
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Public Health , 07 November 2023
Sec. Disaster and Emergency Medicine
Volume 11 - 2023 | https://doi.org/10.3389/fpubh.2023.1282296
This article is part of the Research Topic Psychological Mechanisms and Mental Health in the Face of Current Conflicts and Crises View all 11 articles
 Sarah E. Neil-Sztramko1,2*
Sarah E. Neil-Sztramko1,2* Emily Belita3
Emily Belita3 Stephanie Hopkins2
Stephanie Hopkins2 Diana Sherifali3Laura Anderson1
Diana Sherifali3Laura Anderson1 Emma Apatu1Lydia Kapiriri4Jean Eric Tarride1,5,6Olivier Bellefleur7Sharon Kaasalainen3Sharon Marr8
Emma Apatu1Lydia Kapiriri4Jean Eric Tarride1,5,6Olivier Bellefleur7Sharon Kaasalainen3Sharon Marr8 Maureen Dobbins2,3
Maureen Dobbins2,3Background: The COVID-19 pandemic has disrupted the healthcare and public health sectors. The impact of working on the frontlines as a healthcare or public health professional has been well documented. Healthcare organizations must support the psychological and mental health of those responding to future public health emergencies.
Objective: This systematic review aims to identify effective interventions to support healthcare workers’ mental health and wellbeing during and following a public health emergency.
Methods: Eight scientific databases were searched from inception to 1 November 2022. Studies that described strategies to address the psychological impacts experienced by those responding to a public health emergency (i.e., a pandemic, epidemic, natural disaster, or mass casualty event) were eligible for inclusion. No limitations were placed based on study design, language, publication status, or publication date. Two reviewers independently screened studies, extracted data, and assessed methodological quality using the Joanna Briggs Institute critical appraisal tools. Discrepancies were resolved through discussion and a third reviewer when needed. Results were synthesized narratively due to the heterogeneity of populations and interventions. Outcomes were displayed graphically using harvest plots.
Results: A total of 20,018 records were screened, with 36 unique studies included in the review, 15 randomized controlled trials, and 21 quasi-experimental studies. Results indicate that psychotherapy, psychoeducation, and mind–body interventions may reduce symptoms of anxiety, burnout, depression, and Post Traumatic Stress Disorder, with the lowest risk of bias found among psychotherapy interventions. Psychoeducation appears most promising to increase resilience, with mind–body interventions having the most substantial evidence for increases in quality of life. Few organizational interventions were identified, with highly heterogeneous components.
Conclusion: Promoting healthcare workers’ mental health is essential at an individual and health system level. This review identifies several promising practices that could be used to support healthcare workers at risk of adverse mental health outcomes as they respond to future public health emergencies.
Systematic review registration: https://www.crd.york.ac.uk/prospero/display_record.php?RecordID=203810, identifier #CRD42020203810 (PROSPERO).
The COVID-19 pandemic has been a significant disruption to health systems worldwide. Throughout the lifting and reinstatement of public health restrictions and waves of heightened pandemic activity, there was a growing recognition of a “shadow pandemic” of adverse mental health effects due to the pandemic (1). Healthcare workers (HCWs) in various settings are particularly at risk for significant and prolonged impacts given their frontline role in pandemic response. Previous research has demonstrated long-standing psychological consequences experienced by HCWs after SARS (2, 3), and it is expected that there will be large-scale and long-term psychological impacts due to responding to COVID-19 among several occupational groups (4–8). Several systematic reviews of studies exploring the effects of the COVID-19 pandemic on the mental health of HCWs have reported a high prevalence of anxiety, depressive symptoms, insomnia, burnout, emotional exhaustion, and somatic symptoms (9, 10). Notably, factors such as the incidence of infection in the local setting, peer infections or deaths, and a shortage of personal protective equipment all increased the likelihood of experiencing adverse mental health outcomes (9, 10). At the same time, the availability of psychological support resources had a protective effect (9). With this knowledge, an action plan, support, and resources for individuals and organizations are needed to adequately support those experiencing or at risk for psychological distress or adverse mental health outcomes.
There is currently limited guidance on how best to support HCWs in response to and following public health emergencies, such as pandemics. Recent syntheses have gathered very low- to moderate-certainty evidence about interventions that may positively affect healthcare workers’ mental health during a disease outbreak. However, these reviews have focused only on narrow categories of intervention, for example, online mindfulness programs (11), or limited populations, for example, those experiencing burnout (12). There is a need for a high-quality systematic review that captures a broad range of mental health-promoting interventions delivered during various public health emergencies to further inform strategies to improve mental health in HCWs. This review aims to answer the question: What are effective strategies to address the psychological impacts [i.e., anxiety, depression, and Post Traumatic Stress Disorder (PTSD)] experienced by HCWs responding to a public health emergency?
The protocol for this systematic review was registered (PROSPERO #CRD42020203810) and published a priori. There were no deviations from this protocol. The Cochrane Handbook for Systematic Reviews of Interventions guided our review protocol (13).
In collaboration with a health sciences librarian, a comprehensive search strategy was developed and executed in MEDLINE, PsycINFO, Embase, EMCARE, CINAHL, Sociological Abstracts, Business Source Premier, and the Cochrane Central Register of Controlled Trials from inception to 1 November 2022. Search terms related to (1) healthcare personnel; (2) pandemic, epidemic, COVID-19, natural disaster, or public health emergency; (3) psychological supports, interventions, and programs; and (4) mental health outcomes were used (see Supplementary Files, Figure 1 for complete MEDLINE search strategy). Reference lists of included studies and relevant systematic reviews were hand-searched, and relevant experts were contacted to identify any studies that were not captured via our search. Gray literature sources were searched until 22 January 2022, following the Canadian Agency for Drugs and Technologies in Health Grey Matters tool for searching health-related gray literature to identify unpublished studies (14).
Figure 1. PRISMA diagram.
Eligible studies described interventions to prevent, minimize, or treat adverse psychological or mental health or wellbeing at an individual, organizational, or systemic level resulting from a public health emergency, defined as emergent situations as those in which the scale, timing, and unpredictability of health consequences threaten to overwhelm routine capabilities (15); for our purposes, we defined these as an epidemic, pandemic, natural disaster, or mass casualty event. The population was limited to frontline HCWs who were involved in the response to the public health emergency. Ongoing public health crises without distinct starting points are excluded from this contextual requirement (e.g., the opioid epidemic, poverty, homelessness as epidemics, or the prolonged HIV/AIDS epidemic). HCWs included medically trained healthcare professionals typically considered at the frontlines (e.g., nurses and physicians in acute care, outpatient, public health, and long-term care) and allied health professions (e.g., personal support workers, infection control professionals, and social workers). Emergency and law enforcement workers whose work is not primarily associated with health (e.g., police and firefighters; non-health-related essential workers such as grocery store employees and cleaning staff; and civilian volunteer emergency responders) were excluded. Any comparison group, such as placebo control, standard care, or pre-intervention data, was included. Studies that reported occupational, psychological, or mental health outcomes were all included. For this review, mental health is defined per the World Health Organization’s definition as “a state of mental wellbeing that enables people to cope with the stresses of life, realize their abilities, learn well and work well, and contribute to their community” (16). These outcomes were defined a priori by the research team as anxiety, depression, burnout, exhaustion, resilience, altered mood, or clinical diagnoses of mental disorders such as depression or PTSD. Descriptive-only or in-progress studies that described interventions without reporting on mental health or wellbeing outcomes were excluded. No restrictions were placed on study design, language, publication status, publication date, or study location.
Once databases were searched and duplicates were removed, the title and abstract of each reference were screened independently by two trained reviewers. Full texts of all potentially relevant articles were retrieved and screened independently by two experienced reviewers. Disagreements were resolved through discussion or a third team member when needed.
Two trained team members independently completed data extraction and critical appraisal, with discrepancies resolved through discussion or a third team member when needed. A data extraction form was created and trialed with three studies and contained 42 items related to study characteristics (study aim, study design, and country); study sample (participant age, gender, professional role, organization, and sample size); intervention and comparator groups; and outcomes (primary and secondary outcomes, measurement methods including anxiety; depression; PTSD; burnout; quality of life; resilience and coping; and mood-related outcomes). Mean differences between groups were extracted to compare outcomes across studies with expected results. Where within-group baseline and end-of-study data were reported, they were transformed into the mean difference and standard deviation of the difference using guidance from the Cochrane Handbook for Systematic Reviews (17). The intervention-related information was extracted using the template for intervention description and replication (TIDieR) checklist (18). Critical appraisal was completed using the appropriate Joanna Briggs Institute critical appraisal tool for the study design extracted (19). Studies rated as unclear or high risk of bias on more than half of domains were defined as having an increased risk of bias; those rated as unclear or high for three or more domains were defined as having some concerns.
