 Christopher Sundström
Christopher Sundström David Forsström
David Forsström Anne H. Berman
Anne H. Berman Zarnie Khadjesari
Zarnie Khadjesari Kristina Sundqvist1
Kristina Sundqvist1- 1Department of Psychology, Stockholm University, Stockholm, Sweden
- 2Centre for Psychiatry Research, Department of Clinical Neuroscience, Karolinska Institutet and Stockholm Health Care Services, Stockholm, Sweden
- 3Department of Psychology, Uppsala University, Uppsala, Sweden
- 4Behavioral and Implementation Science Research Group, School of Health Sciences, University of East Anglia, Norwich, United Kingdom
Background: Internet interventions are a promising avenue for delivering alcohol prevention to employees. The objective of this scoping review was to map all research on alcohol internet interventions aimed at employees regardless of design, to gain an overview of current evidence and identify potential knowledge gaps.
Methods: We conducted a literature search in three data bases (PsycInfo, PubMed, and Web of Science). Eligibility criteria were that (1) the study targeted employees age ≥18 years; (2) the intervention was delivered predominantly online; (3) the study focused specifically or in part on alcohol use; and (4) the study was published in English in a peer-reviewed academic journal. Two reviewers independently screened, reviewed, and extracted data.
Results: Twenty studies were included, of which 10 were randomized controlled trials, five were secondary analyses, three were feasibility trials, one was a cohort study and one described the rationale and development of an intervention. No qualitative studies were found. Randomized trials tended to show effects when interventions were compared to waitlists but not when more intensive interventions were compared to less intensive ones. We identified two design-related aspects where studies differed; (1) whether all applicants were included regardless of alcohol use level and (2) whether the intervention was explicitly framed as alcohol-focused or not. Significant recruitment problems were noted in several studies.
Conclusions: Alcohol internet interventions hold promise in delivering alcohol prevention to employees, but heterogeneity in study design and difficulties in recruitment complicate interpretation of findings.
Systematic review registration: https://osf.io/25x7e/, Open Science Framework.
1. Introduction
Alcohol remains a major risk factor for burden of disease in most parts of the world (1), but only one in six receive treatment (2). Since the majority of adults are employed and people spend most of their time at work, the workplace has been regarded as a valuable setting for provision of alcohol prevention (3, 4). Aside from the potential benefit for employees suffering from alcohol misuse, such as access to free and confidential evidence-based help, alcohol prevention is likely of great value for employers as the cost of alcohol problems in the workplace, measured in both absenteeism (being away from work due to consequences of alcohol use), presenteeism (being less productive at work due to consequences of alcohol use) and accidents, is substantial (5, 6). In recent decades, implementation of alcohol prevention programs in the workplace has therefore become increasingly common (3), complementing general workplace policies (7).
Despite the appropriateness and potential of alcohol prevention aimed at employees, there is a general lack of research in the area, with systematic reviews identifying few randomized controlled trials (8, 9). The lack of research may partly be attributed to the challenging context; workplace demands may be prioritized over research projects, insufficient support from the organization and from managers of the research project may create resistance among employees, and staff turnover and retirement may have negative consequences for follow-up. Aside from these issues common to all research conducted in the workplace, research on alcohol prevention introduces an additional challenge; there may be a significant fear of disclosing alcohol problems to one's employer, as this may negatively impact one's work situation.
A major development in mental health research in recent decades is the area of internet interventions, i.e., therapeutic interventions delivered via the internet. These interventions range widely in content from full cognitive behavior therapy treatment manuals delivered on internet platforms over weeks or months, to smartphone applications consisting of brief tips and techniques to address the problem in question “just-in-time.” They can also be delivered in blended format (i.e., face-to-face and internet combined), as well as with or without written guidance from a coach or health care professional (10). By now, a large body of evidence shows internet interventions to be effective in helping people with a range of mental health problems (11) and, although most of this evidence stems from research in community samples, these interventions are increasingly being integrated with routine mental health care (12). Internet interventions targeting both mental health (i.e., stress, depression, and alcohol) and general health (i.e., obesity, cardiovascular disease, and sedentary behavior) have been investigated specifically in the workplace (13), and two systematic reviews have attempted to summarize the evidence; one an analysis of 22 randomized controlled trials (RCTs) (14), and the second an analysis of 50 RCTs including a series of focused meta-analyses (15). The first of these, the systematic review by Howarth et al. (14), concluded that interventions targeting specific health behaviors such as sedentary behavior, insomnia, and heart health were moderately effective, while studies targeting more complex health behaviors such as alcohol problems and smoking, were less effective. Results from the six included studies on alcohol internet interventions were mixed, with significant findings only related to different subgroups. The second of these, the systematic review with a series of meta-analyses conducted by Philips et al. (15), showed moderate effects for interventions aimed at stress, insomnia and burnout, and lower effects for interventions aimed at depression and anxiety. The effects were non-significant for alcohol consumption, but only two studies were included in this meta-analysis. Further, in the only individual patient data meta-analysis (IPDMA) on alcohol internet interventions, a sub-group analysis of settings (community, healthcare, and workplace) was performed. Interventions conducted in community and healthcare settings were found effective in reducing alcohol consumption, while findings on interventions conducted in workplace settings were inconclusive. Of note, only three RCTs conducted in the workplace were included in the IPDMA, compared with seven in healthcare settings and 17 in community settings (16).
The aforementioned reviews were restricted to RCTs. However, focusing solely on RCTs may provide limited information on the current evidence in a setting such as the workplace where controlled trials are evidently rare and complicated to conduct (9). As there have been no previous attempts to summarize the wider literature on alcohol internet interventions in the workplace, a broad approach looking at all available research regardless of design, would be most likely to help the field advance at this stage. In order to gain an overview of the field and identify knowledge gaps, we therefore conducted a scoping review of all available evidence (17). We define alcohol internet interventions as any primary, secondary, tertiary prevention or treatment program designed to reduce alcohol consumption, delivered through the internet. Specifically, we were interested in mapping the characteristics of published research on internet alcohol interventions aimed at employees, asking the following specific questions:
1. What study designs were used?
2. What were the characteristics of the workplace setting where the studies were conducted?
3. How were employees approached?
4. What types of interventions were used?
5. What were the demographics of participants?
6. What were the main findings?
2. Materials and methods
2.1. Study design
This study was a scoping review attempting to summarize all published literature on internet alcohol interventions aimed at employees, using established methodology (17). All reporting was conducted in accordance with the PRISMA extension for Scoping Reviews (18).
