
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health, 05 January 2024
Sec. Public Health Education and Promotion
Volume 11 - 2023 | https://doi.org/10.3389/fpubh.2023.1326760
This article is part of the Research TopicCommunity Health Workers: Describing the Breadth of Interventions and Contexts Across the WorldView all 18 articles
 Tayebeh Rakhshani1Sepahdar Nikeghbal2Seyyed Mansour Kashfi3
Tayebeh Rakhshani1Sepahdar Nikeghbal2Seyyed Mansour Kashfi3 Amirhossein Kamyab4
Amirhossein Kamyab4 Pooyan Afzali Harsini5
Pooyan Afzali Harsini5 Ali Khani Jeihooni6*
Ali Khani Jeihooni6*Background: Hospital staff represent a vulnerable population for respiratory diseases. Consequently, the implementation of training programs becomes imperative as a preventive measure against such infections in these populations. The current study was conducted to examine the impact of an educational intervention based on the Protection Motivation Theory (PMT) on preventive behaviors for respiratory infections among a group of hospital staff.
Methods: This experimental study involves a sample of 150 hospital staff from Gachsaran City, Iran, in 2021–2022. The sampling technique involved the utilization of a random assignment approach to allocate individuals into two distinct groups: the experimental group, consisting of 75 participants, and the control group, also including 75 individuals. The data collection instrument was a questionnaire designed in accordance with the PMT. This questionnaire was administered to both the experimental and control groups prior to the intervention as well as two months following the intervention. The intervention program consisted of a total of five sessions, each lasting for 60 min, for the experimental group. These sessions were conducted on a weekly basis over a period of two and a half months. Specifically, there were two sessions held every month and one session held every two weeks. Following the completion of the program, the data was entered into SPSS-24 statistical software for analysis using paired t-tests, independent t-tests, and chi-square tests.
Results: The results indicated that prior to the intervention, there was no significant difference between the two groups in terms of perceived vulnerability constructs (p = 0.25), perceived severity (p = 0.63), perceived response (p = 0.32), and perceived reward (p = 0.11). Besides, there was no considerable distinction in perceived self-efficacy (p = 0.84), perceived response cost (p = 0.33), fear (p = 0.45), behavior motivation (p = 0.51), knowledge (p = 92), or vaccination behavior (p = 0.12) before the educational intervention. However, a significant change was noticed in each of the mentioned variables between the two groups after the intervention (p < 0.05).
Conclusion: The results of this study indicated that the implementation of an educational intervention grounded in the PMT yields positive outcomes in enhancing preventative behaviors pertaining to respiratory infections. Hence, it is recommended to utilize an intervention grounded in this theory among hospital staff as a viable approach to mitigating the occurrence of respiratory infections.
Acute respiratory tract infections are prevalent and can lead to significant and unfavorable health outcomes for patients (1–3). This category of infections encompasses a diverse array of illnesses, including common colds, throat infections, tonsillitis, influenza, COVID-19, and lower respiratory tract diseases (4). The etiological agents responsible for these diseases can be viral, bacterial, fungal, or even parasitic in nature (5–7). This particular ailment is responsible for around one-third of fatalities that occur within hospital settings, while also extending the length of hospital stays and incurring additional expenses related to treatment (8). Consequently, the failure of hospital staff to adhere to infection control protocols was identified as a mental health issue (9, 10). In 2019, a highly perilous respiratory infectious disease emerged and rapidly attained global prevalence, resulting in several fatalities (11). On January 30, 2020, the World Health Organization officially declared the dissemination of this disease the sixth leading cause of a global public health emergency. The causative agent was identified as the coronavirus (12–14).
In contrast to other administrative and service businesses, hospitals and medical facilities pose a higher level of risk to their workers (15). One of the most prevalent occupational risks faced by healthcare workers is the potential exposure to biological agents, which is subsequently associated with the risk of infection (15). Healthcare professionals are at the forefront of combating infectious diseases and thus face a higher risk of infection, making them more susceptible to the consequences associated with such disorders (16). The research findings indicate that there was an 8.3% rate of infection among medical care workers during the COVID-19 outbreak. This high percentage of infections can be attributed to the lack of protective measures taken by medical workers during their initial contact with infected patients at the onset of the outbreak (17).
The implementation of preventive measures by healthcare professionals to safeguard their own well-being against respiratory infections is a pivotal component of the respiratory infection prevention and control program (18). One of the crucial and indispensable techniques for the prevention and control of respiratory infections is the implementation of preventive measures, which encompass educational initiatives, the enhancement of public knowledge, and the development of personal protective skills (19). The initial stage in the planning process of a health education program involves the selection of an appropriate model. This model serves as a guiding framework, ensuring that the program remains focused and aligned with its intended objectives (19).
The Protection Motivation Theory (PMT) is a prominent educational framework that has been proposed in the field of health education (20). This idea was posited by Rogers in 1975 as a means to elucidate the impact of fear on attitudes and behaviors pertaining to health (21). This approach posits that the adoption of health behaviors aimed at mitigating health risks is directly influenced by an individual’s incentive to safeguard their own well-being (22). Rogers suggested that fear affects protection motivation (or the intention to perform protective measures against risks) through five constructs, and ultimately protection motivation causes healthy behaviors, these five constructs are: perceived vulnerability (a person’s belief that they are vulnerable to a health hazard), perceived severity (a person’s belief that the hazard is serious), perceived response efficacy (a person’s expectation that an adaptive response can eliminate the hazard), perceived response costs (a person’s estimate of any costs, such as money, people, time, and effort, associated with the protected behavior), and perceived self-efficacy (a person’s belief that they can successfully perform the behavior) (22).
In some studies, the effectiveness of health interventions based on the PMT has been mentioned in preventing various diseases; for example, Kowalski et al. (23), Ekow Arkorful et al. (24), and Salmani et al. (25) have stated that high blood pressure can be controlled by using health interventions (23–25). Healthcare professionals maintain a direct association with both individuals afflicted by respiratory infections and those who are in good health. Consequently, it is imperative to prioritize the well-being of these employees, as it serves the dual purpose of safeguarding them against respiratory infections and curbing the transmission of such infections within the wider community. It is vital to identify the preventative measures and control strategies for respiratory infections, as well as the determinants and factors that influence individuals’ adoption of preventive behaviors in relation to such infections.
