 Chao Xue
Chao Xue Juan Li2*
Juan Li2* Huan Tang
Huan Tang
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Public Health, 01 December 2023
Sec. Aging and Public Health
Volume 11 - 2023 | https://doi.org/10.3389/fpubh.2023.1277995
This article is part of the Research TopicPromoting Healthy Aging Across the LifespanView all 39 articles
Background: Subjective cognitive decline (SCD) is considered a preclinical stage of Alzheimer’s disease. However, reliable prevalence estimates of SCD in the Chinese population are lacking, underscoring the importance of such metrics for policymakers to formulate appropriate healthcare strategies.
Objective: To systematically evaluate SCD prevalence among older Chinese adults.
Methods: PubMed, Web of Science, The Cochrane Library, Embase, CNKI, Wanfang, VIP, CBM, and Airiti Library databases were searched for studies on SCD in older Chinese individuals published before May 2023. Two investigators independently screened the literature, extracted the information, and assessed the bias risk of the included studies. A meta-analysis was then conducted using Stata 16.0 software via a random-effects model to analyze SCD prevalence in older Chinese adults.
Results: A total of 17 studies were included (n = 31,782). The SCD prevalence in older Chinese adults was 46.4% (95% CI, 40.6–52.2%). Further, subgroup analyzes indicated that SCD prevalence was 50.8% in men and 58.9% among women. Additionally, SCD prevalence in individuals aged 60–69, 70–79, and ≥ 80 years was 38.0, 45.2, and 60.3%, respectively. Furthermore, SCD prevalence in older adults with BMI <18.5, 18.5–24.0, and > 24.0 was 59.3, 54.0, and 52.9%, respectively. Geographically, SCD prevalence among older Chinese individuals was 41.3% in North China and 50.0% in South China. In terms of residence, SCD prevalence was 47.1% in urban residents and 50.0% among rural residents. As for retired individuals, SCD prevalence was 44.2% in non-manual workers and 49.2% among manual workers. In the case of education, individuals with an education level of “elementary school and below” had an SCD prevalence rate of 62.8%; “middle school, “52.4%; “high school, “55.0%; and “college and above, “51.3%. Finally, SCD prevalence was lower among married individuals with surviving spouses than in single adults who were divorced, widowed, or unmarried.
Conclusion: Our systematic review and meta-analysis identified significant and widespread SCD prevalence in the older population in China. Therefore, our review findings highlight the urgent requirement for medical institutions and policymakers across all levels to prioritize and rapidly develop and implement comprehensive preventive and therapeutic strategies for SCD.
Systematic review registration: https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42023406950, identifier: CRD42023406950.
Alzheimer’s disease (AD) is the leading cause of dementia (1, 2), with the latest data from the 2023 Alzheimer’s Disease Facts and Figures report indicating that approximately 10% of the world’s population aged over 65 years is living with AD (1). Moreover, the number of individuals with AD is projected to exceed 131 million by 2050 (3). Furthermore, the current status of AD epidemiology in China appears to be much worse than the global average. China, which has the fastest-growing older population in the world, may account for approximately half of the global AD population by 2050 (4, 5). With the increasing aging population in China, dementia (particularly AD) incidence is escalating rapidly (6, 7). AD is now the fifth leading cause of death in China (4, 8), and it is seriously affecting the physical and mental health of patients and family caregivers, utilizing national public health resources, and exacerbating the social and economic burden (1, 4, 5, 9).
Recent studies have indicated that preventive strategies for AD are the key to reducing this disease prevalence (1). Accurate identification and scientific interventions during the early AD stages can result in effective treatments for its comprehensive management (10–12), thereby reducing the financial and caregiving burdens associated with this neurodegenerative disease. In 2014, Jessen et al. (13) formally proposed the concept of subjective cognitive decline (SCD), referring to an individual’s subjective perception of a persistent decline in cognitive function or memory compared to their previous normal state, irrespective of the normal results on objective neuropsychological examinations (13–15). Additionally, Jessen et al. (13, 16) suggested that SCD might serve as a preclinical stage of AD, aiding in the prediction of AD development. SCD has garnered considerable worldwide attention from scholars since its initial proposal, becoming a focal point in the fields of geriatric neurology and cognition (14, 17, 18). A meta-analysis of longitudinal studies found that SCD is associated with an increased risk of developing dementia (HR = 1.90, 95% CI 1.52–2.36; OR = 2.48, 95% CI 1.97–3.14), with an average progression to dementia of 10% (19). However, considering that SCD-related research in China was initiated relatively later, its prevalence and severity may be underestimated in the older adult population of this country.
Epidemiological studies have been prioritized in the Beijing area since 2015 to understand SCD prevalence among older Chinese adults and guide policy-making to address this trend (20). Although concerns regarding SCD emerging as a major public health issue in China have increased (21–24), epidemiological data on SCD in China’s older population are scarce, with existing surveys being limited to the specific characteristics, study methodologies, identification, and classification of SCD (20, 25, 26). Thus, direct comparisons between individual studies are constrained.
In this systematic review and meta-analysis, our primary objective was to evaluate SCD prevalence in older Chinese adults by analyzing all available published data related to this topic. Additionally, we aimed to compare prevalence estimates among various subgroups, including those based on sex, age, body mass index (BMI), marital status, education level, geographical region, residence, and occupation type before retirement.
This review adhered to the guidelines of the Preferred Reporting Items for Systematic Reviews and Meta-Analyzes (PRISMA) (27) and the Meta-Analysis of Observational Studies in Epidemiology (28). Furthermore, this review was registered with PROSPERO (registration no. CRD42023406950).
Here, we systematically searched nine databases, including Embase, PubMed, The Cochrane Library, Web of Science, China National Knowledge Infrastructure Database, Wanfang Database, Chinese Biomedical Literature Database, Chinese Scientific Journal Database (VIP database), and Airiti Library, to locate all relevant publications on SCD epidemiology in China. The search period was from the date of database inception to May 1, 2023, with no language restrictions. Before finalizing the search strategy, we consulted with a librarian knowledgeable about systematic review methodology and the process of refining search terms. We also conducted several preliminary searches to obtain the most comprehensive collection of relevant literature. The search terms entered were as follows: (“subjective cognitive decline” OR “subjective memory decline” OR “subjective memory complain*” OR “subjective cognitive complain*” OR “subjective memory loss”) AND (“incidence” OR “prevalence” OR “occurrence” OR “rate*” OR “epidemiology”) AND (“Chinese” OR “China” OR “Hong Kong” OR “Macao” OR “Taiwan”).
The inclusion criteria were as follows: (1) studies with participants older than 60 years, (2) those including participants residing in China, including mainland China, Hong Kong, Macao, and Taiwan, (3) observational research study types, including cross-sectional and cohort studies, (4) those that applied the SCD diagnostic criteria (13, 16) and reported SCD prevalence, and (5) those published in Chinese or English. The exclusion criteria were as follows: (1) non-research articles such as reviews, case reports, comments, letters, and editorials, (2) duplicate publications, (3) studies without full-text availability, or (4) those of low research quality, i.e., Agency for Healthcare Research and Quality (AHRQ) quality assessment scores <4 (29).