2.2. Eligibility criteria
As this was a scoping review, we did not focus solely on RCTs and other quantitative evaluations but rather included all published research investigating this topic.
In order to be included in the review, the following eligibility criteria had to be met:
1. The study targeted employees ≥18 years old.
2. The intervention was predominantly provided over the internet (including mobile apps).
3. The study focused specifically or in part on alcohol use.
4. The publication was published in English in a peer-reviewed academic journal from January 2000 onwards (considering the fact that internet interventions were rarely investigated before this date).
Reviews and protocols were not included. In some cases, interventions were simultaneously aimed at several health-related behaviors (i.e., alcohol, physical activity, smoking etc). We then included only those studies where an alcohol-related outcome was reported.
2.3. Literature search strategy
A systematic literature search was conducted, with relevant articles published between January 2000 and February 2021 retrieved from the electronic databases PsycInfo, PubMed, and Web of Science. We combined search terms for “internet,” “alcohol problems,” and “employee” to search titles, keywords, or abstracts. Our search terms in PsycInfo were: (((work* or corporate or white-collar or professional or labor or labor or industrial or staff or organization or organization or employ*) and (CBT or cognitive behavio* therapy or treatment or brief intervention or intervention) and (Internet or web or online or compute* or cybertherapy or digital or e-intervention or e-mental health or e-therapy or eHealth or e-Health or tele-therapy or telehealth or app) and (drinking or alcohol))).ab,kw,ti (see Appendix for full search strategy in other databases). Further, reference lists of included studies and previously published reviews on internet interventions and workplace interventions were hand-searched to identify additional eligible studies. In December 2021, we updated the search to identify any studies that had been published since our initial search in February 2021. We made no searches for gray literature.
2.4. Data collection, extraction, and synthesis
Once the literature search had been conducted, all duplicates (studies found in more than one database) were removed. Articles were then independently screened in Excel sheets in three stages (title/abstract/full text) by authors CS and DF. At each stage, articles that clearly failed to meet eligibility criteria were excluded. If during the title and abstract screening stage, either of the two screening authors was unsure of whether or not a study should be excluded, that study was retained to be reconsidered in the next stage of screening. Any uncertainty or disagreement concerning whether a study should be excluded during the full text stage of screening was resolved in discussion with author ZK. After the screening process, authors CS and DF extracted relevant data from each eligible article: study characteristics, intervention characteristics and outcome data. Research was then summarized narratively and inductively with a primary focus on responding to the research questions and identifying research gaps.
3. Results
The combined initial literature search yielded 6,794 articles. Of these, 1,843 were removed as they were duplicates, leaving 4,951 articles for the title screen after which 611 remained. After the abstract screen, 65 remained, and after the full text screen, a total of 18 articles were included in the review. Further, two studies were identified in a hand search, leaving a total of 20 studies. See Figure 1 for a flowchart. See Table 1 for a presentation of the studies included.
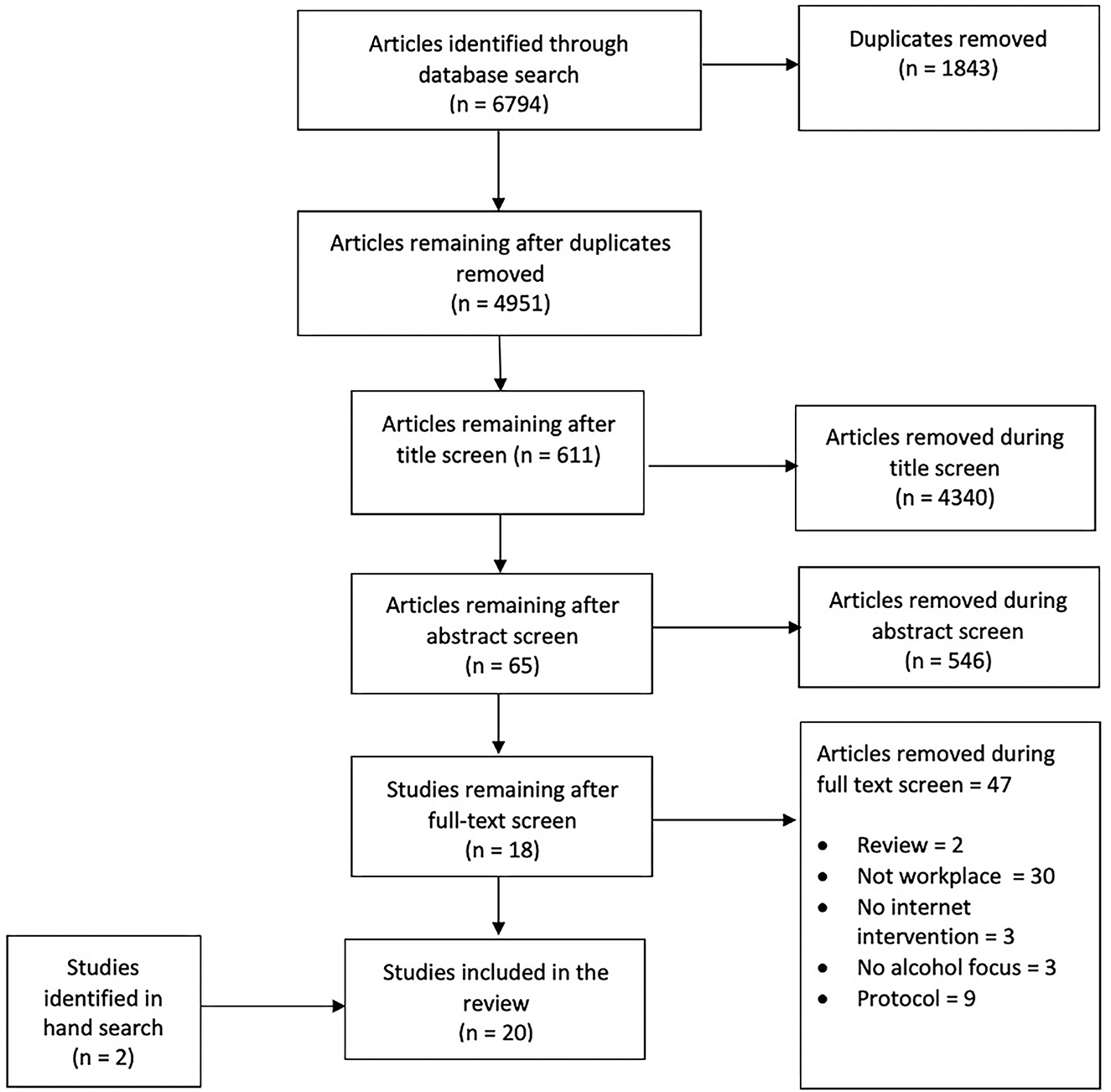
Figure 1. Flow of studies through the selection process.