Given the imperative nature of engaging in protective measures against respiratory infections and adhering strictly to health protocols within the healthcare profession, it is crucial to examine the attitudes and beliefs surrounding the rigorous implementation of these behaviors among healthcare workers. This analysis will inform the development and execution of appropriate educational interventions aimed at fostering a culture of adherence and promoting these protective behaviors. The adoption of protective behaviors is expected to yield positive outcomes. Given their role as guardians of the health and well-being of other individuals within society, it is imperative to assess the health behaviors of these individuals based on the outcomes observed. Consequently, it is crucial to undertake measures aimed at preserving and enhancing their own health. Hence, the current study was devised and executed with the objective of assessing the impact of an educational intervention rooted in the PMT on the adoption of preventive behaviors against respiratory diseases among the hospital staff in Gachsaran city, Iran.
This experimental study was conducted in 2021–2022 among the employees of Gachsaran City Hospital. The criteria for entering the study were having work experience of more than one year at the hospital and having contact with infectious diseases at the time of the study. Exclusion criteria were not wanting to cooperate at any time during the study, changing the workplace during the implementation of the study, and not participating in more than two training sessions.
Considering the mean comparison formula in two communities and also according to the results of similar research by Bashirian et al. (26), the sample size was determined to be 150 people using the census method (26).
A demographic characteristics questionnaire was initially completed, including age, sex, marital status, education, related ward, work experience, and monthly income.
Then, the PMT questionnaire was completed. It included three parts: knowledge and behavior, PMT constructs, and vaccination behavior. Knowledge questions included 15 questions based on a 5-point Likert scale (strongly agree, agree, no opinion, disagree, and strongly disagree) regarding knowledge of preventive behaviors against respiratory infections. Behavior questions included nine questions based on a 5-point Likert scale (strongly agree, agree, no opinion, disagree, and strongly disagree) regarding the preventive behaviors of respiratory infections.
In the PMT constructs section, perceived sensitivity, perceived severity, perceived response cost, perceived reward, and perceived self-efficacy were assessed. Perceived sensitivity was evaluated using four questions based on a 5-point Likert scale (strongly agree, agree, no opinion, disagree, and strongly disagree) regarding the subjects’ perceptions of the preventive behaviors of respiratory infections. The lowest and highest scores were 8 and 40, respectively.
Perceived severity was evaluated using seven questions based on a 5-point Likert scale (strongly agree, agree, no opinion, disagree, and strongly disagree) regarding the subjects’ perceptions of the preventive behaviors of respiratory infections. The lowest and highest scores were 6 and 25, respectively. Perceived response cost was evaluated using six questions based on a 5-point Likert scale (strongly agree, agree, no opinion, disagree, and strongly disagree) regarding the subjects’ perceptions of the preventive behaviors of respiratory infections. The lowest and highest scores were 5 and 30, respectively.
Perceived reward was evaluated using five questions based on a 5-point Likert scale (strongly agree, agree, no opinion, disagree, and strongly disagree) regarding the subjects’ perceptions of the preventive behaviors of respiratory infections. The lowest and highest scores were 6 and 25, respectively. Perceived self-efficacy was evaluated using 10 questions based on a 5-point Likert scale (strongly agree, agree, no opinion, disagree, and strongly disagree) regarding the subjects’ ability to perform preventive behaviors for respiratory infections. The lowest and highest scores were 3 and 15, respectively.
Lastly, the vaccination questionnaire was designed based on similar studies, including Salimi et al. (27), Kashmiri et al. (28), Rahimi et al. (29), and Fakharian Moghadam et al. (30). This part included 17 questions based on a 5-point Likert scale (strongly agree, agree, no opinion, disagree, strongly disagree) regarding the subjects’ perception of vaccination. The lowest and highest scores were 7 and 40, respectively.
The questionnaire was based on a study by Bashirian et al., whose validity and reliability were confirmed (26). In the present study, content validity was confirmed using the opinions of 10 health education and promotion specialists, and internal consistency methods were used to measure the reliability of the tool. Using SPSS version 24, the Cronbach’s alpha coefficient was determined for the entire questionnaire. Cronbach’s alpha coefficient for perceived sensitivity, severity, self-efficacy, response cost, and behavior motivation was measured as 0.86, 0.88, 0.86, 0.85, 0.83, and 0.86, respectively. The coefficient for the entire questionnaire was measured at 0.87.
Upon receipt of the code of ethics from the ethics commission, the researchers commenced their job, and individuals who met the criteria for participation in the study were selected. The researchers provided a detailed explanation of the project’s objectives to the prospective participants, who expressed their interest in taking part. Subsequently, these individuals were admitted into the study upon completion of their written informed consent. Following this, the participants were administered questionnaires, which were subsequently completed by the selected sample population. The individual in question established the designation for the intervention cohort after revisiting the hospital to extend invitations to the members of said cohort. During this encounter, the individual provided a comprehensive explanation about the training sessions, their objectives, and the designated location for the meetings. Furthermore, the individuals were cordially invited to actively partake in these gatherings. The researchers subsequently facilitated the scheduling of sessions in collaboration with the retraining unit within the aforementioned center, with the assistance of a health expert and a health promotion expert. Following the educational intervention, the questionnaires were gathered after a period of two months.