All of the retrieved literature was imported into Endnote 20. After deleting duplicate initial search results within and between different databases, the two authors (C XUE and M HAO) independently reviewed the titles and abstracts to identify potentially eligible articles requiring a full assessment. In the case of multiple publications utilizing the same sample or original data, the publication with the largest sample size and the most thorough information on data extraction was given preference. To resolve differing opinions between the two reviewers, a third researcher (L CHEN) was consulted and asked to deliberate and vote on the specific issue. The two reviewers (C XUE and M HAO) then used a standardized form to independently extract and record the following information: first author, publication year, geographical location, sample size, number and age of participants, assessment tools, and SCD prevalence.
Two researchers (C XUE and M HAO) independently evaluated the bias risk in the included studies and cross-checked their assessments. In the case of disagreement, a discussion or a third-party consultation was used to obtain a judgment. To examine the methodological quality of the cross-sectional studies, we used an 11-item checklist recommended by the AHRQ (30). In this checklist, each item contained three options: “Yes, ““No, “or “Not clear.” A score of 1 point was given for “Yes,” whereas 0 points were scored for “No” and “Not clear.” The overall score ranged from 0 to 11, wherein articles with scores of 0–3 were classified as low quality; 4–7, moderate quality; and 8–11, high quality.
The metaprop command in Stata 16.0 (StataCorp, College Station, TX, United States) was used to statistically analyze SCD prevalence in the older Chinese population. Furthermore, the χ2 (with a test level of α = 0.1) and I2 tests were employed to analyze the heterogeneity of the results. For study results with no statistical heterogeneity (p ≥ 0.1 and I2 ≤ 50%), a fixed-effects model was utilized for the meta-analysis. Conversely, in those involving statistical heterogeneity (p < 0.1 or I2 > 50%), the results were further analyzed to identify the heterogeneity source (31). After eliminating the obvious clinical heterogeneity, a random-effects model was employed for the meta-analysis. The significance level for the meta-analysis was α = 0.05. Additionally, subgroup analysis was performed to evaluate SCD prevalence based on sex, age, BMI, marital status, education level, occupation type before retirement, and geographical region. Additionally, sensitivity analysis was conducted by sequentially excluding each study and then recalculating the pooled estimates of the remaining studies to determine the effect of individual studies on the overall prevalence estimates. Lastly, publication bias was evaluated using funnel plots and Egger’s test (32, 33).
The initial database search yielded 532 relevant literature, which was imported into the EndNote Literature Manager software. After deleting duplicates, 447 studies remained. Next, the two researchers (C XUE and M HAO) independently read the titles and abstracts and deleted studies that did not meet the review’s inclusion and exclusion criteria, resulting in 44 remaining studies. Further, the full text of the articles was read, leading to the deletion of 27 articles. Among them, seven had no available data, six were duplicates of previous publications, three did not have accessible full text, eight consisted of noncompliant study designs, and three involved noncompliant study populations. References of the included literature were also checked to identify any potentially missed publications. After this step-by-step filtering procedure, 17 studies were included in the final meta-analysis. The included studies had a total sample size of 31,782 participants, of which 14,390 were from the SCD population. The literature screening process and results are shown in Figure 1.

Figure 1. PRISMA flowchart for study selection.
Table 1 presents the characteristics of the studies included in the meta-analysis. A total of 17 studies were included, comprising 31,782 older adults. Regarding the inclusion criteria, all 17 studies stated that the study subjects were permanent local residents aged 60 years and above. Additionally, they were required to have normal objective cognitive function and daily living ability, as well as the ability to answer the relevant questionnaires independently. In terms of the exclusion criteria, all 17 studies mentioned excluding mild cognitive impairment and dementia. Thirteen studies mentioned excluding diseases that might affect objective cognitive function. Furthermore, 14 studies mentioned excluding severe mental disorders, 10 studies mentioned excluding severe visual or hearing impairment that could hinder normal assessment, and 9 studies mentioned excluding severe organ failure. Moreover, 6 studies mentioned excluding substance abuse, 2 studies mentioned excluding alcohol dependence, and 2 studies mentioned excluding participation in other interventional studies. Lastly, only 1 study mentioned excluding shift-workers. The sample sizes in these studies ranged from 173 to 10,312 individuals. The data examined in these studies were obtained from the years 2016 to 2023. The studies were conducted in 16 administrative divisions, including provinces, autonomous regions, and municipalities directly under the central government in China. Geographically, 10 studies were conducted in South China, whereas seven in North China. In terms of residence, 12 studies (70.6%) were performed in urban settings, three in rural areas (17.6%), and two (11.8%) involved urban and rural locations. Furthermore, the evaluation of literature quality yielded AHRQ scores of 5–9 for the included articles, indicating medium- to high-quality articles and confirming reliability in our review results.

Table 1. Characteristics of the included studies.
As illustrated in Figure 2, SCD prevalence in older Chinese individuals ranged from 18.8 to 76.3%. Further, the estimated pooled prevalence of SCD in the 17 studies was 46.4% (95% CI, 40.6–52.2%).