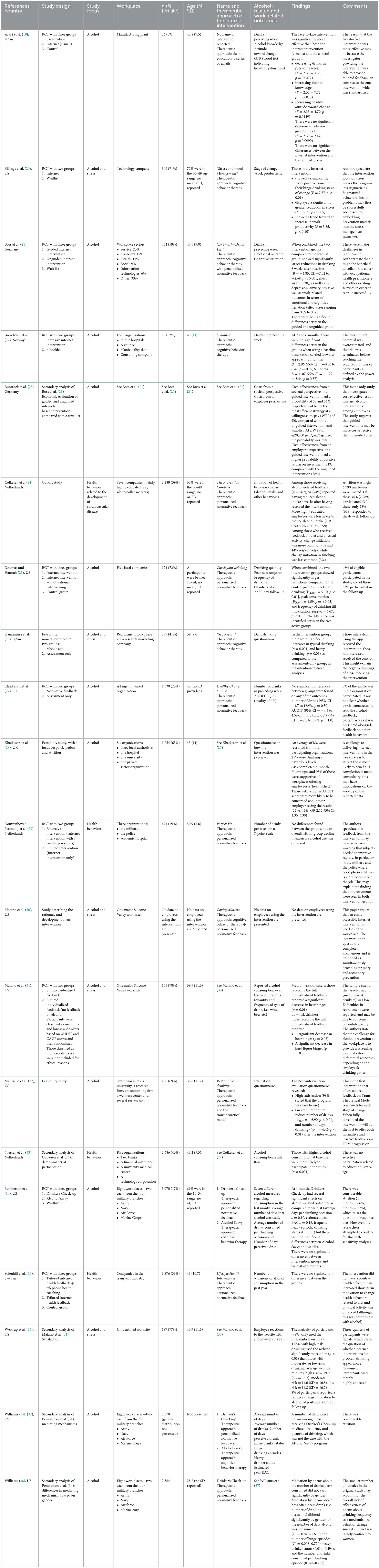
Table 1. Extraction data from the included studies.
3.1. Characteristics of included studies
The 20 articles reflected 16 unique studies and 13 projects; (see Table 1). Geographically, nine of the studies were conducted in the US, three in the Netherlands, with two studies conducted in the UK, Germany, and Japan respectively, and one each in Norway and Sweden. A total of 14,166 participants were included in the studies.
3.2. What study designs were used?
Of the 20 studies identified, 10 were randomized controlled trials (19–22, 25, 27, 29, 31, 34, 35), five were feasibility, non-randomized trials or cohort trials (24, 26, 28, 32, 36), four were secondary analyses of previously conducted randomized controlled trials or cohort studies (23, 33, 37, 38) and one was a paper describing the rationale and development of an intervention (30). No qualitative studies were identified.
3.3. What were the characteristics of the workplace setting where the studies were conducted?
Of the 20 included articles, 11 were conducted in several workplaces simultaneously (22, 24, 25, 28, 29, 32–35, 37, 38) and six were conducted in one single workplace (19, 20, 27, 30, 31, 36). Three studies were not formally conducted in a workplace but recruited employees through health insurance companies' websites and print membership magazines as well as in print newspaper articles (21, 23), or used a research marketing company to recruit participants who reported being employed (26).
There was large variation both between and within studies in terms of sectors. In the six articles reporting on studies conducted in a single workplace, information about sector was sparse; only two revealed the sector of the workplace where the study was being conducted (19, 20), three simply stated recruiting from “a large Silicone Valley work site” (30, 31, 36) and one stated recruiting from a “large UK-based organization” (27). Among the 12 articles reporting on studies recruiting participants from several different workplaces, information about sector was usually brief (see Table 1). For example, Brendryen et al. (22) recruited from both public hospitals, a county, the municipality, and a consulting company and Kouwenhoven-Pasmooij et al. (29) recruited from the military, the police and an academic hospital. Three articles reported on a study conducted solely in the military, albeit from four different branches (34, 37, 38). One study used a research marketing company to recruit participants and did not report information on the sectors in which the participants worked (26).
The most common way of informing employees about the study was through employee emails or web portals belonging to the workplace(s) where the study was being conducted (20, 22, 24, 27, 33, 35). In some studies, both emails and/or web portals, as well as more traditional methods such as magazines, posters, recruitment flyers and television advertisements were used (28, 29, 32, 34, 37, 38), while in other studies only newspapers, brochures and flyers were used (30, 31, 36). In one study, only employees with abnormal levels in their serum y-GTP (i.e., blood test indicating hepatic dysfunction) from a workplace health check were approached (19). As previously mentioned, in three articles, no workplace was included in the recruitment process (21, 23, 26). One study did not specify which recruitment method was used (25).
