 David Elvira1,2†
David Elvira1,2† Ferran Torres3*†
Ferran Torres3*† Roser Vives1,4†Gemma Puig4
Roser Vives1,4†Gemma Puig4 Mercè Obach2†Daniel Gay4Daniel Varón5Thais de Pando4,6Josep Tabernero7†
Mercè Obach2†Daniel Gay4Daniel Varón5Thais de Pando4,6Josep Tabernero7† Caridad Pontes1,3,6†
Caridad Pontes1,3,6†- 1Departament de Farmacologia, de Terapèutica i de Toxicologia, Universitat Autònoma de Barcelona, Sabadell, Barcelona, Spain
- 2Sanofi, Paris, France
- 3Biostatistics Unit, Medical School, Universitat Autònoma de Barcelona, Cerdanyola del Vallés, Barcelona, Spain
- 4Gerència del Medicament, Servei Català de la Salut, Barcelona, Spain
- 5Institut Català d’Oncologia, Barcelona, Spain
- 6Digitalization for the Sustainability of the Healthcare System (DS3), Servei Català de la Salut, Barcelona, Spain
- 7Vall d’Hebron Hospital Campus and Institute of Oncology (VHIO), Barcelona, Spain
Introduction: Even using well-established technology assessment processes, the basis of the decisions on drug price and reimbursement are sometimes perceived as poorly informed and sometimes may be seen as disconnected from value. The literature remains inconclusive about how Health Technology Assessment Bodies (HTAb) should report the determinants of their decisions. This study evaluates the relationship between oncology and hematology drug list prices and structured value parameters at the time of reimbursement decision in Spain.
Methods: The study includes all new onco-hematological products (22), with a first indication authorized between January 2017 and December 2019 in Spain and pricing decisions published up until October 2022. For each product, 56 contextual and non-contextual indicators reflecting the structured multiple criteria decision analysis (MCDA) – Evidence-based Decision-Making (EVIDEM) framework were measured. The relationship between prices and the MCDA-EVIDEM framework was explored using univariate statistical analyses.
Results: Higher prices were observed when the standard of care included for combinations, if there were references to long-lasting responses, for fixed-duration treatment compared to treatment until progression and treatment with lower frequencies of administration; lower prices were observed for oral administration compared to other routes of administration. Statistically significant associations were observed between prices and the median duration of treatment, the impact on patient autonomy, the ease of use of the drug, and the recommendations of experts.
Discussion: The study suggests that indicators related to the type of standard of care, references to long-lasting responders, the convenience of the use of the drug, and the impact of treatment on patient autonomy, as well as contextual indicators such as the existence of previous clinical consensus, are factors in setting oncology drug prices in Spain. The implementation of MCDA-EVIDEM methodologies may be useful to capture the influence on pricing decisions of additional factors not included in legislation or consolidated assessment frameworks such as the European Network for Health Technology Assessment (EunetHTA) core model. It may be opportune to consider this in the upcoming revision of the Spanish regulation for health technology assessments and pricing and reimbursement procedures.
1. Introduction
Concerns about the increasing cost of oncological and hematologic innovation in Europe are growing as prices of cancer drugs are high but not always related to a proportional improvement in patient health status (1). In Europe, the increase in the rate of health spending on cancer has been faster than the increase in cancer incidence during the last 20 years. Similarly, the loss of productivity related to premature cancer mortality has decreased, while productivity loss related to morbidity is still uncertain (2).
Progressively flexible regulatory criteria for authorization in the setting of precision medicine aims to accelerate market access decisions at the pricing and reimbursement process. Studies of authorization decisions in Europe have estimated that after monitoring post-authorization real-world evidence for 3.3 years, benefits on survival of those authorized drugs were only observed in 7% of cases, and improvement in reported quality of life was achieved in only 11% of them (3). A recent study (4) confirms that this trend is consolidated, and regulatory practice is biased toward earlier access at the expense of the production of post-authorization robust evidence, especially when the drug covers clinical unmet needs in diseases with poor prognosis (5). Pricing and reimbursement decisions are tough when evidence is scarce and lacking comparative data, risking opportunity costs (6). In order to minimize this, new access management models have been implemented across Europe during the last decades (7), although to a limited extent and with a lack of methodological harmonization (8). The increase in prices of oncologic products has generated additional international concerns (9) about the disconnection between price and value.
There is still an open debate in Europe about which are the adequate methods to assess the value of drugs (10). Methods of setting “fair prices” are generally focused on clinical benefits or expanded to the so-called value-based pricing, which is usually focused on cost-effectiveness analysis (11–13). Cancer drugs are normally classified as innovation based on implicit clinical value through Quality-Adjusted Life-Years – QALYS (e.g., United Kingdom, Australia, Sweden) or using innovation scales (e.g., Canada, Japan, France, Germany, Austria, Italy) (14). However, healthcare authorities do not normally unveil the details of the methodology applied to assess value, while new cancer drugs are increasingly reimbursed at a higher price than the available alternatives (15).
Recent studies (16) show that even in countries with well-established technology assessment processes (such as the UK, Germany, France, and Switzerland), prices may still be considered disconnected from value. In fact, in countries such as France, Australia, or the UK, prices are only weakly associated with drug clinical benefits (17–19).
Besides a lack of elements to check consistency between price and value, the literature remains inconclusive about the factors that Health Technology Assessment Bodies (HTAb) are using to make their decisions on value and how the payers are deciding and reporting price decisions, especially when applying managed entry agreements (20). Recent studies (21) show that EVIDEM’s framework provides a complete and suitable value assessment framework, including contextual dimensions, and it has been progressively adopted by some HTAb in Europe. Additionally, differences may exist in the concept of value between payers and patients: while payers are generally focused on objective clinical outcomes to determine reimbursement conditions, the importance of patient preferences is not clear (22, 23).
