
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health , 11 January 2024
Sec. Public Health and Nutrition
Volume 11 - 2023 | https://doi.org/10.3389/fpubh.2023.1326418
This article is part of the Research Topic Dietary and Nutrigenetic Contributors to Metabolic Syndrome View all 8 articles
 Noara Alhusseini1
Noara Alhusseini1 Nawra Alsinan1
Nawra Alsinan1 Shahad Almutahhar1Majd Khader1Rawand Tamimi1Mazin Ibrahim Elsarrag1Rabah Warar1Sara Alnasser1,2Majed Ramadan3,4
Shahad Almutahhar1Majd Khader1Rawand Tamimi1Mazin Ibrahim Elsarrag1Rabah Warar1Sara Alnasser1,2Majed Ramadan3,4 Aamir Omair5
Aamir Omair5 Sihem Aouabdi6*
Sihem Aouabdi6* Rimah Saleem1
Rimah Saleem1 Alaa Alabadi-Bierman7,8
Alaa Alabadi-Bierman7,8Introduction: Dietary habits in Saudi Arabia have been shifting toward the Western diet, which is high in fat, salt, and sugar, leading to a high obesity rate. Different dietary strategies such as the Ketogenic Diet (KD), Intermittent Fasting (IF), Gluten Free Diet (GFD), and Calorie Restriction Diet (CRD) have shown an influential role in weight loss. This study aimed to compare trending diets and correlate different types of diet with obesity and lifestyle among adults in Saudi Arabia.
Methods: A cross-sectional study was performed on Saudis and non-Saudis over 18 years old. We used convenience sampling, an online questionnaire distributed via social media channels, including WhatsApp, LinkedIn, and Twitter. SPSS 28 software was applied for data analysis. The chi-square test was used to determine associations between different variables. Statistical significance was considered at a value of p less than 0.05.
Results: Most participants were females residing in the Eastern and Central regions of Saudi Arabia. Although most do not follow any dietary plan, they exhibited acceptable exercise and lifestyle. The minority of the study population followed different types of diet plans, such as KD, IF, and GFD. The purpose of most of the participants who have used these strategies was for weight loss but failed to sustain the dietary plan for more than 1 month.
Conclusion: Obesity remains a challenging issue in Saudi Arabia. Adherence to dietary regimes could help in controlling obesity. Increasing the awareness of the benefits of each dietary plan for health, choosing the appropriate one, and sustaining a balanced nutrition pattern.
Obesity is a medical condition characterized by the excessive accumulation of body fat to the extent that it may have a negative impact on health. It is often determined by body mass index (BMI), which is a measure of body fat based on a person’s weight and height. BMI is calculated by dividing a person’s weight in kilograms by the square of their height in meters. The World Health Organization (WHO) classifies adults’ BMI into the following categories: Underweight: BMI less than 18.5 kg/m2, Normal weight: BMI 18.5 to 24.9, kg/m2 Overweight: BMI 25 to 29.9 kg/m2, Obesity (Class 1): BMI 30 to 34.9 kg/m2, Obesity (Class 2): BMI 35 to 39.9 kg/m2, Obesity (Class 3 - severe or morbid obesity): BMI of 40 or higher kg/m2 (1). Sedentary behaviors and unhealthy dietary patterns are significant risk factors for obesity. Obesity is associated with an increased risk of type 2 diabetes, hypertension, and cardiovascular disorders. (2, 3). Addressing obesity often involves lifestyle modifications, including adopting a healthy diet, increasing physical activity, and, in some cases, medical interventions. (4, 5).
Obesity is a significant health concern worldwide, and Saudi Arabia is no exception. The prevalence of obesity has been on the rise in Saudi Arabia over the past few decades, with several factors contributing to this trend. Approximately 20% of Saudis are obese, with the majority being older adult married women (6). Urbanization and economic development in Saudi Arabia have led to changes in lifestyle, including increased sedentary behavior and a shift toward more energy-dense diets. These changes, often associated with urban living, have contributed to the obesity epidemic. Obesity rates will likely continue escalating due to the increased dependence on fast food chains, which are high in fat, salt, and sugar (7–9). More than 15,000 bariatric surgeries are performed annually in Saudi Arabia, costing up to 40,000 Saudi Riyals (SAR) for each surgery. Such high obesity rates and chronic conditions cause a burden on the public health and healthcare systems (10). Healthy diet and exercise are cost-effective and positively impact human weight loss and well-being (11). Several dietary strategies have shown a role in weight loss, such as a ketogenetic diet (KD), Intermittent Fasting (IF), Gluten-Free Diet (GFD), and the Calorie Restriction Diet (CRD).
The KD, is a popular diet that has been used since the 1920s to treat epilepsy. It is often referred to as the keto diet, which is a low-carbohydrate, high-fat diet designed to induce a state of ketosis in the body. Ketosis is a metabolic state where the body shifts from using glucose as its primary source of energy to relying on ketones, which are molecules produced from the breakdown of fats. This change in fuel source has various effects on the body, including increased fat burning. The macronutrient distribution in a standard ketogenic diet typically involves three components. High Fat: Approximately 70–75% of total daily calories come from fats. This includes sources like avocados, nuts, seeds, oils, and fatty cuts of meat. Moderate Protein: About 20–25% of calories come from protein. Protein sources include meat, poultry, fish, eggs, and dairy. Low Carbohydrate: Carbohydrates are severely restricted, making up only about 5–10% of total daily calories. This often limits daily carbohydrate intake to around 20–50 grams, depending on individual needs (12). The initial weight loss on a ketogenic diet is often rapid due to water loss associated with glycogen depletion. This can be motivating for some individuals, but it’s essential to differentiate between water weight and actual fat loss. Some people experience reduced appetite when following a ketogenic diet, which can contribute to weight loss. Recent studies using low-carbohydrate, high-fat diets, such as KD, show promising outcomes on weight loss, reversing the symptoms of metabolic syndrome, lowering or eliminating the need for insulin in type II diabetes mellitus, reducing inflammation, improving epigenetic profiles, changing the microbiome, enhancing lipid profiles, and assisting cancer treatment (13).
Another popular diet is intermittent fasting (IF), which relies on consuming food for eating for a specific timeframe followed by fasting for the rest of the day (14). Intermittent fasting (IF) is an eating pattern that cycles between periods of eating and fasting. There are several variations of intermittent fasting, but common methods include the 16/8 method (fasting for 16 h and eating within an 8-h window), the 5:2 method (eating normally for 5 days and significantly reducing calorie intake on two non-consecutive days), and the eat-stop-eat method (24-h fasts once or twice a week). Intermittent fasting can lead to various metabolic changes in the body and some of these changes may include insulin sensitivity. Improved sensitivity means that cells are better able to respond to insulin, which can be beneficial for managing blood sugar levels. Moreover, fasting periods can lead to an increase in the breakdown of fat stores for energy, promoting the process of lipolysis. This can contribute to weight loss and fat reduction. In addition, intermittent fasting may influence lipid profiles, including reducing triglyceride levels and improving cholesterol levels, which could contribute to cardiovascular health (15).
Fasting improves physical and mental performance by increasing metabolic and nervous system activities (16). IF is an effective dietary plan for weight loss and reversing metabolic parameters such as cholesterol, triglycerides, and oxidative stress markers (14, 17).
On the other hand, the GFD constricts the consumption of wheat, barley, and rye sources. This diet relies on gluten-free, food such as eggs, fruits, vegetables, meat, fish, legumes, dairy products, and wheat-based food manufactured without gluten (18). GFD is usually medicated for patients with celiac disease as it improves clinical manifestation and blood parameters (19, 20). Although people who are not suffering from celiac disease use GFD, they are susceptible to nutritional deficiencies such as iron and vitamin B. Adopting a gluten-free diet may impact nutrient intake. Whole grains containing gluten, such as wheat, provide essential nutrients like fiber, B vitamins, and minerals. When removing gluten-containing grains, individuals must ensure they get these nutrients from alternative sources. Some people may experience weight changes when they switch to a gluten-free diet. Various factors, including the types of gluten-free foods chosen, can influence this. Some gluten-free products may be higher in calories, sugar, and fat compared to their gluten-containing counterparts (21).
In addition, the calorie restriction diet (CRD) entails a sustained reduction in daily caloric intake of roughly 25–30% from the average calorie intake (22). The CRD is effective in terms of weight loss and disease risk (23). The most immediate and noticeable effect of a calorie-restricted diet is often weight loss. When the body receives fewer calories than it needs for its daily activities, it starts utilizing stored energy, primarily in the form of glycogen and fat, leading to a reduction in body weight. The Calorie Restriction Society reports that participants who adhere to a self-imposed CRD program have more extended life expectancies. Moreover, caloric restriction may enhance insulin sensitivity, which is the body’s ability to respond to insulin and regulate blood sugar levels. Improved insulin sensitivity is associated with better metabolic health and a reduced risk of type 2 diabetes. (24).
Therefore, this study aimed to describe different diet trends and assess which type of diet correlates with obesity among adults residing in Saudi Arabia. This included exploring the prevalence of KD, IF, GFD, and CRD alongside the correlation between diet trends and obesity and assessing predictors of diet trends among the Saudi population.
This cross-sectional study focused on different diets used among residents of Saudi Arabia. Convenience sampling was used, and the minimum sample size requirement was (n = 384) by a confidence interval of 95% and a 5% margin of error with an expected outcome response of 50%. However, the authors collected (n = 608) responses. The inclusion criteria were adults above 18 years old, including Saudi citizens and Non-Saudi residents at the time of the data collection.
