
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health , 04 January 2024
Sec. Public Health Education and Promotion
Volume 11 - 2023 | https://doi.org/10.3389/fpubh.2023.1321457
 Xuehai Zhang1†
Xuehai Zhang1† Xinxin Zhang2†
Xinxin Zhang2† Songjia Zhang2
Songjia Zhang2 Lizheng Ge2
Lizheng Ge2 Yue Xu1
Yue Xu1 Dingning Yao1Xiujing Hu1Zishuo Huang3
Dingning Yao1Xiujing Hu1Zishuo Huang3 Tingting Zhu4Zixia Wang5*
Tingting Zhu4Zixia Wang5* Chun Chen2*
Chun Chen2*Objectives: The worldwide popularity of electronic cigarettes (ECIG) is becoming a public health concern. Compared to conventional cigarettes (CIG), the harm caused by ECIG is more insidious. Studies have shown that lower health literacy (HL) is associated with CIG use; however, the relationship between HL and ECIG use remains controversial. Because ECIG emerged more recently than CIG, there are fewer relevant studies, and the sample populations and evaluation methods of HL in existing studies differ. This study conducted a large-sample survey to examine the relationship between HL and ECIG use.
Methods: As part of the 2022 China Health Literacy Survey, a total of 60,998 valid questionnaires were collected from September to November in 2022 using a stratified multistage probability proportional to the population size sampling frame. Chi-square tests and multinomial logistic regression was used to analyze the relationship between HL and ECIG use. Some demographic variables were included as covariates in the analysis.
Results: The study showed that the average HL score and the HL level of Zhejiang residents in 2022 were 42.8 and 30.8%, respectively. The prevalence of CIG and ECIG was 19.7 and 1.0%, respectively; 19% of participants exclusively used CIG, while only 0.3% of participants used ECIG exclusively; dual users accounted for 0.6%. After adjusting for covariates, adequate HL was associated with lower odds of ECIG-exclusive use (odds ratio [OR] = 0.452, p < 0.001), CIG-exclusive use (OR = 0.833, p < 0.001), and dual use (OR = 0.632, p < 0.001). Young age, male sex, unmarried status, high-income status, and absence of chronic disease were also associated with ECIG use.
Conclusion: HL was a protective factor against both patterns of ECIG use, especially ECIG-exclusive use. Health policymakers and public health practitioners should consider HL as a potential measure for ECIG control.
Conventional cigarette (CIG) use has been proven to be associated with negative health conditions, such as cardiovascular diseases and lung cancer (1–3). Consequently, laws have been introduced worldwide to restrict CIG use (4, 5), and a variety of smoking cessation products have emerged. Since 2007, electronic cigarettes (ECIG) have been swiftly promoted (6–8) as an alternative to CIG. People believe that ECIG use is less harmful and addictive; however, in practice, its use has been proven hazardous to human health (9, 10). The US Centers for Disease Control and Prevention recommend young adults not use ECIG or vaping products (containing nicotine or tetrahydrocannabinol) because of the effects of nicotine on brain development (11). ECIG use among Chinese adults aged 18–29 increased significantly from 2.0% in 2015–16 to 2.7% in 2018–19 (11). China currently regulates the sale and promotion of ECIG only for those under the age of 18 years (12, 13). In addition to legislation, research on the factors influencing ECIG use can provide policymakers with additional ECIG control ideas.
Health literacy (HL) refers to the ability of individuals to access and understand health information and use this information to maintain and promote their own health (14). Existing literature suggests that HL contributes to the adoption of healthy behaviors (15, 16), including reduced smoking behavior (17, 18). Recent studies have shown that individuals with low HL have higher rates of CIG use compared to those with high HL (19). In addition, there is literature suggesting that different levels of HL were associated with prevention of smoking (20).Thus, improving HL is a potential measure for controlling smoking behavior. Does HL have the same effect on ECIG use? Few studies have examined this question, and the results are controversial (21–23). Therefore, we conducted a large-sample survey of 60,998 people in Zhejiang Province, China, to address the role of HL in ECIG use.
Relevant surveys have shown that most ECIG users are dual users and have converted from being CIG-exclusive users (11). Therefore, ECIG users comprise two groups: dual users and ECIG-exclusive users. The HL status of these two groups likely differs. To eliminate potential confusion, we divided tobacco users into three categories: CIG-exclusive, ECIG-exclusive, and dual users, and then calculated the odds ratio (OR) of each group separately.
With its increasing popularity, ECIG is becoming the first tobacco product to which young people are exposed. It is important to clarify the relationship between HL and ECIG use. We wanted to determine whether HL remains significantly associated with ECIG use after excluding the effects of CIG use. We then provide a reference for policymakers regarding ECIG control.
