertension are a strategy used to control blood hypertension in Canada and Thailand. In total, 128 participants aged 35–74 years with hypertension received a weekly email newsletter regarding hypertension management in a user-and-expert-driven web-based hypertension program during 2012–2014 in Canada. This program allowed participants to choose their intervention goals such as self-care tips for exercise or a heart-healthy diet (96). Self-management programs were implemented for Thais with essential hypertension in 2009 and 2018–2019. The program included group discussions to assess knowledge and health beliefs regarding hypertension, sodium restriction strategies, developing a self-care behavior booklet, and coaching family caregivers concerning monitoring older adults with uncontrolled hypertension (97, 98). Japan used a screening program for the detection of hypertension through an annual health checkup of 30 years and older residents during 1963–1966. This intervention led to a substantial decline in the prevalence of severe hypertension and a decline in stroke incidence in the 1960s (99). Developing a national plan to reduce dietary sodium is another strategy used in Canada (100) (Table 2).
3.2.9. Integrated strategies
The identified integrated strategies are developing a national strategic plan for NCDs, developing and passing an act on providing long-term care and insurance, and developing a regional action plan for NCDs by international agencies. National strategic plans of Korea, Iran, Thailand, and Malta were reviewed in this study, designed for 6–10 years of implementation (101–105). Japan passed different acts to address the NCDs throughout the country including Health and medical service Act (1983), the long-term care insurance Act (1997), and the health promotion Act (2004) which all aimed at primary prevention as the main strategy for NCDs control in Japan (106). Some international agencies such as World Health Organization also developed a regional action plan for preventing and controlling non-communicable diseases in terms of intervention for population and individual levels for all member states (107). In a Chronic Diseases Self-Management Program (CDSMP) in Canada, patients aged between 18 and 80 years were enrolled. This standardized program proposed weekly 2.5 h meetings of 10–12 people for 6 weeks, facilitated by two peer leaders with chronic diseases. During the meetings, several issues are discussed: techniques to deal with problems such as frustration, fatigue, pain, and isolation; appropriate exercise for maintaining and improving strength, flexibility, and endurance; and appropriate use of medication and communicating effectively with family, friends, and health professionals (108) (Table 2).
4. Discussion
We conduct this study to identify strategies used for the prevention and control of non-communicable diseases in 15 countries (Canada, Finland, Iran, Ireland, Japan, Malta, New Zealand, Norway, Portugal, Republic of Korea, Singapore, Spain, Sweden, Thailand, and the United Kingdom). These countries had a percentage of death from NCDs higher than 70% and the probability of premature mortality from target NCDs <14%. It means that these countries designed and implemented effective strategies for preventing and controlling NCDs despite their high mortality rate. We explored the strategies for the four main risk factors of NCDs (tobacco use, unhealthy diets, physical inactivity, and harmful consumption of alcohol) and the four major non-communicable diseases (heart diseases, cancers, diabetes, and chronic obstructive pulmonary diseases) (14). There were more publications after 2017, the main reason for this could be including the non-communicable diseases in the Sustainable Development Agenda and assigning one target to these diseases (target 3.4), which has been followed by several publications, especially by WHO. Multi-sectoral and population-based preventive measures are advised in many literature studies including regulation, policy change, and market control toward NCDs prevention and control (14).
We identified 35 strategies in this study, among which the highest belongs to tobacco use (10 strategies) followed by unhealthy diet (6 strategies). We compared the identified strategies with the Best Buys intervention of WHO and proposed the cost-effective ones for Afghanistan that have not been addressed in the Afghanistan NCD strategy. Afghanistan Ministry of Public Health has only endorsed one strategy for NCDs for the duration of 2015–2020 (Afghanistan MoPH-NCD strategy) and we use it as a reference in this study (12).
Several articles have shown that tobacco use and an unhealthy diet are linked to increasing NCDs (109–112). Tobacco use causes at least 16 different types of cancer. Thakur Jha et al. showed that smoking would lead to around 930,000 adult deaths in India alone in 2011. Reducing tobacco use is one of the best strategies for preventing NCDs, along with reducing the harmful use of alcohol and promoting a healthy diet and physical activity (113). Tobacco control has an important effect on NCDs burden, and the related programs have high feasibility toward the whole population with the most benefit for the poor resulting in reducing inequities. Therefore, the priority of all countries in the world should be achieving the global goal by 2040 of a world essentially free from tobacco where <5% of the population uses tobacco (14). Different strategies were introduced in various articles to control tobacco use (Table 2), of which, the smoking cessation program; fiscal policy; and restriction and ban on smoking in public places were the most common ones. In the Afghanistan MoPH NCD strategy, there was no intervention addressing smoking in the general population. Comparing our identified strategies with the “best buys interventions,” the cost-effective interventions that Afghanistan can use to control and prevent smoking are restrictions and ban on smoking in public places, development of fiscal policy on tobacco, regulation of tobacco as a product if Afghanistan produces tobacco, increasing government restrictions on cigarette promotion, use warning labels on packs of cigarettes, prohibiting sales of tobacco to children, and conducting public education and information campaigns. A study using the data from the 2015 Afghanistan Demographic and Health Survey of about 40,000 participants showed that smoking cigarettes was the most prevalent form of tobacco use among men (21.9%, 95% CI 21.2–22.7), and the prevalence rates were lower for women. The study also showed an inverse association between education and tobacco use and a positive association between occupation (agriculture and skilled and unskilled manual labor occupations) and smoking (114). Afghanistan MoPH introduced earmarked taxes for health in Afghanistan including the tax on tobacco, vehicle, and fuel (115). But the recommended strategies have not been implemented yet due to a lack of good coordination between different ministries including the Ministry of Finance, Ministry of Interior Affairs, and MoPH. However, due to non-coordinated activities, MPOWER policies led to the enforcement of smoke-free public places. In addition, the government promotes direct and indirect bans on tobacco advertising, but still, the country does not have a national anti-tobacco media campaign to alert the public about the dangers of tobacco. Health warning labels are also in the text-only form on tobacco product packaging (114). So, the most important interventions we recommend for Afghanistan are enforcing taxes on tobacco products, conducting media campaigns to alert the public about the tobacco dangers, and adding pictorial warning labels on the packaging of cigarettes.