In Spain, the pricing and decision process starts after the European marketing authorization is formally adopted by the Spanish Agency of Medicines and Medical Devices (AEMPS) (24). Subsequently, a Therapeutic Positioning Report (TPR) is issued by the REvalMed network (25) to inform about the added therapeutic value of the drug compared to current therapeutic alternatives. The TPR includes a therapeutic evaluation from the AEMPS, an economic assessment from the General Directorate for Common Portfolio of the NHS and Pharmacy Services (DGCCSF), and a final technical revision by external experts and scientific societies appointed by the REvalMed network. The TPR, together with the application dossier filed by the marketing authorization holder and DGCCSF’s reports, is supposed to be the main driver for reimbursement decisions. The Inter-ministerial Committee on Pricing of Medicines and Healthcare Products (CIPM) is the body responsible for the final resolution of price and reimbursement conditions (26). The CIPM decision is published as a listed price (not net price) and motivation in general terms, which are based on the criteria listed in the RDL 1/2015, but the information provided by the Ministry of Health (MoH) is not detailed enough to know how the value of the drug has been established. It has been questioned whether the Spanish pricing model is based only on budgetary impact and lower European nominal price, without accounting for contextual criteria and societal needs.
Detailed information on how Spanish healthcare authorities define price and reimbursement conditions of new drugs is not available, and a lack of predictability, potentially leading to inconsistency between value and price, has been alleged (27, 28). The Royal Legislative Decree 1/2015 (RDL 1/2015) of the Law on Guarantees and Rational Use of Medicines and Health Products (29) lists only a restricted set of criteria to be used by the Spanish National Health System to establish prices of publicly funded medicines.
Based on recent data released by MoH (30), 90% of assessed oncologic medicines in Spain are publicly funded, with a listed price 15 times higher than the average price of new non-cancer-related drugs. By 2021, cancer drug costs represented 16.9% of the global pharmaceutical Spanish public budget, and the cost of cancer drugs at the hospital level has grown by 105.9% since 2016. The main objective of this study is to externally evaluate whether there is a relationship between the prices of oncology and hematology drugs and the evidentiary and contextual information available at the time of reimbursement decision in Spain by applying a structured assessment of parameters measuring drug value and to identify the most relevant criteria related to price decisions made by health authorities.
2. Materials and methods
All new chemical entities with a first EMA authorization for a single onco-hematologic indication between January 2017 and December 2019 were identified, and price and reimbursement decisions of the Spanish MoH, including the notified price and public funding authorization, were tracked based on the publicly available database Bifimed (31) and the resolutions published by the MoH up until the end of October 2022 (Supplementary Table 2).
For standardization and comparison purposes, a daily treatment cost based on notified prices was assigned following the Summary of Product Characteristics recommended posology for the studied indication. When the treatment duration was fixed, the cost was annualized. Products with a negative decision were assigned a price of zero; no other data imputation was applied.
For each product, a set of indicators from the MCDA-EVIDEM framework was used. A literature review was carried out to identify the indicators (32–36) for each MCDA-EVIDEM dimension (Table 1). The inclusion criteria for the review were articles published from January 2017 to December 2021 that included MCDA-EVIDEM-related indicators to assess onco-hematologic drugs as well as country legislation and HTAb official documents available in English or Spanish. The review did not include outdated documents. The indicators for each product were extracted from available European Public Assessment Report (EPAR), TPR (37), European Society of Medical Oncology-Magnitude of Clinical Benefit Scale (ESMO-MCBS) evaluations (38), National Institute for Health and Care Excellence (NICE) economic assessments (39), and freely available information from national and regional healthcare authorities (40). The indicators were informed by a stepwise approach including two independent reviewers for each product, and discrepancies were resolved through discussion. Public notified reimbursed prices per product (expressed as annual cost per treatment) were also included.
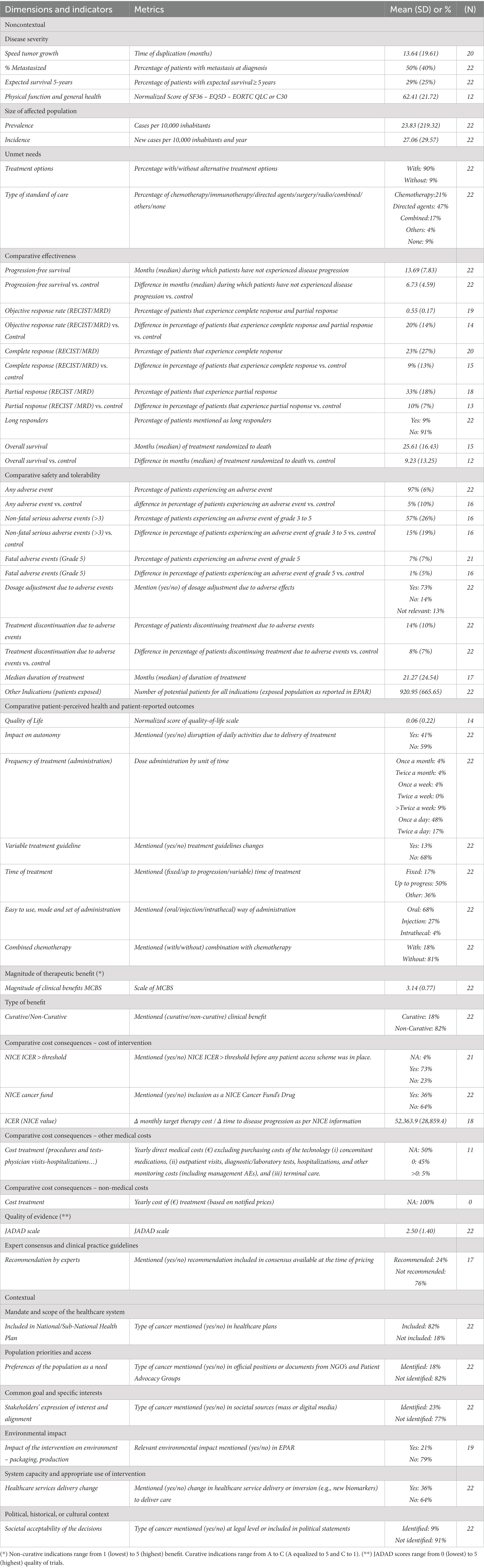
Table 1. Description of MCDA-EVIDEM dimensions and metrics.
