 Qian Li1†
Qian Li1† Zheng Guo2†
Zheng Guo2† Fangli Hu3†
Fangli Hu3† Mengfei Xiao1†
Mengfei Xiao1† Qiang Zhang4
Qiang Zhang4 Jun Wen5Tianyu Ying6Danni Zheng7
Jun Wen5Tianyu Ying6Danni Zheng7 Youxin Wang8
Youxin Wang8 Song Yang9*
Song Yang9* Haifeng Hou1
Haifeng Hou1- 1School of Public Health, Shandong First Medical University and Shandong Academy of Medical Sciences, Jinan, China
- 2Division of Epidemiology, Department of Medicine, Vanderbilt Epidemiology Center, Vanderbilt-Ingram Cancer Center, Vanderbilt University Medical Center, Nashville, TN, United States
- 3Centre for Precision Health, Edith Cowan University, Joondalup, WA, Australia
- 4Department of Thoracic Surgery, The Second Affiliated Hospital of Shandong First Medical University, Taian, China
- 5School of Business and Law, Edith Cowan University, Joondalup, WA, Australia
- 6Department of Tourism and Hotel Management, Zhejiang University, Hangzhou, China
- 7Department of Tourism, Fudan University, Shanghai, China
- 8Beijing Key Laboratory of Clinical Epidemiology, School of Public Health, Capital Medical University, Beijing, China
- 9Department of Endocrinology, The Affiliated Taian City Central Hospital of Qingdao University, Taian, China
Background: Given the etiological complexity of cognitive impairment, no effective cure currently exists for precise treatment of dementia. Although scholars have noted tourism’s potential role in managing cognitive impairment and mild dementia, more robust empirical investigation is needed in this area. This study aimed to examine the associations between tourism and cognitive impairment and dementia in older Chinese adults.
Method: From a nationwide community-based cohort, 6,717 individuals aged ≥60 were recruited from 2011 to 2014, of whom 669 (9.96%) had had at least one tourism experience in the 2 years prior to enrollment. All the participants were then prospectively followed up until 2018. The association between tourism and cognitive impairment was examined by the Cox proportional hazards regression model. The adjusted hazard ratio (aHR) and its 95% confidence interval (CI) were calculated to evaluate the effect of tourism experience on cognitive impairment and dementia.
Results: A total of 1,416 individuals were newly diagnosed with cognitive impairment and 139 individuals with dementia onset during follow-up. The incidence of cognitive impairment was significantly lower among participants with tourism experiences (316.94 per 10,000 person-years) than those without such experiences (552.38 per 10,000 person-years). Cox regression showed that tourism decreased the risk of cognitive impairment (aHR = 0.69, 95% CI: 0.41–0.62) when adjusted for behavioral covariates and characteristics. Compared with participants without tourism experiences, those with 1, 2, and ≥3 tourism experiences had a lower risk of cognitive impairment with the aHRs of 0.72 (95% CI: 0.52–0.99), 0.65 (0.42–1.01), and 0.68 (0.44–0.98), respectively. Tourism experiences also reduced participants’ risk of dementia (aHR = 0.41, 95% CI: 0.19–0.89).
Conclusion: Our findings demonstrated associations between tourism and reduced risks of cognitive impairment and dementia in older Chinese adults. Thus, tourism could serve as a novel approach to dementia prevention.
Introduction
Cognitive impairment is characterized by declines in language, attention, and other cognitive functions, most notably memory (1, 2). Cognitive impairment and dementia represent major public health challenges: over 55 million people are living with dementia worldwide, with this figure expected to rise to 78 million by 2030 (3). The incidence of dementia in China was 788.3 per 100,000 people in 2019, exceeding the global rate (682.5 per 100,000) (4). Approximately one-quarter of people with dementia live in China (5). The country’s older adult population is growing as people live longer: China was home to 254 million people above age 60 and 176 million people above age 65 in 2019, representing 17.2 and 12.6% of the general population, respectively (6, 7). Cognitive impairment and dementia, which are common among older adults, thus continue to place increasingly heavy burdens on society.
Cognitive impairment can accompany Alzheimer’s disease, neurological injuries, psychiatric conditions, Parkinson’s disease, and genetic factors, among other causes (8, 9). Given their etiological complexity, no cure currently exists for cognitive impairment and dementia. Approved medications have limited efficacy and substantial side effects (10, 11). Psychosocial and other non-pharmacological therapies (e.g., physical exercise, music therapy, dance movement therapy, nostalgia, and game-based interventions) (12) are preferred to alleviate symptoms (13–16). Of these, recreational therapy has been widely recognized as a useful intervention for people with cognitive decline and dementia (17–19): leisure activities may reduce the risk of cognitive decline and dementia in later life in addition to relieving behavioral and psychological symptoms of dementia (20–23). Tourism, one of the most popular leisure and vacation activities of the 21st century, could offer a way to minimize or even prevent the negative effects of cognitive impairment and dementia on individuals’ health and quality of life (24). However, empirical research on this therapeutic potential is scarce.
Tourism encompasses “the activities of persons traveling to and staying in places outside their usual environment for not more than one consecutive year for leisure, business, and other purposes not related to the exercise of an activity remunerated from within the place visited” (25). Although this domain appears far removed from medical science, the two disciplines are in fact related. Travelers’ inherent mobility facilitates the transmission of infectious diseases and exacerbates public health crises. For instance, the COVID-19 pandemic dealt a devastating blow to the tourism and hospitality industry. Tourism can also play a role in responding to public health priorities (e.g., non-communicable disease epidemics and healthy aging) by enhancing people’s well-being and quality of life (26, 27). As a part of healthy lifestyles, tourism can improve individuals’ physical and mental health through physical activity, social engagement, and positive emotions, potentially contributing to disease prevention and treatment. Tourism is a positive experience, presenting the experiences of relaxing, social interaction, increasing physical activity, seeking knowledge, promoting learning, experiencing different cultures, and escaping routines (28, 29), these activities could energize brain, boost mental health and maintain positive emotion, which are beneficial for cognitive function (30).
Positive tourism experiences may serve as a promising non-pharmacological therapy for multiple populations, such as healthy people, those in suboptimal health, and vulnerable populations with chronic conditions (31, 32). Amid growth in vulnerable groups and their experienced inequities (e.g., stigma, discrimination, exclusion), there is a pressing need for high-quality interdisciplinary research that integrates tourism and medical science. The neglected public health value of tourism can provide a unique perspective on managing cognitive impairment and dementia (33).
Recognition of the benefit of tourism on well-being elevates the demand of older adults for tourism when they tend to have more free time (34). Compared with the younger people, the old people are more actively involved in travel (35). Studies have suggested that active participation in tourism promotes the health condition and longevity of the older adult (36). In details, old tourists have better self-perceived physical and mental health, and better capacity to carry out instrumental activities in daily life than those without tourism experiences (37).
However, there were no studies evidencing the effects of tourism on dementia or cognitive impairment in older adults. Hereby, this study aimed to examine the associations between tourism and cognitive impairment and dementia in older Chinese adults.
