 Ángel Ramos-Macías1
Ángel Ramos-Macías1 Leo De Raeve2*
Leo De Raeve2* Meredith Holcomb3
Meredith Holcomb3 Ella Connor4
Ella Connor4 Aiya Taylor5Irene Deltetto4Colman Taylor4,5
Aiya Taylor5Irene Deltetto4Colman Taylor4,5- 1Department of Otolaryngology, School of Medicine, University of Las Palmas, Las Palmas, Spain
- 2Independent Information and Research Centre on Cochlear Implants (ONICI), European Association of Cochlear Implant Users (EURO-CIU) and Cochlear Implant International Community of Action (CIICA), Zonhoven, Belgium
- 3Department of Otolaryngology, University of Miami Miller, School of Medicine, Miami, FL, United States
- 4HTANALYSTS, Sydney, NSW, Australia
- 5Critical Care, The George Institute for Global Health, Sydney, NSW, Australia
Introduction: Clinical guidelines for cochlear implants (CI) exist in several countries, however, they lack consistency and often do not encompass the full user journey. This study aims to explore the barriers and facilitators for implementing global Living Guidelines for cochlear implantation in adults with severe, profound or moderate sloping to profound sensorineural hearing loss (SPSNHL) as well as identify guideline implementation (GI) tools that may support uptake.
Methods: A convenience sample of Task Force members were recruited for semi-structured interviews. Interview transcripts were thematically analysed to group country-specific barriers, facilitators and GI tools into three levels: health care provider (HCP), consumer and structural. Once identified, barriers and facilitators were classified into four themes related to awareness, economic, guideline or other.
Results: Interviews were conducted with 38 Task Force members, representing 20 countries. Lack of CI and hearing loss awareness was a major barrier at the HCP (85% of countries), consumer (80%) and structural (20%) levels. Economic and guideline barriers followed at the HCP (35%; 25%), consumer (45%; 0%) and structural (55%; 30%) levels, respectively. Facilitators focused on raising awareness of hearing loss and CIs as well as guideline related initiates at the HCP (80%; 70%), consumer (70%; 10%) and structural (25%; 70%) levels. GI tools including education, economic evaluations, quick reference resources and social media can help improve awareness and uptake.
Conclusion: Awareness is the primary barrier to implementing Living Guidelines globally for adults with SPSNHL. Endorsement from key professional bodies and using the best available evidence can enhance uptake.
1 Introduction
Hearing loss is one of the most prevalent and undertreated disabilities worldwide (1). Despite cochlear implants (CIs) being a safe and effective treatment option for adults with severe, profound or moderate sloping to profound sensorineural hearing loss (SPSNHL) (2), it is estimated that at best only one in 20 adults who would benefit from a CI have received one (2–4).
In 2020, an international group of clinical hearing loss experts highlighted that while cochlear implantation should be standard of care in adults with SPSNHL, it is underutilized as a treatment option, suggesting there is an urgent need to address the lack of globally consistent CI guidelines (2, 5).
Currently, some countries have detailed guidelines with varying levels of uptake for candidacy requirements [United states (US)] (2, 6), pre-operative evaluation (Australia, Germany, France, Spain, US) (6–12), CI surgery (Australia, England, Germany, France, Spain, US) (6–10, 13–16), and post-operative care (Australia, Germany, US) (6–8, 11, 12). However, holistic international guidelines on adult CI treatment are limited (2).
Therefore, in 2022, an independent global CI Task Force was established to guide the development of new global ‘Living’ Guidelines for CI in adults with SPSNHL, with the aim to improve the standard of care for these individuals and provide guidance on treatment options. The concept of living guidelines is a new approach to driving evidence-based practice, and will ensure that recommendations within the Living Guidelines are always underpinned by a rigorous evidence base and remain relevant within a continuously evolving field of research (17).
Once published in early 2023, the Living Guidelines will be implemented in multiple countries. Although, numerous studies emphasize challenges with translating recommendations from clinical guidelines into practice, suggesting they require adaptation and adoption at micro- (e.g., patients and clinicians), meso- (e.g., the healthcare system) or macro- (e.g., government and regulation) environments (18).
Thus, the primary objective of this study was to explore the barriers and facilitators for successful implementation of the Living Guidelines, and to understand what guideline implementation (GI) tools will be required to support uptake.
2 Methods
2.1 Study design
The global CI Task Force comprised of 52 Task Force members, including 30 Ear, Nose and Throat Specialists (ENTs), 16 audiologists, 4 cochlear impact users and 2 hearing specialists (one ENT and one audiologist) who are also users. Three co-chairs were appointed to lead the CI Task Force, who represented each stakeholder group at a leadership level (one ENT, one audiologist and one user). The members of the CI Task Force were selected and recommended by peers to ensure a balance of global geographical location, gender and expertise.
All Task Force members were invited to participate in semi-structured interviews. Task Force members were contacted via email in September 2022 and one-on-one interviews were conducted remotely in October 2022. Participants provided both written and verbal consent prior to commencing their interview.