An online survey was distributed via social media channels such as WhatsApp, LinkedIn, Facebook, and Twitter in Arabic and English. Clinical nutrition experts and an official translator achieved face and content validity. The survey included two sections; section 1 comprised demographic questions such as age, gender, nationality, marital status, employment status, educational level, income and residence. Section 2 covered dietary habits-related questions which was categorized into KD, IF, GFD, CRD, and no dietary restrictions. In addition, the mean body mass index (BMI) values were calculated for each group. The SPSS version 28 statistical software was used for data analysis. Frequencies and percentages were applied for data representation. In addition, the Pearson chi-square (χ2) and logistic regression were used to evaluate the potential association between dietary trends and obesity, and potential confounding variables were added to the multivariable model with odds ratios (ORs) and 95% confidence intervals (CIs) reported.
No identifying information, such as names or emails, was collected in this study, and data access was restricted to the authors only. Participation was voluntary, and the consent form was provided to all participants before participation and participants were able to withdraw at any time. The study was conducted upon approval from the Institutional Review Board (IRB) at King Abdullah International Medical Research Center under the reference number NRJ22J/288/11.
The total of 608 participants who responded to the survey were included in this study. We initially assessed the demographic characteristics of the respondents, such as age, gender, nationality, marital status and employment status, employment status, type of qualification, income, and residence. Most of the participants in this study were less than 45 years old, where females (66%) and Saudis (76%) represented the majority of the study population. More than half were married (58%), and the highest proportion were employed (39%). Most participants hold bachelor’s degrees or diplomas, and 32% have no income. Interestingly, the highest number of participants were residing in the eastern region (45%), followed by the central region (44%) of Saudi Arabia (Table 1).
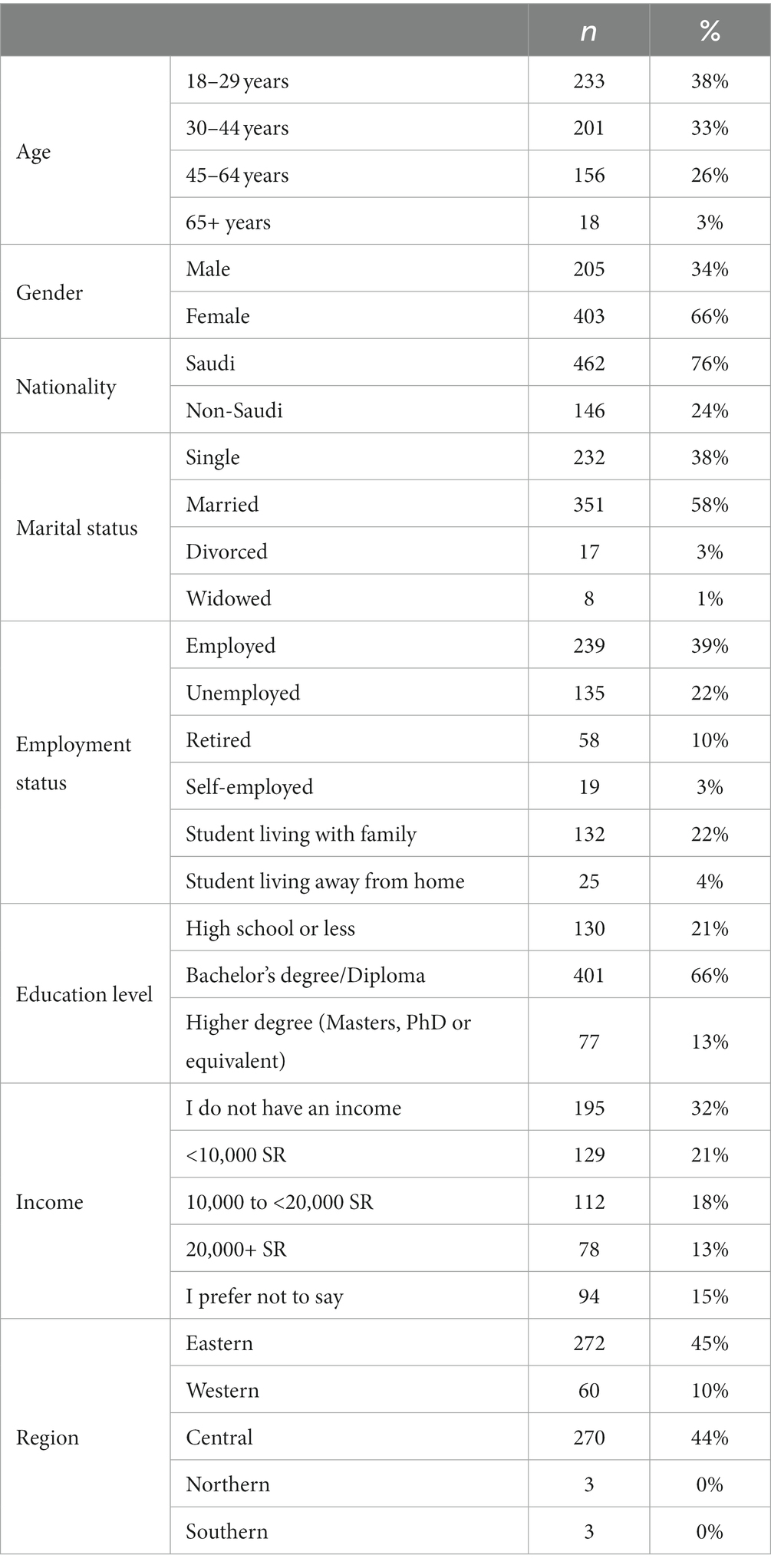
Table 1. Demographic characteristics of the respondents.
The respondents’ BMI was 26.7 ± 5.4 kg/m2, with a range of 14.5 to 48.6 kg/m2. Next, we evaluated exercise and dietary habits, where 30% of the respondents did not exercise, and 45% often followed a balanced diet. In addition, 63% of the participants have fruits and 57% vegetables, about 1–3 times per week. More than half of the study population eat from restaurants (61%), have 2 meals a day (51%), and their last meal is between 7 and 10 pm (61%) (Table 2). Interestingly, 75% of the respondents do not follow any diet plan, while the minority follow intermittent fasting (10%), low-fat diet (8%), and low carbohydrate or Atkins diet (4%) (Table 3).
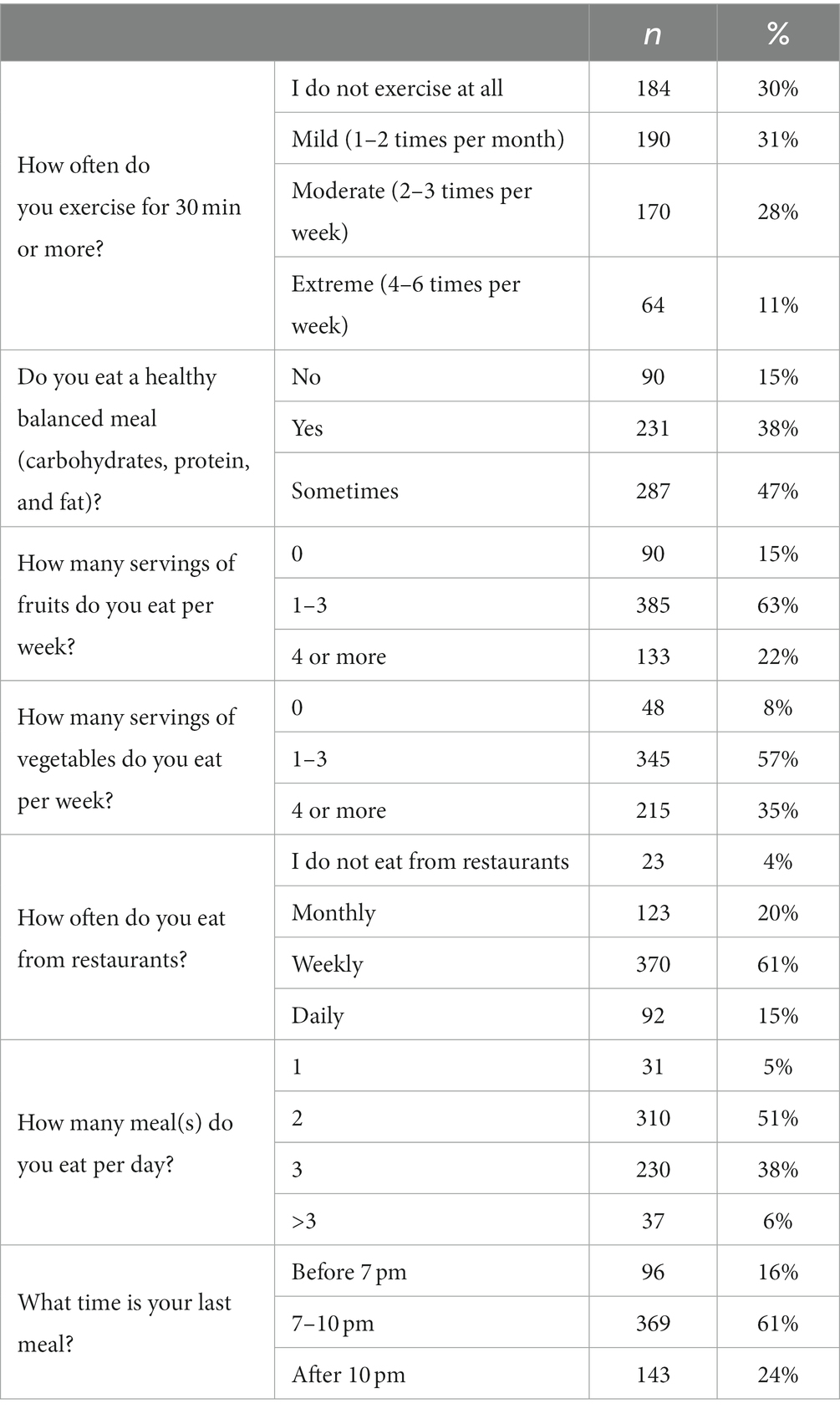
Table 2. Exercise and dietary habits as self-reported by the respondents.