This cross-sectional study was conducted in Zhejiang Province as part of the 2022 China Health Literacy Survey. The target population of this survey is the non-collective resident population with Chinese nationality aged 15–69 years old in all counties (cities and districts) in Zhejiang Province, excluding residents living in military bases, hospitals, prisons, nursing homes, and dormitories. The permanent population comprises residents who have resided in the local area for more than six months in the past 12 months, regardless of whether they have a local household registration status. We excluded people under the age of 15 years because this is the age at which compulsory education has typically not been completed. We also excluded people over the age of 69 years, because people over this age are more likely to have cognitive impairment (24).
The survey was voluntary and anonymous, and this information was communicated to participants prior to the survey. Potential participants were asked to indicate that they had read and understood the consent instructions information and agreed to participate before taking the questionnaire. Questionnaires were completed through face-to-face interviews, and the interviewers had received professional training in advance. This study was reviewed and approved by the Research Ethics Committee of Zhejiang Provincial Center for Disease Control and Prevention.
The minimum sample size for each county (city or district) is calculated as N = ×deff. According to the HL level of Zhejiang Province in 2021—36.11%—p is set as 0.3611; the allowable relative error is 15%; the allowable absolute error δ = 0.3611 × 0.15 = 0.0542, μα = 1.96, deff = 1, and the minimum sample size per county is finally calculated as 302. Considering the invalid questionnaires and the low vaping rate of e-cigarettes, we expanded the sample size to 640 per county (city or district).
This survey covered all 90 counties (cities or districts) in Zhejiang Province. The field investigation officially began in September 2022 and was completed by the end of November 2022. Sampling methods were carried out in accordance with national guidance (25), which was divided into the following four steps: (1) each county (city, district) adopted stratified multistage probabilities proportional to the population size (PPS) sampling frame to select four townships; (2) each township adopted a PPS sampling frame to select two communities (villages); (3) 100 households were selected from each community (village) by random sampling; and (4) one participant from each household was selected for a face-to-face interview using Kish’s grid (26). At least 80 participants were required to complete the questionnaire for each community (village). Through the above sampling steps, we collected a total of 60,998 qualified questionnaires.
We adopted the Zhejiang Citizen Health Literacy and Tobacco Use Questionnaire (2022), which was modified from the Chinese Citizen Health Literacy Questionnaire (2022). The questionnaire comprised three parts (HL, Tobacco Use, and Personal Characteristics) and was issued by the Zhejiang Provincial Center for Disease Control and Prevention.
The Chinese Health Literacy Scale was used to assess HL in the first part of the questionnaire. This scale was developed by the Chinese Center for Health Education using the Delphi method (27). The scale consists of 50 items and is divided into three dimensions: knowledge and attitudes, behavior and lifestyle, and health-related skills (28). The scale comprises three types of questions: true or false (one point for a correct answer), single answer (choose the only correct answer from several available answers and score one point for a correct response) and multiple answers (several possible answers are correct; a “correct response” comprises selecting all the correct answers and two points are awarded for a correct response). A score of 53 out of 66 (80%) is considered to have adequate HL, and a score of 0–52 is considered to have limited HL. The overall Cronbach’s alpha for the scale was 0.95, and the Spearman-Brown coefficient was 0.94 (29).
The second part contained seven questions related to tobacco use; we analyzed two of them, “Do you currently smoke conventional cigarettes?” and “Do you currently use e-cigarettes?” These two questions have four possible answers: 1 “yes, I do, and I smoke every day”; 2 “yes, I do, but not every day”; 3 “I used to smoke, but have now quit”; and 4 “I have never smoked.” Participants were classified as users of a particular tobacco product if they chose answers 1 or 2 and as non-users if they chose answers 3 or 4. A 4-level categorical variable was calculated. Those who chose 3 or 4 for both questions were defined as non-users and coded as 1. Using only CIG and not ECIG was defined as a CIG-exclusive user and coded as 2. Using only ECIG and not CIG denoted an ECIG-exclusive user and was coded as 3. Dual users were defined as those who use both CIG and ECIG and were coded as 4.
At the end of the questionnaire, we collected personal characteristics, some of which were used as covariates in logistic regression. Sex was included as a covariate as a binary variable (male/female) because studies have reported that males are much more likely to use tobacco than females (30). Age was regarded as a four-level ordinal variable (15–24, 25–44, 45–64, 65–69 years); studies have found that middle-aged (25–64 years) people are associated with more tobacco use than other age groups (31). Marital status is divided into married and other status (single/widow/divorced) because studies have reported that married people use less tobacco than other married status groups (32). Educational level was considered a three-level ordinal variable (less than junior high school, junior/senior high school, and college or above); previous studies have suggested that people with less education tend to use tobacco more frequently (33). Occupation was treated as a five-level categorical variable (technical/professional, commercial/service, student, manual, unemployed/other). Previous studies have demonstrated that managers and/or professionals are more likely to smoke (33). Annual household income was treated as a four-level ordinal variable (0–49,999, 50,000–99,999, 100,000–149,999, or ≥ 150,000 Yuan). Previous research has shown that smoking is more widespread among the least well-off (34). Chronic condition was a binary variable (yes/no) because many studies have reported associations between smoking and chronic diseases (35).