2.2 Sampling and recruitment
The study recruited a convenience sample of members from the Task Force. Overall, 38 Task Force members from 20 countries consented to be interviewed and this sample size was expected to be sufficient to meet the project objectives. The overall response rate was 73%, ranging from 67% (Latin America) to 80% (Asia-Pacific) (please see Supplementary Table 1).
2.3 Data collection
Interviews were conducted remotely by two investigators (AT, EC) who had minimal prior experience conducting research on hearing loss and CI care. Thus, researchers had minimal existing biases, which allowed themes to emerge naturally. Interviews lasted approximately 1 h and were audio-recorded and transcribed verbatim.
2.4 Data analysis
Three investigators (ID, AT, EC) categorized barriers and facilitators into three levels: health care provider (HCP) (audiologists, otolaryngologists), consumer (CI users, families) and structural (the healthcare system). This methodology was considered appropriate, as these categories related to the interview questions (please see Supplementary Appendix A). Following this analysis, two researchers (AT, EC) further grouped themes into four categories including awareness (related to the knowledge of hearing loss and CIs in each county), economic (related to the economic environment, laws and regulations), guideline specific (related to the actual implementation of the Living Guidelines) and other (additional barriers and facilitators).
To analyse the results, the proportion of countries (N = 20) that reported an individual barrier and facilitator within each of these pre-defined levels and categories were calculated. When multiple participants from the same country reported a barrier or facilitator, this was considered to be one vote for the respective barrier or facilitator category.
GI tools were also grouped according to the HCP, consumer and structural levels, to facilitate these being mapped to the barriers and facilitators identified. The results were presented according to the proportion of countries (N = 20) that recommended each category of GI tool.
2.5 Ethics
Ethics approval was granted by the Bellberry Human Research Ethics Committee (No. 2022 06656).
3 Results
3.1 Barriers and facilitators
The proportion of countries that reported barriers and facilitators in each category is summarized in Table 1. Overall, a total of 28 barriers and 28 facilitators were identified across all levels, presented in Tables 2, 3, respectively.
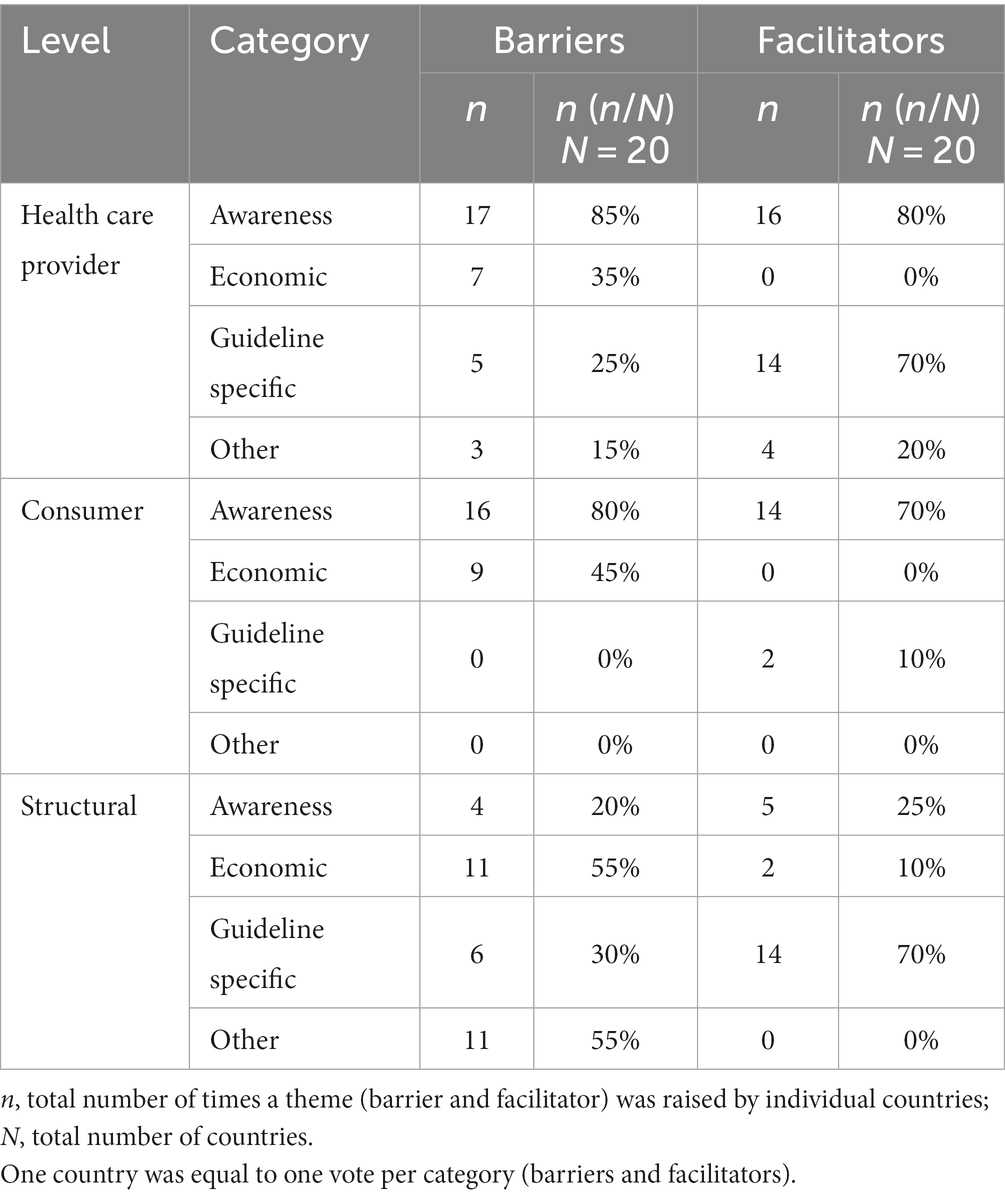
Table 1. Summary of themes (barriers and facilitators) identified by countries at health care provider, consumer and structural levels.