According to WHO, one of the important risk factors for a range of chronic diseases is an unhealthy diet (116). An unhealthy diet is connected to four of the world's top 10 risk factors causing death (Hypertension, high blood glucose, overweight and obesity, and high cholesterol) (117). Hence, evidence-based nutrition interventions should be a global health priority (118). Several strategies and programs were discussed in the reviewed articles in this study. The most frequent stricter food policies include feasible reductions in saturated fats, industrial trans fats, salt consumption, restriction on commercial marketing of unhealthy foods to children, taxation of sugary drinks, Children's Food and Beverage Advertising Initiative, Nutrition Labeling Regulation, and Food marketing policies. There is no intervention in the Afghanistan NCD strategy for controlling unhealthy diets. Compared to “best buys interventions,” we recommend the development of dietary guidelines especially to reduce salt intake for public institutions such as hospitals, schools, workplaces, and nursing homes; regulating food and beverage advertising in social media; taxation on unhealthy foods especially sweetened beverages; a public awareness campaign about healthy diet focusing on reducing salt intake through a behavior change communication and mass media campaign; and food labeling strategy by a focus on reducing salt intake through the implementation of front-of-pack labeling. A review study was conducted for mapping the current nutrition policies and capacity development initiatives in Afghanistan. The study found that limited policy provisions are available to address nutrition issues due to the rising burden of non-communicable diseases, urbanization, and changing dietary patterns (119). So, the provision of policies to address the mentioned challenges in Afghanistan should be mandatory for the Ministry of Public Health.
Afghanistan is one of the countries in the world where alcohol drinking at any age is illegal for all citizens. If the locals violate the law, they will be punished under Sharia law. The total alcohol consumption per capita is 0.2 liters of pure alcohol in 2018 in Afghanistan for people 15+ years of age, compared to the average of 6.2 liters worldwide (120). So, considering the current Afghanistan context for alcohol use, we do not provide any recommendations here.
A national survey in 2018 in Afghanistan showed that the prevalence of overweight is 25.5% and the prevalence of obesity is 17.2% in Afghanistan, and these are positively associated with ages 30–44 and 45–69 years, hypertension, and type 2 diabetes. High physical activity was negatively associated with overweight/obesity in Afghanistan (121). In this review, we highlighted four strategies to promote physical activity and control overweight/obesity, but comparing with “the best buys interventions,” we recommend the following strategies to be implemented in Afghanistan: implement a community-wide mass media campaign to educate and raise awareness to the public about physical activity aimed at supporting behavioral change of physical activity levels. In addition, integrating physical activity counseling and referral into primary healthcare services, developing guidance documents on healthy eating, physical activity, and health weights for professional health staff, and workplace and school-based physical activity programs are other implementable interventions in Afghanistan.
A study conducted in northern Afghanistan in 2018 showed that the prevalence of coronary artery disease among patients was 17.4%, with female patients having a higher prevalence rate than male patients (20.1 vs. 14.9%, P = 0.02) (122). In addition, a systematic review and meta-analysis study in 2021 showed that the prevalence of diabetes in Afghanistan is 12.13% and the main risk factors include increasing age, obesity, and hypertension (123). While there are some services and medicines in BPHS to control and treat heart diseases and diabetes, no intervention was mentioned in the AFG NCD strategy to control and treat these diseases. So, comparing with “the best buys intervention,” we recommend development guidelines for self-care especially for managing heart diseases and diabetes, integrating heart health into the existing community health system and providing consultation to individuals who have had a heart attack or stroke and to persons with moderate to high risk (≥20%) of a fatal and non-fatal cardiovascular event in the next 10 years.
The Afghanistan Mortality Survey in 2010 shows that 8.3% of female and 7.3% of male patients die due to cancer in Afghanistan. However, the only specific intervention to address cancer in the Afghanistan NCD strategy is the establishment of the National Cancer Control Program lacking any specific detailed intervention. Considering our findings in this review, we recommend to the Afghanistan MoPH that despite establishing a national cancer screening program especially cervical cancer among women, they can start the vaccination against human papillomavirus (2 doses) for girls aged 9–13 years.
The fourth objective of WHO's Global Action Plan for Prevention and Control of NCDs 2013–2020 is “strengthen and orient health systems to address the prevention and control of non-communicable diseases and the underlying social determinants through people-centered primary health care and universal coverage.” The enabling actions to reach this objective are focusing on promoting a referral system, viable health financing mechanism, enhancing preventive care at the primary level, improving the availability of affordable basic techniques and essential medicines, training the health workforce, and strengthening the capacity of the health system, particularly in the primary care level, and developing and implementing a palliative care policy (124). Considering the findings of this review, we recommend conducting a situation analysis of the NCDs management system in Afghanistan and developing a national NCDs strategy based on the six building blocks of WHO.
A limitation of our study was identifying countries with a similar context to Afghanistan which has low premature mortality rates. Most low-income countries face a dual burden of diseases (communicable and non-communicable) and have a high rate of premature mortality, which means they are not successful in controlling and preventing NCDs. So, we had to select high- and middle-income countries to explore the strategies.
5. Conclusion
This study highlighted the strategies to control and prevent non-communicable diseases which have already been implemented in countries with low levels of premature mortality rates. The findings of this review can be used by the Afghanistan Ministry of Public Health, the WHO Afghanistan country office, and other involved stakeholders to design and implement strategies to control and prevent NCDs in Afghanistan. The political declaration of the high-level meeting of the general assembly on the prevention and control of non-communicable diseases in 2011 highlighted the need for a whole-of-government and a whole-of-society response. It acknowledged the importance and need for a multisectoral approach and including health at all government levels to address NCDs risk factors and consider determinants of health in all programs (125). So, international organizations such as the World Health Organization, United Nations Agencies, the World Bank, and other involved communities should invest in strengthening good health governance in Afghanistan. The Afghan government should focus and invest in promoting health literacy among the public and self-care toward controlling and preventing NCDs. The proposed interventions and strategies in this study are cross-sectional approaches and need good collaboration between multiple sectors.
