 Julia Szymczyk1
Julia Szymczyk1 Wioletta Mędrzycka-Dąbrowska
Wioletta Mędrzycka-Dąbrowska- 1Student Scientific Club of Anesthesia and Intensive Care, Medical University of Gdańsk, Gdańsk, Poland
- 2Student Nursing Programme, Swedish Red Cross University, Huddinge, Sweden
- 3Department of Anesthesiology Nursing & Intensive Care, Faculty of Health Sciences, Medical University of Gdańsk, Gdańsk, Poland
Introduction: The use of reusable tourniquets is widespread around the world, and reports suggest they may be overused. Several studies have shown that reusable tourniquets can affect the spread of pathogens between patients. Based on available studies, this review aims to analyse the indirect transmission of antimicrobial-resistant pathogens present on blood collection tourniquets, which may spread infectious diseases between patients in daily clinical practice.
Methods: A systematic review of the literature was conducted according to the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analysis) protocol guidelines. The contents of PubMed, EBSCO (electronic databases), and Scopus were screened. Keywords used in the search included: “tourniquet,” “cross infection,” “nosocomial infection,” “staphylococcus aureus,” “MRO,” “pathogen,” “infectious disease,” “anti-microbial,” or a combination of these using AND or OR operators. Finally, 13 publications were included. Data were analysed both descriptively and quantitatively by calculating a balanced average for specific synthesized data.
Results: The proportional observation based on the number sampled median was 77. The genus MRSA was the type of bacteria most commonly found: on 12% of all tested tourniquets. The amount of MRSA found on tourniquets was mean ± SD 14.6 ± 45.89. A review of studies also revealed the presence of coagulase-negative staphylococci, grew Bacillus, and Staphylococcus aureus.
Conclusion: Patient safety may be at risk due to elevated contamination rates of reusable tourniquets. The microorganisms responsible for this contamination include a variety of species, the most common being the genus Staphylococcus. For this reason, we recommend the use of disposable tourniquets.
Introduction
Collecting blood through peripheral venous access using tourniquets is one of the most common invasive procedures in hospitals and other medical facilities. However, tourniquets for venipuncture are non-sterile and potentially reusable equipment. The usual technique for providing venous access is to apply a reusable tourniquet to the patient’s arm (1). Conventional tourniquets are made of fabric, and their porous structure can be a potential reservoir of infection. Usual tourniquets can be recycled through sterilization or dipping in disinfectants. Such methods are time-consuming and unsuitable for immediate use between patients (2). The most common way to disinfect reusable tourniquets is to spray them with disinfectant and hang the tourniquet to dry, but such a disinfection method is not effective as it is time-consuming. The use of such tourniquets, transferred between multiple patients, contributes to the transmission of multiresistant microorganisms (MROs) between patients and contradicts basic infection control principles (3–6). Reusable tourniquets used for blood collection are a potential carrier of multiresistant microorganisms. Disinfection of reusable equipment is not clear-cut, thus the use of disposable tourniquets, which do not require disinfection and are disposable, is preferable to reusable tourniquets. Several studies have shown that the use of reusable tourniquets can contribute to the transmission of MRO between patients. This is particularly important for immunocompromised patients who are at risk for nosocomial infections (2, 7). Improving the quality of health care involves increasing the quality and safety of medical devices used by health care workers, such as during blood draws (1). Since a review of the literature can identify major epidemiological and clinical findings, our purpose was to provide a comprehensive report on the proportion of sampled specimens between the use of reusable tourniquets and the pathogens detected on them based on recent studies.
Methods
Study design
The literature review was performed in the second quarter of 2023. This systematic review was carried out in accordance with the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) statement using PICO-based questions (patients, interventions, comparisons, and outcomes). The resources of PubMed, EBSCO (electronic databases), Scopus, and MEDLINE were searched. No filters were used during the search, and the search included backward citation of eligible full-text trials.
Evidence acquisition
In May 2023, three independent researchers (JS, MM, and WM-D) conducted a search of the targeted online databases for eligible studies. The keywords used were “tourniquet,” “cross-infection,” “nosocomial infection,” “staphylococcus aureus,” “MRO,” “pathogen,” “infectious disease,” “anti-microbial” or a combination of these using AND or OR operators. The preliminary search returned 291 articles, 13 of which were included in further analysis. Papers published in English were included in the analyses.
