 Vanessa Wenig1*
Vanessa Wenig1* Eileen Heumann1
Eileen Heumann1 Christiane Stock1,2
Christiane Stock1,2 Heide Busse3
Heide Busse3 Sarah Negash4
Sarah Negash4 Claudia R. Pischke5
Claudia R. Pischke5 Katherina Heinrichs1
Katherina Heinrichs1- 1Charité – Universitätsmedizin Berlin, corporate member of Freie Universität Berlin and Humboldt-Universität zu Berlin, Institute of Health and Nursing Science, Berlin, Germany
- 2Unit for Health Promotion Research, University of Southern Denmark, Esbjerg, Denmark
- 3Department Prevention and Evaluation, Leibniz Institute for Prevention Research and Epidemiology—BIPS, Bremen, Germany
- 4Institute for Medical Epidemiology, Biometrics and Informatics, Interdisciplinary Center for Health Sciences, Medical School of the Martin-Luther University Halle-Wittenberg, Halle, Germany
- 5Institute of Medical Sociology, Centre for Health and Society, Medical Faculty, Heinrich-Heine-University Duesseldorf, Duesseldorf, Germany
Introduction: University students are at high risk for loneliness with a potential negative impact on health. The COVID-19 measures disrupted students’ academic routine and social life, which might have affected their perception of loneliness. This study investigated the prevalence of perceived loneliness among university students in Germany during the COVID-19 pandemic and its associations with mental health, behavioral outcomes, and sociodemographic characteristics.
Methods: COVID-19 German student well-being study (C19 GSWS) collected data from five German universities from October 27th to November 14th, 2021, resulting in a sample of 7,203 respondents. Associations of loneliness with depressive symptoms, anxiety, social and physical activity, as well as sociodemographic characteristics, were analyzed using multivariable logistic regressions.
Results: A total of 20.6% of students reported loneliness. Students with depressive or anxiety symptoms had more than eight- or sixfold odds, respectively, for reporting loneliness (depressive symptoms: OR = 8.29; 95% CI: 7.21–9.52; anxiety: OR = 6.48; 95% CI: 5.65–7.43) compared with students who did not report any symptoms. Students who were less physically active were more likely to experience loneliness compared with students who were more physically active (no moderate physical activity: OR = 1.39; 95% CI: 1.21–1.59; no vigorous physical activity: OR = 1.19; 95% CI: 1.04–1.36). We found no association between loneliness and social activity. However, loneliness was associated with being single (OR = 2.93; 95% CI: 2.55–3.36), living alone (OR = 1.31; 95% CI: 1.13–1.52), or having a temporary residency status in Germany (OR = 2.24; 95% CI: 1.65–3.04).
Conclusion: Our findings highlight the importance of loneliness as a relevant factor associated with health. Further research is needed to determine potential protective factors to tackle loneliness and to investigate how study conditions at higher education institutions may affect students’ perceived loneliness.
1. Introduction
Feeling lonely is an unpleasant individual experience, which is not synonymous with social or objective isolation. Loneliness occurs when the network of social relations is quantitatively or qualitatively insufficient (1). Whether or not social networks are considered to be deficient depends on the individual relationship correlates (e.g., relationship aims, type of relationship) (2). Evidence suggests that a sense of belongingness or social connectedness might act as a buffer against loneliness (3). Conversely, the lack of social connectedness might result in feelings of loneliness (4).
Evidence further suggests that loneliness is associated with an increased all-cause mortality (5), being female (6–9), living alone (7–9), and being single (8, 9). Loneliness is also strongly linked to mental health: depression, generalized anxiety disorder, and suicidality have been shown to be strongly associated with loneliness (8, 10, 11). Moreover, loneliness is an important predictor of long-term health and is not only limited to older individuals (12). Adolescents and young adults are also widely affected by feelings of loneliness, and strong associations with depressive symptoms and anxiety have been demonstrated (12, 13). Generally, previous research indicated that loneliness, anxiety, and depression were distinct but interrelated phenomena (11, 14). Furthermore, loneliness in youth is a relevant predictor of the health status in adulthood (15) and correlates with future mental health problems. As the duration of loneliness in youth seems to be an important predictor for depression later in life, the prevention of loneliness among young people is a pressing issue (16, 17). It appears, therefore, important to identify and address loneliness at an early stage in childhood or in young adulthood in order to prevent its negative effects on mental health later on in life.
The prevalence of perceived loneliness and mental illness among young adults, in particular among university students, is generally at high levels (18–20). Former studies on loneliness among university students and young adults examined associations with age, gender, living situation, relationship status, immigration status, and mental health problems. In general, younger age groups were found to be more likely to experience loneliness (6, 7, 9, 21). Within this age group, younger and older students were reported to have higher feelings of loneliness compared with middle-aged students (19), indicating a U-shaped association between age and loneliness among university students. Similarly, being female (22, 23), living alone (18, 19, 24), being single (18, 19, 23, 25), and studying abroad (19) were associated with more feelings of loneliness. In contrast, some studies could not confirm these associations between loneliness and gender among higher education students (18, 25).
Loneliness is a mental health issue that has received particular attention during the COVID-19 pandemic (26). The pandemic caused governments to implement measures to contain the disease such as school and university closures and social distancing. In Germany, the first lockdown started in March 2020 with easing steps over the subsequent summer. When the incidence rates increased again in autumn 2020 (27), the second lockdown began and lasted until May 2021. Whereas elementary and secondary school students had already been able to return to their institutions earlier, higher education institutions remained closed and, thus, online teaching continued. From April 2022 onwards, universities were reopened throughout Germany and returned to face-to-face teaching.
Some studies found that during the pandemic, social isolation and its consequences led to increased prevalence rates of loneliness (28–30). Especially for children and adolescents, the disease containment measures had effects on their mental health and were associated with increased loneliness (16, 29, 30). Even before the pandemic, loneliness was shown to pose significant health risks in terms of anxiety and depressive symptoms for young adults and students (12, 16, 18). During the pandemic, an increase of mental health issues (31) and loneliness (31, 32) among university students was observed. The pre-existing predictors of loneliness observed prior to the pandemic appeared to remain unchanged throughout the course of the pandemic: Bu et al. (33) found that being female or of younger age, living alone, having lower education or income, and belonging to ethnic minorities were risk factors for loneliness.
To reduce or prevent loneliness, recent studies revealed the benefits of social networks regarding life satisfaction and well-being (34, 35). The social interactions during physical activity (e.g., with other participants or with an instructor) could influence individuals’ perceptions of social support (36). In this sense, physical activity could offer various relationship opportunities and could create a sense of belonging (37). The evidence of the association between physical activity and loneliness is inconclusive. On the one hand, physical activity might reduce feelings of loneliness; on the other hand, loneliness may decrease the engagement in physical activity (38). In university students, physical activity seems to be a protective factor against loneliness (18, 39). A low level of physical activity (less than 1 hour per week) was associated with loneliness (18). However, Jennen et al. (40) found that just being physically active was insufficient to have an effect on loneliness. Another study found that young adults had to experience physical activity as enjoyable in order to experience decreased feelings of loneliness (41).
The literature regarding the impact of social contact on loneliness among university students is mixed. Generally, work by Diehl and Hilger (24) revealed that the transitional phase between school and university is often connected with a change of residency and, thus, the loss of existing social networks and close family connections. In a Finnish study, loneliness was associated with less social contact with friends in younger ages (21). However, especially for students, friendships and frequent social contact were beneficial to their mental health during the pandemic (42). Rumas et al. (43) found that a larger social network was accompanied by less loneliness, but frequent virtual contact did not help to reduce loneliness. Earlier studies found that the lack of quality of social contact, rather than quantity, was associated with loneliness (41).
Overall, we conclude from the present literature that university students are at risk of exposure to loneliness and its negative health outcomes. Beutel et al. (8) noted that loneliness should be regarded as a relevant health variable on its own. In order to address the research gaps regarding loneliness and mental health, and the role of social networks, and physical activity for loneliness among university students, the aims of this study were (1) to examine the prevalence of perceived loneliness among German university students in a later phase of the COVID-19-pandemic and (2) to identify factors associated with loneliness. Factors of interest included (2a) anxiety and depressive symptoms, (2b) social and physical activities as well as (2c) sociodemographic characteristics. First, we expected anxiety and depressive symptoms to be positively associated with loneliness. Second, we hypothesized that students who engaged in at least one social activity per week are less likely to feel lonely. In addition, our third hypothesis was that students who were physically active were also less likely to experience feelings of loneliness.