Continuous variables for MCDA-EVIDEM dimension indicators were expressed as mean ± standard deviation, and categorical variables were expressed as percentages.
To evaluate the relation between oncology and hematology treatment prices and MCDA-EVIDEM indicators at the time of reimbursement decision, univariate analyses were performed. For correlation analyses, categories were normalized, summaries were calculated by dimension, and prices were categorized by terciles where required. To compare variables, the non-parametric Mann–Whitney test was used for continuous variables and the Fisher exact test was used for categorical variables. Spearman’s coefficients and 95% confidence intervals were calculated to assess correlations. The statistical definition was set at 5% two-tailed. The analysis was deemed exploratory, and, thus, no measures to account for multiplicity were applied.
3. Results
From January 2017 to December 2019, 24 oncological new chemical entities were granted a first indication marketing authorization in Europe. One product was excluded due to a conflict of interest in the team, and an adjuvant product for photodynamic therapy was deemed not suitable for the exercise (41) (Figure 1). Eventually, 22 products that aimed to treat 11 different tumors were analyzed. By October 2022, pricing and reimbursement had been granted for 18 products and denied for four products (Table 2). The most frequent indications were breast and lung cancer, and nine drugs had orphan designation (Table 2). Only two products had no therapeutic alternatives (in lung and agnostic indications) and roughly half of the products had targeted therapies as alternative options. Likewise, half of the treatments had an impact on patient autonomy (long intravenous administration, daycare admission), mostly in acute leukemia, lymphomas, melanoma, and neuroblastoma. Products for the treatment of melanoma, breast, neuroblastoma, and agnostic indications showed longer Progression Free Survival (PFS), observed and compared to control, over the median (14 months), and better Overall Survival (OS) vs. control was seen for products to treat leukemia and neuroblastoma. Most of the products were aimed at non-curative settings (19/22), with a moderate MCBS score (13/22 products under the score of 4) and low quality of evidence (17/22 products under a JADAD score of 3). Most did not require new healthcare service delivery routes (14/22) and were administered orally (15/22). Many had an Incremental Cost-Effectiveness Ratio (ICER) over the NICE threshold and were included in the NICE Cancer Drugs Fund (16/22), and most were related to cancers included in National or Regional Health Plans (18/22). More than half of the products (12/22) were explicitly recommended by expert consensus or included in clinical practice guidelines, while 4/22 products were explicitly not recommended (Table 1).
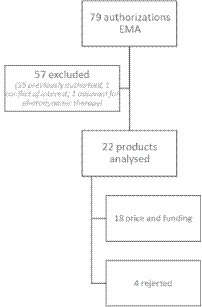
Figure 1. Product selection.
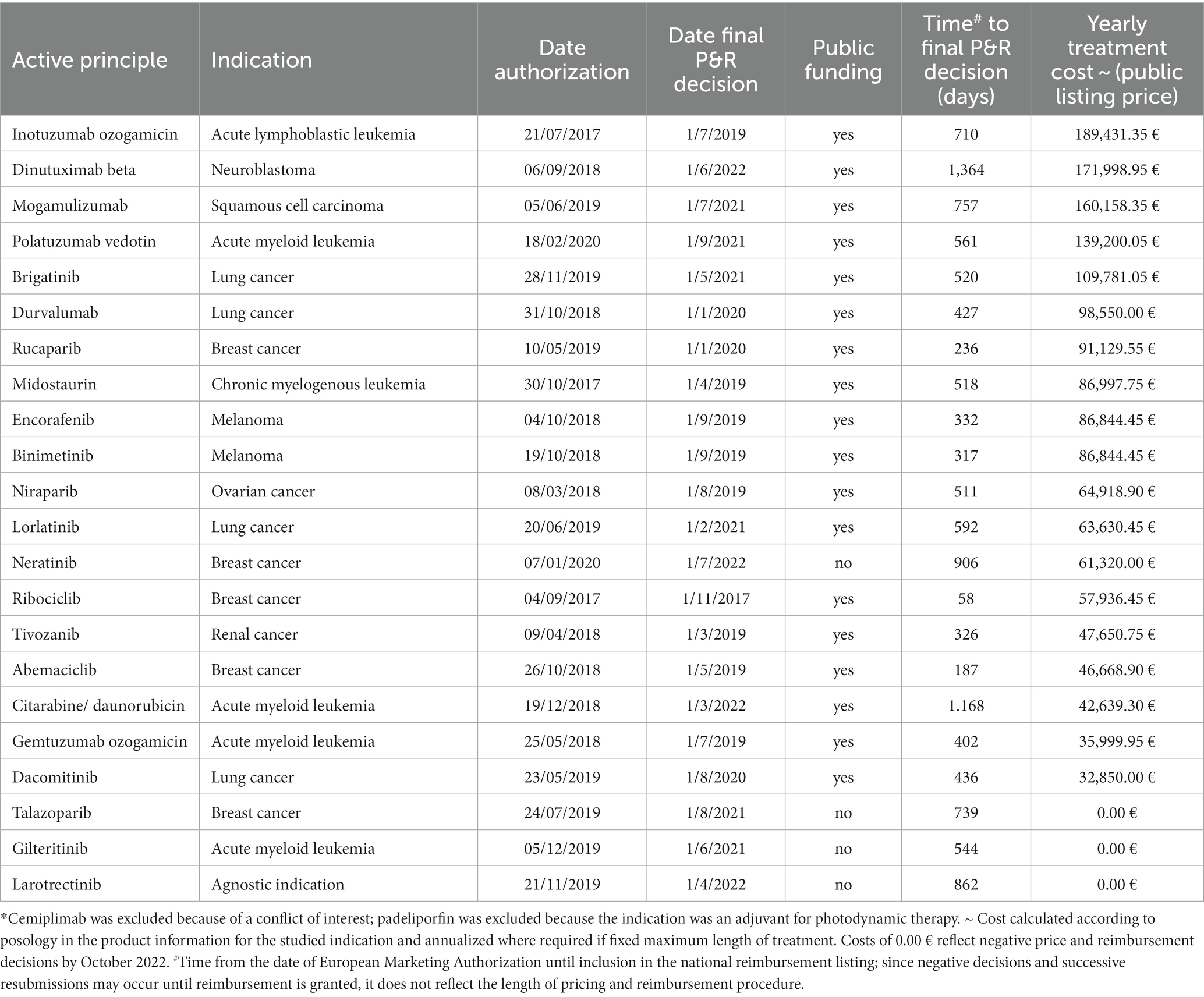
Table 2. Price and funding decisions by October 2022 for oncological products with first regulatory authorization* from January 2017 to December 2019.