Author contributions
NN, MA, AM, and PI designed the research, conducted it, and wrote the paper. NN, MA, and PI extracted the data. AM had primary responsibility for the final content. NS reviewed the article and provided technical input to enrich the paper and also edited the language of the manuscript. All authors read and approved the final manuscript.
Funding
Researchers conducted this study with research funding from the Tehran University of Medical Science.
Acknowledgments
We thank Dr. Saber Perdes for his contribution to the English editing of the manuscript.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2023.982416/full#supplementary-material
Abbreviations
NCDs, non-communicable diseases; GHD, global health diplomacy; UN, United Nations; WHO, World Health Organization; LMIC, low- and middle-income countries; LIC, low-income countries; NGOs, non-governmental organizations; APEC, Asia-Pacific economic cooperation; FCTC, framework convention on tobacco control; NCDA, non-communicable diseases alliance; NCSP, national cancer screening program; SDGs, sustainable development goals; NCSP, national screening programs.
References
1. Allotey P, Reidpath DD, Yasin S, Chan CK, Aikins AD. Rethinking health-care systems: a focus on chronicity. Lancet. (2011) 377:450–1. doi: 10.1016/S0140-6736(10)61856-9
2. Institute for Health Metrics Evaluation. GBD. Seattle: Institute for Health Metrics and Evaluation (2019). Available online at: https://vizhub.healthdata.org/gbd-compare/ (accessed January 20, 2022).
3. World Health Organization. Non-Communicable Diseases Progress Monitor. Geneva: World Health Organization (2020). Available online at: https://www.who.int/publications/i/item/9789240000490 (accessed October 13, 2022).
4. Boutayeb A, Boutayeb S. The burden of non-communicable diseases in developing countries. Int J Equity Health. (2005) 4:2. doi: 10.1186/1475-9276-4-2
5. The World Bank. Maternal Mortality Ratio (Modeled Estimate, Per 100,000 Live Births). Washington, DC: The World Bank (2022). Available online at: https://data.worldbank.org/indicator/SH.STA.MMRT (accessed August 27, 2022).
6. United Nation Development Program. Human Development Report 2016. New York, NY: United Nation Development Program (2016). Available online at: https://hdr.undp.org/sites/default/files/HDR2016_EN_Overview_Web.pdf (accessed January 15, 2022).
7. Afghanistan Central Statistics Organization. Afghanistan Living Conditions Survey 2016–2017. Highlights Report. Kabul: Afghanistan Central Statistics Organization (2018). Available online at: https://www.adsp.ngo/wp-content/uploads/2018/12/PS-24_AFGHANISTAN-LIVING-CONDITIONS-SURVEY-2016-2017.pdf (accessed January 20, 2022).
8. World Economics. Afghanistan Population. Geneva: World Economics (2022). Available online at: https://www.worldeconomics.com/Demographics/Median-Age/Afghanistan.aspx (accessed December 11, 2022).
9. Afghanistan Ministry of Public Health. The Essential Package of Hospital Services for Afghanistan. Kabul: Afghanistan Ministry of Public Health (2005). Available online at: http://lyon-kaboul.univ-lyon1.fr/politique_de_sante_en_afghanistan/rapports/EPHS%20v10%20Mar%202005.pdf (accessed October 13, 2022).
10. Afghanistan Ministry of Public Health. The Afghanistan Non-Communicable Diseases and Injuries (NCDI) Poverty Commission Report. Kabul: Afghanistan Ministry of Public Health (2019). Available online at: https://static1.squarespace.com/static/55d4de6de4b011a1673a40a6/t/5d4b19724dae61000188ed7d/1565202805716/Afghanistan+NCDI+Poverty+Commission+Report_Final.pdf (accessed October 13, 2022).
11. Indian Institute for Health Management Research (IIHMR) Central Statistics Organization (CSO). Afghanistan Mortality Survey. New Delhi: IIHMR, CSO (2010).
12. Afghanistan Ministry of Public Health. National Strategy for Prevention and Control of Non-communicable Diseases (NCDs) 2015–2020. Kabul: Afghanistan Ministry of Public Health (2015). Available online at: https://extranet.who.int/ncdccs/Data/AFG_B3_National-NCD-Strategy-2015-2020-English25122016124118927553325325.pdf (accessed January 02, 2022).
13. Afghanistan Ministry of Public Health. Afghanistan National health Accounts. Kabul: Afghanistan Ministry of Public Health (2019). Available online at: https://moph.gov.af/sites/default/files/2021-12/Afghanistan%20National%20Health%20Accounts%20with%20Disease%20Account%20%2C2019.pdf (accessed January 02, 2022).
14. Beaglehole R, Bonita R, Alleyne G, Horton R, Li L, Lincoln P, et al. UN high-level meeting on non-communicable diseases: addressing four questions. Lancet. (2011) 378:449–55. doi: 10.1016/S0140-6736(11)60879-9
15. World Health Organization. Package of Essential Non-Communicable (PEN) Disease Interventions for Primary Health Care in Low-Resource Settings. Geneva: World Health Organization (2010). Available online at: http://apps.who.int/iris/bitstream/handle/10665/44260/9789241598996_eng.pdf;jsessionid=2F82F6F4BA98D399A9E4E4908E4F409D?sequence=1 (accessed October 13, 2022).
16. Alleyne G, Stuckler D, Alwan, A. The hope and the promise of the UN Resolution on non-communicable diseases. Global Health. (2010) 6:15. doi: 10.1186/1744-8603-6-15
17. United Nations General Assembly. Political Declaration of the High-Level Meeting of the General Assembly on the Prevention Control of Non-Communicable Diseases. New York, NY: United Nations General Assembly (2011), 1–13. Available online at: https://digitallibrary.un.org/record/710899?ln=en (accessed October 13, 2022).