2. Materials and methods
2.1. Study design and procedures
The COVID-19 German student well-being study (C19 GSWS) is a cross-sectional study and followed the COVID-19 International Student Well-being Study (C19 ISWS) (44). The online questionnaire of the C19 GSWS was implemented at five German universities: Charité – Universitätsmedizin Berlin, University of Bremen, University of Siegen, Martin-Luther-University Halle/Wittenberg, and Heinrich-Heine-University Düsseldorf. Using LimeSurvey, data collection was conducted at the same time at all five participating universities between October 27th and November 14th, 2021, i.e., at the beginning of the winter semester. During this time, the learning and teaching situation at German universities varied widely due to different regional COVID-19 regulations. In general, face-to-face interaction was limited in favor of online teaching: only few seminars with smaller learning groups were offered in person, whereas most of the lectures were held remotely throughout the whole winter semester.
The questionnaire used was a modified version of the C19 ISWS questionnaire. The core questionnaire used can be found elsewhere (45). The participants invited were students aged 18 years and above who were enrolled at one of the five universities. University students were invited to participate in the online survey via e-mail, e-learning platforms (Martin-Luther-University Halle/Wittenberg and University of Bremen), or via Instagram (Heinrich-Heine-University Duesseldorf). Students had the option of answering the survey in German or English. More information about the design and recruitment of the C19 GSWS study is available elsewhere (46). Further, the dataset is openly accessible via 10.5281/zenodo.7659845 (47).
All participants gave their informed consent before participating in the survey. The ethics committees of the five participating universities have obtained ethical approval (University of Bremen 2021-28-EIL, University Halle-Wittenberg 2020–066, Heinrich-Heine-University Duesseldorf 2020-958_1, Charité – Universitätsmedizin Berlin and University of Siegen have accepted the ethic vote of the University of Bremen). We used the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guideline for reporting this cross-sectional study (48).
2.2. Measures
2.2.1. Loneliness
Loneliness was assessed with a single item from the Center for Epidemiologic Studies Depression Scale (CES-D) (49): ‘Please indicate how much of the time during the past week you felt lonely’. Response options included: ‘none or almost none of the time’, ‘some of the time’, ‘most of the time’, and ‘all or almost all of the time’. Responses were converted to binary coding to allow for a comparison of those who reported feeling lonely most, almost all and all of the time (in the following referred to as ‘major loneliness’) with those who reported feeling lonely ‘none or almost none of the time’ or ‘some of the time’ (in the following referred to as ‘minor loneliness’ (reference category)).
2.2.2. Anxiety and depressive symptoms
Anxiety symptoms were assessed with the 2-item Generalized Anxiety Disorder Scale (GAD-2), which is based on the GAD-7 (50). The GAD-2 is a valid and reliable instrument for assessing generalized anxiety symptoms in a university context (51). The GAD-2 was conducted with the following basic question: ‘Over the last 2 weeks, how often have you been bothered by the following problems’ and the two items were ‘feeling nervous, anxious, or on edge’ and ‘not being able to stop or control worrying’. For each item, there were the following answer options: (0) ‘not at all’, (1) ‘several days’, (2) ‘more than half the days’, and (3) ‘nearly every day’. The GAD-2 sum score can range from 0 to 6, and as suggested in the literature, we chose a cut-off point of 3 (50) to indicate whether the participants showed anxiety symptoms (0 to 3 ‘no anxiety symptoms’ (reference category); 4 to 6 ‘anxiety symptoms’). The Cronbach’s alpha in our sample was 0.85 for GAD-2.
Depressive symptoms were measured with the short-form version of the Patient Health Questionnaire (PHQ-2) (50, 52). The PHQ-2 includes the first two items (‘feeling down, depressed, or hopeless’ and ‘little interest or pleasure in things’) of the PHQ-9, and we used the same basic question, response options, and cut off as for GAD-2 (53). In addition, the PHQ-2 is also validated in the university context (54). The Cronbach’s alpha in our sample was 0.79 for PHQ-2.
2.2.3. Social activity
A new variable was generated based on 10 items assessing social activity. Participants were asked to indicate whether, in the last week, they had engaged in any of the following activities: (1) a walk with another person; (2) a bike ride with another person; (3) drinks or a picnic with friends or family; (4) talked to friends or family on the street; (5) participated in a recreational class online (e.g., yoga, aerobics, fitness); (6) played a game or a quiz online with friends or family; (7) talked to friends or family through a video-call; (8) talked to friends or family over the phone; (9) chatted with friends or family online (excluding video-calls or phone calls); (10) none of the above. Multiple responses were possible. First, we summed all social activities per participant and second, chose a cutoff >0, similar to Nyqvist et al. (21). This resulted in a new variable with two categories: those who had participated in at least one social activity (reference category) and those who had not participated in any activity in the previous week.
2.2.4. Physical activity
In our study, physical activity was assessed using two items: ‘On average, during the last week, how often did you perform vigorous physical activities like lifting heavy things, running, aerobics, or fast cycling for at least 30 min?’ and ‘On average, during the last week, how often did you perform moderate physical activities like easy cycling or walking for at least 30 min?’. For each item, there were the following answer options: (1) (almost) never; (2) less than once a week; (3) once a week, (4) more than once a week; (5) (almost) daily. For the analysis, we recoded the variables into a binary variable. As suggested by Shankar et al. (55), participants who reported moderate or vigorous physical activity only once a week or less (answers 1–3) were classified as not meeting the criteria for being physically active. Participants who reported levels of physical activity (answers 4–5) were classified as being physically active (reference category).
2.2.5. Sociodemographic characteristics
We included the following variables in our analyses: self-identification with gender (‘female’, ‘male’, ‘diverse’), age (categorized into ‘between 18 and 20 years old’, ‘between 21 and 25 years old’, and ‘aged 26 and older’, as done by Hysing et al. (19)), relationship status (‘single’, ‘in a relationship’, ‘it is complicated’), residence status in Germany (‘permanent residency’ and ‘temporary residency’), and living situation (‘living alone’ and ‘living with other persons in the household’).
2.3. Data analyses
First, frequencies were calculated for sociodemographic characteristics, as well as prevalence of loneliness, by the different sociodemographic characteristics. Second, a multivariable logistic regression model was employed to examine the associations of social activity, physical activity, and sociodemographic variables as independent variables with loneliness as dependent variable. The co-variates included in the model were age, gender, relationship status, living situation, and residency status. Thus, the regression model was adjusted for all variables included simultaneously in a single block. Third, two multivariable logistic regression models for anxiety and depressive symptoms as independent variables were carried out to determine associations with loneliness as dependent variable, adjusting for sociodemographic characteristics (age, gender, relationship status, living situation, and residency status). Respondents with missing values in the variables of interest were excluded from the regression models. Before entering the independent variables into the models, we tested for multicollinearity. Correlations between the independent variables were low (r < 0.70), indicating that multicollinearity was not a confounding factor in the analysis. The results from the logistic regression analyses were presented as odds ratios (ORs) with 95 percent confidence intervals (CIs). All statistical analyses were performed with IBM SPSS, version 26, on a Windows 10 Education system.
3. Results
The sociodemographic characteristics of the sample are presented in Table 1. Of the 7,203 students in the sample, most identified themselves as female (67.9%) and were between 21 and 25 years old (54.4%). A little more than half of the participants were not in a steady relationship and were either single (52.8%) or had a complicated relationship status (4.2%). Further, most of the participants lived together with others (78.8%) and had a permanent residency in Germany (96.3%). Almost half of the students were currently enrolled in a bachelor’s program (47.2%), one quarter was enrolled in a health-related field of study (26.4%), and the largest proportions were studying in Halle/Wittenberg (30.1%), Bremen (25.3%) and Siegen (21.7%). Most of the students (91.0%) participated in at least one social activity within the last week. Regarding moderate and vigorous physical activity in the last week, 31.7% or 58.1%, respectively, of the participants were physically inactive.