3.4. What types of interventions were used?
The content of the interventions in the studies fell into two main categories; personalized normative feedback (PNF) and cognitive behavior therapy (CBT). PNF is a form of brief intervention aiming to inform individuals about their consumption patterns in comparison to those in the general population (39), while CBT is a form of psychological treatment that focused on the interplay of behaviors and thoughts. It should be noted that these interventions blend into one another sometimes, with some PNF interventions including CBT strategies and drinking diaries, and some CBT interventions including a PNF component.
Most interventions included PNF. Some of these interventions offered PNF for alcohol only (25, 32, 34, 37, 38), while in others, the intervention provided PNF on a host of health behaviors such as smoking, fruit/vegetable intake and physical activity (24, 27–29, 33, 35). In two of these later studies, the explicit objective of the researchers was to investigate the effects of PNF on alcohol consumption, with other health-related behaviors included in the intervention only to mask the alcohol focus of the study (27, 28), while in the other studies, the explicit research question did not focus exclusively on alcohol but on effects of PNF on all health behaviors (24, 29, 35). In one study, the intervention consisted of alcohol education, seemingly without any PNF (19).
Of the interventions based on CBT, two had an explicit focus on alcohol consumption (21, 22), while three interventions were mainly framed as focusing on stress and how to avoid using alcohol when coping with stress (20, 26, 30).
Four studies included some form of human contact in one of the groups. In one study, the intervention was delivered together with optional guidance from a therapist over the treatment platform (21), in a second study the intervention was delivered with coaching sessions (29), in a third study with telephone calls (35) and in a fourth study with motivational interviewing sessions (25).
3.5. What were the demographics of participants?
There was variation between the studies, with some including a large majority of females (20, 25, 31) some including a majority of males (24, 27, 29, 34), and one study including men only (19). Pemberton et al. (34) included 17% females in the military and Solenhill et al. (35) included 33% females in the transport industry, whereas Doumas and Hannah et al. (25) included 73% females among young people working in local companies, and Billings et al. (20) included 71% females from a technology company. The mean age of participants in most studies was between 40 and 50 years, with the exception of one study which only included young adults between the ages of 18 and 24 (25). Profession, education level and socioeconomic status were rarely reported.
3.6. What were the main findings?
A host of different alcohol outcomes were used in the studies of which the most common one was number of standard drinks consumed or some similar calendar-based way of assessing recent consumption (21, 22, 25–27). Other forms of self-reported alcohol outcomes were also used, such as alcohol knowledge (19), stage of change (20) and initiation of alcohol-related change (24). Only one study included a biological outcome measure (19).
In terms of intervention effects in the RCTs, seven studies used wait-lists as control groups to assess effects. In four of these, the internet interventions were found more effective than the waitlist in at least one alcohol-related outcome (20, 21, 25, 34) while in three studies, no such differences were found (19, 27, 35). Three studies compared the internet intervention to an active control group: Brendryen et al. (22) compared the internet intervention to an e-booklet with alcohol education, Matano et al. (31) compared a more extensive internet intervention to a less extensive internet intervention and Pemberton et al. (34) compared two different internet interventions; one based on CBT and one based on PNF. None of these studies found significant differences between the internet intervention and the active control. One study was non-randomized, with those wishing to use the internet intervention (a mobile app) receiving it and those not interested receiving assessment only. In this study, those choosing the internet intervention reported a significant increase in typical drinking and heavy drinking compared to the assessment group (26). The four studies comparing an intervention with and without human contact, found no significant differences between the groups (21, 25, 29, 35). A cost-effectiveness analysis of one of these studies (21), however, found that the guided intervention was more cost-effective than then unguided intervention (23). In the only study comparing a human-delivered intervention with an internet intervention, the human-delivered intervention was found to be more effective (19).
Some studies also investigated mental health outcomes. Billings et al. (20) found that those receiving the internet intervention reduced their stress as well as increased their knowledge about anxiety and depression compared to the waitlist and Boss et al. (21) found that the internet intervention reduced stress, anxiety and depression compared to the waitlist. Khadjesari et al. (27) found no significant differences in quality of life between the intervention and the control group. Hamamura et al. (26) found that those using the internet intervention (mobile app) had an increase in anxiety. As mentioned, this study was non-randomized thereby greatly reducing internal validity.
Only two studies reported work-related outcomes: Billings et al. (20) found that users of the intervention improved their ability to handle time and scheduling demands of their job when compared to controls, and also that they improved the quantity and quality of completed work. Boss et al. (21) found significantly greater reductions in emotional and cognitive irritation, a way of assessing rumination in the workplace context (40).
One study described the rationale and development of an intervention, building the case for developing an alcohol internet intervention that can simultaneously offer primary and secondary prevention (30). Three studies were feasibility studies looking at recruitment potential and/or user satisfaction (27, 32, 36). Four studies presented secondary analyses of randomized trials: One looked at mediating mechanisms, finding that the effects of one internet intervention (Drinker's Check-up) were largely mediated by perceived descriptive norms of alcohol consumption (37) and a subsequent study finding that these mediations were moderated by gender (38). Another study looked at determinants of participation, finding that those with higher alcohol consumption at baseline were more likely to participate in the study (33). As already mentioned, one study looked at cost-effectiveness, finding that the guided intervention was more cost-effective than the unguided intervention (23).
3.7. Synthesis of findings
When synthesizing our results, we identified two main differences in study design in the RCTs, that may bear consequences for interpretation of results. Below, we formulate these differences as questions (see Table 2).