Methods
Study participants and follow-up
The Chinese Longitudinal Healthy Longevity Survey (CLHLS) is a nationwide longitudinal cohort study that included older adults from 631 cities across 22 provinces in China between 1998 and 2018 (38). Our study initially enrolled 9,765 participants recruited in 2011 and 1,126 recruited in 2014, who were prospectively followed until 2018. The survey was administered as a face-to-face interview in each participant’s home with assistance from family members, neighbors, or nursing home staff. Several inclusion criteria applied: (1) tourism data available at baseline, (2) no severe somatic or psychological diseases, (3) aged 60 years and above, and (4) normal cognitive function. The following persons were excluded: individuals with (1) cognitive impairment or dementia at baseline, (2) physical disabilities, or (3) other severe somatic or psychological diseases. Data from 6,717 participants were ultimately retained for analysis. All participants were followed from enrollment until 2018. Within this sample, 1,060 participants died and 541 were lost to follow-up from enrollment to the year 2014 when face-to-face interviews were held. During the second stage of follow-up (i.e., 2014–2018), 774 deaths and 849 losses to follow-up were identified before the final visit in 2018. A flow chart depicting the participant selection process appears in Figure 1.

Figure 1. Flowchart of the inclusion of participants.
Measurements
Tourism experiences
Information on tourism experiences was obtained at baseline and follow-up using the question “How many times have you traveled outside your home county/city within the past 2 years?.” To investigate the effects of tourism experiences on the incidence of cognitive impairment and dementia, participants were divided into two groups: (1) a tourism group (individuals with at least one tourism experience) and (2) a control group (individuals without tourism experience) (39). In the dose–response analysis, participants with tourism experiences were further classified into three groups: (1) one tourism experience, (2) two tourism experiences, and (3) three or more tourism experiences.
Cognitive impairment and dementia
The primary outcome of interest in this cohort study was the onset of cognitive impairment. Cognitive function was measured with the Chinese version of the Mini-Mental State Examination (CMMSE), a modified version of the original MMSE. Considering participants’ low literacy rates, the CMMSE was adapted for comprehensibility (38, 40–42). CMMSE score ≥ 25 was considered as normal cognitive function; those with the score ≤ 24 were with cognitive impairment (41). The severity of cognitive impairment was graded as either mild (18 ≤ CMMSE ≤ 24), moderate (10 ≤ CMMSE ≤ 17), or severe (0 ≤ CMMSE ≤ 9) (43, 44). The secondary outcome of interest was dementia onset. Related information was acquired by referring to participants’ clinical diagnostic reports or disease history.
Demographic and socioeconomic characteristics.
Participants’ baseline data included the following: (1) demographics: age, gender, body mass index (BMI), and education level; (2) family/social support: marital status, residence, and living pattern; (3) socioeconomic status: economic status, annual household income; (4) lifestyle and habits: smoking, alcohol consumption, regular physical exercise, sleep quality, and hours of sleep per day.
Statistical analysis
Normally distributed continuous variables were reported as means and standard deviations, and between-group differences were identified using a student’s t test or one-way analysis of variance. Non-normally distributed parameters were listed as a median with interquartile range [P25–P75] and compared using non-parametric tests. Categorical variables were assessed via chi-square tests. The incidence rates of cognitive impairment and dementia were estimated using the Kaplan–Meier methodology. Moreover, the log-rank test was conducted to identify the difference of survival time between the groups with and without tourism experiences. The Cox proportional hazards model was employed to evaluate the associations between tourism and the incidence of cognitive impairment and dementia, through which hazard ratios (HRs) and their 95% confidence intervals (CIs) were computed. A sensitivity analysis was performed to test the robustness of our estimation by fitting the results to three models: a univariate model (Model 1); a model adjusted for demographics (i.e., age, gender, education level, residence, marital status, and living pattern; Model 2); and a model with further demographic adjustments (i.e., smoking, alcohol consumption, regular physical exercise, BMI, economic status, annual household income, sleep quality, and sleep duration; Model 3) (7). Subgroup analyses were carried out according to participants’ age, gender, marital status, education level, residence, living pattern, smoking, alcohol consumption, regular physical exercise, BMI, sleep quality, sleep duration, economic status, and annual household income. We also explored each interaction between the above factors and tourism experiences in Model 3. All statistical analyses were completed in R Studio (version 4.1.0, R Project for Statistical Computing) and SPSS 26.0 (IBM Corporation, NY, United States). A two-sided p value < 0.05 was considered statistically significant.
Results
Participants’ baseline characteristics
A total of 6,717 participants (mean age: 81.77 years; 3,125 females, 3,592 males) were included in this study, of whom 669 (9.96%) had had at least one tourism experience in the 2 years prior to enrollment. Participants’ baseline characteristics are listed in Table 1. Nearly half (46.79%) of participants with tourism experiences were between the ages of 70 and 79. Most were married (56.25%), educated (71.75%), lived in urban areas (62.48%), and had a strong economic status (94.47%) and relatively healthy lifestyles.

Table 1. Characteristics of the study participants at baseline.
Association between tourism experiences and cognitive impairment
The median follow-up time was 48.12 months (47.40 months for participants without tourism experiences and 55.20 months for participants with tourism experiences). Of the 669 participants with tourism experiences, 97 (14.50%) developed cognitive impairment compared with 1,319 (21.81%) of the 6,048 participants without such experiences. The incidence density (ID) of cognitive impairment was lower in participants with tourism experiences (ID = 316.94 per 10,000 person-years) than in those without (ID = 552.38 per 10,000 person-years) (Table 2).

Table 2. Association between tourism experiences and cognitive impairment.
As shown in Figure 2A, the Kaplan–Meier analysis illustrated that individuals with tourism experiences had lower incidence cognitive impairment compared with those without tourism experiences. In the univariate analysis, participants with tourism experiences were at a lower risk of cognitive impairment (crude hazard ratio [cHR] = 0.51, 95% CI: 0.41–0.62, p < 0.001). In Model 2, after adjusting for age, gender, education level, residence, marital status, and living pattern, a lower risk of cognitive impairment was also observed (adjusted hazard ratio [aHR] = 0.68, 95%CI: 0.55–0.84, p < 0.001) in people with tourism experiences. Upon adjusting for all covariates (i.e., Model 3), we observed a significantly lower risk of cognitive impairment (aHR: 0.69, 95% CI: 0.55–0.87, p = 0.002) in this group.
