 Diana Morales-Jadán1
Diana Morales-Jadán1 Claire Muslin1
Claire Muslin1 Carolina Viteri-Dávila1Barbara Coronel1
Carolina Viteri-Dávila1Barbara Coronel1 Bernardo Castro-Rodríguez1
Bernardo Castro-Rodríguez1 Alexander Paolo Vallejo-Janeta1Aquiles Rodrigo Henríquez-Trujillo1
Alexander Paolo Vallejo-Janeta1Aquiles Rodrigo Henríquez-Trujillo1 Miguel Angel Garcia-Bereguiain1
Miguel Angel Garcia-Bereguiain1 Ismar A. Rivera-Olivero2*
Ismar A. Rivera-Olivero2*- 1One Health Research Group, Universidad de Las Américas, Quito, Ecuador
- 2One Health Research Group, Faculty of Medicine. Universidad de Las Américas, Quito, Ecuador
Worldwide, the COVID-19 pandemic caused by SARS-CoV-2 has enormously impacted healthcare systems, especially in low and middle-income countries. Coinfections with respiratory pathogens in COVID-19 patients may contribute to worse outcomes. This study identified the presence of 12 viral coinfections and pneumococcal carriers among individuals with SARS-CoV-2 infection in outpatient and community settings in Ecuador. From January 2020 to November 2021, 215 nasopharyngeal and nasal swabs were taken from individuals who reported symptoms of COVID-19 or had known exposure to someone with confirmed or suspected COVID-19. One hundred fifty-eight tested positive for SARS-CoV-2 by RT-qPCR and coinfections were detected in 12% (19/158) of SARS-CoV-2-positive patients; the most frequent coinfection was with influenza A virus at 4.4% (7/158; 95% CI: 1.2–7.6), followed by respiratory syncytial virus with 3.1% (5/158; 95% CI: 0.4–5.8), and finally rhinovirus and human coronavirus NL63 with 1.2% (2/158). Pneumococcal carriage was detected in 3.7% (6/158; 95% CI: 0.76–6.64) of SARS-CoV-2 cases. Influenza B, adenovirus, human metapneumovirus (HMPV), parainfluenza virus types 1, 2, and 3, and human coronavirus HKU1 were undetected. To our knowledge, this is the first study of coinfection of SARS-CoV-2 and respiratory pathogens performed on outpatients in Latin America. The high proportion of outpatients with viral coinfections reported in our cohort allows us to suggest that testing for SARS-CoV-2 and other common respiratory pathogens should be carried out to ensure accurate diagnoses, prompt patient treatment, and appropriate isolation.
1. Introduction
Coronavirus disease 2019 (COVID-19), caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), was first reported in China in December 2019 (1). In Ecuador, the first case was confirmed on February 29th, 2020 (2), and between February 2020 and May 2023, more than 732,038 cases and 34,533 deaths associated with SARS-CoV-2 were reported (3).
Patients infected with SARS-CoV-2 commonly develop symptoms 4–12 days after viral exposure. Clinical manifestations range from asymptomatic patients to mild symptoms to severe and critical illness. According to World Health Organization (WHO) clinical criteria for COVID-19 infection, signs or symptoms include fever, cough, fatigue, headache, myalgia, a sore throat, coryza, dyspnea, nausea, and diarrhea (4–6).
Despite the first report from China showed that coinfection with other respiratory pathogens was infrequent, with no other viruses detected and 1% of bacterial coinfection among 99 cases of COVID-19 (7), nowadays, several reports worldwide show evidence that the coinfection rates between SARS-CoV-2 and other viral and bacterial pathogens are higher than initially expected.
In a study conducted in Northern California, Kim et al. found that 20.7% of COVID-19 patients were co-infected with at least one other respiratory pathogen. Respiratory viruses are the most common co-infecting agents (8). In China, 5.8% of patients testing positive for COVID-19 also tested positive for other respiratory viruses (9).
A meta-analysis by Lansbury et al. revealed that common viral coinfections reported in patients positive for SARS-CoV-2 include influenza virus, respiratory syncytial virus (RSV), and adenovirus (10).
In addition, bacterial coinfection is more prevalent among hospitalized patients compared to outpatients, and significantly increases the risk of complications. A nationwide study in Spain performed in 2020 showed that 2.3% of hospitalized COVID-19 patients had bacterial coinfections, which increased to 17% among patients admitted to the intensive care unit (ICU). Pseudomonas spp., H. influenzae and S.pneumoniae were bacteria that caused most infections (11).
Overall, the proportion of bacterial coinfections in SARS-CoV-2 infected patients is estimated to range from 3 to 9% suggesting that bacterial coinfection in patients with COVID-19 is lower than in previous viral pandemics (10, 12–14). During the H1N1 influenza pandemic in 2009, fatal cases were associated with bacterial coinfections, particularly by S. pneumoniae (15–17). Reports of coinfection with S. pneumoniae during the COVID-19 pandemic range from 0.4 to 11%. Although the lower incidence of bacterial coinfection in COVID-19 patients is not fully understood as well as the impact of S. pneumoniae coinfections on COVID-19 severity and the possible interactions between SARS-CoV-2 and S. pneumoniae in the nasopharyngeal niche are still being investigated (18–20).
Nevertheless, most of these reports come from Europe, Asia, and the United States, whereas scarce data are available on COVID-19 and respiratory tract coinfections in Latin America. In Peru, two studies detected coinfection with respiratory pathogens in 52.2 and 40.86% of COVID-19 cases, respectively, at hospital admission. The most frequent pathogens were bacteria, while influenza viruses were not detected (21, 22). In Brazil, Pucarelli-Lebrerio et al. reported a 3.5% prevalence of viral coinfection in children diagnosed with COVID-19 infection (23).
The development of molecular tests has improved our ability to detect respiratory pathogens, providing an accurate and more sensitive detection of several pathogens in a faster turnaround time compared to viral and even bacterial cultures. It is a powerful tool because clinically differentiating between an isolated viral infection related to COVID-19 and a possible bacterial or fungal superinfection is challenging (24).
Providing information on both viral and bacterial coinfections associated with community-acquired pneumonia has diagnostic value that may be useful in predicting patient prognosis (8, 25–28) and initiating antiviral therapy (29). Coinfections may have clinical implications associated with increased complications, such as a severe inflammatory process leading to lung damage (30), an extended hospital stay (31), varied treatment approach and duration, and increased mortality rate. Therefore, early detection of coinfection will improve patient management.
In Ecuador, despite the presence of an integrated surveillance plan for COVID-19 and other respiratory viruses established by the National Reference Laboratory of the National Institute for Research and Public Health (INSPI), data on co-infection rates remain inaccessible (32). This study aims to address this gap by determining the prevalence of viral coinfections and pneumococcal carriers detected by molecular methods among outpatients with SARS-CoV-2 infection in Ecuador.
2. Materials and methods
2.1. Patient recruitment and sample collection
This cross-sectional study describes the prevalence of coinfection with other respiratory pathogens in SARS-CoV-2 infected patients in outpatient and community settings. From January 2020 to November 2021, we evaluated 215 individuals: 121 from hospital outpatient care (San Francisco de Quito, Eugenio Espejo and IESS Sur hospitals) and 94 from primary care settings and/or domiciliary assistance in Quito, Ecuador.
After physician evaluation all patients, regardless of age, who met the inclusion criteria and provided consent, were enrolled in the study, and nasopharyngeal swabs were collected. During the consultation, clinical and sociodemographic data were collected. Comorbidity was categorized according to the International Statistical Classification of Diseases and Problems Related to Health registered by the Pan-American Health Organization (PAHO).
The criteria for inclusion in the study were individuals who had not been hospitalized in the past 15 days at the time of sampling, reported symptoms of COVID-19, or had been exposed to someone with confirmed or suspected COVID-19.
2.2. Experimental analysis
All samples were processed in the BSL2-certified molecular biology laboratory at Universidad de Las Américas. Nasopharyngeal and nasal swabs were collected on 0.5 mL TE pH 8 buffer for SARS-CoV-2 diagnosis. All nasal or nasopharyngeal samples were divided into two. The first sample was submitted to a digestion step before DNA extraction and used for identifying S. pneumoniae. Nucleic acids were directly extracted from the second sample to detect SARS-CoV-2 and other respiratory viruses.