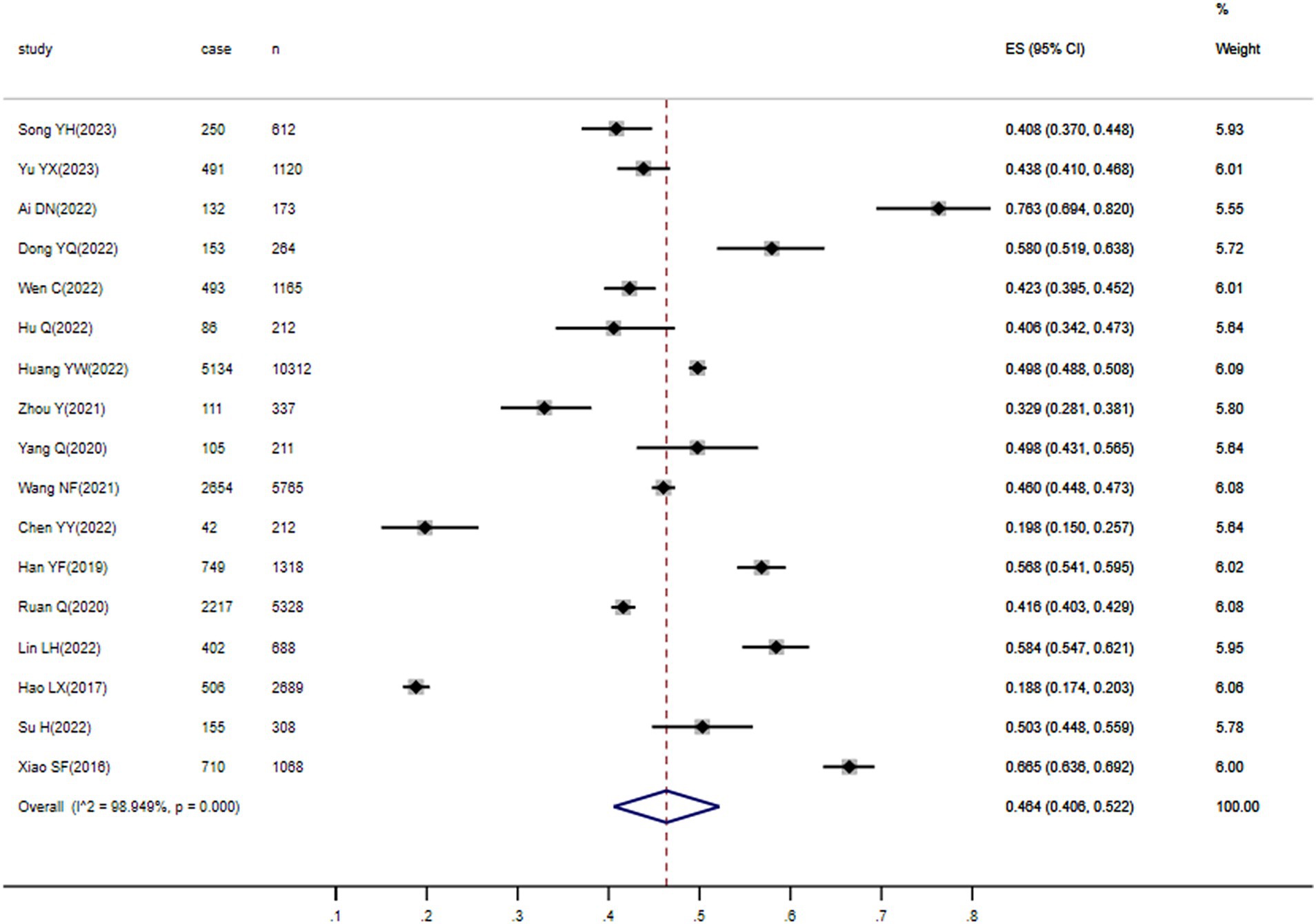
Figure 2. Forest plot of overall SCD prevalence in Chinese older adults.
Table 2 presents the subgroup analysis findings of SCD prevalence among older Chinese adults in the included studies. The results indicated that men had a significantly lower SCD prevalence (50.8, 95% CI, 41.4–60.2%) than women (58.9, 95% CI, 50.3–67.3%, p < 0.001).
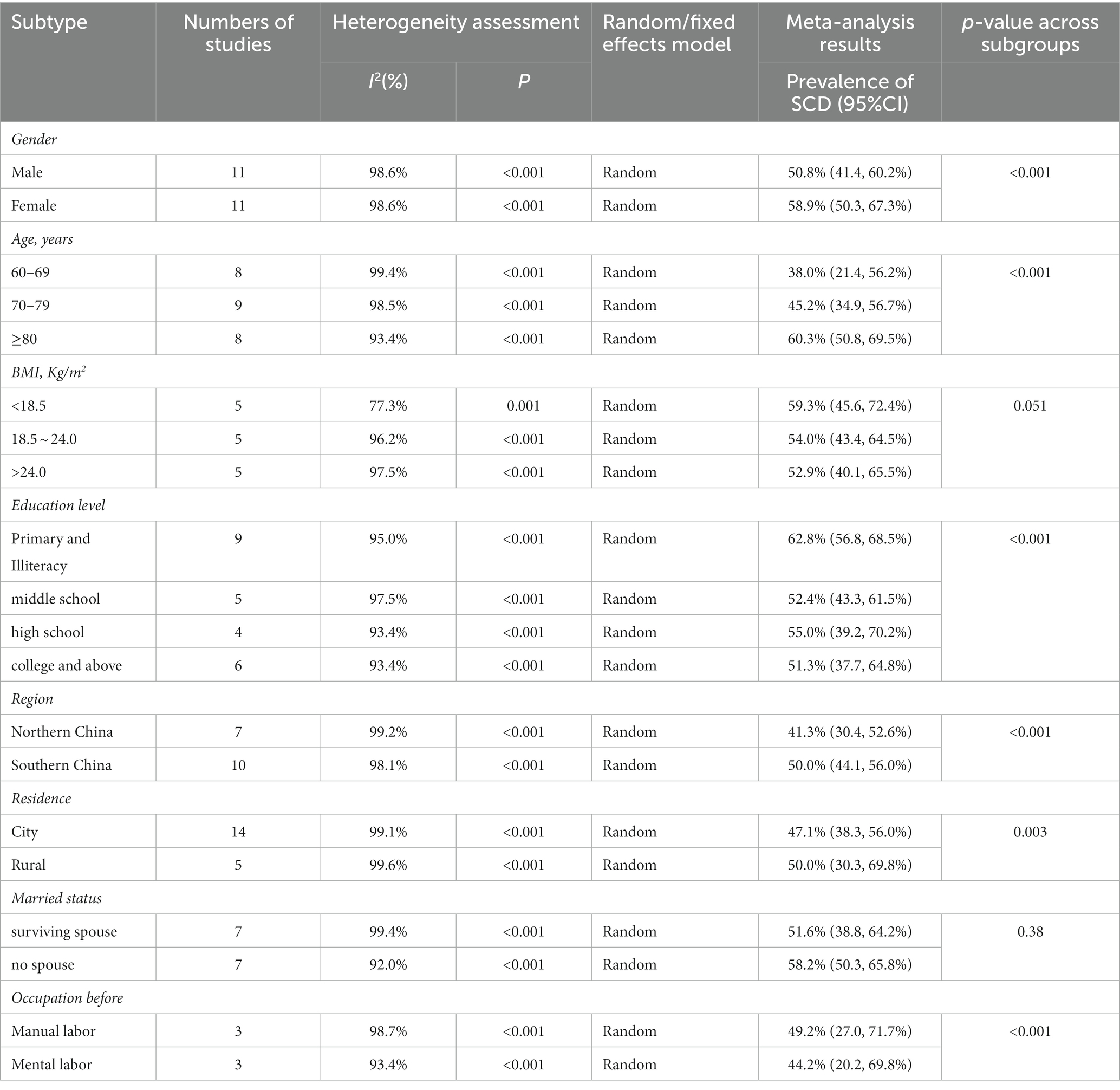
Table 2. Various subgroup analyzes of SCD prevalence in Chinese older adults.
Additionally, SCD prevalence was found to significantly increase with age (p < 0.001), with the 60–69 years age group exhibiting an SCD prevalence of 38.0% (95% CI, 21.4–56.2%); 70–79 years, 45.2% (95% CI, 34.9–56.7%); and ≥ 80 years, 60.3% (95% CI, 50.8–69.5%).
Furthermore, SCD prevalence in older adults decreased with increasing BMI. In particular, SCD prevalence in older adults with BMI <18.5, 18.5–24.0, and > 24.0 was 59.3% (95% CI, 45.6–72.4%), 54.0% (95% CI, 43.4–64.5%), and 52.9% (95% CI, 40.1–65.5%), respectively. Although this difference was only marginally significant (p = 0.051), this observation is still worth noting.