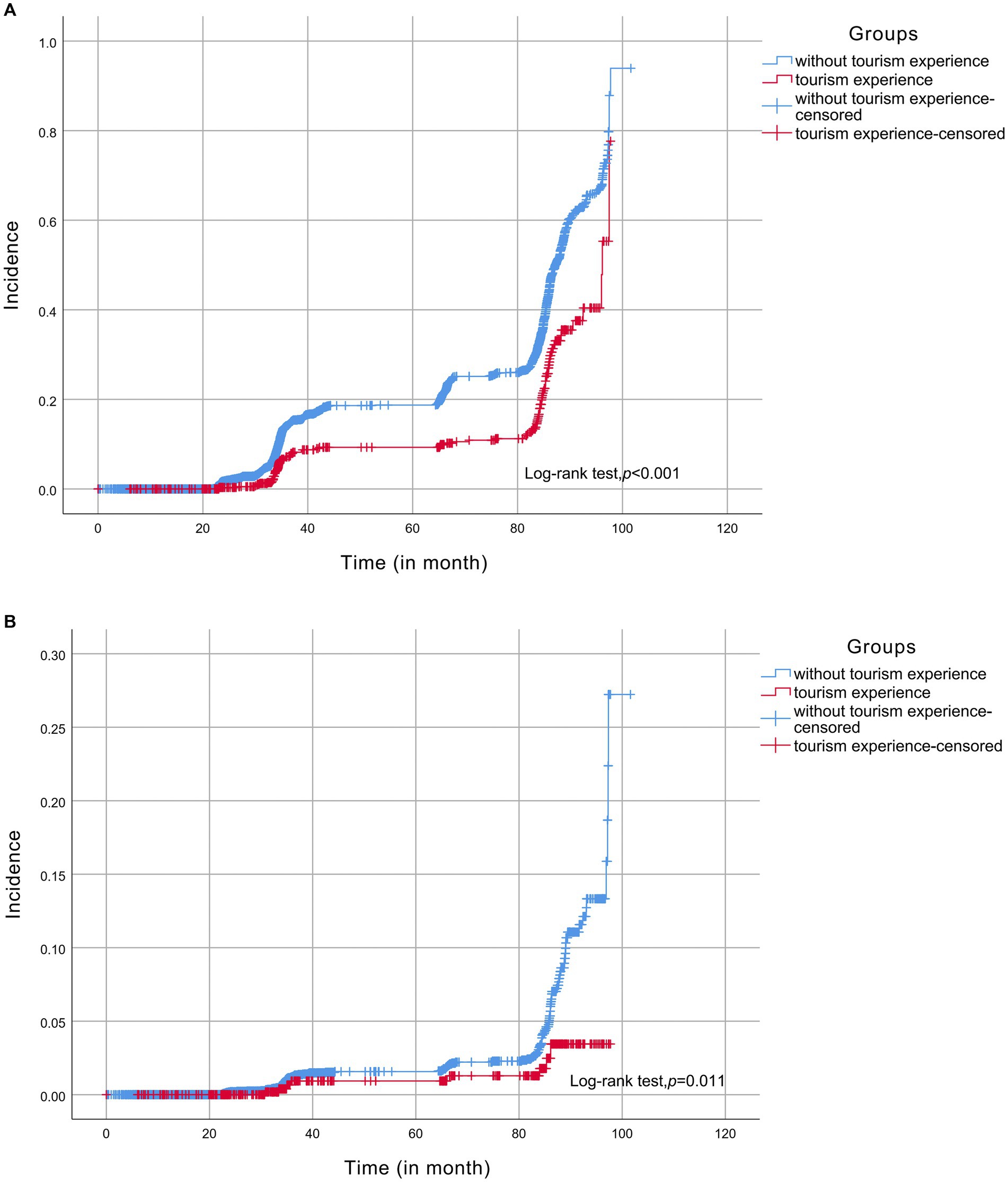
Figure 2. Kaplan-Meier analysis; (A) cognitive impairment, (B) dementia.
During subgroup analysis, on the bases of age, gender, education level, residence, marital status, living pattern, smoking, alcohol consumption, regular physical exercise, BMI, economic status, annual household income, sleep quality, and hours slept per day, the association between the risk of cognitive impairment and tourism experiences was robust (Supplementary Table S1; Figure 3). The estimates of interaction between tourism experiences and covariates were not significant (Supplementary Table S1).
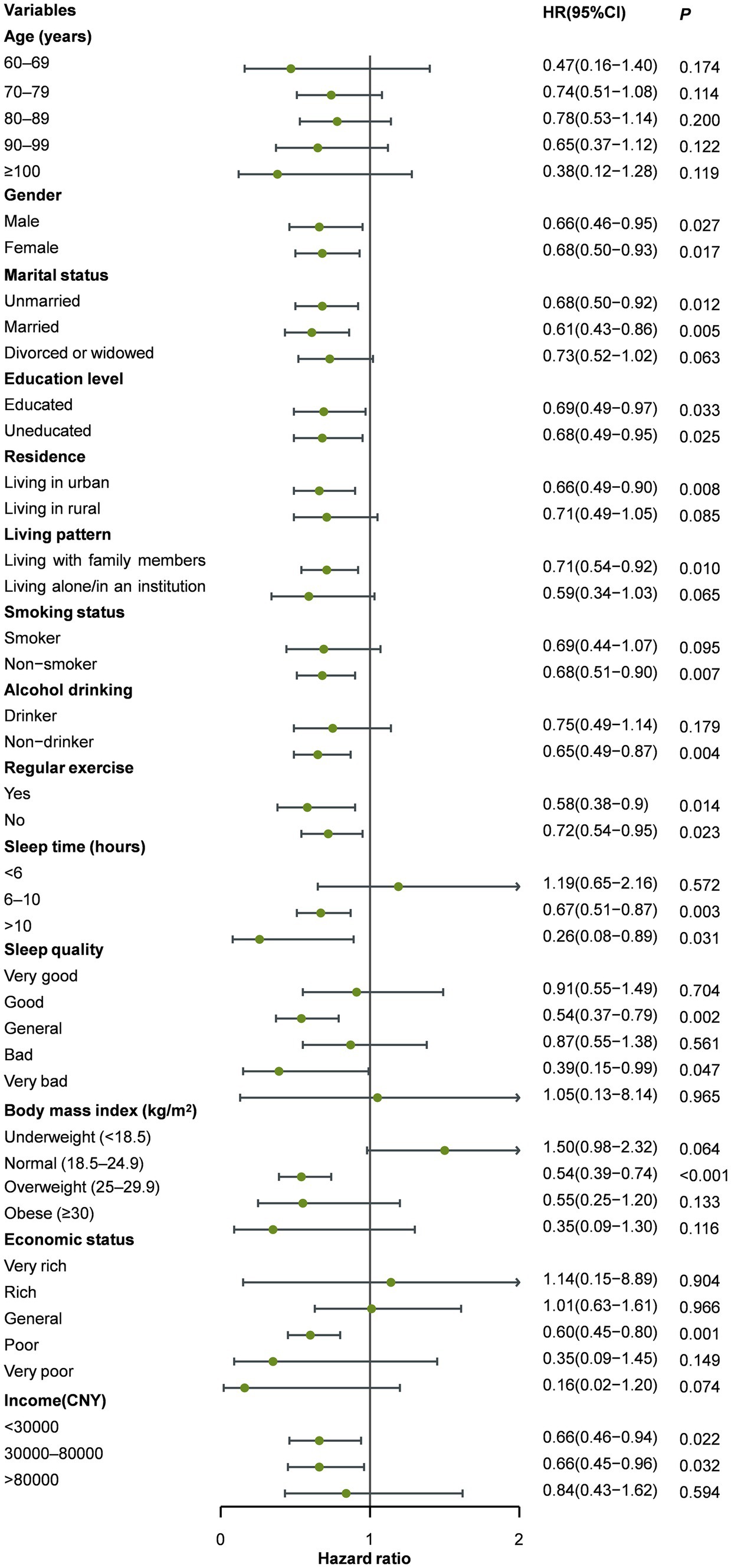
Figure 3. Subgroup analysis on cognitive impairment.