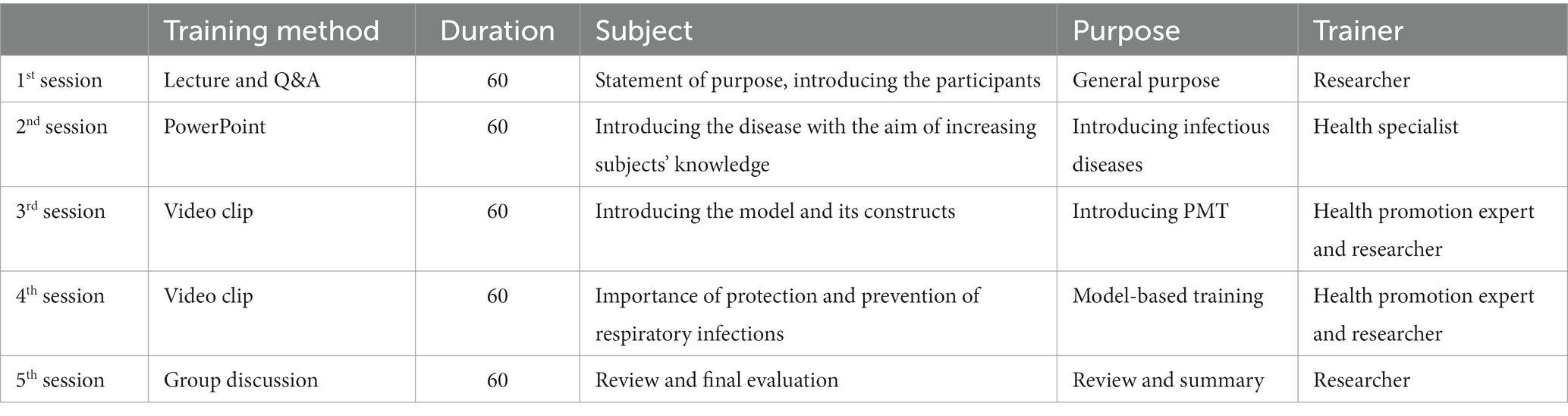
To design the intervention, first a PMT questionnaire was completed by the participants. Then, after finding the weaknesses and strengths of the participants, the educational design was developed based on their weak points. Finally, the intervention included five 60-min sessions and was considered in the form of teaching methods (lectures, questions and answers, group discussions, PowerPoint presentations, pamphlets, and video clips) in the retraining center of health programs in Gachsaran City under the supervision of the health network to instruct behaviors to prevent respiratory infections in the intervention group. Two months after the intervention, the data was collected again and compared with before the intervention. During intervention, an expert group, including a health expert and a health promotion expert, collaborated; each of them specialized in training items related to the PMT.
The data was analyzed by SPSS version 24 statistical software, so that the normality of the data was first measured through the Kolmogorov–Smirnov test. Frequency, mean, and standard deviation indexes were used to describe the data, and independent t-test, chi-square test, and paired t-test were used to compare the average data in the two groups before and after the intervention. The significance level was considered to be 0.05 in all tests.
Table 1 shows the demographic characteristics of the hospital staff participating in the study. The mean and standard deviation of the subjects’ ages in the experimental and control groups were 38.19 ± 3.01 and 37.88 ± 4.12 years, respectively. The mean and standard deviation of work experience in the experimental and control groups were 7.14 ± 3.51 and 7.33 ± 4.12 years, respectively. Based on the independent t-test, there was no significant difference between the two groups in terms of age (p = 0.45) or work experience (p = 0.66). Likewise, based on the results of the chi square test, there was no significant difference between the experimental and control groups in terms of gender (p = 0.54), marital status (p = 0.18), education (p = 0.11), related ward (p = 0.35), and monthly income (p = 0.16) (Table 1).
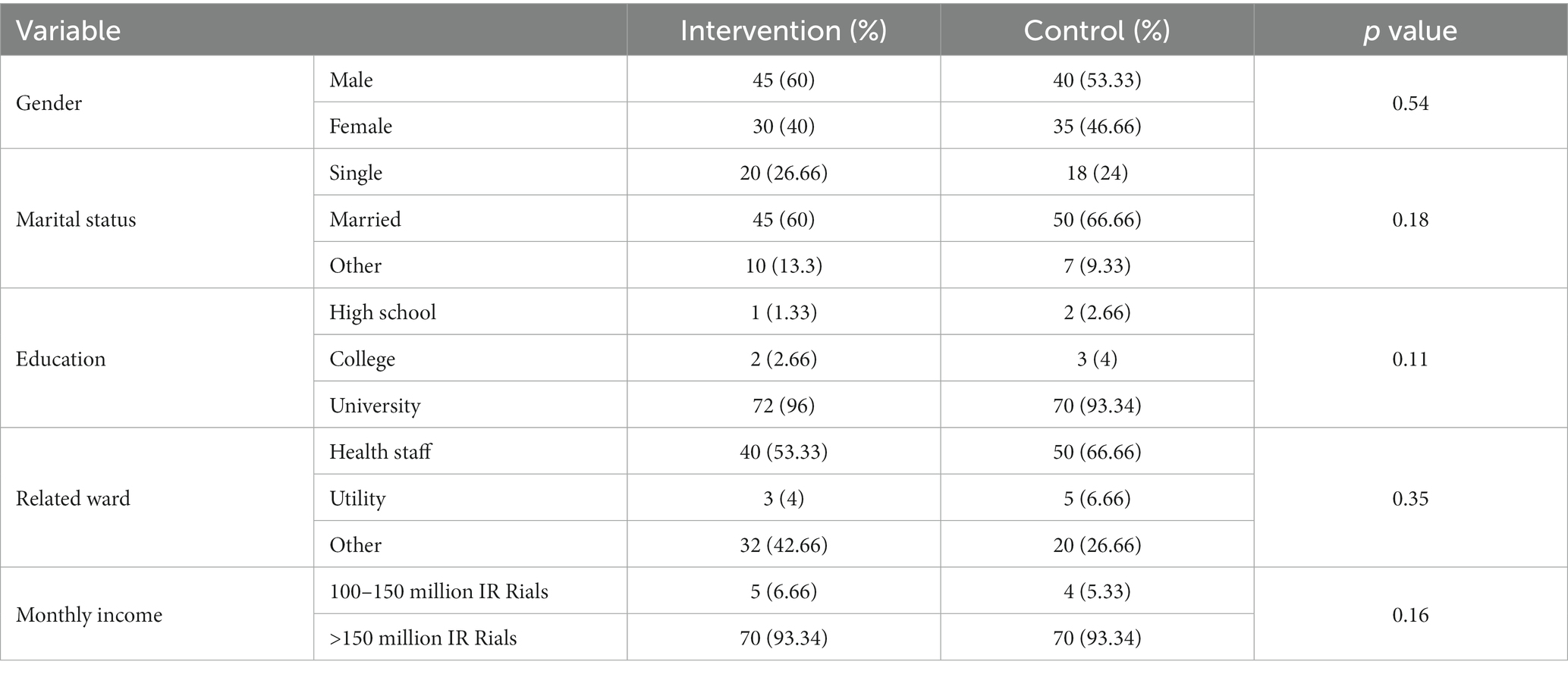
Table 1. Frequency distribution of primary variables of the study participants.