In terms of geographical regions, SCD prevalence significantly varied (p < 0.001) between older adults in South China (50.0, 95% CI, 44.1–56.0%) and those from North China (41.3, 95% CI, 30.4–52.6%). Furthermore, individuals residing in rural areas exhibited significantly higher SCD prevalence (50.0, 95% CI, 30.3–69.8%) than those in urban locations (47.1, 95% CI, 38.3–56.0%, p = 0.003).
Moreover, occupation type before retirement and education level also demonstrated significant differences in SCD prevalence. SCD prevalence among retired non-manual (44.2, 95% CI, 20.2–69.8%) was significantly lower than that in retired manual workers (49.2, 95% CI, 27.0–71.7%, p < 0.001). As for education level, SCD prevalence decreased as education level increased, with a significant difference among the four education levels (p < 0.001), including “elementary school and below,” “middle school,” “high school,” and “college and above.” Of which, individuals with a higher education level (i.e., college and above) had the lowest prevalence (51.3, 95% CI, 37.7–64.8%), followed by those with secondary education (i.e., middle school [52.4, 95% CI, 43.3–61.5%] and high school [55.0, 95% CI, 39.2–70.2%]). Older adults with education levels of elementary school and below had the highest SCD prevalence of 62.8% (95% CI, 56.8–68.5%).
Lastly, SCD prevalence in married individuals with surviving spouses was lower (51.6%; 95% CI, 38.8–64.2%) than in single adults who were divorced, widowed, or unmarried (58.2, 95% CI, 50.3–65.8%). However, this difference was not statistically significant (p = 0.38).
We also conducted a sensitivity analysis by excluding one study at a time to assess whether the variation between studies affected the overall estimate. As depicted in Figure 3, none of the studies caused significant changes in the pooled prevalence. This indicates that the results of the Meta analysis are reliable and stable.
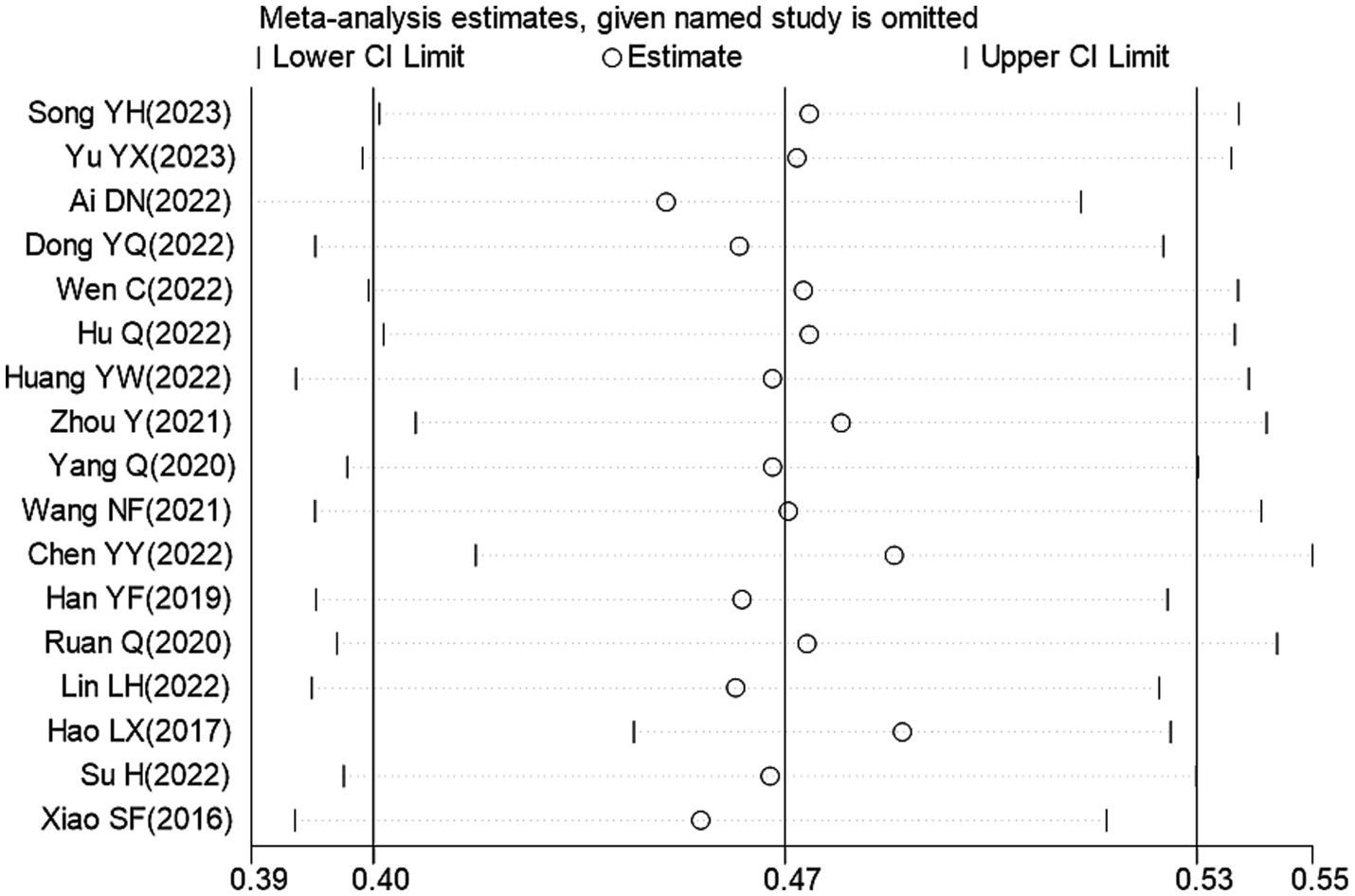
Figure 3. Sensitivity analysis of overall SCD prevalence in Chinese older adults.
Visual inspection revealed slight signs of asymmetry in the funnel plot (Figure 4). Additionally, Egger’s test indicated no significant publication bias, with no statistical significance detected for t (t = 0.16) and (p = 0.878) values. Based on the visual evaluation and Egger’s test results, we concluded that the publication bias risk in this review was low.
