 Helio José Coelho-Junior1*Riccardo Calvani1,2Matteo Tosato2Andrea Russo2
Helio José Coelho-Junior1*Riccardo Calvani1,2Matteo Tosato2Andrea Russo2 Francesco Landi1,2
Francesco Landi1,2 Anna Picca2,3
Anna Picca2,3 Emanuele Marzetti1,2*
Emanuele Marzetti1,2*- 1Department of Geriatrics, Orthopedics and Rheumatology, Università Cattolica del Sacro Cuore, Rome, Italy
- 2Fondazione Policlinico Universitario “A. Gemelli” IRCCS, Rome, Italy
- 3Department of Medicine and Surgery, LUM University, Casamassima, Italy
Introduction: Studies on the associations between hypertension-related parameters and cognitive function, mood, and behavioral symptoms in older adults have produced mixed findings. A possible explanation for these divergent results is that investigations have not adequately adjusted their analyses according to the use of angiotensin-converting enzyme inhibitors (ACEIs). Therefore, the present study examined the cross-sectional associations between hypertension-related parameters, ACEI use, and cognitive function, mood, and behavioral symptoms in very old adults.
Methods: This study was conducted by analyzing the IlSIRENTE database, a prospective cohort study that collected data on all individuals aged 80 years and older residing in the Sirente geographic area (n = 364). Blood pressure (BP) was assessed after 20 to 40 min of rest, while participants sat in an upright position. Drugs were coded according to the Anatomical Therapeutic and Chemical codes. Cognitive function, mood, and behavioral symptoms were recorded using the Minimum Data Set Home Care instrument. Blood inflammatory markers were measured.
Results: Hypertension-related parameters were significantly associated with many cognitive, mood, and behavioral parameters after adjustment for covariates. However, only the inverse association between hypertension and lesser problems with short-term memory remained significant. Participants with hypertension had lower blood concentrations of inflammatory markers in comparison to their normotensive peers.
Conclusion: Findings from the present study indicate that high BP values are associated with fewer complaints about memory problems in very old adults. Furthermore, a lower concentration of inflammatory markers was found in hypertensive participants. ACEI use might affect this scenario.
1 Introduction
Hypertension is a chronic condition characterized by sustained elevations in blood pressure (BP) (1). This disease is highly prevalent in older adults, affecting more than 70% of those aged 65 and over (2). These data deserve concern, given that uncontrolled hypertension predisposes to the occurrence of numerous undesirable health events, including stroke, myocardial infarction, and heart failure (1).
Besides the well-established associations between high BP levels and cardiovascular risk, considerable interest has been given to the possible effects of hypertension on brain functioning. As a matter of fact, many studies have found that the progression of hypertension is associated with cognitive decline and the occurrence of mild cognitive impairment (MCI) and dementia, including Alzheimer’s disease (AD) (3–5). However, these results are conflicting, given that other investigations found that high BP levels might be a protective mechanism, mainly in very old adults, to counteract the deleterious effects of aging on cerebrovascular structure (6–9).
The disturbance of the renin-angiotensin system is one of the major causes of hypertension (10). Augmented and uncontrolled production of angiotensin II (ANGII) is associated with detrimental effects in many organs, including heart, vessels, and kidneys (10, 11). In the brain, ANG II causes important structural and functional changes (12–14), which are exacerbated with aging (13). Treatment with angiotensin-converting enzyme inhibitors (ACEIs) might reduce the deleterious effects of ANGII on the brain in preclinical models (15–17). Such effect might occur through reductions in the inflammatory milieu (15–17).
To expand the knowledge on the subject, the present study was conducted to examine the associations between hypertension-related parameters and cognitive function, mood, and behavioral aspects in a well-characterized cohort of very old adults. The possible role of ACEIs in this relationship was also analyzed.
2 Methods
Data for the present investigation were obtained from the IlSIRENTE study database (18). IlSIRENTE was a prospective cohort study conducted in the mountain community of the Sirente geographic area (L’Aquila, Abruzzo) in Central Italy. The study was compliant with the principles of the Declaration of Helsinki and the protocol was approved by the Ethics Committee of the Università Cattolica del Sacro Cuore (Rome, Italy). All participants signed an informed consent prior to enrolment.
2.1 Study population
A list of all persons living in the Sirente area was obtained in October 2003 from the registry offices of the 13 municipalities involved in the study. Potential study participants were subsequently identified by selecting all those born before 1 January 1924 and currently living in that region. The total sample enrolled in the ilSIRENTE study consisted of 364 older adults.
2.2 Data collection
Baseline assessments began in December 2003 and were completed in September 2004. Follow-up visits took place after 24 months of baseline assessment. Information about medical history, medications, and lifestyle habits (e.g., smoking, alcohol consumption, physical activity) was collected using validated questionnaires (18). Body height and weight were measured through a stadiometer and an analog medical scale, respectively. The body mass index (BMI) was then calculated as the ratio between body weight (kg) and the square of height (m2).
2.3 Hypertension parameters
BP was measured after 20 to 40 min of rest using an aneroid sphygmomanometer and a stethoscope, while participants sat in an upright position. Three measurements were taken from the left arm, and only one from the right arm. BP values were then calculated from the average of the last two measures of the left arm plus the measure obtained from the right arm. Four hypertension groups were generated according to: (a) self-report of physician diagnosis (CLI-HTN), (b) high systolic BP (i.e., ≥130 mmHg) (SBP-HTN), (c) high diastolic BP (i.e., ≥80 mmHg) (DBP-HTN), and (d) high systolic and diastolic BP (BP-HTN). These groups were created to allow an exploratory analysis of HTN-related measures and cognitive, mood, and behavior parameters, since hypertension might be overdiagnosed due to the white coat effect, BP assessment tool, BP variability, physicians’ conduct and compliance to guidelines, and participants’ mood (19–22). In addition, most people with hypertension have problems with adherence to the treatment (23). Then, to provide a current view of the participants’ status and to reduce the risk of report bias, we categorized participants into “normal high” BP groups according to the guidelines of the European Society of Cardiology (24).
Drugs were coded according to the Anatomical Therapeutic and Chemical codes, a classification system that assigns a unique code to medicines according to the organ or system it works on and how it works. Drugs included Benazepril, Captopril, Enalapril, Fosinopril, Lisinopril, Moexipril, Perindopril, Quinapril, Ramipril, and Trandolapril. Analytical variables were created for the use of ACEIs and other antihypertensive drugs.