Inclusion and exclusion criteria
The inclusion and exclusion criteria were based on the PICOS classification. If articles fulfilled predefined criteria, they were included and classified as basic research (animal and cell studies), epidemiological (morbidity and mortality studies), and treatment studies. Articles were excluded if the full text was not publicly available was not available in English and if articles were not original articles or did not support PICO.
Inclusion criteria:
• articles in English
• research group consisting only of reusable tourniquets
• studies describing pathogens on reusable tourniquets
Exclusion criteria:
• articles in a language other than English or Polish
• research where a study group consisted of medical equipment different than reusable tourniquets
Evidence synthesis and quality assessment
Three independent researchers (JS, MM, and WM-D) retrieved and summarized information from the eligible studies in tables. The authors discussed conflicts regarding study inclusion and managed to resolve them by consensus. Studies were considered to be of high quality with a tool created by the Joanna Briggs Institute (JBI) (8). The system created by the JBI was designed to provide reviewers with a comprehensive guide on how to conduct a systematic review and how to rank selected articles (JBL for manual synthesis)1. Additionally, an appraisal checklist with 11 criteria (Q1-Q11) was also used. The questions on the checklist centered on the inclusion criteria of the selected articles, the sources and resources of the selected material, and the type of approaches used in the study. The answers used were yes, no, unclear, or not applicable. The outcomes of the quality assessment are described in Table 1.
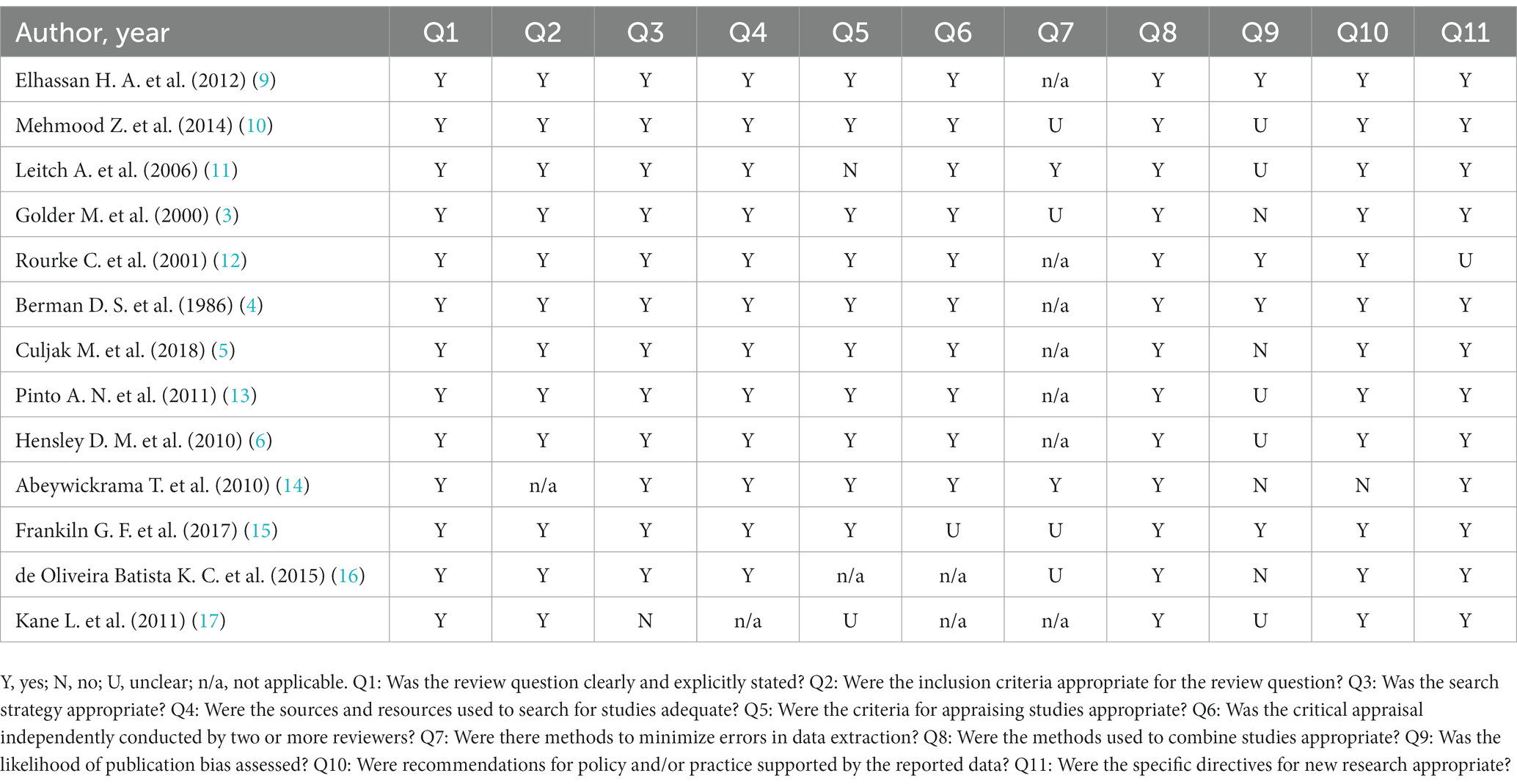
Table 1. Critical appraisal results for included studies.