2.3. Digestion and nucleic acid extraction
Nasal and nasopharyngeal swabs were treated by a two-enzyme digestion process to break the S. pneumoniae capsule for 8 h before nucleic acid extraction and incubated at 36°C. 100 μL of TE buffer (10 mM Tris–HCl, 1 mM EDTA, pH 8.0) containing 0.04 g/mL lysozyme (Sigma) and 75 U/mL mutanolysin (Sigma) were added to 200 μL of the sample (33, 34). Virus DNA and RNA were simultaneously extracted using Spin Column Extraction Kits (Biocomma Limited, Guangdong, China).
2.4. Detection of SARS-CoV-2 by RT-qPCR
The commercial kit ECUGEN SARS-CoV-2 RT-qPCR (Starnewcorp-UDLA, Ecuador) was used to identify the presence of SARS-CoV-2 in nasopharyngeal and nasal swabs. Briefly, the assay is based on The CDC (Centers for Disease Control and Prevention) protocol that includes N1 and N2 probes and RNase P for SARS-CoV-2 detection and RNA extraction quality control, respectively, Freire-Paspuel et al. (35). Also, negative controls (TE pH 8 buffer) were included. A positive control that contains N gene of SARS-CoV-2 (IDT, United States) was used for viral load calculation, provided at 200,000 genome equivalents/mL (36–38).
2.5. Detection of Streptococcus pneumoniae by qPCR
Primers and probes for detecting S. pneumoniae have been previously reported (34). The following primers and probes are designed to target the LytA gene and approved by CDC: LytA (forward): ACGCAATCTAGCAGATGAAGCA; LytA (reverse): TCGTGCGTTTTAATTCCAGCT; and probe: 5’-FAM-TGCCGAAAACGC”T”TGATACAGGGAG-3’-SpC “-T” = BHQ1 number access EA005672. In addition, multiplexes designed for real-time PCR proposed by CDC were used for detecting 21 serotypes or serogroups in 7 PCR reactions with protocol triplex sequential real-time PCR-serotyping for Latin America being 14, 18C/18F/18B/18A, 19\u00B0F, 4, 6A/6B/6C/6D, 9 V/9A, 1, 5, 23F, 3, 7F/7A, 19A, 6C/6D, 12F/12A/12B/44/46, 22F/22A, 15A/15F, 23A, 33F/33A/37, 2, 11A/11D and 16F serogroup (39, 40).
2.6. Detection of 12 respiratory viruses by multiplex RT-qPCR assays
RNA extracted from nasal and nasopharyngeal swabs was used to synthesize single-stranded cDNAs with the aid of Invitrogen™ Reverse transcriptase SuperScript™ II 200 U/mL, RT Buffer (10X), RT random primers (10x), dNTP (10 mM), RNAse out 40 U/mL, and multiscribe reverse transcriptase.
Four real-time multiplex PCR assays were developed for the detection of 12 respiratory viruses, as shown in Supplementary Table S1 (41–47), including influenza A virus, influenza B virus, rhinovirus, adenovirus, RSV A/B, HMPV, parainfluenza virus types 1, 2, and 3, HCoV types NL63, 229E, and HKU1. The final concentrations of each primer and probe were 500 nM and 300 nM, respectively. Real-time PCR conditions for multiplex 1 and 3 were 95°C for 2 min, followed by 40 cycles of 95°C for 15 s and 64°C for 1 min. Real-time PCR conditions for multiplex 2 and 4 were 95°C for 2 min, followed by 40 cycles of 95°C for 15 s and 60°C for 1 min.
Two synthetic double-stranded DNA fragments were made as positive controls (gBlocks Gene Fragments, IDT). For coronaviruses, the requested DNA sequence contained partial genomic sequences (less than 250 bp in length) of the 3 HCoV types. In the case of respiratory viruses, the requested DNA sequence contains partial genomic sequences (less than 300 bp in length) of 9 human viruses: influenza A, influenza B, rhinovirus 1A, RSV B, HMPV, parainfluenza virus 1, parainfluenza virus 2, parainfluenza virus 3, and human adenovirus C. In the case of S. pneumoniae, positive clinical samples were used as controls.
2.7. Statistical analysis
The statistical analyses were carried out utilizing SPSS Version 28 for Windows. The continuous variables were expressed as medians and the categorical variables as percentages. The study involved the examination of participants’ characteristics, including age, sex, occupation, symptoms, and comorbidities. The SARS-CoV-2 positive and negative subjects were counted, and the infection status of 13 respiratory pathogens was analyzed in all subjects and grouped to analyze co-infection.
Univariate analysis was conducted using chi-square tests to assess the differences in clinical data between SARS-CoV-2 positive and negative patient groups and between the SARS-CoV-2-only group and the SARS-CoV-2-coinfected group. Odds ratios (OR) and their 95% confidence intervals (CIs) were estimated and statistical significance was set at p < 0.05.
Variables with significant p-values in the univariate analysis were analyzed with multivariate logistic regression using the stepwise backward Wald method to confirm independence. The Hosmer-Lemeshow test was used to evaluate the goodness of fit of the model.
3. Results
This study included 215 nasal and nasopharyngeal swab samples from individuals in outpatient and community settings suspected of having a SARS-CoV-2 infection from January 2020 to November 2021 in Quito, Ecuador. The population’s median age was 32 years, with 122 female and 93 male patients (female/male ratio 1.31). Patients demographics and clinical characteristics are shown in Table 1.
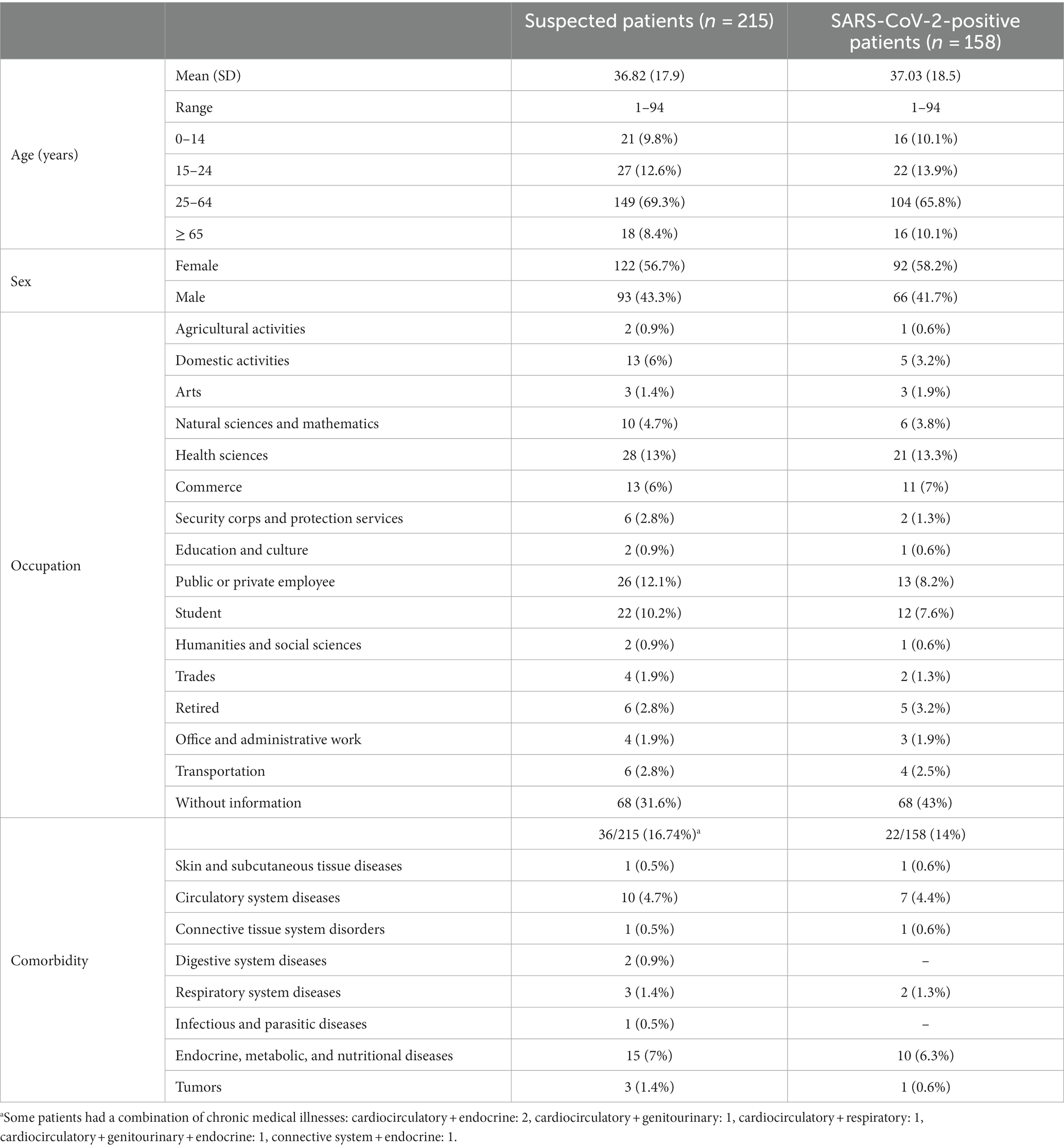
Table 1. Demographics and clinical characteristics of all patients included in the study.