The univariate analysis (Tables 3, 4) showed significantly higher listed prices when the standard of care was combined treatments, if long-lasting responders were reported, and for several characteristics of the treatment: higher prices for fixed-duration compared to treatment until progression and treatment with lower frequencies of administration, and lower prices for oral administration compared to other routes of administration. There were significant correlations between price and the ease of use of the drug, the impact of treatment on patient autonomy, and the existence of recommendations by experts. Regarding summaries by dimensions, the only association with price values was observed for the “expert consensus/clinical practice guidelines recommendations” dimension that contained a single item.
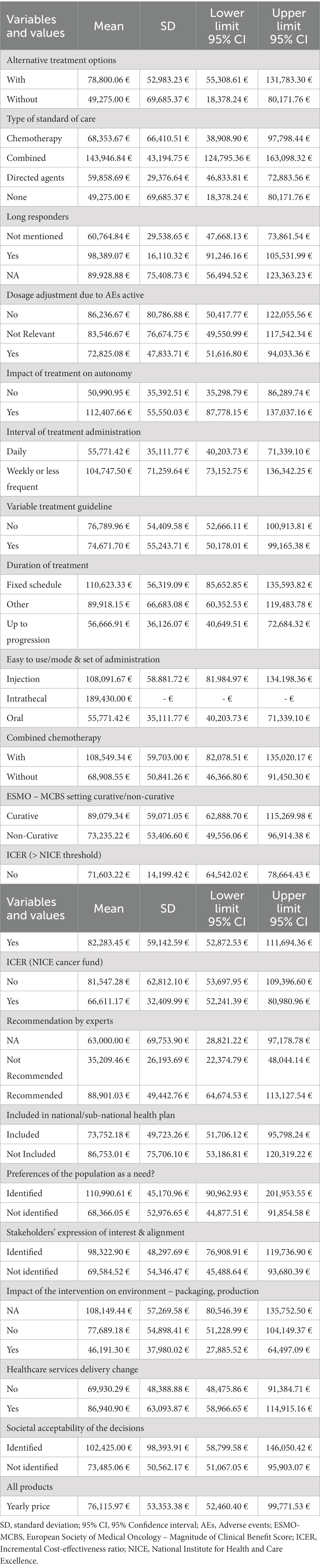
Table 3. Description of the mean (SD) listed yearly prices of oncology drugs according to the values of MCDA categorical items.
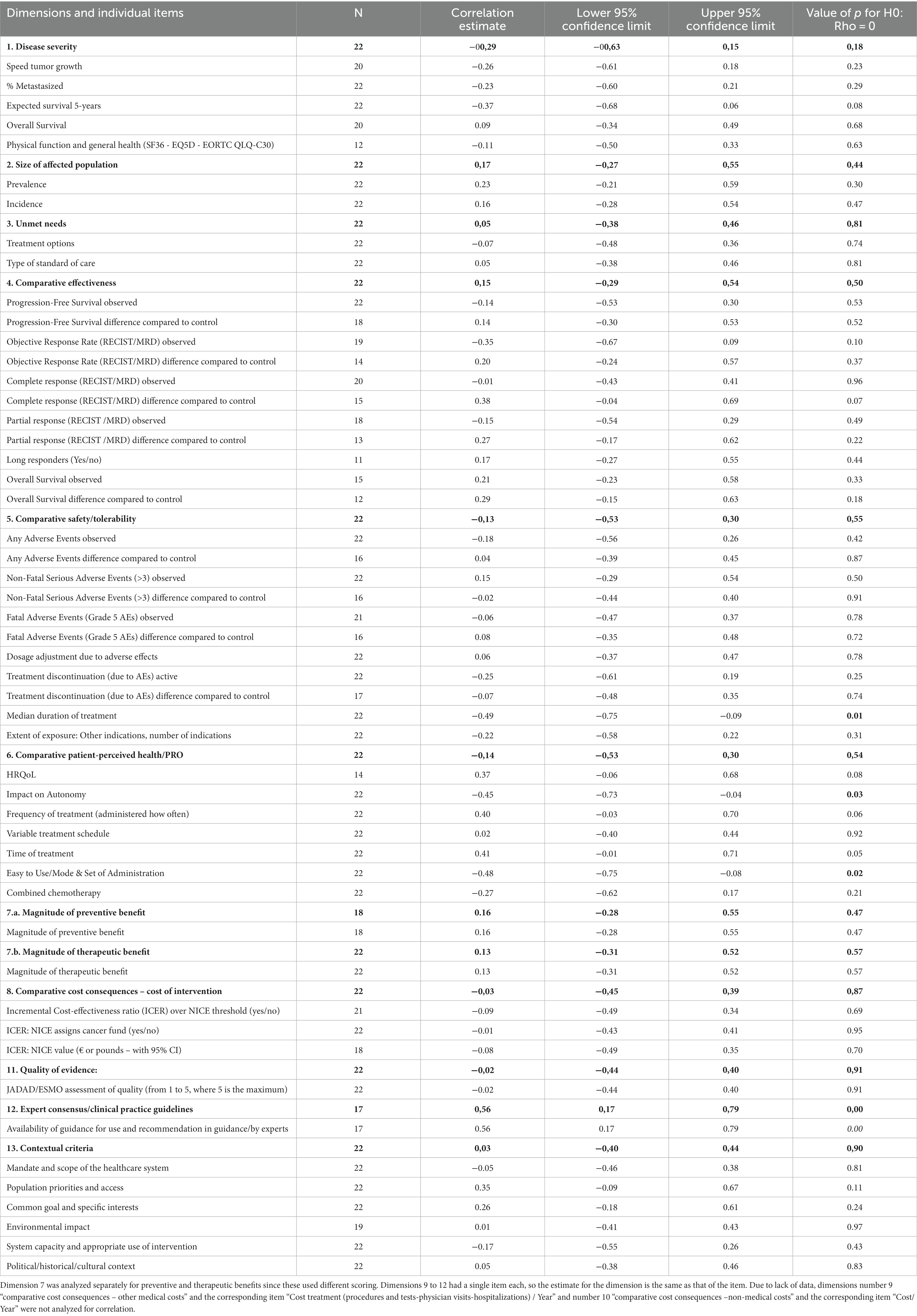
Table 4. Univariate analysis of the association between listed prices of oncology drugs and the dimensions of MCDA and subitems within each dimension.