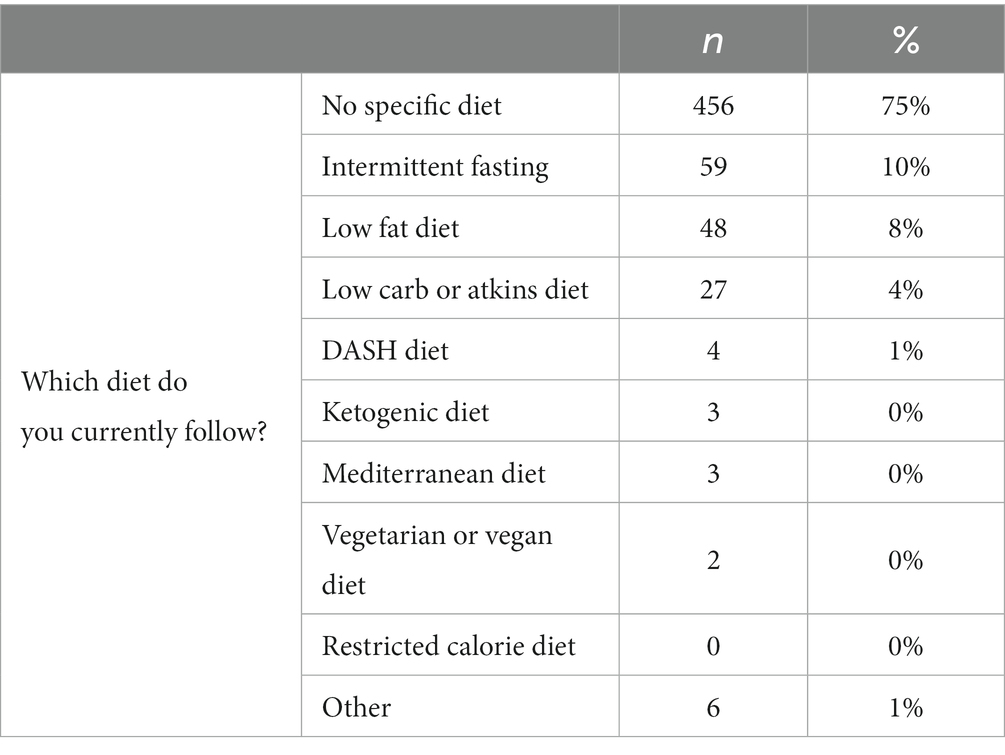
Table 3. Type of diet followed by the respondents.
The majority of this population tried the KD (85%), learned about it from the internet (54%), and primarily followed it for weight loss (84%). However, 52% of the participants have been on the KD for less than a month and tried it once (59%) (Table 4). In addition, 63% of the participants have tried IF and learned about it from the internet (56%). The majority also followed IF for weight loss (75%) and applied this plan for less than 1 month (39%). The fasting pattern was variable as 23% involved 16 h; others used 14 (22%) and 12 h, representing a percentage of 22 and 20%, respectively (Table 5).
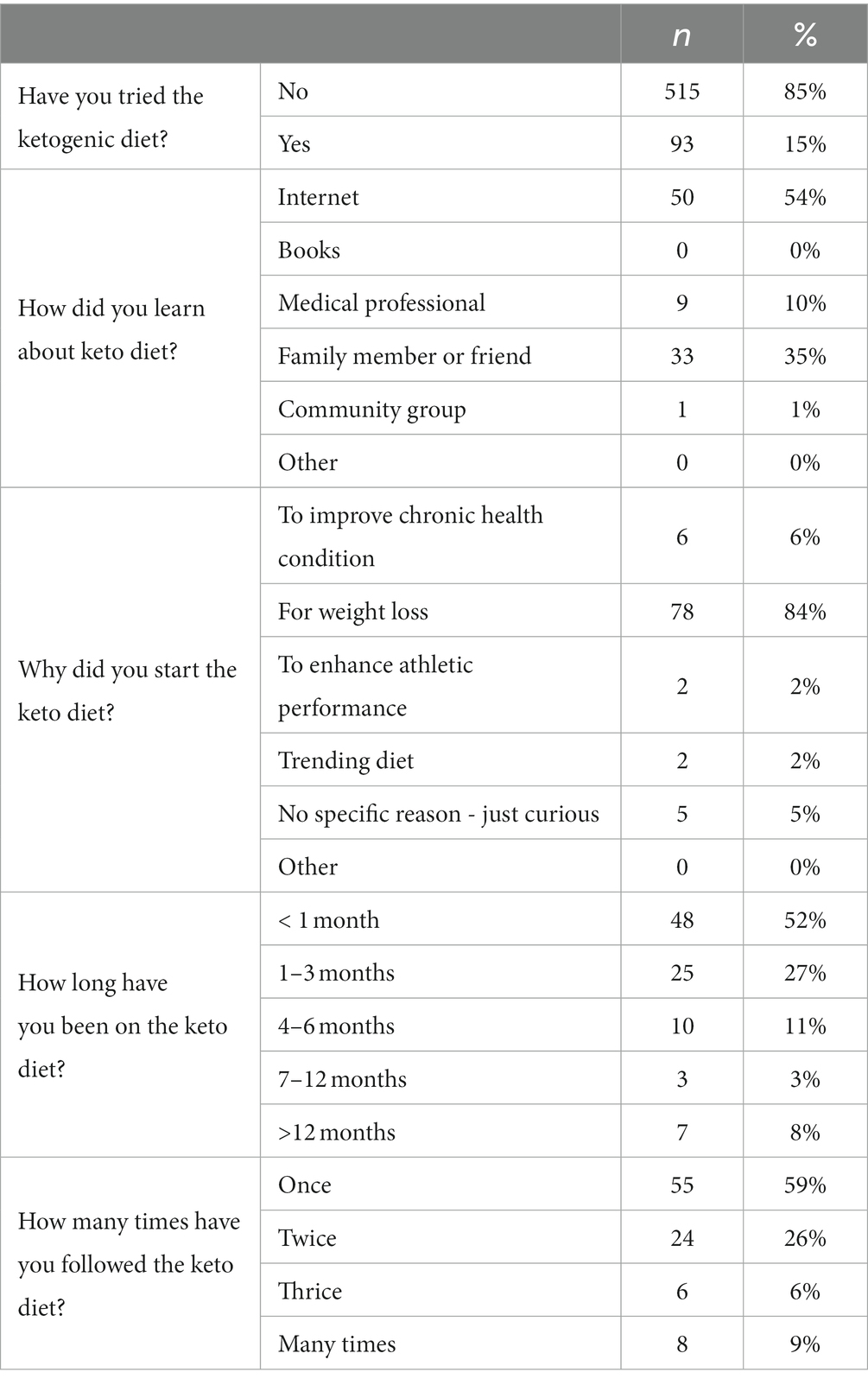
Table 4. Respondents following KD.
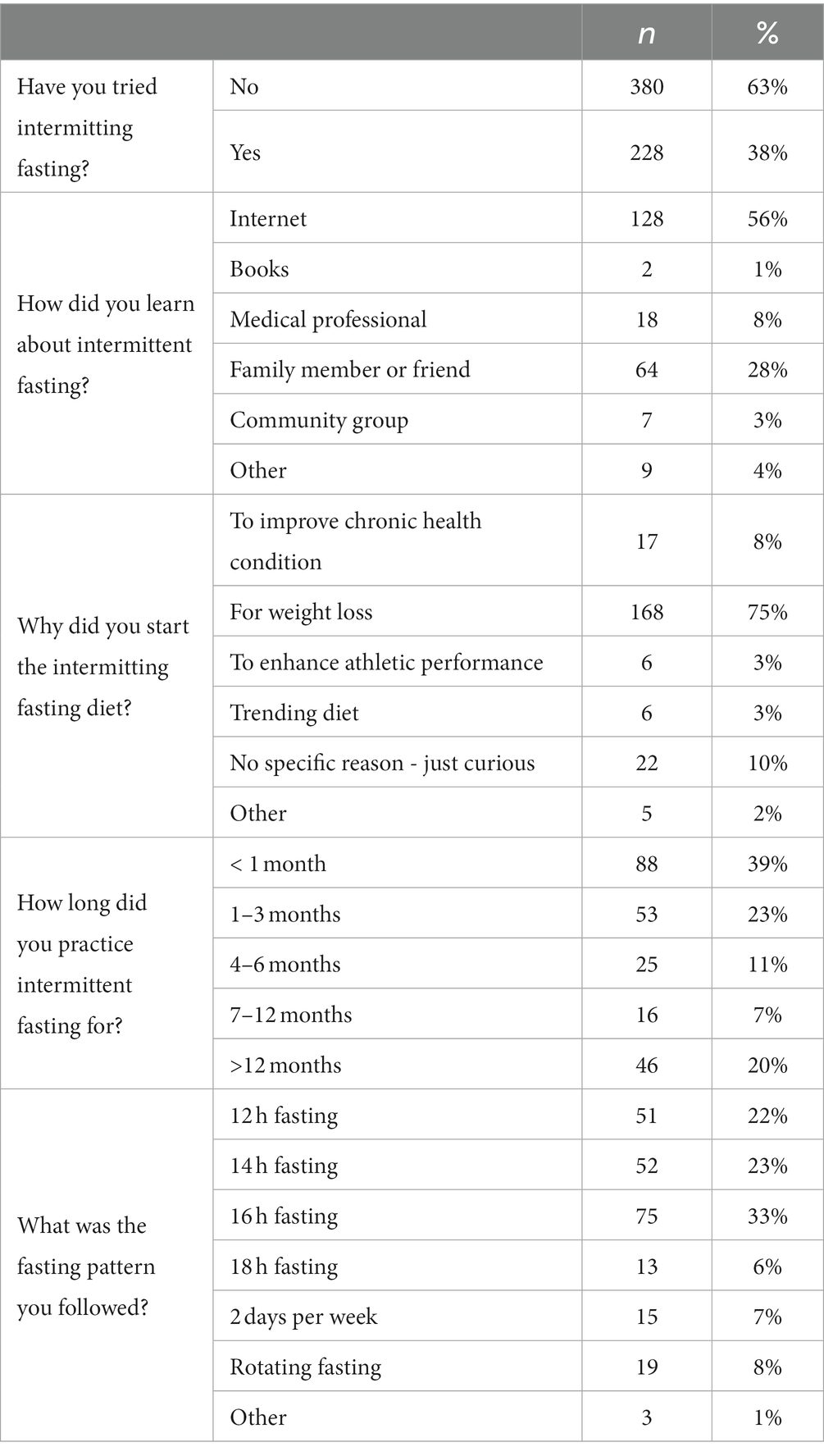
Table 5. Respondents following IF.