Results
A total of 291 articles were found in the scientific databases. After removing duplicates, 56 papers remained for analysis. Then, 51 full-text articles were retained after reviewing abstracts. The next step focused on inclusion and exclusion criteria (38 were rejected). At the stage of qualitative text analysis, four articles were rejected. Finally, 13 articles were accepted for systematic analysis (Figure 1).
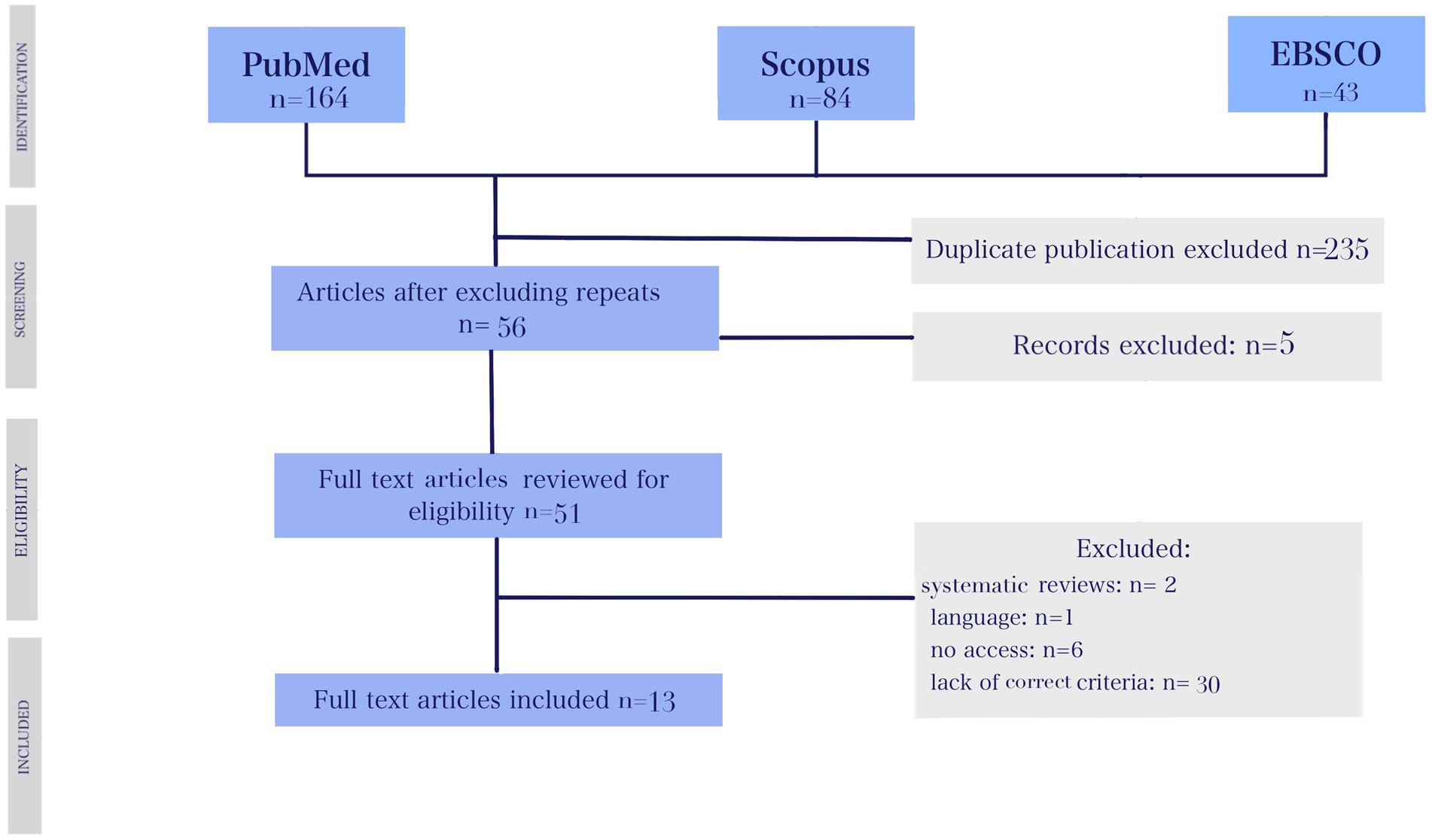
Figure 1. PRISMA flow diagram.