Data were processed in SPSS Statistics, version 25.0. The significance level was set as p < 0.05. First, we conducted a descriptive analysis of the sample data, showing the frequency and percentage of all variables (Table 1). Chi-square tests were then used to examine whether each variable was associated with tobacco use patterns (Table 1). Finally, multinomial logistic regression was used to test whether HL independently affected ECIG use (Table 2). In the multinomial logistic regression model, the outcome reference group was tobacco non-users.
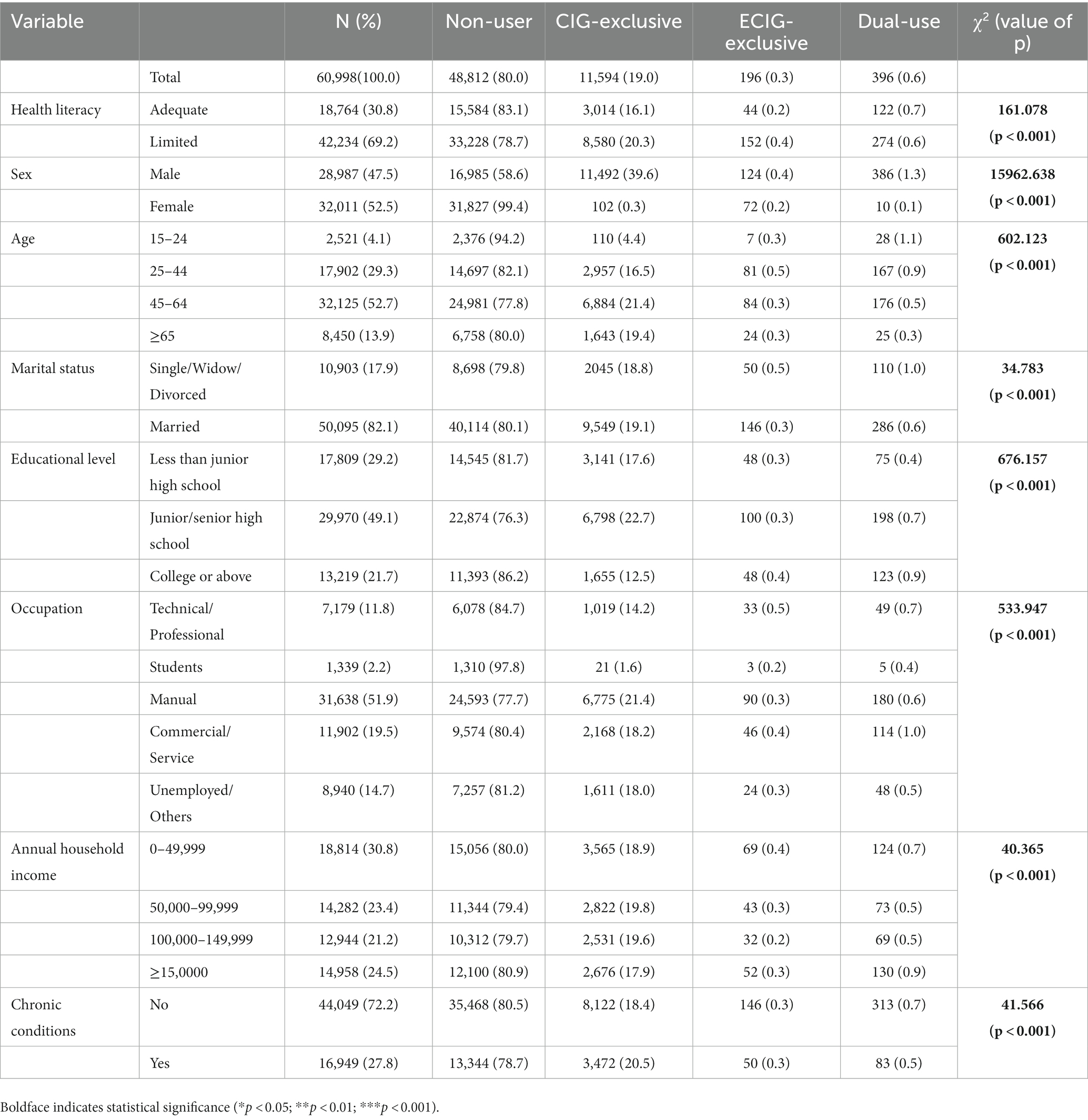
Table 1. Composition of tobacco use by participant characteristics.