4. Discussion
Our findings suggest that the initial price of oncology and hematology products tends to be influenced (higher prices) only by a few variables: the type of standard of care, the reporting of long-lasting responders, the convenience of use of drugs, the impact on patient autonomy, a limited duration of treatment, and contextual indicators such as the existence of previous clinical consensus. None of the individual items for comparative efficacy, safety, or quality of life reached significance for price correlation. Attempts to summarize values by dimensions compared to descriptions of individual items did not improve the explanation of price differences. However, the lack of standardized metrics and harmonized interpretation of contextual indicators limits the interpretation of the results.
The main limitation to moving forward with more transparent and standardized drug pricing processes is the lack of shared convention about the definition of “price” as an expression of “value” (1). For example, concepts such as quality-adjusted life years (to standardize health gains) do not capture the social perception of health benefits when the life expectancy of diseases differs (42). Additionally, price-setting processes are conditioned by available and previous therapeutic alternatives, influencing prices of pharmaceutical innovation based on historical inertia and baseline costs of the disease for the system (43). Additionally, dose, posology, and treatment duration add complexity to the direct comparison of value-based prices of new drugs.
There is a diversity of standardized clinical outcomes (overall survival, progression-free survival, quality of life, and safety) that medical societies and European healthcare authorities (38) are using to guide or define reimbursement conditions of oncology drugs (44). Other reports (17, 19–21, 23, 45) suggest that perceived additional therapeutic benefits based on weak variables (such as response rates) or perception of severity (when this is measured) may be driving oncology drug prices. In our data, these clinical variables and “hard” variables such as overall survival were not good pricing predictors. However, we observed higher prices for products reporting references to long-lasting responders. Furthermore, our research also shows that other intermediate indicators such as PFS, generally accepted as indicators of the capacity of a drug to cure or alter the natural history of the disease (46), were not strong predictors of prices either. The lack of consistent evidence based on long-term efficacy data or relative efficacy data of new drugs vs. frequently used drugs at the time of price negotiations does not seem to have any penalty on the price and reimbursement decisions in Spain. The study also suggests the influence of contextual indicators, such as the existence of expert consensus and the impact of the route of administration to patients, on setting prices.
Several limitations of the study should be considered. Firstly, only a few new oncology drugs authorized for a first indication were analyzed. The influence that multiple indications may have in price negotiations requires further analysis. Secondly, the value assessment was made by evaluators working in the context of payers of healthcare services, so that may not fully reflect the perspectives of pricing and reimbursement decision-making. Third, we did not calculate summary indicators or overall scores for MCDA-EVIDEM, as suggested by others (43), since the exercise aimed to verify whether a more transparent reporting of the criteria used for decisions may help all stakeholders to predict the key determinants of value and to support the expectations of manufacturers, the information given to the lay public, and the consistency of the decision-making by authorities. Finally, we did not run a systematic search of the literature using a diverse range of databases to identify all potential studies analyzing the relationship between prices and the MCDA-EVIDEM framework, and there is a scarcity of references available on methods and definitions for data extraction and analysis; therefore, we cannot exclude that our work may be influenced by publication biases.
Our work may provide a basis for some proposals in the context of upcoming regulations and changes in Health Technology Assessments. The new European regulation (47) states that inclusive joint clinical assessments able to respond to all Member States’ requirements must be produced at the EU level, ideally through consensus, and become part of multi-step national procedures. This new regulation enhances, in this way, the relevance of multiple domains (clinical, social, or economic) of assessment in the process of decision-making by national price and reimbursement organisms, EVIDEM being a solid starting point. From this perspective, further research is needed to standardize measures and determine the socially acceptable weights among EVIDEM dimensions, as well as its translation into economic values by dimension. So far, very limited experiences (48) have been tested with this broader approach aimed at more transparent and fair pricing but there is still a lack of solutions to tackle additional limitations, such as a potential disincentive effect on R&D efficiency discouraging future disruptive innovation.
5. Conclusion
Our exercise shows that, regardless of the paucity of explicative criteria on the decisions, the use of a standardized multidimensional framework allowed us to identify that the listed prices of new cancer products with a single first reimbursed indication in Spain are related to the type of standard of care, references to long-lasting responses, the convenience of use of the drug, and its impact on patient’s autonomy, as well as contextual indicators such as the existence of previous clinical consensus. While individual items are relatively explanatory, grouping by the synthetic MCDA-EVIDEM dimensions does not improve explicative value or information.
Based on our results and the lack of detailed information on how Spanish healthcare authorities define price and reimbursement conditions of new onco-hematologic drugs, we propose that the implementation of MCDA-EVIDEM methodologies may help to capture and report additional factors generally not included in consolidated assessment frameworks, such as the European Network for Health Technology Assessment (EunetHTA) core model. It may be opportune to consider this in the upcoming revision of the Spanish regulation for health technology assessments and pricing and reimbursement procedures (49).