Furthermore, 33% of the participants have been on CRD, mostly learned about this diet plan from the internet (45%) and used it for weight loss (85%). This majority of this group either used this dietary strategy for less than 1 month or more than 12 months (Table 6). However, the GFD was the highest percentage of dietary plans the respondents applied (95%). Some participants learned about this dietary plan from the Internet (39%), whereas others learned about it from medical professionals (29%) or family members and friends (25%). Furthermore, the majority applied this dietary plan for different reasons, such as weight loss (25%), celiac disease (11%), or skin allergy (14%). However, 37% used it for less than 1 month, 29% for more than 12 months, while others used it between 1 and 12 months (Table 7).
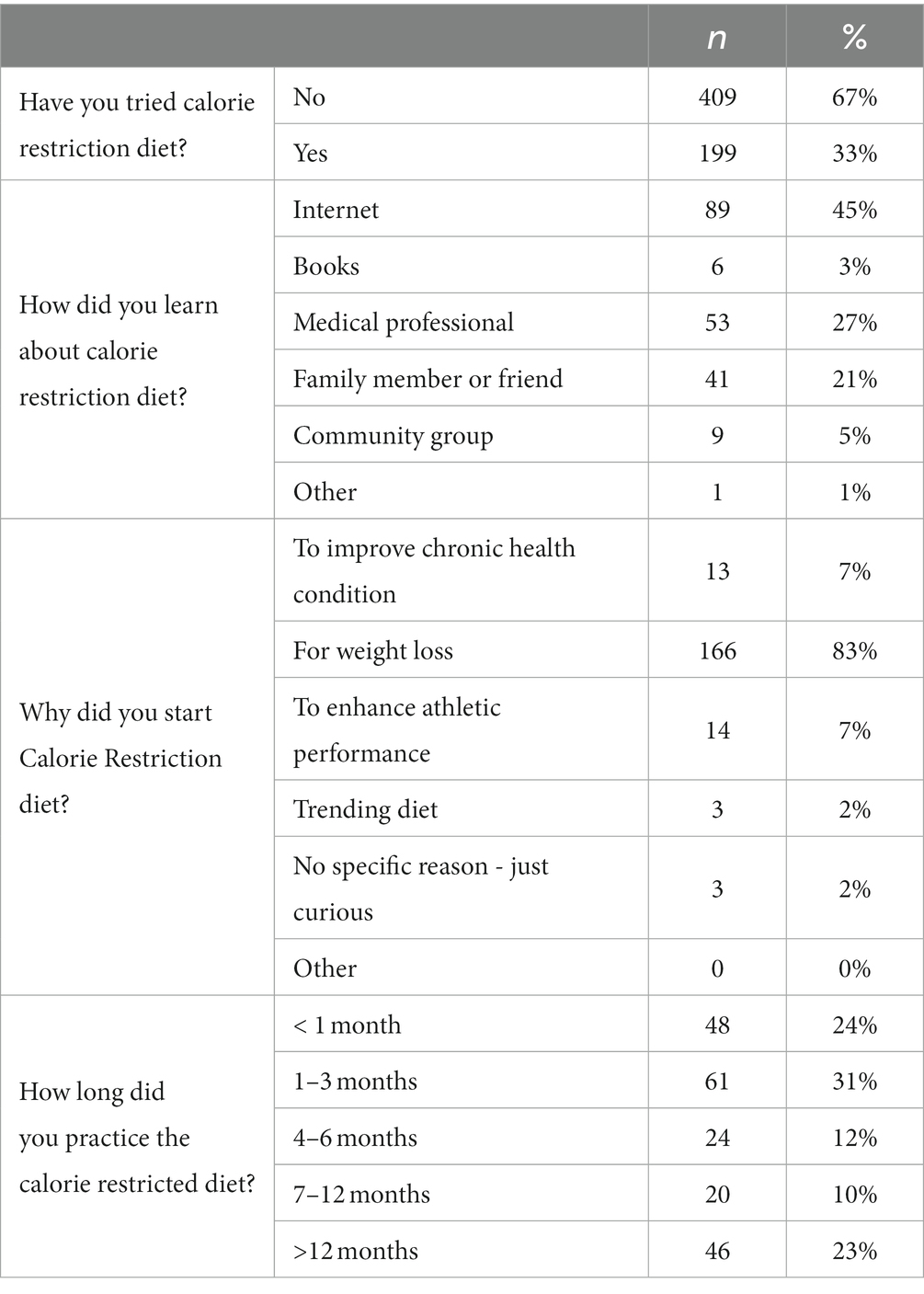
Table 6. Respondents following CRD.

Table 7. Respondents following the GFD.
We then investigated the association between different types of diet with demographic variables (data are provided in the supplementary material) and eating habits. Age and chronic diseases were highly associated with any diet (p = 0.008) (Supplementary Table S1). In addition, exercise and consumption of fruits and vegetables were tightly correlated with any dietary plan (p < 0.001 and p = 0.011, respectively) (Table 8). Next, we investigated the association between IF, low carbohydrate, or low-fat diet with demographic variables and eating habits. Results showed no significant association between IF and demographic variables (Supplementary Table S2). However, exercise (p = 0.001), balanced meals (p = 0.012), number of meals per day (p = 0.006), and the time of participant’s last meal significantly differed between participants following IF and those who did not follow any dietary plan (Table 9). On the other hand, there was no significant association between demographic variables and low carbohydrate or low-fat diet, except for chronic diseases (p = 0.017) (Table S3). In contrast, significant associations existed between exercise (p < 0.001), balanced meals (p < 0.001), and consuming fruits (p = 0.049) and vegetables (p = 0.036) with a low carbohydrate or low-fat diet (Table 10).
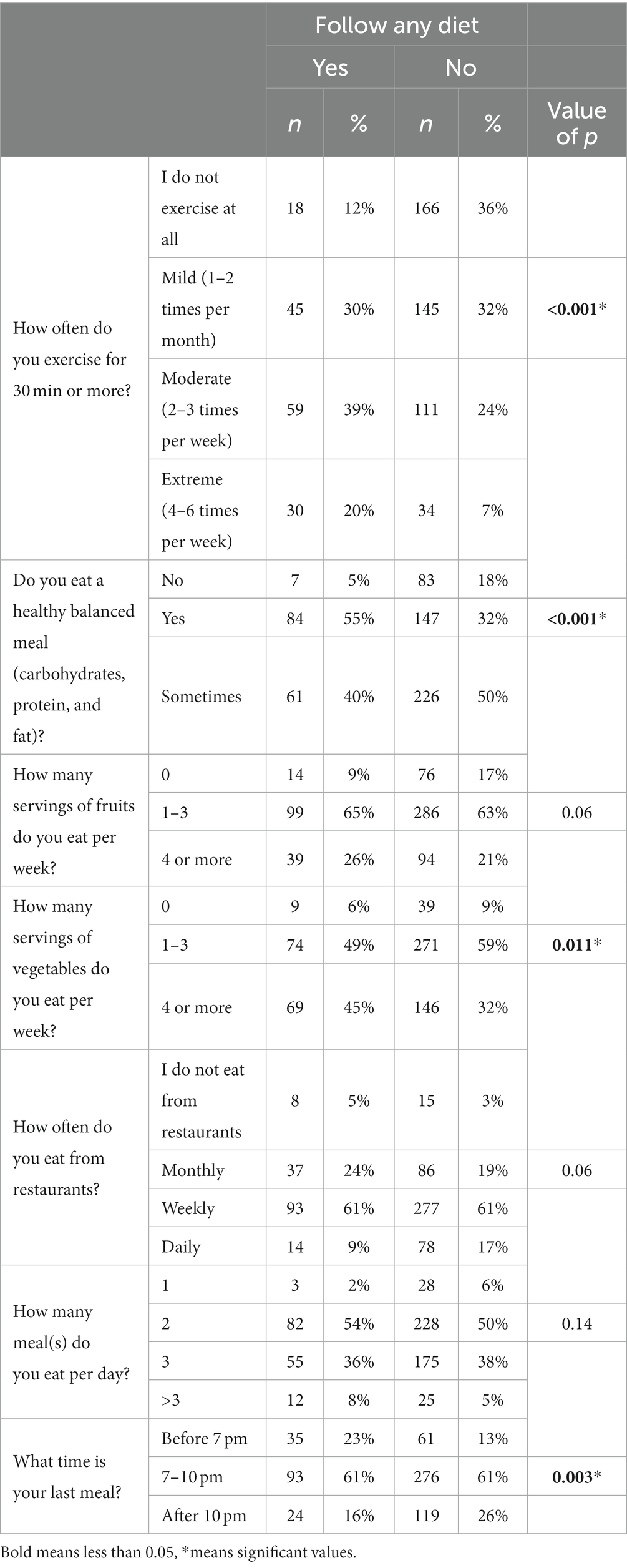
Table 8. Association of eating habits with following any diet following any diet.