Regarding dose–response analysis (Supplementary Table S2; Figure 4), among participants with ≥3 tourism experiences, the HR for cognitive impairment was 0.45 (95% CI: 0.31–0.66)—lower than the HRs for individuals with two tourism experiences (HR = 0.48, 95% CI: 0.32–0.71) or one tourism experience (HR = 0.57, 95% CI: 0.42–0.77). The linear dose–response manner was significant (Z = −4.218, p < 0.001). Multivariate analysis revealed that tourism frequency influenced the incidence of cognitive impairment in a dose–response manner.
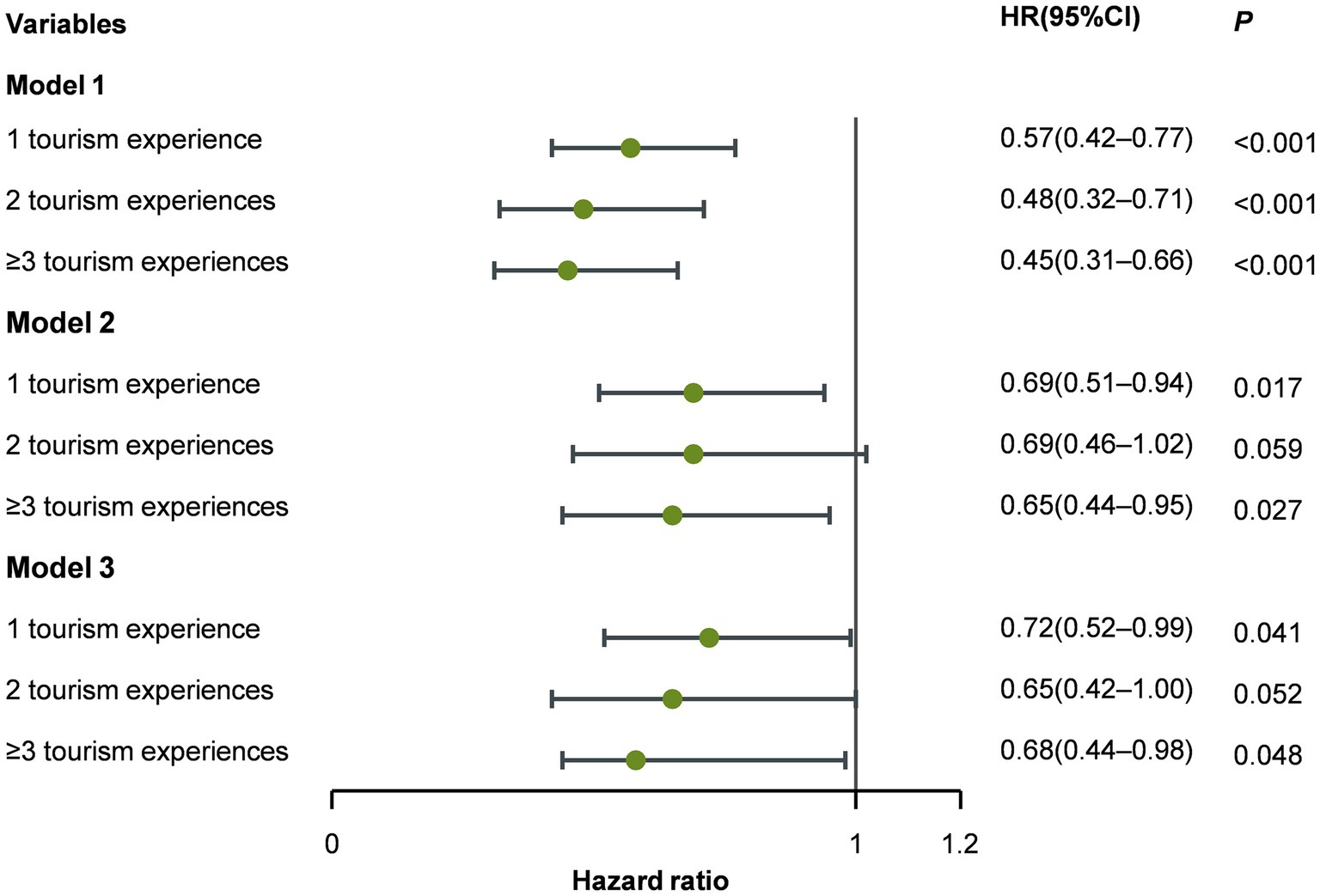
Figure 4. Dose-response association between tourism experiences and cognitive impairment.
In terms of the severity of cognitive impairment, we compared CMMSE scores between participants with and without tourism experiences. As indicated in Supplementary Table S3, the impairment severity was significantly higher for individuals with tourism experiences than for those without.
Association between tourism experiences and dementia
Of the 669 participants with tourism experiences, only 8 (1.20%) developed dementia, whereas 131 (2.17%) of the 6,048 participants without such experiences were diagnosed with dementia. The ID of dementia in participants with tourism experiences (ID = 26.14 per 10,000 person-years) was lower than in participants without tourism experiences (ID = 54.86 per 10,000 person-years) (Table 3). The Kaplan–Meier analysis indicated that the incidence of dementia was significantly lower among individuals with tourism experiences than those without tourism experiences (Figure 2B). Univariate analysis demonstrated that participants with tourism experiences had a lower risk of dementia (cHR = 0.41, 95% CI: 0.20–0.84, p = 0.014) than those without such experiences. In Model 2, upon adjusting for age, gender, education level, residence, marital status, and living pattern, a lower risk of dementia was also observed (aHR = 0.47, 95% CI: 0.23–0.96, p = 0.038). In Model 3, a significantly lower risk of dementia (aHR: 0.41, 95% CI: 0.19–0.89, p = 0.024) was found after adjusting for all covariates. Supplementary Table S4; Supplementary Figure S1 illustrate that the dose–response analysis yielded an insignificant association between the risk of dementia and tourism frequency (Z = −1.514, p = 0.130). In the subgroup analysis, the association between tourism experiences and the risk of dementia was strong (Supplementary Table S5; Supplementary Figure S2). We did not observe significant interactions between tourism experiences and the covariates (Supplementary Table S5).