Some limitations need to be highlighted, such as limited observations due to the number of samples taken and the fact that there was no methodological correlation with regard to nosocomial infections caused by contaminated tourniquets.
The included studies were conducted between 1986 and 2018 in countries such as the United Kingdom, the United States, Canada, and Pakistan. The proportional observation based on the number sampled median was 77. The genus MRSA was the type of bacteria most commonly found: on 12% of all tested tourniquets, with the median of MRSA amounting to 8.5%. The amount of MRSA found on tourniquets was mean ± SD 14.6 ± 45.89. A review of studies also revealed the presence of coagulase-negative staphylococci, grew Bacillus, and Staphylococcus aureus.
A synthesis of the qualitative results of the review of the literature on reusable compression tourniquets in the field of MRO is presented in Table 2.
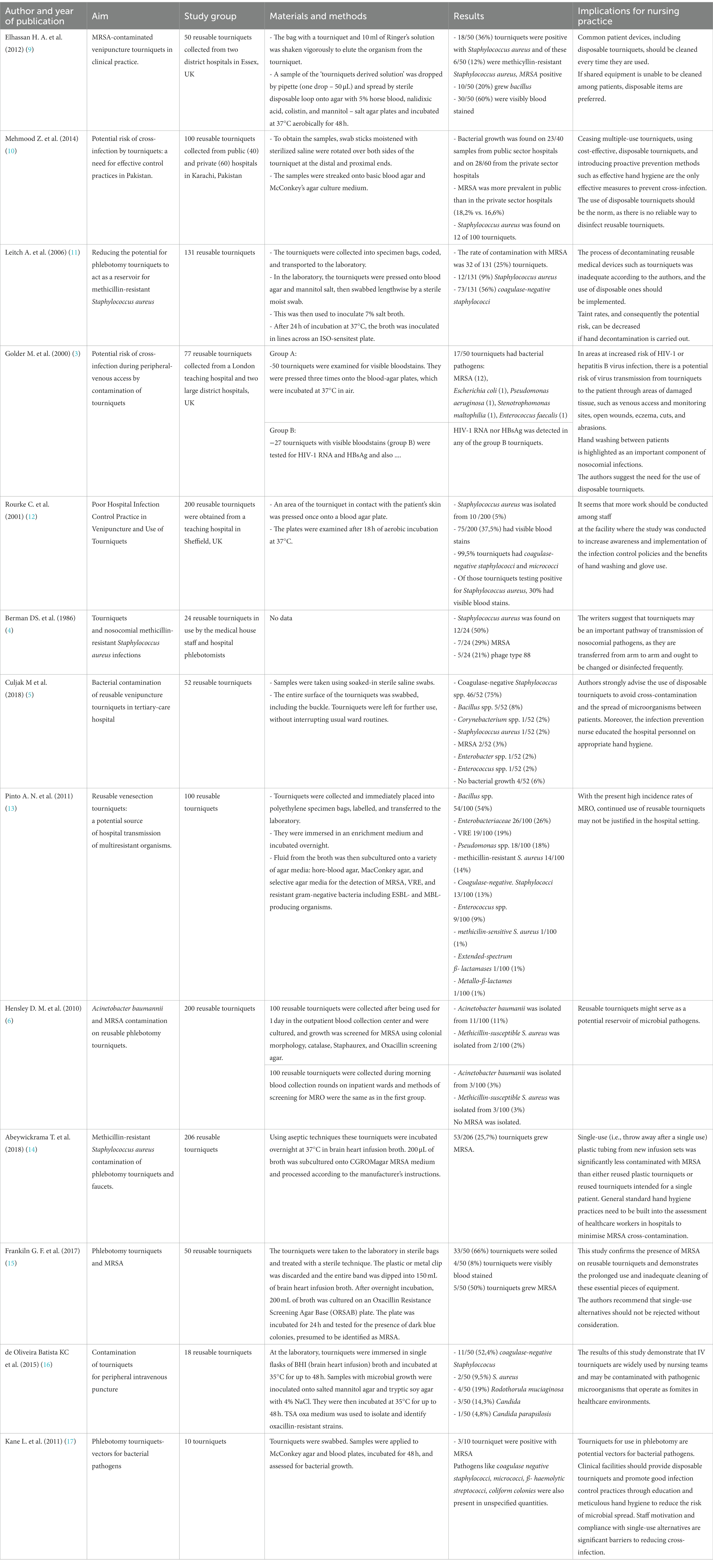
Table 2. Synthesis of qualitative results of literature review relating to reusable tourniquets in the field of MRO.
Discussion
This systematic review of 13 articles summarized the evidence from basic research, epidemiological, and clinical treatment studies of the association between MROs and the use of reusable tourniquets by medical personnel. A previously published research by Pinto et al. primarily focused on the highest rates of multi-resistant organisms in single-patient tourniquets used in intensive care units. In this systematic review, we describe basic research studies on every type of ward in a hospital (13). Evidence suggests that reusable tourniquets may serve as a potential reservoir of bacterial microorganisms in a diverse range of healthcare settings (6, 9). Using disposable tourniquets in hospitals is unpopular; this may be due to the convenience of staff using reusable stasis and a matter of habit. In the study conducted by Grohmann et al., it was shown that there was significantly less bacteria on silicone than on conventional tourniquets. The use of a silicone tourniquet is a more secure, sustainable, and economical alternative to tourniquets made of other materials (1). It is also worth considering if the longer time a patient stays in