2.4 Cognitive, mood, and behavioral aspects
Cognitive, mood, and behavioral aspects were assessed according to items of sections B and E of the Minimum Data Set Home Care (MDS-HC) instrument (25). Section B involves six questions distributed in three cognitive domains (i.e., memory recall ability, decision-making, and indicators of delirium) regarding participants’ perceptions of their cognitive function in the last weeks. Possible answers are binary (i.e., yes or no), except for item 2: How well client made decisions about organizing the day (e.g., when to get up or have meals, which clothes to wear or activities to do)?, which includes five possible answers. A binary variable was created by diving those who reported being independent (i.e., 0) and dependents (i.e., 1). Section E contains 16 questions distributed in four complexes, which include indicators of depression, anxiety, and sad mood, mood decline, behavioral symptoms, and changes in behavioral symptoms. Except for item 2, which involves a binary answer, all other items include 3 potential responses: (a) not exhibited/not occurred, (b) exhibited 1–2 of last 3 days/occurred, easily altered, and (c) exhibited on each of last 3 days/occurred, not easily altered. Binary variables were created by separating answers “a” (i.e., 0) and answers “b” and “c” (i.e.,1). Participants’ self-reports were obtained during interviews conducted by healthcare professionals.
2.5 Inflammatory markers
Blood samples were obtained from approximately 97% of participants. Blood was drawn after overnight fasting by a trained phlebotomist according to a standardized protocol. Blood samples were immediately centrifuged at 4°C and stored at −80°C until analysis. C-reactive protein (CRP), interleukin-6 levels (IL-6), and tumor necrosis factor-α (TNFα) were measured in plasma by enzyme-linked immunosorbent assays (ELISA; High Sensitivity Quantikine KitR&D Systems, Minneapolis, MN). All assays were run in duplicate, and average values were used for the analyses.
2.6 Statistical analysis
Continuous variables are expressed as mean ± standard deviation (SD), while categorical variables are reported as absolute numbers and percentages. Comparisons between groups with and without hypertension (e.g., CLI-HTN and NON-CLI-HTN) were performed using independent t-tests. Chi-square (Χ2) tests and binary regression were used to explore the relationship between BP and cognitive, mood, and behavioral parameters. Χ2 tests were performed within each group (e.g., SBP-HTN) comparing the prevalence of the variables between hypertensive and normotensive participants. Regressions were performed using BP-related parameters as independent variables and each binary answer of the MDS-HC, as the dependent variable. Comparisons were performed between condition (e.g., CLI-HTN) and non-condition (e.g., NON-CLI-HTN), with the last used as the reference group. No comparisons were performed among the different classifications (e.g., CLI-HTN vs. SBP-HTN). The final models were adjusted for age, sex, BMI, physical activity levels, multimorbidity, smoking status, unintentional loss of weight, schooling years, antipsychotic and antidepressant drugs, and ACEI use. For all tests, the level of significance was set at 5% (p < 0.05). All p values were determined by two-tailed tests. Analyses were performed using the SPSS software (version 23.0, SPSS Inc., Chicago, IL, United States).
3 Results
The main characteristics of participants of the present study are shown in Table 1 for CLI-HTN, and in (Supplementary Table S1), for groups classified according to BP levels. Participants categorized as hypertensive according to BP values were younger, lighter, and more physically active than those normotensives. Hypertensive groups had higher systolic BP, whereas higher diastolic BP was observed in SBP-HTN, DBP-HTN, and BP-HTN groups. In the BP-HTN group, normotensive participants took more antipsychotic drugs than those with hypertension. As expected, a high prevalence of participants on ACEI was observed in the hypertensive subgroup of the CLI-HTN group.
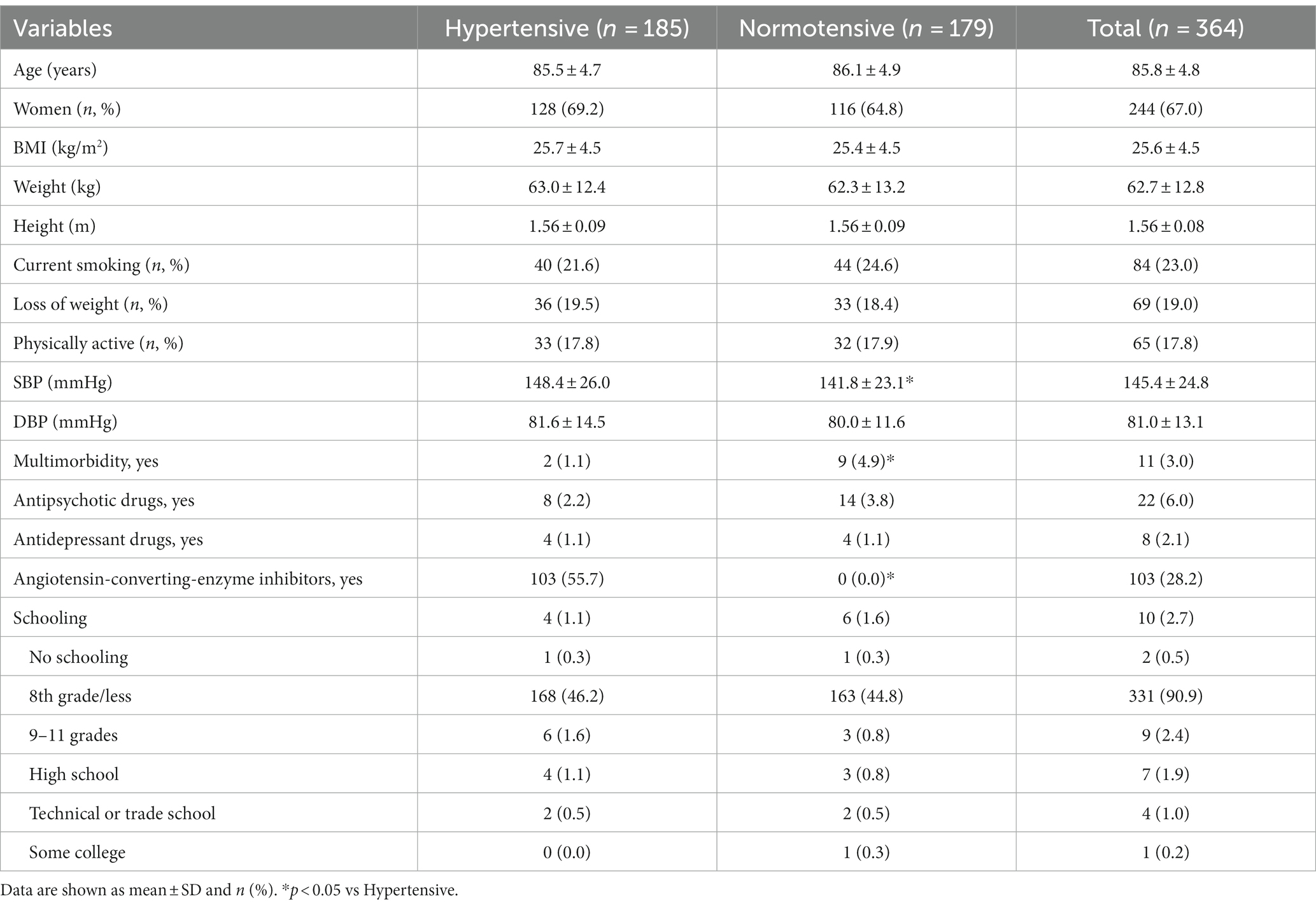
Table 1. Main characteristics of study participants (n = 364).