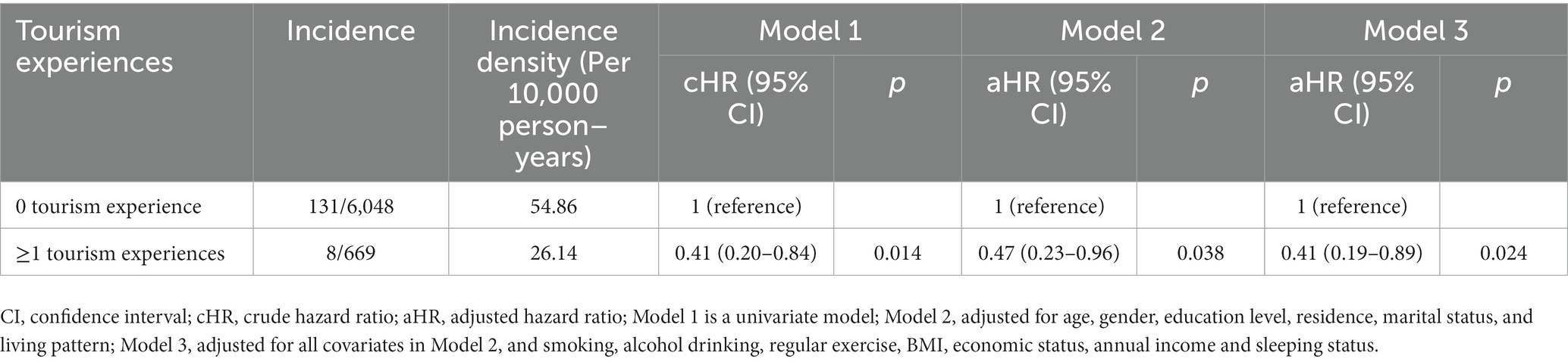
Table 3. Association of tourism experiences with dementia.
Discussion
Our findings showed that tourism experiences reduced the incidence of cognitive impairment and dementia in older Chinese adults. Tourism may even protect against cognitive decline in a dose–response manner. Although tourism has been broadly acknowledged as beneficial to physical and mental health, few studies have examined the protective effects of tourism on cognitive function (24, 45). This nationwide prospective cohort study revealed a correlation between tourism experiences along with declines in cognitive impairment and dementia.
As a multi-component form of leisure, tourism can improve physical and mental health (especially cognitive function) through physical activity, positive emotions, social engagement, therapeutic landscapes (e.g., nature-based tourism, culture-based tourism) and other means. Tourism requires mobility, especially when outdoors, is inextricably linked with physical activity (e.g., walking, hiking, mountain climbing, cycling) (39, 46, 47), therefore supports physical activity (48). Studies have shown that non-participation in tourism is associated with low physical activity (49). Physical activity has numerous positive impacts on physical and mental health, effectively reducing poor health outcomes (50, 51). A systematic review summarized the roles of physical activity in improved fitness and cognitive function and indicated that people with moderate daily physical activity had better physical performance and fewer signs of cognitive delay than people who engaged in less physical activity (52). Evidence further suggests that physical activity affects cognitive function in a dose–response manner, indicating that more intense physical activity correlates with better cognitive function (53–55). A 6-month physical activity intervention was also reported to produce significant but modest enhancements in cognitive function in older adults at high risk of dementia (56). Physical activity is a prominent supportive treatment for cognitive impairment.
Autonomic dysfunction is closely related to the development of dementia (57). Engaging in physical activity and avoiding prolonged sedentary behavior can help maintain the normal function of the autonomic nervous system (ANS) (58). Taking part in domestic nature-based tourism can improve ANS functioning via stress reduction (59). Decreased dopamine levels are associated with dementia and Parkinson’s disease (60), but physical activity can prompt dopamine release and maintain a younger biological age (61, 62). Promoting physical activity through travel, especially outdoors, can therefore contribute to better health and a higher quality of life. Tourism sites that are popular among older travelers should host creative activities to encourage physical movement, particularly for individuals with limited mobility. For example, drum circles and chair dance programs could enable mobility-limited travelers to engage in physical activity while visiting nature centers or other outdoor venues. Older travelers with good mobility could meander along nature trails or take walks on easy terrain to enhance their physical activity while traveling.
Poor psychological functioning also increases dementia risk (63–65). A pleasant mood can upregulate dopamine secretion in tourists, playing an important role in cognitive health (66). Tourists have great access to green environments (e.g., parks, lakes, hills, forests) and friendly people to alleviate stress and maintain a pleasant mental state (67). For instance, forest bathing is a natural therapy to assuage negative emotions and improve bodily functions (68). A large body of evidence indicates that people who regularly participate in tourism activities have better mental well-being than those who do not (69). A cohort study found that people in a poor mood were at higher risk of dementia than those in a better mood (70). Positive tourism experiences relax tourists’ bodies and minds, elicit optimism and pleasant emotions (71), and enhance cognitive function (39). Our study showed that tourism can lessen the symptoms of cognitive impairment and dementia; positive emotions arising during travel may play considerable roles in this improvement. Therefore, tourism and hospitality practitioners should aim to evoke positive emotions among travelers by offering high-quality products and services (e.g., vulnerability-friendly amenities, personalized tours) and meaningful experiences (e.g., cultural immersion, social interaction).
Social engagement is similarly vital for maintaining cognitive function. Greater social engagement reduces dementia risk in the older adult (72, 73). This type of engagement can delay or prevent dementia onset even in people at high risk of cognitive impairment (74). In contrast to physical activity, social engagement allows tourists to interact with their surroundings (e.g., other travelers, residents, tour guides, animals) (75), thus strengthening their connection to society (76). Encouraging older adults to interact socially can ameliorate loneliness and depression, ultimately improving mental health and cognitive function (77). Tourism and hospitality practitioners should take various measures to promote social engagement in destinations: social spaces (e.g., public squares, gardens) and interactive activities (e.g., festivals and events, volunteer activities, interactive technologies) should be coordinated. Front desk attendants at venues and hotels can be instructed to facilitate social engagement at destinations that are welcoming of older travelers.
Limitations
This cohort study demonstrated the preventive effect of tourism on cognitive impairment among the older adult; however, there are several limitations. First, findings from a Chinese population might not generalize elsewhere due to socioeconomic circumstances and lifestyles. Second, we did not investigate tourism activities in depth (e.g., length of tourism experience, and types of tourism). The specific effects of different components of tourism on cognitive impairment and dementia also remain to be further explored. Third, although multivariate analyses were conducted to adjust for regular physical exercise and other covariates, participants’ baseline health status could have biased our findings: we excluded individuals with Parkinson’s disease, physical disabilities, and other severe somatic diseases. In addition, the participants were most married, educated, lived in urban areas and in a strong economic status, which contributed to mitigation of the progress of cognitive impairment. We cannot fully control for these confounding factors that influence the contribution of tourism experience.
Conclusion
Our nationwide prospective cohort analysis documented correlations between tourism experiences and a lower risk of cognitive impairment and dementia. Results suggest that tourism can enhance cognitive function and should be considered as a non-pharmacological intervention to prevent cognitive impairment and dementia.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author.
Ethics statement
The studies involving humans were approved by Ethical Review Committee of Peking University (IRB00001052–13074). The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required from the participants or the participants’ legal guardians/next of kin in accordance with the national legislation and institutional requirements.