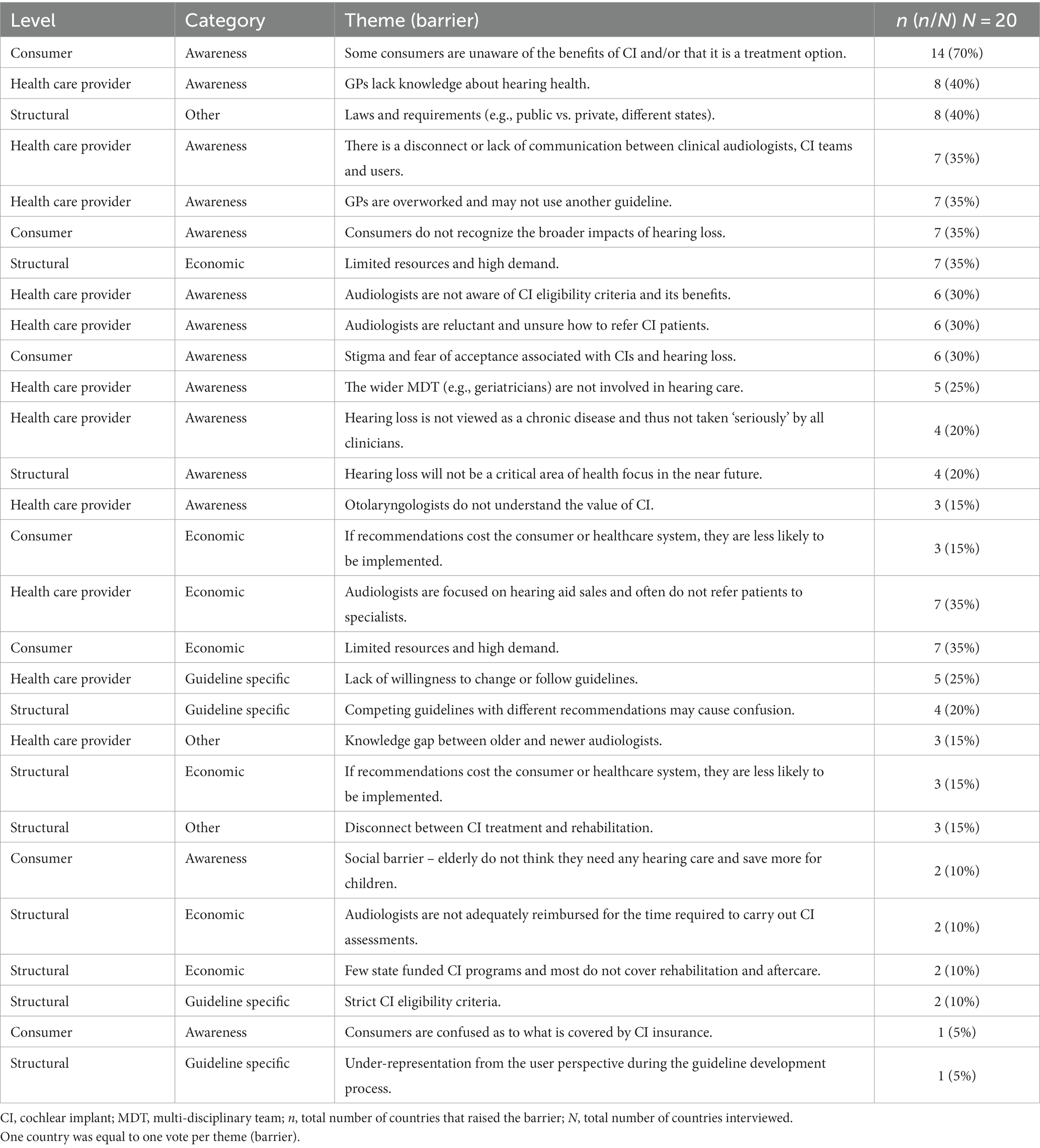
Table 2. Themes (barriers) reported by countries influencing implementation of the Living Guidelines at health care provider, consumer and structural levels.