18. Afshari M, Ahmadi Teymourlouy A, Asadi-Lari M, Maleki M. Global Health diplomacy for non-communicable diseases prevention and control: a systematic review. Global Health. (2020) 16:41. doi: 10.1186/s12992-020-00572-5
19. The World Bank. Life Expectancy at Birth. New York, NY: The World Bank (2022). Available online at: https://data.worldbank.org/indicator/SP.DYN.LE00.IN (accessed January 20, 2022).
20. Halpin HA, Morales-Suárez-Varela MM, Martin-Moreno JM. Chronic disease prevention and the new public health. Public Health Rev. (2010) 32:120–54. doi: 10.1007/BF03391595
21. Bloom DE, Cafiero ET, Jané-Llopis E, Abrahams-Gessel S, Bloom LR, Fathima S, et al. The Global Economic Burden of Non-communicable Diseases. Geneva: World Economic Forum (2011).
22. World Health Organization Regional Office for Europe. Country Experiences in Integrated Policy Development for the Prevention and Control of Non-Communicable Diseases. Geneva: World Health Organization (2015). Available online at: https://www.euro.who.int/__data/assets/pdf_file/0003/282936/Country-experiences-integrated-policy-development-prevention-control-NCDs.pdf (accessed October 13, 2022).
23. World Health Organization. Global Status Report on Non-Communicable Diseases. Geneva: World Health Organization (2014). Available online at: https://apps.who.int/iris/bitstream/handle/10665/148114/9789241564854_eng.pdf (accessed October 13, 2022).
24. World Health Organization. Non-Communicable Diseases Country Profiles. Geneva: World Health Organization (2018). Available online at: https://apps.who.int/iris/handle/10665/274512 (accessed October 13, 2022).
25. Levac D, Colquhoun H, O'Brien KK. Scoping studies: advancing the methodology. Implement Sci. (2010) 5:69. doi: 10.1186/1748-5908-5-69
26. World Health Organization. “Best Buys” and Other Recommended Interventions for the Prevention and Control of Non-communicable Diseases: Tackling NCDs. Geneva: World Health Organization (2017). Available online at: https://apps.who.int/iris/handle/10665/259232 (accessed October 13, 2022).
27. Bussiek P-BV, De Poli C, Bevan G. A scoping review protocol to map the evidence on interventions to prevent overweight and obesity in children. BMJ Open. (2018) 8:e019311. doi: 10.1136/bmjopen-2017-019311
28. Arksey H, O'Malley L. Scoping studies: towards a methodological framework. Int J Soc Res Methodol. (2005) 8:19–32. doi: 10.1080/1364557032000119616
29. Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. (2009) 6:148. doi: 10.1371/journal.pmed.1000097
30. Elo S, Kyngas H. The qualitative content analysis process. J Adv Nurs. (2007) 62:107–15. doi: 10.1111/j.1365-2648.2007.04569.x
31. Lim JH, Ha Y. Effectiveness of a workplace smoking cessation program based on self-determination theory using individual counseling and tailored text messaging: a pilot study. Asian Nurs Res. (2019) 13:53–60. doi: 10.1016/j.anr.2019.01.004
32. Givel M. A comparison of the impact of US and Canadian cigarette pack warning label requirements on tobacco industry profitability and the public health. Health Policy. (2007) 83:343–52. doi: 10.1016/j.healthpol.2006.12.003
33. Jolemore S, Steeves D. A capital approach: tobacco treatment and cessation within Nova Scotia's Capital Health District. Healthcare Quart. (2006) 9:66–70. doi: 10.12927/hcq..18230
34. Dubray JM, Schwartz RM, Garcia JM, Bondy SJ, Victor JC. Vendor compliance with Ontario's tobacco of sale legislation. Can J Public Health. (2009) 100:109–12. doi: 10.1007/BF03405517
35. Clancy L. Progress in tobacco control. Health Policy. (2009) 91(Suppl. 1):S3–14. doi: 10.1016/S0168-8510(09)70003-X
37. Chalermrueangrong J, Preechawong S. Effect of the motivation program to quit smoking in Royal Thai Air Force officers' with non-communicable diseases risks. J Health Res. (2019) 33:416–24. doi: 10.1108/JHR-11-2018-0143
38. Junnual N, Sota C, Chaikoolvatana A. Effectiveness of a smoking cessation program on self-esteem, attitude, perception, and practice regarding control over smoking among male high school. J Health Res. (2019) 33:366–74. doi: 10.1108/JHR-05-2018-0016
39. Kang H, Cho SI. Cohort effects of tobacco control policy: evidence to support a tobacco-free norm through smoke-free policy. Tob Control. (2020) 29:96–102. doi: 10.1136/tobaccocontrol-2018-054536
40. Choi SE. Are lower income smokers more price sensetive?: the evidence from Korean cigarette tax increase. Tob Control. (2016) 25:141–6. doi: 10.1136/tobaccocontrol-2014-051680
41. Brett J, Davies EL, Matley F, Aveyard P, Wells M, Foxcroft D, et al. Electronic cigarettes as a smoking cessation aid for patients with cancer: beliefs and behaviours of clinicians in the UK. BMJ Open. (2020) 10:e037637. doi: 10.1136/bmjopen-2020-037637
42. Lidón-Moyano C, Sampedro-Vida M, Matilla-Santander N, Martín-Sánchez JC, González-Marrón A, Bunch K, et al. Attitudes towards tobacco product regulations and their relationship with the tobacco control policies. Prevent Med. (2018) 111:67–72. doi: 10.1016/j.ypmed.2018.02.019
43. Charoenca N, Kungskulniti N, Sritabutra D, Pitayarangsarit S, Hamann SL. Using an assessment tool to further tobacco control accomplishment in Thailand. Tobacco Use Insights. (2018) 11:1–5. doi: 10.1177/1179173X18759945
44. Brown R, Van Godwin J, Page N, Bauld L, McKell J, Hallingberg B, et al. Implementation of e-cigarette regulation through the EU Tobacco Products Directive (2016) in Wales, Scotland and England from the perspectives of stakeholders involved in policy introduction and enforcement. Tobacco Prevent Cessation. (2021) 7:144. doi: 10.18332/tpc/134370