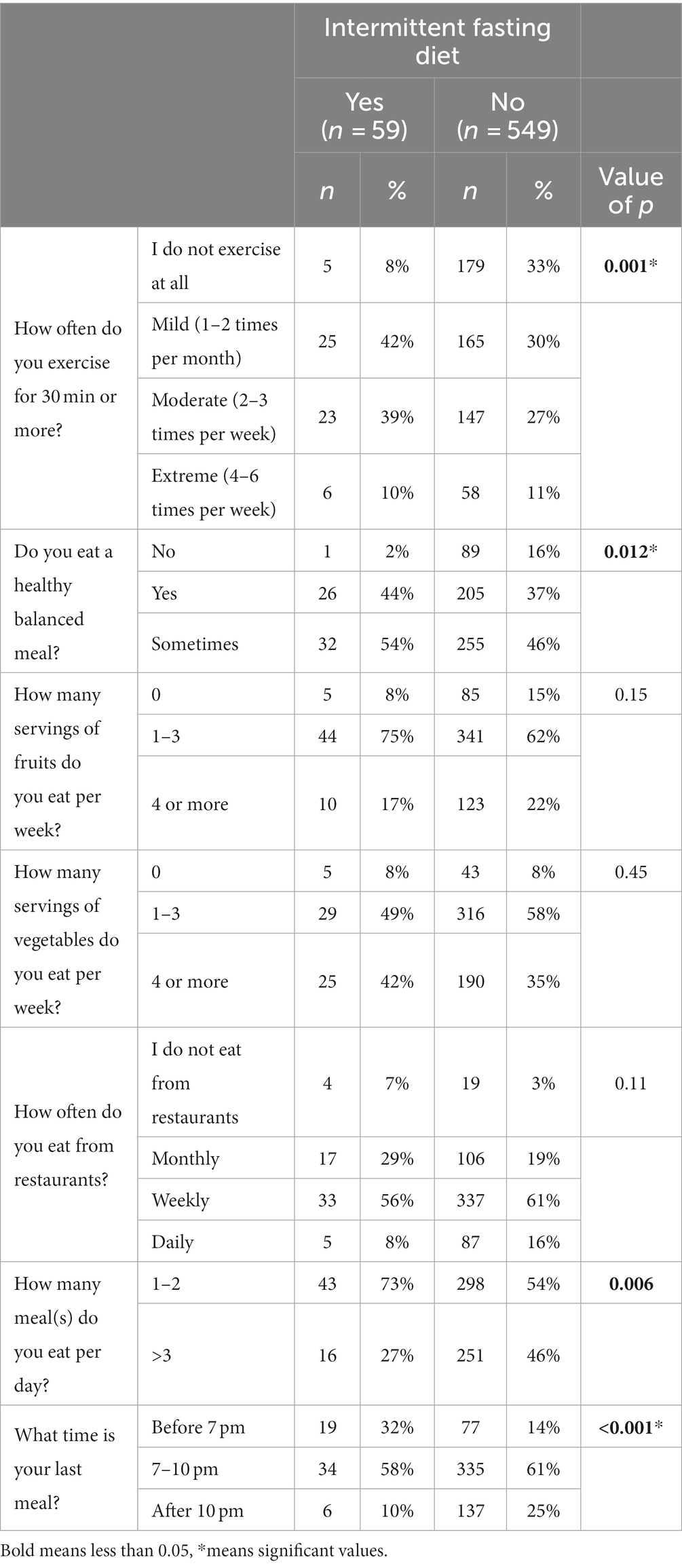
Table 9. Association of eating habits with following IF diet.
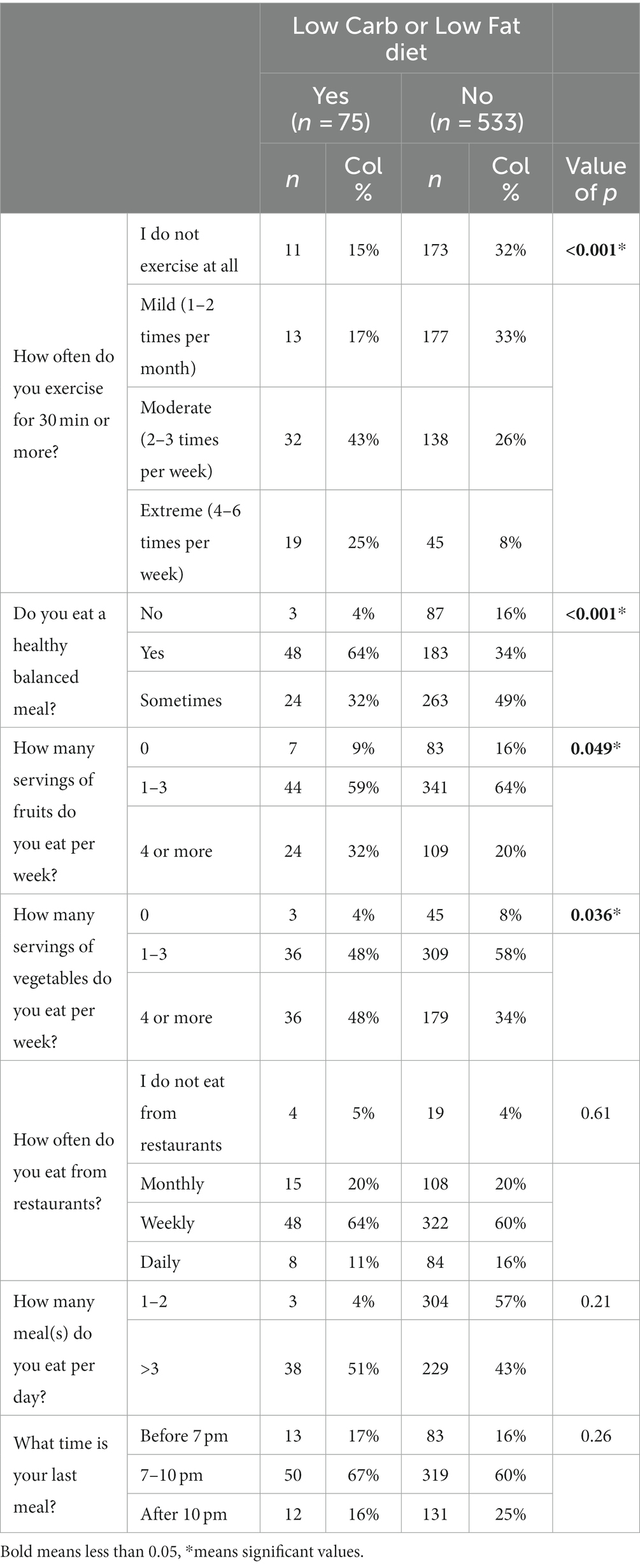
Table 10. Association of eating habits with following low carb or low-fat diet.
In addition, there was a significant association between BMI and type of diet (p = 0.005) and low carbohydrate or low-fat diet (p = 0.004). We also performed logistic regression to assess the probability of different dietary plans with demographic variables and eating habits. Our data showed that participants between 18 and 64 years old are 9–13 times more likely to follow any dietary plan. However, the 30–44 age group was the highest compared to other age groups (p = 0.02). In addition, participants residing in the eastern region of Saudi Arabia are 3 times more likely to apply any dietary plan than other regions of Saudi Arabia. It was demonstrated that participants who would approach any diet plan would exercise from 1 to 2 times up to 4–6 times per week. Participants are more likely to avoid unbalanced meals if a dietary plan is considered (Table 11). It also appears the following any dietary plan and low carbohydrate and low fat are significantly correlated with the BMI (Supplementary Table S4).