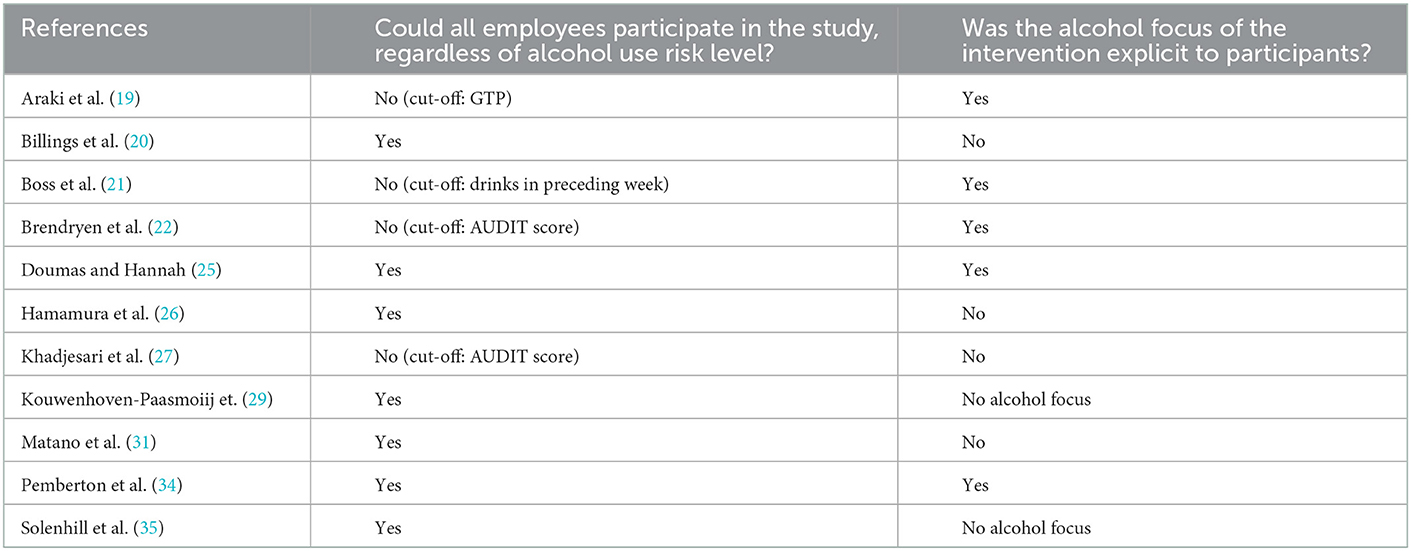
Table 2. Study design aspects of the 10 RCTs.
3.7.1. Could all employees participate in the study, regardless of alcohol use risk level?
In six RCTs and one non-randomized trial, all employees were welcome to participate in the study regardless of their level of alcohol use (20, 25, 26, 29, 31, 32, 35) while in four studies only those reporting alcohol problems were able to participate. In these latter studies, inclusion was based on cut-off scores on either AUDIT (22, 27), drinks preceding week (21) or levels of GTP (19). Including everyone in the study regardless of level of alcohol use may introduce a floor effect which could potentially dilute the impact of the intervention, and some researchers tried to handle this risk without explicitly excluding participants. For example, Khadjesari et al. (27) included only those exceeding cut-off scores in the actual study, but everyone was welcome to receive the intervention. In Matano et al. (31), although both low- and medium-risk participants were included and given access to the intervention, participants were categorized according to their alcohol use risk level and then analyzed separately, even though this strategy led to greatly reduced power.
3.7.2. Was the alcohol focus of the intervention explicit to participants?
In some studies, participants were explicitly informed about the alcohol focus of the intervention, while in other studies the focus on alcohol was intentionally masked. This was done, for example, by framing the intervention as how to deal with stress (20, 26, 31) or by having the intervention focus on several different health behaviors, even though the researchers were specifically interested in alcohol (27). As mentioned, some studies focused on health behaviors, with equal weight given to alcohol, physical activity, diet etc (29, 33, 35).
3.7.3. Difficulties in recruitment and follow-up
Recruitment problems were reported in several studies (21, 22, 31). Brendryen et al. (22) discussed these difficulties most extensively; not all employees appeared to use their email account, and the mailing list used by some organizations had not been updated for a long time. Further, a significant amount of time passed between the researchers' first contact with an organization and invitations being sent out to the employees; due to the unexpectedly slow process, recruitment had to be stopped before reaching the number of participants needed. The researchers also noted concerns in organizations about participating in the project related to the randomization aspect of the trial, and about employees spending too much time with the intervention when at work. Matano et al. (31) also encountered recruitment challenges regarding those with more severe problems, citing confidentiality issues as a likely explanation for the difficulty in recruiting this group. In some studies, recruitment issues were discussed in terms of how large a percentage of the organization workforce that participated in the study. In a feasibility study specifically assessing eligibility, recruitment, and attrition, Khadjesari et al. (27, 28) reported that the researchers reached between 4 and 8% of the total workforce in the six organizations with their intervention (PNF for health behaviors), which was considered low when compared to other feasibility studies of brief interventions. Several studies also reported low follow-up rates. For example, Pemberton et al. (34) reported that 35% participated in the 1-month follow-up and 17% participated in the 6-month follow-up, although analyses of missing data suggested that this did not bias the (largely positive) results; Colkesen et al. (24) reported that only 28% participated in the 4-week follow-up.
4. Discussion
4.1. Summary of findings
In this scoping review, we identified 20 studies about alcohol internet interventions in the workplace. Half of the studies were randomized controlled trials, five were secondary analyses, three were feasibility studies, one was a cohort study and one described the rationale and development of an intervention. No qualitative studies were identified. The interventions consisted of personalized normative feedback and/or cognitive behavior therapy. The gender distribution among participants was similar in most studies and the average age was similar to other alcohol internet intervention studies (16). Organizations where studies were conducted were sparsely described, and the variety of sectors included in the studies (i.e., technology, service, transport, military, and health care) prevent conclusions regarding whether these interventions might be particularly beneficial in certain sectors. All studies except one used only self-report measures to report alcohol-related outcomes and only two studies used work-related outcomes. Effects on alcohol-related outcomes in randomized trials tended to be present when interventions were compared to waitlists but when more intensive interventions were compared to less intensive ones, differential effects were rare. Two design aspects that differed among the studies were identified; one related to inclusion criteria (i.e., some studies included all employees while others used an alcohol-related cut-off) and one related to the framing of the intervention (i.e., some studies were explicit about the alcohol focus of the intervention while others were framed as targeting stress or general health). Several studies reported major difficulties regarding both recruitment and attrition.