Table 2 shows the results for the associations between hypertension-related parameters and cognitive function, mood, and behavioral aspects. Hypertensive participants reported fewer problems with short-term and procedural memory and worsening in decision-making in comparison to normotensive participants, regardless of the categorization method, except for procedural memory in the CLI-HTN subgroup. In the SBP-HTN subgroup, hypertensive participants had a lower frequency of changes in mental function. Regarding mood and behavioral aspects, hypertensive participants of the BP-HTN subgroup reported experiencing fewer feelings of sadness, unrealistic fears, repetitive health and anxious complaints, displayed more facial expressions of sadness, had more episodes of recurrent crying, withdrawal from activities of interest, and reduced social interaction. Persistent anger was mostly observed in hypertensive participants categorized according to systolic and diastolic BP. In the CLI-HTN and DBP-HTN subgroups, hypertensive participants reported having more recurrent crying. Furthermore, hypertensive participants in the CLI-HTN had reduced social interaction. No other significant associations were observed.
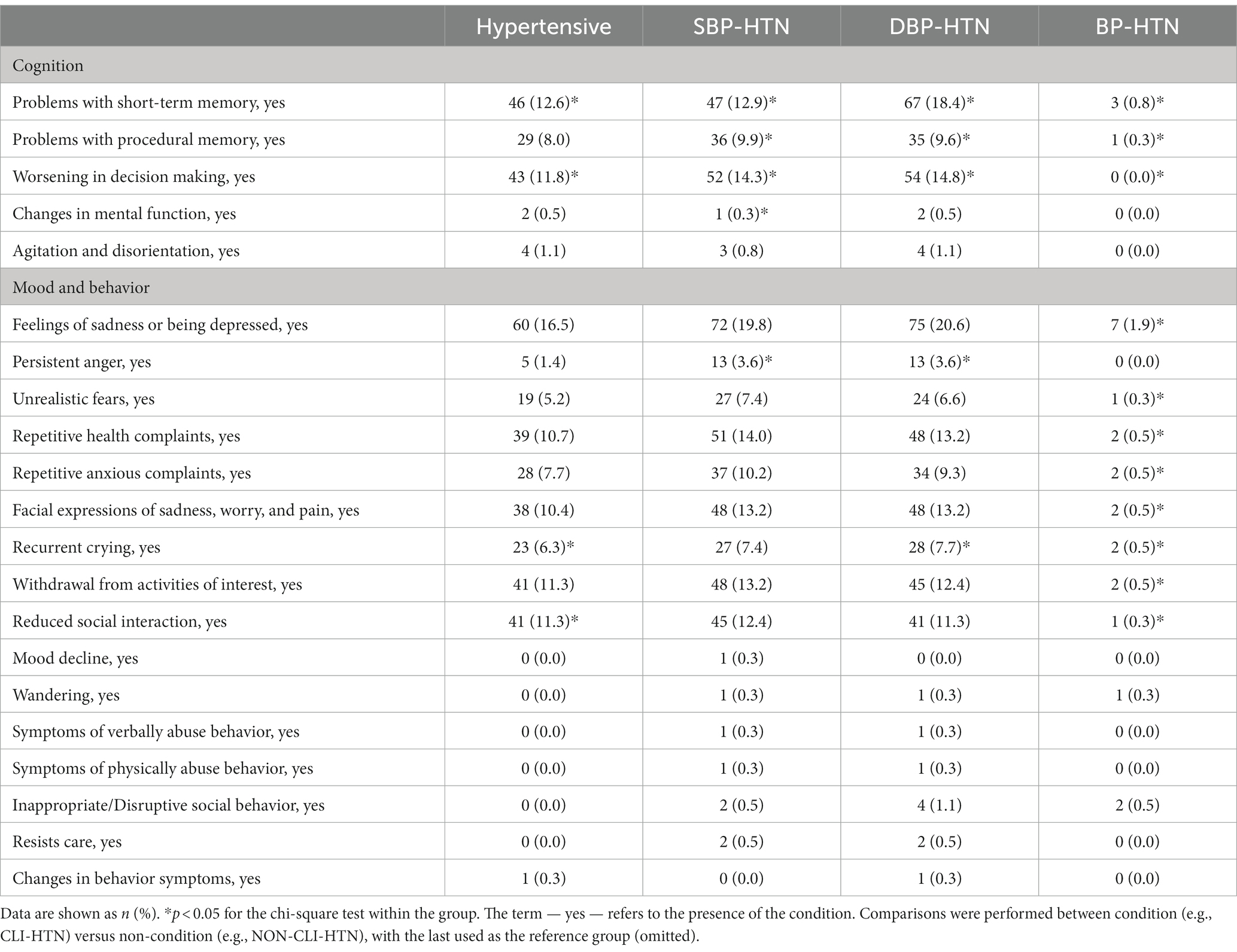
Table 2. Non-adjusted associations between hypertension-related parameters and cognitive function, mood, and behavioral aspects.