A visual examination of the data extraction table organized by contextual information (i.e., disaster type, setting, and intervention) revealed significant heterogeneity in the data; thus, a meta-analysis was deemed inappropriate. Interventions were categorized post-hoc as falling within four broad categories to support the narrative synthesis: psychotherapy, psychoeducation, mind–body, and organizational interventions; studies that did not fit within one of these categories were classified as “other.” Harvest plots were created for each intervention type and mode of delivery to display study outcomes graphically. Each row of the plot showed effect sizes for each category of results extracted (e.g., anxiety, depression, PTSD, burnout, quality of life, resilience or coping, and mood), with the size of the bar indicating the effect size. Effect size estimates were extracted from the published articles when reported as Cohen’s d or Hedge’s g or were calculated using the Carlson–Schmidt method for paired pre-treatment and post-treatment data (20, 21) or the Campbell Collaboration’s effect size calculator created by Wilson (22, 23). Bars were color-coded by study design (RCT vs. quasi-experimental) and risk of bias (low, some concerns, and high), and studies with a statistically significant change were labeled.
Across databases, 30,492 records were identified, along with 47 from reference lists and gray literature (Figure 1). Following de-duplication, the remaining 20,018 records were screened by title and abstract. Of the 1,856 articles assessed at the full-text level, 39 publications describing 36 unique interventions met eligibility criteria (Figure 1) (24–62).
Studies were published between 1994 and 2022 (Table 1). Nine studies were conducted in the United States (26, 29, 38, 39, 41, 42, 44, 50, 56), three in the United Kingdom (25, 36, 59), China (27, 34, 52), Italy (40, 60, 61), and Taiwan (28, 37, 58), Turkey (46, 54, 57), and two in Sierra Leone (24, 53). The remaining 10 studies were conducted in Armenia (37), Chile (30), Indonesia (48), Iran (62), Israel (45), Japan (49) and the Philippines (55), Singapore (51), South Africa (31), and Spain (35). Interventions were delivered in response to an infectious disease pandemic or epidemic (n = 24, 67%), namely COVID-19 (n = 20, 56%) (25, 27, 31, 34–36, 40, 44, 46–48, 50–52, 54, 57, 59–62), Ebola (n = 3, 8%) (24, 29, 53), and SARS (n = 1, 2%); natural disasters (n = 10, 38%), namely earthquakes (n = 4, 11%) (28, 30, 37, 49), hurricanes (n = 5, 14%) (38, 39, 41, 42, 56), and typhoons (n = 1, 3%) (55); or mass casualty events (n = 2, 6%) (26, 45).
Table 1. Description of interventions.
Fifteen studies (42%) were randomized controlled trials (25, 26, 34–36, 39, 45–47, 50–52, 54, 57, 62), 17 (47%) were single-group pre–post quantitative studies (24, 27–29, 31, 37, 40–42, 44, 49, 55, 56, 58–61), and four (11%) were non-randomized interventions with a comparator group (30, 38, 48, 53). Interventions were categorized into four intervention types: psychotherapy interventions (n = 9, 25%) defined as comprehensive psychological support including cognitive behavioral therapy (CBT) or training in psychological first aid (PFA), usually delivered or supported by a mental health professional (24–34); psychoeducation interventions (n = 11, 31%) which consisted of primarily didactic or interactive educational strategies to promote the use of self-management techniques and build resilience and coping ability (35–45); mind–body interventions (n = 12, 33%), such as meditation, yoga, and exercise (46–57); and workplace-based interventions (n = 3, 8%) such as in-service-training and workplace hubs (58–60). Two identified interventions using music therapy (61), and aromatherapy (62) did not fit well within other intervention categories and are thus presented separately as ‘other’. Most studies (n = 22, 61%) were delivered to a diverse group of HCWs (24, 26, 28, 30, 31, 35, 36, 39–42, 44, 49–53, 56, 59, 61, 62). In contrast, others specifically targeted nurses (n = 9, 25%) (27, 34, 45, 47, 48, 54, 57, 58, 60), social workers (n = 6) (38, 46), counselors (n = 1, 3%) (37), mental health professionals (n = 1, 3%) (55), and public health workers (n = 1, 3%) (29). Complete details on each intervention following the TIDieR framework can be found in the Supplementary Files, Table 1.
The risk of bias was moderate to high in most studies; within the RCTs, one study (7%) was defined as having a low risk of bias (35), nine (60%) as having some risk of bias concerns (25, 26, 36, 45, 47, 50, 51, 57, 62), and five (33%) as having a high risk of bias (34, 39, 46, 52, 54) (Figure 2). Of quasi-experimental studies, seven (33%) were rated as having a lower risk of bias (24, 27, 31, 40, 44, 58, 60), seven (33%) were rated as having some concerns (30, 38, 41, 48, 53, 59, 61), and seven (33%) as having a high risk of bias (28, 29, 37, 42, 49, 55, 56) (Figure 3). The most problematic domains within the RCTs were lack of blinding (participant, interventionist, and assessor), allocation not concealed, appropriateness of the statistical analysis, and incomplete follow-up. The most problematic domains within quasi-experimental studies were lack of a comparator group, incomplete follow-up, and the use of multiple assessment outcome measures. Full critical appraisal results can be found in Supplementary Files, Table 2.
Figure 2. Risk of bias in randomized controlled trials.
Figure 3. Risk of bias in quasi-experimental studies.
Table 2. Results.
Nine studies were included that used psychotherapy to support healthcare workers’ mental health: three RCTs (25, 26, 34) and six quasi-experimental studies (24, 27–31). The components of the psychotherapy varied widely: five included CBT (24–26, 30, 34), two used psychological first aid (28, 29), one focused on mindfulness-based stress reduction (31), and one on acceptance and commitment therapy (27). Interventions were delivered in groups (n = 5, 56%) (24, 27, 29–31), one-on-one (n = 2, 22%) (26, 28), and electronically (n = 2, 22%) (25, 34). Interventions varied from a single session (28) to 12 weeks in duration.
Overall positive effects were reported across mental health outcomes (Figure 4, Table 2). However, most studies had some concerns or a high risk of bias. Many were not statistically significant: group CBT during Ebola and e-CBT during COVID-19 both significantly decreased anxiety scores with small–moderate effect sizes (24, 34), but a CBT- and positive-psychology-focused app during COVID-19 and group-based Acceptance and Commitment Therapy (ACT) did not (25, 27). Group-based CBT during Ebola also significantly reduced depression with small to moderate effect sizes, as did group-based ACT (24, 27); however, this was not seen in interventions of a CBT and positive psychology-based app or e-CBT during COVID-19 or in-person CBT in response to the September 11th attacks (25, 26, 34). Symptoms of PTSD generally improved across four studies with moderate to large effect sizes (24, 26, 28, 30); however, in one study that compared the effect of in-person group CBT following a natural disaster, those with and without diagnosed PTSD only improved in the group with a clinical diagnosis of PTSD (30). Only a single study each found statistically significant improvements in burnout (31), mood (24), and coping self-efficacy (29) with small effect sizes following mindfulness-based stress reduction, group-based CBT, and psychological first aid training, respectively; a single study also explored quality of life (25), with no statistically significant effects found using a CBT and positive psychology-based app.
Figure 4. Harvest plot of the effects of psychotherapy on mental health outcomes.
Ten studies were identified that used psychoeducation to promote healthcare workers’ mental health: four RCTs (35, 36, 39, 45) and six quasi-experimental studies (37, 38, 40–42, 44). All interventions included workshops or educational materials; 60% (n = 6) focused on physical stress management (35, 36, 38–40, 45). Few incorporated direct support from a mental health professional (n = 4, 40%) (35, 37, 38, 44), peer support (n = 2, 20%) (37, 42), or a basis in CBT (n = 2, 20%) (35, 36). Half of the interventions consisted of only one session (37, 39–42), with the longest lasting 12 weeks (45). While two interventions (20%) were self-paced apps (35, 36), most were delivered face-to-face (n = 6, 60%) (37–39, 41, 42, 45) and in a group setting (n = 7, 70%) (37–39, 41, 42, 44, 45).
Generally, psychoeducational interventions promoted positive effects on mental health outcomes, although many changes were not statistically significant (Figure 5, Table 2). Both a virtual reality-based stress management intervention and resilience coaching program studies with low risk of bias found moderate to large statistically significant reductions in anxiety (40, 44); two app-based psychoeducation interventions found small, non-significant decreases (35, 36). Four studies explored burnout. Two group-based psychoeducation interventions resulted in small, statistically significant decreases (44, 45). In contrast, a single, group-based session did not result in a statistically significant change. HCWs who used a CBT-based app reported slightly higher burnout scores at the end of the intervention (35). Moderate-to-large reductions in depression and PTSD symptoms were observed after using a psychoeducation app and group-based workshops (36, 37, 39). However, differences were generally not statistically significant; a fourth study of an app-based intervention found no change in either outcome (35). Concerning positive mental health outcomes, group-based resilience workshops and a mental wellbeing app resulted in moderate improvements in quality of life, although with some concerns of risk of bias (36, 45). A similar improvement was found following a resilience-focused group-based workshop, although the findings were not statistically significant (41). Resilience measures improved following group-based resilience training (38, 44) and group-based stress reduction (42) with moderate to large effect sizes. A single resilience training workshop and app-based intervention did not result in statistically significant improvements in resilience among HCWs (36, 41).