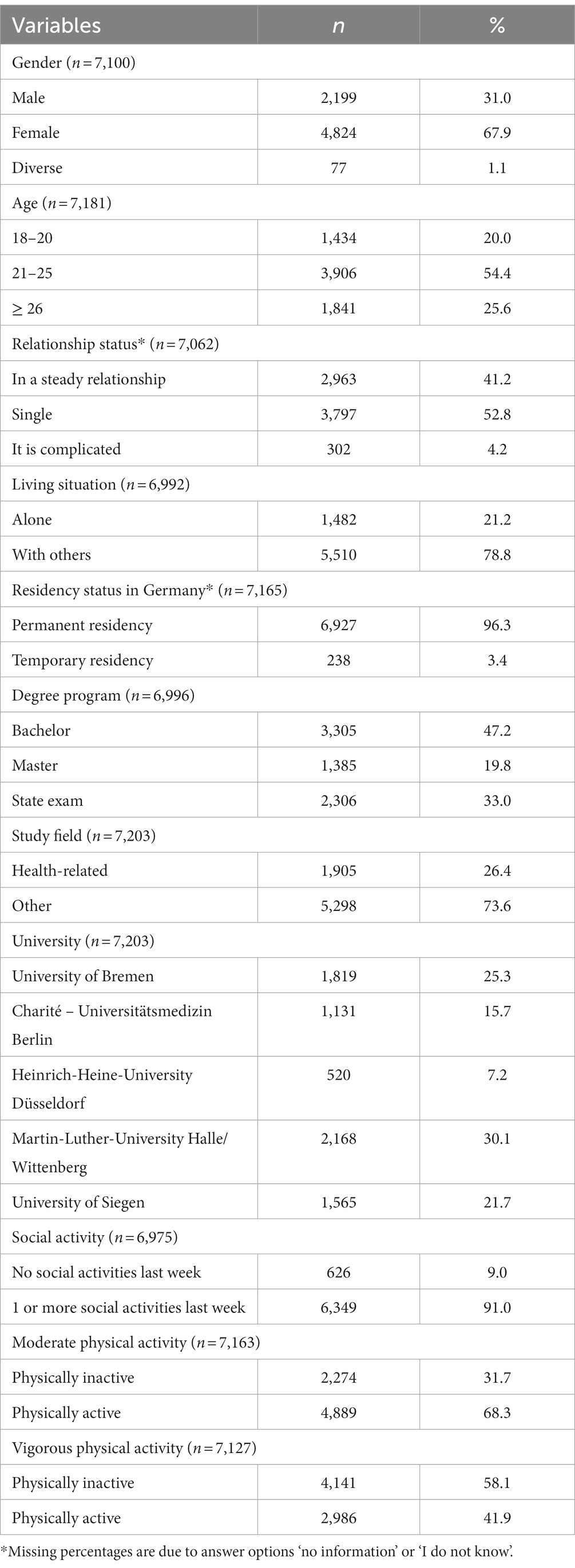
Table 1. Characteristics of the sample (n = 7,203).
Table 2 presents self-reported major loneliness in the overall sample. In total, 20.6% of the students reported major loneliness in the past week. Feelings of major loneliness were more prevalent among participants being single (29.6%), living alone (26.2%), or having a temporary residency in Germany (38.1%). See prevalence of major loneliness by sociodemographic characteristics in Table 3.
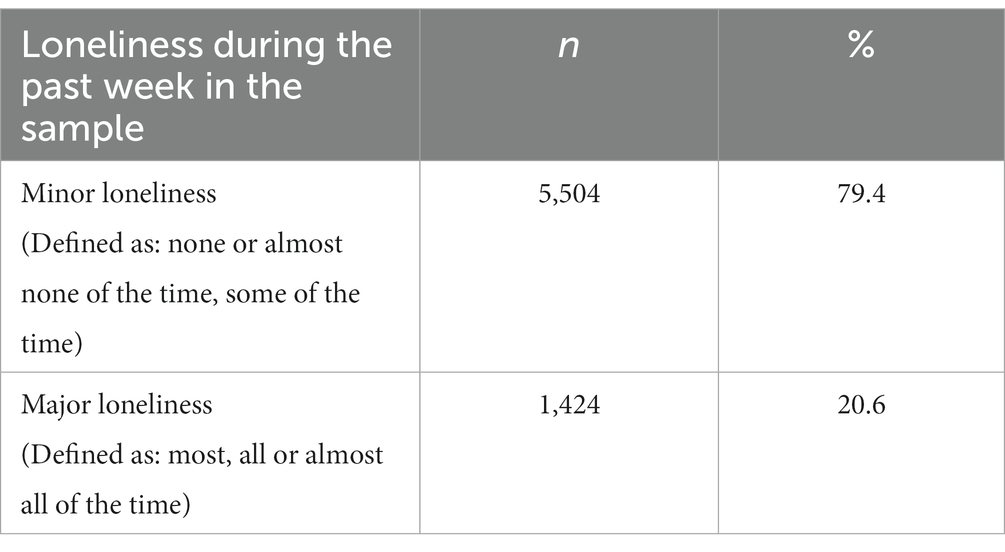
Table 2. Prevalence of loneliness in the sample (n = 6,928).
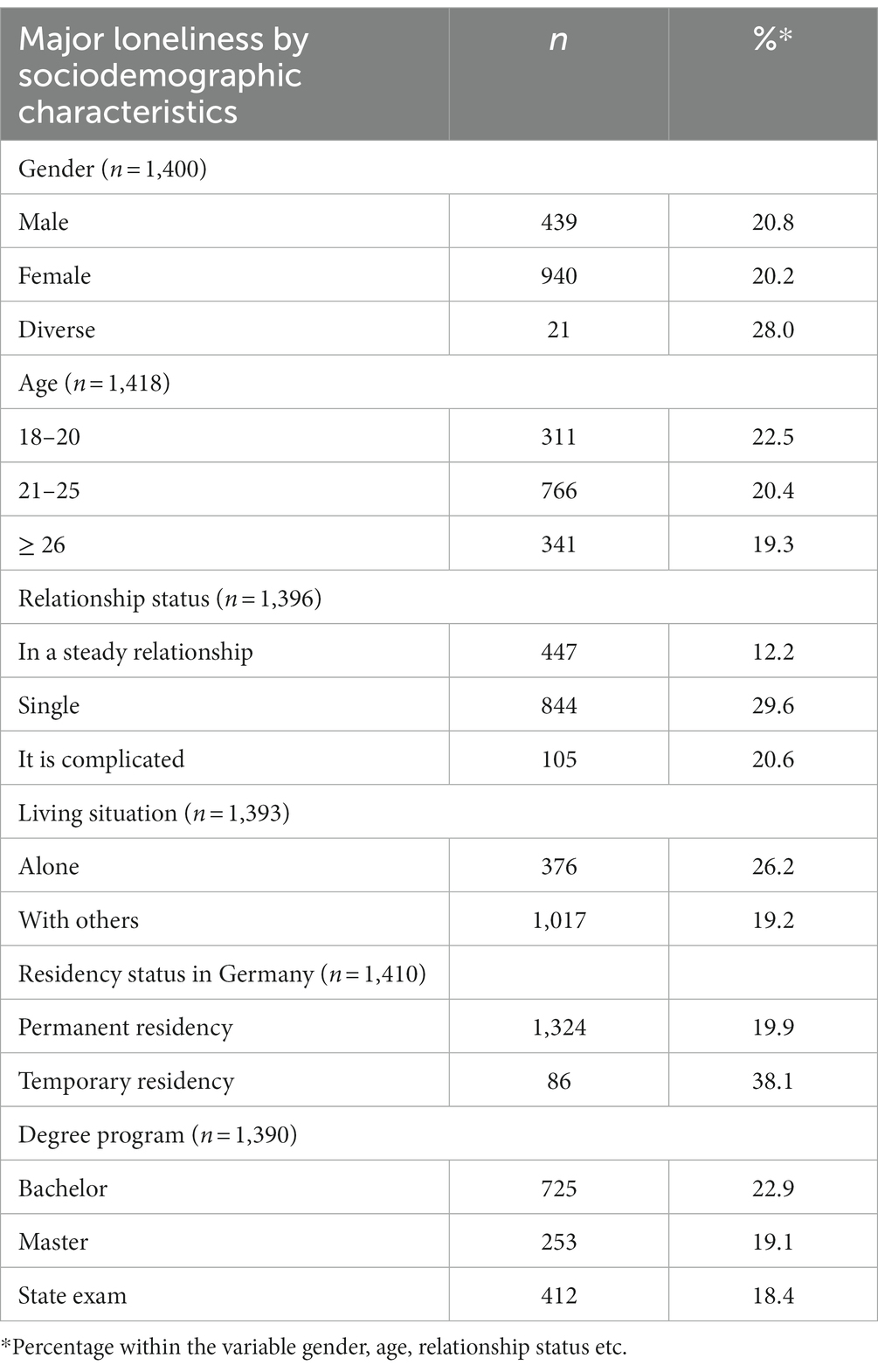
Table 3. Prevalence of major loneliness by sociodemographic characteristics.