4.2. What is needed for the field to advance?
The field of alcohol internet interventions is small and the trials conducted to date have evidently encountered many challenges. Improved methodological stringency paired with an awareness of the unique challenges this context provides is needed. Below, we discuss some targeted efforts that the field would benefit from at this stage.
First, the education level of those participating was not reported in most studies. This should be studied in greater detail, especially considering the fact that some research suggests that education level is negatively associated with outcomes in alcohol internet interventions (16). We therefore encourage researchers to collect data on participants' education level and profession. Second, although all RCTs used some form of alcohol-related outcome, specific outcomes in the studies varied (i.e., drinks preceding week, drinking pattern in the preceding month, number of binge episodes, readiness to change etc), complicating comparisons of effects across studies. A consensus statement regarding standardization of outcomes would facilitate future systematic reviews or meta-analyses. Third, only two studies reported on work-related outcomes. Future trials should investigate such outcomes further, for example work productivity and effort-reward imbalance (41). Fourth, as several studies reported major difficulties regarding recruitment, we recommend qualitative studies in order to better understand barriers and facilitators (42). It is still not well understood how these interventions are best implemented within the workplace setting (43), and researchers should prepare meticulously to prevent setbacks related to recruitment and attrition. Fifth, wait lists were common in these trials but there are limitations to using these as they may lead to treatment outcomes being overestimated (16). Active controls should therefore be considered to a greater extent. Sixth, researchers need to be consciously aware of pros and cons of design decisions. For example, if no alcohol-related inclusion criteria is used, the participation pool will be greater which in turn may facilitate recruitment. This may, however, dilute the treatment effect as some participants will not present with alcohol problems and so will not be able to improve. Similarly, framing the focus of an alcohol internet intervention as being about stress or general health may facilitate recruitment, attracting some with alcohol problems who are in denial or who may not have realized that they have an alcohol problem, However, some with alcohol problems but without for example stress issues might neglect an opportunity to participate in such an intervention, as they may feel that this other focus does not apply to them. Future studies could potentially investigate whether this later assumption holds true by randomizing participants to interventions framed in different ways, comparing demographic and clinical characteristics. However, there are also obvious ethical dilemmas in using deception. Lastly, all studies in this review were conducted in high-income countries. As low-and middle income countries tend to have less accessibility to substance use services in general (44, 45), alcohol internet interventions in the workplace could potentially have even more significance in these countries. We therefore strongly encourage research conducted in low- and middle income countries.
4.3. Summary of recommendations for future research
1. Detailed information about demographic characteristics such as education level and profession, should be collected, as this might aid in understanding which participants benefit most from these interventions.
2. In order to facilitate comparisons of effects across studies, researchers should include the most common alcohol-related outcome measures in the field.
3. Work-related outcomes should be included to a greater extent.
4. Qualitative studies would likely help in understanding how studies could be designed to decrease problems in recruitment.
5. Researchers should be conscious of how design decisions regarding inclusion criteria and framing of the intervention may influence what conclusions can be drawn.
6. Future studies should include active controls rather than wait list controls.
7. Studies conducted in low- and middle-income countries are sorely needed.
4.4. Limitations
This review made use of a broad search strategy and we conducted searches in three widely used databases. Although these databases are large, it is possible that some studies were not identified in this process. Also, we did not search for gray literature. Scoping reviews generally are limited in what can be generalized, in comparison to systematic reviews.
5. Conclusions
Alcohol internet interventions hold promise in delivering alcohol prevention in the workplace. However, heterogeneity in study design and difficulties in recruitment complicate interpretation of findings. The field would benefit from a consensus statement on issues related to study design and outcomes.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author.
Author contributions
CS: conceptualization, data curation, formal analysis, funding acquisition, investigation, methodology, project administration, writing—original draft, and writing—review and editing. DF: conceptualization, data curation, formal analysis, funding acquisition, investigation, methodology, project administration, and writing—review and editing. AB: funding acquisition, investigation, and writing—review and editing-equal. ZK: conceptualization, formal analysis, investigation, methodology, and writing—review and editing. KS: conceptualization, formal analysis, funding acquisition, investigation, methodology, project administration, writing—original draft, and writing—review and editing. All authors contributed to the article and approved the submitted version.
Funding
This work was funded by AFA Försäkring. The funder was not involved in the study design, collection, analysis, interpretation of data, the writing of this article, or the decision to submit it for publication.
Conflict of interest
CS has been on the clinical review board of the digital mental health company Alavida.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2023.929782/full#supplementary-material
References
1. Peacock A, Leung J, Larney S, Colledge S, Hickman M, Rehm J, et al. Global statistics on alcohol, tobacco and illicit drug use: 2017 status report. Addiction. (2018) 113:1905–26. doi: 10.1111/add.14234
2. Mekonen T, Chan GCK, Connor J, Hall W, Hides L, Leung J. Treatment rates for alcohol use disorders: a systematic review and meta-analysis. Addiction. (2021) 116:2617–34. doi: 10.1111/add.15357
3. Roman PM, Blum TC. The workplace and alcohol problem prevention. Alcohol Res Health. (2002) 26:49–57. Available online at: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6683807/pdf/49-57.pdf
4. Anderson P. Alcohol and the Workplace. Alcohol in the European Union: Consumption, Harm and Policy Approaches. Copenhagen: World Health Organisation Regional Office for Europe (2012), p. 69–82.