Author contributions
QL: Software, Writing – original draft, Data curation. ZG: Writing – original draft, Software. FH: Writing – original draft, Data curation. MX: Writing – original draft, Data curation, Software. QZ: Writing – review & editing, Conceptualization. JW: Writing – review & editing, Conceptualization, Methodology. TY: Writing – review & editing. DZ: Writing – review & editing, Formal analysis. YW: Resources, Writing – review & editing, Formal analysis. SY: Writing – review & editing, Formal analysis. HH: Writing – review & editing, Conceptualization, Formal analysis.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This study was supported by European Commission Horizon 2020 (779238-PRODEMOS); National key research and development program of China (2017YFE0118800).
Acknowledgments
We thank the members of the CLHLS study group for data collection and all the participants.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2023.1271319/full#supplementary-material
References
1. Kuang, W, Gao, M, Tian, L, Wan, Y, and Qiu, P. Trends in the prevalence of cognitive impairment in Chinese older adults: based on the Chinese longitudinal healthy longevity survey cohorts from 1998 to 2014. Int Health. (2020) 12:378–87. doi: 10.1093/inthealth/ihz114
2. Jia, L, du, Y, Chu, L, Zhang, Z, Li, F, Lyu, D, et al. Prevalence, risk factors, and management of dementia and mild cognitive impairment in adults aged 60 years or older in China: a cross-sectional study. Lancet Public Health. (2020) 5:e661–71. doi: 10.1016/S2468-2667(20)30185-7
3. International ASD. World Alzheimer report 2021: Journey through the Diagnosis of Dementia. (2021).
4. Chuanhua, LTY. Analysis on the status and trend of dementia burden in China based on the global perspective. Chinese J Dis Control Prevent. (2022) 26:684–90. doi: 10.16462/j.cnki.zhjbkz.2022.06.012
5. Ren, RJ, Yin, P, Wang, ZH, et al. Chinese Alzheimer disease report 2021. J Diagn Concepts Pract. (2021) 20:317–37. doi: 10.16150/j.1671-2870.2021.04.001
6. Fang, EF, Xie, C, Schenkel, JA, Wu, C, Long, Q, Cui, H, et al. A research agenda for ageing in China in the 21st century (2nd edition): focusing on basic and translational research, long-term care, policy and social networks. Ageing Res Rev. (2020) 64:101174. doi: 10.1016/j.arr.2020.101174
7. Du, M, Tao, L, Liu, M, and Liu, J. Tourism experiences and the lower risk of mortality in the Chinese elderly: a national cohort study. BMC Public Health. (2021) 21:996. doi: 10.1186/s12889-021-11099-8
8. Hugo, J, and Ganguli, M. Dementia and cognitive impairment: epidemiology, diagnosis, and treatment. Clin Geriatr Med. (2014) 30:421–42. doi: 10.1016/j.cger.2014.04.001
9. Reith, W, and Mühl-Benninghaus, R. Differential diagnostics of dementia type diseases. Radiologe. (2015) 55:378–85. doi: 10.1007/s00117-014-2799-z
10. Cummings, JL, Tong, G, and Ballard, C. Treatment combinations for Alzheimer's disease: current and future pharmacotherapy options. J Alzheimers Dis. (2019) 67:779–94. doi: 10.3233/JAD-180766
11. Arvanitakis, Z, and Bennett, DA. What is dementia? JAMA. (2019) 322:1728. doi: 10.1001/jama.2019.11653
12. Szeto, JY, and Lewis, SJ. Current treatment options for Alzheimer's disease and Parkinson's disease dementia. Curr Neuropharmacol. (2016) 14:326–38. doi: 10.2174/1570159X14666151208112754
13. Gómez-Romero, M, Jiménez-Palomares, M, Rodríguez-Mansilla, J, Flores-Nieto, A, Garrido-Ardila, EM, and González López-Arza, MV. Benefits of music therapy on behaviour disorders in subjects diagnosed with dementia: a systematic review. Neurologia. (2017) 32:253–63. doi: 10.1016/j.nrl.2014.11.001
14. Ismail, S, Christopher, G, Dodd, E, Wildschut, T, Sedikides, C, Ingram, TA, et al. Psychological and mnemonic benefits of nostalgia for people with dementia. J Alzheimers Dis. (2018) 65:1327–44. doi: 10.3233/JAD-180075
15. Zheng, J, Chen, X, and Yu, P. Game-based interventions and their impact on dementia: a narrative review. Australas Psychiatry. (2017) 25:562–5. doi: 10.1177/1039856217726686
16. Karkou, V, and Meekums, B. Dance movement therapy for dementia. Cochrane Database Syst Rev. (2017) 2017:CD011022. doi: 10.1002/14651858.CD011022.pub2
17. Vink, AC, Zuidersma, M, Boersma, F, de Jonge, P, Zuidema, SU, and Slaets, JP. The effect of music therapy compared with general recreational activities in reducing agitation in people with dementia: a randomised controlled trial. Int J Geriatr Psychiatry. (2013) 28:1031–8. doi: 10.1002/gps.3924
18. Li, DM, and Li, XX. The effect of folk recreation program in improving symptoms: a study of Chinese elder dementia patients. Int J Geriatr Psychiatry. (2017) 32:901–8. doi: 10.1002/gps.4543
19. Cohen-Mansfield, J, and Jensen, B. Barriers to the success of recreational groups for persons with dementia. J Geriatr Psychiatry Neurol. (2022) 35:38–46. doi: 10.1177/0891988720978816
20. Sommerlad, A, Sabia, S, Livingston, G, Kivimäki, M, Lewis, G, and Singh-Manoux, A. Leisure activity participation and risk of dementia: An 18-year follow-up of the Whitehall II study. Neurology. (2020) 95:e2803–15. doi: 10.1212/WNL.0000000000010966
21. Yates, LA, Ziser, S, Spector, A, and Orrell, M. Cognitive leisure activities and future risk of cognitive impairment and dementia: systematic review and meta-analysis. Int Psychogeriatr. (2016) 28:1791–806. doi: 10.1017/S1041610216001137
22. Verghese, J, Lipton, RB, Katz, MJ, Hall, CB, Derby, CA, Kuslansky, G, et al. Leisure activities and the risk of dementia in the elderly. N Engl J Med. (2003) 348:2508–16. doi: 10.1056/NEJMoa022252
23. Almeida-Meza, P, Steptoe, A, and Cadar, D. Is engagement in intellectual and social leisure activities protective against dementia risk? Evidence from the English longitudinal study of ageing. J Alzheimers Dis. (2021) 80:555–65. doi: 10.3233/JAD-200952
24. Wen, J, Zheng, D, Hou, H, Phau, I, and Wang, W. Tourism as a dementia treatment based on positive psychology. Tour Manag. (2022) 92:104556. doi: 10.1016/j.tourman.2022.104556
25. Govers, R, Van Hecke, E, and Cabus, P. Delineating tourism: defining the usual environment. Ann Tour Res. (2008) 35:1053–73. doi: 10.1016/j.annals.2008.09.001
26. Hu, F, Wen, J, Zheng, D, and Wang, W. Travel medicine in hospitality: An interdisciplinary perspective. Int J Contemp Hosp. (2023) 35:3134–53. doi: 10.1108/IJCHM-05-2022-0574
27. Hu, F. Thinking global about health research medical forum. (2023). Available at: https://mforum.com.au/thinking-global-about-health-research/.