45. Asukai Y, Torii Y, Chikamoto Y. Tobacco control: recent movements in Japan. Am J Health Promot. (2005) 19:260–7. doi: 10.4278/0890-1171-19.3s.260
46. Berridge V, Hall W, Taylor S, Gartner C, Morphett K, A. first pass, using pre-history and contemporary history, at understanding why Australia and England have such different policies toward electronic nicotine delivery systems, 1970s-c, 2018. Addiction. (2021) 116:2577–85. doi: 10.1111/add.15391
47. Buonocore F, Gomes AC, Nabhani-Gebara S, Barton SJ, Calabrese G. Labelling of electronic cigarettes: regulations and current practice. Tob Control. (2017) 26:46–52. doi: 10.1136/tobaccocontrol-2015-052683
48. Pley C, Heijden MR, Tulinius C. A health professional's guide to the intersection of public health with intellectual property rights in trade and investment: the case of tobacco plain packaging. J Public Health Policy. (2019) 41:52–62. doi: 10.1057/s41271-019-00195-0
49. Hammond D, Reid JL, Driezen P, Thrasher JF, Gupta PC, Nargis N, et al. Are the same health warnings effective across different countries? An experimental study in seven countries. Nicotine Tob Res. (2019) 21:887–95. doi: 10.1093/ntr/nty248
50. Hoek J, Wilson N, Allen M, Edwards R, Thomson G, Li J. Lessons from New Zealand's introduction of pictorial health warnings on tobacco packaging. Bull World Health Org. (2010) 88:861–6. doi: 10.2471/BLT.10.076695
51. Hwang JH, Park SW. Harm perception in response to pictorial warning labels predict higher non-smoking intention among Korean adolescents. Int J Environ Res Public Health. (2021) 18:1404. doi: 10.3390/ijerph18041404
52. Khayyati F, Jafarabadi MA, Lotfizadeh M, Karimi A, Rahmani K. Effectiveness of a community and school-based intervention to control and prevent of tobacco use in adolescents: a field randomized controlled trial. Iran J Public Health. (2019) 48:187. doi: 10.18502/ijph.v48i1.812
53. Sandford A. Government action to reduce smoking. Respirology. (2003) 8:7–16. doi: 10.1046/j.1440-1843.2003.00436.x
54. Kim SY, Jang M, Yoo S, JeKarl J, Chung JY, Cho SI. School-based tobacco control and smoking in adolescents: Evidence from multilevel analyses. Int J Environ Res Public Health. (2020) 17:3422. doi: 10.3390/ijerph17103422
55. Kim S, Yoo S, Cho SI, Jung H, Yang Y. Experiences of the first-year implementation of a nationwide school-based smoking prevention program in Korea. Int J Environ Res Public Health. (2021) 18:3291. doi: 10.3390/ijerph18063291
56. Park KY, Park HK, Hwang HS. Group randomized trial of teaching tobacco-cessation counseling to senior medical students: a peer role play module vs. a standardized patient module. BMC Med Educ. (2019) 12:231. doi: 10.1186/s12909-019-1668-x
57. Lawrence MA, Pollard CM, Weeramanthri TS. Positioning food standards programmes to protect public health: current performance, future opportunities and necessary reforms. Public Health Nutr. (2019) 22:912–26. doi: 10.1017/S1368980018003786
58. Magnusson R, Reeve B. Food reformulation, responsive regulation, and “Regulatory Scaffolding”: strengthening performance of salt reduction programs in Australia and the United Kingdom. Nutrients. (2015) 7:5281–308. doi: 10.3390/nu7075221
59. Ministry of Health. Sodium Reduction Strategy for Canada. Washington, DC: Ministry of Health (2010). Available online at: https://www.canada.ca/en/health-canada/services/publications/food-nutrition/sodium-reduced-targets-2020-2025.html (accessed November 20, 2022).
60. Vergeer L, Vanderlee L, Potvin Kent M, Mulligan C, L'Abbé MR. The effectiveness of voluntary policies and commitments in restricting unhealthy food marketing to Canadian children on food company websites. Appl Physiol Nutr Metab. (2019) 44:74–82. doi: 10.1139/apnm-2018-0528
61. Critchlow N, Bauld L, Thomas C, Hooper L, Vohra J. Awareness of marketing for high fat, salt or sugar foods, and the association with higher weekly consumption among adolescents: a rejoinder to the UK government's consultations on marketing regulation. Public Health Nutr. (2020) 23:2637–46. doi: 10.1017/S1368980020000075
62. Bhawra J, Reid JL, White CM, Vanderlee L, Raine K, Hammond D. Are young Canadians supportive of proposed nutrition policies and regulations? An overview of policy support and the impact of socio-demographic factors on public opinion. Can J Public Health. (2018) 109:498–505. doi: 10.17269/s41997-018-0066-1
63. Kent MP, Dubois L, Wanless A. Food marketing on children's television in two different policy environments. Int J Pediat Obesity. (2011) 6:e433–441. doi: 10.3109/17477166.2010.526222
64. Labonté ME, Emrich TE, Scarborough P, Rayner M, L'Abbé MR. Traffic light labelling could prevent mortality from non-communicable diseases in Canada: a scenario modelling study. PLoS ONE. (2019) 14:e0226975. doi: 10.1371/journal.pone.0226975
65. Nogueira PJ, Nunes AM, Graça P, Lopes C, Miraldo M, Breda J. Modelling impacts of food industry co-regulation on non-communicable disease mortality, Portugal. Bull World Health Org. (2019) 97:450. doi: 10.2471/BLT.18.220566
66. Bernstein JT, Labonté MÈ, Franco-Arellano B, Schermel A, L'Abbé MR. A free sugars daily value (DV) identifies more “less healthy” prepackaged foods and beverages than a total sugar DV. Prevent Med. (2018) 109:98–105. doi: 10.1016/j.ypmed.2017.12.031