5. Sullivan T, Edgar F, McAndrew I. The hidden costs of employee drinking: a quantitative analysis. Drug Alcohol Rev. (2019) 38:543–53. doi: 10.1111/dar.12935
6. Ames GM, Bennett JB. Prevention interventions of alcohol problems in the workplace. Alcohol Res Health. (2011) 34:175–87. Available online at: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3860571/pdf/arh-34-2-175.pdf
7. Pidd K, Kostadinov V, Roche A. Do workplace policies work? An examination of the relationship between alcohol and other drug policies and workers' substance use. Int J Drug Policy. (2016) 28:48–54. doi: 10.1016/j.drugpo.2015.08.017
8. Yuvaraj K, Eliyas SK, Gokul S, Manikandanesan S. Effectiveness of workplace intervention for reducing alcohol consumption: a systematic review and meta-analysis. Alcohol Alcohol. (2019) 54:264–71. doi: 10.1093/alcalc/agz024
9. Webb G, Shakeshaft A, Sanson-Fisher R, Havard A. A systematic review of work-place interventions for alcohol-related problems. Addiction. (2009) 104:365–77. doi: 10.1111/j.1360-0443.2008.02472.x
10. Andersson G. Internet interventions: past, present and future. Internet Interv. (2018) 12:181–8. doi: 10.1016/j.invent.2018.03.008
11. Andersson G, Titov N, Dear BF, Rozental A, Carlbring P. Internet-delivered psychological treatments: from innovation to implementation. World Psychiatry. (2019) 18:20–8. doi: 10.1002/wps.20610
12. Titov N, Dear B, Nielssen O, Staples L, Hadjistavropoulos H, Nugent M, et al. ICBT in routine care: a descriptive analysis of successful clinics in five countries. Internet Interv. (2018) 13:108–15. doi: 10.1016/j.invent.2018.07.006
13. Lehr D, Geraedts A, Persson Asplund R, Khadjesari Z, Heber E, de Bloom J, et al. Occupational e-mental health: current approaches and promising perspectives for promoting mental health in workers. In: Wiencke M, Cacace M, Fischer S, editors. Healthy at Work: Interdisciplinary Perspectives. Cham: Springer International Publishing (2016), p. 257–81. doi: 10.1007/978-3-319-32331-2_19
14. Howarth A, Quesada J, Silva J, Judycki S, Mills PR. The impact of digital health interventions on health-related outcomes in the workplace: a systematic review. Digital Health. (2018) 4:2055207618770861. doi: 10.1177/2055207618770861
15. Phillips EA, Gordeev VS, Schreyögg J. Effectiveness of occupational e-mental health interventions: a systematic review and meta-analysis of randomized controlled trials. Scand J Work Environ Health. (2019) 45:560–76. doi: 10.5271/sjweh.3839
16. Riper H, Hoogendoorn A, Cuijpers P, Karyotaki E, Boumparis N, Mira A, et al. Effectiveness and treatment moderators of internet interventions for adult problem drinking: an individual patient data meta-analysis of 19 randomised controlled trials. PLoS Med. (2018) 15:e1002714. doi: 10.1371/journal.pmed.1002714
17. Arksey H, O'Malley L. Scoping studies: towards a methodological framework. Int J Soc Res Methodol. (2005) 8:19–32. doi: 10.1080/1364557032000119616
18. Tricco AC, Lillie E, Zarin W, O'Brien KK, Colquhoun H, Levac D, et al. PRISMA extension for scoping reviews (prisma-scr): checklist and explanation. Ann Intern Med. (2018) 169:467–73. doi: 10.7326/M18-0850
19. Araki I, Hashimoto H, Kono K, Matsuki H, Yano E. Controlled trial of worksite health education through face-to-face counseling vs. e-mail on drinking behavior modification. J Occup Health. (2006) 48:239–45. doi: 10.1539/joh.48.239
20. Billings DW, Cook RF, Hendrickson A, Dove DC. A web-based approach to managing stress and mood disorders in the workforce. J Occup Environ Med. (2008) 50:960–8. doi: 10.1097/JOM.0b013e31816c435b
21. Boss L, Lehr D, Schaub MP, Paz Castro R, Riper H, Berking M, et al. Efficacy of a web-based intervention with and without guidance for employees with risky drinking: results of a three-arm randomized controlled trial. Addiction. (2018) 113:635–46. doi: 10.1111/add.14085
22. Brendryen H, Johansen A, Duckert F, Nesvag S. A pilot randomized controlled trial of an internet-based alcohol intervention in a workplace setting. Int J Behav Med. (2017) 24:768–77. doi: 10.1007/s12529-017-9665-0
23. Buntrock C, Freund J, Smit F, Riper H, Lehr D, Boß L, et al. Reducing problematic alcohol use in employees: economic evaluation of guided and unguided web-based interventions alongside a three-arm randomized controlled trial. Addiction. (2021). 117:611–22. doi: 10.1111/add.15718
24. Colkesen EB, Niessen MA, Peek N, Vosbergen S, Kraaijenhagen RA, van Kalken CK, et al. Initiation of health-behaviour change among employees participating in a web-based health risk assessment with tailored feedback. J Occup Med Toxicol. (2011) 6:5. doi: 10.1186/1745-6673-6-5
25. Doumas DM, Hannah E. Preventing high-risk drinking in youth in the workplace: a web-based normative feedback program. J Subst Abuse Treat. (2008) 34:263–71. doi: 10.1016/j.jsat.2007.04.006
26. Hamamura T, Suganuma S, Ueda M, Mearns J, Shimoyama H. Standalone effects of a cognitive behavioral intervention using a mobile phone app on psychological distress and alcohol consumption among japanese workers: pilot nonrandomized controlled trial. JMIR Mental Health. (2018) 5:e24. doi: 10.2196/mental.8984
27. Khadjesari Z, Freemantle N, Linke S, Hunter R, Murray E. Health on the web: randomised controlled trial of online screening and brief alcohol intervention delivered in a workplace setting. PLoS ONE. (2014) 9:e112553. doi: 10.1371/journal.pone.0112553