Figure 5. Harvest plot of the effects of psychoeducation on mental health outcomes.
Twelve mind–body interventions were identified: seven RCTs (46, 47, 50–52, 54, 57) and five quasi-experimental studies (48, 49, 53, 55, 56). Nearly all interventions included a focus on physical stress management (n = 10, 91%) (46, 48–57), and over half of the interventions had an educational workshop (n = 6, 55%) (46, 49, 50, 53, 55, 56) or educational materials (n = 6, 55%) (46, 48, 51, 54–56). Only two (18%) involved interaction with a mental health professional (46, 50), and none incorporated peer support. The length of interventions ranged from a single session (49, 57) to 8 weeks (55, 56). Interventions were predominantly delivered in groups (n = 8, 73%) (48–50, 52–57), with one (9%) (51) provided asynchronously via a mobile application and two (18%) (46, 47) not reporting whether interventions were delivered in group or individual format. Five interventions (45%) used virtual delivery (46, 48, 51, 52, 54), and five (45%) were delivered in person (47, 49, 53, 55, 56); one did not report the mode of delivery (50).
Findings from mind–body interventions suggest moderate to large reductions in anxiety, burnout, and depression, and small to moderate decreases in PTSD as well as large increases in quality of life; however, many did not reach statistical significance, and all studies had some concerns or a high risk of bias (Figure 6, Table 2). Of eight studies that measured anxiety, statistically significant improvements were found following a transcendental meditation intervention, a meditation retreat followed by a home study program following Hurricane Katrina, and a mindfulness-based breathing and music therapy intervention (50, 56, 57). These improvements did not reach statistical significance in interventions consisting of mindfulness training for social workers (46), a mindfulness app (51), a Ba Duan Jin intervention (53), or a meditation retreat and home practice following Typhoon Haiyan (55). In an RCT of brief mindfulness meditation, decreases in anxiety following the intervention period were large in the control group (52). Significant reductions in burnout were reported following Gong meditation (47), transcendental meditation (50), and laughter yoga (54), but not following a meditation app (51).
Figure 6. Harvest plot of the effects of mind–body interventions on mental health outcomes.
Statistically significant decreases in depression were only found following mindfulness training plus daily meditation (46); moderate effect sizes were found following transcendental meditation (50), a meditation app (51), and meditation retreats following Hurricane Katrina (56). In one RCT of brief mindfulness meditation and a quasi-experimental study of a meditation retreat, depression scores were higher in the intervention vs. comparator group (52, 55). Concerning PTSD symptoms, a meditation retreat following home practices resulted in statistically significant reductions (56); however, reductions were not significant following the use of a mindfulness app (51). Ba Duan Jin exercises (53), laughter yoga (54), and mindfulness breathing and music therapy (57) resulted in large and statistically significant improvements in quality of life; these improvements were not significant following a mindfulness breathing intervention delivered via WhatsApp (48) or the use of a meditation app (51). Only one study explored the impact of transcendental meditation on resilience, which did not find a statistically significant difference between groups (50).
Three different interventions were delivered at the organizational level during the 2003 SARS pandemic in Taiwan (58) and the COVID-19 pandemic in the UK (59) and Italy (60), all with low or some concerns concerning the risk of bias (Figure 7, Table 2). These interventions included enhanced training and surveillance infection prevention and control measures (58, 60), reorganization of care and staffing levels (58, 60), and supports such as yoga, mindfulness, and general mental health support (58, 59). The effect of these changes was evaluated after 1 month (59) and up to 5 months (60). An intervention focused on staffing, infection prevention and control measures, and mental health supports resulted in statistically significant reductions in anxiety and depression; effect sizes were moderate, and the risk of bias was low (58). An intervention delivering a mental health support hub within the hospital resulted in a large improvement in mood but was not statistically significant, and there were some concerns about the risk of bias (59). Finally, an intervention including proactive management, reorganized care settings, an increase in staffing, and online education resulted in small but statistically significant improvements in quality of life among nurses (60).

Figure 7. Harvest plot of the effects of organizational interventions on mental health outcomes.
Finally, two interventions were identified that did not fall into one of the categories above. Giordano et al. used trained music therapists to develop relaxation playlists and listening guides to reduce stress and anxiety and improve energy and concentration among HCWs in Italy during the COVID-19 pandemic, with some concerns about the risk of bias (61). After 5 weeks, playlists decreased tiredness, sadness, fear, and worry compared to pre-intervention. Mahdood et al. tested aromatherapy before a work shift and during sleep on HCW with anxiety and insomnia during the COVID-19 pandemic in Iran; some concerns were identified with the risk of bias (62). Those in the intervention group displayed statistically significant reductions in anxiety compared to the control group after 30 days.
When intervention categories were combined, few clear patterns emerged for differences in effect size by mode of delivery (in-person, virtual, individual, and group-based, Figures 8–13). With respect to anxiety, interventions that were delivered in a group-based format were more consistently statistically significant than interventions delivered individually, with effect sizes generally moderate, and in-person compared to virtually delivered interventions had more consistently positive findings for reductions in depression. In the remaining comparisons, there were either similar findings by mode of delivery or too few studies in one or more categories to make meaningful comparisons.
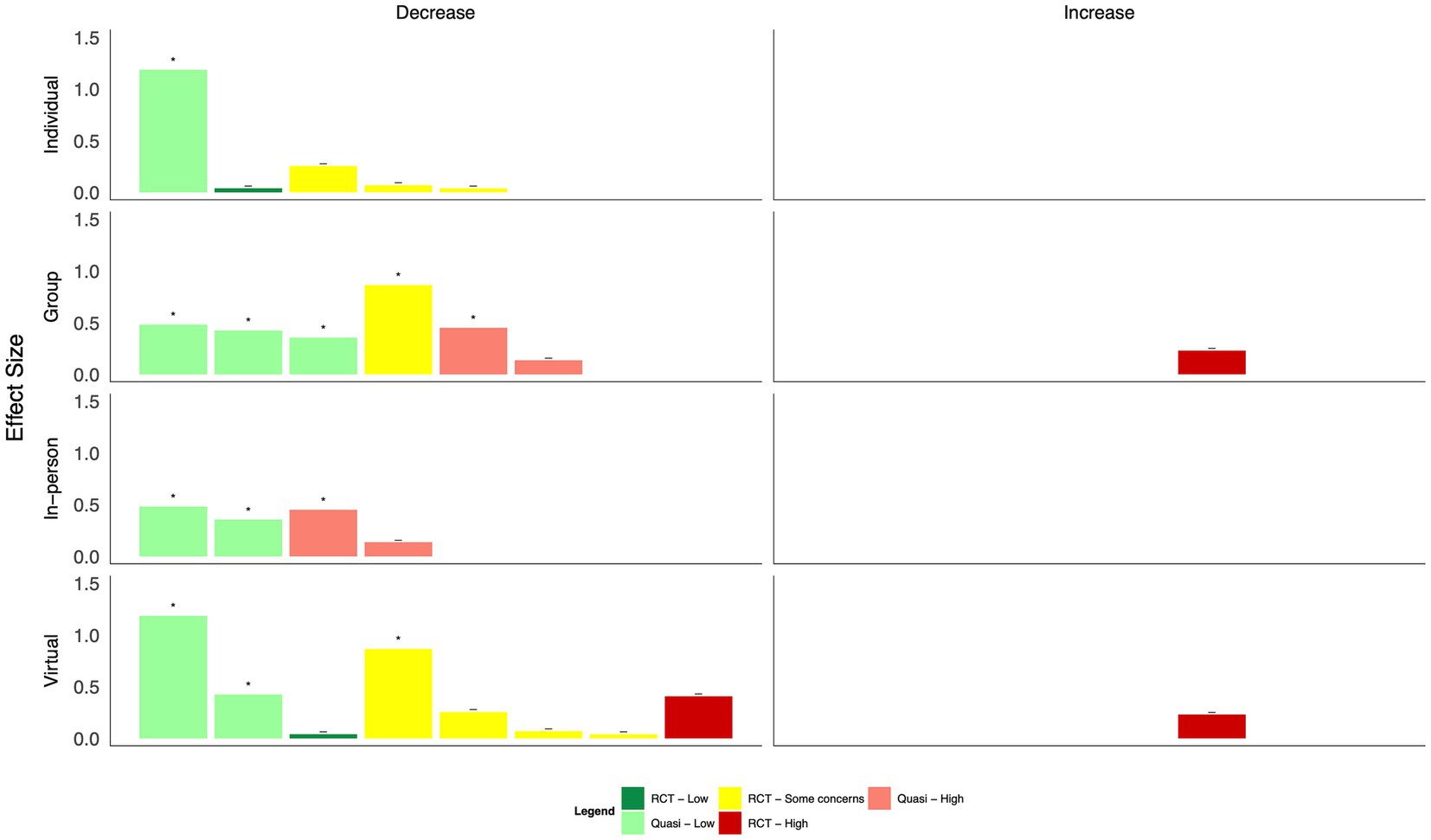
Figure 8. Harvest plot of changes in anxiety by mode of delivery.