Table 4 presents the results of the multivariable logistic regression analysis to determine the associations of social activity, physical activity, and sociodemographic characteristics with loneliness as dependent variable. There was no association between feelings of loneliness and participation in social activities. Being physically inactive was associated with major loneliness (no moderate physical activity: OR = 1.39; 95% CI: 1.21–1.59; no vigorous physical activity: OR = 1.19; 95% CI: 1.04–1.36). Furthermore, the analysis showed that the odds of experiencing major loneliness increased for students being single (OR = 2.93; 95% CI: 2.55–3.36), reporting a complicated relationship status (OR = 3.86; 95% CI: 2.94–5.08), living alone (OR = 1.31; 95% CI: 1.13–1.52), or having a temporary residency in Germany (OR = 2.24; 95% CI: 1.65–3.04).
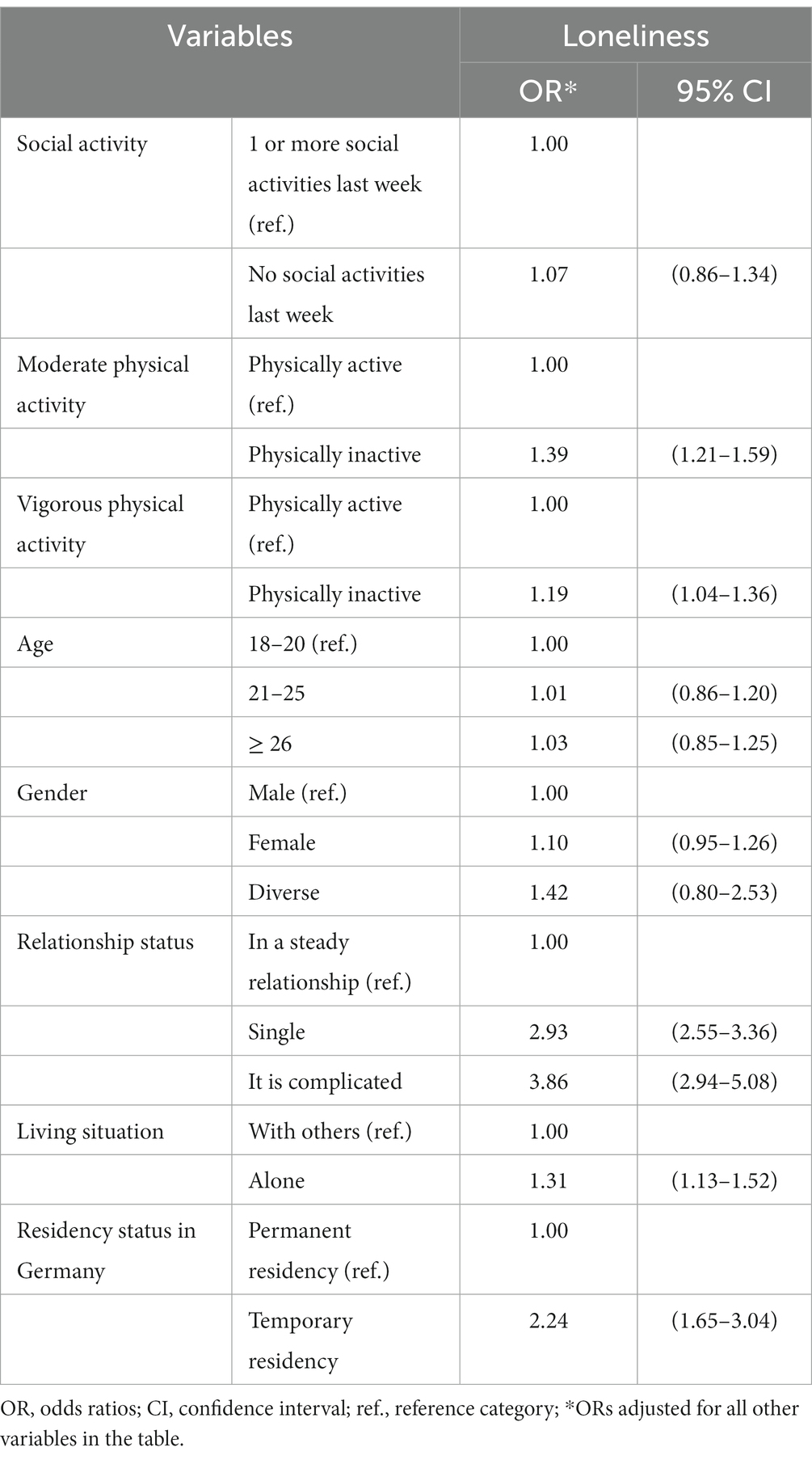
Table 4. Associations between social activity, moderate and vigorous physical activity and loneliness as dependent variable: a multivariable logistic regression model (n = 6,396).
Table 5 and Table 6 present the results of the regression models analyzing the associations between depressive symptoms and anxiety, respectively, as independent variables, and loneliness as dependent variable, while controlling for sociodemographic variables. We found a more than eightfold chance of suffering from loneliness among students who reported depressive symptoms (OR = 8.29; CI: 7.21–9.52), compared with students in the reference group. Reporting anxiety symptoms was also associated with a more than sixfold likelihood for reporting loneliness (OR = 6.48; CI: 5.65–7.43).
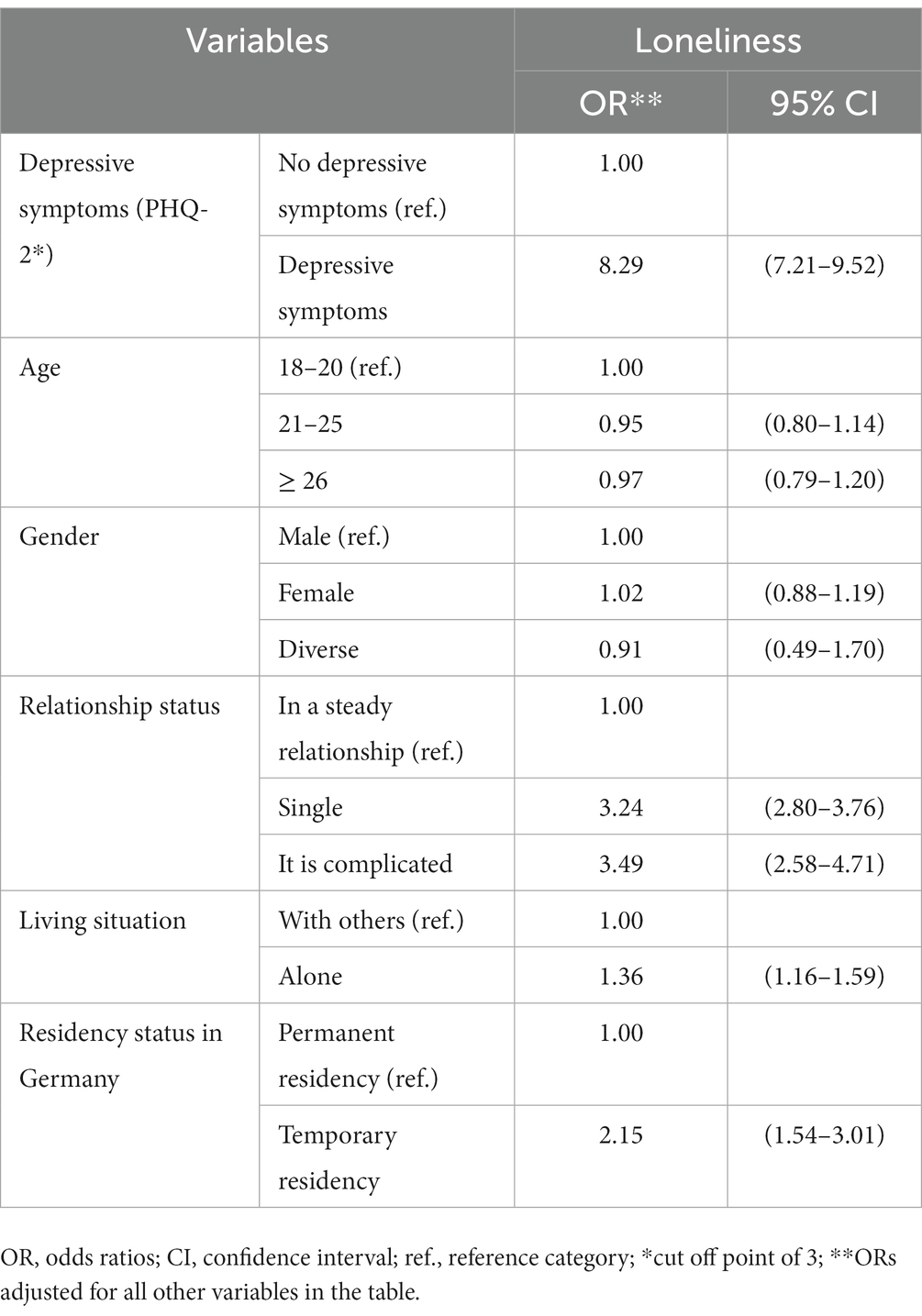
Table 5. Associations between depressive symptoms and loneliness as dependent variable: a multivariable logistic regression model (n = 6,499).