Results of the binary regression for the associations between hypertension-related parameters and cognitive function, mood, and behavioral aspects adjusted for covariates are shown in Table 3. We observed that hypertensive participants in the CLI-HTN and BP-HTN groups had a lower likelihood of having problems with short-term memory. Hypertensive participants of the BP-HTN subgroup had also lesser reductions in social interactions, whereas those in the CLI-HTN reported more reduced social interaction. Furthermore, high systolic BP (continuous) was significantly associated with fewer reports of worsening in decision-making. Hypertensive participants who had high systolic and diastolic BP values (BP-HTN) reported fewer feelings of sadness and depressive symptoms, unrealistic fears, and anxious complaints, as well as showed fewer facial expressions associated with feelings of sadness, pain, and worry, and had a lesser withdrawal from activities of interest. In contrast, hypertensive participants categorized according to systolic BP reported more episodes of recurrent crying.
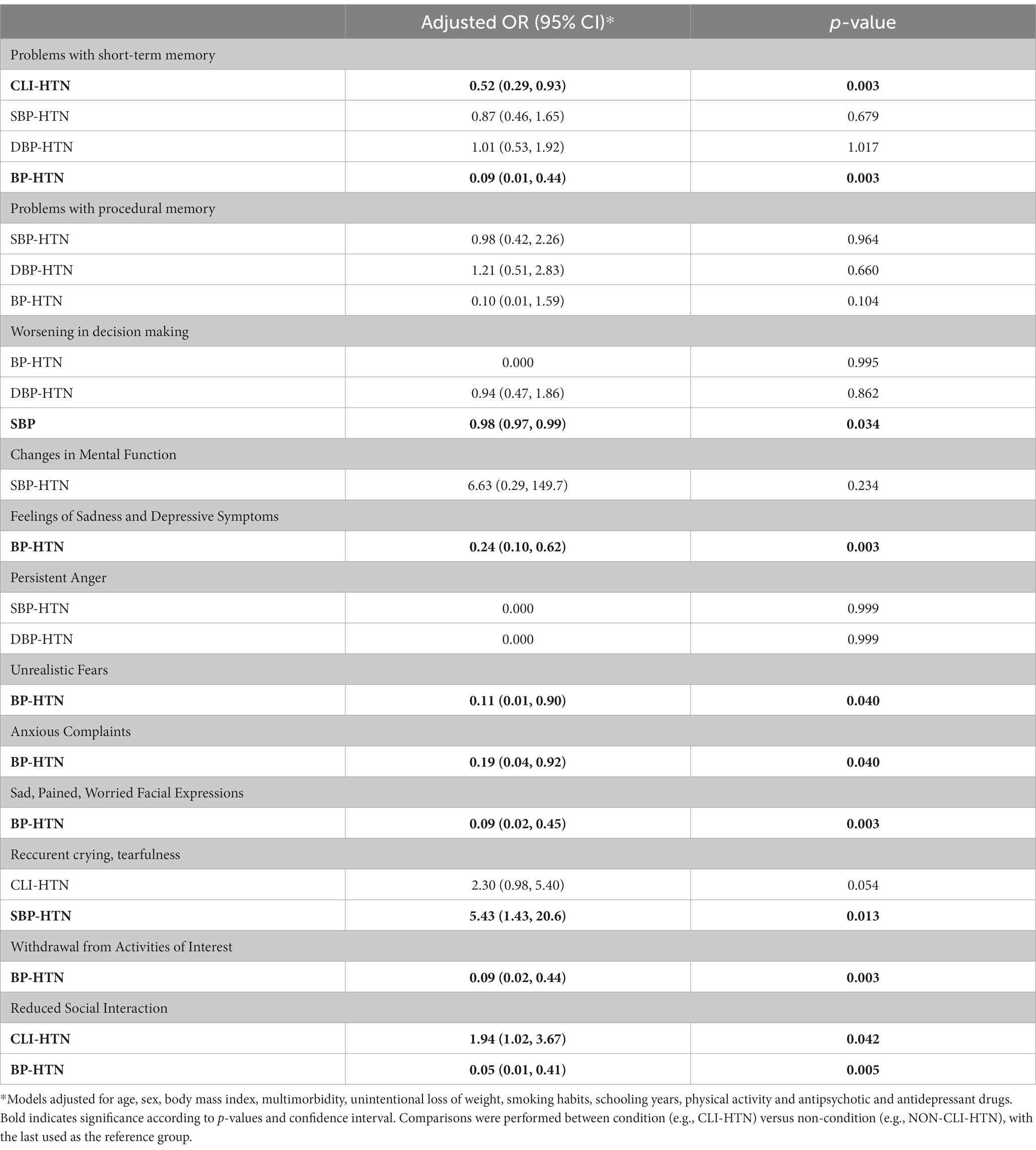
Table 3. Associations between hypertension-related parameters and cognitive aspects.
Table 4 shows binary regression results for the association between hypertension-related parameters and cognitive function, mood, and behavioral aspects according to ACEI use. After adjusting the analysis for ACEI use, only the associations between hypertension and lesser problems with short-term memory in CLI-HTN and BP-HTN remained significant.