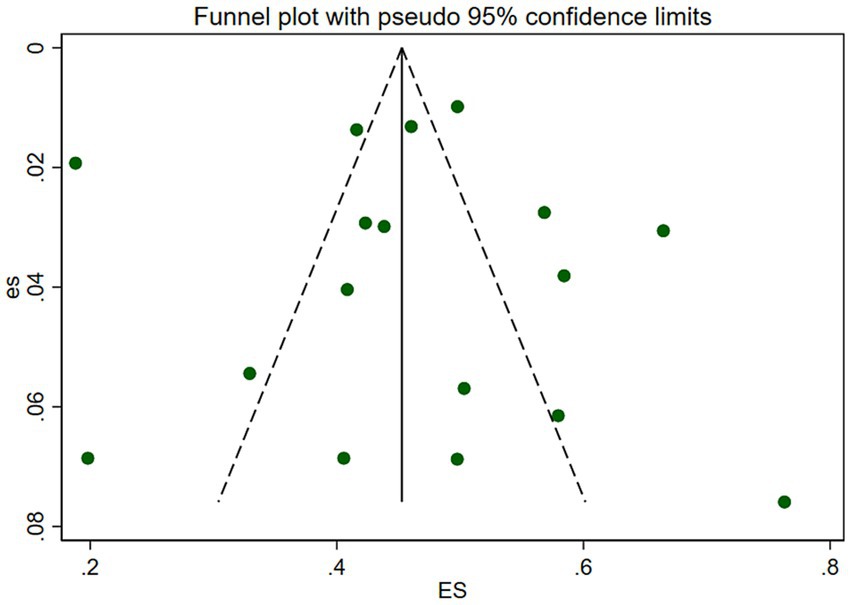
Figure 4. Funnel chart of overall SCD prevalence in Chinese older adults.
AD has become a public health priority in the context of aging (4, 5, 7). In recent years, SCD, a proposed preclinical stage of AD, has received considerable global interest (14, 16). To the best of our knowledge, this is the first systematic review to investigate SCD prevalence in older adults in China. We found that SCD prevalence was 46.4% among older Chinese adults, suggesting that this condition was particularly common within this population. Moreover, this result was higher than the SCD prevalence of 25.5 and 36.7% reported in the United States of America (48) and Australia (49), respectively, and comparable to that of 36.1–68.6% in Japan (50, 51). However, attention should be given to the fact that SCD prevalence in older adults may vary greatly between studies conducted in different countries due to the differences in sample source, sample size, geographical environment, and cultural background.
The 17 studies included in this review established strict inclusion and exclusion criteria when selecting study subjects to ensure homogeneity. All studies applied SCD diagnostic criteria consistent with those proposed by the Subjective Cognitive Decline Initiative (SCD-I) (13), ensuring the authenticity and accuracy of the reported SCD prevalence.
Additionally, our review found some distinctive findings during the subgroup analyzes. First, SCD prevalence was higher in women than in men. This difference may be because women are more sensitive to perceiving dynamic changes in their cognitive functioning than men; therefore, they are more likely to show concern about SCD (38, 40).
Second, SCD prevalence was positively correlated with increasing age, indicating that advanced age was associated with a higher risk of developing SCD. As individuals grow older, they may experience stressor overload, chronic inflammation (52, 53), and accelerated aging of brain cells (54), resulting in the gradual reduction of the brain’s cognitive reserve along with a continuous decline in cognitive function (55).
Third, older adults with an elementary school education or less had a higher SCD prevalence rate (62.8%). This observation suggests that higher education may be a protective factor for healthy cognitive functioning, consistent with previous findings (20, 34, 56, 57). This protective benefit could be attributed to the better knowledge base, stronger compensation function of the brain network, and increased neuronal vitality in older adults with higher education levels compared to those with an elementary school education or less (34, 35). These advantages could in turn lead to a better subjective cognitive status and relatively higher health literacy, making them more receptive to health knowledge and preventive and curative measures for SCD (34, 58). Therefore, medical professionals and policymakers should focus on the older population with lower education levels, develop a comprehensive cognitive screening and assessment process, and increase SCD awareness in the general population to improve health literacy and promote healthy behavior in older adults.
Fourth, this study found a higher prevalence of SCD in individuals with a BMI <18.5, at 59.3%. Although the difference in prevalence between BMI subgroups was only marginally statistically significant, these findings suggest that older adults with a lower BMI are more likely to experience SCD compared to those with a normal BMI. Previous research has also demonstrated a greater risk of concurrent malnutrition in older adults with a lower BMI (59), which can potentially contribute to persistent cognitive impairment (60). Therefore, it is recommended that the older population strive to maintain a normal BMI to preserve their ability to perform daily activities and retain good cognitive function.
Fifth, SCD prevalence in North and South China was >40.0%, implying a higher SCD prevalence in the Chinese population across different regions. Accordingly, physicians should conduct early comprehensive screening of subjective cognitive function in the Chinese population. This strategy will enable the timely detection and prevention of further cognitive function deterioration in individuals with SCD. Additionally, SCD prevalence in urban communities was found to be slightly lower than that in rural areas. This difference may be ascribed to the previously reported higher prevalence of cognitive disorders, including SCD, mild cognitive impairment, and dementia, in the rural areas of China (61).
Finally, manual laborers had a higher SCD prevalence than non-manual workers, possibly due to the better cognitive performance associated with higher education levels among the non-manual workers included in this study (34, 40, 41). Conversely, non-manual workers have been suggested to experience comparatively greater work stress, prolonged sedentary behavior, and a lack of appropriate physical activity (25, 62), potentially leading to excessive concern about their emotional state and cognitive functioning. Therefore, encouraging middle-aged and older populations to actively participate in community cultural activities is important (63). Such activities will help them avoid prolonged stress or negative emotions, ultimately enhancing their cognitive reserve as well as physical and mental well-being.
Our systematic review and meta-analysis revealed that women, individuals of advanced age, those with low education levels, residents in the southern region and rural areas, and those with manual work before retirement may exhibit higher SCD prevalence. Consequently, studies focusing on these specific populations should be prioritized by future researchers. Furthermore, we observed that most original studies relied on the SCD questionnaire (including SCD-Q9, SCD-Q, and COWAT, etc.) alone to assess subjective cognitive function. However, using only one tool to evaluate SCD might not provide adequate diagnostic value (13, 16). Nonetheless, considering the wide and convenient clinical application of SCD-Q9/SCD-Q, subsequent studies should build upon this questionnaire as well as emphasize the development of an in-depth SCD assessment process and tools. Moreover, the aging and health trend will likely become exacerbated in China due to the increasing life expectancy accompanied by worsening health conditions (64). This trend will eventually impose substantial stress on the necessity for population-wide cognitive screening. Therefore, the widespread implementation of AI technology in SCD screening and diagnosis could be a potential research area to help address this issue.
This study has many strengths that are worth mentioning. To the best of our knowledge, this is the first systematic review and meta-analysis to evaluate SCD prevalence in older Chinese adults. Additionally, our review adopted a thorough search strategy encompassing nine databases in the Chinese and English languages. We also utilized a double review process, thereby enhancing the comprehensiveness of our search results on SCD epidemiology in China. Furthermore, the original studies included in our analysis were classified as moderate- to high-quality articles, ensuring the reliability of our findings. Finally, we conducted extensive subgroup analyzes to explore the epidemiological characteristics of SCD in older Chinese adults.