Table 2 shows the subjects’ knowledge of respiratory infections. Most of the participants in the two groups (96% of the experimental group and 93.33% of the control group) had received training about respiratory infections, and most of them (97.33% of the experimental group and 96% of the control group) had received the COVID-19 vaccine. Most of the participants (60% of the experimental group and 66.66% of the control group) mentioned the Internet as their main source of information.
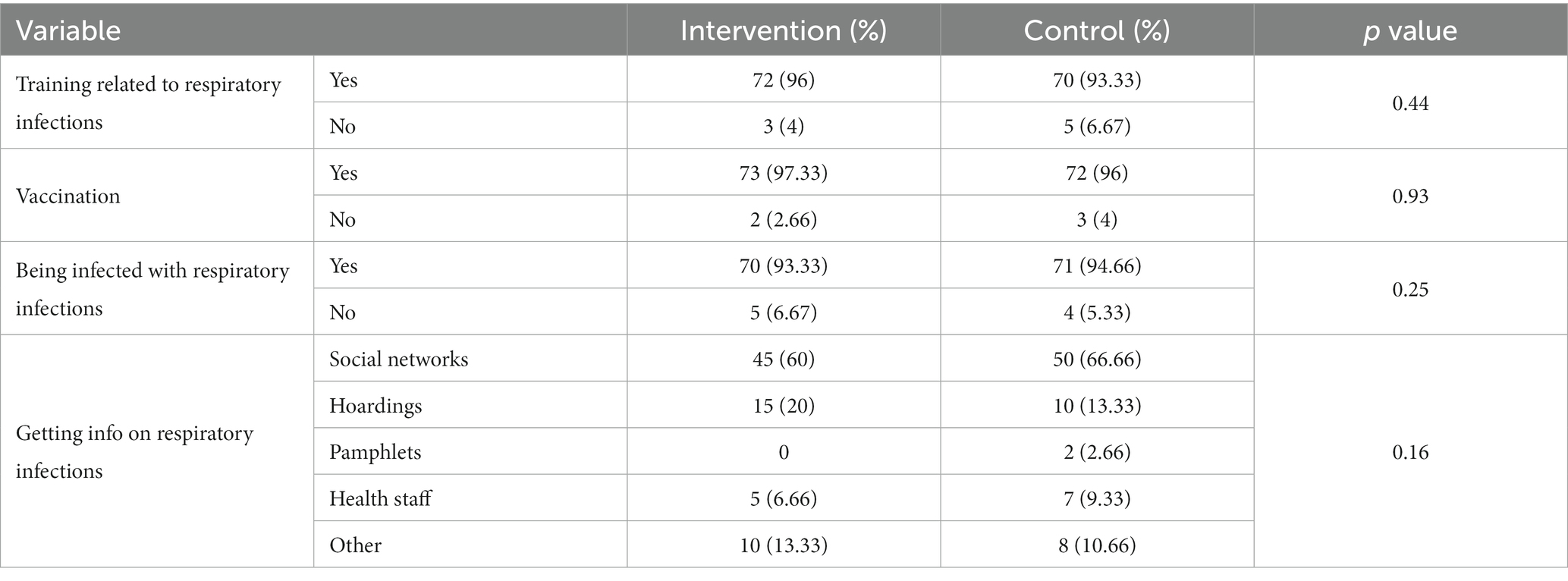
Table 2. Frequency distribution of the participants’ knowledge about respiratory infections.
Table 3 shows the mean and standard deviation of the PMT constructs before and after the intervention in the two experimental and control groups. Based on the results, there was no significant difference between the two groups before the intervention in terms of perceived sensitivity (p = 0.25), perceived severity (p = 0.63), perceived response (p = 0.32), perceived reward (p = 0.11), perceived self-efficacy (p = 0.84), perceived response cost (p = 0.33), fear (p = 0.45), behavior motivation (p = 0.51), knowledge (p = 0.92), behavior (p = 0.12), and vaccination behavior (p = 0.35). However, after the intervention, there was a significant difference between the two groups in terms of perceived sensitivity, perceived severity, perceived response, perceived reward, perceived self-efficacy, perceived response cost, fear, behavior motivation, knowledge, behavior, and vaccination behavior (p < 0.001).