hospital due to several infections caused by pathogens is better than using disposable tourniquets, which may prevent the spread of infections. Hospital-acquired infections can lead to increased length of stay and higher costs (18). According to US estimates, the cost of a single episode of MRSA bacteraemia is US$26,446, meaning that one episode corresponds to the cost of at least 130,000 disposable tourniquets, considering that a disposable tourniquet costs £ 0.07, according to UK cost estimates quoted by Leitch et al. (11, 19). It is also interesting to explore if pathogens from tourniquets may contribute to infections within the IV. Disposable tourniquets are ideal, but as long as reusable tourniquets are used for various reasons, adequate infection prevention is required. Kerstain et al. recommended the use of disposable tourniquets, claiming that, taking into account the cost of hospital-acquired infections and the length of time a patient stays in the hospital due to infection, it is more cost-effective to reduce infection transmission to patients by the use of disposable tourniquets (20). Contamination of tourniquets depends on the hospital as a whole. Poor hygiene in combination with the careless use of tourniquets makes them a source of hospital-acquired infections. (2). Kerstain et al. found that disposable tourniquets are favored by patients and phlebotomists for their convenience and practicality (20). Using single-use devices for blood sampling and drawing is proposed by the WHO Guidelines on Drawing Blood: Best Practices in Phlebotomy (7). Compression tourniquets, as nursing medical devices, should be stored and managed with greater care to limit negative effects on patients. Steps to be taken should include adopting protocols, educating staff, and providing stasis disinfection between uses (21). A study by Schauer et al. demonstrated that the quantitative risk of reusable tourniquets appears to be low using standard infection control practices (22). Regular supervision and rules for sterilization or disinfection of tourniquets are advised in the Infection Control program to reduce hospital-acquired infections. (23).
National guidance on the use and cleaning of venipuncture tourniquets is recommended (24).