28. Khadjesari Z, Newbury-Birch D, Murray E, Shenker D, Marston L, Kaner E. Online health check for reducing alcohol intake among employees: a feasibility study in six workplaces across England. PLoS ONE. (2015) 10:e0121174. doi: 10.1371/journal.pone.0121174
29. Kouwenhoven-Pasmooij TA, Robroek SJW, Kraaijenhagen RA, Helmhout PH, Nieboer D, Burdorf A, et al. Effectiveness of the blended-care lifestyle intervention ‘PerfectFit’: a cluster randomised trial in employees at risk for cardiovascular diseases. BMC Public Health. (2018) 18:766. doi: 10.1186/s12889-018-5633-0
30. Matano RA, Futa KT, Wanat SF, Mussman LM, Leung CW. The employee stress and alcohol project: the development of a computer-based alcohol abuse prevention program for employees. J Behav Health Serv Res. (2000) 27:152–65. doi: 10.1007/BF02287310
31. Matano RA, Koopman C, Wanat SF, Winzelberg AJ, Whitsell SD, Westrup D, et al. A pilot study of an interactive web site in the workplace for reducing alcohol consumption. J Subst Abuse Treat. (2007) 32:71–80. doi: 10.1016/j.jsat.2006.05.020
32. Mauriello LM, Gökbayrak NS, Van Marter DF, Paiva AL, Prochaska JM. An internet-based computer-tailored intervention to promote responsible drinking: findings from a pilot test with employed adults. Alcohol Treat Q. (2011) 30:91–108. doi: 10.1080/07347324.2012.635528
33. Niessen MA, Laan EL, Robroek SJ, Essink-Bot ML, Peek N, Kraaijenhagen RA, et al. Determinants of participation in a web-based health risk assessment and consequences for health promotion programs. J Med Internet Res. (2013) 15:e151. doi: 10.2196/jmir.2387
34. Pemberton MR, Williams J, Herman-Stahl M, Calvin SL, Bradshaw MR, Bray RM, et al. Evaluation of two web-based alcohol interventions in the US military. J Stud Alcohol Drugs. (2011) 72:480–9. doi: 10.15288/jsad.2011.72.480
35. Solenhill M, Grotta A, Pasquali E, Bakkman L, Bellocco R, Trolle Lagerros Y. The effect of tailored web-based feedback and optional telephone coaching on health improvements: a randomized intervention among employees in the transport service industry. J Med Internet Res. (2016) 18:e158. doi: 10.2196/jmir.4005
36. Westrup D, Futa KT, Whitsell SD, Mussman L, Wanat SF, Koopman C, et al. Employees' reactions to an interactive website assessing alcohol use and risk for alcohol dependence, stress level and coping. J Subst Use. (2003) 8:104–11. doi: 10.1080/1465989031000109789
37. Williams J, Herman-Stahl M, Calvin SL, Pemberton M, Bradshaw M. Mediating mechanisms of a military Web-based alcohol intervention. Drug Alcohol Depend. (2009) 100:248–57. doi: 10.1016/j.drugalcdep.2008.10.007
38. Williams J. Gender differences in descriptive norms as mediators of a military web-based alcohol intervention. J Stud Alcohol Drugs. (2021) 82:659–67. doi: 10.15288/jsad.2021.82.659
39. Neighbors C, Rodriguez LM, Rinker DV, Gonzales RG, Agana M, Tackett JL, et al. Efficacy of personalized normative feedback as a brief intervention for college student gambling: a randomized controlled trial. J Consult Clin Psychol. (2015) 83:500–11. doi: 10.1037/a0039125
40. Mohr G, Müller A, Rigotti T, Aycan Z, Tschan F. The assessment of psychological strain in work contexts. Eur J Psychol Assess. (2006) 22:198–206. doi: 10.1027/1015-5759.22.3.198
41. Skogen JC, Thørrisen MM, Bonsaksen T, Vahtera J, Sivertsen B, Aas RW. Effort-reward imbalance is associated with alcohol-related problems. WIRUS-screening study. Front Psychol. (2019) 10:2079. doi: 10.3389/fpsyg.2019.02079
42. Broyles LM, Rodriguez KL, Kraemer KL, Sevick MA, Price PA, Gordon AJ, et al. qualitative study of anticipated barriers and facilitators to the implementation of nurse-delivered alcohol screening, brief intervention, and referral to treatment for hospitalized patients in a Veterans Affairs medical center. Addict Sci Clin Pract. (2012) 7:7. doi: 10.1186/1940-0640-7-7
43. Thørrisen MM, Skogen JC, Kjeken I, Jensen I, Aas RW. Current practices and perceived implementation barriers for working with alcohol prevention in occupational health services: the WIRUS OHS study. Subst Abuse Treat Prev Policy. (2019) 14:30. doi: 10.1186/s13011-019-0217-2
44. Satinsky EN, Kleinman MB, Tralka HM, Jack HE, Myers B, Magidson JF. Peer-delivered services for substance use in low- and middle-income countries: a systematic review. Int J Drug Policy. (2021) 95:103252. doi: 10.1016/j.drugpo.2021.103252
Keywords: alcohol, digital intervention, internet intervention, workplace, employee, scoping review
Citation: Sundström C, Forsström D, Berman AH, Khadjesari Z and Sundqvist K (2023) What do we know about alcohol internet interventions aimed at employees?—A scoping review. Front. Public Health 11:929782. doi: 10.3389/fpubh.2023.929782
Received: 27 April 2022; Accepted: 02 January 2023;
Published: 26 January 2023.
Edited by:
Joel Msafiri Francis, University of the Witwatersrand, South AfricaReviewed by:
Mikkel Magnus Thørrisen, Oslo Metropolitan University, NorwayClaire Garnett, University College London, United Kingdom
Copyright © 2023 Sundström, Forsström, Berman, Khadjesari and Sundqvist. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Christopher Sundström,  Y2hyaXN0b3BoZXIuc3VuZHN0cm9tQHN1LnNl
Y2hyaXN0b3BoZXIuc3VuZHN0cm9tQHN1LnNl