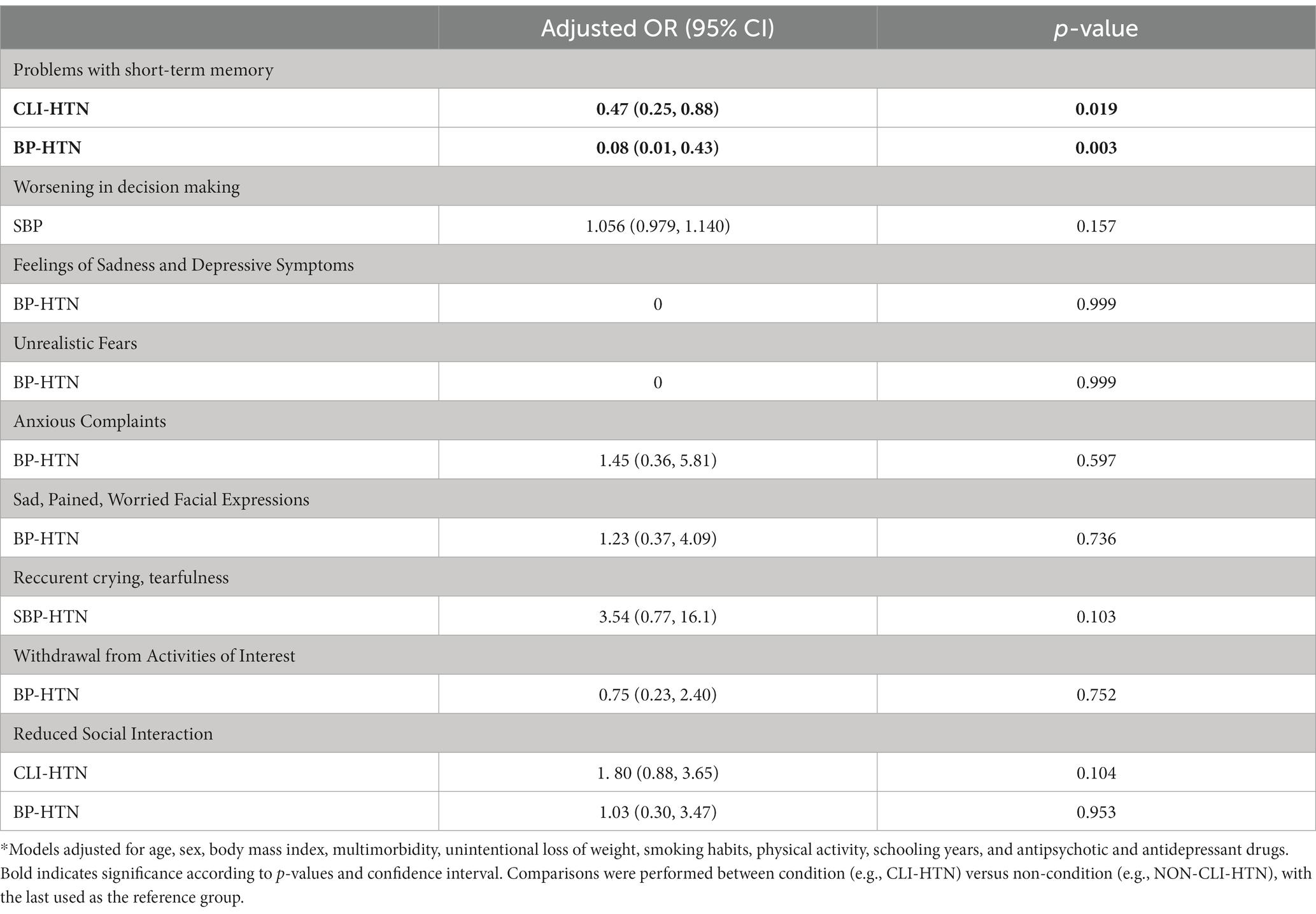
Table 4. Associations between hypertension-related parameters and cognitive aspects according to ACEI use.
Blood concentrations of inflammatory markers according to HTN are shown in Figure 1. Hypertensive participants in the BP-HTN group had lower IL-6 and CRP levels in comparison to normotensive peers. No other significant differences were observed.
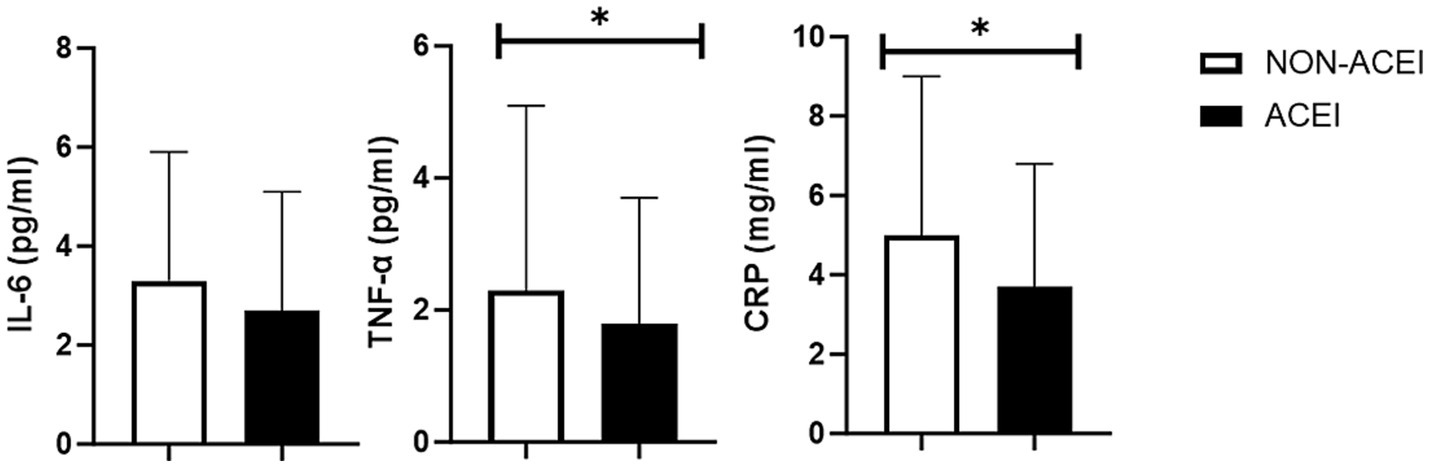
Figure 1. Blood concentration of interleukin 6 (IL-6), tumor necrosis factor alpha (TNF-α), and C-reactive protein according to the use of ACE-inhibitors. * p < 0.05.
4 Discussion
Findings of the present study indicate that HTN-related parameters are associated with many cognitive, mood, and behavioral aspects in very old adults. However, only associations with problems in short-term memory remained significant after adjusting the analysis for ACEI use. When possible candidate biomarkers to explain this scenario were examined, hypertensive participants, categorized according to BP values, had lower blood concentrations of IL-6 and CRP.
Our findings are partially supported by other studies that reported inverse associations between BP levels and cognitive function in very old adults. Nakamura et al. (6) found that high BP was a predictor of better global cognitive function 3 years later in a cohort of very old Japanese adults. Similar results were reported by Corrada et al. (7) and Chen et al. (26) after examining North American and Japanese older adults aged 90 years and older, respectively. Ruitenberg et al. (8) observed that lower systolic and diastolic BP values at baseline were associated with a higher risk of dementia in Dutch older adults. Another important finding was that reductions in BP during the follow-up were associated with the occurrence of dementia (8). Verghese et al. (9) followed up older adults over a median of 6.7 years and observed that each 10-mmHg decrement in BP was associated with a significant increase in the risk of dementia. Furthermore, individuals with mild to moderate systolic hypertension had a reduced risk of developing AD compared white those with normal BP (9). These findings were expanded by Li et al. (27), who showed that the association between BP and cognitive deterioration varies with age, given that high BP was a significant predictor of dementia in young older adults (approximately 60–70 years), whereas a negative association among these factors were found in those very old (≥85 years).