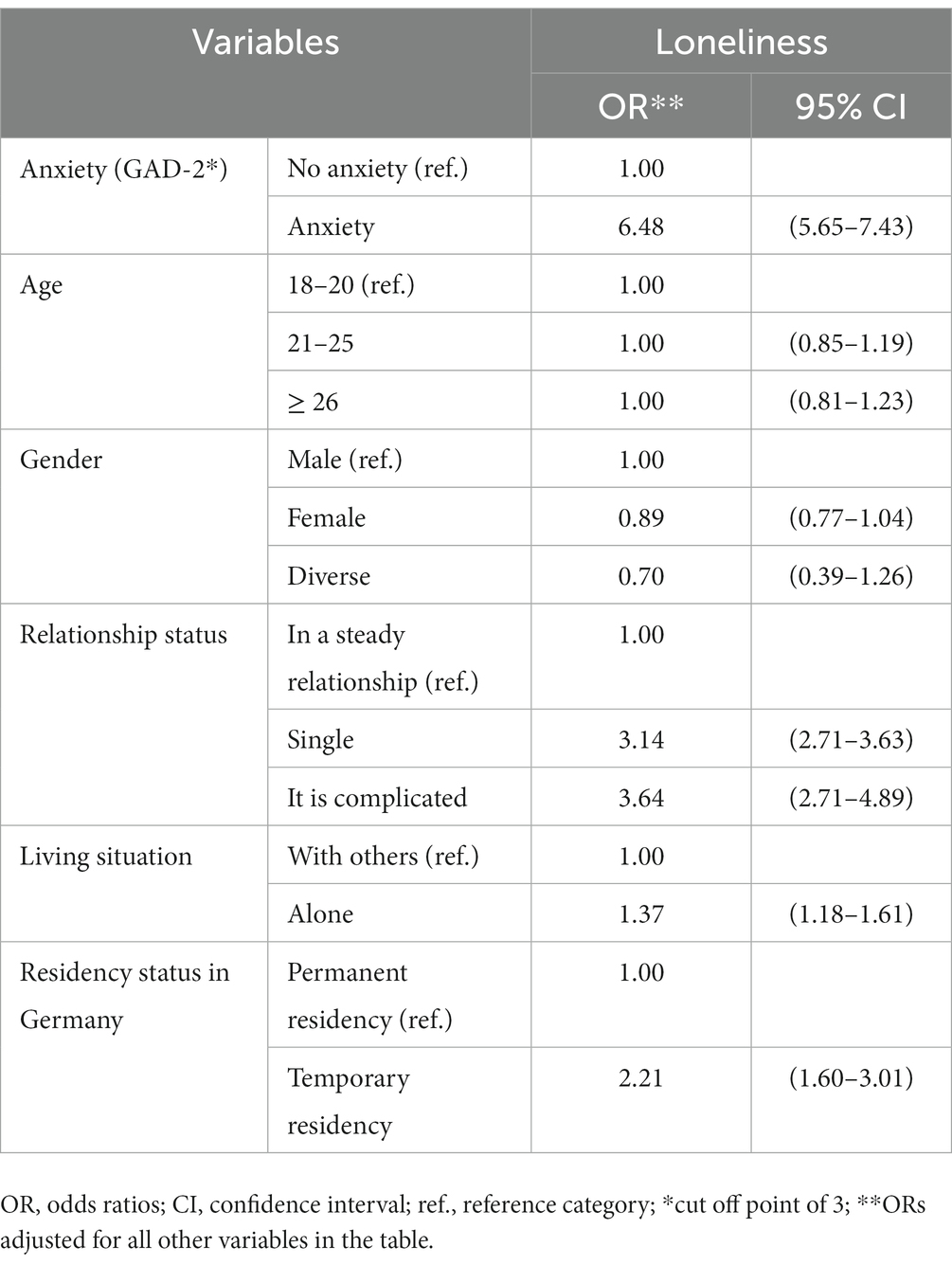
Table 6. Associations between anxiety and loneliness as dependent variable: a multivariable logistic regression model (n = 6,498).
4. Discussion
This study investigated the prevalence of loneliness among university students and its association with mental health, social and physical activity, as well as sociodemographic characteristics, during the late phase of the COVID-19 pandemic at five German universities using the C19 GSWS dataset.
With respect to our first study objective, we found that one-fifth of the respondents reported feelings of loneliness most or almost all the time. Our findings are consistent with and add to previous work showing that the prevalence of loneliness among students is similarly high as before the pandemic in, e.g., Norway (19) and Iran (56). Some previous research showed a lower pre-pandemic prevalence of loneliness among students in Germany (18) and another study, investigating the prevalence of loneliness in the adult population, showed that it was only half that reported in our study (8). It is difficult, however, to make direct comparisons, because different studies used various ways to measure the prevalence of loneliness. In addition, it is important to consider, however, that the risk of infection with the potentially lethal coronavirus caused anxiety and self-isolation (57). Therefore, social isolation can be considered as a normal, non-pathological reaction to cope with the risk of infection during the pandemic (9). According to Shiovitz-Ezra and Ayalon (58), situational loneliness is a temporary experience due to a major change in social life but with the likelihood of fast remission. While situational loneliness might not be a severe problem, suffering from feelings of loneliness over a long period of time could lead to chronic loneliness. Finally, chronic loneliness increases the overall mortality risk (58) and is associated with future mental health problems (16). It remains unclear from our data whether the loneliness reported by our study participants reflects situational or chronic loneliness. As the studies of Zahedi et al. (56) and Hysing et al. (19) showed similar prevalence rates of loneliness among university students before the pandemic, we assume that both situational and chronic loneliness may have contributed to the prevalence rate observed.
Regarding our first hypothesis, our findings are in agreement with the hypothesis and with previous research showing that loneliness is associated with depressive symptoms and anxiety (12, 13). Previous research reported loneliness, anxiety, and depression to be interrelated (11, 14). However, similar to Lee et al. (29), our results also suggest that loneliness could be a crucial mechanism for the increase in depressive symptoms during the pandemic. An important consideration in interpreting the results is that depression is likely to make people rate their social support as insufficient, to let them withdraw from their social network, and to make them feel lonely (10). It is possible that students with stronger social networks experienced greater disruption in their social lives and, as a result, felt lonelier during the pandemic (29). In this context, previous research emphasized that especially COVID-19-specific worries, social and physical isolation, and the lack of interaction were associated with negative mental health outcomes for students (23).
A second aim (2b) of our study was to examine associations between loneliness and social and physical activity. In contrast to our second hypothesis, our analyses did not reveal an association between social activities and loneliness. However, we were only able to consider the number of weekly activities in our analyses. Previous research suggests that simply increasing the number of social contacts is unlikely to be sufficient to reduce loneliness, because loneliness can also be experienced in the company of other people (12). Further, previous research indicated that the quality of social contact, rather than the quantity, is a predictor of loneliness (41, 59). However, the results of Elmer et al. (23) suggested that students with smaller personal networks were more likely to become lonely during the pandemic. In addition, during the pandemic, students were forced to use digital communication with their social networks, and they may have experienced this shift in communication and social interaction as both negative and positive (60). Studies on older adults showed that sharing activities and experiences with peers created a sense of belonging and could decrease feelings of loneliness during the pandemic (61). In addition, Masi et al. (62) found in their meta-analyses, among others, that interventions increasing opportunities for social interaction could reduce loneliness for different age groups. However, the literature on loneliness interventions is inconsistent and mainly available for older age groups (63).