Overall, 158 patients (73.5%; 158/215) tested positive for SARS-CoV-2 infection in the RT-qPCR assay. Of those, 53.8% (85/158) were from primary care centers and 46.2% (73/158) were outpatients. Fifty-eight percent (92/158) of positive patients were female and 41.7% (66/158) were male. The highest frequency of SARS-CoV-2 infections was in the age group of 25–64 years with 104/158 positives (65.8%).
Of a total of 215 individual enrolled 73% (157/215) reported symptoms and were categorized according to the organ and system affected; all these details are described in Table 2. Several clinical sign and symptom as dysnea, chest pain, anosmia, ageusia, asthenia, arthralgia, and fever were significant more present in patients with SARS-CoV-2 infection than in those without SARS-CoV-2 (p < 0.05). The odds ratios of patients with COVID-19 increased by 17.1-fold for asthenia, 12.6-fold for ageusia, 9-fold for arthralgia, and 8.7-fold for anosmia (Table 2). When these factors were analyzed by multivariate logistic regression, only anosmia (odd ratio [OR] 5.23, 95% CI 1.11–24.74) and asthenia (odd ratio [OR]15.25, 95% CI 1.83–127.0) were positively associated to SARS-CoV-2 infection p = 0.037 and p = 0.012, respectively.
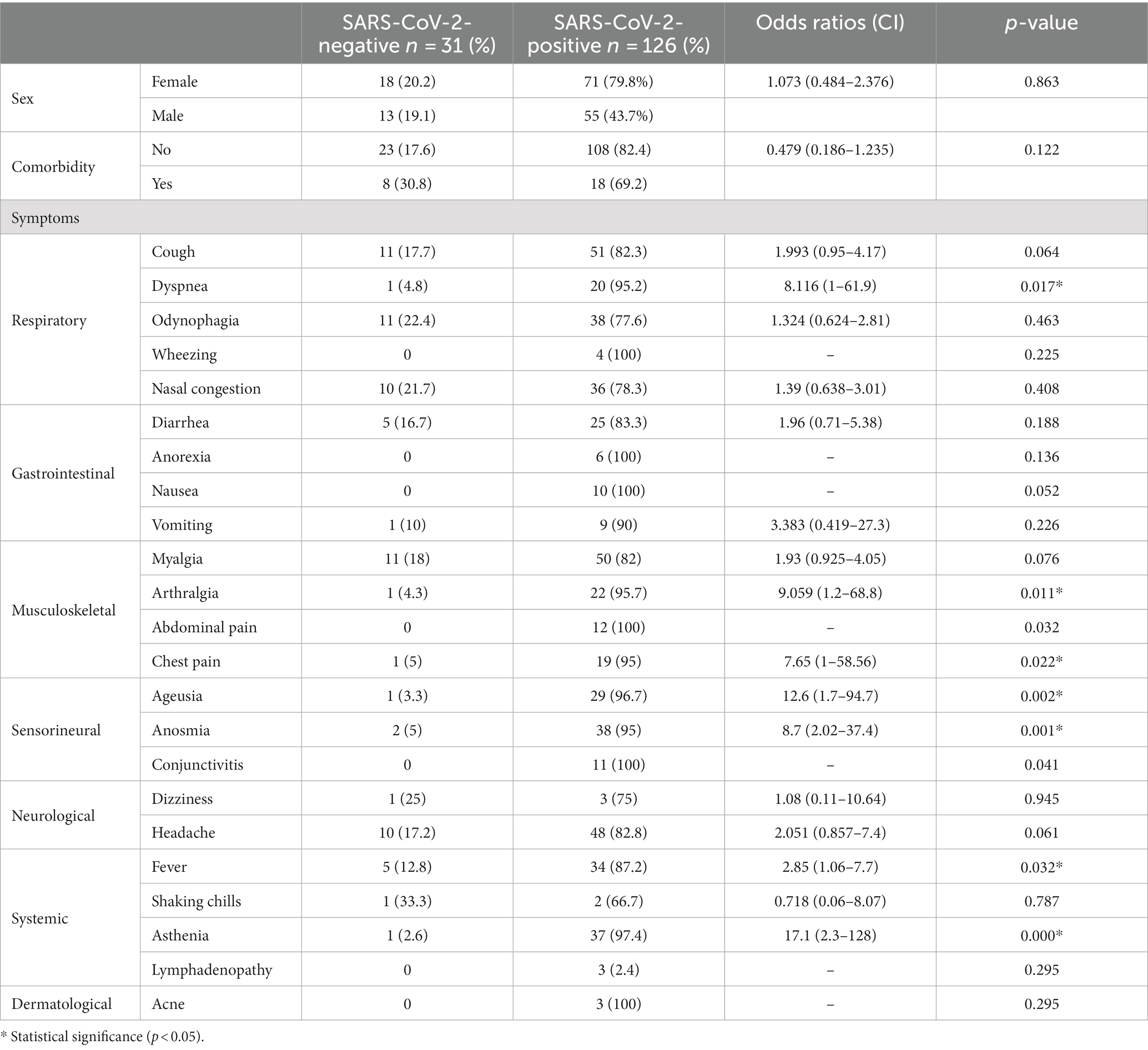
Table 2. Descriptive information of sex, comorbidity and symptoms of COVID-19 positive patients.
Overall, the prevalence of respiratory pathogens other than SARS-CoV-2 in this study was 5.6% (12/215; 95% CI: 2.53–8.67) for influenza A, 4.7% (10/215; 95% CI: 1.87–7.53) for rhinovirus, 2.8% (6/215; 95% CI: 0.59–5.01) for RSV, 0.9% (2/215) for HCoV-NL63, 0.5% (1/215) for HCoV-229E, and 2.8% (6/215) for S. pneumoniae. Influenza B, adenovirus, HMPV, parainfluenza 1, 2, and 3, and HCoV-HKU1 were not detected.
The infection rates for influenza A, RSV, HCoV-NL63, S. pneumoniae and HCoV 229E do not show significant differences in patients with or without SARS-CoV-2 infection. Only rhinovirus infections were significantly higher in SARS-CoV-2 negative patients (p < 0.05) in univariate and multivariate analysis.
Coinfection was detected in 12.02% (19/158; 95% CI: 6.95–17.09) of the SARS-CoV-2 positive cases most of these patients were 25–64 years old (57.9%; 11/19). Fifty-eight point 6 % of them were female and 47.3% were male. Clinical symptoms more present in patients with SARS-CoV-2 coinfection than in those without SARS-CoV-2 coinfection were shaking chills (50%), dizziness (33%), wheezing (25%) and abdominal pain (16.6%).
Coinfection SARS-CoV-2 with influenza A virus (6.3%, 10/158, 95% CI: 1.2–7.6) was the most frequent followed by RSV with 3.1% (5/158, 95% CI: 0.4–5.8) and finally rhinovirus and HCoV-NL63 with 1.2% (2/158). Regarding pneumococcal carriage, 3.8% (6/158, 95% IC, 0.76–6.64) of the SARS-CoV-2 patients were colonized. Of the 6 patients positive for S. pneumoniae, only 5 could be serotyped. Three patients were identified with a single serotype: 3, 6C, and 23F, respectively. The other 2 patients were children of 5 and 6 years colonized with more than one serotype. One patient had serotypes 33A/33F/37, 4, 3, and 18A/18B/18C, and the other had serotypes 3 and 4. Figure 1 summarizes the total number of positive samples for SARS-CoV-2 and presented coinfection.