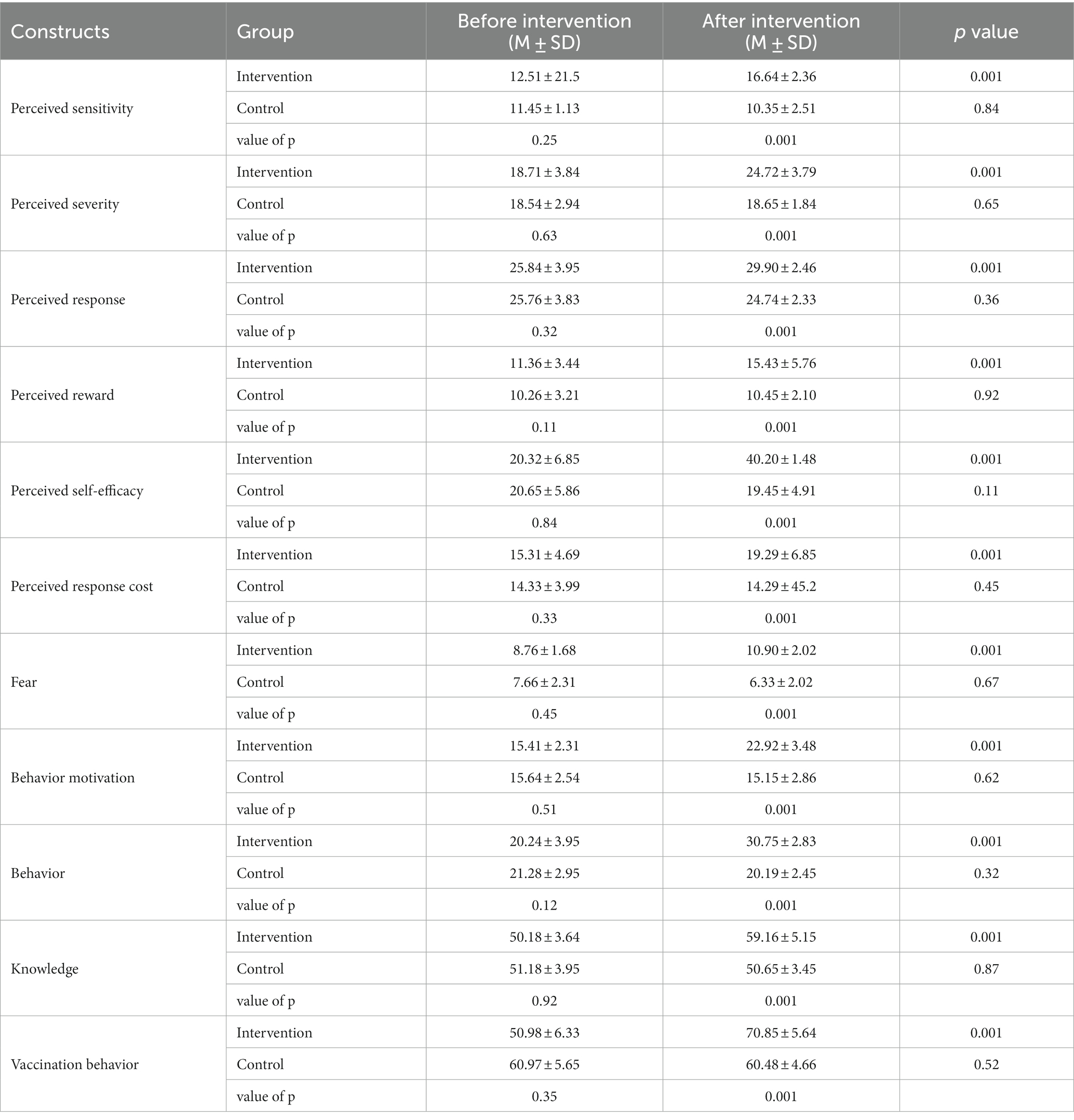
Table 3. Mean and standard deviation of PMT constructs before and after the intervention.
The present study was conducted with the aim of determining the effect of an educational intervention based on the PMT on the preventive behaviors of respiratory infections in a group of hospital staff in Gachsaran City. The results of the present study showed that, after the educational intervention, there was a significant difference between the experimental and control groups in terms of perceived sensitivity. The mean of this construct in the experimental group was higher than in the control group, which could somehow be attributed to the training. In justification of this, in addition to the training given based on the PMT, due to the coincidence of the study with the pandemic, the participants became more sensitive to infectious diseases and took more preventive measures against infectious diseases. This finding was consistent with the results of studies by Nguyen et al. (31)and Ryu et al. (32).
The results of the present study showed that after the intervention, there was a significant difference between the experimental and control groups in terms of perceived severity. The mean of this construct in the experimental group was higher than the control group. One of the possible reasons for this issue is that when people feel vulnerable about something, they try hard to refrain from doing it; the same is the case with infectious diseases (33). In this way, when a person understands his vulnerability, he tries to prevent the disease by observing a series of health principles. These results were consistent with the results of studies by Byrd et al. (34) and Khaday et al. (35).
The results of the present study showed that after the educational intervention, there was a significant difference between the experimental and control groups in terms of perceived response. The mean of this construct in the experimental group was higher than the control group, which is consistent with the results of studies by Grano et al. (36) aimed at the application of PMT in COVID-19 (2022), and Nawabi et al. (37).
Our results showed that after the intervention, there was a significant difference between the experimental and control groups in terms of perceived reward. The mean of this construct in the experimental group was higher than the control group. In justification of this finding, it can be stated that training based on the PMT can make the learner aware of the reward they receive as a result of protection; in other words, they accept that there is a reward in doing so. Regarding infectious diseases, hospital staff are well aware that by observing health and protection issues, there is safety against infectious diseases. This could be the reward itself. These findings are in agreement with the results of studies by Hedayati et al. (38) and Elgzar et al. (39).
Based on our results, after the intervention, there was a significant difference between the experimental and control groups in terms of perceived self-efficacy. The mean of this construct in the experimental group was higher than the control group. When a person does not have the necessary self-efficacy, they cannot observe their preventive behaviors and are exposed to respiratory infections (40). Consistently, in a meta-analysis by Zaildo et al. (41), they stated many obstacles and benefits for preventing respiratory infections (41).
According to the findings, after the educational intervention, there was a significant difference between the experimental and control groups in terms of perceived response cost. It can be said that perceived response cost is an important factor in preventing respiratory infections. It is natural that people seek to reduce unnecessary costs, and preventing respiratory infections can be an unwanted cost. These findings are in line with the results of studies by Calcagni et al. (42) and Lapoirie et al. (43).
The results of the present study showed that after the educational intervention, there was a significant difference between the experimental and control groups in terms of behavior motivation. For the possible justification of this finding, it can be stated that motivation is an important factor in performing a healthy behavior, and the main factor in performing a healthy behavior or leaving an unhealthy behavior is actually motivation. Consistently, the results of studies by Yoon et al. (44), Acar et al. (45), Meng et al. (46), and Leung et al. (47) reported similar findings in improving behavior in their studied groups (44–47).
Our results noted that after the educational intervention, there was a significant difference between the experimental and control groups in terms of fear, and the mean of this construct was higher in the experimental group than the control group, which is consistent with the results of studies by Howell et al. (48), Downing et al. (49), and Hodge et al. (50).
Our findings indicated that after the educational intervention, there was a significant difference between the experimental and control groups in terms of knowledge. It can be stated that the nature of education is that it makes a person aware of the subject that is taught to him; on the other hand, hospital staff have passed training courses on respiratory diseases and are fully aware of these diseases. The influence of education on knowledge and knowledge is similarly reported in the studies by Unger et al. (36), Grano et al. (51), and Abdel-Aziz et al. (52).
Finally, the outcomes of the present study highlighted that after the educational intervention, there was a significant difference between the experimental and control groups in terms of vaccination behavior. The present study coincided with COVID-19, when the only way to prevent the disease was to receive a vaccine. Therefore, the hospital staff, through the training provided by the researcher and other means, were fully aware of receiving the vaccine. Also, since vaccination was mandatory, the employees were forced to receive it. The efficacy of education on vaccination behavior was similarly reported in the studies by Hadizadeh et al. (6), Prince et al. (53), and Wu et al. (54).