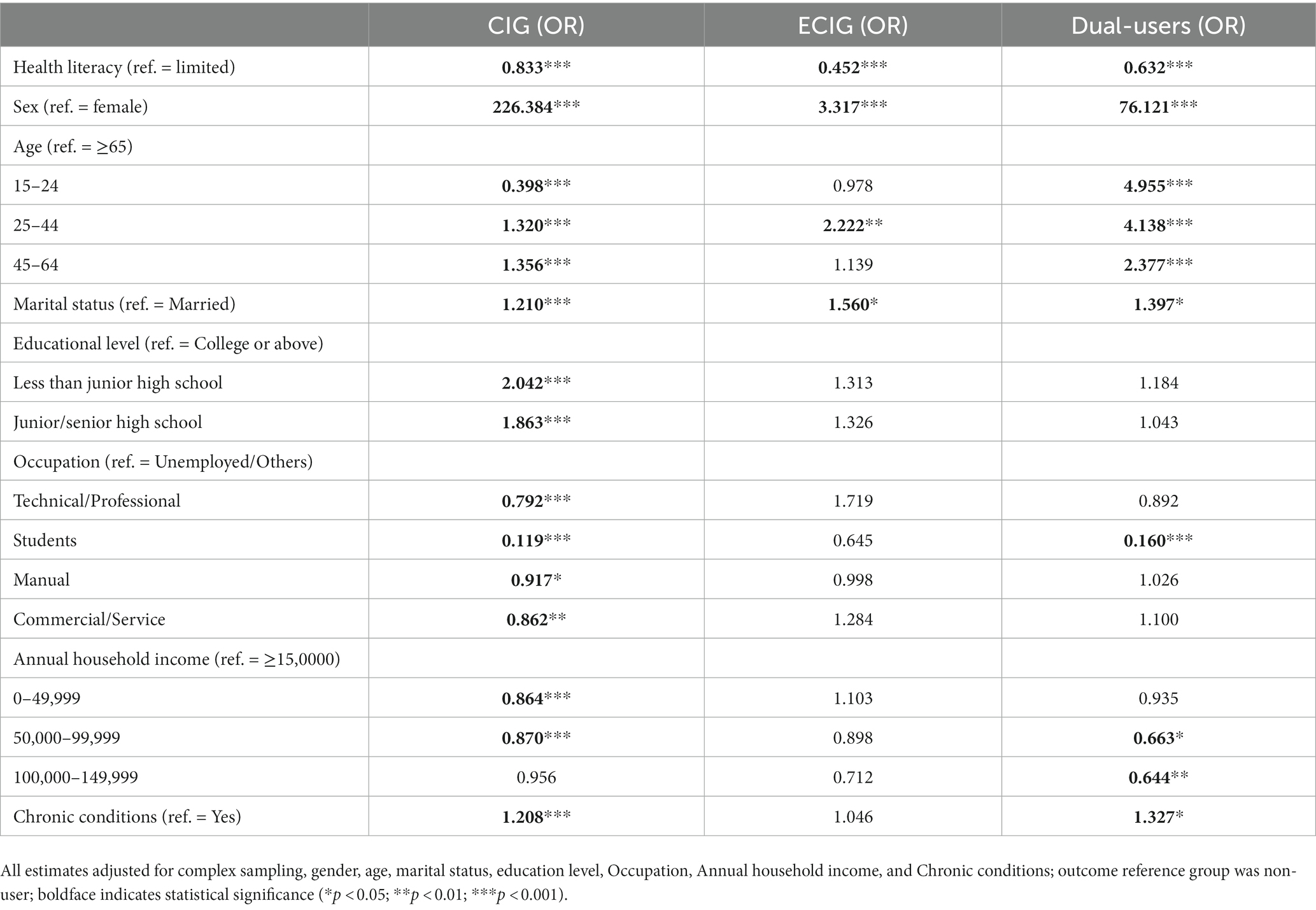
Table 2. Multinomial logistic regression.
The characteristics of the participants are shown in Table 1. A total of 60,998 qualified questionnaires were collected in the survey, of which 0.3% were ECIG-exclusive users, 19.0% were CIG-exclusive users, 0.6% were dual users, and the rest were non-tobacco users. Among the participants, 30.8% had adequate HL. Most participants were female (52.5%), middle-aged (25–64, 82.0%), married (82.1%), with junior/senior high school education (49.1%), and manual workers (51.9%). Most participants did not have chronic diseases (72.2%). The participants’ household incomes were evenly distributed (0–49,999 [30.8%], 50,000–99,999 [23.4%], 100,000–149,999 [21.2%], ≥15,0000 [24.5%]).
The chi-squared (χ2) test was performed to compare the composition of ECIG use among different demographic groups (Table 1). Statistically significant differences were observed among all groups: HL composition (χ2 = 161.078, p < 0.001), sex composition (χ2 = 15962.638, p < 0.001), age composition (χ2 = 602.123, p < 0.001), marital status composition (χ2 = 34.783, p < 0.001), educational level composition (χ2 = 676.157, p < 0.001), occupation composition (χ2 = 533.947, p < 0.001), annual household income (χ2 = 40.365, p < 0.001), and chronic condition composition (χ2 = 41.566, p < 0.001). The chi-square test results showed that the value of ps of all variables were < 0.001, indicating that these variables were correlated with ECIG use and could be included in subsequent logistic regression models as covariables.