Limitations
Some important scientific research was left out of the search and selection process due to the nature of the publication date (research since 1986) and language (English). Tests have been carried out in different regions, so the cultural aspect and general hospital policy environment in the country should be taken into account. It is necessary to mention the methodological limitations of the systematic review, including inherent biases that include selection, different quantitative sampling based on unspecified reusable tourniquet methods, various locations for collecting materials, miscellaneous infection control policies in medical facilities, and effective enforcement of glove and hand hygiene. Furthermore, internal validity was achieved in this study as there was no bias in the study design, analysis, and how the study was conducted. To ensure the internal validity of the study, the selection of tourniquets was randomized and we followed specific procedures during the study. There were limitations in that generalization to external validation was not possible.
Conclusion
Patient well-being may be at risk due to the high level of proportional observation based on the number of sampled contamination of reusable tourniquets. The micro-organisms responsible for this contamination belong to different species, the most common being the genus Staphylococcus. For this reason, we suggest the use of disposable tourniquets.
Implications for practice
The review identified weaknesses in the use of reusable tourniquets in medical settings. Safely collecting blood using tourniquets that will not threaten the patient’s safety should be a priority even if it is challenging for medical facilities, which should focus on the adoption of clear rules of conduct. In practice, more emphasis should be placed on monitoring the epidemiological status of reusable tourniquets in medical facilities.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
Author contributions
JS: Conceptualization, Data curation, Formal analysis, Software, Writing – original draft. MM: Conceptualization, Data curation, Writing – original draft. WM-D: Conceptualization, Methodology, Visualization, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. The publication fee was financed by the Medical University of Gdańsk from the “Excellence Initiative - Research University” Program.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Author’s Note
The article was written as part of the Journal Club Nursing project at the Medical University of Gdańsk.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Footnotes
References
1. Grohmann, M, Schomakers, L, Wolschendorf, F, Grosch, J, Lindner, S, and Witte, AK. Reduced bacterial contamination rates detected on silicone tourniquets compared to conventional tourniquets in clinical routine. BMC Infect Dis. (2020) 20:247. doi: 10.1186/s12879-020-04975-y
2. Salgueiro-Oliveira, A, Oliveira, V, Costa, P, Gama, F, Graveto, J, Parreira, P, et al. Tourniquets used in peripheral venipuncture as a potential vehicle for transmission of microorganisms: scoping review. Infectio. (2020) 24:92–7. doi: 10.22354/in.v24i2.839
3. Golder, M, Chan, CL, O'Shea, S, Corbett, K, Chrystie, IL, and French, G. Potential risk of cross-infection during peripheral-venous access by contamination of tourniquets. Lancet. (2000) 355:44. doi: 10.1016/s0140-6736(99)04051-9
4. Berman, DS, Schaefler, S, Simberkoff, MS, and Rahal, JJ. Tourniquets and nosocomial methicillin-resistant Staphylococcus aureus infections. N Engl J Med. (1986) 315:514–5. doi: 10.1056/NEJM198608213150812
5. Culjak, M, Gveric Grginic, A, and Simundic, AM. Bacterial contamination of reusable venipuncture tourniquets in tertiary-care hospital. Clin Chem Lab Med. (2018) 56:e201–3. doi: 10.1515/cclm-2017-0994
6. Hensley, DM, Krauland, KJ, and McGlasson, DL. Acinetobacter baumannii and MRSA contamination on reusable phlebotomy tourniquets. Clin Lab Sci. (2010) 23:151–6. doi: 10.29074/ascls.23.3.151
7. Dhingra, N, and Diepart, M. WHO guidelines on drawing blood: Best practices in phlebotomy. Available at: https://www.who.int/publications/i/item/9789241599221 (Accessed May 15, 2023).
8. Aromataris, E, Fernandez, R, Godfrey, C, Holly, C, Khalil, H, and Tungpunkom, P. The Joanna Briggs institute reviewers’ manual 2014 methodology for JBI umbrella reviews. The Joanna Briggs Institute: Adelaide, Australia (2014).
9. Elhassan, HA, and Dixon, T. MRSA contaminated venepuncture tourniquets in clinical practice. Postgrad Med J. (2012) 88:194–7. doi: 10.1136/postgradmedj-2011-130411
10. Mehmood, Z, Mubeen, SM, Afzal, MS, and Hussain, Z. Potential risk of cross-infection by tourniquets: a need for effective control practices in Pakistan. Int J Prev Med. (2014) 5:1119–24.