Data availability statement
The datasets presented in this study can be found in online repositories. The names of the repository/repositories and accession number(s) can be found in the article/Supplementary material.
Author contributions
DE: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Resources, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. FT: Conceptualization, Data curation, Investigation, Methodology, Validation, Writing – review & editing. RV: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Validation, Writing – review & editing. GP: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Validation, Writing – review & editing. MO: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Validation, Writing – review & editing. DG: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Writing – review & editing. DV: Conceptualization, Data curation, Investigation, Methodology, Writing – review & editing. TP: Conceptualization, Data curation, Formal analysis, Investigation, Methodology. JT: Conceptualization, Supervision, Validation, Writing – review & editing. CP: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Supervision, Validation, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Conflict of interest
DE and MO are full-time employees of Sanofi. JT reports personal financial interest in the form of scientific consultancy roles for Array Biopharma, AstraZeneca, Bayer, Boehringer Ingelheim, Chugai, Daiichi Sankyo, F. Hoffmann-La Roche Ltd., Genentech Inc., HalioDX SAS, Hutchison MediPharma International, Ikena Oncology, Inspirna Inc., IQVIA, Lilly, Menarini, Merck Serono, Merus, MSD, Mirati, Neophore, Novartis, Ona Therapeutics, Orion Biotechnology, Peptomyc, Pfizer, Pierre Fabre, Samsung Bioepis, Sanofi, Scandion Oncology, Scorpion Therapeutics, Seattle Genetics, Servier, Sotio Biotech, Taiho, Tessa Therapeutics, TheraMyc, and Tolremo Therapeutics. Stocks: Oniria Therapeutics and educational collaboration with Imedex/HMP, Medscape Education, MJH Life Sciences, PeerView Institute for Medical Education, and Physicians Education Resource (PER).
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2023.1265323/full#supplementary-material
Abbreviations
AEMPS, Spanish Agency of Medicines and Medical Devices; CIPM, Inter-ministerial Committee on Pricing of Medicines and Healthcare Products; DGCCSF, General Directorate for Common Portfolio of the NHS and Pharmacy Services; EPAR, European Public Assessment Report; ESMO-MCBS, European Society of Medical Oncology-Magnitude of Clinical Benefit Scale; EUnetHTA, European Network for Health Technology Assessment; EVIDEM, Evidence and Value Impact on Decision-Making; HTAb, Health Technology Assessment Bodies; ICER, Incremental Cost-Effectiveness Ratio; MCDA, Multi-Criteria Decision Analysis; MoH, Ministry of Health; NHS, National Health Service; NICE, National Institute for Health and Care Excellence; OS, Overall Survival; PFS, Progression-Free Survival; QALYS, Quality-Adjusted Life-Years; TPR, Therapeutic Positioning Report.
References
1. Godman, B , Hill, A , Simoens, S , Selke, G , Selke Krulichová, I , Zampirolli Dias, C, et al. Potential approaches for the pricing of cancer medicines across Europe to enhance the sustainability of healthcare systems and the implications. Expert Rev Pharmacoecon Outcomes Res. (2021) 21:527–40. doi: 10.1080/14737167.1884546
2. Hofmarcher, T , Lindgren, P , Wilking, N , and Jönsson, B . The cost of cancer in Europe 2018. Eur J Cancer. (2020) 129:41–9. doi: 10.1016/j.ejca.2020.01.011
3. Davis, C , Naci, H , Gurpinar, E , Poplavska, E , Pinto, A , and Aggarwal, A . Availability of evidence of benefits on overall survival and quality of life of cancer drugs approved by European medicines agency: retrospective cohort study of drug approvals 2009-13. BMJ (Clinical Res Ed). (2017) 359:j4530. doi: 10.1136/bmj.j4530
4. Falcone, R , Lombardi, P , Filetti, M , Duranti, S , Pietragalla, A , Fabi, A, et al. Oncologic drugs approval in Europe for solid tumors: overview of the last 6 years. Cancers (Basel). (2022) 14:889. doi: 10.3390/cancers14040889
5. Pontes, C , Zara, C , Torrent-Farnell, J , Obach, M , Nadal, C , Vella-Bonanno, P, et al. Time to review authorisation and funding for new Cancer medicines in Europe? Inferences from the case of Olaratumab. Appl Health Econ Health Policy. (2019) 18:5–16. doi: 10.1007/s40258-019-00527-x
6. Godman, B , Malmstrom, RE , Diogene, E , Gray, A , Jayathissa, S , Timoney, A, et al. Are new models needed to optimize the utilization of new medicines to sustain healthcare systems? Expert Rev Clin Pharmacol. (2015) 8:77–94. doi: 10.1586/17512433.2015.990380
7. Pauwels, K , Huys, I , Vogler, S , Casteels, M , and Simoens, S . Managed entry agreements for oncology drugs: lessons from the European experience to inform the future. Front Pharmacol. (2017) 8:171. doi: 10.3389/fphar.2017.00171
8. Piatkiewicz, TJ , Traulsen, JM , and Holm-Larsen, T . Risk-sharing agreements in the EU: a systematic review of major trends. Pharmacoecon Open. (2018) 2:109–23. doi: 10.1007/s41669-017-0044-1
9. WHO . Technical report: Pricing of cancer medicines and its impacts. Geneva: World Health Organization (2018).
10. Uyl-de Groot, CA , and Löwenberg, B . Sustainability and affordability of cancer drugs: a novel pricing model. Nat Rev Clin Oncol. (2018) 15:405–6. doi: 10.1038/s41571-018-0027-x
11. Chandra, A , Shafrin, J , and Dhawan, R . Utility of cancer value frameworks for patients, payers, and physicians. JAMA. (2016) 315:2069–70. doi: 10.1001/jama.2016.4915
12. Tuffaha, H , Aitken, J , Chambers, S , and Scuffham, P . A framework to prioritise Health Research proposals for funding: integrating value for money. Appl Health Econ Health Policy. (2019) 17:761–70. doi: 10.1007/s40258-019-00495-2
13. Wilsdon, T , Attridge, J , and Fiz, E . Assessing the value of biopharmaceitical innovation in key therapy areas in middle-income countries. (2013). Available at: https://www.ifpma.org/publications/assessing-the-value-of-biopharmaceutical-innovation-in-key-therapy-areas-in-middle-income-countries/ (Accessed August 24, 2023).