A possible explanation for these findings is that high BP might be a compensatory mechanism to maintain adequate cerebral perfusion in the face of vascular detriments caused by aging (6–9). Indeed, the old vessel is commonly characterized by losses in structural integrity and function, which involves significant impairment of endothelium dilation, resulting in reduced blood flow to major tissues, including the brain (28–30). In preclinical models, low cerebral blood flow (CBF) destroys the blood–brain barrier ultrastructure, causes microglial activation, increases the expression of proinflammatory markers, provokes overexpression of β-amyloid precursor protein, and reduces spatial learning and memory abilities (31–33).
Low CBF, regardless of the brain region affected, is associated with a higher risk of cognitive decline in hypertensive people and in mixed samples (34, 35). Furthermore, hypoperfusion of the medial temporal and posterior cingulate cortexes is found in individuals with memory impairments (35). In contrast, a high CBF is associated with greater hippocampal and amygdalar volumes and lower dementia risk (35). This scenario led experts in the field to propose the vascular hypothesis of AD, an alternative or complementary (or even substitutive) view to the classical neurodegenerative disorder model, in which it is stated that chronic insufficient brain perfusion underlies the metabolic and physiopathological aspects of AD (36).
Another important result of the present study was that hypertension-related parameters were no longer significantly associated with many cognitive, mood, and behavioral aspects when analyses were further adjusted for ACEI use. ANGII might contribute to cognitive decline and mood alteration by affecting cerebral structure and function. ANGII reduces CBF in response to vasodilator agents (e.g., bradykinin), disrupts the integrity of the blood–brain barrier, causes loss of pericytes and capillaries, and increases the cleavage of the amyloid precursor protein and amyloid deposition (12–14). This scenario induces microglia activation (13) and increases the expression of inflammatory and oxidative stress markers in brain cells (12, 13, 37). Although these changes have been noted in both young and old animals, aging exacerbates the effects of ANGII-induced hypertension on cerebral dysfunction (13).
On the other hand, ACEIs increase CBF, maintain the integrity of white and gray matter, reduce the presence and expression of inflammatory and oxidative markers in the brain, and increase neurotrophins levels (15–17). Furthermore, a growing number of investigations have reported that ACEI treatment might improve traits of cognitive dysfunction and psychiatric diseases in animal models, including immobility time, social deficits, and spatial learning (17, 38). In humans, those on ACEI treatment have a lower risk of cognitive decline, MCI, and AD (3–5). These results have been confirmed by systematic reviews and meta-analyses (33, 34). Regarding psychiatric aspects, individuals taking ACEI were at a lower risk of admission due to mood disorders in comparison to their peers taking other antihypertensive medications (35).
Taken together, these findings suggest that hypertensive participants on ACEI treatment might have fewer complaints about cognitive, mood, and behavioral problems in comparison to their counterparts taking other antihypertensive drugs. Such results could be mediated by the effects of ACEI on inflammatory markers (12, 13, 37) and explain the lower blood concentrations of IL-6 and CRP found in hypertensive older adults of the BP-HTN group. However, when we compared hypertensive ACEI users and non-users, significant differences in the agitation and disorientation item were observed (Supplementary Table S2). These findings suggest that other parameters might have influenced inflammation and better cognitive function in the hypertensive group (35). Nevertheless, the small sample size (<200 participants) and the lack of adjustments for covariates indicate that results should be carefully extrapolated and that more studies examining this scenario are still needed.
The present study is not free of limitations. First, cognitive, mood, and behavioral aspects were assessed using self-reported instruments, and no specific screening and diagnosis instruments were used. Second, results were not adjusted according to the onset of HTN (7). Third, participants were not screened according to the presence of the apolipoprotein E4 allele, which might influence our results (36). Fourth, blood concentrations of other possible mediators (e.g., reactive oxygen species) were not measured. Fifth, other aspects of ACEI treatment, such as dosage, duration, and adherence were not recorded (37, 38). Sixth, it is possible that the effects of ACEI on cognitive function are mediated by their capacity to cross the blood–brain barrier. This information was only available for some participants of the present study which prevented us from conducting further analysis. Seventh, the cross-sectional design of the study does not allow any inference to be drawn on the time course of changes in the variables considered or on cause–effect relationships. Eight, data regarding adherence to the antihypertensive pharmacological therapy was not recorded. Ninth, no screening instruments (e.g., mini-mental state examination) were used to examine participants’ cognitive status. Tenth, the lack of a detailed description of the antihypertensive treatment (e.g., use of diuretics) prevented us from conducting deeper analyses. Eleventh, the use of an oscillometric device might have produced different results (39). Finally, we examined a cohort of very old adults who lived in a mountain region, and extrapolations to other groups should be made with caution.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Ethic Committee of the Università Cattolica del Sacro Cuore (Rome, Italy). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