Multinomial logistic regression was performed to explore the factors associated with ECIG use (Table 2). In addition, there were significant associations between HL and the two patterns of ECIG use. Based on the OR values, people were more likely to use both CIG and ECIG (OR = 0.638, p < 0.001) than they were to exclusively use ECIG (OR = 0.457, p < 0.001). Sex was also associated with ECIG and CIG use. Males were more likely to use ECIG and CIG than females (ORCIG = 226.579, p < 0.001; ORECIG = 3.352, p < 0.001; ORdual use = 74.780, p < 0.001). Middle-aged (25–64 years) people were more likely to dual use CIG/ECIG than older (≥65) people (OR25–44 = 4.138, p < 0.001; OR45–64 = 2.377, p < 0.001). Younger people (15–24 years) were more likely to dual use CIG and ECIG (OR = 4.955, p < 0.001) than CIG-exclusive use (OR = 0.398, p < 0.398). ECIG-exclusive users were mainly concentrated among those aged 25–44 (OR = 2.222, p < 0.01). People who were single, widowed, or divorced were more likely to use ECIG and CIG (ORCIG = 1.210, p < 0.001; ORECIG = 1.560, p < 0.05; ORdual use = 1.397, p < 0.05) than married individuals. Educational level, occupation, annual household income, and chronic conditions were associated with CIG-exclusive use. However, these variables were not associated with ECIG-exclusive use. Occupation, annual household income, and chronic conditions were associated with dual use.
In our study, ECIG users were divided into ECIG-exclusive and CIG/ECIG dual user groups. To the best of our knowledge, this is the first study to describe the association between HL and different types of ECIG use among Chinese citizens. Our study demonstrates that HL is a protective factor against ECIG use behavior, and the effect is stronger for ECIG-exclusive use.
The HL level in this study (30.8%) was slightly higher than the national level (27.8%), but similar to that in the eastern region (31.9%) (36). This was because Zhejiang Province is located in the eastern part of China, where the urbanization rate is relatively high, and the economic level and education level are higher than the national average. Studies have shown that economic level and education level have a significant impact on residents’ HL (37, 38). The prevalence of CIG (19.7%) and ECIG (1.0%) in the study sample were both lower than the national level in 2018 (CIG 26.6%; ECIG 1.6%) (11, 30). This was mainly because the smoking rate varies greatly among different provinces, with the highest in the southwest and lowest in the eastern region (southwest China is the country’s main tobacco producing region, while eastern cities have stricter anti-smoking measures); Zhejiang Province is an eastern province with a lower smoking rate (39).
Adequate HL was significantly associated with lower odds of ECIG-exclusive use. According to previous studies, ECIG is generally considered to be less harmful than CIG but is still a health hazard (6, 40). Because HL helps people choose healthy behaviors (15, 16), people with adequate HL are more likely to be aware of the dangers of ECIG and reduce its use. However, previous studies have not reached such a conclusion (21, 23). We believe that this is mainly due to differences in the study samples. Previous studies have limited their sample groups to certain subgroups, such as college students, older adults, or those with a history of smoking. Our sample covers a wide range of people and is more representative. The variation in HL in the sample population was larger than that in previous studies; therefore, we could find an association between HL and ECIG that had not been found previously.
HL was also significantly associated with dual use after adjusting for several covariates. People with adequate HL were less likely to dual use CIG and ECIG. An American study found an association between oral HL and dual use of CIG and ECIG (21), which is consistent with our findings. As mentioned, people with high HL can realize the harm of ECIG and reduce its use. Previous studies have also shown that people with high HL will reduce the use of CIG (19); thus, people with high HL have lower odds of dual use.
We found that dual users had a higher OR than ECIG-exclusive users, indicating that people are more likely to engage in dual use of CIG/ECIG than be ECIG-exclusive users. A previous study found a high proportion of dual use among ECIG users in China (11). This is mainly because current conventional smokers are more likely to use ECIG than nonsmokers. Conventional smokers have lower HL levels than non-smokers, leaving them more receptive to ECIG products; however, conventional smokers may also have increased exposure to information about new tobacco products, such as ECIG. When conventional smokers begin using ECIG, they may abandon their CIG. However, based on the low smoking cessation rate in China (39, 41), we infer that most conventional smokers will continue to use CIG after exposure to ECIG and become dual users rather than ECIG-exclusive users.
Additionally, we found that young age was associated with ECIG use; ECIG were most popular among adolescents and young adults. This is consistent with past findings (6, 7, 11). Unsurprisingly, males were more likely to use ECIG, but the gap between males and females is smaller than that for CIG, suggesting that ECIG are more attractive to females than CIG. Because the effects of ECIG on fetal brain development are unknown (42, 43), policymakers should pay more attention to female ECIG users when developing control programs. Notably, the highest income group was the most likely to use ECIG. This implies that public knowledge about the harm of ECIG remains low. Another explanation is that ECIG were first launched in China as a luxury product targeted to high-income earners (44). Further, married individuals were less likely to use both CIG and ECIG, which may have been due to family requirements (45) or fertility concerns (46). Chronic patients are less likely to use CIG and ECIG because they curtail their unhealthy habits when they perceive that their physical condition is worsening.