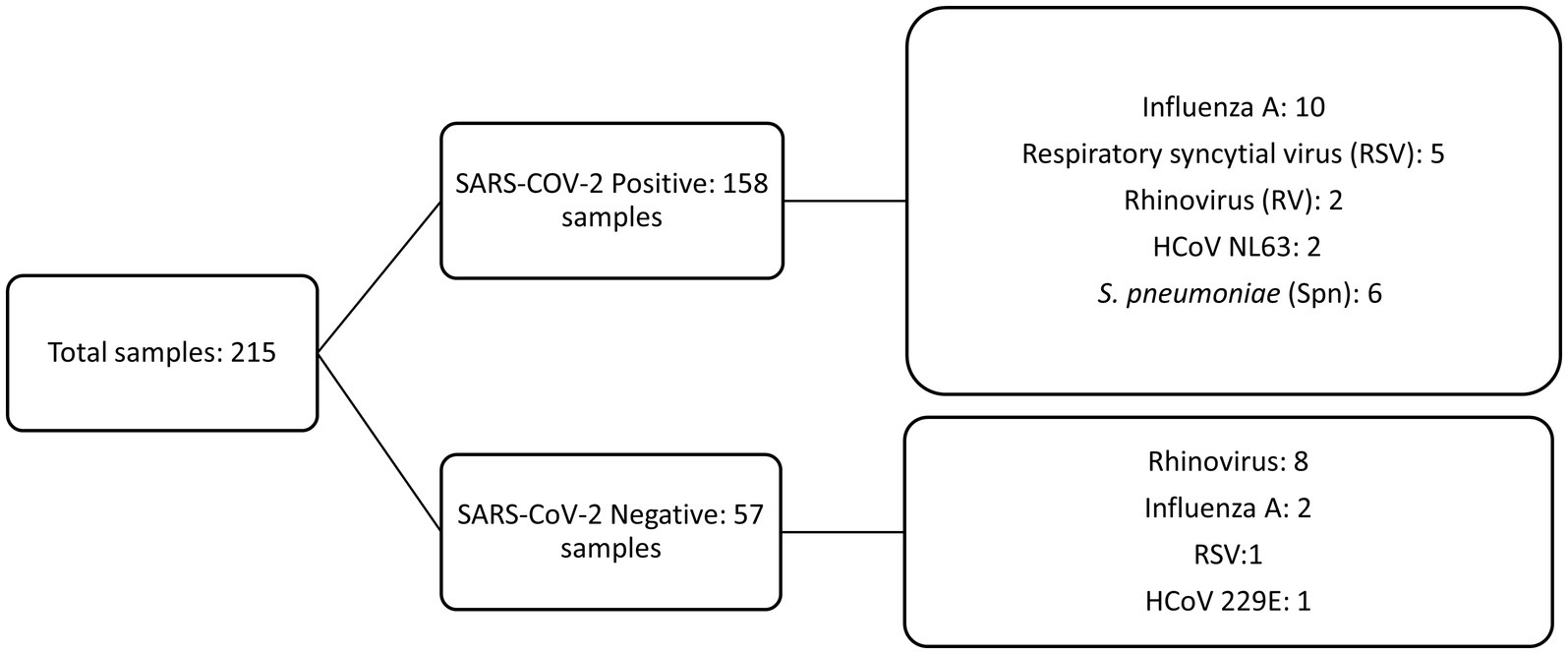
Figure 1. Detection of SARS-CoV-2 infection and coinfection with 13 respiratory pathogens.
In two SARS-CoV-2 positive patients, we detected 2 additional pathogens: rhinovirus and S. pneumoniae in the first and RSV and S. pneumoniae in the second.
Patients coinfected with SARS-CoV-2 and influenza A virus presented significant more wheezing, dizziness and shaking chills (p < 0.05). When these factors were analyzed by multivariate logistic regression, wheezing (odd ratio [OR] 10.5, 95% CI 1.01–116) and shaking chill (odd ratio [OR] 15,7, 95% CI 1.25–19.8) keep significant (p < 0.05).
The SARS-CoV-2 viral load reported in the 19 coinfected patients had an average of 3.16 × 104 copies/μL for the N1 target. The range was between 1.01 × 101 to 4.48 × 105 copies/μL. Remarkably, all patients with coinfections had a SARS-CoV-2 viral load lower than 5 × 105 copies/μL (Figure 2).
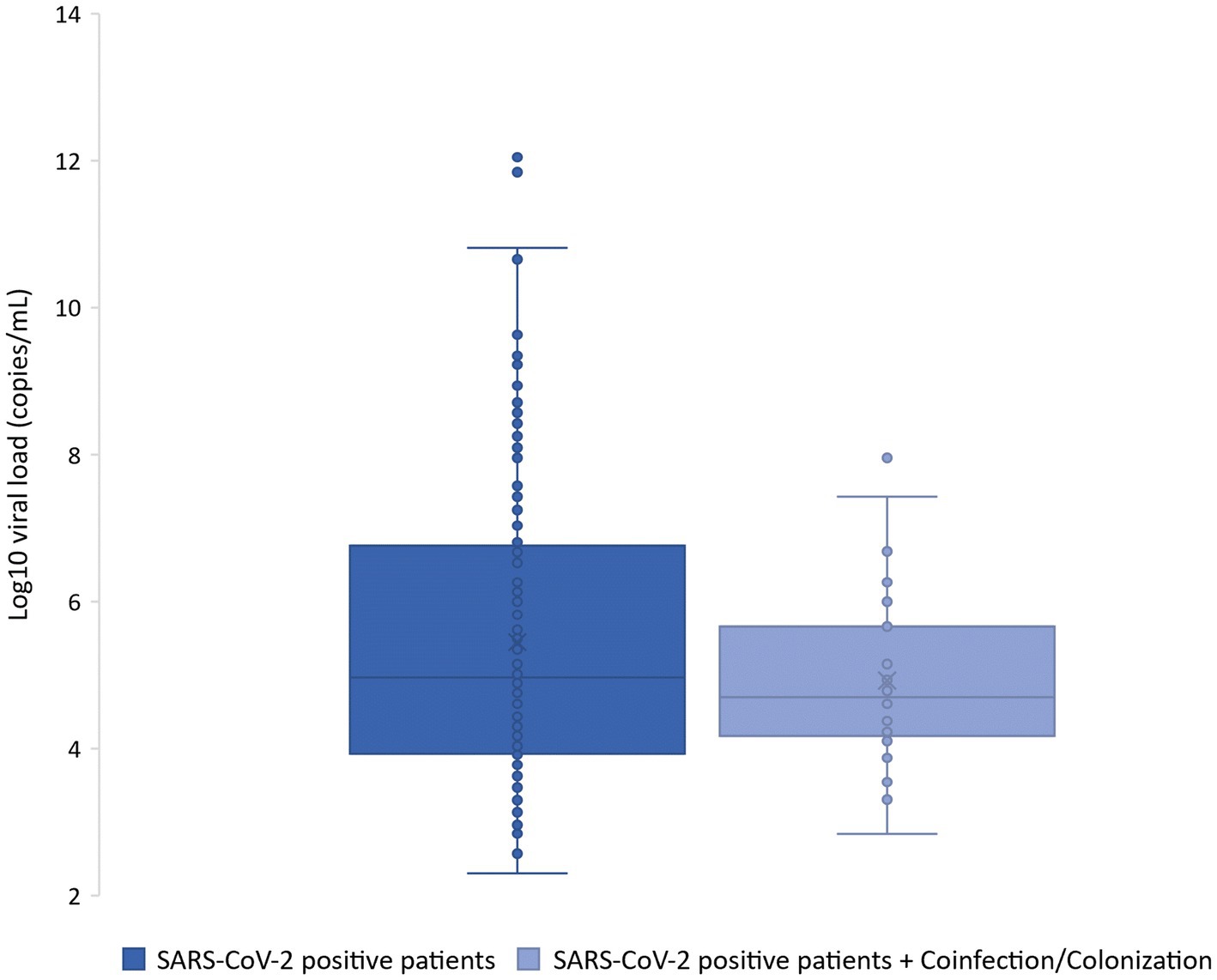
Figure 2. Box plot indicating the log10 of the viral loads in SARS-CoV-2 positive patients and those with coinfection and/or colonization.
All the symptomatic individuals studied had mild illnesses that could be managed in an ambulatory setting or at home through telemedicine. Interestingly, the highest frequency of coinfections was observed within a family group from the south of Quito with 4 cases of SARS-CoV-2 and influenza A, 1 case of SARS-CoV-2 with RSV and S. pneumoniae, and 1 case of SARS-CoV-2 with HCoV-NL63, showing a possible household circulation. Also, we observed an increased detection of coinfection from July to August (Figure 3).