Nonetheless, our study has several limitations that should be addressed in future research. First, a substantial amount of heterogeneity was detected in the subgroup analyzes. However, this heterogeneity is unavoidable in the meta-analysis of epidemiological surveys (65). Second, the SCD assessment tools and diagnostic criteria employed in the included studies were not standardized, potentially introducing measurement bias and reducing our results’ reliability. Third, most studies we reviewed were conducted in eastern China, thus underrepresenting the country’s western region. Consequently, our sample does not adequately represent all 34 Chinese provinces, including provincial-level municipalities, autonomous regions, and special administrative regions. Lastly, although our findings are promising, they should be interpreted cautiously owing to the high heterogeneity observed among studies, moderate bias risk in certain studies, and the likelihood of mild publication bias.
Our review suggests that monitoring SCD prevalence in older adults in China is crucial for the effective planning and organization of related healthcare services. Based on the available literature, our systematic review and meta-analysis indicate that SCD has a prevalence of 46.4% in older Chinese adults. However, these values may be an underestimation of the true prevalence because of insufficient high-quality data. Therefore, future research should focus on investigating the incidence, risk factors, and causes of SCD. Furthermore, the relevant authorities in China are critically required to accelerate the development and implementation of a broad range of preventive and therapeutic strategies for SCD. Moreover, initiatives for the early screening, diagnosis, and prevention of SCD will further help alleviate the social care and economic burdens caused by AD in the older population in China.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
CX: Data curation, Investigation, Methodology, Software, Writing – original draft, Writing – review & editing. MH: Data curation, Investigation, Methodology, Software, Writing – original draft. LC: Investigation, Methodology, Software, Writing – original draft. ZC: Methodology, Software, Validation, Visualization, Writing – original draft. ZT: Methodology, Software, Validation, Visualization, Writing – original draft. HT: Methodology, Software, Validation, Visualization, Writing – original draft. QF: Conceptualization, Formal analysis, Supervision, Writing – review & editing. JL: Conceptualization, Formal analysis, Funding acquisition, Supervision, Visualization, Writing – review & editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This study was supported by funding from the National Natural Science Foundation of China (No. 72364005), and Guizhou Administration of Traditional Chinese Medicine (No. QZYY-2023-115).
We thank Bullet Edits Limited for the linguistic editing and proofreading of the manuscript.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. 2023 Alzheimer's disease facts and figures. Alzheimers Dement. (2023) 19:1598–695. doi: 10.1002/alz.13016
2. Feigin, VL, Nichols, E, Alam, T, Bannick, MS, Beghi, E, Blake, N, et al. Global, regional, and national burden of neurological disorders, 1990–2016: a systematic analysis for the global burden of disease study 2016. Lancet Neurol. (2019) 18:459–80. doi: 10.1016/S1474-4422(18)30499-X
3. Arvanitakis, Z, Shah, RC, and Bennett, DA. Diagnosis and management of dementia: review. JAMA. (2019) 322:1589–99. doi: 10.1001/jama.2019.4782
4. Ren, R, Qi, J, Lin, S, Liu, X, Yin, P, Wang, Z, et al. The China alzheimer report 2022. Gen Psychiatr. (2022) 35:e100751. doi: 10.1136/gpsych-2022-100751
5. Jia, L, Quan, M, Fu, Y, Zhao, T, Li, Y, Wei, C, et al. Dementia in China: epidemiology, clinical management, and research advances. Lancet Neurol. (2020) 19:81–92. doi: 10.1016/S1474-4422(19)30290-X
6. Qi, S, Yin, P, Zhang, H, Zhang, Q, Xiao, Y, Deng, Y, et al. Prevalence of dementia in China in 2015: a nationwide community-based study. Front Public Health. (2021) 9:733314. doi: 10.3389/fpubh.2021.733314
7. Li, R, Qi, J, Yang, Y, Wu, Y, Yin, P, Zhou, M, et al. Disease burden and attributable risk factors of alzheimer's disease and dementia in China from 1990 to 2019. J Prev Alzheimers Dis. (2022) 9:306–14. doi: 10.14283/jpad.2021.69
8. Jia, J, Wei, C, Chen, S, Li, F, Tang, Y, Qin, W, et al. The cost of alzheimer's disease in China and re-estimation of costs worldwide. Alzheimers Dement. (2018) 14:483–91. doi: 10.1016/j.jalz.2017.12.006
9. Chhetri, JK, Chan, P, Vellas, B, Touchon, J, and Gauthier, S. Report from the first clinical trials on alzheimer’s disease (ctad) asia-China 2018: bringing together global leaders. J Prev Alzheimers Dis. (2019) 6:144–7. doi: 10.14283/jpad.2019.2
10. Sperling, RA, Aisen, PS, Beckett, LA, Bennett, DA, Craft, S, Fagan, AM, et al. Toward defining the preclinical stages of alzheimer's disease: recommendations from the national institute on aging-alzheimer's association workgroups on diagnostic guidelines for alzheimer's disease. Alzheimers Dement. (2011) 7:280–92. doi: 10.1016/j.jalz.2011.03.003
11. Zhang, J, Gao, Y, Gao, Y, Munsell, BC, and Shen, D. Detecting anatomical landmarks for fast alzheimer's disease diagnosis. IEEE Trans Med Imaging. (2016) 35:2524–33. doi: 10.1109/TMI.2016.2582386
12. Xu, X, Li, W, Tao, M, Xie, Z, Gao, X, Yue, L, et al. Effective and accurate diagnosis of subjective cognitive decline based on functional connection and graph theory view. Front Neurosci. (2020) 14:577887. doi: 10.3389/fnins.2020.577887
13. Jessen, F, Amariglio, RE, Boxtel, M, Breteler, M, Ceccaldi, M, Chételat, G, et al. A conceptual framework for research on subjective cognitive decline in preclinical alzheimer's disease. Alzheimers Dement. (2014) 10:844–52. doi: 10.1016/j.jalz.2014.01.001
14. Rabin, LA, Smart, CM, and Amariglio, RE. Subjective cognitive decline in preclinical alzheimer's disease. Annu Rev Clin Psychol. (2017) 13:369–96. doi: 10.1146/annurev-clinpsy-032816-045136
15. Molinuevo, JL, Rabin, LA, Amariglio, R, Buckley, R, Dubois, B, Ellis, KA, et al. Implementation of subjective cognitive decline criteria in research studies. Alzheimers Dement. (2017) 13:296–311. doi: 10.1016/j.jalz.2016.09.012
16. Jessen, F, Amariglio, RE, Buckley, RF, van der Flier, WM, Han, Y, Molinuevo, JL, et al. The characterisation of subjective cognitive decline. Lancet Neurol. (2020) 19:271–8. doi: 10.1016/S1474-4422(19)30368-0