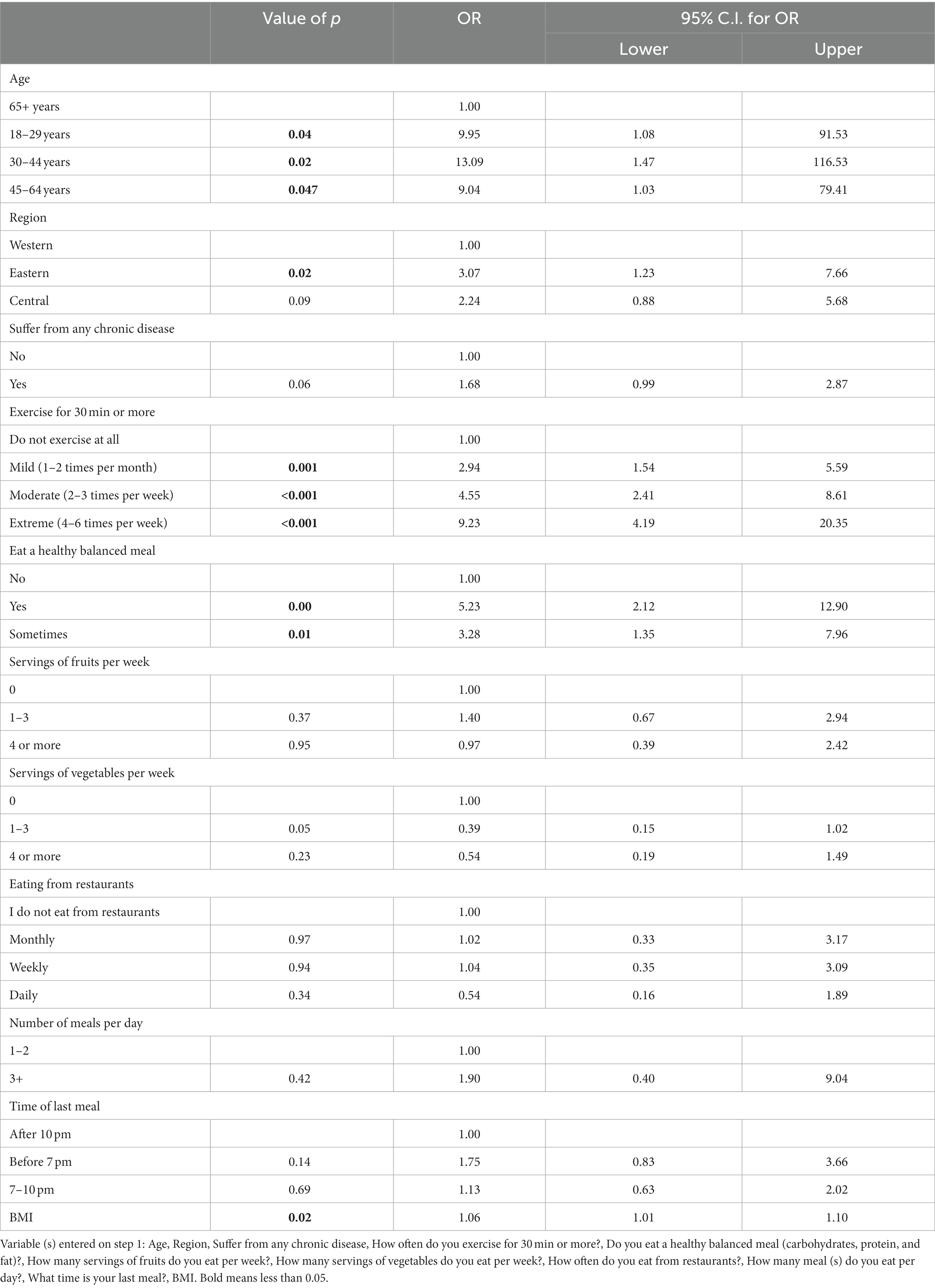
Table 11. Logistic regression for following any diet.
In contrast, the participants are five times more likely to exercise if they follow IF than those who do not follow any dietary restrictions but eight times more likely to sometimes have a balanced diet, have 1–2 meals a day, and have their last meal before 7 pm (Table 12).
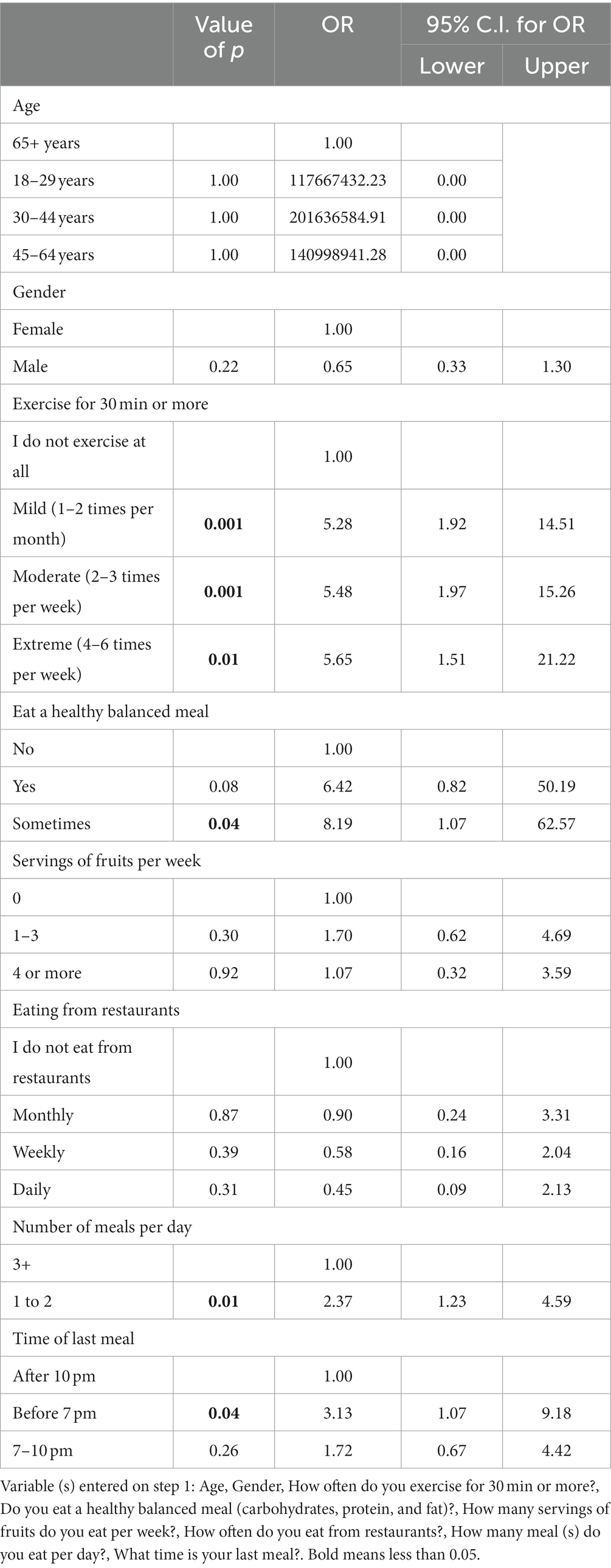
Table 12. Logistic regression for following intermittent fasting.
The logistic regression also shows that participants following a low-carbohydrate or Low-fat diet are expected to exercise 2–3 times or 406 times per week. They will be more likely to follow balanced meals (Table 13).
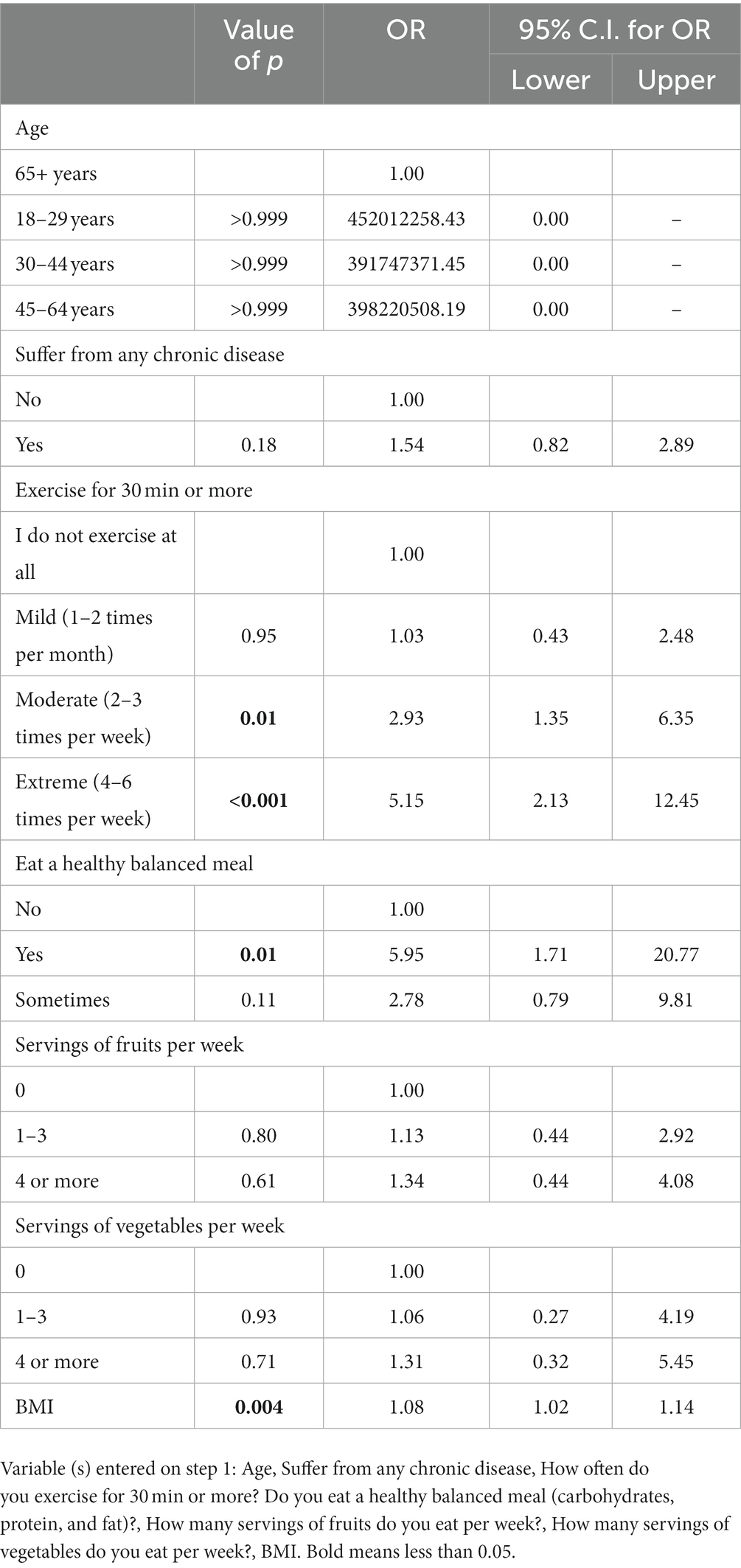
Table 13. Logistic regression for following low carb or low fat diet.
Overweight and obesity represent global health issues affecting 1.9 billion and more than 650 million people worldwide, respectively (25, 26). This health issue increases the risk of developing high blood pressure, dyslipidemia, diabetes, and other conditions, putting a substantial economic burden on many countries (27, 28). A sedentary lifestyle and consumption of fast food play a role in weight gain (29), and an increase in BMI above 40 kg/m2 would reduce life expectancy up to 20 years (27).