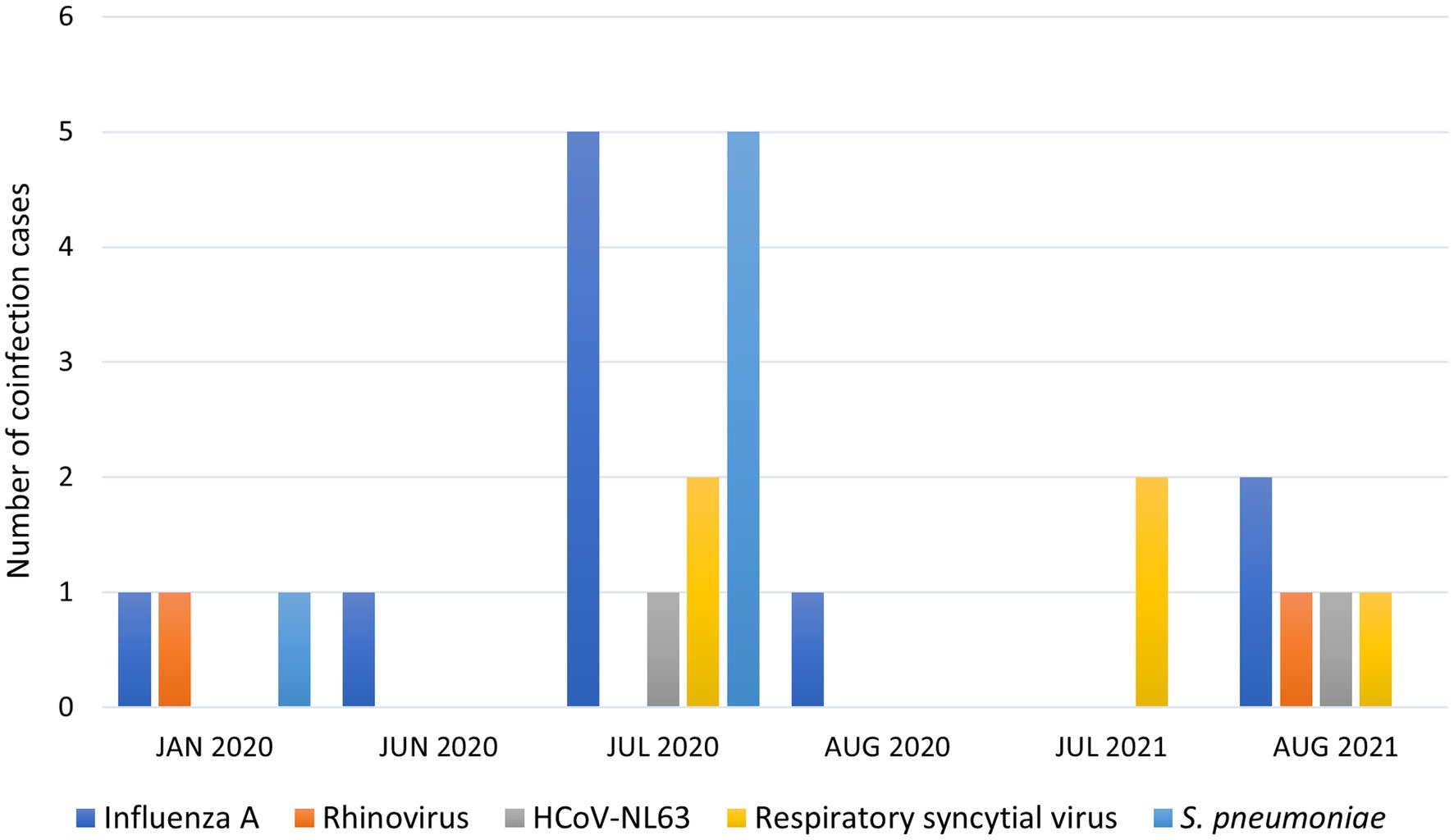
Figure 3. Coinfection cases and date of detection by respiratory pathogens.
4. Discussion
The COVID-19 pandemic, caused by SARS-CoV-2, has had a profound impact on global public health, resulting in more than 6.9 million deaths worldwide by April 2023 (48). This pandemic has severely tested the resilience of healthcare systems in low- and middle-income countries, where resources were already limited prior to the outbreak (49, 50). Furthermore, numerous cases of coinfections with respiratory viruses, bacteria, and fungi have been reported in patients infected with SARS-CoV-2 (51, 52).
In Latin America, data on coinfections is scarce. However, in southern Brazil, 19% of patients with SARS-CoV-2 tested positive for rhinovirus, 4.3% for adenovirus, and 1.4% for influenza A (53). In Colombia, Orozco-Hernandez et al. reported a case of SARS-CoV-2 and rhinovirus/enterovirus coinfection in a patient who developed severe respiratory disease and required intensive care unit (ICU) care (54, 55). Additionally, in a Peruvian hospital, 10% of patients with COVID-19 had Mycoplasma pneumoniae coinfection (56).
Furthermore, some studies have suggested that coinfections with SARS-CoV-2 and other viruses are less common than bacterial coinfections, particularly with pneumococcus, the most prevalent bacterium in community-acquired pneumonia (39–48).
Coinfection data for COVID-19 are mainly based on hospitalized patients with severe disease. Although most COVID-19 patients do not require hospitalization, very little is known about coinfections among outpatients (57).
This study aimed to fill this knowledge gap by identifying the prevalence of upper respiratory tract coinfections in SARS-CoV-2 positive outpatients. The results showed a 12% prevalence of upper respiratory tract coinfections in SARS-CoV-2 positive outpatients. This study is the first to provide data on the infection rate of SARS-CoV-2, along with other respiratory pathogens, in non-hospitalized patients in Latin America.
Influenza A virus is a common and important coinfecting respiratory pathogen that has been detected in several studies worldwide. Prevalence rates for influenza A virus infection in SARS-CoV-2 positive patients range from 0.08 to 52% in various geographical regions (8, 31, 51, 52, 58, 59). However, each region has a unique profile, and significant variations can exist even within the same country. For example, in China, coinfection rates with influenza A virus have been reported to be as high as 60% in Qingdao, while no coinfection was detected in Wuhan (7, 60). Similarly, in Brazil, coinfection rates with influenza A virus range from 0.04% in Rio de Janeiro to 53% in São Paulo (61). In contrast, in Peru, influenza A virus has not been detected in patients with COVID-19 (21, 22).
Our study found that the prevalence of SARS-CoV-2 co-infection with influenza A virus was 6.3%, followed by RSV at 3.1%, and rhinovirus and HCoV-NL63 at 1.2% among outpatients and the community setting population aged 25–62 years. This suggests the importance of simultaneously screening patients with respiratory tract infections for SARS-CoV-2 and other respiratory viral pathogens.
The prevalence of influenza A virus coinfection in our study was higher than that reported in previous studies of hospitalized patients from Peru and Colombia, where this pathogen was not detected (22, 62). Furthermore, our data showed that patients with influenza co-infection had a higher risk of respiratory symptoms, such as wheezing, and other symptoms, such as dizziness and chills. Coinfection can increase the severity of the disease and the risk of death among high-risk COVID-19 patients, such as the older adult, children, and patients with COPD.
In Ecuador, the high prevalence of SARS-CoV-2/influenza A virus co-infection does not appear to be associated with seasonal influenza, which typically occurs from November to March. Instead, our highest peak of co-infection detection was in July–August. Influenza A virus circulates in Ecuador throughout the year and causes sporadic outbreaks between August and September, though these may occur earlier or later due to various factors (63).
The COVID-19 pandemic has affected the seasonal circulation of many respiratory pathogens, particularly influenza and RSV (64), underscoring the public health risk of co-infection with Influenza A virus and SARS-CoV-2. Therefore, vaccination during seasonal peaks is crucial.
Our study found that RSV was the second most prevalent virus, accounting for 3.1% of coinfections. Worldwide, RSV is a leading cause of bronchitis, bronchiolitis, and viral pneumonia in young, older adult, and immunocompromised patients (65, 66). A report from the UK between February 2020 and December 2021 showed results similar to ours, with a SARS-CoV-2/RSV coinfection rate of approximately 3.2%. Our result was lower than that of a report on hospitalized children in Brazil, which reported a coinfection rate of 18.7% (31, 67).
Regarding pneumococcal colonization, we only detected S. pneumoniae in SARS-CoV-2-positive patients. It was the second most frequent pathogen after influenza A virus in our outpatient group, with 3.7% of patients being carriers. These findings are consistent with recent reports in the UK showing that pneumococcal colonization is more frequent among outpatients with mild SARS-CoV-2 infection (34.5%) than in SARS-CoV-2-positive patients (27.4%). This is probably associated with the reduced cellular and mucosal immune responses to SARS-CoV-2 (68, 69). There have been no other studies on pneumococcal colonization in SARS-CoV-2-positive patients in Latin America.