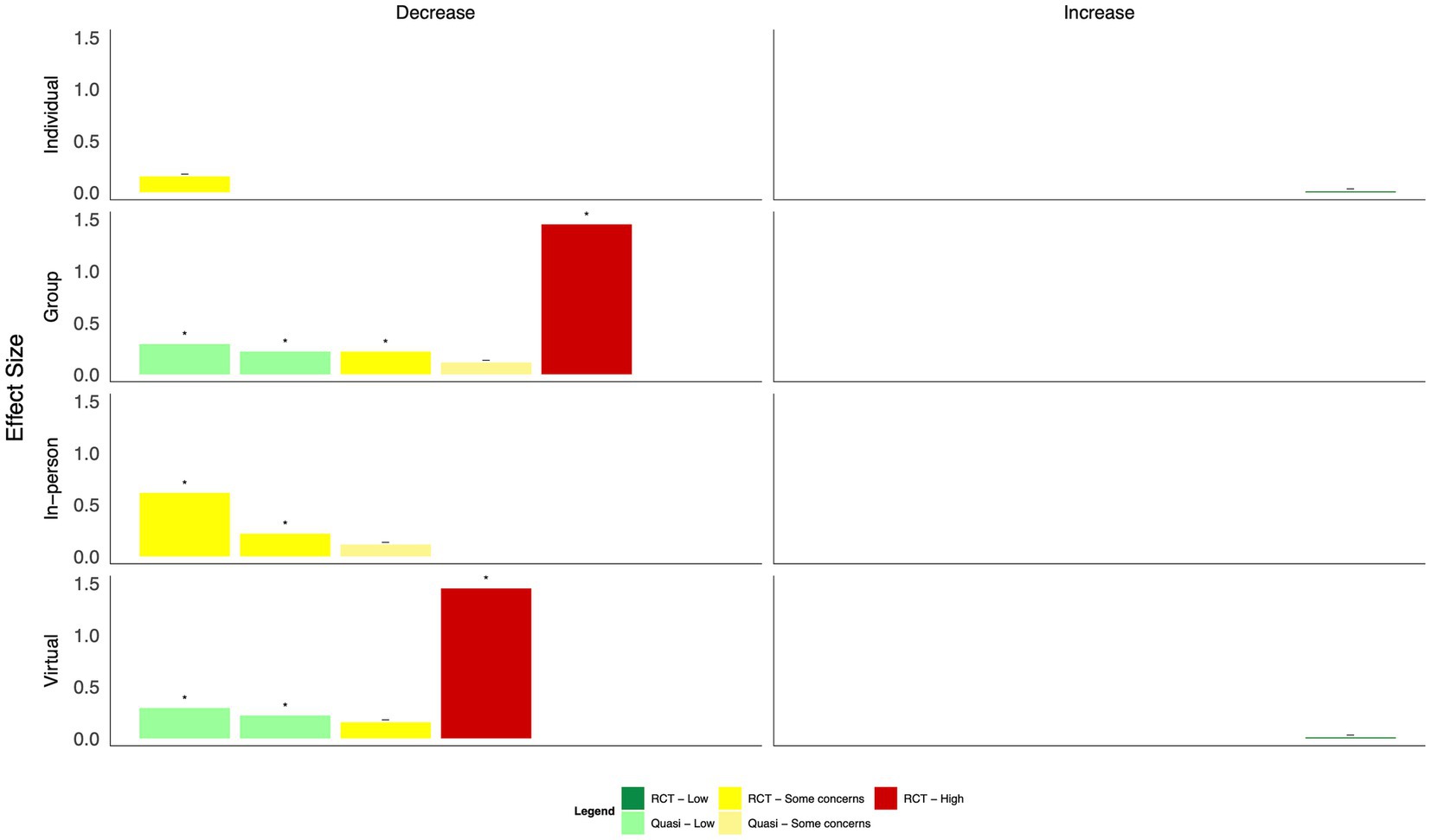
Figure 9. Harvest plot of changes in burnout by mode of delivery.
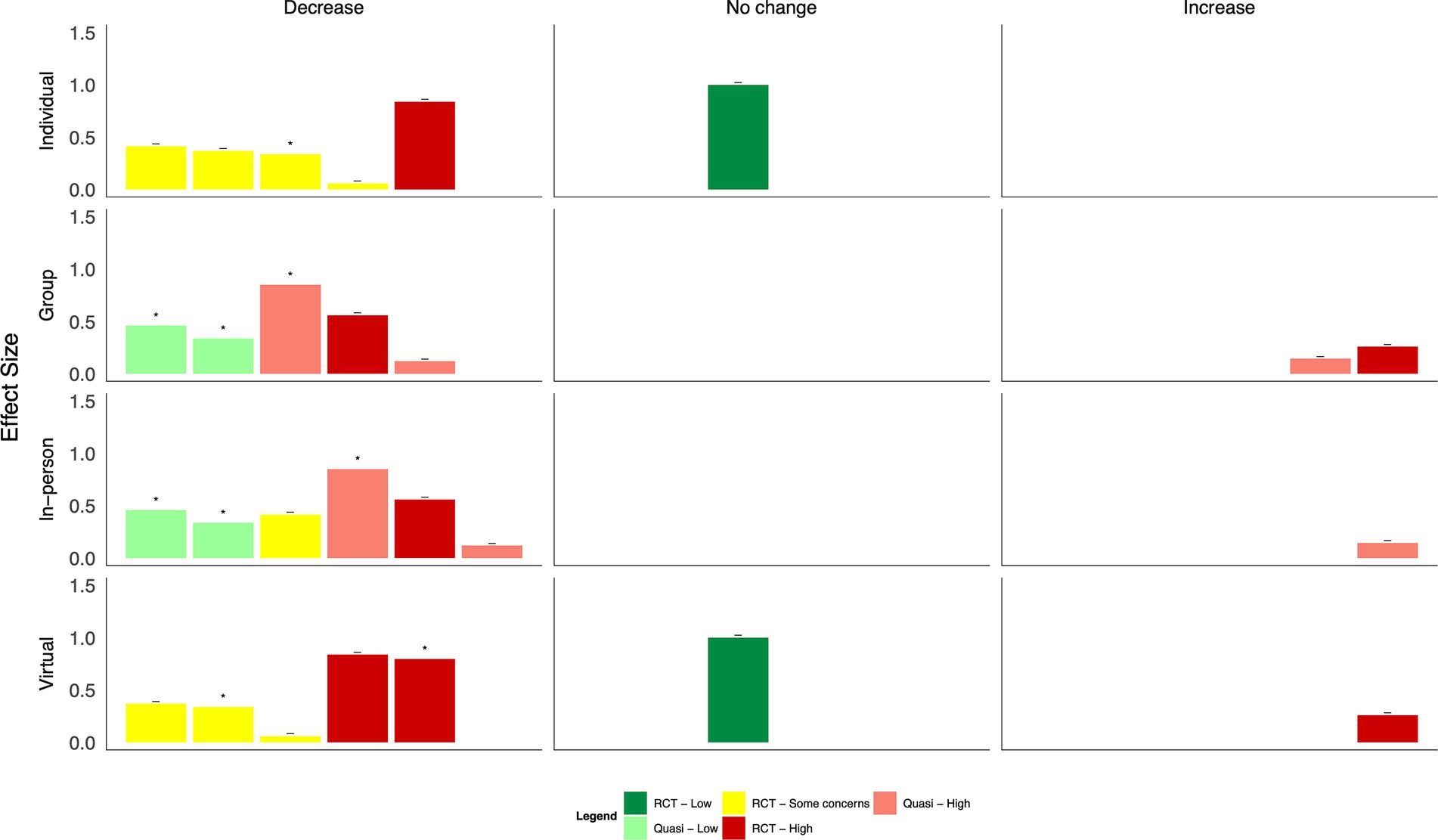
Figure 10. Harvest plot of changes in depression by mode of delivery.