67. Boon HS, Kachan N. Natural health product labels: is more information always better? Patient Educ Counsel. (2007) 68:193–9. doi: 10.1016/j.pec.2007.06.005
68. O'Flaherty M, Flores-Mateo G, Nnoaham K, Lloyd-Williams F, Capewell S. Potential cardiovascular mortality reductions with stricter food policies in the United Kingdom of Great Britain and Northern Ireland. Bull World Health Org. (2012) 90:522–31. doi: 10.2471/BLT.11.092643
69. Howatson A, Wall C, Turner-Benny P. The contribution of dietitians to the primary health care workforce. J Prim Health Care. (2015) 7:324–32. doi: 10.1071/HC15324
70. Manios Y, Lambrinou CP, Mavrogianni C, Cardon G, Lindström J, Iotova V, et al. Lifestyle changes observed among adults participating in a family-and community-based intervention for diabetes prevention in Europe: the 1st year results of the feel4diabetes-study. Nutrients. (2020) 12:1949. doi: 10.3390/nu12071949
71. Kim J, Kim G, Park J, Wang Y, Lim H. Effectiveness of teacher-led nutritional lessons in altering dietary habits and nutritional status in preschool children: adoption of a NASA mission X-based program. Nutrients. (2019) 11:1590. doi: 10.3390/nu11071590
72. Casswell S, Meier P, MacKintosh AM, Brown A, Hastings G, Thamarangsi T, et al. The international alcohol control (IAC) study—evaluating the impact of alcohol policies. Alcohol Clin Exp Res. (2012) 36:1462–7. doi: 10.1111/j.1530-0277.2012.01738.x
73. Casswell S, Huckle T, Wall M, Yeh LC. International alcohol control study: pricing data and hours of purchase predict heavier drinking. Alcohol Clin Exp Res. (2014) 38:1425–31. doi: 10.1111/acer.12359
74. Giesbrecht N. Community-based prevention of alcohol problems: addressing the challenges of increasing deregulation of alcohol. Substance Use Misuse. (2007) 42:1813–34. doi: 10.1080/10826080701530688
75. Stockwell T, Solomon R, O'Brien P, Vallance K, Hobin E. Cancer warning labels on alcohol containers: a consumer's right to know, a government's responsibility to inform, and an industry's power to thwart. J Stud Alcohol Drugs. (2020) 81:284–92. doi: 10.15288/jsad.2020.81.284
76. Rehm J, Anderson P, Prieto JA, Armstrong I, Aubin HJ, Bachmann M, et al. Towards new recommendations to reduce the burden of alcohol-induced hypertension in the European Union. BMC Med. (2017) 15:1–0. doi: 10.1186/s12916-017-0934-1
77. Lee EJ, So WY, Youn HS, Kim J. Effects of school-based physical activity programs on health-related physical fitness of korean adolescents: a preliminary study. Int J Environ Res Public Health. (2021) 18:2976. doi: 10.3390/ijerph18062976
78. Khumros W, Vorayingyong A, Suppapitiporn S, Rattananupong T, Lohsoonthorn V. Effectiveness of modified health belief model-based intervention to reduce body mass index for age in overweight junior high school students in Thailand. J Health Res. (2019) 33:162–72. doi: 10.1108/JHR-08-2018-0065
79. Thiabpho C, Changbumrung S, Soonthornworasiri N, Yoddumnern-Attig B, Thaboot P, Nissayan P, et al. Intensive lifestyle modification program on weight loss and metabolic syndrome risk reduction among obese women in rural areas of Thailand. J Health Res. (2018) 32:203–16. doi: 10.1108/JHR-05-2018-022
80. Pattanapongsa T, Jiamjarasrangsi W, Hanvoravongchai P, Pekthong D. Effectiveness of social media for weight reduction on overweight undergraduage students in Thailand. J Health Res. (2019) 34:90–9. doi: 10.1108/JHR-03-2019-0044
81. Motlagh Z, Hidarnia A, Kaveh MH, Kojuri J. Effect of theory-based training intervention on physical activity and blood pressure in hypertensive patients: a randomized control trial. Iran Red Crescent Med J. (2017) 19:e55610. doi: 10.5812/ircmj.55610
82. Hoekstra F, Roberts L, van Lindert C, Martin Ginis KA, van der Woude LHV, McColl MA. National approaches to promote sports and physical activity in adults with disabilities: examples from the Netherlands and Canada. Disabil Rehabil. (2019) 41:1217–26. doi: 10.1080/09638288.2017.1423402
83. Stubbs RJ, Brogelli DJ, Barber J, Pallister C, Whybrow S, Avery A, et al. Service evaluation of weight outcomes as a function of initial BMI in 34,271 adults referred to a primary care/commercial weight management partnership scheme. BMC Res Notes. (2013) 6:1–4. doi: 10.1186/1756-0500-6-161
84. Barber J, Hillier SE, Middleton G, Keegan R, Henderson H, Lavin J. Providing weight management via the workplace. Int J Workplace Health Manag. (2015) 8:230–43. doi: 10.1108/IJWHM-10-2014-0040
85. Hunter RF, Murray JM, Gough A, Tang J, Patterson CC, French DP, et al. Effectiveness, and cost-effectiveness of a loyalty scheme for physical activity behavior change maintenance: results from a cluster randomized controlled trial. Int J Behav Nutr Phys Act. (2018) 15:1–3. doi: 10.1186/s12966-018-0758-1
86. Hunt K, Wyke S, Bunn C, Donnachie C, Reid N, Gray CM. Scale-up and scale-out of a gender-sensitized weight management and healthy living program delivered to overweight men via professional sports clubs: the wider implementation of Football Fans in Training (FFIT). Int J Environ Res Public Health. (2020) 17:584. doi: 10.3390/ijerph17020584
87. Canada Ministry of Health Promotion. Healthy Eating, Physical Activity, and Health Weights. Guidance Document. Washington, DC: Canada Ministry of Health Promotion (2010). Available online at: http://www.health.gov.on.ca/en/pro/programs/publichealth/oph_standards/docs/mhp/HealthyEating-PhysicalActivity-HealthyWeights.pdf (accessed November 20, 2022).