To our knowledge, this is the first study in Latin America to show the prevalence of viral coinfections and S. pneumoniae colonization in nonhospitalized SARS-CoV-2-positive patients (outpatients). All symptomatic individuals in our cohort had mild illnesses that could be managed in an ambulatory setting or at home using telemedicine.
The high prevalence of coinfections in this patient group reveals the importance of simultaneous testing for SARS-CoV-2 and other common respiratory pathogens. Molecular screening allows rapid detection, and several commercial panels are available for detecting SARS-CoV-2 and other pathogens in a single reaction to ensure accurate diagnosis, prompt patient treatment, and appropriate isolation, as recommended in several studies (70–74).
Our results must be interpreted in light of our limitations, as this research was restricted to a single region of the country with a limited sample size and could be affected by temporal variation in viral epidemiology. Another limitation of our study is that there was no information about the vaccine status of patients, previous treatment, use of antibiotics, time of disease onset, etc. Moreover, as the study was conducted during the early part of the pandemic and resources were limited, it was not possible to include control group controls to evaluate the presence of asymptomatic infections.
Coinfections in outpatients may lead to changes in the transmission of respiratory pathogens in community settings, allowing pathogens to reach families and community groups and exposing vulnerable populations, such as children and the older adult.
This study provides novel baseline data, highlighting the need for continued surveillance and detection of other pathogens, co-circulation of SARS-CoV-2 and other respiratory pathogens will represent a challenge for health systems globally, but particularly in Latin America, where the health system has not yet fully recovered from the impact of the pandemic.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author.
Ethics statement
The study design was approved by the Ethics Committee with code N° 008-2020 and CEISH-HGSF-2021-002 and participants signed a written informed consent after being fully informed.
Author contributions
DM-J: Formal analysis, Investigation, Writing – original draft. CM: Investigation, Writing – review & editing, Methodology. CV-D: Investigation, Writing – review & editing. BC: Investigation, Writing – review & editing. BC-R: Formal analysis, Writing – review & editing. AV-J: Formal analysis, Writing – review & editing. AH-T: Investigation, Writing – review & editing. MG-B Writing – review & editing. IR-O: Writing – review & editing, Investigation, Methodology, Conceptualization, Supervision.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This research was funded by Universidad de las Americas, research grant MED.IRO.20.08 led by IR-O.
Acknowledgments
Thanks to Helen Pugh for proofreading the manuscript.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2023.1264632/full#supplementary-material
References
1. Wang, C, Horby, PW, Hayden, FG, and Gao, GF. A novel coronavirus outbreak of global health concern. Lancet. (2020) 395:470–3. doi: 10.1016/S0140-6736(20)30185-9
2. Dirección de Relaciones Públicas Se registra el primer caso de coronavirus en Ecuador – Secretaría General de Comunicación de la Presidencia. Available at: https://www.comunicacion.gob.ec/se-registra-el-primer-caso-de-coronavirus-en-ecuador/ (Accessed Oct 31, 2021).
3. Ministerio de Salud Pública. Actualización de casos de coronavirus en Ecuador – Ministerio de Salud Pública [Internet]. Ministerio De Salud Publica. (2020). Available at: https://www.salud.gob.ec/actualizacion-de-casos-de-coronavirus-en-ecuador/ (Accessed June 11, 2021).
4. WHO. (2020). Clinical management of COVID-19: interim guidance, 27 May 2020. Geneve: In Proceedings of the World Health Organization, 1–10.
5. World Health Organization WHO COVID-19 Case definition. Updated in public health surveillance for COVID-19 vol. 1 (2020). Available at: https://apps.who.int/iris/handle/10665/333912
6. Huang, C, Wang, Y, Li, X, Ren, L, Zhao, J, Hu, Y, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet. (2020) 395:497–506. doi: 10.1016/S0140-6736(20)30183-5
7. Chen, N, Zhou, M, Dong, X, Qu, J, Gong, F, Han, Y, et al. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: a descriptive study. Lancet. (2020) 395:507–13. doi: 10.1016/S0140-6736(20)30211-7
8. Kim, D, Quinn, J, Pinsky, B, Shah, NH, and Brown, I. Rates of co-infection between SARS-CoV-2 and other respiratory pathogens. JAMA. (2020) 323:2085–6. doi: 10.1001/jama.2020.6266
9. Wang, M, Wu, Q, Xu, W, Qiao, B, Wang, J, Zheng, H, et al. Clinical diagnosis of 8274 samples with 2019-novel coronavirus in Wuhan. Med Rxiv. (2020). doi: 10.1101/2020.02.12.20022327
10. Lansbury, L, Lim, B, Baskaran, V, and Lim, WS. Co-infections in people with COVID-19: a systematic review and meta-analysis. J Infect. (2020) 81:266–75. doi: 10.1016/j.jinf.2020.05.046
11. López-Herrero, R, Sánchez-De Prada, L, Tamayo-Velasco, A, Lorenzo-López, M, Gómez-Pesquera, E, Sánchez-Quirós, B, et al. Epidemiology of bacterial co-infections and risk factors in COVID-19-hospitalized patients in Spain: a nationwide study. Eur J Public Health. (2023) 33:675–81. doi: 10.1093/eurpub/ckad060
12. Westblade, LF, Simon, MS, and Satlin, MJ. Bacterial coinfections in coronavirus disease 2019. Trends Microbiol. (2021) 29:930–41. doi: 10.1016/j.tim.2021.03.018
13. Alhumaid, S, Alabdulqader, M, Al Dossary, N, Al Alawi, Z, Alnaim, AA, Al Mutared, KM, et al. Global coinfections with Bacteria, Fungi, and respiratory viruses in children with SARS-CoV-2: a systematic review and meta-analysis. Trop Med Infect Dis. (2022) 7:380. doi: 10.3390/tropicalmed7110380
14. Lehmann, CJ, Pho, MT, Pitrak, D, Ridgway, JP, and Pettit, NN. Community acquired co-infection in COVID-19: a retrospective observational experience. Clin Infect Dis. (2021) 72:1450–2. doi: 10.1093/cid/ciaa902
15. Klein, EY, Monteforte, B, Gupta, A, Jiang, W, May, L, Hsieh, YH, et al. The frequency of influenza and bacterial coinfection: a systematic review and meta-analysis. Influenza Other Respir Viruses. (2016) 10:394–403. doi: 10.1111/irv.12398
16. Palacios, G, Hornig, M, Cisterna, D, Savji, N, Bussetti, AV, Kapoor, V, et al. Streptococcus pneumoniae coinfection is correlated with the severity of H1N1 pandemic influenza. PLoS One. (2009) 4:e8540. doi: 10.1371/journal.pone.0008540
17. Leggiadro, RJ. Bacterial coinfections in lung tissue specimens from fatal cases of 2009 pandemic influenza a (H1N1) – United States, May–august 2009. Pediatr Infect Dis J. (2010) 29:22. doi: 10.1097/01.inf.0000366838.82857.78
18. Stahlfeld, A, Glick, LR, Ott, IM, Craft, SB, Yolda-Carr, D, Harden, CA, et al. Detection of pneumococcus during hospitalization for SARS-CoV-2. FEMS Microbes. (2022) 3:xtac026. doi: 10.1093/femsmc/xtac026
19. Toombs, JM, Van den Abbeele, K, Democratis, J, Mandal, AKJ, and Missouris, CG. Pneumococcal coinfection in COVID-19 patients. J Med Virol. (2021) 93:177–9. doi: 10.1002/jmv.26278