Bariatric surgeries are commonly performed in patients with a BMI greater than or equal to 40 kg/m2 or 35 mg/m2 with weight-related comorbidities (30). Some medications also help reduce weight by increasing metabolism; however, following dietary plans such as Ketogenic, intermittent fasting, a gluten-free diet, and a calorie restriction diet, alongside maintaining a healthy lifestyle, is suggested to complement these medications (31, 32).
This study provided insights into the dietary trends and eating habits of 608 individuals in Saudi Arabia. The demographic data showed that most participants were females. The high number of females interested could reflect their obsession with social norms than males and their self-consciousness about their figure (33, 34). In addition, the high responses observed from the eastern followed by the central regions of Saudi Arabia. This could be related to the higher BMI than 30 reported recently in these regions (7).
Obesity and overweight are major health concerns in Saudi Arabia that affect 20% of the population (6). However, the participants generally displayed a satisfactory level of awareness about maintaining a healthy lifestyle despite 75% of them not adhering to any specific dietary plan. The remainder followed either KD, IF, low carbohydrates, or GFD. Each of the dietary strategies serves a vital role in weight loss and health index. For example, the KD shows therapeutic value for obesity, polycystic ovarian syndrome, and cardiovascular diseases (35). The IF has also been reported to reduce body weight and improve dyslipidemia and blood pressure (36). This includes religious fasting named Ramadan IF, which has shown a protective role against inflammatory and oxidative stress markers (37). However, it is still unclear whether IF is beneficial for weight loss over a long period (38).
Additionally, a low-carbohydrate diet reduces cardiovascular risk factors in the short term, but further research is needed to determine long-term benefits (39). Although it is an efficient approach for weight loss, it is has been reported that many individuals quit as they find it difficult to adhere to this dietary plan (40). In this study, participants were advised to follow a gluten-free diet either for Celiac disease (CD) or food/skin allergy management. Despite the benefits of GFD, it could contribute to nutritional deficiencies such as vitamins, calcium, iron, and fiber (41). Also, adherence to a GFD is even more difficult due to the high cost of gluten-free products (42).
Furthermore, respondents were more likely to choose the IF as the dieting program in the first place, followed by the low-fat diet. People who decided those dieting programs would exercise (moderate to extreme) and observe healthy, balanced food. Not everyone would respond similarly to a specific diet because of metabolism variability between individuals (43).
Internet use has been shown to promote a healthy diet by increasing the intake of fruits, vegetables, and eggs and decreasing salt and oil intake (44). Our survey showed that the internet was the primary tool by which responders learned about these dietary schemes.
The timing of the last meal (after 7 p.m.) was previously associated with weight gain, dyslipidemia, high glucose levels, and metabolic syndrome and was frequently observed in obese individuals (45, 46). Data showed that most respondents would have their last meal after 7 p.m., highlighting the urge to increase awareness on the risk of obesity, hyperglycemia and metabolic syndromes (47, 48).
Most weight loss studies last at least 3 months or more (43). In most dietary types, participants following any diet involved in this study failed to continue for more than 3 months. The metabolism variability between individuals in response to similar food could explain why individuals would respond differently to a specific diet (43). This suggests that a personalized diet program might help sustain their dietary regimen. A recent study on personalized diet was suggested to aid in weight loss (49). Mithbavka et al. (50) presented an application for customized diet regimens, meeting the requirements for healthy food, depending on the user’s dietary preferences, and adapted to their health status (51).
Dietary guidelines for recommended healthy and balanced meals were released by the Saudi Ministry of Health in 2012. A study showed that the Saudi population needs to follow the guidelines for a healthy diet (52). These findings emphasize the need to increase awareness, as obesity and overweight are alarming issues affecting the Saudi population.
There are several limitations of this study. The cross-sectional nature creates temporal bias and limits any causal inferences. Moreover, selection bias due to convenience sampling is highly possible, limiting our study’s generalizability. However, this study is novel and bridges the gap in the literature due to the limited studies about dietary trends in Saudi Arabia.
Obesity remains a challenge in Saudi Arabia. Adherence to dietary regimes can help in controlling obesity. Increasing the public’s awareness of trending diets can aid in healthy lifestyles. Implementing a healthy lifestyle among the Saudi population to prevent weight gain and help in weight loss becomes necessary. Different methods can carry this out; one that seems efficient is through advertisements on social media and websites of general interest. Increasing the price of high-sugar or high-fat foods might help prevent weight gain and obesity.
Efforts to combat obesity in Saudi Arabia and globally require a multi-faceted approach, including promoting healthy eating habits, increasing physical activity, and raising awareness about the health risks associated with obesity. Public health interventions, community engagement, and policy changes are essential components of addressing the obesity epidemic in the country.
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author.
The studies involving humans were approved by King Abdullah International Medical Research Center. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
NoA: Writing – original draft, Writing – review & editing, Conceptualization, Data curation, Formal analysis. NaA: Data curation, Formal analysis, Investigation, Methodology, Writing – original draft, Writing – review & editing. ShA: Formal analysis, Writing – review & editing. MK: Writing – original draft, Writing – review & editing. RT: Data curation, Writing – original draft, Writing – review & editing. ME: Data curation, Writing – original draft. RW: Writing – original draft, Writing – review & editing. SaA: Writing – original draft, Writing – review & editing, Data curation. MR: Data curation, Formal analysis, Writing – review & editing. AO: Data curation, Formal analysis, Writing – review & editing. SiA: Formal analysis, Writing – original draft, Writing – review & editing. RS: Conceptualization, Data curation, Writing – original draft, Writing – review & editing. AA-B: Conceptualization, Data curation, Writing – original draft.
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. The authors give thanks to Alfaisal University for providing financial aid for the article processing charges.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2023.1326418/full#supplementary-material
1. Upadhyay, J, Farr, O, Perakakis, N, Ghaly, W, and Mantzoros, C. Obesity as a disease. Medical Clinics. (2018) 102:13–33. doi: 10.1016/j.mcna.2017.08.004
2. Church, TS, Thomas, DM, Tudor-Locke, C, Katzmarzyk, PT, Earnest, CP, Rodarte, RQ, et al. Trends over 5 decades in U.S. occupation-related physical activity and their associations with obesity. PLoS One. (2011) 6:e19657. doi: 10.1371/journal.pone.0019657
3. Njike, VY, Smith, TM, Shuval, O, Shuval, K, Edshteyn, I, Kalantari, V, et al. Snack food, satiety, and weight. Adv Nutr. (2016) 7:866–78. doi: 10.3945/an.115.009340
4. Singh, GM, Danaei, G, Farzadfar, F, Stevens, GA, Woodward, M, Wormser, D, et al. The age-specific quantitative effects of metabolic risk factors on cardiovascular diseases and diabetes: a pooled analysis. PLoS One. (2013) 8:e65174. doi: 10.1371/journal.pone.0065174
5. Lauby-Secretan, B, Scoccianti, C, Loomis, D, Grosse, Y, Bianchini, F, and Straif, K. Body fatness and cancer--viewpoint of the IARC working group. N Engl J Med. (2016) 375:794–8. doi: 10.1056/NEJMsr1606602
6. Salem, V, AlHusseini, N, Abdul Razack, HI, Naoum, A, Sims, OT, and Alqahtani, SA. Prevalence, risk factors, and interventions for obesity in Saudi Arabia: a systematic review. Obes Rev. (2022) 23:e13448. doi: 10.1111/obr.13448
7. Althumiri, NA, Basyouni, MH, AlMousa, N, AlJuwaysim, MF, Almubark, RA, Bin Dhim, NF, et al. Obesity in Saudi Arabia in 2020: prevalence, distribution, and its current association with various health conditions. Healthcare. (2021) 9:311. doi: 10.3390/healthcare9030311
8. AlHusseini, N, Sajid, M, Akkielah, Y, Khalil, T, Alatout, M, Cahusac, P, et al. Vegan, vegetarian and meat-based diets in Saudi Arabia. Cureus. (2021) 13:e18073. doi: 10.7759/cureus.18073
9. Alali, AS, Alshehri, AO, Assiri, A, Khan, S, Alkathiri, MA, Almohammed, OA, et al. Demographics, comorbidities, and outcomes among young and middle-aged COVID-19 patients in Saudi Arabia. Saudi Pharm J. (2021) 29:833–42. doi: 10.1016/j.jsps.2021.06.005