There are some limitations in this study. First, the sample of this study was collected in Zhejiang Province. Because of differences in HL levels and smoking/vaping rates across the country, we cannot generalize these results to other provinces. Second, because this study adopted a cross-sectional research design, we cannot prove a causal relationship between HL and ECIG use. Despite the above limitations, the results of this study demonstrated an association between HL and ECIG use, providing evidence for policy makers to control EIG use. Specifically, limiting adolescents’ ECIG use can begin with HL. Future studies should continue to explore the causal relationship and specific impact mechanisms of HL and ECIG use.
In conclusion, HL is a protective factor against both patterns of ECIG use, especially ECIG-exclusive use. Adequate HL was associated with lower odds of ECIG-exclusive and dual use. Thus, health policymakers and public health practitioners should consider increasing HL as a potential measure for ECIG control. Other factors associated with ECIG use were young age, male sex, unmarried status, high-income status, and absence of chronic disease. Health policymakers should pay more attention to people with these characteristics and implement targeted ECIG control measures, including improving their HL.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving humans were approved by Zhejiang Provincial Center for Disease Control and Prevention, Hangzhou, China. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required from the participants or the participants' legal guardians/next of kin in accordance with the national legislation and institutional requirements.
XuZ: Data curation, Investigation, Project administration, Writing – review & editing. XiZ: Writing – original draft, Writing – review & editing, Methodology, Software. SZ: Software, Writing – review & editing. LG: Methodology, Writing – review & editing. YX: Data curation, Writing – review & editing. DY: Data curation, Investigation, Writing – review & editing. XH: Validation, Writing – review & editing. ZH: Writing – review & editing. TZ: Validation, Writing – review & editing. ZW: Conceptualization, Supervision, Writing – review & editing. CC: Conceptualization, Project administration, Supervision, Writing – review & editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This work was supported by the National Natural Science Foundation of China [grant number 72274141]; National Social Science Foundation of China [grant number BIA200197]; Zhejiang Provincial Nature Foundation [grant number LY22G030006]; Philosophy and Social Science Project of Zhejiang Province, China [grant number 22NDJC104YB]; 2023 Joint Project of Science and Technology Department of National Administration of Traditional Chinese Medicine and Zhejiang Administration of Traditional Chinese Medicine [grant number GZY-ZJ-KJ-23084]; Point Leader Research and Development Project [grant number 2022C03G1890052]; 2023 Leading Talents Program [grant number 2023C03165].
The authors thank the 2022 China Health Literacy Survey team for their hard work and unselfish sharing of survey data. We also acknowledge the Editage editorial team for their English editing.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2023.1321457/full#supplementary-material
1. Pan, B, Jin, X, Jun, L, Qiu, S, Zheng, Q, and Pan, M. The relationship between smoking and stroke: a meta-analysis. Medicine. (2019) 98:e14872. doi: 10.1097/MD.0000000000014872
2. Kondo, T, Nakano, Y, Adachi, S, and Murohara, T. Effects of tobacco smoking on cardiovascular disease. Circulation journal: official journal of the Japanese Circulation Society. (2019) 83:1980–5. doi: 10.1253/circj.CJ-19-0323
3. Larsson, SC, Carter, P, Kar, S, Vithayathil, M, Mason, AM, Michaëlsson, K, et al. Smoking, alcohol consumption, and cancer: a mendelian randomisation study in UK biobank and international genetic consortia participants. PLoS Med. (2020) 17:e1003178. doi: 10.1371/journal.pmed.1003178
4. Linnansaari, A, Ollila, H, Pisinger, C, Scheffels, J, Kinnunen, JM, and Rimpelä, A. Towards tobacco-free generation: implementation of preventive tobacco policies in the Nordic countries. Scand J Public Health. (2022) 51:1108–1121. doi: 10.1177/14034948221106867 [Epub ahead of print].
5. China TSCIOotPsRo . Regulations for controlling smoking in public places (2014) Available at: http://www.scio.gov.cn/xwfbh/xwbfbh/wqfbh/2015/33038/xgbd33046/Document/1439368/1439368.htm.
6. Dockrell, M, Morrison, R, Bauld, L, and McNeill, A. E-cigarettes: prevalence and attitudes in Great Britain. Nicotine & tobacco research: official journal of the Society for Research on Nicotine and Tobacco. (2013) 15:1737–44. doi: 10.1093/ntr/ntt057
7. Dai, H, and Leventhal, AM. Prevalence of e-cigarette use among adults in the United States, 2014-2018. JAMA. (2019) 322:1824–7. doi: 10.1001/jama.2019.15331
8. Cullen, KA, Gentzke, AS, Sawdey, MD, Chang, JT, Anic, GM, Wang, TW, et al. E-cigarette use among youth in the United States, 2019. JAMA. (2019) 322:2095–103. doi: 10.1001/jama.2019.18387
9. Meo, SA, and Al Asiri, SA. Effects of electronic cigarette smoking on human health. Eur Rev Med Pharmacol Sci. (2014) 18:3315–9.