With respect to physical activity, however, we found support for our third hypothesis that loneliness and physical activity were inversely related. Our results are in line with previous research showing that students’ physical activity seems to protect against loneliness (18, 39). Prior evidence showed that the way students experience physical activity is also very important to decrease feelings of loneliness (40). Students may compensate any lack of trustworthy friendships and meaningful social interactions with social bonds in team sports (39). Previous studies suggested that students’ physical activity decreased during the pandemic (64). It is possible that team athletes, in particular, experienced greater social isolation and loneliness during the pandemic, because COVID-19 measures included social distancing and cancelation of team sport activities. More research is needed to disentangle the interplay between different types of physical activity and loneliness.
Regarding sociodemographic variables and their association with loneliness, our results are in line with previous research showing that students being single (18, 19, 23, 25), living alone (18, 19, 24), and studying abroad, i.e., having a temporary residence status (19), are more likely to suffer from loneliness. Moreover, we found no association between gender or age and loneliness, which is consistent with some previous studies (18, 25). Other studies, however, describe that students who are female or younger are more affected by loneliness (22, 23). Such associations with gender and age may be attributed to different sample compositions, a gender imbalance in the samples, and time of data collection. Labrague et al. (22) studied a sample of nursing school students with a high percentage of female students, and Elmer et al. (23) studied a sample of students, mainly from engineering and science programs with a low percentage of female students. Age and gender may be relevant determinants of loneliness within different subject groups. Further, both studies were conducted during the first lockdown in April 2020 (22, 23). This was the students’ first exposure to closed campuses and online teaching. Before the COVID-19 pandemic (18) and later during the first lockdown (23), gender and age were not associated with loneliness. At the time of our survey, it was the fourth semester under the COVID-19 restrictions, so younger and female students may have been able to develop better coping strategies to deal with social isolation.
Overall, our findings confirm that loneliness is a severe mental health outcome among university students, and early intervention is needed to prevent loneliness from persisting over an extended period of time. Our results suggest that close social relationships seem to be an important protective factor, while the number of social activities does not appear to play a significant role. During the pandemic, when students were forced to follow social distancing measures, it seemed to make a considerable difference whether they lived alone, were single, or were international students. Health promotion programs should focus on the role of friendship and promote social contact, especially during the transition phase from school to university and particularly target international students. Overall, physical and social activity may help to connect students in the setting of their university and can be addressed in student health programs. Interventions to reduce loneliness should focus on improving social skills and increasing social support and opportunities for social contact including group based physical activity (62).
5. Strengths and limitations
The multi-center COVID-19 German student well-being study (C19 GSWS) contributes to the existing knowledge on associations of loneliness with depressive symptoms, anxiety and physical activity among university students in Germany during the pandemic based on a large sample. Despite these strengths, the current results could not analyze any differences according to teaching situations across universities during the pandemic and should be interpreted with consideration of several limitations. First, we cannot make a causal claim due to the cross-sectional design. Longitudinal research is needed to distinguish between situational and chronic loneliness, as chronic loneliness has a major impact on health outcomes later on in life. Second, this study used a single-item measure of loneliness, a question from the CES-D (49), which might explain the strong associations of loneliness with mental health outcomes. However, using one single item measure for loneliness is common (8, 58), including the university context (19, 65). Future studies could validate or compare the single item measurement to other validated measures such as the University of California, Los Angeles Loneliness Scale (UCLA Loneliness Scale) (66). Third, the C19 GSWS was performed with a convenience sample and, thus, a selection bias cannot be ruled out. This might have affected the prevalence rates reported in this study. Students with severe loneliness could be less likely to participate which would have led to an under-reporting of loneliness. However, we assume that the effect of any selection bias on the reported associations is low. More than a quarter of the participants were university students of medicine or health-related subjects. Hence, the results are not representative of the general German student population. Similarly, our sample had a higher proportion of female participants which resulted in a gender imbalance. Previous studies have shown the same gender distribution: women are more likely to participate in health-related research (67). However, the effects of this imbalance on the associations presented can be considered as low, since the analysis was adjusted for gender and no significant gender differences in loneliness were found. Furthermore, the present study used self-reported measures. The PHQ-2 and GAD-2 measured the symptoms of the last 2 weeks; the items assessing loneliness, physical activity and social activity only referred to the last week. Although the PHQ-2 and GAD-2 are well-validated scales, interview-based scales are the gold standard for mental health assessment.
6. Conclusion
The present study underlines the importance of loneliness as a relevant health variable among university students. About one in five students reported major feelings of loneliness during the pandemic. We found associations of loneliness with depressive symptoms, anxiety, and physical activity. Loneliness among university students was linked to being single or having a complicated relationship status, living alone, or having a temporary residency in Germany. Unlike other previous research, we did not find associations between loneliness and participation in social activities. Moreover, our results could not identify gender and age as correlates of loneliness among university students. Further research is needed to study potentially protective factors and to investigate how conditions at universities may affect loneliness among students. Students’ health management programs should implement interventions to tackle loneliness and to build a health-promoting study environment.
Data availability statement
The dataset presented and analyzed in this study can be found in an online repository, namely Zenodo: https://zenodo.org/record/7659846.
Ethics statement
The studies involving humans were approved by University of Bremen 2021-28-EIL, University Halle-Wittenberg 2020-066, Heinrich-Heine-University Duesseldorf 2020-958_1, Charité – Universitätsmedizin Berlin and University of Siegen have accepted the ethic vote of the University of Bremen. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
VW: Conceptualization, Methodology, Visualization, Writing – original draft. EH: Conceptualization, Data curation, Writing – review & editing. CS: Conceptualization, Writing – review & editing. HB: Conceptualization, Writing – review & editing. SN: Conceptualization, Writing – review & editing. CP: Conceptualization, Writing – review & editing. KH: Conceptualization, Methodology, Supervision, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. We acknowledge financial support from the Open Access Publication Fund of Charité – Universitätsmedizin Berlin and the German Research Foundation (DFG) for the publication of this article.
Acknowledgments
We thank all university students for their participation in the survey.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Perlman, D, and Peplau, LA. Toward a social psychology of loneliness In: RG SD, editor. Personal relationships: 3 relationships in disorder. London: Academic Press (1981). 31–56.
2. de Jong, GJ, van Tilburg, T, and Dykstra, PA. Loneliness and social isolation In: AL Vangelisti and D Perlman, editors. The Cambridge handbook of personal relationships. Cambridge: Cambridge University Press (2006). 485–500.
3. Mellor, D, Stokes, M, Firth, L, Hayashi, Y, and Cummins, R. Need for belonging, relationship satisfaction, loneliness, and life satisfaction. Pers Individ Differ. (2008) 45:213–8. doi: 10.1016/j.paid.2008.03.020
4. Bowins, B. Chapter 4 - social connectedness In: B Bowins, editor. States and processes for mental health. MA, United States: Academic Press (2021). 41–8.