88. Wheeler S, MacKay J, Moody L, D'Souza J, Gilbert J. Engaging patient and family advisors in health-care system planning: experiences and recommendations. J Patient Exp. (2020) 7:331–7. doi: 10.1177/2374373519840343
89. Partanen VM, Anttila A, Heinävaara S, Pankakoski M, Sarkeala T, Bzhalava Z, et al. NordScreen: an interactive tool for presenting cervical cancer screening indicators in the Nordic countries. Acta Oncol. (2019) 58:1199–204. doi: 10.1080/0284186X.2019.1615637
90. Aoki ES, Yin R, Li K, Bhatla N, Singhal S, Ocviyanti D, et al. National screening programs for cervical cancer in Asian countries. J Gynecol Oncol. (2020) 31:6617. doi: 10.3802/jgo.2020.31.e55
91. Nygard M, Daltveit AK, Thoresen SO, Nygard JF. Effect of an antepartum Pap smear on the coverage of a cervical cancer screening programme: a population-basedprospective study. BMC Health Serv Res. (2007) 7:10. doi: 10.1186/1472-6963-7-10
92. O'Connor R, O'Driscoll R, O'Doherty J, Hannigan A, O'Neill A, Teljeur C, et al. The effect of ‘paying for performance ‘on the management of type 2 diabetes mellitus: a cross-sectional observational study. BJGP Open. (2020) 4:7512. doi: 10.3399/bjgpopen20X101021
93. Riangkam C, Sriyuktasuth A, Pongthavornkamol K, Kusakunniran W, Sriwijitkamol A. Effects of a mobile health diabetes self-management program on HbA1C, self-management and patient satisfaction in adults with uncontrolled type 2 diabetes: a randomized controlled trial. J Health Res. (2020) 36:878–88. doi: 10.1108/JHR-02-2021-0126
94. Lee SK, Shin DH, Kim YH, Lee KS. Effect of diabetes education through pattern management on self-care and self-efficacy in patients with type 2 diabetes. Int J Environ Res Public Health. (2019) 16:3323. doi: 10.3390/ijerph16183323
95. Yong LM, Koe LW. War on Diabetes in Singapore: a policy analysis. Health Res Policy Syst. (2021) 19:1–0. doi: 10.1186/s12961-021-00678-1
96. Liu S, Brooks D, Thomas SG, Eysenbach G, Nolan RP. Effectiveness of user-and expert-driven web-based hypertension programs: an RCT. Am J Prevent Med. (2018) 54:576–83. doi: 10.1016/j.amepre.2018.01.009
97. Sukpattanasrikul S, Monkong S, Leelacharas S, Krairit O, Viwatwongkasem C. Comparison of hypertensive outcome after the implementation of self-management program for older adults with uncontrolled hypertension in Krabi, Thailand: a quasi-experimental study. J Health Res. (2021) 36:641–51. doi: 10.1108/JHR-12-2020-0626
98. Rujiwatthanakorn D, Panpakdee O, Malathum P, Tanomsup S. Effectiveness of a self-management program for Thais with essential hypertension. Pacific Rim Int J Nurs Res. (2011) 15:97–110.
99. Baba S, Eshak SE, Iso H. Successful reduction of blood pressure and stork risk in Japan. Global Health Leadership. (2018) 14:47–55. doi: 10.1007/978-3-319-95633-6_5
100. Campbell NR, Willis KJ, L'Abbe M, Strang R, Young E. Canadian initiatives to prevent hypertension by reducing dietary sodium. Nutrients. (2011) 3:756–64. doi: 10.3390/nu3080756
101. Ban JW, Perera R, Stevens R. GPs' familiarity with and use of cardiovascular clinical prediction rules: a UK survey study. BJGP Open. (2020) 4:1081. doi: 10.3399/bjgpopen20X101081
102. Malta Ministry for Health The The Elderly Community Care. A Strategy for the Prevention and Control of Non-Communicable Diseases in Malta. Washington, DC: Malta Ministry for Health, The Elderly and Community Care (2010). Available online at: https://deputyprimeminister.gov.mt/en/strategy-development-and-implementation-unit/Documents/Strategies_and_Policies/Noncommunicable_Disease_Control_Strategy_2010.pdf (accessed November 20, 2022).
103. Iran Iran Ministry of Public Health Iranian National Committee for NCDs Prevention Control. National Document for Prevention and Control of Non-Communicable Diseases and the Related Risk Factors in the Islamic Republic of Iran 2015–2025. Kabul: Iran Ministry of Public Health, Iranian National Committee for NCDs Prevention and Control (2015). Available online at: https://extranet.who.int/nutrition/gina/en/node/40358 (accessed November 20, 2022).
104. Thailand Ministry of Public Health. 5-Year National NCDs Prevention and Control Plan (2017–2021). Mueang Nonthaburi: Thailand Ministry of Public Health (2017). Available online at: https://www.who.int/docs/default-source/thailand/ncds/national-ncd-prevention-and-control-plan-2017-2021-eng.pdf (accessed November 20, 2022).
105. DPR Korea Ministry of Public Health. National Strategic Plan for the Prevention and Control of Non-Communicable Diseases in DPR Korea 2014–2020. Pyongyang: DPR Korea Ministry of Public Health (2014). Available online at: https://cdn.who.int/media/docs/default-source/searo/ncd/dprk-ncd-action-plan-2014-2020.pdf?sfvrsn=fb3364f8_2 (accessed November 20, 2022).
106. Wu F, Narimatsu H, Li X, Nakamura S, Sho R, Zhao G, et al. Non-communicable diseases control in China and Japan. Global Health. (2017) 13:8. doi: 10.1186/s12992-017-0315-8
107. WHO Regional Office for Europe. Action Plan for the Prevention Control of Non-Communicable Diseases in the WHO European Region 2016–2025. Geneva: WHO (2016). Available online at: https://apps.who.int/iris/handle/10665/341522 (accessed November 20, 2022).