11. Leitch, A, McCormick, I, Gunn, I, and Gillespie, T. Reducing the potential for phlebotomy tourniquets to act as a reservoir for meticillin-resistant Staphylococcus aureus. J Hosp Infect. (2006) 63:428–31. doi: 10.1016/j.jhin.2006.03.006
12. Rourke, C, Bates, C, and Read, RC. Poor hospital infection control practice in Venepuncture and use of tourniquets. J Hosp Infect. (2001) 49:59–61. doi: 10.1053/jhin.2001.1038
13. Pinto, AN, Phan, T, Sala, G, Cheong, EY, Siarakas, S, and Gottlieb, T. Reusable venesection tourniquets: a potential source of hospital transmission of multiresistant organisms. Med J Aust. (2011) 195:276–9. doi: 10.5694/mja11.10333
14. Abeywickrama, T, Amarasinghe, K, Wijerathne, S, Dharmaratne, C, Fernando, D, Senaratna, BC, et al. Methicillin resistant Staphylococcus aureus contamination of phlebotomy tourniquets and faucets. Ceylon Med J. (2018) 63:5–10. doi: 10.4038/cmj.v63i1.8627
15. Franklin, GF, Bal, AM, and McKenzie, H. Phlebotomy tourniquets and MRSA. J Hosp Infect. (2007) 65:173–5. doi: 10.1016/j.jhin.2006.10.010
16. Batista, KCO, Tipple, AFV, Leão-Vasconcelos, LSNO, Ribeiro, EL, and Prado, MA. Contamination of tourniquets for peripheral intravenous puncture. Acta Paulista Enfermagem. (2015) 28:426–32. doi: 10.1590/1982-0194201500072
17. Kane, L, and Krischock, L. Lucas C phlebotomy tourniquets- vectors for bacterial pathogens. Arch Dis Child. (2011) 96:A47–8. doi: 10.1136/adc.2011.212563.105
18. Spelman, DW. 2: hospital acquired infection. Med J Aust. (2002) 176:286–91. doi: 10.5694/j.1326-5377.2002.tb04412.x
19. Abramson, MA, and Sexton, DJ. Nosocomial methicillin-resistant and methicillin-susceptible Staphylococcus aureus primary bacteremia: at what costs? Infect Control Hosp Epidemiol. (1999) 20:408–11. doi: 10.1086/501641
20. Kerstain, R, and Fellowes, C. Novel fit for purpose single use tourniquet: best of both worlds. J Med Eng Technol. (2009) 33:475–80. doi: 10.1080/03091900902952667
21. Pădureţ, G, Primosa, F, Bujdos, MJ, Artioli, G, Sarli, L, La Sala, R, et al. The nursing Management of Tourniquet: the infective risk related to its use. Acta Biomed. (2021) 92:e2021361. doi: 10.23750/abm.v92iS2.12190
22. Schauer, CK, and Hammer, DA. Quantifying patient bacterial exposure risk from reusable phlebotomy tourniquets in a New Zealand secondary level hospital. J Infect Prev. (2015) 16:262–5. doi: 10.1177/1757177415600242
23. Kalyani, CS, Koripella, R, and Valli, SKN. Isolation of potentially pathogenic Bacteria from reusable venesection tourniquets in a tertiary care hospital. Int JCurrMicrobiolAppSci. (2016) 5:153–7. doi: 10.20546/ijcmas.2016.505.016
Keywords: tourniquet, cross infection, nosocomial infection, Staphylococcus aureus, MRO, pathogen, infectious disease
Citation: Szymczyk J, Månsson M and Mędrzycka-Dąbrowska W (2023) Reusable tourniquets for blood sampling as a source of multi-resistant organisms– a systematic review. Front. Public Health. 11:1258692. doi: 10.3389/fpubh.2023.1258692
Edited by:
Huiyin Tu, University of Nebraska Medical Center, United StatesReviewed by:
Paul Kwon, Walter Reed Army Institute of Research, United StatesAnthony Evans, University of Nebraska Medical Center, United States
Copyright © 2023 Szymczyk, Månsson and Mędrzycka-Dąbrowska. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Wioletta Mędrzycka-Dąbrowska, d2lvbGV0dGEubWVkcnp5Y2thQGd1bWVkLmVkdS5wbA==