17. Wang, X, Huang, W, Su, L, Xing, Y, Jessen, F, Sun, Y, et al. Neuroimaging advances regarding subjective cognitive decline in preclinical alzheimer's disease. Mol Neurodegener. (2020) 15:55. doi: 10.1186/s13024-020-00395-3
18. Jessen, F, Spottke, A, Boecker, H, Brosseron, F, Buerger, K, Catak, C, et al. Design and first baseline data of the dzne multicenter observational study on predementia alzheimer's disease (delcode). Alzheimers Res Ther. (2018) 10:15. doi: 10.1186/s13195-017-0314-2
19. Pike, KE, Cavuoto, MG, Li, L, Wright, BJ, and Kinsella, GJ. Subjective cognitive decline: level of risk for future dementia and mild cognitive impairment, a meta-analysis of longitudinal studies. Neuropsychol Rev. (2022) 32:703–35. doi: 10.1007/s11065-021-09522-3
20. Hao, L, Wang, X, Zhang, L, Xing, Y, Guo, Q, Hu, X, et al. Prevalence, risk factors, and complaints screening tool exploration of subjective cognitive decline in a large cohort of the chinese population. J Alzheimers Dis. (2017) 60:371–88. doi: 10.3233/JAD-170347
21. Xu, S, Ren, Y, Liu, R, Li, Y, Hou, T, Wang, Y, et al. Prevalence and progression of subjective cognitive decline among rural chinese older adults: a population-based study. J Alzheimers Dis. (2023) 93:1355–68. doi: 10.3233/JAD-221280
22. Hao, L, Xing, Y, Li, X, Mu, B, Zhao, W, Wang, G, et al. Risk factors and neuropsychological assessments of subjective cognitive decline (plus) in chinese memory clinic. Front Neurosci. (2019) 13:846. doi: 10.3389/fnins.2019.00846
23. Cheng, G, Liu, D, Huang, L, Han, G, Hu, F, Wu, Z, et al. Prevalence and risk factors for subjective cognitive decline and the correlation with objective cognition among community-dwelling older adults in China: results from the Hubei memory and aging cohort study. Alzheimers Dement. (2023) 19:5074–85. doi: 10.1002/alz.13047
24. Jiang, X, Hu, X, Daamen, M, Wang, X, Fan, C, Meiberth, D, et al. Altered limbic functional connectivity in individuals with subjective cognitive decline: converging and diverging findings across chinese and german cohorts. Alzheimers Dement. (2023) 19:4922–34. doi: 10.1002/alz.13068
25. Lin, LH, Wang, SB, Xu, WQ, Hu, Q, Zhang, P, Ke, YF, et al. Subjective cognitive decline symptoms and its association with socio-demographic characteristics and common chronic diseases in the southern chinese older adults. BMC Public Health. (2022) 22:127. doi: 10.1186/s12889-022-12522-4
26. Su, H, Zhou, YQ, Sun, YJ, and Cai, YJ. The relationship between depression and subjective cognitive decline in older adults of China: the mediating role of general self-efficacy. Psychol Health Med. (2022) 28:1057–67. doi: 10.1080/13548506.2022.2125165
27. Page, MJ, McKenzie, JE, Bossuyt, PM, Boutron, I, Hoffmann, TC, Mulrow, CD, et al. The prisma 2020 statement: an updated guideline for reporting systematic reviews. BMJ. (2021) 372:n71. doi: 10.1136/bmj.n71
28. Stroup, DF, Berlin, JA, Morton, SC, Olkin, I, Williamson, GD, Rennie, D, et al. Meta-analysis of observational studies in epidemiology: a proposal for reporting. Meta-analysis of observational studies in epidemiology (moose) group. JAMA. (2000) 283:2008–12. doi: 10.1001/jama.283.15.2008
29. Hu, S, Pan, N, Liu, C, Wang, Y, and Zhang, T. Age matching is essential for the study of cerebrospinal fluid strem2 levels and alzheimer's disease risk: a meta-analysis. Front Aging Neurosci. (2021) 13:775432. doi: 10.3389/fnagi.2021.775432
30. Zeng, X, Zhang, Y, Kwong, JSW, Zhang, C, Li, S, Sun, F, et al. The methodological quality assessment tools for preclinical and clinical studies, systematic review and meta-analysis, and clinical practice guideline: a systematic review. J Evid Based Med. (2015) 8:2–10. doi: 10.1111/jebm.12141
31. Ullah, I, Bibi, S, Ul Haq, I, Safia, UK, Ge, L, et al. The systematic review and meta-analysis on the immunogenicity and safety of the tuberculosis subunit vaccines m72/as01e and mva85a. Front Immunol. (2020) 11:1806. doi: 10.3389/fimmu.2020.01806
32. Egger, M, Davey Smith, G, Schneider, M, and Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ (Clinical research ed). (1997) 315:629–34. doi: 10.1136/bmj.315.7109.629
33. Sterne, JA, and Egger, M. Funnel plots for detecting bias in meta-analysis: guidelines on choice of axis. J Clin Epidemiol. (2001) 54:1046–55. doi: 10.1016/S0895-4356(01)00377-8
34. Song, Y, Liu, Y, Yang, Q, Wang, S, Hu, Q, Zheng, C, et al. Correlation of subjective cognitive decline with multimorbidity among elderly people. Chinese Gen Pract. (2023) 26:1241–9. doi: 10.12114/j.issn.1007-9572.2022.0800
35. Yu, Y, Bai, R, Yu, W, Guo, X, and Wu, L. Occurrence status and influencing factors of cognitive dysfunction in population aged 60 and above in Inner Mongolia. Chinese Gen Pract. (2023) 26:2581–8. doi: 10.12114/j.issn.1007-9572.2023.0004
36. Ai, D, Nie, J, Lin, X, Gu, C, Fei, C, Li, L, et al. Correlation analysis between subjective cognitive decline and emotional state of the community elderly. Geriatr Health Care. (2022) 28:978–82. doi: 10.3969/j.issn.1008-8296.2022.05.008
37. Dong, Y, and Wang, W. Correlation study between subjective cognitive decline and grip strength in elderly community population. Chinese Gen Pract. (2022) 20:1363–6. doi: 10.16766/j.cnki.issn.1674-4152.002598
38. Wen, C. Risk factors for subjective cognitive decline and association of subjective cognitive decline with cerebrospinal fluid biomarkers of Alzheimer’s disease pathology in cognitively intact older adults: the CABLE study. Qingdao: Qingdao University (2022).
39. Hu, Q, Song, Y, Wang, S, Zhao, W, Liu, Y, and Zhang, P. Subjective cognitive decline among institutionalized older adults and its influencing factor. J Nurs Sci. (2022) 37:87–90. doi: 10.3870/j.issn.1001-4152.2022.09.087
40. Huang, Y. Study on the prevalence and risk factors of subjective cognitive decline in the community-dwelling old adults. Wuhan: Wuhan University of Science and Technology (2022).
41. Zhou, Y, Gan, S, and Li, Z. Status quo of subjective cognitive decline and its influencing factors among community-dwelling elder adults. Nurs J Chin PLA. (2021) 38:21–4. doi: 10.3969/j.issn.1008-9993.2021.04.006
42. Yang, Q. Subjective cognitive decline and its behavioral and psychological symptoms in community-dwelling elderly. Huazhong: Huazhong University of Science & Technology (2020).