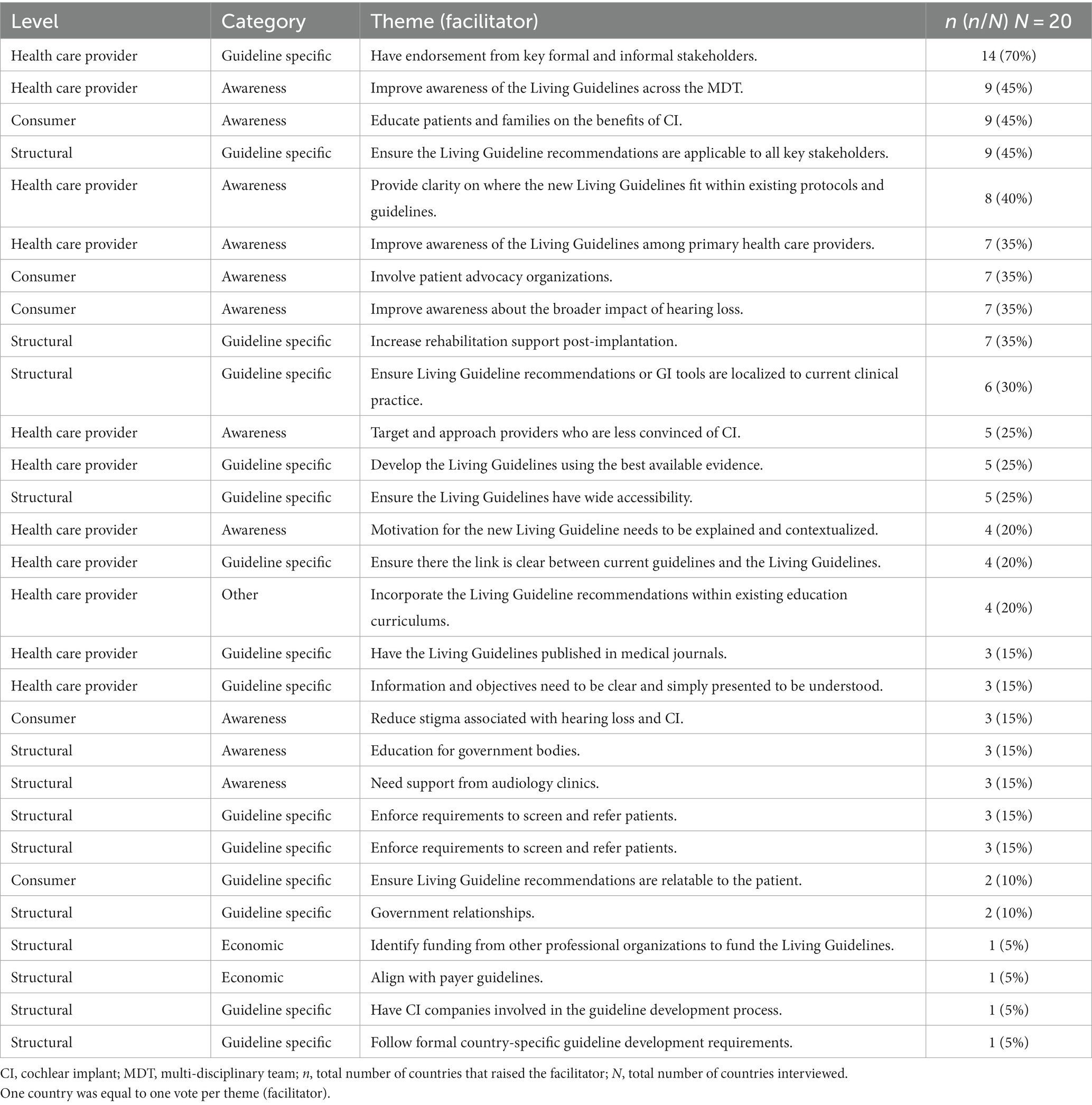
Table 3. Themes (facilitators) reported by countries influencing implementation of the Living Guidelines at health care provider, consumer and structural levels.
3.1.1 Health care provider
Awareness was identified as the largest HCP barrier (85%) that could impact the successful adoption of the Living Guidelines (Table 1). Frequently reported themes included a lack of general practitioner (GP) (40%) and audiologist (30%) knowledge about hearing health or the value of CIs, and a disconnect or lack of communication between primary HCPs, audiologists and otolaryngologists (35%) (Table 2). Additionally, the largest economic barrier was a lack of referrals from audiologists (35%), and the largest guideline specific barrier was a lack of willingness to change practice or follow guidelines (25%) (Table 2).
“Awareness is key. I've been doing this for years and every day I'm surprised by how many GPs and audiologists don't know about cochlear implants (CIs).” – Task Force member, Canada
“I think one of the biggest issues is that lots of people do not realise that they do better with a CI than they would do with hearing aids.” – Task Force member, Australia
Most countries (80%) reported improving awareness as the most important facilitator for HCPs (Table 1). Specifically, improving awareness of the Living Guidelines across the multi-disciplinary team (MDT) (45%) and primary HCPs (35%) (Table 3). Furthermore, providing clarification on how the Living Guidelines align with existing national protocols or guidelines (40%) and having them endorsed by key professional bodies (70%) were the common guideline specific facilitators reported (Table 3). Others included using the best available evidence (25%) to develop recommendations and ensuring there is a clear link between current guidelines and the Living Guidelines (20%) (Table 3).