HJC-J: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Writing – original draft, Writing – review & editing. RC: Conceptualization, Data curation, Formal analysis, Investigation, Writing – original draft. MT: Conceptualization, Investigation, Writing – original draft. AR: Investigation, Writing – review & editing. FL: Conceptualization, Formal analysis, Funding acquisition, Investigation, Methodology, Resources, Supervision, Writing – original draft, Writing – review & editing. AP: Conceptualization, Formal analysis, Investigation, Methodology, Writing – original draft, Writing – review & editing. EM: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Resources, Supervision, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Acknowledgments
The authors recognized support from the Italian Ministry of Health (Ricerca Corrente 2023). Authors would like to thank Claudia Palmegiani for her help with data management.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2023.1268983/full#supplementary-material
References
1. Williams, B, Mancia, G, Spiering, W, Rosei, EA, Azizi, M, Burnier, M, et al. 2018 ESC/ESH guidelines for the management of arterial hypertension. Eur Heart J. (2018) 39:3021–104. doi: 10.1093/EURHEARTJ/EHY339
2. Lloyd-Sherlock, P, Beard, J, Minicuci, N, Ebrahim, S, and Chatterji, S. Hypertension among older adults in low-and middle-income countries: prevalence, awareness and control. Int J Epidemiol. (2014) 43:116–28. doi: 10.1093/IJE/DYT215
3. Sink, KM, Leng, X, Williamson, J, Kritchevsky, SB, Yaffe, K, Kuller, L, et al. Angiotensin-converting enzyme inhibitors and cognitive decline in older adults with hypertension: results from the cardiovascular health study. Arch Intern Med. (2009) 169:1195–202. doi: 10.1001/ARCHINTERNMED.2009.175
4. Khachaturian, AS, Zandi, PP, Lyketsos, CG, Hayden, KM, Skoog, I, Norton, MC, et al. Antihypertensive medication use and incident Alzheimer disease: the Cache County study. Arch Neurol. (2006) 63:686–92. doi: 10.1001/ARCHNEUR.63.5.NOC60013
5. Solfrizzi, V, Scafato, E, Frisardi, V, Seripa, D, Logroscino, G, Kehoe, PG, et al. Angiotensin-converting enzyme inhibitors and incidence of mild cognitive impairment. The Italian longitudinal study on Aging. Age. (2013) 35:441–53. doi: 10.1007/S11357-011-9360-Z
6. Nakamura, Y, Kabayama, M, Godai, K, Tseng, W, Akasaka, H, Yamamoto, K, et al. Longitudinal association of hypertension and dyslipidemia with cognitive function in community-dwelling older adults: the SONIC study. Hypertens Res. (2023) 46:1829–39. doi: 10.1038/S41440-023-01271-5
7. Corrada, MM, Hayden, KM, Paganini-Hill, A, Bullain, SS, DeMoss, J, Aguirre, C, et al. Age of onset of hypertension and risk of dementia in the oldest-old: the 90+ study. Alzheimers Dement. (2017) 13:103–10. doi: 10.1016/J.JALZ.2016.09.007
8. Ruitenberg, A, Skoog, I, Ott, A, Aevarsson, O, Witteman, JCM, Lernfelt, B, et al. Blood pressure and risk of dementia: results from the Rotterdam study and the Gothenburg H-70 study. Dement Geriatr Cogn Disord. (2001) 12:33–9. doi: 10.1159/000051233
9. Verghese, J, Lipton, RB, Hall, CB, Kuslansky, G, and Katz, MJ. Low blood pressure and the risk of dementia in very old individuals. Neurology. (2003) 61:1667–72. doi: 10.1212/01.WNL.0000098934.18300.BE
10. Te Riet, L, Van Esch, JHM, Roks, AJM, Van Den Meiracker, AH, and Danser, AHJ. Hypertension: renin-angiotensin-aldosterone system alterations. Circ Res. (2015) 116:960–75. doi: 10.1161/CIRCRESAHA.116.303587
11. Oliveira Leite, AP, Li, XC, Hassan, R, Zheng, X, Alexander, B, Casarini, DE, et al. Sex differences in angiotensin II-induced hypertension and kidney injury: role of AT1a receptors in the proximal tubule of the kidney. Clin Sci (Lond). (2021) 135:1825–43. doi: 10.1042/CS20201574
12. Capone, C, Faraco, G, Park, L, Cao, X, Davisson, RL, and Iadecola, C. The cerebrovascular dysfunction induced by slow pressor doses of angiotensin II precedes the development of hypertension. Am J Physiol Heart Circ Physiol. (2011) 300:H397–407. doi: 10.1152/AJPHEART.00679.2010
13. Toth, P, Tucsek, Z, Sosnowska, D, Gautam, T, Mitschelen, M, Tarantini, S, et al. Age-related autoregulatory dysfunction and cerebromicrovascular injury in mice with angiotensin II-induced hypertension. J Cereb Blood Flow Metab. (2013) 33:1732–42. doi: 10.1038/JCBFM.2013.143
14. Faraco, G, Park, L, Zhou, P, Luo, W, Paul, SM, Anrather, J, et al. Hypertension enhances Aβ-induced neurovascular dysfunction, promotes β-secretase activity, and leads to amyloidogenic processing of APP. J Cereb Blood Flow Metab. (2016) 36:241–52. doi: 10.1038/JCBFM.2015.79
15. Wiesmann, M, Roelofs, M, van der Lugt, R, Heerschap, A, Kiliaan, AJ, and Claassen, JAHR. Angiotensin II, hypertension and angiotensin II receptor antagonism: roles in the behavioural and brain pathology of a mouse model of Alzheimer’s disease. J Cereb Blood Flow Metab. (2017) 37:2396–413. doi: 10.1177/0271678X16667364
16. Constantinescu, CS, Ventura, E, Hilliard, B, and Rostami, A. Effects of the angiotensin converting enzyme inhibitor captopril on experimental autoimmune encephalomyelitis. Immunopharmacol Immunotoxicol. (1995) 17:471–91. doi: 10.3109/08923979509016382
17. Beheshti, F, Akbari, HR, Baghcheghi, Y, Mansouritorghabeh, F, Mortazavi Sani, SS, and Hosseini, M. Beneficial effects of angiotensin converting enzyme inhibition on scopolamine-induced learning and memory impairment in rats, the roles of brain-derived neurotrophic factor, nitric oxide and neuroinflammation. Clin Exp Hypertens. (2021) 43:505–15. doi: 10.1080/10641963.2021.1901112
18. Landi, F, Russo, A, Cesari, M, Barillaro, C, Onder, G, Zamboni, V, et al. The ilSIRENTE study: a prospective cohort study on persons aged 80 years and older living in a mountain community of Central Italy. Aging Clin Exp Res. (2005) 17:486–93. doi: 10.1007/BF03327416