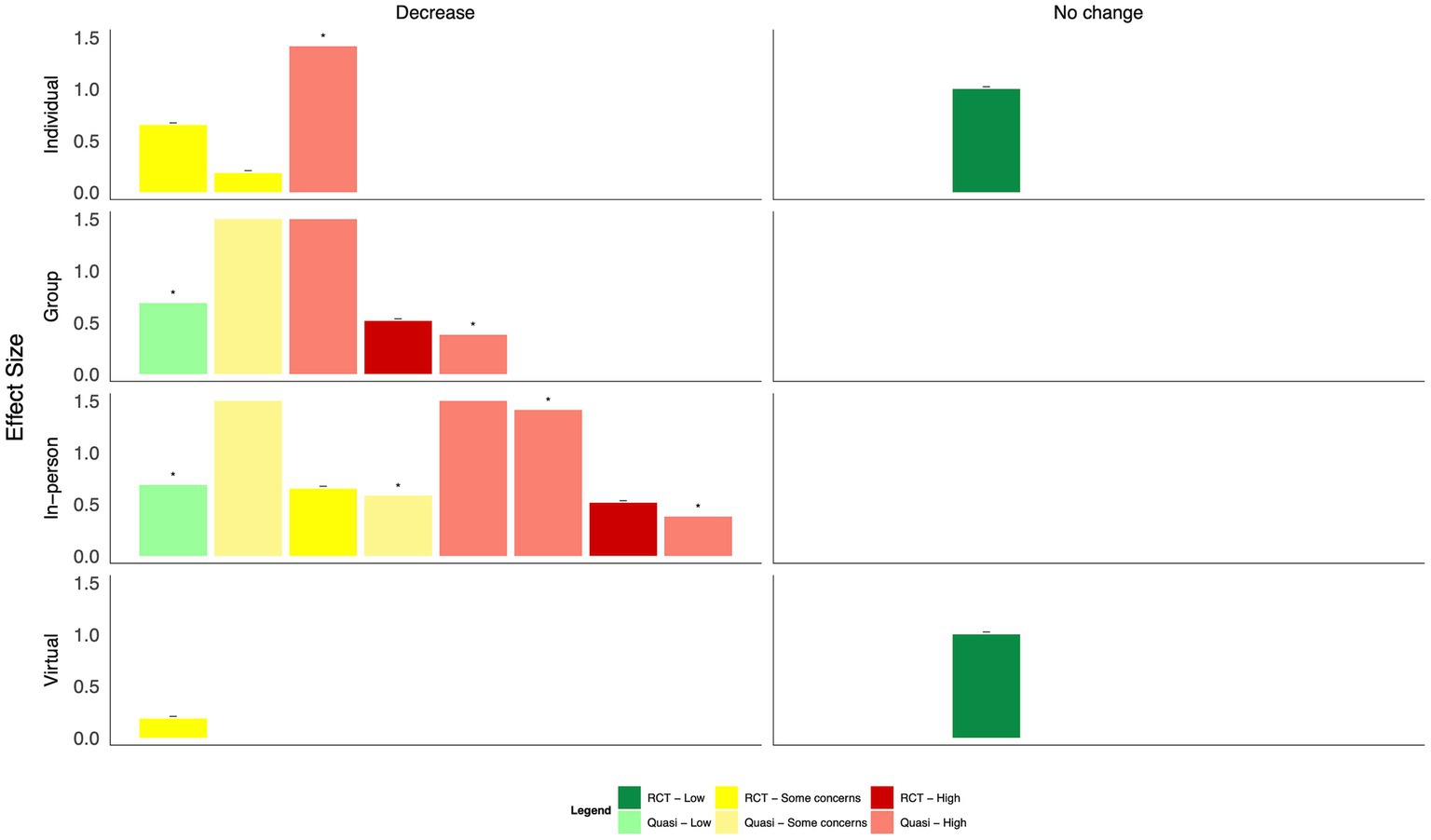
Figure 11. Harvest plot of changes in Post traumatic stress disorder by mode of delivery.
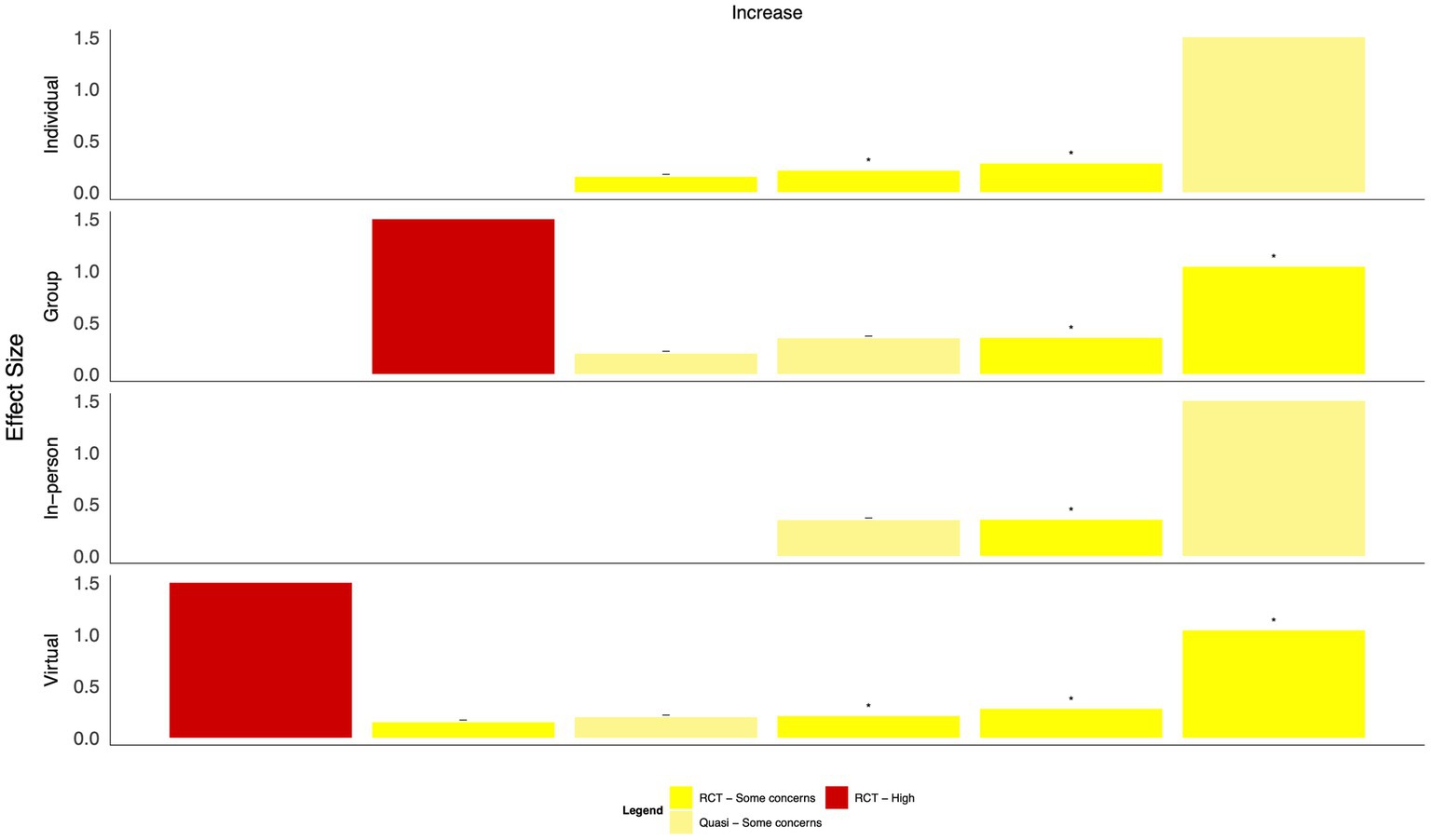
Figure 12. Harvest plot of changes in quality of life by mode of delivery.

Figure 13. Harvest plot of changes in resilience by mode of delivery.
This review examined the use and effectiveness of strategies implemented at the individual and organizational levels to mitigate the psychological impacts experienced by those responding to a public health emergency. Recent systematic reviews focused on the COVID-19 pandemic have reported on the growing prevalence of adverse mental health outcomes in HCWs, which adds to the body of literature from previous public health emergencies (63–68). In addition to documenting the burden, there is also a need to identify effective interventions that can be used in recovery from the early, acute phases of the pandemic and a knowledge of the types of interventions that could be efficiently implemented in future public health emergencies.
This review found that psychotherapy had the strongest effect on decreasing several negative mental health outcomes and that psychoeducation may also be effective. Mind–body interventions seem particularly promising for improving quality of life, but more high-quality research is needed. These findings are consistent with the findings of a rapid synthesis of strategies to support the mental health and resilience of the public health workforce (including studies that were not focused on public health emergencies) (69). This review found that effective interventions were multi-sessional, built on existing evidence-based practices such as CBT, aimed to increase knowledge and skills in safety, problem-solving, resilience, and coping, and incorporated aspects of physical stress management. Another review focused on only eHealth interventions to reduce stress and promote the mental health of healthcare professionals and also found preliminary effectiveness for ‘third wave’ psychotherapies, such as mindfulness, compassion, and acceptance therapies. Like in this review, high heterogeneity was found across studies (70). Finally, a 2020 Cochrane review found very low certainty evidence that resilience training, which included mindfulness and cognitive behavioral therapy, may result in higher resilience and lower depression and stress in healthcare professionals. Importantly, this review only included studies published up to June 2019, thus did not include important lessons learned during the COVID-19 pandemic.