14. Hidalgo-Vega, A. Evaluación, financiación y regulación de los medicamentos innovadores en los países desarrollados. Fundación Weber. (2018). Available at: https://weber.org.es/wp-content/uploads/2017/11/interactivo_informe_evaluacion_financiacion_y_regulacion_de_los_medicamentos_innovadores_en_los_paises_desarrollado.pdf (Accessed August 24, 2023).
15. Cohen, D . Cancer drugs: high price, uncertain value. BMJ. (2017) 359:j4543. doi: 10.1136/bmj.j4543
16. Vokinger, KN , Hwang, TJ , Grischott, T , Reichert, S , Tibau, A , Rosemann, T, et al. Prices and clinical benefit of cancer drugs in the USA and Europe: a cost–benefit analysis. Lancet Oncol. (2020) 21:664–70. doi: 10.1016/S1470-2045(20)30139-X
17. Russo, P , Marcellusi, A , Zanuzzi, M , Carletto, A , Fratto, ME , Favato, G, et al. Drug prices and value of oncology drugs in Italy. Value Health. (2021) 24:1273–8. doi: 10.1016/j.jval.2021.04.1278
18. Salas-Vega, S , Shearer, E , and Mossialos, E . Relationship between costs and clinical benefits of new cancer medicines in Australia, France, the UK, and the US. Soc Sci Med. (2020) 258:113042. doi: 10.1016/j.socscimed.2020.113042
19. Vogler, S , Paris, V , and Panteli, D . Ensuring access to medicines: How to redesign pricing, reimbursement, and procurement? Copenhagen: World Health Organization, Regional Office for Europe (2018).
20. Efthymiadou, O , and Kanavos, P . Determinants of managed entry agreements in the context of health echnology assessment: a comparative analysis of oncology therapies in four countries. Int J Technol Assess Health Care. (2021) 37:1–7. doi: 10.1017/S0266462321000039
21. Elvira, D , Obach, M , and Pontes, C . Description of the use of multicriteria to support pricing and reimbursement decisions by European health technology assessment bodies. BMC Health Serv Res. (2021) 21:814. doi: 10.1186/s12913-021-06784-8
22. Lorgelly, P , Pollard, J , Cubi-Molla, P , Cole, A , Sim, D , and Sussex, J . Outcome-based payment schemes: what outcomes do patients with Cancer value? Patient-Cent Outcomes Res. (2020) 13:599–610. doi: 10.1007/s40271-020-00430-x
23. Weiss, J , Kirchberger, MC , and Heinzerling, L . Therapy preferences in melanoma treatment—willingness to pay and preference of quality versus length of life of patients, physicians, healthy individuals, and physicians with oncological disease. Cancer Med. (2020) 9:6132–40. doi: 10.1002/cam4.3191
24. AEMPS. Agencia Española de Medicamentos y Productos Sanitarios (2021). Available at: https://www.aemps.gob.es/ (Accessed August 1, 2022).
25. Comisión Permanente de Farmacia (Reval Med-SNS) . Plan para la consolidación de los informes de posicionamiento terapéutico (IPT) de los medicamentos en el sistema nacional de salud (SNS), 1–16. (2020). Available at: https://www.sanidad.gob.es/profesionales/farmacia/IPT/docs/20201126._Preguntas_y_respuestas_Plan_Consolidacion_IPT.pdf (Accessed August 24, 2023).
26. de Espana, G . Comisión Interministerial de Precios De Medicamentos y Productos Sanitarios. (2022). Available at: https://www.sanidad.gob.es/profesionales/farmacia/CIPMyPS.htm (Accessed August 1, 2022).
27. Calleja, MA , and Badia, X . Feasibility study to characterize price and reimbursement decision-making criteria for the inclusion of new drugs in the Spanish National Health System: the cefiderocol example. Int J Technol Assess Health Care. (2022) 38:e48–9. doi: 10.1017/S0266462322000332
28. Epstein, D , and Espín, J . Evaluation of new medicines in Spain and comparison with other European countries. Gac Sanit. (2020) 34:133–40. doi: 10.1016/j.gaceta.2019.02.009
29. de Espana, G . Disposición 8343 del BOE núm. 177 de 2015 Real Decreto Legislativo 1/2015, de 24 de julio, por el que se aprueba el texto refundido de la Ley de garantías y uso racional de los medicamentos y productos sanitarios. (2015).
30. Dirección General de Cartera Común del SNS y farmacia . Informe evaluación de la financiación y fijación de precios de los medicamentos oncológicos en el SNS (2016–2021). (2022). Available at: https://www.sanidad.gob.es/profesionales/farmacia/pdf/20220402_Informe_Evol_SNS_Medicamentos_Oncologicos_L01L02_Def2.pdf (Accessed August 1, 2022).
31. Ministerio de Sanidad . Buscador de Información sobre la situación de FInanciación de los MEDicamentos en el SNS (BIFIMED). (2022). Available at: https://www.sanidad.gob.es/profesionales/medicamentos.do (Accessed October 21, 2022).