28. Hsu, CH, Cai, LA, and Wong, KK. A model of senior tourism motivations—anecdotes from Beijing and Shanghai. Tour Manag. (2007) 28:1262–73. doi: 10.1016/j.tourman.2006.09.015
29. Sangpikul, A. Travel motivations of Japanese senior travellers to Thailand. Int J Tour Res. (2008) 10:81–94. doi: 10.1002/jtr.643
30. Buckley, RC, and Cooper, MA. Tourism as a tool in nature-based mental health: Progress and prospects post-pandemic. Int J Environ Res Public Health. (2022) 19:13112. doi: 10.3390/ijerph192013112
31. Wen, J, Zheng, D, and Hu, F. The emerging concept of travel therapy in health science: will it be applied to tourists visiting sub-frigid climate zones. Frigid Zone Med. (2022) 2:200–3. doi: 10.2478/fzm-2022-0027
32. Guo, Z, Wen, J, Zheng, D, Yulu, Z, Hou, H, and Wang, W. Proposing an avenue for suboptimal health research through the lens of tourism. J Glob Health. (2022) 12:03058. doi: 10.7189/jogh.12.03058
33. Zheng, D, Wen, J, Kozak, M, Phau, I, Hou, H, and Wang, W. Vulnerable populations with psychological disorders in tourism: methodological challenges and recommended solutions for empirical research. Tour Manag. (2023) 98:104760. doi: 10.1016/j.tourman.2023.104760
34. Hwang, J, Kim, JJ, Lee, JS, and Sahito, N. How to form wellbeing perception and its outcomes in the context of elderly tourism: moderating role of tour guide services. Int J Environ Res Public Health. (2020) 17:1029. doi: 10.3390/ijerph17031029
35. Friman, M, and Olsson, LE. Daily travel and wellbeing among the elderly. Int J Environ Res Public Health. (2020) 17:2342. doi: 10.3390/ijerph17072342
36. Kobayashi, T, Tani, Y, Kino, S, Fujiwara, T, Kondo, K, and Kawachi, I. Prospective study of engagement in leisure activities and all-cause mortality among older Japanese adults. J Epidemiol. (2022) 32:245–53. doi: 10.2188/jea.JE20200427
37. Ferrer, JG, Sanz, MF, Ferrandis, ED, McCabe, S, and García, JS. Social tourism and healthy ageing. Int J Tour Res. (2016) 18:297–307. doi: 10.1002/jtr.2048
38. Feng, T, Feng, Z, Liu, Q, Jiang, L, Yu, Q, and Liu, K. Drinking habits and water sources with the incidence of cognitive impairment in Chinese elderly population: the Chinese longitudinal healthy longevity survey. J Affect Disord. (2021) 281:406–12. doi: 10.1016/j.jad.2020.12.044
39. Gu, D, Zhu, H, Brown, T, Hoenig, H, and Zeng, Y. Tourism experiences and self-rated health among older adults in China. J Aging Health. (2016) 28:675–703. doi: 10.1177/0898264315609906
40. Zhang, Q, Wu, Y, Han, T, and Liu, E. Changes in cognitive function and risk factors for cognitive impairment of the elderly in China: 2005-2014. Int J Environ Res Public Health. (2019) 16:2847. doi: 10.3390/ijerph16162847
41. An, R, and Liu, GG. Cognitive impairment and mortality among the oldest-old Chinese. Int J Geriatr Psychiatry. (2016) 31:1345–53. doi: 10.1002/gps.4442
42. Zhang, Z. Gender differentials in cognitive impairment and decline of the oldest old in China. J Gerontol B Psychol Sci Soc Sci. (2006) 61:S107–15. doi: 10.1093/geronb/61.2.S107
43. Cao, Z, Wang, R, Cheng, Y, Yang, H, Li, S, Sun, L, et al. Adherence to a healthy lifestyle counteracts the negative effects of risk factors on all-cause mortality in the oldest-old. Aging (Albany NY). (2019) 11:7605–19. doi: 10.18632/aging.102274
44. Bauer, JM, de Castro, A, Bosco, N, Romagny, C, Diekmann, R, Benyacoub, J, et al. Influenza vaccine response in community-dwelling German prefrail and frail individuals. Immun Ageing. (2017) 14:17. doi: 10.1186/s12979-017-0098-z
45. Smith, MK, and Diekmann, A. Tourism and wellbeing. Ann Tour Res. (2017) 66:1–13. doi: 10.1016/j.annals.2017.05.006
46. Vada, S, Prentice, C, Scott, N, and Hsiao, A. Positive psychology and tourist well-being: a systematic literature review. Tour Manag Perspect. (2020) 33:100631. doi: 10.1016/j.tmp.2019.100631
47. Zheng, D, Jiang, Y, Wen, J, Phau, I, Hou, H, and Wang, W. Suboptimal health status, COVID-19 psychology, and cultural value impact on post-pandemic outbound travel. Tour Recreat Res. (2023) 1-18:1–18. doi: 10.1080/02508281.2023.2177468
48. Zabłocki, M, Branowski, B, Kurczewski, P, Gabryelski, J, and Sydor, M. Designing innovative assistive technology devices for tourism. Int J Environ Res Public Health. (2022) 19:14186. doi: 10.3390/ijerph192114186
49. Przybysz, K, and Stanimir, A. Tourism-related needs in the context of Seniors' living and social conditions. Int J Environ Res Public Health. (2022) 19:15325. doi: 10.3390/ijerph192215325
50. Nuzum, H, Stickel, A, Corona, M, Zeller, M, Melrose, RJ, and Wilkins, SS. Potential benefits of physical activity in MCI and dementia. Behav Neurol. (2020) 2020:1–10. doi: 10.1155/2020/7807856
51. Kroesen, M, and Handy, S. The influence of holiday-taking on affect and contentment. Ann Tour Res. (2014) 45:89–101. doi: 10.1016/j.annals.2013.12.006
52. Kramer, AF, and Colcombe, S. Fitness effects on the cognitive function of older adults: a Meta-analytic study-revisited. Perspect Psychol Sci. (2018) 13:213–7. doi: 10.1177/1745691617707316
53. Kerr, J, Marshall, SJ, Patterson, RE, Marinac, CR, Natarajan, L, Rosenberg, D, et al. Objectively measured physical activity is related to cognitive function in older adults. J Am Geriatr Soc. (2013) 61:1927–31. doi: 10.1111/jgs.12524
54. Blondell, SJ, Hammersley-Mather, R, and Veerman, JL. Does physical activity prevent cognitive decline and dementia?: a systematic review and meta-analysis of longitudinal studies. BMC Public Health. (2014) 14:510. doi: 10.1186/1471-2458-14-510
55. Demurtas, J, Schoene, D, Torbahn, G, Marengoni, A, Grande, G, Zou, L, et al. Physical activity and exercise in mild cognitive impairment and dementia: An umbrella review of intervention and observational studies. J Am Med Dir Assoc. (2020) 21:1415–22.e6. doi: 10.1016/j.jamda.2020.08.031
56. Lautenschlager, NT, Cox, KL, Flicker, L, Foster, JK, van Bockxmeer, FM, Xiao, J, et al. Effect of physical activity on cognitive function in older adults at risk for Alzheimer disease: a randomized trial. JAMA. (2008) 300:1027–37. doi: 10.1001/jama.300.9.1027
57. Beishon, LC, Hosford, P, Gurung, D, Brassard, P, Minhas, JS, Robinson, TG, et al. The role of the autonomic nervous system in cerebral blood flow regulation in dementia: a review. Auton Neurosci. (2022) 240:102985. doi: 10.1016/j.autneu.2022.102985
58. Scherder, E, Scherder, R, Verburgh, L, Königs, M, Blom, M, Kramer, AF, et al. Executive functions of sedentary elderly may benefit from walking: a systematic review and meta-analysis. Am J Geriatr Psychiatry. (2014) 22:782–91. doi: 10.1016/j.jagp.2012.12.026
59. Chang, LC. The relationship between nature-based tourism and autonomic nervous system function among older adults. J Travel Med. (2014) 21:159–62. doi: 10.1111/jtm.12108
60. Klein, MO, Battagello, DS, Cardoso, AR, Hauser, DN, Bittencourt, JC, and Correa, RG. Dopamine: functions, signaling, and association with neurological diseases. Cell Mol Neurobiol. (2019) 39:31–59. doi: 10.1007/s10571-018-0632-3