A future focus on widespread organizational-level interventions is also important to inform future emergency response. While individual-level interventions do appear to have positive impacts, there may be important equity and access implications. Many of the interventions tested during the COVID-19 pandemic were offered virtually, given widespread public health protocols in place to reduce the spread of infection; this mode of delivery may have also enhanced the participation of HCWs who may be unable or unwilling to take part in in-person programming. An important factor that is not considered in research-tested interventions is the cost of delivery. Out-of-pocket expenses for mental health treatment by a qualified professional may be prohibitive for many HCWs. Similarly, there is a need for more cultural competency in psychological interventions (i.e., CBT and PFA). Differing cultural perspectives may lead to conflicting views on how some think about and understand mental health and wellness, and research literature has highlighted the importance of considering cultural components in the spread and scale of evidence-based mental health interventions (71). Recognizing diversity within the workforce is a critical step in providing adequate mental health support.
Based on the visual inspection of the harvest plots, the data suggest that group-based interventions may be more effective than individually delivered interventions, including one-on-one intervention delivery or delivery via the internet or mobile applications, suggesting that a sense of group cohesion is relevant to effective interventions. This is in line with data from qualitative reviews, which have identified feelings of camaraderie and team building as important components that may mediate the efficacy of the intervention on individuals’ mental health (72, 73). A recently published scoping review synthesized evidence on the key concerns of healthcare providers with respect to COVID-19 (74). Based on the findings, the authors recommended timely and personalized mental health support, particularly through interdisciplinary teams, to minimize burnout; this recommendation is supported by the findings presented here.
To answer our research question, we employed a comprehensive search strategy of multiple databases and gray literature and followed best practices for evidence synthesis, following the Cochrane Handbook for Systematic Review of Interventions to reduce bias in our study. The certainty of the findings of this review is limited by the quality of the included single studies. Most studies were quasi-experimental, using a pre-test and post-test design rather than RCTs. This is not surprising given that many were evaluations of real-world programs that were implemented in response to an unexpected public health emergency and were not pre-designed for the purpose of determining intervention efficacy. Thus, positive findings from studies without an appropriate control group may be confounded by other factors. At the same time, these real-world evaluations may be more generalizable than studies that are conducted in tightly controlled trial conditions. Within the included studies, effect sizes do appear to be larger in studies with a higher risk of bias. A large loss to follow-up was observed across both RCTs and quasi-experimental studies, which may overinflate the effect estimates if those who withdraw from a study are those who are not experiencing a benefit of the intervention. Heterogeneity within categories was high, precluding the use of statistical techniques such as meta-analyses to estimate effect sizes more precisely. These factors should be considered when using the evidence presented here in decision-making.
In addition, studies measuring anxiety, burnout, depression, and PTSD included in this review rarely provided a diagnostic criterion for inclusion. It is possible that the types of interventions needed to effectively treat a clinical diagnosis of a mental health disorder such as generalized anxiety disorder or major depressive disorder may be different than the type of intervention needed to reduce the risk of developing such disorders. Further studies should clearly describe recruitment strategies and eligibility criteria and perform subgroup analyses by baseline scores to better understand whether tailoring of interventions may be needed based on one’s baseline mental health status. This is particularly important for including diverse populations who are less likely to acknowledge psychological symptoms and report being concerned about the stigma associated with mental illness (75). Finally, most of the interventions included were of relatively short duration; the medium- or long-term impact of these interventions is unknown.
This review adds to a growing body of evidence on strategies to mitigate the adverse psychological effects of frontline HCWs responding to a variety of public health emergencies, including pandemics and natural disasters. This review highlights the need for ongoing, rigorous research and evaluation of mental health programming implemented at the individual and organizational levels to mitigate the mental health risks in future pandemics or public health emergencies. Strategies to improve the mental health and wellbeing of HCWs following the COVID-19 pandemic will not be a “one size fits all” approach; however, the data to date elucidate promising areas to invest in to support the mental health of HCWs.
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author.
SN-S: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. EB: Conceptualization, Data curation, Methodology, Supervision, Writing – review & editing. SH: Conceptualization, Formal analysis, Project administration, Writing – original draft, Writing – review & editing. DS: Methodology, Writing – review & editing. LA: Methodology, Writing – review & editing. EA: Methodology, Writing – review & editing. LK: Methodology, Writing – review & editing. JT: Methodology, Writing – review & editing. OB: Methodology, Writing – review & editing. SK: Methodology, Writing – review & editing. SM: Methodology, Writing – review & editing. MD: Conceptualization, Funding acquisition, Investigation, Methodology, Supervision, Validation, Writing – original draft, Writing – review & editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This scoping review was funded by the Public Health Agency of Canada, as part of the work of the National Collaborating Centre for Method and Tools (NCCMT). The views expressed herein do not necessarily represent the views of the Public Health Agency of Canada.
The authors would like to acknowledge the members of the National Collaborating Centre for Methods and Tools Rapid Evidence Service team for their contributions to searching, screening, data extraction, and critical appraisal.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2023.1282296/full#supplementary-material
1. Nabavi, N. Covid-19: pandemic will cast "a long shadow" on mental health, warns England's CMO. BMJ. (2021) 373:n1655. doi: 10.1136/bmj.n1655
2. Maunder, RG, Lancee, WJ, Balderson, KE, Bennett, JP, Borgundvaag, B, Evans, S, et al. Long-term psychological and occupational effects of providing hospital healthcare during SARS outbreak. Emerg Infect Dis. (2006) 12:1924–32. doi: 10.3201/eid1212.060584
3. Maunder, RG, Leszcz, M, Savage, D, Adam, MA, Peladeau, N, Romano, D, et al. Applying the lessons of SARS to pandemic influenza: an evidence-based approach to mitigating the stress experienced by healthcare workers. Can J Public Health. (2008) 99:486–8. doi: 10.1007/BF03403782
4. Chen, Q, Liang, M, Li, Y, Guo, J, Fei, D, Wang, L, et al. Mental health care for medical staff in China during the COVID-19 outbreak. Lancet Psychiatry. (2020) 7:e15–6. doi: 10.1016/S2215-0366(20)30078-X
5. Kisely, S, Warren, N, McMahon, L, Dalais, C, Henry, I, and Siskind, D. Occurrence, prevention, and management of the psychological effects of emerging virus outbreaks on healthcare workers: rapid review and meta-analysis. BMJ. (2020) 369:m1642. doi: 10.1136/bmj.m1642
6. Wu, PE, Styra, R, and Gold, WL. Mitigating the psychological effects of COVID-19 on health care workers. CMAJ. (2020) 192:E459–60. doi: 10.1503/cmaj.200519
7. Tan, BYQ, Chew, NWS, Lee, GKH, Jing, M, Goh, Y, Yeo, LLL, et al. Psychological impact of the COVID-19 pandemic on health Care Workers in Singapore. Ann Intern Med. (2020) 173:317–20. doi: 10.7326/M20-1083
8. Li, Z, Ge, J, Yang, M, Feng, J, Qiao, M, Jiang, R, et al. Vicarious traumatization in the general public, members, and non-members of medical teams aiding in COVID-19 control. Brain Behav Immun. (2020) 88:916–9. doi: 10.1016/j.bbi.2020.03.007
9. Braquehais, MD, Vargas-Caceres, S, Gomez-Duran, E, Nieva, G, Valero, S, Casas, M, et al. The impact of the COVID-19 pandemic on the mental health of healthcare professionals. QJM. (2020) 113:613–7. doi: 10.1093/qjmed/hcaa207
10. Li, Y, Scherer, N, Felix, L, and Kuper, H. Prevalence of depression, anxiety and post-traumatic stress disorder in health care workers during the COVID-19 pandemic: a systematic review and meta-analysis. PLoS One. (2021) 16:e0246454. doi: 10.1371/journal.pone.0246454
11. Yang, JM, Ye, H, Long, Y, Zhu, Q, Huang, H, Zhong, YB, et al. Effects of online mindfulness-based interventions on anxiety, depression, and stress among frontline healthcare workers during the COVID-19 pandemic: a systematic review and meta-analysis. J Med Internet Res. (2023) 25:e44000. doi: 10.2196/44000
12. Alzailai, N, Barriball, KL, and Xyrichis, A. Impact of and mitigation measures for burnout in frontline healthcare workers during disasters: a mixed-method systematic review. Worldviews Evid-Based Nurs. (2023) 20:133–41. doi: 10.1111/wvn.12633
13. Cochrane. Cochrane handbook for systematic reviews of interventions version 6.3 (2023). Available at: www.training.cochrane.org/handbook.
14. CADTH Information Services. Grey matters: a practical tool for searching health-related grey literature. (2015).
15. Nelson, C, Lurie, N, Wasserman, J, and Zakowski, S. Conceptualizing and defining public health emergency preparedness. Am J Public Health. (2007) 97 Suppl 1:S9–S11. doi: 10.2105/ajph.2007.114496
16. World Health Organization. Fact sheets: Mental health. Geneva: WHO (2022) Available from: https://www.who.int/news-room/fact-sheets/detail/mental-health-strengthening-our-response.