20. Parker, AM, Jackson, N, Awasthi, S, Kim, H, Alwan, T, Wyllie, AL, et al. Association of upper respiratory Streptococcus pneumoniae colonization with severe acute respiratory syndrome coronavirus 2 infection among adults. Clin Infect Dis. (2023) 76:1209–17. doi: 10.1093/cid/ciac907
21. Soto, A, Quiñones-Laveriano, DM, Valdivia, F, Juscamayta-López, E, Azañero-Haro, J, Chambi, L, et al. Detection of viral and bacterial respiratory pathogens identified by molecular methods in COVID-19 hospitalized patients and its impact on mortality and unfavorable outcomes. Infect Drug Resist. (2021) 14:2795–807. doi: 10.2147/IDR.S306439
22. Pérez-Lazo, G, Silva-Caso, W, Del Valle-Mendoza, J, Morales-Moreno, A, Ballena-López, J, Soto-Febres, F, et al. Identification of coinfections by viral and bacterial pathogens in COVID-19 hospitalized patients in Peru: molecular diagnosis and clinical characteristics. Antibiotics (Basel, Switzerland). (2021) 10:1358. doi: 10.3390/antibiotics10111358
23. Pucarelli-Lebreiro, G, Venceslau, MT, Cordeiro, CC, Maciel, FQ, Anachoreta, TD, De Abreu, TF, et al. Clinical manifestations and complications of children with COVID-19 compared to other respiratory viral infections: a cohort inpatient study from Rio de Janeiro, Brazil. Front Pediatr. (2022) 10:934648. doi: 10.3389/fped.2022.934648
24. Caméléna, F, Moy, AC, Dudoignon, E, Poncin, T, Deniau, B, Guillemet, L, et al. Performance of a multiplex polymerase chain reaction panel for identifying bacterial pathogens causing pneumonia in critically ill patients with COVID-19. Diagn Microbiol Infect Dis. (2021) 99:115183. doi: 10.1016/j.diagmicrobio.2020.115183
25. Ruuskanen, O, Lahti, E, Jennings, LC, and Murdoch, DR. Viral pneumonia. Lancet. (2011) 377:1264–75. doi: 10.1016/S0140-6736(10)61459-6
26. Sharifipour, E, Shams, S, Esmkhani, M, Khodadadi, J, Fotouhi-Ardakani, R, Koohpaei, A, et al. Evaluation of bacterial co-infections of the respiratory tract in COVID-19 patients admitted to ICU. BMC Infect Dis. (2020) 20:646. doi: 10.1186/s12879-020-05374-z
27. Lai, CC, Wang, CY, and Hsueh, PR. Co-infections among patients with COVID-19: the need for combination therapy with non-anti-SARS-CoV-2 agents? J Microbiol Immunol Infect. (2020) 53:505–12. doi: 10.1016/j.jmii.2020.05.013
28. Singh, V, Upadhyay, P, Reddy, J, and Granger, J. SARS-CoV-2 respiratory co-infections: incidence of viral and bacterial co-pathogens. Int J Infect Dis. (2021) 105:617–20. doi: 10.1016/j.ijid.2021.02.087
29. Malekifar, P, Pakzad, R, Shahbahrami, R, Zandi, M, Jafarpour, A, Rezayat, SA, et al. Viral coinfection among COVID-19 patient groups an update systematic review and meta-analysis. Biomed Res Int. (2021) 2021:1–10. doi: 10.1155/2021/5313832
30. Kim, E-H, Nguyen, T-Q, Casel, MAB, Rollon, R, Kim, S-M, Kim, Y-I, et al. Coinfection with SARS-CoV-2 and influenza a virus increases disease severity and impairs neutralizing antibody and CD4+ T cell responses. J Virol. (2022) 96:e0187321. doi: 10.1128/jvi.01873-21
31. Swets, MC, Russell, CD, Harrison, EM, Docherty, AB, Lone, N, Girvan, M, et al. SARS-CoV-2 co-infection with influenza viruses, respiratory syncytial virus, or adenoviruses. Lancet. (2022) 399:1463–4. doi: 10.1016/S0140-6736(22)00383-X
32. Ministerio de Salud Pública. Lineamiento de vigilancia integrada para covid-19 y otros virus respiratorios. Vol. 3. (2022). Available at: http://www.acess.gob.ec/wp-content/uploads/2022/08/Lineamiento_vigilancia_integrada_COVID-19_OVR_Version-final_Agosto_2022.pdf
33. Mcgee, L., Velusamy, S., Vidal, J. E., and Sakai, F. (2018). DNA extraction and CDC multiplex real-time PCR standard operating procedure (SOP).
34. Carvalho, MDGS, Tondella, ML, McCaustland, K, Weidlich, L, McGee, L, Mayer, LW, et al. Evaluation and improvement of real-time PCR assays targeting lyt a, ply, and psaA genes for detection of pneumococcal DNA. J Clin Microbiol. (2007) 45:2460–6. doi: 10.1128/JCM.02498-06
35. Freire-Paspuel, B, Morales-Jadan, D, Zambrano-Mila, M, Perez, F, and Garcia-Bereguiain, MA. Analytical sensitivity and clinical performance of “COVID-19 RT-PCR real TM FAST (CY5) (ATGen, Uruguay) and ‘ECUGEN SARS-CoV-2 RT-qPCR’ (UDLA-STARNEWCORP, Ecuador)”: high quality-low cost local SARS-CoV-2 tests for South America. PLoS Negl Trop Dis. (2022) 16:e0010082. doi: 10.1371/journal.pntd.0010082
36. Freire-Paspuel, B, Vega-Mariño, P, Velez, A, Cruz, M, Perez, F, and Garcia-Bereguiain, MA. Analytical and clinical comparison of Viasure (Cer test Biotec) and 2019-nCoV CDC (IDT) RT-qPCR kits for SARS-CoV2 diagnosis. Virology. (2021) 553:154–6. doi: 10.1016/j.virol.2020.10.010
37. Freire-Paspuel, B, and Garcia-Bereguiain, MA. Analytical sensitivity and clinical performance of a triplex RT-qPCR assay using CDC N1, N2, and RP targets for SARS-CoV-2 diagnosis. Int J Infect Dis. (2021) 102:14–6. doi: 10.1016/j.ijid.2020.10.047
38. Freire-Paspuel, B, Vega-Mariño, P, Velez, A, Cruz, M, and Garcia-Bereguiain, MA. Sample pooling of RNA extracts to speed up SARS-CoV-2 diagnosis using CDC FDA EUA RT-qPCR kit. Virus Res. (2020) 290:198173. doi: 10.1016/j.virusres.2020.198173
39. Centers for disease control and prevention Streptococcus Lab Resources and Protocols | CDC. Available at: https://www.cdc.gov/streplab/pneumococcus/resources.html (Accessed Jun 12, 2023).
40. Centers for disease control and prevention. Streptococcus Lab Resources and Protocols (2014). Available at: https://www.cdc.gov/streplab/pneumococcus/resources.html (Accessed June 11, 2023).
41. Sanghavi, S, Bullotta, A, Husain, S, and Rinaldo, C. Clinical evaluation of multiplex real-time PCR panels for rapid detection of respiratory viral infections. Antivir Ther. (2006) 55:52–55.
42. Tiveljung-Lindell, A, Rotzén-Ostlund, M, Gupta, S, Ullstrand, R, Grillner, L, Zweygberg-Wirgart, B, et al. Development and implementation of a molecular diagnostic platform for daily rapid detection of 15 respiratory viruses. Antivir Ther. (2006) 55:52–55.
43. Kuypers, J, Wright, N, and Morrow, R. Evaluation of quantitative and type-specific real-time RT-PCR assays for detection of respiratory syncytial virus in respiratory specimens from children. J Clin Virol. (2004) 31:123–9. doi: 10.1016/j.jcv.2004.03.018
44. Watzinger, F, Suda, M, Preuner, S, Baumgartinger, R, Ebner, K, Baskova, L, et al. Real-time quantitative PCR assays for detection and monitoring of pathogenic human viruses in immunosuppressed pediatric patients. J Clin Microbiol. (2004) 42:5189–98. doi: 10.1128/JCM.42.11.5189-5198.2004
45. Klemenc, J, Asad Ali, S, Johnson, M, Tollefson, SJ, Talbot, HK, Hartert, TV, et al. Real-time reverse transcriptase PCR assay for improved detection of human metapneumovirus. J Clin Virol. (2012) 54:371–5. doi: 10.1016/j.jcv.2012.05.005
46. Kaida, A, Kubo, H, Takakura, KI, Sekiguchi, JI, Yamamoto, SP, Kohdera, U, et al. Associations between CO-detected respiratory viruses in children with acute respiratory infections. Jpn J Infect Dis. (2014) 67:469–75. doi: 10.7883/yoken.67.469
47. Gunson, RN, Collins, TC, and Carman, WF. Real-time RT-PCR detection of 12 respiratory viral infections in four triplex reactions. J Clin Virol. (2005) 33:341–4. doi: 10.1016/j.jcv.2004.11.025
48. World Health Organization WHO Coronavirus Disease (COVID-19) dashboard. Available at: https://covid19.who.int/ (Accessed May 2, 2023).