The study exhibits several notable strengths. Firstly, it demonstrates active engagement from the hospital staff in the study’s execution. Secondly, the questionnaire employed encompasses all relevant questions pertaining to the idea of protection. Moreover, the education initially targeted the weak points of the participants for more efficacy. Lastly, it is worth mentioning that the researcher was present throughout all stages of data collection.
The short-term evaluation of the impact of the educational program and the data collection via questionnaires, which were collected using a self-reporting method, were subject to certain limitations. One limitation relates to the potential inaccuracies and lack of authenticity in the information provided by some participants. Additionally, the specific cultural context present in Gachsaran City limited the generalizability of the findings to other places.
The results of the present study showed that the use of PMT was able to lead to a change in constructs such as perceived sensitivity, perceived severity, knowledge, and behavior motivation in employees toward respiratory diseases, so it can be suggested that educational interventions aimed at applying the PMT be implemented in the case of other diseases. In the same way, it is possible to teach compliance with health issues using this model in staff retraining courses.
The data that support the findings of this study are available from the corresponding author upon reasonable request.
The studies involving humans were approved by the Human Research Ethics Committee at the Shiraz university of medical sciences (IRSUMS.SCHEANUT.REC.1400.077). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
TR: Conceptualization, Investigation, Methodology, Project administration, Supervision, Visualization, Writing – review & editing. SN: Conceptualization, Methodology, Writing – review & editing, Data curation, Formal analysis, Software, Writing – original draft. SK: Conceptualization, Methodology, Writing – original draft, Project administration, Supervision, Visualization. AK: Conceptualization, Supervision, Visualization, Investigation, Resources, Software, Validation, Writing – review & editing. PH: Conceptualization, Investigation, Resources, Software, Supervision, Validation, Visualization, Writing – review & editing, Data curation, Formal analysis, Methodology. AJ: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Resources, Supervision, Validation, Visualization, Writing – review & editing, Project administration, Writing – original draft.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This study was approved by the Shiraz University of Medical Sciences.
Our warm thanks go to the Research and Technology Dept. of Shiraz University of Medical Sciences, as well as health personnel of Abadan city for their participation in the study.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
PMT, Protection Motivation Theory.
1. Murarkar, S, Gothankar, J, Doke, P, Dhumale, G, Pore, PD, Lalwani, S, et al. Prevalence of the acute respiratory infections and associated factors in the rural areas and urban slum areas of western Maharashtra, India: a community-based cross-sectional study. Front Public Health. (2021) 9:723807. doi: 10.3389/fpubh.2021.723807
2. Chen, N, Zhou, M, Dong, X, Qu, J, Gong, F, Han, Y, et al. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: a descriptive study. Lancet. (2020) 395:507–13. doi: 10.1016/S0140-6736(20)30211-7
3. Shakerinejad, G, Navak, T, Hatemzadeh, N, Haghi, M, and Haghigizadeh, MH. Investigating the effect of multimedia education based on the health belief model in preventing COVID-19 in pregnant women. BMC Public Health. (2023) 23:1–8. doi: 10.1186/s12889-022-14965-1
4. Ahmadi Gohari, M, Chegeni, M, Haghdoost, AA, Mirzaee, F, White, L, Kostoulas, P, et al. Excess deaths during the COVID-19 pandemic in Iran. Infect Dis. (2022) 54:909–17. doi: 10.1080/23744235.2022.2122554
5. Yu, Y, Lau, MM, and Lau, JT. Application of the protection motivation theory to understand determinants of compliance with the measure of banning gathering size> 4 in all public areas for controlling COVID-19 in a Hong Kong Chinese adult general population. PLoS One. (2022) 17:e0268336. doi: 10.1371/journal.pone.0268336
6. Wu, F, Yuan, Y, Deng, Z, Yin, D, Shen, Q, Zeng, J, et al. Acceptance of COVID-19 booster vaccination based on the protection motivation theory: a cross-sectional study in China. J Med Virol. (2022) 94:4115–24. doi: 10.1002/jmv.27825
7. Lai, J, Ma, S, Wang, Y, Cai, Z, Hu, J, Wei, N, et al. Factors associated with mental health outcomes among health care workers exposed to coronavirus disease 2019. JAMA Netw Open. (2020) 3:3976. doi: 10.1001/jamanetworkopen.2020.3976
8. Chowdhary, A, Agarwal, K, and Meis, JF. Filamentous fungi in respiratory infections. What lies beyond aspergillosis and Mucormycosis? PLoS Pathog. (2016) 12:e1005491. doi: 10.1371/journal.ppat.1005491
9. Abadi, TSH, Askari, M, Miri, K, and Nia, MN. Depression, stress and anxiety of nurses in COVID-19 pandemic in Nohe-Dey Hospital in Torbat-e-Heydariyeh city. Iran J Military Medicine. (2020) 22:526–33.