“A global standard for treatment for hearing loss would go a long way in helping patients.” – Task Force member, United States of America
3.1.2 Consumer
Awareness was identified as a major consumer barrier (80%) (Table 1). This included a lack of awareness of the potential benefits of CIs (70%) and hearing loss consequences (35%), as well as the associated stigma and fear of acceptance (30%) (Table 2). Approximately half of the participating countries (45%) (Table 1) reported economic barriers associated with the cost of CIs (40%) and travel required for care (30%) (Table 2).
Improving consumer awareness was seen as a critical facilitator in most countries (70%) (Table 1). Specific awareness facilitators related to educating (45%) and improving awareness (35%) about the broader impacts of hearing loss and the value of CIs (Table 3). Furthermore, involving patient advocacy organizations during implementation was also considered essential (35%) (Table 3).
“The biggest thing is to make sure we (users) have access to the information” – Task Force member, Australia
3.1.3 Structural
Economic (55%) and other barriers (55%) were the most frequently reported for the structural level (Table 1). For instance, having limited resources to meet patient demand (35%) and the laws and regulations across healthcare systems (40%) (Table 2).
“The economics of hearing care do not incentivise providers to offer cochlear implants because every time a private practice audiologist or hearing instrument specialist offers an implant, they're offering to give away a patient.” – Task Force member, United States of America
Regarding structural facilitators, most suggestions related to the content of the Living Guidelines (70%) (Table 1). This included ensuring the recommendations will be applicable to all key stakeholders (45%) and increasing rehabilitation support services (35%) (Table 3).
3.2 Guideline implementation tools
The proportion of countries that identified GI tools for each level is summarized in Table 4. Overall, 42 different GI tools were recommended to support implementation and uptake of the Living Guidelines (see Supplementary Appendix B).
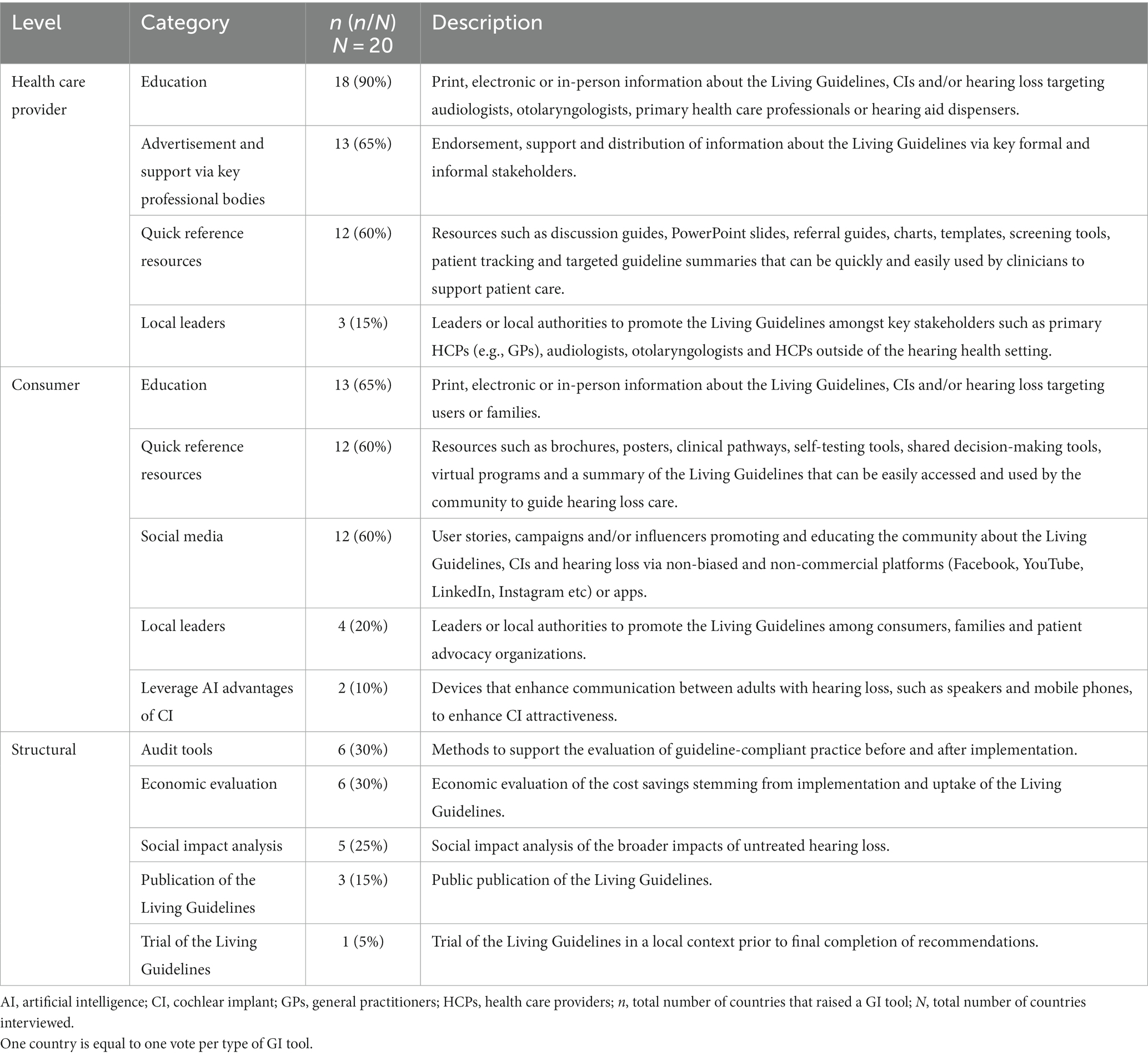
Table 4. Summary of themes (GI tools) identified by countries at health care provider, consumer and structural level.