10. Al-Khaldi, Y . Bariatric surgery in Saudi Arabia: the urgent need for standards. Saudi J Obes. (2016) 4:1. doi: 10.4103/2347-2618.184930
11. Wirnitzer, K . Vegan diet in sports and exercise—health benefits and advantages to athletes and physically active people: a narrative review. Int J Sports Exerc Med. (2020) 6:165. doi: 10.23937/2469-5718/1510165
12. O'Neill, B, and Raggi, P. The ketogenic diet: pros and cons. Atherosclerosis. (2020) 292:119–26. doi: 10.1016/j.atherosclerosis.2019.11.021
13. Dowis, K, and Banga, S. The potential health benefits of the ketogenic diet: a narrative review. Nutrients. (2021) 13:1654. doi: 10.3390/nu13051654
14. Mattson, MP, Longo, VD, and Harvie, M. Impact of intermittent fasting on health and disease processes. Ageing Res Rev. (2017) 39:46–58. doi: 10.1016/j.arr.2016.10.005
15. Patterson, RE, and Sears, DD. Metabolic effects of intermittent fasting. Annu Rev Nutr. (2017) 37:371–93. doi: 10.1146/annurev-nutr-071816-064634
16. Alrowaili, MG, Hussein, AM, Eid, EA, Serria, MS, Abdellatif, H, and Sakr, HF. Effect of intermittent fasting on glucose homeostasis and bone remodeling in glucocorticoid-induced osteoporosis rat model. J Bone Metab. (2021) 28:307–16. doi: 10.11005/jbm.2021.28.4.307
17. Johnson, JB, Summer, W, Cutler, RG, Martin, B, Hyun, DH, Dixit, VD, et al. Alternate day calorie restriction improves clinical findings and reduces markers of oxidative stress and inflammation in overweight adults with moderate asthma. Free Radic Biol Med. (2007) 42:665–74. doi: 10.1016/j.freeradbiomed.2006.12.005
18. Melini, V, and Melini, F. Gluten-free diet: gaps and needs for a healthier diet. Nutrients. (2019) 11:170. doi: 10.3390/nu11010170
19. Bascuñán, KA, Vespa, MC, and Araya, M. Celiac disease: understanding the gluten-free diet. Eur J Nutr. (2017) 56:449–59. doi: 10.1007/s00394-016-1238-5
20. Ciacci, C, Cirillo, M, Cavallaro, R, and Mazzacca, G. Long-term follow-up of celiac adults on gluten-free diet: prevalence and correlates of intestinal damage. Digestion. (2002) 66:178–85. doi: 10.1159/000066757
21. Jones, AL . The gluten-free diet: fad or necessity? Diabetes Spectr. (2017) 30:118–23. doi: 10.2337/ds16-0022
22. Most, J, Tosti, V, Redman, LM, and Fontana, L. Calorie restriction in humans: an update. Ageing Res Rev. (2017) 39:36–45. doi: 10.1016/j.arr.2016.08.005
23. Varady, KA . Intermittent versus daily calorie restriction: which diet regimen is more effective for weight loss? Obes Rev. (2011) 12:e593–601. doi: 10.1111/j.1467-789X.2011.00873.x
24. Di Daniele, N, Marrone, G, Di Lauro, M, Di Daniele, F, Palazzetti, D, Guerriero, C, et al. Effects of caloric restriction diet on arterial hypertension and endothelial dysfunction. Nutrients. (2021) 13:274. doi: 10.3390/nu13010274
25. Alsulami, S, Baig, M, Ahmad, T, Althagafi, N, Hazzazi, E, Alsayed, R, et al. Obesity prevalence, physical activity, and dietary practices among adults in Saudi Arabia. Front Public Health. (2023) 11:1124051. doi: 10.3389/fpubh.2023.1124051
26. NCD Risk Factor Collaboration (NCD-RisC) . Trends in adult body-mass index in 200 countries from 1975 to 2014: a pooled analysis of 1698 population-based measurement studies with 19·2 million participants. Lancet. (2016) 387:1377–96. doi: 10.1016/S0140-6736(16)30054-X
28. Tremmel, M, Gerdtham, U-G, Nilsson, PM, and Saha, S. Economic burden of obesity: a systematic literature review. Int J Environ Res Public Health. (2017) 14:435. doi: 10.3390/ijerph14040435
29. Meltzer, DO, and Chen, Z. The impact of minimum wage rates on body weight in the United States. National Bureau of Economic Research: University of Chicago Press; (2011). p. 17–34.
30. Arterburn, DE, Telem, DA, Kushner, RF, and Courcoulas, AP. Benefits and risks of bariatric surgery in adults: a review. JAMA. (2020) 324:879–87. doi: 10.1001/jama.2020.12567
31. Aaseth, J, Ellefsen, S, Alehagen, U, Sundfør, TM, and Alexander, J. Diets and drugs for weight loss and health in obesity - an update. Biomed Pharmacother. (2021) 140:111789. doi: 10.1016/j.biopha.2021.111789
32. Joshi, S, Kalantar-Zadeh, K, Chauveau, P, and Carrero, JJ. Risks and benefits of different dietary patterns in CKD. Am J Kidney Dis. (2023) 81:352–60. doi: 10.1053/j.ajkd.2022.08.013
33. Bhogal, MS, and Langford, R. Gender differences in weight loss; evidence from a NHS weight management service. Public Health. (2014) 128:811–3. doi: 10.1016/j.puhe.2014.06.019
34. Connor-Greene, PA . Gender differences in body weight perception and weight-loss strategies of college students. Women Health. (1988) 14:27–42. doi: 10.1300/J013v14n02_03
35. Paoli, A, Rubini, A, Volek, JS, and Grimaldi, KA. Beyond weight loss: a review of the therapeutic uses of very-low-carbohydrate (ketogenic) diets. Eur J Clin Nutr. (2013) 67:789–96. doi: 10.1038/ejcn.2013.116
36. Ahmed, N, Farooq, J, Siddiqi, HS, Meo, SA, Kulsoom, B, Laghari, AH, et al. Impact of intermittent fasting on lipid profile-a quasi-randomized clinical trial. Front Nutr. (2020) 7:596787. doi: 10.3389/fnut.2020.596787
37. MeA-IE, F, Jahrami, HA, Obaideen, AA, and Madkour, MI. Impact of diurnal intermittent fasting during Ramadan on inflammatory and oxidative stress markers in healthy people: systematic review and meta-analysis. J Nutr Intermed Metab. (2019) 15:18–26. doi: 10.1016/j.jnim.2018.11.005
38. Varady, KA, Cienfuegos, S, Ezpeleta, M, and Gabel, K. Clinical application of intermittent fasting for weight loss: progress and future directions. Nat Rev Endocrinol. (2022) 18:309–21. doi: 10.1038/s41574-022-00638-x
39. Dong, T, Guo, M, Zhang, P, Sun, G, and Chen, B. The effects of low-carbohydrate diets on cardiovascular risk factors: a meta-analysis. PLoS One. (2020) 15:e0225348. doi: 10.1371/journal.pone.0225348
40. Del Corral, P, Chandler-Laney, PC, Casazza, K, Gower, BA, and Hunter, GR. Effect of dietary adherence with or without exercise on weight loss: a mechanistic approach to a global problem. J Clin Endocrinol Metab. (2009) 94:1602–7. doi: 10.1210/jc.2008-1057
41. La Vieille, S, Pulido, OM, Abbott, M, Koerner, TB, and Godefroy, S. Celiac disease and gluten-free oats: a Canadian position based on a literature review. Can J Gastroenterol Hepatol. (2016) 2016:1–10. doi: 10.1155/2016/1870305
42. Al-Sunaid, FF, Al-Homidi, MM, Al-Qahtani, RM, Al-Ashwal, RA, Mudhish, GA, Hanbazaza, MA, et al. The influence of a gluten-free diet on health-related quality of life in individuals with celiac disease. BMC Gastroenterol. (2021) 21:330–9. doi: 10.1186/s12876-021-01908-0
43. Popp, CJ, Hu, L, Kharmats, AY, Curran, M, Berube, L, Wang, C, et al. Effect of a personalized diet to reduce postprandial Glycemic response vs a low-fat diet on weight loss in adults with abnormal glucose metabolism and obesity: a randomized clinical trial. JAMA Netw Open. (2022) 5:e2233760. doi: 10.1001/jamanetworkopen.2022.33760
44. Ma, T, Wang, H, Wei, M, Lan, T, Wang, J, Bao, S, et al. Application of smart-phone use in rapid food detection, food traceability systems, and personalized diet guidance, making our diet more health. Food Res Int. (2022) 152:110918. doi: 10.1016/j.foodres.2021.110918
45. Davis, R, Rogers, M, Coates, AM, Leung, GKW, and Bonham, MP. The impact of meal timing on risk of weight gain and development of obesity: a review of the current evidence and opportunities for dietary intervention. Curr Diab Rep. (2022) 22:147–55. doi: 10.1007/s11892-022-01457-0
46. Okada, C, Imano, H, Muraki, I, Yamada, K, and Iso, H. The Association of Having a late dinner or bedtime snack and skipping breakfast with overweight in Japanese women. J Obes. (2019) 2019:1–5. doi: 10.1155/2019/2439571
47. Kutsuma, A, Nakajima, K, and Suwa, K. Potential association between breakfast skipping and concomitant late-night-dinner eating with metabolic syndrome and proteinuria in the Japanese population. Scientifica. (2014) 2014:1–9. doi: 10.1155/2014/253581
48. Lopez-Minguez, J, Gómez-Abellán, P, and Garaulet, M. Timing of breakfast, lunch, and dinner. Effects on obesity and metabolic risk. Nutrients. (2019) 11:2624. doi: 10.3390/nu11112624
49. Ho, H-P, Lin, Y-C, James, FC, and Chang, C-T. On the personal diet considering qualitative and quantitative issues. Comput Ind Eng. (2022) 164:107857. doi: 10.1016/j.cie.2021.107857
50. Mithbavkar, S. Diet planner using deep learning. Journal of Emerging Technologies and Innovative Research. (2023).
Keywords: diet, Saudi Arabia, dietary trends, ketogenic diet, intermittent fasting, gluten-free diet, calorie restriction
Citation: Alhusseini N, Alsinan N, Almutahhar S, Khader M, Tamimi R, Elsarrag MI, Warar R, Alnasser S, Ramadan M, Omair A, Aouabdi S, Saleem R and Alabadi-Bierman A (2024) Dietary trends and obesity in Saudi Arabia. Front. Public Health. 11:1326418. doi: 10.3389/fpubh.2023.1326418
Edited by:
Maroof Alam, University of Michigan, United StatesReviewed by:
Asim Rizvi, Aligarh Muslim University, IndiaCopyright © 2024 Alhusseini, Alsinan, Almutahhar, Khader, Tamimi, Elsarrag, Warar, Alnasser, Ramadan, Omair, Aouabdi, Saleem and Alabadi-Bierman. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Sihem Aouabdi, YW91YWJkaXNpQG5naGEubWVkLnNh
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.