10. Sarboozi-Hoseinabadi, T, Askari, M, Miri, K, and Namazi, NM. Depression, anxiety, and stress of Nurses' family members in Covid–19 pandemic; a case study of Torbat-e Heydariyeh hospitals. Iranian J War and Public Health. (2020) 12:241–8. doi: 10.52547/ijwph.12.4.241
11. Baloch, S, Baloch, MA, Zheng, T, and Pei, X. The coronavirus disease 2019 (COVID-19) pandemic. Tohoku J Exp Med. (2020) 250:271–8. doi: 10.1620/tjem.250.271
12. Desforges, M, Le Coupanec, A, Dubeau, P, Bourgouin, A, Lajoie, L, Dubé, M, et al. Human coronaviruses and other respiratory viruses: underestimated opportunistic pathogens of the central nervous system? Viruses. (2019) 12:7–8. doi: 10.3390/v12010014
13. Mehrtash, B, and Siahpoosh, M. A review on epidemiology, pathophysiology and clinical manifestations of covid-19 infection in order to guide policy making and promotion of knowledge, attitude and practice of the society associated with COVID-19. A validity review. (2021) 19:1195–224. doi: 10.29252/jrums.19.11.1195
14. Cirrincione, L, Plescia, F, Ledda, C, Rapisarda, V, Martorana, D, Moldovan, RE, et al. COVID-19 pandemic: prevention and protection measures to be adopted at the workplace. Sustainability. (2020) 12:3603. doi: 10.3390/su12093603
15. Fathi, Y, Barati, M, Zandiyeh, M, and Bashirian, S. Prediction of preventive behaviors of the needlestick injuries during surgery among operating room personnel: application of the health belief model. The intern J occupational and environmental med. (2017) 8:232–40. doi: 10.15171/ijoem.2017.1051
16. Liu, C-Y, Yang, Y-z, Zhang, X-M, Xu, X, Dou, Q-L, Zhang, W-W, et al. The prevalence and influencing factors in anxiety in medical workers fighting COVID-19 in China: a cross-sectional survey. Epidemiol & Infection. (2020) 148:148. doi: 10.1017/S0950268820001107
17. Wu, Z, and McGoogan, JM. Characteristics of and important lessons from the coronavirus disease 2019 (COVID-19) outbreak in China: summary of a report of 72 314 cases from the Chinese Center for Disease Control and Prevention. JAMA. (2020) 323:1239–42. doi: 10.1001/jama.2020.2648
18. Rahman, I, Nanu, L, Bernard, S, and Liu, S. Does perceived control matter in the early days of COVID-19 in USA? A protection motivation approach examining hospitality and tourism service patronage. Int J Hosp Tour Adm. (2022) 1-27:1–27. doi: 10.1080/15256480.2022.2142995
19. Al-Rasheed, M. Protective behavior against COVID-19 among the public in Kuwait: an examination of the protection motivation theory, trust in government, and sociodemographic factors. Soc Work Public Health. (2020) 35:546–56. doi: 10.1080/19371918.2020.1806171
20. Norman, P, Boer, H, Seydel, ER, and Mullan, B. Protection motivation theory. Predicting and changing health behaviour: Research and practice with social cognition models. (2015) 3:70–106.
21. Tanner, JF Jr, Hunt, JB, and Eppright, DR. The protection motivation model: a normative model of fear appeals. J Mark. (1991) 55:36–45. doi: 10.1177/002224299105500304
22. Ezati Rad, R, Mohseni, S, Kamalzadeh Takhti, H, Hassani Azad, M, Shahabi, N, Aghamolaei, T, et al. Application of the protection motivation theory for predicting COVID-19 preventive behaviors in Hormozgan, Iran: a cross-sectional study. BMC Public Health. (2021) 21:1–11. doi: 10.1186/s12889-021-10500-w
23. Kowalski, RM, Deas, N, Britt, N, Richardson, E, Finnell, S, Evans, K, et al. Protection motivation theory and intentions to receive the COVID-19 vaccine. Health Promot Pract. (2023) 24:465–70. doi: 10.1177/15248399211070807
24. Ekow Arkorful, V, Kweku Lugu, B, Shuliang, Z, and Mamley, CS. Investigating COVID-19 vaccine uptake intention using an integrated model of protection motivation theory and an extended version of the theory of planned behavior. Health Commun. (2023) 1-14:1–14. doi: 10.1080/10410236.2023.2201730
25. Salmani, B, and Prapavessis, H. Using a protection motivation theory framework to reduce vaping intention and behaviour in Canadian university students who regularely vape: a randomized controlled trial. J Health Psychol. (2023) 28:832–45. doi: 10.1177/13591053221144977
26. Bashirian, S, Jenabi, E, Khazaei, S, Barati, M, Karimi-Shahanjarini, A, Zareian, S, et al. Factors associated with preventive behaviours of COVID-19 among hospital staff in Iran in 2020: an application of the protection motivation theory. J Hosp Infect. (2020) 105:430–3. doi: 10.1016/j.jhin.2020.04.035
27. Salimi, Y, Paykani, T, Ahmadi, S, Shirazikhah, M, Almasi, A, Biglarian, A, et al. Covid-19 vaccine acceptance and its related factors in the general population of Tehran and Kermanshah. Iran J Epidemiol. (2021) 16:1–9.
28. Keshmiri, S, Darabi, AH, Tahmasebi, R, Vahdat, K, and Noroozi, A. Factors influencing COVID-19 vaccine acceptance based on the behavioral change wheel model in Bushehr province in 2021: a web-based study. HAYAT. (2021) 27:190–205.
29. Rahimi Kahkashi, S, and Adeli, OA. Knowledge and attitude of Iranian people towards COVID-19 vaccines and related factors. J Modern Medical Information Sciences. (2022) 8:36–47.
30. Fakharian Moghaddam, S, Ahi, Q, and Moharreri, F. Fear of Covid-19 and the desire to get vaccinated Covid 19: the mediating role of complacency and perceived effectiveness of the COVID-19 vaccine. J Res Behavioural Sci. (2023) 20:760–74. doi: 10.52547/rbs.20.4.15
31. Nguyen, DT, Tran, VD, and Ghafoor, A. The impact of covid-19 lockdown on intention to follow preventive measures in Vietnam: integrated protection motivation theory and theory planed behavior. Cogent Business & Management. (2022) 9:2054502. doi: 10.1080/23311975.2022.2054502
32. Ryu, K, Jarumaneerat, T, Promsivapallop, P, and Kim, M. What influences restaurant dining out and diners’ self-protective intention during the COVID-19 pandemic: applying the protection motivation theory. Int J Hosp Manag. (2023) 109:103400. doi: 10.1016/j.ijhm.2022.103400
33. Tagini, S, Brugnera, A, Ferrucci, R, Mazzocco, K, Compare, A, Silani, V, et al. It won't happen to me! Psychosocial factors influencing risk perception for respiratory infectious diseases: a scoping review. Appl Psychol Health Well Being. (2021) 13:835–52. doi: 10.1111/aphw.12274
34. Byrd, K, Fan, A, Her, E, Liu, Y, Leitch, S, and Almanza, B. Restaurant patronage during the COVID-19 pandemic and the protection motivation theory: influence of consumers’ socio-demographic, situational, and psychographic factors. J Foodserv Bus Res. (2023) 26:247–75. doi: 10.1080/15378020.2021.2006036
35. Khaday, S, Li, K-W, and Dorloh, H, Factors affecting preventive behaviors for safety and health at work during the COVID-19 pandemic among Thai construction workers. In Healthcare (2023) 11, (3) 426. MDPI.