3.2.1 Health care provider
Eighteen GI tools were recommended to support HCPs (Appendix B). Overall, education (90%), advertisement or support by key professional bodies (65%) and quick reference resources (60%) were the most frequently reported (Table 4).
“It is important to get endorsement from all of the professional groups who already create these kinds of document.” – Task Force member, Sweden
3.2.2 Consumer
Nineteen GI tools were recommended to support consumers (Appendix B). Education (65%), social media (60%) and quick reference resources (60%) were the most commonly nominated (Table 4).
“We need to build "pro-tools”, which are built from the ground up, built from the recipients, from patients, from people. This is going to be the most important thing. – Task Force member, United States of America
3.2.3 Structural
Five GI tools were recommended to support implementation at the structural level (Appendix B). An audit tool (30%), economic evaluation (20%) and social impact analysis (25%) were the most frequently suggested (Table 4).
“There must be an audit or evaluation tool. It is important to monitor the impact of these guidelines - take up rates, influence, impact”– Task Force member, India
4 Discussion
In this convenience sample of representatives from the CI Task Force, we identified several barriers, facilitators and GI tools related to the successful implementation of the Living Guidelines globally. Awareness of CIs and the impact of hearing loss were identified as major barriers across the HCP, consumer and structural levels. This was followed by economic barriers, such as out-of-pocket costs, and barriers related to the Living Guidelines, such as under-representation of CI users in guideline development. Facilitators mainly focused on increasing awareness of CIs and the impact of hearing loss as well as guideline related initiatives, such as gaining endorsement from key professional bodies. Finally, education, economic evaluations and ‘wrap-around tools’ including quick reference resources and social media campaigns were nominated to facilitate uptake.
To ensure this is successful, our findings demonstrate that the lack of GP, audiologist and consumer awareness must be addressed. These results are consistent with implementation research previously conducted in other healthcare areas that also identified a lack of HCP knowledge and time as significant barriers (18–21). For this to be addressed, CI specialists must receive appropriate training and education on the Living Guideline recommendations to ensure key stakeholders in their countries understand how they align with current clinical practice. Furthermore, gaining endorsement from these stakeholders will be a critical step to ensuring rapid uptake.
Additionally, educating non-CI specialists — including GPs, audiologists not CI trained, otolaryngologists who do not perform CI surgeries and hearing aid dispensers — about hearing health and CI benefits is crucial. These clinicians are commonly the first point of contact for potential CI candidates. Thus, enhancing their knowledge is important for improving CI referrals and patient management. This can be supported with quick reference resources, such as a lay summary of the Living Guideline recommendations. Improving knowledge, motivation and sense of responsibility among GPs have previously been identified in literature as influential facilitators for greater compliance of guidelines (22).
Increasing primary HCPs awareness will ultimately address knowledge concerns at a consumer level, by improving access to information. This may reduce the stigma related to CIs and empower adults with hearing loss to be involved in their treatment decisions, especially if supported by social media and quick reference resources. Specifically, a tool able to drive demand for a hearing assessment or intervention should be developed, using lay language to ensure equity and inclusion. Our results encourage the development of such resources to improve universal awareness about the broader consequences of untreated hearing loss such as depression, dementia, diabetes or heart disease (2, 23). Globally, it was suggested that this is not well understood and is thus a key facilitator to ensure successful adoption.
Our findings address several gaps in the literature regarding implementation strategies, as majority of existing GI tools target clinicians (52%) rather than patients (24%), implementation (14%) or evaluation (10%) (24). Furthermore, the importance of evaluating the uptake of guidelines is consistently recognized in literature (24, 25), but performing economic and social impact analyses are newly identified tools to our knowledge.
4.1 Strengths and limitations
Worldwide, this research is the first to examine living guideline implementation strategies for adults with SPSNHL, which is a key strength. Additionally, the inclusion of expert and influential audiologists, otolaryngologists and CI users, who represented a diverse range of developed and developing countries, may enhance the transferability of research findings.
However, some limitations may impact the interpretation and application. First, recruitment was restricted to the Task Force, which included a relatively small proportion of CI users, and excluded GPs and HCPs outside of the hearing health setting. Therefore, it is possible that important barriers, facilitators or GI tools may have been overlooked. Second, all findings are based on expert opinion from top leaders in the field and are not supported by evidence-based data. Third, some of the structural barriers identified, such as country-specific laws or CI cost and reimbursement, will be difficult to address without significant reform. Fourth, several Task Force members from African countries were unavailable to participate, and therefore this study was not representative of the global population.