49. Boussarsar, M, Meddeb, K, Toumi, R, Ennouri, E, Ayed, S, Jarraya, F, et al. Resource utilization and preparedness within the COVID-19 pandemic in Tunisian medical intensive care units: a nationwide retrospective multicentre observational study. J Infect Public Health. (2023) 16:727–35. doi: 10.1016/j.jiph.2023.02.022
50. Ortiz-Prado, E, Simbaña-Rivera, K, Barreno, LG, Diaz, AM, Barreto, A, Moyano, C, et al. Epidemiological, socio-demographic and clinical features of the early phase of the COVID-19 epidemic in Ecuador. PLoS Negl Trop Dis. (2021) 15:e0008958. doi: 10.1371/journal.pntd.0008958
51. Miatech, JL, Tarte, NN, Katragadda, S, Polman, J, and Robichaux, SB. A case series of coinfection with SARS-CoV-2 and influenza virus in Louisiana. Respir Med Case Rep. (2020) 31:101214. doi: 10.1016/j.rmcr.2020.101214
52. Rawson, TM, Moore, LSP, Zhu, N, Ranganathan, N, Skolimowska, K, Gilchrist, M, et al. Bacterial and fungal coinfection in individuals with coronavirus: a rapid review to support COVID-19 antimicrobial prescribing. Clin Infect Dis. (2020) 71:2459–68. doi: 10.1093/cid/ciaa530
53. Antunes Eisen, AK, Gularte, JS, Demoliner, M, De Abreu Goés Pereira, VM, Heldt, FH, Filippi, M, et al. Low circulation of influenza a and coinfection with SARS-CoV-2 among other respiratory viruses during the COVID-19 pandemic in a region of southern Brazil. J Med Virol. (2021) 93:4392–8. doi: 10.1002/jmv.26975
54. Orozco-Hernández, JP, Montoya-Martínez, JJ, Pacheco-Gallego, MC, Céspedes-Roncancio, M, and Porras-Hurtado, GL. Coinfección por SARS-CoV-2 y rinovirus-enterovirus en una paciente adulta joven críticamente enferma en Colombia. Biomedica. (2020) 40:34–43. doi: 10.7705/biomedica.5516
55. Nowak, MD, Sordillo, EM, Gitman, MR, and Mondolfi, AEP. Coinfection in SARS-CoV-2 infected patients: where are influenza virus and rhinovirus/enterovirus? J Med Virol. (2020) 92:1699–700. doi: 10.1002/jmv.25953
56. Morales-Avalos, A, Vargas-Ponce, KG, Salas-López, JA, Llanos-Tejada, FK, Morales-Avalos, A, Vargas-Ponce, KG, et al. Coinfección por SARS-CoV-2 y Mycoplasma pneumoniae: reporte de 6 casos en un hospital peruano. Rev Peru Med Exp Salud Publica. (2020) 37:776–8. doi: 10.17843/rpmesp.2020.374.5922
57. Wu, Z, and McGoogan, JM. Characteristics of and important lessons from the coronavirus disease 2019 (COVID-19) outbreak in China: summary of a report of 72 314 cases from the Chinese Center for Disease Control and Prevention. JAMA. (2020) 323:1239–42. doi: 10.1001/jama.2020.2648
58. Zhou, X, Ding, G, Shu, T, Fu, S, Tong, W, Tu, X, et al. The outbreak of coronavirus disease 2019 interfered with influenza in Wuhan. SSRN Electron J. (2020). doi: 10.2139/ssrn.3555239
59. Alosaimi, B, Naeem, A, Hamed, ME, Alkadi, HS, Alanazi, T, Al Rehily, SS, et al. Influenza co-infection associated with severity and mortality in COVID-19 patients. Virol J. (2021) 18:127. doi: 10.1186/s12985-021-01594-0
60. Xing, Q, Li, G, Xing, Y, Chen, T, Li, W, Ni, W, et al. Precautions are needed for COVID-19 patients with coinfection of common respiratory pathogens. SSRN Electron J. (2020). doi: 10.2139/ssrn.3550013
61. Fujita, DM, dos Santos Soares, G, Sartori, GP, da Silva, H, and Nali, L. COVID-19 and influenza coinfection: the rise of Ômicron and H3N2 in Brazil – 2022. Travel Med Infect Dis. (2022) 46:102262. doi: 10.1016/j.tmaid.2022.102262
62. Molina, FJ, Botero, LE, Isaza, JP, Cano, LE, López, L, Tamayo, L, et al. Diagnostic concordance between bio fire® film Array® pneumonia panel and culture in patients with COVID-19 pneumonia admitted to intensive care units: the experience of the third wave in eight hospitals in Colombia. Crit Care (London, England). (2022) 26:130. doi: 10.1186/s13054-022-04006-z
63. Ministerio de Salud Pública del Ecuador Información General – Influenza – Ministerio de Salud Pública. Available at: https://www.salud.gob.ec/informacion-general-influenza/ (Accessed Jun 12, 2023).
64. Lee, SS, Viboud, C, and Petersen, E. Understanding the rebound of influenza in the post COVID-19 pandemic period holds important clues for epidemiology and control. Int J Infect Dis. (2022) 122:1002–4. doi: 10.1016/j.ijid.2022.08.002
65. Busack, B, and Shorr, AF. Going viral—RSV as the neglected adult respiratory virus. Pathogens. (2022) 11:1324. doi: 10.3390/pathogens11111324
66. Panitch, HB, Callahan, CW, and Schidlow, DV. Bronchiolitis in children. Clin Chest Med. (1993) 14:715–31. doi: 10.1016/S0272-5231(21)00934-5
67. Alvares, PA. SARS-CoV-2 and respiratory syncytial virus coinfection in hospitalized pediatric patients. Pediatr Infect Dis J. (2021) 40:E164–6. doi: 10.1097/INF.0000000000003057
68. Mitsi, E, Reiné, J, Urban, BC, Solórzano, C, Nikolaou, E, Hyder-Wright, AD, et al. Streptococcus pneumoniae colonization associates with impaired adaptive immune responses against SARS-CoV-2. J Clin Investig. (2022) 132:1–13. doi: 10.1172/JCI157124
69. Parker, AM, Jackson, N, Awasthi, S, Kim, H, Alwan, T, Wyllie, AL, et al. Association of upper respiratory Streptococcus pneumoniae colonization with severe acute respiratory syndrome coronavirus 2 infection (SARS-CoV-2) among adults. Clin Infect Dis. (2022) 76:1209–1217. doi: 10.1093/CID/CIAC907
70. Khaddour, K, Sikora, A, Tahir, N, Nepomuceno, D, and Huang, T. Case report: the importance of novel coronavirus disease (COVID-19) and coinfection with other respiratory pathogens in the current pandemic. Am J Trop Med Hyg. (2020) 102:1208–9. doi: 10.4269/ajtmh.20-0266
71. Kambouche, N, Merah, B, Bellahouel, S, Bouayed, J, Dicko, A, Derdour, A, et al. Chemical composition and antioxidant potential of Ruta montana L. essential oil from Algeria. J Med Food. (2008) 11:593–5. doi: 10.1089/jmf.2007.0515
72. Lieberman, D, Lieberman, D, Shimoni, A, Keren-Naus, A, Steinberg, R, and Shemer-Avni, Y. Identification of respiratory viruses in adults: nasopharyngeal versus oropharyngeal sampling. J Clin Microbiol. (2009) 47:3439–43. doi: 10.1128/JCM.00886-09
73. Townsend, L, Hughes, G, Kerr, C, Kelly, M, O’Connor, R, Sweeney, E, et al. Bacterial pneumonia coinfection and antimicrobial therapy duration in SARS-CoV-2 (COVID-19) infection. JAC Antimicrob Resist. (2020) 2:2–5. doi: 10.1093/jacamr/dlaa071
Keywords: coinfection, SARS-CoV-2, outpatients, Latin America, influenza A, Ecuador, S. pneumoniae
Citation: Morales-Jadán D, Muslin C, Viteri-Dávila C, Coronel B, Castro-Rodríguez B, Vallejo-Janeta AP, Henríquez-Trujillo AR, Garcia-Bereguiain MA and Rivera-Olivero IA (2023) Coinfection of SARS-CoV-2 with other respiratory pathogens in outpatients from Ecuador. Front. Public Health. 11:1264632. doi: 10.3389/fpubh.2023.1264632
Edited by:
Joaquín Zúñiga, National Institute of Respiratory Diseases-Mexico (INER), MexicoReviewed by:
Barbara Camilloni, University of Perugia, ItalyLaura Sánchez-de Prada, Hospital Clínico Universitario de Valladolid, Spain
Copyright © 2023 Morales-Jadán, Muslin, Viteri-Dávila, Coronel, Castro-Rodríguez, Vallejo-Janeta, Henríquez-Trujillo, Garcia-Bereguiain and Rivera-Olivero. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ismar A. Rivera-Olivero, aWFyaXZlcmEub2xpdmVyb0BnbWFpbC5jb20=