43. Wang, N, Song, Z, Liu, X, Wang, L, Cao, J, and Du, Y. The characteristics and influencing factors of subjective cognitive decline in rural elderly. Chin J Behav Med Brain Sci. (2021):30, 402–407. doi: 10.3760/cma.j.cn371468-20210107-00016
44. Chen, Y, Zhang, Z, Zuo, Q, and Gao, Y. Status quo of reversible cognitive frailty among the elderly in a community of Guangzhou and its influencing factors. Nurs J Chin PLA. (2022):39, 13–16. doi: 10.3969/j.issn.1008-9993.2022.06.004
45. Han, Y, Yuan, M, and Fang, Y. Impact of common chronic diseases on preexisting mild cognitive dysfunction in older adults. Chin J Health Stat. (2019) 36:232–5.
46. Ruan, Q, Xiao, F, Gong, K, Zhang, W, Zhang, M, Ruan, J, et al. Prevalence of cognitive frailty phenotypes and associated factors in a community-dwelling elderly population. J Nutr Health Aging. (2020) 24:172–80. doi: 10.1007/s12603-019-1286-7
47. Xiao, SF, Lewis, M, Mellor, D, McCabe, M, Byrne, L, Wang, T, et al. The China longitudinal ageing study: overview of the demographic, psychosocial and cognitive data of the shanghai sample. J Ment Health. (2016) 25:131–6. doi: 10.3109/09638237.2015.1124385
48. Liew, TM. Depression, subjective cognitive decline, and the risk of neurocognitive disorders. Alzheimers Res Ther. (2019) 11:70. doi: 10.1186/s13195-019-0527-7
49. Brodaty, H, Aerts, L, Crawford, JD, Heffernan, M, Kochan, NA, Reppermund, S, et al. Operationalizing the diagnostic criteria for mild cognitive impairment: the salience of objective measures in predicting incident dementia. Am J Geriatr Psychiatry. (2017) 25:485–97. doi: 10.1016/j.jagp.2016.12.012
50. Tomata, Y, Sugiyama, K, Kaiho, Y, Sugawara, Y, Hozawa, A, and Tsuji, I. Predictive ability of a simple subjective memory complaints scale for incident dementia: evaluation of japan's national checklist, the “kihon checklist”. Geriatr Gerontol Int. (2017) 17:1300–5. doi: 10.1111/ggi.12864
51. Tsutsumimoto, K, Makizako, H, Doi, T, Hotta, R, Nakakubo, S, Makino, K, et al. Subjective memory complaints are associated with incident dementia in cognitively intact older people, but not in those with cognitive impairment: a 24-month prospective cohort study. Am J Geriatr Psychiatry. (2017) 25:607–16. doi: 10.1016/j.jagp.2016.12.008
52. Fulop, T, Larbi, A, Pawelec, G, Khalil, A, Cohen, AA, Hirokawa, K, et al. Immunology of aging: the birth of inflammaging. Clin Rev Allergy Immunol. (2023) 64:109–22. doi: 10.1007/s12016-021-08899-6
53. Franceschi, C, Garagnani, P, Parini, P, Giuliani, C, and Santoro, A. Inflammaging: a new immune-metabolic viewpoint for age-related diseases. Nat Rev Endocrinol. (2018) 14:576–90. doi: 10.1038/s41574-018-0059-4
54. Boots, A, Thomason, ME, Espinoza-Heredia, C, Pruitt, PJ, Damoiseaux, JS, Roseboom, TJ, et al. Sex-specific effects of prenatal undernutrition on resting-state functional connectivity in the human brain at age 68. Neurobiol Aging. (2022) 112:129–38. doi: 10.1016/j.neurobiolaging.2022.01.003
55. Dong, Y. Study on subjective cognitive decline and grip strength and related risk factors in elderly population in community. Anhui: Anhui Medical University (2022).
56. Wen, C, Hu, H, Ou, YN, Bi, YL, Ma, YH, Tan, L, et al. Risk factors for subjective cognitive decline: the cable study. Transl Psychiatry. (2021) 11:576. doi: 10.1038/s41398-021-01711-1
57. Mondini, S, Pucci, V, Montemurro, S, and Rumiati, RI. Protective factors for subjective cognitive decline individuals: trajectories and changes in a longitudinal study with italian elderly. Eur J Neurol. (2022) 29:691–7. doi: 10.1111/ene.15183
58. Meier, C, Vilpert, S, Borrat-Besson, C, Jox, RJ, and Maurer, J. Health literacy among older adults in Switzerland: cross-sectional evidence from a nationally representative population-based observational study. Swiss Med Wkly. (2022) 152:w30158. doi: 10.4414/SMW.2022.w30158
59. Sun, B, Zhao, Y, Lu, W, and Chen, Y. The relationship of malnutrition with cognitive function in the older chinese population: evidence from the chinese longitudinal healthy longevity survey study. Front Aging Neurosci. (2021) 13:13. doi: 10.3389/fnagi.2021.766159
60. Caçador, C, Teixeira-Lemos, E, Martins, SO, and Ramos, F. The role of nutritional status on polypharmacy, cognition, and functional capacity of institutionalized elderly: a systematic review. Nutrients. (2021) 13:3477. doi: 10.3390/nu13103477
61. Jia, L, Du, Y, Chu, L, Zhang, Z, Li, F, Lyu, D, et al. Prevalence, risk factors, and management of dementia and mild cognitive impairment in adults aged 60 years or older in China: a cross-sectional study. Lancet Public Health. (2020) 5:e661–71. doi: 10.1016/S2468-2667(20)30185-7
62. Ma, C, Li, M, and Wu, C. Cognitive function trajectories and factors among chinese older adults with subjective memory decline: charls longitudinal study results (2011-2018). Int J Environ Res Public Health. (2022) 19:19. doi: 10.3390/ijerph192416707
63. Zhang, W, Zhang, Y, and Wang, J. Effect and mechanism of reading habits on physical and mental health among the elderly: evidence from China. Front Public Health. (2022) 10:1031939. doi: 10.3389/fpubh.2022.1031939
64. Yao, Y, Zhang, S, and Li, A. Effects of educational attainment and housing condition on self-rated health in old age: heterogeneity and tendency in China. Front Public Health. (2022) 9:774364. doi: 10.3389/fpubh.2021.774364
Keywords: Chinese, subjective cognitive decline, prevalence, meta-analysis, Alzheimer’s disease
Citation: Xue C, Li J, Hao M, Chen L, Chen Z, Tang Z, Tang H and Fang Q (2023) High prevalence of subjective cognitive decline in older Chinese adults: a systematic review and meta-analysis. Front. Public Health. 11:1277995. doi: 10.3389/fpubh.2023.1277995
Edited by:
Miriam Rodriguez-Monforte, Ramon Llull University, SpainReviewed by:
Xue Lan, China Medical University, ChinaCopyright © 2023 Xue, Li, Hao, Chen, Chen, Tang, Tang and Fang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Juan Li, Njk0ODA3MDU1QHFxLmNvbQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.