Furthermore, it is important to acknowledge that inherent biases to specialist observations may be present in the results, as the reasons provided and presumed countermeasures are based on consensus, rather than scientific exploration of root causes. However, there is value in using these assessments as a starting point, recognizing that successful adoption of future living guidelines will need to be monitored, and plans adjusted based on observation and data.
5 Conclusion
This study emphasizes the importance of utilizing GI implementation tools to ensure the successful implementation and widespread adoption of the Living Guidelines, based on expert opinion. In particular, findings indicate that addressing the limited awareness of hearing loss and CIs worldwide, as well as economic barriers such as referral channels and out-of-pocket costs, are key to achieving this goal. Although, many practical steps can be undertaken to assist implementation including endorsement by professional bodies and ensuring the recommendations adhere to the best available evidence. Supporting these with economic evaluations, quick reference resources and social media campaigns could help facilitate uptake of the Living Guidelines in individual countries.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Bellberry Human Research Ethics Committee. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
ÁR-M: Validation, Writing – review & editing. LR: Validation, Writing – review & editing. MH: Validation, Writing – review & editing. EC: —. AT: Writing – review & editing. ID: Writing – review & editing. CT: Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. The study received funding from Cochlear Limited. The funder was not involved in the study design, collection, analysis, interpretation of data, the writing of this article or the decision to submit it for publication.
Acknowledgments
The authors thank members of the Cochlear Implant Task Force who contributed to the activities.
Conflict of interest
MH is an Associate Professor and the Director of the Hearing Implant Program at the University of Miami Department of Otolaryngology. She has received grants, contracts, support for attending meetings and/or consulting fees from Cochlear Limited and Med-EL Limited, Advanced Bionics, Hemeideina and Institute for Cochlear Implant Training. LR is the director of ONICI, President of FEAPDA (European Federation of Teachers of the Deaf), chair of CIICA (Cochlear Implant International Community of Action). He has received support (accommodation and travel) from Cochlear to present content of Living Guidelines project for multiple conferences. AMR is a Professor at the Department of Otolaryngology, and Head and Neck Surgery, AT, ID, and CT are employed by HTANALYSTS, which through an unrestricted grant supported the Living Guidelines project by Cochlear Limited and in accordance with Good Publications Practice 2022 Guidelines.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2023.1272437/full#supplementary-material
Abbreviations
ADA, Academy of Doctors of Audiology; AQC, Audiology Quality Consortium; AT, Analysis, two; CI, Cochlear implant; CIICA, Cochlear Implant International Community of Action; ENT, Ear, Nose and Throat; GI, Guideline implementation; GP, General practitioner; HCP, Health care provider; MAA, Maryland Academy of Audiology; MDT, Multi-disciplinary team; SPSNHL, Sloping to profound sensorineural hearing loss.
References
1. Wilson, BS, Tucci, DL, Merson, MH, and O'Donoghue, GM. Global hearing health care: new findings and perspectives. Lancet. (2017) 390:2503–15. doi: 10.1016/S0140-6736(17)31073-5
2. Buchman, CA, Gifford, RH, Haynes, DS, Lenarz, T, O'Donoghue, G, Adunka, O, et al. Unilateral Cochlear implants for severe, profound, or moderate sloping to profound bilateral sensorineural hearing loss: a systematic review and consensus statements. JAMA Otolaryngol Head Neck Surg. (2020) 146:942–53. doi: 10.1001/jamaoto.2020.0998
3. Sorkin, DL. Access to cochlear implantation. Cochlear Implants Int. (2013) 14:S1. doi: 10.1179/1467010013Z.00000000081
4. Nassiri, AM, Sorkin, DL, and Carlson, ML. Current estimates of Cochlear implant utilization in the United States. Otol Neurotol. (2022) 43:e558–62. doi: 10.1097/MAO.0000000000003513
5. Loth, A, Vazzana, C, Leinung, M, Guderian, D, Issing, C, Baumann, U, et al. Quality control in cochlear implant therapy: clinical practice guidelines and registries in European countries. Eur Arch Otorhinolaryngol. (2022) 279:4779–86. doi: 10.1007/s00405-022-07263-4
6. American Academy of Audiology. Clinical practice guidelines: Cochlear implants (2019) Available at: https://www.audiology.org/wp-content/uploads/2021/05/CochlearImplantPracticeGuidelines.pdf.
7. Department of Health WA. Clinical guidelines for adult Cochlear implantation (2011) Available at: https://adulthearing.com/wp-content/uploads/2020/11/Govt-of-Western-Australia-Clinical-Guidelines-for-Adult-Cochlear-Implantation-2013.pdf.
8. German Society of Oto-Rhino-Laryngology Head and Neck Surgery. Whitebook, Cochlear implant (CI) fitting (2018) Available at: https://cdn.hno.org/media/PDF/ci-weissbuch-und-register-dghno-1-auflage-stand-04-2018.pdf.
9. De Sante, Haute Autorite. Development of good practice guidelines (2016). Available at: https://www.has-sante.fr/upload/docs/application/pdf/2018-02/good_practice_guidelines_cpg_method.pdf.