108. Hudon C, Chouinard MC, Diadiou F, Bouliane D, Lambert M, Hudon É. The chronic disease self-management program: the experience of frequent users of health care services and peer leaders. Fam Pract. (2016) 33:167–71. doi: 10.1093/fampra/cmw007
109. Doan TT, Tan KW, Dickens BS, Lean YA, Yang Q, Cook AR. Evaluating smoking control policies in the e-cigarette era: a modelling study. Tob Control. (2020) 29:522–30. doi: 10.1136/tobaccocontrol-2019-054951
110. Bertoncello C, Cocchio S, Fonzo M, Bennici SE, Russo F, Putoto G. The potential of mobile health clinics in chronic disease prevention and health promotion in universal healthcare systems. An on-field experiment. Int J Equity Health. (2020) 19:1–9. doi: 10.1186/s12939-020-01174-8
111. O'Kane SM, Carlin A, Gallagher AM, Lahart IM, Jago R, Faulkner M, et al. study protocol for a clustered randomised controlled trial to evaluate the effectiveness of a peer-led school-based walking intervention on adolescent girls' physical activity: the Walking in ScHools (WISH) study. BMC Public Health. (2020) 20:1–2. doi: 10.1186/s12889-020-08600-0
112. Fernstrom MH, Reed KA, Rahavi EB, Dooher CC. Communication strategies to help reduce the prevalence of non-communicable diseases: proceedings from the inaugural IFIC Foundation Global Diet and Physical Activity Communications Summit. Nutr Rev. (2012) 70:301–10. doi: 10.1111/j.1753-4887.2012.00480.x
113. Thakur JS, Garg R, Narain JP, Menabde N. Tobacco use: a major risk factor for non-communicable diseases in South-East Asia region. Indian J Public Health. (2011) 55:155. doi: 10.4103/0019-557X.89943
114. Alemi Q, Stempel C, Montgomery S. Prevalence and social determinants of tobacco use in Afghanistan. Int Health. (2021) 13:3–12. doi: 10.1093/inthealth/ihaa010
115. Afghanistan Ministry of Public Health. Introducing Earmarked Taxes for Health in Afghanistan: Learning from Country Experiences. Kabul: Afghanistan Ministry of Public Health (2017).
116. WHO. Non-Communicable Diseases Risk Factors. Geneva: WHO (2022). Available online at: http://www.emro.who.int/noncommunicable-diseases/causes/index.html (accessed February 06, 2022).
117. World Heart Federation. Global Dietary Changes Threaten Health. Geneva: World Heart Federation (2021). Available online at: https://world-heart-federation.org/wpcontent/uploads/2021/05/Factsheet_Unhealthy_diet.pdf (accessed November 25, 2021).
118. Billingsley HE, Carbone S, Lavie CJ. Dietary fats and chronic non-communicable diseases. Nutrients. (2018) 10:1385. doi: 10.3390/nu10101385
119. Sharma J, Ludin H, Chauhan M, Zodpey S. Public health nutrition in Afghanistan-policies, strategies and capacity-building: current scenario and initiatives. East Mediterr Health J. (2021) 27:728–37. doi: 10.26719/emhj.21.043
120. The World Bank. Total Alcohol Consumption Per Capita (Liters of Pure Alcohol, Projected Estimates, 15+ Years of Age). New York, NY: The World Bank. Available online at: https://data.worldbank.org/indicator/SH.ALC.PCAP.LI (accessed August 27, 2022).
121. Pengpid S, Peltzer K. Underweight and overweight/obesity among adults in Afghanistan: prevalence and correlates from a national survey in 2018. J Health Popul Nutr. (2021) 40:25. doi: 10.1186/s41043-021-00251-0
122. Hamrah MN, Hamrah AE, Hamrah MH, Hamrah MH, Hamrah AE, Dahi T. Prevalence of coronary artery disease and its risk factors among outpatients in northern Afghanistan: a cross-sectional study in Andkhoy City. Pak J Med Health Sci. (2020) 14:1140–5. doi: 10.2147/CCIDE.S323428
123. Akhtar S, Nasir JA, Javed A, Saleem M, Sajjad S, Khan M, et al. The prevalence of diabetes in Afghanistan: a systematic review and meta-analysis. BMC Public Health. (2021) 21:941. doi: 10.1186/s12889-021-10993-5
124. World Health Organization. Global Action Plan for the Prevention and Control of Non-communicable Diseases, 2013–2020. Geneva: World Health Organization (2013).
125. World Health Organization United Nation Development Program. What Government Ministries Need to Know About Non-communicable Diseases. Sectoral Briefs. Geneva: World Health Organization and United Nation Development Program (2016). Available online at: https://www.undp.org/publications/what-government-ministries-need-know-about-non-communicable-diseases (accessed November 20, 2022).
Keywords: Afghanistan, non-communicable diseases, prevention and control, strategies, hypertension, diabetes, heart diseases, risk factors
Citation: Neyazi N, Mosadeghrad AM, Afshari M, Isfahani P and Safi N (2023) Strategies to tackle non-communicable diseases in Afghanistan: A scoping review. Front. Public Health 11:982416. doi: 10.3389/fpubh.2023.982416
Received: 30 June 2022; Accepted: 31 January 2023;
Published: 22 February 2023.
Edited by:
Stefanie Harsch, University of Education Freiburg, GermanyReviewed by:
Maziar Moradi-Lakeh, Iran University of Medical Sciences, IranKhwaja Mir Islam Saeed, Islam Saeed, Afghanistan
Copyright © 2023 Neyazi, Mosadeghrad, Afshari, Isfahani and Safi. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Narges Neyazi,  bmV5YXppbmFyZ2VzQGdtYWlsLmNvbQ==; Ali Mohammad Mosadeghrad, bW9zYWRlZ2hyYWRAZ21haWwuY29t
bmV5YXppbmFyZ2VzQGdtYWlsLmNvbQ==; Ali Mohammad Mosadeghrad, bW9zYWRlZ2hyYWRAZ21haWwuY29t