17. Cumpston, M, Li, T, Page, MJ, Chandler, J, Welch, VA, Higgins, JP, et al. Updated guidance for trusted systematic reviews: a new edition of the Cochrane handbook for systematic reviews of interventions. Cochrane Database Syst Rev. (2019) 10:ED000142. doi: 10.1002/14651858.ED000142
18. Hoffmann, TC, Glasziou, PP, Boutron, I, Milne, R, Perera, R, Moher, D, et al. Better reporting of interventions: template for intervention description and replication (TIDieR) checklist and guide. BMJ. (2014) 348:g1687. doi: 10.1136/bmj.g1687
20. Lakens, D. Calculating and reporting effect sizes to facilitate cumulative science: a practical primer for t-tests and ANOVAs. Front Psychol. (2013) 4:863. doi: 10.3389/fpsyg.2013.00863
21. Uanhoro, JO. Effect size calculators (2017). Available at: https://effect-size-calculator.herokuapp.com/ (accessed August 2 2023).
22. Lipsey, MW, and Wilson, D. Practical Meta-analysis (applied social research methods). 1st ed. Thousand Oaks, California: SAGE Publications (2000).
23. Wilson, DB. Practical meta-analysis effect size calcualtor. (2001). Available at: https://www.campbellcollaboration.org/escalc/html/EffectSizeCalculator-Home.php (accessed August 2 2023).
24. Cole, CL, Waterman, S, Hunter, ECM, Bell, V, Greenberg, N, Rubin, GJ, et al. Effectiveness of small group cognitive behavioural therapy for anxiety and depression in Ebola treatment Centre staff in Sierra Leone. Int Rev Psychiatry. (2021) 33:189–97. doi: 10.1080/09540261.2020.1750800
25. De Kock, JH, Latham, HA, Cowden, RG, Cullen, B, Narzisi, K, Jerdan, S, et al. Brief digital interventions to support the psychological well-being of NHS staff during the COVID-19 pandemic: 3-arm pilot randomized controlled trial. JMIR Ment Health. (2022) 9:e34002. doi: 10.2196/34002
26. Difede, J, Malta, LS, Best, S, Henn-Haase, C, Metzler, T, Bryant, R, et al. A randomized controlled clinical treatment trial for world trade center attack-related PTSD in disaster workers. J Nerv Ment Dis. (2007) 195:861–5. doi: 10.1097/NMD.0b013e3181568612
27. Jing, H, Zhang, L, Liu, Y, Zhang, C, Zhang, Y, Tang, R, et al. Effect of a group-based acceptance and commitment therapy program on the mental health of clinical nurses during the COVID-19 sporadic outbreak period. J Nurs Manag. (2022) 30:3005–12. doi: 10.1111/jonm.13696
28. Ke, YT, Chen, HC, Lin, CH, Kuo, WF, Peng, AC, Hsu, CC, et al. Posttraumatic psychiatric disorders and resilience in healthcare providers following a disastrous earthquake: an interventional study in Taiwan. Biomed Res Int. (2017) 2017:2981624–7. doi: 10.1155/2017/2981624
29. Klomp, RW, Jones, L, Watanabe, E, and Thompson, WW. CDC's multiple approaches to safeguard the health, safety, and resilience of Ebola responders. Prehosp Disaster Med. (2020) 35:69–75. doi: 10.1017/S1049023X19005144
30. Leiva-Bianchi, M, Cornejo, F, Fresno, A, Rojas, C, and Serrano, C. Effectiveness of cognitive-behavioural therapy for post-disaster distress in post-traumatic stress symptoms after Chilean earthquake and tsunami. Gac Sanit. (2018) 32:291–6. doi: 10.1016/j.gaceta.2017.07.018
31. Osman, I, Hamid, S, and Singaram, VS. Efficacy of a brief online mindfulness-based intervention on the psychological well-being of health care professionals and trainees during the COVID-19 pandemic: a mixed method design. Health SA. (2021) 26:1682. doi: 10.4102/hsag.v26i0.1682
32. Waterman, S, Cole, CL, Greenberg, N, Rubin, GJ, and Beck, A. A qualitative study assessing the feasibility of implementing a group cognitive-behavioural therapy-based intervention in Sierra Leone. BJPsych Int. (2019) 16:31–4. doi: 10.1192/bji.2018.7
33. Waterman, S, Hunter, ECM, Cole, CL, Evans, LJ, Greenberg, N, Rubin, GJ, et al. Training peers to treat Ebola Centre workers with anxiety and depression in Sierra Leone. Int J Soc Psychiatry. (2018) 64:156–65. doi: 10.1177/0020764017752021
34. Zhou, K, Kong, J, Wan, Y, Zhang, X, Liu, X, Qu, B, et al. Positive impacts of e-aid cognitive behavioural therapy on the sleep quality and mood of nurses on site during the COVID-19 pandemic. Sleep Breath. (2022) 26:1947–51. doi: 10.1007/s11325-021-02547-1
35. Fiol-DeRoque, MA, Serrano-Ripoll, MJ, Jimenez, R, Zamanillo-Campos, R, Yanez-Juan, AM, Bennasar-Veny, M, et al. A Mobile phone-based intervention to reduce mental health problems in health care workers during the COVID-19 pandemic (PsyCovidApp): randomized controlled trial. JMIR Mhealth Uhealth. (2021) 9:e27039. doi: 10.2196/27039
36. Gnanapragasam, SN, Tinch-Taylor, R, Scott, HR, Hegarty, S, Souliou, E, Bhundia, R, et al. Multicentre, England-wide randomised controlled trial of the 'Foundations' smartphone application in improving mental health and well-being in a healthcare worker population. Br J Psychiatry. (2023) 222:58–66. doi: 10.1192/bjp.2022.103
37. Karakashian, M. Countertransference issues in crisis work with natural disaster victims. Psychother Theory Res Pract Train. (1994) 31:334–41. doi: 10.1037/h0090228
38. Leitch, ML, Vanslyke, J, and Allen, M. Somatic experiencing treatment with social service workers following hurricanes Katrina and Rita. Soc Work. (2009) 54:9–18. doi: 10.1093/sw/54.1.9
39. Mahaffey, BL, Mackin, DM, Rosen, J, Schwartz, RM, Taioli, E, and Gonzalez, A. The disaster worker resiliency training program: a randomized clinical trial. Int Arch Occup Environ Health. (2021) 94:9–21. doi: 10.1007/s00420-020-01552-3
40. Pallavicini, F, Orena, E, di Santo, S, Greci, L, Caragnano, C, Ranieri, P, et al. A virtual reality home-based training for the management of stress and anxiety among healthcare workers during the COVID-19 pandemic: study protocol for a randomized controlled trial. Trials. (2022) 23:451. doi: 10.1186/s13063-022-06337-2
41. Powell, T, and Yuma-Guerrero, P. Supporting community health workers after a disaster: findings from a mixed-methods pilot evaluation study of a psychoeducational intervention. Disaster Med Public Health Prep. (2016) 10:754–61. doi: 10.1017/dmp.2016.40
42. Powell, TM, Wegmann, KM, and Shin, OJ. Stress and coping in social service providers after superstorm Sandy: an examination of a postdisaster psychoeducational intervention. Traumatology. (2019) 25:96–03. doi: 10.1037/trm0000189
43. Serrano-Ripoll, MJ, Ricci-Cabello, I, Jimenez, R, Zamanillo-Campos, R, Yanez-Juan, AM, Bennasar-Veny, M, et al. Effect of a mobile-based intervention on mental health in frontline healthcare workers against COVID-19: protocol for a randomized controlled trial. J Adv Nurs. (2021) 77:2898–07. doi: 10.1111/jan.14813
44. Yi-Frazier, JP, O'Donnell, MB, Adhikari, EA, Zhou, C, Bradford, MC, Garcia-Perez, S, et al. Assessment of resilience training for hospital employees in the era of COVID-19. JAMA Netw Open. (2022) 5:e2220677. doi: 10.1001/jamanetworkopen.2022.20677
45. Berger, R, and Gelkopf, M. An intervention for reducing secondary traumatization and improving professional self-efficacy in well baby clinic nurses following war and terror: a random control group trial. Int J Nurs Stud. (2011) 48:601–10. doi: 10.1016/j.ijnurstu.2010.09.007
46. Hosseinzadeh Asl, NR. A randomized controlled trial of a mindfulness-based intervention in social workers working during the COVID-19 crisis. Curr Psychol. (2021) 41:8192–9. doi: 10.1007/s12144-021-02150-3
47. Hsieh, HF, Huang, YT, Ma, SC, and Wang, YW. Occupational burnout and stress of nurses in Taiwan regarding COVID-19: an intervention with gong medication. J Nurs Manag. (2022) 30:3909–17. doi: 10.1111/jonm.13653
48. Ibrahim, K, Komariah, M, and Herliani, YK. The effect of mindfulness breathing meditation on psychological well-being: a quasi-experimental study among nurses working for COVID-19 patients. Holist Nurs Pract. (2022) 36:46–51. doi: 10.1097/HNP.0000000000000464
49. Iwakuma, M, Oshita, D, Yamamoto, A, and Urushibara-Miyachi, Y. Effects of breathing-based meditation on earthquake-affected health professionals. Holist Nurs Pract. (2017) 31:177–82. doi: 10.1097/HNP.0000000000000211
50. Joshi, SP, Wong, AI, and Brucker, A. Efficacy of transcendental meditation to reduce stress among health care workers: a randomized clinical trial. JAMA Netw Open. (2022) 5:e2231917. doi: 10.1001/jamanetworkopen.2022.31917
51. Keng, SL, Chin, JWE, Mammadova, M, and Teo, I. Effects of Mobile app-based mindfulness practice on healthcare workers: a randomized active controlled trial. Mindfulness (N Y). (2022) 13:2691–04. doi: 10.1007/s12671-022-01975-8
52. Li, JM, Wu, R, Zhang, T, Zhong, SY, Hu, T, Wang, D, et al. Psychological responses of medical staff during COVID-19 and the adjustment effect of brief mindfulness meditation. Complement Ther Clin Pract. (2022) 48:101600. doi: 10.1016/j.ctcp.2022.101600
53. Liu, B, Zhu, Y, and Huang, S. Influence of TCM Baduanjing exercise on physical and mental condition of international medical team members fighting against Ebola virus. (English). Chin Nurs Res. (2015) 29:2629.