5. Leigh-Hunt, N, Bagguley, D, Bash, K, Turner, V, Turnbull, S, Valtorta, N, et al. An overview of systematic reviews on the public health consequences of social isolation and loneliness. Public Health. (2017) 152:157–71. doi: 10.1016/j.puhe.2017.07.035
6. Wickens, CM, McDonald, AJ, Elton-Marshall, T, Wells, S, Nigatu, YT, Jankowicz, D, et al. Loneliness in the COVID-19 pandemic: associations with age, gender and their interaction. J Psychiatr Res. (2021) 136:103–8. doi: 10.1016/j.jpsychires.2021.01.047
7. Li, LZ, and Wang, S. Prevalence and predictors of general psychiatric disorders and loneliness during COVID-19 in the United Kingdom. Psychiatry Res. (2020) 291:113267. doi: 10.1016/j.psychres.2020.113267
8. Beutel, ME, Klein, EM, Brähler, E, Reiner, I, Jünger, C, Michal, M, et al. Loneliness in the general population: prevalence, determinants and relations to mental health. BMC Psychiatry. (2017) 17:97. doi: 10.1186/s12888-017-1262-x
9. Ernst, M, Niederer, D, Werner, AM, Czaja, SJ, Mikton, C, Ong, AD, et al. Loneliness before and during the COVID-19 pandemic: a systematic review with meta-analysis. Am Psychol. (2022) 77:660–77. doi: 10.1037/amp0001005
10. Wang, J, Mann, F, Lloyd-Evans, B, Ma, R, and Johnson, S. Associations between loneliness and perceived social support and outcomes of mental health problems: a systematic review. BMC Psychiatry. (2018) 18:156. doi: 10.1186/s12888-018-1736-5
11. Santini, ZI, Jose, PE, York Cornwell, E, Koyanagi, A, Nielsen, L, Hinrichsen, C, et al. Social disconnectedness, perceived isolation, and symptoms of depression and anxiety among older Americans (NSHAP): a longitudinal mediation analysis. Lancet Public Health. (2020) 5:e62–70. doi: 10.1016/S2468-2667(19)30230-0
12. Matthews, T, Danese, A, Caspi, A, Fisher, HL, Goldman-Mellor, S, Kepa, A, et al. Lonely young adults in modern Britain: findings from an epidemiological cohort study. Psychol Med. (2019) 49:268–77. doi: 10.1017/S0033291718000788
13. Christiansen, J, Qualter, P, Friis, K, Pedersen, SS, Lund, R, Andersen, CM, et al. Associations of loneliness and social isolation with physical and mental health among adolescents and young adults. Perspect Public Health. (2021) 141:226–36. doi: 10.1177/17579139211016077
14. Owczarek, M, Nolan, E, Shevlin, M, Butter, S, Karatzias, T, McBride, O, et al. How is loneliness related to anxiety and depression: a population-based network analysis in the early lockdown period. Int J Psychol. (2022) 57:585–96. doi: 10.1002/ijop.12851
15. Goosby, BJ, Bellatorre, A, Walsemann, KM, and Cheadle, JE. Adolescent loneliness and health in early adulthood. Sociol Inq. (2013) 83:505–36. doi: 10.1111/soin.12018
16. Loades, ME, Chatburn, E, Higson-Sweeney, N, Reynolds, S, Shafran, R, Brigden, A, et al. Rapid systematic review: the impact of social isolation and loneliness on the mental health of children and adolescents in the context of COVID-19. J Am Acad Child Adolesc Psychiatry. (2020) 59:1218–1239.e3. doi: 10.1016/j.jaac.2020.05.009
17. Qualter, P, Brown, SL, Munn, P, and Rotenberg, KJ. Childhood loneliness as a predictor of adolescent depressive symptoms: an 8-year longitudinal study. Eur Child Adolesc Psychiatry. (2010) 19:493–501. doi: 10.1007/s00787-009-0059-y
18. Diehl, K, Jansen, C, Ishchanova, K, and Hilger-Kolb, J. Loneliness at universities: determinants of emotional and social loneliness among students. Int J Environ Res Public Health. (2018) 15:1865. doi: 10.3390/ijerph15091865
19. Hysing, M, Petrie, KJ, Bøe, T, Lønning, KJ, and Sivertsen, B. Only the lonely: a study of loneliness among university students in Norway. Clin Psychol Eur. (2020) 2:1–16. doi: 10.32872/cpe.v2i1.2781
20. Auerbach, RP, Alonso, J, Axinn, WG, Cuijpers, P, Ebert, DD, Green, JG, et al. Mental disorders among college students in the World Health Organization world mental health surveys. Psychol Med. (2016) 46:2955–70. doi: 10.1017/S0033291716001665
21. Nyqvist, F, Victor, CR, Forsman, AK, and Cattan, M. The association between social capital and loneliness in different age groups: a population-based study in Western Finland. BMC Public Health. (2016) 16:542. doi: 10.1186/s12889-016-3248-x
22. Labrague, LJ, los Santos JAA, D, and Falguera, CC. Social and emotional loneliness among college students during the COVID-19 pandemic: the predictive role of coping behaviors, social support, and personal resilience. Perspect Psychiatr Care. (2021) 57:1578–84. doi: 10.1111/ppc.12721
23. Elmer, T, Mepham, K, and Stadtfeld, C. Students under lockdown: comparisons of students’ social networks and mental health before and during the COVID-19 crisis in Switzerland. PLoS One. (2020) 15:e0236337. doi: 10.1371/journal.pone.0236337
24. Diehl, K, and Hilger, J. Physical activity and the transition from school to university: a cross-sectional survey among university students in Germany. Sci Sports. (2016) 31:223–6. doi: 10.1016/j.scispo.2016.04.012
25. Werner, AM, Tibubos, AN, Mülder, LM, Reichel, JL, Schäfer, M, Heller, S, et al. The impact of lockdown stress and loneliness during the COVID-19 pandemic on mental health among university students in Germany. Sci Rep. (2021) 11:22637. doi: 10.1038/s41598-021-02024-5
26. Killgore, WDS, Cloonan, SA, Taylor, EC, and Dailey, NS. Loneliness: a signature mental health concern in the era of COVID-19. Psychiatry Res. (2020) 290:113117. doi: 10.1016/j.psychres.2020.113117
27. Schilling, J, Tolksdorf, K, Marquis, A, Faber, M, Pfoch, T, Buda, S, et al. Die verschiedenen Phasen der COVID-19-Pandemie in Deutschland: Eine deskriptive Analyse von Januar 2020 bis Februar 2021. Bundesgesundheitsbl Gesundheitsforsch Gesundheitsschutz. (2021) 64:1093–106. doi: 10.1007/s00103-021-03394-x
28. Buecker, S, and Horstmann, KT. Loneliness and social isolation during the COVID-19 pandemic. Eur Psychol. (2021) 26:272–84. doi: 10.1027/1016-9040/a000453
29. Lee, CM, Cadigan, JM, and Rhew, IC. Increases in loneliness among Young adults during the COVID-19 pandemic and association with increases in mental health problems. J Adolesc Health. (2020) 67:714–7. doi: 10.1016/j.jadohealth.2020.08.009
30. Rogers, AA, Ha, T, and Ockey, S. Adolescents' perceived socio-emotional impact of COVID-19 and implications for mental health: results from a U.S.-based mixed-methods study. J Adolesc Health. (2021) 68:43–52. doi: 10.1016/j.jadohealth.2020.09.039
31. Dogan-Sander, E, Kohls, E, Baldofski, S, and Rummel-Kluge, C. More depressive symptoms, alcohol and drug consumption: increase in mental health symptoms among university students after one year of the COVID-19 pandemic. Front Psych. (2021) 12:790974. doi: 10.3389/fpsyt.2021.790974
32. Weber, M, Schulze, L, Bolzenkötter, T, Niemeyer, H, and Renneberg, B. Mental health and loneliness in university students during the COVID-19 pandemic in Germany: a longitudinal study. Front Psych. (2022) 13:848645. doi: 10.3389/fpsyt.2022.848645
33. Bu, F, Steptoe, A, and Fancourt, D. Who is lonely in lockdown? Cross-cohort analyses of predictors of loneliness before and during the COVID-19 pandemic. Public Health. (2020) 186:31–4. doi: 10.1016/j.puhe.2020.06.036
34. Amati, V, Meggiolaro, S, Rivellini, G, and Zaccarin, S. Social relations and life satisfaction: the role of friends. Genus. (2018) 74:7. doi: 10.1186/s41118-018-0032-z
35. Blieszner, R, Ogletree, AM, and Adams, RG. Friendship in later life: a research agenda. Innov Aging. (2019) 3:igz005. doi: 10.1093/geroni/igz005
36. Sheridan, D, Coffee, P, and Lavallee, D. A systematic review of social support in youth sport. Int Rev Sport Exerc Psychol. (2014) 7:198–228. doi: 10.1080/1750984X.2014.931999
37. Walseth, K. Sport and belonging. Int Rev Sociol Sport. (2006) 41:447–64. doi: 10.1177/1012690207079510
38. Pels, F, and Kleinert, J. Loneliness and physical activity: a systematic review. Int Rev Sport Exerc Psychol. (2016) 9:231–60. doi: 10.1080/1750984X.2016.1177849
39. Lippke, S, Fischer, MA, and Ratz, T. Physical activity, loneliness, and meaning of friendship in Young individuals - a mixed-methods investigation prior to and during the COVID-19 pandemic with three cross-sectional studies. Front Psychol. (2021) 12:617267. doi: 10.3389/fpsyg.2021.617267
40. Jennen, L, Mazereel, V, Vansteelandt, K, Menne-Lothmann, C, Decoster, J, Derom, C, et al. The within-person bidirectional association between physical activity and loneliness in the daily lives of adolescents and young adults. Ment Health Phys Act. (2023) 24:100499. doi: 10.1016/j.mhpa.2022.100499
41. Cacioppo, JT, Ernst, JM, Burleson, MH, McClintock, MK, Malarkey, WB, Hawkley, LC, et al. Lonely traits and concomitant physiological processes: the MacArthur social neuroscience studies. Int J Psychophysiol. (2000) 35:143–54. doi: 10.1016/S0167-8760(99)00049-5
42. Kulcar, V, Bork-Hüffer, T, and Schneider, AM. Getting through the crisis together: do friendships contribute to university Students' resilience during the COVID-19 pandemic? Front Psychol. (2022) 13:880646. doi: 10.3389/fpsyg.2022.880646
43. Rumas, R, Shamblaw, AL, Jagtap, S, and Best, MW. Predictors and consequences of loneliness during the COVID-19 pandemic. Psychiatry Res. (2021) 300:113934. doi: 10.1016/j.psychres.2021.113934
44. Van de Velde, S, Buffel, V, Bracke, P, Van Hal, G, Somogyi, NM, Willems, B, et al. The COVID-19 international student well-being study. Scand J Public Health. (2021) 49:114–22. doi: 10.1177/1403494820981186
45. Heumann, E, Helmer, SM, Busse, H, Negash, S, Horn, J, Pischke, CR, et al. Anxiety and depressive symptoms of German university students 20 months after the COVID-19 outbreak – a cross-sectional study. J Affect Disord. (2023) 320:568–75. doi: 10.1016/j.jad.2022.09.158
46. Trümmler, J, Heumann, E, Helmer, SM, Busse, H, Stock, C, Negash, S, et al. Determinants of vaccination behavior among university students 20 months after the COVID-19 outbreak: results of the COVID-19 German student well-being study (C19 GSWS). Hum Vaccin Immunother. (2022) 18:2141497. doi: 10.1080/21645515.2022.2141497
47. Heumann, E, Helmer, SM, Busse, H, Trümmler, J, Pischke, CR, Negash, S, et al. COVID-19 German Student Well-being Study (C19 GSWS). Stuttgart, Germany: Zenodo (2023).