61. Hemmeter, UM, and Ngamsri, T. Physical activity and mental health in the elderly. Praxis (1994). 2022;110:193–198.
62. Sacheli, MA, Neva, JL, Lakhani, B, Murray, DK, Vafai, N, Shahinfard, E, et al. Exercise increases caudate dopamine release and ventral striatal activation in Parkinson's disease. Mov Disord. (2019) 34:1891–900. doi: 10.1002/mds.27865
63. Kessing, LV. Depression and the risk for dementia. Curr Opin Psychiatry. (2012) 25:457–61. doi: 10.1097/YCO.0b013e328356c368
64. Rubin, R. Exploring the relationship between depression and dementia. JAMA. (2018) 320:961–2. doi: 10.1001/jama.2018.11154
65. Diniz, BS, Butters, MA, Albert, SM, Dew, MA, and Reynolds, CF 3rd. Late-life depression and risk of vascular dementia and Alzheimer's disease: systematic review and meta-analysis of community-based cohort studies. Br J Psychiatry. (2013) 202:329–35. doi: 10.1192/bjp.bp.112.118307
66. Babu, MGR, Kadavigere, R, Koteshwara, P, Sathian, B, and Rai, KS. Rajyoga meditation induces grey matter volume changes in regions that process reward and happiness. Sci Rep. (2020) 10:16177. doi: 10.1038/s41598-020-73221-x
67. Lanki, T, Siponen, T, Ojala, A, Korpela, K, Pennanen, A, Tiittanen, P, et al. Acute effects of visits to urban green environments on cardiovascular physiology in women: a field experiment. Environ Res. (2017) 159:176–85. doi: 10.1016/j.envres.2017.07.039
68. Liao, YH, Kao, TW, Peng, TC, and Chang, YW. Gender differences in the association between physical activity and health-related quality of life among community-dwelling elders. Aging Clin Exp Res. (2021) 33:901–8. doi: 10.1007/s40520-020-01597-x
69. Furuyashiki, A, Tabuchi, K, Norikoshi, K, Kobayashi, T, and Oriyama, S. A comparative study of the physiological and psychological effects of forest bathing (Shinrin-yoku) on working age people with and without depressive tendencies. Environ Health Prev Med. (2019) 24:46. doi: 10.1186/s12199-019-0800-1
70. Sjöberg, L, Fratiglioni, L, Lövdén, M, and Wang, HX. Low mood and risk of dementia: the role of marital status and living situation. Am J Geriatr Psychiatry. (2020) 28:33–44. doi: 10.1016/j.jagp.2019.08.014
71. Lin, HH, Chang, KH, Tseng, CH, Lee, YS, and Hung, CH. Can the development of religious and cultural tourism build a sustainable and friendly life and leisure environment for the elderly and promote physical and mental health? Int J Environ Res Public Health. (2021) 18:11989. doi: 10.3390/ijerph182211989
72. Mortimer, JA, Ding, D, Borenstein, AR, DeCarli, C, Guo, Q, Wu, Y, et al. Changes in brain volume and cognition in a randomized trial of exercise and social interaction in a community-based sample of non-demented Chinese elders. J Alzheimers Dis. (2012) 30:757–66. doi: 10.3233/JAD-2012-120079
73. Kelly, ME, Duff, H, Kelly, S, McHugh Power, JE, Brennan, S, Lawlor, BA, et al. The impact of social activities, social networks, social support and social relationships on the cognitive functioning of healthy older adults: a systematic review. Syst Rev. (2017) 6:259. doi: 10.1186/s13643-017-0632-2
74. Amano, T, Park, S, Morrow-Howell, N, and Carpenter, B. The association between patterns of social engagement and conversion from mild cognitive impairment to dementia: evidence from the health and retirement study. Alzheimer Dis Assoc Disord. (2022) 36:7–14. doi: 10.1097/WAD.0000000000000486
75. Sirgy, MJ, Kruger, PS, Lee, D-J, and Yu, GB. How does a travel trip affect tourists’ life satisfaction? J Travel Res. (2011) 50:261–75. doi: 10.1177/0047287510362784
76. Chen, J, Liu, C, Si, Y, Law, R, and Zhang, M. A study on the mediating role of emotional solidarity between authenticity perception mechanism and tourism support behavior intentions within rural homestay inn tourism. Behav Sci (Basel). (2022) 12:341. doi: 10.3390/bs12090341
Keywords: tourism, cognitive impairment, dementia, incidence, prevention, cohort study
Citation: Li Q, Guo Z, Hu F, Xiao M, Zhang Q, Wen J, Ying T, Zheng D, Wang Y, Yang S and Hou H (2023) Tourism experiences reduce the risk of cognitive impairment in the Chinese older adult: a prospective cohort study. Front. Public Health. 11:1271319. doi: 10.3389/fpubh.2023.1271319
Edited by:
Marco Filardi, University of Bari Aldo Moro, ItalyReviewed by:
Andrés Godoy, Universidad Autónoma de Chile, ChileFahad Naveed Ahmad, Wilfrid Laurier University, Canada
Copyright © 2023 Li, Guo, Hu, Xiao, Zhang, Wen, Ying, Zheng, Wang, Yang and Hou. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Song Yang, bGFvdG9uZ3h1ZV84ODhAMTYzLmNvbQ==
†These authors have contributed equally to this work