54. Si, SCKA, and Kilinc, T. The effect of laughter yoga on perceived stress, burnout, and life satisfaction in nurses during the pandemic: a randomized controlled trial. Complement Ther Clin Pract. (2022) 49:101637. doi: 10.1016/j.ctcp.2022.101637
55. Waelde, LC, Hechanova, M, Ramos, PAP, Macia, KS, and Moschetto, JM. Mindfulness and mantra training for disaster mental health workers in the Philippines. Mindfulness. (2018) 9:1181–90. doi: 10.1007/s12671-017-0855-2
56. Waelde, LC, Uddo, M, Marquett, R, Ropelato, M, Freightman, S, Pardo, A, et al. A pilot study of meditation for mental health workers following hurricane Katrina. J Trauma Stress. (2008) 21:497–00. doi: 10.1002/jts.20365
57. Yıldırım, D, and Çiriş, YC. The effect of mindfulness-based breathing and music therapy practice on nurses stress, work-related strain, and psychological well-being during the COVID-19 pandemic: a randomized controlled trial. Holist Nurs Pract. (2022) 36:156–65. doi: 10.1097/HNP.0000000000000511
58. Chen, R, Chou, KR, Huang, YJ, Wang, TS, Liu, SY, and Ho, LY. Effects of a SARS prevention programme in Taiwan on nursing staff's anxiety, depression and sleep quality: a longitudinal survey. Int J Nurs Stud. (2006) 43:215–25. doi: 10.1016/j.ijnurstu.2005.03.006
59. Saqib, A, and Rampal, T. Quality improvement report: setting up a staff well-being hub through continuous engagement. BMJ Open Qual. (2020) 9:e001008. doi: 10.1136/bmjoq-2020-001008
60. Zaghini, F, Fiorini, J, Livigni, L, Carrabs, G, and Sili, A. A mixed methods study of an organization's approach to the COVID-19 health care crisis. Nurs Outlook. (2021) 69:793–04. doi: 10.1016/j.outlook.2021.05.008
61. Giordano, F, Scarlata, E, Baroni, M, Gentile, E, Puntillo, F, Brienza, N, et al. Receptive music therapy to reduce stress and improve wellbeing in Italian clinical staff involved in COVID-19 pandemic: a preliminary study. Arts Psychother. (2020) 70:101688. doi: 10.1016/j.aip.2020.101688
62. Mahdood, B, Imani, B, and Khazaei, S. Effects of inhalation aromatherapy with Rosa damascena (damask Rose) on the state anxiety and sleep quality of operating room personnel during the COVID-19 pandemic: a randomized controlled trial. J. Perianesth. Nur. Off. J. Am. Soc. (2022) 37:493–00. doi: 10.1016/j.jopan.2021.09.011
63. Tong, J, Zhang, J, Zhu, N, Pei, Y, Liu, W, Yu, W, et al. Effects of COVID-19 pandemic on mental health among frontline healthcare workers: a systematic review and meta-analysis. Front Psychol. (2022) 13:1096857. doi: 10.3389/fpsyg.2022.1096857
64. Aldhamin, RA, and Al Saif, AZ. The mental health of healthcare workers in GCC countries during the COVID-19 pandemic: a systematic review and meta-analysis. J Taibah Univ Med Sci. (2023) 18:45–60. doi: 10.1016/j.jtumed.2022.07.014
65. Garcia-Vivar, C, Rodriguez-Matesanz, I, San Martin-Rodriguez, L, Soto-Ruiz, N, Ferraz-Torres, M, and Escalada-Hernandez, P. Analysis of mental health effects among nurses working during the COVID-19 pandemic: a systematic review. J Psychiatr Ment Health Nurs. (2023) 30:326–40. doi: 10.1111/jpm.12880
66. Umbetkulova, S, Kanderzhanova, A, Foster, F, Stolyarova, V, and Cobb-Zygadlo, D. Mental health changes in healthcare workers DURING COVID-19 pandemic: a systematic REVIEW of longitudinal studies. Eval Health Prof. (2023) 76:11650. doi: 10.1177/01632787231165076
67. Ury, E. Mental health conditions of pandemic healthcare workers: findings from a systematic review and meta-analysis. Evid Based Nurs. (2023) 26:27. doi: 10.1136/ebnurs-2022-103552
68. Zhu, H, Yang, X, Xie, S, and Zhou, J. Prevalence of burnout and mental health problems among medical staff during the COVID-19 pandemic: a systematic review and meta-analysis. BMJ Open. (2023) 13:e061945. doi: 10.1136/bmjopen-2022-061945
69. Public Health Ontario. COVID-19 – Strategies adaptable from healthcare to public health settings to support the mental health and resilience of the workforce during the COVID-19 pandemic recovery. Toronto, ON: Public Health Ontario (2021).
70. Kunzler, AM, Stoffers-Winterling, J, Stoll, M, Mancini, AL, Lehmann, S, Blessin, M, et al. Mental health and psychosocial support strategies in highly contagious emerging disease outbreaks of substantial public concern: a systematic scoping review. PLoS One. (2021) 16:e0244748. doi: 10.1371/journal.pone.0244748
71. Sangraula, M, Kohrt, BA, Ghimire, R, Shrestha, P, Luitel, NP, Van't Hof, E, et al. Development of the mental health cultural adaptation and contextualization for implementation (mhCACI) procedure: a systematic framework to prepare evidence-based psychological interventions for scaling. Glob Ment Health (Camb). (2021) 8:e6. doi: 10.1017/gmh.2021.5
72. Cunningham, T. The use and role of narrative practices to mitigate compassion fatigue among expatriate health workers during the Ebola outbreak of 2013-2016. Dissertation abstracts international: Section B: The sciences and engineering (2017) 77 11-B(E)
73. Powell, R, Scott, NW, Manyande, A, Bruce, J, Vogele, C, Byrne-Davis, LM, et al. Psychological preparation and postoperative outcomes for adults undergoing surgery under general anaesthesia. Cochrane Database Syst Rev. (2016) 2016:CD008646. doi: 10.1002/14651858.CD008646.pub2
74. Nashwan, AJ, Mathew, RG, Anil, R, Allobaney, NF, Nair, SK, Mohamed, AS, et al. The safety, health, and well-being of healthcare workers during COVID-19: a scoping review. AIMS Public Health. (2023) 10:593–09. doi: 10.3934/publichealth.2023042
Keywords: mental health, healthcare workers, COVID-19, public health emergency, education/awareness and skill development/training, prevention
Citation: Neil-Sztramko SE, Belita E, Hopkins S, Sherifali D, Anderson L, Apatu E, Kapiriri L, Tarride JE, Bellefleur O, Kaasalainen S, Marr S and Dobbins M (2023) What are effective strategies to respond to the psychological impacts of working on the frontlines of a public health emergency? Front. Public Health. 11:1282296. doi: 10.3389/fpubh.2023.1282296
Edited by:
Hubert Annen, ETH Zurich, SwitzerlandReviewed by:
Ling Wang, King's College London, United KingdomCopyright © 2023 Neil-Sztramko, Belita, Hopkins, Sherifali, Anderson, Apatu, Kapiriri, Tarride, Bellefleur, Kaasalainen, Marr and Dobbins. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Sarah E. Neil-Sztramko, bmVpbHN6dHNAbWNtYXN0ZXIuY2E=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.