48. von Elm, E, Altman, DG, Egger, M, Pocock, SJ, Gøtzsche, PC, and Vandenbroucke, JP. The strengthening the reporting of observational studies in epidemiology (STROBE) statement: guidelines for reporting observational studies. PLoS Med. (2007) 4:e296. doi: 10.1371/journal.pmed.0040296
49. Radloff, LS. The CES-D scale:a self-report depression scale for research in the general population. Appl Psychol Meas. (1977) 1:385–401. doi: 10.1177/014662167700100306
50. Kroenke, K, Spitzer, RL, Williams, JB, Monahan, PO, and Löwe, B. Anxiety disorders in primary care: prevalence, impairment, comorbidity, and detection. Ann Intern Med. (2007) 146:317–25. doi: 10.7326/0003-4819-146-5-200703060-00004
51. Byrd-Bredbenner, C, Eck, K, and Quick, V. GAD-7, GAD-2, and GAD-mini: psychometric properties and norms of university students in the United States. Gen Hosp Psychiatry. (2021) 69:61–6. doi: 10.1016/j.genhosppsych.2021.01.002
52. Löwe, B, Kroenke, K, and Gräfe, K. Detecting and monitoring depression with a two-item questionnaire (PHQ-2). J Psychosom Res. (2005) 58:163–71. doi: 10.1016/j.jpsychores.2004.09.006
53. Kroenke, K, Spitzer, RL, and Janet, BWW. The patient health Questionnaire-2: validity of a two-item depression screener. Med Care. (2003) 41:1284–92. doi: 10.1097/01.MLR.0000093487.78664.3C
54. Ghazisaeedi, M, Mahmoodi, H, Arpaci, I, Mehrdar, S, and Barzegari, S. Validity, reliability, and optimal cut-off scores of the WHO-5, PHQ-9, and PHQ-2 to screen depression among university students in Iran. Int J Ment Heal Addict. (2022) 20:1824–33. doi: 10.1007/s11469-021-00483-5
55. Shankar, A, McMunn, A, Banks, J, and Steptoe, A. Loneliness, social isolation, and behavioral and biological health indicators in older adults. Health Psychol. (2011) 30:377–85. doi: 10.1037/a0022826
56. Zahedi, H, Sahebihagh, MH, and Sarbakhsh, P. The magnitude of loneliness and associated risk factors among university students: a cross-sectional study. Iran J Psychiatry. (2022) 17:411–7. doi: 10.18502/ijps.v17i4.10690
57. Arslan, G, Yıldırım, M, and Aytaç, M. Subjective vitality and loneliness explain how coronavirus anxiety increases rumination among college students. Death Stud. (2022) 46:1042–51. doi: 10.1080/07481187.2020.1824204
58. Shiovitz-Ezra, S, and Ayalon, L. Situational versus chronic loneliness as risk factors for all-cause mortality. Int Psychogeriatr. (2010) 22:455–62. doi: 10.1017/S1041610209991426
59. Hawkley, LC, Burleson, MH, Berntson, GG, and Cacioppo, JT. Loneliness in everyday life: cardiovascular activity, psychosocial context, and health behaviors. J Pers Soc Psychol. (2003) 85:105–20. doi: 10.1037/0022-3514.85.1.105
60. Maloy, A, Main, A, Murphy, C, Coleman, L, Dodd, R, Lynch, J, et al. "I think friendship over this lockdown like saved my life"-student experiences of maintaining friendships during COVID-19 lockdown: an interpretative phenomenological study. Front Psychol. (2022) 13:861192. doi: 10.3389/fpsyg.2022.861192
61. Savikko, N, Routasalo, P, Tilvis, R, and Pitkälä, K. Psychosocial group rehabilitation for lonely older people: favourable processes and mediating factors of the intervention leading to alleviated loneliness. Int J Older People Nurs. (2010) 5:16–24. doi: 10.1111/j.1748-3743.2009.00191.x
62. Masi, CM, Chen, HY, Hawkley, LC, and Cacioppo, JT. A meta-analysis of interventions to reduce loneliness. Pers Soc Psychol Rev. (2011) 15:219–66. doi: 10.1177/1088868310377394
63. Quan, NG, Lohman, MC, Resciniti, NV, and Friedman, DB. A systematic review of interventions for loneliness among older adults living in long-term care facilities. Aging Ment Health. (2020) 24:1945–55. doi: 10.1080/13607863.2019.1673311
64. Busse, H, Buck, C, Stock, C, Zeeb, H, Pischke, CR, Fialho, PMM, et al. Engagement in health risk behaviours before and during the COVID-19 pandemic in German university students: results of a cross-sectional study. Int J Environ Res Public Health. (2021) 18:1410. doi: 10.3390/ijerph18041410
65. Gestsdottir, S, Gisladottir, T, Stefansdottir, R, Johannsson, E, Jakobsdottir, G, and Rognvaldsdottir, V. Health and well-being of university students before and during COVID-19 pandemic: a gender comparison. PLoS One. (2021) 16:e0261346. doi: 10.1371/journal.pone.0261346
66. Russell, DW. UCLA loneliness scale (version 3): reliability, validity, and factor structure. J Pers Assess. (1996) 66:20–40. doi: 10.1207/s15327752jpa6601_2
67. Otufowora, A, Liu, Y, Young, H 2nd, Egan, KL, Varma, DS, Striley, CW, et al. Sex differences in willingness to participate in research based on study risk level among a community sample of African Americans in north central Florida. J Immigr Minor Health. (2021) 23:19–25. doi: 10.1007/s10903-020-01015-4
Keywords: loneliness, mental health, university students, COVID-19 pandemic, depressive symtoms, anxiety, physical activity
Citation: Wenig V, Heumann E, Stock C, Busse H, Negash S, Pischke CR and Heinrichs K (2023) Associations of loneliness with mental health and with social and physical activity among university students in Germany: results of the COVID-19 German student well-being study (C19 GSWS). Front. Public Health. 11:1284460. doi: 10.3389/fpubh.2023.1284460
Edited by:
Yuka Kotozaki, Iwate Medical University, JapanReviewed by:
Giulio Gabrieli, Italian Institute of Technology (IIT), ItalyGiuseppina Lo Moro, University of Turin, Italy
Copyright © 2023 Wenig, Heumann, Stock, Busse, Negash, Pischke and Heinrichs. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Vanessa Wenig, dmFuZXNzYS53ZW5pZ0BjaGFyaXRlLmRl