36. Grano, C, Singh Solorzano, C, and Di Pucchio, A. Predictors of protective behaviours during the Italian COVID-19 pandemic: an application of protection motivation theory. Psychol Health. (2022) 37:1584–604. doi: 10.1080/08870446.2022.2062355
37. Navabi, ZS, Ahmadi, A, Sabri, MR, Kholenjani, FB, Ghaderian, M, Dehghan, B, et al. Factors associated with preventive behaviors of COVID-19 among children with congenital heart disease: application of protection motivation theory. J Educ Health Promotion. (2022) 11:332. doi: 10.4103/jehp.jehp_1720_21
38. Hedayati, S, Damghanian, H, Farhadinejad, M, and Rastgar, AA. Meta-analysis on application of protection motivation theory in preventive behaviors against COVID-19. Intern J Disaster Risk Reduction. (2023) 94:103758. doi: 10.1016/j.ijdrr.2023.103758
39. Elgzar, WT, Sayed, SH, Hussien, NK, and Allam, TH. The effect of an educational intervention based on protection motivation theory on pregnant Women’s knowledge and self-protection regarding COVID-19. An intervention study. Iranian journal of nursing and midwifery. Research. (2023) 28:264–72.
40. Mahmood, QK, Jafree, SR, Mukhtar, S, and Fischer, F. Social media use, self-efficacy, perceived threat, and preventive behavior in times of COVID-19: results of a cross-sectional study in Pakistan. Front Psychol. (2021) 12:562042. doi: 10.3389/fpsyg.2021.562042
41. Zaildo, T, Santino, TA, Chaves, G, da Silva, BAK, Alchieri, JC, Patino, CM, et al. Barriers to and facilitators of populational adherence to prevention and control measures of COVID-19 and other respiratory infectious diseases: a qualitative evidence synthesis. Eur Respir Rev. (2023) 32:220238. doi: 10.1183/16000617.0238-2022
42. Calcagni, N, Venier, A-G, Nasso, R, Boudin, G, Jarrige, B, Parneix, P, et al. Respiratory infection prevention: perceptions, barriers and facilitators after SARS-CoV-2. Infection, Disease & Health. (2023) 28:54–63. doi: 10.1016/j.idh.2022.08.001
43. Martin-Lapoirie, D, D’onofrio, A, McColl, K, and Raude, J. Testing a simple and frugal model of health protective behaviour in epidemic times. Epidemics. (2023) 42:100658. doi: 10.1016/j.epidem.2022.100658
44. Yoon, H, You, M, and Shon, C. An application of the extended parallel process model to protective behaviors against COVID-19 in South Korea. PLoS One. (2022) 17:e0261132. doi: 10.1371/journal.pone.0261132
45. Acar, D, and Kıcali, ÜÖ. An integrated approach to COVID-19 preventive behaviour intentions: protection motivation theory, information acquisition, and trust. Soc Work Public Health. (2022) 37:419–34. doi: 10.1080/19371918.2021.2018082
46. Meng, G, Li, Q, Yuan, X, Zheng, Y, Hu, K, Dai, B, et al. The roles of risk perception, negative emotions and perceived efficacy in the association between COVID-19 infection cues and preventive behaviors: a moderated mediation model. BMC Public Health. (2023) 23:1–10. doi: 10.1186/s12889-022-14870-7
47. Leung, M-W, O’Donoghue, M, and Suen, LK-P. Personal and household hygiene measures for preventing upper respiratory tract infections among children: a cross-sectional survey of parental knowledge, attitudes, and practices. Int J Environ Res Public Health. (2022) 20:14. doi: 10.3390/ijerph20010229
48. Howell, P, and Abdelhamid, M. Protection motivation perspective regarding the use of COVID-19 Mobile tracing apps among public users: empirical study. JMIR Formative Research. (2023) 7:e36608. doi: 10.2196/36608
49. Downing, ST, Mccarty, RJ, Guastello, AD, Cooke, DL, and Mcnamara, JP. Assessing the predictors of adaptive and maladaptive Covid-19 preventive behaviours: an application of protection motivation theory. Psychol Health Med. (2023) 28:460–74. doi: 10.1080/13548506.2022.2093925
50. Hodge, DP. Motivations of collegiate student-athletes to protect against COVID-19: An application of protection motivation theory Troy, Alabama: Troy University (2022).
51. Unger, JB, Herzig, E, Rodriguez, V, Soto, D, Lee, R, and Sood, N. Application of protection motivation theory to COVID-19 vaccination among a predominantly Hispanic sample of adolescents. Prev Med Rep. (2023) 34:102245. doi: 10.1016/j.pmedr.2023.102245
52. Abdel-Aziz, HR, and Atia, NS. Respiratory infections prevention in rural older adults: an interventional study. Clin Nurs Res. (2022) 31:1445–53. doi: 10.1177/10547738221081981
53. Hadizadeh-Talasaz, F, Mohammadzadeh, F, and Noghabi, AD. Predictors of the social distancing behaviors during the COVID-19 pandemic using protection motivation theory in Iran: a cross sectional study. J Prev Med Hyg. (2022) 63:E35–43. doi: 10.15167/2421-4248/jpmh2022.63.1.2228
Keywords: educational intervention, preventive behaviors, respiratory infections, respiratory infections, protection motivation theory
Citation: Rakhshani T, Nikeghbal S, Kashfi SM, Kamyab A, Harsini PA and Jeihooni AK (2024) Effect of educational intervention based on protection motivation theory on preventive behaviors of respiratory infections among hospital staff. Front. Public Health. 11:1326760. doi: 10.3389/fpubh.2023.1326760
Edited by:
Nicolas Vignier, Université Sorbonne Paris Nord, FranceReviewed by:
Vishnunarayan Girishan Prabhu, University of North Carolina at Charlotte, United StatesCopyright © 2024 Rakhshani, Nikeghbal, Kashfi, Kamyab, Harsini and Jeihooni. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ali Khani Jeihooni, S2hhbmlfMTUxMkB5YWhvby5jb20=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.