32. Angelis, A , Linch, M , Montibeller, G , Molina-Lopez, T , Zawada, A , Orzel, K, et al. Multiple criteria decision analysis for HTA across four EU member states: piloting the advance value framework. Soc Sci Med. (2020) 246:112595. doi: 10.1016/j.socscimed.2019.112595
33. Angelis, A , Montibeller, G , Hochhauser, D , and Kanavos, P . Multiple criteria decision analysis in the context of health technology assessment: a simulation exercise on metastatic colorectal cancer with multiple stakeholders in the English setting. BMC Med Inform Decis Mak. (2017) 17:149. doi: 10.1186/s12911-017-0524-3.2017
34. Hsu, JC , Lin, JY , Lin, PC , and Lee, YC . Comprehensive value assessment of drugs using a multi-criteria decision analysis: an example of targeted therapies for metastatic colorectal cancer treatment. PloS One. (2019) 14:e0225938. doi: 10.1371/journal.pone.0225938
35. Trotta, F , Mayer, F , Barone-Adesi, F , Esposito, I , Punreddy, R , da Cas, R, et al. Anticancer drug prices and clinical outcomes: a cross-sectional study in Italy. BMJ Open. (2019) 9:e033728. doi: 10.1136/bmjopen-2019-033728
36. Wagner, M , Samaha, D , Cuervo, J , Patel, H , Martinez, M , O'Neil, WM, et al. Applying reflective multicriteria decision analysis (MCDA) to patient–clinician shared decision-making on the Management of Gastroenteropancreatic Neuroendocrine Tumors (GEP-NET) in the Spanish context. Adv Ther. (2018) 35:1215–31. doi: 10.1007/s12325-018-0745-6
37. Agencia Española del Medicamento y Productos Sanitarios . Informes de Posicionamiento Terapéutico. (2022). Available at: https://www.aemps.gob.es/medicamentos-de-uso-humano/informes-de-posicionamiento-terapeutico/?lang=en Published online (August 2022).
38. ESMO (European Society of Medical Oncology) . Magnitude of clinical benefit scale. (2022). Available at: https://www.esmo.org/guidelines/esmo-mcbs Published online (August 2022).
39. NICE (National Institute for Health and Care Excellence) . Guidance on new and existing medicines and treatments in the NHS. (2022). Available at: https://www.nice.org.uk/guidance/published?ngt=Technology%20appraisal%20guidance&ndt=Guidance (Accessed August 1, 2022).
40. Goetghebeur, M , Wagner, M , Khoury, H , Levitt, R , Erickson, L , and Rindress, D . Evidence and value: impact on DEcisionMaking - the EVIDEM framework and potential applications. BMC Health Serv Res. (2008) 8:270. doi: 10.1186/1472-6963-8-270
41. Agencia Española del Medicamento y Productos Sanitarios . Centro de información online de medicamentos. (2022). Available at: https://cima.aemps.es/cima/publico/home.html (Accessed August 1, 2022).
42. Attema, AE , Brouwer, WB , and Pinto, JL . The role of perceived utility of full health in age weighting. Value Health. (2022) 25:1559–65. doi: 10.1016/j.jval.2022.04.1733
43. Okunade, AA , and Suraratdecha, C . The pervasiveness of pharmaceutical expenditure inertia in the OECD countries. Soc Sci Med. (2006) 63:225–38. doi: 10.1016/j.socscimed.2005.11.046
44. Kleijnen, S , Lipska, I , Leonardo Alves, T , Meijboom, K , Elsada, A , Vervölgyi, V, et al. Relative effectiveness assessments of oncology medicines for pricing and reimbursement decisions in European countries. Ann Oncol. (2006) 27:1768–75. doi: 10.1093/annonc/mdw233
45. Gandjour, A , Schüßler, S , Hammerschmidt, T , and Dintsios, CM . Predictors of negotiated prices for new drugs in Germany. Eur J Health Econ. (2020) 21:1049–57. doi: 10.1007/s10198-020-01201-z
46. Fortinguerra, F , Tafuri, G , Trotta, F , and Addis, A . Using GRADE methodology to assess innovation of new medicinal products in Italy. Br J Clin Pharmacol. (2020) 86:93–105. doi: 10.1111/bcp.14138
47. Directorate-General for Health and Food Safety of the European Comission . A pharmaceutical strategy for Europe. (2023). Available at: https://health.ec.europa.eu/publications/pharmaceutical-strategy-europe_en Publish online (February 2023). (Accessed August 17, 2023).
48. AIM . AIM proposes to establish a European drug pricing model for fair and transparent prices for accessible pharmaceutical innovations. (2019). Available at: https://www.aim-mutual.org/wp-content/uploads/2019/12/AIMfairpricingModel.pdf (Accessed August 24, 2023).
49. Ministerio de Sanidad. Consulta publica previa sobre el anteproyecto de ley que modifica el real decreto legislativo 1/2015, de 24 de julio, por el que se aprueba el texto refundido de la ley de garantias y uso racional de los medicamentos y productos sanitarios . Available at: https://www.sanidad.gob.es/normativa/docs/Documento_CPP_LGURM.pdf (Accessed February 1, 2023).
Keywords: health technology assessment, multicriteria assessment methods, price and reimbursement systems, onco-hematologic prices, value assessment
Citation: Elvira D, Torres F, Vives R, Puig G, Obach M, Gay D, Varón D, de Pando T, Tabernero J and Pontes C (2023) Reporting reimbursement price decisions for onco-hematology drugs in Spain. Front. Public Health. 11:1265323. doi: 10.3389/fpubh.2023.1265323
Edited by:
Jay J. Shen, University of Nevada, Las Vegas, United StatesReviewed by:
Tomas Tesar, Comenius University, SlovakiaIlda Hoxhaj, Agostino Gemelli University Polyclinic (IRCCS), Italy
Sherif Abaza, Syreon, Egypt
Copyright © 2023 Elvira, Torres, Vives, Puig, Obach, Gay, Varón, de Pando, Tabernero and Pontes. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ferran Torres, ZmVycmFuLnRvcnJlc0B1YWIuY2F0
†ORCID: David Elvira https://orcid.org/0000-0002-0567-9791
Ferran Torres https://orcid.org/0000-0002-7355-7913
Roser Vives https://orcid.org/0000-0002-4369-778X
Mercè Obach https://orcid.org/0000-0002-2756-6181
Josep Tabernero https://orcid.org/0000-0002-2495-8139
Caridad Pontes https://orcid.org/0000-0002-3274-6048