10. Bold, KW, Krishnan-Sarin, S, and Stoney, CM. E-cigarette use as a potential cardiovascular disease risk behavior. Am Psychol. (2018) 73:955–67. doi: 10.1037/amp0000231
11. Zhao, Z, Zhang, M, Wu, J, Xu, X, Yin, P, Huang, Z, et al. E-cigarette use among adults in China: findings from repeated cross-sectional surveys in 2015-16 and 2018-19. Lancet Public Health. (2020) 5:e639–49. doi: 10.1016/S2468-2667(20)30145-6
12. Administration SAfMRaSTM . Notice on prohibiting the sale of electronic cigarettes to minors (2018) Available at: https://www.gov.cn/zhengce/zhengceku/2018-12/31/content_5438414.htm.
13. Administration SAfMRaSTM . Notice on further protecting minors from electronic cigarettes (2019) Available at: https://www.gov.cn/gongbao/content/2020/content_5488930.htm.
14. Institute of Medicine Committee on Health L. In: L Nielsen-Bohlman, AM Panzer, and DA Kindig, editors. Health literacy: A prescription to end confusion. Washington (DC): National Academies Press (US) (2004)
15. Fleary, SA, Joseph, P, and Pappagianopoulos, JE. Adolescent health literacy and health behaviors: a systematic review. J Adolesc. (2018) 62:116–27. doi: 10.1016/j.adolescence.2017.11.010
16. Liu, YB, Liu, L, Li, YF, and Chen, YL. Relationship between health literacy, health-related behaviors and health status: a survey of elderly Chinese. Int J Environ Res Public Health. (2015) 12:9714–25. doi: 10.3390/ijerph120809714
17. Fawns-Ritchie, C, Starr, JM, and Deary, IJ. Health literacy, cognitive ability and smoking: a cross-sectional analysis of the English longitudinal study of ageing. BMJ Open. (2018) 8:e023929. doi: 10.1136/bmjopen-2018-023929
18. Harsch, S, Jawid, A, Jawid, E, Saboga-Nunes, L, Sørensen, K, Sahrai, D, et al. Health literacy and health behavior among women in Ghazni, Afghanistan. Front Public Health. (2021) 9:629334. doi: 10.3389/fpubh.2021.629334
19. Stewart, DW, Cano, MA, Correa-Fernández, V, Spears, CA, Li, Y, Waters, AJ, et al. Lower health literacy predicts smoking relapse among racially/ethnically diverse smokers with low socioeconomic status. BMC Public Health. (2014) 14:716. doi: 10.1186/1471-2458-14-716
20. Panahi, R, Osmani, F, Javanmardi, K, Ramezankhani, A, Dehghankar, L, Amini, R, et al. The relationship between different levels of health literacy and smoking prevention among medical sciences student. Int J Prev Med. (2021) 12:124. doi: 10.4103/ijpvm.IJPVM_460_20
21. Clifford, JS, Lu, J, Blondino, CT, Do, EK, and Prom-Wormley, EC. The association between health literacy and tobacco use: results from a nationally representative survey. J Community Health. (2022) 47:63–70. doi: 10.1007/s10900-021-01019-7
22. Duplaga, M, and Grysztar, M. The use of E-cigarettes among high school students in Poland is associated with health locus of control but not with health literacy: a cross-sectional study. Toxics. (2022) 10:41. doi: 10.3390/toxics10010041
23. Marx, JM, Miller, A, Windsor, A, Locke, J, and Frazier, E. Perceptions of cigarettes and e-cigarettes: does health literacy matter? Journal of American college health: J of ACH. (2023) 71:2595–2603. doi: 10.1080/07448481.2021.1979008 [Epub ahead of print].
24. Li, Z, Tian, Y, Gong, Z, and Qian, L. Health literacy and regional heterogeneities in China: a population-based study. Front Public Health. (2021) 9:603325. doi: 10.3389/fpubh.2021.810577
25. Nie, XQLY, and Li, L. Statistical analysis method of 2012 China health literacy survey data. Chin J Health Educ. (2014) 30:178–81. doi: 10.16168/j.cnki.issn.1002-9982.2014.02.021
26. Kish, L . A procedure for objective respondent selection within the household. J Am Stat Assoc. (1949) 44:380–7. doi: 10.1080/01621459.1949.10483314
27. Health CMo. Basic knowledge and skills of people’s health literacy 2016 [cited (2023). Available at: http://www.nhc.gov.cn/xcs/s3582/201601/766ff12e01844a64a80f23949f5d351b.shtml.
28. Shen, M, Hu, M, Liu, S, Chang, Y, and Sun, Z. Assessment of the Chinese resident health literacy scale in a population-based sample in South China. BMC Public Health. (2015) 15:637. doi: 10.1186/s12889-015-1958-0
29. Rong, H, Cheng, X, Garcia, JM, Zhang, L, Lu, L, Fang, J, et al. Survey of health literacy level and related influencing factors in military college students in Chongqing, China: a cross-sectional analysis. PLoS One. (2017) 12:e0177776. doi: 10.1371/journal.pone.0177776
30. Commission NH . (2020). Available at: https://www.gov.cn/xinwen/2021-05/30/content_5613994.htm.
31. Prevention CCfDCa. China Adult Tobacco Survey (2018). Available at: https://www.chinacdc.cn/jkzt/sthd_3844/slhd_12885/201905/t20190530_202932.html.