10. Manrique, M, Ramos, Á, de Paula, VC, Gil-Carcedo, E, Lassaletta, L, Sanchez-Cuadrado, I, et al. Guideline on cochlear implants. Acta Otorrinolaringol Esp (Engl Ed). (2019) 70:47–54. doi: 10.1016/j.otorri.2017.10.007
11. Turton, L, Souza, P, Thibodeau, L, Hickson, L, Gifford, R, Bird, J, et al. Guidelines for best practice in the audiological Management of Adults with severe and profound hearing loss. Semin Hear. (2020) 41:141–246. doi: 10.1055/s-0040-1714744
12. Holder, JT, Holcomb, MA, Snapp, H, Labadie, RF, Vroegop, J, Rocca, C, et al. Guidelines for best practice in the audiological Management of Adults Using Bimodal Hearing Configurations. Otol Neurotol Open. (2022) 2:e011. doi: 10.1097/ONO.0000000000000011
13. National Institute for Health and Care Excellence. Hearing loss in adults: Assessment and management (2018). Available at: https://www.nice.org.uk/guidance/ng98/resources/hearing-loss-in-adults-assessment-and-management-pdf-1837761878725.
14. National Institute for Health and Care Excellence. Cochlear implants for children and adults with severe to profound deafness (2019) Available at: https://www.nice.org.uk/guidance/ta566/resources/cochlear-implants-for-children-and-adults-with-severe-to-profound-deafness-pdf-82607085698245.
15. British Society of Hearing Aid Audiologists. Referral guidelines for HCPC registered hearing aid dispensers (2017). Available at: https://bshaa.org/wp-content/uploads/2020/05/BSHAA_Guidance_For_Further_Referral_In_Audiology_Clinic_-_Jan_2018.pdf.
16. Britich Cochlear Implant Group. Quality standards Cochlear implant Services for Children and Adults (2018) Available at: https://www.bcig.org.uk/wp-content/uploads/2018/05/QS-update-2018-PDF-final.pdf.
17. Corias, G, Deltetto, I, and Taylor, A. Improving the standard of care for adults with hearing loss and the role of cochlear implantation: a systematic review of the evidence to develop clinical practice guidelines; (2022) Available at: https://www.crd.york.ac.uk/prospero/display_record.php?RecordID=325393.
18. Correa, VC, Lugo-Agudelo, LH, Aguirre-Acevedo, DC, Contreras, JAP, Borrero, AMP, Patiño-Lugo, DF, et al. Individual, health system, and contextual barriers and facilitators for the implementation of clinical practice guidelines: a systematic metareview. Health Res Policy Syst. (2020) 18:74. doi: 10.1186/s12961-020-00588-8
19. McArthur, C, Bai, Y, Hewston, P, Giangregorio, L, Straus, S, and Papaioannou, A. Barriers and facilitators to implementing evidence-based guidelines in long-term care: a qualitative evidence synthesis. Implement Sci. (2021) 16:70. doi: 10.1186/s13012-021-01140-0
20. Légaré, F, Ratté, S, Gravel, K, and Graham, ID. Barriers and facilitators to implementing shared decision-making in clinical practice: update of a systematic review of health professionals’ perceptions. Patient Educ Couns. (2008) 73:526–35. doi: 10.1016/j.pec.2008.07.018
21. Carlson, ML, Nassiri, AM, Marinelli, JP, Lohse, CM, and Sydlowski, SA. Awareness, perceptions, and literacy surrounding hearing loss and hearing rehabilitation among the adult population in the United States. Otol Neurotol. (2022) 43:e323–30. doi: 10.1097/MAO.0000000000003473
22. Goderis, G, Borgermans, L, Mathieu, C, Van Den Broeke, C, Hannes, K, Heyrman, J, et al. Barriers and facilitators to evidence based care of type 2 diabetes patients: experiences of general practitioners participating to a quality improvement program. Implement Sci. (2009) 4:41. doi: 10.1186/1748-5908-4-41
23. American Academy of Audiology. Heart disease and hearing loss (n.d.) Available at: https://www.audiology.org/consumers-and-patients/hearing-and-balance/heart-disease-and-hearing-loss/#2
24. Liang, L, Abi Safi, J, and Gagliardi, AR. Members of the guidelines international network implementation working G. Number and type of guideline implementation tools varies by guideline, clinical condition, country of origin, and type of developer organization: content analysis of guidelines. Implement Sci. (2017) 12:136. doi: 10.1186/s13012-017-0668-7
Keywords: living guidelines, cochlear implantation, hearing loss, guideline implementation strategies, guideline implementation tools
Citation: Ramos-Macías &, De Raeve L, Holcomb M, Connor E, Taylor A, Deltetto I and Taylor C (2023) Strategies for the implementation of the living guidelines for cochlear implantation in adults. Front. Public Health. 11:1272437. doi: 10.3389/fpubh.2023.1272437
Edited by:
Christiane Stock, Charité – Universitätsmedizin Berlin, GermanyReviewed by:
Paul Merkus, Amsterdam University Medical Center, NetherlandsRichard Charles Dowell, The University of Melbourne, Australia
Copyright © 2023 Ramos-Macías, De Raeve, Holcomb, Connor, Taylor, Deltetto and Taylor. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Leo De Raeve, bGVvLmRlLnJhZXZlQG9uaWNpLmJl