19. Morris, JN, Fries, BE, Steel, K, Ikegami, N, Bernabei, R, Carpenter, GI, et al. Comprehensive clinical assessment in community setting: applicability of the MDS-HC. J Am Geriatr Soc. (1997) 45:1017–24. doi: 10.1111/J.1532-5415.1997.TB02975.X
20. Chen, J, Chen, X, Mao, R, Fu, Y, Chen, Q, Zhang, C, et al. Hypertension, sleep quality, depression, and cognitive function in elderly: a cross-sectional study. Front Aging Neurosci. (2023) 15:1051298. doi: 10.3389/FNAGI.2023.1051298
21. Li, G, Rhew, IC, Shofer, JB, Kukull, WA, Breitner, JCS, Peskind, E, et al. Age-varying association between blood pressure and risk of dementia in those aged 65 and older: a community-based prospective cohort study. J Am Geriatr Soc. (2007) 55:1161–7. doi: 10.1111/J.1532-5415.2007.01233.X
22. Toda, N. Age-related changes in endothelial function and blood flow regulation. Pharmacol Ther. (2012) 133:159–76. doi: 10.1016/J.PHARMTHERA.2011.10.004
23. El Assar, M, Angulo, J, Vallejo, S, Peiró, C, Sánchez-Ferrer, CF, and Rodríguez-Mañas, L. Mechanisms involved in the aging-induced vascular dysfunction. Front Physiol. (2012) 3:132. doi: 10.3389/FPHYS.2012.00132
24. El Assar, M, Angulo, J, and Rodríguez-Mañas, L. Oxidative stress and vascular inflammation in aging. Free Radic Biol Med. (2013) 65:380–401. doi: 10.1016/J.FREERADBIOMED.2013.07.003
25. Shi, J, Yang, SH, Stubley, L, Day, AL, and Simpkins, JW. Hypoperfusion induces overexpression of beta-amyloid precursor protein mRNA in a focal ischemic rodent model. Brain Res. (2000) 853:1–4. doi: 10.1016/S0006-8993(99)02113-7
26. Wang, Z, Li, T, Du, M, Zhang, L, Xu, L, Song, H, et al. β-Hydroxybutyrate improves cognitive impairment caused by chronic cerebral hypoperfusion via amelioration of neuroinflammation and blood-brain barrier damage. Brain Res Bull. (2023) 193:117–30. doi: 10.1016/J.BRAINRESBULL.2022.12.011
27. Li, T, Zheng, J, Wang, Z, Xu, L, Sun, D, Song, H, et al. Maresin 1 improves cognitive decline and ameliorates inflammation and blood-brain barrier damage in rats with chronic cerebral hypoperfusion. Brain Res. (2022) 1788:) 1788:147936. doi: 10.1016/J.BRAINRES.2022.147936
28. Kitagawa, K, Oku, N, Kimura, Y, Yagita, Y, Sakaguchi, M, Hatazawa, J, et al. Relationship between cerebral blood flow and later cognitive decline in hypertensive patients with cerebral small vessel disease. Hypertens Res. (2009) 32:816–20. doi: 10.1038/HR.2009.100
29. Ruitenberg, A, Den Heijer, T, Bakker, SLM, Van Swieten, JC, Koudstaal, PJ, Hofman, A, et al. Cerebral hypoperfusion and clinical onset of dementia: the Rotterdam study. Ann Neurol. (2005) 57:789–94. doi: 10.1002/ANA.20493
30. De La Torre, JC. Is Alzheimer’s disease a neurodegenerative or a vascular disorder? Data, dogma, and dialectics. Lancet Neurol. (2004) 3:184–90. doi: 10.1016/S1474-4422(04)00683-0
31. Watanabe, K, Taniguchi, M, Miyoshi, M, Shimizu, H, Imoto, T, Sato, K, et al. Effects of central injection of angiotensin-converting-enzyme inhibitor and angiotensin type 1 receptor antagonist on the brain NF-kappa B and AP-1 activities of rats given LPS. Peptides. (2006) 27:1538–46. doi: 10.1016/J.PEPTIDES.2005.11.005
32. Luo, H, Wu, PF, Cao, Y, Jin, M, Shen, TT, Wang, J, et al. Angiotensin-converting enzyme inhibitor rapidly ameliorates depressive-type behaviors via bradykinin-dependent activation of mammalian target of rapamycin complex 1. Biol Psychiatry. (2020) 88:415–25. doi: 10.1016/J.BIOPSYCH.2020.02.005
33. Shah, K, Qureshi, SU, Johnson, M, Parikh, N, Schulz, PE, and Kunik, ME. Does use of antihypertensive drugs affect the incidence or progression of dementia? A systematic review. Am J Geriatr Pharmacother. (2009) 7:250–61. doi: 10.1016/J.AMJOPHARM.2009.11.001
34. Ding, J, Davis-Plourde, KL, Sedaghat, S, Tully, PJ, Wang, W, Phillips, C, et al. Antihypertensive medications and risk for incident dementia and Alzheimer’s disease: a meta-analysis of individual participant data from prospective cohort studies. Lancet Neurol. (2020) 19:61–70. doi: 10.1016/S1474-4422(19)30393-X
35. Boal, AH, Smith, DJ, McCallum, L, Muir, S, Touyz, RM, Dominiczak, AF, et al. Monotherapy with major antihypertensive drug classes and risk of hospital admissions for mood disorders. Hypertension. (2016) 68:1132–8. doi: 10.1161/HYPERTENSIONAHA.116.08188
36. Qiu, WWQ, Lai, A, Mon, T, Mwamburi, M, Taylor, W, Rosenzweig, J, et al. Angiotensin converting enzyme inhibitors and Alzheimer disease in the presence of the apolipoprotein E4 allele. Am J Geriatr Psychiatry. (2014) 22:177–85. doi: 10.1016/J.JAGP.2012.08.017
37. Gray, SL, Aragaki, AK, Lamonte, MJ, Cochrane, BB, Kooperberg, C, Robinson, JG, et al. Statins, angiotensin-converting enzyme inhibitors, and physical performance in older women. J Am Geriatr Soc. (2012) 60:2206–14. doi: 10.1111/JGS.12029
38. Di Bari, M, Van De Poll-Franse, LV, Onder, G, Kritchevsky, SB, Newman, A, Harris, TB, et al. Health, aging and body composition study. Antihypertensive medications and differences in muscle mass in older persons: the health, aging and body composition study. J Am Geriatr Soc. (2004) 52:961–6. doi: 10.1111/j.1532-5415.2004.52265.x
Keywords: cardiovascular disease, antihypertensive drugs, cognitive function, psychiatric disorders, depression, mood, aged
Citation: Coelho-Junior HJ, Calvani R, Tosato M, Russo A, Landi F, Picca A and Marzetti E (2024) Associations between hypertension and cognitive, mood, and behavioral parameters in very old adults: results from the IlSIRENTE study. Front. Public Health. 11:1268983. doi: 10.3389/fpubh.2023.1268983
Edited by:
Yucong Zhang, Huazhong University of Science and Technology, ChinaReviewed by:
Warren Lockette, Wayne State University, United StatesJu Wang, Tianjin Medical University, China
Copyright © 2024 Coelho-Junior, Calvani, Tosato, Russo, Landi, Picca and Marzetti. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Helio José Coelho-Junior, Y29lbGhvanVuaW9yQGhvdG1haWwuY29tLmJy; Emanuele Marzetti, ZW1hbnVlbGUubWFyemV0dGlAcG9saWNsaW5pY29nZW1lbGxpLml0