32. Ramsey, MW Jr, Chen-Sankey, JC, Reese-Smith, J, and Choi, K. Association between marital status and cigarette smoking: variation by race and ethnicity. Prev Med. (2019) 119:48–51. doi: 10.1016/j.ypmed.2018.12.010
33. Wang, Q, Shen, JJ, Sotero, M, Li, CA, and Hou, Z. Income, occupation and education: are they related to smoking behaviors in China? PLoS One. (2018) 13:e0192571. doi: 10.1371/journal.pone.0192571
34. Carnazza, G, Liberati, P, Resce, G, and Molinaro, S. Smoking and income distribution: inequalities in new and old products. Health policy (Amsterdam, Netherlands). (2021) 125:261–8. doi: 10.1016/j.healthpol.2020.11.012
35. Wang, X, Zhang, T, Wu, J, Yin, S, Nan, X, Du, M, et al. The association between socioeconomic status, smoking, and chronic disease in Inner Mongolia in northern China. Int J Environ Res Public Health. (2019) 16:169. doi: 10.3390/ijerph16020169
36. China NHCotPsRo. Health literacy monitoring of Chinese residents in (2022) Available at: https://www.gov.cn/govweb/lianbo/bumen/202308/content_6899405.htm.
37. Zheng, Q, Peng, Z, and Ding, S. Financial Literacy Health engagement, and Residents' health: evidence from China. Int J Environ Res Public Health. (2021) 18:4202. doi: 10.3390/ijerph18084202
38. Park, CL, Cho, D, and Moore, PJ. How does education lead to healthier behaviours? Testing the mediational roles of perceived control, health literacy and social support. Psychol Health. (2018) 33:1416–29. doi: 10.1080/08870446.2018.1510932 [Epub ahead of print].
39. Zhang, M, Yang, L, Wang, L, Jiang, Y, Huang, Z, Zhao, Z, et al. Trends in smoking prevalence in urban and rural China, 2007 to 2018: findings from 5 consecutive nationally representative cross-sectional surveys. PLoS Med. (2022) 19:e1004064. doi: 10.1371/journal.pmed.1004064
40. Dai, HD, Ratnapradipa, K, Michaud, TL, King, KM, Guenzel, N, Tamrakar, N, et al. Vaping media literacy, harm perception, and susceptibility of E-cigarette use among youth. Am J Prev Med. (2022) 63:852–60. doi: 10.1016/j.amepre.2022.05.012
41. Rababah, JA, and Al-Hammouri, MM. Health literacy and smoking habits among a sample of Jordanian university students. J Community Health. (2023) 48:30–7. doi: 10.1007/s10900-022-01139-8
42. Sailer, S, Sebastiani, G, Andreu-Férnández, V, and García-Algar, O. Impact of nicotine replacement and electronic nicotine delivery systems on fetal brain development. Int J Environ Res Public Health. (2019) 16:5113. doi: 10.3390/ijerph16245113
43. Xiao, L, Parascandola, M, Wang, C, and Jiang, Y. Perception and current use of E-cigarettes among youth in China. Nicotine & tobacco research: official journal of the Society for Research on Nicotine and Tobacco. (2019) 21:1401–7. doi: 10.1093/ntr/nty145
44. Eric, A, and Feldman, CY. E-cigarette regulation in China: the road ahead. Faculty Scholarship. (2017):1704. Available at: https://scholarship.law.upenn.edu/alr/vol11/iss3/2
45. Ukai, T, Tabuchi, T, and Iso, H. The impact of spousal behavior changes on smoking, drinking and physical activity: the longitudinal survey of middle-aged and elderly persons in Japan. Prev Med. (2022) 164:107293. doi: 10.1016/j.ypmed.2022.107293
Keywords: health literacy, electronic cigarettes, conventional cigarettes, dual use, multinomial logistic regression, 2022 China health literacy survey
Citation: Zhang X, Zhang X, Zhang S, Ge L, Xu Y, Yao D, Hu X, Huang Z, Zhu T, Wang Z and Chen C (2024) The association between health literacy and e-cigarette use: evidence from Zhejiang, China. Front. Public Health. 11:1321457. doi: 10.3389/fpubh.2023.1321457
Edited by:
Maryam Khazaee-Pool, Mazandaran University of Medical Sciences, IranReviewed by:
Rahma Panahi, Tarbiat Modares University, IranCopyright © 2024 Zhang, Zhang, Zhang, Ge, Xu, Yao, Hu, Huang, Zhu, Wang and Chen. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Zixia Wang, VGltb25iZWV0bGVAZm94bWFpbC5jb20=; Chun Chen, Y2hlbmNodW40MDhAMTI2LmNvbQ==
†These authors have contributed equally to this work and share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.